
Down Syndrome 2004
80
Fundació Catalana Síndrome de Down Services and Methodology
-
Upload
firoz-reza -
Category
Documents
-
view
214 -
download
0
Transcript of Down Syndrome 2004

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 1/80
Fundació Catalana Síndrome de Down
Services and Methodology

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 2/80
Title: Fundació Catalana Síndrome de Down. Services and Methodology
Author: Beatriz Garvía. CMD Psychologist and FCSD Coordinator of Research andTuition.Contributors: FCSD Technical staff; R. Borbonès, M. Golanó, M.J. Miquel, M. Peralta, J.Ruf and K. Trias.Coordinator: Katy Trias.Photography: Ivana Gutiérrez and Katy Trias.Translator: Mary Fons1st. edition: 19992nd. edition (revised and expanded): 2004Publishing secretary: Núria BoronatThis book was made possible by Caixa Catalunya.
This book may not be reproduced or transmitted in any form, whether in full or in part, by any means, electronic or
mechanical, including photocopying and recording, or by any information storage or retrieval system, without priorwritten permission from the copyright holders.
© FUNDACIÓ CATALANA SÍNDROME DE DOWN (FCSD)Comte Borrell, 201, entresòl, 08029 BarcelonaE-mail: [email protected]: www.fcsd.orgDirector: Katy TriasChair of the FCSD Board: Montserrat TruetaCover design and layout: Barcelona Digital, S.L.Printed by: Barcelona Digital, S.L.
ISBN: 84-921020-5-5Copyright registration: B-11272-2005
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 3/80
FCSD
INDEX
Foreword to the 2nd edition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Fundació Catalana Síndrome de Down Board of Directors . . . . . .10
Organization chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
Down Syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
Centre for Child Development and Early Intervention . . . . . . . . . . .17
Mainstream School Support Service . . . . . . . . . . . . . . . . . . . . . . . .25
Social Skills and Preparation Programme -PAS- . . . . . . . . . . . . . . .33
Col·labora, Job Integration Service . . . . . . . . . . . . . . . . . . . . . . . . .41
“I am going home”, Independent Living Support Service . . . . . . . .47
Down Medical Centre . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .53
Tuition and Training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .65
External Relations and New Projects Service . . . . . . . . . . . . . . . . .71
Begoña Raventós Data Centre . . . . . . . . . . . . . . . . . . . . . . . . . . .75
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .80
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 4/80

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 5/80
FCSD
5
FOREWORD TO THE 2ND EDITION
The second edition of this book was produced on the occasion of the
20th anniversary of Fundació Catalana Síndrome de Down (FCSD),
founded in 1984 by Montserrat Trueta, who had been working for
children with Down Syndrome (DS) and their families since 1978 both in
a private and in a professional capacity. Her co-founders were a team ofprofessionals and parents. The following year, she travelled with a team
of specialists to Washington University in Seattle, WA (USA) for training,
information-gathering and observation purposes. They returned with a
wealth of new knowledge which they put to use in the Centre for Early
Care and Stimulation which had been set up by the Foundation.
Since then, the Foundation has been growing and expanding itsservices, as well as adapting its methods according to emerging needs.
Those new needs arose as the original newborns with DS and other
children with DS or other mental disabilities grew up. The Foundation’s
mission was clear from the outset: to work towards better quality of life
for persons with mental disabilities and secure true integration in society,
based on the idea that quality of life is linked with gains in autonomy,acceptance of disability, and capacity for self-management. This overall
mission gave rise to the Down Medical Centre; to the Mainstream School
Support Service, developed to support school integration; to the Social
Skills and Preparation Programme, to ensure leisure time and foster the
social skills of its clients; and to the Col·labora, Job Integration Service,
which places clients in mainstream employment, following the model
implemented in Genoa, Italy, which uses a pioneering mediation method.
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 6/80
FCSD
The original babies seen in 1984 and the ones that followed (up to a
current figure of 1,000 clients) have now grown up, received an
education and, in many cases, are placed in mainstream companies,
earning wages, enjoying social and affectionate relationships, andorganizing their own outings, travel, and leisure. Sooner or later, they
come to want emancipation; they want to live, like their siblings, in a home
of their own. Parents who adhered to our philosophy and who had
already taken the risk of giving their children freedom and autonomy also
supported this endeavour, so Katy Trias, like her mother 17 years before,
travelled to the US and the UK to learn about independent living in those
two countries. Using this information and working with the support of herteam, she set up “I'm going home”, (Me’n vaig a casa), an Independent
Living Support Service to afford individuals with disabilities the chance to
pursue a normalized life, choosing where and with whom to live. The
Programme provides tailored support for clients and their families to
achieve this objective. It was launched on an experimental basis in 2001
and is now consolidated as a FCSD Service receiving government
funding.
The present edition of the Services and Methodology book has been
revised and expanded to include the new Services as well as changes to
existing ones, bearing witness to the dynamism, usefulness and on-going
development of FCSD.
6
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 7/80
FCSD
7
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
INTRODUCTION
The Fundació Catalana Síndrome de Down (FCSD) is a non-profit
private organization founded on March 30, 1984 and declared to be of
public utility on October 24 of that year. Its registry number in the Catalan
Government's Registry of Catalan Foundations is 61.
The FCSD was born out of a common interest, shared by parents and
professionals alike, to gain a better understanding of Down Syndrome
(DS) by carrying out research and doing practical work in the fields of
education, psychology, medicine and welfare. From its very beginning,
outstanding international scientists specialized in subjects relating to DS
have given the FCSD their valuable support and on some occasions even
their personal participation, if necessary.
The FCSD technical team is made up of a group of professional
psychologists, educationalists and physicians and a group of scientific
advisors. Its pioneering spirit led the FCSD to be regarded as a
reference centre consulted by a large number of public and private
organizations, both in Spain and abroad. The message which the FCSD
wishes to convey is that people with DS have inherent capacities and are
entitled to obtain resources as appropriate to meet their individual needs
for optimal development.
The FCSD's main goals may be outlined as follows:
G To work for better quality of life for persons with DS, in order for them
to attain full social integration. This aim extends to all persons withlearning difficulties.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 8/80
FCSD
8
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
G To act as a permanent body, promoting studies and research in the
medical, psychological and educational fields, and providing the
experience and knowledge thus gained to public and private
organizations, institutions, and to society in general.
G To broaden, improve and create services, which may be deemed
necessary to meet the social, personal, and family demands of
persons with DS. As DS people integrate and participate more
effectively in society, new set of needs arise, which the FCSD covers
by widening the scope of its services.
Acting as a Resource Centre, the FSCD furnishes information and
advice, organizes training courses and other activities, not only for people
with DS but also for their families and professionals working in this field.
The FCSD has been battling for years to achieve full, effective,
favourable social integration for all.
Since 1982 when the Spanish parliament enacted the LISMI (a law
for social integration of people with disabilities), boys and girls with
disabilities have had access to state schools and to mainstream
education. This law has proved highly positive not only for mentally
disabled children but for the rest of the children as well. Students
become more tolerant, show their solidarity and learn about disability. Asa result, they approach their disabled schoolmates in a natural, prejudice-
free way, allowing real integration to take place. The FCSD strives
constantly for the rights of people with disabilities to be safeguarded,
both by pressing for compliance with existing legislation and by lobbying
for new or improved laws to defend and promote the full social integration
of people with disabilities.
Finally, biomedical research on DS is also part of the FCSD mission,

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 9/80
FCSD
9
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
in the form of constant research per se and regular publication of the
latest findings.
For this reason, the FCSD confers the Ramon Trias Fargas Prize on
DS Research every two years. This prize is awarded for scientific
research or experimental work concerning genetic, perinatological,
psychological or medical aspects related to DS. A specialized scientific
committee evaluates entries and decides on the winner. Research must
be carried out within Spanish territory to be eligible. Candidates for this
prize may be individuals or teams, and must have the support of ascientific or academic institution, or any institution related to DS.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 10/80
FCSD
10
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
FUNDACIÓ CATALANA SÍNDROME DEDOWN BOARD OF DIRECTORS
Honorary Members of the Board
Victoria de Los Ángeles (RIP)Maria del Mar RaventósJosep M. EspinàsRamon Trias Fargas (RIP)Francisco Domínguez del BrioRobert Vergés (RIP)
Members of the Board:
Chair: Montserrat TruetaVice-President: Antoni TriasSecretary: Immaculada BoschTreasurer: Carmen BuxeresMember: Juan Manuel Cabrera
Member: Joan UriachMember: Katy TriasMember: Marta Corachán
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 11/80
FCSD
11
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
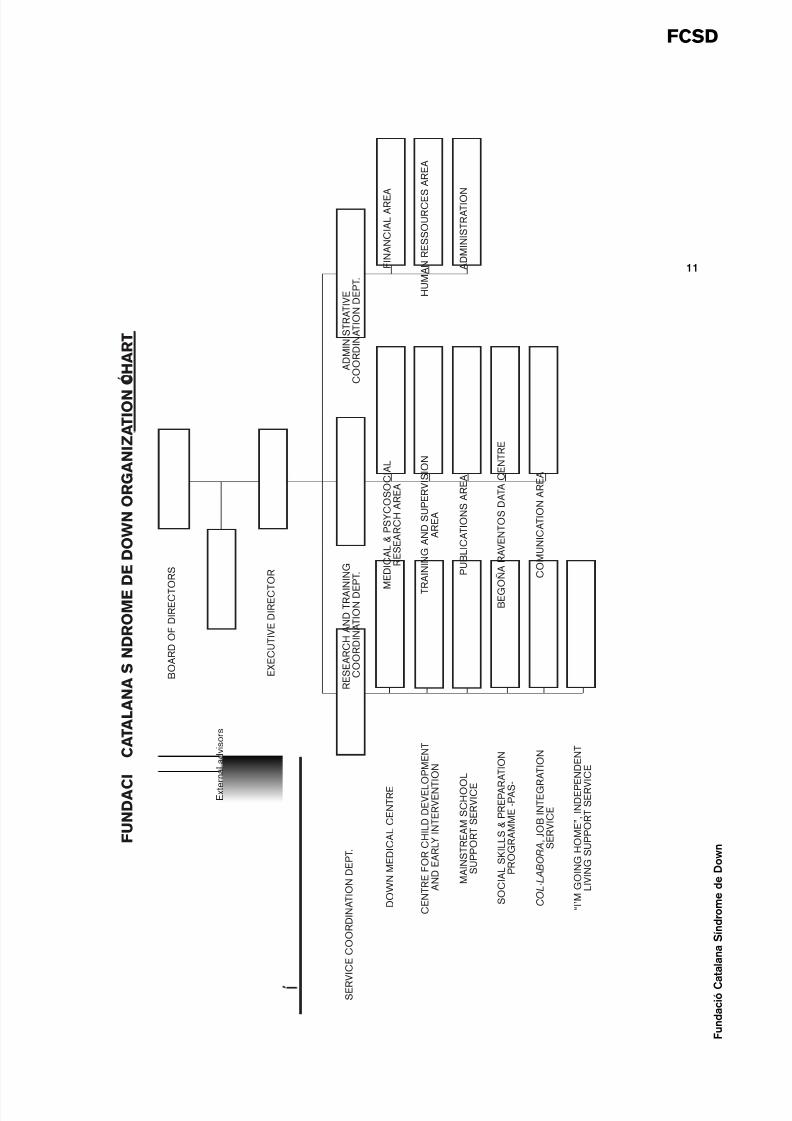
F U N D A C
I C
A T A L A N A S N D R O M E D E D O W N O R G A N I Z A T I O N
C H A R T
B O A R D O F D I R E C T O R S
E x t e
r n a l a d v i s o r s
E X E C U T I V E D I R E C T
O R
S E R V I C E C O O R D I N A T I O N D E P T .
D O W N M E D I C A L C E N T R E
C E N T R E F O R C H I L D D E V E L O P M E N T
A N D E A R L Y I N T E R V E N T
I O N
M A I N S T R E A M S C H O O
L
S U P P O R T S E R V I C E
S O C I A L S K I L L S & P R E P A R
A T I O N
P R O G R A M M E - P A S -
C O L · L A B O R A ,
J O B I N T E G R A T I O N
S E R V I C E
“ I ’ M G O I N G H O M E ” , I N D E P E N D E N T
L I V I N G S U P P O R T S E R V
I C E
R E S E A R C H A N D T R A I N I N G
C O O R D I N A T I O N D E
P T .
M E D I C A L & P S Y C O S O C I A L
R E S E A R C H A R E A
T R A I N I N G A N D S U P E R V I S I O N
A R E A
P U B L I C A T I O N S A R E A
B E G O Ñ A R A V E N T O S D A T A C E N T R E
C O M U N I C A T I O N A R E A
A D M I N I S T R A T I V E
C O O R D I N A T I O N D E P T .
F I N A N C I A L A R E A
H U M A N R E S S O U R C E S A R E A
A D M I N I S T R A T I O N

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 12/80
FCSD
12
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 13/80
FCSD
13
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
DOWN SYNDROME
Down syndrome (DS) is a genetic alteration caused by the presence ofan extra chromosome in the 21 set; for this reason, it is also known astrisomy 21. It was first described clinically by John Langdon Down in 1866.The extra genetic material alters the normal development of the individual,affecting certain physical features and intellectual level. Most people withDS (95%) present the trisomy 21 type called 'free' or 'regular', because
the extra chromosome appears from the outset in all the living cells of theorganism, due to an error in the disjunction of chromosome 21 in the germcells of one or both parents. This phenomenon is known as chromosomenon-disjunction. There are other types of DS, such as mosaic DS (wheretrisomy only occurs in certain cells) and translocation DS (wherechromosome 21 is attached to another chromosome). Diagnosis of DS isobtained by means of a chromosome study (Karyotype), which reveals thepresence of the extra chromosome in the 21 set. This type of analysis wasfirst used by Jerome Lejeune in 1958. More recent discoveries, some of
them sponsored by the FCSD, have shown that there are areas andgroups of genes in chromosome 21 which are specifically related to theappearance of some of the most significant physical features of thesyndrome.
The precise reasons why the non-disjunction mechanisms that causeDS are triggered remain unknown, though it has been proven that non-disjunction occurs regardless of race, education, social background, and
standard of living. However, it has been shown that DS is more likely toappear when the mother is over 35 years old at the time of conception, withthe risk of bearing a child with DS increasing progressively from age 35onwards. But paradoxically, DS births occur far more frequently amongwomen under 35, first, because they are the chief child-bearing group; andsecond, because pregnant women over 38 are routinely subjected toprenatal screening.
Two of the screening methods are amniocentesis (extraction of amnioticfluid through the abdominal wall between the 14th and the 18th week ofpregnancy) and chorion villus sampling or CVS (extraction of a small piece

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 14/80
FCSD
14
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
of placental tissue). Both can be used reliably to diagnose DS and otherchromosome abnormalities. Additional methods to determine the risk ofgiving birth to a child with DS have been recently incorporated in medical
practice. One is biochemical screening (measuring certain chemicals inmaternal blood, which are altered if DS is present). This test is carried outbetween the 14th and the 17th week of pregnancy. Another method isultrasound imaging, which screens for DS pregnancies by looking forsonographic markers, especially the nuchal fold; sonograms can bechecked for this from the 10th week of pregnancy. It is important to stressthat these tests should not be regarded as conclusive; if an alteration isfound, amniocentesis or chorion villous sampling must always be used toestablish whether the embryo actually has DS.
Though all DS carriers have a chromosomal aberration, they do not allpresent the same characteristics or physical features; malformations arenot even always present. The only distinct characteristic shared by allpersons with DS is a lowered intellectual level. There are no varyingdegrees of DS; traits and personality vary as widely among individuals withDS as among individuals without DS. In fact, people with DS are more
similar to people without DS than different from them. Ninety-five percentof children with DS present mild to moderate intellectual disability after

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 15/80
FCSD
15
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
receiving appropriate early intervention. Whatever the case may be, everyperson with DS possesses inherent values, which should be nourished.
Children with DS have a 40% rate of heart malformations, some ofthem so serious that they will require surgery during the first years of life. Amuch smaller number (5%) present gastrointestinal problems that requireimmediate neonatal surgery. While many different medical treatments forDown syndrome have been recommended over time, none has proven tohave a beneficial effect on DS so far. Early intervention alone has beenfound to be highly useful in stimulating the potential of each individual.Medical care primarily focuses on prevention of the most likely healthproblems to ensure that easily treated conditions do not become chronic.
It must be stressed that DS is not an illness, but a genetic disorder, whichis sometimes accompanied by health problems.
Individuals with DS must be considered from a whole-personperspective and offered the social assistance, medical care andeducational services best suited to their full personal development.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 16/80

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 17/80
FCSD
17
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
CENTRE FOR CHILD DEVELOPMENT ANDEARLY INTERVENTION
The birth of a child entails a series of deep psychological changesfor the parents, connected with their wishes as child-bearers. Thesechanges usually begin during or even before pregnancy. The baby-to-be already exists in the parents' imagination before birth. Both parents
imagine a baby in whom they will see themselves reflected. Moreover,the baby also stands for continuity of its parents' own values. A wholeseries of fantasies revolve around the child, to such an extent that theyare part of the initial bond, which the parents create with the baby. Afterbirth, these fantasies are gradually adjusted to the reality of thecharacteristics of the newborn baby. The whole of this adjustment is acomplex process of significant importance for the baby's futuredevelopment as an individual.
Faced with the news that the baby has a learning difficulty such asDS, parental narcissism is struck to the core. The cause is not only thediagnosis as such, but a whole welter of intense feelings towards thebaby and towards themselves and each other. There is a break with thepreviously established bond, and a process of mourning for the loss ofthe desired child then begins.
This mourning process is complicated, as it involves breaking theinternal bond with the ideal child and coming to terms with reality, thatis, with the fact of having a child with a disability. It takes a long time,but it is necessary in order to reconstruct a new internal place for thereal baby, which enables a desire to become its parent. This processleads to a progressive acceptance of the facts.
Parents find ways to identify with their DS newborn by thinking ofthe child as someone who is growing up with his or her ownpersonality, at a certain rate of development, with a range ofpossibilities ahead – in short, someone with an essence of his or her

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 18/80
FCSD
18
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
own – but also with a family likeness. This will also allow a new set offantasies to be created around this baby, so that the parents may lookforward to unexpected gratification from their unexpected child.
When a baby has DS (or any other disability), the idea of disabilityis wrapped around the identity of the newborn, preventing parents fromseeing the actual infant. Like any other child, a baby with a handicapneeds to be spoken to, to be played with and to be loved, but theseneeds are often complicated and hard to fulfil because the parents
wanted a different baby and either cannot approach their child or do notknow how to do so; if they do try, they may do so inappropriately. Thebirth of a child with a disability causes a great deal of anguish, andgenerates many complex psychological reactions, which varyaccording to the nature of the disability or condition, and the factorsthat caused it.
Briefly, from a state of shock and anguish, followed by denial ("Thedoctors got it wrong"), anger, and sorrow, parents reach a state ofequilibrium; with it emerges a feeling of confidence in their own abilityto care for the child just as it is. Ultimately, the family reorganizes its life

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 19/80
FCSD
19
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
according to the child's needs and adjusts to the situation. The parentsneed to be able to complete the mourning process produced by thearrival of a child unlike the expected one. All this points to the
importance of early intervention not only for the baby, but for itsparents, too. The intense and complex feelings and emotionsexperienced by parents when first faced with the diagnosis of DSclearly show that reporting this diagnosis is not a single event but awhole process with the dual purpose of imparting the relevantinformation and providing a space to contain parental anguish andemotional reactions.
After the baby's birth, emotional vulnerability arouses of self-doubtas to parenting ability. At the Centre for Child Development and EarlyIntervention (CCDEI), where children with different types ofdevelopment difficulties receive care from birth to five years, one of themain objectives is to provide support to parents in order to facilitate theearly relationship and help them regain their parental self-confidence.This support is regarded as working with the parents in order todiscover the baby's individual characteristics, observe and interpret its
demands, and seek satisfactory ways to meet the baby's manifestneeds. Every child reacts differently; development will only be seen asit unfolds.
The CCDEI of the FCSD, is part of the Early Intervention SectoralProgramme of the Institut Català d'Assistència i Serveis Socials(Catalan Institute of Social Care and Services), which reports to theCatalan Department of Social Welfare. The catchment area assigned tothe CCDEI within the programme comprises the districts of Sarrià-SantGervasi (District 5) and Esquerra de l'Eixample (District 2) in the city ofBarcelona. The CCDEI was originally founded as the “Servei d’AtencióPrimerenca” (Early Care Service) of the FCSD in 1984 andsubsequently took on the functions and objectives outlined in thedistrict-based Early Intervention Programme.
In October 1998, the FCSD service began to operate undercontract to the Catalan Institute of Social Care and Services; as aresult, the assistance provided is now fully a public service. In 2001 thename was changed to Centre de Desenvolupament Infantil i Atenció
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 20/80
FCSD
20
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
Primerenca (CCDEI - Centre for Child Development and EarlyIntervention).
Early intervention, a form of treatment basically directed at childrenwith developmental disorders as well as their families, is intended toassist in the process of structuring the child's personality, enhancinghis or her development, providing the necessary resources foradjustment and growth, and last but not least, assisting and supportingthe child's family.
The Centre operates as an outpatient clinic, providing assistance on
an individual basis; frequency of visits depends on each child's age andneeds.
The functions performed by CCDEI are outlined below:
1.- Diagnosis of requirements: At the family's request, a diagnosticprocess is set up, including interviews with both parents, assessmentof the child's developmental stage, and interviews with the child's
teachers when deemed necessary, if the child attends school. Oncethis information is obtained, it is discussed with the parents prior tobeginning treatment.
Basically, the purpose is to establish a functional diagnosis of thechild's problem, and, if possible, to determine the aetiology of the casewhen it is undefined.
Tending to the parents is also of paramount importance at this firstcontact. As a rule, when they first come, parents are full of anguish andvery uninformed concerning the nature of the problem. The Centre'sprofessionals provide care for the child and support for its parents inorder to contain the fear and anxiety and help them discover the childbehind the disability.
When the child is older (2-3 years old), the parents' anxiety is by nomeans lesser. Not knowing the child's specific problem is a source ofworry and anxiety. Sometimes, a highly unspecific diagnosis that is notbased on an underlying organic explanation may be hard to grasp.Delayed language acquisition or slow maturity, difficulties in socializing,

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 21/80
FCSD
21
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
or personality or behavioural disorders all cause highly ambivalentfeelings in the child's parents, who must therefore receive assistanceat the same level of intensity as the child in order to encourage positive
outcomes.
2.- Establishing and implementing treatment objectives: Once anapproximate diagnosis has been established, the aims of therapy aredetermined and intervention strategies are put in place to reach out to theindividual child.
Treatment approaches can be summed up as follows:
A) Direct treatmentEach child receives individually tailored treatment by a qualifiedprofessional according to the nature of his or her problems. Theinterdisciplinary team working at the Centre, which includespsychologists, education specialists, speech therapists,physiotherapists, a neurologist, and a social worker, allowstreatment to be individually designed for each case instead of having
a pre-established pattern of intervention
B) Family careAs mentioned earlier, treating the child's whole family is consideredessential from the very first. A key part of intervention is monitoringfamily relationships, especially the child's role within the family andthe meaning attributed by the parents to their child's disability orproblem.
C) Mainstream School Support ServiceThe child's process of adaptation to the school environment isconsidered a fundamental element in the social and personaldevelopment of the individual.
The Centre for Child Development and Early Intervention’s follow-upfunction therefore has a two fold role:
G On the one hand, the therapist in charge of the case should identifywhat kind of needs the child will have in this expanded environment

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 22/80
FCSD
22
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
and evaluate how the child socializes with its schoolmates andadults. This is done by direct observation of the child, in real-life
school situations, and by interviewing the schoolteacher.
G On the other hand, it is important for school staff to be given supportand advice, helping them to identify the needs and to detect thedifferences within a class, and to identify resources to meet theseneeds. More often than not, teachers focus on the things a child isunable to do, and this can be very frustrating for the child, to suchan extent that it may block his or her desire to learn. On some
occasions, this may also lead to a passive attitude — "I don’t know"or "I can't do it" —, which is actually masking the child’s despair atthe realization that he or she is unable to do the same things as therest of the schoolmates. Addressing this situation may give the childthe required self-confidence.
3.- As the FCSD's Early Intervention Service, the CCDEI deals with allkinds of enquiries from parents who seek early counselling orinformation about DS, resources available, where to apply for otherassistance, and so forth.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 23/80
FCSD
23
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
4.- Another important CCDEI activity is screening and prevention,identifying children with developmental disorders or who are at risk,reaching out to all children within the catchment area so that they may
benefit from CDIAP services whenever they are required.
To this aim, the CCDEI works in many different ways to raiseawareness and heighten professional sensitivity to the importance ofidentifying any signs of potential developmental disorders as soon aspossible and providing specialised early intervention to prevent futuretrouble.
5.- Finally, the CCDEI also provides training for professionals byholding lectures, courses, and seminars. CCDEI professional staffmembers frequently take part in symposia, courses and seminars heldby the FCSD or by other institutions, and they often advise and provideinformation to students and fellow professionals on request.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 24/80
FCSD
24
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 25/80
FCSD
25
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
MAINSTREAM SCHOOL SUPPORTSERVICE
The Mainstream School Support Service (MSSS) was set up in 1985in order to provide support and counselling to all children with DS aged 6to 16 who are attending mainstream schools and guidance to theirschoolteachers and parents. A major milestone for the social inclusion of
people with disabilities was Decree 117/1984 by the Government ofCatalonia, which regulated the structure of special education to ensure theintegration of children with special needs in mainstream schools inCatalonia according to the guidelines set in the Spanish LISMI Act (the"Act for Social Integration of People With Disabilities"). In order to providea school environment that is as unrestrictive as possible and diversifyschool response to individual pupils' needs, schooling objectives must begeneralized so that the child can develop satisfactorily after suitablecurricular adjustments have been made.
Since its founding in 1984, the FCSD has directed all its efforts toimproving the quality of life of people with DS through social integration.Any action undertaken by the FCSD is the result of elaborate analysisreached by its team of professionals through careful observation andevaluation of daily practice. This team of professionals has shown a highdegree of flexibility in its work, so FCSD methodology has varied asdifferent needs have become apparent. Team methodology has evolvedand specialized over the years in response to identified needs.
Thus, as mainstream schools gradually came to receive moreinstitutional resources and support, the FCSD turned to other importantaspects of development, such as acceptance of disability, personalautonomy, the construction of an identity, and the attainment of a certaindegree of maturity, setting the individual foundation for better socialintegration. The purpose is not to interfere with the school'sresponsibilities, but to concentrate on those aspects which may lead,with specific care, to a better development of the individual, who will

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 26/80
FCSD
26
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
therefore adapt more successfully at school, within family, and insociety.
With this goal in mind, the MSSS has devised a working procedurewhich relies on groups as a specific resource and a form of therapeuticintervention to enhance maturity and integration.
The service focuses on groups because they provide two majorelements which are considered indispensable in the quest for identity,namely, acknowledgement of the disability and confirmation of the greatmany differences within any group of people with DS.
The group introduces the individual to vital peer-group forms ofrelationship ranging from complicity to open confrontation to a desired and
self-built reciprocity; these relationships mould friendships, which play amajor role in the development of the individual
A group of people who share similar personal characteristics (Downsyndrome, in this case) offers all of its members the opportunity to discusswhat it means to each one of them to be an individual with a disability. The

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 27/80
FCSD
27
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
possibility of sharing disability-related aspects of everyday life, such asinstances of clumsiness, rejection, confusion, speech trouble, and so forth,enables individuals to express and acknowledge this side of themselves.
Likewise, group members observe, analyse, and come to realize whateach person is able to do, what each person is like, each member's likesand dislikes, and the different skills and capabilities that they each have. Inso doing they become aware of the fact that there are as many differencesamong them as in any other group of people: children with DS are alsodifferent from each other.
Analysing similarities and differences is a fundamental element for theconstruction of one's personal identity, a fundamental task within a group.To the extent that individuals can consider the ways in which they are similarto or different from other people in the different groups they belong to, theywill gradually be able to discover their own uniqueness.
The Mainstream School Support Service of the FCSD has evolved fromindividual therapy to its current group therapy approach, though individual
treatment is not ruled out if required. Groups are set up according tochronological age and individual needs.
When age and disability are similar, group work enables members tohelp each other and to express more freely what they feel. It also makesthem aware that there are other people with the same or similar problems,so they become less inhibited when talking about themselves.
Groups get together to facilitate creative work and to help memberscope with psychological issues. Members feel that they have to cooperate,to give their own opinions, and so forth, eventually enhancing socialization.The treatment group establishes firm bonds of friendship which improveindividual and mutual understanding of self and may be carried forth toother groups.
Belonging to a group is in itself therapeutic and ties in with the healthieraspects of group membership in everyday life (e.g., sports team, hikinggroup, or class). Doing things in the company of others and sharing in acommon task is rewarding and therapeutic per se.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 28/80
FCSD
28
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
As mentioned earlier, different types of groups are set up according toage and needs:
1.- Groups of children aged 7 to 9 have the following goals:
G To contribute to a better self-understanding of each member.G To develop typical forms of social interaction among children.G To promote the organization and structuring of personal activities
(symbolic play).
2.- Groups of children aged 9 to 13 have the following fundamental goals:
G To understand and accept their own personal situation.G To create strategies and develop resources which will help members
find their place in their immediate social and cultural environment andlearn the rules that apply in this environment.
G To help enhance the communication skills of group members.
3.- Groups of teenagers aged 13 to 16 have the following goals:
G To contribute to the development of each individual's personal identity,including aspects such as age, gender, disability, position within the

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 29/80
FCSD
29
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
family and society, and promote an awareness of age-appropriatereferences.
G To promote personal and psychological autonomy.G
To influence the teenager's view of the future, encouraging areconciliation of possibilities and limitations.
Personal identity - defined as self-image - is first moulded by parentalperceptions of the child within the family structure and marked by the placethe child holds in other people's desires. It is important for children to knowwhom they resemble, to find the roots that make them part of their family,of their genealogical tree. This is difficult for individuals with DS. Very oftenparents say things like: «DS children all look alike but we don't see anylikeness to anyone in the family». This is because parents have troubleidentifying with a son or a daughter with DS, which makes them feel upset.Raising a child is a complex matter, so working with parents as their childwith DS develops and grows is a basic priority of the Follow-up Service.
Once a child has found his or her own identity, accepting theweaknesses and more developed aspects of DS, he or she is in the best

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 30/80
FCSD
30
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
conditions for social integration not out of a desire to be like others or tomake comparisons or focus on the things that he or she cannot do orachieve, but rather from the acceptance of his or her own identity, with its
limitations but also with full awareness of his or her own possibilities.
Peer group work is considered fundamental as it provides a spacewhere children with disability can talk to each other, be listened to, reaffirmthemselves, and say what they think; a space where their personalexperiences can emerge and subsequently, as mentioned, be carried forthto larger groups and society at large.
Group dynamics and methodology allow a child to join different groupsas he or she develops and matures. Group influence has a direct bearingon the capacity to feel at ease, enjoy a pleasing social life, use the group'stherapeutic resources, and solve problems successfully.
One of the main advantages of group work is an overall improvementof interpersonal relationships. Each boy or girl becomes closer to his or herfriends and family and, last but not least, becomes more flexible, in the
sense that he or she can accept and adapt more readily to social andpersonal circumstances, and change his or her initial aspirations of, say,"becoming a doctor".
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 31/80
FCSD
31
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
Once the effectiveness of group work had been established, in 1997the MSSS decided to open group treatment to younger children (5-6 year-olds). At this age, groups consist of twosomes. The reason is the Follow-
up Programme's main aim, which is to facilitate the discovery of the otherperson as an equal. This highly controlled situation helps the child tounderstand, take the other person into account as an individual andsocialize with him or her, learn to share and communicate, and realize thatthere are other children with DS.
The Service also provides individual therapy for children who, forspecific reasons, are unable to adapt to group work.
In addition to all this, the MSSS organizes teaching activities on requestfor teachers and professionals.
It also provides guidance and advice to professionals involved in thechild's or teenager's education. Psychoeducational follow-up takes placewithin the school with all the professionals involved.
Finally, in conjunction with the Programme Co-ordination Departmentand the External Relations Departments, the MSSS deals with inquiriesfrom parents or from school staff, members of Psychological-EducationalCounselling Teams, and professionals from other organisations. FCSDexperts lecture at school faculty meetings in order to discuss what isinvolved in mainstreaming children or teenagers with DS, and how tohandle it.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 32/80
FCSD
32
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 33/80
FCSD
33
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
SOCIAL SKILLS AND PREPARATIONPROGRAMME -PAS-
Development and growth of individuals with disabilities are oftenhindered by a number of matters which often bear no connection withintellectual disability as such or with lack of possibilities or potential.
The concept of disability calls to mind thoughts of retardation orimmaturity; because of this, children with DS are as a rule notencouraged to face the little problems of everyday life, problems theycould probably cope with themselves.
Though training programmes for people with disabilities includeacademic tuition and the acquisition of social habits, these remainincomplete. There is still a gap in terms of teaching people with DS tosolve small everyday problems by using their own practical judgementand creativity.
To this purpose, the FCSD runs a number of services that worktowards a thorough development of the capacities of individuals with DSand other forms of mental handicap. The implementation of the LISMI Actin Catalonia showed that children with DS are able to attend mainstreamschools, a possibility extended to other mainstream social environments.
The expectations of young people with disabilities are changingsignificantly. Although few individuals with DS are in regular jobs today,many young people are getting ready to join the world of mainstreamemployment in the near future.
In order to meet their needs, in 1999 the FCSD set up its SocialPreparation Programme (from now on PAS) for young people withdisabilities. It was rooted in other existing FCSD programmes andactivities, such as:

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 34/80
FCSD
34
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
G The leisure programme.G The groups for ages 16-20 in the Mainstream School Support Service.
The admittance of children and teenagers with DS into regular schoolsis contributing to full integration in society and in the job market as well.However, mainstream schools at present still tend to disregard certainissues that are not very academic but which are essential for people withdisabilities to join the adult world, things like getting ready to have a sociallife and to face everyday problems. These are the points that the FCSD isseeking to develop.
Very often FCSD staff have come across adults with disabilities who areintellectually and academically capable of doing a specific job, but who
have serious difficulties when it comes to accepting rules, getting abouttown, expressing their choices, opinions and problems, or socializing withfellow workers.
Efforts are being made from different spheres so that this type oftraining is included in special programmes in order to support youngpeople, adults, and their families in the process of leading normal lives.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 35/80
FCSD
35
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
A 1985 Organization for Economic Cooperation and Development(OECD) report on the social integration of people with disabilities statedthat job training is unlikely to succeed unless social preparation is provided.
The report also warned that "protracting school even further cannot be asolution. The point is not to provide more of a given type of education, butto change it qualitatively. In this change, special reference must be made tosocial aspects and therefore to autonomy. This sort of education is a slow,gradual process beginning at childhood".
According to the OECD's experts, the transition from childhood toadulthood can be defined by the following characteristics:
G Personal autonomy and acknowledgement of adulthood.G Active or productive life to ensure economic independence.
G Social relationships and active involvement in society.G Role change within the family.
The FCSD relies on the PAS programme to help young people developin these ways so they will grow ready to join the adult world when the timecomes.
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 36/80
FCSD
36
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
The programme offers the group a space for trial and error, a testingground where members can go wrong and later learn from their mistakes,look for alternatives when faced with a conflict so that they can feel control
over their own progress. The overall intention is to help young people feelcapable in ways appropriate to their age so they can claim their rightfulplace within the family and in society.
The programme comprises the following:
1.- Preparation and training to develop social competencies. Courses.
The Service runs specific training courses at three stage levels:introduction, consolidation, and maintenance for young people andadults to develop different skills that enable adult individuals to functionat full capacity in their daily and social lives.
These courses are designed and adapted as the needs of clients whoare joining adult life are gradually identified.
Course examples include Basic Cooking, Independent Travel, MoneyUse and Management, or Use of New Technologies. All courses arerun on a 2-hour weekly basis.
2.- Leisure.
Promotion and encouragement of leisure activities that help enhancesocial competencies in order to increase the chances of individualswith mental disability and provide access to different types of leisureactivities offered by mainstream public services.
Convening of youth and adult groups that receive support to choose,plan and carry out recreational activities in town during their leisuretime.
3.- Participation Area.
Areas are set up in town to encourage settings that lead to socialexchange and relationships.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 37/80
FCSD
37
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
G Punt Cafè. A gathering spot.G Espai Cançons. Singing and learning together.G Promotion of holiday activities.
4.- Guidance and awareness.
G Guidance, advice and cooperation are offered to other institutionsand/or professional specialists working in this area.
G Care and guidance are provided to parents and potential clientsregarding the participation of individuals with disabilities in society.
G The Service's clients are encouraged to join mainstream activities and
monitored in that context.
The PAS programme operates with these goals in mind:
G Preparing members to acquire knowledge of themselves, of their ownneeds and of the role they play within the family and in society,accepting their limitations, but also being aware of their capabilities.
G Helping to develop social skills.
G Helping to develop awareness of the social environment.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 38/80
FCSD
G Developing the individual's autonomy, paying attention to psycho-logical as well as functional aspects.
G
Conveying information concerning the rights and duties of everyindividual as an active member of society, so as to facilitate realparticipation in society.
G Increasing the range of possibilities that people with a disability mayhave, in terms of various forms of recreation, access to existingactivities in the community (municipal centres, public sports, etc).
G
Helping participants to organize their own leisure time.
G Promoting group play and recreation activities, enabling groups ofpeople with DS to experience leisure activities offered to the public atlarge.
G Training volunteers and students in leisure activities and providingsocial preparation of people with disabilities.
G Assisting and guiding families and their family members with DS onmatters concerning social integration.
G Guiding, advising and collaborating with institutions and/or pro-fessionals who work with people with DS.
G Identifying the needs of people with disabilities so as to ensure theirsocial integration.
G Organizing courses and activities to promote independent living.
What is intended is to give training to people with disabilities, to providea realistic experience of how to function autonomously in social andeveryday life.
The PAS service works closely with the other adult programmes (forhousing and job placement) ensuring that clients can interact smoothly withall FCSD services and encounter the same philosophy and approach
38
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 39/80
FCSD
39
everywhere, so that they can mature to become adults and integrate fullywithin society.
The PAS is cross-sectional, involving all FCSD services.
In addition to its professional staff, the PAS service also has theassistance of students and volunteers on a university practicum course.
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 40/80
FCSD
40
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 41/80
FCSD
41
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
COL·LABORA, JOB INTEGRATIONSERVICE
Entering the job market means fully entering the world of adults. Thisis a difficult process for anyone, but even more so for young people withlearning difficulties. For them, as for everyone else, work is a humanactivity undertaken to address personal, economic and social needs.
Work also means coming into contact with a group of people we arenot accustomed to, heterogeneous people with whom we establishrelationships and ways of communicating completely different fromeveryday life.
This new type of relationship is basically co-operation-oriented. Co-operation implies thinking and acting in collective terms, as a groupmember, and it also involves adopting a new role. The workplace mayvery well be the place where the individual with learning difficulties firstabandons a passive role as a service recipient ("I am taught and caredfor by others") and takes on an agent role ("I am producing something").The result of this change of situation becomes apparent and leads toimportant changes not only in activities or behaviour (learning capacity,change of relationships, methodology, specific vocabulary, habits, etc.)
but also in mental attitudes (basically self-esteem). These changes in turntrigger changes in attitude and behaviour which reveal themselves insideand outside the work environment.
Experience in the field of job integration has shown that manymentally handicapped people may find jobs in normal enterprises. Butsuccess in this process hinges on different issues: prior training,individual skills and abilities, learning capacity, personal habits, and thecapacity to adapt to a new environment. It is a slow process, which onthe one hand requires a solid structure to ensure appropriate training and

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 42/80
FCSD
42
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
growth to maturity and, on the other hand, a flexible structure whichshould adapt readily to a wide range of individual capacities.
Based on this perspective, and given that FCSD programs andservices are geared to training and advising people with disabilities intothe mainstream, the Col·labora Job Integration Service, was set up in1995. Col·labora is now a service and it is sponsored by the CatalanDepartment of Labour.
The ultimate goal of this programme is to ensure successfulworkplace integration of people with disabilities in mainstreamenterprises.
The chart below illustrates how the programme functions:
Training Module
NATURALLY SUPPORTED EMPLOYMENT PROGRAMMECOL.LABORA
Advice and Guidance Service
Prevocational Training - Knowledge of oneself
- Training- Choice making- Personal image- Autonomy- Work and the world of work
Job training
Practical work
Integration

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 43/80
FCSD
43
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
The process of job integration consists of two key stages:
G first, training takes place in a normal productive environment, allowing
candidates to become familiar with technologies and workorganization systems that would be impossible to reproduce in aschool or a job-training centre.
G Second, candidates obtain work contracts. This in turn maydemonstrate to employers that people with disabilities are a real workforce.
When a candidate applies for the programme Col·labora, a number
of steps are taken:
G Interview with the family to explain the content of the programme.G Interview with the candidate.G Assessment of the candidate's skills and abilities.G Job training course and job search activities.G Search for employers and definition of targets.G On-site training through worksite experience.G
Follow-up and assessment of work done during on-site training byprogramme staff.
The FCSD professionals responsible for the success of thisprogramme harness natural support by applying a mediation method inwhich they act as brokers between the company and the employee. Theirmain task is focused on making the worker's own characteristicscompatible with those expected for the job. Professionals facilitate theprocess of integration by encouraging an exchange of views andinformation leading to normal conditions for the worker with a disability.
The moment a person with disability begins to form part of a normalworking situation, he or she acquires a new social role (the role of aworker). People with disabilities who behave childishly and immaturely inenvironments that create dependence and overprotection behave quitedifferently when they are placed in an environment with role-basedexpectations. This concept changes the professional role of those whotend to their needs. If the aim is for people with disabilities to take onsocial roles, professionals are no longer there to give assistance, but to

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 44/80
FCSD
44
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
mediate in a process that enables distancing, a requisite for adulthood.Therefore it is no longer a matter of providing care, but of mediating in a
process which will enable candidates to have the necessary space foradult life.
Thus, a mediating methodology emphasizes the importance of naturalsupport, giving advice, guidance and other kinds of information to thecandidate's fellow workers and immediate supervisors, who provide on-the-job training, rather than to professionals not belonging to theworkplace, such as teachers, employment trainers, etc.).
FCSD staff acting as mediators will basically operate in the worker'simmediate surrounding and discuss the following:
G Technical working conditions that may influence the worker'sefficiency to a significant degree.
G Personal relationships with fellow workers. Professionals may takepreventive action, forestalling potential problems, or in case of
conflict, they may advise fellow workers on the best course of actionand provide guidance for the worker to cope with the problem.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 45/80
FCSD
45
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
The mediator works from an objective, logical position that placespositive solutions within reach and thus establishes a pattern of co-operation so that the example set by fellow workers becomes valid
training for the disabled individual.
Over time, we have observed highly positive progress in manycandidates. These improvements specifically lie in the sphere ofautonomy and initiative-taking regarding the technical side of the job,reducing dependence on fellow workers. Likewise, social behaviour andresponses also improve, rewarding the worker with better acceptancewithin the group. Consequently, self-esteem is heightened, together with
an overall improvement of personal satisfaction.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 46/80

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 47/80
FCSD
47
“I‘M GOING HOME”, INDEPENDENTLIVING SUPPORT SERVICE
As Katy Trias wrote when she was designing the independent livingProgramme, «from ancient times, human beings have felt the need to findplaces of their own. Traditionally, however, individuals with mental disabilitieseither remained in the family dwelling or else only had access to institutionalsettings or group homes, probably because of the mistaken belief that they
could not tell the differences or choose among different options, as well asover-protectiveness. While living options evolved considerably over the years,they still consist of external, closed, rigid structures: the individual is expectedto live in a non-chosen community setting where the rules are imposedexternally, rather than self-imposed.
After centuries of confinement to institutions, group homes of varyingsizes and degrees of comfort were set up, usually in the outskirts of townsand cities. Then came sheltered apartments: functional housing with a smallnumber of residents who all share some of the housework. Developed as aresult of the drive for more autonomy for individuals with disabilities, the latterare meant to be “like” a real home. Some of them come pretty close, but theyare not the real thing. Because of their structure, there is considerableexternal oversight which in no way respects individual independence. Often,residents do not even have a say in basic choices affecting their livesdecisions that most people take for granted, such as where they want to liveand with whom.
Now that many of our young people have attended mainstream schools,are employed in mainstream workplaces and enjoy social integration, theirparents and relatives do not wish them to be confined within group homes ofany sort, but would rather have them enjoy a life that is closer to their ownideal choice. This does not really constitute a new “model” – rather than ahousing model or a housing option, this new approach is about respectingevery individual’s wishes, about pursuing a way of life that tries to fulfill thosewishes with the necessary support, about making different lifestyles possible.
This new approach is a valid one for any person with a disability, for anyonewho wants to pursue the “dream” of living in a home of their own.
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 48/80
FCSD
A person’s home is not just a place, a bit of space. Home is like a nest;it is where we feel safe and at ease; the place we have chosen anddecorated ourselves; above all, a place where all rules or restrictions areself-imposed. We each have control over our own space, our own lives;we decide who may enter or leave our home and what may happen insideit. Home is, perhaps, the place where we feel most at ease, where wehave the things that we want or like, and the people we love. This is abasic necessity for everybody, including persons with mental disabilities».
With all this in mind, FCSD set up its Programme for IndependentLiving to offer individuals with disabilities the chance to live “in a home oftheir own”, including any support or assistance necessary to ensure
safety and peace of mind. The Programme is therefore person-centeredfrom the start; the whole process is driven by the client.
Traditional residential services, including many programmes in thiscountry, are designed to provide support and housing as a package;when the support provided turns out to be inappropriate, clients may bedeprived of their home, as well. FCSD therefore believes that housingshould not be operated by the same body that provides the support; onlyif the person with a disability has direct ownership or rental can he or she
be sure not to have to move against his or her will. This is also the onlyway to create a sense of “ownership” through having to pay forhousehold expenses, decorate the rooms, etc.
This was a ground-breaking programme in Catalonia. It’s innovative,pioneering quality is highlighted by the fact that the individual with adisability is the main actor in the whole process. At the same time, it relieson the proven experience gained in similar programmes in the US(“Home of your own”, originally launched by the University of New
Hampshire and now catering for over 1500 persons in a number ofstates) or the UK (the Paradigm scheme), not to mention extensiveliterature on the subject.
In 2001, the programme was launched experimentally. It has nowbecome a full-fledged FCSD Service supported by the CatalanDepartment of Social Welfare, which passed Order 6/2002 regulatingand acknowledging this form of support as a way to provide home andlifestyle choice for individuals with disabilities. This legal text also lists allcurrent legislation concerning individuals with disabilities (LISMI and Act21/87) and the regulation of social services in Catalonia (the Catalan Act
48
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 49/80
FCSD
49
regulating the governance and registration of Social Services) and is afurther step along the road to full social integration.
The Service is intended for persons with mental disabilities; specifically, inkeeping with the new AAMR definition of mental retardation, it is for adultpersons (over 18) with “significant limitations both in intellectual functioningand in adaptive behavior as expressed in conceptual, social, and practicaladaptive skills.”
Throughout the planning and followup process, the programme isunderpinned and inspired by its pursuit of quality of life as defined by theindividuals themselves, which is ultimately the same as quality of life for any
ordinary citizen. This informs the principles underlying intervention anddetermines which indicators will be used during the followup process. Qualityof life is a multidimensional concept that may be defined by consensusamong those who are close to the person who is the recipient of the service;it entails both meeting basic needs and affording the same opportunitiesavailable to any other person setting life goals or objectives.
Mental disability (equal to or greater than 33%) has to be rated officiallyby a public Assistance Center for People with Disabilities before the person
can use the service. Additionally, the individual him or herself must make therequest and this must have the support and approval of the person’s familyand/or legal representatives.
The client must also be able to have access to a home of his or her own,whether owned or rented in their own name. Legal title to the premisesmeans that control of the home will not be lost. In order to avoiddiscrimination, no specific socioeconomic indicators have been set asaccess criteria; the point is that the individual and his or her legal
representatives should be able to manage the expense of keeping up theirhome. The Service can advise prospective applicants on this matter.
The third and last requirement is for the client to agree to set up a Circleof Trust, a number of key persons who will organize around him or her toprovide a web of relationships and whatever support the circle agrees isnecessary. The Service acts as facilitator and matches needs to coverage ofthose needs to ensure the utmost safety and welfare of the client. The Circlewill never decide or choose in place of the recipient, who will have nominatedand accepted each Circle member. The Circle meets at varying intervals inthe person’s place of residence.
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 50/80
FCSD
The criteria used to assess the person’s functioning and the influence ofdisability on the overall set of abilities and skills displayed will not provide asingle or exclusionary profile of the client. Steps must always be taken toensure that needed support is provided, wishes fulfilled and personalexpectations met in full comfort and safety under the Personal Care Plandeveloped. Considerable importance is attached to personal and contextualattitudes linked to self-awareness of personal status, requests for andacceptance of support tailored to specific individual needs, and respect andsupport for the person’s own expressed or consensus-inferred decision.
G Methodology
The work of planning home support and developing action plans iscarried out by the team in five main stages:
1.- Client and family members are interviewed to explain how the Serviceoperates and record every family member’s agreement to carry through theprogramme.
2.- Client is interviewed alone or with one trusted companion to initiate
information gathering, emphasising the following points:
G Preferences.G Problems.G Things they find difficult.G How they learn.G What kind of help they receive.
This may entail a number of interviews at different key places (place ofwork, current neighbourhood, neighbours’ homes, etc.).
Depending on the person’s communication skills, interviews may requirethe presence of an interpreter, a family member, or a caregiver who knowsthem well.
3.- Preparing a place. Assessing socio-economic conditions (to decide onpurchase or rental and identify available resources). Designing the new
home. While the Service may provide assistance in finding a suitable place,it cannot own the place itself.
50
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 51/80
FCSD
51
4.- Designing support. All necessary meetings are held in the person’s placeof residence, and all planning and decision-making is person-centered.
5.- Moving in. The plans are set in motion, the Action Plan is confirmed andthe Follow-Up stage is launched after checking on point such as:
G The new place (are adaptations needed?).G Furniture (does anything need to be changed or adapted?).G Where things go.G Filling the pantry (food).G Home decor.G Rules for survival, both in terms of safety (use of gas, electricity, water,
locking doors and windows, etc.) and in terms of hygiene (personal care,food handling, clothes care, etc.).
6.- Adapting to the new situation and establishment of regular support basedon the person’s new routines and wishes.
This launches lifelong follow-up. A person’s needs will fluctuate over time,waxing and waning back and forth; support must therefore be flexible and
resourceful. The group has a key role in regularly analysing and reviewing thecurrent situation.
Support is structured following a number of basic principles on the basisof a plan that is tailored to the person’s situation and which should not be tootechnology-oriented.
Specific planning, implementation and follow-up stages are thus definedfor the support element.
G Onset: This begins with the person’s application to join the programme.Includes whole-person assessment, autobiographical data collection toidentify personal history, identifying personal goals and preparing fortransition. This stage involves a number of interviews with the client, visitsand interviews with persons who have a key role in his or her life, and theforming of the Circle of Trust.
G Transition stage: Comprises original home location and preparationdecisions and support, getting to know the new setting (neighbourhood),local resources, and all work done prior to moving in.
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 52/80
FCSD
G Intensive support stage: As soon as the person moves into the newhome, intensive support is allocated to ensure maximum safety and
backup and help design an appropriate Personal Assistance Plandepending on how he or she is adapting and functioning in the newenvironment.
G Regular support stage: After initial adaptation and once new habits androutines are in place, support is gradually phased out down to the levelset forth in the Personal Assistance Plan.
The stages in the process do not have a predefined duration, but dependon the person’s circumstances and requirements.
Critical stages must be planned for: namely, any foreseeablecircumstance following the onset of the regular support stage that maychange the person’s way of life and require intensive work to redesign thePersonal Assistance Plan.
In addition to the Service’s formal provisions and the hazard prevention
mechanisms agreed for each person, an agreement has been entered withthe Red Cross remote assistance service and the Provincial Council ofBarcelona to ensure round-the-clock emergency assistance tailored to ourclients’ needs and situations.
52
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 53/80
FCSD
53
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
DOWN MEDICAL CENTRE
Ever since John Langdon Down first described the syndrome that wasto bear his name, in 1866, there has been remarkable interest in associatedmedical problems. In the second half of the twentieth century, the cause ofthe syndrome was discovered – namely, the extra chromosome 21.Molecular cytogenetic studies of chromosome 21 DNA have been under waysince the 1990s.
DS cannot be regarded as an illness, though it is true that people with DShave a greater tendency to suffer from more or less serious health problems,especially if not diagnosed or treated at an early stage. They are known tohave a higher rate of congenital malformations, especially heartmalformations; later in life, there is also a higher rate of metabolic diseasesand other conditions. The physical traits and psychological factors most oftenassociated with DS have also aroused great scientific interest.
The FCSD has always paid particular attention to the medical aspects ofDS, since good physical health is necessary to begin a proper educationalintervention. For this reason, the Down Medical Centre (DMC) was createdin 1987. Although the first Service founded by the FCSD was the Centre forChild Development and Early Intervention, there soon emerged a real needfor a Health Programme to provide information and ensure full medical care,at a time when medical information about this syndrome was very little. ThisCentre was the first in Spain to give specific medical care to people with DS.It started out with few physicians and has undergone many changes,
especially in terms of services offered to the public and in the number ofpatients. Currently, it is considered a major health care centre for people withDS, both on account of the number of services offered as for their quality. Itsmain function is to watch over the state of health of people with DS, forpreventive purposes. It offers treatment in 18 medical specialities. Well over1600* persons have been treated, most of them from Catalonia. There areeasily over 2,000 appointments a year.
(*2003 data)

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 54/80
FCSD
54
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
The DMC provides specialized medical care in the following areas:
Cardiology Neurophysiology DermatologyPediatric Dentistry Endocrinology PaediatricOphthalmology Dietetics and Nutrition Adult OphthalmologyOral Health adult Orthodontics Genetics
Ear, Nose and Throat Gynaecology PaediatricsInternal Medicine Clinical Psychology Paediatric NeurologyPsychiatry Adult Neurology Orthopaedics andOral health pediatric Traumatology
In addition to providing health care, the DMC is involved in disseminatingmedical information. In 1986 it launched the still-ongoing publicationSíndrome de Down. Articles i Resums Científics, now expanded andreformatted under the new masthead SD.Revista Mèdica Internacional sobre
la Síndrome de Down/DS. International Medical Review on Down Syndrome,to present and update current knowledge of medical aspects of DS and keepthe reader up to date on the most promising developments in basic science(molecular biology and genetics) and everyday medical practice. It alsoaddresses psychological and educational aspects of practical interestbecause they tie in with medical concerns.
Clinical research is also encouraged by the DMC, which has beendirectly and indirectly involved in a number of research projects, especially
since the 1993 TV3 Telethon. Moreover, the DMC serves a teachingpurpose, targeting both health care professionals and parents or other

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 55/80
FCSD
55
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
individuals with an interest in the subject. Its research mission has led it to linkup with hospitals, universities and other institutions.
From the outset, the DMC was set up for maximum effectiveness.Pioneering medical centres caring for people with DS at the time of itsfoundation were reviewed, and the original medical staff came to aconsensus and approved an annual checkup schedule involving differentspecialists and varying with patient age. This was the Health Programme(PS) first published in Spain within the Butlletí de la Societat Catalana dePediatria (1987, 47:33-41), which now covers patients from birth or DSdiagnosis through life.
FCSD HEALTH PROGRAMME FOR CHILDREN AND ADULTS WITHDOWN SYNDROME AND NO OTHER ASSOCIATED CONDITIONS
The programme is designed according to universally acceptedguidelines for its stated purposes. It is regularly updated in the light ofrelevant scientific developments and its own accrued experience,currently numbering over 1650 cases since 1987. Implementation of thisschedule together with the early stimulation programme ensures that
every participant with DS will reach his or her highest potential.The health programme provides basic prevention on a separate basis
for children and adults, and is fleshed out with whatever additionalmonitoring is required if any other condition is identified.
I – HEALTH PROGRAMME FOR CHILDREN AND TEENAGERS
This comprises all the routine checkups that must be made byspecialists from the first pediatric assessment at the DMC to adulthood(18 years).
1) BIRTH TO THREE MONTHS
a) GeneticistG DS diagnosis. Chromosome study using karyotyping or fluorescence
in situ hybridization (FISH) to determine whether it is a regular, mosaic
or translocation trisomy. Family assessment and counselling ifrequired.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 56/80
FCSD
56
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
b) PaediatricianGeneral examination of the newborn, with a special emphasis on:
G Screening for congenital cataracts.G Screening for potential congenital malformations, both external and
internal.G Hearing examination.G Thorough checking for metabolic disorders, particularly
hypothyroidism.G Screening for congenital hip dislocation.
c) CardiologistG Forty to fifty percent of DS babies have congenital heart disorders, so
a full range of ECGs and other tests are required. The need for
medical treatment or surgery is assessed.d) Paediatric NeurologyG Examination of muscle tone and neurological function.G Co-ordinating action with the Early Intervention Programme and other
professionals.
Other tests:G Karyotyping -FISH-.G Metabolic screening.G Cardiac assessment.G Blood work-up.G Abdominal assessment.G Others as required.
2) 3-12 MONTHS
a) PaediatricianExamination of the baby, with an emphasis on the following:G
Assessment of general condition and nutritional status.G Genitals; check for undescended testes.G Initiation and follow-up of the adapted immunization schedule.G Monitoring of immune status due to a greater tendency to develop
infections, particularly respiratory infections.G Assessment of skin moisture and flexibility.
b) Paediatric ophthalmologistG Diagnosis of eye alterations if previously undetected.
c) Ear, Nose and Throat specialistG General check-up. Children with DS seem to suffer more often from
middle ear infections and wax plugs.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 57/80
FCSD
57
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
d) Paediatric NeurologyG Assessment of psychomotor development.
Other tests:G Haematological analysesG Anti-HB antibodies (post vaccine)G Check of thyroid function
3) 1-3 YEARS
a) PaediatricianAnnual assessment of:G Growth, weight and head circumference according to the specific
tables for DS published by the Fundació Catalana Síndrome deDown.G Health and hygiene habits.G Compliance with immunization schedule.G Thyroid and haematological functions (due to potential hypothyroidism
and a higher likelihood of certain forms of leukaemia).G Compliance with immunization schedule (immunoglobulins, etc)
b) Paediatric ophthalmologistG Annual check-up to screen for errors of refraction (nearsightedness
or farsightedness, etc.).
c) Ear, Nose and Throat specialistG Yearly check-up looking for disorders, using complementary tests
such as brainstem evoked response audiometry or tympa-nometry.).
d) Paediatric NeurologistG Assessment of psychomotor development.
e) OrthopaedistG Control of walking ability and use of both feet.G Screening for potential joint dislocations.
f) DentistG Teeth: routine prophylaxis.
Other tests:G Haematological, biochemical, thyroid, and immunological tests,
biennial.G Assessment of development.G IgA anti-tissue transglutaminase or anti-endomysium (after 18-24
months).

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 58/80
FCSD
58
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
4) 3-10 YEARS
a) PaediatricianAnnual assessment of:
G Growth, weight, and skull circumference, including checking forobesity.
G Health and hygiene habits.G Compliance with immunization schedule.G Thyroid function, biochemistry, and blood work-up.
b) Paediatric ophthalmologistG Annual or biennial eyesight check-up.
c) Ear, Nose and Throat specialistG Yearly or biennial hearing check-up, including associated structures.
d) Paediatric NeurologistG Assessment of neurological development.
e) NeurophysiologistG Assessment of sleep disorders.
f) OrthopaedistG Assessment for atlantoaxial subluxation.G Check of walking ability.
g) DentistG Teeth: routine prophylaxis.G Orthodontics: as required.
h) PsychologistG
Monitoring of childhood development.Other tests:G Cervical spine study.G Haematological, thyroid and immunological clinical tests. Annual or
biennial.G IgA anti-endomysium or IgA anti-tissue transglutaminase test (if
previously not studied or repetition at 6-7 years).G Assessment of development.G Hearing examination.G Sleeping Polysomnography.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 59/80
FCSD
59
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
5) 11-17 YEARS
a) PaediatricianAnnual assessment of:G Health and hygiene habits.G Thyroid function.G Routine check-ups for children of the same age.G Compliance with immunization schedule.G Weight and growth
b) Paediatric ophthalmologistG Eyesight check-up every two years.
c) Ear, Nose and Throat specialistG General hearing check-up every two years.
d) Paediatric Neurologist (<14years old) Neurologist (>15 years old)G Assessment of neurological development.
e) OrthopaedistG Regular checks of atlanto-axial joint and others.
f) GynaecologistG Assessment of sexual development.
g) PsychologistG Regular check through puberty and adolescence.
Other tests:G Cervical spine study.G Haematological and thyroid clinical tests annual or biennial.G Assessment of development.G
Hearing examination.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 60/80
FCSD
60
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
II – HEALTH PROGRAMME FOR ADULTS
Comprises routine check-ups after 18 years old.
a) InternistAnnual assessment, especially of the following:
G Weight (obesity).G Health and hygiene habits.G Thyroid function.G Development and sleep issues.G Immunization status (Td, influenza, pneumococcal).
b) PsychologistG
Yearly examination.c) NeurologistG Neurological assessment: every 5 years up to age 40, then annually.
d) OrthopaedistG Regular general check-ups.
e) Other annual check-ups:G DentistG Gynaecologist
f) Other 2-yearly check-ups:G OphthalmologistG Endocrinologist
g) Other 5-yearly check-ups:G Cardiologist
Other tests:G Haematological, thyroid and immunological clinical tests, as requiredand evolution.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 61/80
FCSD
61
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
III- FREQUENTLY-NEEDED MEDICAL SPECIALTIES NOT
INCLUDED IN THE PREVENTIVE MEDICINE CHECKLIST:
G Dietetics and NutritionG EndocrinologyG DermatologyG GastroenterologyG PsychiatryG OrthodonticsG Haematology
As far as research is concerned, the fundraising telethon campaignorganized by TV3 (1993 La Marató de TV3), aimed at securing a better
understanding of chromosome 21 dysfunction, and preventing andalleviating the effects produced by the excess chromosomal material,enabled the FCSD to compile the first specific database on DS. Thisdatabase consists of 17 groups of data, one for each speciality. Theyinclude all the relevant medical data of the more than 1,600 case historiesof the Down Medical Centre (CMD)*. This database has proven to be ahighly valuable tool to further knowledge of some medical conditions andthus enable preventive action for specific health problems. It is theworld's largest DS-specific database of its kind, and has thus drawn theattention of other institutions related to DS. It has also enabled the FCSDto plot the first specific growth charts for DS in Catalonia. With datagathered over twelve years, the FCSD was able to chart normal growthcurves for DS, distributed by age and gender. Weight, height and skullcircumference are measured regularly up to age 17. The data are splitinto two groups aged 0-3 and 3-17 respectively. These charts are ofgreat value for paediatricians and can be requested free of charge fromthe FCSD.
With the remainder of the funds obtained from the La Marató de TV3telethon, the FCSD sponsored the following research projects:
G Gene mapping of various regions of chromosome 21. Various genesin the 21q11.2 region have been identified, including DSCR1 (thefirst specific gene in this region leading to DS traits), MNBH, c21-LRP, WRB, SH3BGR and others. In addition, genes from otherregions which may be directly or indirectly linked with DS have been
identified, as well as some of the proteins they express.
(* 2003 data)
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 62/80
FCSD
62
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
G Potential indirect diagnosing of chromosome error in male andfemale germ cells has also been studied. Sperm testing using FISHand detection of the extra chromosome in the 21 pair have been
done for parents of children with and without DS. It has been shownthat some parents of children with DS tend to present errors in thesperm cells. This study may allow diagnosis of chromosomealterations in sperm prior to in vitro fertilization.
The short term useful projects are those ones; also there are othersthat should also be mentioned:
G The database was also used for a comprehensive study of the most
frequent disorders affecting adults with DS; the case histories of 200people kept at the CMD were used as a sample. Through this study,prevalence rates have been identified for a number of health problemsthat were not previously apparent.
G A comparative study was done for over 270 children and adults withDS using new technologies such as fluorescence in situ hybridization(FISH), molecular studies (DNA), PCR and CGH. The frequency ofappearance of certain variations in the structure of chromosome 21and of other specific cases of DS has thus been established.Surprisingly, some cases do not present trisomy but do present DSfeatures. Phenotype/genotype correlation was also studied.
G Microsatellites were used to study 151 cases of DS. This made itpossible to determine the paternal or maternal origin of the extrachromosome in the 21 pair, and at which phase of cell division theerror occurred.
G Transgenic animals with chromosome alterations in the regionhomologous to where the extra chromosome appears in DS were
bred and studied.G There was a study of lipoprotein E4, thought to foster trisomies.G Studies were also made of genes and proteins, such as GAPDH, aB-
chrystalline, Bcl-2 and Bcl-xL, which play an active role in cell divisionand cell death.
G The spatial distribution of chromosomes within the cell nucleus wasstudied, along with its active role in the mechanisms of chromosomenon-separation (nondisjunction) and its parental origin.
G The cause of nondisjunction of chromosome 21 was determinedusing new technologies in a high-prevalence population; phase ofonset was also determined.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 63/80
FCSD
63
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
More recently, research collaboration agreements have been reachedwith a number of university and foundations.
G
The effects of Donepezil as a first-line treatment for individuals with DSand Alzheimer's disease are being investigated. This drug has beenshown to have beneficial effects for some dementia cases.
G A study of adult DS brain metabolism assessment using PET (PositronEmission Tomography) was performed and the presence of areas withlowered metabolism was demonstrated.
G Study and assessment of visual capacity and quality in adults with DS.G A study of celiac disease in children with DS, a frequent co-occurrence
in which the body does not tolerate the gluten found in certain types of
cereal.G A study of upper GI tract motility, especially of the oesophagus, in adults
with DS.G An assessment of sleep disorders, a frequent occurrence in children
with DS.
Besides the services mentioned above, the Down Medical Centre offersparents of children with DS every manner of advice and support, so that theymay make the necessary decisions for the sake of their child's physical andmental health. Therefore, one of the DMC's special services is ClinicalPsychology. This service includes treatment for people with DS and theirfamilies.There are many reasons why parents come for an interview, andthese vary according to age and personal or family circumstances. Someparents seek advice on particular issues of their child's development (schoolintegration, trouble relating to others, when and how they ought to tell theirchild about the disability, age of puberty and adolescence, sexuality, wish forparenthood, etc.). Other cases may call for a psychological diagnosis, in
order to assess the need for psychotherapy, often for personality orbehavioural disorders requiring treatment. Finally, siblings, parents orgrandparents may require family counselling and guidance in some cases.
Needless to say, the Clinical Psychology service operates in closecollaboration with the rest of FCSD services. If a child or young persontaking part in any FCSD programmes (PAS, Job Integration, MainstreamSchool Support Service, etc) shows any signs of disorders which call fordiagnosis and treatment, they are referred to the Clinical Psychology
Service for care.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 64/80
FCSD
64
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
DMC professional staff also work closely with each other. If aspecialist deems the intervention of another specialist necessary, he orshe will immediately contact this specialist either personally or in writing,in order to care for the physical and psychological well-being of theperson.
Finally, the DMC promotes general information for parents andteachers alike. This is done by organizing lectures regularly on variousaspects of DS. Research is another major concern, which is promotedby awarding prizes and organizing scientific sessions.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 65/80
FCSD
65
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
TUITION AND TRAINING
One of the aims of FCSD is to serve as a reference centre forprofessionals, parents and family members. Therefore, acting as aResource Centre, FCSD runs a Tuition and Training Service open tofamilies, professionals and people interested in DS issues. The team ismade up mostly of professionals working in the FCSD and professionalsfrom other institutions specialized in a specific issue so as to ensure the
best quality in any activity organized concerning DS.
PROFESSIONAL TRAINING ACTIVITIES
Courses and seminars are organized and taught every year on a regularbasis.
Open Classroom. This is a basic training course, intended to bringtogether all professionals involved in the school integration process.The course aims to give information and training on the needs that achild with a disability may have in a regular school.
Case Discussion Seminar - Guidance and Counselling. This seminaruses case studies contributed by course participants to assess the
variety of psychological and educational techniques that may be usedto address problems in different stages of schooling. This course isopen to teachers, educationalists, psychologists and professionalsworking in ordinary schools or special education schools. Eachparticipant presents a case, which is then discussed and analysed froma theoretical and practical perspective. References and material areprovided for each case as required.
Seminar on catering for diversity in secondary school (grades 7 to 10).Secondary-school professionals discuss their experience regarding
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 66/80
FCSD
66
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
children with special educational needs (NEE), the organization of acurricular adaptation unit (UAC), integration, and so forth.
Seminar on language in children with DS. Ways of fostering languagedevelopment in school are discussed. The theory of languagedevelopment is used as a framework for discussion and analysis oflanguage in the child with DS in order to come up with resources andstrategies which may be useful for everyday school life.
Since 2002, this seminar is also being taught as an open learningcourse hosted by the Universitat Oberta de Catalunya (UOC).
International Conferences. FCSD regularly organizes conferences onDS. They are basically a means of disseminating information on DS-related matters. Up until 1997, all conferences dealt with both medicaland psychoeducational issues. Due to the enormous interest of thesetwo fields, it was decided to separate them by alternating the contents;separate conferences are now held on alternating years since 1997.Thus, the International Congress on Chromosome 21 and MedicalResearch on DS was held in 1997. The Congress allowed scientistsand DS specialists to exchange information and discuss the latestadvances in DS. Participants included a wide spectrum of experts,from laboratory researchers to specialized physicians.
In addition to the regular courses and conferences outlined above,other teaching activities are organized by the FCSD as needs or
interest arise.
PUBLICATIONS
SD. Revista Mèdica Internacional sobre la Síndrome de Down. DS.International Medical Review on Down Syndrome. A pioneeringpublication intended for pediatricians, other physicians and other
interested individuals. It is regularly sent to all pediatricians in Spainand to other physicians, professionals or parents on request. Total
8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 67/80
FCSD
67
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
circulation is 16,000 copies, 4,000 in Catalan and 12,000 in Spanish(including individual subscribers and Down Syndrome-relatedassociations in Latin America). It is available online from 2002 in
Catalan, Spanish and English and indexed in EMBASE/ExcerptaMedica and Índice Médico Español (IME).
Its chief interest lies in the fact that, as well as being themouthpiece of the FCSD Down Medical Center and providinginformation on its activities and methods, it routinely includes twooriginal medical papers (one research study and one case review)along with one article covering issues of psychology, education, and
existing models for mainstreamed life choices. The underlying idea is toinclude both organic and psychological aspects to present the personas a single, whole entity.
PRACTICUM TRAININGS
Practicum agreements are in place with the following universities:
G University of Barcelona. Educational Science Division of the Schools
(*2003 figures)

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 68/80
FCSD
68
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
of Education and Psychology. School of Library Science andDocumentation and School of Psychology.
G
Autonomous University of Barcelona. School of Educational Science.Social Educator Diploma. School of Education and School ofPsychology.
G Universitat Ramon Llull. Blanquerna School of Psychology, EducationScience and Sports. Fundació Pere Tarrés (operator of the UniversitySchools of Social Work and Social Education of Universitat RamonLlull). Social Education Diploma.
G Universitat Oberta de Catalunya (UOC). Psychology, Psychology &Education, and Education Science.
Guidance and support are provided for research papers(dissertations, projects, etc.) produced by schoolteachers, universitylecturers and students in Catalonia, in Spain, or abroad.
WEBSITE
The FCSD has a website that is highly dynamic and open to userparticipation. Users usually ask about medical and psycho-educationaltopics and come from all over Spain and Latin America.
FAMILY-ORIENTED ACTIVITIES
Parent encounter group: For parents of people with DS, facilitated bytwo therapists and designed to foster sharing and thinking around thepersonal experience of having a child with a disability.
Seminars for parents:, A variety of theoretical content is taught andopinions are exchanged among parents of people with DS.
Sibling group: For siblings of children with DS to share their personalexperiences and perspectives.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 69/80
FCSD
69
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
LECTURES
The FCSD regularly holds lectures and talks for professionals andfamily members. At least three lectures are held during the school-year,two of them health-care-oriented and one focusing more on psycho-educational aspects.
Lectures and talks on issues related to DS or disabilities at large arealso given year-round at schools, institutions, workplaces, etc., onrequest

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 70/80
FCSD
70
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 71/80
FCSD
71
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
EXTERNAL RELATIONS AND NEWPROJECTS SERVICE
The Service for External Relations and New Projects was created
in 1998 to develop FCSD commercial and marketing activities; to co-o
rdinate, structure and launch awareness campaigns; to facilitate co-
operation with other institutions; and periodically to evaluate the needfor new projects. This Service operates jointly with General
Management and works in close co-ordination with professionals in
other FCSD services.
The External Relations and New Projects Service manages the
following activities:
1.- Awareness campaigns: regarding the right to normalization and full
social integration of people with DS and other disabilities, using:
G Internet vehicles (website, banner ads).
G TV (spots and special programmes).
G Radio (advertisements and interviews).
G Press (advertisements and articles).
G Public and private official ceremonies (promoting the services of the
FCSD).
This new marketing policy serves a twofold purpose. Firstly, from an
informative and practical point of view, it is aimed at making the public
more aware of the aims and philosophy behind the FCSD. Secondly, in

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 72/80
FCSD
72
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
terms of commitment, it is aimed at arousing solidarity for our cause,
collecting funds for financing new projects, and obtaining volunteers,
assistants, and students willing to collaborate in some of the FCSD's
activities.
2.- Publishing service: This service aims to use publications to promote
new trends found in educating children, youth and adults with
disabilities, as well as psychological, educational, medical and genetic
advances. In order to achieve its aims, this service encourages FCSD
professionals to publish the analysis and methodology used in everydaypractice. Foreign-language articles which may be of interest to are
reviewed and sometimes translated and published. In addition, the
proceedings of all the International Conferences regularly organized by
the FCSD are always published.
3.- Encouraging mutual collaboration: with either local, national or
international institutions so as to coordinate joint activities. Some ofthese activities are:
G Joint promotion of campaigns to increase awareness and collect
funds.
G Organization of training courses for families, professionals or
institutions, according to demand. Institutions may be in Spain or ina foreign country.
G Promotion and fund-raising for research projects which may be of
interest to physicians, geneticians, educationalists and
psychologists. Demand has increased considerably since the 1993
TV3 telethon La Marató de TV3.
G Co-publishing of the most recent studies in the field and
methodological aspects considered most relevant to our aims.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 73/80
FCSD
73
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
4.- New Projects: the main aim of the service in this regard is to run
preliminary studies and ultimately design new services, research projects
and dissemination schemes in order to strengthen the capabilities and
technical knowledge of FCSD. New Projects operates in close
coordination with the Programme Coordinator.
Its functions are:
G Studying FCSD research needs.
G
Investigating new ideas which may lead to the creation of newservices, research projects, and dissemination schemes.
G Establishing and supervising FCSD information channels, library
procedures, and so forth, to keep FCSD up to date on technical
matters.
G Supervising the development of methods and procedures for report
creation, documentation, and course organization.
G
Establishing institutional relationships.
One of the functions of FCSD is to be on the alert to understand the
needs of the families or professionals. Through joint studies between
the Programme Co-ordinator and the corresponding service, FCSD
investigates and assesses the need and the practicability of starting a
new project by following a specified procedure: needs study, feasibility
study, economic study, and search for a sponsor.
5.- Information Service: The prestige earned by FCSD over several years
since its creation has led it in recent years to become an important point
of reference in Latin American countries for many newly created
institutions, for parents who have just had a baby with DS, or simply
parents seeking specific advice. To meet their requirements, the
International Relations service was created within this department to

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 74/80
FCSD
74
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
provide information to anyone in need of it. The web site has brought on
a spate of new inquiries.
Much of this demand comes from Latin America. Information seekers
range from people wishing to create a Centre or an Association for
people with DS, or simply individuals seeking specific advice for their son
or daughter. Other inquiries come from professionals, students and family
members. There are many requests for general information about the
FCSD, about specific aspects of DS and about intervention types and
methodological issues. Meetings are held every quarter, inquiries aregrouped by similarity and answered, and in some cases, they are dealt
with in person when parties spontaneously choose to come to us.
Many inquiries are received via e-mail, largely from Latin America and
from other parts of Spain (Galicia, Andalucía, the Canary Islands, etc).
Last but not least, FCSD wishes to establish and maintain a bond withthe families of people with DS, to learn about their experiences,
concerns, goals and needs. For it is they who drive and motivate our
actions, our striving for change and the new services FCSD is constantly
offering. Finally, the disinterested help offered by many parents towards
our common cause is deeply acknowledged.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 75/80
FCSD
75
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
BEGOÑA RAVENTÓS DATA CENTRE
The Begoña Raventós Data Centre (BRDC) specializes in all formsof disability. It holds an updated stock of 4,909 books, 5,262catalogued and updated magazine articles, 284 audio tapes, 956videotapes, 97 subscriptions to specialized journals, and 4,280 articlesfrom other catalogued sources (2003 data). For its size and wealth ofinformation on DS, this centre is unique in Spain. It began operating in1985 as a donation made by Mr. Jesús Raventós of the Begoña
Raventós Information Service book collection.
Since then, the collection has been constantly expanded andupdated to include audio, video and other media. The catalogue hasbeen automated to increase points of access and speed up searches.Relevant articles from reviews are constantly selected and indexed foreasy public access. For people who live far away, or who find theopening hours unsuitable, a special service arranges for information to
be sent directly. All these activities are backed up by disseminationactivities to make people aware of existing resources. The Centre isalso in constant contact with associations, federations, academicinstitutions, hospitals, etc.
Since the Data Centre complements the materials available inuniversity libraries, university lecturers regularly refer their students tothe centre. For this reason, it receives inquiries from people studying to
become teachers, nurses, psychologists, educationalists, speechtherapists, physiotherapists, or social workers, as well as professionalsand school psychologists team preparing lifelong training sessions orseeking disability-related information on issues pertaining to school,employment, psychology, medicine, law, personal development, leisure,social services and assistance, etc.
Objectives
G To provide specialized information in order to support research andthe daily work of professionals, parents, and students in the field ofdisabilities.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 76/80
FCSD
76
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
G To contribute to the initial and continued education of students andprofessionals.
G To support FCSD activities and courses: the Master's Degree in
Early Intervention, the Open Classroom, conferences and seminars.
1. The Begoña Raventós Data Centre collection
As mentioned earlier, the centre holds over 5,000 monographsspecializing in the issue of disabilities.
The Periodicals section stocks over 250 different journals andbulletins, 100 of them currently subscribed to. Besides, many relevantarticles from journals are recorded and catalogued; there are over3,500 articles currently available from the centre 's database. A generalpress section collects articles printed in Spanish daily newspaperssince the late 1960s.
Also, more than 5,000 pamphlets including conference abstracts,
offprints, etc. are recorded and catalogued.
The video library stocks over 300 different videotapes which may beviewed in the library or borrowed for use as a visual aids for talks,debates, special training or other activities.
There is also a collection of audiotapes which record theconferences and seminars organized by FCSD.
Other specialized items include posters, charts and theprogrammes of seminars and conferences. The information containedin these items has been collected over more than 20 years.
The Centre obtains most of its material through purchase, exchangeor donations. The Centre's relationship with international institutesinterested in the issue of disability enables it to keep abreast of thelatest material published in this field, as several publications are notdistributed through the normal channels and are produced in smallvolume.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 77/80
FCSD
77
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
2. Services for the users
The BRDC is open to the public: visitors have free access to the
library and may also use the photocopier, borrow tapes, researchmaterial, find bulletins listing abstracts or recent acquisitions andsearch the online catalogue over the Internet.
3. On-site browsing
The BRDC is open to anyone interested in disability. Material isavailable for direct browsing. Videotapes can be watched, audio tapes
heard, and there is even an online service for Internet-based cataloguesearches.
The catalogue is automated for easy searching. All material listed inthe catalogue are available in the centre. Searches cover all printedmaterial: books, articles from reviews and bulletins. Documents andinformation can be located either through standard bibliographicreference searches (by author, title, publisher) or by using descriptors,
keyword searches or full-text searches. Staff will readily help users toensure a prompt and successful search.
4. Internet Catalogue Searches
The Centre's automated catalogue can be searched atwww.fcsd.org. Documents may be searched by title, author, otherresponsible parties, subject descriptors, language, etc. Free-textsearches for any word in the catalogue are also possible.
This service provides round-the-clock access to the Data Centrewherever the user is located. It also enables users to requestdocuments using the bibliographic search service, as long as currentlegislation concerning use and restrictions is observed.
5. Photocopying
A self-service photocopier is available to users who require copiesof parts of documents. Current legislation concerning the use and

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 78/80
FCSD
78
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
restrictions applying to this service must be observed.
6. Bibliographic search service
This service makes printed documents available without having tocome to the library. Document photocopies may simply be requestedvia letter, fax or e-mail.
The request must be sent to the BRDC address, specifying title,author and number of pages. For journal articles, the name of the journal, issue number and year must be added. All photocopies are
sent cash-on-delivery.
7. Audiovisual lending service
The BRDC has a wide range of videotapes dealing with variousforms of disability (physical, mental and sensory). This material is highlysuitable for use in talks, lectures and seminars or for initial contact withdisabled people, to get used to how they express themselves and how
they behave. It also enables professionals to learn about educationalexperiences and tasks performed by other professionals andinstitutions.
Tapes come from various countries and may contain films, debates,documentaries, general information, workshops, etc.
Videotapes may be viewed in the library or borrowed for a fortnight.The lending service is also available for people who live far away andcannot come to the Centre in person.
8. Table of Contents Bulletin Service
This bulletin photocopies the contents page of each of the reviewsreceived in the library.
It is published every two months and comprises all issues of journalsreceived during this period. It is sent by regular post, except for the firstissue, which is sent cash-on-delivery to pay for the yearly subscriptionfee.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 79/80
FCSD
79
F u n d a c i ó C a t a l a n a S í n d r o m e d e D o w n
Photocopies of articles listed in the bulletin may be requested byletter, fax or e-mail stating the full title of the article, author, number ofpages, journal name and issue number and year. This service is paid
separately for every request sent to the BRDC.
9. New Books Bulletin Service
This bulletin lists all the new books coming into the library. It ispublished every three months and is sent to subscribers who pay asubscription fee.
It contains the bibliographic references of all new books as well astheir subject descriptors and summaries.
10. Activities with other institutions
Acting as a documentation centre in association with Spain's RealPatronato de Prevención y de Atención a Personas con Minusvalía, theBRDC forwards the biannual publications catalogue of the Real
Patronato to more than 200 disability-related organizations andinstitutions based in Catalonia. This catalogue may also be consulted atthe centre.
The BRDC also collaborates with the Escola Universitària JordiRubió i Balaguer de Biblioteconomia i Documentació (which trainslibrarians and archivists) by allowing third-year students to use the DataCentre as a site for guided work experience.

8/14/2019 Down Syndrome 2004
http://slidepdf.com/reader/full/down-syndrome-2004 80/80
FCSD
80
ACKNOWLEDGEMENTS
The FCSD wishes to express its deepest gratitude to all institutions,public and private, collaborating institutions, members, enterprises andprivate individuals for their support and financial aid, since without it ourtasks and projects aimed at improving the quality of life of the disabled sothat they attain full social integration at all levels, in school, employment
and society, would not be possible.
Every idea, every new project, every extension of a service, or of aproposal needs financial aid. The FCSD could not function without thissupport.
Our heartfelt thanks to all.




