
DIPG - The Cristian Rivera Foundation · • 7 children with DIPG / 8 healthy adults ... ASL . Not...
96
DIPG Biopsy technique S. PUGET Hopital Necker, Paris Barcelone 2012
Transcript of DIPG - The Cristian Rivera Foundation · • 7 children with DIPG / 8 healthy adults ... ASL . Not...
DIPG
Biopsy technique
S. PUGET Hopital Necker, Paris
Barcelone 2012

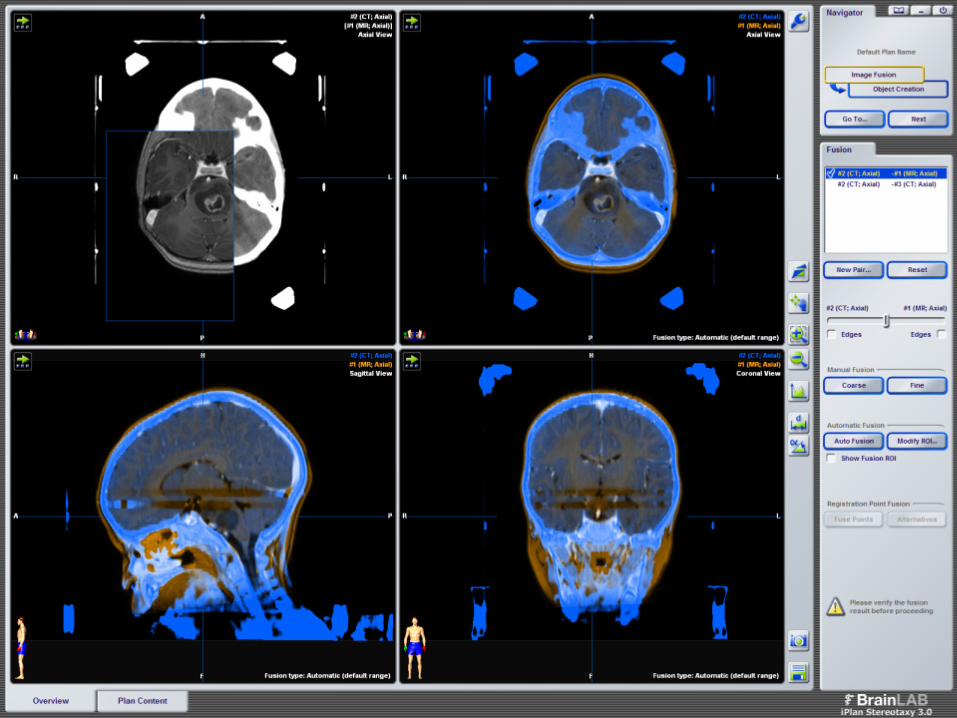
Image Guidance
• Frame-based (stereotactic)
• Frame less (neuronavigation) – No indication for DIPG yet…..
Stereotaxy
• Stereo " tridimensional " and taxis "arrangement »
• Reach any part of the brain with pinpoint accuracy (less than one thousandth of a degree)
• Use of cartesian coordinates
• 2 elements:
– Stereotactic atlas / image-guided
– Stereotactic apparatus
Stereotactic Frame
• Form of a cube or a sphere
• Attached to the patient’s skull
• Coordinates in the 3 axes of space
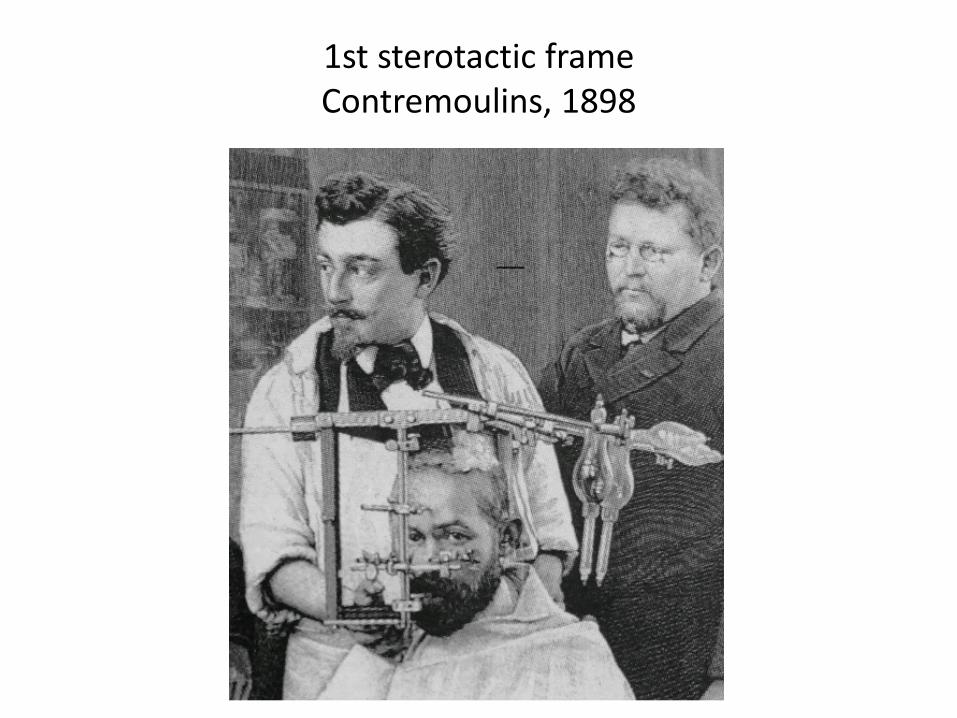
1st sterotactic frame Contremoulins, 1898
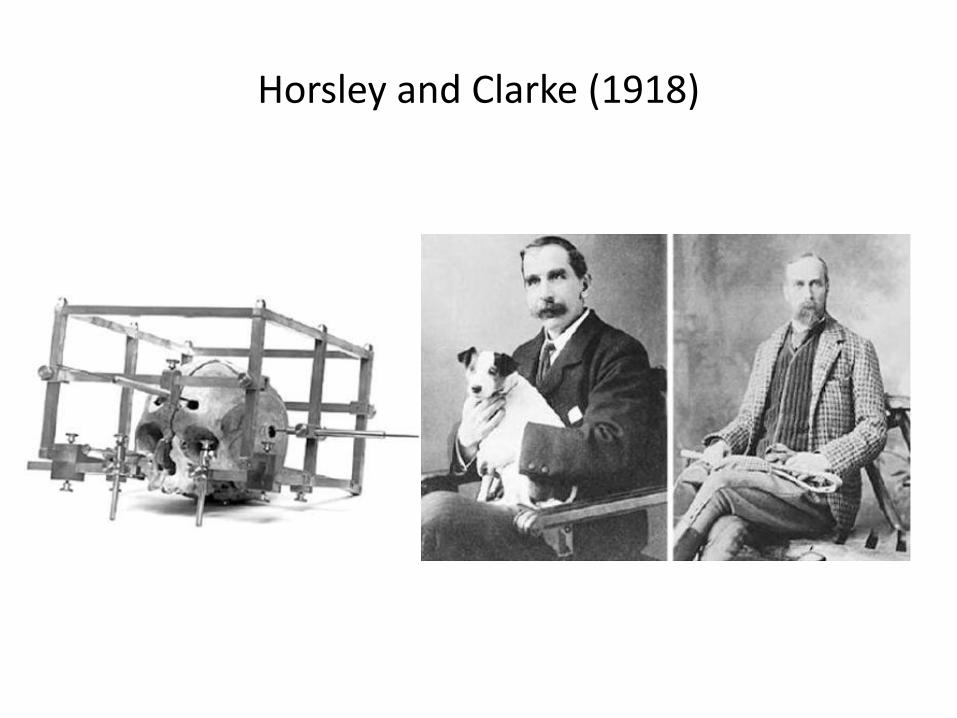
Horsley and Clarke (1918)
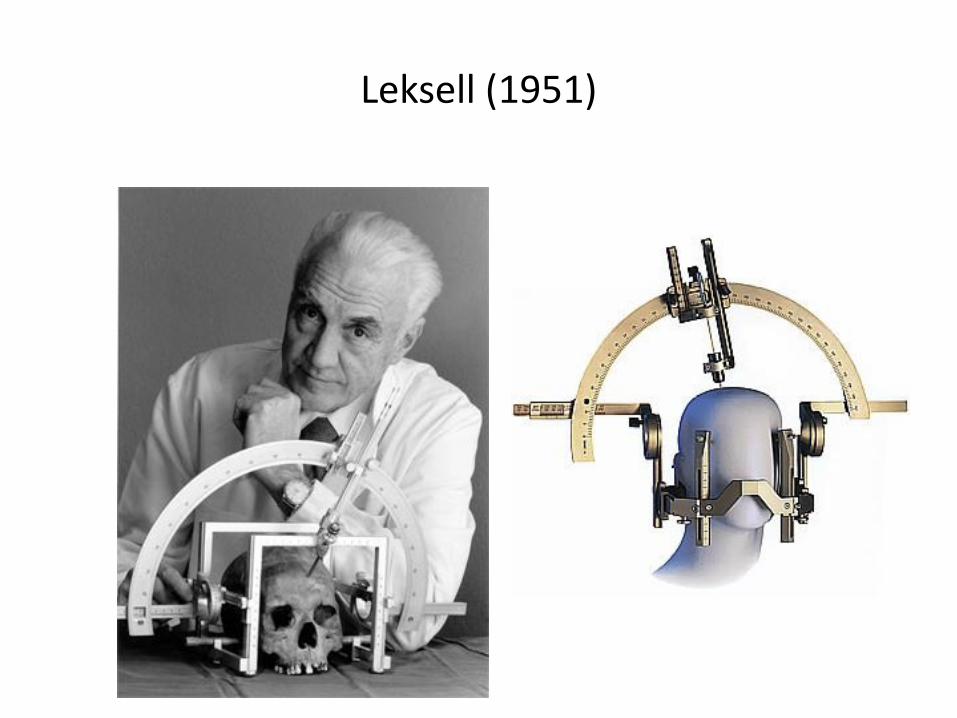
Leksell (1951)
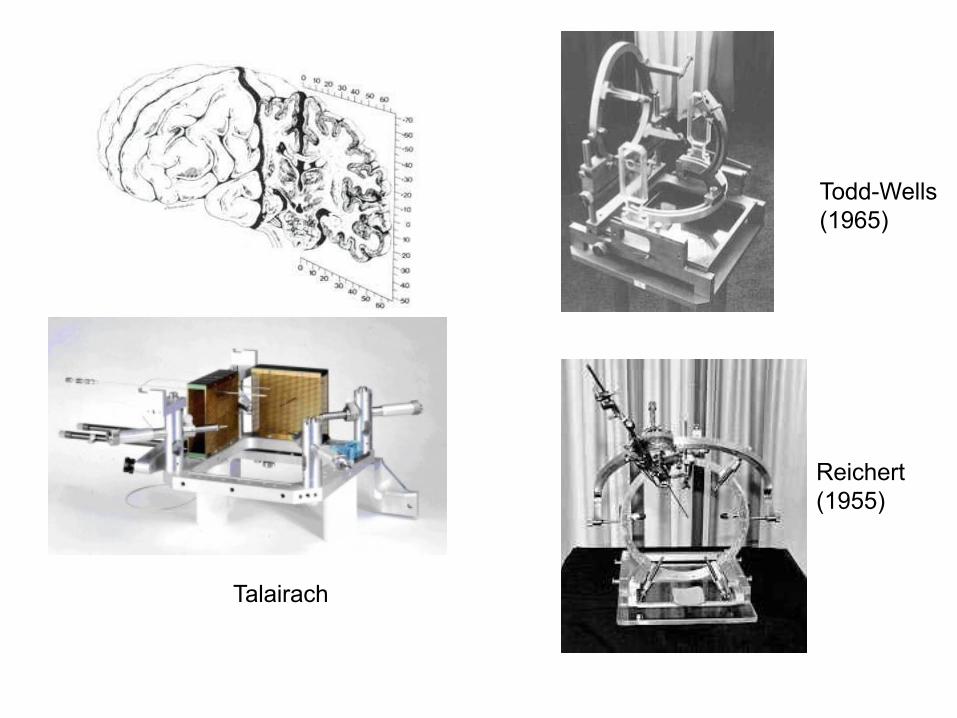
Talairach
Todd-Wells (1965)
Reichert (1955)
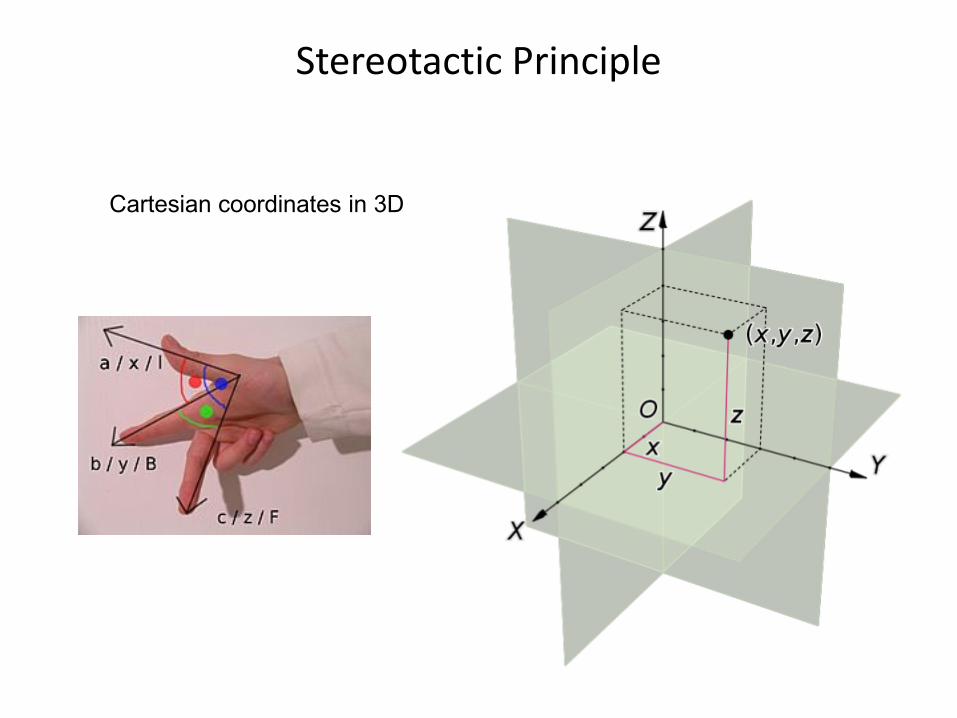
Stereotactic Principle
Cartesian coordinates in 3D
Stereotactic Procedure
• Local or general anesthesia
• The device is fixed to the skull
• Stereotactic coordinates (entry point & targets)
• Needle placed according the coordinates to reach the target
• Allows to: – Tissue sample
– Remove fluid
– Inject fluid
– Radiosurgery
– Functional Neurosurgery
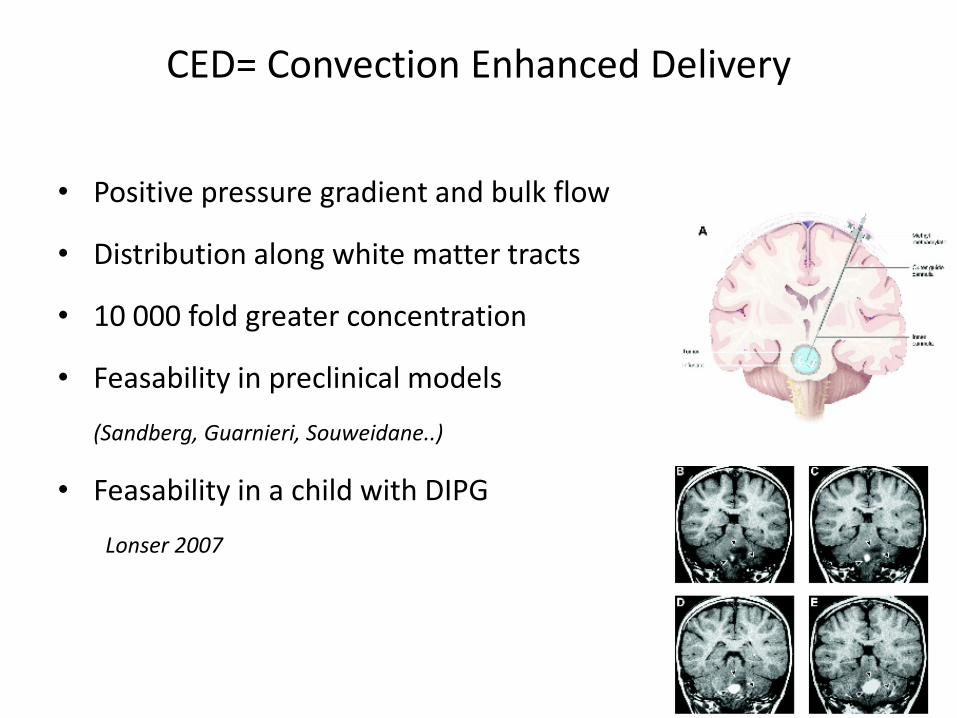
CED= Convection Enhanced Delivery
• Positive pressure gradient and bulk flow
• Distribution along white matter tracts
• 10 000 fold greater concentration
• Feasability in preclinical models
(Sandberg, Guarnieri, Souweidane..)
• Feasability in a child with DIPG
Lonser 2007
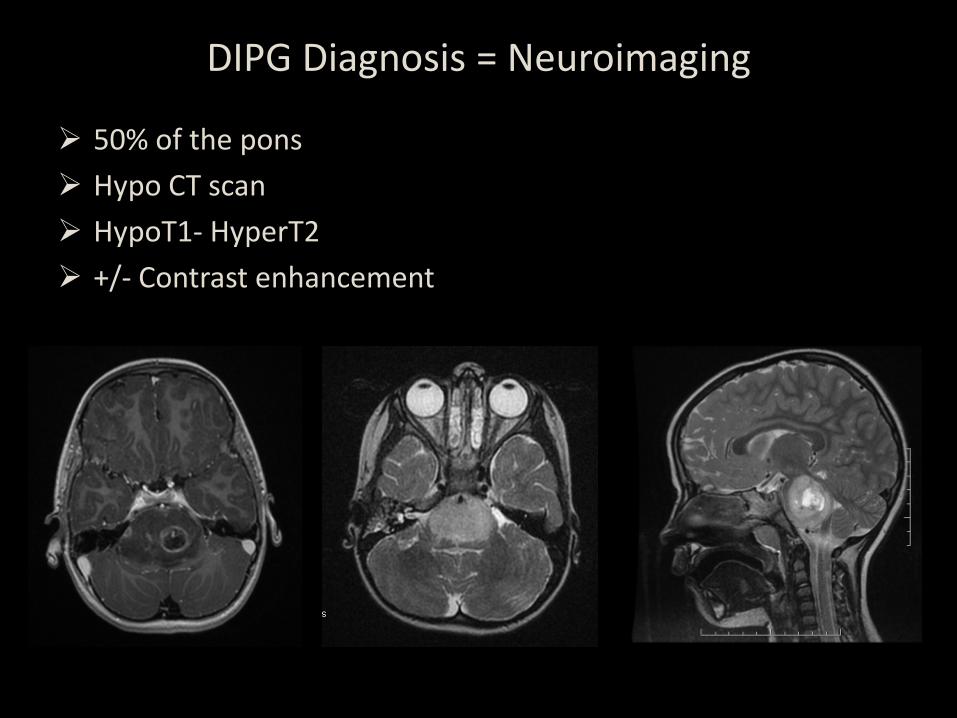
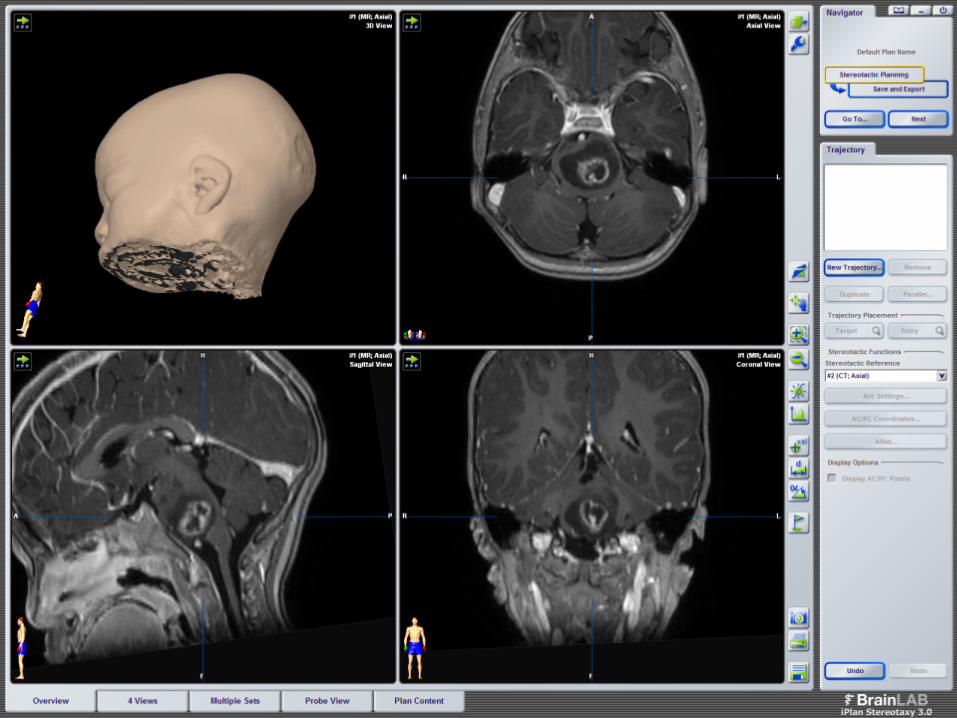
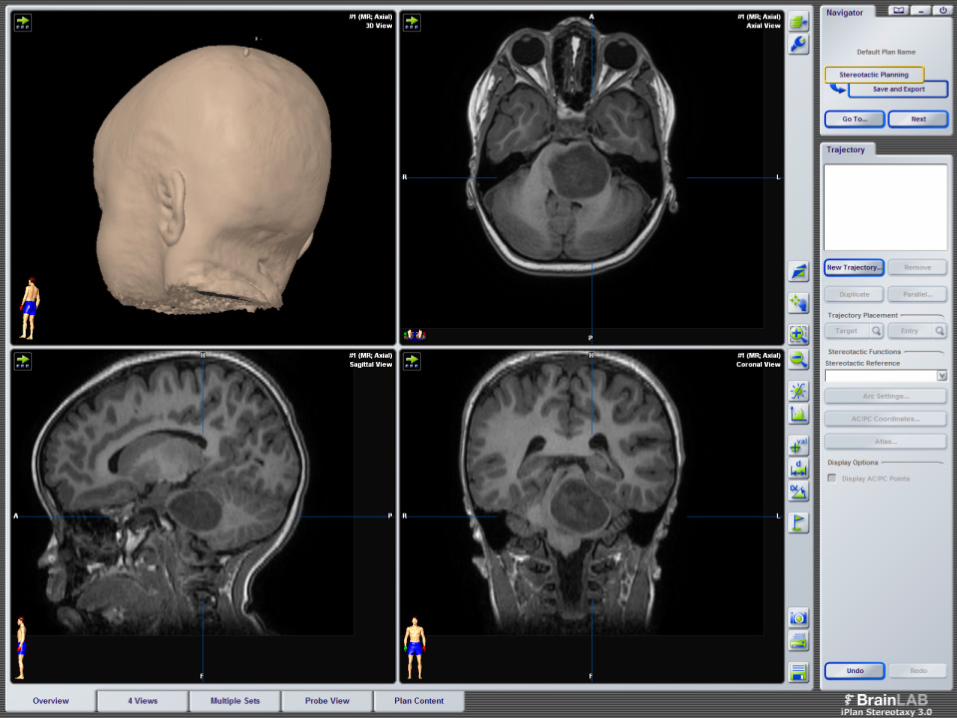
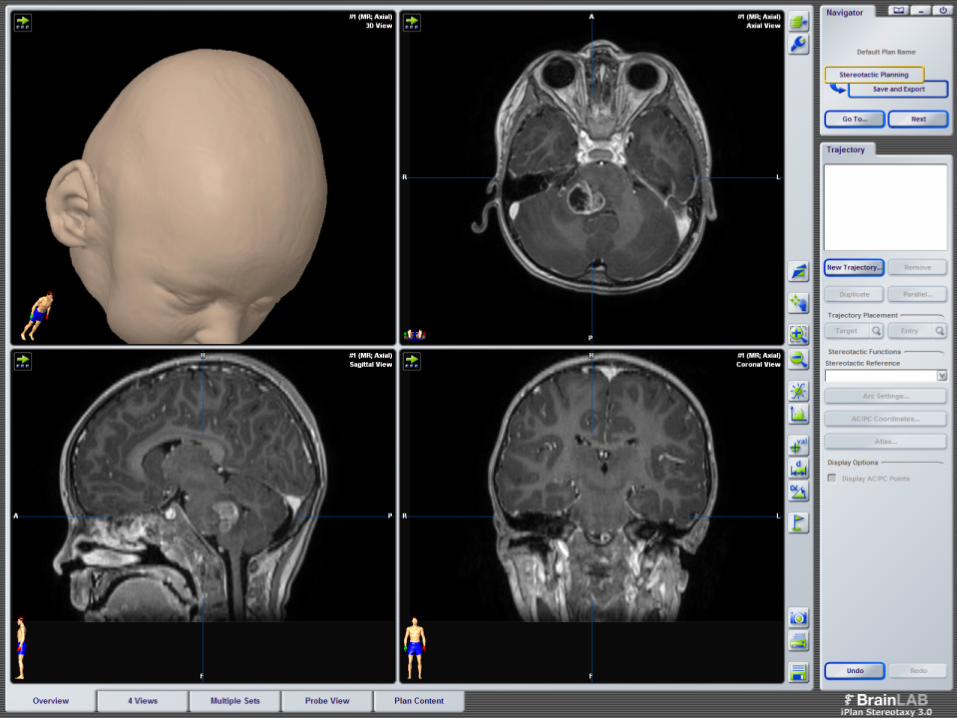
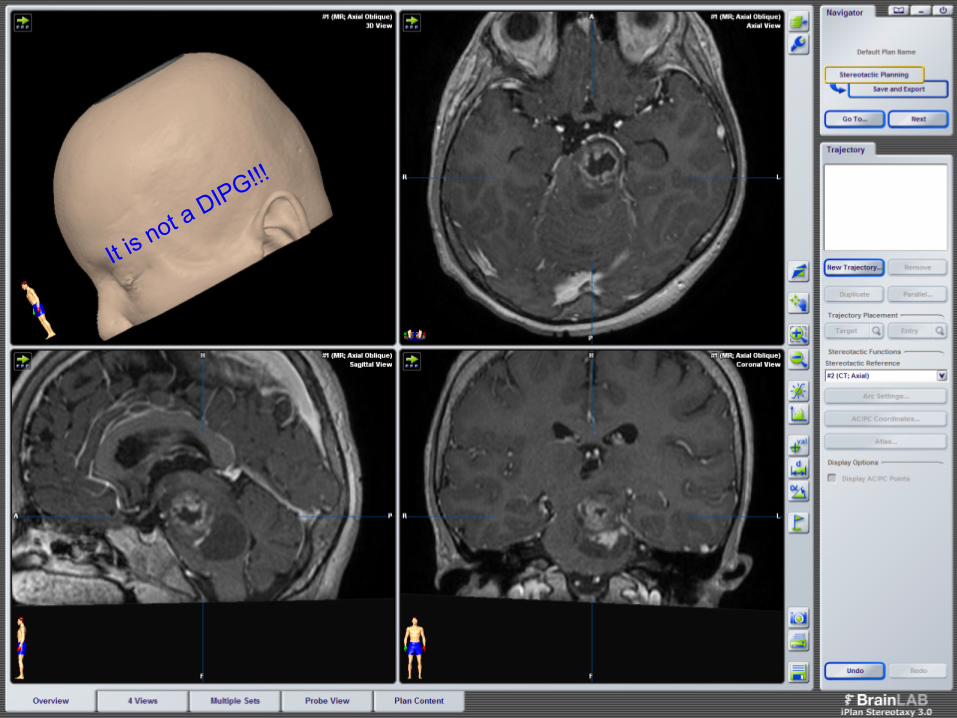
DIPG Diagnosis = Neuroimaging
50% of the pons Hypo CT scan HypoT1- HyperT2 +/- Contrast enhancement
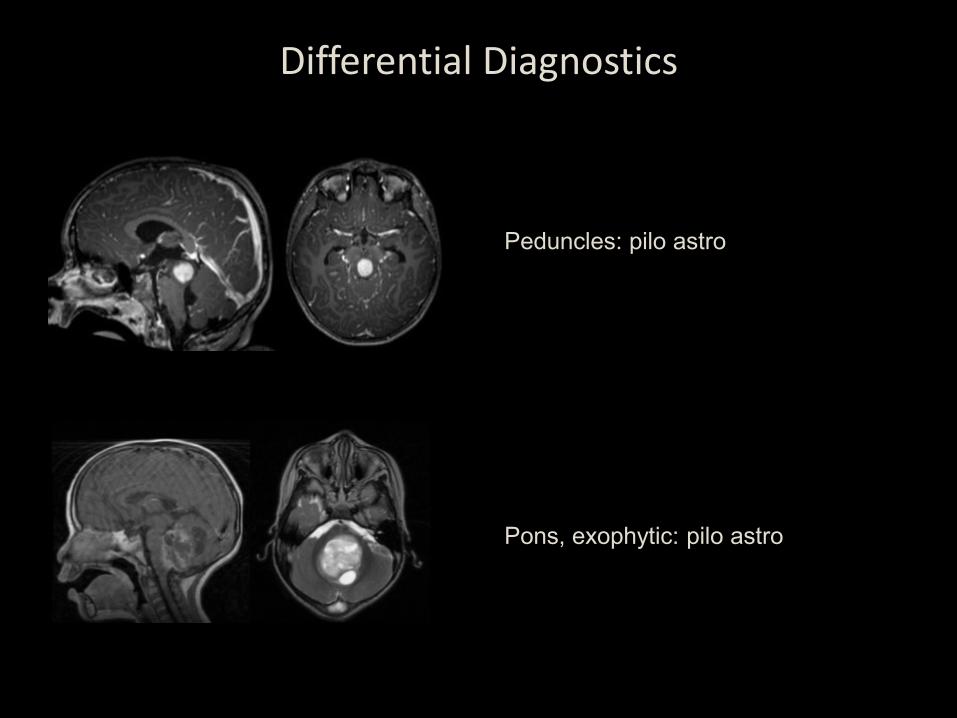
Differential Diagnostics
Peduncles: pilo astro
Pons, exophytic: pilo astro
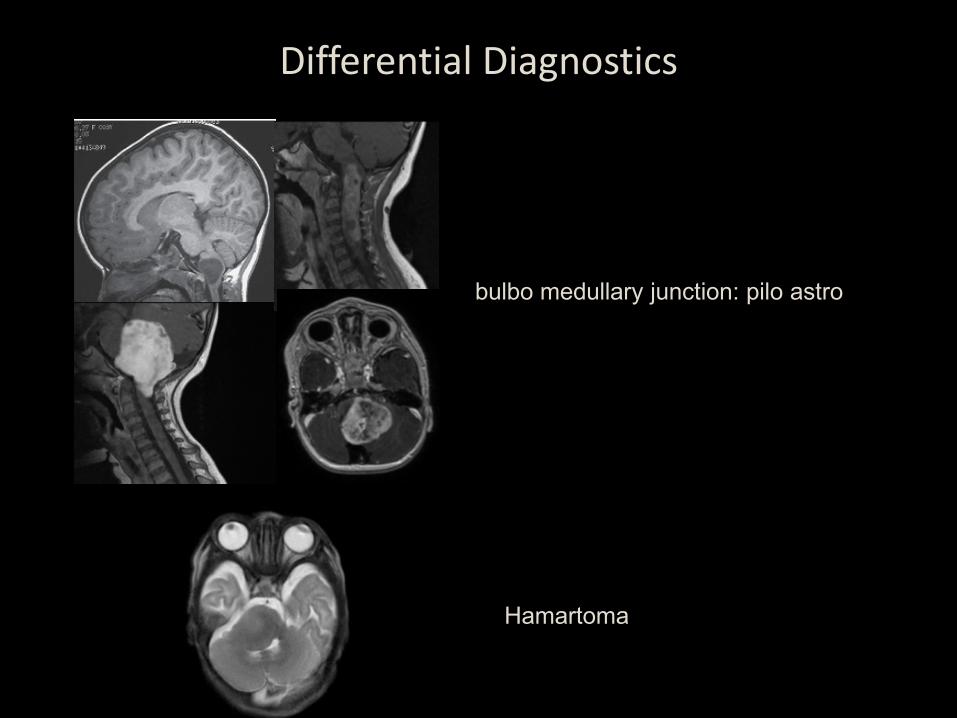
Hamartoma
bulbo medullary junction: pilo astro
Differential Diagnostics
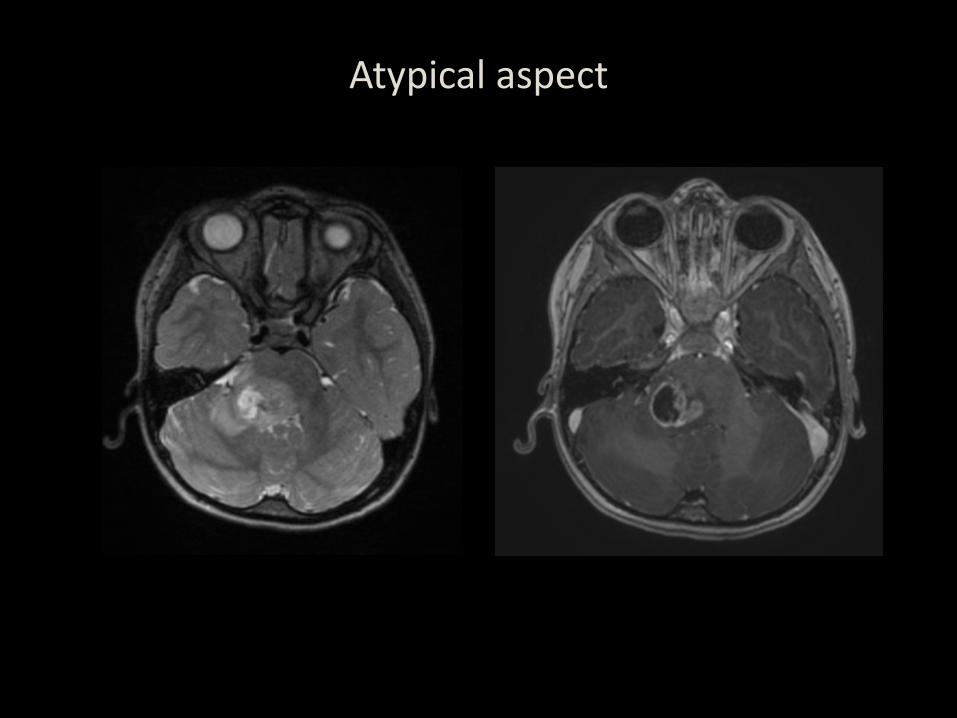
Atypical aspect
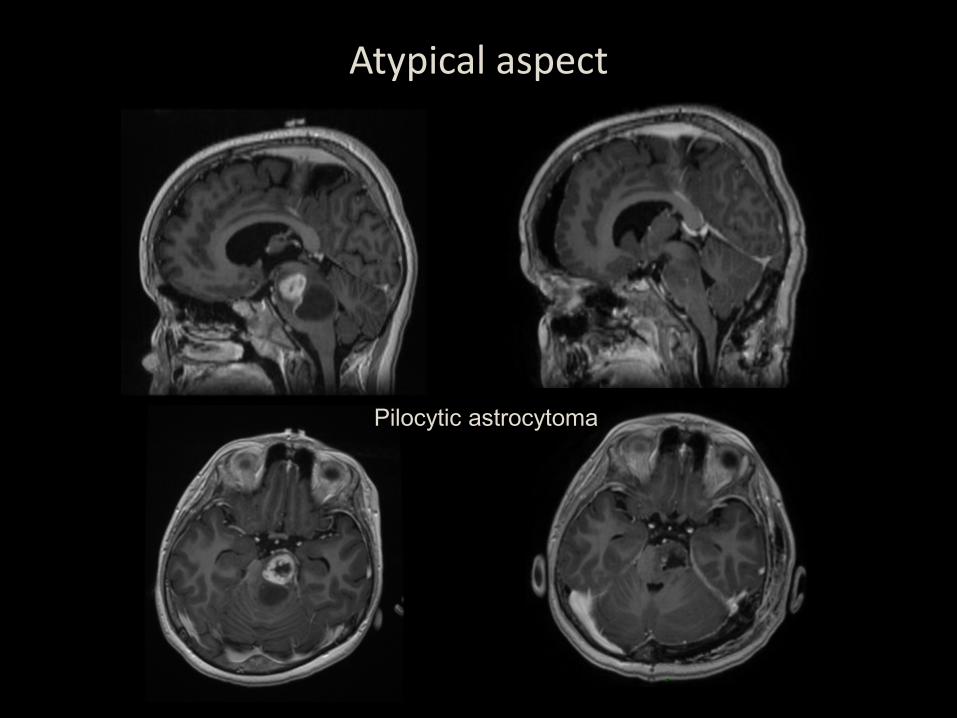
Atypical aspect
Pilocytic astrocytoma
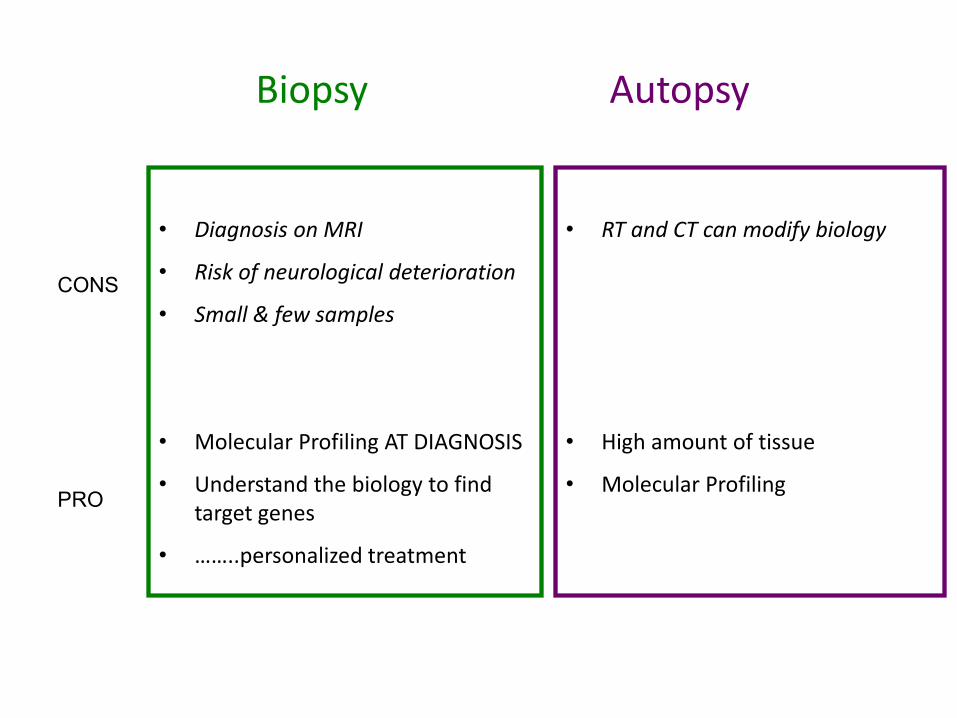
Biopsy Autopsy
• Diagnosis on MRI
• Risk of neurological deterioration
• Small & few samples
• Molecular Profiling AT DIAGNOSIS
• Understand the biology to find target genes
• ……..personalized treatment
• RT and CT can modify biology
• High amount of tissue
• Molecular Profiling
CONS
PRO
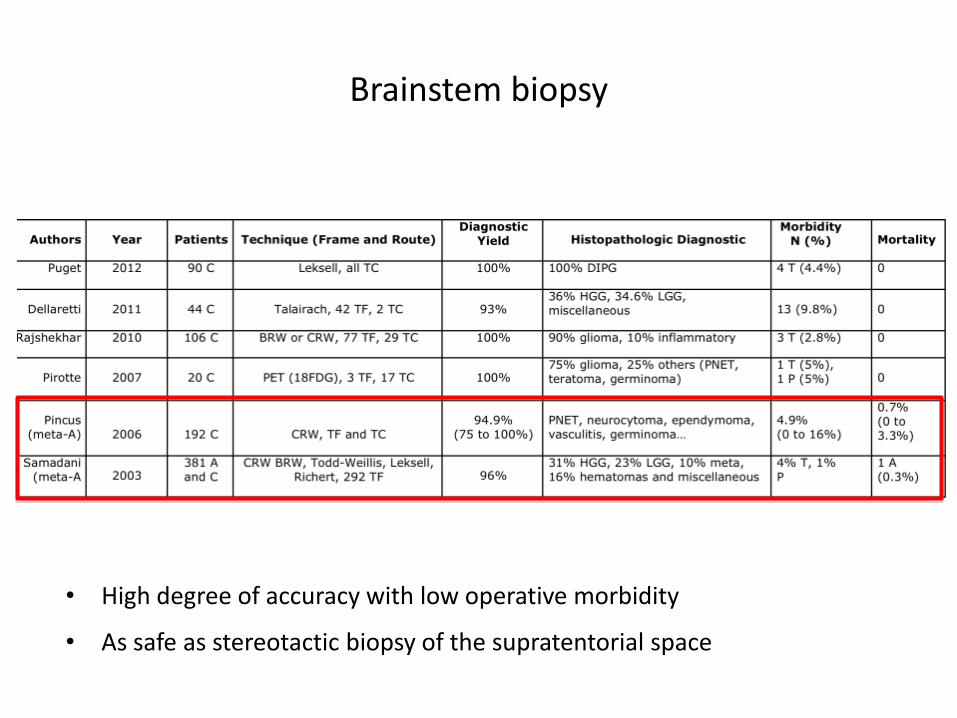
Brainstem biopsy
• High degree of accuracy with low operative morbidity
• As safe as stereotactic biopsy of the supratentorial space
ROUTES FOR BRAINSTEM BIOPSY
Routes
Transfrontal
• Precoronal entry
• Long
• All the segments of the brainstem
• Important to avoid ventricles, vessels, tentorium
Transcerebellar
• Through the middle cerebellar peduncle
• Short • Pontine and upper
medullary • Cross less eloquent
structures • Important to avoid the 4th
ventricle and CN nuclei
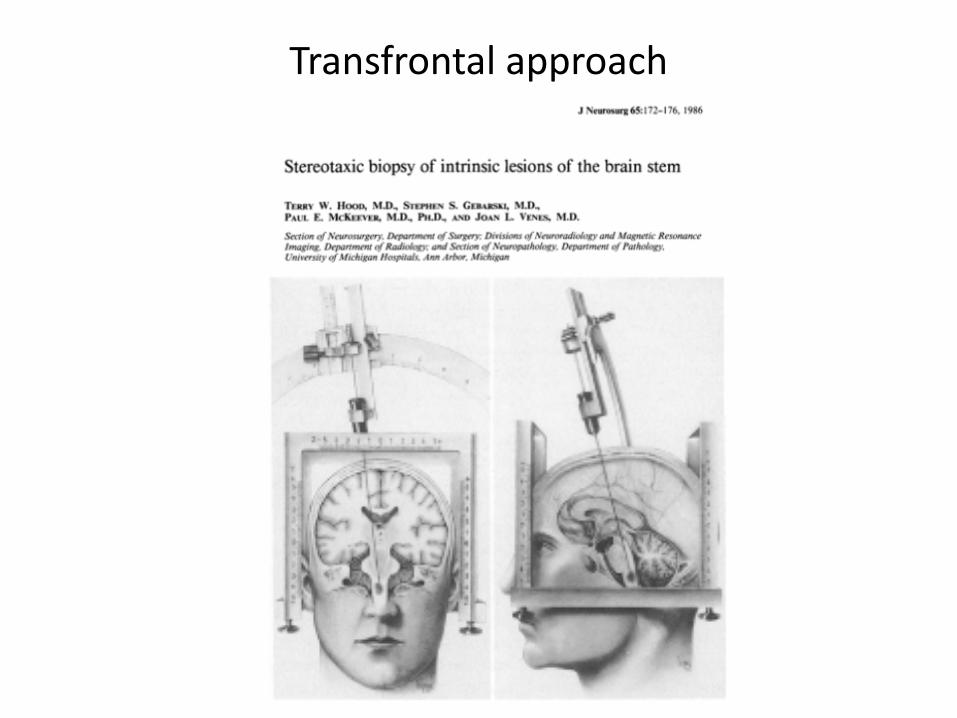
Transfrontal approach
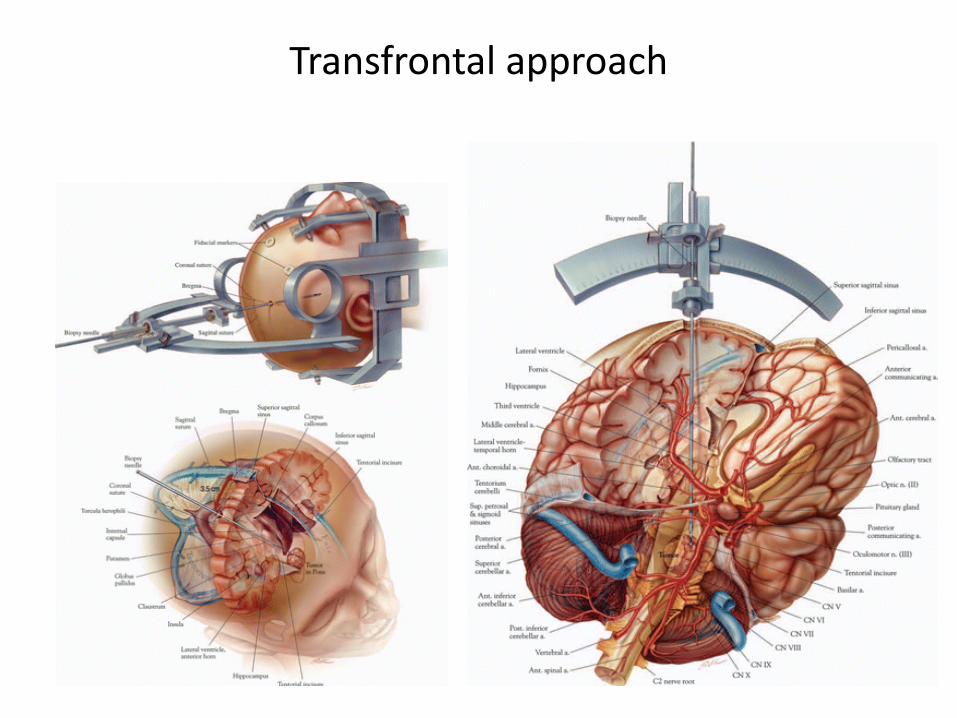
Transfrontal approach
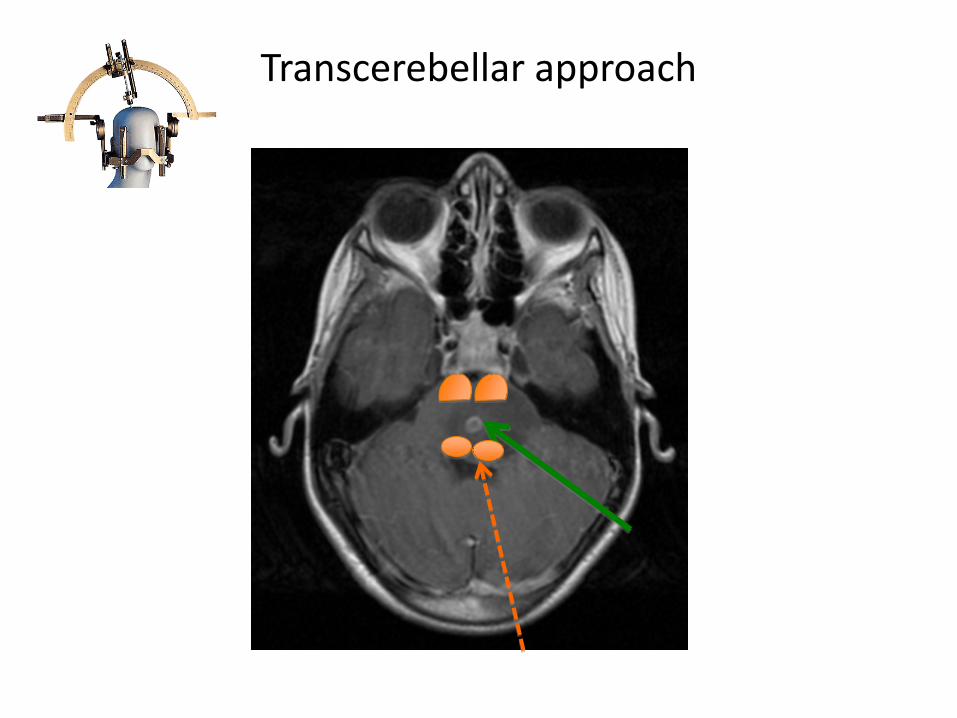
Transcerebellar approach
Right or left side?
• Depends on the tumor extension & clinical signs
• Choose the most disabled size
• Avoid to add controlateral deficits
HOW TO CHOOSE THE TARGET ?
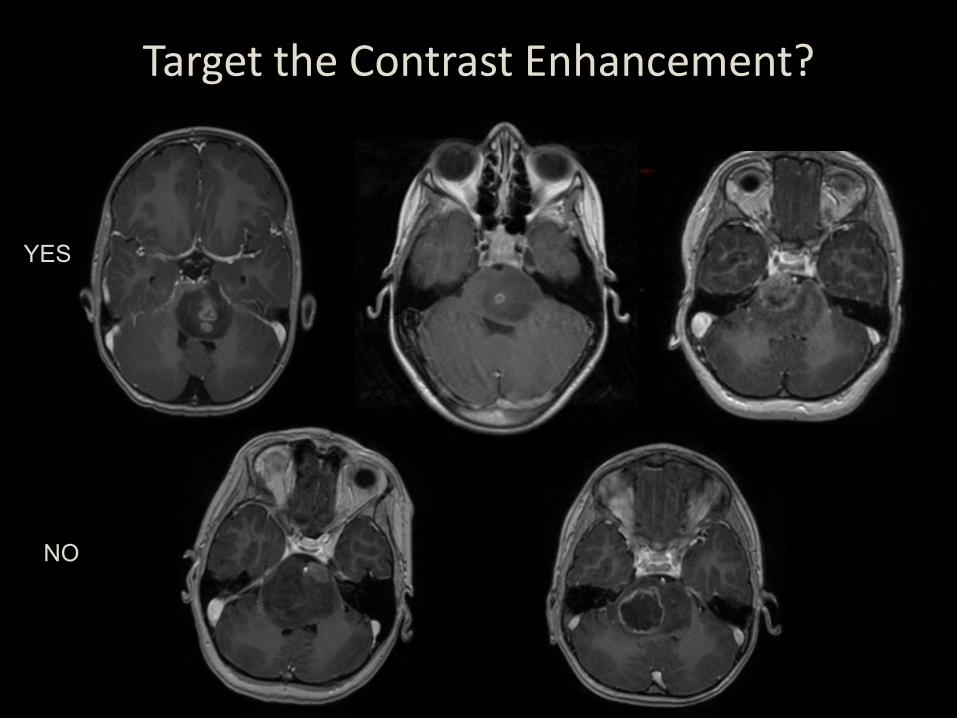
Target the Contrast Enhancement?
YES
NO
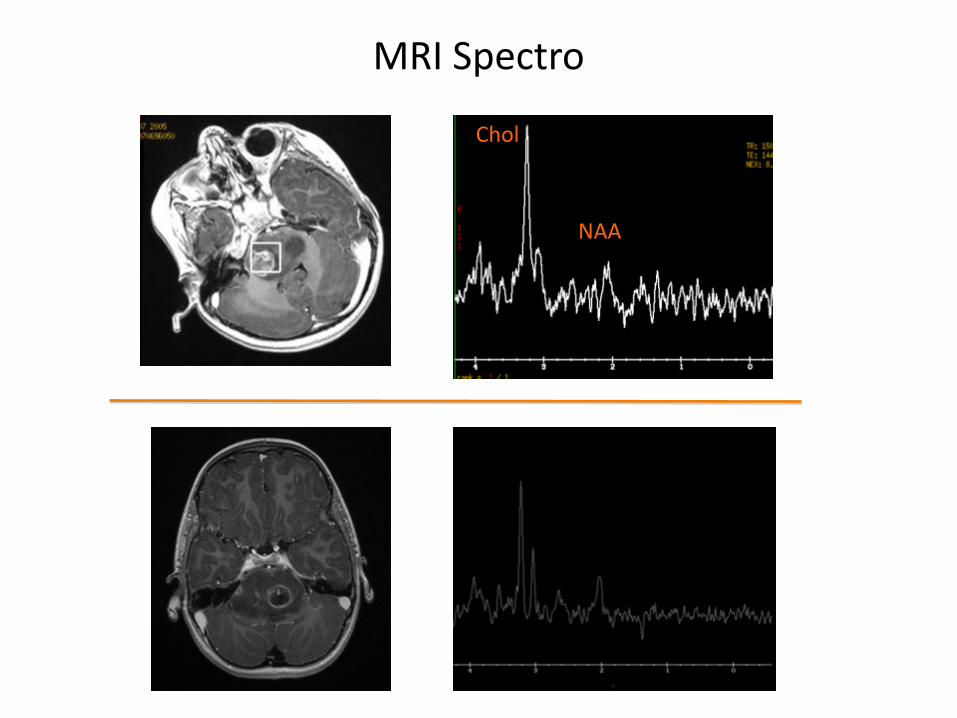
MRI Spectro
Chol
NAA
• Chernov Clin Neurol Neurosurg 2009 Jul – 30 MRI-spectro and 39 MRI. – No significant difference for diagnostic yield
• Not helpful to choose a target
MRI Spectro
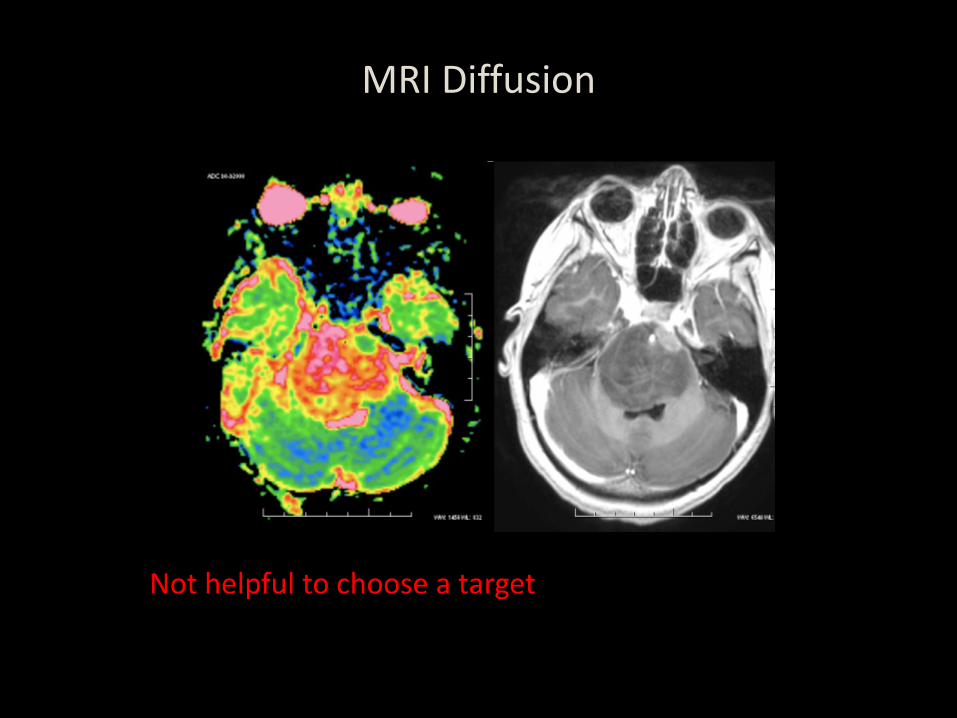
MRI Diffusion
Not helpful to choose a target
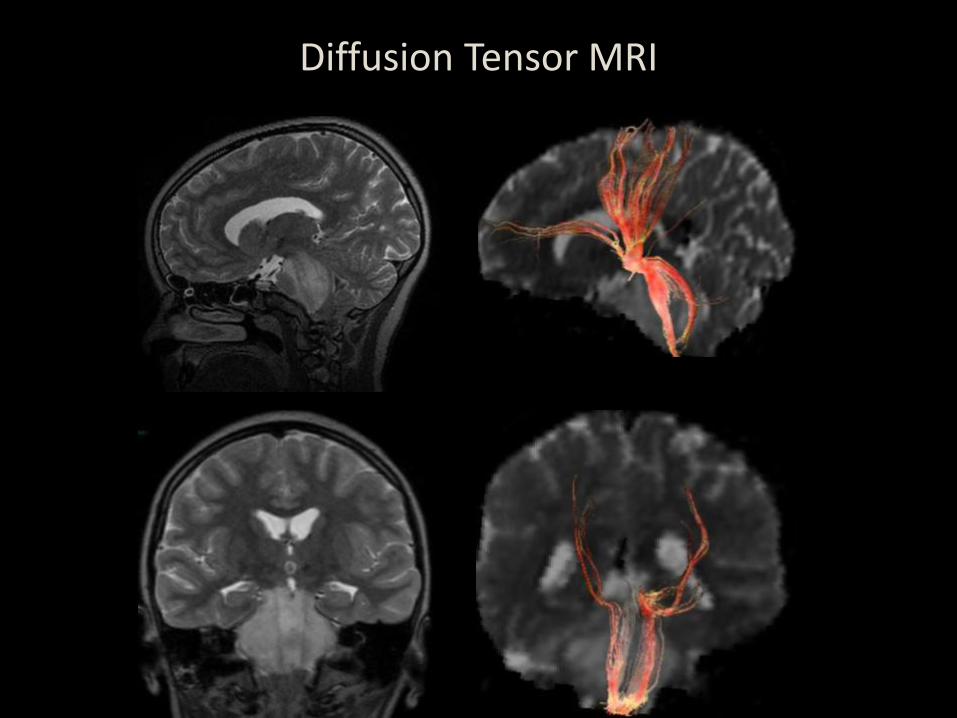
Diffusion Tensor MRI
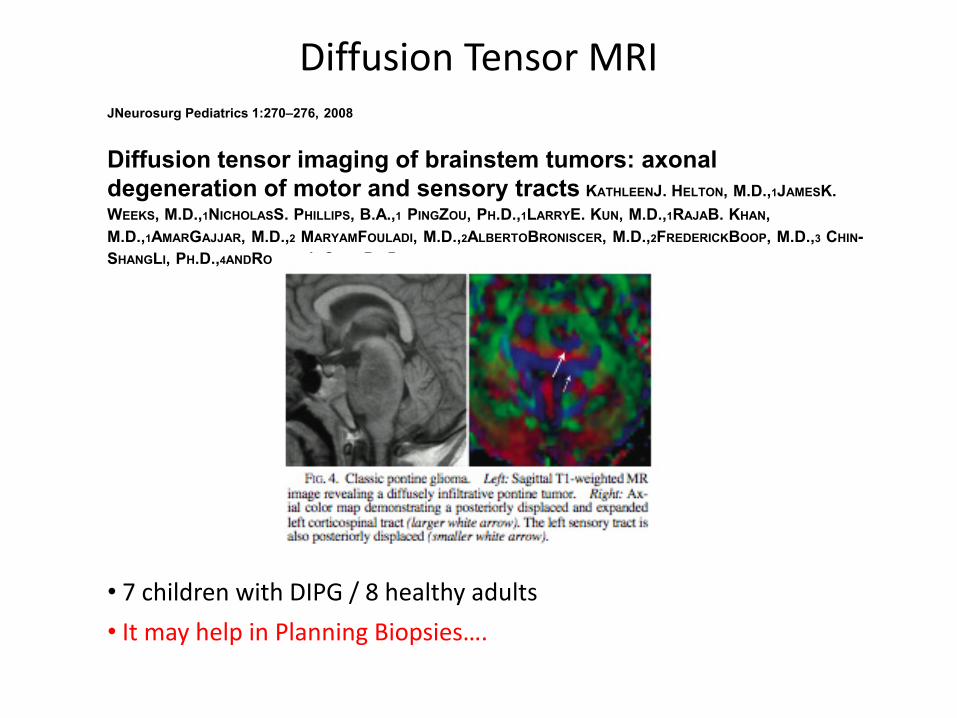
JNeurosurg Pediatrics 1:270–276, 2008 Diffusion tensor imaging of brainstem tumors: axonal degeneration of motor and sensory tracts KATHLEENJ. HELTON, M.D.,1JAMESK. WEEKS, M.D.,1NICHOLASS. PHILLIPS, B.A.,1 PINGZOU, PH.D.,1LARRYE. KUN, M.D.,1RAJAB. KHAN, M.D.,1AMARGAJJAR, M.D.,2 MARYAMFOULADI, M.D.,2ALBERTOBRONISCER, M.D.,2FREDERICKBOOP, M.D.,3 CHIN-SHANGLI, PH.D.,4ANDROBERTJ. OGG, PH.D.1
Diffusion Tensor MRI
• 7 children with DIPG / 8 healthy adults • It may help in Planning Biopsies….
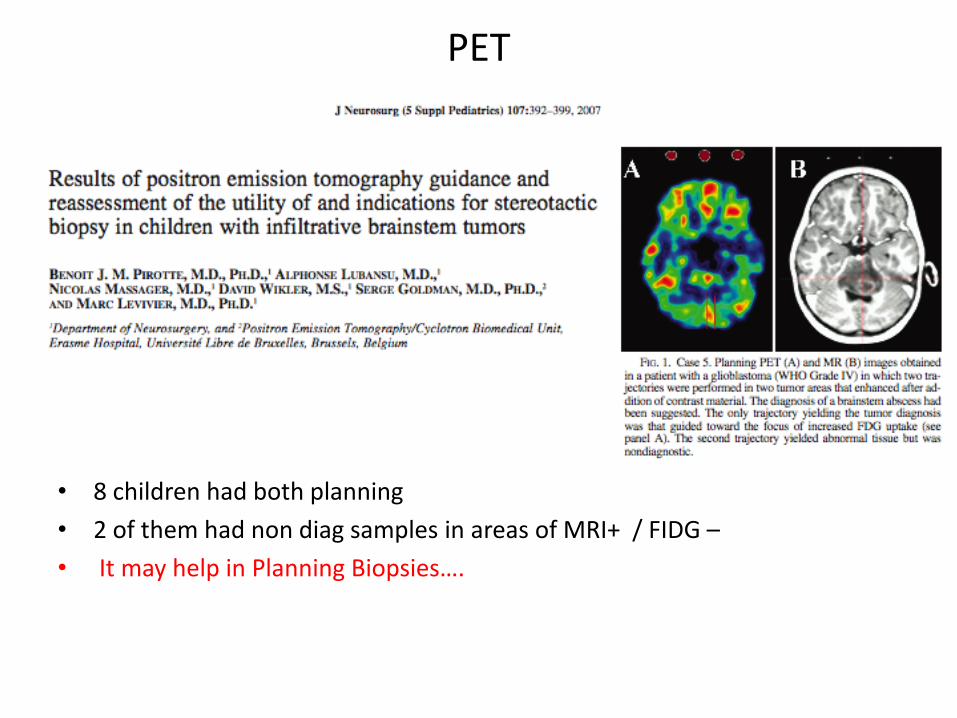
PET
• 8 children had both planning • 2 of them had non diag samples in areas of MRI+ / FIDG – • It may help in Planning Biopsies….
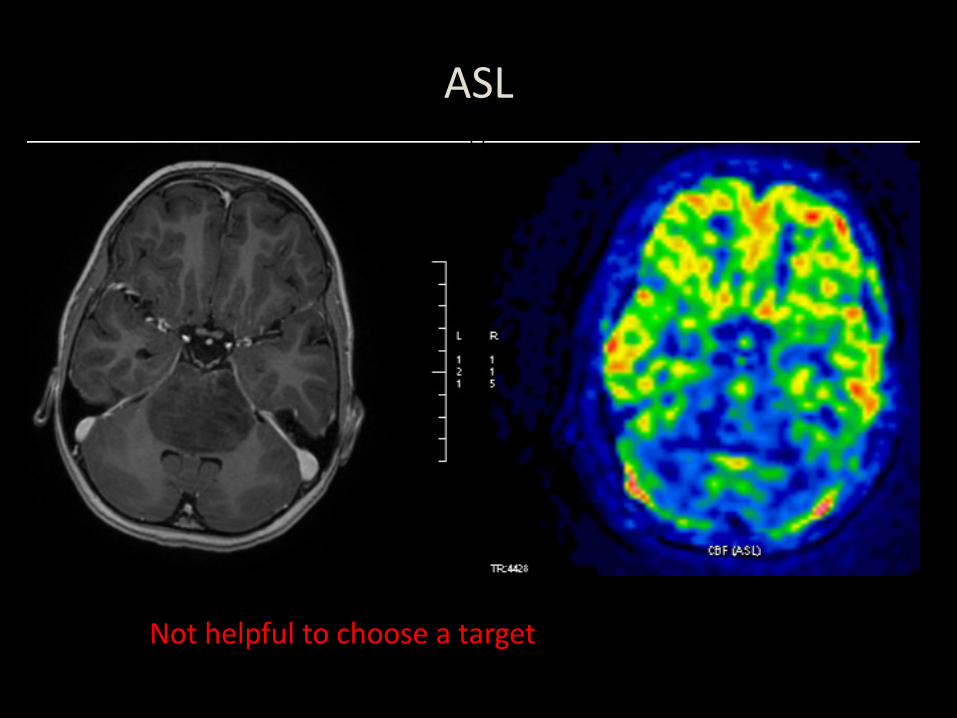
ASL
Not helpful to choose a target
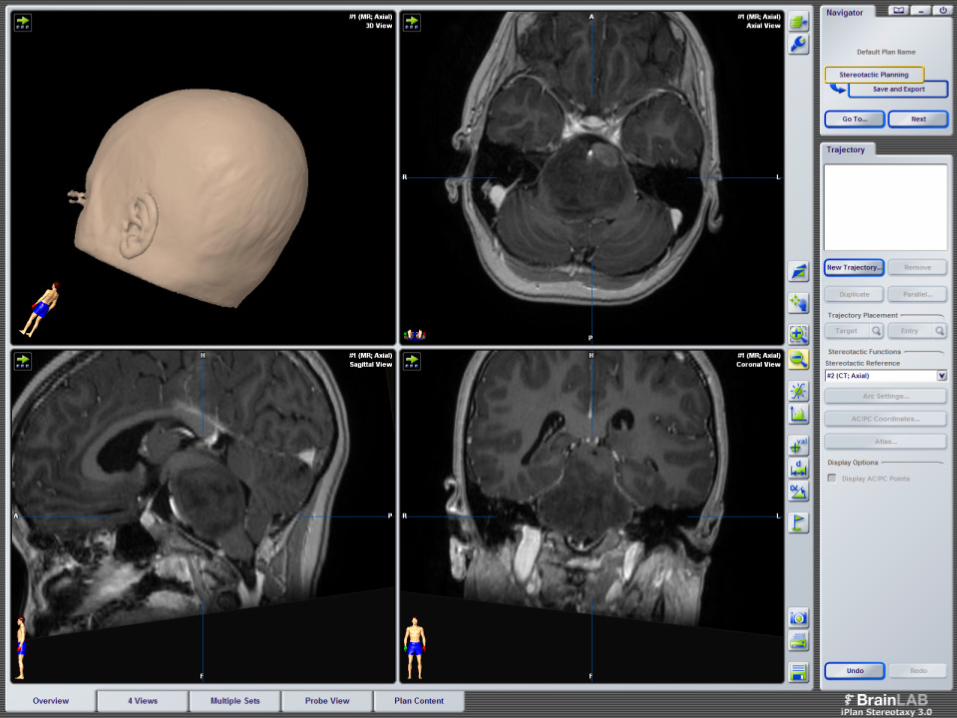
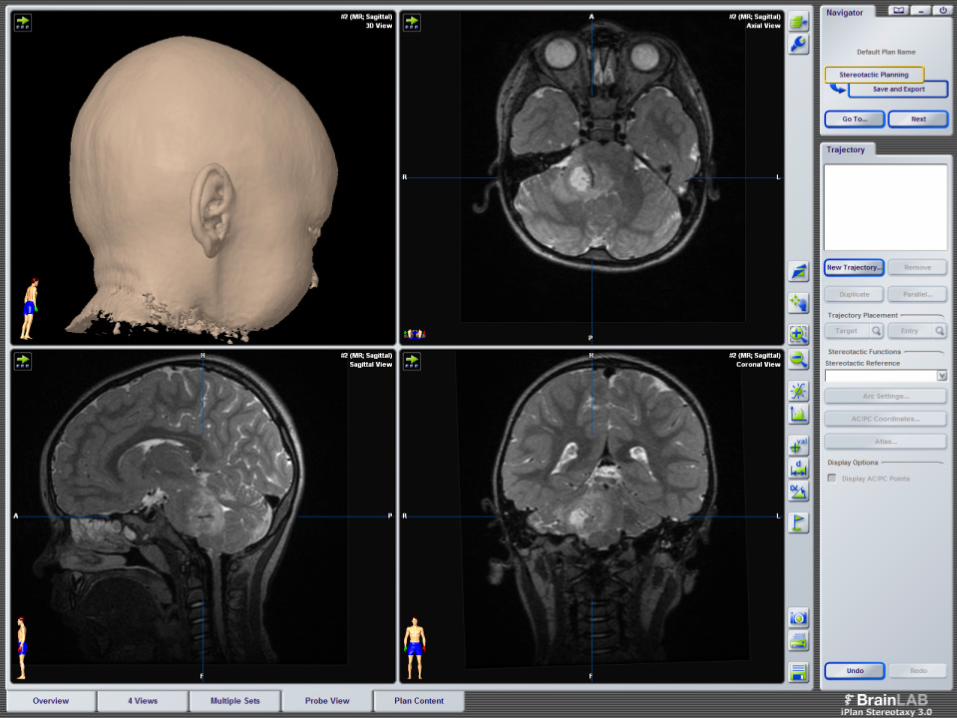
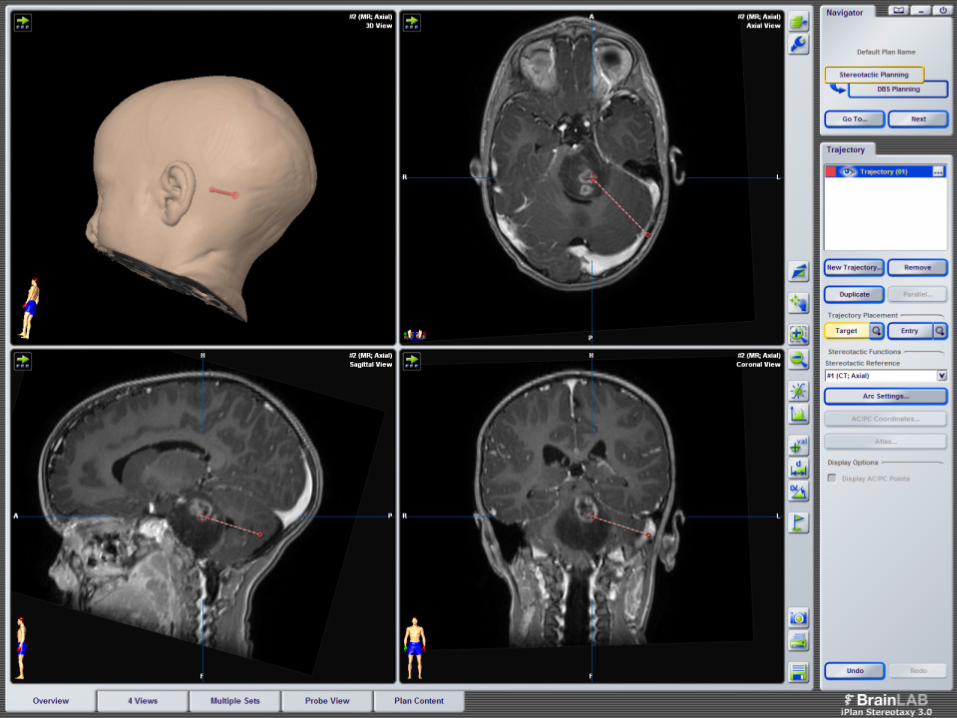
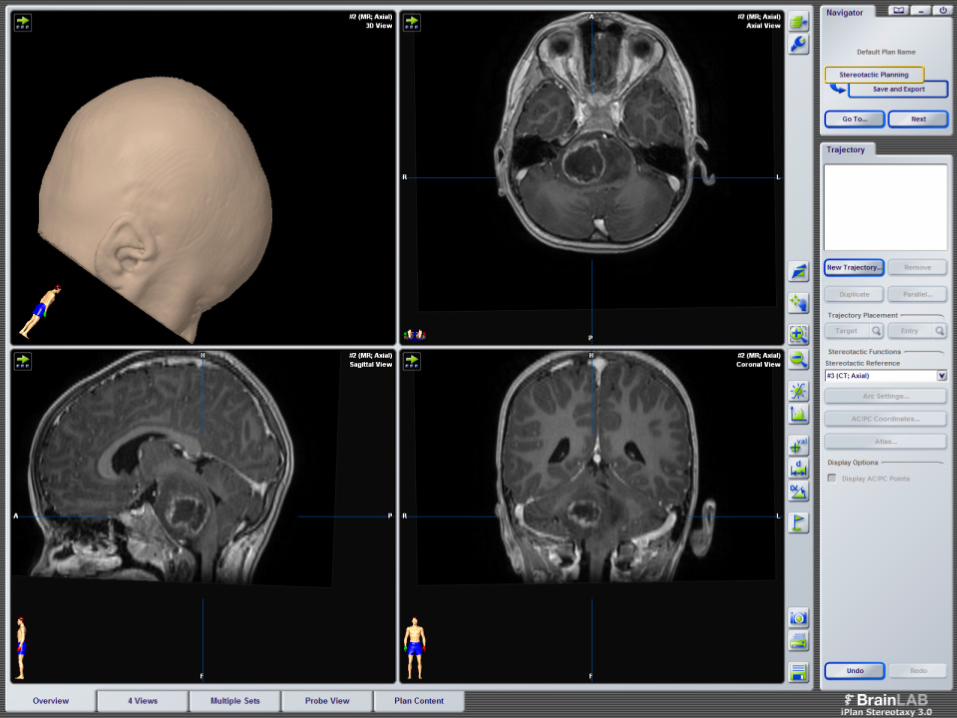
TECHNICAL PROCEDURE DIPG biopsy
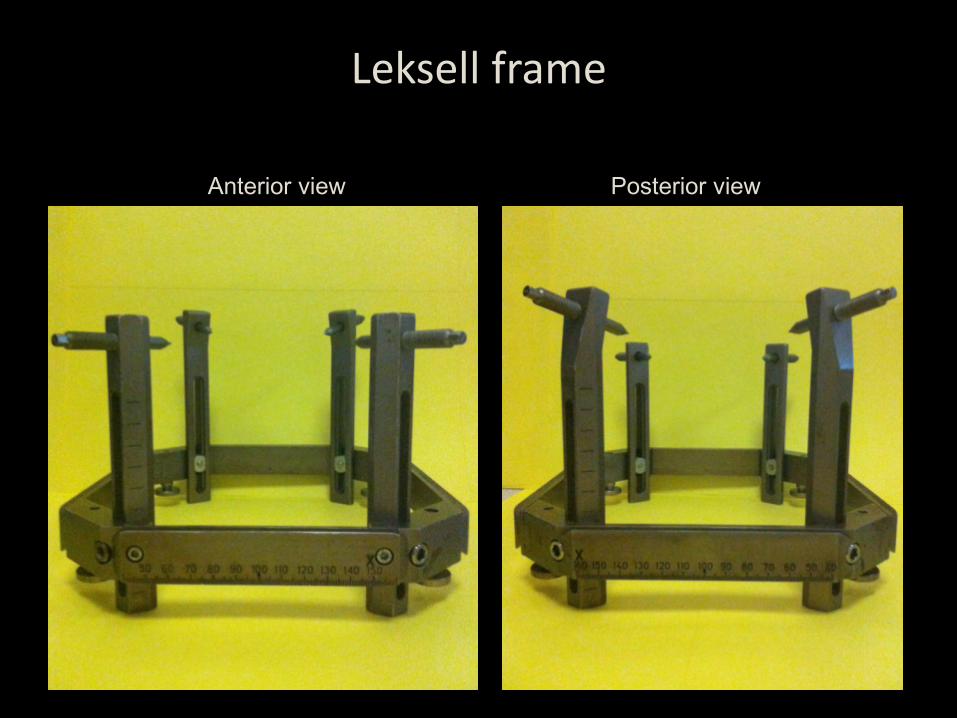
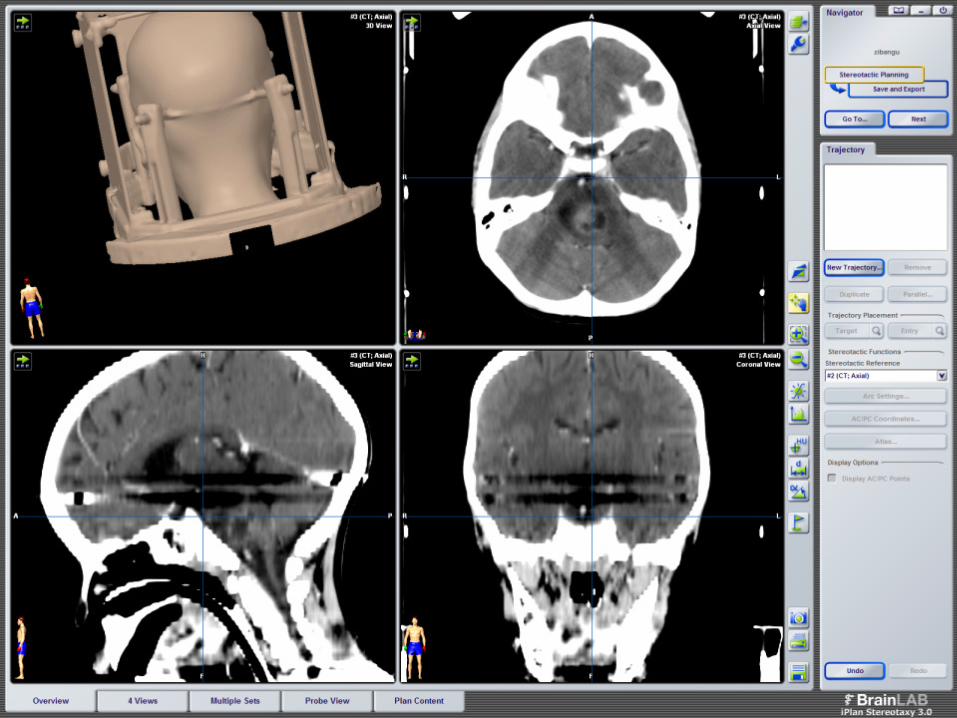
Leksell frame
Anterior view Posterior view
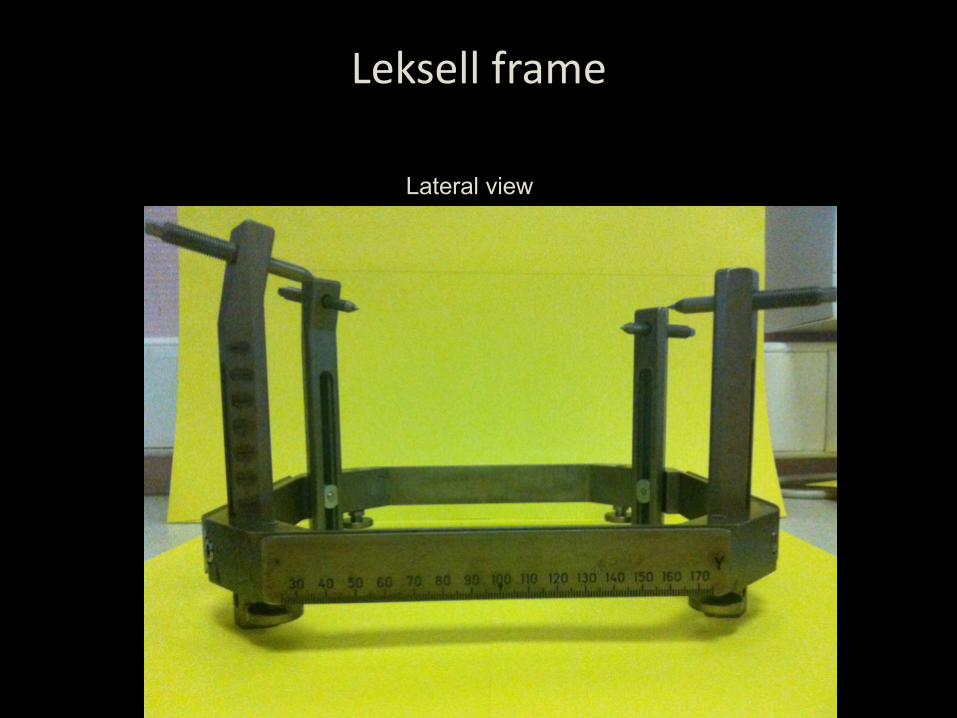
Lateral view
Leksell frame
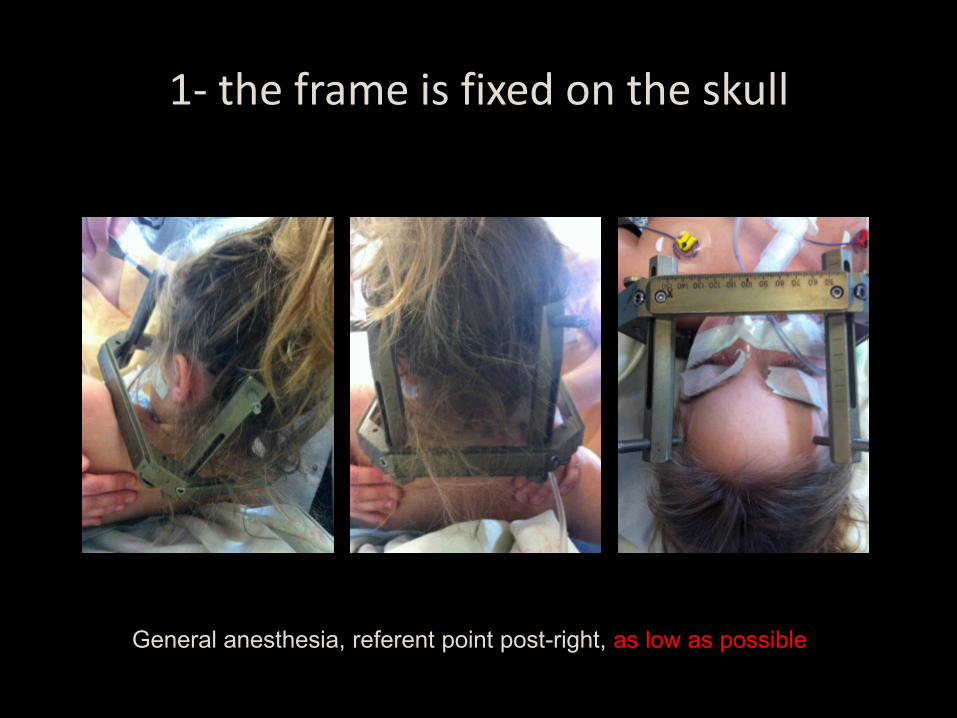
1- the frame is fixed on the skull
General anesthesia, referent point post-right, as low as possible
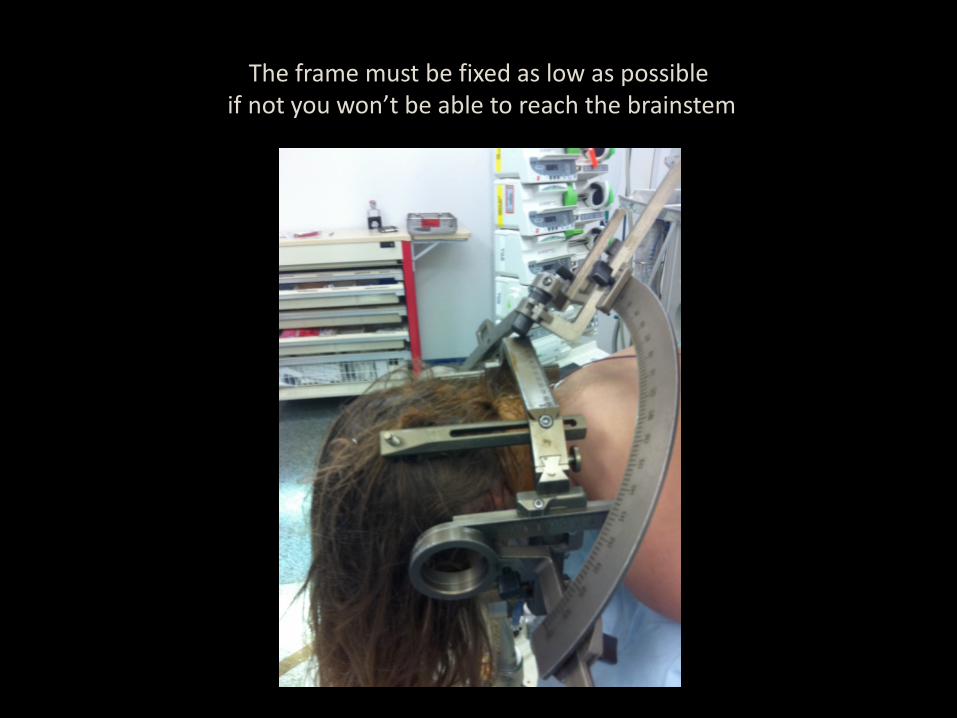
The frame must be fixed as low as possible if not you won’t be able to reach the brainstem
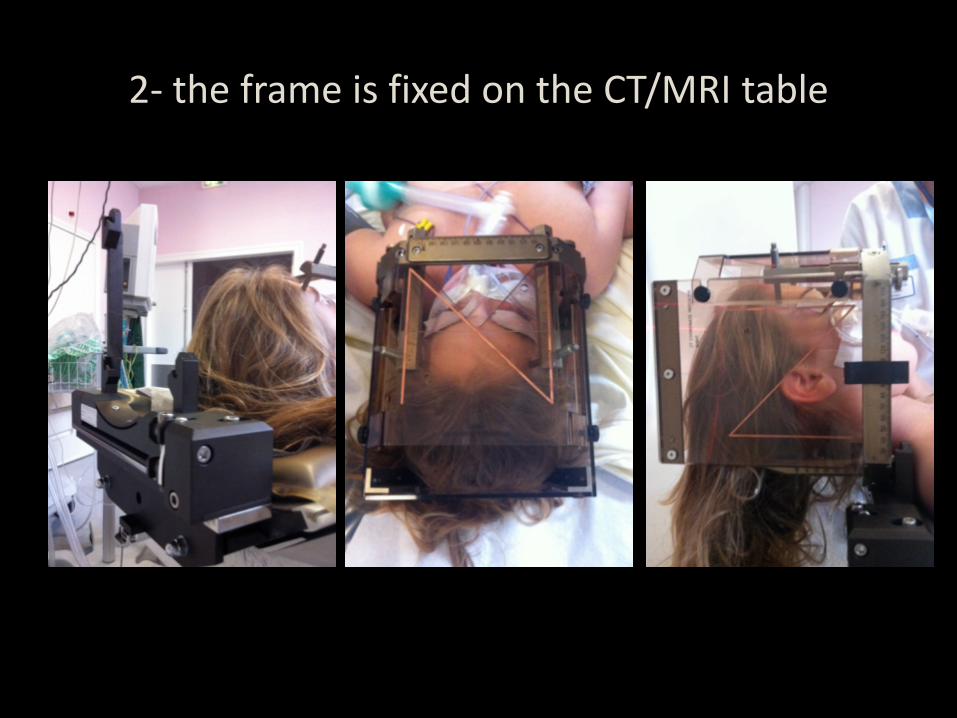
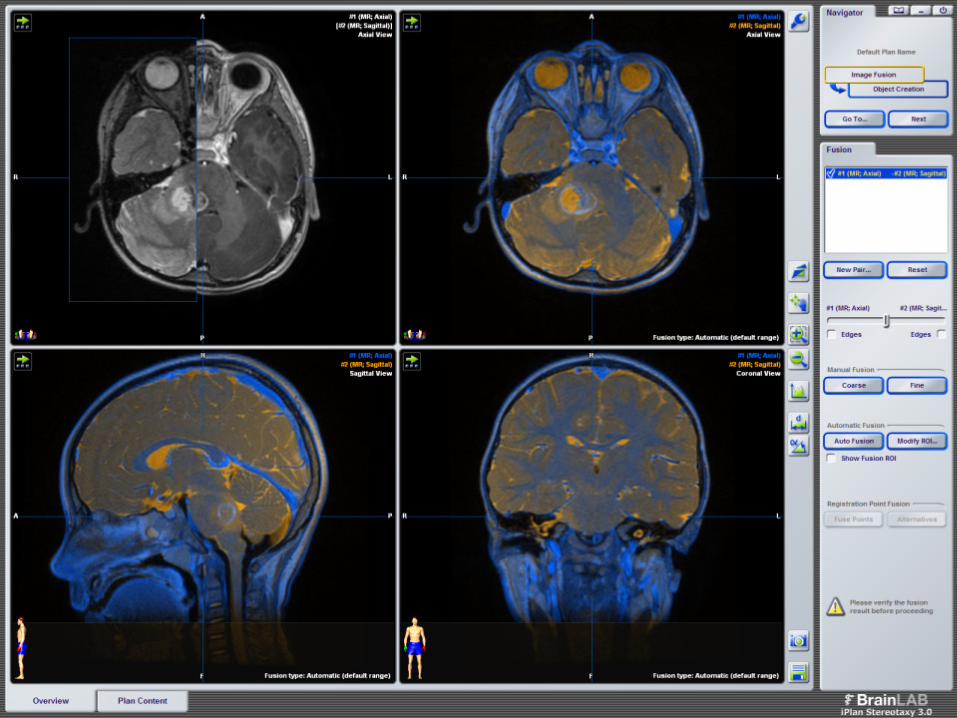
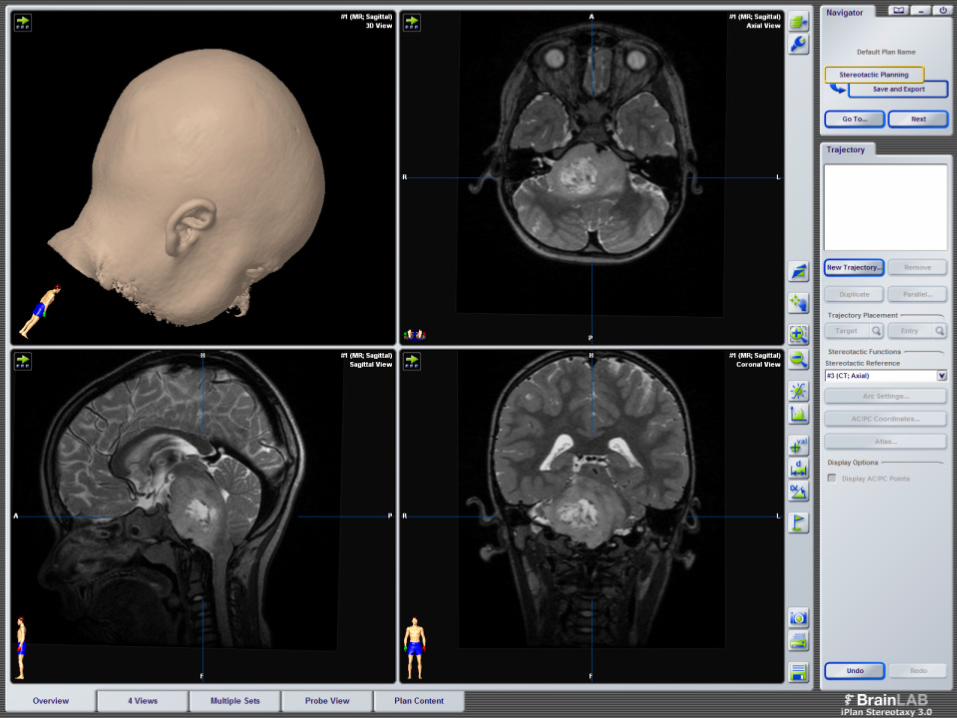
2- the frame is fixed on the CT/MRI table
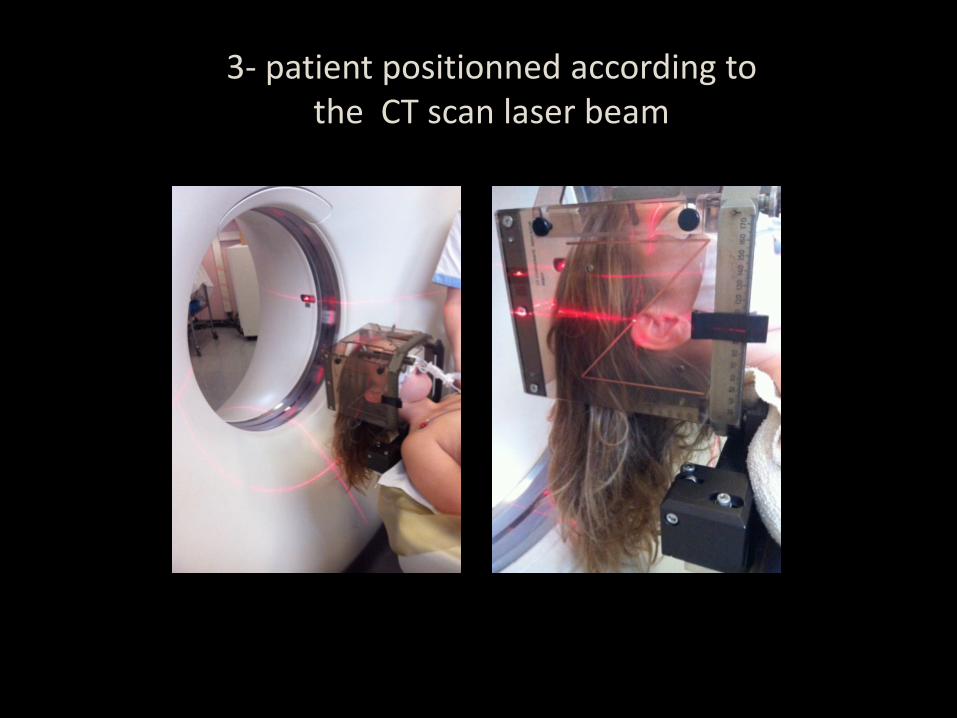
3- patient positionned according to the CT scan laser beam
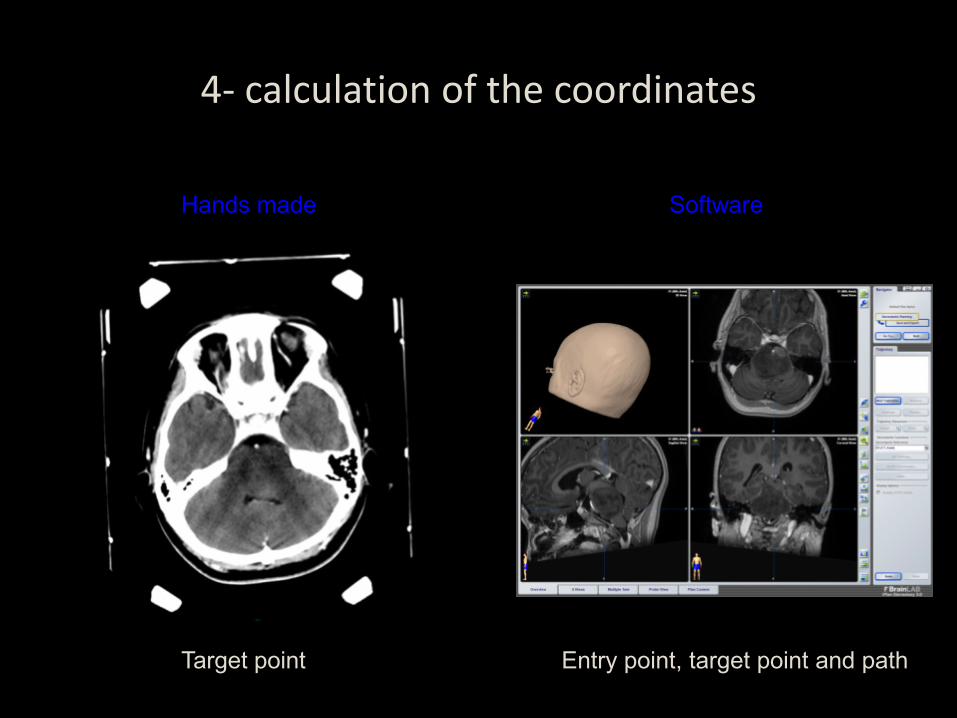
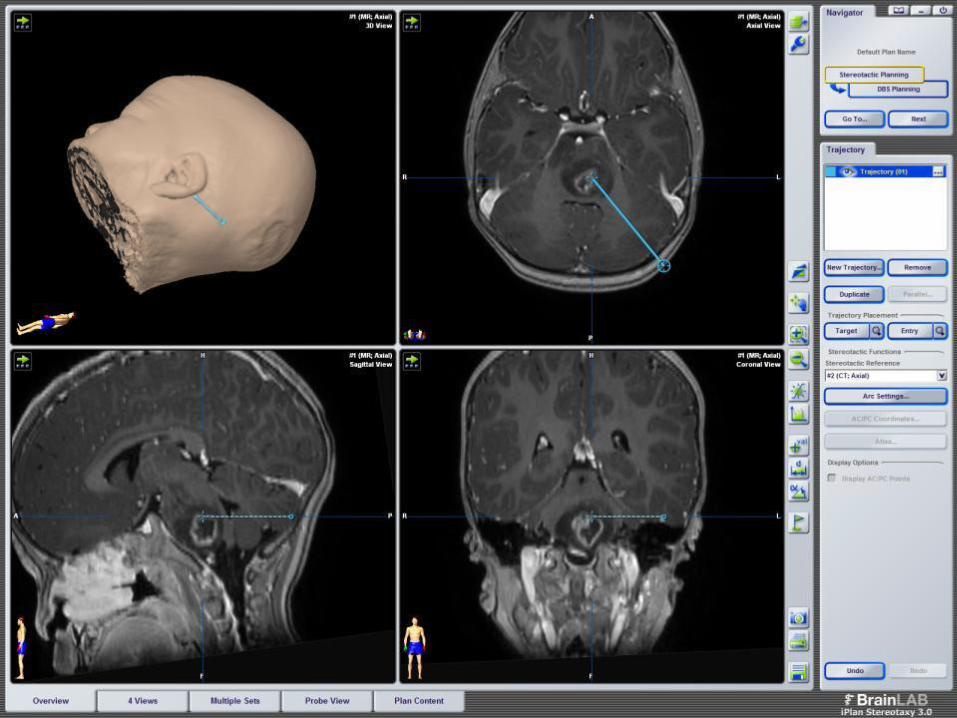
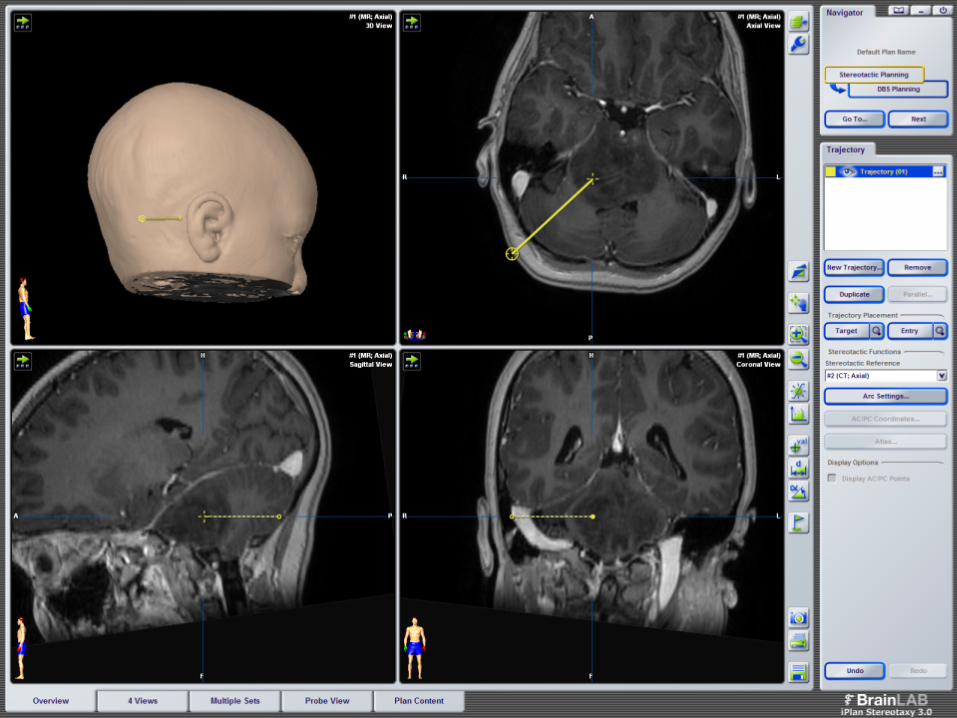
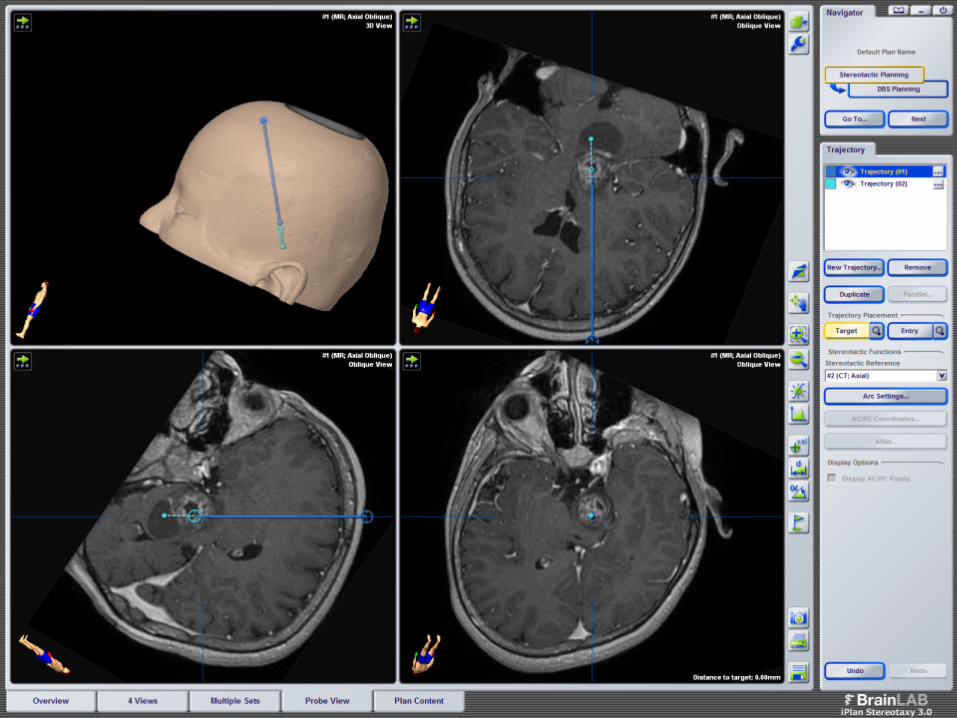
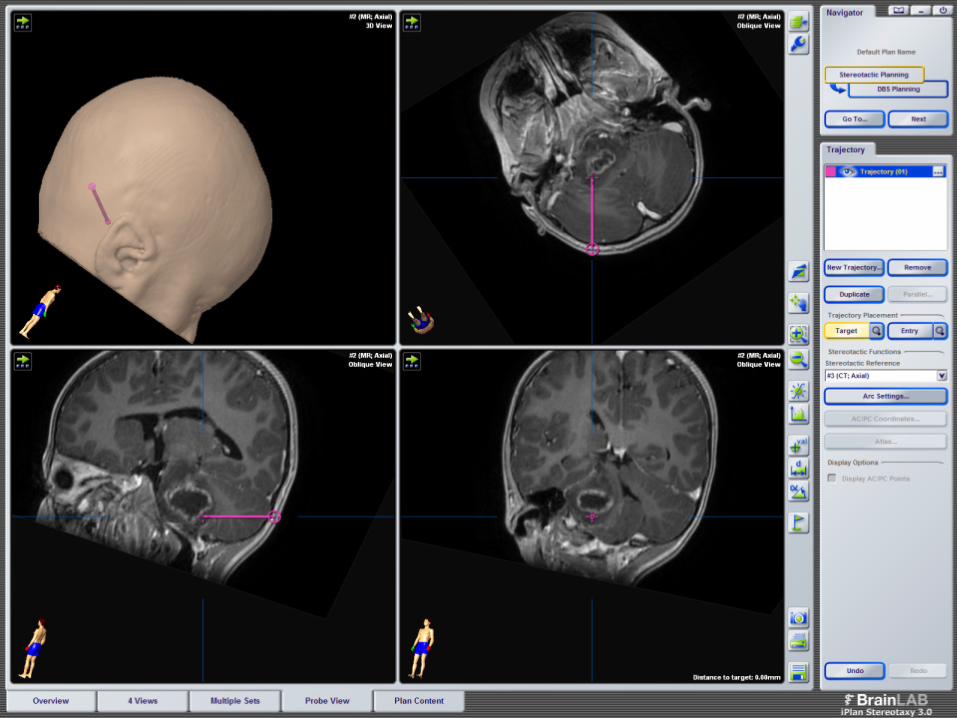
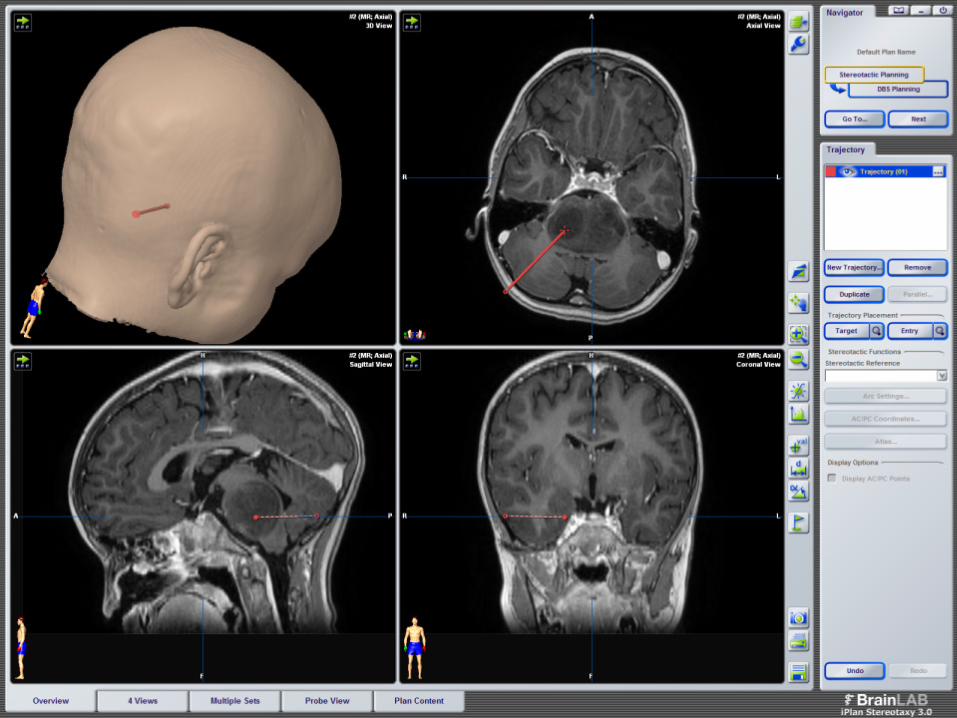
4- calculation of the coordinates
Software
Entry point, target point and path
Hands made
Target point

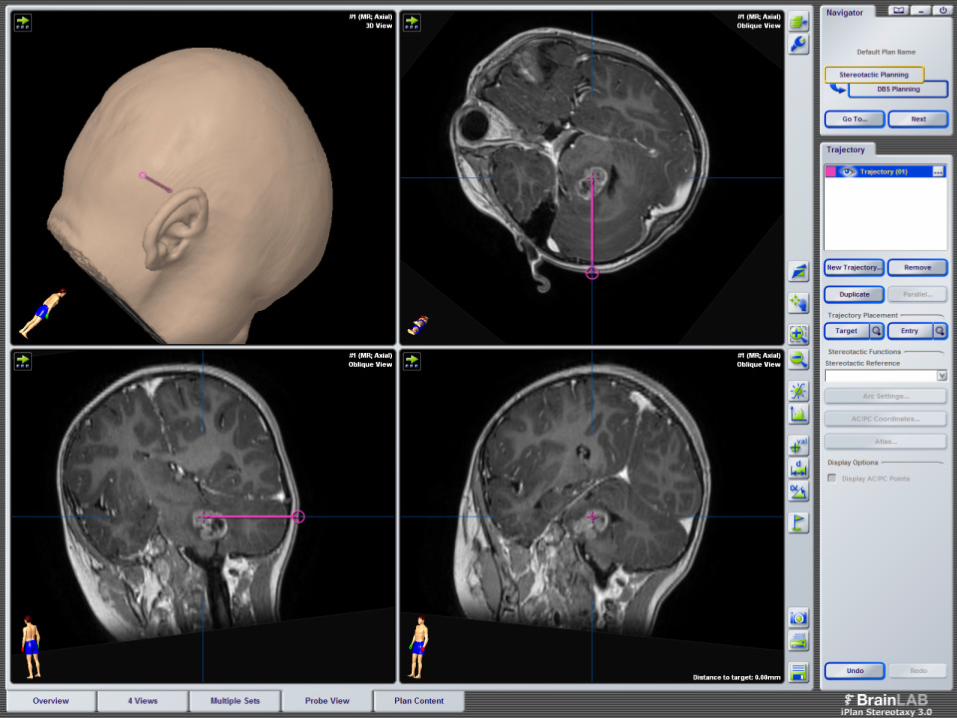
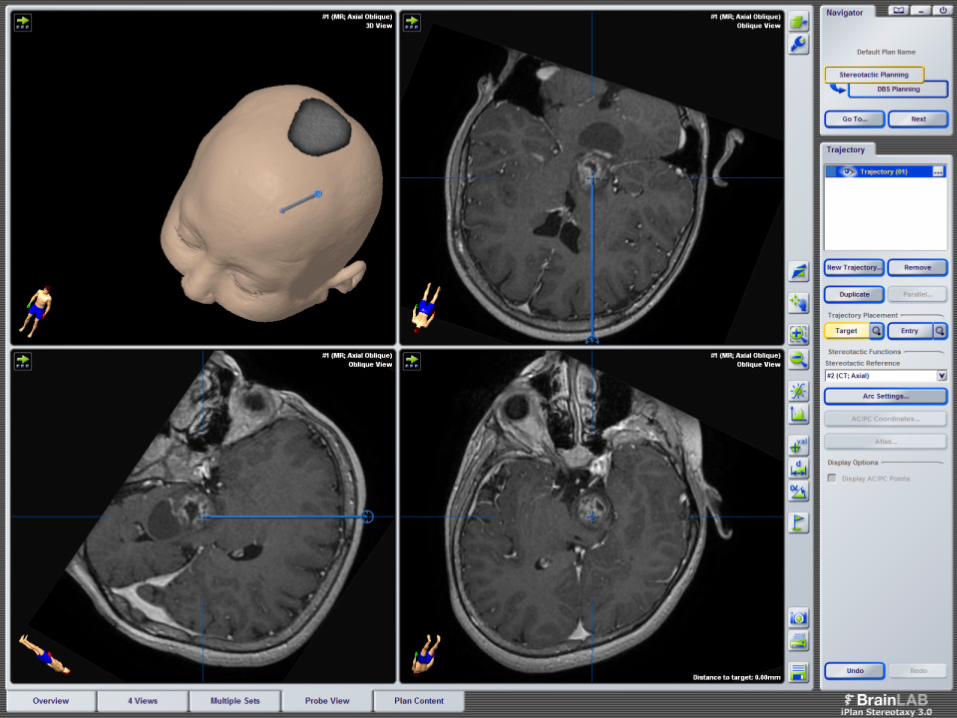
5- transfert in the operating room

Prone position (transcerebellar approach)
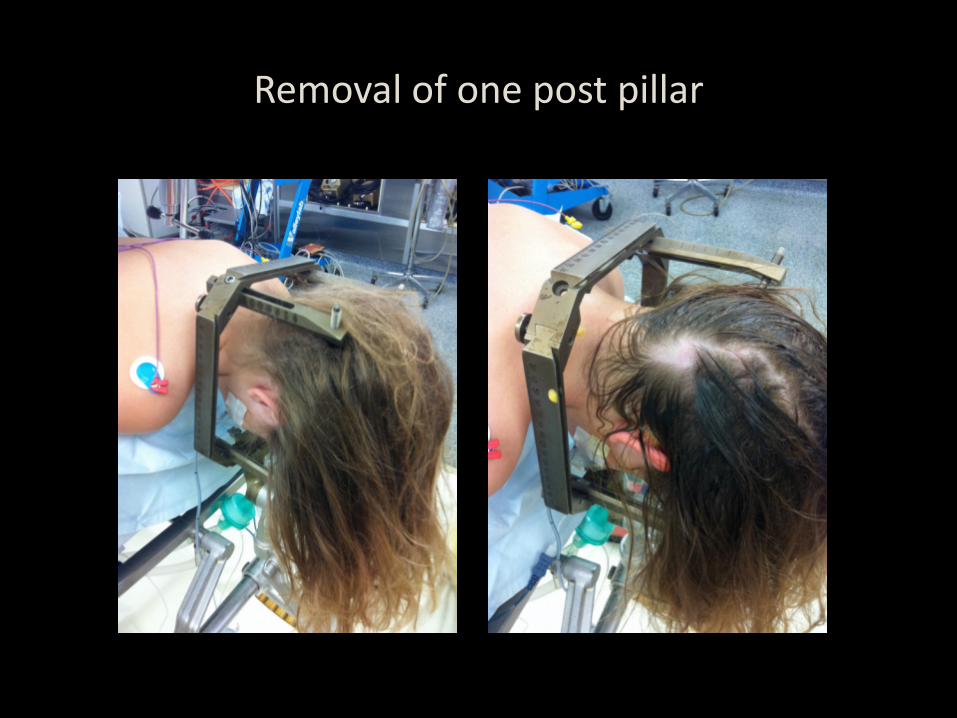
Removal of one post pillar


Installation of the whole frame

Burr hole


Installation of the needle support
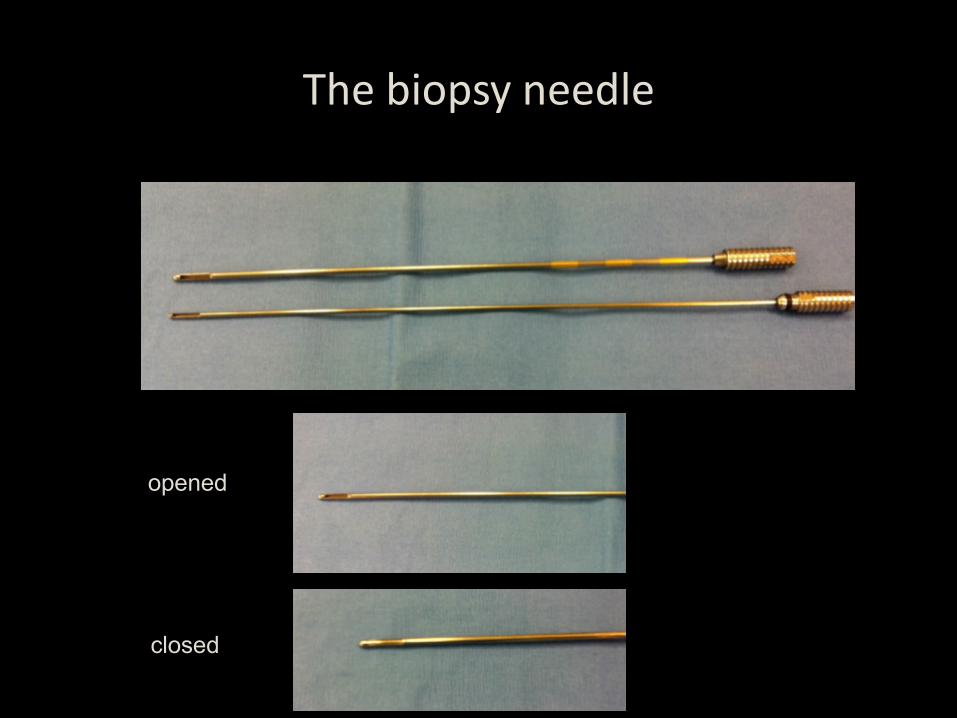
The biopsy needle
opened
closed
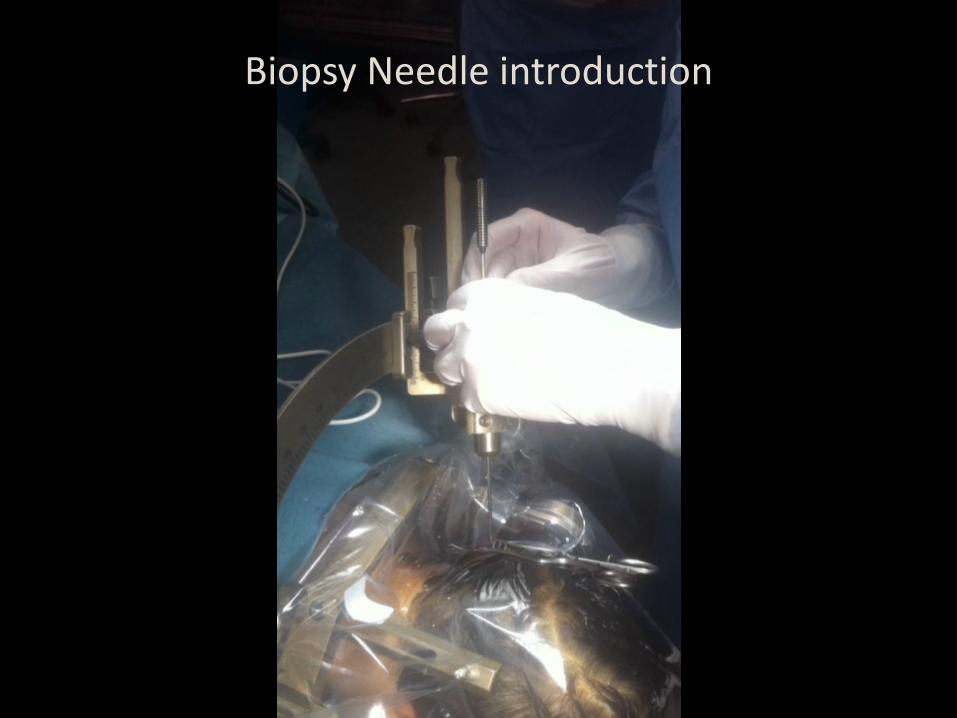
Biopsy Needle introduction


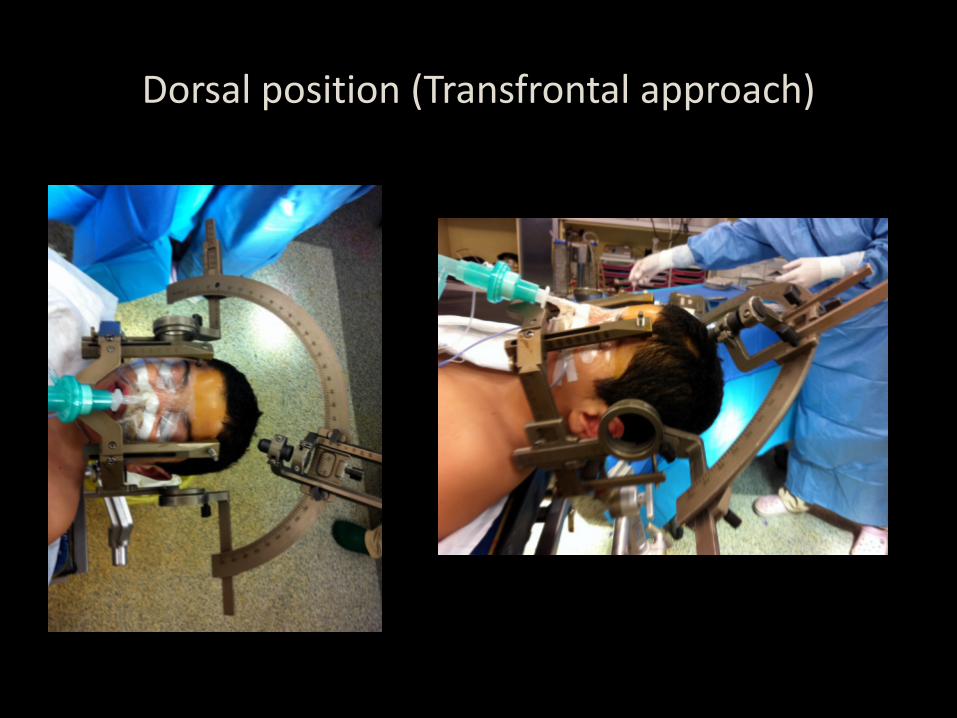
Dorsal position (Transfrontal approach)

Cyst aspiration
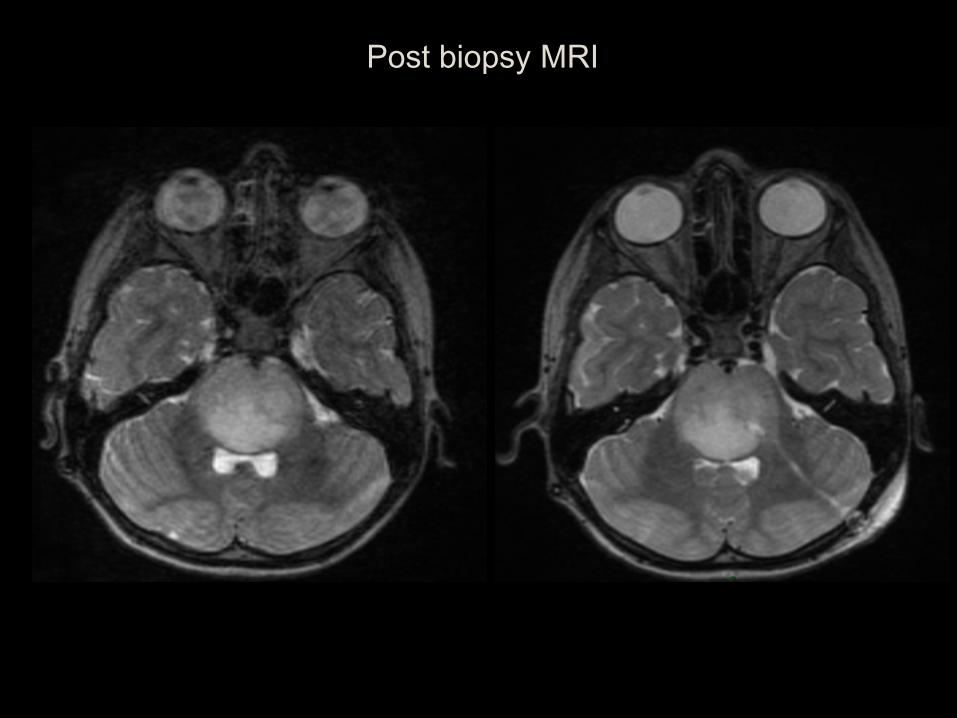
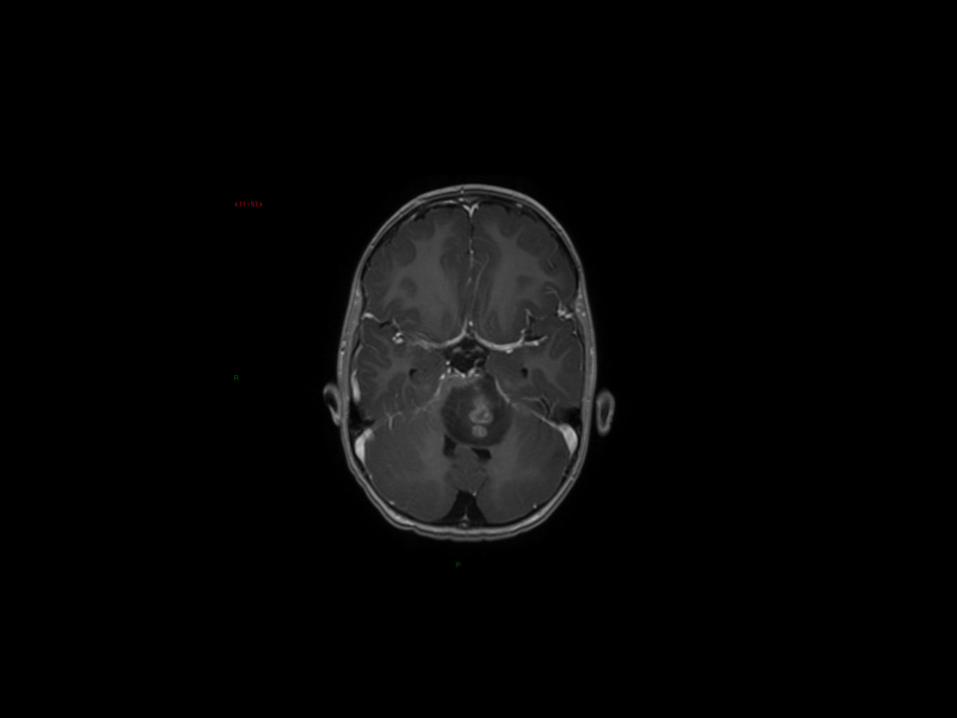
Post biopsy MRI
NECKER SERIES
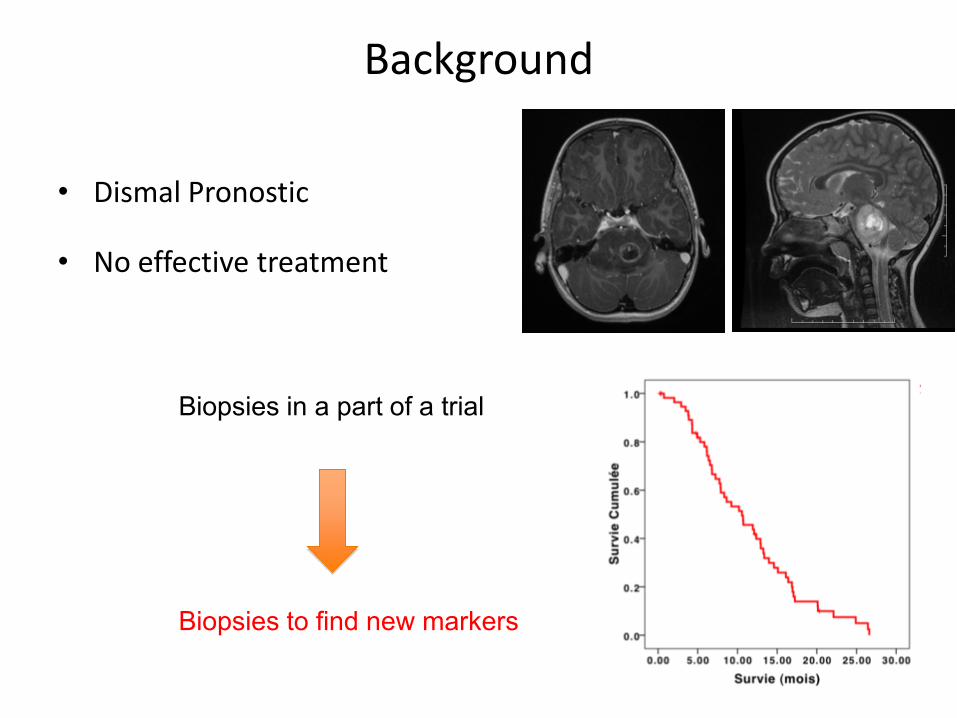
Background
• Dismal Pronostic
• No effective treatment
Biopsies in a part of a trial
Biopsies to find new markers
DIPG biopsy Necker Series
• 90 (2002-2012)
• 4 parents refused
• Number of samples (up to 8)
• No Mortality
• 4 Transient worsening (VII + hemiparesis)
• 2 disseminations along the trajectory at relapse
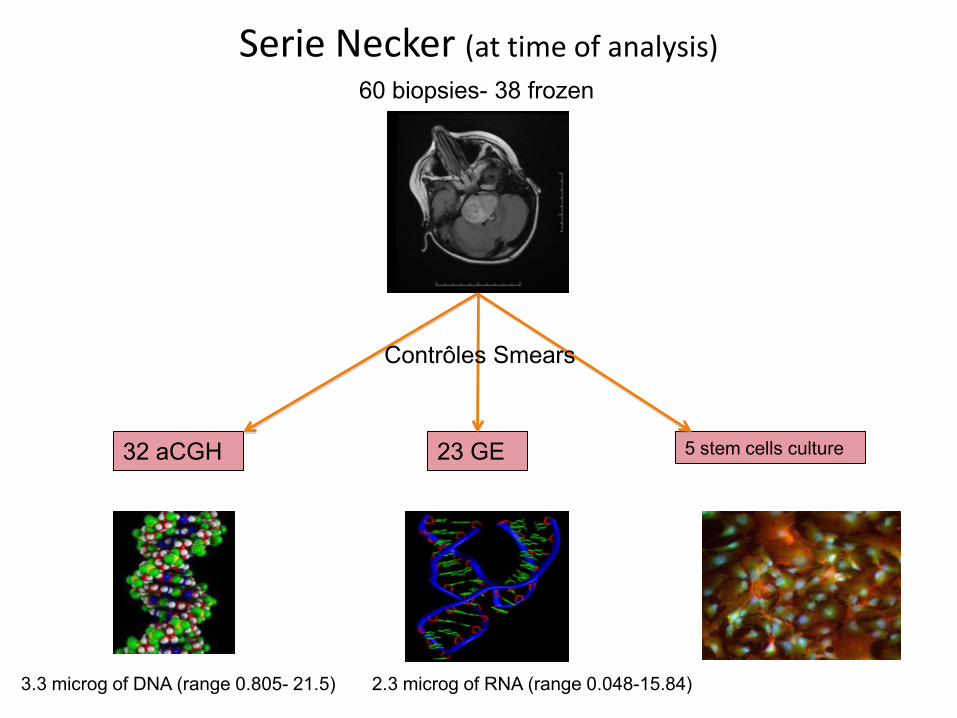
Serie Necker (at time of analysis)
32 aCGH 23 GE 5 stem cells culture
60 biopsies- 38 frozen
3.3 microg of DNA (range 0.805- 21.5) 2.3 microg of RNA (range 0.048-15.84)
Contrôles Smears
Histological grading
• « DIPG » 6.2%
• Grade II 27.5%
• Grade III 37.5%
• Grade IV 28.8%
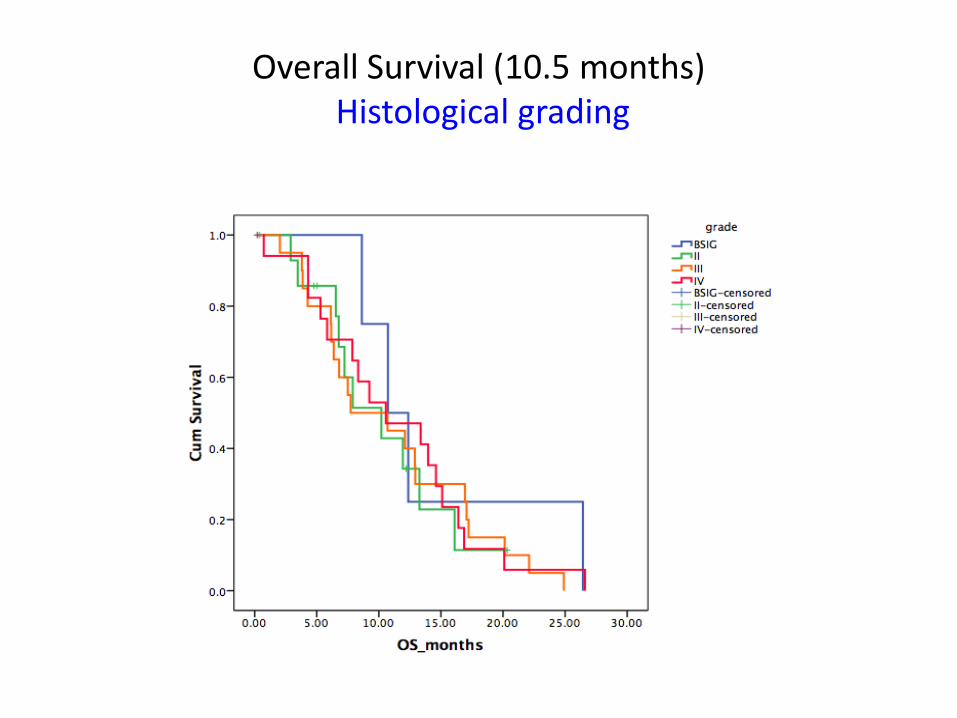
Overall Survival (10.5 months) Histological grading
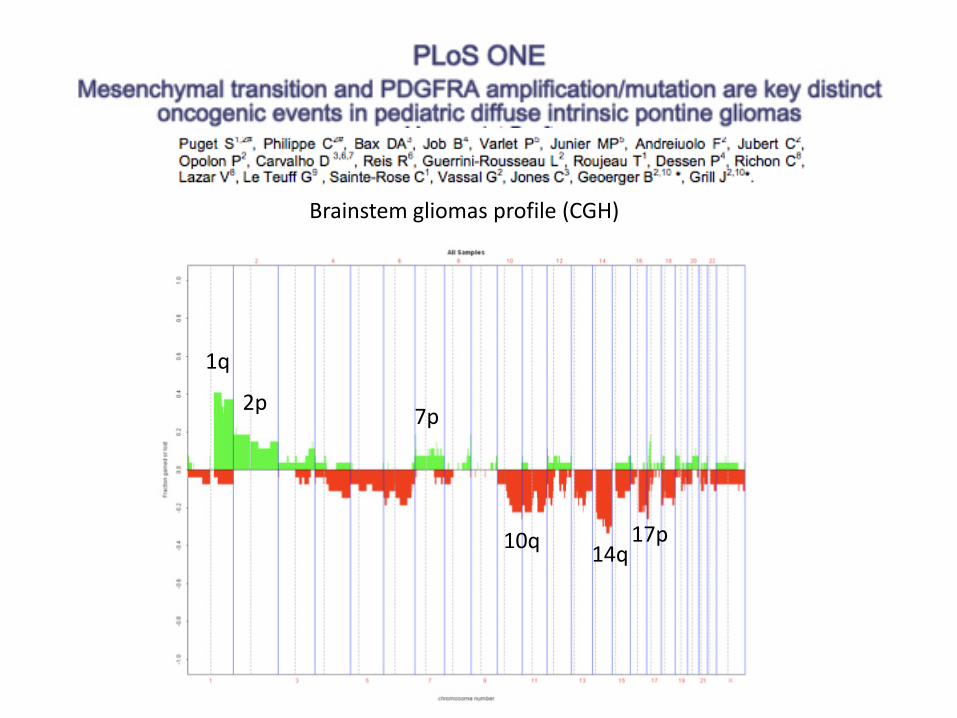
Brainstem gliomas profile (CGH)
1q
14q 10q 17p
2p 7p
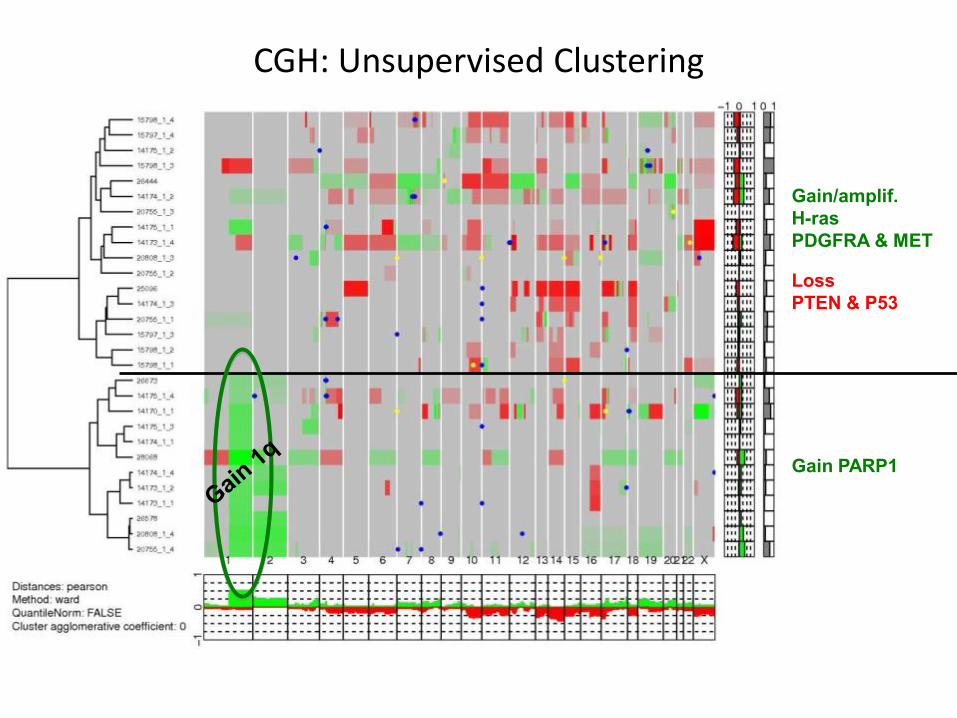
CGH: Unsupervised Clustering
Gain/amplif. H-ras PDGFRA & MET Loss PTEN & P53
Gain PARP1
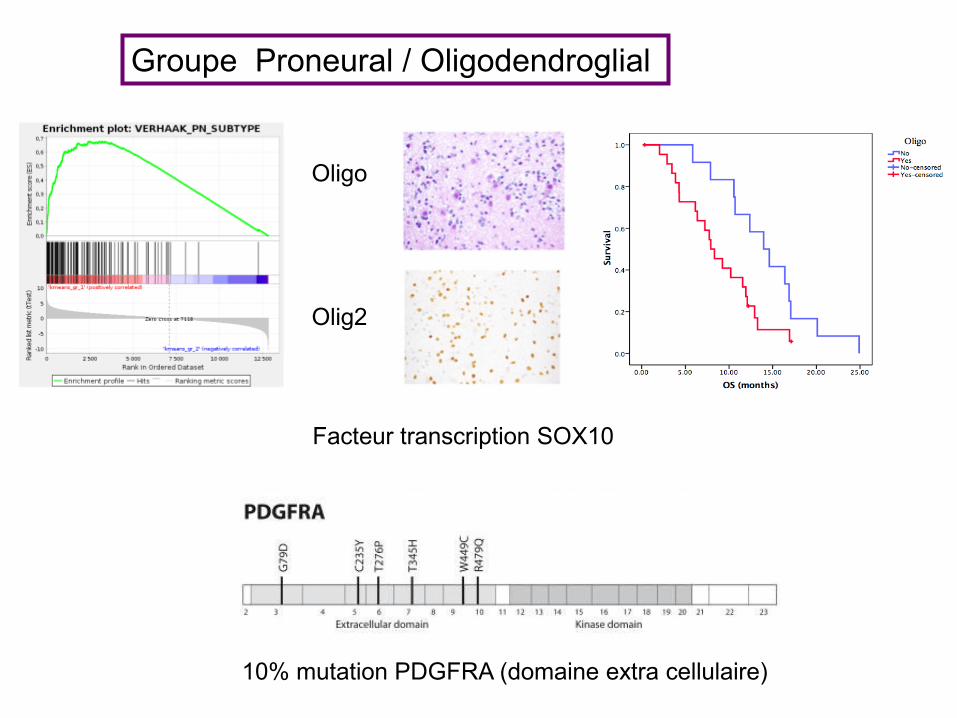
Groupe Proneural / Oligodendroglial
Oligo Olig2
10% mutation PDGFRA (domaine extra cellulaire)
Facteur transcription SOX10
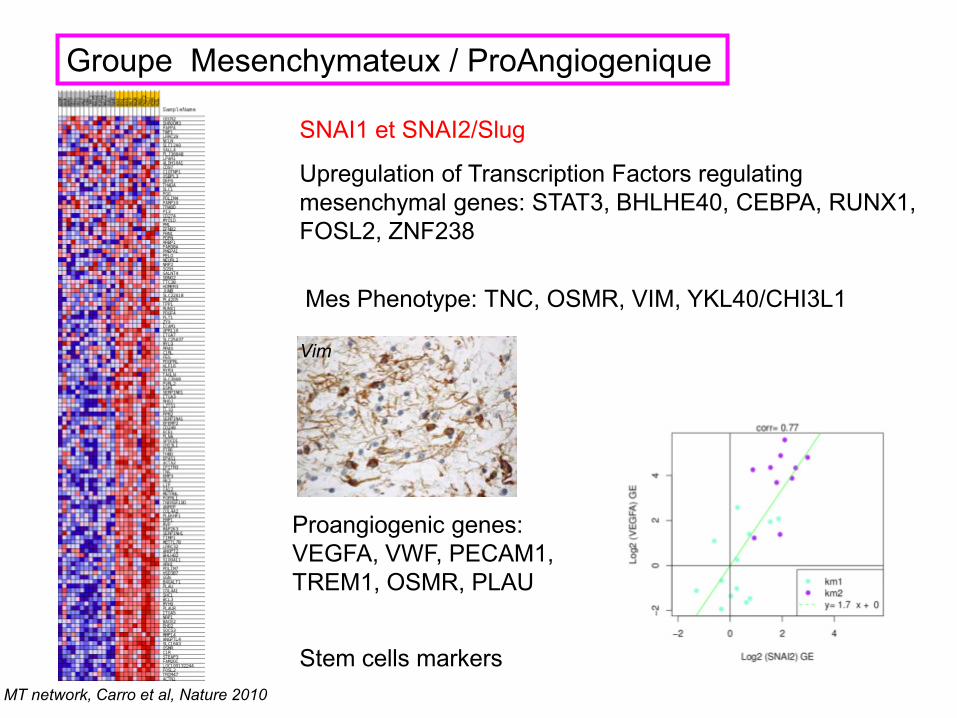
Groupe Mesenchymateux / ProAngiogenique
MT network, Carro et al, Nature 2010
Upregulation of Transcription Factors regulating mesenchymal genes: STAT3, BHLHE40, CEBPA, RUNX1, FOSL2, ZNF238
SNAI1 et SNAI2/Slug
Mes Phenotype: TNC, OSMR, VIM, YKL40/CHI3L1
Vim
Proangiogenic genes: VEGFA, VWF, PECAM1, TREM1, OSMR, PLAU
Stem cells markers
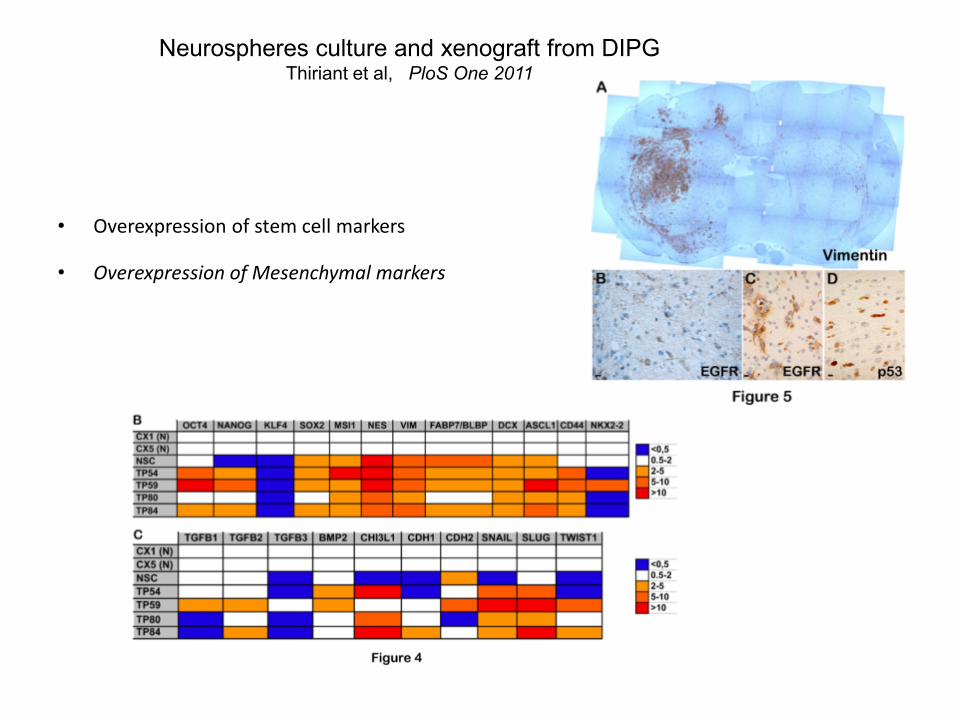
Neurospheres culture and xenograft from DIPG Thiriant et al, PloS One 2011
• Overexpression of stem cell markers
• Overexpression of Mesenchymal markers
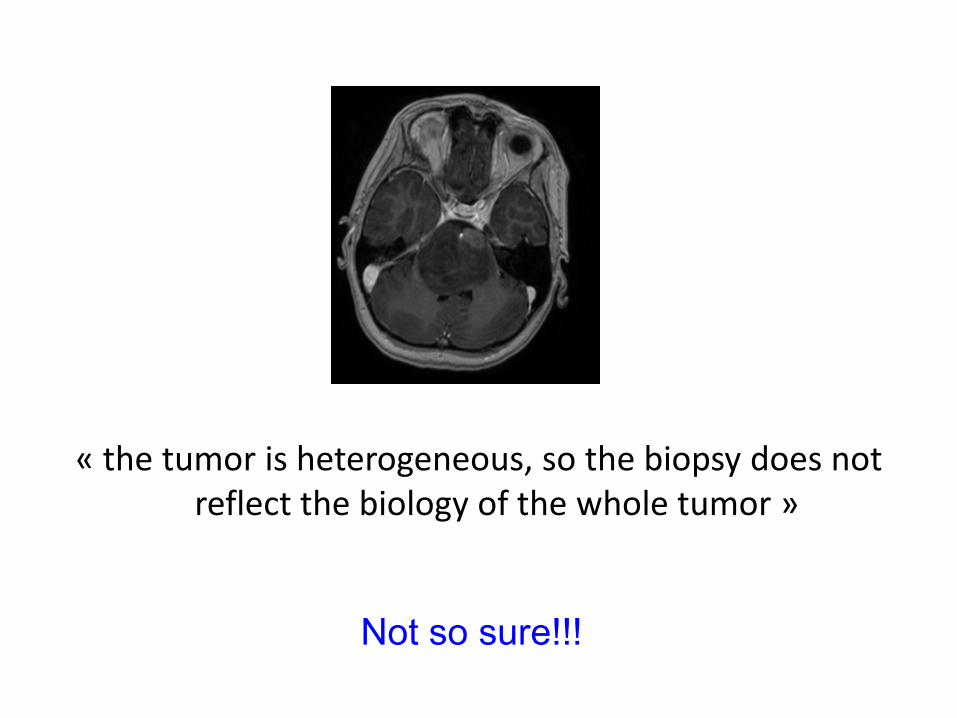
« the tumor is heterogeneous, so the biopsy does not reflect the biology of the whole tumor »
Not so sure!!!
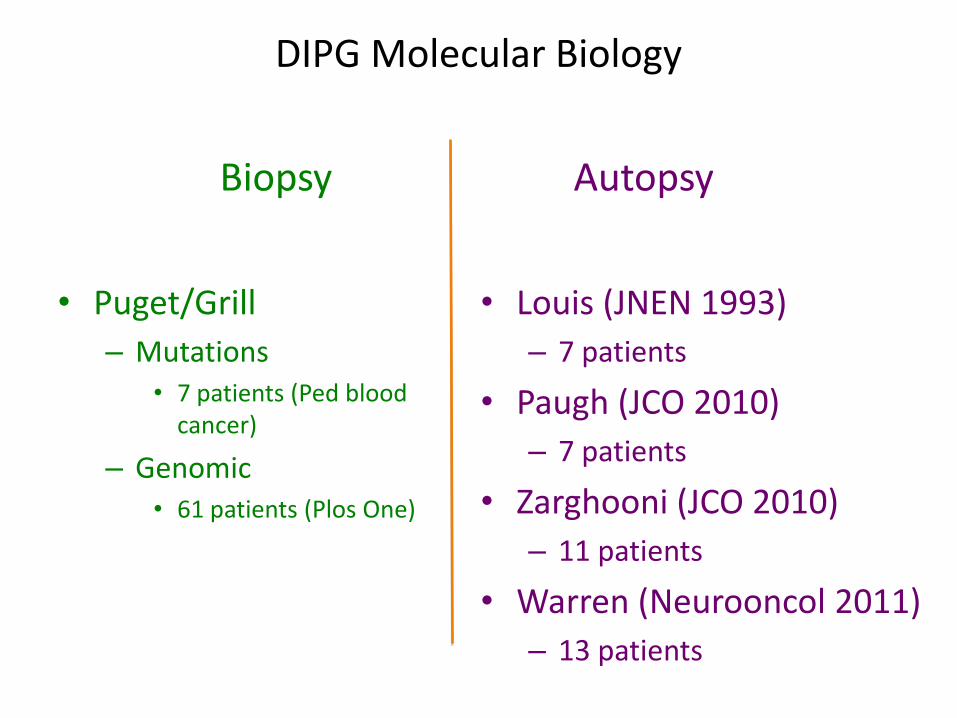
DIPG Molecular Biology
• Puget/Grill – Mutations
• 7 patients (Ped blood cancer)
– Genomic • 61 patients (Plos One)
• Louis (JNEN 1993) – 7 patients
• Paugh (JCO 2010) – 7 patients
• Zarghooni (JCO 2010) – 11 patients
• Warren (Neurooncol 2011) – 13 patients
Biopsy Autopsy
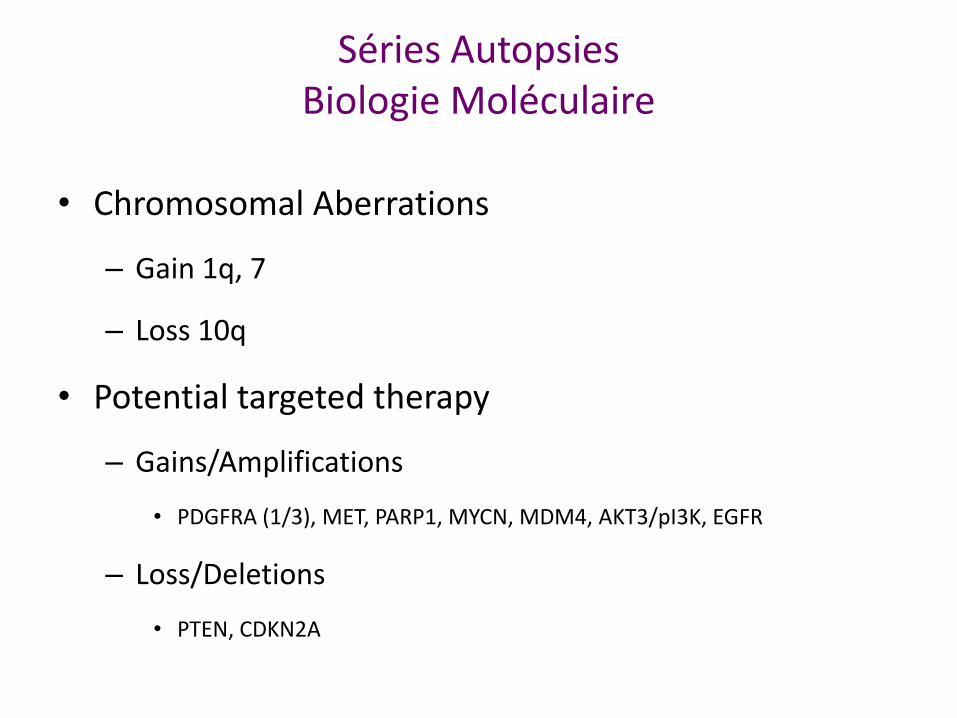
• Chromosomal Aberrations
– Gain 1q, 7
– Loss 10q
• Potential targeted therapy
– Gains/Amplifications
• PDGFRA (1/3), MET, PARP1, MYCN, MDM4, AKT3/pI3K, EGFR
– Loss/Deletions
• PTEN, CDKN2A
Séries Autopsies Biologie Moléculaire
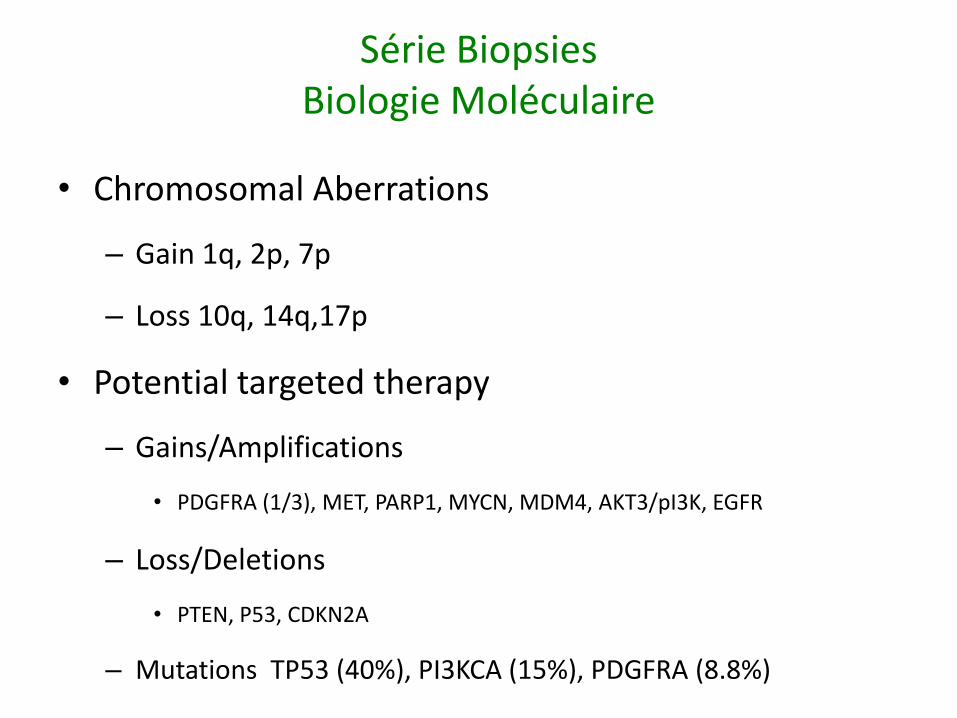
• Chromosomal Aberrations
– Gain 1q, 2p, 7p
– Loss 10q, 14q,17p
• Potential targeted therapy
– Gains/Amplifications
• PDGFRA (1/3), MET, PARP1, MYCN, MDM4, AKT3/pI3K, EGFR
– Loss/Deletions
• PTEN, P53, CDKN2A
– Mutations TP53 (40%), PI3KCA (15%), PDGFRA (8.8%)
Série Biopsies Biologie Moléculaire
The BIOlogical MEdicine for DIPG Eradication (BIOMEDE) trial
95
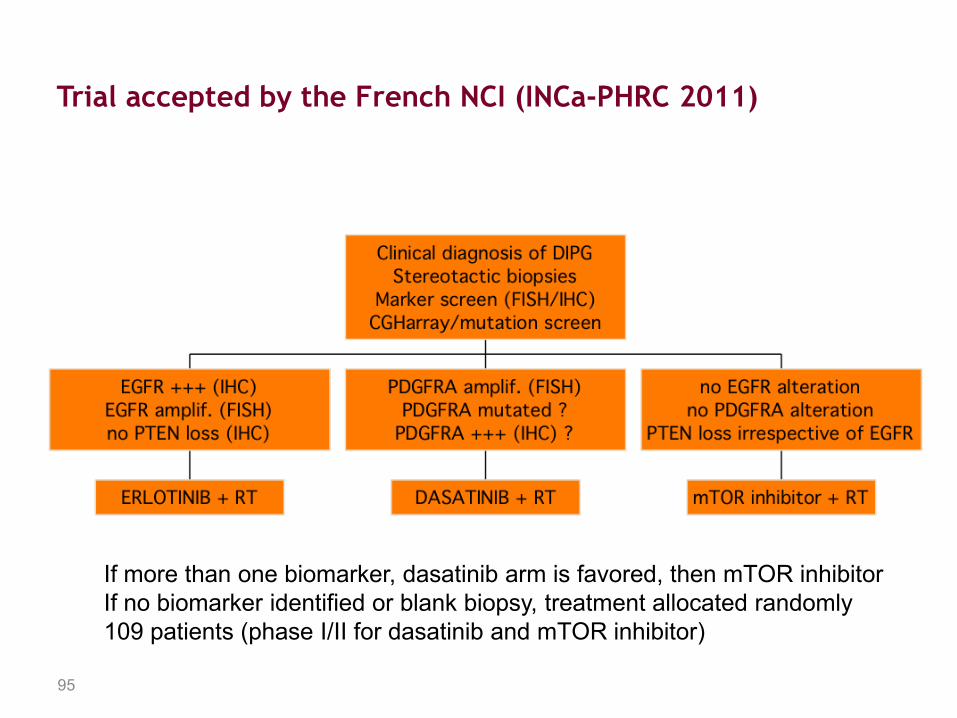
Trial accepted by the French NCI (INCa-PHRC 2011)
If more than one biomarker, dasatinib arm is favored, then mTOR inhibitor If no biomarker identified or blank biopsy, treatment allocated randomly 109 patients (phase I/II for dasatinib and mTOR inhibitor)
Thanks to parents and children who participated in this research, especially to Liv.
CNRS UMR 8203 (IGR): L. Mir, G. Vassal, B. Geoerger, S. Puget, J. Grill, C. Barbosa, V. Scott, E. Daudigos, E. DeCarli, F. Andreiuolo, L. Guerrini-Rousseau, C. Jubert, P. Opolon.
Functional Genomics and Bioinformatics (IGR): C. Philippe, B. Job, C. Richon, P. Dessen, V. Lazar.
Neuropathology (Sainte-Anne Hospital) P. Varlet, C. Miquel
INSERM U752 (Sainte-Anne) H. Chneiweiss, M.P Junier, B. Bessette
CRB Necker S. Dubleumortier, N. Brousse
Neurochirurgie pédiatrique (Necker) S. Puget, C. Sainte-Rose, M.Zerah, T.Roujeau, T. Blauwblomme
Royal Marsden (Sutton) C. Jones, R. Reis, D. Bax, D. Carvalho
Financial Support LEEM recherche, Etoile de Martin, ARNP, INCA-Cancéropole


















