
DIGITAL NERVE COMPRESSION - Northwestern...
9
NERVE COMPRESSION SYNDROMES 0749-0712/92 $0.00 + .20 DIGITAL NERVE COMPRESSION It is more than intriguing that the most common instance of irritative (compression, traction, friction, impact, and so on) neurop- athv in the body, that of the superficial cu- taneous nerves of the distal forearm, ~an-ist, and hand, has received the least attention in print and often in practice. After a decade of submitting abstracts about these problems to national meetings with never an acceptance, I finally concluded that no one was inter- ested. Any physidans who use dressings, anesthesia, casts or external fixation should be interested because the majority of these lesions arise from the contact of the body part and the enx~onment, and a good bit of that etiologic enx~onmentis provided bv the dex~ces that we use and the devices thdt are placed on us, including every treatment de- x~ce known, that is placed in or on that portion of the bodv. Such knowledgd of these conditions, as is passed from one generation of physidans to the next, seems usually to be in the form of test or trick questions about presumably rare entities with exotic names such as Warten- berg’s cheiralgia, s manacle wrist, 6 bowlers’ thumb, 7 "frisbee finger," and so on. From mv perspective of 45 vears of examining pdtients and 40.vears with a special interest m neuropathies of the hands, I have con- cluded that (1) nerve lesions of both the open type (lacerating) and the closed types (com- pression and oth6r ~types of physical and chemical trauma) are more common in the hands and feet than anywhere else, and (2) irritation or damage of some nerve or nerve element is present to some degree at some time in almost all of the forearm-wrist-hand conditions that we treat with either external apparatus or internal devices; commonly, of course, we use both and change frequently, giving ourselves exponential opportunities to irritate both nerves and patients. I have fre- quently played a game with myself, of seeing howlong it will take to find a nerve problem in a patient being treated for other than a nerve injury, when reviewing patients in a clinic or office. It never takes long! ANATOMY There is probably no nerve anatomy in the body that is better known to more people than the usual pattern of innervation in the wrist and hand. From every anatomy text to the color-coded Netter maps in the Ciba publications to the first article of this volume, this information has been disseminated - widely and well. It would be unrewarding to reiterate here these well-documented details of the cutaneous nerve distribution in the forearm, wrist, and hand, but it should be useful to discuss the risk factors inherent in the anatomy concerned, as follows: (1) Tissue depth of the nerve. Even in this area there are significant differences in the superfidal placement and the tissue thick- ness over the nerve. Almost all of the cuta- From the Departments of OrthopedicSurgeD, , Mayo GraduateSchoolof Medicine,Rochester, Minnesota;The University.of Texas HealthScience Centerat SanAntonio; Audie Murphy Veterans Administration Hospital; and The Han~ Center. San Antonio, Texas FL-LN-D CLINICS VOLL-~.fE 8 ¯ N~fBER 2. ~L-XY 1992 359
Transcript of DIGITAL NERVE COMPRESSION - Northwestern...

NERVE COMPRESSION SYNDROMES 0749-0712/92 $0.00 + .20
DIGITAL NERVE COMPRESSION
It is more than intriguing that the mostcommon instance of irritative (compression,traction, friction, impact, and so on) neurop-athv in the body, that of the superficial cu-taneous nerves of the distal forearm, ~an-ist,and hand, has received the least attention inprint and often in practice. After a decade ofsubmitting abstracts about these problems tonational meetings with never an acceptance,I finally concluded that no one was inter-ested. Any physidans who use dressings,anesthesia, casts or external fixation shouldbe interested because the majority of theselesions arise from the contact of the bodypart and the enx~onment, and a good bit ofthat etiologic enx~onment is provided bv thedex~ces that we use and the devices thdt areplaced on us, including every treatment de-x~ce known, that is placed in or on thatportion of the bodv.
Such knowledgd of these conditions, as ispassed from one generation of physidans tothe next, seems usually to be in the form oftest or trick questions about presumably rareentities with exotic names such as Warten-berg’s cheiralgia, s manacle wrist, 6 bowlers’thumb,7 "frisbee finger," and so on. Frommv perspective of 45 vears of examiningpdtients and 40.vears with a special interestm neuropathies of the hands, I have con-cluded that (1) nerve lesions of both the opentype (lacerating) and the closed types (com-pression and oth6r ~types of physical andchemical trauma) are more common in the
hands and feet than anywhere else, and (2)irritation or damage of some nerve or nerveelement is present to some degree at sometime in almost all of the forearm-wrist-handconditions that we treat with either externalapparatus or internal devices; commonly, ofcourse, we use both and change frequently,giving ourselves exponential opportunities toirritate both nerves and patients. I have fre-quently played a game with myself, of seeinghow long it will take to find a nerve problemin a patient being treated for other than anerve injury, when reviewing patients in aclinic or office. It never takes long!
ANATOMY
There is probably no nerve anatomy in thebody that is better known to more peoplethan the usual pattern of innervation in thewrist and hand. From every anatomy text tothe color-coded Netter maps in the Cibapublications to the first article of this volume,this information has been disseminated
- widely and well. It would be unrewarding toreiterate here these well-documented detailsof the cutaneous nerve distribution in theforearm, wrist, and hand, but it should beuseful to discuss the risk factors inherent inthe anatomy concerned, as follows:
(1) Tissue depth of the nerve. Even in thisarea there are significant differences in thesuperfidal placement and the tissue thick-ness over the nerve. Almost all of the cuta-
From the Departments of Orthopedic SurgeD,, Mayo Graduate School of Medicine, Rochester, Minnesota; TheUniversity. of Texas Health Science Center at San Antonio; Audie Murphy Veterans Administration Hospital; andThe Han~ Center. San Antonio, Texas
FL-LN-D CLINICS
VOLL-~.fE 8 ̄ N~fBER 2. ~L-XY 1992 359

~360 DOBYNS
" Figure 1. Digital nerve section froma bowler’s thumb operation showingsome atrophy of nerve fascicles,which are surrounded, separated,and engulfed by extensive, prolif-erative fibrous tissue. (Photo-graphed from an H & E slide, re-duced from x 28; from Dobyns JH:
~ _. "~--~;~ t Bowler’s thumb: Diagnosis andtreatment. J Bone Joint Surg
~ 54A:752, 754, 1972; with permis-,~. .- ~-~-- -_. sion.)
neous nerves can be palpated, but some,such as the branches of the dorsal radial andulnar sensor)." nerves, can be pinched becausethey are so close to the surface and so thi_rflypadded bv stretchable skin and minimumfat.
(2) Nearness qf the ne~,e to bone, joint, or hardforeign body. If the external trauma is thoughtof as the "hammer," then a firm, unyielding,tissue "anx4.1," against which to impactnerve, constitutes another risk factor. Thenerves at the side and dorsum of the wristand hand are at such risk, as are the nervespassing near sesamoids, near protuberantjoint margins, or other bony projections andnerves near foreign bodies, tumors, andother masses.
(3) Nerves that are relatively fixed in positionwith the normal excursion abili~ and lateraltranslational ability not present. This can be dueto various abnormalities of the normal ana-tomic restraints: carpal tunnel and Guvon’scanal at the proximal palm, fascial septae inthe digits, or to anomalies of nerve, muscle,vessel, musculotendinous unit, or fascia.This also applies to nerve end organs, suchas Padnian bodies, which have relativelysmall patterns of mobility,.
(4) Nerve communication. Another anatomic/physiologic fact about nerves is that they arecommunication systems, which confus~ dis-tally by overlap patterns and confuse at alllevels l~v reporting their perception messages(pain ahd esthesias) from all parts of thesystem to all parts of the system. It is notshfe, therefore, to assume that even the mostobvious and most distal lesion is the whole
problem without checking the rest of thesystem.
HISTOPATHOLOGY
The pathobhysiology of the compressivenerve lesion has been dealt with at lengthelsewhere in this issue, but it is not likelythat the bottom line will have changed fromthe multiple factor-multiple response reportsthat have filled the literature for several dec-ades. As indicated in the introduction, thehand is a battleground where even suchdamaging factors as toxic materials and vi-bration may be etiologic. The characteristiclesions for digital nerve compression have,so far, been restricted to two. Both are oftencalled "neuroma" in the literature, s" ~o, 2L 2~Because it is more probable that the twolesions are hyperplastic responses to irrita-tion than "new growths," ie, "neoplasms,"the term "neuroma" may be inappropriate.The terms "compressive" or "entrapment"or "traction" neuropathy are also often usedin the literature,3’ ~-6, s, 19, 20, 22, 23 but these terms
¯ imply nothing directly about the pathology.The more commonly recognized of the twoconditions at present is perhaps best termed"perineural fibrosis" and demonstrates a pro-liferation of perineural fibrous elements,which first surround and separate the neuralelements and eventually cause the neuralelements to atrophy, close, or disrupt (Fig.1). The fibrosis, of course, is seldom confined
to ttpartfibreadjaneotTheentitPaci~of difindipuscsuallcourtendeinstaclesdigit~mighin dineopcinimClini,histodeter
ETIO
Mato th(~)f pe~wrist,follo~ "constlMostbecau
Figure :the areadisplaye,of a bo~extensiwgraphedduced fr(Bowler’streatmen54A:752,sion.)

DIGITAL NERVE COMPRESSION361
;ration showingerve fascicles,ed, separated,,"tensive, profif-~sue. (Photo-& E slide, re-)m Dobyns JH:)iagnosis and,~ Joint SurgI; with pennis-
rest of the
to the nerve alone. Neighboring tissues alsoparticipate or mav even precede the nerve infibrotic response." Frequently affected are theadjacent fibrous tissues, vessels, subcuta-neous tissues, and even the skin7 (Fig. 2).The second of the two clinically recognizedentities involves a sensory end-organ, the
............ ,.~.. == ; - ....... ~a_~_a_~. c_orpus~le,- =~though: tiny branches::: ::: :ofdi~ita:!-nerve areaIs6i~v0tved::The ~pieai
section from findings are collections of large Pacinian cor-puscles with fibrosis around them and unu-sually prominent and numerous small nervescoursing between them. These nerves showendoneural and epineural fibrosis.l° In someinstances, the h~vperplastic Pacinian corpus-cles develop within the epineurium of thedigital nerves.11. :1 It is apparent that therercdght be considerable difficulty on occasionin differentiating hyperplastic lesions fromneoplastic lesions such as schwannomas, Pa-cinian schwannomas, or neurofibromas.Clinical history coupled with sophisticatedhistopathology will usually give a satisfactorydeterrnination.
:ompressiveh at length~ not likelyanged from~nse reports~everal dec-,ruction, theeven such
ials and vi-~hracteristic~sion have,th are oftenare?’ lo, 21, 24at the twoes to irrita-~eoplasms,’"~ppropriate.ntrapment"~ often used~hese terms~bathology.of the two
best termedtrates a pro-
elements,e the neuralthe neural
!isrupt (Fig.~m confined
ETIOLOGY
Manv references have already been madeto the almost unlimited sources for irritationof peripheral nerve elements in the forearm,~Tist, and hand. Thev can be grouped asfollows: (1) normal or ~nomalous restriction,cons~cfion or tether/rig sites for nerves.Most of the normal sites are well knownbecause of the clinical syndromes associated
Figur~ 2. Subcutaneous fat fromthe area lying between the tissuedisplayed in Figure 1 and the skinof a bowler’s thumb. There is ane~ensive fibrous reaction. (Photo-graphed from an H & E slide, re-duced from x 50; from Dobyns JH:B~wier’s thumb: Diagnosis andtreatment. J Bone Joint Surg54A:752, 754, 1972; with permis-sion.)
with them. Anomalous sites are bighJy vari-able but have been investigated in manyreports6, ~6; (2) repetitive irritation1, 4-s. ~0. ~-~s.~9’ ~; (3) peripheral neuropathy of any cause6, 23;(4) physical or toxic irritation other than com-pression, impact, or traction, such as chemi-cals, thermal injury, and vibration injury ~, ~,
" ~; ~s" ~S; and (5) nearby space:oc~upyin~ tissue-alfering lesions, such as tumors,masses, foreign bodies, and scar.
In spite of the ubiquitous nature of handuse and of hand damage, it is amazing howlittle information is processed about themany ways, other than by open wounding,that nerves are damaged. One exceedinglycommon way is by diagnostic and treatmentmethods applied to the hands. Damage byneedles and biopsy tools are open woundsof a sort, but they are often unrecognized atthe time and present as a closed lesion prob-lem, until and if an appropriate history isobtained. Damage by tourniquet, ring, wrap,bandage, tape, splint (even a simple fingersplint and maintenance materials can becausative), cast, pad, external fixator, pro~longed positioning of hand against object orvice versa--all these and more have beenadd continue to be culpable in creating nervedamage. The level of nerve damage can varyfrom an imperceptible irritation, at the clini-cal level, coming to attention only with ad-ditional insults, to complete closed disrup-tion of nerve fascicles, ie, from very minorneuropraxia to neurotmesis. The timing ofthe insult may vary from a quick, singleepisode (closed ring injury, for instance)

362 DOBYNS
constant repetition of the trauma over days,months, or vears.
DIAGNOSIS
As in all diagnoses, the first principle isawareness. So availabie are the handS forreview bv the patient and for examination bythe phys~ician that it is startling how much isoverlooked by both parties. Much pathologicinformation can be obtained by merely doingnerve status examination on patients withother complaints. Of those whose complaintsare related to the nerve pathology, most havepain or esthesias (hyp-, hyper-, or par-) their presenting complaint. Many of thesepatients have noted a thickening or a mass;in a few instances, the mass may be the onlycomplaint. The mass is usually related to thenerve pathology directly, altffough there areassociations such as ganglia, foreign bodygranulomas, and tumors of other sorts. If thelesion is not in the terminal branches, thenerve can usually be located proximal anddistal to the lesion level, and differentialmobility of those segments compared withthe lesion level can be demonstrated. Suchmanipulation of the nerve, or pressure,stretch, percussion, flipping, vibrating, andso on, will often result in tingling or otherparesthesias and a Tinel type of radiation.Sensor~, disturbance is often present to con-tact, t~vo-point discrimination (2PD), fiberstimulation, or vibration testing and may besevere to the point of anesthesia. Local fibro-sis of the skin and subcutaneous tissue isoften present; nutritional and sweat changesof the skin distal to the lesion may be noted.Most useful of all is reproduction of the painby pressure or other stress applied to thenerve at or near the lesion level. Cold, vibra-tion, or other stimulus may also be useful; ifa provocative cause can lde identified, utili-zation of this mechanism to reproduce thesymptoms is also confirmatory.
Differential diagnosis inclu~les the follow-hng: (1) All causes of masses and tumors the hand; on occasion, some of these maycoexist with the nerve lesion. (2) Peripheralneuropathy from any cause; this may alsocoexist with the lesion. (3) More proximalnerve lesions. These may coexist with thedigital lesions but are more likely to be pro-ducing the symptoms themselves. It is par-ticularly common for neuropathy of the radialsensorv nerves at the wrist or the dorsal
sensory branch of the ulnar nerve to mimicdigital neuropathy, because they do normallysupply the dorsum of the hand and thedorsum of digits 1 and 5, thumb, and littlefinger, as far as the dorsal tip and sometimespart of the palmar aspect also. (4) Musclecompartment syndromes in the hand or tis-sue ~compartment syndromes in the digits._Clasgi~ presentations give no problems, butthe early or mild compartment syndromewith its vague discomfort and mild firmnessmay suggest a nerve problem. (5) Vascularthrombosis, particularly of a vessel accom-panying a nerve in the hand or digit, willoften give similar symptoms because of irri-tation of the adjacent nerve; lesions of bothstructures may exist together. (6) Tenosyno-vitis, of the flexor tendons in particular, butsometimes even joint synovitis, may irritatenearbv nerves enough to produce similarsymptoms.
CLINICAL MANIFESTATIONS
Interestingly, the best known instance ofdigital nerve compression to the majority ofph~icians is not in the hand but in the foot,-and it is called Morton’s neuroma.~ It too isalmost certainly a repetitive insult and de-vice-related lesion, the device in questionbeing the shoe. Because there is an anatomicpredisposition risk factor, Morton’s neuromamight develop even in a barefoot population,but I have never heard of it. In the shoe-wearing population it is all too common, asmight be expected of an organ whose com-plaints are studiously ignored, whose sup-port device, the shoe, is often poorly fitting,and whose functional requirements are pro-longed and invariably bilateral. The plantarnerve or nerves involved are tethered by theiranatomy and abused bv their neighbors, themetatarsal heads. The pathology is identicalto that described in this article, ie, perineuraland endoneural fibrosis resulting in atrophy,then disruption of nerve fascicles. In thehand the most commonly reported lesion isthat of bowler’s thumb,~’ 7, 2~ although therehave been miscellaneous reports about anumber of other similar lesions, such as fris-bee finger, jeweler’s thumb, cheerleader’shand, harpist’s hand, guitar finger, penpusher’s paresthesia, batter’s thumb, tennisplayer’s finger, and so on.~’ 4, 5, 13, 14, 19, 22-24
From my experience, I can add the followingto this list: violinist’s finger, pipettist’s pulp,

DIGITAL NERVE COMPRESSION363
~ to mimico normally:1 and the, and littlesometimes
surgeon’s finger, dental hygenist’s finger,dentist’s thumb and fingers, wire twister’sdigit, electronic assembler’s tips, and a num-ber of other assorted occupational and avo-cational causes of digital neuropathv, from
tent myself with giving the data on threeinstances in which digital nerves were in-volved.
Case 1 in this group was a 54-year-old woman(4) Muscle transient to incapacitating. I am certain the with a comminuted Colles fracture, reduced else-~and or tis, ¯ list is inexhaustible, but with this publication where and treated with a snuggly fitting cast~the digitS~i-~@-~-- ¯ ~ ~’I h~i~-:-t0~il;~i~fe aal.int~ati~t :cteari~ ~ which .was :molded around the index metacarpalblems, bur ............ house f0i ~ thos6 wiH~ indtan~es Of the vast and head to maintain an ulnar deviation of thesyndrome
[d firmness~) Vascular;sel accom-digit, will
~use of irri-)ns of bothTenosyno-
#icular, but~nav irritateuce similar
instance ofmajority ofin the foot,a. ~’- It too isult and de-in questionan anatomica’s neuromapopulation,n the shoe-:ommon, aswhose com-whose sup-~orly fitting,.nts are pro-The plantar.~red by theirighbors, the: is identical.~, perineural~ in atrophy,cles. In theted lesion ishough th4re,rts about asuch as fris-
:heerleader’sfinger, pen
~umb, tennis5, 13, 14, 19, 22-24
:he following,ettist’s pulp,
and varied experience with manual neurop-athy, an experience that has never been as-sembled and correlated. My own experienceis overwhelmingly tilted, quantitatively, toinstances of manual neuropathv encounteredduring the treatment processes for upperlimb conditions. Both patients and medical
¯ managers permit pressures and apply ban-dages and devices, which can and of}en dodamage nerve. The amount of force involved,the trapped position and undeHying pressurepoints of the nerve, the frequent change involume of the soft-tissue compartment, thelack of congruence of device to part, theallergic and sensitivity responses of tissues,the time involved, an~J other factors make itimpossible to predict the safety factors ofsuch treatments. The response t~ this risk isdiscussed in the Treatment section.
A few case reports will be given to illustratethe above themes. In 1972 my co]Jeagues andI reported on 17 instances o(bowler’s thumbproblems, and I have seen about a dozensince then. 7 The best role model for thisgroup and for the other similar neuropathiesat the palmar base of the thumb (bat andracket holders, saw and hammer holders,and so on) remains case 1 from that report.The patient was a 27-year-old, ri~ht-handedman who had gradually develope~d a painfullump at the base of his right thumb alongwith callus of the overlying s’kin and numb-ness in the distribution of the ulnar digitalnerve of the thumb. He had been a leaguebowler for several years and had noted thatboth bowling and handling IBM cards, aregular part of his job, were aggravating. Histreatment will be discussed in the next sec-tion.
As mentioned many times before, the mostcommon group of f6rearm-wrist-hand neu-ropathies that I have encountered have beenin patients being treated for some conditionin those areas. Other contributors to thisissue discuss those problems associated withirritation of the forearm and wrist and dorsalhand sensory nerves, which are the mostfrequently seen in my experience. I will con-
wrist and hand. At 2 days after reduction, therewas mild swelling and moderate pain. One of thepain sites was at the molded area around theindex metacarpal, and it was further noted thatshe had tingling and numbness in the distributionof both the radial palmar sensory nerve and thedorsal radial sensory nerve to the index finger.With fingertrap traction and light countertractionapplied, the cast was removed and a new, morepadded cast applied with plaster only to themidlevel of the index metacarpal and without somuch molding. LucKily, position was maintained,pain and swelling were controlled, and fracturehealing occurred. ’The recovering cutaneousnerves went through a period of hyperpathia,with special treatment measures required for afew weeks, but recovery was complete in 3months.
Qase 2 of this group was a 60-year-old womanwho had a giant cell tumor of tendon sheathremoved from the distal portion of a finger withpalmar digital nerve block for anesthesia and a ~rubber glove ring at the base of the digit fortourniquet (in place about 45 minutes). She com-plained of numbness and tingling in the distri-
¯ ..bution of the digital nerve opposite to the side ofthe tumor, when sensation returned the followingday. No treatment was required, but a Tinel’s signdeveloped at the site of the tourniquet and slowlymoved distally over the next few months.
Case 3 of this group was a 22-year-old man whowas seen about 1 week after a PIP dislocation hadbeen reduced and a snug dorsal, digit-based,monarticular splint had been applied to the prox-imal phalanx area, but extending out over the PIPjoint to act as an extension block splint. The fingerwas massively swollen, painful, and numb. Thesplint and the fight tape wrap that anchored itwere removed, and the entire hand was placed ina soft, resilient dressing for a few days. It was not
necessary to splint the finger again~ Joint motionand nerve recovery gradually improved, but whenhe was last seen at 1 vear, mild hypesthesia inthe finger pad was still "present.
The final group of cases will consist ofoccupational causes of digital neuropathy.
Case 1 of this group was a 58-year-old gyneco-logic surgeon who had numbness and tingling of
364 DOBYNS
all fingers of his nondommant hand, present forabout 2 years and increasing to the point that it:’.as interfering with his surgeD’ (he liked to retractfor himself and held a retractor tightly in thatiaand for most of the case). He had a mild gener-~ed peripheral neuropathy, but there were lo-ca!izing signs at the digital nerves that held theretractor, so it was believed that the many yearsof retractor holding represented the principalcause of i~eatOp~!thy. With g6rne dffficui@ he waspersuaded to allow an assistant to hold the retrac-tor and he had improved when seen 1 year later.
Case 2 of this group was a dental hygienist whobegan to note pain and numbness in several digits,but particularly the index finger of her left hand,which was the holder for a new ~qbrating tool thatshe had begun to use about 18 months previously.5he had pulp tenderness in several fingers, alongwith hypesthesia and paresthesias in the distalhalf of the index finger. She stopped using the~brating tool and returned to manual instrumen-ta~on, but she was unable to continue full-timeden~al-hygiene work, even though she improved.5he later sued the dental instrument companyand was awaiting a worker’s compensation ap-peal.
Case 3 in this group was a 28-vear-old womanwho was first violin and assistant conductor of arnux’dcipal symphony orchestra. In addition to herperformance duties, she practiced about 6 hoursper day and had done so for about 20 vears. Shewas finding it increasingly difficult to p~actice andto play, however, because of a painful mass at thetip of the ring finger of her fingering hand. Shehad first ignored it, then used a small bandage,simddar to a Dr. Scholl’s bunion pad, over it.However, the mass continued to increase in sizeand discomfort and was interfering badly withher technique. The mass was subcutaneous, verynear the tip of the pad, and her pain was repro-duced exactly when pressure was applied. Shedid not feel "able to alter her work or schedule,and no protection could b~ dex%ed that did notin:e.ffere with her performance technique. Treat-ment is presented in the next section.
TREATMENT
The most effective treatment is prevention.Next is protedVion ’and modification or evencessation bf the provocative activitv. Surgeryis useful in some instances, but it fs a sign offaiiure because it means the diagnosis wasdeiaved too long or that protective treatmenthas been inadequate, usually owing to non-compliance. Because many bf the problemsdi%mssed here are iatrog~nic, it is obviousthat ~eater care in the use of positioning,
the application of external materials, and thepost-treatment counseling of patients is re-quired. Knowledge of anatomy, materials,and techniques are all important, but proba-bly most important is ensuring that the pa-tient is so comfortable in the bandage orsupport that little or no pain medication is
........required. If ~uch medication is required, vig-ilance must be redoubled. In occupationaland avocational risk areas, it also should bepossible to anticipate and avoid the prob-lems, if all who are involved are alert for risksituations. In retrospect, it is nearly ahvaysquite obvious what should have beenavoided. So many of the digital compressionlesions are of the repetitive stress variety thatthe usual rules for controlling repetitivestress lesions apply, ie, modify or stop theaggravating activity. The effect of both pre-vention and protection has been seen inbowling, not because of any sustained, ur-gent, industry-wide action but simply be-cause the problem is well known to all con-cerned and the measures to avoid it arepracticed with fair consistency. These meas-ures consist of stopping the provocative ac-tivity until symptoms improve. Then, a grad-uated return to bowling is attempted withpreliminary retooling of the thumb inserthole or an alteration of other features of thetechnique, such as digit insert depth or num-ber, hole placement, ball weight, and so on.For other activities that may also aggravatethe damage area, the use of a digit-based,short, thumb shell (from carpometacarpal tointerphalangeal levels) is adequate prote¢-..ti0n. If symptoms cannot be controlled inthese ways, complete cessation of the pro-vocative activities and/or surgery are to beconsidered.
SURGICAL TREATMENT
As already indicated, surgery is usually alast resort, if the diagnosis is known u:ithnear certainty. A good history of either sig-nificant single or repetitive episode traumaplus the findings of nerve symptoms, nervedysfunction, and findings suggestive of alocalized nerve lesion is not always obtained.The hand is the locale of so many injuriesand so many masses and tumors, some ofwhich are of life-threatening import, thatsurgical examination and biopsy may be theonly foolproof way of establishing a certaindiagnosis. Furthermore, granulomas, gan-glions, and other masses may be found in
conthoMRfereit isandNo~appWhposprodireobv"frctheonematquemattrea
S~pre~,ure,~seglgenconoptibraIPaci
¯ excit-hattum-sub~marservthecontner~exp~waspainof s~damThe~nervor lecapaMu~ana[~excisgeneleadas re
M~nerv,perirof thboth
?rials, and the~atients is re-Ly, materials,nt, but proba-,~ that the pa-.~ bandage ormedication isrequired, vig- ....occupational
so should be,id the prob-~ alert for risk~earlv alwavs
ha(’e be6ncompressions varie~- that~g repetitive¯ or stop theof both pre-een seen in~stained, ur-’ simply be-n to all con-avoid it areThese meas-)vocative ac-hen, a grad-’mpted with~umb insert~tures of theFth or num-, and so on..o aggravatedigit-based,.etacarpal tolate protec-~ntrolled inof the pro:v are to be
is usually anown ~:itheither sig-..
)de traumaoms, nerve~stive of as obtained.ny injuriess, some of~port, thatnay be theg a certainmas, gan-
found in
DIGITAL NERVE COMPRESSION365
conjunction with areas of nerve fibrosis. AI- sionallv, an epineural release may be consid-though new imaging techniques, such as ered if the intraneural scar seems very firm.MRI, are becoming very valuable in the dif- Electrical conductivity testing at the tableferentiation of tissues, including neoplasms, may well be the best method of selectingit is unlikely that they will supplant surgery nerves for any type of internal lysis, but theand histolo~ic study ~or diagnostic certainty, crude instrumentation traditionally availableNor are needle or i~unch biopsy techni_ques has~_l_ed me~ t_o~ _chog_s..e. the~-~o~td~=~teetmique of ....approp~ate for: lesions in or near nerves.When surgery is elected for diagnostic pur-poses, it is carried out in the usual tumorprotocol manner with a longitudinal incisiondirectly over the lesionat area. If it becomesob~io~s from the gross examination or from"frozen section" pathologic examination thatthe problem is a straightforward example ofone of the two lesions discussed, surgicalmanagement proceeds as outlined subse-quently. If there is doubt about tissue confir-mation, the incision is closed and furthertreatment awaits tissue diagnosis.
Surgical treatment for a specific nerve com-pression lesion usually consists of (1) meas-ures to lyse and protect the damaged nervesegment, or (2) excision of the lesion. general, option (1) is applied to lesions continuity along the course of a nerve branch;option (2) is applied to small terminalbranches and to the Pacinian tumors. If thePacinian tumor is located terminally, it isexcised along with any small nerve branchesthat are included in tl-[e mass. If the Paciniantumor is located along the nerve trunk ~n asubepineural position, it is removed, but asman?, nerve fascicles as possible are p{e-served in the adjacent nerve trunk. In theo~,the option of excising one of the "lesions incontinuity" followed by direct repair or bynerve graft replacement exists. I have ha~experience with only one case in which thiswas done.v Results Were satisfactory, loss ofpain and return of 2PD of 8 mm, but returnof sensibility was better in cases in which thedamaged nerve segment was preserved.There is a surprising capacity of the damagednerve, even when sigrLificantly enlarged and/or len~hened, to regain adequate functionalcapacib,, if it can be kept from, further abut.Much experience with Morton s neuroma~ ~i,analogous problem in the foot, indicates, thatexcision of the lesions in continuity, althoughgenerally controlling the pain, ~ccasionallylead to "pain dysfunction syndromes’" suchas reflex sympathetic dystrophy. ~-~
Mobilization and lvsis of the involvedner,-e segment begins with extraneural andperineural lysis, with exdsion of all or mostof the scar until the nerve is freely mobile inboth longitudinal and lateral planes. Occa-
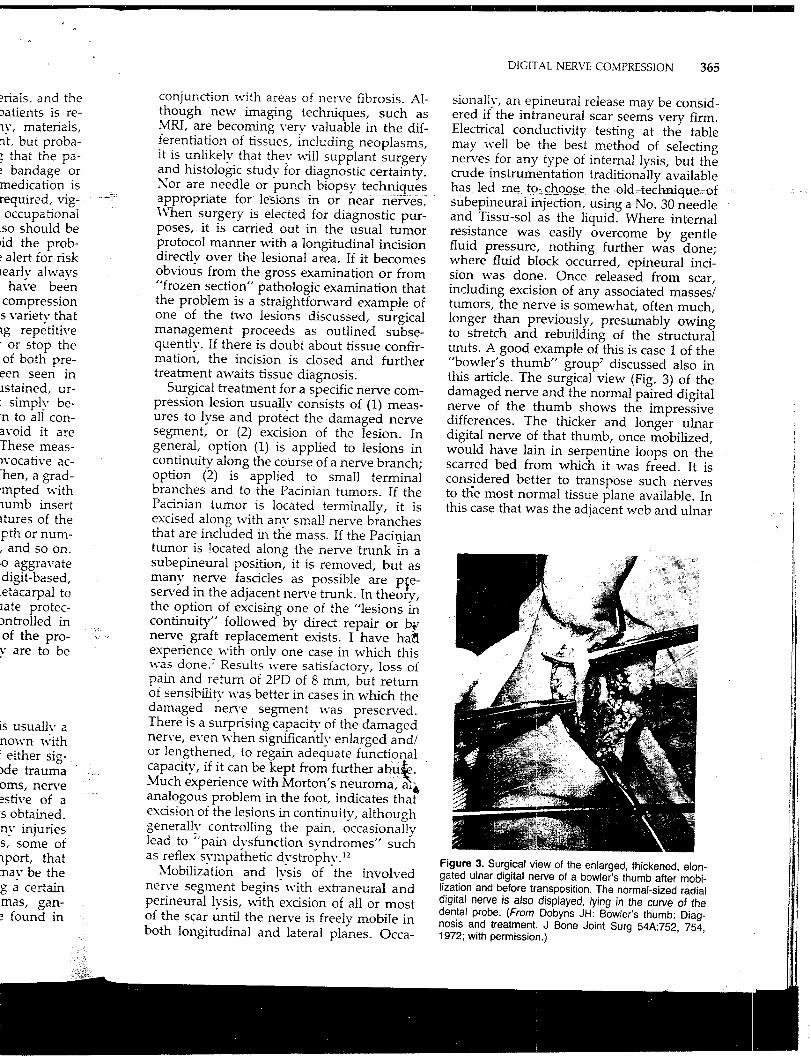
subepineurai injection, using a No. 30 needleand Tissu-sol as the liquid. Where internalresistance was easily overcome by gentlefluid pressure, nothing further was done;where fluid block occurred, epineural inci-sion was done. Once released from scar,including excision of any associated masses/tumors, the nerve is somewhat, often much,longer than previously, presumably owingto stretch and rebuilding of the structuralunits. A good example of this is case 1 of the"bowler’s thumb" group 7 discussed also inthis article. The surgical view (Fig. 3) of thedamaged nerve and the normal paired digitalnerve of the thumb shows the impressivedifferences. The thicker and longer ulnardigital nerve of that thumb, once mobilized,would have lain in serpentine loops on thescarred bed from which it was freed. It isconsidered better to transpose such nervesto tl~e most normal tissue plane available. Inthis case that was the adjacent web and ulnar
Figure 3. Surgical view of the enlarged, thickened, elon-gated ulnar digital nerve of a bowler’s thumb after mobi-lization and before transposition. The normal-sized radialdigital nerve is also displayed, lying in the curve of thedental probe. (From Dobyns JH: Bowler’s thumb: Diag-nosis and treatment. J Bone Joint Surg 54A:752, 754,1972; with permission.)
366 DOB~.~S
midlateral aspect of the thumb, maintaining the device). There is much that professionals
the new position bv fascial flaps obtained can do in medicine and in trade and specialfrom the thenar fasc~a and the adductor apo- interest journals to alert each other to theneurosis. In other cases it has been more dangers inherent in the use of certain devicesfeasible to place the damaged nerve in the and certain techniques, particularly medical
.same compartment as the other neurovascu- treatment techniques, and particularly tech-..... ~)i-r i~ndl~~fn--~lq~’ di~L"~r~-so-~e a~~~uch ni~[ues permRting or requiring repetitive
as the distal palm, lumbricals or other mus- compression, traction, or impact. I renew mydes are available to be transferred over thenerve segments.~; The ingenious surgeon cannearh" ahvays find a site to which to trans-pose the nerve and a method by which tomaintain it.
As previously noted, exdsion is occasion-ally the preferred treatment, particularlywlqen the lesion is in terminal branches or
involves Pacinian corpuscle hyperplasia. Incase 3 in the occupational neuropathy group,the violinist/conductor had such a lesion, ie,a combination of terminal branch nerve hy-perplasia and Pacinian bodv hyperplasia atexactly the spot where finger tip met violinstring. The mass was exdsed and she didlose sensibility in that area, 10 mm in diam-eter, but gradually diminishing to half ofthat. The numbness and the eventual callusin the area were somewhat bothersome also,but not nearly as much as the prior lesion.At some 10 years postoperatively, she wasstill pursuing~ her profession, although in ateaching capad~’:
Results, in general, have been good withboth dosed and open treatment of digitalnerve compression lesions, except in thosefew in which "pain-dysfunction s,vndromes"developed. Even in these, the neuroma painwas nearly ahvavs controlled; Other aspectsof these svndromes seemed responsible forthe contin~aed problems. Nevertheless, thereare often permanent residua, usually in termsof sensitivity to the provocative activity orsimilar activities. The bowler described in thisarticle did not return to bowling, but othersdid, kno~q.ng tha~ it involved a risk. The~-iokinist continued the provocative activitybut did modify, her activities to diminish theamount of provocation. Only those, personsin whom the diagnosis is made" very earlyand adequate protection and relief are ob-tained immediately seem to recover withoutresidual sensitivity to similar abuse. Littlecan be done about the incidence of single-episode accidental injury to digital nerves,except to point out the risk element in suchactivities as opening sofa-drink-can openingrings (the consumer should be wary, but themanufactxtrer should be induced to change
offer to act as a clearinghouse for informationabout the clinical incidence of distal upperlimb compression neuropathy. I am certainthat the reported incidence of such problemsis but the tip of a very large iceberg.
SUMMARY
A review of the relatively small body ofliterature about digital nerve compressioninjuries has been supplemented by the au-thor’s experience and interest of over 40years. The principal lesions involved are oftwo types: (1) fibrosis about, around, and the nerve; and (2) reactive hyperplasia of thenerve support elements and sometimes ofspecial end organs, Pacinian corpuscles, andeven of tl~e nerve fibers themselves. Nervesigns and symptoms often accompanied bya mass in chronic cases are diagnostic. Themost important features of the topic are therecognition by all of the risk elements, em-bodied in many personal and professionaldevices and techniques. These risk elementsare present in all parts of our society, includ-ing home and occupational, avocational, andmedical situations. Treatment is best pro-.vided by awareness of risk and avoidance ofrisk activities, particularly repetitive risk ac-tivities. Surgery is preferably avoided, butwhen indicated it is effective. It consists prin-cipally of lysis and protective positioning ofthe damaged nerve or, on occasion, of exci-sion of terminal or end-organ lesions. Moreinformation must be gathered about theseexceedingly common but notably under-re-ported problems.
References
1. Belsky MR, MilIender LH: Bowler’s thumb in abaseball player: A case report. Orthopedics 3(2):122-123, 1980
2. Brammer AJ: Assessing the severity of the neurolog-ical component of the hand-arm vibration syndrome.Scand J Work Environ Health 12(4):428-431, 1986
3. Brown FE: Compression neuropathies of the upperextremities. In Jupiter JB (ed): Flynn’s Hand Surgery ...............
ofessionalsand special .~:her to theain devicesIv medicallfarlv tech-
repetitive ~:~.--renew mv - =: -
~formafio~astal upperam certain~ problems ,.
.11 body of~mpressionbv the au-~f over 40ved are ofnd, and in[asia of theaetimes oflsc]es, andees. Nervetpanied byaostic. Thepic are thenents, em-rofessionalk elements!,ty, includ-tional, andbest pro-
’oidance ofve risk ac-3ided, but~sists prin-itioning of~n, of exd-ons. More)out theseunder-re-
ed 4. Baltimore, Williams and Wilkins, 1991, pp 518-
4. Carragee El Hentz VR: Repetitive trauma and nervecompression. Orthop CIin North Am 19(1):157-164,i988
5. Chaplin E, Kasdan ML, Corwin HM: Occupationalneurology and the hand. Hand Clin 2(3):513-524,1986
6. Dellon AL, MacKinnon SE:_Radial sensor3,, nerveentrapment in the forearm. J Hand Surg 1!A:199-205, 1986
- Dobvns JH, O’Brien E, Linscheid R, et al: Bowler’sthumb: Diagnosis and treatment. J Bone Joint Surg54A(4):751-755, 1972
8. Ehrlich W, Dellon AL, MacKinnon SE: Cheiralgiaparesthetica (entrapment of the radial sensory,nerve). J Hand Surg tlA:196-198, 1986
9. Ekenvall L: Is vibration white finger a primaD, sym-pathetic nerve injury? Br J Ind Med 43(10):702-706,1986
10. Fletcher CDM, Theaker JM: Digital Pacinian neu-roma: A disfi.ncfive hyperplastic lesion. Histopa-thotogy 15:249-256, 1989
11. Friedman HI: Subepineural pacinian corpuscle: Acause of distal pain. Plast Recon_-tr Surg 74(5):699-703, 1984
12. Gauthier G: Thomas Morton’s disease: A nerveentrapment syndrome. Clin Orthop 142:90-92, 1979
13. Hauswatd M: Pen pusher’s paresthesia [letter].JAMA 255:2164, 1986
14. Hochberg FH, Leffert RD, Heller MD, et al: Handdifficulties among musicians. JAMA 249:1869-1872,1983
Address reprint req ~es.’ts to
James H. Dob.vns, MD7940 Floyd Curl Drive, Suite 900San Antonio, -IX 78229
DIGITAL NERVE COMPRESSION 367
15. Itoh Y: Circulatory disturbances in the throwinghand of baseball pitchers. Am J Sports Med15(3):264-269, 1987
16. Kaplan EB, Spinner M: Normal and anomalousinnervation patterns in the upper extremity. In OmerGE Jr, Spinner M (eds): Management of PeripheralNerve Problems. Philadelphia, W.B. Saunders, 1980,pp 75-99
, 1Z Karev A, Stahl A: Treatment of painful nerve lesionsin the palm by ’rerouting’ of the digital nerve. JHand Surg 11A(4):539-542, 1986
18. Lundborg G, Dahlin LB, Hansson H-A, et al: Vibra-tion Exposure and Peripheral Nerve Damage. J HandSurg 15A:346-351, 1990
19. Naso SJ Jr: Compression of the digital nerve, a newentity in tennis players. Orthop Rev 13(9):47-49,1984
20. Ochoa J: Nerve fiber pathology in acute and chroniccompression. In Omer GE Jr, Spinner M (eds):Management of Peripheral Nerve Problems. Phila-delphia, W.B. Saunders, 1980, pp 487-501
21. Rhode CM, Jennings WD: Pacinian corpuscle neu-roma of digital nerves. South Med J 68:86-89, 1975
22. Shields RW Jr: Median palmar digital neuropathy ina cheerleader. Arch Phys Med Rehabil 67(11):824-826, 1986
23. Spinner M: Management of nerve compression le-sions of the upper extremity. In Omer GE Jr, SpinnerM (eds): Management of Peripheral Nerve Problems.Philadelphia, W.B. Saunders, 1980, pp 569-592
24. Thirupathi R, Forman D: The jeweler’s thumb--anoccupational neuroma: A case report. Orthopedics6:438-440, 1983
thumb in adics 3(2):122-
the neurolog-)n syndrome.
of the upper~and~urlse~y,


















