
DISSERTATION SUBMITTED TO UNIVERSITY OF … Sudhir Seth.pdf · DISSERTATION SUBMITTED TO UNIVERSITY...
34
MANAGEMENT OF SCOLIOSIS A STUDY DONE AT SAFDARJUNG HOSPITAL DELHI DISSERTATION SUBMITTED TO UNIVERSITY OF SEYCHELLES AMERICAN INSTITUTE OF MEDICINE IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE M.Ch (Orthopaedic Surgery) By DR. SUDHIR SETH Orthopaedic Surgeon November 2011
Transcript of DISSERTATION SUBMITTED TO UNIVERSITY OF … Sudhir Seth.pdf · DISSERTATION SUBMITTED TO UNIVERSITY...

MANAGEMENT OF SCOLIOSIS
A STUDY DONE AT SAFDARJUNG HOSPITAL DELHI
DISSERTATION SUBMITTED TO
UNIVERSITY OF SEYCHELLES
AMERICAN INSTITUTE OF MEDICINE
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE
M.Ch (Orthopaedic Surgery)
By
DR. SUDHIR SETH
Orthopaedic Surgeon
November 2011

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
MANAGEMENT OF SCOLIOSIS
BACKGROUND
Scoliosis is derived from a Greek word ‘SKOLIOS’ meaning curvature. Scoliosis remains as one of the important and difficult orthopedic problems and an unsolved mystery. Management of this unpredictable problem of teenage is very difficult and unpredictable. Management is divided broadly into CONSERVATIVE( observation-exercises-orthrosis) and SURGERY.
METHOD
Fifty consecutive patients of scoliosis were treated using conservative or surgical methods.
RESULTS
Fifty cases of scoliosis were treated over one year, of which 26 patients were on observation, exercises and braces while 24 patients were operated; of these 24 patients, 14 patients had posterior spinal fusion and 10 had Harrington Instrumentation with posterior spinal fusion.
Congenital scoliosis was the commonest cause accounting for 38%
Average age of seeking advice was 14.8 years.
Males were 54% while females were 46% of the series.
Average correction achieved was 23.2%
30.7% correction was achieved after instrumentation surgery, while it was meager 2.6% after simple fusion.
Rib hump resection achieved good cosmetic correction.
Allogenic bone graft mixed with autogenous graft gave good outcome.
CONCLUSION
Early surgery especially in advancing curvature gives good and lasting results.
KEYWORDS
Scoliosis, Congenital Scoliosis, Neuromuscular Scoliosis, Harrington Instrumentation, Posterior Spinal Fusion.
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
INTRODUCTION
Scoliosis is defined as a rotatory lateral curvature; tilt or angular deviation of the spine from its normal straight course.
SCOLIOSIS RESEARCH SOCIETY- CLASSIFICATION
1) Idiopathic 2) Congenital 3) Neuromuscular 4) Curve because of Neurofibromatosis 5) Mesenchymal- Marfan’s Syndrome 6) Trauma- fractures, radiation, surgery 7) Secondary to irritative phenomenon 8) Others like metabolic, nutritional, endocrinal
TREATMENT
1) Observation 2) Orthrosis 3) Operation
OBSERVATION
Observation with exercises in early stage of scoliosis is very important to improve posture and to strengthen the muscles.
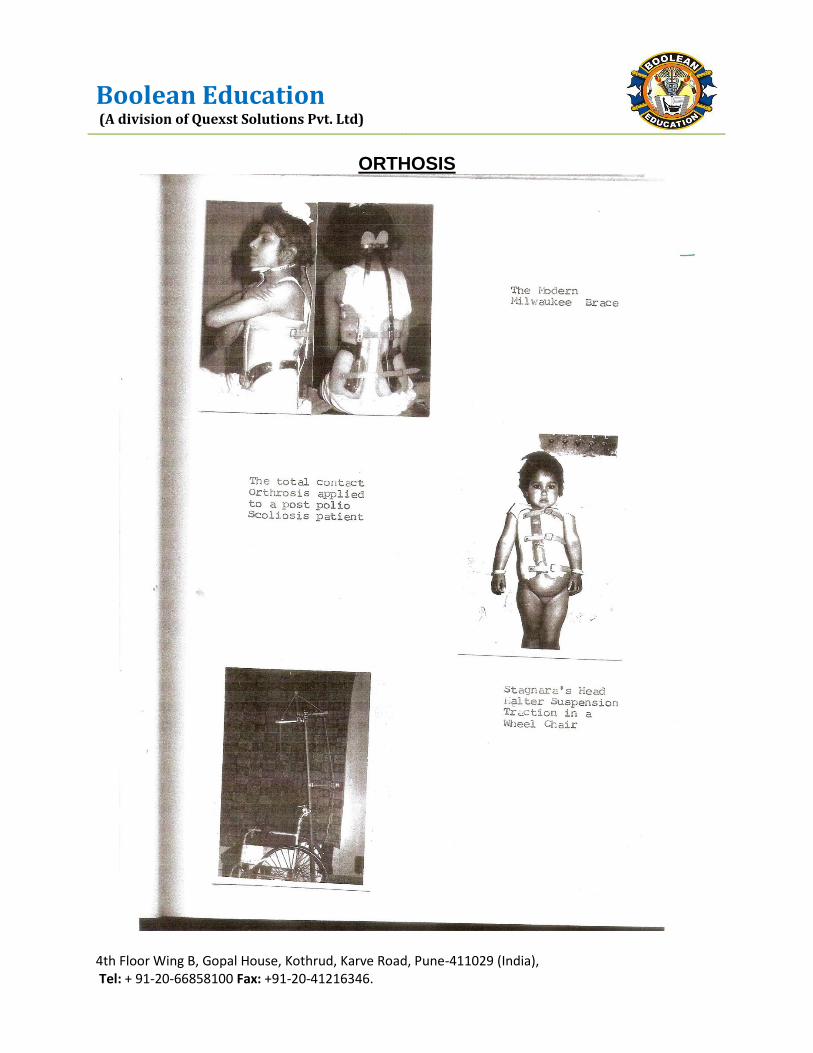
ORTHOSIS
Orthrosis or braces are very important to halt the progression of the disease and to allow healing and maturation of Arthrodesis after surgery.

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
PRE OPERATIVE TRACTION
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
ORTHOSIS

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
SURGERY
1) Posterior Spinal Fusion after achieving pre-operative correction by traction. 2) Posterior spinal fusion with Harrington Instrumentation. 3) Luques segmental spinal instrumentation and Galveston’s Technique for L Rod
Insertion(L.R.I.) 4) Rib resection. 5) Epyphyseodysis- Roaf’s Technique. 6) Anterior spinal surgery- Dwyer’s Instrumentation. 7) Dwyer’s Instrumentation and Zielke’s Instrumentation.
MATERIALS AND METHODS
Fifty cases of scoliosis were studied over 5 years at C.I.O. Safdarjung Hospital. All cases were worked up in the Out Patient Department with details of history, examination and investigations. Detailed physical examination of all patients was done.
Neurofibromatosis, Marfan’s Syndrome, Neuromuscular diseases and other congenital anomalies were ruled out. Detailed investigations like X-rays, CT Scans, blood tests, urine test, pulmonary function tests, electrophysiological test, muscle charting were done in selected patients. All patients were classified etiologically and severity wise.
Treatment of patients was divided into 3 groups-
1) Observation group- Observation was mean for curves measuring less than 20o
Those with no structural changes in the spine
And those predicted and resolving infantile curves by Mehta’s Method.
During observation the scrutiny was kept for curve progression and patients were advised postural exercises to check progression.
2) Orthosis Treatment- Was advised for curves measuring 30o to 50o.
For skeletaly immature patients
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
For curves of 20o showing an alarming progression during observation period
For curves of 20o showing structural change.
3) Surgery Group-
Surgery was taken up for cases:
for progressive curves and/or those above 50o.
when orthosis had failed to check the progression
patients who had completed skeletal maturity but leaving the orthrosis will again cause progression
congenital scoliosis caused by unfermented bar and unbalanced Hemi vertebrae showing galloping progression.
After a detailed pre-operative work-up and investigations, a mandatory course of pre-operative correction was done by
o Cotrel’s Static Traction o Cotrel’s Dynamic Traction o Halo femoral technique
Surgeries that were performed were
-Simple posterior fusion
-Harrington Instrumentation with posterior spinal fusion
-Rib resection for cases where rib hump exists. This is usually done before the above two surgeries.
Modified Hibb’s Technique of posterior spinal fusion with Moe’s Technique of facet joint fusion was done.
Harrington Instrumentation was done as a distraction rod to correct the curves. In three cases of Paralytic Scoliosis with Pelvic obliquity a sacral rod was used for curves going to the pelvis. Bone graft was both autogenous and allogenic.
POSTOPERATIVELY patients with Harrington Instrumentation were nursed in a posterior plaster shell. Patients who had no instrumentation were given a body cast after 15 days of surgery after stitch removal.
In young patients autogenic graft was insufficient, so deep freeze dried stored allogenic graft was used.

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
FOLLOW UP. On subsequent visits a 60 right and left oblique view XRAYS were done at 3 month follow up. A static MILWAUKEE BRACE was used till year after surgery. Weaning of brace was done if XRAY reveals a mature fusion. Patients with a curve below T6 were given a TAYLOR’S BRACE while those with curves above T6 were given a MILWAUKEE Brace after surgery.
SURGERY HAARINGTON INSTRUMENTS

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
REVERSED HARRINGTON ROD TECHNIQUE
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
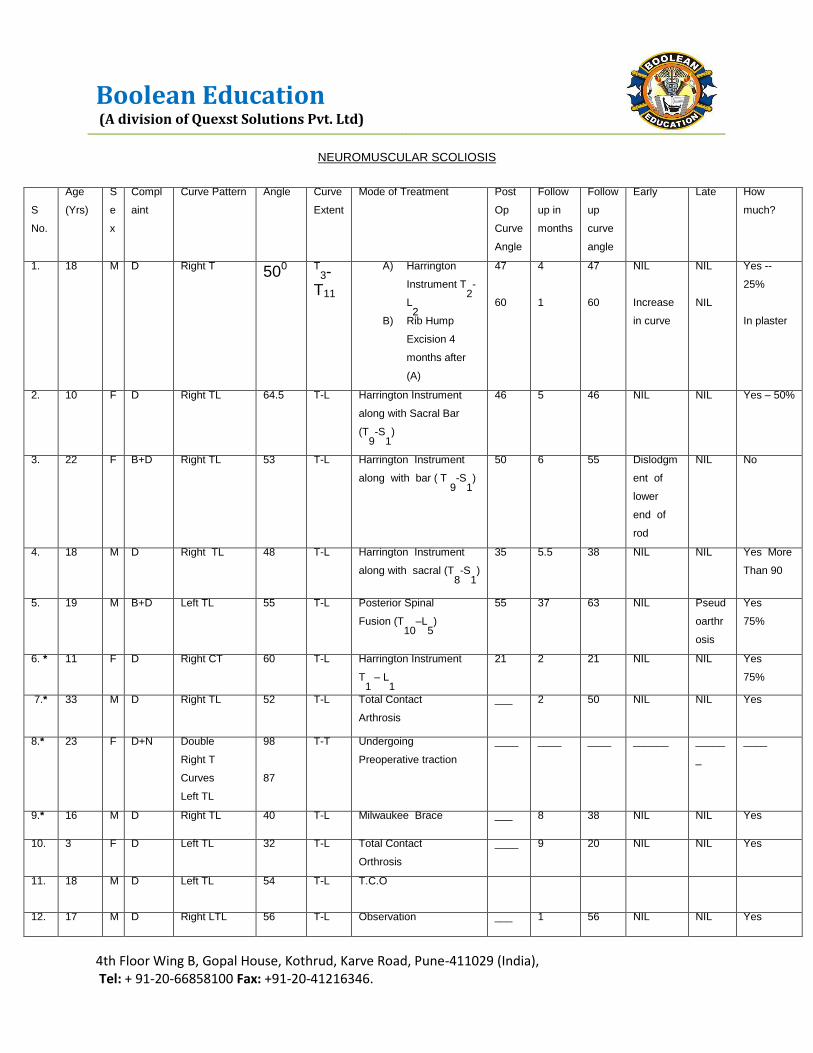
NEUROMUSCULAR SCOLIOSIS
S
No.
Age
(Yrs)
S
e
x
Compl
aint
Curve Pattern Angle Curve
Extent
Mode of Treatment Post
Op
Curve
Angle
Follow
up in
months
Follow
up
curve
angle
Early Late How
much?
1. 18 M D Right T 500 T3-
T11
A) Harrington
Instrument T2-
L2
B) Rib Hump
Excision 4
months after
(A)
47
60
4
1
47
60
NIL
Increase
in curve
NIL
NIL
Yes --
25%
In plaster
2. 10 F D Right TL 64.5 T-L Harrington Instrument
along with Sacral Bar
(T9-S
1)
46 5 46 NIL NIL Yes – 50%
3. 22 F B+D Right TL 53 T-L Harrington Instrument
along with bar ( T 9-S
1)
50 6 55 Dislodgm
ent of
lower
end of
rod
NIL No
4. 18 M D Right TL 48 T-L Harrington Instrument
along with sacral (T8-S
1)
35 5.5 38 NIL NIL Yes More
Than 90
5. 19 M B+D Left TL 55
T-L Posterior Spinal
Fusion (T10
–L5)
55 37 63 NIL Pseud
oarthr
osis
Yes
75%
6. * 11 F D Right CT 60 T-L Harrington Instrument
T1 – L
1
21
2 21 NIL NIL Yes
75%
7.* 33 M D Right TL 52 T-L Total Contact
Arthrosis
___ 2 50 NIL NIL Yes
8.* 23 F D+N Double
Right T
Curves
Left TL
98
87
T-T Undergoing
Preoperative traction
____ ____ ____ ______ _____
_
____
9.* 16 M D Right TL 40 T-L Milwaukee Brace ___ 8 38 NIL NIL Yes
10. 3 F D Left TL 32 T-L Total Contact
Orthrosis
____ 9 20 NIL NIL Yes
11. 18 M D Left TL 54 T-L T.C.O
12. 17 M D Right LTL 56 T-L Observation ___ 1 56 NIL NIL Yes

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
OUTCOMES
In this series, a total of 50 unselected patients of scoliosis of various etiologies have been studied. The various causes found in our series are tabulated as follows:-
AETIOLOGY
S.no
Aetiology No. of Patients Affected
Percentage of Total
I. Congenital 19 38%
II. Idiopathic 11 22%
III. Neuromuscular
A. Postpolio B. Others
12
8 4
24%
16% 8%
IV. Others
8
16%
Total
50
100%
The commonest single cause of scoliosis was congenital vertebral anomalies (amounting to 38%). Neuromuscular scoliosis and idiopathic scoliosis contribute 24% and 22% respectively to the series.
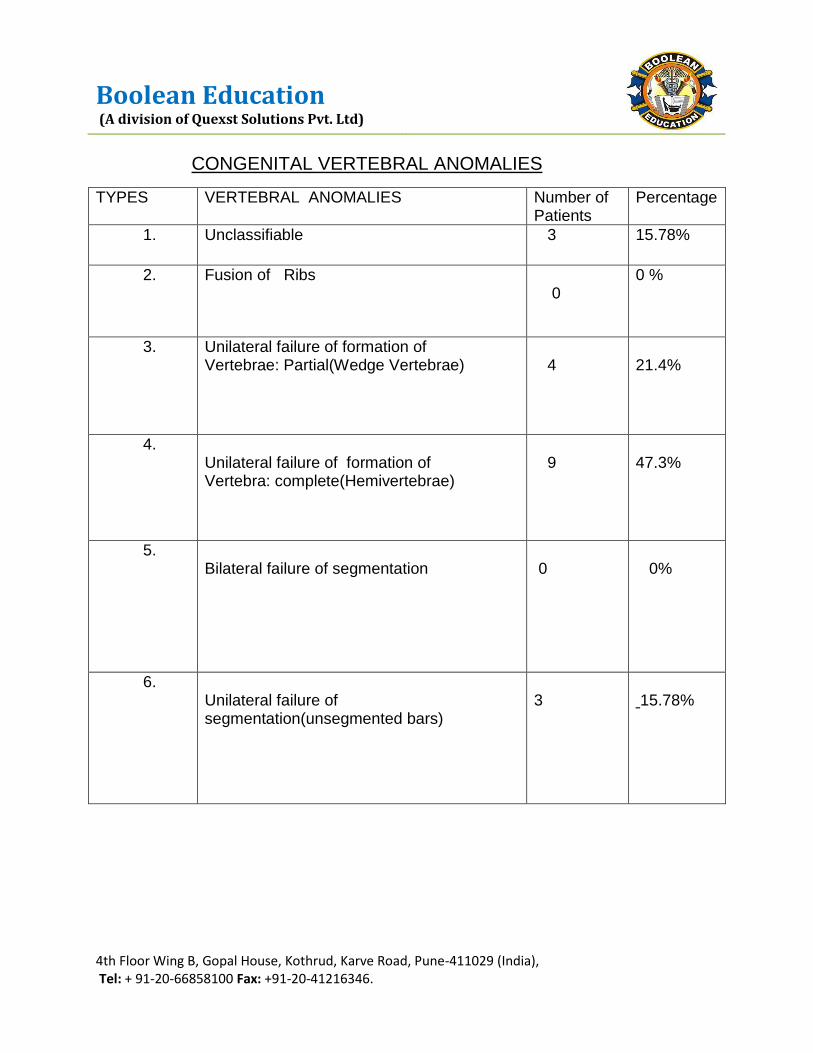
The commonest vertebral anomaly in our series was a result of the unilateral complete failure of formation of the vertebrae (in 47.3%)
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
CONGENITAL VERTEBRAL ANOMALIES
TYPES VERTEBRAL ANOMALIES Number of Patients
Percentage
1. Unclassifiable 3 15.78%
2. Fusion of Ribs 0
0 %
3. Unilateral failure of formation of Vertebrae: Partial(Wedge Vertebrae)
4
21.4%
4. Unilateral failure of formation of Vertebra: complete(Hemivertebrae)
9
47.3%
5. Bilateral failure of segmentation
0
0%
6. Unilateral failure of segmentation(unsegmented bars)
3
15.78%

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
TREATMENT
Number and Percentage of Patients in Groups
The total number of patients who received conservative treatment were 26, while rest of the twenty four were operated out of these 24, posterior
Spinal fusion was done in 14, Harrington instrumentation in 9 patients and Harrington instrumentation with posterior spinal fusion coupled with rib hump resection was done in one patients.
Mode of Treatment Congential Post Polio Neuromuscular Idiopathic Neuro
fibromatosis
Others
No. % No. % No. %
No. % No. % No. %
Conservative 9 47.4 3 37.5 3 75 7
57.5 1 33.3 4 80
Posterior Spinal fusion 10 56.6 1 12.5 - - - - 2 66.6 1 20
Posterior Spinal fusion
and Harrington
Instrument
- - 3 37.5 1 25 5 42.5 - - -
Excision of Rib Hump
with Instrumentation and
PSF
- - 1 12.5 -
- - - - - - -
Total 19 100 8 100 4
100 12 100 3 100 5 100

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
NEUROFIBROMATOSIS

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
SCOLIOSIS DUE TO NEUROFIBROMATOSIS
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
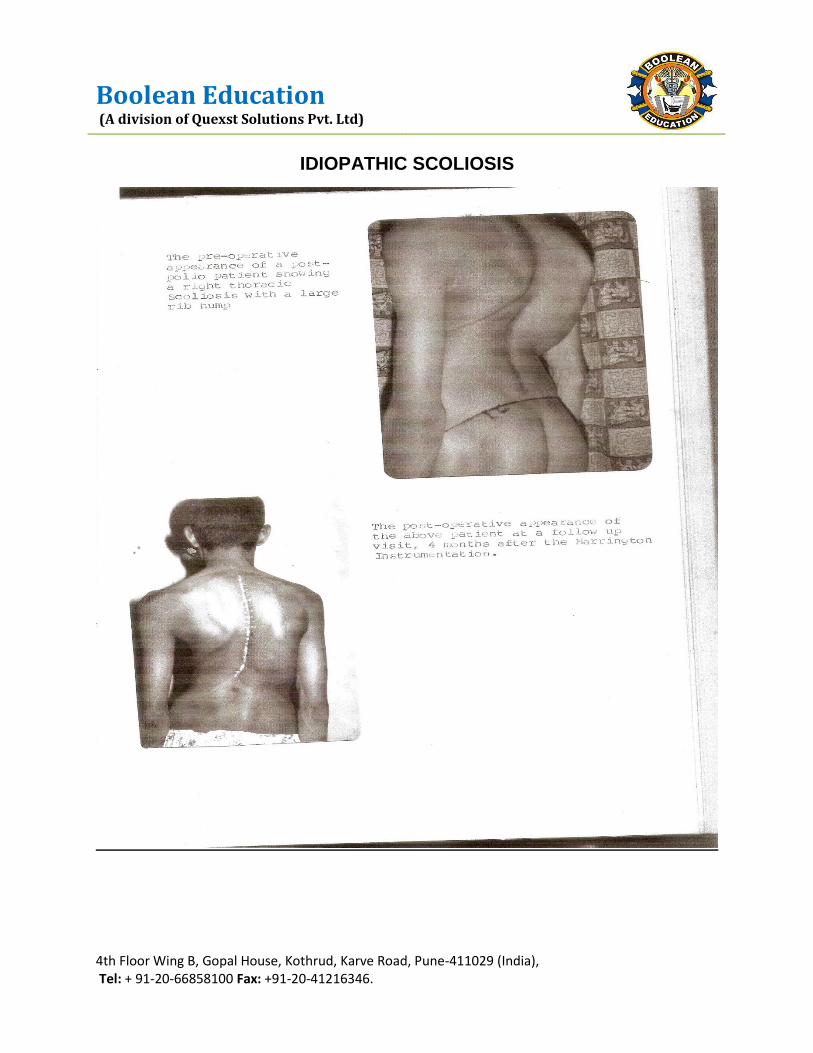
IDIOPATHIC SCOLIOSIS

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
IDIOPATHIC SCOLIOSIS

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
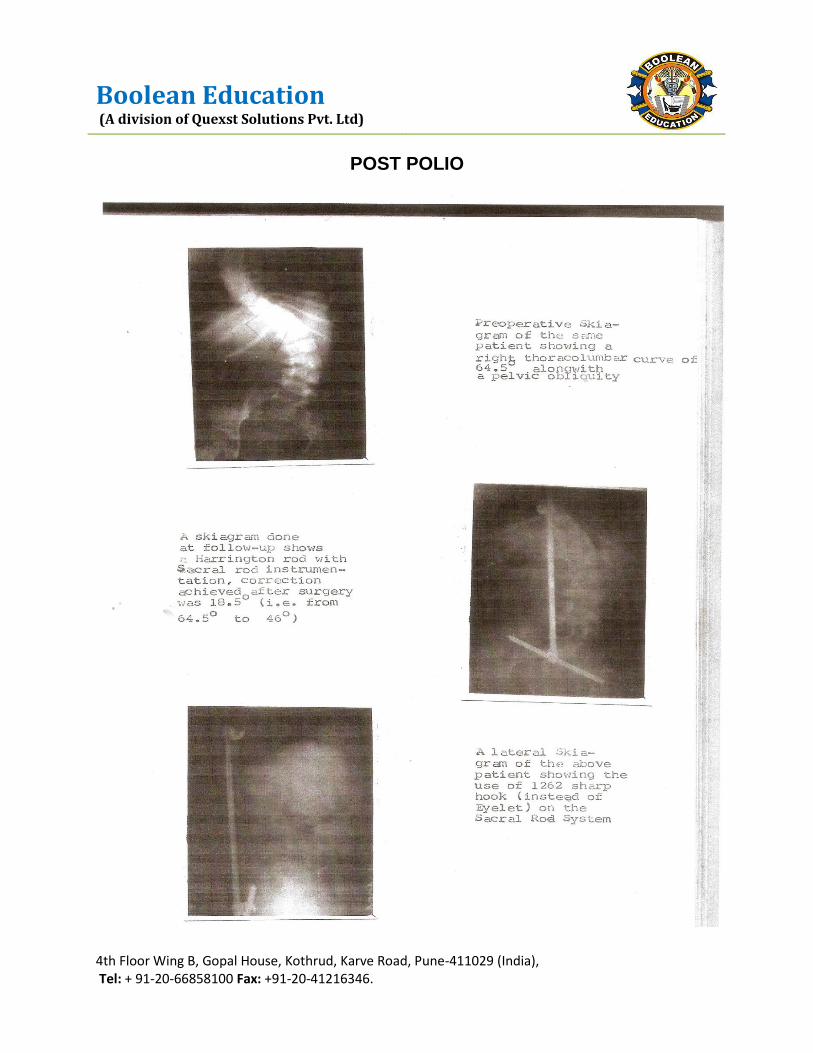
POST POLIO
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
POST POLIO

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
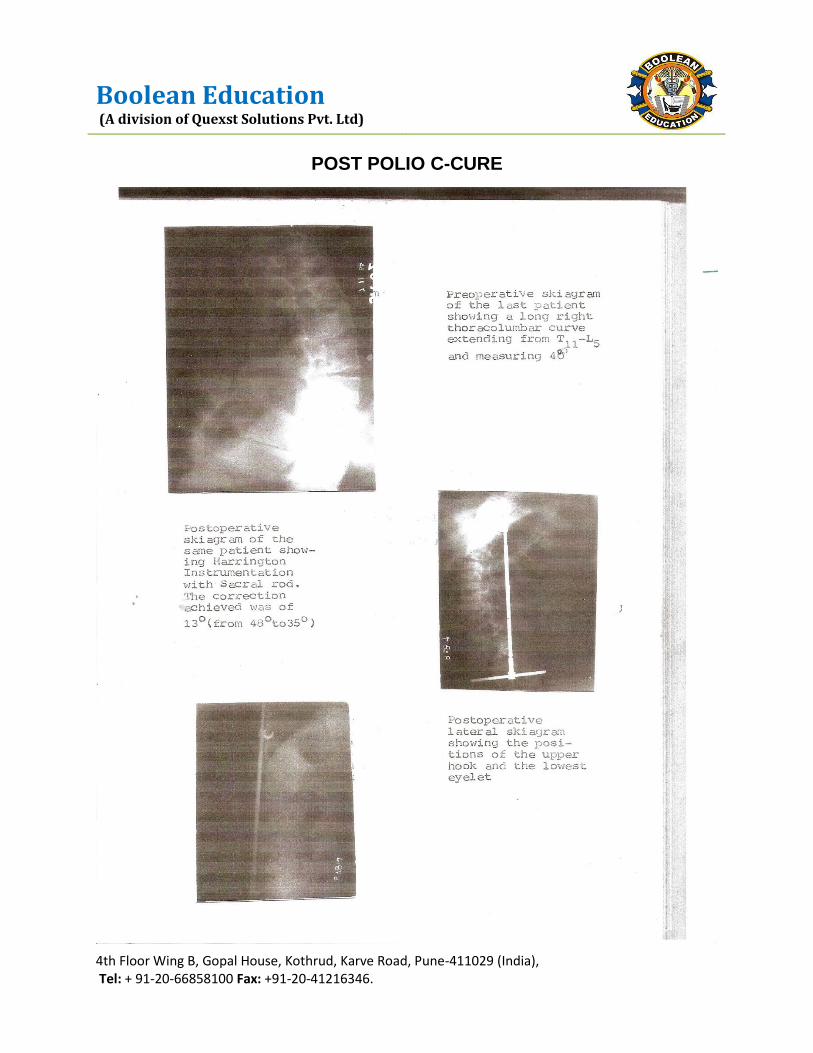
POST POLIO C-CURE
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
POST POLIO C-CURE
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
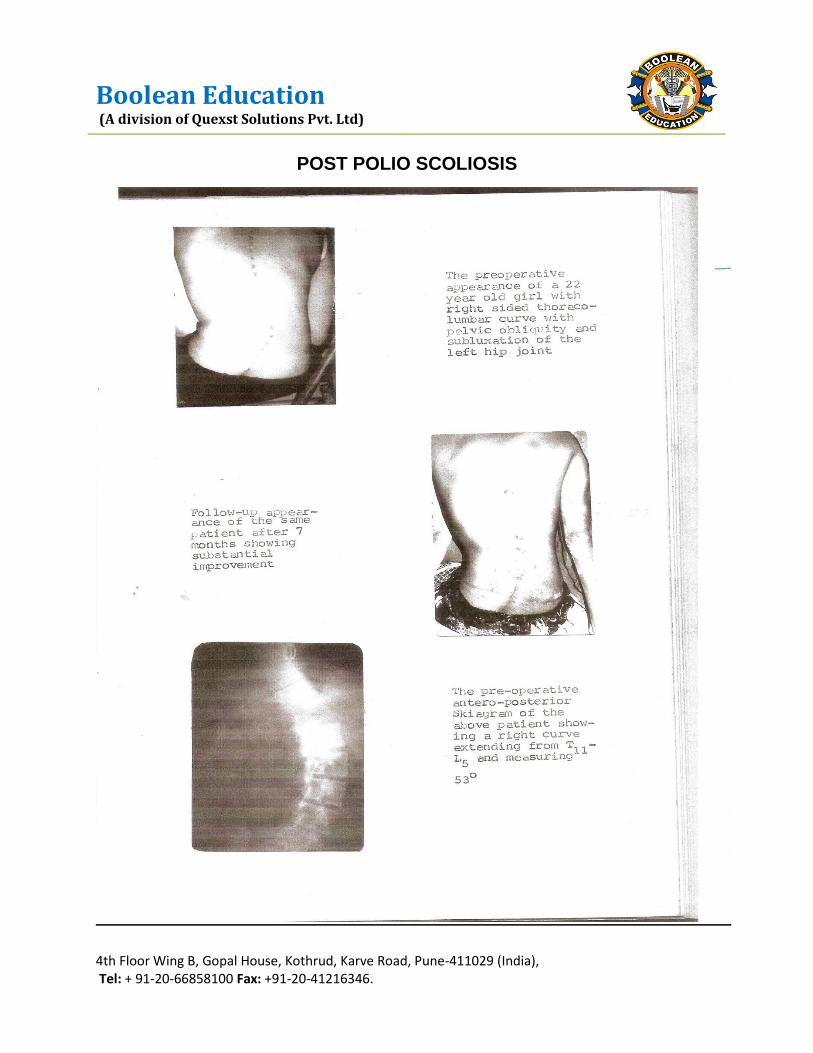
POST POLIO SCOLIOSIS
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
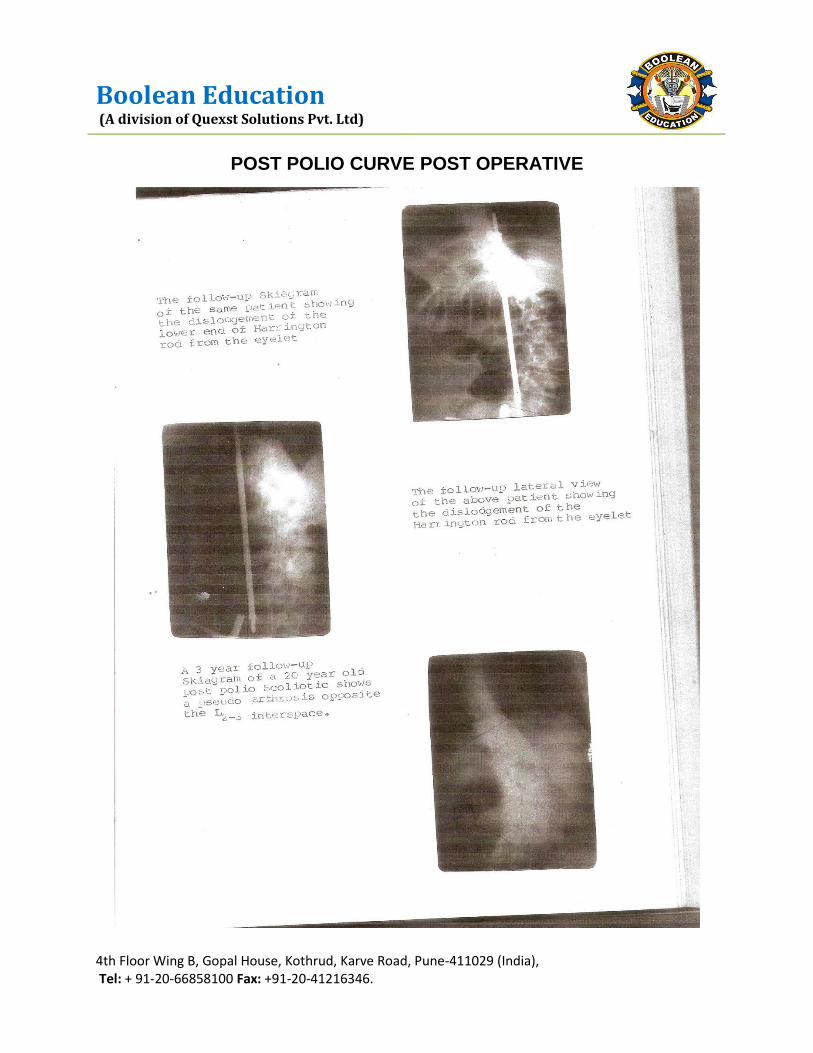
POST POLIO CURVE POST OPERATIVE
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
DISCUSSION
This series is based on 50 cases of Scoliosis that were studied at the Central Institution of Orthopaedics, Safdarjang Hospital, New Delhi, between April 84 to 85 of these 50 cases, 42 (i.e. 84%) were due to congenitial , idiopathic and neuromuscular Scoliosis . treatment for each of the patient was individualized . however, various types of treatment can be classified as under :
A. Conservative treatment including observation and postural exercises (26 cases)
B. Posterior spinal fusion (14 cases)
C. Harrington instrumentation augmented with Posterior spinal fusion (10
cases)
D. Later on rib hump resection was done in an Operated cases of paralytic scoliosis for Cosmetic reasons.
During the study maximum numbers of patients encountered were of congenital Scoliosis. These constituted 38% of the total cases, while idiopathic and neuromuscular scoliosis contributed 22% and 24% respectively to the series. These figures are markedly different from the western figures, which reveal that idiopathic scoliosis constitutes 75-80% of the Scoliosis patients in the west. This has been done to the virtual disappearance of poliomyelitis from the western hemisphere. Our results are similar to that obtained earlier by Dr. R.K.Gupta. During his work at C .I.O (1977) which revealed that 35.6% had congenital, 24.5% had paralytic and 28.9% had idiopathic Scoliosis .
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
CONGENITAL SCOLIOSIS
In this series, nineteen patients with congenital scoliosis were treated. Their age range was between 6 months to 18 years, the average being 10.4 years. In 13 out of the 19 patients, the age exceed 10 years of these 13 cases, 38.4% had curves. Between 20 to 40 while 61.6% had curves exceeding 40. In rest of 6 patients aged less than 10 years, 33.3% had curves between 20 – 40 while 66.6% had a curve exceeding 40. Our results resemble very closely to those of M.J.Mac Master et al (1984) who found that 64%of their patients of congenital Scoliosis about 10 years age had curves exceeding 40. Our series and M.J. Mc Master’s series reveal a poor prognosis for untreated cases of congenital scoliosis.

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
CONGENITAL SCOLIOSIS

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
CONGENITAL SCOLIOSIS

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
SUMMARY
A series of fifty cases of scoliosis was studied at the central institute of orthopedics, Safdarjang Hospital, between April 1984 to March,1985. For these, following three main types of treatments were adopted :-
A. Observations and postural exercises (in 26 patients ) B. Posterior spinal fusion (in 14 cases) C. Harrington instrumentation augmented with posterior spinal fusion ( in 10
patients)
Beside these, a thoracoplasty for rib hump was done in a case of paralytic Scoliosis for cosmetic reasons. A follow up Study was done in two cases of scoliosis; those cases were operated upon about three years ago.
On the basis of the study following conclusions could be drawn:
1) The congenital, idiopathic and neuromuscular scoliosis together constituted 84% of the total cases and among these three, the Scoliosis arising from congenital vertebral anomalies accounted for the maximum number (38%) of the cases.
2) The average age of patients at the time of seeking medical advice was 14.8 years.
3) Males (56%) were affected more than the females (44%)
4) The usual curve pattern seen among the patients was - thoracolumbar which was been in 25 out of the 53 curves affecting 50 patients.
5) The range of curves in the patients varied from 19o to 98o, the average curve being 47%.
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
6) The average overall correction achieved by surgery was 23%.
7) The average correction achieved by posterior spinal fusion with post-operative
plaster was 2.6% while that achieved by Harrington Instrumentation was 30.7%.
8) Sacral bar was found to give satisfactory correction of the Paralytic pelvic
obliquity in two out of the three cases operated upon by this technique.
9) Major complications were found in four cases out of the twenty four cases, of
which two had instrument failure and two had peseudoarthrosis.
10) Application of inverted Harrington instrument for high cervicothoracic curves gave
excellent results.
11) Rib hump resection (thoracoplasty) done in a case of severe paralytic scoliosis
gave good cosmetic results.
12) The use of allogenic bone graft for posterior spinal fusion gave good results in
90% of all the cases so operated.
13) Follow up study done on two cases operated about three years ago revealed
solid fusion in one case and asymptomatic pseudarthrosis in other case.

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
CONCLUSIONS AND RECOMMENDATIONS
Early detection of scoliosis and early treatment is the cornerstone of success.
Observation and corrective exercises are important in resolving curves and
curves detected at less than 20o.
Early surgical invention in progressive curves with structural changes
and exceeding 50 degree.
Harrigton Instrumentation if combined with fusion gives more gratifying
results than fusion alone.
Allogeneic bone graft combined with autogenous graft can help where
autogenous graft insufficient.
Sacral rods were used in long C shaped thoracolumbar curves involving
the pelvis causing pelvic obliquity.
Rib hump resection should precede the correction of spine curvature.

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
REFERNECES
Alam W. Wolf (1981): Transverse traction in the treatment of Scoliosis – A
preliminary report spine vol.6.2:134
Albert C. Schmidt (1971): The Halo Tibial Traction combined with Milwaukee Brace, Clinical Orthopedics & Related Research No.77:73
Andy Sullivan J &Strephen B.Conner (1982): Comperison of Harrington and Segmentation Spinal Instrumentation in management of neuromuscular spinal deformities, Spine Vol. 7 No. 3:299
Armstrong,GWD &HG.Connect(1975): A Transverse Loading System applied to a
modified Harrington Instrumentation, Clinical Orthopaedics & Related Research 108:70.
Ben L.Allen and Ron L.Fergusson (1984): Galveston technique of Pelvic fixation of the L- Rod Instrumentation of the Spine, Spine Vol.9, No. 4:388
Bonnet C. Brown, JC Perry, J.Nickel etal (1975): Evaluation of treatment of Paralytic Scoliosis at Rancho Los Amigos Hospital J. Bone & Joint Surg. 57- A:206.
Brooks, B and Lehman E.P. (1924): The bone changes in Recklinghausen’s Neurofibromatosis, Surg. Gynecal, obset, 38:587
Busch, L.F. (1947): The use of homogenous bone grafts J. Bone & Joint Surg. 29- A:206
Colonna P.C. and Vom Saal F. (1941): A study of paralytic scoliosis based on 500
cases of poliomyelitis. J. Bone & Joint Surg. 23-335

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
Daniel R. Benson, Ronald, LD and Albert B.S. (1977) : Harrington Rod distraction. Instrumentation- Its effect on vertebral rotation and Thoracic compensation. Clinical Orthopaedics & Related Research No. 125:40
Dwyer, A.F. and Schaffer, M.F. (1974): Anterior approach to scoliosis. Results of
treatment in 51 cases J. Bone & Joint Surgery 56- B:218
Gaines R.W., Leatherman,K.D. (1982): Benefits of Harrington compression system in Lumbar and thoracolumbar Idiopathic Scoliosis in Adolescents and Adults, Spine Vol.6 No.5: 483
Garrett, AL, Perry, J and Nickel, V.C. (1961): Stabilization of the collapsing Spines, J.Bone & Joint Surg., 43A:474
Hamel,A andMoe, J.H.(1964): The collapsing spine, Surgery,56:364
Harrington, PR(1962) : Treatment of Scoliosis: Correction and internal fixation by spine instrumentation J.Bone Joint surg.44A:5 91-610
Hilal, SK, Marton, D and Pollack E(1974): Diastematomyelia in children, Radiology 112:609
Howard H.Steel(1983): Rib resection and spine fusion in correction of the convex deformity in Scoliosis. J.Bone & Joint Sur.65-A920
James, J.I.P,(1954): Idiopathic scoliosis, the prognosis, diadfnosis and operative indications related to curve patterns and the age of onset.
James, J.I.P. (1957): Paralytic scoliosis , and . R. Coll. Surgery: 21: 21-42.
Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
Kuhn , J.G and Hormel , RS (1952): Management of congenital Scoliosis Arch- surg : Chicago, 65: 250
Levine , D.B . (1974) : Poliomyelitis, hardy , J. H. (Ed) : Spinal Deformities in Neurological and Muscular Disorders , St. Louis , C.V. Mosby ,
Lyones, R .D . (1972): Scoliosis after Thoraceplasty , J. Bone & joint Surg .54-B : 484 .
Mehta M.H.(1972): The rib – vertebra angle in the early diagnosis between resolving and progressive infantile Scoliosis J. Bone & joint Surg. 54 –B : 230
Michael J . M.C. Master & Kuntyoshi Ohtsuka (1982): The natural history of congenital scoliosis – A study of 251 patients . J.Bone & Joint Surg . 64- A:1128
Moe, J. H . & Kettleson , D. N. ( 1970): Idiopathic Scoliosis – Analysis of curve Patterns and preliminary results of Milwaukee Brace treatment in 169 patients J.Bone Joint Surg . 52 –A : 1509
Nasea, R.J, stelling , F.H. and steel, H.H (1975): Progression of congential Scoliosis due to hemivertebrae and hemivertebrae with bars J.Bone Joint Surg . 57 –A:457.
Phillip , J. M. and John Dove (1981): Post poliomyelitis paralytic Scoliosis Spine,Vol.6,No.5:573
Ponte, A (1974): A brace for the non-operative treatment of Lumbar and thoraco-lumbar curves- Presented at the Annual Meeting of the Scoliosis Research Society, San Francisco, September.
Rob ert, L.W., David, B.L and John, H.D (1971): Surgical treatment of idiopathic Scoliosis, Clinical Orthopeadics & Related Research No. 81:34.

Boolean Education (A division of Quexst Solutions Pvt. Ltd)
4th Floor Wing B, Gopal House, Kothrud, Karve Road, Pune-411029 (India), Tel: + 91-20-66858100 Fax: +91-20-41216346.
Sally Rudicel and Thomas S. Renshaw (1983): The effect of the Milwaukee Brace on Spinal Decompensation in Idiopathic Scoliosis Spine Vol. 8, No. 4:385
Stig. Aaro and Gunnar O Hlein (1983): The effect of Harrington Instrumentation on the Saggital Configuration and mobility of the spine in Scoliosis Spine Vol.8, No. 6:570
Stig. Aaro, Rogir Burstom and Mats Dallborn (1981): The derotation effect of the Boston Brace- A comparison between a Conventional Method and CAT Spine Vol.6 No. 5:477
Wedge, J.H. and Gillespie, R: The problems of Scoliosis surgery in paralytic children J.Bone Joint Surg . 57 – B:536.
William Bunnell, Dean Mac Ewen (1980): The use of plastic jackets in the Non-Operative treatment of Idiopathic Scoliosis J.Bone Joint Surg . 62- A:1.
Winter R.B.,Haven, J.J. Moe, J.H and Lagaards. M.(1974): Diastematomyelia and Congenital Spine deformities, J.Bone and Joint Surg 56- A:27
Winter R.B, Moe, J.H. Bradford, DS, Lonstein J.E Pedras, C.V and Weber A.H. (1979): Spine deformity in neurofibromatosis. A review of one hundred and two patients J.Bone and Joint Surg 61-A:677
Winter, R.B (1979): Posterior spinal fusion on Scoliosis indications, technique and results. From Symposium on Scoliosis and related Spinal disorders. Orthopaed. Clinics of North America 1979


















