Doppler ultrasound of the kidneys 1
60
Doppler ultrasound of the kidneys Dr. Muhammad Bin Zulfiqar PGR FCPS SHL
-
Upload
muhammad-bin-zulfiqar -
Category
Education
-
view
1.906 -
download
17
description
Selection of Patients for Renal Doppler. and Technique
Transcript of Doppler ultrasound of the kidneys 1

Doppler ultrasound of the kidneys
Dr. Muhammad Bin Zulfiqar
PGR FCPS SHL

Doppler US of the kidneys
• Normal anatomy of the kidney
• Normal US of the kidney
• Normal Doppler US of the kidney
• Indications of renal Doppler US

Normal anatomy of the kidney
Paspulati RM et al. Ultrasound Clin 2006 ; 1 : 25 – 41.
Renal parenchyma: cortex & medullary pyramids
Renal sinus: arteries, veins, lymphatics, collecting system, & fat
Renal hilum: Concave, in continuity with renal sinus

Anatomy of renal arteries
RRA: Usually passes posterior to inferior vena cava
LRA: Usually courses posterior to left renal vein
Multiple renal arteries in 25% (inferior polar artery from aorta)

Arterial blood supply to the Kidney
Myers KA & Clough A. Making sense of vascular ultrasound. Arnold, London, 2004.
Segmental arteryApical, upper, middle, lower, posterior
Interlobular arteryBetween renal pyramids
Glomerular arteriole
Main renal artery
Arcuate arteryBetween cortex & medulla

Left renal vein
• Longer than right renal vein
• Averages 85 mm in length (range: 60 – 110 mm)
• Joined by adrenal, gonadal, lumbar, & hemiazygousveins before crossing the aorta
• Different types: Pre-aortic 80 – 95% Retro-aortic 2 – 3%Circum-aortic 7 – 9%
Sidhu R et al. Semin Ultrasound CT MRI 2009 ; 30 : 271 – 288.

Variants of left renal vein Retro-aortic LRV
Incidence: 2 – 3%
Circum-aortic LRV
Incidence: 7 – 9%
Sidhu R et al. Semin Ultrasound CT MRI 2009 ; 30 : 271 – 288.

Left-sided IVC
Myers KA & Clough A. Making sense of vascular ultrasound. Arnold, London, 2004.
Normal anatomy of IVC Anomalous left-sided IVC
Persistence of embryological AV

Doppler US of the kidneys
• Normal anatomy of the kidney
• Normal US of the kidney
• Normal Doppler US of the kidney
• Indications of renal Doppler US

Gray scale imaging first
• Kidneys Maximum renal length Echogenicity of renal cortexThickness of renal cortexMasses – hydronephrosis – renal calculi
• Aorta Plaque – thrombus – dissection – aneurysm
• Adrenal glands

Normal kidneyLongitudinal section Cross section
Rumack CM et al. Diagnostic Ultrasound. Elsevier-Mosby, St. Louis, USA, 3rd edition, 2005.
Renal capsule: echogenic line
Renal parenchyma: outer cortex & inner medulla pyramid
Central sinus complex: high echogenicity (vessels, fat, fibrous tissue)

Renal dimensions
• Length of normal kidney: 9 – 14 cm
Right kidney smaller than left kidney
• Discrepancy > 2 cm between two kidneys:
Considered significant & needs further evaluation
• Renal length between 8 – 9 cm
Correlated to patient’s phenotype particularly height
• Renal length < 8 cm definitely reduced
Should be attributed to chronic renal failure
Fiorini F et al. J Ultrasound 2007 ; 10 : 161 – 167.

Measurement of parenchymal & cortical thickness
Cortical thickness: Normal 8 – 10 mm
Parenchymal thickness: Normal 14 – 18 mm
Tuma J et al. European course book: Genitourinary ultrasound.
European Foundation of Societies of Ultrasound in Medicine & Biology.

Renal volume
Length: 9 – 14 cm (longitudinal section) Width: 4 – 6 cm (cross section) Depth: 4 – 6 cm (cross section)
Ellipsoid formula: length . width . thickness . π/6
Derchi LE et al. Acad Radiol 1994 ; 1 : 100 – 105.
Fiorini F et al. J Ultrasound 2007 ; 10 : 161 – 167.
Adjusted to BMI
(V / BMI) . 25
Appropriate renal volume
231 ± 50 ml

Classification of renal parenchymal echogenicity
4 types based of US appearance
Hypoechoic compared to liver
Isoechoic compared to liver
Hyperechoic compared to liver
Isoechoic to renal sinus
Normal
Normal
Pathological
Pathological
Grade 0
Grade I
Grade II
Grade III

Kidney parenchyma compared to liver parenchyma
Hypoechoic Isoechoic
Hyperechoic
Fiorini F et al. J Ultrasound 2007 ; 10 : 161 – 167.

Congenital normal variants of kidney
• Dromedary hump
• Persistent fetal lobulation
• Prominent column of Bertin
• Junctional parenchymal defect
• Hypoechoic renal sinus
Paspulati RM et al. Ultrasound Clin 2006 ; 1 : 25 – 41.

Dromedary humpCommon renal variation
Paspulati RM et al. Ultrasound Clin 2006 ; 1 : 25 – 41.
Focal bulge on lateral border of left kidney
Result from adaptation of renal surface to adjacent spleen
Easily differentiated from renal mass by Doppler

Persistent fetal lobulation
Paspulati RM et al. Ultrasound Clin 2006 ; 1 : 25 – 41.
Renal surface indentations between pyramids
May be single or multiple

Prominent column of Bertin (PCB)Mistaken for intrarenal tumor
Paspulati RM et al. Ultrasound Clin 2006 ; 1 : 25 – 41.
Continuity with renal cortex
Similar echo pattern as renal parenchyma
Similar vascular pattern by color & power Doppler

Junctional fusion defect
Paspulati RM et al. Ultrasound Clin 2006 ; 1 : 25 – 41.
Mistaken for cortical scar or angiomyolipoma
Continuity with central sinus
by echogenic line
“inter-renicular septum”
Triangular hyperechoic structure
Antero-superior or postero-inferior
surface of kidney

Abdominal aorta
• Normal abdominal aorta 1.5 – 2.5 cm
• Ectatic aorta 2.5 – 3 cm
• Aortic aneurysm > 3 cm
• Annual growth of aneurysms 0.33 cm/year between 4 & 5.5 cm
* Bhatt S et al. Ultrasound Clin 2008 ; 3 : 83 – 91.

Cross-section at adrenal glands Compared to seagull, Y, or V letter
Y-shaped structures lying antero-medial to kidneys
Composed of body & medial & lateral “wing” or “limb”
Tuma J et al. European course book: Genitourinary ultrasound.
European Foundation of Societies of Ultrasound in Medicine & Biology, 2011.

US of normal adrenal glandsDocumented in 1980 1
1 Dietrich CF et al. Endoscopy 1997 ; 29 : 859 – 864.2 Jenssen C et al. Ultraschall Med 2010 ; 31: 228 – 250.
With modern equipment (high-resolution) & good trainingUS can image right gland in 99% & left gland in 70%1
Transcostal scan in LLDBetween RLL, IVC & diaphragm
Right adrenal gland Left adrenal gland
Transverse scan of epigastriumDorsal to pancreatic tail & SV

Normal adrenal gland / Inverted Y-shape
Hypoechoic right adrenal gland
Horizontally inverted Y-shape
Coronal scan of right upper abdomen through MAL
Wan YL. J Med Ultrasound 2007 ;15 : 213 – 227.

Doppler US of the kidneys
• Normal anatomy of the kidney
• Normal US of the kidney
• Normal Doppler US of the kidney
• Indications of renal Doppler US

Technical points
• Fasting for at least 6 hours before the exam
• Duration of the examination: 30 – 45 min
• Rare failure: Non-cooperant patient – Gas
• Intestinal preparation: not necessary
Operator-dependent technique
Slow learning curve
Most complex & difficult Doppler examination1

Sites for pulsed Doppler of renal arteries
Aorta Ostium of main renal artery Trunk of main renal artery Hilum of kidney Upper pole of kidney Middle pole of kidney Lower pole of kidney

Transverse scan with probe angulationsMain renal arteries
Schäberle W. Ultrasonography in vascular diagnosis. Springer-Verlag, Berlin, 2nd edition, 2011.

Norma right renal artery
Moukaddam H et al. Ultrasound Clin 2007 ; 2 : 455 – 475.
Transverse gray scale image
Right main renal artery
Transverse color Doppler image
Right main renal artery

Gray scale alone without color DopplerPatients with difficulty to hold breath
Moukaddam H et al. Ultrasound Clin 2007 ; 2 : 455 – 475.
Entire RRA well visualizedColor flash artifact from patient motion may obscure visualization
Better spatial resolution & and faster frame rate
Gray scale image

Norma left renal artery
Gray scale image Color Doppler image
Moukaddam H et al. Ultrasound Clin 2007 ; 2 : 455 – 475.
Proximal main left renal artery Proximal main left renal artery

‘‘banana peel’’ or “Isikoff” view
Moukaddam H et al. Ultrasound Clin 2007 ; 2 : 455 – 475.Isikoff MB et al. Am J Roentgenol 1980 ; 134 : 1177 – 1179.
Origins of right & left renal arteries
Gray scale image
Origins of right & left renal arteries
Color Doppler image
Longitudinal transhepatic view in Left lateral decubitus

Normal right renal artery
Coronal images of IVC
Moukaddam H et al. Ultrasound Clin 2007 ; 2 : 455 – 475.
RRA is the only vessel to course laterally under the IVC
Often slightly indents the IVC

Two renal arteries or early branching?
Hélénon O et al. EMC-Radiologie 2005 ; 2 : 367 – 412.
Longitudinal view of IVC
Two right renal arteries
Transverse view of aorta
Early branching of RRA

Longitudinal scan in left lateral decubitus
Multiple renal arteries (25%)
Moukaddam H et al. Ultrasound Clin 2007 ; 2 : 455 – 475.

Two left renal arteries
Hélénon O et al. EMC-Radiologie 2005 ; 2 : 367 – 412.
PSV: 90 cm/sec
Dominant left renal artery
PSV: 60 cm/sec
Accessory left renal artery

Axial scan in left lateral decubitusUsing right kidney as acoustic window
Right main renal artery & vein
Color Doppler USSchematic drawing
Meola M et al. J Ultrasound 2008 ; 11 : 55 – 73.

Axial scan in right lateral decubitus
Using left kidney as acoustic windowSchematic drawing
Left main renal artery & vein
Color Doppler US
Zubarev AV. Eur Radiol 2001 ; 11 : 1902 – 1915.

Pre caval right renal artery

Pre-aortic left renal vein (80 – 95%)
Hélénon O et al. EMC-Radiologie 2005 ; 2 : 367 – 412.
Reduction in diameter in pre-aortic segment to IVC
with physiologic acceleration

Left renal vein variants
Sidhu R et al. Semin Ultrasound CT MRI 2009 ; 30 : 271 – 288.
Hélénon O et al. EMC-Radiologie 2005 ; 2 : 367 – 412.
Retro-aortic LRV (2 – 3%) Circum-aortic LRV (7 – 9%)
Pre & retro-aortic LRV

Color Doppler of RRV & retro-hepatic IVC
Hélénon O et al. EMC-Radiologie 2005 ; 2 : 367 – 412.
Righ renal vein Inferior vena cava

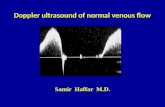
Pulsed Doppler of renal veins
Hélénon O et al. EMC-Radiologie 2005 ; 2 : 367 – 412.
Right renal vein
Resembles pulsed Doppler of IVC
Triphasic waveform
Left renal vein
Little modulation
Wall artifact due to systolic peak

Limits in visualization of main renal arteries
•Obesity•Overlying bowel gas•Dyspnea•Shadowing from arterial calcifications•Cardiac arrhythmias•Poor angle of Doppler insonation•Accessory renal arteries (small size)
Moukaddam H et al. Ultrasound Clin 2007 ; 2 : 455 – 475.
Expert sonographers detect 80 – 90% of main RACEUS improves success rate to 95%

Angle of insonation
Difficulty in case of tortuous or curved renal artery
Correct angle Incorrect angle
Schäberle W. Ultrasonography in vascular diagnosis.
Springer-Verlag, Berlin Heidelberg, 2nd edition, 2011.

Adjustment of Doppler controlLow flow settings
• Lowest pulse repetition frequency without aliasing
• Small color box
• Greatest gain without background noise
• Lowest wall filter
• High color priority

Normal segmental & interlobar renal arteries
Normal segmental renal arteries (long arrows)
Color Doppler image of the kidney
Moukaddam H et al. Ultrasound Clin 2007 ; 2 : 455 – 475.
Normal inter-lobar renal arteries (short arrows)

Study of intra-renal arteriesPerfusion study / Low PRF
Hélénon O et al. EMC-Radiologie 2005 ; 2 : 367 – 412.
Cortical perfusion
Tumoral vascularization

Study of intra-renal arteriesMorpho-hemodynamic study
Hélénon O et al. EMC-Radiologie 2005 ; 2 : 367 – 412.
Arterio-venous fistula Pseudo-aneurysm
Intermediate PRF
Renal stones Vascular calcifications
High PRF

Normal kidneyPower Doppler
Increases sensitivity to low flow
Less angle-dependent
Good visualization of the entire renal vascular tree
Zubarev AV. Eur Radiol 2001 ; 11 : 1902 – 1915.

Normal pulse Doppler waveformRenal segmental artery
Sharp systolic upstroke
Low resistance waveform
Continuous forward diastolic flow

Pourcelot’s resistive index
RI S – ED / S
Normal 50 – 70 %
Abnormal > 80 %

Accleration time (AT)or Rise time (RT)
• Length of time in sec from
onset of systole to peak systole
• Normal value: < 0.07 second

Acceleration Index (AI)
AI = X (KHz)
Probe frequency (MHz)
Normal value: > 3.5 m/s2
Systolic upslope/transducer frequency

Measurement of PSV
Early systolic peak
Am J Roentgenol – Dec 1995
Biphasic with late systolic peak
Monophasic with late systolic peak

Early systolic notch
Moukaddam H et al. Ultrasound Clin 2007 ; 2 : 455 – 475.
Some normal waveforms have early systolic notch
1. Measuring to point of PSV results in prolonged AT & AI
2. Excellent negative predictive value of stenosis > 60%

Extrasystole
Hélénon O et al. EMC-Radiologie 2005 ; 2 : 367 – 412.
Correct RI calculated in normal sinusoidal rhythm

Spectral Doppler of renal arteriesNormal values
• PSV < 180 cm/sec
• Renal Aortic Ratio (RAR) < 3
• Resistive index (RI) < 0.70
• ∆ RI (right – left) < 0.05
• Acceleration Time (AT) < 0.07 sec
• Acceleration Index (AI) > 3.5 m/s2