
Doppler-detected paradoxus of mitral and tricuspid valve ...Doppler-DetectedParadoxus ofMitral and...
4
706 lACC Vol. 8. No.3 September 1986:706-9 Doppler-Detected Paradoxus of Mitral and Tricuspid Valve Flows in Chronic Lung Disease BRIAN HOlT, MD, DAVID J. SAHN, MD, FACC, RALPH SHABETAI, MD, FACC San Diego. California An echocardiographic Doppler study in a patient with pulsus paradoxus of respiratory origin demonstrated a large inspiratory increase of tricuspid flow velocity and a corresponding decrease of mitral flow velocity. This "flow paradoxus" is therefore not specific for cardiac Although most physicians recognize that cardiac tamponade is in large measure a clinical diagnosis, a number of M- mode and, especially, two-dimensional echocardiographic methods to determine the presence and assess the hemo- dynamic severity of tamponade have been proposed (1-3). Nonetheless, the diagnosis of cardiac tamponade after car- diac surgery remains a difficult problem (4). Recent!y, it was demonstrated that during cardiac tamponade there is an inspiratory increase in velocity through the tricuspid and pulmonary valves and a decrease in velocity through the mitral and aortic valves measured by Doppler echocardi- ography, which is termed, somewhat inappropriately, "flow velocity paradoxus" (5,6). However, the specificity and clinical value of this sign have not been determined. Ac- cordingly, we describe a patient with a postoperative peri- cardial effusion and severe lung disease who demonstrated flow paradoxus that was respiratory, not pericardial, in origin. Case Report A 66 year old Caucasian man who has severe chronic lung disease required prednisone for control of symptoms. He underwent a four vessel coronary artery bypass graft operation on March II, 1985. Two weeks later, he com- plained of severe dyspnea and orthopnea, but had no chest pain. The blood pressure was 150/70 mm Hg with 35 mm Hg of pulsus paradoxus. The pulse rate was 110 beats/min, From the University of California. San Diego and Cardiology Section. San Diego Veterans Administration Medical Center, San Diego, California. Manuscript received November 13, 1985; revised manuscript received March II, 1986, accepted April 4, 1986. Address for reprints: Brian Hoit, MD, Veterans Administration Medical Center, Cardiology (IlIA), San Diego, California 92161. © 1986 by the American College of Cardiology tamponade, and provides evidence that decreased left ventricular filling is an important mechanism of pulsus paradoxus observed in severe chronic lung disease. (J Am Call Cardiol 1986;8:706-9) the temperature 102° F and the respiratory rate 28/min. Sternocleidomastoid retractions obscured the jugular venous pulse, but the carotid pulsations were brisk. The patient's breath sounds were diminished, particularly in the left lung base. Expiration was prolonged and diffuse wheezes were heard. The apical cardiac impulse was not displaced and the heart sounds were normal. A fourth heart sound, but no pericardial friction rub, was present. The liver was not en- larged; there was no edema. The electrocardiogram con- firmed sinus tachycardia and showed low voltage and poor R wave progression across the precordial leads. A lingular infiltrate was noted on the chest radiogram. Arterial blood gas analysis while the patient was receiving 3 liters of ox- ygen revealed pH 7.44, partial pressure of oxygen 76 torr and partial pressure of carbon dioxide 34 torr. Doppler echocardiographic and cardiac catheteriza- tion findings. Real-time echocardiography demonstrated a moderate-sized anterior pericardial effusion. There was no right ventricular diastolic collapse or right atrial compres- sion. During inspiration, the right ventricular dimension increased from 1.4 to 3. I em, the ventricular septum bowed to the left and the left ventricular dimension decreased from 5.9 to 4.7 em. Also during inspiration, mitral flow velocity (Fig. IA) dropped from 95 to 55 cm/s (a decrease of 42%) and tricuspid flow velocity (Fig. 2A) increased from 55 to 90 cm/s (an increase of 64%). Right heart catheterization was performed to exclude cardiac tamponade. The right atrial pressure was 6 mm Hg; the waveform showed a normal y descent. The right ven- tricular pressure was 28/7 mm Hg, the pulmonary artery pressure 25/15 mm Hg and the pulmonary artery wedge pressure 9 mm Hg. The arteriovenous oxygen difference was 4.8 vol% and a thermodilution cardiac output was 7.0 liters/min. After vigorous treatment with prednisone and 0735-1097/86/$3.50
Transcript of Doppler-detected paradoxus of mitral and tricuspid valve ...Doppler-DetectedParadoxus ofMitral and...

706 lACC Vol. 8. No.3September 1986:706-9
Doppler-Detected Paradoxus of Mitral and Tricuspid Valve Flowsin Chronic Lung Disease
BRIAN HOlT, MD, DAVID J. SAHN, MD, FACC, RALPH SHABETAI, MD, FACC
San Diego. California
An echocardiographic Doppler study in a patient withpulsus paradoxus of respiratory origin demonstrated alarge inspiratory increase of tricuspid flow velocity anda corresponding decrease of mitral flow velocity. This"flow paradoxus" is therefore not specific for cardiac
Although most physicians recognize that cardiac tamponadeis in large measure a clinical diagnosis, a number of Mmode and, especially, two-dimensional echocardiographicmethods to determine the presence and assess the hemodynamic severity of tamponade have been proposed (1-3).Nonetheless, the diagnosis of cardiac tamponade after cardiac surgery remains a difficult problem (4). Recent!y, itwas demonstrated that during cardiac tamponade there is aninspiratory increase in velocity through the tricuspid andpulmonary valves and a decrease in velocity through themitral and aortic valves measured by Doppler echocardiography, which is termed, somewhat inappropriately, "flowvelocity paradoxus" (5,6). However, the specificity andclinical value of this sign have not been determined. Accordingly, we describe a patient with a postoperative pericardial effusion and severe lung disease who demonstratedflow paradoxus that was respiratory, not pericardial, inorigin.
Case ReportA 66 year old Caucasian man who has severe chronic
lung disease required prednisone for control of symptoms.He underwent a four vessel coronary artery bypass graftoperation on March II, 1985. Two weeks later, he complained of severe dyspnea and orthopnea, but had no chestpain. The blood pressure was 150/70 mm Hg with 35 mmHg of pulsus paradoxus. The pulse rate was 110 beats/min,
From the University of California. San Diego and Cardiology Section.San Diego Veterans Administration Medical Center, San Diego, California.
Manuscript received November 13, 1985; revised manuscript receivedMarch II, 1986, accepted April 4, 1986.
Address for reprints: Brian Hoit, MD, Veterans Administration MedicalCenter, Cardiology (IlIA), San Diego, California 92161.
© 1986 by the American College of Cardiology
tamponade, and provides evidence that decreased leftventricular filling is an important mechanism of pulsusparadoxus observed in severe chronic lung disease.
(J Am Call Cardiol 1986;8:706-9)
the temperature 102° F and the respiratory rate 28/min.Sternocleidomastoid retractions obscured the jugular venouspulse, but the carotid pulsations were brisk. The patient'sbreath sounds were diminished, particularly in the left lungbase. Expiration was prolonged and diffuse wheezes wereheard. The apical cardiac impulse was not displaced andthe heart sounds were normal. A fourth heart sound, but nopericardial friction rub, was present. The liver was not enlarged; there was no edema. The electrocardiogram confirmed sinus tachycardia and showed low voltage and poorR wave progression across the precordial leads. A lingularinfiltrate was noted on the chest radiogram. Arterial bloodgas analysis while the patient was receiving 3 liters of oxygen revealed pH 7.44, partial pressure of oxygen 76 torrand partial pressure of carbon dioxide 34 torr.
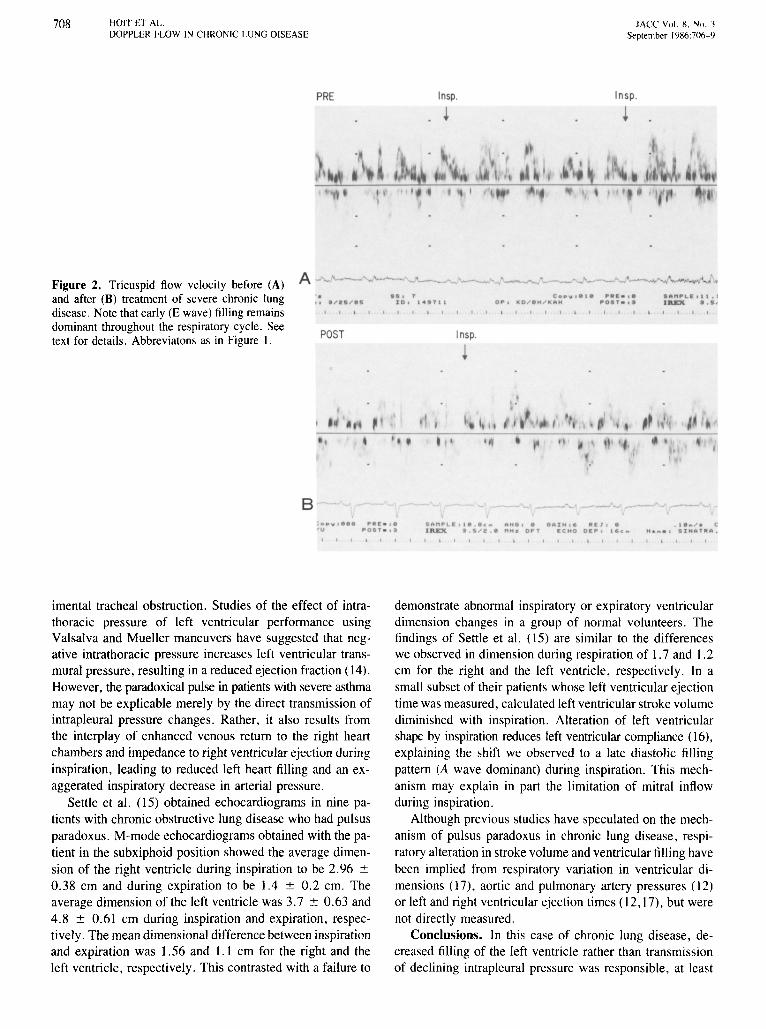
Doppler echocardiographic and cardiac catheterization findings. Real-time echocardiography demonstrated amoderate-sized anterior pericardial effusion. There was noright ventricular diastolic collapse or right atrial compression. During inspiration, the right ventricular dimensionincreased from 1.4 to 3. I em, the ventricular septum bowedto the left and the left ventricular dimension decreased from5.9 to 4.7 em. Also during inspiration, mitral flow velocity(Fig. IA) dropped from 95 to 55 cm/s (a decrease of 42%)and tricuspid flow velocity (Fig. 2A) increased from 55 to90 cm/s (an increase of 64%).
Right heart catheterization was performed to excludecardiac tamponade. The right atrial pressure was 6 mm Hg;the waveform showed a normal y descent. The right ventricular pressure was 28/7 mm Hg, the pulmonary arterypressure 25/15 mm Hg and the pulmonary artery wedgepressure 9 mm Hg. The arteriovenous oxygen differencewas 4.8 vol% and a thermodilution cardiac output was 7.0liters/min. After vigorous treatment with prednisone and
0735-1097/86/$3.50

lACC Vol. 8, No.3September 1986:706-9
HOlT ET AL.DOPPLER FLOW IN CHRONICLUNG DISEASE
707
intravenous theophylline, symptoms decreased and pulsusparadoxus fell to 15 mm Hg. Another Doppler echocardiographic study (Fig. IB and 2B) showed a reduction in respiratory variation of both mitral (from 85 to 60 cmls) andtricuspid (from 60 to 80 cmls) flow velocities, but no changein the pericardial effusion.
Comments
Respiratory variations in transvalvular flow and velocity. This is the first report of which we are aware oftransvalvular flow (velocity) alteration associated with pulsus paradoxus of respiratory origin. The clinical importanceof this case is that the presence of a pericardial effusion anda paradoxical pulse made the clinically crucial distinctionbetween exacerbation of chronic lung disease and perioperative tamponade difficult. Although respiratory variationin flow velocity across the atrioventricular and semilunarvalves may occur in pulsus paradoxus because of cardiactamponade, our case is the first to demonstrate that the samerespiratory variation in flow velocity also occurs in pulsusparadoxus of respiratory origin. The changes we observedare consistent with the findings of Pandian et al. (6). Working with a canine model of cardiac tamponade, they founda 17 ± 2% inspiratory increase in tricuspid flow velocityduring the control period, and a 117 ± 19% increase duringcardiac tamponade. The inspiratory decrease in mitral flow
velocity was 10 ± 2% during the control period, and 42± 3% during tamponade.
Whereas Doppler-determined flow velocity correlates wellwith volume flow, estimates of volume flow require measurement of the cross-sectional area of the flow channel (7).Although we did not measure anular diameter or flow area,our findings and those of others (8) that left ventriculardimension decreases during inspiration suggest that transmitral volume flow was reduced and that this reductionmight be underestimated by velocity tracings alone. Similarly, both the velocity across the tricuspid valve and thedimension of the right ventricle increased during inspiration,indicating augmented flow.
Mechanisms of pulsus paradoxus. A paradoxical pulsemay result from a combination of several mechanisms. Posterior ventricular septal bulging and competition betweenthe two ventricles for a reduced intrapericardial space arethought to be the primary mechanisms causing pulsus paradoxus in cardiac tamponade (9). Impedance to left ventricular ejection (10) and impairment of left ventricular filling resulting from a variety of mechanisms play lesser roles(11,12).
The genesis ofpulsus paradoxus in obstructive lung disease is more controversial. Shabetai et al. (13) stated thatpulse pressure and left ventricular stroke volume do notdecrease abnormally in patients with obstructive lung disease who have pulsus paradoxus or in animals with exper-
PRE Insp. Insp.
AI t . I IIII N' " *.1.. . 1 1 .. " . C ALI ., op, le MO 0... . I I'tllil ' . ". ' 0 . ' .
POST Insp. Insp.
•• I ,
10 I , .,,, I'c •• •
0_ I .0 ... . ... ' .....
Figure 1. Mitral flow velocity before(PRE) (A) and after (POST) (B) treatmentof severe chronic lung disease. Note theprominent A wave on the velocity tracingduring inspiration (Insp.). See text for details.
B --' ,.--.... .... CAL. ., • ., c •• " , •• , ' _"_L. I , • . "••• t ,. . .. 0 .. ".. . r e , ' 4,TII OP. ''''' .0 ' I'U _0 1 , _ . 1 IIlEX 1
• I I I I I • I I I • I • I I ~ I I I I I I I I I I I I I I I I I I
708 HOlT ET AL.DOPPLER FLOW IN CHRONICLUNG DISEASE
PRE Insp.
~
lACC Vol. S, No.3September 1986:706-9
Insp.
Figure 2. Tricuspid flow velocity before (A)and after (B) treatment of severe chronic lungdisease. Note that early (E wave) filling remainsdominant throughout the respiratory cycle. Seetext for details. Abbreviatons as in Figure I.
A --'--'.r. 1/ ....... 5
POST
~- ' - -•• • r c •• 'W . e •• 1" "• • , .
10 , 1 .'''11 0"" KO ... . H ....k.H "'OIT • • I
Insp.
•I .
l #Il n "'LI. I 1 . 1I ftEX • . s .
8: ".1: - ,.-u "' OST_ , .
I A I1P'LEI I • • • c_ AH I , • • IllIN , •• I J ,. . I e .." . c1ft£X • . 5 ....2 . • MH. 0 T I CHO 0.'" I~ c .. H. ... I I I NA ' It"'.
I I I I I I I I I , I I
imental tracheal obstruction. Studies of the effect of intrathoracic pressure of left ventricular performance usingValsalva and Mueller maneuvers have suggested that negative intrathoracic pressure increases left ventricular transmural pressure, resulting in a reduced ejection fraction (14).However, the paradoxical pulse in patients with severe asthmamay not be explicable merely by the direct transmission ofintrapleural pressure changes. Rather, it also results fromthe interplay of enhanced venous return to the right heartchambers and impedance to right ventricular ejection duringinspiration, leading to reduced left heart filling and an exaggerated inspiratory decrease in arterial pressure.
Settle et al. (15) obtained echocardiograms in nine patients with chronic obstructive lung disease who had pulsusparadoxus. M-mode echocardiograms obtained with the patient in the subxiphoid position showed the average dimension of the right ventricle during inspiration to be 2.96 ±0.38 em and during expiration to be 1.4 ± 0.2 em. Theaverage dimension of the left ventricle was 3.7 ± 0.63 and4.8 ± 0.61 em during inspiration and expiration, respectively. The mean dimensional difference between inspirationand expiration was 1.56 and 1.1 cm for the right and theleft ventricle, respectively. This contrasted with a failure to
demonstrate abnormal inspiratory or expiratory ventriculardimension changes in a group of normal volunteers. Thefindings of Settle et al. (15) are similar to the differenceswe observed in dimension during respiration of 1.7 and 1.2em for the right and the left ventricle, respectively. In asmall subset of their patients whose left ventricular ejectiontime was measured, calculated left ventricular stroke volumediminished with inspiration. Alteration of left ventricularshape by inspiration reduces left ventricular compliance (16),explaining the shift we observed to a late diastolic fillingpattern (A wave dominant) during inspiration. This mechanism may explain in part the limitation of mitral inflowduring inspiration.
Although previous studies have speculated on the mechanism of pulsus paradoxus in chronic lung disease, respiratory alteration in stroke volume and ventricular filling havebeen implied from respiratory variation in ventricular dimensions (17), aortic and pulmonary artery pressures (12)or left and right ventricular ejection times (12,17), but werenot directly measured.
Conclusions. In this case of chronic lung disease, decreased filling of the left ventricle rather than transmissionof declining intrapleural pressure was responsible, at least

JACC Vol. 8. No. JSeptember 1986:706-9
HOlT ET AL.DOPPLER FLOW IN CHRONIC LUNG DISEASE
709
in part, for pulsus paradoxus. Thus, transvalvular flow velocity paradox us is nonspecific for cardiac tamponade, butis observed in pulsus paradoxus of chronic lung disease.
We thank Diane Foster for expert word processing.
ReferencesI. Schiller NB, Botvinick EH. Right ventricular compression as a sign
of cardiac tamponade: an analysis of echocardiographic ventriculardimensions and their clinical implications. Circulation 1977;56:774-9.
2. Gillam LD, Guyer DE, Gibson TC, King ME, Marshall JE, WeymanAE. Hemodynamic compression of the right atrium: a new echocardiographic sign of cardiac tamponade. Circulation 1983;68:294-301.
3. Sinah S, Wann S, Schuchard GH, et al. Right ventricular and rightatrial collapse in patients with cardiac tamponade-a combined echocardiographic and hemodynamic study. Circulation 1984;70:966-71.
4. D'Cruz lA, Kensey K, Campbell C, Replogle R, Jain M. Two-dimensional echocardiography in cardiac tamponade occurring after cardiac surgery. J Am Coli Cardiol 1985;5:1250-2.
5. Pandian NG, Rifkin RD, Wang SS. Flow velocity paradoxus-a Doppler echocardiographic sign of cardiac tamponade: exaggerated respiratory variation in pulmonary and aortic blood flow velocities (abstr).Circulation I984:70(suppl 11):11-381.
6. Pandian NG, Wang SS, McInery K, et al. Doppler echocardiographyin cardiac tamponade. Abnormalities in tricuspid and mitral flow response to respiration in experimental and clinical tamponade (abstr).J Am Coli Cardiol 1985;5:485.
7. Magnin PA, Stewart JA, Myers S, Von Ramm 0, Kisslo JA. Combined Doppler and phased array echocardiographic estimation of cardiac output. Circulation 1981;63:388-92.
8. Brenner JI. Waugh RA. Effect of phasic respiration on left ventriculardimension and performance in a normal population. Circulation1978;57:122-7.
9. Shabetai R. Mangiardi L, Bhargava V, Ross J Jr, Higgins CB. Thepericardium and cardiac function. Prog Cardiovasc Dis 1979;22:107-34.
10. Schrijen F. Ehrlich W, Permutt S. Cardiovascular changes in consciousdogs during spontaneous deep breaths. Pflueg Arch 1975;355:205-15.
II. Dock W. Inspiratory traction on the pericardium. The cause of pulsusparadoxus in pericardial disease. Arch Intern Med 1961;108:837-40.
12. Ruskin JR. Bache RJ, Renbert JC, et al. Pressure-flow studies in man:effect of respiration on left ventricular stroke volume. Circulation1973;48:79-85.
13. Shabetai R, Fowler NO, Guntheroth WG. The hemodynamics of cardiac tamponade and constrictive pericarditis. Am J Cardiol 1970;6:480-9.
14. Buda AJ. Pinsky MR, Ingles NB, Daughters GT II, Stinson EB,Alderman EL. Effect of intrathoracic pressure on left ventricular performance. N Engl J Med 1979;301:453-9.
15. Settle HP Jr. Engel PJ, Fowler NO, et al. Echocardiographic studyof the paradoxical arterial pulse in chronic obtrusive lung disease.Circulation 1980;62: 1297-307.
16. Kitabatake A, Inque M, Asa M, et al. Transmitral blood flow reflectingdiastolic behavior of the left ventricle in health and disease. A studyby pulsed Doppler technique. Jpn Circ J 1982;46:92-102.
17. Settle HP, Adolph RJ, Fowler NO, et al. Echocardiographic study ofventricular dimensions in cardiac tamponade. Effects of respirationand pericardiocentesis. Circulation 1977;56:951-9.


















