Disclosure, Objective
35
Rational Use of Rheumatologic Lab Tests: aka “Choosing Wisely” Maryland ACP Scientific Meeting David B. Hellmann, M.D., M.A.C.P. Johns Hopkins Bayview January 31, 2014
description
Rational Use of Rheumatologic Lab Tests: aka “Choosing Wisely” Maryland ACP Scientific Meeting David B. Hellmann, M.D., M.A.C.P . Johns Hopkins Bayview January 31, 2014. Disclosure, Objective. Disclosure: none Objective: - PowerPoint PPT Presentation
Transcript of Disclosure, Objective

Rational Use of Rheumatologic Lab Tests:aka “Choosing Wisely”
Maryland ACP Scientific Meeting
David B. Hellmann, M.D., M.A.C.P.Johns Hopkins BayviewJanuary 31, 2014

2
Disclosure, Objective
Disclosure: noneObjective:
◦To use a case-based approached to discuss wise use of laboratory tests in rheumatic diseases
Methods—Accenting … Choosing Wisely, Cases, and Differential Diagnosis

Published simultaneously in 2002 in Annals of Internal
Medicine, The Lancet and the European Journal of
Internal Medicine
Charter articulated 3 principles
1. Primacy of the patient
2. Autonomy of the patient
3. Social justice
◦ Includes aspiring to be good stewards of society’s resources
Medical Professionalism in the New Millennium: A Physician
Charter

1. Don’t test ANA sub-serologies without a positive ANA and clinical suspicion of immune-mediated disease.
2. Don’t test for Lyme disease as a cause of musculoskeletal symptoms without an exposure history and appropriate exam findings
3. Don’t perform MRI of peripheral joints to routinely monitor inflammatory arthritis
Choosing Wisely: ACR Top 5
4. Don’t prescribe biologics for rheumatoid arthritis before a trial of methotrexate (or other conventional non-biologic DMARDs)
5. Don’t routinely repeat DXA scans more often than once every two years
Choosing Wisely: ACR Top 5

1. Don’t do imaging for low back pain within the first 6 weeks, unless red flags are present
2. Don’t use DEXA screening for osteoporosis in women < 65 or men < 70 with no risk factors.
AAFP Choosing Wisely

7
Case PresentationCC: 42 y.o. man with acute LBP
HPI: Moved office 48 hrs ago Awoke with acute LBP; worse with activity, better with rest. Naprosyn helps some.
ROS: No fever, weakness, bowel/bladder sxs
PMH: negativeExamination: VS normal; tenderness LB; neuro exam (-)
What tests should you order?

8
Red Flags for LBP:AHRQ Criteria for X-ray for Acute LBP
Possible fracture◦ Major trauma, minor trauma > age 50◦ Long-term corticosteroid use◦ Osteoporosis◦ Age > 70
Possible Tumor or Infection◦ Age > 50, < 20◦ History of cancer, injection drug use,recent bacterial
infection, constitutional symptoms, immunosuppression
◦ Pain when supine or at night

9
Case PresentationCC: 78 y.o woman with headache
HPI: 2 months fatigue, malaise, 5 lb weight loss 1 month of intermittent dull headache
PMH: hypertension, osteoarthritis
ROS: occasional jaw pain
Medications: HCTZ, acetaminophen
PE: 36.8 145/83 84 pale
Labs: Hct 32, WBC 6,700 Platelets 532k CMP-nl ESR 105

10
Erythrocyte Sedimentation Rate (ESR)
Ancient Methods: Westergren, Wintrobe Inexpensive Uses:
◦ Not diagnostic of any disease◦ Supports diagnosis of GCA, PMR, Osteomyelitis◦ Helpful in monitoring (GCA, PMR, RA,
Osteomyelitis)

Erythrocyte Sedimentation Rate

12
Erythrocyte Sedimentation Rate (ESR)
Influenced by concentration of [asymmetric particles] = fibrinogen
Requires fresh sample Normal values <20 mm
◦ But affected by age (5/decade), gender, hematocrit, red cell morphology, many plasma proteins, medications (heparin)

Giant Cell Arteritis: Accuracy of History, PE, LAB
Symptom (+) LR (-) LRJaw claudication 4.2 (2.8-6.2) 0.72 (.57-.81)
Diplopia 3.4 (1.3-8.6) 0.95 (.91-.99)Beaded TA 4.6 (1.1-18.4) 0.93 (.88-.99)Any TA abnl 2.0 (1.4-3) 0.53 (.38-.75)ESR abnl 1.1 (1-1.2) 0.2 (.08-.51)
JAMA 2002;101:287-292

Giant cell Arteritis with Low ESR Salvarani C, Hunder G. Arthritis Rheum 2001
9 (5%)# with ESR < 40 mm/hr
18 (11%)# with ESR < 50 mm/hr
167Total GCA patients
(1950-1998)
N

15
ESR: Frequently Asked Questions
1. Can the ESR be normal in GCA?Yes
2. Does a ESR > 100 have special significance?
Maybe
3. In an older person with >100 ESR and no obvious disease other than GCA, what else should I consider?
Multiple Myeloma
16
ESR Frequently Asked Questions
1. What gives false positives?Pregnancy, multiple myeloma, oral
contraceptives, MGUS
2. What gives false negatives? Polymyositis. Cryoglobulinemia,
congestive heart failure

17
ESR: Frequently Asked Questions
1. Can the ESR be used as a screening test to determine if a patient with vague symptoms is sick?
Not known!Only 31% of patients with gastric cancer have
ESR > 20
2. What’s the maximum ESR a person can have?
200 – (2 x Hct)3. Is CRP better than ESR?

18
Case Presentation CC: 19 y.o. AA woman polyarthralgia, feverHPI: 5 wks polyarthralgia, fever, malar rash, pleuritic chest pain, nocturia, ankle swellingFH: Mother had SLEPMH: negativeMeds: ibuprofenPE: T=37.9, malar erythema, alopecia, edemaLabs: Hct 32, WBC 2.7 Platelets 110k Creatinine 1.2Albumin 3.2, Urine 3+ protein, RBC casts, BC/RPR -
What autoantibodies should you order?

19
ANA: Commonly Asked Questions
What is a positive ANA? 1-10% of well people have ANA >1:80 20 of “sick” people have ANA>1:80
What is value of ANA? negative ANA excludes SLE; no value monitoring
What autoantibodies are specific for SLE? ds-DNA antibodies 99% specific; sensitivity 50% anti-SM specific (95%); sensitivity 30% low Complement: specificity ~90%, sensitivity 50%

20
ANA Prevalence
Disorder % (+) ANASLE 99RA 30-50Fibromyalgia 20Multiple Sclerosis 20Thyroid disease 40

21
Case PresentationCC: 24 y.o. woman with polyarthritisHPI: 5 wks polyarthritis mcps, pips, wrists, knees 2 hrs morning stiffness; fatigueROS: (-) fever, weight loss, rash, weakness, chest pain, back pain, travel, tick exposure, neuropathyFH: negative Meds: naproxenPE: polyarthritis; no nodulesLabs: Hct 35, ESR 58, CMP/UA negative
What autoantibodies should you order?

22
Rheumatoid Arthritis:Diagnostic Tests
TEST Sensitivity Specificity
RF 40-90% 40-90%
Anti-CCP 70-80% 85-95%
RF = rheumatoid factorAnti-CCP = anti-cyclic citrillinated
peptide

23
Differential Diagnosis Polyarthritis:If Host
Is a 26 year old day care worker with faint, diffuse rash?
Is a 55 year old smoker with new clubbing? Is a 49 year old with large joint arthritis and
red eye? Is 34 year injection drug user with recurrent
purpura?

24
Case PresentationCC: 46 yo man oligoarthralgia, nasal stuffinessHPI: 3 months oligoarthralgia knees, shoulders nasal stuffiness, crusting, bleeding red eye, cough, fever, hearing loss left earPMH: negativeSH: no cocainePE: scleritis, nasal crusting, otitis media, no joint effusionLabs: Hct 41, WBC 11k, Creatinine 1.6, urine 10-15 RBC’s; Chest CT: multiple nodules
What autoantibodies should you order?

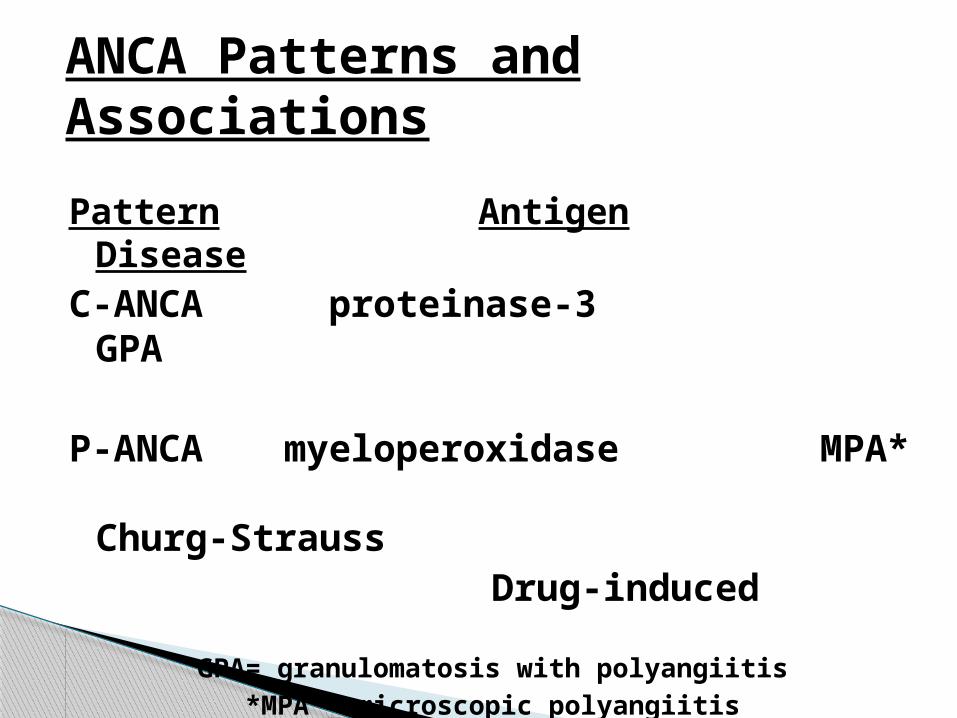
ANCA Patterns and Associations
Pattern Antigen DiseaseC-ANCA proteinase-3 GPA
P-ANCA myeloperoxidase MPA* Churg-Strauss
Drug-induced
GPA= granulomatosis with polyangiitis
*MPA = microscopic polyangiitis

Cocaine Induced Midline Destructive Lesions

Levamisole Vasculitis

29
Summary Choosing wisely is part of professionalism Avoid ordering imaging for acute LBP unless
red flags are present Most blood tests in rheumatology should be
ordered when the probability of disease is intermediate
Don’t test ANA sub-serologies without a positive ANA and clinical suspicion

30
CRP Levels
< 1 mg/dl 1-10 mg/dl >10 mg/dlNormal MI bacterial INFPregnancy CTD vasculitisDepressionObesityGingivitis

31
ANCA Do IF first; confirm result with ELISA C-ANCA = anti-PR3 = GPA P-ANCA = anti-MPO = GPA, MPA etc “Atypical” ANCA = anti-Lactoferin, etc = IBD Cocaine, levamisole can cause vasculitis
with positive C-ANCA, P-ANCA


33
CRP vs ESR C-Reactive Protein (CRP) is an acute phase
protein whose concentration reflects level of inflammation
Unaffected by age (?), gender, monoclonal antibodies; fresh sample not required
Quantification is precise; wide range of clinically relevant values
May be more sensitive than ESR in GCA, PMR

ANCA
Disease Sensitivity SpecificityGPA 70-90% 30-
90%?
MPA 70-90% 30-80%
GPA= granulomatosis with polyangiitis
*MPA = microscopic polyangiitis

c-ANCA p-ANCA