Diuretics - PBworks
15
Diuretics • Dr. Majdi Bkhaitan • Department of Pharmaceutical Chemistry • www.medchem1432.pbworks.com • www.uqu.edu.sa/mmbakhaitan Clinical Significance It is important for the clinician to understand the medicinal chemistry of the diuretics to appropriately use them in individual patients. This diverse group of medications is classified in many ways: mechanism of action, site of action, chemical class, and effect on urine contents. Knowledge of structure–activity relationships helps to predict indications, possible off- label uses, magnitude of diuresis, potency, and side effect profile. Consequently, diuretics have a variety of uses. Thiazide diuretics may be used either alone or in combination with other pharmacotherapy for the treatment of hyper tension. Loop diuretics can provide immediate diuresis and are used for heart failure and in lieu of thiazides in patients with compromised renal function. In addition to more traditional uses, certain potassium-sparing diuretics provide added benefit to other pharmacotherapy in patients with primary hyperaldosteronism, heart failure, or post –acute myocardial infarction. Carbonic anhydrase inhibitors have limited use for diuresis; however, they may be used to reduce intraocular pressure and treat acute mountain sickness. A thorough understanding of the medicinal chemistry, mechanisms of action, and pharmacokinetics helps the clinician to use available diuretics appropriately. As new medications are developed, the clinician will rely on these basic concepts to continue tailoring therapy to the individual patient with the goals to maximize outcomes, improve quality of life, and minimize adverse events. Kimberly Birtcher Pharm.D. Clinical Assistant Professor, Department of Clinical Sciences and Administration, University of Houston College of Pharmacy Diuretics Primary target of diuretics is the kidney, where these compounds interfere with the re-absorption of sodium and other ions from the Lumina of nephrons. Definition Diuretics are chemicals that increase the rate of urine formation. By increasing the urine flow rate, diuretic usage leads to increased excretion of electrolytes (especially sodium and chloride ions) and water from the body without affecting protein, vitamin, glucose, or amino acid reabsorption. These pharmacological properties have led to the use of diuretics in the treatment of edematous conditions resulting from a variety of causes (e.g., congestive heart failure,
Transcript of Diuretics - PBworks

Diuretics
• Dr. Majdi Bkhaitan
• Department of Pharmaceutical Chemistry
• www.medchem1432.pbworks.com
• www.uqu.edu.sa/mmbakhaitan
Clinical Significance
It is important for the clinician to understand the medicinal chemistry of the diuretics to appropriately use
them in individual patients. This diverse group of medications is classified in many ways: mechanism of
action, site of action, chemical class, and effect on urine contents. Knowledge of structure–activity
relationships helps to predict indications, possible off- label uses, magnitude of diuresis, potency, and side
effect profile.
Consequently, diuretics have a variety of uses. Thiazide diuretics may be used either alone or in
combination with other pharmacotherapy for the treatment of hyper tension. Loop diuretics can provide
immediate diuresis and are used for heart failure and in lieu of thiazides in patients with compromised
renal function. In addition to more traditional uses, certain potassium-sparing diuretics provide added
benefit to other pharmacotherapy in patients with primary hyperaldosteronism, heart failure, or post–acute
myocardial infarction. Carbonic anhydrase inhibitors have limited use for diuresis; however, they may be
used to reduce intraocular pressure and treat acute mountain sickness.
A thorough understanding of the medicinal chemistry, mechanisms of action, and pharmacokinetics helps
the clinician to use available diuretics appropriately. As new medications are developed, the clinician will
rely on these basic concepts to continue tailoring therapy to the individual patient with the goals to
maximize outcomes, improve quality of life, and minimize adverse events.
Kimberly Birtcher Pharm.D.
Clinical Assistant Professor, Department of Clinical Sciences and Administration,
University of Houston College of Pharmacy
Diuretics Primary target of diuretics is the kidney, where these compounds interfere with the
re-absorption of sodium and other ions from the Lumina of nephrons.
Definition
Diuretics are chemicals that increase the rate of urine formation. By increasing the urine flow
rate, diuretic usage leads to increased excretion of electrolytes (especially sodium and chloride
ions) and water from the body without affecting protein, vitamin, glucose, or amino acid
reabsorption. These pharmacological properties have led to the use of diuretics in the treatment
of edematous conditions resulting from a variety of causes (e.g., congestive heart failure,

nephrotic syndrome, and chronic liver disease) and in the management of hyper tension. Diuretic
drugs also are useful as the sole agent or as adjunct therapy in the treatment of a wide range of
clinical conditions, including hypercalcemia, diabetes insipidus, acute mountain sickness,
primary hyperaldosteronism, and glaucoma.
Functions of the kidney
• To maintain a homeostatic balance of electrolytes and water.
• To excrete water-soluble end products of metabolism.
Uses
• Treatment of different edematous conditions, resulting from a variety of
causes (e.g. congestive heart failure, nephrotic syndrome, and chronic
liver disease).
• Management of hypertension.
• Adjunctive therapy in the treatment of a wide range of clinical conditions,
including hypercalcemia, acute mountain sickness, primary
hyperaldosterism, glaucoma and mountain sickness.
Physiology
• Urine formation begins with the filtration of blood at the glomerulus.
Approximately 1,200 mL of blood per minute flows through both kidneys and
reaches the nephron by way of afferent arterioles.
• Approximately 20% of the blood entering the glomerulus is filtered into
Bowman's capsule to form the glomerular filtrate.
• The glomerular filtrate is composed of blood components with a molecular weight
less than that of albumin (~69,000 daltons) and not bound to plasma proteins.
• The glomerular filtration rate (GFR) averages 125 mL/min in humans but can
vary widely even in normal functional states.
• The glomerular filtrate leaves the Bowman's capsule and enters the proximal
convoluted tubule where the majority (50–60%) of filtered sodium is reabsorbed
osmotically. Sodium reabsorption is coupled electrogenetically with the
reabsorption of glucose, phosphate, and amino acids and non-electrogenetically
with bicarbonate reabsorption.
• Glucose and amino acids are completely reabsorbed in this portion of the
nephron, whereas phosphate reabsorption is between 80 and 90% complete.

• The early proximal convoluted tubule also is the primary site of bicarbonate
reabsorption (80–90%) , a process that is mainly sodium dependent and coupled
to hydrogen ion secretion.
• The reabsorption of sodium and bicarbonate is facilitated by the enzyme carbonic
anhydrase, which is present in proximal tubular cells and catalyzes the formation
of carbonic acid from water and carbon dioxide.
• The carbonic acid provides the hydrogen ion, which drives the reabsorption of
sodium bicarbonate. Chloride ions are reabsorbed passively in the proximal
tubule, where they follow actively transported sodium ions into tubular cells.
•
There are four Anatomical sites for diuretic action in the nephron: • Site 1: proximal convoluted tubule.
• Site 2: thick ascending Henle’s loop (TAL)
• Site 3: distal tubule
• Site 4: connecting tubule and collecting duct.

Site 1 diuretics “Carbonic anhydrase inhibitors” “CA inhibitors”:
• These are infrequently used as diuretics, because of their low efficacy and
the early development of tolerance. They played, however, an important
role in the development of other major classes of diuretics that are
currently largely used.
There are two groups of CA inhibitors:
• Simple heterocyclic sulfonamides
• Metadisulfamoylbenzene derivatives.

SAR
• In case of the simple heterocyclic compounds:
• The unsubstituted sulfonamide is essential for the diuretic activity.
• This sulfonamide group has to be attached directly to an aromatic group.
• The derivative with the highest Pc “partition coefficient” and the lowest
ionization “pKa” has the greatest CA inhibitory and diuretic activities.
In case of metadisulfamoylbenzene derivatives series:
• The parent 1,3 metadisulfamoylbenzene lacked diuretic activity.
• Key substitutions in 4 and 5 positions lead to compounds with diuretic
activity.
Site and Mechanism of action
• CA is located both intracellularly and in the luminal brush border membrane of
proximal convoluted tubule cells; these two sites are targets of CA inhibitors.
• During the first 4-7 days of treatment, we observe an excretion in sodium and
bicarbonate. We observe also an increase in potassium excretion, because the
proximal tubule actions of CA inhibitors present a greater percentage of the
Cl
S
O
O
H2N
Cl
S
O
O
NH2
Dichlorphenamide Chloraminophenamide
NH2Cl
S
O
O
H2N S
O
O
NH2
NN
S N H C
O
C H 3S
O
O
H 2 N
A c e t o z o l a m i d e
NN
S N C
O
C H 3S
O
O
H 2 N
C H 3
M e t h a z o l a m i d e

filtered load of sodium at site 4, this with other factors increases the exchange of
the luminal fluid sodium for intracellular potassium at site 4.
T
Therefor CA inhibitors are considered:
• Natriuretic(increse the execretion of Sodium)
• Bicarbonaturetic (increse the execretion of bicarbonate)
• Kaluretic (increse the execretion of Potassium)
• Toward the end of the first week of continuous therapy with CA inhibitors,
resistance to its diuretic effect develops. This is due primarily to two factors. First,
there is a marked reduction in the filtered load of Bicarbonate because CA
inhibitors produce both a reduction in the plasma concentration of Bicarbonate
and a 20% reduction in the GFR (glomerular filtration rate).
• When there is less bicarbonate present in the luminal fluid, there is less
bicarbonate reabsorption to inhibit.
• Second, the metabolic acidosis created by these diuretics provides a sufficient
amount of non-CA generated intracellular hydrogen ions to exchange for the

luminal fluid sodium. Sodium reabsorption at site1 progressively returns to
normal and the diuresis disappears.
Uses:
• Primarily in the treatment of glaucoma, by inhibiting CA in the eye,
reducing the formation of aqueous humor in the eye.
• In the prophylaxis of mountain sickness, Adjuvant in the treatment of
epilepsy, to create alkaline urine when it is needed.
Adverse effects:
• Metabolic acidosis, Hypokalemia, Typical sulfonamide-associated
hypersensitivity reactions, such as urticaria, drug fever, blood dyscrasias,
and interstitial nephritis.
Products
Simple heterocyclic sulfonamides: Acetozolamide ,Methazolamide
Metadisulfamoylbenzene derivatives: Dichlorphenamide: Given orally
• Chloraminophenamide: Doesn’t possess oral
bioavailability. It is a precursor for site 3
diuretics
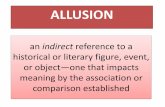
Site 3 diuretics: Thiazide and Thiazide-like derivatives
• Chloraminophenamide became a logical key intermediate in the development of a
new class of Diuretics.
• In fact, when
Chloraminophenami
de was treated with
an acylating reagent,
cyclization occured,
with the result of
formation 1,2,4-
thiadiazine-1,1-
dioxide “ thiazide
derivatives”.
• On the other hand,
when
Chloraminophenamide is treated with aldehyde or ketone, in place of the acylating
reagent, this produces the corresponding hydrothiazide derivatives.
SN H
N R
O O
X
S
O
O
N H 2
SN H
N R
O O
X
S
O
O
N H 2
H
H
T h i a z i d e
H y d r o t h i a z i d e
C h l o r a m i n o p h e n a m i d e
N H 2C l
S
O
O
H 2 N S
O
O
N H 2
RC
OC l
RC
OR

These represent the first oral active saluretic agents (increase the excretion of NaCl).
Site and Mechanism of action
• These agents block the reabsorption of sodium (and thereby the reabsorption of
chloride) in the distal convoluted tubules by inhibiting the luminal membrane
bound Na+/Cl- cotransport system.
• Thus, all diuretics in this class are responsible for the urinary loss of about (5-
8%) of the filtered load of sodium. Although they differ in their potencies, they
are equally efficacious.
• As a result of their action, these diuretics deliver more sodium to site 4, resulting
in an increase exchange between Na and K, producing also K elimination.
• On the other hand this family possesses a residual CA inhibition producing a very
mild elimination of HCO3-.
Site 3 diuretics are considered
• Natriuretic chloruretic, saluretic kaliuretic and extremely weak
bicarbonaturetic agents.
SAR
• Position 2 can tolerate the presence of a small alkyl group (such as a CH3 or
better an H)
• Position 3 is an extremely important site of
molecular modification. In fact, substituents at
position 3 play an important role in determining
the potency, duration of action, and other
pharmacokinetic properties of the derivative.
• Loss of double bond between C3-C4 increases the
potency approximately of 3-10 folds “this means
that in general, hydrothiazide derivatives are more
potent than thiazide derivatives”.
• Direct substitution for the 4,5, and 8 position results in an activity decrease.
• Substitution at position 6 with a deactivating group “ such as Cl, Br, CF3,
CHCl3, i.e. electron withdrawing groups” is essential for the activity.
• The unsubstituted sulfonamide group in position 7 is a prerequisite for the
activity.
SN H
N
O O
H
1
2
3
4
5
6
7
8

• Substitution of the sulfone group in position 1 with another similar electrophilic
group (carboxyl, carbamoyl) can produce an activity increase.
Products
• Thiazide derivatives
• Chlorthiazide ( X= Cl, R=H)
• Benthizide (X= Cl, R= CH2-CH2-Ph)
Hydrothiazide derivatives
Hydrochlorthiazide ( X= Cl, R=H)
Hydroflumethiazide ( X= CF3, R=H)
Trichlomethiazide ( X= Cl, R=CHCl2)
• Thiazide like derivatives
• Meta disulfamoyl benzens
• Mefruside
• Salicylanilide
• xipamide
• Benzhydrazides
• Indapamide
• Phthalimidines
• Chlorthalidone
• Others
• Metolazone,etc.
These diuretics were developed as an outgrowth of the thiazide research that involved molecular
modification of aromatic sulfamoyl-containing compounds.
SNH
N R
O O
X
S
O
O
NH2
SNH
N R
O O
X
S
O
O
NH2
H
H

Uses
• Treatment of edema associated with mild to moderate congestive heart
failure, hepatic cirrhosis, and nephrotic syndrom. This after treating the
underlying cause of the disease.
• In the treatment of hypertension, either alone or in combination with other
drugs depending on the severity of the condition.
• An advantage in their use as antihypertensive agents is that their diuretic
effect is weakened after one week of use but their antihypertensive effect
remains.
• Treatment of type II renal tubular acidosis.
Adverse effects
• Typical sulfonamide-associated hypersensitivity reactions, such as
urticaria, drug fever, blood dyscrasias, and interstitial nephritis. This is
usually a crossed hypersensitivity, even with other agents of other sites
diuretics, containing sulfonamide groups
• Hypokalemia.
• Acute reduction in GFR, and Hyperglycemia.
Site 2 Diuretic “High ceiling” “loop” diuretics
• The diuretics that belong to this class are of diverse chemical structure. And these
are:
• 5-sulfamoyl-2-aminobenzoic acid derivatives “anthranilic acid
derivatives”. E.g. Furosemide, Azosemide.
• 5-sulfamoyl-3-aminobenzoic acid derivatives “metanilic acid
derivatives”. E.g. Bumetanide, Piretanide.
• Phenoxyacetic acid derivatives. E.g. ethacrynic acid.
• 4-amino-3-pyridine sulfonylurea. E.g. Torsemide.
• Organomercurials “not in use because not available orally and for other
unfavorable conditions”.

Site and mechanism of action
• These diuretics have a tremendous efficacy because they inhibit the Na/K/2Cl co-
transport system located on the luminal membrane of cells of the thick ascending
limb of Henle’s loop. Importantly, the carboxylate moieties of Furosemide and
Bumetanide are thought to be responsible for their competing with Cl- for the Cl-
binding site on the Na/K/2Cl co-transport system.
• Because site 2 is such a high capacity site for Na reabsorption, up to (20-25%) of
the filtered load of Na that normally is absorbed in this nephron segment may be
excreted in the urine. On the other hand this inhibition destroys the hypertonicity
of the medullar interstitium preventing the reabsorption of water at the descending
limb of Henle’s loop.
• Other factors and mechanisms participate also to make of this class the most
efficacious of all diuretics.
• All diuretics acting on site 2 are
equally efficacious (20-25%), and are
more efficacious than any other
diuretic acting on other sites. Site 2
diuretics are referred to according to
the site of action or efficacy as “loop”
or High ceiling” diuretics.
• The high ceiling diuretics enhance
the urinary loss of K+ and H+,
because they block the reabsorption
of K+ at site 2, and they deliver
more of the filtered load of sodium
at a faster rate to site 4. This leads to an enhanced exchange of the luminal fluid
sodium ions for the potassium ions and the hydrogen atoms.
• When the loop diuretics are used in “submaximal” doses for the treatment of
hypertension, they produce diuresis comparable of thiazide diuretics with little
effect upon potassium elimination, on the other hand their use in their maximum
potency they produce serious hypokalemia.
Uses
• Treatment of edema that may accompany congestive heart failure,
cirrhosis of the liver and nephrotic syndrome.

• In particular high ceiling diuretics are agents of choice in the treatment of
pulmonary edema. No other group of diuretics is more effective than the
loop diuretics in this situation.
• Treatment of symptomatic hypercalcemia.
• In the treatment of hypertension, even though thiazides are more advised
because of their longer duration of action and their less toxicity.
Adverse effects
• Hypokalemia. Caution should be taken in case of combined treatment with
cardiac glycosides, because hypokalemia intensifies the toxicity of the
cardiac glycosides.
• Reduction in GFR, observed only in long term therapies.
• Typical sulfonamide-associated hypersensitivity reactions, such as
urticaria, drug fever, blood dyscrasias, and interstitial nephritis. This is
usually a crossed hypersensitivity, even with other agents of other sites
diuretics, containing sulfonamide groups.
• Ototoxicity, usually transient.
SAR
Regarding the anthranilic acid and metanilic acid derivatives
• The substituent at C1 must be acidic, the best possible acidic group is the
carboxyl group (COOH), other acidic functions (such as the tetrazole
ring), however, maintain the diuretic activity.
• A sulfamoyl group in position 5 is a prerequisite for the high ceiling
diuretic activity.
• The electron withdrawing group at C4 can be Cl, CF3, or yet better a
phenoxy, alkoxy, anilino, benzyl, or benzoyl group.
• Only furfyryl, benzyl, thienylmethyl groups are allowed in position 2 in
the anthranilic acid derivative, however we can observe decreased activity
going from the furfyl and on.
• In case of metanilic acid derivatives a wide range of substituents are
tolerated.
Regarding the anthranilic acid and metanilic acid derivatives

• The substituent at C1 must be acidic, the best possible acidic group is the
carboxyl group (COOH), other acidic functions (such as the tetrazole
ring), however, maintain the diuretic activity.
• A sulfamoyl group in position 5 is a prerequisite for the high ceiling
diuretic activity.
• The electron
withdrawing group at
C4 can be Cl, CF3, or
yet better a phenoxy,
alkoxy, anilino,
benzyl, or benzoyl
group.
• Only furfyryl, benzyl,
thienylmethyl groups
are allowed in
position 2 in the
anthranilic acid
derivative, however we can observe decreased activity going from the
furfyl and on. In case of metanilic acid derivatives a wide range of
substituents are tolerated.
Site 4 diuretics “Potassium sparing” or “Antikaluretic” Diuretics.
• A negative feature of all previous diuretic classes is that they induce an
increase in the renal excretion rate of potassium. Potassium sparing
diuretics increase sodium and chloride secretion without causing an
increase in potassium excretion.
• Potassium sparing diuretics are derived from different chemical roots, they
have however, similar anatomic site of action in the nephron, efficacy, and
electrolyte excretion pattern. They even share certain adverse effects.
The Potassium sparing diuretics include
Spirolactones
Spironolactone
Canrenone
The 2,4,7-triamino-6- arylpteridine
Ttrimeteren
The pyrazinoylguanidine
Amiloride
Bumetanide
COOHS
O
O
H2N
O
NH
C4H9
Furosemide
COOH
NH CH2
OCl
S
O
O
H2N
NH CH2
OCl
S
O
O
H2N
N N
NN
COOHS
O
O
H2N
ON
Azosemide
Piretinide
1
23
4
56
65
4
3
2
1

Spirolactones (e.g. spironolactone)
• Spironolactone is a structural similar of progesterone. Progesterone was
observed to possess an antialdosteronic activity, inhibiting the
antitinatriuretic and kaluretic activity.
• Phramacokinetic • Spironolactone is absorbed well after oral administration (>90%);
biotransformed rapidly and extensively by the liver (about 80%) to
canrenone, an active
metabolite and excreted
primarily as metabolites in
urine.
Phramacokinetic
• Spironolactone is absorbed
well after oral administration
(>90%); biotransformed
rapidly and extensively by
the liver (about 80%) to
canrenone, an active
metabolite and excreted
primarily as metabolites in
urine. Spironolactone metabolism
Site and Mechanism of action
• Spironolactone inhibits the reabsorption of (2-3%) of the filtered load of
sodium at site 4 by competitively inhibiting the actions of aldosterone.
This inhibition prevents the biosynthesis of transport proteins such as
Na,K ATPase, luminal membrane channels that are involved in the
exchange of sodium for potassium, and the H+ ATPase that actively
pumps H+ into the luminal fluid at site 4.
• Thus inhibiting the passage of luminal fluid sodium into and potassium
and H+ out of the late distal convoluted tubule and early collecting tubule
cells.
O
O
O
S C
O
CH3
O
O
O
Metabolism in liver

Spironolactone is Natriuretic, chloruretic, saluretic and Antikaluretic agent. It is considered to
be a very weak diuretic and of low efficacy (2-3%)
Uses
It may be used for the following indications
• To remove edema from individuals suffering Congestive heart failure,
cirrhosis, or nephrotic syndrome
• Antihypertensive agent.
• Primarily it is used in combination with diuretics that act at site 2 or 3 in
an attempt to reduce the urinary potassium loss associated with these latter
groups of diuretics.
• The principal side effect is hyperkalemia and mild metabolic acidosis.
2,4,7-triamino-6-arylpteridine “Trimeteren” & The pyrazinoylguanidine “Amiloride”.
• These agents are both well absorbed orally and act by the plugging the sodium
channel in the luminal membrane of the principal cells at site 4. And thereby
inhibits the electrogenic entry of 2-3% of the filtered load of sodium into these
cells.
• Because the secretion of potassium and H+ at site 4 is linked to sodium
reabsorption, a concomitant reduction in the excretion rate of potassium and H+
occurs. The presence of aldosterone is not a prerequisite for the activity of these
agents.
• They are considered mild diuretics. They are Natriuretic, chloruretic, saluretic
and Antikaluretic agent.
N
N N
N
H2N
H2N
H2NN
N
H2NH2N
Cl C
O
C
NH
NH2NH
Amiloride Trimeterene