
Dka & hhs
26
EMERGENCY IN DIABETES MELLITUS 1. Diabetic Ketoacidosis (DKA) 2. Hyperosmolar Hyperglycemic State (HHS) 3. Hypoglycemia
-
Upload
joseph-evangelist -
Category
Education
-
view
104 -
download
5
Transcript of Dka & hhs
EMERGENCY IN DIABETES MELLITUS
1. Diabetic Ketoacidosis (DKA)
2. Hyperosmolar Hyperglycemic State (HHS)
3. Hypoglycemia
Case Presentation R.T., a 25-year-old African-American man with
type 2 diabetes presented with a 5-day history of nausea and vomiting. He also reported a 2-week history of polyuria and polydipsia and a 10-lb weight loss. A review of symptoms was pertinent for a 5-day history of persistent lower back pain. The patient was diagnosed with type 2 diabetes 5 years ago when he presented to a different hospital with symptoms of polyuria, polydipsia, and weight loss. He was given a prescription for a sulfonylurea, which he says he took until his initial prescription ran out 1 month later. He had not taken any other medication since that time.
Case Presentation Physical examination revealed an afebrile, obese man
(BMI 40 kg/m2) with prominent acanthosis nigricans, no retinopathy by direct funduscopic exam, and a normal neurological exam, including motor function and sensation. The patient had no tenderness to palpation over the lumbrosacral spine or paraspinous muscles despite his complaint of lower back pain. The laboratory data showed an anion gap, metabolic acidosis, and hyperglycemia (pH of 7.14, anion gap of 24, bicarbonate 6 mmol/l, urinary ketones 150 mg/dl, glucose 314 mg/dl) consistent with the diagnosis of DKA. His white blood count was 20,400/l. Urinalysis demonstrated no evidence of infection. The patient’s hemoglobin A1c (A1C) was 13.5%.
Case Presentation The patient was admitted and treated aggressively
with intravenous fluid and an insulin-glucose infusion.
A non-contrast magnetic resonance imaging (MRI) of the lumbosacral spine (L-spine) was obtained because of the patient’s persistent complaint of lower back pain. The Lspine MRI results were negative for pathology. However, R.T. reported increasing discomfort and now noted weakness and numbness in his bilateral lower extremities.
Case Presentation Neurology was consulted, and during their
assessment, the patient became incontinent and was found to have 0/5 strength in the lower extremities, severely compromised sensation, and decreased rectal tone. A contrast MRI of both the thoracic and lumbar spine was ordered, and the patient was found to have a T10–T12 epidural abscess. The patient’s antibiotic coverage was broadly expanded, high-dose intravenous steroids were initiated, and neurosurgery was urgently consulted. Emergent evacuation of the epidural abscess with laminectomies of T10–T12 was performed without complication.
Case Presentation
R.T.’s neurogenic bladder resolved without further intervention. After intensive inpatient rehabilitation, he had 3/5 strength in bilateral lower extremities and was still unable to ambulate.
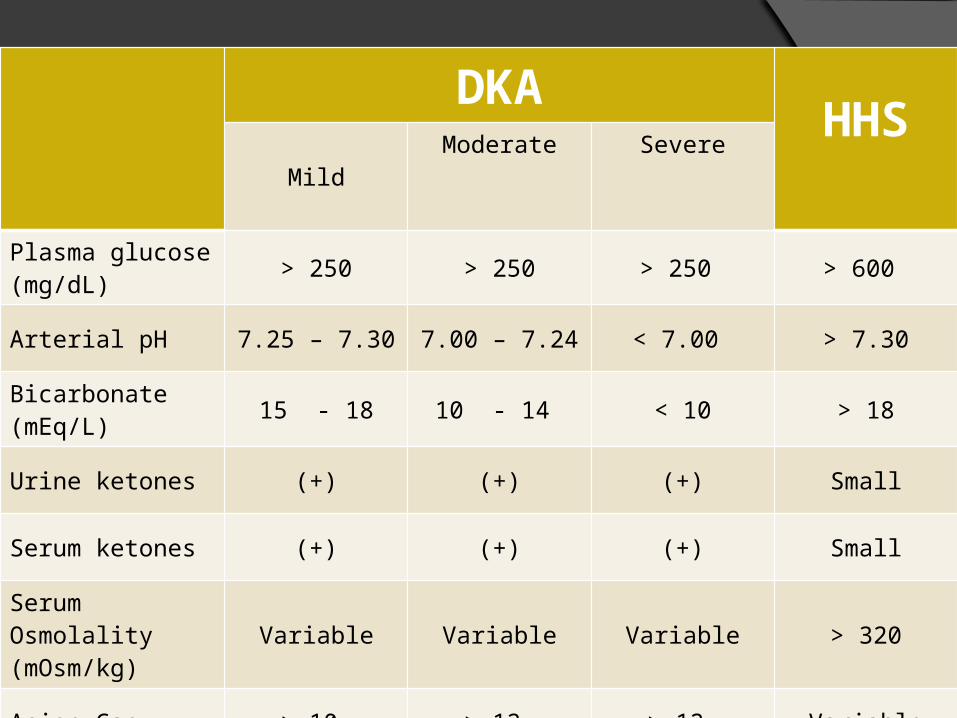
DKAHHS
MildModerate Severe
Plasma glucose (mg/dL)
> 250 > 250 > 250 > 600
Arterial pH 7.25 – 7.30 7.00 – 7.24 < 7.00 > 7.30
Bicarbonate (mEq/L)
15 - 18 10 - 14 < 10 > 18
Urine ketones (+) (+) (+) Small
Serum ketones (+) (+) (+) Small
Serum Osmolality (mOsm/kg)
Variable Variable Variable > 320
Anion Gap > 10 > 12 > 12 Variable
Consciousness Alert Alert/drowsy Stupor/Coma Stupor/Coma
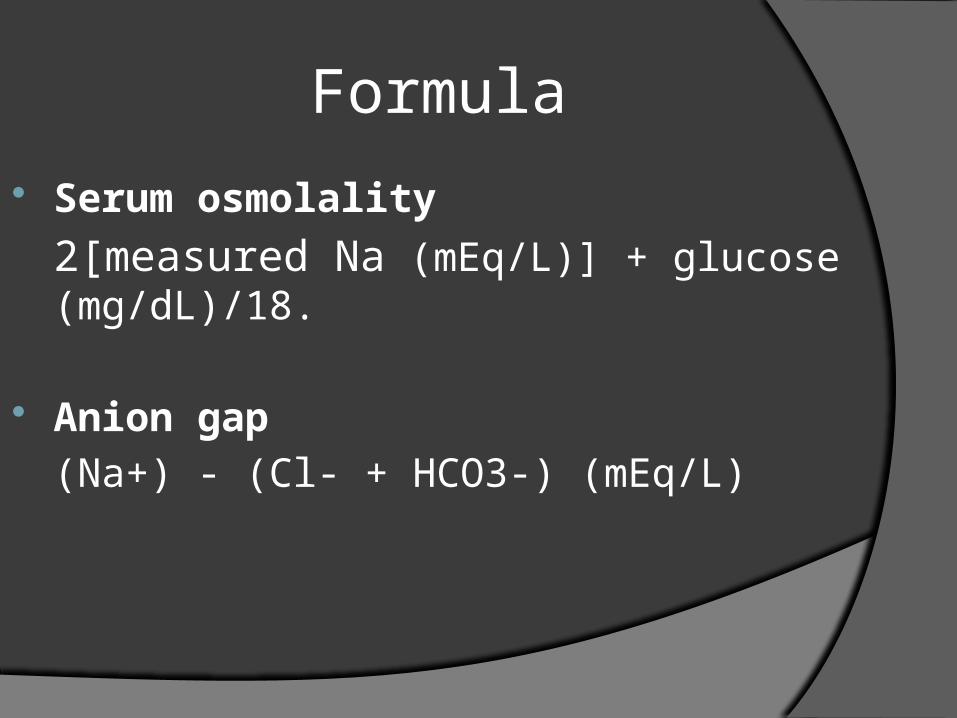
Formula
Serum osmolality
2[measured Na (mEq/L)] + glucose (mg/dL)/18.
Anion gap
(Na+) - (Cl- + HCO3-) (mEq/L)
Precipitating Factors
Infection (pneumonia, UTI) Inadequate insulin therapy Acute myocardial infarction, stroke,
pancreatitis New onset DM type 1 (especially DKA)
Anamnesis
Symptoms of marked hyperglycemia: polyuria, polydipsia, and weight loss
Neurologic symptoms: lethargy, coma Hyperventilation and abdominal pain:
limited to patients with DKA
Pathophysiology
Hyperosmolarity neurologic symptoms (more frequent in HHS because greater degree of hyperosmolarity in HHS than DKA hemiparesis or hemianopsia, and/or seizures
Severe acidosis in DKA neurologic symptoms
Pathophysiology
Osmotic diuresis: glucose osmotic diuresis water loss in excess of sodium and potassium hyperosmolar state
The presence of stupor or coma in diabetic patients with an effective plasma osmolality lower than 320 mosmol/kg demands immediate consideration of other causes of the mental status change.
Pathophysiology
Abdominal pain in DKA: has never been found in HHS
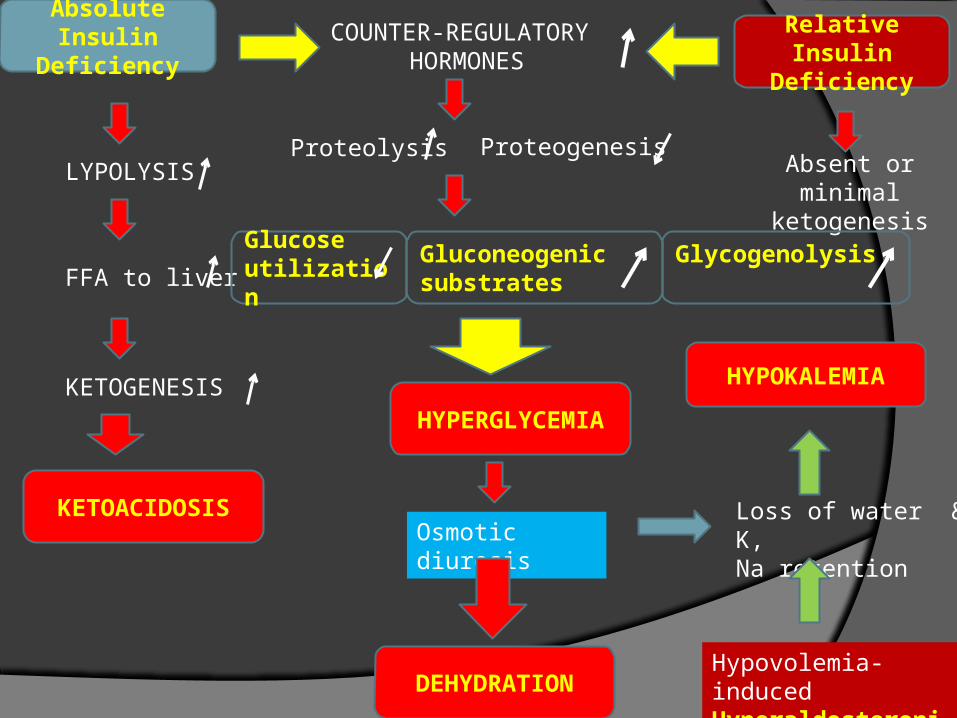
Absolute Insulin Deficiency
LYPOLYSIS
FFA to liver
KETOGENESIS
KETOACIDOSIS
COUNTER-REGULATORY HORMONES
Relative Insulin Deficiency
Absent or minimal ketogenesis
Proteolysis Proteogenesis
Gluconeogenic substrates
Glucose utilization
Glycogenolysis
HYPERGLYCEMIA
Osmotic diuresisLoss of water & K,Na retention
DEHYDRATIONHypovolemia-induced Hyperaldosteronism
HYPOKALEMIA
Clinical features of DKA DKA usually evolves rapidly over a 24-hour period. Common, early signs of ketoacidosis include nausea,
vomiting, abdominal pain, and hyperventilation. The earliest symptoms of marked hyperglycemia are
polyuria, polydipsia, and weight loss. As hyperglycemia worsens, neurologic symptoms appear, and may progress to include lethargy, focal deficits, obtundation, seizure, and coma.
Common causes of DKA include: infection; noncompliance, inappropriate adjustment, or cessation of insulin; new onset diabetes mellitus; and myocardial ischemia.
Evaluation and laboratory findings of DKA Assess vital signs, cardiorespiratory status, and
mental status. Assess volume status: vital signs, skin turgor,
mucosa, urine output. Obtain the following studies: serum glucose,
urinalysis and urine ketones, serum electrolytes, BUN and creatinine, plasma osmolality, arterial blood gas, venous blood gas, electrocardiogram; add serum ketones if urine ketones present.
Additional testing is obtained based on clinical circumstances and may include: blood or urine cultures, lipase, chest x-ray.
Evaluation and laboratory findings of DKA Diabetic ketoacidosis (DKA) is characterized by
hyperglycemia, an elevated anion gap metabolic acidosis, and ketonemia. Dehydration and potassium deficits are often severe.
Serum glucose is usually greater than 250 mg/dL (13.9 mmol/L) and less than 800 mg/dL (44.4 mmol/L). In certain instances (eg, insulin given prior to ED arrival), the glucose may be only mildly elevated.
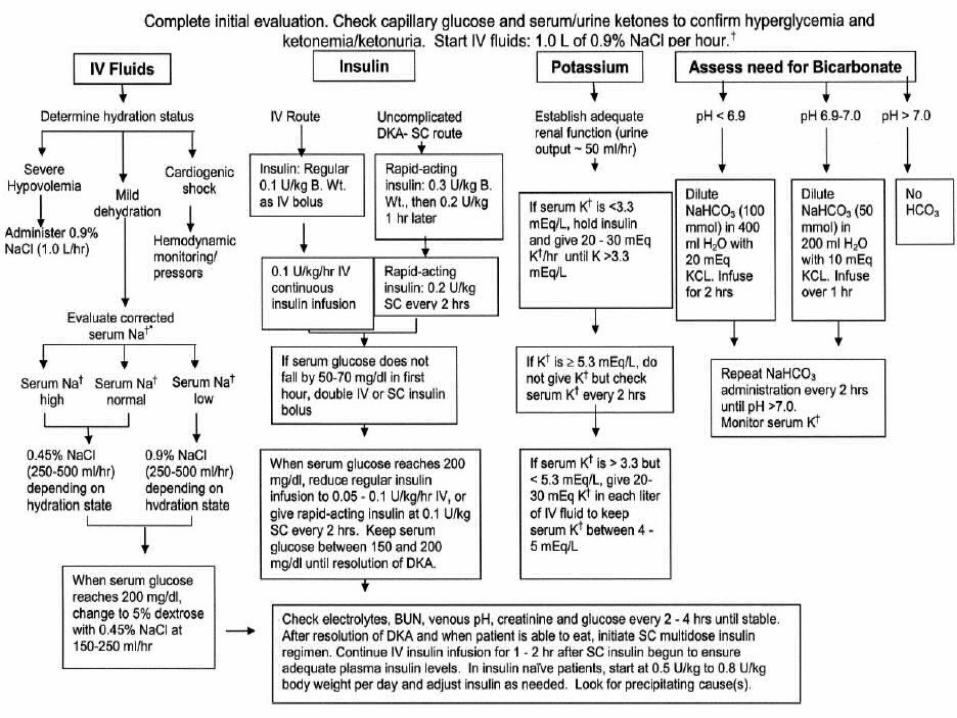
Management of DKA: Replete fluid deficits
Give several liters of isotonic (0.9 percent) saline as rapidly as possible to patients with signs of shock.
Give isotonic saline at 15 to 20 mL/kg per hour, in the absence of cardiac compromise, for the first few hours to hypovolemic patients without shock.
After intravascular volume is restored, give one-half isotonic (0.45 percent) saline at 4 to 14 mL/kg per hour if the corrected serum sodium is normal or elevated; isotonic saline is continued if the corrected serum sodium is reduced.
Add dextrose to the saline solution when the serum glucose reaches 200 mg/dL (11.1 mmol/L).
Management of DKA: Replete K+ deficits
Regardless of the initial measured serum potassium, patients with DKA have a large total body potassium deficit.
If initial serum K+ is below 3.3 mEq/L, hold insulin and give K+ 20 to 30 mEq/hour IV until K+ concentration is above 3.3 mEq/L.
If initial serum K+ is between 3.3 and 5.3 mEq/L, give K+ 20 to 30 mEq per liter IV fluid; maintain K+ between 4 to 5 mEq/L.
If initial serum K+ is above 5.3 mEq/L do not give K+; check K+ every 2 hours.
Management of DKA: Give insulin
Do not give insulin if initial serum K+ is below 3.3 mEq/L; replete K+ first.
Give all patients without a serum K+ below 3.3 mEq/L regular insulin. Either of two regimens can be used: 0.1 units/kg IV bolus, then start a continuous IV infusion 0.1 units/kg per hour; OR do not give bolus and start a continuous IV infusion at a rate of 0.14 units/kg per hour.
Continue insulin infusion until ketoacidosis is resolved, serum glucose is below 200 mg/dL (11.1 mmol/L), and subcutaneous insulin is begun.
Management of DKA: Give sodium bicarbonate to patients with pH below 7.00
If the arterial pH is between 6.90 and 7.00, give 50 meq of sodium bicarbonate plus 10 meq of potassium chloride in 200 mL of sterile water over two hours.
If the arterial pH is below 6.90, give 100 meq of sodium bicarbonate plus 20 meq of potassium chloride in 400 mL sterile water over two hours.
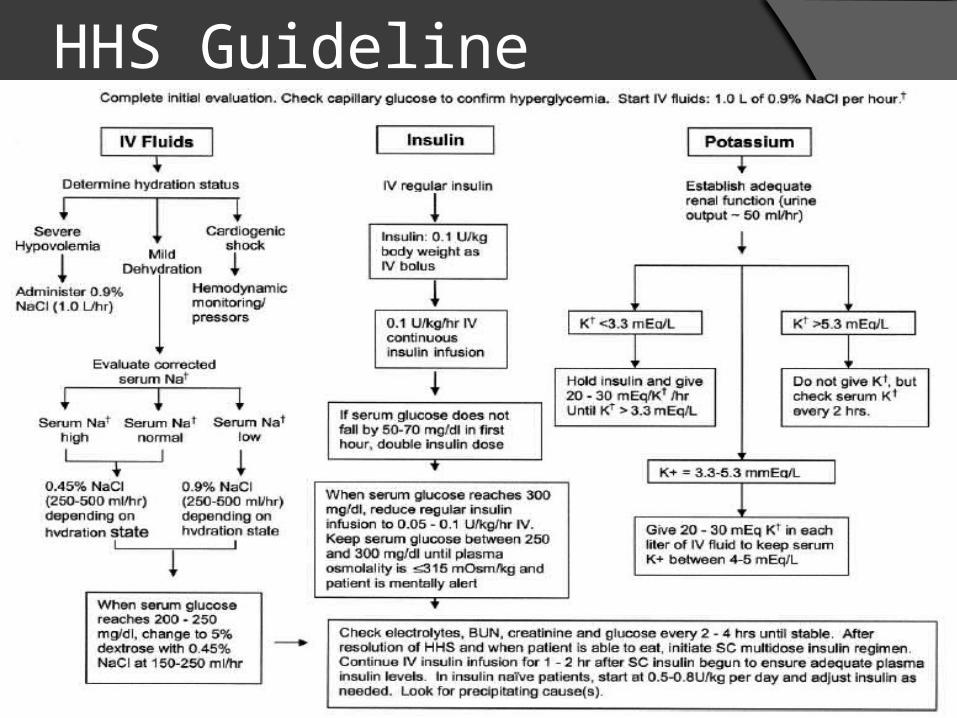
HHS Guideline
HYPOGLYCEMIA
Blood glucose < 70 mg/dL
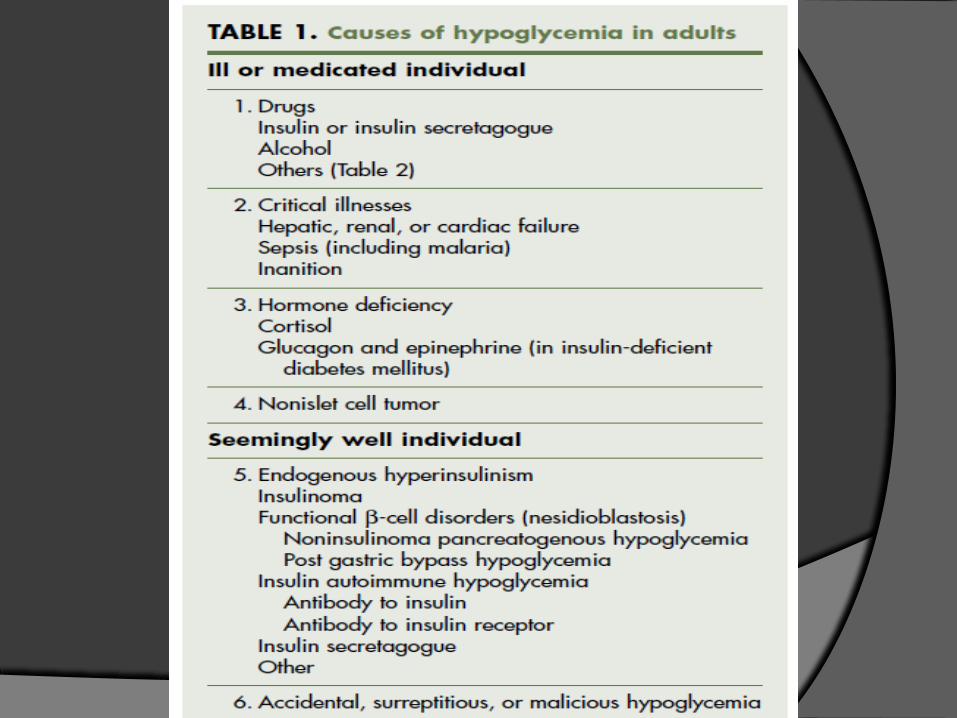
Although a comatose diabetic patient may have marked hyperglycemia (with
or without ketoacidosis) rather than hypoglycemia, these disorders can be
distinguished by estimating blood glucose with a glucose stick. If this is not available, then glucose should be
given empirically. This will correct hypoglycemia and will not be
particularly deleterious if the blood glucose concentration is high.


















