Dissecting the tumor-immune landscape in chimeric antigen ... · machine learning methods, such as...
30
1 Dissecting the tumor-immune landscape in chimeric antigen receptor T-cell therapy: key challenges and opportunities for a systems immunology approach Gregory M. Chen 1,4,5 , Andrew Azzam 4 , Yang-Yang Ding 1 , David M. Barrett 1 , Stephan A. Grupp 1,2,6 , Kai Tan 1,3-8,* 1 Division of Oncology, Center for Childhood Cancer Research, Children’s Hospital of Philadelphia 2 Division of Oncology, Cancer Immunotherapy Program, Children's Hospital of Philadelphia 3 Department of Biomedical and Health Informatics, Children’s Hospital of Philadelphia 4 Perelman School of Medicine, University of Pennsylvania 5 Graduate Group in Genomics and Computational Biology, University of Pennsylvania 6 Department of Pediatrics, Perelman School of Medicine, University of Pennsylvania 7 Department of Cell and Developmental Biology, Perelman School of Medicine, University of Pennsylvania 8 Department of Genetics, Perelman School of Medicine, University of Pennsylvania * Corresponding author Running title: Systems Biology of CAR T-cell Therapy Contact information for the corresponding author: Kai Tan The Children’s Hospital of Philadelphia 4002 Colket Translational Research Building (CTRB) 3501 Civic Center Boulevard Philadelphia, PA 19104 USA Phone: 267-425-0050 Email: [email protected] Disclosure of potential conflicts of interest The authors declare no competing interests. Research. on July 16, 2020. © 2020 American Association for Cancer clincancerres.aacrjournals.org Downloaded from Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888
Transcript of Dissecting the tumor-immune landscape in chimeric antigen ... · machine learning methods, such as...

1
Dissecting the tumor-immune landscape in chimeric antigen receptor T-cell therapy: key
challenges and opportunities for a systems immunology approach
Gregory M. Chen1,4,5
, Andrew Azzam4, Yang-Yang Ding
1, David M. Barrett
1, Stephan A.
Grupp1,2,6
, Kai Tan1,3-8,*
1Division of Oncology, Center for Childhood Cancer Research, Children’s Hospital of
Philadelphia 2Division of Oncology, Cancer Immunotherapy Program, Children's Hospital of Philadelphia
3Department of Biomedical and Health Informatics, Children’s Hospital of Philadelphia
4Perelman School of Medicine, University of Pennsylvania
5Graduate Group in Genomics and Computational Biology, University of Pennsylvania
6Department of Pediatrics, Perelman School of Medicine, University of Pennsylvania
7Department of Cell and Developmental Biology, Perelman School of Medicine, University of
Pennsylvania 8Department of Genetics, Perelman School of Medicine, University of Pennsylvania
* Corresponding author
Running title: Systems Biology of CAR T-cell Therapy
Contact information for the corresponding author:
Kai Tan
The Children’s Hospital of Philadelphia
4002 Colket Translational Research Building (CTRB)
3501 Civic Center Boulevard
Philadelphia, PA 19104
USA
Phone: 267-425-0050
Email: [email protected]
Disclosure of potential conflicts of interest
The authors declare no competing interests.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

2
Abstract
The adoptive transfer of genetically engineered Chimeric Antigen Receptor (CAR) T-cells has
opened a new frontier in cancer therapy. Unlike the paradigm of targeted therapies, the efficacy
of CAR T-cell therapy depends not only on the choice of target, but also on a complex interplay
of tumor, immune, and stromal cell communication. This presents both challenges and
opportunities from a discovery standpoint. Whereas cancer consortia have traditionally focused
on the genomic, transcriptomic, epigenomic, and proteomic landscape of cancer cells, there is an
increasing need to expand studies to analyze the interactions between tumor, immune, and
stromal cell populations in their relevant anatomical and functional compartments. Here, we
focus on the promising application of systems biology to address key challenges in CAR T-cell
therapy, from understanding the mechanisms of therapeutic resistance in hematologic and solid
tumors to addressing important clinical challenges in biomarker discovery and therapeutic
toxicity. We propose a systems biology view of key clinical objectives in CAR T-cell therapy,
and suggest a path forward for a biomedical discovery process that leverages modern
technological approaches in systems biology.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

3
Introduction
CAR T-cell therapy has seen exceptional success in several hematologic malignancies (1–5),
marked by the first round of FDA approvals and Phase II trials (4,6). Yet these studies have also
highlighted key clinical challenges including therapeutic resistance in a subset of patients,
challenges in translation to solid tumors, and therapeutic toxicity (7–9). As clinical knowledge
increases, there is a promising opportunity to apply modern molecular technologies under a
systems immunology approach to accelerate progress. Furthermore, the limited availability of
clinical samples from early clinical trials is a major motivating factor for using advanced
technologies to gain the most knowledge from the samples that exist. Broadly speaking, systems
immunology encompasses the tools of systems biology framework to the unique biological
characteristics of innate and adaptive immunity (10,11). The modern roots of systems biology
date to the turn of the 21st century, as genome sequencing technologies began to rapidly
accelerate (12,13). Under a systems biology paradigm, biological entities are modeled as a
network of interacting units, typically requiring high-throughput data generation paired with
integrative computational and statistical models. Each foundational unit may be defined as an
intracellular entity such as a gene or metabolite, or a cellular entity such as an individual cell or
cell type (10). Technological advances have made possible many approaches that were
previously untenable except under theoretical circumstances. Massively parallel molecular
assays can quantify not only the levels of various molecular analytes such as RNA, protein, and
metabolites, but also interrogate their interactions at increasingly higher throughput. These
molecular assays can also be applied to measure the cellular states and interactions after either
genetic or chemical perturbations in a high-throughput fashion (14–16). The advent of single-cell
technologies in particular has led to an influx of data, and ongoing consortia such as the Human
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

4
Cell Atlas (17), the Human BioMolecular Atlas Program (18), and the Human Tumor Atlas
Network will provide key resources to characterize the underlying basis of normal and malignant
cellular phenotypes and tumor microenvironment. The immune system has been an important
focus in multiple consortia, leading to opportunities to integrate knowledge into the field of CAR
T-cell therapy and other immunotherapies.
In parallel to experimental technology development, a vast array of computational and statistical
approaches have been developed to advance systems biology. Mathematical models of tumor-
immune interactions have been developed using principles of optimal control theory, treating
cellular populations as interacting units within a dynamic system (19,20). Another key class of
systems biology algorithms model biological processes as molecular interaction networks, and
both computational and technological advancements have allowed for construction and analysis
of these networks at a tissue- or cell type- specific resolution (21,22). The relatively high sample
sizes produced by single-cell experiments have been increasingly capable of powering for
machine learning methods, such as probabilistic graphical models and deep learning, to interpret
the data and identify regulatory mechanisms (23–25). A major ongoing challenge in the field is
the integration of data across experimental protocols and molecular assays, and approaches such
as factor analysis and transfer learning have been developed to address this challenge (26,27).
The mechanisms of CAR T-cell treatment success and failure are likely multimodal and involve
tumor, T-cell, and microenvironmental factors (9). From a systems biology perspective, tumor-
immune interactions can be viewed as a complex adaptive system that underlies the major
clinical challenges, from treatment failures to therapeutic toxicities (Figure 1). In hematological
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

5
malignancies such as B-cell acute lymphoblastic leukemia (B-ALL), cancer cells may be present
in large numbers in peripheral circulation as well as the bone marrow, allowing T-cells to have
relatively free access to the tumor throughout the body and in the marrow microenvironment. In
contrast, CAR T-cell therapy for solid tumors faces multiple additional barriers including T-cell
exclusion, vascular and hypoxic constraints, and immune suppression mediated by additional cell
types such as cancer associated fibroblasts, tumor-associated macrophages, and myeloid-derived
suppressor cells (28,29). Understanding these factors will be a crucial component of improving
existing CAR T-cell therapies and developing new therapies for hematological and solid tumors.
As the number of clinical and preclinical trials of CAR T-cell therapies expand, a systems
biology approach will become a powerful complement to advance biological discovery (Table
1). Paramount to a systems biology approach is an understanding of the strengths and limitations
of each technology, including sources of technical variability and the fundamental role of each
molecular analyte in a biological system.
Biomarker discovery: leveraging prior immunological knowledge
The identification of prognostic biomarkers of response to CAR T-cell therapy is of great clinical
interest due to the potential to aid in risk stratification and identification of patients most likely to
benefit from therapy. There is an urgent need to define T-cell characteristics in the CAR T-cell
product that predict key attributes such as proliferation and persistence of CAR T-cells after
infusion. A number of cellular and molecular biomarkers have been identified in immune
checkpoint blockade: circulating factors such as lactate dehydrogenase (LDH) (30,31);
immunological markers such as immune cell composition, T-cell activation pathways,
lymphocytic infiltration, and T-cell repertoire (32–35); and tumor markers such as PD-L1
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

6
signaling (36) and mutational load (36–38). Some, but not all, of these biomarkers have the
potential to generalize to CAR T-cell therapy. Transcriptomic phenotypes of lymphocytic
activation and migration may be shared between immunotherapy modalities. On the other hand,
biomarkers that assess the diversity in antigen recognition, such as T-cell repertoire and
mutational load, may be of lesser significance in CAR T-cell therapy compared to
immunotherapies that depend primarily on cytotoxicity through endogenous T-cell receptor
signaling. The utility of these biomarkers in combined checkpoint blockade and CAR T-cell
therapy, or in future CAR T-cell therapies that may require general T-cell activation and epitope
spreading for efficacy, has yet to be assessed in clinical trials.
Circulating factors may play a general role in suppression or activation of adaptive immune
responses. Lactic acid has been shown to blunt antitumor responses by T-cell and NK-cells (39),
and serum lactate dehydrogenase (LDH) has been shown to correlate with clinical outcomes in
immune checkpoint blockade. In CAR T-cell therapy, post-infusion serum cytokine markers
have been shown to be predictive of cytokine release syndrome (CRS) (40), the most significant
characteristic adverse effect of the therapy; but biomarkers predicting or modulating efficacy in
either the product or the patient have not been clearly identified. Transcriptional pathways in T-
cell populations, such as T-cell exhaustion, have been associated with resistance to both immune
checkpoint blockade and CAR T-cell therapy (41,42). Insights related to tumor evasion of
adaptive immunity may be shared between CAR T-cell therapy and other therapeutic modalities.
Among the best-known example is expression of the programmed death-ligand 1 (PD-L1) on
tumor cells, which interacts with PD-1 on T-cells to suppress T-cell activity. In an in vivo mouse
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

7
model of pleural mesothelioma, tumor-cell PD-L1 expression inhibited CAR T-cell effector
functions (43).
The transfer of knowledge from prior studies of immunology and cancer immunotherapy to CAR
T-cell therapy will be key to the systems biology approach. The Immunological Genome Project
(44) and more recently, the Human Cell Atlas (17), the Human Tumor Atlas Network, and the
Immuno-Oncology Translational Network will provide a wealth of reference data on the
molecular physiology of multiple immune populations in normal and malignant environments. In
clinical and pre-clinical studies of cancer immunotherapy, particularly in immune checkpoint
blockade, there has been an expansion in the use of high-throughput technologies to generate
large datasets and computational models of tumor and immune populations. For example, Jiang
et al. used publicly available bulk RNA-Seq profiles to derive a predictive signature of T-cell
exclusion and dysfunction in anti-PD1 and anti-CTLA4 therapy (45); and Krieg et al. used
single-cell mass cytometry to assess cell surface protein phenotypes of peripheral blood
mononuclear cells at multiple therapeutic time points (46).
The computational framework for biomarker discovery for CAR T-cell therapy from prior
immunological data can be formulated under the principles of transfer learning, which involves
the exchange of knowledge from a source domain and task to a target domain and task (47).
Under this framework, the source domain consists of data generated from a previous
immunological study, and target domain consists of data generated from one or more CAR T-cell
studies (Figure 2). Knowledge transfer can occur in the form of model parameters, feature
representations, or instances in an integrative model. In the case of immunological data, the most
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

8
direct methods of knowledge transfer can involve gene signatures, pathway signatures, gene
network topology and edge weights, or model coefficients to be used as a statistical prior.
Transfer learning has been successfully used for prediction of MHC class I protein binding,
clinical and histopathological image analysis, integration of molecular data from genomic and
RNAi screens, and integration of single-cell RNA-Seq data (48–52). Immune cell populations
are among the most common cells to be studied by high-throughput technologies, and the wealth
of publicly available immunological data is an opportunity for the development and deployment
of integrative computational methods to be used in studies of CAR T-cell therapy.
Pre-treatment effects and the search for combination therapy
Patients on clinical trials of CAR T-cell therapy to date have received CAR T-cell therapy
subsequent to other treatments, often including multiple rounds of cytotoxic chemotherapy.
These prior treatment effects may have a profound impact on the immune cells, tumor cells, and
tumor microenvironment involved in CAR T-cell therapy. In studies of other immunotherapies,
chemotherapeutic agents have been shown to increase immunogenicity of tumor cells through
increased antigenicity and depletion of suppressive immune cell populations (53,54) and increase
tumor infiltration by T-cells in solid tumors (55). Combination therapy between certain
chemotherapeutic agents and immune checkpoint blockade is the standard of care in some
cancers (56). It is unclear to what extent these factors apply to CAR T-cell therapy.
Lymphodepleting chemotherapy is routinely given to patients prior to CAR T-cell infusion, and
has been associated with improved in vivo expansion and persistence (57), owing to cytokine
upregulation as well as suppression of regulatory T-cells and myeloid-derived suppressor cells
that has been observed in earlier adoptive cell transfer therapies (58). Clinical and preclinical
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

9
studies comparing the impact of prior therapy on CAR T-cells themselves are scarce, and such
studies are limited by the heterogeneity of prior treatment regimens among patients enrolled in
clinical trials. It is possible that certain chemotherapies could have a deleterious impact on CAR
T-cell therapy due to their impact on T-cells and activation of pathways hindering expansion in
vitro or post-infusion (59).
With over a hundred approved anticancer drugs and over a thousand in development (60), the
identification of agents that sensitize cancer cells or augment immunological function in CAR T-
cell therapy is a promising objective. Some drug combinations, such as combining immune
checkpoint blockade and CAR T-cell therapy, have initial clinical evidence of benefit (61). A
highly active area of systems biology has been the development of technologies and
computational methods to identify synergistic and antagonistic drug combinations in cancer
therapy. High-throughput drug sensitivity screens on cell lines, paired with genomic and
transcriptomic data, have provided a resource for modelling individual drug perturbations in
cancer cells (62,63), and CRISPR screens of gene pairs provide a functional assay to assess for
genetic interactions among known drug targets in cancer cells (64). A number of computational
methods have been developed to model the gene regulatory networks of cancer cells, with the
objective of identifying synergistic drug combinations or pairs of potentially targetable genes
that exhibit synthetic lethality or synthetic dose lethality (65–68). These approaches, however,
are challenging to generalize to immunotherapy. Immunotherapy fundamentally differs from
conventional pharmacotherapy, in that the mechanism of tumor cell killing is dependent on
complex interactions between immune cells and tumor cells, which are not adequately modeled
in assays of cancer cell lines. One approach has been to identify differentially expressed genes
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

10
and gene modules between immunotherapy responders and non-responders, and consider
regulators of these pathways as candidate targets. For example, Lesterhuis et al. performed
network analysis of immunotherapy responsive and resistant tumor transcriptomes to identify
candidate target genes to augment checkpoint blockade (69), and Jerby-Arnon et al. performed
single-cell RNA-Seq on 33 melanoma tumors to identify an immune evasion cellular program
that suggested CDK4/6 inhibition in combination with immune checkpoint blockade (70).
Intratumor targets, however, only represent a subset of drug targets among the potentially
targetable cellular populations. For example, stimulation of innate immunity, modification of the
tumor immunosuppressive environment, and modulation of T-cell function represent classes of
potential drug targets directed toward non-tumoral cells (71). To address these broader
opportunities of combination therapies, computational models must consider immune cell
populations and tumor-immune interactions.
Use of single-cell technology to better understand the T-cell contribution to CAR T-cell
therapy
The underlying T-cell populations used for generation of CAR T-cell products likely play a
substantial role in determining the ability of the CAR T-cells to proliferate and kill tumor cells in
vivo. Until recently, most protocols for CAR T-cell generation have not selected for T-cell
subtypes for engineering, and thus contain a heterogeneous mix of CD4+ and CD8
+ T-cells along
the full spectrum of naive to effector phenotypes. A recent exception to this is the JCAR017
approach, using defined populations of CD4 and CD8 cells, with impacts on efficacy and
persistence that are still being studied (72). A number of studies have assessed T-cell predictors
of therapeutic response in chronic lymphocytic leukemia (42), non-Hodgkin lymphoma (73), and
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

11
multiple myeloma (74). Fraietta et al. found that sustained response to CAR T-cell therapy in
chronic lymphocytic leukemia was associated with increased prevalence of CD27+CD45RO
-
CD8+ memory-like T-cells prior to CAR T-cell generation, and the presence of CD27
+PD-1
-
CD8+ CAR T-cells expressing high levels of the IL-6 receptor-β chain was predictive of
therapeutic response (42). In a study of non-Hodgkin lymphoma, Rossi et al. applied a single-
cell secreted cytokine assay on pre-infusion CAR T-cells, and developed a predictive score based
on the proportion of cells secreting multiple cytokines and the mean fluorescence intensity of
secreted proteins per cell; they reported that their score was significantly associated with
treatment response (73). In a study of multiple myeloma, Cohen et al. found that a higher
CD4:CD8 ratio in the initial leukapheresis product was associated with greater CAR T-cell
expansion in vivo (74). An important area of study has been understanding of the role of early
memory phenotypes (75), such as naive T-cells, in establishing proliferative populations and
long-term memory. Selection or enrichment of T-cell subtypes has been proposed as a major area
of interest for improving CAR T-cell therapies (76,77), which may be aided by the recent
proliferation of single-cell transcriptomic, epigenomic, and proteomic technologies.
T-cell subset assessment has conventionally relied on the use of individual cell-surface protein
markers, but recent technologies have made it possible to interrogate large numbers of markers at
a single-cell level in combination with other molecular and imaging assays. Single-cell mass
cytometry uses flow cytometry and mass spectrometry with discrete isotopes to characterize
large numbers of cell surface protein markers simultaneously at a single-cell level (78).
Simultaneous profiling of single-cell RNA transcriptomes with proteomics has been made
possible with CITE-Seq and REAP-Seq, methods that combine single-cell RNA-Seq with
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

12
oligonucleotide-labeled antibodies that bind to cell surface proteins (79,80). These methods may
be used to distinguish between CAR T-cells and non-CAR T-cells in single-cell transcriptomic
studies, allowing for the capacity to identify gene expression pathways specific to the
endogenous and engineered cell populations.
Single-cell RNA-Seq has been a breakthrough technology for characterizing whole-
transcriptome gene expression at a single-cell resolution. Single-cell RNA-Seq has been used to
profile infiltrating T-cells in several solid tumor types (81,82), demonstrating the ability to
investigate T-cell populations within the tumor microenvironment. Tikhonova et al. and
Baryawno et al. recently characterized the mouse bone marrow microenvironment using single-
cell RNA-Seq, providing key insights into cellular phenotypes and signaling that underlies the
bone marrow niche (83,84). Applying single-cell transcriptomics to complex populations of
peripheral and infiltrating T-cells in CAR T-cell therapy may aid in identifying subpopulations
and cellular pathways that mediate proliferation, persistence, and memory formation.
Characterization of suppressive cell types in the tumor microenvironment, such as tumor-
associated macrophages, cancer-associated fibroblasts, myeloid-derived suppressor cells, and
regulatory T-cells, may aid in understanding the contribution of these cells in the efficacy of
CAR T-cell therapy. Without doubt, current single-cell technologies still have a number of
limitations, such as coverage and throughput. There has been significant work to address these
and other technical challenges in single-cell RNA-Seq, including variability in sequencing depth
and cell size, drop out, and batch effect correction (85).
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

13
Improving the engineering of CAR T-cells with the goal of increasing efficacy, speeding
manufacturing, and decreasing toxicity is a central challenge in the field, with the potential to
enhance existing therapies and accelerate the adoption of cellular therapeutics to other cancer
types. Beyond cancer therapy, CAR T-cells have been designed for other therapeutic purposes,
including autoimmune disease (86), prevention of allogeneic transplant rejection (87), and
against infectious disease (88,89). Modeling of intracellular and extracellular interactions may
play an important role in the design of novel engineering of CAR components. The intracellular
pathway mediating cytotoxic response in CAR T-cells is incompletely understood, and recent
studies have applied computational modeling to understand phosphorylation kinetics of certain
CAR constructs (90). A number of synthetic biology approaches have been designed to augment
and enhance CAR construction, including T-cells engineered with kill switches, growth switches,
chemokine receptors, multiple targets, and avoidance of allogeneic rejection (91,92).
Addressing challenges in solid tumors
CAR T-cell therapies have seen their greatest success in hematological B-cell malignancies, and
the design of an effective CAR T-cell therapy for solid tumors is a key objective in pediatric and
adult clinical oncology. In contrast to hematological cancers, solid tumors pose particular
challenges including the need for CAR T-cell trafficking and infiltration, overcoming a hypoxic
and metabolically constrained tumor microenvironment, and the presence of suppressive cell
populations (29). These factors have been hypothesized to be major barriers to the effective
implementation of CAR T-cell therapy in solid tumors.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

14
In CAR T-cell therapy, T-cells are typically extracted from and re-infused into the peripheral
circulation, making it necessary for CAR T-cells to enter the tumor microenvironment. To
address this challenge, some groups have explored intracavitary or intratumoral injection of CAR
T-cells (93,94). This strategy may be technically challenging, and even more importantly, it is
unclear to what extent regionally delivered CAR T-cells can migrate to other tumor sites in
highly disseminated disease. The level of T-cell infiltration into solid tumors has been correlated
with chemokine expression in the tumor microenvironment, and variability in chemokine
expression may explain the low level of T-cell infiltration in some tumors (95). Some groups
have focused on engineering approaches to localize CAR T-cells, such as the manufacturing of
T-cells with receptors for chemokine CCR2 to increase cellular migration (96) or injection of
amphiphile CAR T-cell ligands that traffic with endogenous albumin to lymph nodes and
enhance the interaction between CAR T-cells and antigen-presenting cells (97).
Recent technological advances in proteomics and single-cell RNA-sequencing has improved our
understanding of the composition and cellular interactions within the tumor-immune
microenvironment (98). For example, Spitzer et al. performed mass cytometry of immune cells
in multiple anatomical compartments of a mouse model of cancer immunotherapy, and
demonstrated that immune activation occurs systemically in initial therapy but only in the
peripheral compartment during tumor rejection (99). In particular, the role of regulatory T-cells,
M2 macrophages, and myeloid-derived suppressor cells in immune evasion has been
demonstrated in clinical and pre-clinical studies of other immunotherapies in solid tumors (100);
however, limited sample sizes and technical challenges in raising immunocompetent mouse
models have made it challenging to directly study these interactions of CAR T-cells with these
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

15
cellular populations (28). Ongoing consortia, such as the Human Tumor Atlas Network and the
Adult Immunotherapy Network, have dedicated significant resources into generating publicly
accessible data that will be key to unravelling the basis of immune suppression in the tumor-
immune microenvironment. An exciting advance in the field has been the integration of cellular
imaging with single-cell molecular profiling. Technologies such as Spatial Transcriptomics and
Slide-Seq have been recently developed to integrate single-cell RNA-Seq with cellular imaging
(101,102), providing an opportunity to understand the spatial context of cellular populations in
the tumor-immune microenvironment. Highly multiplexed analysis of proteins in the context of
tissue imaging has been made possible with several imaging technologies, including Imaging
Mass Cytometry (IMC) (103), Multiplexed Ion Beam Imaging (MIBI) (104), and co-detection by
indexing (CODEX) (105). These resources will provide rich datasets for modeling the signal
transduction pathways within the tumor microenvironment in CAR T-cell therapy.
Identifying tumor-specific antigens is a challenge for the development of future CAR T-cell
therapies for non-hematopoietic malignancies. One of the reasons for the success of CAR T-cell
therapies for B-cell malignancies is that the ablation of normal B-cell populations is a
manageable toxicity via immunoglobulin replacement. Cancer-associated antigens have to be
chosen carefully to avoid off-tumor, on-target toxicity, which has been a challenge in some solid
tumor CAR T-cell trials (14). Computational and functional screens have been designed to
identify cell surface proteins that are ubiquitously expressed on tumor cells but not on normal
cells (106,107). A major challenge to this approach is the lack of a comprehensive reference
catalog of normal cell populations. Consortia such as GTEx have performed bulk RNA-Seq on
multiple normal human tissues (108), but bulk assays may miss rare but important cell
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

16
populations such as adult stem cells and non-parenchymal cells. Single-cell data sources have the
potential to address this problem through their capacity to characterize rare and previously
unknown cell populations (109). Designing CAR T-cell therapies to target multiple antigens may
be an approach to circumvent antigen escape, as well as increase tumor specificity. Toward this
goal, an integration of single-cell atlases with data from individual studies may provide the
much-needed reference from which tumor-specific antigens and combinatorial antigen targets
may be identified.
Therapy-induced toxicity
CRS is the most common and significant toxicity of CAR T-cell therapy, reported to occur in 54-
91% of patients receiving anti-CD19 CAR T-cell therapy (110). This syndrome was not apparent
in preclinical models, and only became manifest in early clinical trials (2). Neurotoxicity,
referred to as immune effector cell-associated neurotoxicity syndrome, or ICANS (111), has
been observed as an adverse event, with the most concerning trait being cerebral edema. While
the underlying pathophysiology of these toxicities remain incompletely understood, clinical trials
have implicated macrophages, IL-1, endothelial activation, and especially IL-6 in the
pathogenesis of CRS. IL-6 blockage with tocilizumab is the only currently approved therapy for
CRS (2,112). Novel murine models have been recently developed, and have suggested a role of
myeloid lineages and endothelial activation in CRS (113). Giavirdis et al. (114) found that CAR
T-cells recruit and activate macrophages, leading the myeloid cells to produce IL-6 and iNOS
which contribute CRS. Norelli et al. (115) found that monocytes and macrophages were
primarily responsible for increases in IL-1 and IL-6 in their mouse model of CRS, with IL-1
production preceding and possibly stimulating IL-6 production. In a clinical trial of CD19 CAR
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

17
T-cell therapy in B-ALL, CLL, and NHL, investigators reported evidence of increased
endothelial activation in patients with severe CRS, via elevated Von Willebrand Factor and
increased Ang2:Ang1 ratio (110). Moreover, IL-6 has been shown to disrupt the blood-brain
barrier in vitro, suggesting a possible mechanistic explanation for neurotoxicity that has been
reported in some patients.
Toxicities of CAR T-cell therapy such as CRS and ICANS remain as important concerns that
may or may not be class effects of the therapy, and prognostic and therapeutic strategies will
require a deeper understanding of the underlying biological basis. While initial clinical studies
have focused on tumor cells and T-cells, a systems immunology approach will involve
investigation of cell-cell interactions with various other immune cell types in the peripheral and
marrow microenvironments. Comprehensive analyses of myeloid and lymphoid compartments in
clinical trials, as well as expansion of murine models, will be important paths forward for the
study of these therapy-limiting toxicities.
Conclusions and future directions
CAR T-cell therapy has been a breakthrough in clinical oncology. Understanding the T-cell,
tumor-cell, and tumor microenvironment factors mediating therapeutic efficacy will play a
significant role in optimizing current therapies and applying CAR T-cells to other tumor types.
Modern omics and systems biology technologies provide opportunities for biomarker discovery
and therapeutic development. As clinical cohorts of patients treated with CAR T-cell therapy
continue to grow, there will be increasing availability of clinical samples from which rich multi-
omic profiling can advance the discovery process. Like many biomedical challenges in the 21st
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

18
century, translational research will be best performed through a collaborative effort by
interdisciplinary teams of clinicians, experimental and computational biologists.
Acknowledgements
This work was supported by National Institutes of Health of United States of America grants, GM108716,
GM104369, CA226187, CA233285 (to K.T.), CA232361 (to D.B. and S.G.) and a Doris Duke Charitable
Foundation Clinical Scientist Development Award (to D.B.).
Figure Legend
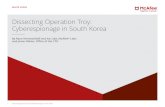
Figure 1. A systems immunology view of biomedical discovery for CAR T-cell therapy.
Immunotherapy requires cellular interactions between tumor and immune populations in multiple
physiological compartments including the peripheral circulation, tumor microenvironment, and
lymphoid tissues. Addressing the key challenges in CAR T-cell therapy will require an
understanding of these interactions among cellular phenotypes and microenvironments.
Experimental and computational advances in systems immunology provide the capacity to
simultaneously profile multiple cellular populations within each anatomical component, making
it possible to investigate the tumor-immune interactions that underlie the major challenges in
CAR T-cell therapy. Recent technological advances enable investigators to query genomic,
transcriptomic, proteomic, and epigenomic features at a single-cell level. A number of methods
for joint profiling of multiple molecular features have been developed, and imaging-based
approaches have been developed to resolve spatial context of transcriptomic and proteomic data.
Figure 2. The challenge of integrating data from heterogeneous molecular assays and
experimental sources. Prior and ongoing consortia have provided a wealth of data for multiple
immune cell populations in isolation and in interaction with each other and tumor cells.
Integrative data analysis is a major challenge in the field, and leveraging publicly available
immunological data may be a valuable approach for systems immunology model development.
The use of unlabeled immune cell data may be framed under an unsupervised transfer learning
framework, in which the target task may be dimensionality reduction or clustering of immune
cell populations. The use of labeled source data - for example, transcriptomic profiles paired with
clinical outcome of another immunotherapy modality – may follow a framework of inductive
transfer learning, in which the target task is the prediction of CAR T-cell clinical outcome.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

19
Table 1. A framework for addressing the major clinical challenges of CAR T-cell therapy
using systems immunology approaches*
Clinical challenge Systems immunology approach
Biomarker discovery Profiling of serum, tumor, and immune factors prior to
infusion
Leveraging pre-existing immunological data from other
domains using principles of transfer learning
Pre-treatment effects
and identifying
combination therapies
Modeling the perturbation of immune cell populations in
the tumor and peripheral compartments
Development of computational methods that account for
gene-gene as well as cell-cell interactions between tumor
and immune populations
Understanding T-cell
aspects to therapy failure
Joint analysis of endogenous and CAR T-cell populations
in circulation and in the tumor microenvironment
Characterization of the interactions between T-cells and
suppressive cell populations
Expanding CAR T-cell
therapy to solid tumors
Joint molecular profiling and imaging of cells in the tumor-
immune microenvironment
Leveraging data generation by ongoing consortia to
understand activating and suppressive immune factors
Antigen escape and
novel target
identification
Understanding genetic and non-genetic causes of antigen
loss
Systematic identification of candidate targets in tumor and
normal tissues
Addressing major
toxicities
Understanding immune cell interactions, particularly
interactions between lymphoid and myeloid phenotypes
Investigating the interactions between CAR T-cells,
cytokines, and organ-specific cell types
*Completed and ongoing clinical trials have brought to light a number of major clinical
challenges for CAR T-cell therapy moving forward: Biomarker discovery, pre-treatment effects
and identifying combination therapies, understanding T-cell aspects to therapeutic failure,
expanding CAR T-cell therapy to solid tumors, antigen escape and novel target identification,
and addressing major toxicities. For each of these major clinical challenges, the tools of systems
immunology provide a strategy to better understand the complex interactions between tumor and
immune cell populations, providing a path forward for the next generation of cellular
therapeutics.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

20
References
1. Maude SL, Frey N, Shaw PA, Aplenc R, Barrett DM, Bunin NJ, et al. Chimeric Antigen Receptor
T Cells for Sustained Remissions in Leukemia. N Engl J Med. 2014;371:1507–17.
2. Grupp SA, Kalos M, Barrett D, Aplenc R, Porter DL, Rheingold SR, et al. Chimeric Antigen
Receptor–Modified T Cells for Acute Lymphoid Leukemia. N Engl J Med. 2013;368:1509–18.
3. Park JH, Rivière I, Gonen M, Wang X, Sénéchal B, Curran KJ, et al. Long-Term Follow-up of
CD19 CAR Therapy in Acute Lymphoblastic Leukemia. N Engl J Med. 2018;378:449–59.
4. Neelapu SS, Locke FL, Bartlett NL, Lekakis LJ, Miklos DB, Jacobson CA, et al. Axicabtagene
Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N Engl J Med.
2017;377:2531–44.
5. Porter DL, Hwang W-T, Frey NV, Lacey SF, Shaw PA, Loren AW, et al. Chimeric antigen
receptor T cells persist and induce sustained remissions in relapsed refractory chronic lymphocytic
leukemia. Sci Transl Med. 2015;7:303ra139-303ra139.
6. Maude SL, Laetsch TW, Buechner J, Rives S, Boyer M, Bittencourt H, et al. Tisagenlecleucel in
Children and Young Adults with B-Cell Lymphoblastic Leukemia. N Engl J Med. 2018;378:439–
48.
7. Brown CE, Mackall CL. CAR T cell therapy: inroads to response and resistance. Nat Rev
Immunol. 2019;19:73.
8. Majzner RG, Mackall CL. Clinical lessons learned from the first leg of the CAR T cell journey.
Nat Med. 2019;25:1341–55.
9. Shah NN, Fry TJ. Mechanisms of resistance to CAR T cell therapy. Nat Rev Clin Oncol. 2019;1.
10. Davis MM, Tato CM, Furman D. Systems immunology: just getting started. Nat Immunol.
2017;18:725.
11. Villani A-C, Sarkizova S, Hacohen N. Systems Immunology: Learning the Rules of the Immune
System. Annu Rev Immunol. 2018;36:813–42.
12. Kitano H. Computational systems biology. Nature. 2002;420:206.
13. Ideker T, Galitski T, Hood L. A new approach to decoding life: systems biology. Annu Rev
Genomics Hum Genet. 2001;2:343–72.
14. Shifrut E, Carnevale J, Tobin V, Roth TL, Woo JM, Bui CT, et al. Genome-wide CRISPR Screens
in Primary Human T Cells Reveal Key Regulators of Immune Function. Cell. 2018;175:1958-
1971.e15.
15. Horlbeck MA, Xu A, Wang M, Bennett NK, Park CY, Bogdanoff D, et al. Mapping the Genetic
Landscape of Human Cells. Cell. 2018;174:953-967.e22.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

21
16. Dixit A, Parnas O, Li B, Chen J, Fulco CP, Jerby-Arnon L, et al. Perturb-Seq: Dissecting
Molecular Circuits with Scalable Single-Cell RNA Profiling of Pooled Genetic Screens. Cell.
2016;167:1853-1866.e17.
17. Regev A, Teichmann SA, Lander ES, Amit I, Benoist C, Birney E, et al. The Human Cell Atlas.
Gingeras TR, editor. eLife. 2017;6:e27041.
18. Snyder MP, Lin S, Posgai A, Atkinson M, Regev A, Rood J, et al. Mapping the Human Body at
Cellular Resolution -- The NIH Common Fund Human BioMolecular Atlas Program.
ArXiv190307231 Q-Bio [Internet]. 2019 [cited 2019 Aug 3]; Available from:
http://arxiv.org/abs/1903.07231
19. Castiglione F, Piccoli B. Cancer immunotherapy, mathematical modeling and optimal control. J
Theor Biol. 2007;247:723–32.
20. Mostolizadeh R, Afsharnezhad Z, Marciniak-Czochra A. Mathematical model of Chimeric Anti-
gene Receptor (CAR) T cell therapy with presence of cytokine [Internet]. Numer. Algebra Control
Optim. Vol. 8 Pages 63-80. 2018 [cited 2019 Jul 31]. Available from:
http://www.aimsciences.org.proxy.library.upenn.edu/article/doi/10.3934/naco.2018004
21. Vidal M, Cusick ME, Barabási A-L. Interactome networks and human disease. Cell.
2011;144:986–98.
22. Mitra K, Carvunis A-R, Ramesh SK, Ideker T. Integrative approaches for finding modular
structure in biological networks. Nat Rev Genet. 2013;14:719–32.
23. Iacono G, Massoni-Badosa R, Heyn H. Single-cell transcriptomics unveils gene regulatory
network plasticity. Genome Biol. 2019;20:110.
24. Lopez R, Regier J, Cole MB, Jordan MI, Yosef N. Deep generative modeling for single-cell
transcriptomics. Nat Methods. 2018;15:1053–8.
25. Aibar S, González-Blas CB, Moerman T, Huynh-Thu VA, Imrichova H, Hulselmans G, et al.
SCENIC: single-cell regulatory network inference and clustering. Nat Methods. 2017;14:1083–6.
26. Stuart T, Satija R. Integrative single-cell analysis. Nat Rev Genet. 2019;20:257–72.
27. Finotello F, Rieder D, Hackl H, Trajanoski Z. Next-generation computational tools for
interrogating cancer immunity. Nat Rev Genet. 2019;20:724–46.
28. Newick K, O’Brien S, Moon E, Albelda SM. CAR T Cell Therapy for Solid Tumors. Annu Rev
Med. 2017;68:139–52.
29. Long KB, Young RM, Boesteanu AC, Davis MM, Melenhorst JJ, Lacey SF, et al. CAR T Cell
Therapy of Non-hematopoietic Malignancies: Detours on the Road to Clinical Success. Front
Immunol [Internet]. 2018 [cited 2019 Feb 15];9. Available from:
https://www.frontiersin.org/articles/10.3389/fimmu.2018.02740/full
30. Weide B, Martens A, Hassel JC, Berking C, Postow MA, Bisschop K, et al. Baseline biomarkers
for outcome of melanoma patients treated with pembrolizumab. Clin Cancer Res Off J Am Assoc
Cancer Res. 2016;22:5487–96.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

22
31. Syn NL, Teng MWL, Mok TSK, Soo RA. De-novo and acquired resistance to immune checkpoint
targeting. Lancet Oncol. 2017;18:e731–41.
32. Romano E, Kusio-Kobialka M, Foukas PG, Baumgaertner P, Meyer C, Ballabeni P, et al.
Ipilimumab-dependent cell-mediated cytotoxicity of regulatory T cells ex vivo by nonclassical
monocytes in melanoma patients. Proc Natl Acad Sci U S A. 2015;112:6140–5.
33. Carthon BC, Wolchok JD, Yuan J, Kamat A, Ng Tang DS, Sun J, et al. Preoperative CTLA-4
blockade: tolerability and immune monitoring in the setting of a presurgical clinical trial. Clin
Cancer Res. 2010;16:2861–71.
34. Hamid O, Schmidt H, Nissan A, Ridolfi L, Aamdal S, Hansson J, et al. A prospective phase II trial
exploring the association between tumor microenvironment biomarkers and clinical activity of
ipilimumab in advanced melanoma. J Transl Med. 2011;9:204.
35. Postow MA, Manuel M, Wong P, Yuan J, Dong Z, Liu C, et al. Peripheral T cell receptor diversity
is associated with clinical outcomes following ipilimumab treatment in metastatic melanoma. J
Immunother Cancer [Internet]. 2015 [cited 2019 Apr 18];3. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4469400/
36. Carbognin L, Pilotto S, Milella M, Vaccaro V, Brunelli M, Caliò A, et al. Differential Activity of
Nivolumab, Pembrolizumab and MPDL3280A according to the Tumor Expression of Programmed
Death-Ligand-1 (PD-L1): Sensitivity Analysis of Trials in Melanoma, Lung and Genitourinary
Cancers. PloS One. 2015;10:e0130142.
37. Van Allen EM, Miao D, Schilling B, Shukla SA, Blank C, Zimmer L, et al. Genomic correlates of
response to CTLA-4 blockade in metastatic melanoma. Science. 2015;350:207–11.
38. Rizvi NA, Hellmann MD, Snyder A, Kvistborg P, Makarov V, Havel JJ, et al. Mutational
landscape determines sensitivity to PD-1 blockade in non–small cell lung cancer. Science.
2015;348:124–8.
39. Brand A, Singer K, Koehl GE, Kolitzus M, Schoenhammer G, Thiel A, et al. LDHA-Associated
Lactic Acid Production Blunts Tumor Immunosurveillance by T and NK Cells. Cell Metab.
2016;24:657–71.
40. Teachey DT, Lacey SF, Shaw PA, Melenhorst JJ, Maude SL, Frey N, et al. Identification of
Predictive Biomarkers for Cytokine Release Syndrome after Chimeric Antigen Receptor T cell
Therapy for Acute Lymphoblastic Leukemia. Cancer Discov. 2016;CD-16-0040.
41. Twyman-Saint Victor C, Rech AJ, Maity A, Rengan R, Pauken KE, Stelekati E, et al. Radiation
and dual checkpoint blockade activate non-redundant immune mechanisms in cancer. Nature.
2015;520:373–7.
42. Fraietta JA, Lacey SF, Orlando EJ, Pruteanu-Malinici I, Gohil M, Lundh S, et al. Determinants of
response and resistance to CD19 chimeric antigen receptor (CAR) T cell therapy of chronic
lymphocytic leukemia. Nat Med. 2018;24:563.
43. Cherkassky L, Morello A, Villena-Vargas J, Feng Y, Dimitrov DS, Jones DR, et al. Human CAR
T cells with cell-intrinsic PD-1 checkpoint blockade resist tumor-mediated inhibition. J Clin
Invest. 2016;126:3130–44.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

23
44. Shay T, Kang J. Immunological Genome Project and systems immunology. Trends Immunol.
2013;34:602–9.
45. Jiang P, Gu S, Pan D, Fu J, Sahu A, Hu X, et al. Signatures of T cell dysfunction and exclusion
predict cancer immunotherapy response. Nat Med. 2018;24:1550.
46. Krieg C, Nowicka M, Guglietta S, Schindler S, Hartmann FJ, Weber LM, et al. High-dimensional
single-cell analysis predicts response to anti-PD-1 immunotherapy. Nat Med. 2018;24:144–53.
47. Pan SJ, Yang Q. A Survey on Transfer Learning. IEEE Trans Knowl Data Eng. 2010;22:1345–59.
48. Coudray N, Ocampo PS, Sakellaropoulos T, Narula N, Snuderl M, Fenyö D, et al. Classification
and mutation prediction from non–small cell lung cancer histopathology images using deep
learning. Nat Med. 2018;24:1559–67.
49. Esteva A, Kuprel B, Novoa RA, Ko J, Swetter SM, Blau HM, et al. Dermatologist-level
classification of skin cancer with deep neural networks. Nature. 2017;542:115–8.
50. Bhattacharya R, Sivakumar A, Tokheim C, Guthrie VB, Anagnostou V, Velculescu VE, et al.
Evaluation of machine learning methods to predict peptide binding to MHC Class I proteins.
bioRxiv. 2017;154757.
51. Sanchez-Garcia F, Villagrasa P, Matsui J, Kotliar D, Castro V, Akavia U-D, et al. Integration of
Genomic Data Enables Selective Discovery of Breast Cancer Drivers. Cell. 2014;159:1461–75.
52. Stein-O’Brien GL, Clark BS, Sherman T, Zibetti C, Hu Q, Sealfon R, et al. Decomposing Cell
Identity for Transfer Learning across Cellular Measurements, Platforms, Tissues, and Species. Cell
Syst. 2019;8:395-411.e8.
53. Liu WM, Fowler DW, Smith P, Dalgleish AG. Pre-treatment with chemotherapy can enhance the
antigenicity and immunogenicity of tumours by promoting adaptive immune responses. Br J
Cancer. 2010;102:115–23.
54. Galluzzi L, Buqué A, Kepp O, Zitvogel L, Kroemer G. Immunological Effects of Conventional
Chemotherapy and Targeted Anticancer Agents. Cancer Cell. 2015;28:690–714.
55. Pfirschke C, Engblom C, Rickelt S, Cortez-Retamozo V, Garris C, Pucci F, et al. Immunogenic
Chemotherapy Sensitizes Tumors to Checkpoint Blockade Therapy. Immunity. 2016;44:343–54.
56. Mahoney KM, Rennert PD, Freeman GJ. Combination cancer immunotherapy and new
immunomodulatory targets. Nat Rev Drug Discov. 2015;14:561–84.
57. Turtle CJ, Berger C, Sommermeyer D, Hanafi L-A, Pender B, Robinson EM, et al. Anti-CD19
Chimeric Antigen Receptor-Modified T Cell Therapy for B Cell Non-Hodgkin Lymphoma and
Chronic Lymphocytic Leukemia: Fludarabine and Cyclophosphamide Lymphodepletion Improves
In Vivo Expansion and Persistence of CAR-T Cells and Clinical Outcomes. Blood. 2015;126:184–
184.
58. Wrzesinski C, Paulos CM, Kaiser A, Muranski P, Palmer DC, Gattinoni L, et al. Increased
intensity lymphodepletion enhances tumor treatment efficacy of adoptively transferred tumor-
specific T cells. J Immunother Hagerstown Md 1997. 2010;33:1–7.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

24
59. Das RK, Storm J, Barrett DM. Abstract 1631: T cell dysfunction in pediatric cancer patients at
diagnosis and after chemotherapy can limit chimeric antigen receptor potential. Cancer Res.
2018;78:1631–1631.
60. Al-Lazikani B, Banerji U, Workman P. Combinatorial drug therapy for cancer in the post-genomic
era. Nat Biotechnol. 2012;30:679–92.
61. Li AM, Hucks GE, Dinofia AM, Seif AE, Teachey DT, Baniewicz D, et al. Checkpoint Inhibitors
Augment CD19-Directed Chimeric Antigen Receptor (CAR) T Cell Therapy in Relapsed B-Cell
Acute Lymphoblastic Leukemia. Blood. 2018;132:556–556.
62. Barretina J, Caponigro G, Stransky N, Venkatesan K, Margolin AA, Kim S, et al. The Cancer Cell
Line Encyclopedia enables predictive modelling of anticancer drug sensitivity. Nature.
2012;483:603–7.
63. Garnett MJ, Edelman EJ, Heidorn SJ, Greenman CD, Dastur A, Lau KW, et al. Systematic
identification of genomic markers of drug sensitivity in cancer cells. Nature. 2012;483:570–5.
64. Han K, Jeng EE, Hess GT, Morgens DW, Li A, Bassik MC. Synergistic drug combinations for
cancer identified in a CRISPR screen for pairwise genetic interactions. Nat Biotechnol.
2017;35:463–74.
65. Jerby-Arnon L, Pfetzer N, Waldman YY, McGarry L, James D, Shanks E, et al. Predicting
Cancer-Specific Vulnerability via Data-Driven Detection of Synthetic Lethality. Cell.
2014;158:1199–209.
66. Hu Y, Chen C-H, Ding Y-Y, Wen X, Wang B, Gao L, et al. Optimal control nodes in disease-
perturbed networks as targets for combination therapy. Nat Commun. 2019;10:2180.
67. Lee JS, Das A, Jerby-Arnon L, Arafeh R, Auslander N, Davidson M, et al. Harnessing synthetic
lethality to predict the response to cancer treatment. Nat Commun. 2018;9:2546.
68. Sinha S, Thomas D, Chan S, Gao Y, Brunen D, Torabi D, et al. Systematic discovery of mutation-
specific synthetic lethals by mining pan-cancer human primary tumor data. Nat Commun.
2017;8:15580.
69. Lesterhuis WJ, Rinaldi C, Jones A, Rozali EN, Dick IM, Khong A, et al. Network analysis of
immunotherapy-induced regressing tumours identifies novel synergistic drug combinations. Sci
Rep. 2015;5:12298.
70. Jerby-Arnon L, Shah P, Cuoco MS, Rodman C, Su M-J, Melms JC, et al. A Cancer Cell Program
Promotes T Cell Exclusion and Resistance to Checkpoint Blockade. Cell. 2018;175:984-997.e24.
71. Gotwals P, Cameron S, Cipolletta D, Cremasco V, Crystal A, Hewes B, et al. Prospects for
combining targeted and conventional cancer therapy with immunotherapy. Nat Rev Cancer.
2017;17:286–301.
72. Abramson JS, Gordon LI, Palomba ML, Lunning MA, Arnason JE, Forero-Torres A, et al.
Updated safety and long term clinical outcomes in TRANSCEND NHL 001, pivotal trial of
lisocabtagene maraleucel (JCAR017) in R/R aggressive NHL. J Clin Oncol. 2018;36:7505–7505.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

25
73. Rossi J, Paczkowski P, Shen Y-W, Morse K, Flynn B, Kaiser A, et al. Preinfusion polyfunctional
anti-CD19 chimeric antigen receptor T cells are associated with clinical outcomes in NHL. Blood.
2018;132:804–14.
74. Cohen AD, Melenhorst JJ, Garfall AL, Lacey SF, Davis M, Vogl DT, et al. Predictors of T Cell
Expansion and Clinical Responses Following B-Cell Maturation Antigen-Specific Chimeric
Antigen Receptor T Cell Therapy (CART-BCMA) for Relapsed/Refractory Multiple Myeloma
(MM). Blood. 2018;132:1974–1974.
75. Singh N, Perazzelli J, Grupp SA, Barrett DM. Early memory phenotypes drive T cell proliferation
in patients with pediatric malignancies. Sci Transl Med. 2016;8:320ra3-320ra3.
76. Sadelain M, Rivière I, Riddell S. Therapeutic T cell engineering. Nature. 2017;545:423.
77. Qin H, Dong Z, Wang X, Cheng WA, Wen F, Xue W, et al. CAR T cells targeting BAFF-R can
overcome CD19 antigen loss in B cell malignancies. Sci Transl Med. 2019;11:eaaw9414.
78. Bendall SC, Simonds EF, Qiu P, Amir ED, Krutzik PO, Finck R, et al. Single-Cell Mass
Cytometry of Differential Immune and Drug Responses Across a Human Hematopoietic
Continuum. Science. 2011;332:687–96.
79. Stoeckius M, Hafemeister C, Stephenson W, Houck-Loomis B, Chattopadhyay PK, Swerdlow H,
et al. Simultaneous epitope and transcriptome measurement in single cells. Nat Methods.
2017;14:865–8.
80. Peterson VM, Zhang KX, Kumar N, Wong J, Li L, Wilson DC, et al. Multiplexed quantification of
proteins and transcripts in single cells. Nat Biotechnol. 2017;35:936–9.
81. Azizi E, Carr AJ, Plitas G, Cornish AE, Konopacki C, Prabhakaran S, et al. Single-Cell Map of
Diverse Immune Phenotypes in the Breast Tumor Microenvironment. Cell. 2018;174:1293-
1308.e36.
82. Zheng C, Zheng L, Yoo J-K, Guo H, Zhang Y, Guo X, et al. Landscape of Infiltrating T Cells in
Liver Cancer Revealed by Single-Cell Sequencing. Cell. 2017;169:1342-1356.e16.
83. Tikhonova AN, Dolgalev I, Hu H, Sivaraj KK, Hoxha E, Cuesta-Domínguez Á, et al. The bone
marrow microenvironment at single-cell resolution. Nature. 2019;569:222.
84. Baryawno N, Przybylski D, Kowalczyk MS, Kfoury Y, Severe N, Gustafsson K, et al. A Cellular
Taxonomy of the Bone Marrow Stroma in Homeostasis and Leukemia. Cell. 2019;177:1915-
1932.e16.
85. Stegle O, Teichmann SA, Marioni JC. Computational and analytical challenges in single-cell
transcriptomics. Nat Rev Genet. 2015;16:133–45.
86. Ellebrecht CT, Bhoj VG, Nace A, Choi EJ, Mao X, Cho MJ, et al. Reengineering chimeric antigen
receptor T cells for targeted therapy of autoimmune disease. Science. 2016;353:179–84.
87. Noyan F, Zimmermann K, Hardtke‐Wolenski M, Knoefel A, Schulde E, Geffers R, et al.
Prevention of Allograft Rejection by Use of Regulatory T Cells With an MHC-Specific Chimeric
Antigen Receptor. Am J Transplant. 2017;17:917–30.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

26
88. Kumaresan PR, Manuri PR, Albert ND, Maiti S, Singh H, Mi T, et al. Bioengineering T cells to
target carbohydrate to treat opportunistic fungal infection. Proc Natl Acad Sci. 2014;111:10660–5.
89. Scholler J, Brady TL, Binder-Scholl G, Hwang W-T, Plesa G, Hege KM, et al. Decade-Long
Safety and Function of Retroviral-Modified Chimeric Antigen Receptor T Cells. Sci Transl Med.
2012;4:132ra53-132ra53.
90. Rohrs JA, Zheng D, Graham NA, Wang P, Finley SD. Computational Model of Chimeric Antigen
Receptors Explains Site-Specific Phosphorylation Kinetics. Biophys J. 2018;115:1116–29.
91. Chakravarti D, Wong WW. Synthetic biology in cell-based cancer immunotherapy. Trends
Biotechnol. 2015;33:449–61.
92. Fesnak AD, June CH, Levine BL. Engineered T cells: the promise and challenges of cancer
immunotherapy. Nat Rev Cancer. 2016;16:566.
93. Adusumilli PS, Cherkassky L, Villena-Vargas J, Colovos C, Servais E, Plotkin J, et al. Regional
delivery of mesothelin-targeted CAR T cell therapy generates potent and long-lasting CD4-
dependent tumor immunity. Sci Transl Med. 2014;6:261ra151-261ra151.
94. van Schalkwyk MCI, Papa SE, Jeannon J-P, Urbano TG, Spicer JF, Maher J. Design of a Phase I
Clinical Trial to Evaluate Intratumoral Delivery of ErbB-Targeted Chimeric Antigen Receptor T-
Cells in Locally Advanced or Recurrent Head and Neck Cancer. Hum Gene Ther Clin Dev.
2013;24:134–42.
95. Harlin H, Meng Y, Peterson AC, Zha Y, Tretiakova M, Slingluff C, et al. Chemokine Expression
in Melanoma Metastases Associated with CD8+ T-Cell Recruitment. Cancer Res. 2009;69:3077–
85.
96. Moon EK, Carpenito C, Sun J, Wang L-CS, Kapoor V, Predina J, et al. Expression of a Functional
CCR2 Receptor Enhances Tumor Localization and Tumor Eradication by Retargeted Human T
cells Expressing a Mesothelin-Specific Chimeric Antibody Receptor. Clin Cancer Res.
2011;17:4719–30.
97. Ma L, Dichwalkar T, Chang JYH, Cossette B, Garafola D, Zhang AQ, et al. Enhanced CAR–T cell
activity against solid tumors by vaccine boosting through the chimeric receptor. Science.
2019;365:162–8.
98. Binnewies M, Roberts EW, Kersten K, Chan V, Fearon DF, Merad M, et al. Understanding the
tumor immune microenvironment (TIME) for effective therapy. Nat Med. 2018;24:541.
99. Spitzer MH, Carmi Y, Reticker-Flynn NE, Kwek SS, Madhireddy D, Martins MM, et al. Systemic
Immunity Is Required for Effective Cancer Immunotherapy. Cell. 2017;168:487-502.e15.
100. Gajewski TF, Schreiber H, Fu Y-X. Innate and adaptive immune cells in the tumor
microenvironment. Nat Immunol. 2013;14:1014.
101. Ståhl PL, Salmén F, Vickovic S, Lundmark A, Navarro JF, Magnusson J, et al. Visualization and
analysis of gene expression in tissue sections by spatial transcriptomics. Science. 2016;353:78–82.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

27
102. Rodriques SG, Stickels RR, Goeva A, Martin CA, Murray E, Vanderburg CR, et al. Slide-seq: A
scalable technology for measuring genome-wide expression at high spatial resolution. Science.
2019;363:1463–7.
103. Giesen C, Wang HAO, Schapiro D, Zivanovic N, Jacobs A, Hattendorf B, et al. Highly
multiplexed imaging of tumor tissues with subcellular resolution by mass cytometry. Nat Methods.
2014;11:417–22.
104. Angelo M, Bendall SC, Finck R, Hale MB, Hitzman C, Borowsky AD, et al. Multiplexed ion
beam imaging of human breast tumors. Nat Med. 2014;20:436–42.
105. Goltsev Y, Samusik N, Kennedy-Darling J, Bhate S, Hale M, Vazquez G, et al. Deep Profiling of
Mouse Splenic Architecture with CODEX Multiplexed Imaging. Cell. 2018;174:968-981.e15.
106. Hinrichs CS, Restifo NP. Reassessing target antigens for adoptive T-cell therapy. Nat Biotechnol.
2013;31:999–1008.
107. Li L-P, Lampert JC, Chen X, Leitao C, Popović J, Müller W, et al. Transgenic mice with a diverse
human T cell antigen receptor repertoire. Nat Med. 2010;16:1029–34.
108. Lonsdale J, Thomas J, Salvatore M, Phillips R, Lo E, Shad S, et al. The Genotype-Tissue
Expression (GTEx) project. Nat Genet. 2013;45:580–5.
109. Rozenblatt-Rosen O, Stubbington MJT, Regev A, Teichmann SA. The Human Cell Atlas: from
vision to reality. Nat News. 2017;550:451.
110. Hay KA, Hanafi L-A, Li D, Gust J, Liles WC, Wurfel MM, et al. Kinetics and biomarkers of
severe cytokine release syndrome after CD19 chimeric antigen receptor–modified T-cell therapy.
Blood. 2017;130:2295–306.
111. Lee DW, Santomasso BD, Locke FL, Ghobadi A, Turtle CJ, Brudno JN, et al. ASTCT Consensus
Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated with Immune
Effector Cells. Biol Blood Marrow Transplant. 2019;25:625–38.
112. O’Leary MC, Lu X, Huang Y, Lin X, Mahmood I, Przepiorka D, et al. FDA Approval Summary:
Tisagenlecleucel for Treatment of Patients with Relapsed or Refractory B-Cell Precursor Acute
Lymphoblastic Leukemia. Clin Cancer Res. 2018;clincanres.2035.2018.
113. van der Stegen SJC, Davies DM, Wilkie S, Foster J, Sosabowski JK, Burnet J, et al. Preclinical in
vivo modeling of cytokine release syndrome induced by ErbB-retargeted human T cells:
identifying a window of therapeutic opportunity? J Immunol Baltim Md 1950. 2013;191:4589–98.
114. Giavridis T, van der Stegen SJC, Eyquem J, Hamieh M, Piersigilli A, Sadelain M. CAR T cell–
induced cytokine release syndrome is mediated by macrophages and abated by IL-1 blockade. Nat
Med. 2018;24:731–8.
115. Norelli M, Camisa B, Barbiera G, Falcone L, Purevdorj A, Genua M, et al. Monocyte-derived IL-1
and IL-6 are differentially required for cytokine-release syndrome and neurotoxicity due to CAR T
cells. Nat Med. 2018;24:739–48.
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

Figure 1:
Peripheral circulation Solid tumor microenvironmentKey technologies in systems immunology
Key challenges in CAR T-cell therapy
Genomics:- Whole-genome and whole-exome sequencing- Single-cell DNA-Seq- Deep genomic sequencing- TCR/BCR sequencing
Transcriptomics and proteomics:- Single-cell RNA-Seq- CITE-Seq and REAP-Seq- Mass cytometry- Slide-Seq, spatial transcriptomics- Imaging mass cytometry (IMC), multiplexed ion beam imaging (MIBI), co-detection by indexing (CODEX)
Epigenomics:- Single-cell ATAC-Seq- Single-cell DNA methylation- Single-cell Hi-C
Prior treatment e�ects and circulating factorsIntrinsic T-cell dysfunctionInadequate T-cell infiltrationSuppressive tumor microenvironmentDevelopment of antigen-negative subclonesFailure of T cells to establish memoryCytokine release syndrome and other toxicities
1
EndogenousT cell
FibroblastAntigen (-)cancer cell
Myeloid-derivedsuppressor cell
RegulatoryT cell
Antigen-presenting
cell
Bone marrow microenvironment
Blast cell
Lymphoid tissue
5
4CAR T cell
Antigen (+)cancer cell
Endothelialcell
Macrophage
IL-6IL-1IFNγ
1
2
3
6
7
2
3
4
5
6
7
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

Figure 2:
Publicly available immunological data
CAR T-cell clinical and preclinical data
DNA
Tumor/immune cellsfrom human cell atlas,ImmGen, or immunecheckpoint blockade
study
High-throughput datageneration
Clinical or phenotypicannotation
Computationalmodels of cell-cell
and gene-geneinteractions
Knowledgetransfer
Computationalmodels of cell-cell
and gene-geneinteractions
Biomarker discovery for patient selection and prognosis
Mechanistic insights to guide CAR T-cell engineering in solid and liquid tumors
Synergistic and antagonistic combination therapies
Tumor/immune cellsfrom peripheral
circulation,tumor-immune
microenvironment
High-throughput datageneration Clinical annotation
RNAProtein
Imaging
DNARNA
ProteinImaging
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888

Published OnlineFirst March 3, 2020.Clin Cancer Res Gregory M Chen, Andrew Azzam, Yang-Yang Ding, et al. systems immunology approachreceptor T-cell therapy: key challenges and opportunities for a Dissecting the tumor-immune landscape in chimeric antigen
Updated version
10.1158/1078-0432.CCR-19-3888doi:
Access the most recent version of this article at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2020/03/03/1078-0432.CCR-19-3888To request permission to re-use all or part of this article, use this link
Research. on July 16, 2020. © 2020 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3888