Doppler velocimetry for predicting fetal death in a twin ...784 P. Soikkeli et al. Fig.2. Blood...
4
Doppler velocimetry for predicting fetal death in a twin pregnancy. Soikkeli, Pia; Dubiel, Mariusz; Gudmundsson, Saemundur Published in: Acta Obstetricia et Gynecologica Scandinavica DOI: 10.1034/j.1600-0412.2002.810817.x 2002 Link to publication Citation for published version (APA): Soikkeli, P., Dubiel, M., & Gudmundsson, S. (2002). Doppler velocimetry for predicting fetal death in a twin pregnancy. Acta Obstetricia et Gynecologica Scandinavica, 81(8), 783-785. https://doi.org/10.1034/j.1600- 0412.2002.810817.x Total number of authors: 3 General rights Unless other specific re-use rights are stated the following general rights apply: Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal Read more about Creative commons licenses: https://creativecommons.org/licenses/ Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim.
Transcript of Doppler velocimetry for predicting fetal death in a twin ...784 P. Soikkeli et al. Fig.2. Blood...

LUND UNIVERSITY
PO Box 117221 00 Lund+46 46-222 00 00
Doppler velocimetry for predicting fetal death in a twin pregnancy.
Soikkeli, Pia; Dubiel, Mariusz; Gudmundsson, Saemundur
Published in:Acta Obstetricia et Gynecologica Scandinavica
DOI:10.1034/j.1600-0412.2002.810817.x
2002
Link to publication
Citation for published version (APA):Soikkeli, P., Dubiel, M., & Gudmundsson, S. (2002). Doppler velocimetry for predicting fetal death in a twinpregnancy. Acta Obstetricia et Gynecologica Scandinavica, 81(8), 783-785. https://doi.org/10.1034/j.1600-0412.2002.810817.x
Total number of authors:3
General rightsUnless other specific re-use rights are stated the following general rights apply:Copyright and moral rights for the publications made accessible in the public portal are retained by the authorsand/or other copyright owners and it is a condition of accessing publications that users recognise and abide by thelegal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private studyor research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal
Read more about Creative commons licenses: https://creativecommons.org/licenses/Take down policyIf you believe that this document breaches copyright please contact us providing details, and we will removeaccess to the work immediately and investigate your claim.

Acta Obstet Gynecol Scand 2002: 81: 783–785 Copyright C Acta Obstet Gynecol Scand 2002
Printed in Denmark . All rights reservedActa Obstetricia et
Gynecologica ScandinavicaISSN 0001-6349
CASE REPORT
Doppler velocimetry forpredicting fetal death in a twinpregnancy
PIA SOIKKELI1, MARIUSZ DUBIEL2 AND
SAEMUNDUR GUDMUNDSSON1
From the 1Department of Obstetrics and Gynecology,University Hospital MAS, Malmö, Sweden, and 2Departmentof Perinatology and Gynecology, University School ofMedical Sciences, Poznan, Poland
Acta Obstet Gynecol Scand 2002; 81: 783–785. C Acta Obstet GynecolScand 2002Key words: Doppler; ultrasound; twin pregnancy; fetal hypoxiaSubmitted 28 June, 2001Accepted 7 January, 2002
Diagnosis of discordant twins is easily accomplished withmodern ultrasound equipment, though diagnosing twin-to-twintransfusion syndrome (TTS) at an early stage might be aproblem. The possibility of excluding TTS by Dopplerultrasound is demonstrated in a case with early severe growthrestriction of one fetus. Characteristic blood velocity changesin a dying fetus are also illustrated.
The Doppler technique has become an accepted method inobstetrics for antenatal surveillance, permitting evaluation offetal circulation in a non-invasive manner and providingimportant physiological information on the fetal condition.Absent end-diastolic flow in the umbilical artery (UA) canwarrant operative delivery for fetal distress (1).
Perinatal mortality is increased fivefold in multiple gestation,as compared with singleton pregnancy (2). The majorcomplications include preterm labor, intrauterine growthretardation (IUGR), TTS, polyhydramnios, oligohydramnios,fetal malformations, and pre-eclampsia. Twin fetuses aregenerally smaller than singletons and IUGR and intrauterinefetal deaths are more common (3).
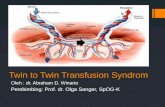
Before the introduction of the Doppler technique,ultrasound-imaging evaluation of discordant fetal size in twinpregnancy was a problem. Differential diagnosis of TTS and atrue growth retardation of one fetus was a frequent worry forthe clinician. Doppler examination of the fetal venouscirculation with pulsating flow in the umbilical vein has beenfound helpful in the diagnosis of fetal congestive heart failure(4, 5). The general ultrasound imaging and Doppler findings inTTS are listed in Fig.1. The information provided byultrasound imaging and Doppler can thus distinguish betweenTTS and growth retardation of one fetus and assist the clinicianin making a diagnosis and predict the outcome. The followingcase illustrates characteristic blood velocity findings in a dyingfetus.
C Acta Obstet Gynecol Scand 81 (2002)
Case
The case focuses on a 23-year-old primigravid woman with aspontaneous twin pregnancy. In the 19th week of gestation adiscrepancy in fetal size was noticed: 242 vs. 92g, respectively.There was one placenta with rather thick amniotic membranes,suggesting a dichorionic pregnancy. The fetuses were of thesame gender and the amniotic fluid was normal. Doppler ex-amination showed normal blood flow in UA, umbilical vein andmiddle cerebral artery (MCA) in the larger twin. In the smallertwin, end-diastolic blood flow was found to be absent in theumbilical artery without signs of brain sparing in MCA. Um-bilical venous flow was normal.
At 21weeks of gestation, the discordance in growth becamemore pronounced, fetal weights estimated to be 415 and 166g,respectively. Doppler examinations performed repeatedly,showed normal blood velocimetry in the larger twin and absentend-diastolic blood flow in the umbilical artery of the smallerone.
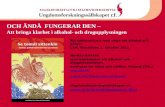
At 25weeks of gestation, Doppler examination showed re-versed end-diastolic blood flow in UA in the smaller twin asillustrated in Fig.2, along with double pulsations in the umbili-cal vein, both in a free loop of the umbilical cord and in theintra-abdominal part, along with signs of brain sparing inMCA. Ductus venosus velocimetry was abnormal, with re-versed flow during atrial contractions (Fig.2). These findingsare associated with perinatal mortality (6). Oligohydramnioswas present. The larger twin manifested normal blood veloci-metry in all vessels studied. After discussion with the parents,their decision was to concentrate on long-term survival of thelarger twin.
Serial twice-weekly Doppler measurements were performed,showing abnormal velocimetry in the smaller fetus, but normal
Fig.1. A schematic time sequence of characteristic ultrasoundfindings in twin-to-twin transfusion syndrome (TTS). ARED:absent or reversed end diastolic in the umbilical artery; UV:umbilical vein; MCA: middle cerebral artery; IVC: inferiorvena cava.

784 P. Soikkeli et al.
Fig.2. Blood velocity recording at the last examination before intrauterine death of the small twin. Blood flow in the large twin isnormal, but in the smaller twin reversal of flowing diastole is obvious in the umbilical artery, brain sparing in the middle cerebralartery, pulsations in umbilical venous flow, reversal of flow in ductus venosus and inferior vena cava.
in the larger. At 26weeks of gestation, discordance in growthbetween twins was ª8% (915g) vs. ª69%(318g), respectively,from reference curves. Doppler velocimetry showed similar re-sults to those presented at 25weeks. Similar Doppler veloci-metry results were recorded until 29weeks of pregnancy, whenthe smaller twin was deemed to have died. Doppler velocimetryin the survivor was normal. The pregnancy continued unevent-fully until 34weeks of gestation, when a healthy girl weighing2210g, Apgar score 9–10, was born prematurely vaginally. Thedead fetus, also a girl, had a velamentous cord placental inser-tion. The neonatal period was uneventful.
Discussion
Early ultrasound examination in twin pregnancy is of greatvalue. The ‘lamba sign’ can define dichorionicity and thus ex-clude the possibility of TTS later in gestation. Thick amnioticmembranes also suggest dichorionicity, and different genderwill confirm the fetus to be dizygotic. Diagnosis of discordanttwin size is thus not a clinical problem with modern ultrasound
C Acta Obstet Gynecol Scand 81 (2002)
equipment. However, differentiating between TTS and IUGRin one fetus is not so simple at mid-gestation if a dizygotictwin pregnancy cannot be confirmed. The likelihood of TTSincreases, however, when oligo- and/or polyhydramniosis de-velops. Hydrodramniosis is also a characteristic sign of conges-tive heart failure in the large TTS fetus. Ultrasound examina-tion of the larger twin can thus differentiate between TTS andtrue IUGR in the smaller twin.
Umbilical artery Doppler velocimetry can diagnose severevascular resistance, which can be seen in the smaller twin inboth IUGR and TTS. Signs of brain sparing in the MCA mightalso be seen in both twins. Venous Doppler flow examinationin the larger twin can, however, distinguish between IUGR andTTS. In a case of a true IUGR, due to poor placental functionor chromosomal aberration, venous blood flow in the largertwin is normal. However, abnormal flow in the ductus venosusand pulsations in the umbilical vein are characteristic signs ofimminent fetal heart failure in TTS due to circulation overloadin the recipient.
Blood flow in the fetal systemic veins pulsates normally inresponse to changes in central venous pressure. Umbilical ve-

Predicting fetal death in a twin pregnancy 785
nous flow is, however, even and without pulsations. By the de-velopment of the fetal heart failure, both due to overload as inTTS or during hypoxia as in IUGR, blood velocity pulsationsin the venous system increase in strength. Especially reversal offlow during atrial contraction is magnified and can cause a re-versal of flow in the ductus venosus and cause pulsations inthe umbilical vein (Fig.2). These findings are associated withincreased perinatal mortality (6).
The Doppler ultrasound signs of imminent fetal death givenin Fig.2 lasted for 3weeks. This is in agreement with our experi-ence from the early third trimester of pregnancy (�29weeks)and in accordance with findings by Arduini et al. (7). A moremature fetus might not withstand this stress for such a longtime. In our experience, a fetus of more than 34weeks of ges-tation can usually not withstand similar circulation alternationsfor more than 3days before intrauterine demize.
Signs of fetal brain sparing in the middle cerebral artery areknown to disappear prior to fetal death (8). This might be dueto cerebral autoregulation failure, cerebral edema, or heart fail-ure. This reversal of compensation seems to be a sudden and alate sign of fetal compromise with poor prognosis (9). In thepresent study, the fetus was examined weekly. Signs of brainsparing were observed at the last examination. Reversal of com-pensation might thus have occurred later.
The clinical dilemma is whether and when to intervene – ornot. If the larger twin is judged viable in TTS, the pregnancyshould be terminated by caesarean section before the smallertwin dies, in order to minimize deleterious effects on the largeror recipient after death of the smaller twin. LongitudinalDoppler examination can thus be of value for predicting fetaldeath and timing of delivery in TTS.
In IUGR in one fetus, letting the growth-restricted fetus diein utero is of minimal risk for the larger twin. Passing 25weeksof gestation is an obvious cause of anxiety. The clinical dilemmais trying to rescue one or both. Performing a caesarean sectionafter 25weeks might result in a small, severely injured newborndue to protracted hypoxemia. The unstressed larger twin mightalso suffer severely in the neonatal period, with varying degreeof morbidity due to immaturity. In the present case, the parentswere informed of the different options and chose to focus onone healthy baby. The decision is controversial and difficult forall parties concerned.
In conclusion, this case report illustrates characteristic bloodvelocity patterns in a dying fetus. The experience from this casereport might also be of value in distinguishing between TTSand IUGR of a fetus.
C Acta Obstet Gynecol Scand 81 (2002)
References
1. Gudmundsson S, Marsal K. Blood velocity waveforms infetal aorta and umbilical artery as predictors of fetal out-come – a comparison. Am J Perinatol 1991; 8: 1–6.
2. Jones JM, Sbarra AJ, Cetrulo CL. Antepartum manage-ment of twin gestation. Clin Obstet Gynecol 1990; 33: 32–41.
3. Manlan G, Scott KE. Contribution of twin pregnancy toperinatal mortality and fetal growth retardation; reversalof growth retardation after birth. Can Med Assoc J 1978;118: 365–8.
4. Gudmundsson S, Tulzer G, Huhta JC, Marsal K. VenousDoppler in the fetus with absent end-diastolic flow in theumbilical artery. Ultrasound Obstet Gynecol 1996; 7: 262–7.
5. Gudmundsson S, Huhta JC, Wood DC, Tulzer G, CohenAW, Weiner S. Venous Doppler ultrasonography in the fetuswith non-immune hydrops. Am J Obstet Gynecol 1991;164: 33–97.
6. Hofstaetter C, Dubiel M, Gudmundsson S. Two types ofumbilical venous pulsations and outcome of high-risk preg-nancy. Early Human Dev 2001; 61: 111–7.
7. Arduini D, Rizzo G, Romanini C. The development of ab-normal heart rate patterns after absent end-diastolic velo-city in umbilical artery: analysis of risk factors. Am J Ob-stet Gynecol 1993; 168: 43–50.
8. Weiner Z, Farmakides G, Schulman H, Penny B. Centraland peripheral hemodynamic changes in fetuses with ab-sent end-diastolic velocity in umbilical artery: correlationwith computerized fetal heart rate pattern. Am J ObstetGynecol 1994; 170: 509–15.
9. Konje JC, Bell SC, Taylor DJ. Abnormal Doppler veloci-metry and blood flow Volume in the middle cerebral arteryin very severe intrauterine growth restriction: is the occur-rence of reversal of compensatory flow too late? Br J ObstetGynaecol 2001; 108: 973–9.
Address for correspondence:Saemundur GudmundssonUniversity of LundDepartment of Obstetrics and GynecologyUniversity Hospital MASS – 205 02, MalmöSweden