
Dipstick Urinalysis Screening, Asymptomatic Microhematuria, and
6
Robert A. Hiatt2 and Juan D. Ordo#{241}ez Division of Research, Kaiser Permanente Medical Care Program IR. A. HI, and the Department of Medicine Ii. D. 0.1, Kaiser Permanente Medical Center, Oakland, California Received 1 1/1 5/93; revised 4/1 5/94; accepted 4/1 5/94. 1 Presented at Bladder Cancer Hematuria Screening Workshop, Madison, WI, October 1 8-1 9, 1 991 . The research was supported in part by the Northern California Kaiser Foundation Hospitals, Inc., Community Service Program; the Medical Editing department of Kaiser Foundation Research Institute provided editorial assistance. 2 To whom requests for reprints should be addressed, at Division of Re- search, Kaiser Permanente Medical Care Program, 3505 Broadway, 1 3th floor, Oakland, CA 9461 1. Vol. 3, 439-443, July/August 1994 Cancer Epidemiology, Biomarkers & Prevention 439 tuna. Review Dipstick Urinalysis Screening, Asymptomatic Microhematuria, and Subsequent Urological Cancers in a Population-based Sample” Abstract Screening urine for microhematuria as an indicator of serious disease is controversial because of the low positive predictive value of such screening and the costs and risks of the associated evaluation. To further evaluate test properties, we retrospectively examined the outcomes of 20,571 men aged 35 years and women aged 55 years who voluntarily had a Personal Health Appraisal in 1 980 as members of a large prepaid health plan. Hematuria was deteded by dipstick in 876 cases (4.3%); 278 were excluded because of evidence of previous urological disease which could cause hematuria. Review of the medical records of 598 patients with asymptomatic microhematuria as shown by a positive dipstick result indicated that 99% had a follow-up evaluation within 3 months of positive test results for hematuria and had various levels of urological evaluation thereafter. However, urological cancers (2 prostate, i bladder) developed in only 3 patients within the next 3 years. On the basis of San Francisco-Oakland Surveillance, Epidemiology, and End Results program data, rates of urological cancer were evaluated among patients whose test results were negative for hematuria, and these cancer rates were found to be almost the same as the rate among patients with asymptomatic microhematuria. Sensitivity of a single dipstick urinalysis result using microhematuria to indicate urological cancer within 3 years was 2.9%; specificity was 96.7%; and positive predictive value was 0.5%. Multivariate analysis which adjusted for age, gender, and race showed that the relative risk of 2.i (95% confidence interval, 0.7-6.6) for urological cancer was not significantly elevated among patients with asymptomatic microhematuria compared with patients who had negative test results. These findings based on a single test are consistent with the current lack of recommendations for screening for microhematuria among asymptomatic adults. Introdudion Dipstick urinalysis is a simple, quick, and inexpensive method of detecting microhematunia and other urinary ab- normalities (1 ). However, the value of dipstick urinalysis in screening for urological malignancies and other serious diseases of the urinary tract has not been supported by several population-based studies (2, 3), except perhaps in populations aged >60 years (4, 5). Clinicians are concerned about whether an evaluation for microhematunia is justified considering the associated risks: morbidity generated by irradiation (1); potential allergic reactions from iv. pyelo- grams (6); and complications from renal biopsy (7). Further- more, the cost of screening and a complete urinalysis eval- uation for hematunia can be substantial. An estimated $150 million is spent on dipstick urinalysis testing annually in the United States (1 ). However, although about 52,300 cases of bladder cancer and 27,200 cases of kidney and other un- nary cancers were estimated for 1 993 (8), no effective screening measures for these cancers have been found. To find these cases, we would currently test many people to benefit a few (9). Is this approach justified? To date, studies that evaluated dipstick urinalysis for microhematunia reported only the positive predictive value of the test, and no randomized trials or case-control studies of screening have been conducted. Further, only 2 studies, in which a group of patients had negative test results for microhematunia from dipstick screening, followed patients to determine “false-negatives” (1 0, 11 ), and selection fac- tons may have played a role in one of these studies (1 1). We have used a continuing program of screening and health appraisal within a large prepaid health plan to eval- uate the outcomes associated with dipstick screening for microhematunia, including outcomes of patients whose dip- stick tests showed no evidence of microhematuria. We sought to confirm the results of other population-based cohort studies concerning the positive predictive value of the test and to reassess sensitivity and specificity of screen- ing dipstick analysis in this setting. Methods Population. The KPMCP3 is a large prepaid health plan which serves about 30% of the population in the major urban areas of northern California. The age and sex distri- bution of the membership parallels that of the U.S. Census population (i 2), and, on the basis of census block group characteristics analysis, the racial and socioeconomic status of the membership is closely comparable with that of the U.S. Census population except for extremes of income (1 3). 3 The abbreviations used are: KPMCP, Kaiser Permanente Medical Care Program; PHA, Personal Health Appraisal; AMH, asymptomatic microhema- on April 9, 2019. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Transcript of Dipstick Urinalysis Screening, Asymptomatic Microhematuria, and

Robert A. Hiatt2 and Juan D. Ordo#{241}ez
Division of Research, Kaiser Permanente Medical Care Program IR. A. HI,
and the Department of Medicine Ii. D. 0.1, Kaiser Permanente MedicalCenter, Oakland, California
Received 1 1/1 5/93; revised 4/1 5/94; accepted 4/1 5/94.
1 Presented at Bladder Cancer Hematuria Screening Workshop, Madison,
WI, October 1 8-1 9, 1 991 . The research was supported in part by theNorthern California Kaiser Foundation Hospitals, Inc., Community Service
Program; the Medical Editing department of Kaiser Foundation ResearchInstitute provided editorial assistance.
2 To whom requests for reprints should be addressed, at Division of Re-
search, Kaiser Permanente Medical Care Program, 3505 Broadway, 1 3thfloor, Oakland, CA 9461 1.
Vol. 3, 439-443, July/August 1994 Cancer Epidemiology, Biomarkers & Prevention 439
tuna.
Review
Dipstick Urinalysis Screening, Asymptomatic Microhematuria, andSubsequent Urological Cancers in a Population-based Sample”
Abstract
Screening urine for microhematuria as an indicator ofserious disease is controversial because of the lowpositive predictive value of such screening and the costsand risks of the associated evaluation. To furtherevaluate test properties, we retrospectively examined theoutcomes of 20,571 men aged �35 years and womenaged �55 years who voluntarily had a Personal HealthAppraisal in 1 980 as members of a large prepaid healthplan. Hematuria was deteded by dipstick in 876 cases(4.3%); 278 were excluded because of evidence ofprevious urological disease which could causehematuria. Review of the medical records of 598patients with asymptomatic microhematuria as shown bya positive dipstick result indicated that 99% had afollow-up evaluation within 3 months of positive testresults for hematuria and had various levels of urologicalevaluation thereafter. However, urological cancers (2prostate, i bladder) developed in only 3 patients withinthe next 3 years. On the basis of San Francisco-OaklandSurveillance, Epidemiology, and End Results programdata, rates of urological cancer were evaluated amongpatients whose test results were negative for hematuria,and these cancer rates were found to be almost thesame as the rate among patients with asymptomaticmicrohematuria. Sensitivity of a single dipstick urinalysisresult using microhematuria to indicate urologicalcancer within 3 years was 2.9%; specificity was 96.7%;
and positive predictive value was 0.5%. Multivariateanalysis which adjusted for age, gender, and raceshowed that the relative risk of 2.i (95% confidenceinterval, 0.7-6.6) for urological cancer was notsignificantly elevated among patients with asymptomaticmicrohematuria compared with patients who hadnegative test results. These findings based on a singletest are consistent with the current lack ofrecommendations for screening for microhematuriaamong asymptomatic adults.
IntrodudionDipstick urinalysis is a simple, quick, and inexpensivemethod of detecting microhematunia and other urinary ab-normalities (1 ). However, the value of dipstick urinalysis inscreening for urological malignancies and other seriousdiseases of the urinary tract has not been supported byseveral population-based studies (2, 3), except perhaps inpopulations aged >60 years (4, 5). Clinicians are concernedabout whether an evaluation for microhematunia is justifiedconsidering the associated risks: morbidity generated byirradiation (1); potential allergic reactions from iv. pyelo-grams (6); and complications from renal biopsy (7). Further-more, the cost of screening and a complete urinalysis eval-uation for hematunia can be substantial. An estimated $150million is spent on dipstick urinalysis testing annually in theUnited States (1 ). However, although about 52,300 cases ofbladder cancer and 27,200 cases of kidney and other un-nary cancers were estimated for 1 993 (8), no effectivescreening measures for these cancers have been found. Tofind these cases, we would currently test many people to
benefit a few (9). Is this approach justified?To date, studies that evaluated dipstick urinalysis for
microhematunia reported only the positive predictive valueof the test, and no randomized trials or case-control studiesof screening have been conducted. Further, only 2 studies,in which a group of patients had negative test results formicrohematunia from dipstick screening, followed patientsto determine “false-negatives” (1 0, 1 1 ), and selection fac-tons may have played a role in one of these studies (1 1).
We have used a continuing program of screening andhealth appraisal within a large prepaid health plan to eval-uate the outcomes associated with dipstick screening formicrohematunia, including outcomes of patients whose dip-stick tests showed no evidence of microhematuria. Wesought to confirm the results of other population-basedcohort studies concerning the positive predictive value ofthe test and to reassess sensitivity and specificity of screen-ing dipstick analysis in this setting.
MethodsPopulation. The KPMCP3 is a large prepaid health planwhich serves about 30% of the population in the majorurban areas of northern California. The age and sex distri-bution of the membership parallels that of the U.S. Censuspopulation (i 2), and, on the basis of census block groupcharacteristics analysis, the racial and socioeconomic statusof the membership is closely comparable with that of theU.S. Census population except for extremes of income (1 3).
3 The abbreviations used are: KPMCP, Kaiser Permanente Medical CareProgram; PHA, Personal Health Appraisal; AMH, asymptomatic microhema-
on April 9, 2019. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

440 Review: Urological Cancer Screening
Study Population. Patients selected for study were 20,891
members who had a PHA in i 980 at the Oakland on SanFrancisco Kaiser Permanente Medical Centers. Only men
age �35 years and women age �55 years were eligible foranalysis. Women aged <55 years were not evaluated be-cause of the frequency of positive dipstick results frommenstrual bleeding. The PHA included a medical history,routine physical examination, and laboratory evaluation.
The examination is usually performed periodically to estab-lish a baseline of information on a patient’s medical status,
not when the patient is acutely ill. Compared with the totalhealth plan population served by the facilities where thePHA was done, PHA subjects are more highly educated andmore likely to be black (i 2).
Laboratory. Persons taking a PHA were instructed on howto provide a clean catch specimen and were usually fasting.
The dipstick urinalysis obtained as part of the PHA is per-formed on a freshly voided, uncentnifuged sample by using
the Multistix (Ames Co., Miles Inc., Elkhart, IN). Tests wereperformed in the Oakland and San Francisco Medical Cen-ten laboratories within 1 h of voiding. The heme portion ofthe Multistix reacts with hemoglobin to produce a colonwhose intensity is graded as trace, 1 +, 2+, or 3+. The
dipstick can detect hemoglobin concentrations of 0.015-0.062 mg/dl, which equals 5-20 intact erythrocytes/ml.Studies have shown that dipstick testing is 9i to iOO%sensitive and 65 to 99% specific for blood in the urine asshown by microscopy (1).
Data Collection. From a computer-stored file, we selected20,89i persons ages �35 years for men and �55 years forwomen who had a PHA in i980; excluded were 121 per-sons with a previous unological cancer (determined bymatching this file with that of the San Francisco-OaklandSurveillance, Epidemiology, and End Results program forthe 5 contiguous San Francisco Bay Area counties (whichinclude the cities of Oakland and San Francisco). Another19 persons with unusable data were also excluded, whichleft 20,751 study subjects. Persons with a positive dipstickresult of trace or greater were considered to have AMH. Inreporting PHA results, the laboratory did not distinguishbetween trace and 1 +, so we considered trace and 1 + asmild microhematunia, 2+ as moderate microhematunia,and 3+ as severe microhematunia. We then used datarecorded from the PHA questionnaire and from computer-stoned codes of previous hospitalizations to exclude personswith hematunia who had known urinary tract disease, un-nary tract symptoms, or gross hematunia. Finally, medicalrecords from i year before the index urinalysis in i 980 werereviewed to exclude any persons with existing conditionswhich could cause hematunia as defined by Mohr et a!. (2).The conditions included: (a) previously known serious uro-logical disease; (b) urological symptoms of dysunia, ur-gency, fever, weight loss, flank pain, suprapubic discom-fort, evidence of systemic vasculitis, suspect prostate
examination findings, or peniurethral inflammation; (c)other symptoms of retention besides those of stable, benignprostatic hypertrophy; (d) proteinunia, �2+; (e) pyunia,�gnade II; (U serum creatinine level, �2 mg/dl (�i 53 pmol/
liter); (g) documented microhematunia in the previous 2
years; (h) urinary catheter in place or recent catheterizationor instrumentation (�1 week); (i) penimenopausal or post-menopausal bleeding or recent dilation and curettage; and(I) gross hematunia, clots, or hematospermia. This processcreated 3 groups: patients with no hematunia (n = 19,875);
patients with hematunia but with exclusions (n = 278); andpatients with AMH (n = 598).
Records for all 3 groups were linked by a cancer mci-dence file, which is maintained for all health plan members,to identify cancer outcomes from the date of the PHAthrough 1 986. Cancer outcomes in this population wereascertained from the Surveillance, Epidemiology, and EndResults registry supplemented by hospital discharge diag-noses for the entire Northern California Health Plan mem-bership. The records of 598 patients with AMH were re-viewed to determine how the abnormality was followed up,what type of evaluation was done, and what type of uro-logical disease outcomes were recorded. All subsequenturinalysis results were recorded with the type of evaluationassociated with the abnormal urinalysis. Hospital discharge
diagnoses were reviewed and medical records were ab-stracted by an experienced medical record analyst using astandard form. All possible related outcomes which oc-curred before the end of the study period on December 31,1986, were recorded and categorized as minor, moderatelyserious, and serious according to the schema used by Mohret a!. (2, 1 0). These outcomes may not have been directlyassociated with the single episode of microhematunia butwere nevertheless considered as such.
Analysis. Sex-specific cancer rates for each outcome date-gory were calculated on the basis of person-years of fol-low-up in the health plan. End of follow-up was defined aseither the date of an outcome event, the date the patient’shealth plan membership was terminated, or the end of thestudy (December 31 , 1 986). Although we reviewed medicalrecords up to 5 years after index dipstick urinalysis, analyseswere reported for 3 years of follow-up so that results couldbe compared with those from the similar study by Mohr eta!. (2). Relative risks for urological cancer adjusted for age,sex, and race (white, black, Asian, and other) and 95%confidence intervals were determined by using the Coxproportional hazards model for both patients with AMH
and those with hematunia with exclusions compared with
persons with no hematunia (i 4).
Results
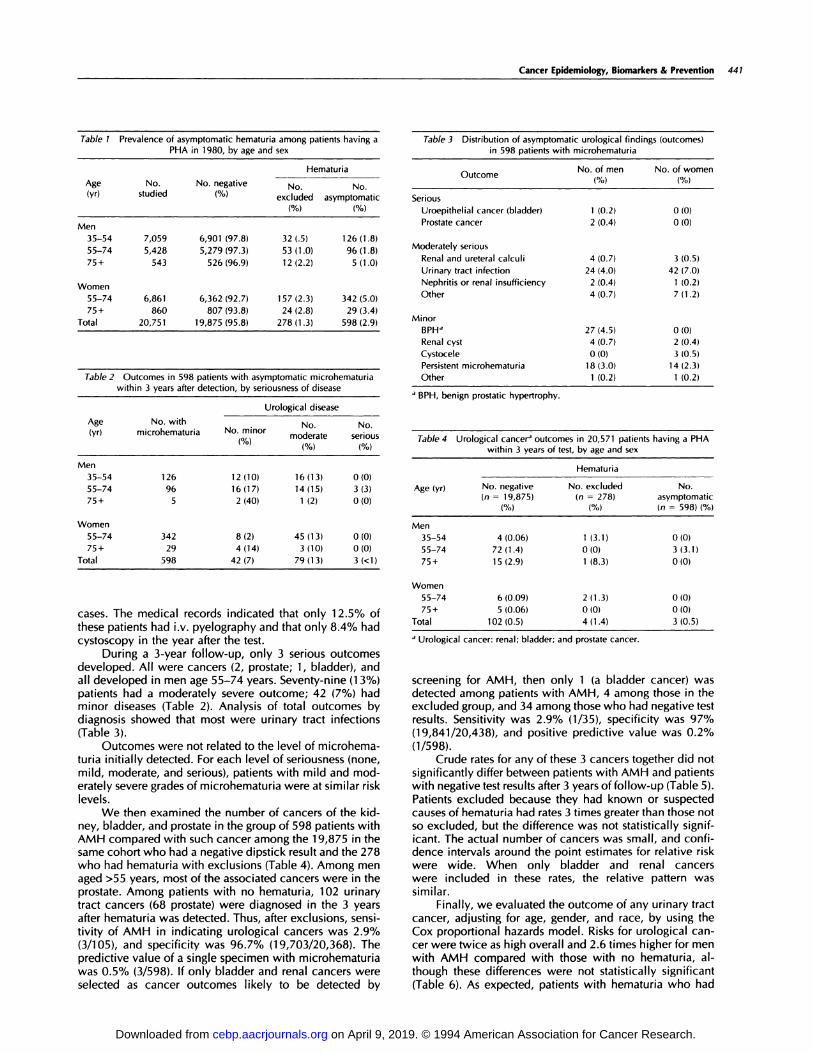
The age and sex distribution ofthe 20,751 patients who haddipstick urinalysis (Table 1 ) indicates that this cohort con-sisted primarily of middle-aged adults. Racial distributionwas either white or Hispanic, 63%; black, 23%; Asian, 7%;and unknown and other races, 7%. The number of patients
age �75 years who received the PHA was small (6.6%), andthe overall frequency of AMH was 2.9%. The racial andethnic distribution of the 598 patients with AMH comparedwith all persons receiving the PHA in the age groups studiedincluded fewer whites and Hispanics (57%), a similar pro-portion of blacks (21%), more Asians (17%), and fewerpatients of other and unknown race (4%). Among the 598patients with AMH, 487 (81 %) had a mild (trace on 1 +)reaction on their dipstick. Moderate reactions (2+) wererecorded for 87 (i 5%), and severe reactions (3+) for 24(4%). Follow-up within the health plan was possible for �3years for 90.8% of those with no hematunia, 91 .0% of thosewith exclusions, and 92.8% of those with AMH. We founddocumentation of a follow-up microscopic urinalysis in themedical record in 99.0% within 3 months after the indexdipstick urinalysis. A doctor’s visit ascertaining the absenceof symptoms was documented within 3 months of the indexurinalysis in 84% and within 6 months in all but 7% of
on April 9, 2019. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Cancer Epidemiology, Biomarkers & Prevention 441
Table 1 Prevalence of asymptomatic hematuria among patients having aPHA in 1980, by age and sex
Hematuria
Age(yr)
No. No. negative No. No.studied (%) excluded asymptomatic
(%) (%)
Men
35-54 7,059 6,901 (97.8) 32 (.5) 126 (1 .8)
55-74 5,428 5,279 (97.3) 53 (1 .0) 96 (1.8)
75+ 543 526 (96.9) 12 (2.2) 5 (1.0)
Women55-74 6,861 6,362 (92.7) 157 (2.3) 342 (5.0)
75+ 860 807 (93.8) 24 (2.8) 29 (3.4)
Total 20,751 19,875 (95.8) 278 (1.3) 598 (2.9)
Table 2 Outcomes in 598 patients with asymptomatic microhematuria
within 3 years after detection, by seriousness of disease
Age(yr)
Urological disease
No. with , No. No.microhematunia No. minor moderate serious
( o) � (0/,,)
Men
35-54 126 12(10) 16(13) 0(0)
55-74 96 16(17) 14(15) 3(3)
75+ 5 2 (40) 1 (2) 0 (0)
Women55-74 342 8 (2) 45 (1 3) 0 (0)
75+ 29 4(14) 3(10) 0(0)
Total 598 42(7) 79(13) 3(<1)
cases. The medical records indicated that only 1 2.5% ofthese patients had i.v. pyelography and that only 8.4% hadcystoscopy in the year after the test.
During a 3-year follow-up, only 3 serious outcomesdeveloped. All were cancers (2, prostate; 1 , bladder), andall developed in men age 55-74 years. Seventy-nine (i 3%)patients had a moderately severe outcome; 42 (7%) hadminor diseases (Table 2). Analysis of total outcomes bydiagnosis showed that most were urinary tract infections(Table 3).
Outcomes were not related to the level of microhema-tuna initially detected. For each level of seriousness (none,mild, moderate, and serious), patients with mild and mod-erately severe grades of microhematunia were at similar risklevels.
We then examined the number of cancers of the kid-ney, bladder, and prostate in the group of 598 patients withAMH compared with such cancer among the 1 9,875 in thesame cohort who had a negative dipstick result and the 278who had hematunia with exclusions (Table 4). Among menaged >55 years, most of the associated cancers were in theprostate. Among patients with no hematunia, i 02 urinarytract cancers (68 prostate) were diagnosed in the 3 yearsafter hematunia was detected. Thus, after exclusions, sensi-tivity of AMH in indicating urological cancers was 2.9%(3/105), and specificity was 96.7% (19,703/20,368). Thepredictive value of a single specimen with microhematuniawas O.S% (3/598). If only bladder and renal cancers wereselected as cancer outcomes likely to be detected by
Table 3 Distribution of asymptomatic urobogical find
in 598 patients with microhematuriaings (outcomes)
No. of menOutcome (0/)
No. of women
(0/)
Serious
Uroepithelial cancer (bladder) 1 (0.2) 0 (0)
Prostate cancer 2 (0.4) 0 (0)
Moderately serious
Renal and ureteral calculi 4 (0.7) 3 (0.5)
Urinary tract infection 24 (4.0) 42 (7.0)
Nephnitis or renal insufficiency 2 (0.4) 1 (0.2)
Other 4(0.7) 7(1.2)
Minor
BPH� 27)4.5) 0(0)
Renal cyst 4 (0.7) 2 (0.4)
Cystocele 0 )0) 3 0.5)
Persistent microhematunia 18 (3.0) 14 (2.3)
Other 1 (0.2) 1 (0.2)
a BPH, benign prostatic hypertrophy.
Table 4 Urological cancer’ outcomes in 20,571 patients having a PHAwithin 3 years of test, by age and sex
Hematuria
Age (yr) No. negative(n = 19,875)
(%)
No. excluded(n = 278)
(%)
No.asymptomatic(n = 598) (%)
Men
35-54 4(0.06) 1 (3.1) 0(0)
55-74 72(1.4) 0(0) 3(3.1)
75+ 15(2.9) 1 (8.3) 0(0)
Women55-74 6(0.09) 2(1.3) 0(0)
75+ 5(0.06) 0(0) 0(0)
Total 102(0.5) 4(1.4) 3(0.5)
a Urobogical cancer: renal; bladder; and prostate cancer.
screening for AMH, then only i (a bladder cancer) wasdetected among patients with AMH, 4 among those in theexcluded group, and 34 among those who had negative testresults. Sensitivity was 2.9% (1/35), specificity was 97%(19,841/20,438), and positive predictive value was 0.2%(1/598).
Crude rates for any of these 3 cancers together did notsignificantly differ between patients with AMH and patientswith negative test results after 3 years offollow-up (Table 5).Patients excluded because they had known on suspectedcauses of hematunia had rates 3 times greater than those notso excluded, but the difference was not statistically signif-icant. The actual number of cancers was small, and confi-dence intervals around the point estimates for relative riskwere wide. When only bladder and renal cancerswere included in these rates, the relative pattern wassimilar.
Finally, we evaluated the outcome of any urinary tractcancer, adjusting for age, gender, and race, by using theCox proportional hazards model. Risks for urological can-cer were twice as high overall and 2.6 times higher for menwith AMH compared with those with no hematuria, al-though these differences were not statistically significant(Table 6). As expected, patients with hematunia who had
on April 9, 2019. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

442 Review: Urological Cancer Screening
Table 5 Urobogical cancer rates among patients having a PHA during
3 years of follow-up
Crude rate/i 000 person-years (95% Cl�)
. AsymptomaticNegative Excluded
hematunia
Men 2.2 (1 .8-2.7) 6.2 (0.7-22.5) 4.0 (0.8-1 1.7)
Women 0.5 (0.2-0.8) 3.3 (0.4-1 i .8) 0 (0-0)
Total 1 .5 (1 .3-1 .9) 4.3 (1 .2-i 1 .0) 1 .5 (0.3-4.4)
.,dl, confidence interval.
Table 6 Relative risk of urological cancer in 3 years after
microhematunia�’
Relative risk (95% Cl)
Asymptomatic. . Exclusion vs.
microhematunia vs.. negative
negative
Men 2.6 0.8-8.3) 1 .9 (0.5-7.7)
Women 9.6(2.0-46.5)Total 2.1 (0.7-6.6) 3.1 (1.1-8.5)
.,Adjusted for age, race, and (for total) sex. CI, confidence interval.
exclusions had a significantly greater chance of unologicalcancer developing in the next 3 years (relative risk, 3.1,95% confidence interval, 1.1-8.5).
Discussion
These results suggest that the probability of detecting seni-ous urinary tract disease with a single screening dipstickurinalysis is small. Specifically, AMH occurred in 2.9% ofthis population of men aged �35 years and women aged�55 years, and urinary tract cancers of the kidney, bladder,and prostate occurred in 0.5% of persons with AMH duringa 3-year period. The proportion of persons with seriousurinary tract disease found among persons with AMH wasnot statistically significantly different than that found amongthe remainder of the cohort in whom no hematunia wasdetected.
A comparable large population-based study of AMHalso found a low rate of serious disease (1.8%) (2). In arecent case-control comparison in the same population,serious disease was found in i .2% of persons with AMHand 0.2% of persons who had negative test results, a smallbut significant difference (P = 0.04) (10). However, otherstudies of selected or referred populations have yieldedhigher rates of both hematunia and associated malignancy(1 , 4, 1 1 , 1 4-1 7). Data on the benefits of screening fromsuch studies must be evaluated with an appreciation of theeffect of selection and referral bias.
Are the current results aberrant, or do they representthe prevalence of urinary tract cancer in a general popula-tion more accurately than has been reflected by the bio-medical literature in English to date? First, the study popu-lation consisted of adult members of a prepaid health planand may have been healthier than the general populationalthough demographically comparable (12, 13). However,other studies have found that KPMCP members who have aPHA have rates of cancers (i8) and inflammatory bowel(i9) and renal disease (12) similar to rates in the generalpopulation, and substantial difference between their healthand the health of the general population is unlikely.
Second, the rate of AMH was 2.9%. Although substan-tially less than the 21 % reported among volunteer men aged�50 years in Wisconsin (20) or the 20% reported from
Leeds, England (21 ), both after multiple screenings, our rateis comparable with other population-based studies (22-24).However, in the population-based study most comparablewith ours, the rate was 1 3% (2) as determined from micro-scopic examination of a spun urine sediment and when �1erythrocyte/high-powered field was defined as hematunia.The younger age of our subjects relative to that in otherstudies could partially explain the lower prevalence ofAMH in our study. However, in this population we did notobserve the expected increase in the prevalence of AMHwith age. Mohr et a!. (2) also noted no age-related increasein the prevalence of AMH. Within the KPMCP PHA popu-lation, we examined the overall frequency of hematuniawithout any exclusion from 1 978 through 1 985 and foundthat the percentage ranged between 3.2 and 9.0%; themean of 4.9% suggested that 4.3% (in 1980) was not anextreme value in this population.
A third factor for comparison was the proportion ofpatients with AMH who had serious disease. We found 3patients (0.5%) (all men) in whom cancer developed duringthe 3-year follow-up period. None of our patients had poly-cystic kidney disease, hydronephrosis, or renal cancer, al-though 7 had renal or ureteral calculi, a serious findingaccording to other schemata used (2). We were uncertainwhether detection of hematunia had led to diagnosis in 2 ofthe 3 patients. Our finding is comparable with the Roches-ten, Ml, study (2) finding of 1 4 patients (1 .8%) with neopla-sia associated with hematunia but is less than the 3 to 6%derived from studies of male volunteers for urine screening(1 , 1 1 , 20, 21 ) which included complete unological evalu-ation of most subjects. If we restrict our evaluation to the101 men �55 years old in our study, 3% had seriousoutcomes (i.e., cancers), or a level of cancer comparable tothat found in the more intensively investigated subjects instudies restricted to olden men (1 1 , 20, 21). Thus, we be-lieve the incidence of unological cancer in our cohort isreasonably comparable with that found in other popula-tions, especially when restricted to men over age 55. Be-cause we assume that cancers of the urinary tract whichcause hematunia would become apparent within 3 yearsand that our detection of cancers in the KPMCP populationis nearly complete, the thoroughness of the evaluation isless relevant in this retrospective analysis of cancer out-comes. Even when we extended our analysis to includedata from a 5-year follow-up, our findings did not changesubstantially.
In summary, we believe that our data are compatiblewith those of the available population-based studies andthat differences with other investigations exist principallybecause of the selected on referred nature of their popula-tions.
The level of sensitivity of AMH for indicating urinarytract neoplasia depends on outcome data from a compara-ble population of patients who had negative test results forhematunia (1, 10). Our data show low sensitivity at 2.9%;
i.e., after excluding patients with known reasons for hema-tuna, 1 05 cancers of the urinary tract developed during the3-year follow-up screening, but only 3 cancers occurred inpatients who had AMH as detected by dipstick. Prostatecancer is less prone to bleed than renal or bladder cancer,but the sensitivity of dipstick urinalysis in detecting the 35renal and bladder cancers which developed during the next
on April 9, 2019. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 443
3 years was the same as that in detecting prostate cancer-2.9% (1/35). Ofcourse, because urological cancer-inducedhematuria is intermittent (4), sensitivity could be increasedby doing repeated dipstick or microscopic unmnalyses (1 1,20, 21 ), although repeating the procedure would producemore false-positive results and lower specificity. We couldnot evaluate this approach in our retrospective study. How-ever, 595 of our 20,368 (2.9%) patients with no cancer hadhematunia which resulted from a source which was notlife-threatening, according to our definition and that ofMohr et a!. (2). These patients may be unnecessarily sub-jected to full-scale urological evaluations and their resultantadverse effects and costs. Recommendations to instituterepeated testing are likely to produce small gains in sensi-tivity of cancer detection but would increase the size of thisfalse-positive population substantially and should, there-fore, be considered carefully.
Our results suggest that no change should be made inthe current recommendation against screening asymptom-atic adults for microhematunia (1 ). Perhaps screening can bemade sufficiently more sensitive and specific by requiringrepeated positive results in a given period, but our data donot help to answer this question. Technical advances arenecessary to produce a more accurate screening test whichwould reduce the morbidity and the cost of urological
evaluation for hematunia. Nonionic contrast media, al-though more costly, lower the risk of fatal reactions (25).Using bladder cytology with hematunia screening has beensuggested (2i). In some populations at especially high risk,such as chemical workers and other occupational groups,more intensive screening may be justified (26).
More complete studies that quantitatively assess risksand benefits of urological evaluation are needed (9). Ourstudy provides insufficient data to make an informed nec-ommendation on the appropriate indications for full-scaleurological evaluation. However, we believe that the lowprobability offmnding patients with treatable life-threatening
lesions must be weighed against the risk of diagnostic eval-uation (1). Our limited conclusion supports those (1, 27)who believe that full urological evaluation should not berecommended for persons with a single positive dipstickscreening test for microhematunia.
AcknowledgmentsWe appreciate the useful comments of Dr. Edward Messing.
References1 . Woolhandler, S., Pels, R. J., Bor, D. H., Himmelstein, D. U., andLawrence, R. S. Dipstick urinalysis screening of asymptomatic adults for
urinary tract disorders: 1. hematunia and proteinunia. JAMA, 262: 1214-
1219, 1989.
2. Mohr, D. N., Offord, K. P., Owen, R. A., and Melton, L. J., Ill. Asymp-
tomatic microhematunia and urobogic disease: a population-based study.JAMA, 256:224-229, 1986.
3. Bard, R. H. The significance of asymptomatic microhematuria in women
and its economic implications: a ten-year study. Arch. Intern. Med., 148:2629-2632, 1988.
4. Messing, E. M., Young, T. B., Hunt, V. B., Emoto, S. E., and Wehbie, J. M.
The significance of asymptomatic microhematuria in men 50 or more yearsold: findings of a home screening study using urinary dipsticks. I. Urol., 137:919-922, 1987.
5. Britton, j. P., Dowell, A. C., and Whelan, P. Dipstick haematunia and
bladder cancer in men over 60: results of a community study. Br. Med. J.,
299: 1010-1012, 1989.
6. Witten, D. M. Reactions to urographic contrast media. JAMA, 231:974-
977, 1975.
7. Cault, H., and Muehrcke, R. C. Renal biopsy: current views and contro-versies. Nephron, 34: 1-34, 1983.
8. Boring, C. C., Squires, T. S., and Tong, T. Cancer statistics, 1993. Cancer
J. dIm., 43: 7-26, 1993.
9. Kassirer, J. P. The wild goose chase and the elephant’s relevance (edito-nab). JAMA, 256: 256-257, 1986.
10. Mohr, D. N., Offord, K. P., and Melton, L. J. Isolated asymptomatichematunia: a cross-sectional analysis of test-positive and test-negative pa-tients. J. Cen. Intern. Med., 2: 318-324, 1987.
1 1 . Messing, E. M., Young, T. B., Hunt, V. B., Wehbie, J. M., and Rust, P.Urinary tract cancers found by homescreening with hematunia dipsticks inhealthy men over 50 years of age. Cancer (Phila.), 64: 2361-2367, 1989.
1 2. Hiatt, R. A., and Friedman, C. D. The frequency of kidney and urinarytract diseases in a defined population. Kidney Int., 22: 63-68, 1982.
1 3. Knieger, N. Overcoming the absence of socioeconomic data in medical
records: validation and application of a census-based methodology. Am. I.
Public Health, 82: 703-710, 1992.
14. The PHCLM Procedure. In: SAS Institute, Inc. SUCI Supplemental
Library User’s Guide, Ed. 5, pp. 437-466, Cary, NC: SAS Institute, 1986.
1 5. Carson, C. C., III, Segura, J. W., and Greene, L. F. Clinical importance of
microhematunia. JAMA, 241: 149-150, 1979.
16. Ritchie, C. D., Bevan, E. A., and Collier, S. J. Importance of occulthematunia found at screening. Br. Med. J., 292:681-683, 1986.
17. Carter, W. C., Ill, and Rous, S. N. Cross hematunia in 110 adult urobogichospital patients. Urology, 18: 342-344, 1981.
1 8. Hiatt, R. A., Friedman, C. D., Bawol, R. D., and Ury, H. K. Breast cancer
and serum cholesterol. I. NatI. Cancer Inst., 68: 885-889, 1982.
1 9. Hiatt, R. A., and Kaufman, L. Epidemiology of inflammatory boweldisease in a defined Northern California population. West. J. Med., 149:
541-546, 1988.
20. Messing, E. M., Young, 1. B., Hunt, V. B., Roecker, E. B., Vaillancourt,
A. M., Hisgen, W. J., et al. Home screening for hematunia: results of a
multiclinic study. J. Urol., 148: 289-292, 1992.
21 . Bnitton, J. P., Dowell, A. C., Whelan, P., and Harris, C. M. A community
study of bladder cancer screening by the detection of occult urinary bleed-ing. J. Urol., 148: 788-790, 1992.
22. Alwall, N., and Lohi, A. A population study on renal and urinary tractdisease: II. Urinary deposits, bacteniunia and ESR on screening and medical
examination of selected cases. Acta Med. Scand., 194: 529-535, 1973.
23. Clark, T. W., Schor, S. S., Elsom, K. 0., Hubbard, J. P., and Elsom, K. A.The periodic health examination: evaluation of routine tests and procedures.Ann. Intern. Med., 54: 1209-1222, 1961.
24. Chen, B. T. M., Ooi, B. S., Tan, K. K., and Lim, C. H. Comparative studiesof asymptomatic proteinunia and hematunia. Arch. Intern. Med., 134: 901-905, 1974.
25. Katayama, H., Yamaguchi, K., Kozuka, T., Takashima, T., Seez, P., and
Matsuura, K. Adverse reactions to ionic and nonionic contrast media: areport from the Japanese Committee on the Safety of Contrast Media. Radiol.,
175: 621-628, 1990.
26. Mason, T. J., and Vogler, W. J. Bladder cancer screening at the DuPontChambers Works: a new initiative. J. Occup. Med., 32: 874-877, 1990.
27. Sutton, J. M. Evaluation of hematuria in adults. JAMA, 263: 2475-2480,1990.
on April 9, 2019. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
1994;3:439-443. Cancer Epidemiol Biomarkers Prev R A Hiatt and J D Ordoñez sample.and subsequent urological cancers in a population-based Dipstick urinalysis screening, asymptomatic microhematuria,
Updated version
http://cebp.aacrjournals.org/content/3/5/439
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/3/5/439To request permission to re-use all or part of this article, use this link
on April 9, 2019. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from


















