Untitled - Idaho Department of Environmental Quality - State of Idaho

DISCHARGE PLANNING BY STATE Alabama
Alaska Arkansas Arizona California Colorado Connecticut Delaware District of Columbia Florida Georgia Hawaii Idaho Illinois Indiana Iowa Kansas Kentucky Louisiana Maine Maryland Massachusetts Michigan
Missouri Montana Nebraska Nevada New Hampshire New Jersey New Mexico New York North Carolina North Dakota Ohio Oklahoma Oregon Pennsylvania Rhode Island South Carolina South Dakota Tennessee Texas Utah Vermont Virginia Washington State West Virginia Wisconsin Wyoming
Minnesota

Alabama Common Discharge Provisions at a Glance Alabama Detailed Discharge Planning Alabama Common Discharge Provision at a Glance Applies to Nursing and Similar Facilities YES Applies to Assisted Living Facilities NO Applies to Hospice NO Applies to Hospitals NO Requires notice to patient prior to discharge
30 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
YES
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate YES For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Alabama Detailed Discharge Planning Nursing Facilities (Ala. Admin. Code 420-5-10 Division of Licensure and Certification, Nursing Facilities) (Adapted from Ala. Admin. Code 420-5-10-.01, -.05, -.06, -.09) When a facility anticipates discharge, they must notify the resident, consult the resident’s physician, and notify the legal representative or interested family member IMMEDIATELY when the facility decides to discharge a resident. (420-5-10-.05) When discharged, a resident must have a discharge summary Requirements for Discharge Summary – 420-5-10-.09
1. A brief review or summary of the resident’s stay 2. A final summary of the resident’s status including at least:
a. Medically defined conditions and prior medical history; b. Medical status measurement; c. Physical and mental functional status; d. Sensory and physical impairments; e. Nutritional status and requirements; f. Special treatments or procedures; g. Mental and psychosocial status; h. Discharge potential; i. Dental condition; j. Activities potential; k. Rehabilitation potential; l. Cognitive status; and m. Drug therapy
3. This final summary must be available for release to authorized persons and agencies with the consent of the resident or legal representative at the time of resident’s discharge
4. A post-discharge plan of care, developed with the participation of the resident and his or her family, to assist the resident in adjusting to his or her new living environment
The facility may only discharge you if: 420-5-10-.06
1. The transfer or discharge is necessary for the resident's welfare and the resident's needs cannot be met in the facility;
2. The transfer or discharge is appropriate because the resident's health has improved sufficiently so the resident no longer needs the services provided by the facility;
3. The safety of individuals in the facility is endangered; 4. The health of individuals in the facility would otherwise be endangered; 5. The resident has failed, after reasonable and appropriate notice, to pay for (or to
have paid under Medicare or Medicaid) a stay at the facility. For a resident who becomes eligible for Medicaid after admission to a nursing facility, the nursing facility may charge a resident only allowable charges under Medicaid; or
6. The facility ceases to operate. The facility must give 30 days notice of the discharge unless:
(i) The safety of individuals in the facility would be endangered, under paragraph (1) (b)3 of this section.
(ii) The health of individuals in the facility would be endangered, under (1)(b)4 of this section.
(iii) The resident's health improves sufficiently to allow a more immediate transfer or discharge, under paragraph (1)(b)2 of this section;

(iv) An immediate transfer or discharge is required by the resident's urgent medical needs, under paragraph (1)(b)1 of this section; or
(v) A resident has not resided in the facility for 30 days. The Notice of Discharge or Transfer Must Include:
1. The reason for transfer or discharge; 2. The effective date of transfer or discharge; 3. The location to which the resident is transferred or discharged; 4. A statement that the resident has the right to appeal the action to the State; 5. The name, address and telephone number of the State long term care ombudsman; 6. For nursing facility residents with developmental disabilities, or are mentally ill,
the mailing address and telephone number of the Alabama Developmental Disabilities Advocacy Program (ADDAP) at the University of Alabama School of Law; and
7. Orientation for transfer or discharge. A facility must provide sufficient preparation and orientation to residents to ensure safe and orderly transfer or discharge from the facility.
There is a basic grievances process outlined (420-5-10-.05) Grievances. A resident has the right to:
1. Voice grievances without discrimination or reprisal. Such grievances include those with respect to treatment which has been furnished as well as that which has not been furnished; and
2. Prompt efforts by the facility to resolve grievances the resident may have, including those with respect to the behavior of other residents.
Source: Alabama State Board Of Health Alabama Department Of Public Health Chapter 420-5-10.pdf
-Page Up- -Discharge Planning Main-

Alaska Common Discharge Provisions at a Glance Alaska Detailed Discharge Planning
Alaska Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Assisted Living Facilities NO Applies to Hospice NO Applies to Hospitals YES Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Detailed Alaska Discharge Planning 7 Alaska Admin. Code 12.890 Patient’s Rights 7 Alaska Admin. Code 12.600 Facilities and Local Units, General Provisions A patient, client, or nursing facility resident has rights that include the following: (13) to participate in the development of a plan of care, or discharge plan, and to receive instructions for self-care and treatment that include explanation of adverse symptoms and necessary precautions, as appropriate; This applies to patients, clients, or residents in:
1. Acute Care Hospitals 2. Rural Primary Care Hospitals 3. Long-term Acute Care Hospitals 4. Critical Access Hospitals 5. Specialized hospitals 6. Nursing Facilities 7. Ambulatory Surgical Facilities 8. Free Standing Birth Centers 9. Frontier Extended Stay Clinics
(7 AAC 12.600 §b, d, e, h) Source: Alaska Patient’s Rights
-Page Up- -Discharge Planning Main-

Arkansas Common Discharge Provisions at a Glance Detailed Arkansas Discharge Planning Arkansas Common Discharge Provisions at a Glance
Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES
Arkansas Detailed Discharge Planning
016 24 CARR 007 – Code of Arkansas Rules and Regulations, Hospitals and Related Institutions 007 05 CARR 002 – Code of Arkansas Rules and Regulations, Critical Access Hospitals Applies to: (016 24 CARR 007 §3 - Definitions) Alcohol/Drug Abuse Inpatient Treatment Centers Emergency Services Facility General Hospital Maternity and General Medical Care Hospital Maternity Hospital Psychiatric Hospital Recuperation Center Rehabilitation Facility Surgery and General Medical Care Hospital Outpatient Psychiatric Center Outpatient Surgery Center Discharge Planning Generally: (016 24 CARR 007 §6(E) – Medical Staff) There shall (mandatory) be an ongoing plan, consistent with available community and hospital resources to provide or make available social work, psychological and educational services to meet the medically-related needs of the patients and to facilitate the provision of follow up care. Discharge planning shall be started at the time of the patient’s admission There shall be a policy and procedure developed for discharge planning (007 05 CARR 002 – Code of Arkansas Rules and Regulations, Critical Access Hospitals contains the same language as above
Sources: Code of Arkansas Rules and Regulations, Hospitals and Related Institutions Code of Arkansas Rules and Regulations, Critical Access Hospitals
-Page Up- -Discharge Planning Main-

Arizona Common Discharge Provisions at a Glance Detailed Arizona Discharge Planning Arizona Common Discharge Provisions at a Glance
Applies to Nursing and Similar Facilities NO Applies to Assisted Living Facilities NO Applies to Hospice NO Applies to Hospitals YES Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Detailed Arizona Discharge Planning
CHAPTER 10. DEPARTMENT OF HEALTH SERVICES HEALTH CARE INSTITUTIONS: LICENSING, ARTICLE 2. HOSPITALS, R9-10-211. Discharge Planning; Discharge Applies to Hospitals Hospitals are defined as:
“[A] class of health care institution that provides, through an organized medical staff, inpatient beds, medical services, and continuous nursing services for the diagnosis and treatment of patients.”
The Discharge Plan for inpatients 1. Identifies the specific needs of the patient after discharge, if applicable 2. Include participation of the patient or patient’s representative 3. Must be completed before discharge occurs 4. Provides the patient or representative with written information identifying classes or subclasses of health care institutions and the level of care that the health care institutions provide that may meet the patient’s assessed and anticipated needs after discharge, if applicable 5. Is documented in the patient’s medical record The Discharge Plan for Outpatients Receiving Emergency Services Discharge instructions are documented and provided to the patient or the patient’s representative before the patient is discharged unless the patient leaves the hospital against a medical staff member’s advice Transfers fall under R9-10-213 Source: Code of Arizona Rules and Regulations
-Page Up- -Discharge Planning Main-

California Common Discharge Provisions at a Glance Detailed California Discharge Planning
California Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
YES
Detailed California Discharge Planning

California Health and Safety Code Division 2 – Licensing Provisions Chapter 2 – Health Facilities Article 1 – General § 1262.5 Written discharge policy and process; Transfer summary; Contract restrictions
(a) – (f) Applies to Hospitals Discharge Each hospital must have a written discharge planning policy and process requiring that appropriate arrangements for post-hospital care are made prior to discharge for those patients who are likely to suffer adverse health consequences upon discharge if there is no adequate discharge planning. The hospital shall also provide counseling for post-hospital care if the hospital determines that the patient and family members or interested persons need it. The patient must be informed orally or in writing of their continuing health care requirements following discharge from the hospital. Each patient should receive at the time of discharge information regarding the medications dispensed. If the patient is anticipated to need long-term care at the time of discharge with contact information for at least one public or non-profit agency or organization dedicated to providing information or referral services relating to community-based long-term care options in the patient’s county of residence and appropriate to the needs and characteristics of the patient Transfers to a skilled-nursing home or intermediate care facility inside or outside of the hospital A transfer summary shall accompany the patient and will include information relative to the patient’s diagnosis, hospital course, pain treatment and management, medications, treatments, dietary requirement, rehabilitation potential, known allergies, and treatment plan. A copy of the transfer summary shall be given to the patient or their legal representative prior to transfer Source: California Health and Safety Code
-Page Up- -Discharge Planning Main-

Colorado Common Colorado Discharge Provisions at a Glance Detailed Colorado Discharge Planning Colorado Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice YES Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
YES
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO
Detailed Colorado Discharge Planning
10 CCR 2505-10 8.550.6 Applies to Day Treatment by Hospices under CO’s Medical Assistance Program A Hospice can only discharge a client if: 1. The client moves out of the Hospice’s service area or transfers to another Hospice 2. The Hospice determines that the client is no longer Terminally Ill
This situation requires a planning process that includes planning for any necessary family counseling, patient education, or other services before discharge.
3. The Hospice determines, under 42 C.F.R. §418.27, that the client’s behavior is disruptive, abusive, or uncooperative to the extent that delivery of care or the Hospice’s ability to operate effectively is seriously impaired. The Hospice must advise the client discharge is being considered, make a serious effort to resolve the problem, ascertain that the proposed discharge is not due to the client’s use of necessary Hospice services, document the problem and the effort made to resolve the problem, and enter this documentation in the client’s medical record The Hospice Medical Director must give the Hospice a written discharge order prior to discharging a client The Hospice Medical Director shall document that the attending physician has been consulted about the discharge, include the physician’s review and decision in the discharge note Source: Code of Colorado Regulation Titles
-Page Up- -Discharge Planning Main-

Connecticut Common Discharge Provisions at a Glance Detailed Connecticut Discharge Planning Connecticut Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
30 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
YES
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate YES For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Connecticut Detailed Discharge Planning
General Statutes of Connecticut, Title 19a Public Health and Well Being, Chapter 368v, Section 19a-504d Hospital discharge plans, Section 19a-535 Transfer or discharge of patients, Section 19a-535a Residential care home, and Section 19a-535b Chronic disease hospital Hospital Discharge (Sec 19a-504d) If a hospital recommends home health care to a patient, the hospital discharge plan shall include at least two options of home health care agencies. The hospital must disclose any ownership, investment interest, or compensation/remuneration with the home health agency to the patient prior to including the agency as an option in the discharge plan. This information must be verbally disclosed or posted in a conspicuous place visible to patients. Nursing Home Discharge Applies to a certified nursing facility under the Medicare program, a skilled nursing facility under the Medicare program, or a chronic and convalescent nursing home or a rest home with supervision (known collectively as “facilities”) A facility cannot transfer or discharge a patient unless: 1. The welfare of the patient cannot be met in the facility 2. The patient no longer needs the services of the facility due to improved health 3. The health or safety of individuals in the facility is endangered 4. A self-pay patient’s nonpayment or arrearage of more than 15 days the per diem facility room rate 5. The facility ceases to operate The basis for discharge must be documented by a physician in the patient’s medical record. If the basis is the endangerment of the health or safety of individuals, the documentation shall be by the patient’s physician A facility cannot transfer or discharge a patient as a result of a change in status from self-pay or Medicare to Medicaid provided the facility offers services to both categories of patients. A facility cannot involuntarily transfer or discharge a patient if it is medically contraindicated A patient who wishes to be transferred to another facility which has agreed to accept him may do so upon giving at least fifteen days written notice to the administrator of the facility from which he is to be transferred and a copy to the appropriate advocate of such patient A continuing care facility which guarantees life care for its residents may transfer or discharge a resident if: 1. A resident self-pay patient has intentionally transferred assets in a sum which will render the patient unable to pay the costs of the facility care in accordance with the contract 2. A non-resident self-pay patient who has intentionally transferred assets in a sum which will render the patient unable to pay the costs of a total of 42 months from the date of initial admission to the facility

Before effecting transfer or discharge:
1. The facility must notify in writing the patient and the patient’s guardian or conservator, or legally liable relative or other responsible party if known, of the proposed transfer or discharge at least 30 days and no more than 60 days in advance of the transfer or discharge.
2. If the transfer or discharge is due to the endangerment of the health or safety of individuals in the facility, or the patient’s health improves sufficiently to allow a more immediate transfer or discharge, or when immediate transfer or discharge is necessitated by urgent medical needs, or if the patient has not resided in the facility for 30 days, notice shall be given as many days before the transfer or discharge as possible.
Included in the Notice must be:
1. The reasons for the transfer or discharge 2. The effective date of the proposed transfer or discharge 3. The location to which the patient is to be transferred or discharged 4. The right to appeal the proposed transfer or discharge 5. The procedures for initiating such an appeal as determined by the Department of
Social Services 6. The date by which an appeal must be initiated to stay transfer or discharge (10
days from the receipt of notice of transfer or discharge from the facility) 7. That the patient may represent himself or herself or be represented by legal
counsel, a relative, a friend, or other spokesman 8. Information as to bed hold and hospital readmission policy when appropriate 9. The name, mailing address, and telephone number of the State Long-Term Care
Ombudsman The Discharge Plan These rules apply unless the transfer or discharge is an emergency, the patient is transferred to a hospital, or transfer in or out of a Medicare distinct part within the same institution
1. The patient cannot be discharged without a discharge plan developed by the personal physician of the patient or the medical director in conjunction with the nursing director, social worker, or other health care provider.
2. The person in charge of developing the plan shall consider: a. The feasibility of placement near the patient’s relatives b. The acceptability of the placement to the patient and his guardian or
conservator, if any, or his legally liable relative or other responsible party, if known
c. Any other relevant factors which affect the patient’s adjustment to the move
3. The plan shall contain: a. A written evaluation of the effects of the transfer or discharge on the
patient and a statement of the action taken to minimize such effects b. An outline of the care and kinds of services which the patient shall receive
upon transfer or discharge The discharge plan must be presented to the patient’s personal physician (if developed by the medical director) and to the patient and his guardian or conservator, if any, or his legally liable relative or other responsible party, if known, NO LESS THAN 30 DAYS PRIOR TO INVOLUNTARY TRANSFER OR DISCHARGE.

Appeals The Commissioner of Social Services or his designee must hold a hearing no less than 10 but no more than 30 days from the receipt of a request for a hearing to appeal any proposed transfer or discharge. A written decision made by the commissioner or his designee will be made within 60 days of the termination of the hearing or 90 days within the date of the hearing request, which ever is sooner. The patient, his guardian, conservator, legally liable relative or other responsible party shall have an opportunity to examine the contents of the patient’s file maintained by the facility and all documents and records to be used by the commissioner or his designee or the facility at the hearing AT LEAST 3 BUSINESS DAYS, DURING NORMAL BUSINESS HOURS, PRIOR TO THE HEARING. An involuntary discharge shall be stayed pending the decision of the commissioner or his designee If the commissioner or his designee determines that the transfer or discharge is being effected properly, the facility may not transfer or discharge the patient prior to 15 days from the receipt of the decision by the patient and his guardian or conservator, if any, or his legally liable relative or other responsible party, if known Appeals of Emergency Transfer or Discharge A patient who is transferred or discharged on an emergency basis or a patient ho receives notice of such a transfer or discharge may contest the action by requesting a hearing in writing within 10 days of receipt of notice or within 10 days of the transfer or discharge, which ever is later. A hearing shall be held within 7 business days of receipt of the request Residential Home Care Discharge A facility cannot transfer or discharge a resident unless: 1. The transfer or discharge is necessary to meet the resident’s welfare and the resident’s welfare cannot be met in the facility 2. The transfer or discharge is appropriate because the resident’s health has improved sufficiently so the resident no longer needs the services provided by the facility 3. The health or safety of individuals in the facility is endangered 4. The resident has failed, after reasonable and appropriate notice, to pay for a stay or a requested service at the facility 5. The facility ceases to operate Involuntary Transfer or Discharge Resident and, if known, his legally liable relative, guardian, or conservator shall be given a 30 day written notification which includes:
1. The reason for transfer or discharge 2. Notice of the right of the resident to appeal a transfer or discharge by the
facility The facility is responsible for assisting the resident in finding appropriate placement. A discharge plan, prepared by the facility, which indicates the resident’s individual needs, shall accompany the patient. Appeals

A request for a hearing to appeal a transfer or discharge must be filed with the Commissioner of Public Health within 10 days of receipt of the notice of transfer or discharge The hearing shall be held within 7 business days of receipt of such a request A determination must be made within 20 days of the termination of the hearing by the commissioner or their designee Any involuntary transfer or discharge shall be stayed pending a determination by the commissioner or his designee Chronic Disease Hospital Transfer or Discharge A facility shall not transfer or discharge a patient from the facility except: 1. For medical reasons, for the patient’s welfare or the welfare of other patients as documented in the patient’s medical records 2. Or, in the case of a self-pay patient, for nonpayment or arrearage of more than 15 days of the per diem chronic disease hospital room rates for the patient’s stay, except as prohibited by the SSA Involuntary Transfer or Discharge Notice The patient and, if know, the patient’s legally liable relative, guardian or conservator and the patient’s personal physician, if the discharge plan is prepared by the medical director of the chronic disease hospital, shall be given AT LEAST 30 DAYS WRITTEN NOTICE of the proposed action to ensure orderly transfer or discharge. Source: Connecticut Elder Law
-Page Up- -Discharge Planning Main-

Delaware Common Discharge Provisions at a Glance Detailed Discharge Planning Delaware Common Discharge Provision at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
30 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate NO For medical reasons YES It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO
Delaware Detailed Discharge Planning
TITLE 16 Health and Safety Regulatory Provisions Concerning Public Health Chapter 11. Nursing Facilities and Similar Facilities Subchapter II. Rights of Patients § 1121. Patient's rights.
Applies to Nursing and Similar Facilities
Each patient shall receive from the attending physician or the resident physician of the facility complete and current information concerning the patient's diagnosis, treatment and prognosis in terms and language the patient can reasonably be expected to understand, unless medically inadvisable.
The patient or resident shall participate in the planning of the patient's or resident's medical treatment, including attendance at care plan meetings.
No patient or resident shall be transferred or discharged out of a facility except for medical reasons; the patient's or resident's own welfare or the welfare of the other patients; or for nonpayment of justified charges.
If good cause for transferal is reasonably believed to exist, the patient or resident shall be given at least 30 days' advance notice of the proposed action, together with the reasons for the decision, and the patient or resident shall have the opportunity for an impartial hearing to challenge such action if the patient or resident so desires.
In emergency situations such notice need not be given. If a patient or resident is transferred out of a facility to an acute care facility, the facility must accept the patient or resident back into the facility when the resident no longer needs acute care and there is space available in the facility. If no space is available, the resident shall be accepted into the next available bed. Every patient and resident shall have the right to inspect all records pertaining to the patient or resident, upon oral or written request within 24 hours of notice to the facility. Source: DEPARTMENT OF HEALTH AND SOCIAL SERVICES: Division of Long Term Care Residents Protection
-Page Up- -Discharge Planning Main-

District of Columbia Common Discharge Provisions at a Glance Detailed District of Columbia Discharge Planning District of Columbia Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
21 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate YES For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
YES
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

District of Columbia Detailed Discharge Planning
D.C. Code § 44-1003.01 Grounds for involuntary discharge, transfer, or relocation by facility § 44-1003.02. Notice to resident and resident's representative § 44-1003.03. Hearing § 44-1003.04. Discussion and counseling Applies to: NURSING HOMES AND COMMUNITY RESIDENCE FACILITIES A facility can discharge, transfer to another facility, or transfer from one part of facility or room to another if:
1. It is essential to meet the resident’s documented health care needs or to be in accordance with the prescribed level of care 2. It is essential to safeguard that resident or other residents from physical or emotional injury
3. Non payment for maintenance except for: a. No facility that is a District Medicaid provider may discharge, transfer, or relocate a resident on account of his or her conversion from private-pay or Medicare to Medicaid status, or on account of a temporary hospitalization if payment or reimbursement for his or her bed continues to be made available.
b. 42 U.S.C.S. § 1395 et seq. and 42 U.S.C.S. § 1396 et seq. 4. It is essential to meet the facility’s reasonable administrative needs and no practicable alternative is available 5. The facility is closing or officially reducing its licensed capacity
Notice A facility representative shall give the resident and their representative oral and written notice of the reasons for, procedures for contesting, and proposed effective date of the discharge, transfer, or relocation. Notice shall be given at least 21 calendar days before discharge or transfer and at least 07 calendar days before relocation unless:
1. A more immediate discharge, transfer, or relocation is necessitated by resident’s urgent medical needs explicitly stated in the signed, written orders of an attending physician
2. Long-Term Care Ombudsman determines that emergency or other compelling circumstances necessitate a more immediate discharge, transfer, or relocation and the basis for this is documented in the clinical records of the resident
Consent by the resident and representative is only valid if knowingly and voluntarily given at the time the move is proposed The notice must contain:
1. The specific reasons, in detail and not in conclusory language, for the proposed discharge, transfer, or relocation
2. The proposed effective date of the discharge, transfer, or relocation 3. A statement in at least 12-pt type that reads:
"You have a right to challenge this facility's decision to discharge, transfer, or relocate you. If the decision is to discharge you from the facility or to transfer you to another facility and you think you should not have to leave, you or your representative have 7 days from the day you receive this notice to inform the Administrator [Residence Director, if a community residence facility] or a member of the staff that you are requesting a hearing and to complete the enclosed hearing request form and mail it in the preaddressed envelope provided. If you are mailing the hearing request form from the

facility, the day you place it in the facility's outgoing mail or give it to a member of the staff for mailing shall be considered the date of mailing for purposes of the time limit. In all other cases, the postmark date shall be considered the date of mailing. If, instead, the decision is to relocate you within the facility and you think you should not have to move to another room, you or your representative have only 5 days to do the above. "If you or your representative request a hearing, it will be held no later than 5 days after the request is received in the mail, and, in the absence of emergency or other compelling circumstances, you will not be moved before a hearing decision is rendered. If the decision is against you, in the absence of an emergency or other compelling circumstances you will have at least 5 days to prepare for your move if you are being discharge or transferred to another facility, and at least 3 days to prepare for your move if you are being relocated to another room within the facility. "To help you in your move, you will be offered counseling services by the staff, assistance by the District government if you are being discharged or transferred from the facility, and, at your request, additional support from the Long-Term Care Ombudsman program. If you have any questions at all, please do not hesitate to call one of the phone numbers listed below for assistance."
4. A hearing request form, with a postage paid envelope preaddressed to the appropriate District official or agency
5. The name, address, and telephone number of the person charged with the responsibility of supervising the discharge, transfer, or relocation
6. The names, addresses, and telephone numbers of the Long-Term Care Ombudsman program and local legal services organizations
Whenever non-payment is the ground for involuntary discharge or transfer, the resident shall have the right to redeem up to the time that the discharge or transfer is to be effected and, if full payment is made, shall have the right to remain in the facility Hearing The resident, their representative, or Long-Term Care Ombudsman may contest the decision to transfer, discharge or relocate the resident by mailing a written hearing request to the Mayor and notifying the administrator or facility staff of the request Request must be mailed and given within 7 calendar days of receiving notice of proposed discharge or transfer and within 5 calendar days of receiving notice of relocation within the facility Date of mailing shall be the postmarked date unless resident or resident’s representative mails the request from the facility. In that case, the mailing date is the day it is placed in the facility’s outgoing mail or given to a member of the facility staff for mailing. A timely hearing will stay the discharge, transfer, or relocation unless an urgent medical need for discharge, transfer, or relocation develops The major shall hold a hearing at the resident’s facility within 5 calendar days and render a judgment within 7 calendar days after receipt of hearing request The facility holds the burden of proof unless the reason for transfer, discharge, or relocation is a change in the prescribed level of care. If this is the case, the person responsible for prescribing that change shall have the burden of proof. The resident shall have the right to challenge the level of care determination at the hearing

Mayor must find that one of the conditions for discharge, transfer, or relocation has been proven by clear and convincing evidence. If this is found, the resident shall not be:
1. discharged or transferred from the facility before the 22nd calendar day following his or her receipt of notice or the 5th calendar day following the notification of the hearing decision, whichever is later, unless an urgent medical need develops
2. Relocated before the 8th calendar day following receipt of the notice or the 3rd calendar day following notification of the hearing decision, whichever is later, unless an urgent medical need develops
Discussion and counseling Before transfer, discharge, or relocation, a facility representative shall discus the reasons for the move with the resident and their representative and shall answer any questions they must have about the move or the written notice. The discussion shall be summarized in writing, include the names of the individuals involved in the discussion, and be placed in the resident’s clinical record. The facility representative shall strongly recommend and offer to provide counseling services to the resident and their representative before the move. If a hearing has been requested, the staff shall attempt to prepare the resident for moving on 3 or 5 day notice if the hearing decision is not in the resident’s favor. Source: District of Columbia Code
-Page Up- -Discharge Planning Main-

Florida Common Discharge Provisions at a Glance Florida Detailed Discharge Planning
Florida Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
30 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Detailed Florida Discharge Planning
Florida Statutes, Chapter 400, Nursing Homes and Related Health Care Facilities, Part II Nursing Homes (Ss. 400.011-400.334) Applies to Transfers and Discharges Initiated by the Nursing Home Facility Notice of Discharge or Transfer Notice of proposed discharge or transfer must be given to the resident and a family member or the resident’s legal guardian or representative at least 30 days prior to transfer or discharge except:
1. The transfer or discharge is necessary for the resident’s welfare and the resident’s needs cannot be met in the facility, and the circumstances are documented in the resident’s medical records by the resident’s physician
2. The health or safety of other residents or facility employees would be endangered, and the circumstances are documented in the resident’s medical records by the resident’s physician or the medical director if the resident’s physician is not available
Notice must be in writing and contain all information required by state and federal law, rules, or regulations applicable to Medicaid or Medicare cases. The notice shall contain:
1. Means for a resident to request the local long-term care ombudsman council to review the notice and request information or assistance with initiating a fair hearing with the department’s Office of Appeals Hearings.
2. The reason allowed under federal or state law that the resident is being discharged or transferred, with an explanation to support this action
3. The effective date of discharge or transfer and the location to which the resident is being moved
4. The resident’s appeal rights and the procedures for filing an appeal A copy of the notice must be placed in the resident’s clinical record, and a copy must be transmitted to the resident’s legal guardian or representative and to the local ombudsman council within 5 business days after signature by the resident or resident designee. When initiated by nursing home, the administrator or designee must sign the notice of discharge or transfer. If the notice indicates a medical reason for discharge or transfer, it must be signed by the resident’s attending physician or the medical director of the facility or include an attached written order for the discharge or transfer. The notice or the order must be signed by the resident’s physician, medical director, treating physician, nurse practitioner, or physician assistant. Reviews and Hearings A resident of any Medicaid or Medicare certified facility may challenge a decision by the facility to discharge or transfer the resident. The local long-term care ombudsman council must review a request by a resident to review notice of discharge within 7 days after receipt of request.

The nursing home administrator or designee must forward the request for review contained in the notice to the local ombudsman council within 24 hours after such a request is submitted. Failure to forward the request within this time will toll the running of the 30-day advance notice period until the request has been forwarded. A resident is entitled to a fair hearing to challenge a facility’s proposed transfer or discharge and may request the hearing any time within 90 days of the resident’s receipt of the facility’s notice If the hearing is requested within 10 days after receiving the notice of transfer or discharge, the request shall stay the proposed transfer or discharge pending a hearing decision. If the hearing is requested beyond 10 days after receiving the notice of transfer or discharge, the facility may transfer or discharge the resident after 30 days from the date the resident received notice. Initial fair hearing must be completed within 90 days after receipt of request for a hearing An emergency discharge or transfer may be implemented as necessary pursuant to state or federal law during the period of time after the notice is given and before the time a hearing decision is rendered. Notice of this must be given to the resident, the resident’s legal guardian or representative, and the local ombudsman council if a request for review was submitted, by telephone or in person before the transfer or as soon thereafter as practicable. The ombudsman shall conduct review within 24 hours of receipt of request. The resident’s file must be documented to show who was contacted, whether the contact was by telephone or in person, and the date and time of the contact. If the notice is not given in writing, written notice as laid out above must be give the next business day. After receipt of notice, the local ombudsman council may request a private informal conversation with the resident, a family member, or the resident’s legal guardian or designee, to ensure the facility is in accordance with this section. If requested, the local ombudsman shall assist the resident with filing an appeal of the proposed discharge or transfer These persons must be present at all hearings:
1. The resident, or their legal representative or designee 2. The facility administrator, or the legal representative or designee
A representative of the local long-term care ombudsman council may be present at all hearings Hearings shall be conducted by the department’s Office of Appeals Hearings. The office shall notify the facility of a resident’s request for a hearing Burden of Proof – Clear and Convincing Evidence Hearing decision must be rendered within 90 days after receipt of request for hearing If the hearing decision is favorable to the resident, the resident must be readmitted to the facility’s first available bed. The decision of the hearing officer is final and aggrieved parties may appeal the decision to the district court of appeal in the appellate district where the facility is located Source: 2009 Florida Statutes
-Page Up- -Discharge Planning Main-

Georgia Common Discharge Provisions at a Glance Georgia Detailed Discharge Planning Georgia Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO

Georgia Detailed Discharge Planning
Ga. Comp. R. & Regs. r. 290-9-7-.20 Applies to Hospital Inpatients A nursing assessment shall identify patients who are likely to suffer adverse consequences upon discharge in the absence of adequate discharge planning Designated qualified staff shall complete an evaluation of post-hospital needs and shall develop a plan for meeting those needs. The discharge plan shall be revised as needed with changes in the patient's condition. The hospital shall provide education to patients, and their family members or interested persons as necessary or as requested by the patient, to prepare them for the patient's post-hospital care. The hospital shall arrange for the initial implementation of any discharge plan, including, as applicable, any transfer or referral of the patient to appropriate facilities, agencies, or outpatient services for follow-up or ancillary care. The hospital shall be responsible for the transfer of any necessary medical information to other facilities for the purpose of post-hospital care. The hospital shall regularly reassess the discharge planning process to ensure that it is responsive to patients' discharge needs. The hospital shall adopt and enforce a policy requiring annually during influenza season (inclusive of at least October 1st through March 1st) and prior to discharge, any inpatient 65 years of age or older shall be offered vaccinations for the influenza virus and pneumococcal disease unless contraindicated and contingent on availability. Source: Georgia Rules and Regulations for Hospitals
-Page Up- -Discharge Planning Main-

Hawaii Common Discharge Provisions at a Glance Detailed Hawaii Discharge Planning Hawaii Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals YES Applies to Assisted Living Facilities YES: see chapter 90 of code for specific
reasons for transfer Applies to Hospice NO Requires notice to patient prior to discharge
Reasonable Advance Notice
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate NO For medical reasons YES It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES
Detailed Hawaii Discharge Planning
Hawaii Administrative Rules Title 11 Department of Health Chapter 90 Assisted Living §11-90-10 Admission and discharge. (a) The facility shall develop admission policies and procedures which support the principles of dignity and choice. The admissions process shall include completion of or the providing of the following: (1) A service listing which details the services available, the base rates, the services included in the base rate, and the fees for all other additional services. A service listing shall also describe services which the facility does not provide, but will assist to arrange or coordinate; (2) Handbook or house rules which state the assisted living philosophy and clearly define the privileges and responsibilities of the resident and the conditions under which apartment units may be occupied by the residents; (3) A service plan for the resident developed by facility staff with the resident and significant others, specifying care and services to be provided, based on resident needs and choices; (4) A service contract which documents a completed agreement between the resident and the facility, describing services to be provided, rates charged, and conditions under which additional services or fees may be charged; (5) The resident shall be informed of his or her rights, including steps for complaints and appeals upon admission; and (6) Designation of alternative decision-maker or legal representative. (b) The facility shall develop discharge policies and procedures that include, but not be limited to, the following: (1) Residents shall receive a written 14 day notice when: (A) Resident's behavior imposes an imminent danger to self or others; (B) The facility cannot meet the resident's needs with available support services or services are not available; and (C) Resident or responsible person has a documented established pattern in the facility of not abiding by agreements necessary for assisted living; or (2) Residents shall receive a written notice when: (A) The facility has had its license revoked, not renewed, or voluntarily surrendered; or (B) Non-payment of charges by the resident. (3) Residents shall be given the opportunity of an informal conference if requested, in writing, within 10 days of receipt of discharge notice. The purpose of the conference is to determine if a satisfactory resolution can be reached. Participants in the conference may include the facility representative, the resident, and others as designated by the resident, a family member, or all of these individuals. [Eff August 23, 1999] (Auth: HRS §§321-1, 321-9, 321-10, 321-11(10), 321-15.1) (Imp: HRS §§321-9, 321-11(10), 321-15.1) Chapter 94 Skilled Nursing/Intermediate Care Facilities §11-94-14 General policies and practices. (a) There shall be written policies and procedures available to staff, patients, and the public which govern: (1) All services provided by the facility. (2) Admission, transfer, and discharge of patients.

(b) There policies shall insure that: (1) The facility shall not deny admission to any individual on account of race, religion, color, ancestry, or national origin. (2) Only those patients are accepted whose needs can be met by the facility directly or in cooperation with community resources or other providers of care with which it is affiliated or has contracts. (3) As changes occur in a patient's physical or mental condition necessitating a different level of service or care which cannot be adequately provided by the facility, the patients are transferred promptly to a facility capable of providing an appropriate level of care. (4) Except in the case of an emergency, the patient or the patient's guardian, the next of kin, attending physician, and the responsible agency, if any, shall be informed in advance of the transfer or discharge to another facility. §11-94-22 Medical record system. (a) There shall be available sufficient, appropriately qualified staff and necessary supporting personnel to facilitate the accurate processing, checking, indexing, filing, and prompt retrieval of records and record data. (b) If the employee who supervises medical records is not a registered records administrator, or accredited record technician, there shall be regularly scheduled visits by a consultant so qualified who shall provide reports to the administrator. (c) The following information shall be obtained and entered in the patient's record at the time of admission to the facility: (5) Entries describing treatments, medications, tests, and all ancillary services rendered. (e) When a patient is transferred to another facility or discharged, there shall be: (1) Written evidence of the reason. (2) Except in an emergency, documentation to indicate that the patient understood the reason for transfer, or that the guardian and family were notified. (3) A complete summary including current status and care, final diagnosis, and prognosis. §11-94-26 Patients' rights. (a) Written policies regarding the rights and responsibilities of patients during their stay in the facility shall be established and shall be made available to the patient, to any guardian, next of kin, sponsoring agency or representative payee, and to the public. The facility's policies and procedures shall provide that each individual admitted to the facility shall: (5) Be transferred or discharged only for medical reasons, or for their welfare or that of other patients, or for nonpayment for their stay, and be given reasonable advance notice to ensure orderly transfer or discharge; such actions shall be documented in their health record.
-Page Up- -Discharge Planning Main-

Idaho Common Discharge Provisions at a Glance Detailed Idaho Discharge Planning Idaho Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES

Detailed Idaho Discharge Planning
IDAPA 16, Title 03, Chapter 14 16.03.14 - Rules and Minimum Standards for Hospitals In Idaho 200. Governing Body and Administration. Applies to Hospitals There shall be a procedure implemented by hospital administrators to screen each patient for discharge planning needs A qualified person shall be in charge of discharge planning The hospital shall have a transfer agreement with a Medicare and/or Medicaid skilled nursing home Source: Idaho Department of Health and Welfare
-Page Up- -Discharge Planning Main-

Illinois Common Discharge Provisions at a Glance Detailed Discharge Planning Illinois Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
24 hours (Medicare beneficiaries only)
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES (Medicare recipients only)
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES
Detailed Illinois Discharge Planning

Title 77: Public Health, Chapter I: Department of Public Health, Subchapter B: Hospitals and Ambulatory Care Facilities, Part 250 Hospital Licensing Requirements, Section 250.240 Admission and Discharge Applies to Hospitals Hospitals shall have written policies for discharge of all patients who present themselves for care Discharge Plan The discharge plan shall be based on an assessment of the patient's needs by various disciplines responsible for the patient's care. When a patient is discharged to another level of care, the hospital shall ensure that the patient is being transferred to a facility that is capable of meeting the patient's assessed needs.
At least 24 hours prior to discharge from the hospital, each patient who qualifies for the federal Medicare program shall be notified of the discharge. The notification shall be provided by, or at the direction of, a member of the hospital's medical staff. The notification shall include:
The anticipated date and time of discharge.
Written information concerning the patient's right to appeal the discharge pursuant to the federal Medicare program, including the steps to follow to appeal the discharge and the appropriate telephone number to call if the patient intends to appeal the discharge. This written information does not need to be included in the notification, if it has already been provided to the patient. (Section 6.09 of the Act)
The hospital shall develop and implement policies and procedures to provide the notification required this Section. The policies and procedures may provide for waiver of the notification requirement in either or both of the following cases:
When a discharge notice is not feasible due to a short length of stay in the hospital by the patient. The hospital policy shall specify the length of stay when discharge notification will not be considered feasible.
When the patient voluntarily desires to leave the hospital before the expiration of the 24 hour period. (Section 6.09 of the Act)
Source: Illinois Administrative Code
-Page Up- -Discharge Planning Main-

Indiana Common Discharge Provisions at a Glance Detailed Indiana Discharge Planning Indiana Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
30 Days; see code for limitations
Limits reason for transfer or discharge: 1. If necessary for resident’s welfare
and needs cannot be met in the facility YES
2. Resident’s health has improved and he or she no longer needs the services provided by the facility
YES
3. The safety of individuals in the facility are endangered
YES
4. The health of individuals in the facility are endangered
YES
5. The resident has failed to pay after reasonable and appropriate notice given
YES
6. The facility ceases to operate YES 7. For medical reasons NO 8. It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
9. If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES for limitations 1-4
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO
Indiana Detailed Discharge Planning

Article 16.2 Health Facilities; Licensing and Operational Standards Rule 3.1. Comprehensive Care Facilities 410 IAC 16.2-3.1-5 Notification of changes Applies to Comprehensive Care facilities A facility must immediately inform the resident, consult with the resident's physician, and, if known, notify the resident's legal representative or an interested family member when there is a decision to transfer or discharge the resident from the facility Transfer and Discharge Rights When transfer or discharge of a resident is proposed a provision for continuity of care shall be provided by the facility. Health facilities must permit each resident to remain in the facility and not transfer or discharge the resident unless:
1. It is for the resident’s welfare and the resident’s needs can no longer be met in the facility
2. It is appropriate because the resident’s health has improved sufficiently so that the resident no longer needs the services provided by the facility
3. The safety of individuals in the facility is endangered 4. The health of individuals in the facility would otherwise be endangered 5. The resident has failed, after reasonable and appropriate notice, to pay for a stay
at the facility 6. The facility ceases to operate
When the facility proposes a discharge under 1-4, it must be documented in the resident’s clinical records The documentation must be made by the resident’s physician if the transfer or discharge is for 1 or 2, or any physician if the transfer or discharge is for 4. Interfacility Transfer and Discharge Before the transfer or discharge occurs, the facility must: Notify the resident of the transfer or discharge and the reasons for the move in writing and in a language and manner the resident understands. A copy must be placed in the clinical record and copies shall be transmitted to:
1. The resident 2. A family member of the resident if known 3. The resident’s legal representative if known 4. The local long term care ombudsman program (for involuntary relocations
or discharges only) 5. The person or agency responsible for the resident’s placement,
maintenance, and care in the facility 6. In situations where the resident is developmentally disabled, the regional
office of the division of disability, aging, and rehabilitative services, who may assist with placement decisions
7. The resident’s physician when the transfer or discharge is necessary under reasons 3-6 above
Record the reasons in the resident’s clinical record Include in the notice:
1. The reason for transfer for discharge 2. The effective date of transfer or discharge 3. The location to which the resident is transferred or discharged

4. A statement in at least 12-point bold type that reads, “ 5. The name of the director, address, telephone number, and hours of
operation of the division 6. A hearing request form prescribed by the department 7. The name, address, and telephone number of the division and local long
term care ombudsman 8. For facility residents with developmental disabilities or who are mentally
ill, the mailing address and telephone number of the protection and advocacy services commission.
Notice must be given at least 30 days before the resident is transferred or discharged. Notice may be made as soon as practicable before transfer or discharge when: The safety of individuals in the facility would be endangered The health of individuals in the facility would be endangered
The resident’s health improves sufficiently to allow a more immediate transfer or discharge An immediate transfer or discharge is required by the resident’s urgent medical needs A resident has not resided in the facility for 30 days
Source: Indiana Administrative Code
-Page Up- -Discharge Planning Main-


Iowa Common Discharge Provisions at a Glance Detailed Iowa Discharge Planning Iowa Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
YES; 30 Days
Limits reason for transfer or discharge: 1. If necessary for resident’s welfare
and needs cannot be met in the facility YES
2. Resident’s health has improved and he or she no longer needs the services provided by the facility
3. The safety of individuals in the facility are endangered
YES
4. The health of individuals in the facility are endangered
YES
5. The resident has failed to pay after reasonable and appropriate notice given
YES
6. The facility ceases to operate NO 7. For medical reasons YES 8. It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
9. If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Detailed Iowa Discharge Planning Iowa Administrative Code Human Services Department [441] Chapter 81 NURSING FACILITIES/441 — 81.5 (249A) Discharge and transfer. Discharge and transfer. (See subrules 81.13(2)“a” and 81.13(6)“c.”) 81.5(1) Notice. When a public assistance recipient requests transfer or discharge, or another person requests this for the recipient, the administrator shall promptly notify the local office of the department. This shall be done in sufficient time to permit a social service worker to assist in the planning for the transfer or discharge. 81.5(2) Case activity report. A Case Activity Report, Form 470-0042, shall be submitted to the department whenever a Medicaid applicant or recipient enters the facility, changes level of care, or is discharged from the facility. 81.5(3) Plan. The administrator and staff shall assist the resident in planning for transfer or discharge through development of a discharge plan. 81.5(4) Transfer records. When a resident is transferred to another facility, transfer information shall be summarized from the facility’s records in a copy to accompany the resident. This information shall include: a. A transfer form of diagnosis. b. Aid to daily living information. c. Transfer orders. d. Nursing care plan. e. Physician’s orders for care. f. The resident’s personal records. g. When applicable, the personal needs fund record. h. Resident care review team assessment. http://www.legis.state.ia.us/aspx/ACODOCS/DOCS/441.81.5.pdf Inspections and Appeals Department [481] Chapter 57 RESIDENTIAL CARE FACILITIES 481 — 57.13 (135C) Admission, transfer, and discharge. Discharge or transfer. a. Prior notification shall be made to the next of kin, legal representative, attending physician, and sponsoring agency, if any, prior to transfer or discharge of any resident. (III) b. Proper arrangements shall be made by the residential care facility for the welfare of the resident prior to the transfer or discharge in the event of an emergency or inability to reach the next of kin or legal representative. (III) c. The licensee shall not refuse to discharge or transfer a resident when the physician, family, resident, or legal representative requests such transfer or discharge. (II, III) d. Advance notification by telephone will be made to the receiving facility prior to the transfer of any resident. (III) e. When a resident is transferred or discharged, the appropriate record as set forth in 57.16(1) will accompany the resident. (II, III) f. Prior to the transfer or discharge of a resident to another health care facility, arrangements to provide for continuity of care shall be made with the facility to which the resident is being sent. (II, III)

http://www.legis.state.ia.us/aspx/ACODOCS/DOCS/481.57.13.pdf Iowa Administrative Code Inspections and Appeals Department [481] Chapter 58 NURSING FACILITIES 481—57.36 residential care facility Involuntary discharge or transfer 57.36(1) A facility shall not involuntarily discharge or transfer a resident from a facility except: for medical reasons; for the resident’s welfare or that of other residents; for nonpayment for the resident’s stay (as contained in the contract for the resident’s stay), except as prohibited by Title XIX of the Social Security Act, 42 U.S.C. 1396 to 1396k and by reason of action pursuant to Iowa Code chapter 229. (I, II) a. “Medical reasons” for transfer or discharge are based on the resident’s needs and are determined and documented in the resident’s record by the attending physician. Transfer or discharge may be required to provide a different level of care. (II) b. “Welfare” of a resident or that of other residents refers to their social, emotional, or physical well-being. A resident might be transferred or discharged because the resident’s behavior poses a continuing threat to the resident (e.g., suicidal) or to the well-being of other residents or staff (e.g., the resident’s behavior is incompatible with other residents’ needs and rights). Evidence that the resident’s continued presence in the facility would adversely affect the resident’s own welfare or that of other residents shall be made by the administrator or designee and shall be in writing and shall include specific information to support this determination. (II) c. Involuntary transfer or discharge of a resident from a facility shall be preceded by a written notice to the resident or responsible party at least 30 days in advance of the proposed transfer or discharge. The 30-day requirement shall not apply in any of the following instances: (1) If an emergency transfer or discharge is mandated by the resident’s health care needs and is in accord with the written orders and medical justification of the attending physician. Emergency transfers or discharges may also be mandated to protect the health, safety, or well-being of other residents and staff from the resident being transferred. (II) (2) If the transfer or discharge is subsequently agreed to by the resident or the resident’s responsible party, and notification is given to the responsible party, physician, and the person or agency responsible for the resident’s placement, maintenance, and care in the facility. (II) d. The notice required by paragraph “c” shall contain all of the following information: (1) The stated reason for the proposed transfer or discharge. (II) (2) The effective date of the proposed transfer or discharge. (II) (3) A statement in not less than 12-point type (elite), which reads: “You have a right to appeal the facility’s decision to transfer or discharge you. If you think you should not have to leave this facility, you may request a hearing in writing or verbally with the Iowa state department of inspections and appeals (hereinafter referred to as “department”) within seven days after receiving this notice. You have a right to be represented at the hearing by an attorney or any other individual of your choice. If you request a hearing, it will be held no later than 14 days after receipt of your request by the department and you will not be transferred prior to a final decision. Provision may be made for extension of the 14-day requirement upon request to the department of inspections and appeals designee in emergency circumstances. If you lose the hearing, you will not be transferred before the expiration of 30 days following receipt of the original notice of the discharge or transfer, or no sooner than 5 days following final decision of such hearing. To request a hearing or receive further information, call the department at (515)281-4115 or you may write to the department to the attention of: Administrator, Division of Health

Facilities, Department of Inspections and Appeals, Lucas State Office Building, Des Moines, Iowa 50319-0083.” (II) e. A request for a hearing made under http://search.legis.state.ia.us/nxt/gateway.dll/ar/iac/4810___inspections and appeals department __5b481__5d/0570___chapter 57 residential care facilities/_r_4810_0570_0360.xml?f=templates$fn=document-frame.htm$3.0$q=%5Brank, 100 %3A %5Bdomain %3A*%5D%5Bsum %3A 481 57.36 %5D%5D$uq=$x=server$up=157.36(1)“d”(3) shall stay a transfer or discharge pending a hearing or appeal decision. (II) f. The type of hearing shall be determined by a representative of the department. Notice of the date, time, and place of the hearing shall be sent by certified mail or delivered in person to the licensee, resident, responsible party, and Iowa department of elder affairs long-term care ombudsman of record, not later than five full business days after receipt of the request. This notice shall also inform the licensee, resident or responsible party that they have a right to appear at the hearing in person or be represented by their attorneys or other individual. The hearing shall be dismissed if neither party is present or represented at the hearing. If only one party appears or is represented, the hearing shall proceed with one party present. The Iowa department of elder affairs long-term care ombudsman shall have the right to appear at the hearing. g. The hearing shall be heard by a department of inspections and appeals designee pursuant to Iowa Code chapter 17A. (The hearing shall be public unless the resident or representative requests in writing that it be closed.) The licensee or designee shall have the opportunity to present to the representative of the department any oral testimony or written materials to show by a preponderance of the evidence just cause why a transfer or discharge may be made. The resident and responsible party shall also have an opportunity to present to the representative of the department any oral testimony or written material to show just cause why a transfer or discharge should not be made. In a determination as to whether a transfer or discharge is authorized, the burden of proof rests on the party requesting the transfer or discharge. h. Based upon all testimony and material submitted to the representative of the department, the representative shall issue, in accordance with Iowa Code chapter 17A, written findings of fact and conclusions of law and issue a decision and order in respect to the adverse action. This decision shall be mailed by certified mail to the licensee, resident, responsible party, and department of elder affairs long-term care ombudsman within 10 working days after the hearing has been concluded. The representative shall have the power to issue fines and citations against the facility in appropriate circumstances.
A request for review of a proposed decision in which the department is the final decision maker shall be made within 15 days of issuance of the proposed decision, unless otherwise provided by statute. Requests shall be mailed or delivered by either party to the Director, Department of Inspections and Appeals, Lucas State Office Building, Des Moines, Iowa 50319-0083. Failure to request review will preclude judicial review unless the department reviews a proposed decision upon its own motion within 15 days of the issuance of the decision.
i.A copy of the notice required by paragraph “c” shall be personally delivered to the resident and a copy placed in the resident’s record. A copy shall also be transmitted to the department, the resident’s responsible party, physician, the person or agency responsible for the resident’s placement, maintenance, and care in the facility, and the department of elder affairs long-term care ombudsman.

j. If nonpayment is the basis for involuntary transfer or discharge, the resident shall have the right to make full payment up to the date that the discharge or transfer is to be made and then shall have the right to remain in the facility. (II) k. The involuntary transfer or discharge shall be discussed with the resident, the resident’s responsible party, and the person or agency responsible for the resident’s placement, maintenance, and care in the facility within 48 hours after notice of discharge has been received. The explanation and discussion of the reasons for involuntary transfer or discharge shall be given by the facility administrator or other appropriate facility representative as the administrator’s designee. The content of the discussion and explanation shall be summarized in writing and shall include the names of the individuals involved in the discussions and made a part of the resident’s record. (II) l. The resident shall receive counseling services before (by the sending facility) and after (by the receiving facility) the involuntary transfer to minimize the possible adverse effects of the involuntary transfer. Counseling shall be documented in the resident’s record. (II) (1) Counseling shall be provided by a qualified individual who meets one of the following criteria:
1. Has a bachelor’s or master’s degree in social work from an accredited college. (II) 2. Is a graduate of an accredited four-year college and has had at least one year of
full-time paid employment in a social work capacity with a public or private agency. (II)
3. Has been employed in a social work capacity for a minimum of four years in a public or private agency. (II)
4. Is a licensed psychologist or psychiatrist. (II) 5. Is any other person of the resident’s choice. (II)
(2) The facility shall develop a plan to provide for the orderly and safe transfer or discharge of each resident to be discharged or transferred. (II) (3) The receiving health care facility of a resident involuntarily discharged or transferred shall immediately formulate and implement a plan of care which takes into account possible adverse effects the transfer may cause. (II) m. In the case of an emergency transfer or discharge as outlined in http://search.legis.state.ia.us/nxt/gateway.dll/ar/iac/4810___inspections and appeals department __5b481__5d/0570___chapter 57 residential care facilities/_r_4810_0570_0360.xml?f=templates$fn=document-frame.htm$3.0$q=%5Brank, 100 %3A %5Bdomain %3A*%5D%5Bsum %3A 481 57.36 %5D%5D$uq=$x=server$up=157.36(1)“c”(1), the resident must still be given a written notice prior to or within 48 hours following transfer or discharge. A copy of this notice must be placed in the resident’s file and it must contain all the information required by subparagraphs (1) and (2) of http://search.legis.state.ia.us/nxt/gateway.dll/ar/iac/4810___inspections and appeals department __5b481__5d/0570___chapter 57 residential care facilities/_r_4810_0570_0360.xml?f=templates$fn=document-frame.htm$3.0$q=%5Brank, 100 %3A %5Bdomain %3A*%5D%5Bsum %3A 481 57.36 %5D%5D$uq=$x=server$up=157.36(1)“d.” In addition, the notice must contain a statement in not less than 12-point type (elite), which reads: “You have a right to appeal the facility’s decision to transfer or discharge you on an emergency basis. If you think you should not have to leave this facility, you may request a hearing in writing or verbally with the Iowa state department of inspections and appeals within 7 days after receiving this notice. If you request a hearing, it will be held no later than 14 days after receipt of your request by the department. You may be transferred or discharged before the hearing is held or before a final decision is rendered. If you win the hearing, you have

the right to be transferred back into the facility. To request a hearing or receive further information, call the department at (515)281-4115 or you may write to the department to the attention of: Administrator, Division of Health Facilities, Department of Inspections and Appeals, Lucas State Office Building, Des Moines, Iowa 50319-0083.” A hearing requested pursuant to this subrule shall be held in accordance with paragraphs “f,” “g,” and “h.” (II) n. Residents shall not have the right to a hearing to contest an involuntary discharge or transfer resulting from the revocation of the facility’s license by the department of inspections and appeals. In the case of a facility voluntarily closing, a period of 30 days must be allowed for an orderly transfer of residents to other facilities. http://www.legis.state.ia.us/aspx/ACODOCS/DOCS/481.57.36.pdf 57.36(2) Intrafacility transfer: a. Residents shall not be relocated from room to room within a licensed health care facility arbitrarily. (I, II) Involuntary relocation may occur only in the following situations, and the situation shall be documented in the resident’s record. (1) Incompatibility with or disturbing to other roommates, as documented in the resident’s record. (2) For the welfare of the resident or other residents of the facility. (3) For medical, nursing or psychosocial reasons, as documented in the resident’s record, as judged by the attending physician, nurse or social worker in the case of a facility which groups residents by medical, nursing or psychosocial needs. (4) To allow a new admission to the facility which would otherwise not be possible due to separation of roommates by sex. (5) In the case of a resident whose source of payment was previously private, but who now is eligible for Title XIX assistance, the resident may be transferred from a private room to a semiprivate room or from one semiprivate room to another. (6) Reasonable and necessary administrative decisions regarding the use and functioning of the building. b. Unreasonable and unjustified reasons for changing a resident’s room without the concurrence of the resident or responsible party include: (1) Change from private pay status to Title XIX, except as outlined in http://search.legis.state.ia.us/nxt/gateway.dll/ar/iac/4810___inspections and appeals department __5b481__5d/0570___chapter 57 residential care facilities/_r_4810_0570_0360.xml?f=templates$fn=document-frame.htm$3.0$q=%5Brank, 100 %3A %5Bdomain %3A*%5D%5Bsum %3A 481 57.36 %5D%5D$uq=$x=server$up=157.36(2)“a”(5). (II) (2) As punishment or behavior modification (except as specified in http://search.legis.state.ia.us/nxt/gateway.dll/ar/iac/4810___inspections and appeals department __5b481__5d/0570___chapter 57 residential care facilities/_r_4810_0570_0360.xml?f=templates$fn=document-frame.htm$3.0$q=%5Brank, 100 %3A %5Bdomain %3A*%5D%5Bsum %3A 481 57.36 %5D%5D$uq=$x=server$up=157.36(2)“a”(1)). (II) (3) Discrimination on the basis of race or religion. (II) c. If intrafacility relocation is necessary for reasons outlined in paragraph “a,” the resident shall be notified at least 48 hours prior to the transfer and the reason therefor shall be explained. The responsible party shall be notified as soon as possible. The notification shall be documented in the resident’s record and signed by the resident or responsible party. (II) d. If emergency relocation is required to protect the safety or health of the resident or other residents, the notification requirements may be waived. The conditions of the emergency shall be documented. The family or responsible party shall be notified

immediately, or as soon as possible, of the condition requiring emergency relocation and the notification shall be documented. (II) 58.12(2) Discharge or transfer. a. Prior notification shall be made to the next of kin, legal representative, attending physician, and sponsoring agency, if any, prior to transfer or discharge of any resident. (III) b. Proper arrangements shall be made by the nursing facility for the welfare of the resident prior to transfer or discharge in the event of an emergency or inability to reach the next of kin or legal representative. (III) c. The licensee shall not refuse to discharge or transfer a resident when the physician, family, resident, or legal representative requests such a discharge or transfer. (II, III) d. Advance notification by telephone will be made to the receiving facility prior to the transfer of any resident. (III) e. When a resident is transferred or discharged, the appropriate record as set forth in 58.15(2)“k” of these rules will accompany the resident. (II, III) f. Prior to the transfer or discharge of a resident to another health care facility, arrangements to provide for continuity of care shall be made with the facility to which the resident is being sent. (II, III) Source: http://www.legis.state.ia.us/aspx/ACODOCS/DOCS/481.58.12.pdf 58.15 (135C) Records. h. Nurse’s record including: (3) Discharge or transfer notes including time and mode of transportation; resident’s general condition; instructions given to resident or legal representative; list of medications and disposition; and completion of transfer form for continuity of care; (II, III) k. Transfer form. (1) The transfer form shall include identification data from the admission record, name of transferring institution, name of receiving institution, and date of transfer; (III) (2) The nurse’s report shall include resident attitudes, behavior, interests, functional abilities (activities of daily living), unusual treatments, nursing care, problems, likes and dislikes, nutrition, current medications (when last given), and condition on transfer; (III) (3) The physician’s report shall include reason for transfer, medications, treatment, diet, activities, significant laboratory and X-ray findings, and diagnosis and prognosis; (III) Source: http://www.legis.state.ia.us/aspx/ACODOCS/DOCS/481.58.15.pdf 58.40 Involuntary discharge or transfer. Source: http://www.legis.state.ia.us/aspx/ACODOCS/DOCS/481.58.40.pdf
-Page Up- -Discharge Planning Main-

Kansas Common Discharge Provisions at a Glance Detailed Kansas Discharge Planning Kansas Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
30 Days; see code for limitations
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate YES For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
YES; when applicable
Discharge plan/reasons for discharge must be documented in patient’s record
YES; when discharge is involuntary
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES
Detailed Kansas Discharge Planning
Agency 26 Kansas Department on Aging Article 39. Adult Care Homes K.A.R. § 26-39-102 (2009) Applies to Adult Care Homes A patient in an adult care home cannot be discharged or transferred unless the administrator or operator determines one of the following:
1. It is necessary for the patient’s welfare, and his needs cannot be met in the current home
2. The safety of other individuals at the home is endangered 3. The health of other individuals at the home is endangered 4. The resident, after reasonable and appropriate notice, has failed to pay 5. The home ceases to operate
Before involuntary discharge or transfer, the administrator or operator shall notify the resident, the resident’s legal representative, and if known, a designated family member of the transfer or discharge and the reasons
1. The notice must be provided at least 30 days before discharge or transfer, unless a. Safety of others at the home would be endangered, or b. The resident’s urgent medical needs require immediate transfer
2. The notice shall include: a. Reason for transfer or discharge b. Effective date of transfer or discharge c. The address and phone number of the complaint program of the Kansas
Department on Aging where a complaint can be registered d. The address and phone number of the state long-term-care ombudsman,
and e. For residents who have developmental disabilities or are mentally ill, the
address and telephone number of the Kansas advocacy and protection organization
When there is involuntary discharge or transfer, the resident’s physician shall record the rationale for transfer or discharge in the resident’s clinical record. The administrator or operator or designee shall provide adequate preparation and orientation to each resident before discharge to ensure a safe and orderly transfer and discharge from the home. The administrator or operator or designee shall ensure the development of a discharge plan, with the involvement of the resident, the resident’s legal representative and designated family when applicable. (Note: Could not find statute for general hospital discharge—only adult care homes and for mentally ill patients) Source: Kansas Statute Table of Contents
-Page Up- -Discharge Planning Main-

Kentucky Common Discharge Provisions at a Glance Detailed Kentucky Discharge Planning Kentucky Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
30 days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
YES
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate YES For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Detailed Kentucky Discharge Planning Kentucky Administrative Regulations Title 900 Cabinet for Health and Family Services Chapter 2 Long-Term Care 900 KAR 2:050. Transfer and discharge rights. Applies to Long-Term Care State is required to have a fair and impartial decision-making process for appeals related to involuntary discharge and transfer. (Per 42 CFR 483.12.) Facilities must permit each resident to remain at the facility, and not transfer or discharge him from the facility unless:
1. The transfer or discharge is necessary for the resident’s welfare and the resident’s needs cannot be met at the facility; or
2. The resident’s health has improved sufficiently so the resident no longer needs the services provided by the facility; or
3. The health or safety of individuals in the facility is endangered; or 4. The resident, after reasonable and appropriate notice, has failed to pay; or 5. The facility ceases to operate
Before transfer or discharge, the reasons for the transfer or discharge must be noted in the resident’s clinical record. Notice of transfer or discharge shall be made by facility at least thirty days before the resident is discharged or transferred. Notice can be made as soon as practicable before transfer or discharge if:
1. Immediate transfer or discharge is required by resident’s urgent medical needs; or 2. The resident’s health improves sufficiently to allow a more immediate transfer or
discharge; or 3. The health or safety of individuals in the facility would be endangered; or 4. The resident has not resided in the facility for thirty days.
Notice shall include:
1. Reason for transfer or discharge; 2. The effective date; 3. The location to which the resident is transferred or discharged; 4. A statement that the resident has the right to appeal the action to the client; 5. The name, address and phone number of the state long-term-care ombudsman and 6. For nursing facility residents with developmental disabilities, or who are mentally
ill, the mailing address and telephone number of the Department of Public Advocacy.
Facility must provide sufficient preparation and orientation to residents to ensure safe and orderly transfer or discharge from the facility. Before a facility transfers a resident to a hospital or allows a resident to go on therapeutic leave, the facility shall provide information to the resident and a family member or legal representative that specifies:
1. For residents receiving or who have an application pending for Medicaid, that if available under the Medicaid state plan and provider agreement, bed-hold days shall be requested and the time period to the bed-hold policy under the Medicaid

state plan during which the resident is permitted to return and resume residence in the facility;
2. The facility's policies regarding bed-hold periods; and 3. For residents who do not receive or do not have an application pending for
Medicaid, the facility's established policy governing readmission. At the time of transfer to a hospital or for therapeutic leave, facility shall provide written notice to the resident and a family member or legal representative, which specifies the duration of the bed-hold policy. Facility shall establish and follow a written policy under which a resident whose hospitalization or therapeutic leave exceeds the bed-hold period under the Medicaid state plan, is notified and readmitted to the facility immediately upon the first availability of a bed in a semiprivate room if the resident:
1. Chooses to be readmitted; and 2. Requires the services provided by the facility; and 3. Is eligible for Medicaid nursing facility services and the facility is certified to
participate in Title XVIII or Title XIX of the Social Security Act. A facility must establish and maintain identical policies and practices regarding transfer, discharge, and the provision of service under the Medicaid state plan for all individuals regardless of source of payment. Residents may appeal any discharge. Residents may appeal a transfer when he is transferred from:
1. A certified bed into a noncertified bed; or 2. A bed in a certified entity to a bed in an entity which is certified as a different
provider. Residents have no appeal rights when moved from a certified bed to another certified bed of the same certification in the same facility. A resident, or any person acting on behalf of the resident, may request that the cabinet review any proposed transfer or discharge. The cabinet shall investigate this transfer or discharge to ascertain whether there has been a violation of the resident's transfer or discharge rights. A resident may appeal any discharge or appealable transfer to the cabinet. The resident must inform the cabinet in writing of his intent to appeal within fifteen days from the resident's receipt of notice of the facility's intent to transfer or discharge. Hearing shall occur within thirty days (900 KAR 2:060). Title 902 Cabinet for Health and Family Services Department for Public Health Chapter 20 Health Services and Facilities, Section 26 902 KAR 20:026. Operations and services; skilled nursing facilities. The facility shall have a discharge planning program to assure the continuity of care for patients being transferred to another health care facility or being discharged to the home.

The facility shall have written transfer procedures and agreements for the transfer of patients to other health care facilities, which can provide a level of inpatient care not provided by the facility.
Any facility which does not have a transfer agreement in effect but which documents a good faith attempt to enter into such an agreement shall be considered to be in compliance with the licensure requirement.
The transfer procedures and agreements shall specify the responsibilities each institution assumes in the transfer of patients, shall establish responsibility for notifying the other institution promptly of the impending transfer of a patient, and shall arrange for appropriate and safe transportation.
When the patient's condition exceeds the scope of services of the facility, the patient, upon physician's orders (except in cases of emergency), shall be transferred promptly to an appropriate level of care. The procedures and agreements shall provide for the transfer of personal effects, particularly money and valuables, and for the transfer of information related to these items. When a transfer is to another level of care within the facility, the complete patient record or a current summary thereof shall be transferred with the patient. If the patient is transferred to another health care facility or home to be cared for by a home health agency, a transfer form shall accompany the patient.
The transfer form shall include at least the following: Physician's orders (if available), Current information relative to diagnosis with history of problems requiring special care, A summary of the course of prior treatment, special supplies or equipment needed for patient care, and Pertinent social information on the patient and his family. Except in an emergency, the patient, his next of kin, or responsible person if any, and the attending physician shall be consulted in advance of the transfer or discharge of any patient. Source: Kentucky Administrative Regulations: Transfer and Discharge Rights
-Page Up- -Discharge Planning Main-

Louisiana Common Discharge Provisions at a Glance Detailed Louisiana Discharge Planning Louisiana Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
30 Days; limitations for non-certified facilities
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
YES
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate YES For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO
Detailed Louisiana Discharge Planning
Title 40- Public Health and Safety

§2010.8. Residents' bill of rights Applies to Nursing Homes Each resident has the right to
Be adequately informed of his medical condition and proposed treatment, unless otherwise indicated by the resident's physician;
Participate in the planning of all medical treatment, including the right to refuse medication and treatment, unless otherwise indicated by the resident's physician; and
Be informed of the consequences of such actions. Each resident has the right to receive adequate and appropriate health care and protective and support services, including services consistent with the resident care plan, with established and recognized practice standards within the community, and with rules promulgated by the Department of Health and Hospitals. Each resident has the right to be transferred or discharged only if
1. Necessary for his welfare and if his needs cannot be met in the facility; 2. His health has improved sufficiently so that he no longer needs the services
provided by the facility; 3. The safety of individuals in the facility is endangered; 4. The health of individuals in the facility would otherwise be endangered; 5. He has failed after reasonable and appropriate notice to pay or have paid for a stay
at the facility; or 6. The facility ceases to operate.
Both the resident and his legal representative or interested family member, if known and available, have the right to be notified in writing in a language and manner they understand of the transfer and discharge.
1. The notice must be given no less than thirty days in advance of the proposed action, except that the notice may be given as soon as is practicable prior to the action in the case of an emergency.
2. In facilities not certified to provide services under Medicare or Medicaid, the advance notice period may be shortened to fifteen days for nonpayment of a bill for a stay at the facility.
The resident or his legal representative or interested family member, if known and available, has the right to appeal any transfer or discharge to the Department of Health and Hospitals, which shall provide a fair hearing in all such appeals. The facility must ensure that the transfer or discharge is effectuated in a safe and orderly manner. The resident and his legal representative or interested family member, if known and available, shall be consulted in choosing another facility if facility placement is required. Each resident has the right to have any significant change in his health status immediately reported to him and his legal representative or interested family member, if known and available, as soon as such a change is known to the home's staff. Source: Louisiana Public Health and Safety
-Page Up- -Discharge Planning Main-

Maine Common Discharge Provisions at a Glance Maine Detailed Discharge Planning Maine Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES

Maine Detailed Discharge Planning
Maine State Agency Rules 10 144 Chapter 110 Regulations Governing the Licensing and Functioning of Skilled Nursing Facilities and Nursing Facilities Chapter 5 Facility Policies Applies to Skilled Nursing and Nursing Facilities Each facility is required to have written policies providing for prevention of:
1. Transfer of a resident from one part of a facility to another, except from a private room, solely because of Medicaid status, and
2. Discharge of a patient solely because of Medicaid status Source: Maine Department of Health and Human Services: Facility Policies
-Page Up- -Discharge Planning Main-
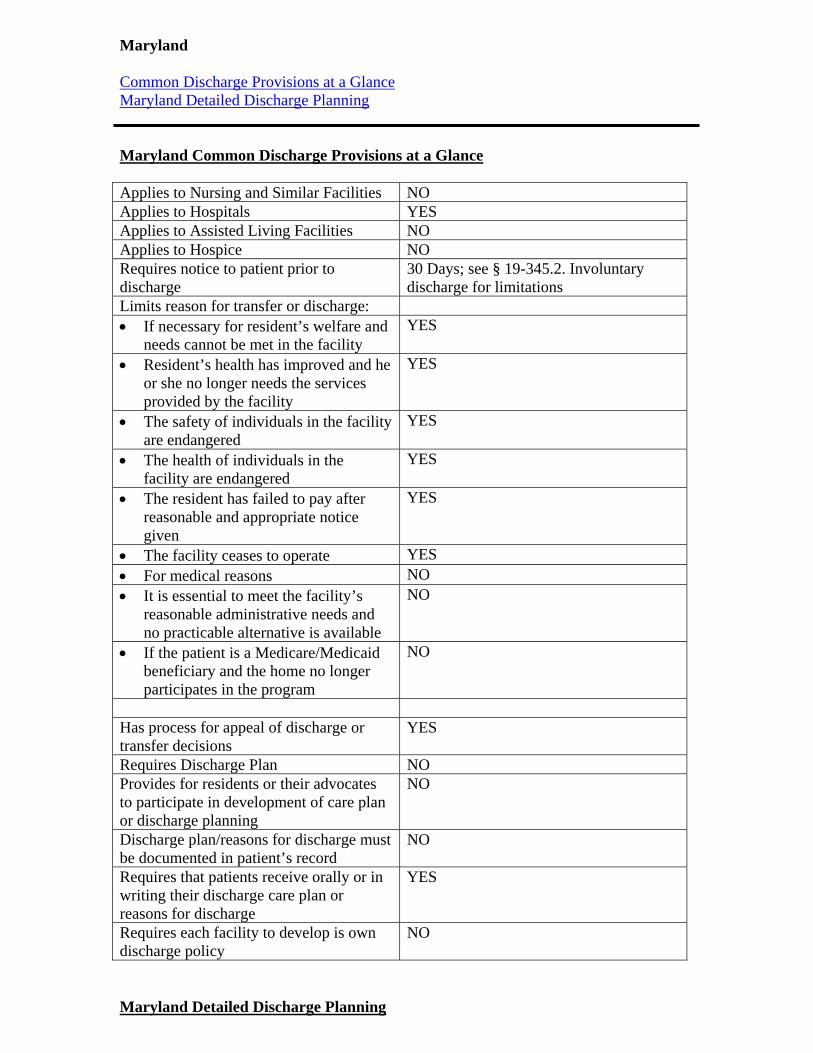
Maryland Common Discharge Provisions at a Glance Maryland Detailed Discharge Planning Maryland Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
30 Days; see § 19-345.2. Involuntary discharge for limitations
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
YES
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate YES For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO
Maryland Detailed Discharge Planning

MD Code-Health General Title 19 Health Facilities Subtitle 3 Hospitals and Related Institutions Part IV Rights of Individuals §19-345 Transfer or Discharge of Resident Applies to hospitals and related institutions Resident cannot be involuntarily discharged or transferred unless:
1. The transfer or discharge is necessary for the resident’s welfare and the resident’s needs cannot be met at the facility; or
2. The resident’s health has improved sufficiently so the resident no longer needs the services provided by the facility; or
3. The health or safety of individuals in the facility is endangered; or 4. The resident, after reasonable and appropriate notice, has failed to pay; or 5. The facility ceases to operate.
A Medicaid certified facility may not:
1. Include in the admission contract of a resident any requirement that, to stay at the facility, the resident will be required to pay for any period of time or amount of money as a private pay resident for any period when the resident is eligible for Medicaid benefits; or
2. Transfer or discharge a resident involuntarily because the resident is a Medicaid benefits recipient.
§19-345.1 Notice of Transfer or Discharge Facilities shall provide the resident with written notice of any proposed discharge or transfer and the opportunity for a hearing. The Department of Health shall provide to each facility a standardized form that provides, in clear and simple language, at least the following information:
1. Notice of the intended discharge or transfer of the resident; 2. Each reason for the discharge or transfer; 3. The right of the resident to request a hearing; 4. The right of the resident to consult with any lawyer the resident chooses; 5. The availability of the services of the Legal Aid Bureau, the Older American Act
Senior Legal Assistance Programs, and other agencies that may provide assistance to individuals who need legal counsel; and
6. The availability of the Department of Aging and local Office on Aging Long-Term Care Ombudsman to assist the resident.
At least thirty days before the facility involuntarily discharges or transfers a resident, the facility shall provide written notice to the resident; the next of kin, guardian, or any other individual known to have acted as the individual’s representative, if any; the Long-Term Care Ombudsman; and the Department of Health.
1. Thirty days’ notice is not required if: An emergency exists and the health or safety of the resident or other residents would be placed in imminent and serious jeopardy if the resident were not transferred or discharged from the facility as soon as possible; or The resident has not resided in the facility for thirty days.

§ 19-345.2. Involuntary discharge A facility may not involuntarily discharge or transfer a resident unless, within 48 hours before the discharge or transfer, the facility has provided or obtained:
1. A comprehensive medical assessment and evaluation of the resident, including a physical examination, that is documented in the resident's medical record;
2. A post discharge plan of care for the resident that is developed, if possible, with the participation of the resident's next of kin, guardian, or legal representative; and
3. Written documentation from the resident's attending physician indicating that the transfer or discharge is in accordance with the post discharge plan of care and is not contraindicated by the resident's medical condition; and
The facility must also provide information to the resident concerning the resident's rights to make decisions concerning health care, including:
1. The right to accept or refuse medical treatment; 2. The right to make an advance directive, including the right to make a living will
and the right to appoint an agent to make health care decisions; and 3. The right to revoke an advance directive.
At the time of transfer or discharge, the facility shall provide the resident or the resident's next of kin, guardian, or legal representative with:
1. A written statement of the medical assessment and evaluation and post discharge plan of care;
2. A written statement itemizing the medications currently being taken by the resident;
3. At least a 3-day supply of the medications currently being taken by the resident (if permitted by law);
4. The information necessary to assist the resident, the resident's next of kin, or legal representative in obtaining additional prescriptions for necessary medication through consultation with the resident's treating physician; and
5. A written statement containing the date, time, method, mode, and destination of discharge.
A facility may not discharge or transfer a resident unless the resident is capable of and has consented in writing to the discharge or transfer, unless the discharge or transfer:
1. Is in accordance with a post discharge plan of care developed; and 2. Is to a safe and secure environment where the resident will be under the care of:
a. Another licensed, certified, or registered care provider; or b. Another person who has agreed in writing to provide a safe and secure
environment. A facility that is certified as a continuing care provider is not subject to these provisions if:
1. The facility transfers a resident to a lesser level of care within the same facility in accordance with a contractual agreement between the facility and the resident; and the transfer is approved by the attending physician.
Sources: Laws of Maryland: 19-345
Laws of Maryland: 19-345.1
Laws of Maryland: 19-345.2
-Page Up- -Discharge Planning Main-

Massachusetts Common Discharge Provisions at a Glance Massachusetts Detailed Discharge Planning Massachusetts Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES; Medicare beneficiaries only Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
24 hours
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Massachusetts Detailed Discharge Planning
Part I. Administration of the Government Title XVI. Public Health Chapter 111. Public Health Section 51D. Discrimination by acute hospitals against Medicare beneficiaries; discharge planning Applies to Medicare beneficiaries in acute hospitals No acute hospital shall impose any discriminatory restrictions or conditions relating to admission, availability of services, treatment, transfer or discharge with respect to any patient because that patient is a Medicare beneficiary. Each acute care hospital is required, to create for each Medicare patient determined to need assistance with post-hospital care, a written comprehensive, individualized, discharge plan consistent with medical discharge orders and identified patient needs.
Plan shall be developed with the participation of appropriate health care professionals, the Medicare patient and, as appropriate, the patient’s family or representative.
The discharge plan shall be given to the patient or the patient’s representative at least twenty-four hours prior to discharge, except where such a requirement is not feasible due to a short length of stay.
If the plan is revised due to the medical needs of the patient or due to a space becoming available in an appropriate institutional setting, the twenty-four hour requirement shall not apply to the amended plan.
The discharge plan shall include:
1. Identification of the post-hospital services needed by the patient, including home health and homemaker services, and of the post-hospital social needs of the patient, as determined in accordance with procedures set forth by the department;
2. The services that have been arranged for the patient; 3. The names, addresses, and telephone numbers of service providers; 4. The service schedule as requested by the hospital; 5. Medications prescribed and instructions for their use or verification that such
information was provided separately; and 6. Scheduled follow-up medical appointments or verification that such information
was provided separately. Each hospital shall have a clear, concise front page on the discharge plan, which front page shall be written in large print and understandable language. The front page shall contain at least the following:
1. The name and telephone number of the hospital discharge planning coordinator to be contacted in the event the patient has any problems with post-hospital services after said patient leaves the hospital;
2. A notice that, in the event the patient or the patient’s representative does not agree with the discharge plan, the discharge planning coordinator and the patient’s physician shall meet with the patient or the patient’s representative in an effort to develop a plan that is acceptable to the patient;
3. A notice, including the advocacy office telephone number, that, if an acceptable resolution is not reached as a result of the meeting, the patient or the patient’s

representative may file a request for review of the discharge plan with the advocacy office;
4. A notice that signing the discharge plan does not necessarily indicate approval of the plan and does not preclude the right to request a meeting or a review; and
5. A signature line for the patient or the patient’s representative acknowledging participation in the development of the discharge plan and receipt of a copy of said plan.
If the patient or the patient’s representative does not sign the plan, the reason for not signing shall be noted on the plan. A signed or noted copy of the plan shall be retained in the patient’s medical record. The patient’s medical record shall also document that the plan was communicated orally to the patient or to the patient’s representative. No hospital may discharge a Medicare patient without the patient or patient’s representative having received, read and signed the front page of the discharge plan or upon decision of the advocacy office. If a discharge plan cannot be agreed upon as a result of the meeting of the patient or the patient’s representative, the discharge planning coordinator and the patient’s physician, the patient or the patient’s representative shall have the right to file a request for a review of the discharge plan with the department’s advocacy office.
The hospital also shall have the right to file a request for a review of discharge. A request for review shall be made with the advocacy office not later than noon of the first working day after the date the patient or the patient’s representative receives the written discharge plan.
The hospital shall deliver to the advocacy office the records required to review the discharge plan by the close of such working day.
The advocacy office shall either approve or disapprove the discharge plan within one working day of receiving the request for review and the hospital records.
If the advocacy office approves the discharge plan, discharge shall occur pursuant to the approved plan by noon of the day following notification of the advocacy office’s decision, unless hospital and patient agree otherwise. If the advocacy office does not approve the discharge plan, said office shall state the problems needing correction, and the hospital shall not charge the Medicare patient for inpatient hospital services until an alternative plan is developed to resolve the problems set forth by the advocacy office. If a timely request for review has been filed with the advocacy office, the hospital shall not charge the Medicare patient for inpatient hospital services furnished before noon of the day after said patient is notified by telephone or otherwise of the advocacy office’s decision.
If notice is made by telephone, the notice shall be made to both parties to the review and shall be followed by written notice as soon as possible.
No patient shall be discharged or transferred without a physician’s order, except where such patient leaves against medical advice.
No patient shall be discharged until the hospital has made all appropriate contacts to initiate the provisions for aftercare services.
A Medicare patient treated at the emergency room of an acute care hospital shall be provided with a discharge plan in accordance with the requirements of this section, with

the exception of the right to request a review of such discharge plan by the advocacy office prior to such discharge. Source: General Laws of Massachusetts
-Page Up- -Discharge Planning Main-

Michigan Common Discharge Provisions at a Glance Michigan Detailed Discharge Planning Michigan Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice YES Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES

Michigan Detailed Discharge Planning
Chapter 333 Health Public Health Code Article 17. Facilities and Agencies Part 201. General Provisions MCLS § 333.20201 (2009) Applies to all health facilities or agencies that provide services directly to patients or residents and are licensed in Michigan. Each facility must adopt a policy describing the rights and responsibilities of patients or residents admitted to the health facility or agency.
The policy shall be posted at a public place in the health facility or agency and shall be provided to each member of the health facility or agency staff.
The policy shall include, at minimum that a patient is: Entitled to know who is responsible for and who is providing his or her direct care, Entitled to receive information concerning his or her continuing health needs and alternatives for meeting those needs, and Entitled to be involved in his or her discharge planning, if appropriate.
Sources: Michigan Public Health Code
-Page Up- -Discharge Planning Main-

Minnesota Common Discharge Provisions at a Glance Minnesota Detailed Discharge Planning Minnesota Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO

Minnesota Detailed Discharge Planning
Chapter 144A Nursing Homes and Home Care Minn. Stat. § 144A.135 (2009) Applies to Nursing Homes and Home Care The Health Commissioner is required to establish an appeals hearing process for transfers or discharge of residents by nursing homes or boarding care homes licensed by the state. To appeal the discharge or transfer, or notification of an intended discharge or transfer, a resident or the resident's representative must request a hearing in writing no later than 30 days after receiving written notice, which conforms to state and federal law, of the intended discharge or transfer.
Hearings will be held no later than 14 days after receipt of the request for hearing, unless impracticable to do so, or if the parties agree otherwise.
Hearings will be held in the facility in which the resident resides, unless impracticable or the parties agree otherwise.
A resident who timely appeals a notice of discharge or transfer may not be discharged or transferred until the appeal has been resolved.
If the resident is required to be hospitalized for medical necessity before resolution of the appeal, the facility shall readmit the resident, unless the resident's attending physician documents, in writing, why the resident's specific health care needs cannot be met in the facility.
Residents also have the right to request or receive assistance from the Office of Ombudsman for Long-Term Care or the Office of Health Facility Complaints with respect to an intended discharge or transfer. Sources: 2009 Minnesota Statutes
-Page Up- -Discharge Planning Main-

Missouri Common Discharge Provisions at a Glance Missouri Detailed Discharge Planning Missouri Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice YES Requires notice to patient prior to discharge
30 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate NO For medical reasons YES It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO

Missouri Detailed Discharge Planning
§ 198.088. Facilities to establish policies and procedures, scope, content -- rights of residents -- complaint – procedure Applies to all Health Facilities Residents can be transferred to a hospital, skilled nursing facility or other appropriate facility when necessary service or car cannot be adequately provided by the facility.
Except in the case of an emergency, the resident, his next of kin, attending physician, and the responsible agency, if any, will be consulted at least thirty days in advance of the transfer or discharge, and
Casework services or other means will be utilized to assure that adequate arrangements exist for meeting his needs through other resources.
A resident may be transferred or discharged only for medical reasons or for his welfare or that of other residents, or for nonpayment for his stay.
No resident may be discharged without notice, provided in writing 30 days in advance of his discharge, of his right to a hearing and an opportunity to be heard on the issue of whether his immediate discharge is necessary.
In emergency discharges a written notice of discharge and right to a hearing shall be given as soon as practicable and an expedited hearing shall be held upon request of the resident, next of kin, legal guardian, or nursing facility Sources: Missouri Discharge Planning
-Page Up- -Discharge Planning Main-

Montana Common Discharge Provisions at a Glance Montana Detailed Discharge Planning Montana Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES (Medicare and Medicaid facilities
only) Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
21 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO
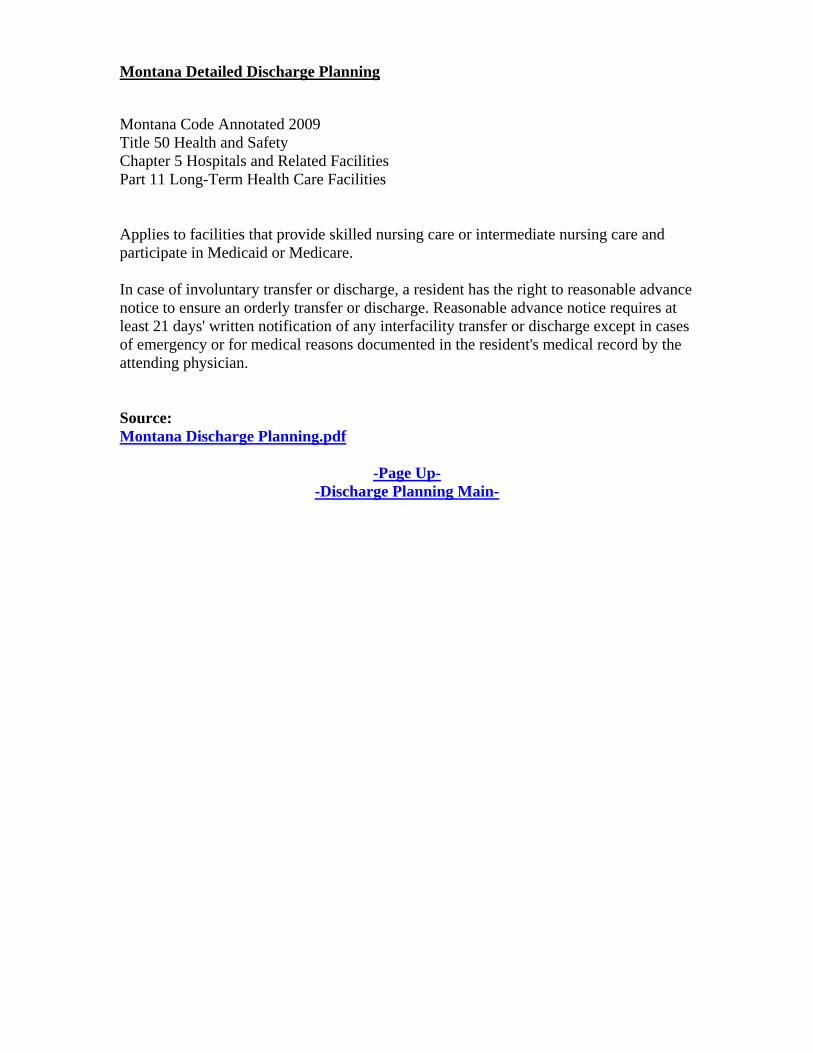
Montana Detailed Discharge Planning
Montana Code Annotated 2009 Title 50 Health and Safety Chapter 5 Hospitals and Related Facilities Part 11 Long-Term Health Care Facilities Applies to facilities that provide skilled nursing care or intermediate nursing care and participate in Medicaid or Medicare. In case of involuntary transfer or discharge, a resident has the right to reasonable advance notice to ensure an orderly transfer or discharge. Reasonable advance notice requires at least 21 days' written notification of any interfacility transfer or discharge except in cases of emergency or for medical reasons documented in the resident's medical record by the attending physician. Source: Montana Discharge Planning.pdf
-Page Up- -Discharge Planning Main-
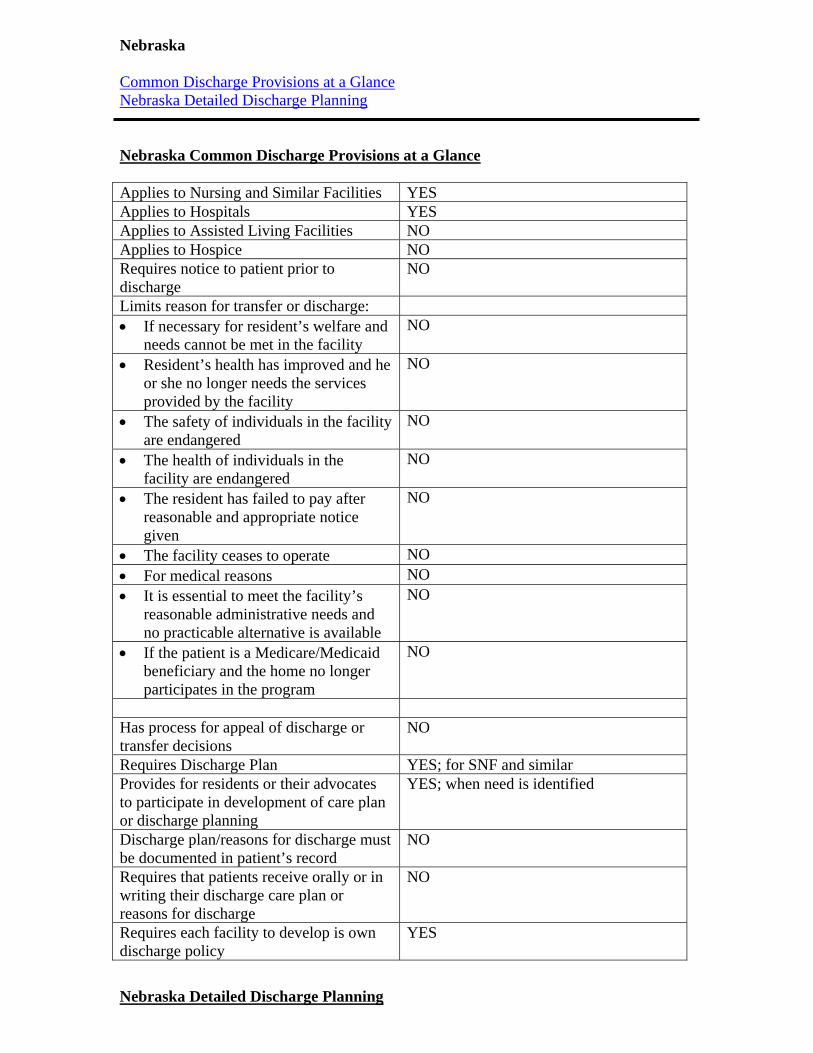
Nebraska Common Discharge Provisions at a Glance Nebraska Detailed Discharge Planning Nebraska Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES; for SNF and similar Provides for residents or their advocates to participate in development of care plan or discharge planning
YES; when need is identified
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES
Nebraska Detailed Discharge Planning

Title 175. Health Care Facilities and Services Licensure (Department of Health and Human Services) Nebraska Admin. Code Title 175, Ch. 9 (2009) Chapter 9 Hospitals 9-006.06 Applies to Hospitals Each hospital must provide discharge planning to patients who request information or who are identified as likely to suffer adverse health consequences upon discharge if there is not adequate discharge planning. The discharge planning program includes, but is not limited to:
1. A system for timely evaluation of any discharge planning needs of patients; 2. Identification of staff responsible for the program; 3. Development of a discharge plan with the patient or representative when need is
identified; 4. Maintenance of a complete and accurate list of community-based services,
resources and facilities to which patients can be referred; and 5. Arrangement for the initial implementation of a discharge plan including transfer
of necessary medical information. Chapter 12. Skilled Nursing Facilities, Nursing Facilities, and Intermediate Care Facilities 12-006.09C1b, 12-006.09C1c, 12-006.09C1c Applies to Skilled Nursing Facilities, Nursing Facilities, and Intermediate Care Facilities The facility must develop a comprehensive interdisciplinary care plan and discharge plan within seven days after the completion of the comprehensive assessment.
The facility must review and revise the care plan at least quarterly or with change in condition or services provided. Review of the care plan must include an interdisciplinary evaluation of the resident's progress relative to the goals established.
The facility must develop a post discharge plan of care for any resident when there is anticipated discharge to a home, same level, or a different level of care.
The discharge plan of care must be developed with the participation of the resident and resident's family.
The post discharge plan of care is developed to assist the resident in planning for post discharge needs and assist the resident to adjust to new living environment.
Source: Nebraska Administrative Code
-Page Up- -Discharge Planning Main-

Nevada Common Discharge Provisions at a Glance Nevada Detailed Discharge Plan Nevada Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice YES Requires notice to patient prior to discharge
No time frame specified
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Nevada Detailed Discharge Planning
Nevada Revised Statutes Chapter 449 Medical and Other Related Facilities Patients Rights 449.700, 449.705 Applies to all medical facilities. A patient may be transferred to another facility or home only if the patient has received an explanation of the need to transfer him and the alternatives available, unless his condition necessitates an immediate transfer to a facility for a higher level of care and he is unable to understand the explanation. If a patient in a medical facility or facility for the dependent is transferred to another facility, the facility shall forward a copy of the medical records of the patient, on or before the date the patient is transferred, to the other facility The facility is not required to obtain the oral or written consent of the patient to forward a copy of the medical records. Source: Nevada Patients Rights
-Page Up- -Discharge Planning Main-
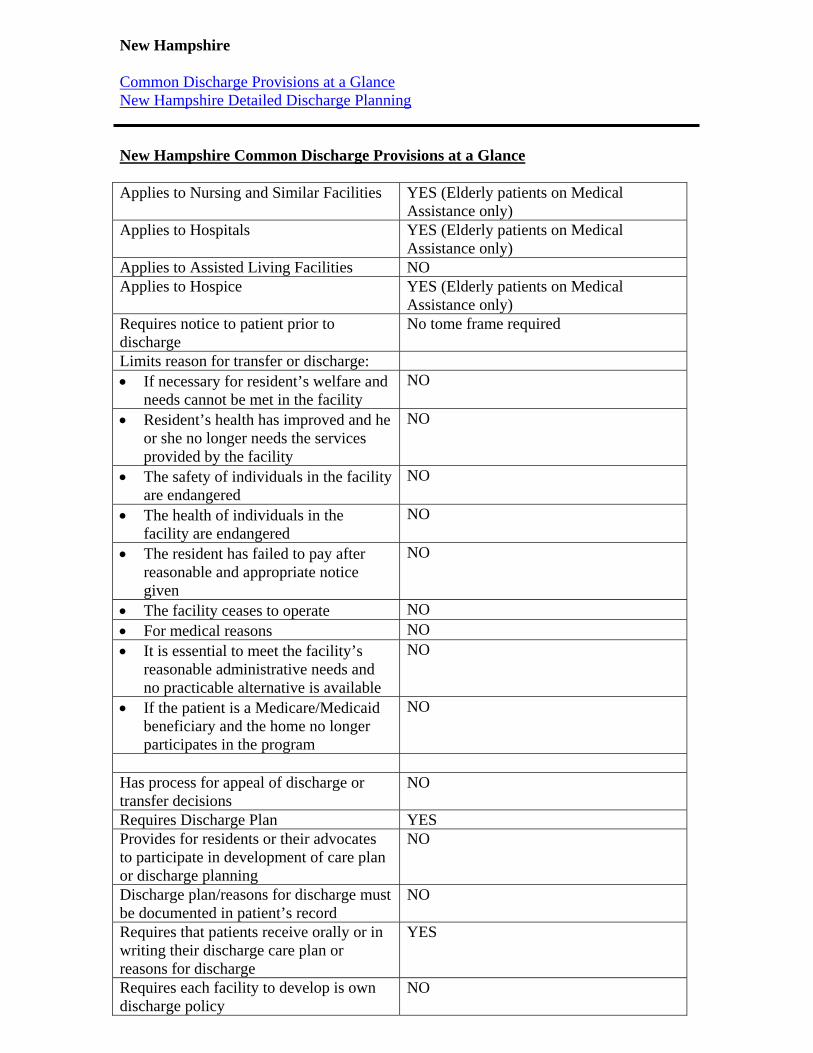
New Hampshire Common Discharge Provisions at a Glance New Hampshire Detailed Discharge Planning New Hampshire Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES (Elderly patients on Medical
Assistance only) Applies to Hospitals YES (Elderly patients on Medical
Assistance only) Applies to Assisted Living Facilities NO Applies to Hospice YES (Elderly patients on Medical
Assistance only) Requires notice to patient prior to discharge
No tome frame required
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

New Hampshire Detailed Discharge Planning
N.H. Admin. Rules, He-E 802.16 HE-E 802.16 Transfer or Discharge Plan. Applies to Elderly on Medical Assistance in all certified facilities Certified facilities shall provide sufficient preparation and assistance to residents in order to ensure their safe and orderly transfer or discharge from the facility. No resident shall be transferred or discharged unless there is a written transfer or discharge plan, which includes the following:
1. The circumstances surrounding the discharge or transfer, including: a. Alternative interventions initiated by the nursing facility before the facility
proposed the discharge or transfer; b. The fact that the facility has exhausted all reasonable alternatives short of
transfer or discharge; and c. Whether the facility used the services of the ombudsman program
2. All efforts that were made to locate the resident to the setting of his or her choice, and if the resident's wishes could not be accommodated, the reasons why;
3. The location of the new setting and, if a facility, confirmation that the facility has accepted the resident;
4. A comprehensive description of the medical, social, and rehabilitative needs of the resident and how the resident's needs will be met in the new setting;
5. Documentation of consultation with the resident, family or other interested parties, if and to the extent that this has been reasonably possible; and
6. The medical opinion of the resident's personal physician regarding the transfer or discharge, including the possible effects on the physical and emotional well-being of the resident.
A copy of the discharge plan shall be provided to the resident and his/her legal representative and the office of the state long-term care ombudsman. Source: New Hampshire Administrative Rules
-Page Up- -Discharge Planning Main-

New Jersey Common Discharge Provisions at a Glance New Jersey Detailed Discharge Planning New Jersey Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO
New Jersey Detailed Discharge Planning
Hospital Licensing Standards

N.J.A.C. 8:43G-11.5 (2010) § 8:43G-11.5 Discharge planning patient services § 8:43G-11.6 Discharge planning continuous quality improvement methods Applies to hospitals. Patients who require post-discharge continuity of care shall be linked to needed resources, such as:
1. Placement in a nursing home; 2. Enrollment with a home care program; 3. Transfer to another health care facility; 4. Referral to community resources; or 5. Information regarding availability of Medicare or Medicaid benefits.
The hospital shall make a diligent effort to find and effect an appropriate placement for any patient ready for discharge but requiring further care. Documentation shall be included in the patient's medical record. Patient care conferences or discharge planning rounds shall be held to discuss planning for patients needing continuity of care. The patient shall participate in the development of the discharge plan, where possible. The family or significant other shall participate in the development of the plan, where possible, and when the patient is able to agree, and does agree, to their involvement. Discharge planning shall be initiated within 24 hours of admission. If a patient's needs for post-discharge care change after a discharge plan is developed, the plan shall be modified to meet the patient's needs. The hospital shall have a mechanism to ensure that each patient receives, upon discharge, written instructions about follow-up care and medications, if relevant, and the telephone number of a contact person to call in case he or she has questions after discharge. For all patients who receive discharge planning, the patient's medical record shall include on-going documentation and a summary or summaries of the patient's discharge plan prepared by a member of the discharge planning team at the time of discharge, or within 30 days of discharge. There shall be a program of continuous quality improvement for discharge planning that is integrated into the hospital continuous quality improvement program and includes regularly collecting and analyzing data to help identify health-service problems and their extent, and recommending, implementing, and monitoring corrective actions on the basis of these data. The program shall monitor at least:
1. That communication occurs among members of the multidisciplinary team, and the patient and family;
2. Appropriateness of referrals; and Implementation of the discharge plan. Source: New Jersey Administrative Code
-Page Up-
-Discharge Planning Main-

New Mexico Common Discharge Provisions at a Glance New Mexico Detailed Discharge Planning New Mexico Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO

New Mexico Detailed Discharge Planning
Title 7. Health Chapter 7. Hospitals Part 2. Requirements for Acute Care, Limited Services and Special Hospitals 7.7.2.18 NMAC (2009) § 7.7.2.18.k Discharge Planning Applies to Hospitals Hospitals must have an effective, ongoing program coordinated with community resources to facilitate the provision of appropriate follow-up care to patients who are discharged. The discharge planning program shall:
1. Have a mechanism to identify patients who require discharge planning to provide continuity of medical care to meet their identified needs;
2. Initiate discharge planning in a timely manner; 3. Identify the role of the patient's provider, nursing staff, social work staff, other
appropriate staff, the patient, and the patient's family or representative in the initiation and implementation of the discharge planning process;
4. Assure documentation in the medical record of the discharge plan; 5. Allow for the timely and effective transmittal of all medical, social, economic
information concerning the patient to persons responsible for subsequent care of the patient;
6. Provide that every patient, or their legal representatives, receive relevant information concerning their health needs and is involved in his or her own discharge planning; and
7. Be reviewed at least once a year to evaluate effectiveness. Source: New Mexico Administrative Code: pg. 10
-Page Up- -Discharge Planning Main-

New York Common Discharge Provisions at a Glance New York Detailed Discharge Planning New York Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
YES
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons YES It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO
New York Detailed Discharge Planning
NY State Public Health Law, Article 28 § 2803-i.
Applies to hospitals
A general hospital inpatient may be discharged on the basis that inpatient hospital service in a general hospital is no longer medically necessary and that an appropriate discharge plan has been established, as long as:
1. A written notice of such determinations and a copy of the discharge plan have been provided to the patient or the appointed personal representative of the patient.
2. The patient or the appointed personal representative of the patient shall have the opportunity to sign the notice and a copy of the discharge plan and receive a copy of both signed documents.
The patient or the appointed personal representative of the patient may request a review of such determinations by the appropriate independent professional review agent. A written copy of the discharge plan, and discharge notice shall be provided to the beneficiary or the appointed personal representative of the beneficiary. The beneficiary or the appointed personal representative of the beneficiary shall have the opportunity to sign the documents and receive a copy of the signed documents. Source: New York State Department of Health
-Page Up- -Discharge Planning Main-

North Carolina Common Discharge Provisions at a Glance North Carolina Detailed Discharge Planning North Carolina Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
5 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate NO For medical reasons YES It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO

North Carolina Detailed Discharge Planning
N.C. Gen. Stat. § 131E-117 Chapter 131E. Health Care Facilities and Services Article 6. Health Care Facility Licensure Act Part 2. Nursing Home Patients’ Bill of Rights Applies to Nursing Homes Every patient has the right to not be transferred or discharged from a facility except for
Medical reasons, The patient's own or other patients' welfare, Nonpayment for the stay, or When the transfer or discharge is mandated under Medicare or Medicaid.
The patient shall be given at least five days' advance notice to ensure orderly transfer or discharge, unless the attending physician orders immediate transfer, and these actions, and the reasons for them, shall be documented in the patient's medical record. Source: North Carolina Declaration of Patients’ Rights
-Page Up- -Discharge Planning Main-

North Dakota Common Discharge Provisions at a Glance North Dakota Detailed Discharge Planning North Dakota Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility
Resident’s health has improved and he or she no longer needs the services provided by the facility
The safety of individuals in the facility are endangered
The health of individuals in the facility are endangered
The resident has failed to pay after reasonable and appropriate notice given
The facility ceases to operate For medical reasons It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO

North Dakota Detailed Discharge Planning Source: Title 33: State Department of Health Article 07: Licensing Medical Hospitals Chapter 01.1: Hospitals 33-07-01.1-09. Governing body. The governing body is legally responsible for the quality of patient care services, for patient safety and security, for the conduct, operation, and obligations of the hospital as an institution, and for ensuring compliance with all federal, state, and local laws. f. The governing body shall ensure that policies and procedures are reviewed at a minimum of every three years and when changes in standards of practice occur and shall at a minimum include: (4) Patient rights to include at least the following and require that each patient admitted be notified of these rights. (7) The transfer and discharge of patients, including discharge planning to meet the patients’ needs. k. The governing body shall ensure that the following patient care practices are implemented and monitored and take corrective action as necessary to attain compliance: (7) Every patient must receive effective discharge planning consistent with identified patient and family needs from the hospital. Discharge planning must be initiated in a timely manner. Patients, along with necessary medical information, must be transferred or referred to appropriate facilities, agencies, or outpatient services, as needed, for followup or ancillary care. 33-07-01.1-17. Patient care plan. c. Discharge planning must be initiated upon admission and kept current. (1) Appropriate discharge instructions must be provided to patients and family members dependent upon the patient’s identified needs. (2) Patients, along with necessary medical information, must be transferred or referred to appropriate facilities, agencies, or outpatient services for followup or ancillary care as needed. 33-07-01.1-30. Recovery services. c. A physician shall be responsible for the conduct of the recovery services and for the establishment of admission and discharge policies and procedures. Source: Chapter 03.2: Nursing Facilties 33-07-03.2-17. Resident record services. The governing body of the facility shall establish and implement policies and procedures to ensure the facility has a resident record service with administrative responsibility for resident records. 2. All records of discharged residents must be preserved for a period of ten years from date of discharge. Records of deceased residents must be preserved to seven years. 4. Each resident record must include: a. The name of the resident, personal licensed health care practitioner, dentist, and designated representative or other responsible person, admitting diagnosis, final diagnosis, condition on discharge, and disposition. Source:

Chapter 05: Nursing Facility Sanctions 33-07-05-06. Scope of sanctions. The following sanctions may be imposed upon a finding that a nursing facility no longer meets the requirements of 42 U.S.C. 1396r(b), (c), or (d) or the requirements of North Dakota Century Code section 23-16-01: 4. Recommendation for denial of payment with respect to any individual admitted to the nursing facility after receipt of the order. Denial of payment may not provide a basis for discharge or transfer of the individual.
-Page Up- -Discharge Planning Main-

Ohio Common Discharge Provisions at a Glance Ohio Detailed Discharge Planning Ohio Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
YES
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate YES For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
YES
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO

Ohio Detailed Discharge Planning
Ohio Revised Code Title 37 Health, Safety and Morals Chapter 3721: NURSING HOMES; RESIDENTIAL CARE FACILITIES 3721.13 Residents' rights. Residents have the right not to be transferred or discharged from the home unless the transfer is necessary because of one of the following:
1. The welfare and needs of the resident cannot be met in the home. 2. The resident’s health has improved sufficiently so that the resident no longer
needs the services provided by the home. 3. The safety of individuals in the home is endangered. 4. The health of individuals in the home would otherwise be endangered. 5. The resident has failed, after reasonable and appropriate notice.
1. A resident shall not be considered to have failed to have the resident’s care paid for if the resident has applied for Medicaid, unless both of the following are the case:
The resident’s application, or a substantially similar previous application, has been denied by the county department of job and family services. If the resident appealed the denial and the director of Job and Family Services has upheld the denial.
6. The home’s license has been revoked, the home is being closed or the home otherwise ceases to operate.
7. The resident is a recipient of Medicaid, and the home’s participation in the Medicaid program is involuntarily terminated or denied.
8. The resident is a beneficiary under the Medicare program, and the home’s participation in the Medicare program is involuntarily terminated or denied.
Source: Ohio Residents’ Rights
-Page Up- -Discharge Planning Main-

Oklahoma Common Discharge Provisions at a Glance Oklahoma Detailed Discharge Planning Oklahoma Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
10 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate NO For medical reasons YES It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Oklahoma Detailed Discharge Planning Title 310 - Oklahoma State Department of Health Chapter 680 - Residential Care Homes Subchapter 17 - Involuntary Transfer or Discharge of Resident 310:680-17-1, 310:680-17-2, 310:680-17-3, and 310:680-17-4 Applies to long-term care facilities A facility shall not involuntary transfer or discharge a resident except
1. For medical reasons, 2. For the resident's safety, or for the safety of other residents, or 3. For nonpayment for the resident's stay.
Involuntary transfer or discharge requires a written notice at least 10 days in advance, except:
1. When an emergency transfer or discharge is mandated by the resident's health care needs and is in accordance with the written orders and medical justification of the attending physician.
2. When the transfer or discharge is necessary for the physical safety of other residents as documented in the resident's record.
The written notice of involuntary transfer or discharge shall contain an explanation of the reasons for transfer or discharge and inform the resident and resident's representative, if any, of the right to request a hearing by the Department if they are aggrieved by the decision. A resident who is aggrieved by an involuntary transfer or discharge may request a hearing by the Department within five (5) days of receipt of the notice. Decisions reached in a hearing shall be binding on all parties, unless appealed to the Commissioner of Health. The Department of Health will initiate the transfer or discharge of a resident in any of the following situations:
1. When the resident's health care needs are not being met according to a licensed medical authority.
2. When the transfer or discharge is necessary for the physical safety of other residents as observed or as documented in the records.
3. When it is determined that a resident's rights have been violated or the resident has been unduly taken advantage of in fiscal matters, or has been physically, mentally, or sexually abused
The resident's wishes, in all situations, will be given careful consideration in determining whether or not the health or safety aspects involved outweigh the trauma of a resident being transferred or discharged. Sources: Oklahoma Statutes Guide to Discharge Planning
-Page Up- -Discharge Planning Main-

Oregon Common Discharge Provisions at a Glance Oregon Detailed Discharge Planning Oregon Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO

Oregon Detailed Discharge Planning
Chapter 411 Department of Human Services, Seniors and People with Disabilities Division Division 86 Nursing Facilities/Licensing – Administration and Services Or. Admin. R. 411-086-0160 (2009) Applies to Nursing Homes Within 14 days of admission, an RN must complete and document a comprehensive assessment of the resident's capabilities and needs for nursing services. The assessment shall include discharge potential. Discharge summary required for each resident before discharge. The discharge summary shall include:
A recapitulation of the resident's stay; A final summary of the resident's status, including the most recent nursing
assessment; and A post-discharge plan of care which will assist the resident to adjust to his/her
new living environment. A post-discharge plan is not required when the resident is discharged to acute care or to the morgue.
Sources: Oregon Administrative Rules: pg. 26
-Page Up- -Discharge Planning Main-

Pennsylvania Common Discharge Provisions at a Glance Pennsylvania Detailed Discharge Planning Pennsylvania Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES
Pennsylvania Detailed Discharge Planning
Title 28. Health and Safety Part IV. Health Facilities Subpart C. Long-Term Care Facilities Chapter 201. Applicability, Definitions, Ownership and General Operation of Long-Term Care Nursing Facilities 28 Pa. Code § 201.25 (2010) Applies to Long-Term Care Facilities There shall be a centralized coordinated discharge plan for each resident to ensure that the resident has a program of continuing care after discharge from the facility. The discharge plan shall be in accordance with each resident's needs. Sources: Pennsylvania Code
-Page Up- -Discharge Planning Main-

Rhode Island Common Discharge Provisions at a Glance Rhode Island Detailed Discharge Planning Rhode Island Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO

Rhode Island Detailed Discharge Planning
Agency 14. Department of Health Sub-Agency 090. Health Facilities, Licensure, Construction Chapter 007. Licensing of Hospitals CRIR 14-090-007 (2009) Applies to Hospitals The hospital shall have a discharge planning process for all inpatients. Discharge planning policies and procedures must be in writing and shall include a mechanism for discharge planners to receive regular updates regarding new offerings of community programs and the complete range of current options available at discharge. The hospital shall identify, at an early stage in hospitalization, all inpatients who are likely to suffer adverse health consequences on discharge if there is no adequate discharge planning. A discharge planning evaluation shall be provided to all inpatients identified as likely to suffer adverse health consequences on discharge, and to other patients on patient request, the request of the person acting on the patient's behalf, or upon the request of the physician.
1. The evaluation shall be timely to avoid unnecessary delays in discharge and must be part of the patient's medical record.
2. The evaluation shall include a needs assessment, the patient's capacity for self-care, and the availability of post-hospital services to meet the needs of the patient.
3. A registered nurse or social worker shall develop or supervise the development of the evaluation.
4. The results of the evaluation shall be discussed with the patient or the individual acting on the patient's behalf.
5. The evaluation shall be used to establish an appropriate discharge plan. The hospital shall transfer or refer inpatients and outpatients to appropriate facilities, agencies, or outpatient services, as needed, for follow-up care. Designated hospital personnel shall complete the "Continuity of Care" form approved by the Department for each patient who is discharged to another health care facility. The Continuity of Care form and instructions for its use should be downloaded from the Department's website: www.healthri.org. Sources: Rules and Regulations for Licensing of Hospitals.pdf: pg. 32
-Page Up- -Discharge Planning Main-

South Carolina Common Discharge Provisions at a Glance South Carolina Detailed Discharge Planning South Carolina Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
30 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate NO For medical reasons YES It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
NO

South Carolina Detailed Discharge Planning
South Carolina Code of Laws Title 44 - Health Chapter 81. Bill of Rights of Residents of Long-Term Care Facilities Section 44-81-40. A resident may be transferred or discharged only
1. For medical reasons, 2. For the welfare of the resident or for the welfare of other residents of the facility,
or 3. For nonpayment
Residents must be given written notice of not less than thirty days, except when: The health, safety, or welfare of other residents of the facility would be endangered by the thirty-day notice requirement, The time for giving notice must be that which is practicable under the circumstances. Source: South Carolina Bill of Rights of Residents of Long-Term Care Facilities
-Page Up- -Discharge Planning Main-

South Dakota Common Discharge Provisions at a Glance South Dakota Detailed Discharge Planning South Dakota Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities YES Applies to Hospice NO Requires notice to patient prior to discharge
YES: 30 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
YES
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate YES For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
YES
South Dakota Detailed Discharge Planning South Dakota Administrative Rules Rule 44:04; Medical Facilities Section 17: Residents’ Rights in Nursing Facilities and Assisted Living Centers 44:04:17:14. Admission, transfer, and discharge policies. A facility must establish and maintain policies and practices for admission, discharge, and transfer of residents which prohibit discrimination based upon payment source and which are made known to residents at or before the time of admission. The policies and practices must include:
(1) The resident may remain in the facility and may not be transferred or discharged unless the resident's needs and welfare cannot be met by the facility, the resident's health has improved sufficiently so the resident no longer needs the services provided by the facility, the safety or health of individuals in the facility is endangered by the resident, the resident has failed to pay for allowable billed services as agreed to, or the facility ceases to operate;
(2) The facility must notify the resident and a family member or client advocate in writing at least 30 days before the transfer or discharge unless a change in the resident's health requires immediate transfer or discharge or the resident has not resided in the facility for 30 days. The written notice must specify the reason for and effective date of the transfer or discharge and the location to which the resident will be transferred or discharged;
(3) Conditions under which the resident may request or refuse transfer within the facility; and
(4) A description of how the resident may appeal a decision by the facility to transfer or discharge the resident.
Source:
Residents’ Rights in Nursing Facilities and Assisted Living Centers
-Page Up- -Discharge Planning Main-

Tennessee Common Discharge Provisions at a Glance Tennessee Detailed Discharge Planning Tennessee Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
YES

Tennessee Detailed Discharge Planning
Rules of the Tennessee Department of Health Bureau of Health Licensure and Regulation; Division of Health Care Facilities; Board for Licensing Health Care Facilities Chapter 1200-08-01 Standards for Hospitals Tenn. Comp. R. & Regs. R. 1200-08-01-.05 (2009)
Applies to Hospitals The hospital must ensure continuity of care and provide an effective discharge planning process that applies to all patients. The hospital's discharge planning process, including discharge policies and procedures, must be specified in writing and must:
1. Be developed and/or supervised by a registered nurse, social worker or other appropriately qualified personnel;
2. Begin upon admission of any patient who is likely to suffer adverse health consequences;
3. Be provided when identified as a need by the patient, a person acting on the patient's behalf, or by the physician;
4. Include the likelihood of a patient's capacity for self-care or the possibility of the patient returning to his or her pre-hospitalization environment;
5. Identify the patient's continuing physical, emotional, housekeeping, transportation, social and other needs and must make arrangements to meet those needs;
6. Be completed on a timely basis to allow for arrangement of post-hospital care and to avoid unnecessary delays in discharge;
7. Involve the patient, the patient's family or individual acting on the patient's behalf, the attending physician, nursing and social work professionals and other appropriate staff, and must be documented in the patient's medical record; and
8. Be conducted on an ongoing basis throughout the continuum of hospital care. Coordination of services may involve promoting communication to facilitate family support, social work, nursing care, consultation, referral or other follow-up.
A discharge plan is required on every patient, even if the discharge is to home. The hospital must arrange for the initial implementation of the patient's discharge plan and must reassess the patient's discharge plan if there are factors that may affect continuing care needs or the appropriateness of the discharge plan. As needed, the patient and family members or interested persons must be taught and/or counseled to prepare them for post-hospital care. Source: Tennessee Standards for Hospitals.pdf: pg. 15
-Page Up- -Discharge Planning Main-

Texas Common Discharge Provisions at a Glance Texas Detailed Discharge Planning Texas Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO

Texas Detailed Discharge Planning
Title 40. Social Services and Assistance Part 1. Department of Aging and Disability Services Chapter 19. Nursing Facility Requirements for Licensure and Medicaid Certification Subchapter I. Resident Assessment 40 TAC § 19.803 (2009) Applies to Nursing Facilities When the facility anticipates discharge, the resident must have a discharge summary that includes:
1. A recapitulation of the overall course of the resident's stay; 2. A final summary of the resident's status, which must be available for release to
authorized persons and agencies with the consent of the resident or legal representative; and
3. A post-discharge plan of care, developed with the participation of the resident, a family representative, responsible party, and/or legal guardian, which will, after discharge, assist the resident to adjust to his new living environment.
The facility discharge summary must be available at the time of discharge when a resident is being discharged to a private residence, another nursing facility, a Medicare skilled nursing facility, another residential facility such as a board and care home, or an intermediate care facility for the mentally retarded. Source: Texas Administrative Code: pg. 7
-Page Up- -Discharge Planning Main-

Utah Common Discharge Provisions at a Glance Utah Detailed Discharge Planning Utah Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities YES Applies to Hospice YES Requires notice to patient prior to discharge
30 DAYS
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
YES
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate YES For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
YES

Utah Detailed Discharge Planning Utah Administrative Code Title 432 Health, Health Systems Improvement, Licensing R432-150 Nursing Care Facility R432-270 Assisted Living Facilities R432-750 Hospice Rule
Source:
R432-150-22. Admission, Transfer, and Discharge.
(1) Each facility must develop written admission, transfer and discharge policies and make these policies available to the public upon request. The facility must permit each resident to remain in the facility, and not transfer or discharge the resident from the facility unless: (a) The transfer or discharge is necessary for the resident's welfare and the resident's needs cannot be met in the facility; (b) The transfer or discharge is appropriate because the resident's health has improved sufficiently so the resident no longer needs the services provided by the facility; (c) The safety of individuals in the facility is endangered; (d) The health of individuals in the facility is endangered; (e) The resident has failed, after reasonable and appropriate notice, to pay for a stay at the facility; or (f) The facility ceases to operate.
(2) The facility must document resident transfers or discharges under any of the circumstances specified in R432-150-22(1)(a) through (f), in the resident's medical record. The transfer or discharge documentation must be made by: (a) the resident's physician if transfer or discharge is necessary under R432-150-22(1)(a) and (b); (b) a physician if transfer or discharge is necessary under R432-150-22(1)(c) and(d).
(3) Prior to the transfer or discharge of a resident, the facility must: (a) provide written notification of the transfer or discharge and the reasons for the transfer or discharge to the resident, in a language and manner the resident understands, and, if known, to a family member or legal representative of the resident; (b) record the reasons in the resident's clinical record; and (c) include in the notice the items described in R432-150-22(5).
(4) Except when specified in R432-150-22(4)(a), the notice of transfer or discharge required under R432-150-22(2), must be made by the facility at least 30 days before the resident is transferred or discharged.
(5) Notice may be made as soon as practicable before transfer or discharge if: (a) the safety or health of individuals in the facility would be endangered if the resident is not transferred or discharged sooner; (b) the resident's health improves sufficiently to allow a more immediate transfer or discharge; (c) an immediate transfer or discharge is required by the resident's urgent medical needs; or (d) a resident has not resided in the facility for 30 days.

(6) The contents of the written transfer or discharge notice must include the following: (a) the reason for transfer or discharge; (b) the effective date of transfer or discharge; (c) the location to which the resident is transferred or discharged; and (d) the name, address, and telephone number of the State and local Long Term Care Ombudsman programs. (e) For nursing facility residents with developmental disabilities, the notice must contain the mailing address and telephone number of the agency responsible for the protection and advocacy of developmentally disabled individuals established under part C of the Developmental Disabilities Assistance and Bill of Rights Act. (f) For nursing facility residents who are mentally ill, the notice must contain the mailing address and telephone number of the agency responsible for the protection and advocacy of mentally ill individuals established under the Protection and Advocacy for Mentally Ill Individuals Act.
(7) The facility must provide discharge planning to prepare and orient a resident to ensure safe and orderly transfer or discharge from the facility.
(8) Notice of resident bed-hold policy, transfer and re-admission must be documented in the resident file. (a) Before a facility transfers a resident to a hospital or allows a resident to go on therapeutic leave, the facility must provide written notification and information to the resident and a family member or legal representative that specifies: (i) the facility's policies regarding bed-hold periods permitting a resident to return; an (ii) the duration of the bed-hold policy, if any, during which the resident is permitted to return and resume residence in the facility. (b) At the time of transfer of a resident to a hospital or for therapeutic leave, the facility must provide written notice to the resident and a family member or legal representative, which specifies the duration of the bed- hold policy. (c) If transfers necessitated by medical emergencies preclude notification at the time of transfer, notification shall take place as soon as possible after transfer. (d) The facility must establish and follow a written policy under which a resident whose hospitalization or therapeutic leave exceeds the bed-hold period is readmitted to the facility.
(9) The facility must establish and maintain identical policies and practices regarding transfer, discharge, and the provision of services for all individuals regardless of pay source.
(10) The facility must have in effect a written transfer agreement with one or more hospitals to ensure that: (a) residents are transferred from the facility to the hospital and ensured of timely admission to the hospital when transfer is medically necessary as determined by the attending physician; (b) medical and other information needed for care and treatment of residents is exchanged between facilities including documentation of reasons for a less expensive setting; and (c) security and accountability of personal property of the individual transferred is maintained.
Source:
R432-270-11. Transfer or Discharge Requirements.

(1) A resident may be discharged, transferred, or evicted for one or more of the following reasons: (a) The facility is no longer able to meet the resident's needs because the resident poses a threat to health or safety to self or others, or the facility is not able to provide required medical treatment. (b) The resident fails to pay for services as required by the admission agreement. (c) The resident fails to comply with written policies or rules of the facility. (d) The resident wishes to transfer. (e) The facility ceases to operate.
(2) Prior to transferring or discharging a resident, the facility shall serve a transfer or discharge notice upon the resident and the resident's responsible person. (a) The notice shall be either hand-delivered or sent by certified mail. (b) The notice shall be made at least 30 days before the day on which the facility plans to transfer or discharge the resident, except that the notice may be made as soon as practicable before transfer or discharge if: (i) the safety or health of persons in the facility is endangered; or (ii) an immediate transfer or discharge is required by the resident's urgent medical needs.
(3) The notice of transfer or discharge shall: (a) be in writing with a copy placed in the resident file (b) be phrased in a manner and in a language the resident can understand; (c) detail the reasons for transfer or discharge; (d) state the effective date of transfer or discharge; (e) state the location to which the resident will be transferred or discharged; (f) state that the resident may request a conference to discuss the transfer or discharge; and (g) contain the following information: (i) for facility residents who are 60 years of age or older, the name, mailing address, and telephone number of the State Long Term Care Ombudsman; (ii) for facility residents with developmental disabilities, the mailing address and telephone number of the agency responsible for the protection and advocacy of developmentally disabled individuals established under part C of the Developmental Disabilities Assistance and Bill of Rights Act; and
(iii) for facility residents who are mentally ill, the mailing address and telephone number of the agency responsible for the protection and advocacy of mentally ill individuals established under the Protection and Advocacy for Mentally Ill Individuals Act.
(4) The facility shall provide sufficient preparation and orientation to a resident to ensure a safe and orderly transfer or discharge from the facility.
(5) The resident or the resident's responsible person may contest a transfer or discharge. If the transfer or discharge is contested, the facility shall provide an informal conference, except where undue delay might jeopardize the health, safety, or well-being of the resident or others. (a) The resident or the resident's responsible person must request the conference within five calendar days of the day of receipt of notice of discharge to determine if a satisfactory resolution can be reached. (b) Participants in the conference shall include the facility representatives, the resident or the resident's responsible person, and any others requested by the resident or the resident's responsible person.

Source:
R432-750-12. Patient Records.
(5) The person who is assigned to supervise or coordinate care for a patient must complete a discharge summary when services to the patient are terminated. The summary shall include: (a) the reason for discharge; and (b) the name of the facility or agency if the patient has been referred or transferred.
(6) The hospice shall safeguard clinical record information against loss, destruction, and unauthorized use. (a) Written procedures shall govern the use and removal of records and conditions for release of patient information. (b) A written consent is required for the release of patient/client information and photographing of recorded information. (c) When a patient is transferred to another facility or agency, a copy of the record or abstract must be sent to that service agency.
-Page Up- -Discharge Planning Main-

Vermont Common Discharge Provisions at a Glance Vermont Detailed Discharge Planning Vermont Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
YES: 30 DAYS
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate NO For medical reasons YES It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
NO
Vermont Detailed Discharge Planning

Vermont Statutes Title 33 Human Services Part 5 Programs and Services for Vulnerable Adults Chapter 73 Nursing Home Residents’ Bill of Rights § 7301 D) is transferred or discharged only for medical reasons, or for the resident's welfare or that of other residents, or for nonpayment of the resident's stay (except as prohibited by Titles XVIII or XIX of the Social Security Act), and is given reasonable advance notice to ensure orderly transfer or discharge, and such actions are documented in the resident's medical record. Residents shall be notified in writing of the proposed transfer or discharge and reasons for it at least 72 hours before a transfer within the facility and 30 days before a discharge from the facility. In cases where the health or safety of individuals would be endangered, or an immediate transfer or discharge is required by the resident's urgent medical needs, notice shall be made as soon as practicable before transfer or discharge. Notice shall explain the resident's right to appeal the proposed action, under the facility's grievance procedure and shall include the address and phone number of the area ombudsman. The resident informed of this right may choose to relocate before the notice period ends. The facility shall make reasonable efforts to accommodate new residents without disrupting room assignments; Source: Nursing Home Residents’ Bill of Rights
-Page Up- -Discharge Planning Main-

Virginia Common Discharge Provisions at a Glance Virginia Detailed Discharge Planning Virginia Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals NO Applies to Assisted Living Facilities YES Applies to Hospice NO Requires notice to patient prior to discharge
30 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan YES Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
YES

Virginia Detailed Discharge Planning
Virginia Administrative Code Title 22. Social Services VAC Agency No.. 40 Department of Social Services Chapter 72. Standards for Licensed Assisted Living Facilities Part V. Admission, Retention and Discharge of Residents When actions, circumstances, conditions, or care needs occur that will result in the discharge of a resident, discharge planning shall begin immediately, and there shall be documentation of such, including the beginning date of discharge planning. As soon as discharge planning begins, the assisted living facility shall notify the resident and the resident's legal representatives and designated contact person if any, of the planned discharge, the reason for the discharge, and that the resident will be moved within 30 days unless there are extenuating circumstances. The facility shall assist the resident and his legal representative, if any, in the discharge or transfer process. The facility shall help the resident prepare for relocation, including discussing the resident's destination. Primary responsibility for transporting the resident and his possessions rests with the resident or his legal representative. The assisted living facility shall provide to the resident and, as appropriate, his legal representative and designated contact person a dated statement signed by the licensee or administrator that contains the following information:
1. The date on which the resident, his legal representative or designated contact person was notified of the planned discharge and the name of the legal representative or designated contact person who was notified;
2. The reason or reasons for the discharge; 3. The actions taken by the facility to assist the resident in the discharge and
relocation process; and 4. The date of the actual discharge from the facility and the resident's destination.
Source: Virginia Administrative Code
-Page Up- -Discharge Planning Main-

Washington Common Discharge Provisions at a Glance Washington Detailed Discharge Planning Washington Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
YES

Washington Detailed Discharge Planning
Title 70. Public Health and Safety Chapter 70.41. Hospital Licensing and Safety Rev. Code Wash. (ARCW) § 70.41.320 (2009) Applies to Discharge from Hospital to Long-Term Care Hospitals and acute care facilities shall work cooperatively with the department of Social and Health Services, area agencies on aging, and local long-term care information and assistance organizations in the planning and implementation of patient discharges to long-term care services. Hospitals and acute care facilities must also establish written policies and procedures to:
1. Identify patients needing further nursing, therapy, or supportive care following discharge from the hospital;
2. Develop a documented discharge plan for each identified patient, including relevant patient history, specific care requirements, and date such follow-up care is to be initiated;
3. Coordinate with patient, family, caregiver, and appropriate members of the health care team;
4. Provide any patient, regardless of income status, written information and verbal consultation regarding the array of long-term care options available in the community, including the relative cost, eligibility criteria, location, and contact persons;
5. Promote an informed choice of long-term care services on the part of patients, family members, and legal representatives; and
6. Ensure timely transition to appropriate home, community residential, or nursing facility care.
7. Work in cooperation with the department which is responsible for ensuring that patients eligible for Medicaid long-term care receive prompt assessment and appropriate service authorization.
Source: Washington State Hospital Licensing and Safety
-Page Up- -Discharge Planning Main-

West Virginia Common Discharge Provisions at a Glance West Virginia Detailed Discharge Planning West Virginia Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities NO Applies to Hospitals YES Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
YES
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES

West Virginia Detailed Discharge Planning
Title 64. Legislative Rule West Virginia Division of Health Series 12. Hospital Licensure W. Va. CSR § 64-12-14 (2009) Applies to Hospitals The hospital shall have in effect a discharge planning process for post-hospital services, including hospice, which includes early assessment of the needs of each patient, particularly those with potential risk for adverse consequences upon discharge. The assessment shall be based upon the patient's functional abilities and probable environment to which the patient shall return. The hospital's policies and procedures shall be specified in writing. A discharge needs assessment, evaluating the factors that affect the patient's need for post-hospital care, shall be performed or supervised by a registered nurse, social worker or other appropriately qualified person, as identified by hospital policy, and be completed in enough time for appropriate arrangements to be made prior to discharge. The assessment shall address the biopsychosocial needs of the patient, the level of understanding of those needs and an identification of post hospital care resources. The hospital shall provide counseling as needed, to the patient and family members or interested persons, to prepare them for post-hospital care, including hospice services. The hospital shall arrange for the initial implementation of the patient's discharge plan, including obtaining post-hospital services as necessary. The hospital shall ensure that the discharge plan be reassessed, as needed, and entered into the patient's record. The hospital shall transfer or refer patients, along with necessary medical information, to appropriate facilities, agencies or outpatient services, as needed, for follow-up or ancillary care. Sources: West Virginia Administrative Law: pg. 34
-Page Up- -Discharge Planning Main-

Wisconsin Common Discharge Provisions at a Glance Wisconsin Detailed Discharge Planning Wisconsin Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals YES: See Detailed Planning for
limitations Applies to Assisted Living Facilities NO Applies to Hospice YES: See Detailed Planning for
limitations Requires notice to patient prior to discharge
YES: 30 Days
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility YES
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
YES
The health of individuals in the facility are endangered
YES
The resident has failed to pay after reasonable and appropriate notice given
YES
The facility ceases to operate NO For medical reasons YES It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
YES
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
YES
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
YES
Requires each facility to develop is own discharge policy
YES

Wisconsin Detailed Discharge Planning
Department of Health Services Chapter 132 Nursing Homes Subchapter V – Admissions, Retentions and Removals DHS 132.53 Transfers and discharges. DHS 132.53(1) (1) SCOPE. This section shall apply to all resident transfers and discharges, except that in the event of conflict with s. 49.45 (6c) (c) and (d), 49.498 (4) or 50.03 (5m) or (14), Stats., the relevant statutory requirement shall apply. DHS 132.53(2) (2) CONDITIONS. DHS 132.53(2)(a) (a) Prohibition and exceptions. No resident may be discharged or transferred from a facility, except: DHS 132.53(2)(a)1. 1. Upon the request or with the informed consent of the resident or guardian; DHS 132.53(2)(a)2. 2. For nonpayment of charges, following reasonable opportunity to pay any deficiency; DHS 132.53(2)(a)3. 3. If the resident requires care other than that which the facility is licensed to provide; DHS 132.53(2)(a)4. 4. If the resident requires care which the facility does not provide and is not required to provide under this chapter; DHS 132.53(2)(a)5. 5. For medical reasons as ordered by a physician; DHS 132.53(2)(a)6. 6. In case of a medical emergency or disaster; DHS 132.53(2)(a)7. 7. If the health, safety or welfare of the resident or other residents is endangered, as documented in the resident's clinical record; DHS 132.53(2)(a)8. 8. If the resident does not need nursing home care; DHS 132.53(2)(a)9. 9. If the short-term care period for which the resident was admitted has expired; or DHS 132.53(2)(a)10. 10. As otherwise permitted by law.

DHS 132.53(2)(b) (b) Alternate placement. DHS 132.53(2)(b)1. 1. Except for transfers or discharges under par. (a) 2. and 6., for nonpayment or in a medical emergency, no resident may be involuntarily transferred or discharged unless an alternative placement is arranged for the resident. The resident shall be given reasonable advance notice of any planned transfer or discharge and an explanation of the need for and alternatives to the transfer or discharge except when there is a medical emergency. The facility, agency, program or person to which the resident is transferred shall have accepted the resident for transfer in advance of the transfer, except in a medical emergency. DHS 132.53(2)(b)2. 2. No resident may be involuntarily transferred or discharged under par. (a) 2. for nonpayment of charges if the resident meets both of the following conditions: DHS 132.53(2)(b)2.a. a. He or she is in need of ongoing care and treatment and has not been accepted for ongoing care and treatment by another facility or through community support services; and DHS 132.53(2)(b)2.b. b. The funding of the resident's care in the nursing home under s. 49.45 (6m), Stats., is reduced or terminated because either the resident requires a level or type of care which is not provided by the nursing home or the nursing home is found to be an institution for mental diseases as defined under 42 CFR 435.1009. DHS 132.53(3) (3) PROCEDURES. DHS 132.53(3)(a) (a) Notice. The facility shall provide a resident, the resident's physician and, if known, an immediate family member or legal counsel, guardian, relative or other responsible person at least 30 days notice of transfer or discharge under sub. (2) (a) 2. to 10., and the reasons for the transfer or discharge, unless the continued presence of the resident endangers the health, safety or welfare of the resident or other residents. The notice shall also contain the name, address and telephone number of the board on aging and long-term care. For a resident with developmental disability or mental illness, the notice shall contain the mailing address and telephone number of the protection and advocacy agency designated under s. 51.62 (2) (a), Stats. DHS 132.53(3)(b) (b) Planning conference. DHS 132.53(3)(b)1. 1. Unless circumstances posing a danger to the health, safety or welfare of a resident require otherwise, at least 7 days before the planning conference required by subd. 2., the resident, guardian, if any, any appropriate county agency, and others designated by the resident, including the resident's physician, shall be given a notice containing the time and place of the conference, a statement informing the resident that any persons of the

resident's choice may attend the conference, and the procedure for submitting a complaint to the department. DHS 132.53(3)(b)2. 2. Unless the resident is receiving respite care or unless precluded by circumstances posing a danger to the health, safety, or welfare of a resident, prior to any involuntary transfer or discharge under sub. (2) (a) 2. to 10., a planning conference shall be held at least 14 days before transfer or discharge with the resident, guardian, if any, any appropriate county agency, and others designated by the resident, including the resident's physician, to review the need for relocation, assess the effect of relocation on the resident, discuss alternative placements and develop a relocation plan which includes at least those activities listed in subd. 3. DHS 132.53(3)(b)3. 3. Transfer and discharge activities shall include: DHS 132.53(3)(b)3.a. a. Counseling regarding the impending transfer or discharge; DHS 132.53(3)(b)3.b. b. The opportunity for the resident to make at least one visit to the potential alternative placement, if any, including a meeting with that facility's admissions staff, unless medically contraindicated or waived by the resident; DHS 132.53(3)(b)3.c. c. Assistance in moving the resident and the resident's belongings and funds to the new facility or quarters; and DHS 132.53(3)(b)3.d. d. Provisions for needed medications and treatments during relocation. DHS 132.53(3)(b)4. 4. A resident who is transferred or discharged at the resident's request shall be advised of the assistance required by subd. 3. and shall be provided with that assistance upon request. DHS 132.53(3)(c) (c) Records. Upon transfer or discharge of a resident, the documents required by s. DHS 132.45 (5) (L) and (6) (h) shall be prepared and provided to the facility admitting the resident, along with any other information about the resident needed by the admitting facility. DHS 132.53(4) (4) TRANSFER AGREEMENTS. DHS 132.53(4)(a) (a) Requirement. Each facility shall have in effect a transfer agreement with one or more hospitals under which inpatient hospital care or other hospital services are available promptly to the facility's residents when needed. Each intermediate care facility shall also have in effect a transfer agreement with one or more skilled care facilities. DHS 132.53(4)(b) (b) Transfer of residents. A hospital and a facility shall be considered to have a transfer
agreement in effect if there is a written agreement between them or, when the 2 institutions are under common control, if there is a written statement by the person or body which controls them, which gives reasonable assurance that: DHS 132.53(4)(b)1. 1. Transfer of residents will take place between the hospital and the facility ensuring timely admission, whenever such transfer is medically appropriate as determined by the attending physician; and DHS 132.53(4)(b)2. 2. There shall be interchange of medical and other information necessary for the care and treatment of individuals transferred between the institutions, or for determining whether such individuals can be adequately cared for somewhere other than in either of the institutions. DHS 132.53(4)(d) (d) Notice requirements. DHS 132.53(4)(d)1. 1. Before a resident of a facility is transferred to a hospital or for therapeutic leave, the facility shall provide written information to the resident and an immediate family member or legal counsel concerning the provisions of the approved state medicaid plan about the period of time, if any, during which the resident is permitted to return and resume residence in the nursing facility. DHS 132.53(4)(d)2. 2. At the time of a resident's transfer to a hospital or for therapeutic leave, the facility shall provide written notice to the resident and an immediate family member or legal counsel of the duration of the period, if any, specified under subd. 1. DHS 132.53 - ANNOT. Note: The "approved state medicaid plan" referred to s. 49.498 (4) (d) 1a, Stats., and subd. 1. states that the department shall have a bedhold policy. The bedhold policy is found in s. DHS 107.09 (4) (j). DHS 132.53(5) (5) BEDHOLD. DHS 132.53(5)(a) (a) Bedhold. A resident who is on leave or temporarily discharged, as to a hospital for surgery or treatment, and has expressed an intention to return to the facility under the terms of the admission statement for bedhold, shall not be denied readmission unless, at the time readmission is requested, a condition of sub. (2) (b) has been satisfied. DHS 132.53(5)(b) (b) Limitation. The facility shall hold a resident's bed under par. (a) until the resident returns, until the resident waives his or her right to have the bed held, or up to 15 days following the temporary leave or discharge, whichever is earlier.

DHS 132.53 - ANNOT. Note: See s. DHS 107.09 (4) (j) for medical assistance bedhold rules. DHS 132.53(6) (6) APPEALS ON TRANSFERS AND DISCHARGES. DHS 132.53(6)(a) (a) Right to appeal. DHS 132.53(6)(a)1. 1. A resident may appeal an involuntary transfer or discharge decision. DHS 132.53(6)(a)2. 2. Every facility shall post in a prominent place a notice that a resident has a right to appeal a transfer or discharge decision. The notice shall explain how to appeal that decision and shall contain the address and telephone number of the nearest bureau of quality assurance regional office. The notice shall also contain the name, address and telephone number of the state board on aging and long-term care or, if the resident is developmentally disabled or has a mental illness, the mailing address and telephone number of the protection and advocacy agency designated under s. 51.62 (2) (a), Stats. DHS 132.53(6)(a)3. 3. A copy of the notice of a resident's right to appeal a transfer or discharge decision shall be placed in each resident's admission folder. DHS 132.53(6)(a)4. 4. Every notice of transfer or discharge under sub. (3) (a) to a resident, relative, guardian or other responsible party shall include a notice of the resident's right to appeal that decision. DHS 132.53(6)(b) (b) Appeal procedures. DHS 132.53(6)(b)1. 1. If a resident wishes to appeal a transfer or discharge decision, the resident shall send a letter to the nearest regional office of the department's bureau of quality assurance within 7 days after receiving a notice of transfer or discharge from the facility, with a copy to the facility administrator, asking for a review of the decision. DHS 132.53(6)(b)2. 2. The resident's written appeal shall indicate why the transfer or discharge should not take place. DHS 132.53(6)(b)3. 3. Within 5 days after receiving a copy of the resident's written appeal, the facility shall provide written justification to the department's bureau of quality assurance for the transfer or discharge of the resident from the facility. DHS 132.53(6)(b)4. 4. If the resident files a written appeal within 7 days after receiving notice of transfer or of discharge from the facility, the resident may not be transferred or discharged from the

facility until the department's bureau of quality assurance has completed its review of the decision and notified both the resident and the facility of its decision. DHS 132.53(6)(b)5. 5. The department's bureau of quality assurance shall complete its review of the facility's decision and notify both the resident and the facility in writing of its decision within 14 days after receiving written justification for the transfer or discharge of the resident from the facility. DHS 132.53(6)(b)6. 6. A resident or a facility may appeal the decision of the department's bureau of quality assurance in writing to the department of administration's division of hearings and appeals within 5 days after receipt of the decision. DHS 132.53 - ANNOT. Note: The mailing address of the Division of Hearings and Appeals is P.O. Box 7875, Madison, Wisconsin 53707. DHS 132.53(6)(b)7. 7. The appeal procedures in this paragraph do not apply if the continued presence of the resident poses a danger to the health, safety or welfare of the resident or other residents. DHS 132.53 - ANNOT. Note: The bureau of quality assurance was renamed the division of quality assurance. Source: http://www.legis.state.wi.us/rsb/code/dhs/dhs132.pdf Department of Health Services Chapter 131 Hospices Subchapter IV – Patient Care DHS 131.44 Discharge DHS 131.44(1) (1) OBLIGATION. Once a hospice has admitted a patient to the program, and the patient or the patient's spokesperson has signed the acknowledgement and authorization for services under s. DHS 131.41 (5), the hospice is obligated to provide care to that patient. DHS 131.44(2) (2) WRITTEN POLICY. The hospice shall have a written policy that details the manner in which the hospice is able to end its obligation to a patient. This policy shall be provided to the patient or patient's spokesperson as part of the acknowledgement and authorization process at the time of the patient's admission. The policy shall include the following bases for discharging a patient: DHS 131.44(2)(a) (a) Voluntary discharge. The hospice shall discharge a patient from the program if the patient:

DHS 131.44(2)(a)1. 1. Elects care other than hospice care at any time; DHS 131.44(2)(a)2. 2. Elects active treatment, inconsistent with the role of palliative hospice care; DHS 131.44(2)(a)3. 3. Moves beyond the geographical area served by the hospice; DHS 131.44(2)(a)4. 4. Decides to transfer to another hospice program; or DHS 131.44(2)(a)5. 5. Chooses to withdraw from the program with or without cause. DHS 131.44(2)(b) (b) Involuntary discharge. The hospice may discharge a patient from the program against the patient's will: DHS 131.44(2)(b)1. 1. If the patient requests services in a setting that exceeds the limitations of the hospice's authority; DHS 131.44(2)(b)2. 2. For the patient's safety and welfare or the safety and welfare of others; or DHS 131.44(2)(b)3. 3. For nonpayment of charges, following reasonable opportunity to pay any deficiency. DHS 131.44(3) (3) PROCEDURE. When a patient is being discharged pursuant to sub. (2) (a) 1., 2. or 3. or (b) 1. or 3., the hospice shall give written notice to the patient or patient spokesperson, family spokesperson and attending physician at least 14 days prior to the date of discharge, with a proposed date for a pre-discharge planning conference. DHS 131.44 - ANNOT. History: Cr. Register, May, 1992, No. 437, eff. 6-1-92. http://nxt.legis.state.wi.us/nxt/gateway.dll?f=templates&fn=default.htm&d=codex&jd=top Department of Health Services Chapter 124 Hospitals Subchapter II – Management DHS 124.05 Governing Body DHS 124.05(2)(j) (j) Discharge planning. DHS 124.05(2)(j)1. 1. The governing body shall ensure that the hospital maintains an effective, ongoing

program coordinated with community resources to facilitate the provision of follow-up care to patients who are discharged. DHS 124.05(2)(j)2. 2. The governing body shall ensure that the hospital has current information on community resources available for continuing care of patients following their discharge. DHS 124.05(2)(j)3. 3. The discharge planning program shall: DHS 124.05(2)(j)3.a. a. Be reviewed periodically for timely initiation of discharge planning on an individual patient basis; DHS 124.05(2)(j)3.b. b. Provide that every patient receive relevant information concerning continuing health needs and is appropriately involved in his or her own discharge planning; DHS 124.05(2)(j)3.c. c. Be reviewed at least once a year and more often if necessary to ensure the appropriate disposition of patients; and DHS 124.05(2)(j)3.d. d. Allow for the timely and effective transmittal of all appropriate medical, social, and economic information concerning the discharged patient to persons or facilities responsible for the subsequent care of the patient. Source: http://nxt.legis.state.wi.us/nxt/gateway.dll?f=templates&fn=default.htm&d=codex&jd=tp
-Page Up- -Discharge Planning Main-
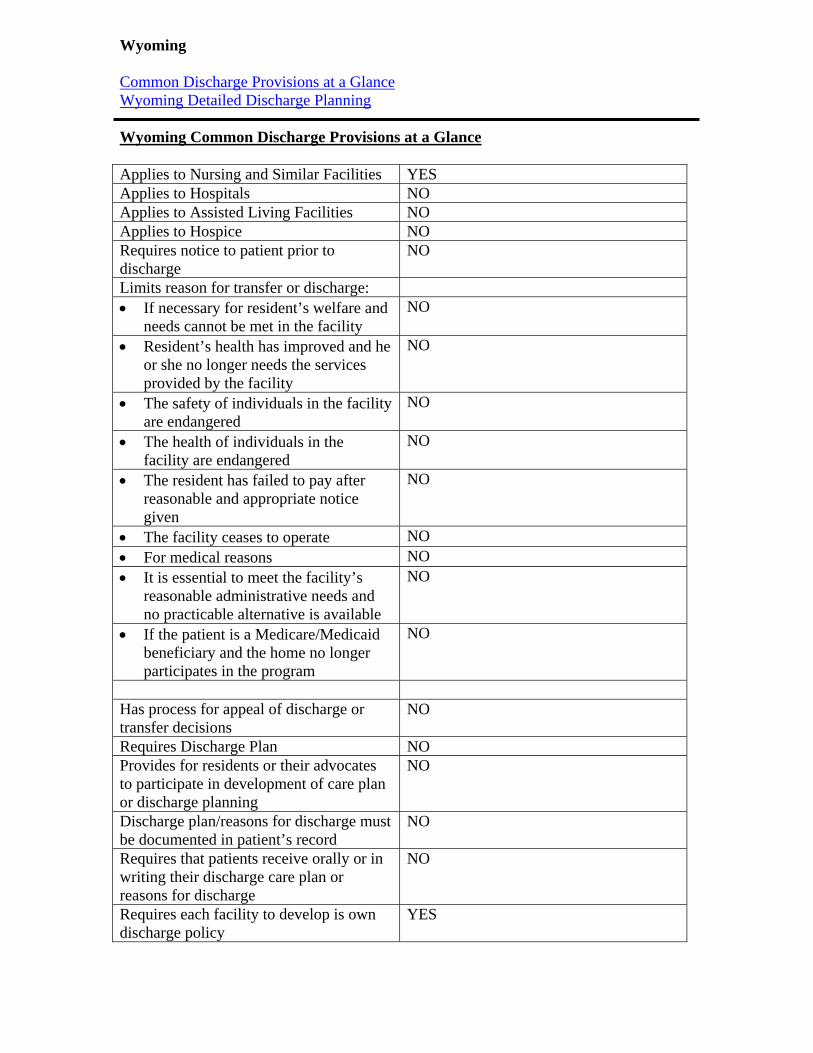
Wyoming Common Discharge Provisions at a Glance Wyoming Detailed Discharge Planning Wyoming Common Discharge Provisions at a Glance Applies to Nursing and Similar Facilities YES Applies to Hospitals NO Applies to Assisted Living Facilities NO Applies to Hospice NO Requires notice to patient prior to discharge
NO
Limits reason for transfer or discharge: If necessary for resident’s welfare and
needs cannot be met in the facility NO
Resident’s health has improved and he or she no longer needs the services provided by the facility
NO
The safety of individuals in the facility are endangered
NO
The health of individuals in the facility are endangered
NO
The resident has failed to pay after reasonable and appropriate notice given
NO
The facility ceases to operate NO For medical reasons NO It is essential to meet the facility’s
reasonable administrative needs and no practicable alternative is available
NO
If the patient is a Medicare/Medicaid beneficiary and the home no longer participates in the program
NO
Has process for appeal of discharge or transfer decisions
NO
Requires Discharge Plan NO Provides for residents or their advocates to participate in development of care plan or discharge planning
NO
Discharge plan/reasons for discharge must be documented in patient’s record
NO
Requires that patients receive orally or in writing their discharge care plan or reasons for discharge
NO
Requires each facility to develop is own discharge policy
YES

Wyoming Detailed Discharge Planning
Agency 048. Department of Health Sub-Agency 020. Aging Division Chapter 011. Rules and Regulations for Program Administration of Nursing Care Facilities WCWR 048-020-011 (2009) Applies to Nursing Care Facilities The facility shall have in operation an organized discharge planning program. This program shall include the resident, physician(s), nurses, social services personnel, dietitian, and therapists to identify problems and goals thus preparing the resident for the next level of care and arranging for placement in the appropriate care environment. The facility shall maintain written discharge planning procedures which describe:
1. How the discharge coordinator will function, and his/her authority and relationship with the facility's staff.
2. The time period in which each resident's need for discharge planning is determined (preferably within seven (7) days after the day of admission).
3. The maximum time period after which a reevaluation of each resident's discharge plan is made.
4. Local resources available to the facility, the resident, and the attending physician to assist in developing and implementing individual discharge plans.
5. Provisions for periodic review and reevaluation of the facility's discharge planning program.
Source: Wyoming Health Department, Aging Division: pg. 13
-Page Up- -Discharge Planning Main-