
When Is A Colonoscopy Not a Colonoscopy Dr Linus Chang Gastroenterologist.
Dr Alex di MambroConsultant Gastroenterologist
Clinical Lead for NutritionGHNHSFT
Where does it hurt?
Acute appendicitis Acute pancreatitis Peptic ulcer Gastroenteritis Hepatitis Bowel obstruction Bowel perforation Herniation Meckel diverticulitis Toxic megacolon Pancreatic pseudocyst Ruptured ectopic pregnancy Septic abortion with peritonitis Acute urinary retention due to retroverted
gravid uterus Adnexal torsion Ureteral calculus Rupture of renal pelvis Ureteral obstruction Superior mesenteric artery syndrome Thrombosis/infarction (specifically, mesenteric
venous thrombosis ) Ruptured visceral artery aneurysm Splenic artery aneurysm
Pneumonia
Pulmonary embolism
Intraperitoneal haemorrhage
Splenic rupture
Abdominal trauma
Acute intermittent porphyria
Diabetic ketoacidosis
Sickle cell disease
Acute pyelonephritis
Acute cystitis
Acute cholecystitis
Acute fatty liver of pregnancy
Rupture of the rectus abdominis
Torsion of the pregnant uterus
Red degeneration of myoma
Torsion of pedunculated myoma
Placental abruption
Placenta percreta
HELLP (haemolysis, elevated liver function, and low platelets) syndrome - spontaneous rupture of the liver
Uterine rupture
Chorioamnionitis
IBSUTIConstipationGastroenteritis
In IBS patients, heightened abdominal pain sensation is observed at the time of low ovarian hormone concentrations
Oestrogens modulate peripheral and central nociceptive pathways
5-HT ? contribute to gender differences in pain-related IBS symptoms via modulation of gut sensitivity
Female IBS patients present higher activity of brain structures involved in emotional processing of pain sensation (i.e., insula, cingulate cortex and amygdala) and greater connectivity between brain structures involved in cortical control (i.e., prefrontal cortex).
Frequent association between hormonal changes during pregnancy and the co-occurrence of GI motility disorders.
GI transit time is significantly prolonged in the third trimester of pregnancy when ovarian hormone levels are increased, compared to the postpartum period.
Although mechanical causes inherent pregnancy can account for bowel habit disturbances, endocrinological changes are also accountable causes of GI motor impairments
Increase in the release of NO in the vascular compartment and from the non-adrenergic, non-cholinergic nerves, innervating the proximal colon, during late pregnancy compared with mid-pregnancy.
This NO increase could be responsible for motility decrease in the GI tract and is thought to be mediated by oestradiol
Inhibitory effects of oestrogen on colonic contractile activity have been confirmed in isolated rabbit distal colon - potentiates the inhibitory effects of oxytocin on distal colonic contraction.
Interestingly, oestradiol had no effects on the oxytocin-induced decrease in motility in the proximal colon, suggesting a fine regulation of intestinal motility by ovarian hormones depending on GI segments.
ORα and ORβ have been identified in the GI tract, where ORβ is preferentially expressed on colon epithelial cells.
Oestrogen functions in the gut: development and regulation of gut barrier, cell differentiation and proliferation, architectural maintenance of the intestinal epithelium. ORs have been implicated in chloride ion secretion Nutrient transluminal transport. Indirect evidence from contraceptive use, pregnancy, and
hormone replacement therapy in patients with gut barrier mediated pathologies such as IBD, show that fluctuations in ovarian hormone levels influence the course of and the risk for these diseases
?Ovarian hormones modulate gut permeability –increased interest in gut barrier integrity
T cell function is particularly affected by hormonal regulation since both oestrogen and progesterone enhance their cytotoxic activity by stimulating reactive oxygen species production.
In mast cells, progesterone inhibits histamine secretion: ?explain the partial remission in certain inflammatory
conditions during pregnancy when progesterone levels are high.
In contrast, mast cells express high affinity oestrogen receptors and their activation by oestradiol has been shown to potentiate histamine and serotonin secretions in mast cells
IBS is predominantly diagnosed in women, with a female to male sex ratio ranging from 2:1 (questionnaire-based diagnostics) to 4:1 (practice-based diagnostics).
Many if not all the comorbid diseases associated with IBS also share this female predominance. migraine, other functional GI disorders such as functional
dyspepsia, chronic pelvic pain, chronic fatigue syndrome, Depression fibromyalgia
Amitriptyline is not used
No RCTs on mebeverine use in pregnancy
Anticholinergics/antispasmodics are not recommended
Simple pain relief (paracetamol)
Fibre
Bulk forming laxatives
Dietary manipulation
nd
olyols
Monosaccharides
Di-
Oligo-
Fermentable
A
P
Fructans,
Lactose
Fructose
E.g. Sorbitol
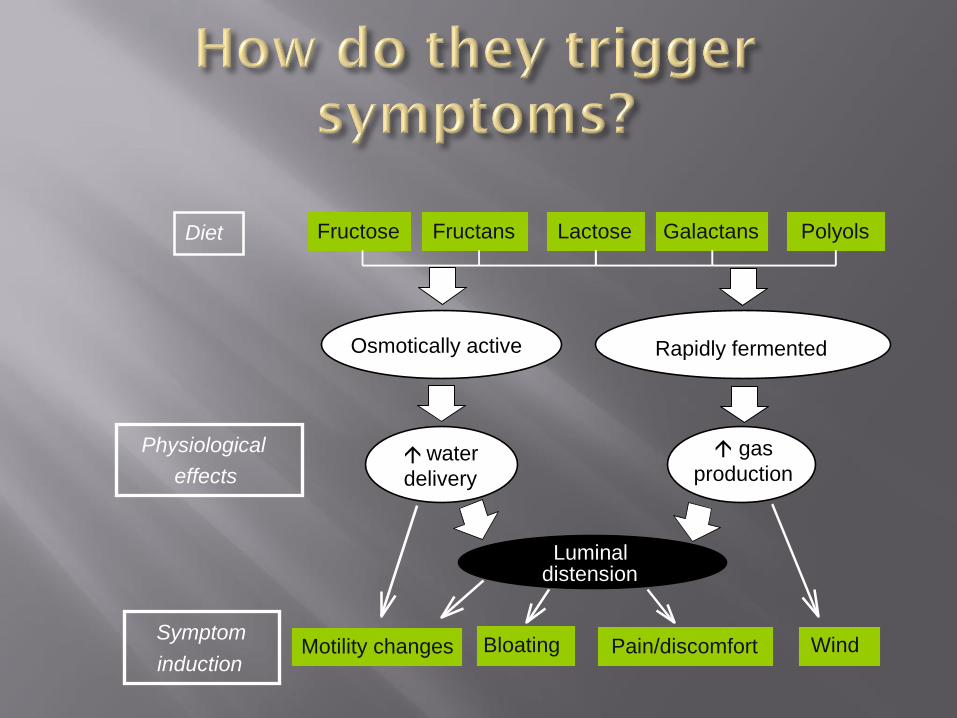
Motility changes Bloating Pain/discomfort WindSymptom
induction
Luminal distension
Fructose Fructans Lactose Galactans PolyolsDiet
Osmotically active Rapidly fermented
water
delivery
Physiological
effects
gas
production
No RCTs in FODMAP diet in pregnancy
They do not advocate the use of the FODMAP diet in pregnancy for that reason
However….referral to a dietician for consideration of dietary manipulation to help manage ROME criteria IBS in pregnancy should be considered.
Safe, supervised, sensible
Probiotics – one small trial looking at effect of combined probiotic in constipation predominant IBS in pregnancy – benefit and safe
Ecologic®Relief (Bifidobacterium bifidum, Bifidobacterium lactis, Bifidobacterium longumW108, Lactobacillus casei, Lactobacillus plantarum and Lactobacillus rhamnosus).
Extensive physiological, biochemical and dietary changes occur during pregnancy.
The body secretes a large amount of progesterone which causes decreased muscle tone and lower motility of the gastrointestinal tract.
As the uterus grows during the third trimester of pregnancy, especially after the foetal head becomes engaged in the pelvis, the lower part of the gastrointestinal tract and rectum become compressed
Pregnant women have an increased protein and fat intake in comparison with vegetable intake.
Many heavily pregnant women have a reduced activity level –
decrease gastrointestinal digestion activity
bloating
constipation .
ALT decreases - lowest levels just before delivery
AST remains stable.
Albumin declines = haemodilution,
Alkaline phosphate increases due to production of placental alkaline phosphatase
Creatinine decreases
Ferritin as well as GGT decreases
Triglycerides, TSH, urea, iron and transferrin increases.
TSH values during pregnancy are more than 50% higher than the postpartum values (measured upto 45 days post partum)
TSH increase, especially during the last trimester, is a response to the increased metabolic demands of the growing foetus
A Larsson et al; Reference values for clinical chemistry tests during normal pregnancy. BJOG. Volume 115, Issue 7 June 2008 Pages 874–881
First trimester: normal reference range (CRP <5)
Second trimester: CRP 5-20
Third trimester: CRP normal upto 8-10
Interpretation of results is dependent on clinical presentation
Confounded by other factors: high protein diet, smoking, obesity, hypertriglyceridaemia, diabetes
Plasma volume increases up to 50% by term.
Red cell volume also increases
Erythropoietin production increases, but not enough to prevent a dilutional anaemia occurring.
There is a 15% drop in haemoglobin.
The platelet count remains normal although there is an increase in turnover.
There is a steady rise in white cell count peaking during labour.
Glomerular filtration rate increases by up to 50% in pregnancy
The clearance of urea, uric acid and creatinine all increase
Plasma concentrations are lower in pregnancy.
BP: Diastolic pressure may fall as much as 20 % and systolic by around 8 %
Cardiac output increases from 5 weeks after conception
increased stroke volume
increased heart rate
decrease in total peripheral resistance.
cardiac output is increased by approximately 40% at the end of the first trimester
ECG – a reflection of changes in cardiac output
left axis deviation
ST segment depression
T wave flattening.
Blood flow to the uterus increases to about 700ml/min by term.
Blood flow to the kidneys and skin increase
Blood flow to the brain and liver remain unaltered.
Hyperventilation occurs due to an increase in tidal volume (40%) and a lesser increase in respiratory rate (15%).
Slight drop in the partial pressure of carbon dioxide (to approximately 32 mmHg or 4.3 kPa) resulting in a mild respiratory alkalosis (pH 7.44)
Both the metabolic demands of the foetus and the increased work of breathing result in an increased oxygen consumption (up to 60 % during labour).
Swedish population-based cohort study 3052 pregnancies exposed to endoscopy (2025 upper
endoscopies, 1109 lower endoscopies, and 58 ERCP) Outcomes (preterm birth, stillbirth, small for gestational age,
or congenital malformations). Secondary outcome measures: induction of labour, low birth
weight (<2500 g), caesarean section, Apgar score <7 at 5 minutes, and neonatal death within 28 days
Endoscopy during pregnancy to be associated with increased risk of preterm birth or small for gestational age, but not of congenital malformation or stillbirth ?due to familial factors or disease activity.
Ludvigsson JF et al; Outcomes of Pregnancies for Women Undergoing Endoscopy While They Were Pregnant: A Nationwide Cohort StudyGastroenterology. 2017 Feb;152(3):554-563
46 pregnant women with and 21 without IBD in Denmark, Australia, and New Zealand. Demographics, clinical parameters, and HBI/SCCAI were recorded.
Stool and blood samples were obtained to determine FC and CRP concentrations.
Julsgaard M et al; Faecal Calprotectin Is Not Affected by Pregnancy: Clinical Implications for the Management of Pregnant Patients with Inflammatory Bowel Disease. Inflamm Bowel Dis. 2017 Jul;23(7):1240-1246
The physiological changes that occur during pregnancy do not affect FC
The combined use of FC and Physician Global Assessment seems optimal to assess disease activity in IBD during pregnancy.
Organogenesis occurs predominantly between 2 and 15 weeks gestation:
microcephaly,
microphthalmia,
mental retardation,
growth retardation,
behavioral defects,
cataracts.
Teratogenic effects are extremely unlikely in foetuses before 2 weeks of gestation and after 15 weeks of gestation
If the abdomen or pelvis is not being imaged, such as in chest or head CT, then there is no risk to the baby.
If the CT scan includes the abdomen or pelvis, then there may be a slight risk to the baby. An unborn baby exposed to CT during pregnancy may have a one in 1,000 greater chance of developing a cancer as a child.
CT contrast material does cross the placenta; however, it has been used in pregnancy for decades without harm
Abdominal radiograph = 0.25
Intravenous pyelogram = 0.8
Lumbar spine radiographs = 0.6
CT pelvis = 1-10
Note: 1 rad = 1 cGy = 10 mGy = 10,000 µGy
Odds of dying of childhood cancer go from 1 in 2000 (baseline) to 2 in 2000 (after 5 rads).
The excess risk (of 1 in 2000) is equivalent to driving 20,000 miles in a car or living in New York City for 3 years
1.Hammer-Jacobsen E. Therapeutic abortion on account of x-ray examination during pregnancy. Danish Med Bull 1959; 6: 113-122.
2.Hall EJ. Radiobiology for the radiologist, 4th ed. Philadelphia: Lippincott; 1994: 363-452.
3.Wagner LK, Archer BR, Zeck OF. Conceptus dose from two state-of-the-art CT scanners. Radiology 1986; 159: 787-792.
4.Bushberg JT, Seibert JA, Leidholdt EM, Boone JM. The essential physics of medical imaging. Williams and Wilkins, Baltimore, 1994; 694.
Ray JG et al. JAMA. 2016;316(9):952-961) states, "Exposure to MRI during the first trimester of pregnancy compared with nonexposure was not associated with increased risk of harm to the foetus or in early childhood. Gadolinium MRI at any time during pregnancy was associated with an increased risk of a broad set of rheumatological, inflammatory, or infiltrative skin conditions and for stillbirth or neonatal death.”
Acute appendicitis complicates approximately 1 in 1500 pregnancies, and is one of the leading indications for surgery in pregnancy
The diagnosis of appendicitis in pregnancy can be clinically difficult, particularly in later pregnancy, as evidenced by a perforation rate of 31% for appendicitis occurring in the first and second trimester but rising to 69% in the third trimester
1.Wittich AC, DeSantis RA, Lockrow EG. Appendectomy during pregnancy: a survey of two army medical activities. Mil Med 1999; 164: 671-674.
2.Weingold AB. Appendicitis in pregnancy. Clin Obstet Gynecol 1983; 26: 801-809. 3.Lim HK, Bae SH, Seo GS. Diagnosis of acute appendicitis in pregnant women: Value of
sonography. Am J Roentgenol. 1992; 159:539-542. 4.Castro MA, Shipp TD, Castro EE, et al. The use of helical computed tomography in
pregnancy for the diagnosis of acute appendicitis. Am J Obstet Gynecol. 2001; 184:954-957.
5.Cobben LP, Groot I, Haans L, Blickman JG,Puylaert J. MRI for clinically suspected appendicitis during pregnancy. AJR 2004; 183: 671-675.
Obstructive urinary calculi complicate approximately 1 in 3300 pregnancies.
Imaging is complicated by the normal physiological hydronephrosis that occurs in pregnancy.
Despite this confounding factor, ultrasound correctly visualized 21 of 35 (60%) stones in a retrospective study. This suggests ultrasound remains the initial study of choice
1.Butler EL, Cox SM, Eberts EG, Cunningham FG. Symptomatic nephrolithiasis complicating pregnancy. Obstet Gynecol 2000 96: 753-756.
2.Tamm EP, Silverman PM, Shuman WP. Evaluation of the patient with flank pain and possible ureteral calculus. Radiology 2003; 228: 319-29.
Pregnancy is lithogenic
Secretion of bile with increased amounts of cholesterol and decreased amounts of chenodeoxycholic acid
Gallbladder stasis
The prevalence of:
biliary sludge 31%
develop new gallstones 2%
biliary pancreatitis 2-11% (1:10000)
Hydration
Narcotics
Antibiotics
Dietary modifications.
Endoscopic retrograde cholangiopancreatography (ERCP) may be needed in cases of cholangitis, biliary obstruction, or pancreatitis.
Laparoscopy safest in 2nd trimester
Abdominal pain in pregnancy is common
GP referral to rapid access pregnancy clinics provide reassurance and early diagnosis in obstetric causes for abdominal pain
Common surgical complaints such as appendicitis, cholecystitis and renal colic are more common in pregnancy
Early recognition and judicious use of investigations lead to better outcomes for both the mother and child
Good baseline knowledge of the physiological, anatomical and serological changes in pregnancy is necessary
Lifestyle changes, dietary manipulation and laxatives remain the main form of treatment for IBS/constipation
Multi-disciplinay team approach

SAFE
SENSIBLE
SUPPORTED
13.01% higher than among the general population 6.00% (Shanghi series)
Pregnant women >35 years old have special considerations for pregnancy with the decline of physiology and degeneration of the pelvis and ligaments, the risk of gestational diabetes, high blood pressure, miscarriage and other complications increased
Prevalence of constipation in pregnancy is 11-38%
Mostly during the third trimester, can also be present from 12 weeks gestation
Caesarean section rate in pregnant women with functional constipation (66.97%) was higher than in the other methods of delivery (27.29%)
Postpartum haemorrhoids in women in the constipation group was higher than in the non-constipation group (23.52% and 13.40%, respectively)
Stimulant laxatives (senna 14 mg/day or dioctyl sodium succinate 120 mg plus dihydroxyanthroquinone 100 mg once daily),
Two arms assessed the effects of bulk-forming laxatives (60% sterculia plus 8% frangula [10 mL once daily] or 60% sterculia [10 mL once daily]).
No RCTs.
polyethylene glycol (PEG)-based osmotic laxatives plus electrolytes (PEG+E) may be the ideal laxative for use in pregnancy because absorption is minimal
No evidence of teratogenicity in animal
Insufficient data about the potential effects of PEG+E on the foetus.
Insufficient evidence about the effects of PEG+E on constipation during pregnancy, and its use cannot therefore be recommended.
No RCTs.
There is limited evidence of benefit for stimulant laxatives compared with bulk-forming laxatives.
Adverse effects profile of stimulant laxatives (abdominal pain and diarrhoea)
High absolute rates of unacceptable adverse effects both with stimulant laxatives and bulk-forming laxatives in pregnant women
Prevalence of gastroesophageal reflux disease (GORD) in pregnancy is up to 80%, with a maximum peak during the third trimester
RCT (50 women with heartburn), which compared three interventions for 7 days: magnesium hydroxide plus aluminium hydroxide (antacid) plus oxethazaine; magnesium hydroxide plus aluminium hydroxide without oxethazaine; and placebo. The RCT found that antacid with or without oxethazaine both produced similar relief from heartburn, and increased heartburn relief compared with placebo, although the improved relief was of borderline significance
1186 infants had been exposed to PPIs during the first trimester of pregnancy.
Exposure to PPIs was not associated with an increased risk of congenital malformations (adjusted OR 1.06; 95% CI = 0.84-1.33).
1148 infants were exposed to H(2)-blockers during the first trimester of pregnancy
Exposure to H(2)-blockers was not associated with congenital birth defects, perinatal mortality, premature delivery, low birth weight, or low Apgar scores.
Matok I et al; The safety of H(2)-blockers use during pregnancy. J Clin Pharmacol. 2010 Jan;50(1):81-7
Matok I et al; The safety of foetal exposure to proton-pump inhibitors during pregnancy. Dig Dis Sci. 2012 Mar;57(3):699-705
In pregnant women, H2 receptor antagonists can be combined with alginate antacids when symptoms persist.
Review. BMJ Clin Evid. 2008: 1411;Juan C Vazquez


















