Downs Syndrome Diagnostic and Patient Care Pathways · Web viewDiagnostic and Patient Care Pathways...
43
Combined Child Health Service Down’s Syndrome Diagnostic and Patient Care Pathways Diagnosis to School Leaver November 2008
Transcript of Downs Syndrome Diagnostic and Patient Care Pathways · Web viewDiagnostic and Patient Care Pathways...

Combined Child Health Service
Down’s Syndrome
Diagnostic and Patient Care Pathways
Diagnosis to School Leaver
November 2008

Combined Child Health Service
Table of Contents
Pathway 1........................................................................................................1Antenatal Screening............................................................................1Guidance on use of Antenatal Screening Pathway..........................2
Blood Test...................................................................................2Diagnostic Test...........................................................................2Combined Ultrasound and Biochemical (CUB) Screening..........3
Pathway 2........................................................................................................4Diagnostic Pathway.............................................................................4
Pathway 3........................................................................................................5Pre-School Patient Care Pathway......................................................5Guidance on the use of Pre-School Down’s Syndrome Diagnostic and Patient Care Pathway...................................................................6
Antenatal Screening and Testing................................................6Down’s Syndrome.......................................................................6Types of Down’s Syndrome........................................................6Physical features associated with Down’s Syndrome.................6Birth of Baby...............................................................................8Information for Parents................................................................9Neonatal Medical Assessment by Paediatrician.......................11Primary Health Care Team.......................................................11Universal Child Health Screening.............................................11Social Work Department...........................................................12Management by Specialist Services.........................................12Refer to Child Development Service.........................................13Developmental Assessment......................................................14Education..................................................................................15Joint Assessment of Needs / Integrated Assessment...............15Individual Educational Plan/ Co-ordinated Support Plan...........16Key worker................................................................................16Regular Review.........................................................................16
Pathway 4......................................................................................................17School Aged Patient Care Pathway.................................................17Guidance on the use of School Age Down’s Syndrome Patient Care Pathway.....................................................................................18
Health........................................................................................18Universal Child Health Screening.............................................19
November 2008

Combined Child Health Service
Social Work...............................................................................19Education..................................................................................19Joint Assessment of Needs / Integrated Assessment...............20Individual Educational Plan / Co-ordinated Support Plan..........20Key worker................................................................................21Review......................................................................................21Transfer to Adult Services.........................................................21
Annex1................................................................................................22Down’s Syndrome – Grampian Schedule of Health Checks.....22
Annex 2...............................................................................................23Down’s Syndrome – Child Development (DSMIG 2000)...........23
References:........................................................................................24Working Group Members.....................................................................25
November 2008

Combined Child Health Service
Pathway 1 Antenatal Screening
November 2008 1
Offer Antenatal Screening for Down’s SyndromeSerum blood test offered at 16 weeks gestation
High Risk :< 1:250Woman informed by letter
Low Risk :> 1:250Woman informed by midwife at
next antenatal appointment
Woman Declines Screening and/or
Diagnostic Tests
Amniocentesis Procedure Carried Out
Down’s Syndrome Karyotype
Positive Diagnosis
Normal KaryotypeNegative Result
Woman chooses termination of pregnancy
Woman Continues PregnancyRoutine Antenatal Surveillance Carried Out
Support of Neonatologist if requested
Birth of BabyPost-natal Examination
Previous baby with Down’s Syndrome
Woman offered CUB screening or diagnostic procedure Chronic Villus Sampling (CVS) at 11-14 weeks gestation orAmniocentesis at 15-16 weeks
Amniocentesis diagnostic procedure
offered
Combined Child Health Service
Guidance on use of Antenatal Screening Pathway
In Scotland all pregnant women are eligible for antenatal screening. Screening tests are not compulsory, they are offered to assist individuals make an informed choice about the health of their unborn baby. The emphasis should be on offering screening and diagnostic tests to women in order to detect where possible any fetal abnormities at an early stage. (NHS Quality Improvement Scotland 2005)
Blood TestAll pregnant women are offered maternal serum screening at 16 weeks of pregnancy. A blood sample is obtained to test for proteins and hormones; these are normally alphafetoprotein (AFP) and human chorionic gonadotrophin (hCG). The level of these proteins and hormones are assessed along with the age of the mother and stage of pregnancy to indicate the ‘risk’ of the baby having Down’s Syndrome.
A low risk result is a risk higher than 1:250 chance of the baby having Down’s syndrome. This does not mean that there is no risk of the baby having Down’s syndrome, it means that it is unlikely.Women in this category will be informed of the result when next seen by the midwife and will not be offered a diagnostic test.
A high risk result is a risk lower than a 1:250 chance of the baby having Down’s syndrome. This does not mean that the baby definitely has Down’s syndrome. Women in this category will be informed by letter and given an appointment to attend the Day Ward to explain and discuss the results and offer further diagnostic testing.
Diagnostic TestThere are two tests available:
Amniocentesis can be performed from 16 weeks of pregnancy. This is when a needle is passed through the woman’s abdomen and into the womb to collect some amniotic fluid which is sent for chromosome karyotyping. There is a 1% risk of miscarriage from this procedure.
Chorionic Villus Sampling (CVS) is performed from 11-14 weeks of pregnancy. This is when cells are taken from the placenta and sent for chromosome karyotyping. In Grampian CVS is available if the women have had a previous child with Down’s Syndrome and have requested an early diagnostic test. There is a 1-2% risk of miscarriage from this procedure.
The rapid test (PCR test) results for Down’s Syndrome take three-five working days and a complete chromosome analysis can take up to three weeks. If Down’s Syndrome is diagnosed this should be discussed fully with the parents and help and advise offered to allow parents to make an informed decision on whether to continue with the pregnancy or terminate the pregnancy.
November 2008 2

Combined Child Health Service
Combined Ultrasound and Biochemical (CUB) ScreeningThis test is available privately in Grampian. It is also offered to women who have had a baby with a previous chromosome problem or if the woman has a multiple pregnancy.The CUB screening test is carried out at 11-14 weeks of pregnancy. This test is a combined nuchal translucency (NT) ultrasound scan and blood test. During the scan the amount of fluid lying under the skin at the back of the baby’s neck is measured. A blood sample is obtained and tested for human chorionic gonadotrophin (hCG) and pregnancy-associated plasma protein (PAPP-A) levels.A computer programme uses these measurements, the size of the baby and the mother’s age to work out a risk of Down’s Syndrome for the baby.
The NHS Antenatal and Newborn Screening Programmes booklet highlights that about a quarter of babies with Down’s syndrome are not detected by screening tests.
November 2008 3

Combined Child Health Service
Pathway 2 Diagnostic Pathway
November 2008 4
Birth of BabyNot Down’s Syndrome
Down’s Syndrome Suspected
Karyotyping carried out with parent’s consent
Normal Karyotype
Negative ResultPositive Result
Definitive Diagnosis of Down’s Syndrome
Information for ParentsVerbal
Relevant websitesDown’s Syndrome, New Parent
Information Packsregarding
Diagnosis, Support and Health Issues
Down’s Syndrome confirmed by Antenatal testing and screening

Combined Child Health Service
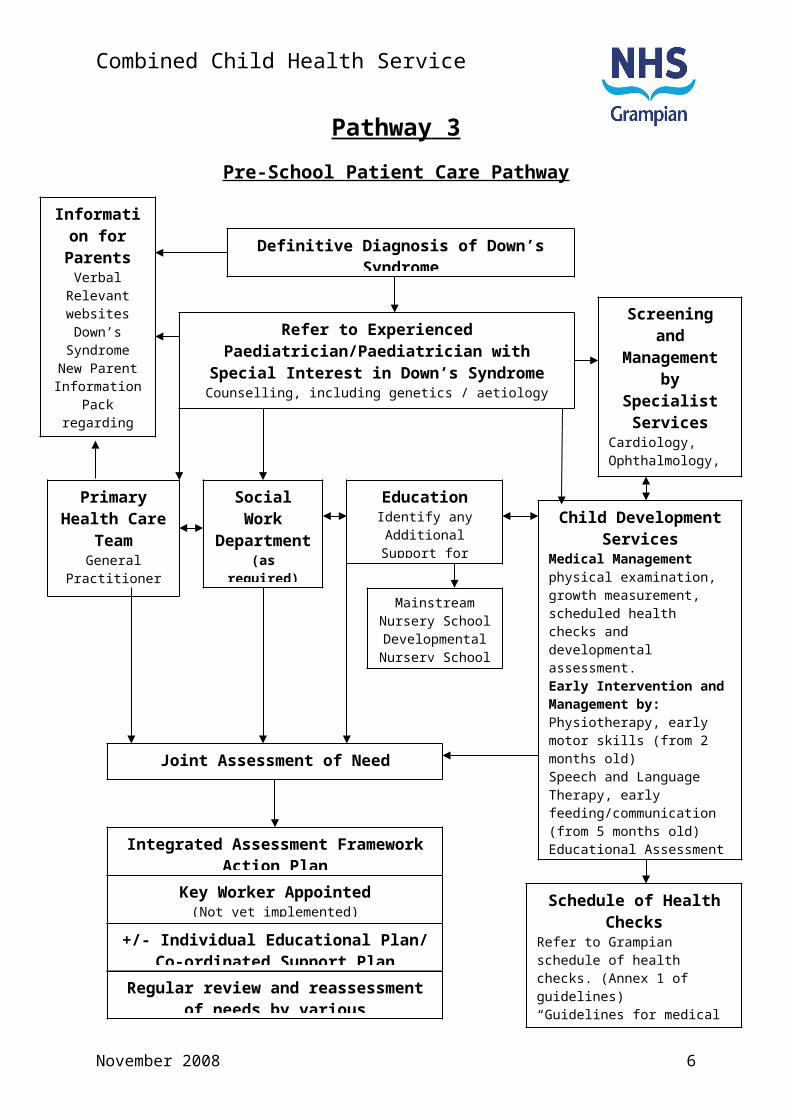
Pathway 3 Pre-School Patient Care Pathway
November 2008 5
Definitive Diagnosis of Down’s SyndromeInformation for Parents
Verbal Relevant websitesDown’s
Syndrome New Parent
Information Pack
regardingDiagnosis,
Support andHealth Issues
Refer to Experienced Paediatrician/Paediatrician with Special Interest in Down’s Syndrome
Counselling, including genetics / aetiology Initial health surveillance carried out as per protocol
Primary Health Care
TeamGeneral
PractitionerHealth Visitor
Social Work Department(as required)Identify Social
Care and Support needs for family.
Screening and Management by
Specialist Services
Cardiology, Ophthalmology, AudiologyOther Specialist Services as required
Child Development Services
Medical Managementphysical examination, growth measurement, scheduled health checks and developmental assessment.Early Intervention and Management by:Physiotherapy, early motor skills (from 2 months old)Speech and Language Therapy, early feeding/communication(from 5 months old)Educational Assessment (refer 2-2½ years old)Occupational Therapy, Clinical Psychology (if indicated)
Joint Assessment of Need
Integrated Assessment Framework Action Plan
Key Worker Appointed(Not yet implemented)
+/- Individual Educational Plan/Co-ordinated Support Plan
Regular review and reassessment of needs by various professionals involved
Schedule of Health Checks
Refer to Grampian schedule of health checks. (Annex 1 of guidelines)“Guidelines for medical Surveillance” (www.dsmig.org.uk)
EducationIdentify any Additional Support for Learning
Needs.
Mainstream Nursery SchoolDevelopmental Nursery School
Combined Child Health Service
Guidance on the use of Pre-School Down’s Syndrome Diagnostic and Patient Care Pathway
Antenatal Screening and TestingIn Scotland all pregnant women are eligible for antenatal screening. Screening tests are not compulsory. They are offered to assist individuals make an informed choice about the health of their unborn baby. The emphasis should be on offering screening and diagnostic tests to women in order to detect where possible any fetal abnormities at an early stage. (NHS Quality Improvement Scotland 2005)
Down’s Syndrome Down’s Syndrome (Trisomy 21) is a genetic condition caused by an extra chromosome 21 appearing in each of the body’s cells i.e. there are three copies of chromosome 21 instead of two. It is the most common identifiable cause of learning disability; with a current incidence in UK of 0.9/1000 live births.Children with Down’s Syndrome have some degree of learning disability, and a characteristic range of physical features. A wide range of health problems are associated with the syndrome so children should have a variety of extra screening tests and health checks to ensure problems are identified and treated as quickly as possible. There is a Grampian protocol for screening as recommended by Down’s Syndrome Medical Interest Group (DSMIG) national guidelines. (see Annex 1)
Types of Down’s Syndrome Trisomy 21 (Non-disjunction): this is the most common form (in 94%) All cells
in the body contain an extra chromosome 21 because the parent’s sperm or egg contained two of chromosome 21 instead of one, giving the child an extra chromosome 21 in each cell.
Translocation: (in 4%) the extra chromosome 21 is translocated or attached to another chromosome. They have 46 chromosomes with one chromosome being larger than usual due to the extra 21 chromosome being attached.
Mosaic: (in 2%) only some cells carry an extra chromosome 21, while others have two as normal.
Physical features associated with Down’s Syndrome Low muscle tone(hypotonia) causing the baby to be floppy Face – round with flatter profile Head – back of head slightly flattened (brachycephaly) Eyes – slight upwards slant, fold of skin running vertically from corner
of eye to bridge of nose (epicanthic fold), white or yellow spots around iris (Brushfield spots)
Neck – short and stocky, newborn babies may have excess skin over the back of their neck.
Mouth – smaller mouth cavity, making the tongue look larger
November 2008 6

Combined Child Health Service
Hands – broad with short fingers, little finger may only have one joint and curve in towards the other fingers, may only have one single crease running across palm.
Feet – broad and short , toes widely spaced between 1st and 2nd toe (sandal gap)
Below average weight and length
Many of these features appear in the general population and not all babies with Down’s Syndrome show all characteristics. Individuals are all different, and have some of their family’s physical features, just like any child. It is important to remember that children with Down’s Syndrome will more closely resemble their parents and siblings in appearance, than other children with Down’s Syndrome. (adapted from Down’s Syndrome Scotland Booklet – “Ages and Stages of Down’s Syndrome”)
November 2008 7
Combined Child Health Service
Birth of BabyDuring the initial examination by the midwife it may be suspected that the baby has Down’s syndrome (if not previously detected during antenatal screening). The midwife may have identified some physical features in the baby that may be associated with Down’s Syndrome.At this stage it is important that the parents are informed of the possible diagnosis of Down’s Syndrome by an appropriate professional.
A senior paediatrician should be contacted as soon as possible to: Confirm the diagnosis Give initial information to parents Medically assess the baby
Although a confident diagnosis can often be made clinically, a definitive diagnosis must be confirmed by obtaining a blood sample from the baby for karyotyping (chromosome analysis) with the parents consent.
The baby should be referred to a paediatrician with special interest in Downs Syndrome, or an experienced paediatrician, and initial screening tests should be arranged as soon as clinicians are confident of the diagnosis, often before results of karyotype are known.
The paediatrician should meet both parents as soon after referral as possible, to offer up-to-date, factual, verbal and written information about:
genetics and aetiology of Downs Syndrome, immediate and future health concerns, the normal developmental pattern expected local resources prognosis.
It is important to ensure that all newborn screening tests have been carried out (see page 11) and follow-up appointments made before discharge from hospital.
The importance of the time of disclosure and way this is managed cannot be over-stressed. Down’s Syndrome Scotland has published a booklet titled “Recommendations for telling parents that their child has Down’s Syndrome” which some professionals may find helpful. They also offer a 24hr helpline for advice and information that professionals can access prior to informing parents, Tel: 0131 313 4225.
Parents do not need to have their chromosomes checked or specialist counselling by a geneticist if their baby has non-dysjunctional Trisomy 21 as this is not associated with chromosomal abnormalities in parents. The chance of having a second baby with Downs’ Syndrome is 1 in 100 in all mothers under 40 (higher in mothers over 40) and all parents will be offered genetic counselling and antenatal CVS/amniocentesis testing in their next pregnancy.
November 2008 8

Combined Child Health Service
Information for ParentsParents of children diagnosed with Down’s Syndrome require clear verbal and written information about the condition and associated health issues.
All parents of children diagnosed with Down’s Syndrome will be supplied with a New Parent Information Pack published by Down’s Syndrome Scotland (DSS) as soon as possible after diagnosis.They will also receive details of New Parent Contacts, these are local parents of a child with Down’s Syndrome who have been trained by DSS to provide voluntary help and support to new parents.Personal Child Health Records (PCHR)The paediatrician visiting the family in hospital, or a member of their team, should contact the family Health Visitor, if possible before the baby is discharged, to offer on-going support to Primary Health Care team and to send them a copy of the Down’s Syndrome insert for the baby’s PCHR. This 20 page insert was developed by Downs Syndrome Medical Interest Group (second edition, 2000) and contains additional information for parents and professionals which will help them maintain the health and well being of babies born with Down's syndrome including:
General information Expected developmental progress Possible health problems Suggested schedule of health checks Advice about immunisation, feeding and growth Down's specific growth charts Sources of additional help and advice
Health Visitors should give parents their PCHR with relevant insert already included.
Personal Child Health Records were introduced to facilitate partnership with parents and to empower them in overseeing their child’s development and health care. It is important that health professionals use this record to allow parent’s to have available written information about their child’s health and development. Information on diagnosis and how to access appropriate information and support can also be recorded in the Personal Child Health Records.
November 2008 9

Combined Child Health Service
Providing further information on local support groups and other national and local resources available will help empower parents in the care of their child.further sources of information include:-
Down’s Syndrome ScotlandChildren’s Centre
City Hospital CampusHucknall Road
NottinghamNG5 1PB
Website: www.dsmig.org.uk
Down’s Syndrome Medical Interest Group158/160 Balgreen Road
EdinburghEH11 3AU
Tel: 0131 313 4225Website: www.dsscotland.org.uk
Down’s Syndrome Association Down’s Heart GroupLangdon Down Centre PO Box 4260 2a Langdon Park Dunstable Teddington BedsTW11 9PS LU6 2ZT Tel: 0845 230 0372 Tel: 0845 166 0861Website www.downs-syndrome.org.uk Website: www.dhg.org.uk
The Family Fund Contact a Family ScotlandUnit 4 Alpha Court Craigmillar Enterprise & Arts CentreMonks Cross Drive 11/9 Harewood RoadHuntington EdinburghYork EH16 4NTYO32 9WN Tel: 0131 659 2930Tel: 0845 130 4542 Website: www.cafamily.org.uk Website: www.familyfund.org.
Gordon Rural Action VSA Carers Centre55 Gordon Street 24-28 Belmont StreetHuntly AberdeenAB54 8EQ AB10 1JHTel: 01466 793676 Tel: 01224 646677
Website: www.vsa.org.uk 15a High StreetInverurieAB51 3QATel: 01467 629072
November 2008 10

Combined Child Health Service
Neonatal Medical Assessment by PaediatricianIt is essential that every newborn baby with Downs’ Syndrome has a comprehensive physical and neurological medical examination by an experienced paediatrician.Many malformations will declare themselves early but for some screening will have to be carried out, therefore all babies in addition to routine newborn screening should have:
Echocardiogram (in newborn period, by trained professional) to detect congenital cardiac disease. Cardiac status should be established by the time the baby is 6 weeks old.
Eyes checked for congenital cataracts (by ophthalmologist in Grampian) Neonatal hearing screening weight, length and head circumference plotted Neonatal screen for hypothyroidism (Guthrie Test)
Further tests may be arranged as appropriate with a high index of suspicion regarding associated abnormalities.For further information and detailed guidance regarding basic medical surveillance of cardiac disease, thyroid disorder, hearing impairment and ophthalmic problems check: www.dsmig.org.uk
Primary Health Care TeamThe child’s General Practitioner and Health Visitor will be notified prior to the child’s discharge from hospital and a copy of the Down’s Syndrome specific insert pages for the Personal Child Health Record (PCHR) will be sent out.
Universal Child Health ScreeningThe universal core programme for child health screening and surveillance is carried out by the Primary Health Care team liaising with Child Development Service, Specialist Services, Allied Health Professionals, Social Work, Educational Psychology and nursery as required.
The early identification of a child requiring an assessment for health problems and developmental disorders is the aim of the child health screening and surveillance programmes. Health for all Children (Hall 4) has led to a significant change in screening and surveillance in Scotland.
Hall 4 states: -Every child and parent should have access to a universal or core programme of preventative pre-school care.Formal screening should be confined to the evidence based programmes agreed by the National Screening Committee.Health professionals must respond promptly to parental concerns.
Scottish Executive 2005
November 2008 11

Combined Child Health Service
Social Work DepartmentAn assessment of need may be carried out to determine what support and services are required by the child and their family. This may include respite care, play schemes for child or siblings and details of available financial assistance.
Management by Specialist ServicesThe child will be referred to the appropriate specialist service to assess, review and treat any specific medical problems they may have.
All babies are reviewed in Cardiac clinic aged 3 months All children are reassessed by Audiology before their first birthday, and then
annually throughout preschool. All children will have a full eye/vision assessment, including refraction (to
check if they need glasses) before they start nursery.
November 2008 12

Combined Child Health Service
Refer to Child Development ServiceThe Child Development Service is available at local clinics throughout Grampian and can be accessed by referral to:-
Community Child Health DepartmentRoyal Aberdeen Children’s Hospital
Westburn RoadAberdeenAB25 2ZG
Dr Pat Charleton, or Dr A LiebenbergRaeden Centre Ward 2Midstocket Road Dr Gray’s HospitalAberdeen Pluscarden RoadAB15 5PD Elgin
IV30 1SN
Children should be offered regular developmental review through Child Development Services to assess and manage health and development needs. Liaison with Health Visitor, Allied Health Professionals, Social Work, Educational Psychology and nursery school may be required to ensure the child’s care and social needs are being met.
A Grampian Schedule of Health Checks, based on the United Kingdom Downs’ Syndrome Medical Information Group (DSMIG) Guidelines, have been drawn up to assist medical professionals with examination and screening tests to detect problems more likely to occur in children with Down’s Syndrome. (See Annex 1)
DSMIG at www.dsmig.org.uk is a useful resource, with in formation about: “Guidelines” for further information and detailed guidance regarding basic
medical surveillance of cardiac disease, thyroid disorder, hearing impairment and ophthalmic problems, cervical spine instability and monitoring of growth.
“key points” and “clinical awareness notes” for additional information on a variety of additional medical conditions.
Early identification, early therapeutic and educational intervention, and seamless delivery of services may help a child to maximise their potential.
November 2008 13

Combined Child Health Service
Developmental AssessmentChildren with Down’s Syndrome progress at a slower rate in their development.A table giving an outline of the approximate age range of when children with Down’s Syndrome reach/achieve some milestones has been adapted by the DSMIG. (See Annex 2)
Development assessments can involve a multidisciplinary and multiagency approach. This involves:-
Medical assessment; physical and neurological examination. Co-ordination with specialist services Thyroid function- checked annually by TSH finger-prick test after the age of 1
year. (Consent required for thyroid screen database.)
Agreed timetable for multidisciplinary early intervention in Grampian: Early referral to Physiotherapist aged 2-3 months or as soon as the infant is
medically fit, for advice and management of early motor development. Input from the Physiotherapist is reduced when the child starts to walk but ongoing orthotic support may continue.
Referral to Speech and Language Therapy (SALT) around 6 months of age for advice on feeding/weaning and on encouraging early communication.
Occupational therapy assessment may be considered (usually just preschool or in early primary years, unless additional concerns.)
Multidisciplinary Developmental Assessment may be arranged if there is concern about developmental progress or the child/ family would benefit from additional specialist nursery support.
Educational assessment to assess the child for any additional support needs and in partnership with the parents and health professionals to decide on preschool placement(s) - a combination of mainstream nursery, local playgroup, developmental nursery. (Should be referred to educational psychology between age 2 and 2½ years)
Clinical psychology referral may be arranged for help and assessment of behavioural difficulties
Social Work assessment
November 2008 14
Combined Child Health Service
EducationThe Health Service may identify a child as appearing to have additional support needs arising from a disability and bring this child to the attention of the education authority.The educational authority will decide whether to assess the child to find out if they have additional support needs and will determine what support is required.The educational authority in partnership with the parents will decide if the child attends a mainstream nursery school, developmental nursery or combination. All 3 and 4 year olds in Scotland are entitled to a funded part time pre-school education placement.
The Education (Additional Support for Learning) (Scotland) Act 2004 (ASL Act) introduced a new framework for providing support to children and young people who require additional help with their learning. The education authority may then, at its discretion, establish whether the child has additional support needs arising from a disability under its arrangements for identifying and providing for children with additional support needs. Once it is established by the educational authority the child has additional support needs, the authority would then have a duty to provide suitable provision to meet those needs. The Additional Support for Learning Act requires an educational authority to provide additional support to certain disabled pre-school children in their area who are under 3 years old.
The ASL Act aims to ensure that all children and young people are provided with the necessary support to help them work towards achieving their full potential. The ASL Act also promotes collaborative working among all agencies involved with supporting children.
Joint Assessment of Needs / Integrated AssessmentJoint assessment of needs is a co-ordinated Multi-Agency approach to gathering information and aims to avoid parents having to repeat information more than once, giving a holistic view of the child within their family and community enabling assessment of medical, social and educational needs.
Action plans are developed using the systematic assessment and analysis of the information obtained about the child. The child and their family may participate in the development of the action plan.An action plan records the needs and the professional responses and responsibilities to the child, outlining the basis for providing support, services and resources to meet the needs of the child.An action plan should state:
what action should be taken by whom to improve the child’s circumstances the reasons for the plan timescales intended outcome and future review date The plan should be as simple as necessary and relevant to the child's needs. It should be updated or amended as needs change.
November 2008 15
Combined Child Health Service
Individual Educational Plan/ Co-ordinated Support PlanAn Individual Educational Plan (IEP) describes in detail the nature of the child’s additional support needs, the ways in which these are to be met, the learning outcomes to be achieved, and specifies what additional support is required, including that required from agencies outwith education. The IEP should be reviewed and updated regularly, involving the parents and child (where possible).
A Co-ordinated support plan is prepared for children who: need support due to complex or multiple factors that have a significant
adverse affect on their education require significant involvement from one or more additional agencies such as
health and social work. will need support for more than a year
The aim of a co-ordinated support plan is to ensure that the various professionals and agencies involved in providing support are working together and that the support is co-ordinated.
A Co-ordinated support plan: is an action plan for children who require significant additional support with
their education supports partnership working to help children achieve educational targets is monitored and reviewed regularly involves the child, their family, education and additional agencies
(Enquire 2007)
Key workerA key worker is a named person who works in partnership with the family and can provide a link between professionals and agencies involved in the child’s care. Key workers can co-ordinate access to, and delivery of services required from various agencies.
Regular ReviewThe child will have regular reviews carried out by the various professionals and agencies involved in their care. Their needs will be reassessed and plans updated as required.
November 2008 16

Combined Child Health Service
Pathway 4 School Aged Patient Care Pathway
Jackie Robertson Parent Representative
Elma Stephen Consultant Paediatrician
Donald Todd Clinical Nurse Manager
November 2008 17
Health Developmental review and scheduled health checks through Child Development Services.Regular review by Specialist Services involved in careLiaise with General Practitioner, Specialist Health Visitors, Learning Disabilities Team, Social Work, School, Allied Health Professional Services
Social WorkIdentify any Social care and
Support Needs for the child/young person and the
family
EducationIdentify any
Additional Support for Learning
Needs
Mainstream School
Specialist Unit Special School
Joint Assessment of Need
Integrated Assessment Framework Action Plan
Key worker Appointed(Not yet implemented)
+/- Individual Education Plan/Co-ordinated Support Plan
Regular review and reassessment of needs by various professionals
involved
Transfer to Community Care Management Team for continued
review and reassessment of needs

Combined Child Health Service
Guidance on the use of School Age Down’s Syndrome Patient Care Pathway
HealthAnnual developmental reviews are offered through Child Development Services to assess and manage developmental and medical health problems. More frequent reviews may be offered depending on the individual child/young person’s needs.Liaison with Specialist Services, General Practitioner, Specialist Health Visitor, Allied Health Professionals, Social work, Educational Psychology and School may be required to ensure the child/young person’s care and social needs are being met.
Recommended Schedule of Health Checks: Thyroid blood test: Annual TSH fingerprick test co-ordinated by Support
Needs System computer database (parental consent required). Grampian protocol followed for positive tests.
Growth monitoring: Annual height and weight. Plot on Down’s Syndrome growth chart. If concerns about obesity calculate BMI and plot on standard chart.
Eye examination: Review 2 yearly by High street Optometrist or hospital Eye clinic.
Hearing check: Review 2 yearly by Audiology department. Advise regarding cervical spine instability.
(British Gymnastics information pack on the participation in gymnastics and trampolining by people with Down’s Syndrome contains the consent and medical screening form which should be completed prior to the child/young person participating in these activities. Available from: http://www.dsmig.org.uk/whatsnew/index.html
Dental check: every 6 months.
www.dsmig.org.uk is a useful resource including- “Guidelines” for further information and detailed guidance regarding basic
medical surveillance of cardiac disease, thyroid disorder, hearing impairment and ophthalmic problems, cervical spine instability and monitoring of growth.
“key points” and “clinical awareness notes” for additional information on a variety of additional medical conditions.
November 2008 18

Combined Child Health Service
Universal Child Health ScreeningHealth for all Children (Hall 4) has led to a significant change in screening and surveillance in Scotland. All children receive a health check when starting primary school, with little formal child health surveillance after that. In school age children detection of problems should be part of mainstream school life.Hall 4 states: -Formal screening should be confined to the evidence based programmes agreed by the National Screening Committee.Health professionals must respond promptly to parental concerns.Children starting school should receive the agreed screening programmes.Health care of school-age children should include support for children with problems and special needs.
Scottish Executive 2005
Social WorkAn assessment of need may be carried out to determine what support and services are required by the child and their family. This may include family support services, mainstream or specialist childcare, respite care, leisure and recreational facilities and details of available financial assistance.
EducationThe Health Service may identify a child as appearing to have additional support needs arising from a disability and bring this child to the attention of the education authority.The educational authority will decide whether to assess the child to find out if they have additional support needs and will determine what support is required.The educational authority in partnership with the parents will decide if the child attends a mainstream school, a specialist unit attached to a mainstream school a special school.or a combination.
The Education (Additional Support for Learning) (Scotland) Act 2004 (ASL Act) introduced a new framework, based on the idea of additional support needs, to provide for children and young people who require additional help with their learning.The education authority may then, at its discretion, establish whether the child has additional support needs arising from a disability under its arrangements for identifying and providing for children with additional support needs. Once it is established by the educational authority the child has additional support needs, the authority would then have a duty to provide suitable provision to meet those needs.
The ASL Act aims to ensure that all children and young people are provided with the necessary support to help them work towards achieving their full potential.The ASL Act also promotes collaborative working among all agencies involved with supporting children.
November 2008 19
Combined Child Health Service
Joint Assessment of Needs / Integrated AssessmentJoint assessment of needs is a co-ordinated Multi-Agency approach to gathering information and aims to avoid parents having to repeat information more than once, giving a holistic view of the child within their family and community enabling assessment of medical, social and educational needs.
Action plans are developed using the systematic assessment and analysis of the information obtained about the child. The child and their family may participate in the development of the action plan. An action plan records the needs and the professional responses and responsibilities to the child, outlining the basis for providing support, services and resources to meet the needs of the child.An action plan should state:
what action should be taken by whom to improve the child’s circumstances the reasons for the plan timescales intended outcome and future review date
The plan should be as simple as necessary and relevant to the child's needs. It should be updated or amended as needs change.
Individual Educational Plan / Co-ordinated Support PlanAn Individual Educational Plan (IEP) describes in detail the nature of the child’s additional support needs, the ways in which these are to be met, the learning outcomes to be achieved, and specifies what additional support is required, including that required from agencies outwith education The IEP should be reviewed and updated regularly, involving the parents and child (where possible).
A Co-ordinated support plan is prepared for children who: need support due to complex or multiple factors that have a significant
adverse affect on their education require significant involvement from one or more additional agencies such as
health and social work will need support for more than a year
The aim of a co-ordinated support plan (CSP) is to ensure that the various professionals and agencies involved in providing support are working together and that the support is co-ordinatedA Co-ordinated support plan:
is an action plan for children who require significant additional support with their education
supports partnership working to help children achieve educational targets is monitored and reviewed regularly involves the child, their family, education and additional agencies
(Enquire, 2007)
November 2008 20

Combined Child Health Service
Key workerA key worker is a named person who works in partnership with the family and can provide a link between professionals and agencies involved in the child’s care. Key workers can co-ordinate access to, and delivery of services required from various agencies.
Review
The child will have regular reviews carried out by the various professionals and agencies involved in their care. Their needs will be reassessed and plans updated as required.
Transfer to Adult Services
Transfer from Paediatric Services to Community Care Management Team will take place when the young person leaves school. Ongoing medical surveillance and health checks are recommended throughout adult life. (see: www.dsmig.org.uk)
Currently in Grampian adults are registered with The Grampian Thyroid Register on leaving school. They will be offered annual Thyroid screening through their General Practioner.
November 2008 21

Combined Child Health Service
Annex1
Down’s Syndrome – Grampian Schedule of Health Checks(Adapted from DSMIG Schedule of Health Checks 2000)
The following are suggested ages for health checks. Checks at any other time if there are parental or other concerns
Age Birth to 6 weeks 6 – 12 months 12months –2½ years
3 - 3½ years 4 - 4½ years
Thyroid bloodTest
Routine Guthrie test Annual TSH fingerprick test. follow protocol for positive test.
Growth Monitoring
Length and weight should be checked frequently and plotted on Down’s Syndrome growth charts.Head circumference should be checked at each routine medical check.
Length and weight should be checked at least annually and plotted on Down’s Syndrome growth charts.
Body Mass Index (BMI) checked and recorded.
Eye CheckVisual Behaviour.
Check for congenital cataract by Ophthalmologist
Orthoptic examination, refraction and
ophthalmic examination
Visual acuity, refraction and
ophthalmic examination. (if
necessary)
Hearing Check Neonatal screeningFull audiological review (hearing,
impedance,otoscopy) by the age of 1 year
Full audiological review(hearing , impedance, otoscopy) annually
Heart check and other
advice
Echocardiogram at birth or diagnosis. review in cardiac clinic three months later
Dental Advice. Check up every 6 months
November 2008 22

Combined Child Health Service
Annex 2
Down’s Syndrome – Child Development (DSMIG 2000)
Area of development Milestone Age range
Down's syndrome Other children
Gross motor skills(moving around)
Holds head steady in sitting
position3-9m 1-4m
Sits alone 6-16m 5-9m
Stands alone 12-38m 9-16m
Walks alone 13-48m 9-17m
Fine motor skills and eye hand coordination
Follows object with eyes 1.5-8m 1-3m
Reaches out and grasps object 4-11m 2-6m
Passes objects from hand to
hand6-12m 4-8m
Builds a tower of two 1" cubes 14-32m 10-19m
Copies a circle 36-60m 24-40m
Communication skills
Babbles "Dada", "Mama" 7-18m 5-14m
Responds to familiar words 10-18m 5-14m
First words spoken with
meaning13-36m 10-23m
Shows needs by gesture 14-30m 11-19m
Two word phrases 18-60m 15-32m
Personal and social skills
Smiles when talked to 1.5-4m 1-2m
Feeds self with biscuit 6-14m 4-10m
Drinks from cup 12-23m 9-17m
Dry by day 18-50m 14-36m
Bowel control 20-60m 16-48m
November 2008 23

Combined Child Health Service
References:
antenatalcare.com, The Early Screening Test for Down’s Syndrome
British Gymnastics, (2006) Alto Axial Information Pack, http://www.dsmig.org.uk/whatsnew/index.html (accessed 2007)
Down’s Syndrome Medical Interest Group (2000), Child Development Chart, www.dsmig.org.uk (accessed 2007)
Down’s Syndrome Medical Interest Group (2000), Schedule of Health Check, www.dsmig.org.uk (accessed 2007)
Down’s Syndrome Scotland, Ages and Stages of Down’s Syndrome, www.dsscotland.org.uk (accessed 2007)
Down’s Syndrome Scotland, Recommendations for telling parents that their child has down’s Syndrome, www.dsscotland.org.uk (accessed 2007)
Enquire, Planning children’s and young peoples learning, www.enquire.co.uk (accessed 2007)
NHS Quality Improvement Scotland (2005), Pregnancy and Newborn Screening – Clinical Standards
Scottish Executive, Education (Additional Support for Learning) (Scotland) Act 2004
Scottish Executive, (2005) Health for all Children
Scottish Executive, (2005) Supporting Children’s Learning, Code of Practice
November 2008 24

Combined Child Health Service
Working Group Members
Jackie Crum (chair) Consultant Paediatrician
Pat Charleton Associate Specialist Paediatrician
Ena Cromar Project Co- Ordinator,Children with Disabilities
Suleman Daud Consultant Paediatrician
Ann Edgar Community Nurse Health Visitor.Learning Disabilities Team Aberdeen
Louise Holliday Clinical Educator
Imogen Kerr Educational Psychologist (in training)
Andre Liebenberg Consultant Paediatrician
Sandra Munro Specialist Health Visitor Aberdeen
Mathew Musset Educational Psychologist Aberdeen
Grace Porter Clinical Midwifery ManagerAberdeen Maternity Hospital
Anne Reid Associate SpecialistAberdeen Maternity Hospital
Brenda Rennie Down’s Syndrome AssociationNew Parent Contact
Jackie Robertson Parent Representative
Norman Smith Consultant Obstetrician Aberdeen Maternity Hospital
Elma Stephen Consultant Paediatrician
Donald Todd Clinical Nurse Manager
November 2008 25