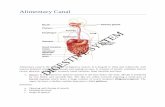
Digestive System (Alimentary Canal + Digestive Glands + Digestive Process)

of 57
Upload
fercilyn-marbanCategory
view
215download
08/8/2019 Digestive System Krva
1/33
8/8/2019 Digestive System Krva
2/33
8/8/2019 Digestive System Krva
3/33
8/8/2019 Digestive System Krva
4/33
8/8/2019 Digestive System Krva
5/33
8/8/2019 Digestive System Krva
6/33
8/8/2019 Digestive System Krva
7/33
*Increased flatulence
Colonoscopy, SigmoidoscopyComplications*Hemorrhage
*Bleeding, cold clammy skin*Hypotension, tachycardia, tachypnea
*Over-sedation*Difficulty arousing, poor resp effort*Maintain open airway, O2, antidote, VS
*Perforation:*Chest or abd pain*Fever, nausea, vomiting, abdominal distention
*Aspiration:*NPO until return gag*Dyspnea, tachypnea, tachycardia, fever
Endoscopy
*ANALYSISNursing Diagnoses*Risk for deficient fluid volume*Imbalanced nutrition: less than body requirement*Diarrhea*Constipation*Pain*Impaired skin integrity
*INTERVENTIONS
*GASTROINTESTINAL FEEDING
*GASTROINTESTINAL INTUBATION (LAVAGE) Tubes:*Short-term: NGT
*Levin: single (low-intermittent)*Salem-Sump: double (low continuous)
Tubes
8/8/2019 Digestive System Krva
8/33
*Long-term:*PEG: Percutaneous endoscopic gastrostomy*PEJ: Percutaneous endoscopic jejunostomy
Nasogastric Tube insertion*High Fowlers position*Measure: Tip of noseearlobesternum*Lubricate:*Hyperextend neck, tilt head forward (oropharnyx), sip water with a straw*Stop: gag, withdraw slightly
Nasogastric tube insertion*Tube placement:
*pH ( 4 - 6), 5-10 ml air, X-ray:*Secure: bridge of nose, gown
Tube Feeding Administration*Nsg considerations:
*Room temp, shake well, check expiry*Flush:
*Assess BS*Aspirate residual, return, hold >100
*Position: HF, right side (comatose)*Patency: Q 4 hours: 30 mL of saline
*Frequent oral care, hard candy, ice chips*Documentation: feeding, skin
Tube Feeding Administration*Bolus
*Resembles normal meal pattern*Large amt: 300-400 ml, 10 min, Q 3-6 h
*Cyclical (infusion pump)*Administered day/nighttime for 8-16h
*Continuous (Infusion pump)*Continually for 24 hrs, change cont daily*Solution: 4hr-period, flush Q 4 hrs
Gastrointestinal intubation*NGT, Intestinal tubes
8/8/2019 Digestive System Krva
9/33
*Insertion:*Recording:
*Suction setting:*Recording: color, consistency, amount*Monitoring: skin breakdown
Nasoenteric (Intestinal) Tubes*Intestinal Tubes: intestinal obstruction
*Cantor, Harris: Single lumen, tungsten*Miller-Abbott: Double lumen:
Intestinal Tube*Removal:
*Remove weight with 5 ml syringe*Exhale: remove 1-2 in Q hour smooth pull
Total Parenteral Nutrition*Nutrients are infused into a vein
*Total Parenteral Nutrition (TPN):*Hypertonic glucose 20 70%
*Peripheral Vein Parenteral Nutrition (PPN)*Glucose < 20%
Central Venous Access*Tunneled caths (Hickman/Groshong cath):
*PICC: antecubital fossa to SVC
*Porta Caths: injection port
Complications*Phlebitis/Thrombophlebitis:
*Mechanical or chemical trauma*Assessment:
*Redness, pain, warmth, swelling
8/8/2019 Digestive System Krva
10/33
*Interventions:*Stop IV, warm moist compress*Change IV site (Q 48 72 hrs)*Never irrigate
Complications*Air Embolism: 5 ml or more
*Dyspnea, cyanosis, tachycardia, hypotension
*Interventions:*Prevention: Prime, do not allow to dry*Stop, Left side with head down*O2, Call MD
Complications*Circulatory Overload (Hypervolemia)
*SOB, frothy sputum, cough, crackles, engorged neck veins, inc BP
*Interventions:*Slow, elevate HOB*VS, Call MD
*PHARMACOLOGYAntacid*Neutralize gastric acid secretions; nonsystemic
*Aluminum Hydroxide (Amphogel)*Aluminum Hydroxide and Magnesium salt (Maalox, Gaviscon)*Sodium Bicarbonate (Rolaids, Tums)*Nsg Interventions:*Avoid within 1-2 hrs of other meds
Histamine (H2) Receptor Antagonists*Reduce gastric acid secretion
*Cimetidine (Tagamet),*Ranitidine (Zantac)*Nizatidine (Axid), Famotidine (Pepcid)
*Nsg Interventions:*Take with or after meals*Do not take with antacids
Proton Pump Inhibitors (PPI)*Inhibit enzyme that produces gastric acid
*Omeprazole (Prilosec)*Lansoprazole (Prevacid)
*Nsg Interventions:*Before meals*Do not crush, do not open
8/8/2019 Digestive System Krva
11/33
Cytoprotective Agent*Provides protective barrier to acid
*Sucralfate (Carafate)
*Nsg Interventions:*Avoid antacids
Prostaglandin Analogue*Suppress gastric acid secretion*Increases protective mucus and mucosal blood flow
*Misoprostol (Cytotec)
*Nsg Interventions:*Contraindicated in pregnancy
Cholinergic Blocker (Antispasmodic)*Inhibit GI motility and gastric secretions
*Dicyclomine hydrochloride (Bentyl)*Hyoscyamine (Levsin)*Propantheline (Pro-Banthine)
*Nsg Interventions:*Do not administer with antacid*Use in caution with glaucoma
Intestinal Antibiotics*Decrease bacteria (GIT), sterilize bowel before surgery
*Kanamycin Sulfate (Kantrex)*Neomycin Sulfate (Mycifradin Sulfate)
*Gastrointestinal DisordersLocation of GI diseasesStomatitisStomatitis*Inflammation of mouth mucous membrane
Stomatitis*Causes:
*Trauma to mucous membranes*Irritation*Vitamin C deficiency (scurvy):*Fungal infection: Candida albicans (Candidiasis)
Stomatitis*Causes:
*Herpes simplex: Cold sore*HIV and AIDS:
8/8/2019 Digestive System Krva
12/33
*Gonorrhea:*Measles*Leukemia:
Stomatitis*Assessment:
*Pain*Ulcerations*Swollen lymph nodes
Stomatitis*Dx Tests:
*CBC*Culture of scraping
Stomatitis*Nursing Interventions:
*Good oral hygiene*Avoid Irritating foods and beverages, spicy foods, Hot foods and drinks*Cool liquids, easily be swallowed*Topical anesthetics: Benzocaine anesthetics (Anbesol), 2% viscous lidocaine
mouthwashStomatitis*Nursing Interventions:
*Acyclovir: herpes simplex*Tetracycline, corticosteroid:*Nystatin oral suspension (Swish and swallow): fungal infections
Achalasia*Ineffective or absent peristalsis of the distal esophagus
*Lack of sphincter relaxation during swallowing
*Cause:*Denervation of muscle layers of esophagus
Achalasia*Assessment:
*Difficulty swallowing*Feeling of food sticking in LE*Chest pain*Weight loss*Regurgitation of undigested food (non acidic)*Halitosis
Achalasia*Diagnostic tests:
*Barium swallow* Esophagoscopy* Biopsy
8/8/2019 Digestive System Krva
13/33
Achalasia*Nursing Interventions:
*Eat slowly and chew food completely*Warm foods and drinks*Drink fluids with meals*Elevate HOB: 6-12 in*Medications:
*Nitrates*CCB: Nifedipine (Procardia)
Achalasia
*Nursing Interventions:*Balloon dilation*Botulinum toxin (Botox) injection*Esophagomyotomy)
Gastroesophageal Reflux Disease (GERD)*Reflux of gastric contents into the esophagus.Gastroesophageal Reflux Disease (GERD)*Causes:
*Insufficient closure of lower esophageal sphincter (LES)*Gastric distention*Hiatal Hernia*Lifestyle*Medications: NSAIDs, nitrates, CCB
Gastroesophageal Reflux Disease (GERD)*Assessment:
*Dyspepsia (heartburn)*Regurgitation (bitter or sour tasting)*Hypersalivation*Nausea*Pain: 30 min after meal*Hoarseness, sore throat*Dysphagia, odynophagia*Coughing
Gastroesophageal Reflux Disease (GERD)*Dx Tests:
*Barium swallow*Endoscopy
Gastroesophageal Reflux Disease (GERD)*Nursing Interventions:
*Losing weight if obese.*Low-fat, high-protein diet*Avoid chocolate, fatty, carbonated, spicy, high-acid foods*Small frequent meals (4 to 6 a day)*Increase fluids
Gastroesophageal Reflux Disease (GERD)
8/8/2019 Digestive System Krva
14/33
*Nursing Interventions:*Avoid meals (3 h) before bedtime*Discontinuing of NSAIDs, as ordered*Elevating HOB (6-12 in)*Stop smoking*Avoid constrictive clothing
Gastroesophageal Reflux Disease (GERD)*Medications:
*PPI:*Omeprazole (Prilosec), Lansoprazole (Prevacid), Esomeprazole
(Nexium), Pantoprazole (Protonix)
*H2 blocker:*Nizatidine (Axid), ranitidine (Zantac)*Famotidine (Pepcid)
Gastroesophageal Reflux Disease (GERD)*Antacid:
*Aluminum magnesium combinations (Mylanta,Maalox)
*Mucosal barrier fortifiers:*Sucralfate (Carafate)
*Laparoscopic Nissen fundoplication (LNF)
GERD*Therapeutic Procedures:
*Surgery (Fundoplication): laparoscopy
*In a fundoplication , the gastric fundus (upper part) of the stomach is wrapped, orplicated, around the lower end of the esophagus and stitched in place,reinforcing the closing function of the lower esophageal sphincter:
*Whenever the stomach contracts, it also closes off the esophagus instead of squeezing stomach acids into it.
*This prevents the reflux of gastric acid (in GERD).*The esophageal hiatus is also narrowed down by sutures to prevent or treat
concurrent hiatal hernia, in which the fundus slides up through theenlarged esophageal hiatus of the diaphragm.
*In a Nissen fundoplication, also called a complete fundoplication, the fundus iswrapped all the way 360 degrees around the esophagus. In contrast, surgeryfor achalasia is generally accompanied by either a Dor or Toupet partialfundoplication, which is less likely than a Nissen wrap to aggravatethedysphagia that characterizes achalasia. In a Dor (anterior) fundoplication,the fundus is laid over the top of the esophagus; while in a Toupet (posterior)fundoplication, the fundus is wrapped around the back of the esophagus.
*The procedure is now routinely performed laparoscopically. When used to alleviategastroesophageal reflux symptoms in patients with delayed gastric emptying,it is frequently combined with modification of the pylorus via pyloromyotomy or pyloroplasty.
8/8/2019 Digestive System Krva
15/33
Hiatal Hernia*Part of the stomach protrudes through the esophageal hiatus
*Types:*Sliding: portion of stomach slip into thoracic cavity*Paraesophageal: fundus rolls out of stomach and forms a pocket
Hiatal Hernia*Causes:
*Malformation*Muscle weakness of esophageal hiatus*Esophageal shortening*Obesity
Hiatal Hernia*Assessment:
*Feeling of fullness, suffocation after meal*Anemia
Hiatal Hernia*Dx Tests:
*Fluoroscopy.*X-ray studies
Hiatal Hernia*Nursing Interventions:
*Dietary and Medical Mx (GERD)*AVOID: HIATAL
*H ot and spicy, Ingestion of large meals, Apparel that constrictive,Twisting/bending/lifting, Alcohol, Limit carbonated beverages
*Monitor for strangulation*Laparoscopic Nissen fundoplication
Gastritis* Inflammation of the stomach lining
* Acute (few days)*Chronic.
Gastritis*Causes:
*Infection*Irritation from medications, alcohol, foods, corrosive substances*Stress*Radiation*Gastrectomy
Gastritis*Assessment:
*Pain or discomfort*Dyspepsia (heartburn)*Gnawing or burning aches in upper abdomen
8/8/2019 Digestive System Krva
16/33
*Nausea and vomitingGastritis*Assessment:
*Loss of appetite (anorexia)*Bloating, belching*Weight loss*Bleeding: hematemesis, melenaanemia
Gastritis*Dx tests:
*EGD*Blood tests*Urea breath*Stool tests
Gastritis*Nursing Interventions:
*Proton-pump inhibitors*H2-receptor blockers*Antacids*Mucosal barrier fortifiers*Lifestyle changes*Avoid aspirin and NSAIDs
Gastritis*Nursing Interventions:
*H. pylori: 2-week course*Bismuth subsalicylate (Pepto-Bismol) or*PPI and metronidazole (Flagyl) and tetracycline (Achromycin) or* Clarithromycin (Biaxin) and amoxicillin (Amoxil).
Gastroenteritis (Stomach Flu)*Inflammation of the GI tract.*Causes:
*Parasitic organisms ( Entamoeba histolytica and Cryptosporidium and Giardiaspecies)
*Bacterial organisms ( Escherichia coli, Vibrio cholerae, and Campylobacter,Salmonella, and Shigella species)
Gastroenteritis (Stomach Flu)*Causes:
*Viral organisms (astroviruses, Norwalk virus, rotaviruses)
*Chemical toxins (lead, arsenic, mercury, poisonous mushroom, seafood,water)
Gastroenteritis (Stomach Flu)*Assessment:
*Diarrhea* Abdominal cramps*Nausea and vomiting* Loss of appetite
8/8/2019 Digestive System Krva
17/33
*Fever and chills*Dehydration*Weakness, fatigue
Gastroenteritis (Stomach Flu)*Dx Tests:
*Stool culture*Blood tests*Potassium, sodium, and other electrolyte levels.
Gastroenteritis (Stomach Flu)*Nursing Inteventions:
*Avoid carbonated, caffeinated, and high-sugar drinks, spicy, dairy*Clear liquids with electrolytes (Pedialyte, Resol)*IV fluid with potassium*bland foods (cream soups, crackers, toast, rice, yogurt, custards)
Gastroenteritis (Stomach Flu)*Nursing interventions:
*Antibiotics: if bacteria.*Antiparasitics*Antidiarrheals (avoided)*Perineal irritation: cleansing, pat dry, barrier creams, witch hazel (Tucks)
Helicobacter pylori (HP)*Gram-negative
*Causes ulcers and chronic gastritis
*Dx tests:*Cultures from ulcer craters.*Blood test or breath test
H. Pylori*Nursing Interventions:
*Clarithromycin, amoxicillin, tetracycline, or metronidazole (Flagyl)*Combined with PPI
Peptic Ulcer DiseasePeptic Ulcer Disease (PUD)*Erosion of the lining of the stomach, pylorus, duodenum, or esophagusPeptic Ulcer Disease (PUD)*Causes:
*H. Pylori*Medications:
*Aspirin, NSAIDs*Theophylline, caffeine, Prednisone
*Smoking*Stress
Peptic Ulcer Disease*Assessment:
8/8/2019 Digestive System Krva
18/33
*Pain: burning, gnawing*Gastric: 1-2 hrs; left epigastric area*Duodenal: 2-4 hrs or at night, food relief, right epigastric area
*Weight loss, weight gainPeptic Ulcer Disease*Dx tests:
*Urea breath test* Serum IgG antibody screening*Upper GI (barium swallow)*EGD*Stool for occult blood
Peptic Ulcer DiseaseNursing Interventions:
*A bland diet, no spicy, high-acid food*Lifestyle changes*Avoid alcohol, and smoking*Meditation.*Herbs and vitamins*No bedtime snacks*No NSAIDs, aspirin
Peptic Ulcer Disease*Nursing Interventions:
*PPI, H2 block, antacids*Mucosal barrier fortifiers*Helicobacter pylori therapy
Peptic Ulcer Disease*Complications:
*Bleeding
*Interventions:*NPO, IV, saline lavage*Endoscopy, Surgery*H2 blockers, PPI
Peptic Ulcer Disease (PUD)*Complications:
*Perforation
*Interventions:*Fluids, electrolytes IV*NG suction*IV antibiotics*Surgery
Gastric Surgery*Gastrectomy*Partial gastrectomy
*Gastroduodenostomy (Billroth 1)*Gastrojejunostomy (Billroth 11)
*Vagotomy: cut vagus nerve
8/8/2019 Digestive System Krva
19/33
*PyloroplastyGastric Surgery*Nsg Interventions:
*Semi-Fowlers,*NPO: 3 days, IV fluids: no peristalsis*NGT: Do not irrigate,
*Bright red (24 h),yellow-green (36-48 h)*Monitor dressing: bleed, infection*Turn, cough, deep breath
Gastric Surgery Complications*Pernicious anemia
*Pallor, glossitis (sore tongue), fatigue, paresthesias*Lifelong B12 inj (Once a month)
Dumping Syndrome*Occurs when large bolus of chyme enter the intestine
Dumping Syndrome*Dizziness*Diaphoresis*Diarrhea*Tachycardia*Lie down after meal*Small frequent meals*high protein, high fat, avoid simple carbohydrates (juice, honey, syrup, jelly)*NO fluid with meal and for 1 hr prior and after meal*Med: Bentyl (antispasmodic)
Hernias*Abnormal protrusion of a loop of bowel through the thin muscular wall of the
abdomen.Hernias*Classifications:
*Reducible*Irreducible (incarcerated)*Strangulated
Hernias
8/8/2019 Digestive System Krva
20/33
*Hernia type:*Inguinal : direct, indirect*Femoral*Umbilical*Incisional (ventral)
Hernias*Causes
*Congenital*Increased abdominal pressure*Abdominal surgery
*Assessment:*Bulging in abdominal*Pain
Hernias*Nursing Interventions:
*Avoid lifting, constipation*Deep-breathing*Stop smoking*S/S strangulation.*Truss (elastic belt)*Herniorrhaphy, Hernioplasty
*Post-op: Urinary retention
Hernias*Complications:
*Incarceration*Gangrene
AppendicitisAppendicitisAppendicitis*Acute inflammation of the appendix
*Cause:*Obstruction
Appendicitis*Assessment:
*Pain:*Peri-umbilicalMc Burneys*Rebound tenderness
*Abdominal rigidity*Nausea and vomiting*Loss of appetite
Appendicitis*Dx tests:
*CBC: WBC > 10,000/mL*CT scan*Urinalysis
8/8/2019 Digestive System Krva
21/33
Appendicitis*Nursing Interventions:
*NPO, IV fluids*Pain: avoid heat*Elevate HOB: perforation*Appendectomy
*Avoid laxative, enema*Antibiotics: post-surgery
AppendicitisPeritonitis*Acute inflammatory disorder of the peritoneum
*Causes:*Rupture of organs.*Infection*Wound
Peritonitis*Assessment:
*Pain*Generalized, rebound tenderness
*Abdominal rigidity*Dec peristalsis, BS*N/V*F/E imbalances, dec urine*Increased pulse
Peritonitis*Nursing Interventions:
*NPO, F/E*Nasogastric tube*O2, Semi-fowlers*Pain management*Antibiotics*Surgery, Temporary colostomy
Types of Ostomy*Colostomy: colon through abd wall
*Semi-soft stool
*Ileostomy: ileum through abd wall*Kocks ileostomy: continent ileostomy; internal reservoir
Ostomy Care:*Nursing Interventions:
*Low-residue diet*Select appropriate sized appliance*Keep skin around stoma clean, dry and free of intestinal juices
ColostomyCrohns disease
8/8/2019 Digestive System Krva
22/33
*Chronic inflammatory bowel disease (IBD)
*Causes:*Smoking*Genetic predisposition
Crohns Disease*Assessment:
*Pain: crampy, abd pain (RLQ)*Chronic diarrhea*Weight loss, malnutrition*Elevated temperature*Fluid and electrolyte imbalances
Crohns Disease*Dx tests:
*Upper GI Series, barium enema*Colonoscopy
Crohns disease*Nursing Interventions:
*NPO, TPN* I and O, weight*Low-fiber, low-fat diet, high calories, protein; supplements*Corticosteroids, sulfasalazine, Antidiarrheal, antibiotics, opiod*Surgery
Ulcerative Colitis*Chronic inflammatory bowel disease that affects large intestine
*Rectumcecum
*Causes:*Autoimmunity*Genetic predisposition
Ulcerative Colitis:*Assessment:
*Pain: crampy, LLQ*Diarrhea: 20 times*Rectal bleed*Anorexia, weight loss
Ulcerative Colitis*Dx tests:
*Sigmoidoscopy or colonoscopy*Barium enema*Stool sample: infectious
Ulcerative Colitis*Nursing Interventions:
*NPO or clear liquids; TPN*Avoid high-bulk foods, milk products, alcohol, caffeinated*Bed rest.*Sulfasalazine
8/8/2019 Digestive System Krva
23/33
Ulcerative Colitis*Surgery:*1. Removing the colon, rectum, and anus and placing an ileostomy*2. Removing the colon, rectum, and anus and forming a pouch*3. Removing the colon and rectum, suturing the ileum to the anal canal and a
temporary ileostomyDiverticulitis*Acute inflammatory bowel disease characterized by inflammation of diverticula in
the bowel mucosa.
*Causes:*Low fiber diet*Decreased colon motility
Diverticulitis*Assessment:
*Pain: LLQ*Fever*Weakness and fatigue*Constipation alternating diarrhea*Anemia*Rectal bleeding
Diverticulitis*Dx Tests:
*CT scan or ultrasound* Abdominal X-rays* CBC*Colonoscopy*Barium enema
Diverticulitis*Nursing Interventions:
*Liquid diet, soft diet, low-fiber*Stool softeners*After healing: High-fiber, inc fluid*IV, oral antibiotics*Pain control*Colon resection
Polyps*Polyps are small growths along the lining of the intestinal tract.
Polyps*Assessment:
*Bleeding*Abdominal pain and cramping*Diarrhea or any change bladder habit
Polyps*Diagnostic tests:
8/8/2019 Digestive System Krva
24/33
*DRE*Sigmoidoscopy*Colonoscopy*Fecal occult blood*Barium Enema
Polyps*Nursing Interventions:
*Polypectomy*Colectomy*Increase calcium intake*NSAIDs/ASA*Exercise, stop smoking, alcohol, low-fat/high-fiber diet.*Routine colorectal screenings.
Colorectal Cancer*Starts as a noncancerous polyp*Adenomas are the types of polyps that have the potential to become cancerous.*Develop slowly over a period of several years*Aspirin may decrease the risk
Colorectal CancerColorectal Cancer*Risks:
*Excess saturated red meats*Age older than 50 years*Low-fiber, high-carbohydrate*Chronic constipation*Diverticulosis*Ulcerative colitis
Colorectal Cancer*Assessment:
*Constipation and diarrhea*Change shape of stool*Rectal bleed, pallor, weakness*Rectal pressure*Anorexia, weight loss
*Screening:
Colorectal Cancer*Diagnostic tests:
*FOBT*DRE*Sigmoidoscopy, Colonoscopy: biopsy*Barium enema: after colonoscopy
Colorectal Cancer*Interventions:*Radiation.
8/8/2019 Digestive System Krva
25/33
* Chemotherapy.*Doxorubicin (Adriamycin)*5-fluorouracil (Adrucil):
*A/R: cerebellar dysfunction, phototoxicity, stomatitis, diarrhea*Antiemetics
Colorectal Cancer*Interventions:
*Surgery*Colectomy*Abdominoperineal resection (sigmoid, rectum, anus) with permanent
colostomy
Colorectal Cancer*Interventions:
*Surgery*Colectomy*Abdominoperineal resection (sigmoid, rectum, anus) with permanent
colostomy
ColostomyColostomy IrrigationColostomy IrrigationHemorrhoids*Are varicose/distended veins of the anal canal.
*External hemorrhoids*internal hemorrhoids
HemorrhoidsHemorrhoids*Causes:
*Chronic constipation*Pregnancy*Obesity*Heavy lifting, straining, standing for long periods
Hemorrhoids*Assessment:
*Bleeding*Itching*Pain
Hemorrhoids*Diagnostic Tests:
*Digital examination* Anoscopy and flexible sigmoidoscopy
Hemorrhoids*Nursing Interventions:
*Sitz bath
8/8/2019 Digestive System Krva
26/33
*Dibucaine (Nupercainal)*Witch hazel (Tucks)*Cleaning anal area by blotting*High-fiber diet, fluids, docusate sodium (Colace)*Sclerotherapy, Band ligation hemorrhoidectomy
Sitz bathHemorrhoids
*ACCESSORY ORGANS
Health History:*Hepatic/Biliary problems:
*Jaundice*Pruritus*Urine color*Clay-colored stools
Pathophysiology of Jaundice Types of JaundiceSerum Laboratory TestsImaging Tests*Oral Cholecystogram (GB Series)
*X-ray visualization of GB*Low fat or fat-free meal: dinner*6 telepaque tabs (5 min) after dinner, then NPO*Post:
*Assess slight dysuria: excretion dye Imaging tests*Percutaneous Transhepatic cholangiography
* Radiopaque dye into a bile duct, then X-rays
*Operative Cholangiography*Injection of dye directly into the biliary duct during GB surgery, then X-rays
Imaging Test*ERCP: Endoscopic Retrograde Cholagiopancreatography
Liver BiopsyParacentesis
Esophageal Tamponade Balloon
8/8/2019 Digestive System Krva
27/33
Cirrhosis*Cirrhosis is severe, potentially fatal scarring and fibrosis of liver tissue.Cirrhosis*Causes:
*Chronic alcoholism*Viral or autoimmune hepatitis*Bile duct obstruction*Right-sided heart failure*Drugs and toxins
Cirrhosis*Assessment:
*Jaundice*Ascites, SOB*Hepatomegaly*Nausea, anorexia, abd discomfort*Malnutrition
Cirrhosis*Assessment:
*Spider angiomas*Increased medication sensitivity*Splenomegaly*Esophageal varices*Confusion, mood changes, behavioral changes*Hepatic encephalopathy, Asterixis
Cirrhosis*Dx Tests:
*Ultrasound or CT scan*Laboratory studiesbilirubin, albumin, alanine transaminase (ALT),*aspartate transaminase (AST), prothrombin*Liver biopsy*Esophagoscopy
Laboratory Studies*Alkaline phosphatase:
*4.5 13 King-Armstrong units/dl* PT: 10-12 sec*Ammonia: 35-65 mg/dl* Cholesterol:
*140 199 mg/dl*Albumin: 3.4 to 5 g/dl
* Amylase: 2 151 units/L* lipase: 10-140 units/L):* Bilirubin: liver, biliary obs*Direct (con/water sol):
*0 to 0.3 mg/dl*Indirect (uncon):
8/8/2019 Digestive System Krva
28/33
*0.1- 1.0 mg/dl*Total:
8/8/2019 Digestive System Krva
29/33
*Assessment:*Early:
*Anorexia, weight loss, fatigue*Hepatomegaly
*Pain: dull RUQ
Paracentesis1. Obtaining consent for the procedure.2. Positioning the client (supine or semi-Fowlers position; or sitting up,if tolerated).3. Educating client4.Monitoring and reporting complications5. Vital signs prior to procedure and frequent vital signs thereafter.Hepatitis A (HAV)*Incubation is about 30 days, and the virus is excreted in the stool for about 2
weeks
Hepatitis A*Assessment:
*Jaundice, clay stools*Dark urine*Pruritus*RUQ abdominal pain* Fever*Fatigue*Loss of appetite, nausea, GI symptoms*Bleeding tendencies*Anemia
Hepatitis A*Dx tests:
*A blood test: detects antibody IgM.*No specific treatment
Hepatitis A*Prevention:
*Hand hygiene*Properly cleaning eating utensils.*Exclusion of food handlers from work.*Providing vaccination.
*Exposure to HAV, immune globulin (within 2 weeks of exposure)
Hepatitis A*INFECTION CONTROL
*Hand hygiene to prevent the spread of HAV.*Vaccine before traveling to places where HAV is endemic.*Standard precautions, when caring for this client.*Contact precautions, for incontinent clients (cannot control bladder/bowel).
Hepatitis B*This virus has a complex structure capable of attacking and destroying liver cells
*architectural changes of the normal structure, of the liver which leads to
8/8/2019 Digestive System Krva
30/33
*disruption in the flow of blood and bile. Illness can range fromHepatitis B*Causes:
*Exposure to infected blood and body fluids*Transfusion of blood and blood products*Hemodialysis
*Assessment:*Fatigue*Fever*Nausea and vomiting*Anorexia*Steatorrhea*Jaundice, pruritus*Dark urine, dark-colored stools*Abdominal pain, ascites
*Hepatitis panel* Liver profile:
*(AST, SGOT), alanine transaminase (ALT, SGPT), alkaline phosphatase*(alk phos), gamma-glutamyltransferase (GGT), and bilirubin.
Hepatitis B*Nursing Interventions:
*Antivirals.*Interferon*Supportive care and symptom relief.*HBV immune globulin for infants*Liver transplantation.*Pregnant women: NO antivirals or interferon
Hepatitis B*Prevention: HBV vaccine (health care workers, hemodialysis clients)
*Avoid razors, nail clippers, and toothbrushes*Avoid tattoo parlors*Practice abstinence or use condom
What can harm my client?
*Alcohol* Acetaminophen* Sedatives.* Any hepatotoxic (toxic to the liver) drug.* Strenuous activities.Hepatitis C (HCV)*One of the five hepatitis viruses that infect the
*80% of those with HCV have no signs or symptoms.
*Causes:*Exposure to infected blood and body fluids*Transfusion of blood and blood products
8/8/2019 Digestive System Krva
31/33
*Hemodialysis*Organ transplantation
Hepatitis C*Assessment:
*Fatigue*Myalgia*Jaundice, pruritus*Dark urine*Abdominal pain*Anorexia*Nausea and vomiting
Hepatitis C*Dx tests:
*Hepatitis profile, Liver enzymes
*Nursing Interventions:*Interferon* Symptomatic treatment for myalgia, nausea, vomiting, and pruritus.*Unlike HBV, HCV does not have a vaccine.
Hepatitis C*Prevention includes:
*Not sharing personal items, such as toothbrushes, razors, or nail clippers.*Avoiding tattoos.*Practicing abstinence or using a condom
Cholecystitis and Cholelithiasis*Cholecystitis
*Inflammation of GB*Associated with cholelithiasis (gall stone)
Cholecystitis and CholelithiasisCholecytitis*Inflammation of the gallbladder. About 90% of cases result from gallstones
obstructing the cystic duct.*If cholecystitis occurs without gallstones, it is usually after a major illness or
injury (acalculous cholecystitis).*Acute or chronic
Cholecystitis*Acute cholecystitis: edema, inflammation, and impaction of bile in gallbladder *Chronic cholecystitis: fibrotic thickening of gallbladder wall and incomplete
emptyingCholecystitis*Assessment:
*Severe acute RUQ and epigastric pain radiating to shoulder and right
8/8/2019 Digestive System Krva
32/33
scapula*Nausea and vomiting*Fever*Indigestion*Steatorrhea
Cholecystitis*Dx Tests:
*Complete blood count (CBC)*Serum amylase levels*Ultrasound to check for gallstones*X-ray to identify gallstones*ERCP (endoscopic retrograde cholangiopancreatography)
Cholecystitis*Nursing Interventions:
*NPO (nothing by mouth)*(IV) fluids and electrolytes* Pain control (opioids* Antispasmodics or anticholinergics* Laparoscopic cholecystectomy
Exercise:*Which of the following food choices might trigger a cholecystitis attack?*__Ice cream*__Chocolate cake*__Fresh noodle with vegetables*__Baked fish*__broccoli with cheese sauce*__Rice and Pork BBQ*__Sweetened strawberries*__Fried eggs and baconExercise*The client who undergone abdominal cholecystectomy had fully recovered from
anesthesia. Which position is best for the client?*A. Side lying position, to prevent aspiration*B. Semi-Fowlers position, to facilitate breathing*C. Supine, to decrease strain on the incision line*D. Prone, to reduce nauseaPancreatitis*Acute or chronic inflammation of the pancreas
*Acute pancreatitis results when pancreatic enzymes are activated while stillin the pancreas
*Chronic pancreatitis results when progressive, recurring episodes cause
structural changes, and functionPancreatitis*Causes:
*Toxic metabolic processes*Biliary obstruction*Trauma*Viral infections
8/8/2019 Digestive System Krva
33/33
*Cancer*Unknown origin
Pancreatitis*Assessment:
*Pain*Nausea and persistent vomiting*Decreased or absent BS*Respiratory distress*Fluctuation in BP
Pancreatitis*Assessment:
*Fever*Malaise and decreased level of consciousness*Steatorrhea*Cullens, Turners, Ascites
Pancreatitis*Increased serum amylase and lipase (enzymes produced in the pancreas).*Amylase may be normal in chronic pancreatitis. Lipase usually elevatesPancreatitis