Distal Single-Incision, Scope-Assisted Carpal Tunnel Release · Inspect the median nerve or the...
12
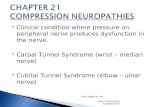
final image to come UPPER EXTREMITY Radius Retractor Median Nerve & its Branches Slotted Cannula Superficial Palmar Arch Incision Scope Mounted Blade Cutting TCL Carpal Ligament Ulna Distal Single-Incision, Scope-Assisted Carpal Tunnel Release Surgical Technique
Transcript of Distal Single-Incision, Scope-Assisted Carpal Tunnel Release · Inspect the median nerve or the...

final image to come
UPPER EXTREMITY
Radius
Retractor
MedianNerve & its
Branches
SlottedCannula
SuperficialPalmar Arch
Incision
Scope Mounted BladeCutting TCL
Carpal Ligament
Ulna
Distal Single-Incision,Scope-Assisted Carpal Tunnel Release
Surgical Technique

Our mission is to develop and produce medical/surgical productsthat are unsurpassed in quality, safety, and simplicity – products that are intuitive for the medical professional,
while providing the patient with the benefits of minimally invasive techniques and rapid recovery times.
Our goal is to be recognized as a leader in developing innovative solutions that are
successful in the medical field.

Distal Single-Incision,Scope-Assisted Carpal Tunnel Release
Surgical TechniqueAther Mirza, MD
Chief of Hand and MicrosurgerySt. Catherine of Siena Medical Center
Assistant Clinical ProfessorSUNY at Stony Brook
Chairman of the BoardNorth Shore Surgery Center
1
UPPER EXTREMITY
IndicationsCarpal tunnel release is indicated in the majority of thosepatients who fail to respond to conservative treatment ofcarpal tunnel syndrome.
ContraindicationsSurgeons should follow the general contraindicationsapplicable to open carpal tunnel release when consider-ing a patient for endoscopic carpal tunnel release. Inaddition, patients with stiff wrists, suspected space-occupying lesions, or other anatomical abnormalitiesshould be excluded.
TrainingFor safe and effective use, surgeons must possess athorough knowledge and understanding of wristanatomy and endoscopic technique using this instru-mentation. Instructional videotapes and cadaverworkshops are available through A.M. Surgical.
Warning: Failure to follow the surgical techniquemay result in permanent injury to the patient. If,while performing this technique, any problemshould arise, such as anatomical anomalies, inade-quate visualization, inability to identify anatomy,or questions concerning technique or instrumenta-tion, the surgeon should abandon the endoscopiccarpal tunnel release and convert to an open carpaltunnel release.
Single Case ofInstruments
Locking Device
ScopeMountingBlade
Obturator Elevator
Rasp SlottedCannula

IntroductionThe advantages of endoscopic carpal tunnel release (ECTR)have been well documented. They include smaller inci-sion(s) with less pain, early recovery and early return towork. Concerns with the various endoscopic techniquesinclude potential complications, as well as steeper learningcurves versus open carpal tunnel release.
The Distal Single-Incision, Scope-Assisted CTR techniqueaddresses these concerns. The one small incision in thepalm permits direct visualization of key anatomy, whilethe instrument design allows for endoscopic visualizationof the median nerve, flexor tendons, and transverse carpalligament (TCL). This technique is less likely to injure thevital structures. The release of the TCL is performed with adistal-to-proximal pass of the patented scope mountingblade which mounts onto a standard endoscope. (See page 7for instrumentation required for this procedure.)
Operative Technique
Positioning of Patient
The hand is secured to the hand table with the wrist inneutral position (Figure 1). (For use of A.M. Surgical HandTable, see diagram on page 9.)
Marking the Skin
Two lines are drawn in the palm: one longitudinal and inline with the third web space; the other, transversely acrossfrom the fully abducted thumb (Figure 2).
The 1.5 cm incision is outlined 0.5 cm proximal to the inter-section of these two lines, preferably in a palmar skincrease (Figure 2). A larger incision can be made while thesurgeon is gaining experience with this technique.
Two lines are then drawn in the distal forearm to identifythe location of the palmaris longus and flexor carpi ulnaristendon. An "x" is placed midway between these two lines.This is done to aim the cannula between the median andulnar neurovascular structures (Figure 2).
1
2
2 Safety • Vision • Quality
Fig. 1
Fig. 2

Incision
The skin is incised using the previously marked line, andthe skin edges are undermined slightly (Figure 3). Thesubcutaneous fat is spread using blunt dissection. Ragnellretractors are placed in either side of the incision. The pal-mar fascia is carefully divided longitudinally, since keyanatomy may lie just dorsal to the palmar fascia. Once thedivided palmar fascia is retracted, the mid-palmar fat isexposed (Figure 3A).
Identification of Key Anatomy
The median nerve, superficial palmar arch, and distaledge of the transverse carpal ligament can now be identi-fied (Figure 4). If the distal edge of the transverse carpalligament is not clearly visible, the incision should beslightly extended in the proximal direction.
Care should be taken throughout the procedure to observefor and protect key anatomy, as well as any anatomicalvariations, such as the recurrent motor branch of themedian nerve.
Creating Extrabursal Path
As the assistant lifts up on the Ragnell retractors, theclamp is introduced on the ulnar side of the TCL, stayingagainst the dorsal surface of the TCL. Care should betaken to stay superficial to the flexor tendons, mediannerve, and ulnar bursa. Spread the clamp gently to createyour path (Figure 5).
Using the A.M. Surgical Hand Table, the forearm is elevatedand the wrist is dorsiflexed. The dissector is introduced intothe carpal canal and a pathway is created by advancing thedissector, aiming towards the “x” previously drawn, whilestaying against the undersurface of the TCL. Move the dis-sector back and forth to clear the synovial membrane fromthe underside of the TCL (Figure 6).
3
Fig. 3
Fig. 4
Fig. 5
3
4
5
UPPER EXTREMITY
Fig. 3A
Fig. 6

Introduction of Dissecting Cannula
Once the pathway is created and the dissector is removed,the dissecting Cannula/Obturator is then introduced intothe same pathway. The cannula tip should always stayagainst the under surface of the TCL and superficial to theflexor tendons and ulnar bursa. The cannula slot shouldface slightly towards the ulnar side (Figure 7).
When the cannula tip is palpable through the skin beneaththe "x", the obturator should be removed, leaving the can-nula in place with the slot facing slightly towards theulnar side.
Note: Throughout the procedure, whenever neces-sary, sterile absorbent swabs may be used to removefluid from within the cannula.
Endoscopic Visualization of Anatomy
A 4 mm, 30° endoscope, oriented towards the slot, is thenintroduced into the cannula to visualize the transversefibers of the TCL (Figure 8 and Figure 9). If most of thetransverse fibers are visible with a small amount oftenosynovium remaining, this tissue can be removed usingthe rasp. Do not use the rasp if the nerve or tendons are vis-ible. If the transverse fibers of the TCL are not clearly seen,the cannula must be removed using the obturator and theprocedure repeated, as outlined in “Introduction ofDissecting Cannula” step 6.
The median nerve is brought into view by rotating the can-nula towards the radial aspect of the hand (Figure 10). Theflexor tendons may also be visualized by rotating the can-nula towards the ulnar side of the hand (Figure 11). Oncethe proper placement of the cannula is verified, rotate thecannula slightly to the ulnar side so that the transversefibers of the TCL are again visualized (Figure 9).
4
Fig. 76
7
Safety • Vision • Quality
Fig. 8
Fig. 10 Fig. 11Fig. 9

5
UPPER EXTREMITY
8 Fig. 12
Fig. 13
Division of Transverse Carpal Ligament
With a clear view of the transverse fibers and no otherintervening structures the endoscope is then removed fromthe cannula. The scope mounting blade is attached to theendoscope using the locking device (see diagram on page 8),with the viewing angle of the endoscope oriented towardsthe blade (Figure 12).
The scope mounted blade is introduced into the cannulaand, as the surgeon observes the monitor, the TCL isdivided by advancing the scope mounted blade through thecannula in a proximal direction (Figure 13 and Figure 14).
To ascertain the proximal extent of the division, the scopemounted blade may be palpated through the skin in thedistal forearm. The scope mounted blade should be locatedproximal to the wrist flexion skin crease.
Warning: The disposable scope mounting blade isdesigned for one-time use only. Resterilization mayresult in blade detachment, potentially causing harmto the patient.
Fig. 14

Verification of Division
The scope mounted blade is removed from the endoscopeand the endoscope is reintroduced into the cannula. Thedivided edges of the TCL should now be visualized alongits entire length (Figure 15). The median nerve can onceagain be brought into view by rotating the cannulatowards the radial aspect of the hand. In addition, theflexor tendon(s) can be visualized by rotating the cannulatowards the ulnar aspect of the hand.
If preserved, the interthenar fascia will be visible above thedivided edges of the TCL.
Remove the endoscope from the cannula and introduce theobturator. Only when the obturator is inserted should youremove the assembly together.
Inspect the median nerve or the common digital nerve tothe third web space with a blunt hook.
Skin Closure/Postoperative Care
The wound is irrigated and then closed using a runningsubcuticular technique (Figure 16).
A soft non-compressive dressing is applied, which isremoved 7 to 10 days following the surgery (Figure 17).
The patient is encouraged to perform finger range-of-motion exercises postoperatively.
6
Fig. 16
Fig. 17
9
10
Safety • Vision • Quality
Fig. 15

InstrumentationA.M. Surgical Instrumentation is designed for both thesurgeon and patient benefit. The instruments are intuitivein design and simple in orientation, providing excellentperformance. The instruments are engineered to providefavorable patient outcomes that feature minimal scarringand rapid recovery.
7
UPPER EXTREMITY
Locking Device9600-04
Scope MountingBlade3310-B
Obturator9600-01
Elevator3300-06
Rasp9600-03
SlottedCannula9600-02
Single Case of Instruments9600-50
Hand Table9500
Table Pad9501-B

Use of Locking Device (use with 4 mm, 30° Scope)
Before attempting to insert scope mounting bladeinto locking device, be sure the lever is positionedtoward the straight side of the device, which is the"open" position (as shown).
1
8
Gently insert the flared end of the scope mountingblade into the angled side of locking device, aligningthe flat side of the scope mounting blade’s ring withthe bottom of locking device. A click will be heardwhen the scope mounting blade is properly engaged.
2
➡openpositionScope Mounting
Blade
lockedposition
Endoscope
lever in open position
Locking Device
straight side
Locking Deviceflared endring(side view)
insertScope Mounting Blade
Endoscope
Locking Device
Scope Mounting Blade insert3
1
2
Insert scope mounting blade onto the 4 mm, 30°endoscope. When the endoscope is almost touchingthe scope mounting blade, gently push the leverforward until finger tight. DO NOT OVERTIGHTENLEVER (TO AVOID DAMAGING ENDOSCOPE).
3
Safety • Vision • Quality

9
Use of A.M. Surgical Hand Table
Use forearm, finger, and thumb straps to secure thepatient's arm to the hand table.
Wrist position can be changed by loosening theorange lever in a counterclockwise direction. Once the desired angle is reached, tighten theorange lever in clockwise direction to lock the wristin that position.
Place patient's arm on hand table with the wristpositioned at the hinge of hand table.
Hand Table (top view)
thumbstrap forearm
strap
finger strap
UPPER EXTREMITY
3
2
4
5
Hand Table
Table Pad
hinge
wristHand Table
Apply pad to top of hand table.1
Forearm and hand elevation can be changed by loos-ening black lever in a counterclockwise direction.Once desired height is reached, tighten the black leverin clockwise direction to lock the arm in that position.
unlock
adjust arm height
lock
unlock lockadjust wrist angle

A.M. SURGICAL290 East Main StreetSuite 200Smithtown, NY 11787800-437-9653
www.amsurgical.com © 2004 500 9/04 8321 TG/PA
UPPER EXTREMITY
Locking Device9600-04
Scope MountingBlade3310-B
Obturator9600-01
Elevator3300-06
Rasp9600-03
Slotted Cannula9600-02