
directLINK 02-18 ENGLISCH final 4.7.18
28
direct LINK customization Custom-made LINK ® Endo-Model ® still intact after 26 years in situ 3D data confirmed intraoperatively Dr. med. Marcus Reinke reports on his first implantation of the SP-CL ® from LINK with 3D planning Magazine for Arthroplasty Issue 2/2018 Affordable high-performance medicine Prof. Dr. med. Hanns-Peter Knaebel on customer needs and the future of the healthcare system »WE ROUTINELY EMPLOY TIBIAL CONES FOR REVISIONS« Prof. Dr. med. Thorsten Gehrke on the advantages of the new TrabecuLink ® Tibial Cones from LINK INTERVIEW
Transcript of directLINK 02-18 ENGLISCH final 4.7.18
directdirect
LINK customizationCustom-made LINK® Endo-Model® still intact after 26 years in situ
3D data confi rmed intraoperativelyDr. med. Marcus Reinke reports on his fi rst implantation of the SP-CL® from LINK with 3D planning
Magazine for Arthroplasty
Issue 2/2018
Affordable high-performance medicineProf. Dr. med. Hanns-Peter Knaebel on customer needs and the future of the healthcare system
»WE ROUTINELY EMPLOY TIBIAL CONES FOR REVISIONS«Prof. Dr. med. Thorsten Gehrke on the advantages of the new TrabecuLink® Tibial Cones from LINK
INTERVIEW
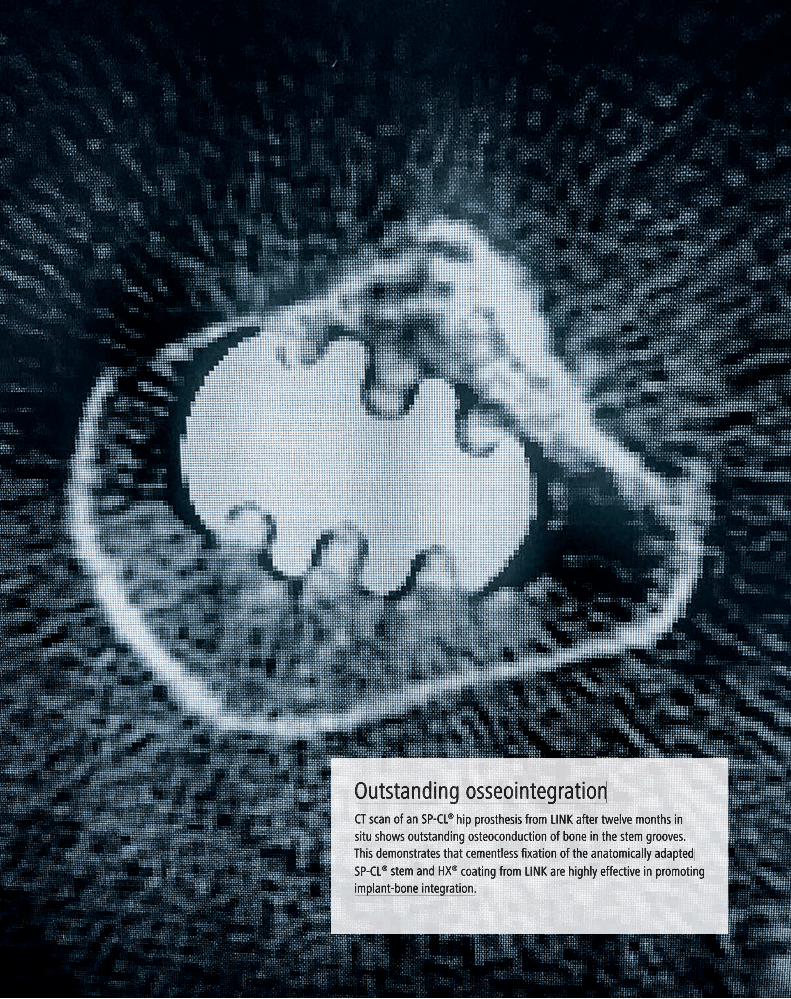
Outstanding osseointegrationCT scan of an SP-CL® hip prosthesis from LINK after twelve months in situ shows outstanding osteoconduction of bone in the stem grooves. This demonstrates that cementless fixation of the anatomically adapted SP-CL® stem and HX® coating from LINK are highly effective in promoting implant-bone integration.
Dear Readers:
Any surgeon who has implanted hip prostheses from American manufacturers will probably have encountered issues of cone corrosion. In the USA, this phenomenon is highly significant because such corrosion can lead to local tissue reactions and even failure of components. This can cause excessive variations in the manufacturing tolerances.*
LINK produces its joint prostheses which exceed the strict specifications laid down by CeramTec for ceramic heads. We use nothing but standard-compliant, high-quality materials, such as cobalt-chrome alloys and titanium, both pure and alloy. You will find more information on the subject of cone corrosion in the abstracts of studies by Mueller and Kretzer et al. and Ninomiya et al. on page 26.
The difference high quality manufacturing processes and materials can mean for your patients is made clear by the case report on a 51-year-old former tumor patient, on page 14. It is therefore, extremely interesting to read what Prof. Dr. med. Hanns-Peter Knaebel has to say about the develop-ment of new technologies, the importance of high quality in medical engineering and the conditions for obtaining regulatory approval of medical devices.
Finally, obtaining regulatory approval is becoming increas-ingly difficult, and LINK has prepared its departments and staff very well for this challenge: LINK has been developing and manufacturing to the required high quality standard for 70 years now – here in Germany.
I hope you enjoy reading this issue of directLINK
Regards,
Helmut D. Link
EDITORIAL
directLINK 2/2018 1
* Ninomiya, JT et al.: What’s New in Hip Replacement; JBJS: September 20, 2017 - Volume 99 - Issue 18 - p 1591–1596; doi: 10.2106/JBJS.17.00704.

»We routinely employ Tibial Cones
for revisions«An interview with Prof. Dr. med. Thorsten Gehrke about the advantages of the
new TrabecuLink® Tibial Cones from LINK
INTERVIEW
2 directLINK 2/2018

INTERVIEW
Prof. Dr. med. Thorsten Gehrke is Medical Director and Head of Department for joint replacement at the Helios ENDO-Klinik in Hamburg, Germany.
directLINK 2/2018 3
Professor Gehrke, the new TrabecuLink® Tibial Cones from LINK differ from other products. Could you explain what these are?TrabecuLink® Tibial Cones from LINK are made of a titanium alloy and have a very open-pored surface, with pores of di�erent sizes. Studies show that titanium is extremely osseointegrative, more so even than tantalum.1 Furthermore, the tibial cones currently on the market are rigid implants, whereas LINK® Tibial Cones are elastic.
Why is that important?Tibial cones are used for restoring defects and for anti-rotational anchorage of knee implants. Elastic cones permit a degree of play, so they are able to adapt well to the bone. TrabecuLink® Tibial Cones can be integrated using the press-fit technique, and their elasticity means that they are constantly pressed against the bone. This mechanism further assists the process of osseointegration.
When do you implant LINK® Tibial Cones?The main indication is revision knee reconstruction, primarily when loosen-ing of the prosthesis is accompanied by a bone defect. In this situation, recement-ing may be problematic. The cones assist in restoration of the defect, providing support for the bone cement, and there-fore allowing the prosthesis rotational stability. These three factors are decisive.Tibial cones are indispensable in modern knee revision surgery.
You were involved in the development of LINK Tibial Cones. How did the idea come about?The idea materialized because we need a certain degree of rotational stability when, for example, we implant prosthe-ses with a stem extension because other-wise they would rotate in their cement mantle and quickly become loose. We also found that substantial defects restored
with allograft do not always function correctly. The reason for this is that the bone used in restoration does not always integrate optimally into the patient’s autochthonous bone due to a lack of pressure.
TrabecuLink® Tibial Cones are specially designed for use with the LINK® Endo-Model®. Why is that?Previously, we often experienced prob-lems because of size di�erences when we implanted other cones in combination with the LINK® Endo-Model® Rota-tional Knee Prosthesis. Consequently, we designed the TrabecuLink® Tibial Cones specifically for use with the LINK®
Endo-Model®.
What are the advantages of TrabecuLink® Tibial Cones, compared to sleeves?The distinction between sleeves and cones is not clearly defined. The purpose of both is essentially the same: namely, to restore a bone defect and provide security against rotation. Cones are employed more in the proximal region of the tibia, whereas sleeves are often located some-what deeper and are more a means of fixation.
INTERVIEW
»In our experience, TrabecuLink® Tibial Cones appear to have an anti-infectious effect.«Prof. Dr. med. Thorsten Gehrke
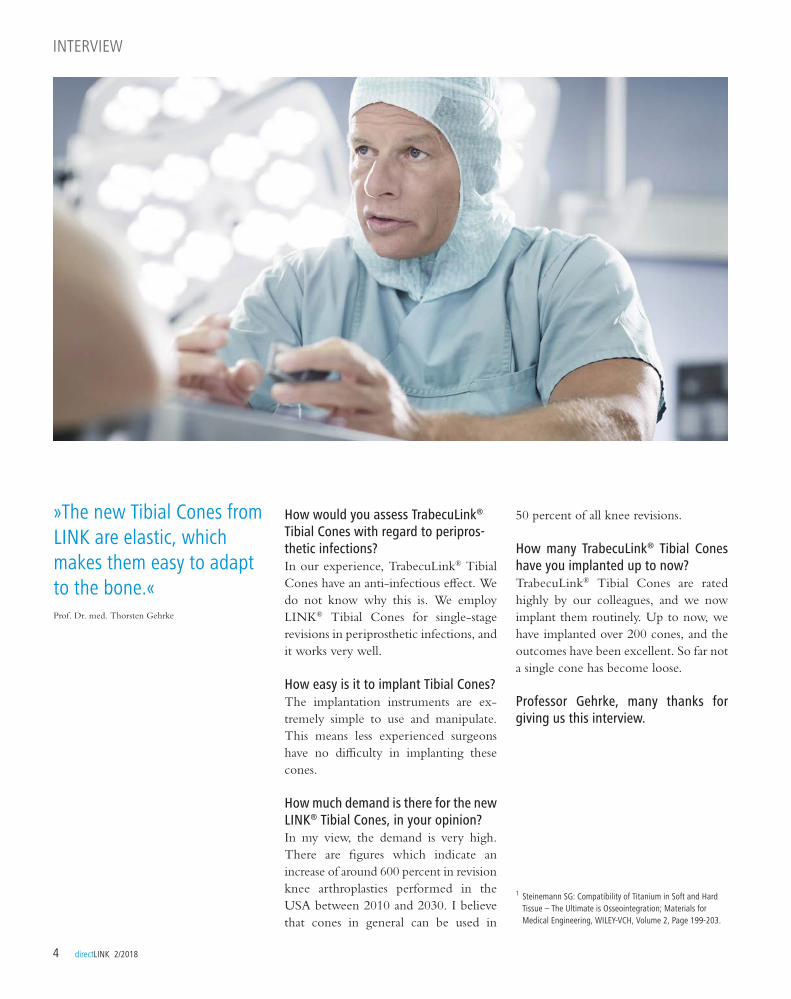
How would you assess TrabecuLink® Tibial Cones with regard to peripros-thetic infections?In our experience, TrabecuLink® Tibial Cones have an anti-infectious e�ect. We do not know why this is. We employ LINK® Tibial Cones for single-stage revisions in periprosthetic infections, and it works very well.
How easy is it to implant Tibial Cones?The implantation instruments are ex- tremely simple to use and manipulate. This means less experienced surgeons have no di�culty in implanting these cones.
How much demand is there for the new LINK® Tibial Cones, in your opinion?In my view, the demand is very high. There are figures which indicate an increase of around 600 percent in revision knee arthroplasties performed in the USA between 2010 and 2030. I believe that cones in general can be used in
INTERVIEW
4 directLINK 2/2018
50 percent of all knee revisions.
How many TrabecuLink® Tibial Cones have you implanted up to now? TrabecuLink® Tibial Cones are rated highly by our colleagues, and we now implant them routinely. Up to now, we have implanted over 200 cones, and the outcomes have been excellent. So far not a single cone has become loose.
Professor Gehrke, many thanks for giving us this interview.
1 Steinemann SG: Compatibility of Titanium in Soft and Hard Tissue – The Ultimate is Osseointegration; Materials for Medical Engineering, WILEY-VCH, Volume 2, Page 199-203.
»The new Tibial Cones from LINK are elastic, which makes them easy to adapt to the bone.«Prof. Dr. med. Thorsten Gehrke

directLINK 2/2018 5
INTERVIEW
Mr Morgan-Jones, you had an advisory role in the development of the TrabecuLink® Tibial Cone? What was your involvement?The TrabecuLink® Tibial Cone had already been designed by Professor Thorsten Gehrke and the LINK team. For me, it was about deciding how useful the cones would be in surgical practice. So I was looking at the sizing, how they would work with LINK implants, and also whether they would be universal in the sense that they could be used with other companies’ products.
Why would that be important?Having used other companies products for many years, the TrabecuLink® Tibial Cones all fi t very well into the tibia. I think they are the only universal cones available.
What do you consider to be the bene-fi ts of the TrabecuLink® Tibial Cone compared to competitor products?A lot of implant manufacturers are pro-ducing tibial cones now. But they pro-duce them in a way which is very specifi c to only their implants. The Tibial Cones from LINK are more universal and can be used with products from di� erent manufacturers.
The TrabecuLink® Tibial Cone is also the fi rst cone which is spring loaded. Why is that signifi cant?Using this cone leads to compression-set bone. Good compression will mean that it’s likely to get more bone ingrowth, be more stable and gives the surgeon a much better reconstruction. You can simply
INTERVIEW
Mr Rhidian Morgan-Jones is a Consultant Orthopedic Surgeon practicing at Spire Cardiff Hospital, Cardiff, UK. He specializes in knee surgery. In addition to his clinical practice, he lectures and publishes research papers regularly. In the development of the TrabecuLink® Tibial Cone he took on an advisory role.
»The TrabecuLink® Tibial Cone is universal and can be used with different products*«
squeeze the little spring at the front of the cone – that is unique and it makes so much sense. If you put it inside the bone, it is going to compress, and that spring allows you to get a perfect tension at the compression site.
Does the TrabecuLink® Tibial Cone bring advantages for the treatment of periprosthetic infections?Yes, indirectly. Because you have to debride properly to remove infected tis-sue, then you have to reconstruct prop-erly. The use of the TrabecuLink® Tibial Cone is a big step forward in this respect. The issue about debriding bone and infected tissue is that you have to be aggressive in order to get every infected bit. Then you’ve got to rebuild it; but if you have this rebuilding option with the cone, you can hopefully get better results with infection because you're not going to be afraid to take more and more bone away because you know you've got to do it. With the cone you can reconstruct well. Before this, you were only thinking about large amounts of cement for recon-struction. This won’t be necessary any longer.
Mr Morgan-Jones, many thanks for this interview.
* The statements in the interview, especially in regard to combining LINK products with those from other manu-facturers, represent the expert medical opinion of the interviewee, and do not constitute a recommendation by LINK (please refer also to the Instructions for Use).

INTERVIEW
6 directLINK 2/2018
»Affordable high-performance medicine remains a major challenge«An interview with Prof. Dr. med. Hanns-Peter Knaebel on the subject of customer requirements, the future of the healthcare system, and what Steve Jobs said about technology development.
Professor Knaebel, you recently became chair and CEO for Medicine at Röchling, the high-performance plas-tics specialists. How do you feel in your new post?Professor Knaebel: It feels good, thank you! To be entrusted with overall responsibil-ity for a company with such a long and distinguished tradition as Röchling is an enormous honor. One strategic focus at
INTERVIEW
Prof. Dr. med. Hanns-Peter Knaebel has been chairman and medical CEO of Röchling SE & Co. KG since 1 January 2018. Before that, he spent eight years as CEO at Aesculap AG and on the Board of B. Braun Melsungen AG, Germany.
Röchling is on expanding the Medical division. I am very familiar with this field, and I am confident we can achieve a great deal here.
What do you regard as the strategic challenges for medical engineering?The digital transformation and a�ordable high-performance medicine are two key challenges. Our aim has to be to utilize

directLINK 2/2018 7
INTERVIEW
»In my view, the healthcare system requires radical reform, but the concept of a centralized health insur-ance fund under which everyone in Germany pays into a single pot cannot be the answer.«Prof. Dr. med. Hanns-Peter Knaebel
the field of medical technology in a tar-geted manner, you first have to under-stand the treatment process and the needs of customers and patients. You must do so quickly, and supply a high-quality product in order to achieve genuine advantages in the market. Companies that succeed in doing this can be very successful – LINK is a good example. Back in the days when I was with Aescu-lap, LINK was already on my radar as an up-and-coming firm. I find it very posi-tive that from such modest beginnings, a business can go on to become a really outstanding medium-sized company.
What is your assessment of the mar-ket authorization hurdles for a firm like LINK?The amendment of the Medical Device Regulation is now complete. But politi-cians are gradually becoming aware that pharmaceutical products and medical devices should be treated di�erently. With a little courage and technical under-standing, the authorities and notified bodies could interpret the regulations in such a way as to promote innovative, quickly available and yet acceptably safe medical technology. If this does not hap-pen, the market will become concen-trated at the expense of small and medium-sized enterprises.
What can patients expect from medi-cal engineering in the next ten years?We will have considerably more e�cient and streamlined treatment processes thanks to automation. Add to this opti-mized visualization in imaging and in the operating room, direct comparison of diagnostic results and assessment of a suc-cessful outcome of planned therapies by direct referencing to database analyses at the place of treatment.
With all this, will it still be the surgeon who takes the final decision?Yes, it will. In fact, the basis on which he makes his decisions will be significantly
better. You could call it evidence-based medicine 2.0. From my point of view, the future of medicine will become so exciting that I sometimes have the desire to be working on the front line again.
If you could be Health Minister for a year, what would you do?First of all, I would ask whether we can and should preserve the current status of our very e�cient healthcare system. In my view, the healthcare system requires radical reform, but the concept of a cen-tralized health insurance fund under which everyone in Germany pays into a single pot cannot be the answer. As I see it, the 30 most common illnesses in Germany should be looked at in rela-tion to the urgency of treatment, together with the acceptable transport times to the next suitable unit. In this way, we can find out which hospitals are needed where geographically, with what facilities and what range of services. This »atlas of Germany« should be discussed with health service providers to establish what services are required where and in what size of hospital.
Then a few brave decisions would no doubt have to be taken.Hospitals that are not »relevant to the sys-tem« should be enabled to transfer to a di�erent task within the healthcare sys-tem. I’m convinced that, in this way, we can future-proof our healthcare system. But a wider intellectual and time horizon are required.
Professor Knaebel, many thanks for this interview.
digital processes to enhance our own business model e�ectively and e�ciently, and to open up new sales opportunities by means of disruptive innovation. Tech-nological innovations must be even more closely attuned to the needs of customers and patients, while still remaining a�ord-able. However, if price was the sole deci-sion-making criteria applied by hospitals’ purchasing departments, this would be short-sighted because key product fea-tures and facets would be overlooked. So it is essential to look beyond the price of a technology when deciding whether or not to invest.
In 1997, Steve Jobs said that a tech-nology has to be »reverse engineered« from the customer’s requirement in order to satisfy this requirement. Does this also apply to medical engineering?For many years, the approach followed in medical engineering was to first develop a technology and then look for a buyer. That’s not the right model for today because the benefit for customer and patient also has to be proven by means of clinical data. If you want to innovate in

8 directLINK 2/2018
INTERVIEW
US surgeons are increasingly implant-ing hinge knees instead of CCKs in revision cases. Why? Dr. Levine: It’s becoming more popular to use the hinge implant because it gives freedom of rotation; the CCK devices al-low almost no rotation at all. And while the hinge devices have been considered overconstrained, now the CCKs are be-ing compared to that standard, and they’re almost overconstrained. Is the increasing popularity of hinge knees in the US more than a trend?People are observing that the longevity of the hinge knee is very similar to, if not better than, that of the CCK. You could
insert a hinge knee and not have to worry about stability – you expect the stability of a hinge knee to be better than that of a CCK. For patients who are seventy-five and older, implanting a hinge knee is a relatively quick and easy way to give them a good knee. In fact, for some older patients, I would choose a hinge knee right away. The long-term CCK survival rates in Europe are around 80%* for ten years. What are the US numbers?American surgeons use the CCK as their workhorse, and they reserve the hinge knee for the next step. But I think that method is going to change because the
»For some older patients, I would choose a hinge knee right away«A conversation with Dr. Brett R. Levine about the increasing popularity among orthopedic surgeons in the USA utilizing hinge knee implants instead of constrained condylar knee (CCK) prostheses in revision arthroplasties.
performance of the CCK in patients who live longer than ten years is not phenom-enal. Also, I think that is the reason why we don’t see any of those reports that show five-year or eight-year results; we don’t see the twelve-year and fifteen-year results because they might not be that great. Poor performance is why people are starting to consider that the rotational constraint of a CCK might not be the best option. Rotational hinge knee prostheses, such as the LINK® Endo-Model®, are said to enable fast, better and less costly treatment for older patients. Can you confirm this?

directLINK 2/2018 9
INTERVIEW
Yes, definitely – at least for our hospital system. The LINK® Endo-Model® comes in at a price point that is very good, particularly for some of the older patients. The nonmodular implant is very low-cost for our system and gives the patient great stability right away. There-fore, he or she doesn’t have to be con-cerned about flexion instability, which is often an issue for certain older patients.
Are the advantages of hinge knees in revision cases similar to those in trauma cases: fast, efficient rehabilita-tion and better clinical results? The advantages of hinge knees in revision cases are similar to those in trauma cases where you proceed directly to a distal femoral replacement. The hinge knee gives patients a quicker and better recov-ery. Obviously, there’s a little more risk involved when you take out part of a pa-tient’s bone, but the advantage of him or her recovering faster seems to be worth it. As long as an infection is prevented, hinge knees also tend to have sustained, good success versus the plating procedure that is used in trauma cases, where a higher rate of nonunion occurs and then results in a subsequent operation.
Some surgeons say that the range of motion with a hinge knee is going to be limited to ninety degrees or less. That’s definitely not the truth, because there are many hinge knees that are flex-ing much more than that. Also, regarding concerns about early loosening, I haven’t observed any instances of that occurring. In fact, certainly with the stems that are o�ered with the LINK® Endo-Model®, the hinge knee fixes well; furthermore, the cost has been competitive, and the lack of the rotational constraint is consis-tent. And last but not least, it’s very easy to implant – easier than a CCK. What is your opinion on the surgical technique for implanting CCKs?With a CCK device, you’re trying to
»Hinge knees also tend to have sustained, good success versus the plating procedure that is used in trauma cases!«Brett R. Levine, M.D., M.S.
preserve the collateral ligaments, because they do help with the flexion and exten-sion gaps. In cases where people are very sti�, you must keep the collaterals, and that makes the surgery a little bit more di�cult. When you release the collaterals with the hinge, it’s so much easier; you could do it in cases where there are muscle flaps and the skin is tenuous. You can alter your incisions and make them even a little bit shorter, if need be. Or you can move them so that you avoid areas of bad skin. The LINK® Endo-Model® is part of an implant family that allows surgeons to go from a simple hinge implant to a distal femoral replacement, and even a total femoral replacement. How valuable is that for your work?With many of the CCK systems, the implant has to fit on the end of the bone well. So you do need to make some cuts and make sure that the fixation at the end of the bone is secure. One more advan-tage of the LINK® Endo-Model® is that there are significant stem options; and with the MEGASYSTEM-C® you can achieve e�ective diaphyseal fixation if needed. Then you have to worry less about how the implant fits on the end of the bone. LINK has an attractive port- folio with the MEGASYSTEM-C® System. I have done cases where we’ve inserted a distal femoral replacement, and then the patient needed a hip replace-ment. We’ve just plugged them in together and created an intermediary total femur, solving a problem that oth-erwise would have required a radical solution, such as removing all of the bone. MEGASYSTEM-C® is an e�ec-tive, comprehensive system that allows us to proceed from a minor revision surgery to the most major revision surgery that we perform.
Dr. Levine, thank you for this interview.
INTERVIEW
Brett R. Levine, M.D., M.S., is an Associate Professor at Rush Univer-sity Medical Center in Chicago, Illinois, USA. His practice is on complex primary and revision hip and knee reconstruc-tions, as well as less invasive total joint replacement surgery.
* Cholewinski P et al. Long-term outcomes of primary constrained condylar knee arthroplasty. Orthop Traumatol Surg Res. 2015 Jun;101(4):449-54. doi: 10.1016/j.otsr.2015.01.020. Epub 2015 May 4.
Camera A et al. Ten-Year Results of Primary and Revision Condylar-Constrained Total Knee Arthroplasty in Patients with Severe Coronal Plane Instability. Open Orthop J. 2015; 9: 379–389. Published online 2015 Aug 31. doi: 10.2174/1874325001509010379.
10 directLINK 2/2018
INTERVIEW
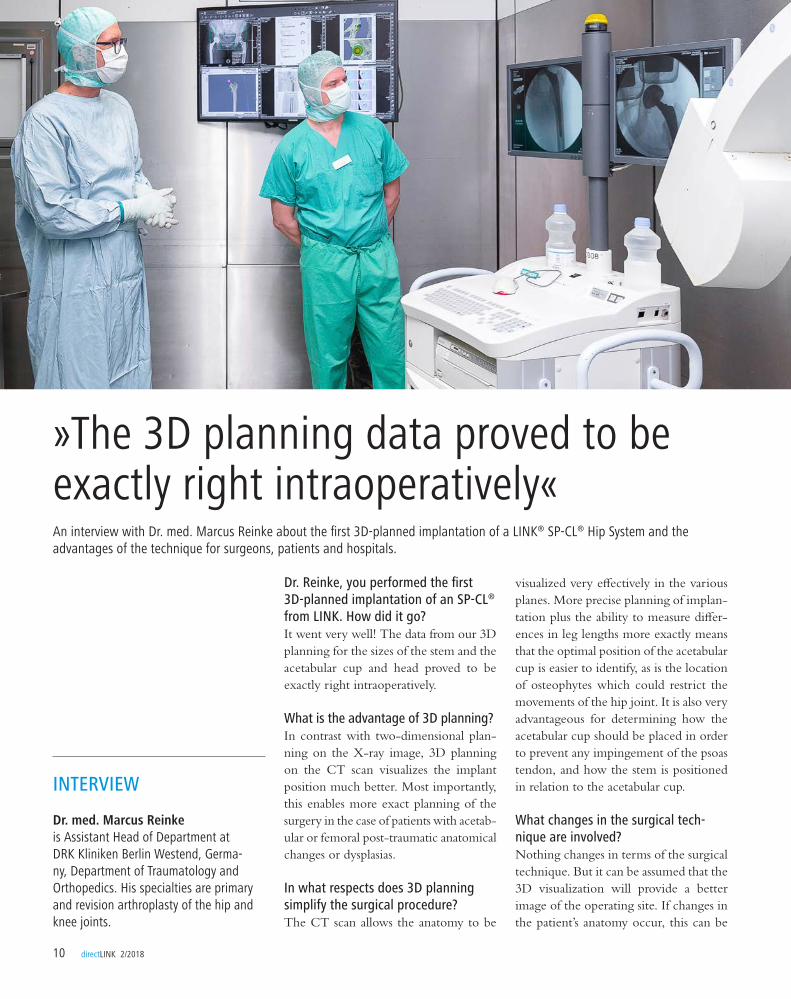
Dr. Reinke, you performed the first 3D-planned implantation of an SP-CL® from LINK. How did it go? It went very well! The data from our 3D planning for the sizes of the stem and the acetabular cup and head proved to be exactly right intraoperatively.
What is the advantage of 3D planning?In contrast with two-dimensional plan-ning on the X-ray image, 3D planning on the CT scan visualizes the implant position much better. Most importantly, this enables more exact planning of the surgery in the case of patients with acetab- ular or femoral post-traumatic anatomical changes or dysplasias.
In what respects does 3D planning simplify the surgical procedure? The CT scan allows the anatomy to be
visualized very e�ectively in the various planes. More precise planning of implan-tation plus the ability to measure di�er-ences in leg lengths more exactly means that the optimal position of the acetabular cup is easier to identify, as is the location of osteophytes which could restrict the movements of the hip joint. It is also very advantageous for determining how the acetabular cup should be placed in order to prevent any impingement of the psoas tendon, and how the stem is positioned in relation to the acetabular cup.
What changes in the surgical tech-nique are involved?Nothing changes in terms of the surgical technique. But it can be assumed that the 3D visualization will provide a better image of the operating site. If changes in the patient’s anatomy occur, this can be
»The 3D planning data proved to be exactly right intraoperatively«An interview with Dr. med. Marcus Reinke about the first 3D-planned implantation of a LINK® SP-CL® Hip System and the advantages of the technique for surgeons, patients and hospitals.
INTERVIEW
Dr. med. Marcus Reinke is Assistant Head of Department at DRK Kliniken Berlin Westend, Germa-ny, Department of Traumatology and Orthopedics. His specialties are primary and revision arthroplasty of the hip and knee joints.
directLINK 2/2018 11
INTERVIEW
What is required for 3D planning?One needs a CT scan, of course. Close consultation with the radiologist is also important. He has to draw up the proto-col for the CT scans in the way that is required for planning.
What will happen next?The first 3D-planned implantation of the SP-CL® was the first step in this direc-tion. If 3D planning with the SP-CL® stem system becomes established, this tool can undoubtedly be used with other implants as well.
Dr. Reinke, many thanks for this interview.
investigated more accurately and appro-priate action taken.
How does 3D planning benefit the patient?Probably a better surgical outcome. But time will tell how much more exact the outcome will be, and whether 3D plan-ning will be able to further improve the already very good outcomes.
Does 3D planning offer any advantages in terms of cost? We expect that implant sizes and types can be predicted much more accurately. This would mean that orders can be placed on the basis of the 3D planning data, thus enabling inventories to mini-mal. Orthopedic departments like to have various types of implants available. If this can be extended to the standard arthroplasty, that would bring a clear cost advantage.
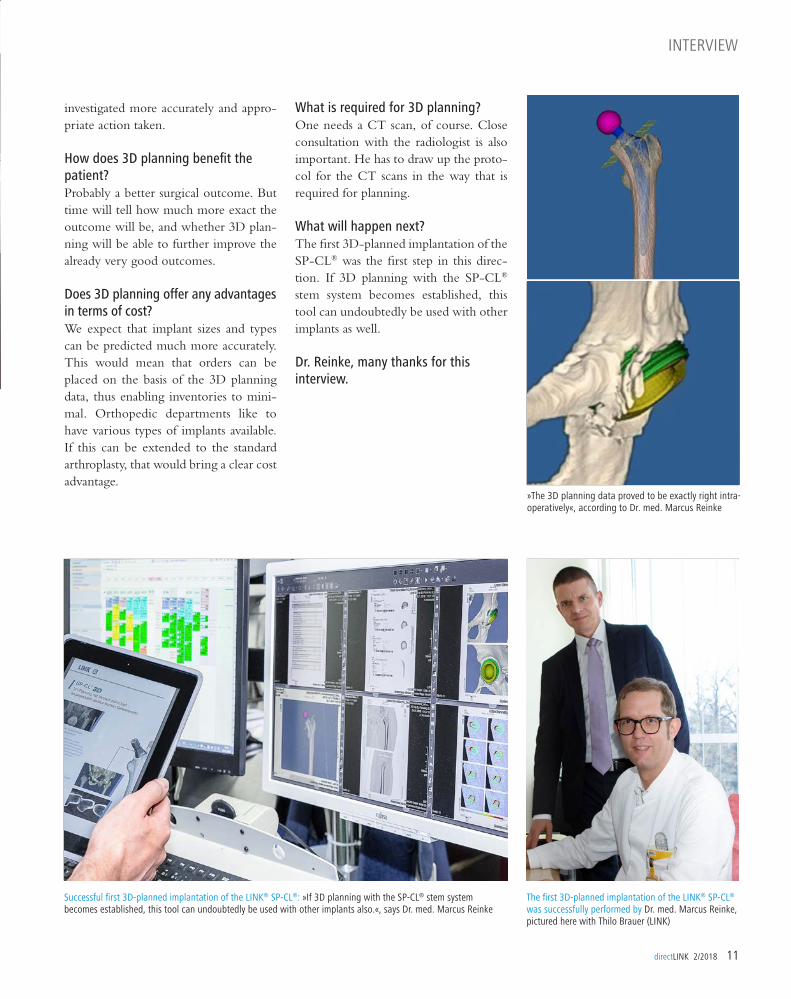
»The 3D planning data proved to be exactly right intra-operatively«, according to Dr. med. Marcus Reinke
The first 3D-planned implantation of the LINK® SP-CL® was successfully performed by Dr. med. Marcus Reinke, pictured here with Thilo Brauer (LINK)
Successful first 3D-planned implantation of the LINK® SP-CL®: »If 3D planning with the SP-CL® stem system becomes established, this tool can undoubtedly be used with other implants also.«, says Dr. med. Marcus Reinke
As the overall number of primary implantations increases, so too does the number of technically demanding revi-sions. These require extremely careful preparation, and also close attention postoperatively: complications such as aseptic loosening and low-grade infection may not be very apparent initially. The consequences can be delayed diagnosis and a delay in beginning the appropriate treatment. Both of these factors can sig-nificantly increase the amount of surgery that is then required.
According to data from the Swedish Register, around 60% of hip revisions are performed because of aseptic loosening, which a�ects the acetabular cup compo-nent approximately twice as often as the stem. Compared to the cemented poly-ethylene inlay acetabular cup, the inci-dence of aseptic loosening has already been reduced considerably by means of modular acetabular cup systems compris-ing a metal back and a polyethylene or ceramic insert.
In the case of cemented acetabular cups for primary and revision cases, there is a choice of either press-fit or screw-in versions, in some cases with optional screw locking for secondary stability. The numerous implants on the market also vary in their surface structure and shape. For press-fit and screw-in acetabular cups
in primary arthroplasties, a 15-year sur-vival rate without loosening of up to 97% is reported.
The first sign of septic or aseptic loosen-ing can be periprosthetic osteolysis, which may be particle-induced or caused by hypersensitivity or biomechanical factors. Dynamic movements in the interface between implant and bone in excess of 50-150 micrometers prevent osseointegration of the implant, and thus lead to loosening and a possible defect.
Clear rules for selecting the revision implant
The choice of treatment in the event of loosening depends on clinical and radio-logical findings; the patient’s state of health, the condition of the joint, the sur- rounding soft tissues, and the in-situ im- plants. If aseptic loosening is confirmed, the bony bed has to be assessed, if necessary with the aid of a CT scan, and then a suit- able revision implant for partial or complete replacement has to be selected. Essentially, the following options are available:
• Exchange with an implant of comparable
size, possibly with additional fixation using
screws, cement or a bone graft
• Exchange with a larger, often modular, revi-
sion implant with bridging of the weakened
bony bed region
12 directLINK 2/2018
PRODUCTS
I. Management of acetabular cup revision
Options for acetabular reconstruction
• Exchange with a revision implant or tumor
implant with resection of the damaged bone
substance
• Arthrodesis or leaving the resection situation
as it is (in individual cases)
Pronounced bone loss can make a revi-sion considerably more di�cult. Ade-quate planning therefore requires classification of the defect situation. Paprosky classification and AAOS classi-fication according to D’Antonio for the acetabular cup are widely used internationally:
• Type I – segmental defects, usually cranial or
ventral
• Type II – cavitary defects with preserved bony
ring
• Type III – combined segmental cavitary de-
fects with preserved pelvic continuity, usually
cranial and ventral
• Type IV – defects with pelvic discontinuity
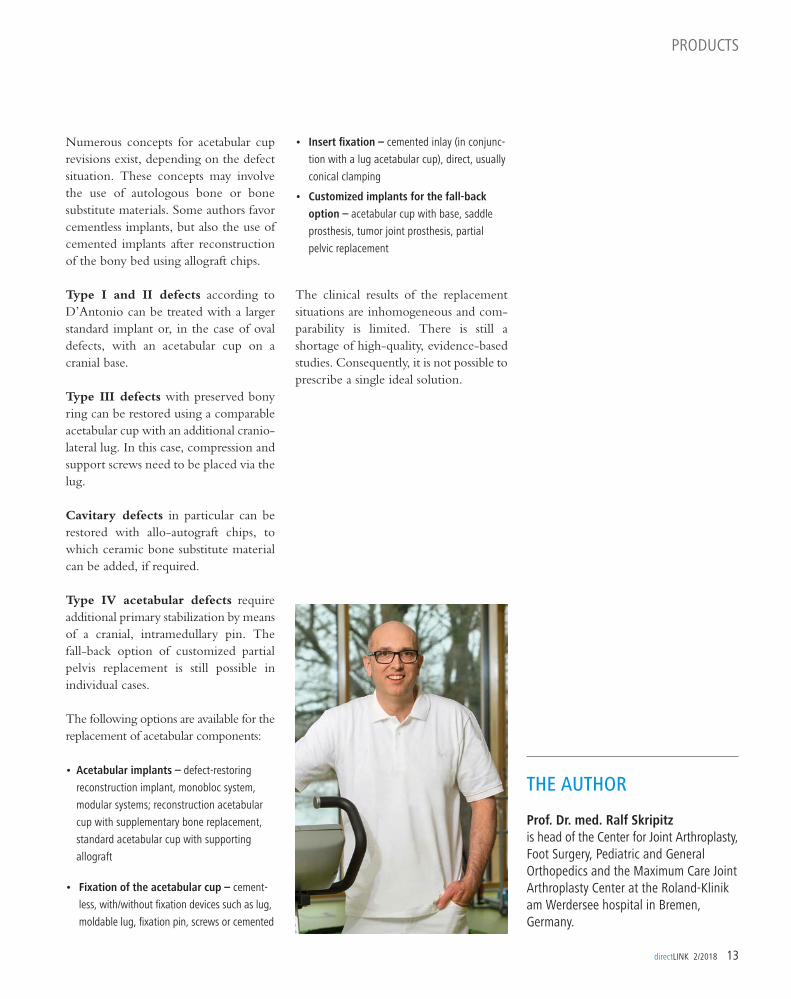
THE AUTHOR
Prof. Dr. med. Ralf Skripitzis head of the Center for Joint Arthroplasty, Foot Surgery, Pediatric and General Orthopedics and the Maximum Care Joint Arthroplasty Center at the Roland-Klinik am Werdersee hospital in Bremen, Germany.
directLINK 2/2018 13
PRODUCTS
Numerous concepts for acetabular cup revisions exist, depending on the defect situation. These concepts may involve the use of autologous bone or bone substitute materials. Some authors favor cementless implants, but also the use of cemented implants after reconstruction of the bony bed using allograft chips.
Type I and II defects according to D’Antonio can be treated with a larger standard implant or, in the case of oval defects, with an acetabular cup on a cranial base.
Type III defects with preserved bony ring can be restored using a comparable acetabular cup with an additional cranio-lateral lug. In this case, compression and support screws need to be placed via the lug.
Cavitary defects in particular can be restored with allo-autograft chips, to which ceramic bone substitute material can be added, if required.
Type IV acetabular defects require additional primary stabilization by means of a cranial, intramedullary pin. The fall-back option of customized partial pelvis replacement is still possible in individual cases.
The following options are available for the replacement of acetabular components:
• Acetabular implants – defect-restoring
reconstruction implant, monobloc system,
modular systems; reconstruction acetabular
cup with supplementary bone replacement,
standard acetabular cup with supporting
allograft
• Fixation of the acetabular cup – cement-
less, with/without fixation devices such as lug,
moldable lug, fixation pin, screws or cemented
• Insert fixation – cemented inlay (in conjunc-
tion with a lug acetabular cup), direct, usually
conical clamping
• Customized implants for the fall-back
option – acetabular cup with base, saddle
prosthesis, tumor joint prosthesis, partial
pelvic replacement
The clinical results of the replacement situations are inhomogeneous and com-parability is limited. There is still a shortage of high-quality, evidence-based studies. Consequently, it is not possible to prescribe a single ideal solution.
CASE REPORT
»Custom-made« LINK®Endo-Model® still completely intact after 26 years in situ
All the technical drawings of cus-tom-made LINK prostheses are held in the LINK archive, including this LINK® Endo-Model®-M Knee Prosthesis implanted in 1991. Spare parts for a sleeve revision are available from stock. Together with the original surgeon, Prof. Dr. med. Martin Salzer, LINK organized the revision procedure for the patient at the Gersthof Orthopedic Hospital in Vienna, Austria, where it was performed by the medical director, Prof. Dr. med. Peter Ritschl.
There, the essentially pain-free patient presented with a flexion deficit in the right knee. The working diagnosis was »a sleeve failure«. Shortly after the patient had presented at the Gersthof Orthope-dic Hospital, she su�ered a fall, resulting in a proximal tibial fracture. For this reason, the planned sleeve revision pro-cedure was brought forward and per-formed in January 2017.
Intraoperatively, the sleeve was found to be intact and, like the associated inlay, displayed scarcely any signs of wear even after 26 years in situ. Therefore, the diagnosed flexion deficit in the right knee, which the patient stated she had experienced for many years, was most likely not due to a mechanical problem. During the further course of the inter-vention, the old, intact sleeve was
THE CASE
A 51-year-old former tumor patient with a cus-
tomized LINK® Endo-Model®-M Knee Prosthesis,
right, in situ for 26 years, contacted LINK on
account of knee instability. An additional prob-
lem was that the surgeon who implanted the
prosthesis had retired, and the hospital where
the operation was performed in 1991 no longer
existed in its original form. Specific data about
the prosthesis was no longer available. Following
a proximal tibia fracture caused by a fall, the
patient feared that she might lose her leg.
removed lege artis, and replaced with a new sleeve. The tibial bone defects incurred in the fall was restored with bone from a bone bank. The patellar tendon was fixated with a screw and stabilized in the proximal tibia by means of two bone anchors.
When the customized prosthesis was implanted in 1991, the tibia was addi-tionally fixated with two screws, whose heads were not countersunk into the tibial plate. This meant that the new inlay supplied by LINK could not be implanted initially. As the two screws were no lon-ger performing any function in terms of tibial stability, they were removed. This produced a smooth tibial surface for implanting the inlay. The in situ Endo-Model®-M Knee Prosthesis was otherwise stable.
»I am now back to my old self, and fully mobile again following the operation and healing of my fractured shinbone«, the patient Manuela Voack reported. »I’m delighted that LINK was able to help me, and that everything worked out perfectly!«
14 directLINK 2/2018
CASE REPORT
directLINK 2/2018 15
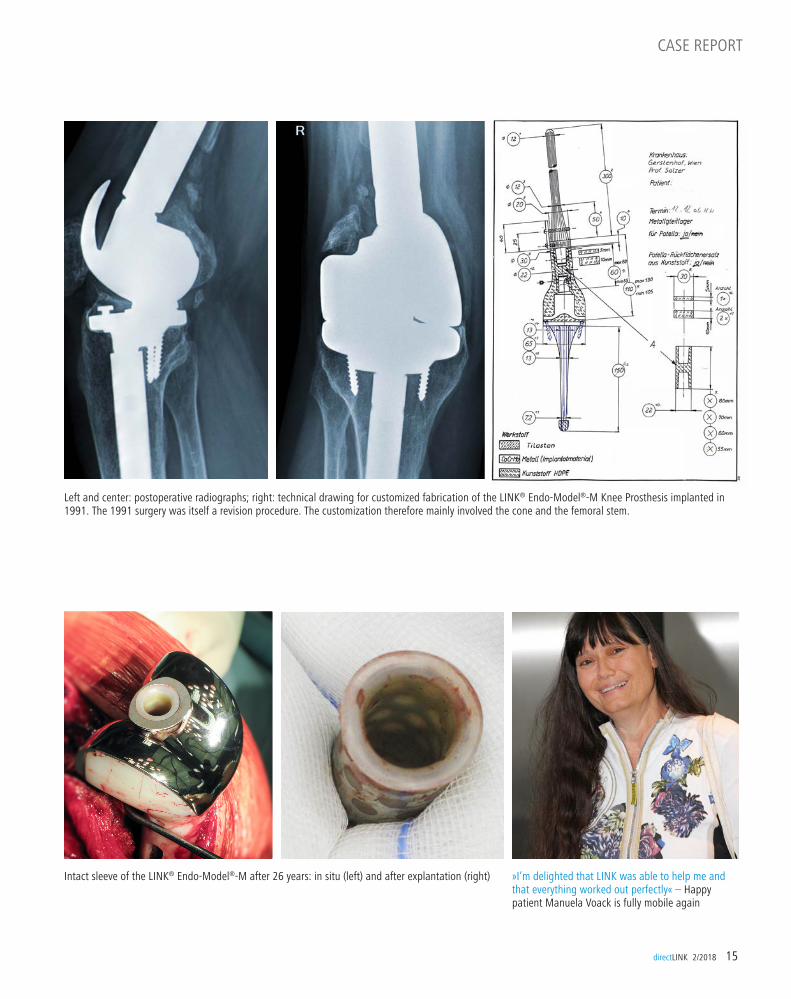
Intact sleeve of the LINK® Endo-Model®-M after 26 years: in situ (left) and after explantation (right) »I’m delighted that LINK was able to help me and that everything worked out perfectly« – Happy patient Manuela Voack is fully mobile again
Left and center: postoperative radiographs; right: technical drawing for customized fabrication of the LINK® Endo-Model®-M Knee Prosthesis implanted in 1991. The 1991 surgery was itself a revision procedure. The customization therefore mainly involved the cone and the femoral stem.

IMPRESSIONS FROM THE
12th International Congress of theChinese Orthopaedic Association
November 15–18, 2017 in Zhuhai, China


18 directLINK 01/2018
INTERVIEW
An interview with Prof. Dr. med. Thorsten Gehrke about the advantages of the new TrabecuLink® Tibial Cones from LINK
Professor Puhl, in 2017 Germany was a guest country at the Congress of the Chinese Orthopaedic Association (COA). You were invited to speak at the opening ceremony. What did that mean to you?Professor Wolfhart Puhl: It meant a great deal to me because it reflects my commit-ment to arthroplasty in China ever since I was first involved in treating a patient there back in 1978. In fact, German arthroplasty and traumatology are fol-lowed with keen interest in China. That’s why, at the COA last November, two full-day German symposia were held for the first time. The growing interest in German arthroplasty that we are
witnessing in China also has a lot to do with the commitment of companies like LINK over a period of many years.
Germany was one of the first guest countries to be invited to the COA congress. Is this a special honor?Norbert Ostwald: Yes, indeed. The hospi-tality extended by the Chinese, and the enormous lengths to which they went to welcome us were amazing. The major players in Chinese orthopedics and trau-matology were there to greet the German delegation. Some of the presentations by German surgeons attracted an audience of over 500, so it was a case of standing room only. The quality of the discussions,
»In China, they value German precision«
INTERVIEW
Prof. Dr. med. Wolfhart Puhl is emeritus professor at the Orthopedic Department of the University of Ulm. Up to 2005 he was Medical Director of the Ulm Rehabilitation Hospital.
Norbert Ostwald is a managing director of Waldemar Link GmbH & Co. KG. He is also one of the directors of the joint venture with the Chinese firm Beijing Power Joint.
An interview with Prof. Dr. med. Wolfhart Puhl and LINK managing director Norbert Ostwald about their commitment to China and the newly established German-Chinese Orthopaedics and Traumatology Association.

directLINK 01/2018 19
INTERVIEW
directLINK 01/2018 19
INTERVIEW
»German arthroplasty is followed with keen interest in China.«Prof. Dr. med. Wolfhart Puhl
which were also followed online by many thousands of Chinese surgeons, was sig-nificantly high due to the audience con- sisting predominantly of top experts from the field of Chinese orthopedics.
How did the invitation to the German delegation come about?Norbert Ostwald: In past years, LINK has been able to build on its friendship with the former president and founder, Prof. Dr. Guixing Qiu, his successor Professor Yan Wang, and the current president Yingzhe Zhang. It was on the basis of this close relationship that Professor Yingzhe Zhang issued the invitation two years ago.
LINK has for many years been very active in the exchange of clinical and scientific knowledge between Chinese and German surgeons. Is this commit-ment being expanded? Norbert Ostwald: Professor Puhl and I were instrumental in the founding of the German-Chinese Association of Orthopedics and Traumatology. In doing so, we created a forum that enables clinical and scientific exchange, shared training, student exchange schemes and fellowships to be organized even more e�ciently; LINK is an industrial partner to the scientific association. In recent years, Professor Puhl has worked extremely hard to bring about the necessary activities, and he has done a superb job as the China represen-tative of the DGOU (German Society for Orthopaedics and Trauma). LINK and its Chinese partners have made sure that
e�ective communication is maintained at all times.
What will be the new associations first project?Professor Wolfhart Puhl: Up to now, the focus of German-Chinese cooperation has been on arthroplasty and traumatol-ogy. But Chinese physicians are also looking to expand their knowledge and skills in the field of pediatric orthopedics, foot surgery and many other areas of orthopedics. The first project will there-fore be to enable German experts to share their knowledge and expertise in these fields with China.Norbert Ostwald: We are able to cover a wide range of subject matter with the new association – an important question will be: In what areas do the Chinese have a requirement for additional train-ing? One example might be optimizing hospital procedures. What LINK can contribute is our personal contacts and the mutual respect that we enjoy. In China, they value German precision in medical matters!
Professor Puhl, Mr Ostwald, many thanks for this interview.
A full house for the opening of COA 2017

20 directLINK 2/2018
The dynamic LINK® Tibial Cones are an attractive solution for cementless resto-ration of bone defects and for providing the prosthesis with additional support if there is bone loss in the proximal tibia. The combination of dynamic design and biocompatible Tilastan®–E is ideal for ensuring stable, permanent fi xation plus successful bone regeneration.
»Several manufacturers now supply tibial cones. But the dynamic e� ect given by the design of the TrabecuLink® Tibial Cone is unique«, explains Helmut D. Link,creative force and joint developer behind TrabecuLink®.
The 3-dimensional TrabecuLink® struturewith its pore size, porosity and structure depth provides an excellent basis for pro-moting osteoconduction and microvas-cularization, also taking into account the structure-covering protein layer (fi bronectin - vitronectin - fi brinogen) required for the bone precursor cells.
LINK® Tibial Cones are combinable with the LINK® Endo-Model® Knee family. The choice of sizes corresponds to the dimensions of the hinged knee prostheses.
TrabecuLink®
• 3-dimensional structure for functional bone integration
• Pore geometry for effective cell ongrowth
• Additive fabrication process for the latest generation of Tibial Cones
The sequence of images (below) shows a pore of the TrabecuLink® structure being fi lled with tissue under in vitro cell culture conditions The fi bronectin laid down by human fi broblasts and continually reorganized over a period of eight days is visible as green fi bers.1
1 Holy et al., PLOSone 2013; https://doi.org/10.1371/journal.pone.0073545, Julius Wolff Institut, Charité - Universitätsmedizin Berlin
The HighlightsTrabecuLink® Tibial Cones
• Reinforcement of tibial, metaphyseal bone defects
• Available in 4 sizes and 4 versions • Proven, biocompatible titanium alloy • Stable – with cementless fi xation • Elastic – due to integral bending axes in
the metal wall• Versatile – for customized solutions
Can be used with all the tibial components of the LINK® Endo-Model® Knee family
PRODUCTS
Stable, Elastic, Versatile: TrabecuLink® Tibial Cones from LINK
to the dimensions of the hinged knee to the dimensions of the hinged knee
NEW:
directLINK 2/2018 21
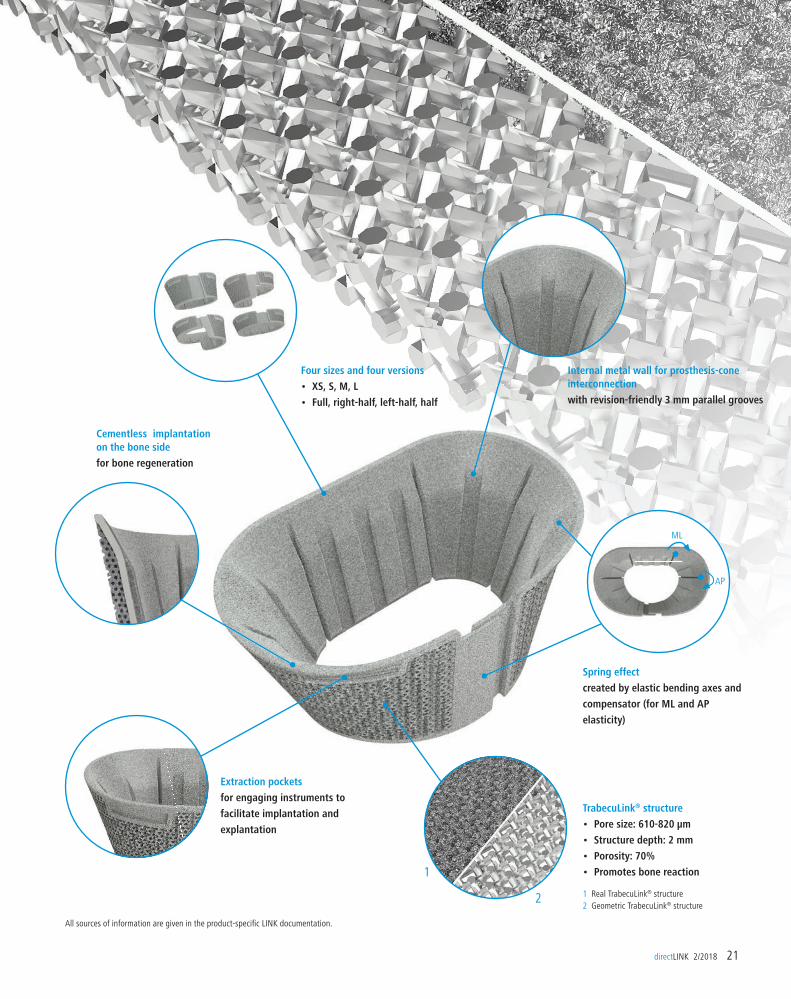
Four sizes and four versions
• XS, S, M, L
• Full, right-half, left-half, half
Cementless implantation on the bone side
for bone regeneration
Extraction pockets
for engaging instruments to
facilitate implantation and
explantation
TrabecuLink® structure
• Pore size: 610-820 µm
• Structure depth: 2 mm
• Porosity: 70%
• Promotes bone reaction
Spring effect
created by elastic bending axes and
compensator (for ML and AP
elasticity)
Internal metal wall for prosthesis-cone interconnection
with revision-friendly 3 mm parallel grooves
1 Real TrabecuLink® structure2 Geometric TrabecuLink® structure
1
2
All sources of information are given in the product-specifi c LINK documentation.
ML
AP

pression of spinal stenoses, and was very impressed by the surgical skills of his German colleagues. Together, they dis-cussed complex cases and exchanged experiences and di� erent approaches.
Motivated by the success of this intercon-tinental exchange, LINKSpine will be organizing more specialist meetings of this kind.
22 directLINK 2/2018
SCHÖLLCHENINTERVIEW
Traumatology of the Elbklinikum hospi-tal in the town of Stade, Germany. »So I was all the more delighted to be able to pass on my knowledge and experience in this very specialised and complex surgical technique to my colleague from the USA.«
Dr. Chaput attended fi ve interventions involving microsurgical decompression of the spinal canal with subsequent fusion. In addition, together with Dr. med. Jan Frischmuth, he held a Biolab workshop for minimally invasive decom-
US spine surgeon on tour of German hospitalsDr. Christopher D. Chaput will shortly becoming head of the Spine Department at the University of San Antonio in Texas, USA. But before taking up the post, the experienced spine surgeon met German colleagues for a mutual exchange of experiences. For a week, Dr. Chaput was the guest of hospitals in Saarlouis, Hamburg and Stade.
Through the close collaboration with LINKSpine, a subsidiary of Waldemar Link GmbH & Co. KG, Dr. Christopher Chaput (top left) has been in close con-tact with German spine surgeons for a considerable time. As a result, he decided to see for himself, the modern surgical techniques employed in Germany. He was especially interested in minimally invasive decompression of spinal stenosis. »Usually it’s the other way round«, says Dr. med. Jan Frischmuth (top right), Head of Department for spinal surgery at the Department of Orthopedics and
Available as MINI (left) for bilat-eral and HEMI (center and right) for unilateral decompression: the new, minimally invasive FacetLINK® Stabilization System for the lumbar spine
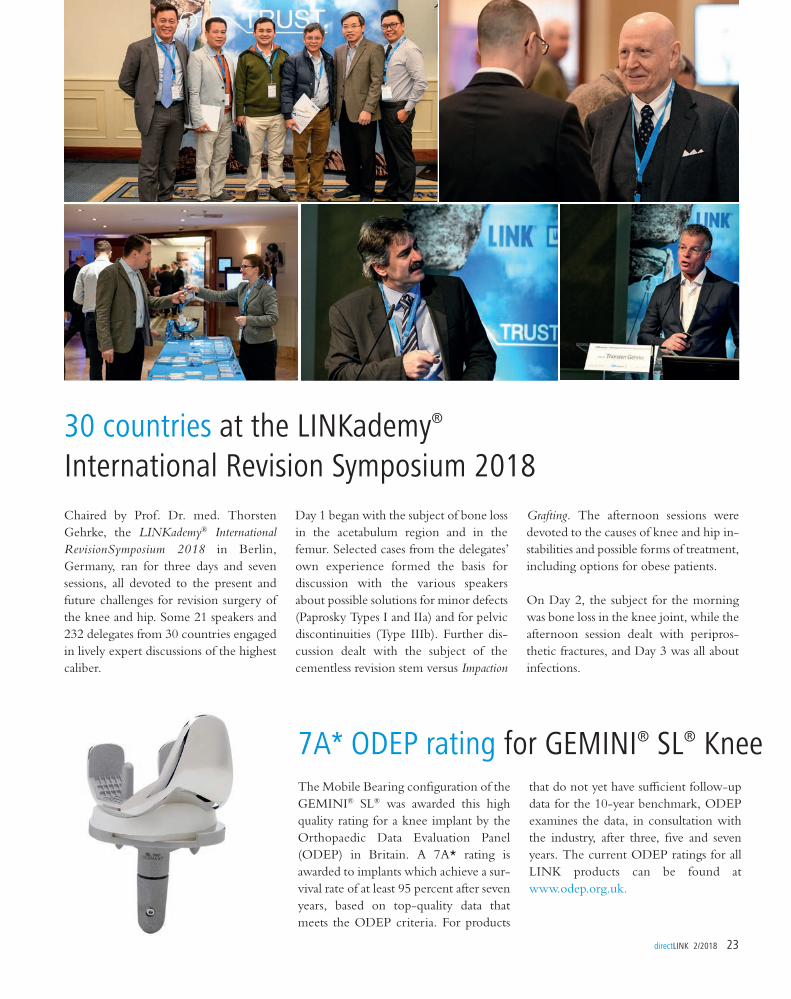
30 countries at the LINKademy® International Revision Symposium 2018
Day 1 began with the subject of bone loss in the acetabulum region and in the femur. Selected cases from the delegates’ own experience formed the basis for discussion with the various speakers about possible solutions for minor defects (Paprosky Types I and IIa) and for pelvic discontinuities (Type IIIb). Further dis-cussion dealt with the subject of the cementless revision stem versus Impaction
Chaired by Prof. Dr. med. Thorsten Gehrke, the LINKademy® International RevisionSymposium 2018 in Berlin, Germany, ran for three days and seven sessions, all devoted to the present and future challenges for revision surgery of the knee and hip. Some 21 speakers and 232 delegates from 30 countries engaged in lively expert discussions of the highest caliber.
7A* ODEP rating for GEMINI® SL® KneeThe Mobile Bearing confi guration of the GEMINI® SL® was awarded this high quality rating for a knee implant by the Orthopaedic Data Evaluation Panel (ODEP) in Britain. A 7A* rating is awarded to implants which achieve a sur-vival rate of at least 95 percent after seven years, based on top-quality data that meets the ODEP criteria. For products
Grafting. The afternoon sessions were devoted to the causes of knee and hip in-stabilities and possible forms of treatment, including options for obese patients.
On Day 2, the subject for the morning was bone loss in the knee joint, while the afternoon session dealt with peripros-thetic fractures, and Day 3 was all about infections.
that do not yet have su� cient follow-up data for the 10-year benchmark, ODEP examines the data, in consultation with the industry, after three, fi ve and seven years. The current ODEP ratings for all LINK products can be found at www.odep.org.uk.
directLINK 2/2018 23
24 directLINK 2/2018
STUDIES
The use of modular joint prostheses such as the LINK® MEGASYSTEMS-C®
following resection of bone metastases is a reliable reconstruction strategy for suitable patients, and the incidence of early complications is exceptionally low. That is the conclusion reached by a study which examined the survival rates of megaprostheses using the MEGASYSTEM-C® for reconstruction following resection of bone metastases.
The study comprised a total of 169 patients, and was conducted from January 2001 to March 2015. Of the
95 female and 74 male patients with an average age of 61 (12-87), 135 (79.9%) underwent a proximal femoral resection. The distal femur was operated on in 24 (14.2%) cases, the proximal tibia in 6 (3.6%), the entire femur in 3 (1.8%), and the intercalar femur in 1 (0.6%). In most cases, metastases from breast tumors (30.8%), kidney tumors (17.8%) and lung tumors (14.2%) were treated.
With an average follow-up of 21 (1-150) months, the authors found an overall sur-vival rate of 99.4% after 1 year, 92.8% after 2 years, and 86.8% after 5 and
Study1: Exceptionally low rate of early complications with LINK® MEGASYSTEM-C®
1 De Gori M et al.: Complications and survival of megaprostheses after resection of bone metastases; J Biol Regul Homeost Agents. 2017 Oct-Dec,; 31 (4 suppl 1):43-50.
10 years. They found 9 (5.3%) cases of mobilization of the proximal femur implant, 3 cases requiring surgical reduc-tion, 2 (1.2%) cases of aseptic loosening of the prosthesis stem, and 2 (1.2%) cases with periprosthetic infections, of which one required a two-stage revision.
Study2, 3: Top stability ratings for stem-head connections of cementless hip prostheses from LINKAccording to Ninomiya et al., fluctua-tions in manufacturing tolerances may be a more important cause of corrosion than hitherto assumed. In the USA, this phe-nomenon plays a major role because eval-uation of the literature indicates that it frequently leads to undesirable tissue reactions and component failures.
When LINK conducted an internal eval-uation of eleven hip stems and cones from several manufacturers, only one of the cones met all the specified tolerances.
LINK produces its joint prostheses to tol-erances that even exceed the specifica-tions laid down by CeramTec for ceramic heads.
These tight tolerances, in combination with LINK’s fabrication quality, produce a reduction in micromovements and therefore greatly minimizes potential friction. Mueller et al. examined several established hip stem-head combinations and confirmed that hip prostheses from LINK achieve top stability ratings.
2 Mueller U, Kretzer JP et al.: Mixing of Head-Stem Com-ponents in Total Hip Arthroplasty; J Arthroplasty. 2017 Nov 1. pii: S0883-5403(17)30959-2. doi: 10.1016/j.arth.2017.10.047.
3 Ninomiya, JT et al.: What’s New in Hip Replacement; JBJS: September 20, 2017 - Volume 99 - Issue 18 - p 1591–1596; doi: 10.2106/JBJS.17.00704.
Publication details Published by: Waldemar Link GmbH & Co. KG · Helmut D. Link · Barkhausenweg 10 · 22339 Hamburg, Germany · Phone.: +49 40 53995-0 · Fax: +49 40 5386929 · E-mail: [email protected]
www.linkorthopaedics.com Editor (responsible): Heike Rasbach · E-mail: [email protected] · Tel.: +49 40 53995-0 Editing/Design: Dr. med. Michael Prang www.michaelprang.de
Photography/Graphics: Stefan Albrecht (Cover, 1–4) · Dr. Massimo Franceschini (inside front cover) · Markus Hertrich (8, 23, 25) · Prof. Dr. med. Hanns-Peter Knaebel (6–7) · LINK (15–17, 19–24, 25,
back cover) Mr Rhidian Morgan-Jones (5) · Dr. med. Michael Prang (10–11, 18) · Sebastian Reich (25) · Dr. med. Markus Reinke (11) · Prof. Dr. med. Peter Ritschl (15) · Fabian Schöllchen (22) · Prof. Dr.
med. Ralf Skripitz (13) Disclaimer: The opinions of the interviewees do not necessarily reflect the views of the publisher. The statements made in the interviews represent the expert medical opinion of
the interviewee, and do not constitute a recommendation on the part of LINK.
NEWS
Mr Reich, LINK was audited by P.E.G.. What does that mean?Sebastian Reich: We audit our suppliers’ quality management systems. In addition, we look at individual production pro-cesses and the material flow in Logistics to ensure its e�ciency. The audit report for LINK brings together the results of these measures: »Very Good, all criteria and requirements are met in full.«
What benefit does an audit bring?The members of our buying association can inspect the supplier audits, and that heightens quality awareness in procurement. At the same time, it enables us to make a decision on whether or not to use a particular supplier on the basis of objective criteria.
Sebastian Reich is deputy-head of Strategic Purchasing at P.E.G. Einkaufs- und Betriebsgenossenschaft eG in Munich, Germany
New LINK distributors in Mongolia
LINK passes audit with »flying colors«How common is it for implant manu-facturers to have themselves audited?The manufacturers are receptive to our audit requests. The rules for marketing authorization of medical devices and the fact of working with the notified bodies mean that external audits have become quite routine for the suppliers. In our case there are many very specific ques-tions, and these often lead to a very constructive discussion.
Mr Reich, many thanks for this interview.
directLINK 2/2018 25
School-leavers on job tour at LINKNine future school-leavers included a visit to LINK on their job tour of di�er-ent companies, and found out about the career options of industrial administrator and industrial mechanic. This familiari-zation visit without the pressure of a job interview, and the associated nerves, resulted in a very relaxing evening. The
LINK has a new distributor in Mongolia. The contract was signed on 1 October 2017 at the LINK factory in Norderstedt, near Hamburg, Germany.
L. to r.: Dr. med. Erdembayar Damdinsuren (Trauma- tologist and orthopedic surgeon, Berlin), Tungalag Tsetsen (Deputy Director Asia Pharma, Mongolia), Bülent Topal (LINK Export Manager), Battsetseg Tsegmid (MonBer Medical Consulting, Mongolia)
job tour has been in existence since 2014. Apart from LINK, many other firms o�er young people the opportunity to find out about interesting careers.
Successful augmentation with TrabecuLink®
Waldemar Link GmbH & Co. KG · www.linkorthopaedics.com · [email protected] · Germany
Additive TrabecuLink® (TL) Manufacturing The TL structure as well as patient-specific customized products are made using our additive manufacturing process. Our design-driven additive manufacturing meets the highest development, implant design and manufacturing requirements. Our production process enables the fabrication of highly complex shapes with structural elasticity comparable to bone. In addition, our technology allows a high degree of individualization for optimal patient care
References (general)1 Cecile M. Bidan, Krishna P. Kommareddy, Monika Rumpler, Philip Kollmannsberger, Yves J.M. Brechet, Peter Fratzl, John W.C. Dunlop. et al.; How Linear Tension Converts to Curvature: Geometric Control of
Bone Tissue Growth; PLoS ONE 7(5): e36336. https://doi.org/10.1371/journal.pone.0036336 (2012)2 Pascal Joly, Georg N. Duda, Martin Schöne, Petra B. Welzel, Uwe Freudenberg, Carsten Werner, Ansgar Petersen, et al.; Geometry-Driven Cell Organization Determines Tissue Growth in Scaffold Pores:
Consequences for Fibronectin Organization; PLoS ONE 8(9): e73545. https://doi.org/10.1371/journal.pone.0073545 (2013)
• Bone reaction-friendly TrabecuLink®
3-dimensional structure 1,2
• 3D printed patient-specific treatment
• Great versatility thanks to highly complex structures and stable elastic shapes







![06 JPK englisch Pötsch final [Kompatibilitätsmodus]](https://static.fdocuments.net/doc/165x107/62e23e0bfd74c60a38691114/06-jpk-englisch-ptsch-final-kompatibilittsmodus.jpg)










