Dose escalation study of ODM-203, a selective dual FGFR ... · ODM-203 exposure in patients vs....
13
Dose escalation study of ODM-203, a selective dual FGFR/VEGFR inhibitor, in patients with advanced solid tumours J Rodon 1 , C Garratt 2 , K Laapas 2 , H Leskinen 2 , H Björklund 2 , J Hietamäki-Zaagman 2 , K Peltola 3 , A Azaro 1 , C Massard 4 , P Bono 3 1 Vall d'Hebron University Hospital and Universitat Autonoma de Barcelona, Barcelona, Spain; 2 Orion Corporation Orion Pharma, Espoo, Finland; 3 Comprehensive Cancer Center, Helsinki University Hospital and University of Helsinki, Helsinki, Finland; 4 Institute Gustave Roussy, University of Paris Sud, Dept. of Cancer Medicine, Villejuif, France
Transcript of Dose escalation study of ODM-203, a selective dual FGFR ... · ODM-203 exposure in patients vs....

Dose escalation study of ODM-203, a selective dual FGFR/VEGFR inhibitor, in patients with advanced solid tumours
J Rodon1, C Garratt2, K Laapas2, H Leskinen2, H Björklund2, J Hietamäki-Zaagman2, K Peltola3, A Azaro1, C Massard4, P Bono3
1Vall d'Hebron University Hospital and Universitat Autonoma de Barcelona, Barcelona, Spain; 2Orion Corporation Orion Pharma, Espoo, Finland; 3Comprehensive Cancer Center, Helsinki University
Hospital and University of Helsinki, Helsinki, Finland; 4Institute Gustave Roussy, University of Paris Sud, Dept. of Cancer Medicine, Villejuif, France

Constitutively active FGFRs are oncogenic in non-clinical studies
FGFR amplifications have an impact on patient survival in studied cancer types (breast, lung, and gastric)
VEGFR expression correlates with survival or progression in tumor types with high incidence of FGFR alterations (bladder, breast, lung, gastric)
Both VEGFR and FGFRs are drivers for angiogenesis, a hallmark of tumorigenesis
FGFR signalling is a known escape mechanism for anti-VEGFR treatments
Both FGFRs and VEGFRs have same direct target and adaptor proteins, such as Frs2
TAT Washington 21-23 March 2016
Rationale for combining FGFR and VEGFR
inhibition

IC50 (nM) ODM-203 Lucitanib AZD4547
FGFR1 11 58 0.3
FGFR2 16 186 0.2
FGFR3 6 253 1
FGFR4 35 > 1000 7
VEGFR1 26 162 87
VEGFR2 9 9 55
VEGFR3 5 34 35
Ratio
FGFR1/VEGFR2 1:1 1:5 200:1
ODM-203 is a balanced selective dual FGFR/VEGFR
inhibitor
In vitro kinase activity*
• In addition to its primary targets ODM-203 only suppresses 9 kinases out of 317 by more than 70% at 1 uM
In vitro kinase selectivity* Number of kinase inhibited to > 70% at 1 uM out of 317
0
20
40
60
80
100
Nu
mb
er
of
kin
ase
s In
hib
ited
> 7
0%
Holmström T., et al. Cancer Res 2015;75(15 Suppl) TAT Washington 21-23 March 2016

ODM-203 shows similar potency in suppressing FGFR and VEGFR cellular signalling
Effect of ODM-203 on FGFR phosphorylation
in a FGFR dependent cell line (SNU16)
Effect of ODM-203 on VEGFR phosphorylation in HUVEC cells
pFGFR
total FGFR
ODM-203
0 1 10 100 1000 nM
pVEGFR2
total VEGFR2
0 0 1 10 100 1000
- + + + + + VEGF
nM ODM-203
Cell based activity (proliferation)
Cell line (receptor) /
IC50 nM ODM-203 Lucitanib AZD4547
H1581 (FGFR1) 104 160 6
SNU 16 (FGFR2) 132 65 5
RT4 (FGFR3) 192 130 21
Angiogenesis (tube
formation) 33 1 260
Ratio
FGFR/Angiogenesis 1:4 1:120 25:1
• ODM-203 is 60-90 times less potent inhibitor of cell proliferation in FGFR independent cell lines
Holmström T., et al. Cancer Res 2015;75(15 Suppl) TAT Washington 21-23 March 2016
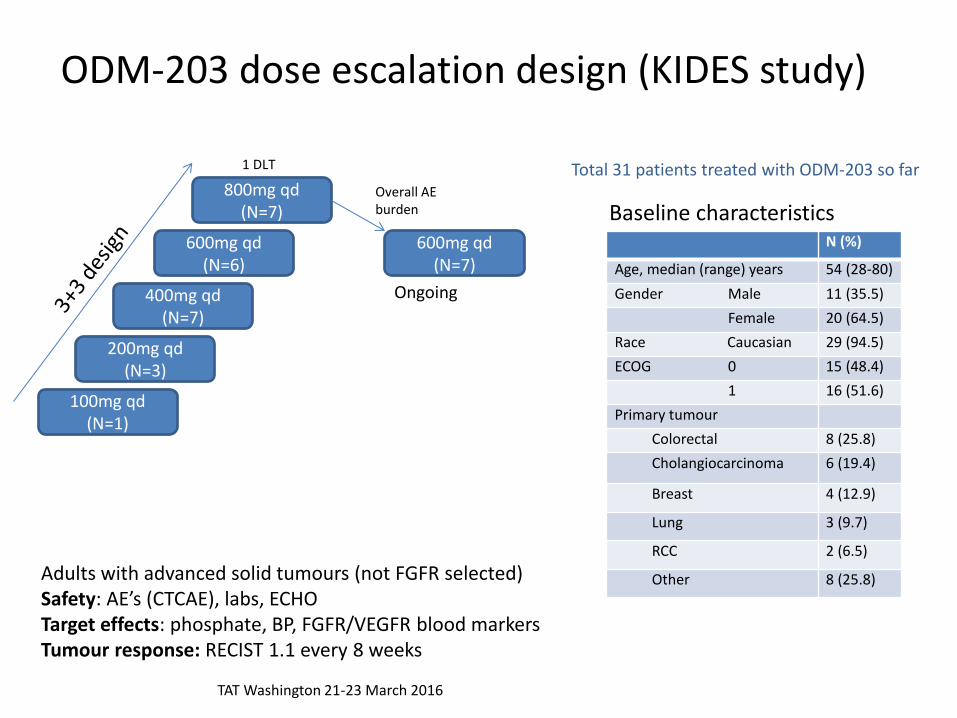
ODM-203 dose escalation design (KIDES study)
Total 31 patients treated with ODM-203 so far 1 DLT
Ongoing
100mg qd (N=1)
200mg qd (N=3)
400mg qd (N=7)
600mg qd (N=6)
800mg qd (N=7)
600mg qd (N=7)
Overall AE burden
Adults with advanced solid tumours (not FGFR selected) Safety: AE’s (CTCAE), labs, ECHO Target effects: phosphate, BP, FGFR/VEGFR blood markers Tumour response: RECIST 1.1 every 8 weeks
N (%)
Age, median (range) years 54 (28-80)
Gender Male 11 (35.5)
Female 20 (64.5)
Race Caucasian 29 (94.5)
ECOG 0 15 (48.4)
1 16 (51.6)
Primary tumour
Colorectal 8 (25.8)
Cholangiocarcinoma 6 (19.4)
Breast 4 (12.9)
Lung 3 (9.7)
RCC 2 (6.5)
Other 8 (25.8)
Baseline characteristics
TAT Washington 21-23 March 2016
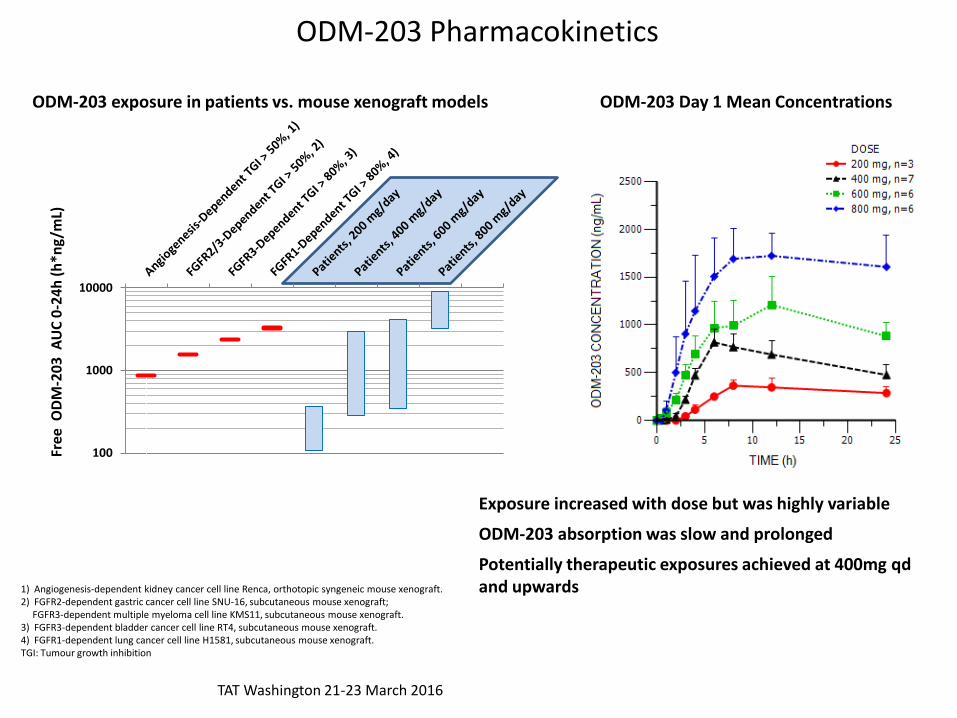
ODM-203 Pharmacokinetics
1) Angiogenesis-dependent kidney cancer cell line Renca, orthotopic syngeneic mouse xenograft. 2) FGFR2-dependent gastric cancer cell line SNU-16, subcutaneous mouse xenograft; FGFR3-dependent multiple myeloma cell line KMS11, subcutaneous mouse xenograft. 3) FGFR3-dependent bladder cancer cell line RT4, subcutaneous mouse xenograft. 4) FGFR1-dependent lung cancer cell line H1581, subcutaneous mouse xenograft. TGI: Tumour growth inhibition
100
1000
10000
Free
OD
M-2
03
AU
C 0
-24
h (
h*n
g/m
L)
ODM-203 Day 1 Mean Concentrations ODM-203 exposure in patients vs. mouse xenograft models
Exposure increased with dose but was highly variable
ODM-203 absorption was slow and prolonged
Potentially therapeutic exposures achieved at 400mg qd and upwards
TAT Washington 21-23 March 2016
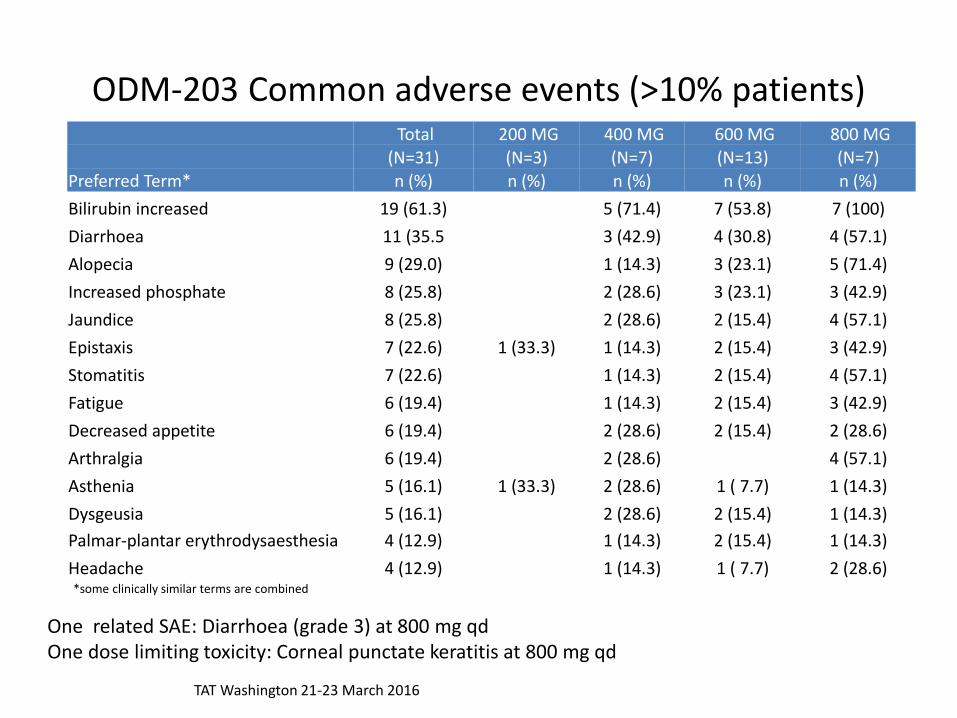
ODM-203 Common adverse events (>10% patients) Total 200 MG 400 MG 600 MG 800 MG
(N=31) (N=3) (N=7) (N=13) (N=7)
Preferred Term* n (%) n (%) n (%) n (%) n (%)
Bilirubin increased 19 (61.3) 5 (71.4) 7 (53.8) 7 (100)
Diarrhoea 11 (35.5 3 (42.9) 4 (30.8) 4 (57.1)
Alopecia 9 (29.0) 1 (14.3) 3 (23.1) 5 (71.4)
Increased phosphate 8 (25.8) 2 (28.6) 3 (23.1) 3 (42.9)
Jaundice 8 (25.8) 2 (28.6) 2 (15.4) 4 (57.1)
Epistaxis 7 (22.6) 1 (33.3) 1 (14.3) 2 (15.4) 3 (42.9)
Stomatitis 7 (22.6) 1 (14.3) 2 (15.4) 4 (57.1)
Fatigue 6 (19.4) 1 (14.3) 2 (15.4) 3 (42.9)
Decreased appetite 6 (19.4) 2 (28.6) 2 (15.4) 2 (28.6)
Arthralgia 6 (19.4) 2 (28.6) 4 (57.1)
Asthenia 5 (16.1) 1 (33.3) 2 (28.6) 1 ( 7.7) 1 (14.3)
Dysgeusia 5 (16.1) 2 (28.6) 2 (15.4) 1 (14.3)
Palmar-plantar erythrodysaesthesia 4 (12.9) 1 (14.3) 2 (15.4) 1 (14.3)
Headache 4 (12.9) 1 (14.3) 1 ( 7.7) 2 (28.6) *some clinically similar terms are combined
One related SAE: Diarrhoea (grade 3) at 800 mg qd One dose limiting toxicity: Corneal punctate keratitis at 800 mg qd
TAT Washington 21-23 March 2016
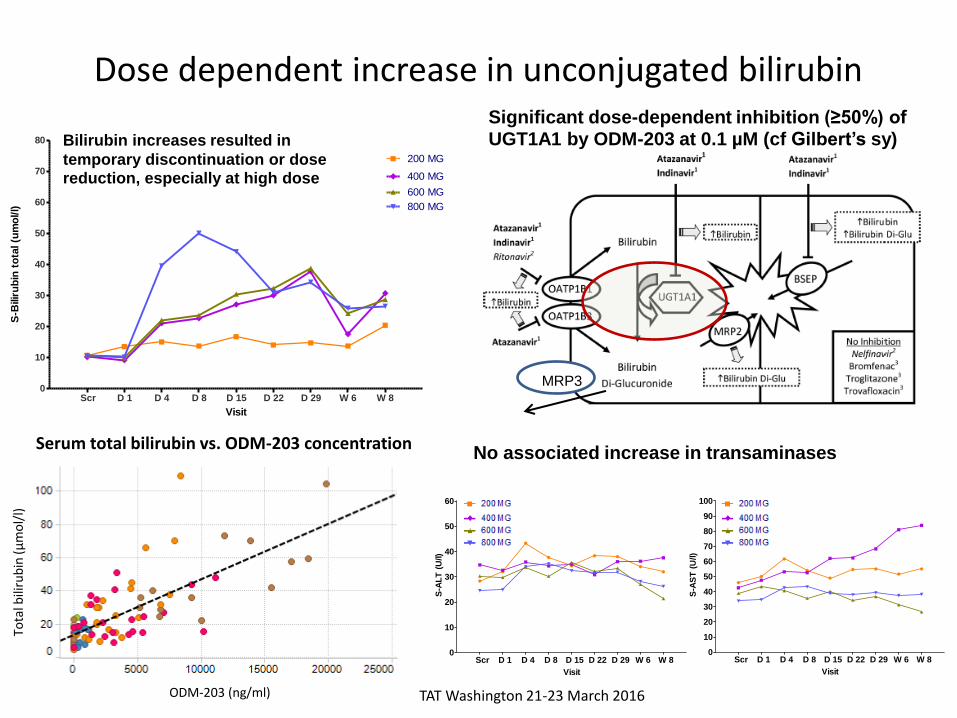
Dose dependent increase in unconjugated bilirubin
TAT Washington 21-23 March 2016
Scr D 1 D 4 D 8 D 15 D 22 D 29 W 6 W 80
10
20
30
40
50
60
70
80
200 MG
600 MG
800 MG
400 MG
Visit
S-B
ilir
ub
in t
ota
l (u
mo
l/l)
MRP3
Significant dose-dependent inhibition (≥50%) of UGT1A1 by ODM-203 at 0.1 µM (cf Gilbert’s sy)
No associated increase in transaminases
Bilirubin increases resulted in
temporary discontinuation or dose reduction, especially at high dose
Scr D 1 D 4 D 8 D 15 D 22 D 29 W 6 W 80
10
20
30
40
50
60
400 MG
600 MG
800 MG
200 MG
Visit
S-A
LT
(U
/l)
Scr D 1 D 4 D 8 D 15 D 22 D 29 W 6 W 80
10
20
30
40
50
60
70
80
90
100
400 MG
600 MG
800 MG
200 MG
Visit
S-A
ST
(U
/l)
Serum total bilirubin vs. ODM-203 concentration
Tota
l bili
rub
in (µ
mo
l/l)
ODM-203 (ng/ml)
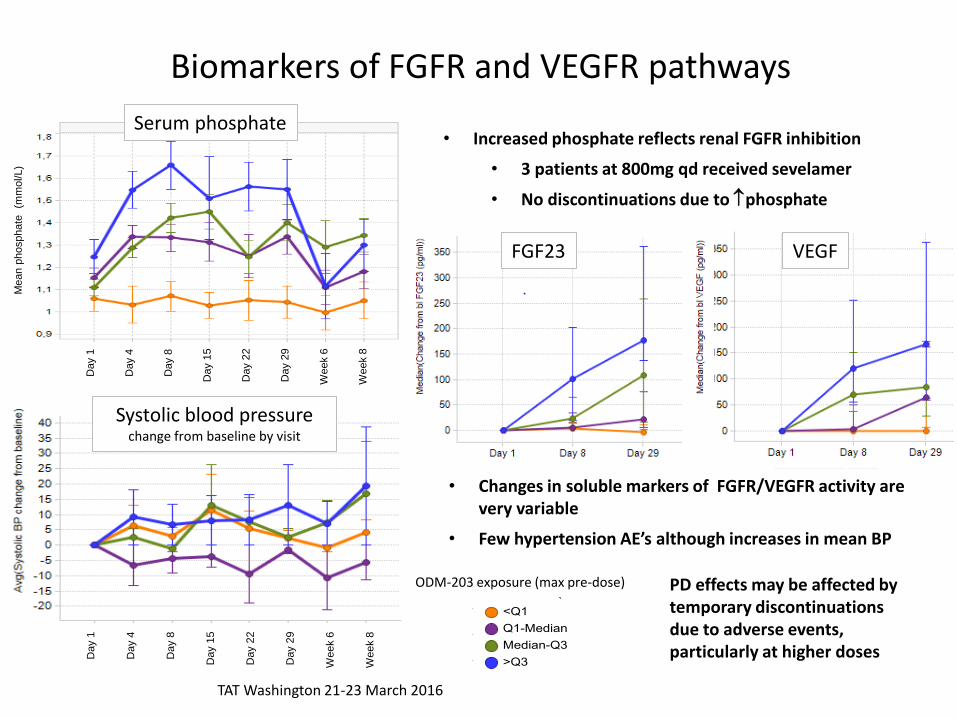
Biomarkers of FGFR and VEGFR pathways
• Changes in soluble markers of FGFR/VEGFR activity are very variable
• Few hypertension AE’s although increases in mean BP
PD effects may be affected by temporary discontinuations due to adverse events, particularly at higher doses
VEGF
Day 1
Day 4
Day 8
Day 1
5
Day 2
2
Day 2
9
Week 6
Week 8
ODM-203 exposure (max pre-dose)
Day 1
Day 4
Day 8
Day 1
5
Day 2
2
Day 2
9
Week 6
Week 8
Serum phosphate
Systolic blood pressure change from baseline by visit
TAT Washington 21-23 March 2016
FGF23
• Increased phosphate reflects renal FGFR inhibition
• 3 patients at 800mg qd received sevelamer
• No discontinuations due to phosphate
Mean p
hosphate
(m
mo
l/L)

-100
-80
-60
-40
-20
0
20
40
60
80
100
Ch
ange
in t
um
ou
r si
ze (
%)
ODM-203 best tumour response
800 mg
600 mg
400 mg
ODM-203 dose
Patients at 100/200mg excluded for low exposure. Evaluable patients with at least baseline and follow up assessments.
Best response at 8 weeks (RECIST)
Progressive disease 7
Stable disease 13
Partial response 2
Complete response 0
TAT Washington 21-23 March 2016
Co
lore
cta
l
Rec
tal
Sig
mo
id
Ren
al
Ch
ola
ng
ioC
a
Ch
ola
ng
ioC
a
NS
CL
C
An
us
sq
Ch
ol;
an
gio
Ca
NS
CL
C
Bre
as
t
Th
ym
om
a
Me
so
the
lio
ma
Co
lan
gio
Ca
Th
yro
id
Ch
ola
ng
ioC
a
Ch
ola
ng
ioC
a
Ch
ola
ng
ioC
a
Ov
ari
an
Bre
as
t
My
oe
pit
he
lia
l
R
en
al
10 8 4 40 8 16 24 18 7 8 29* 26*
12*
9* 13* 21*
15*
Weeks treatment
*ongoing
51*
RET
tra
nsl
oca
tio
n
RET
fu
sio
n
FGFR
2 f
usi
on
FGFR
mu
t
FGFR
1 a
mp
FGFR
2 d
elet
ion
FGFR
1 a
mp
FGFR
1 a
mp
20 9 30*
RET
mu
tati
on
KIDES best tumour response
11*
FGFR
2 f
usi
on

Response in a patient with colangiocarcinoma patient harbouring FGFR2 fusion
Long-standing disease with unequivocal progressive disease at time of starting ODM-203 • 40 weeks ODM-203 treatment • Best response -19% at 24 weeks • FGFR2 fusion (G3BP2) found • Dose 400mg qd
PRE
8 wks
Target lesion 1 Target lesion 2
PRE
8 wks
AE’s: fatigue, taste disorder, stomatitis, increased bilirubin,
epistaxis, alopecia, ↓ ejection fraction
TAT Washington 21-23 March 2016

Response in a patient with myoepithelial carcinoma with FGFR2 mutation (p.C382R)
• 62 yr old male
• Diagnosed 2008
• Radiotherapy after primary surgery
• Previous cisplatin, vinorelbine
• Initial ODM-203 dose 600mg qd: ongoing at 300mg qd after 12 weeks
• Tumour reduction 36.3% at 8 weeks
8 weeks ODM-203
Pre-treatment
TAT Washington 21-23 March 2016

• ODM-203 is a small molecule with balanced FGFR1-4 and VEGFR 1-3 inhibition that is
relatively selective.
• Exposure increased with dose up to 800mg qd, achieving anticipated therapeutic dose,
and was somewhat variable.
• One DLT (Keratitis) was reported at 800mg qd (MAD).
• UGT1A1 inhibition caused dose dependent bilirubin increases, resulting in early dose
reduction, especially at 800mg qd.
• Diarrhoea and mucocutaneous events occurred commonly after several weeks
treatment, and responded to temporary discontinuation or dose reduction of ODM-203.
• Exposure-related mean changes in phosphate, soluble markers and modest blood
pressure increases suggest on-target activity and may be limited by early dose
reductions due to increased bilirubin.
• Significant clinical responses were observed in patients with RCC and FGFR aberrant
cholangio and myoepithelial carcinoma.
• Study expansion and evaluation of dosing schedule is ongoing.
Conclusions
TAT Washington 21-23 March 2016