
Digestive Pathology Lecture 4 - LSU Health New Orleans · Liver function tests Serum proteins...
98
Digestive Pathology Lecture 4 Reproduction Prohibited This file contains original text and images as well as materials adapted from copyrighted sources For use only as a temporary educational aid Partially or completely copying or distributing the contents of this file may constitute an infringement of the fair use exception for teaching faculty of the U.S. Copyright Law LSUHSC-New Orleans, 2015 Last updated on September 25, 2015 ---
Transcript of Digestive Pathology Lecture 4 - LSU Health New Orleans · Liver function tests Serum proteins...
Digestive Pathology Lecture 4
Reproduction Prohibited
This file contains original text and images as well as materials adapted from copyrighted sources
For use only as a temporary educational aid
Partially or completely copying or distributing the contents of this file may constitute an infringement of the fair use exception
for teaching faculty of the U.S. Copyright Law
LSUHSC-New Orleans, 2015
Last updated on September 25, 2015
---
The liver 01
1. Functional reserve
– Liver function tests2. Anatomic considerations
3. Patterns of injury
4. Cirrhosis
5. Liver failure
6. Hyperbilirubinemias, cholestasis
1. Liver functional reserve
Functional reserve: 80% to 90%
– Many disease processes remain subclinical
Functions
– Metabolism of nutrients
– Serum protein synthesis
– Detoxification
– Bile excretion
Liver function tests Serum proteins
Total, albumin
Coagulation factorsProthrombin time/int. normalized ratio(PT/INR),
Partial thromboplastin time (PTT)
AminotransferasesAspartate (AST), alanine (ALT)
Biliary canaliculi enzymes– Alkaline phosphatase (ALP)
– Gamma-glutamyl transferase (GGT)
Bilirubin
The liver 011. Functional reserve
2. Anatomic considerations3. Patterns of injury
4. Cirrhosis
5. Liver failure
6. Hyperbilirubinemias, cholestasis
Hepatomegaly
“Enlargement of the liver”
– Normal adult weight:
• 1,400-1,600 gm
– Normal (percussion, palpatory) span:
• 6-12 cm in the midclavicular line
• 4-8 cm in the midsternal line
– In a normal adult, the liver should not protrude 2 cm or more below the costal margin
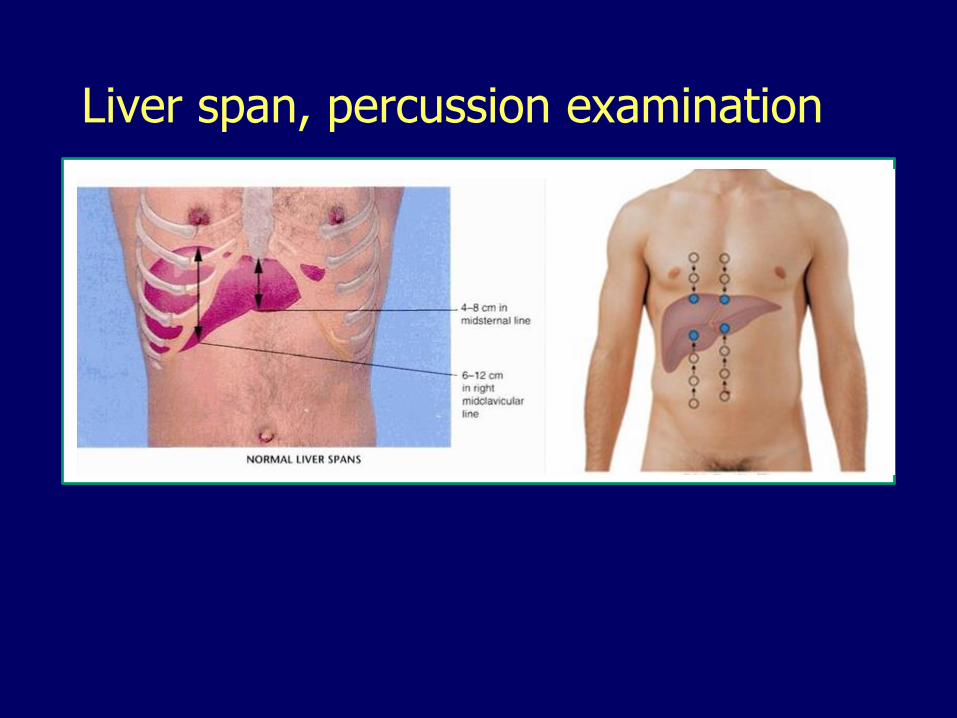
Liver span, percussion examination
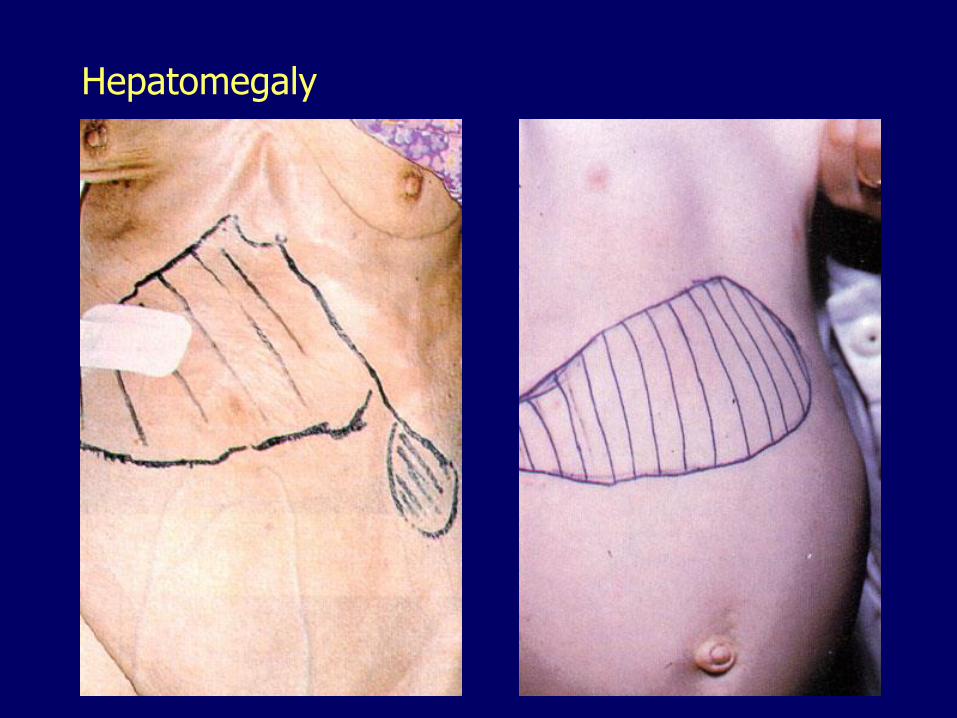
Hepatomegaly
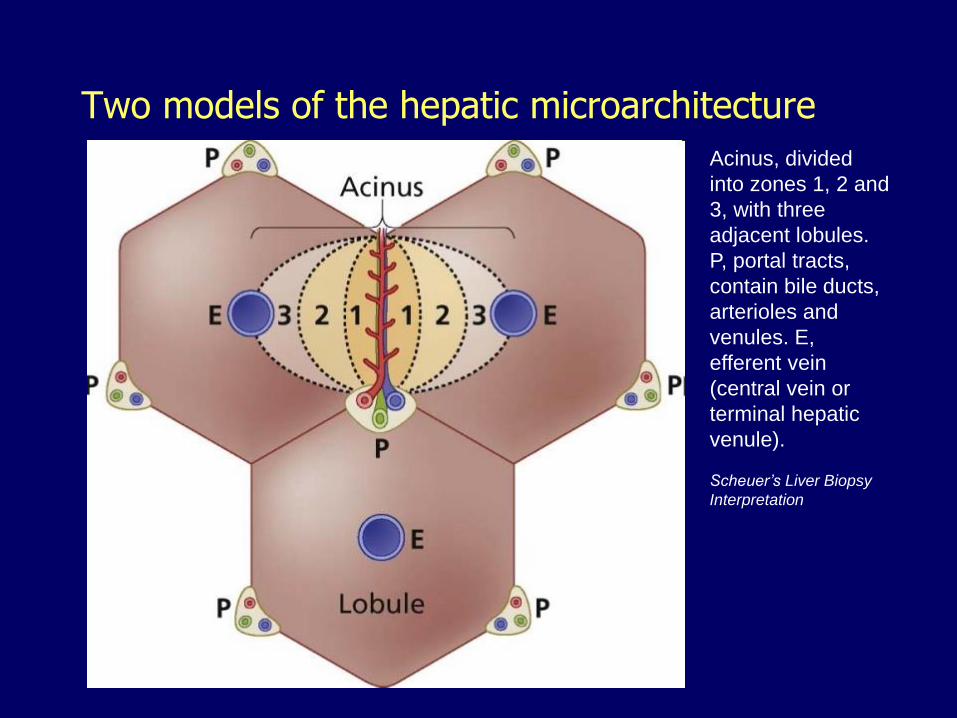
Two models of the hepatic microarchitecture
Acinus, divided
into zones 1, 2 and
3, with three
adjacent lobules.
P, portal tracts,
contain bile ducts,
arterioles and
venules. E,
efferent vein
(central vein or
terminal hepatic
venule).
Scheuer’s Liver Biopsy
Interpretation
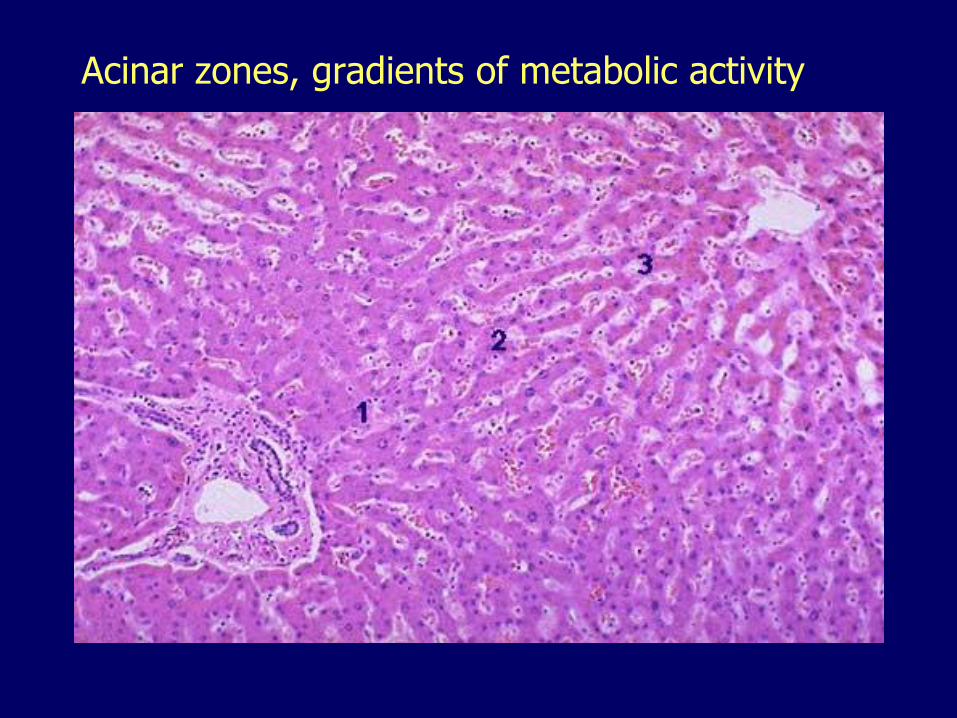
Acinar zones, gradients of metabolic activity
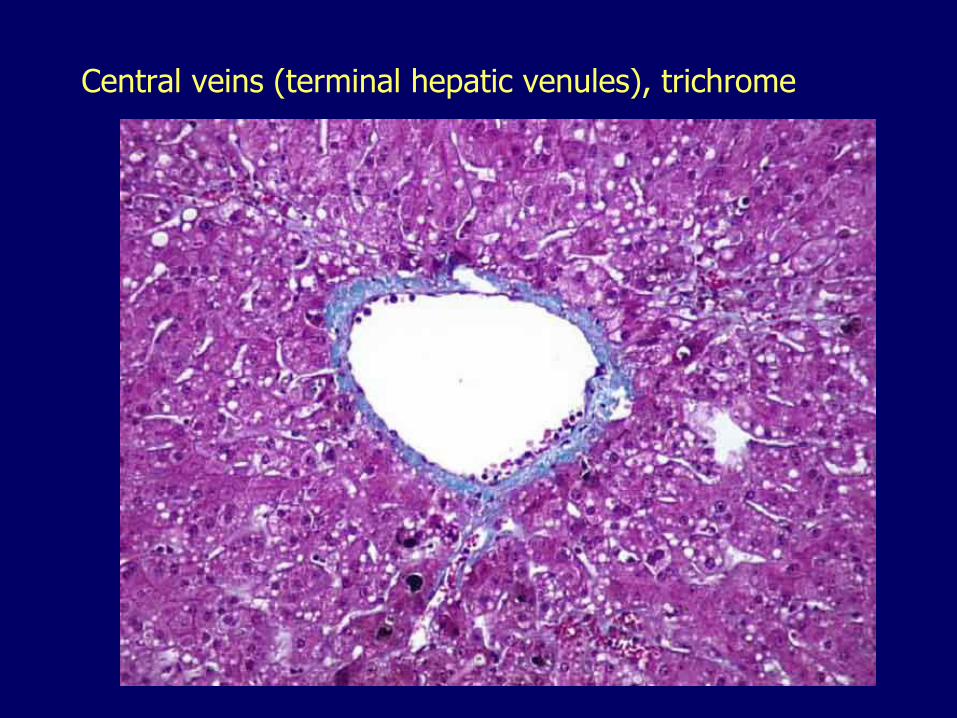
Central veins (terminal hepatic venules), trichrome

Portal triad, limiting plate, trichrome
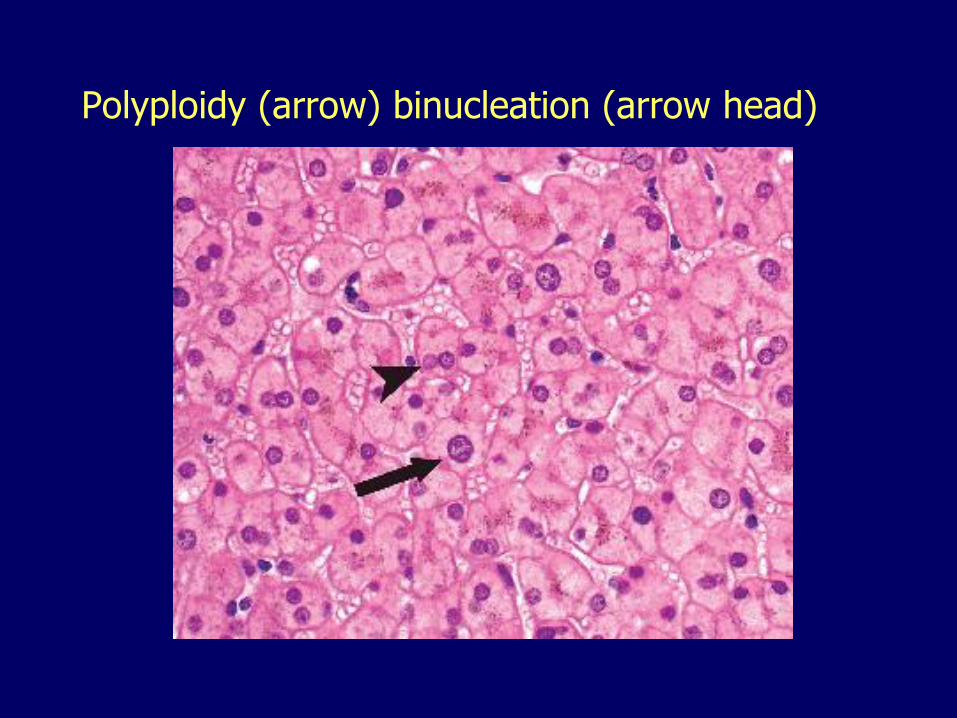
Polyploidy (arrow) binucleation (arrow head)
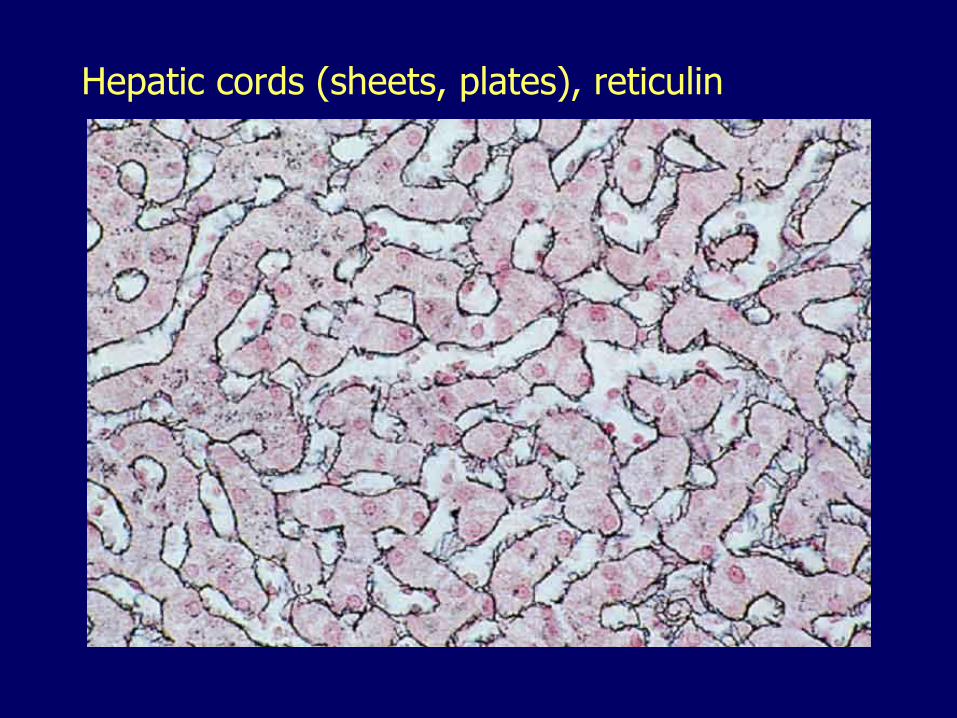
Hepatic cords (sheets, plates), reticulin

Sinusoids, fenestrated, no adventitia
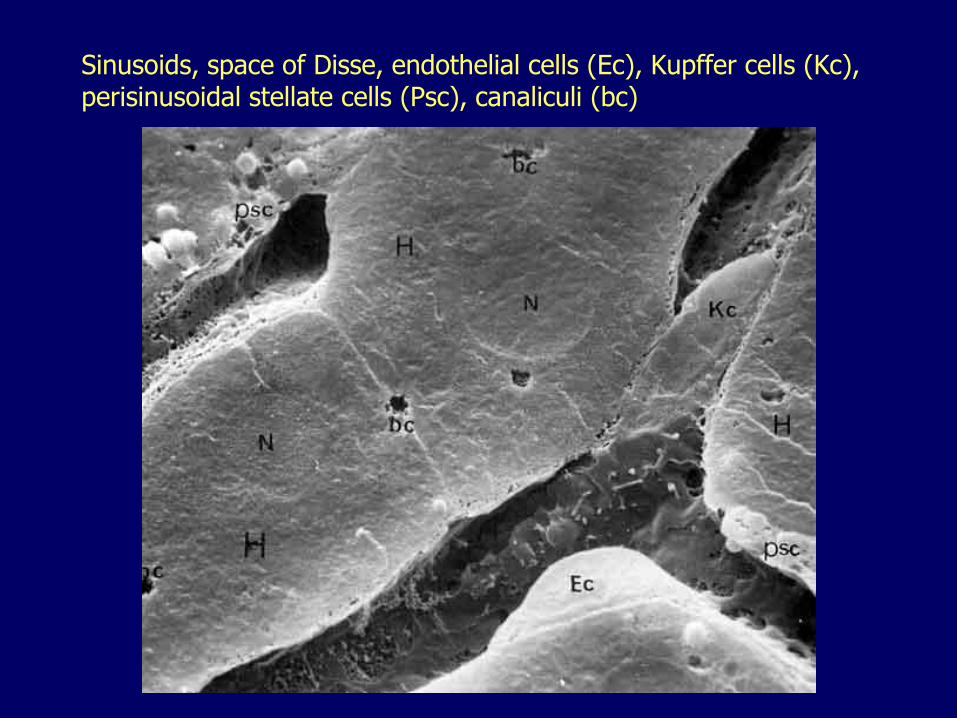
Sinusoids, space of Disse, endothelial cells (Ec), Kupffer cells (Kc), perisinusoidal stellate cells (Psc), canaliculi (bc)
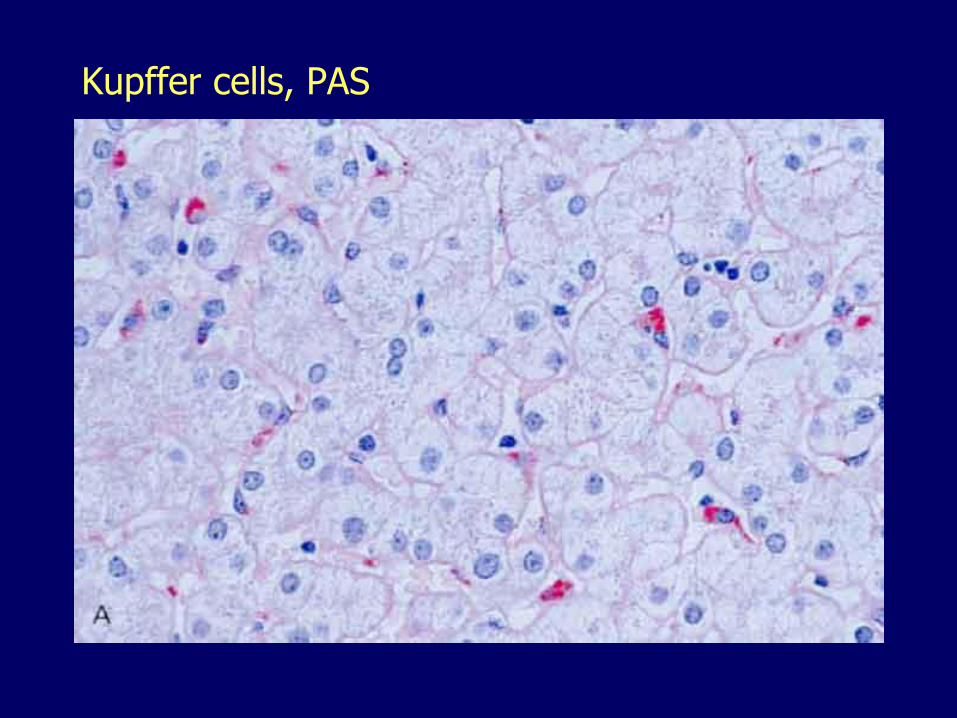
Kupffer cells, PAS
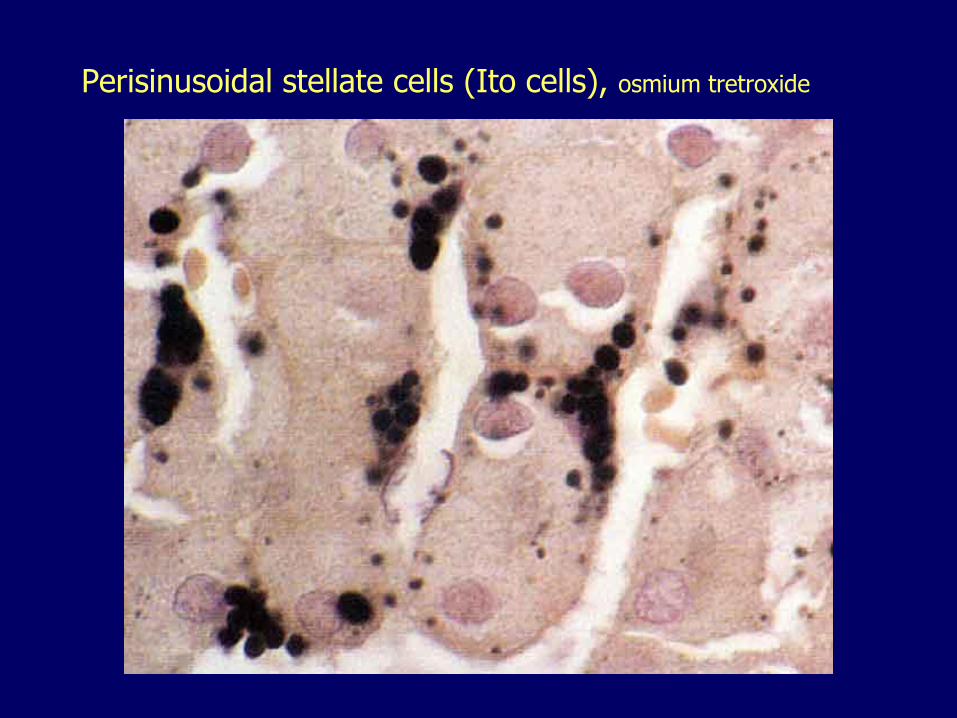
Perisinusoidal stellate cells (Ito cells), osmium tretroxide
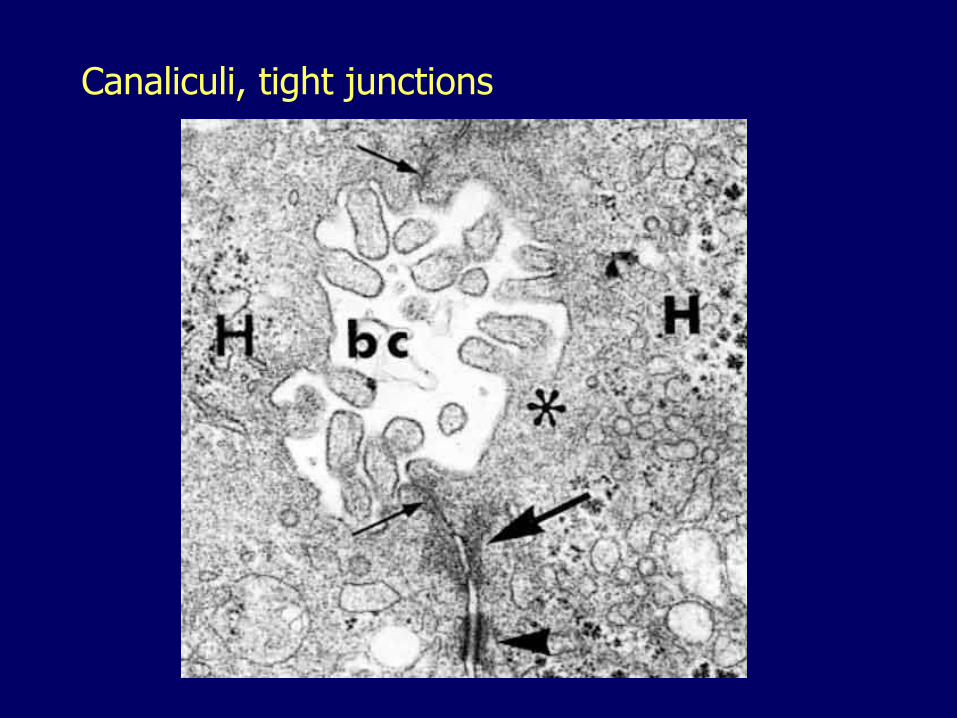
Canaliculi, tight junctions
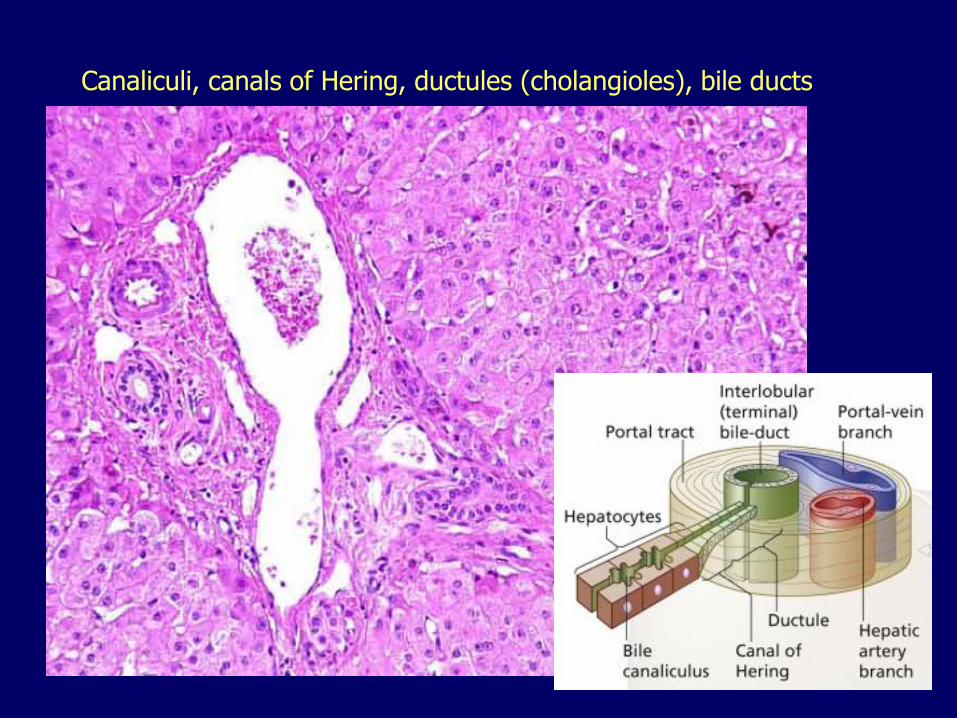
Canaliculi, canals of Hering, ductules (cholangioles), bile ducts
The liver 011. Functional reserve
2. Anatomic considerations
3. Patterns of injury4. Cirrhosis
5. Liver failure
6. Hyperbilirubinemias, cholestasis
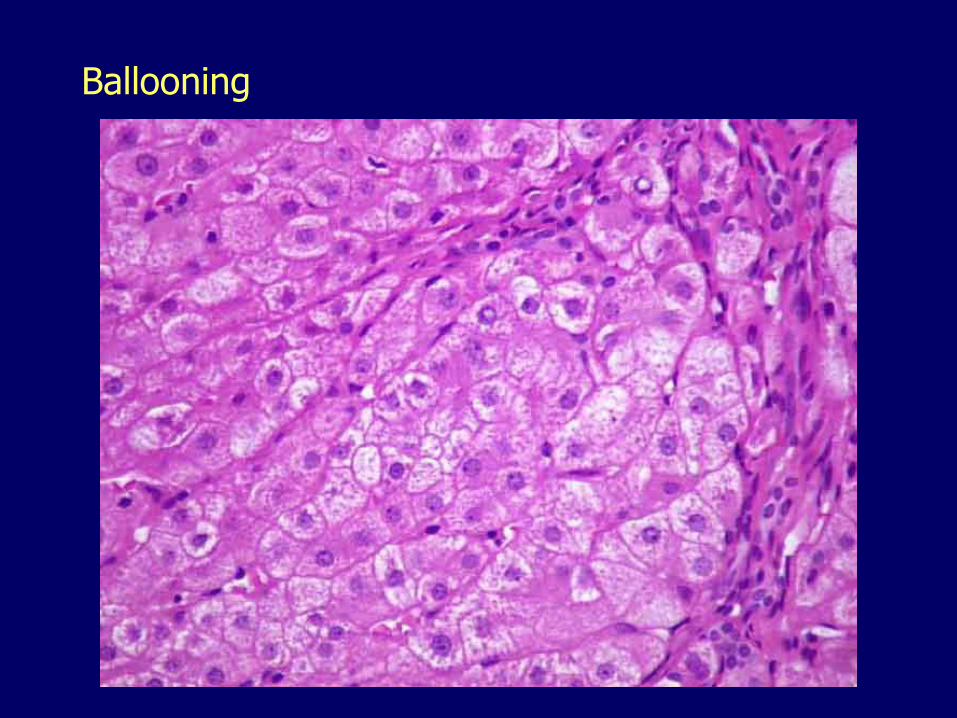
Ballooning
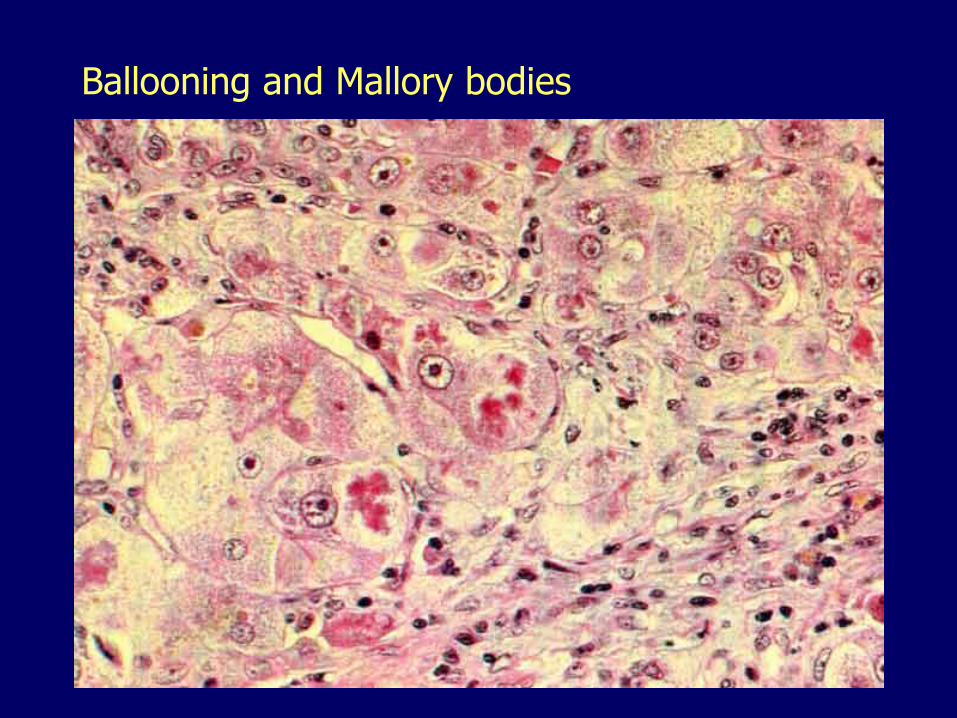
Ballooning and Mallory bodies
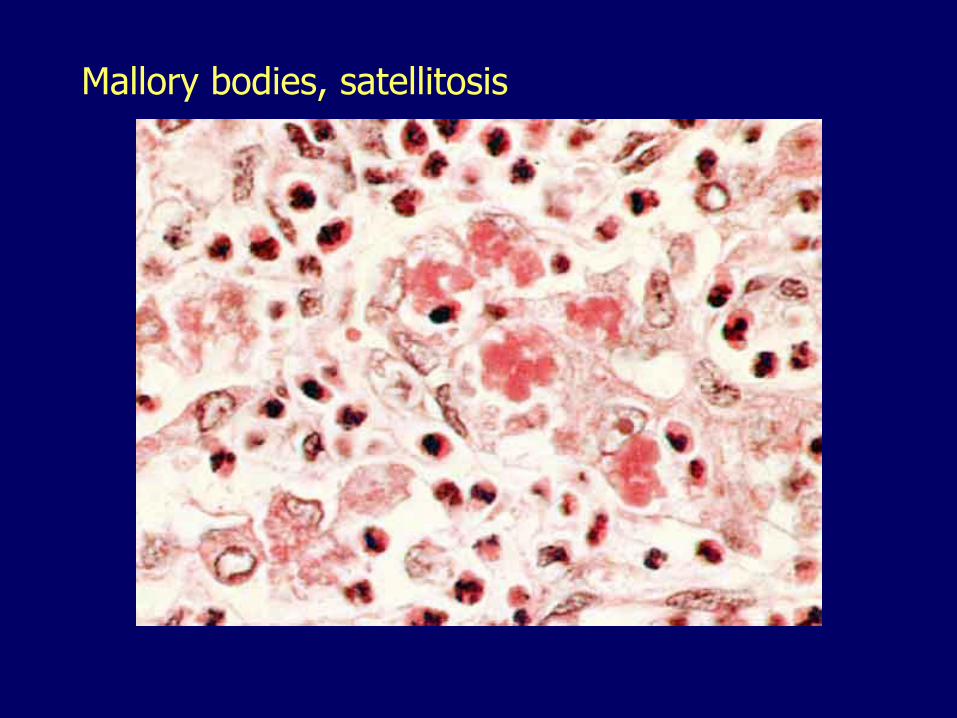
Mallory bodies, satellitosis

Foamy (feathery) degeneration
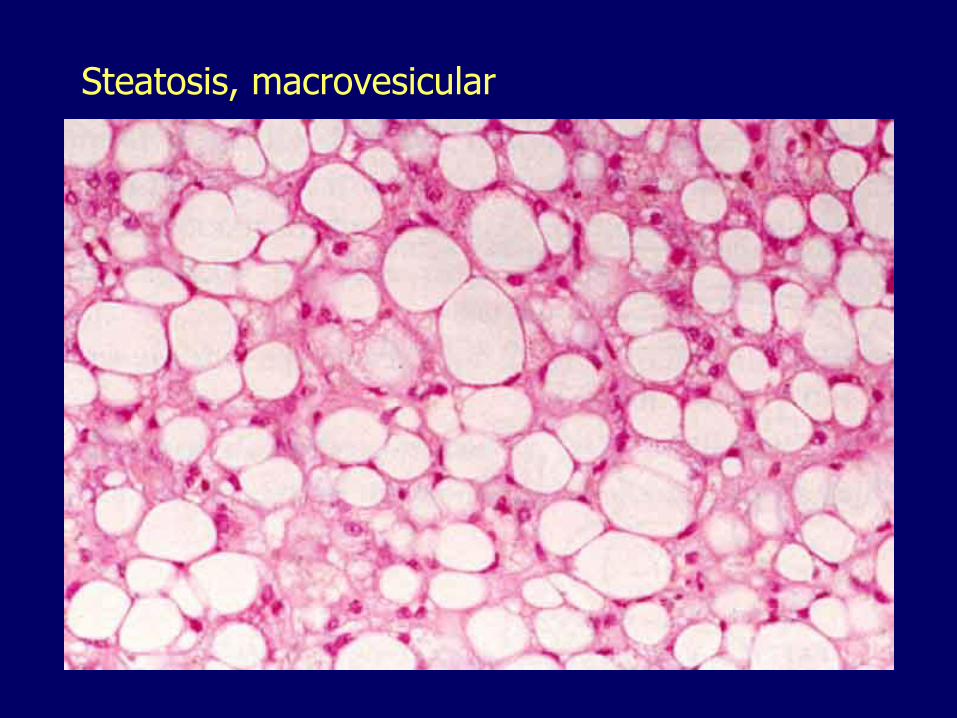
Steatosis, macrovesicular
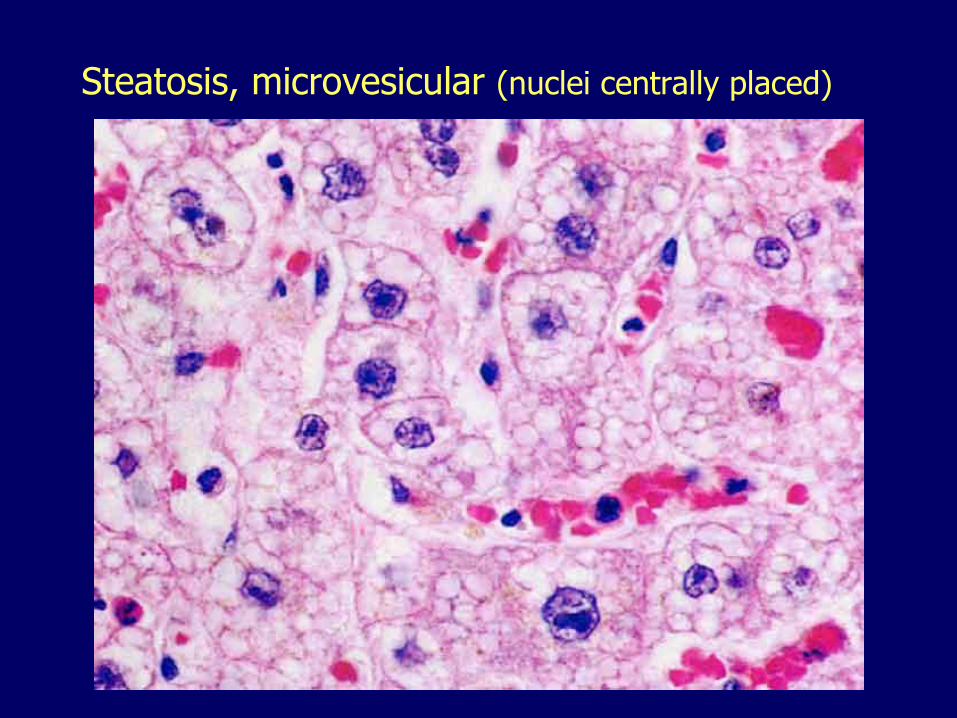
Steatosis, microvesicular (nuclei centrally placed)
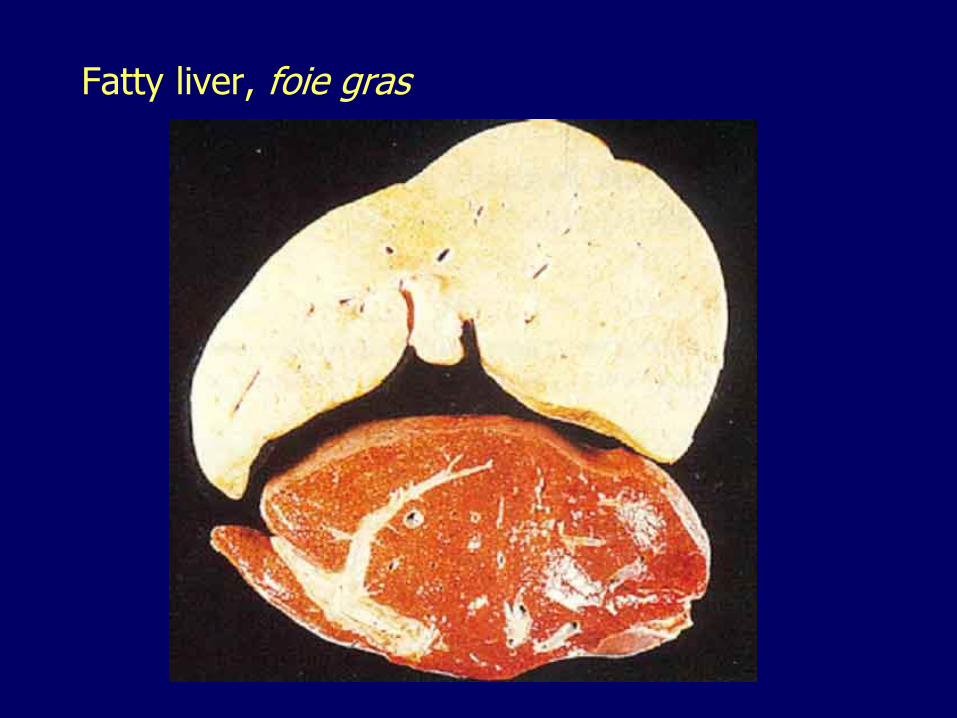
Fatty liver, foie gras
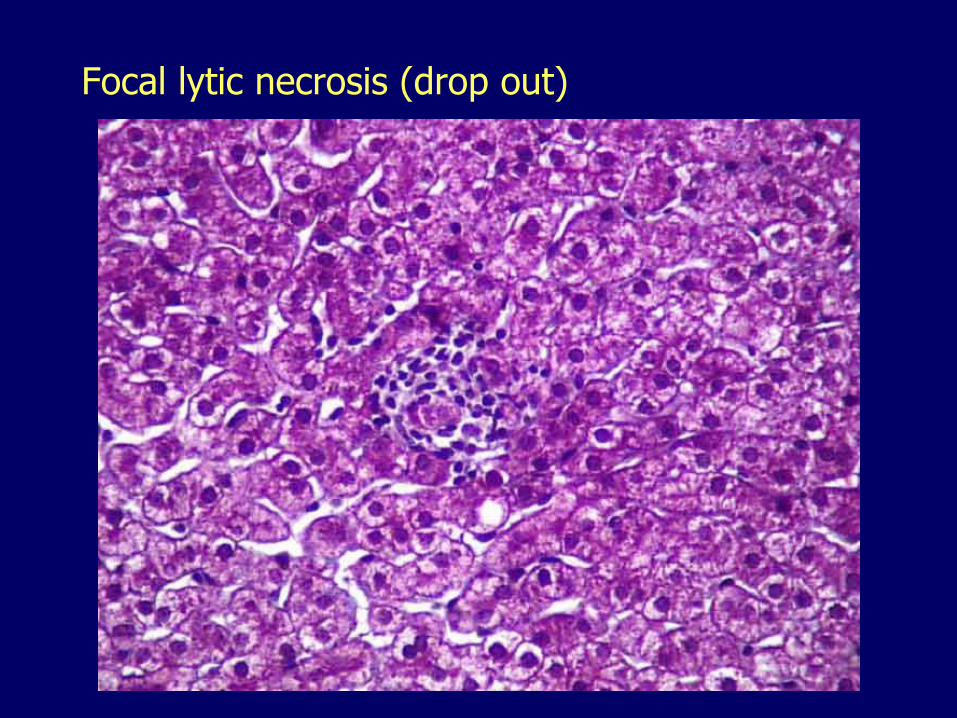
Focal lytic necrosis (drop out)

Apoptosis, apoptotic body
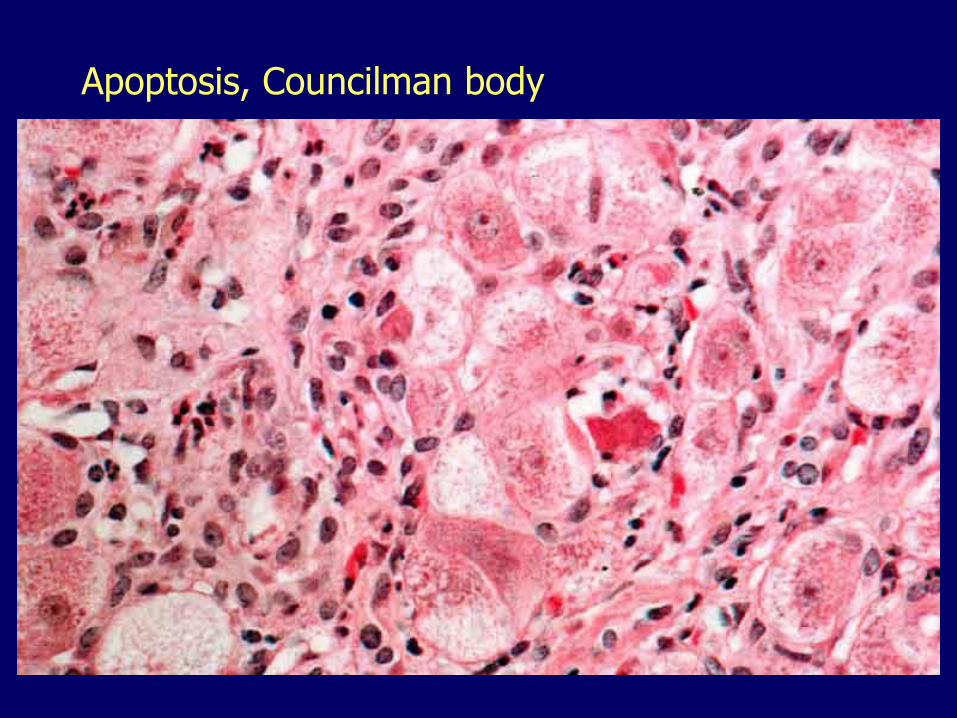
Apoptosis, Councilman body
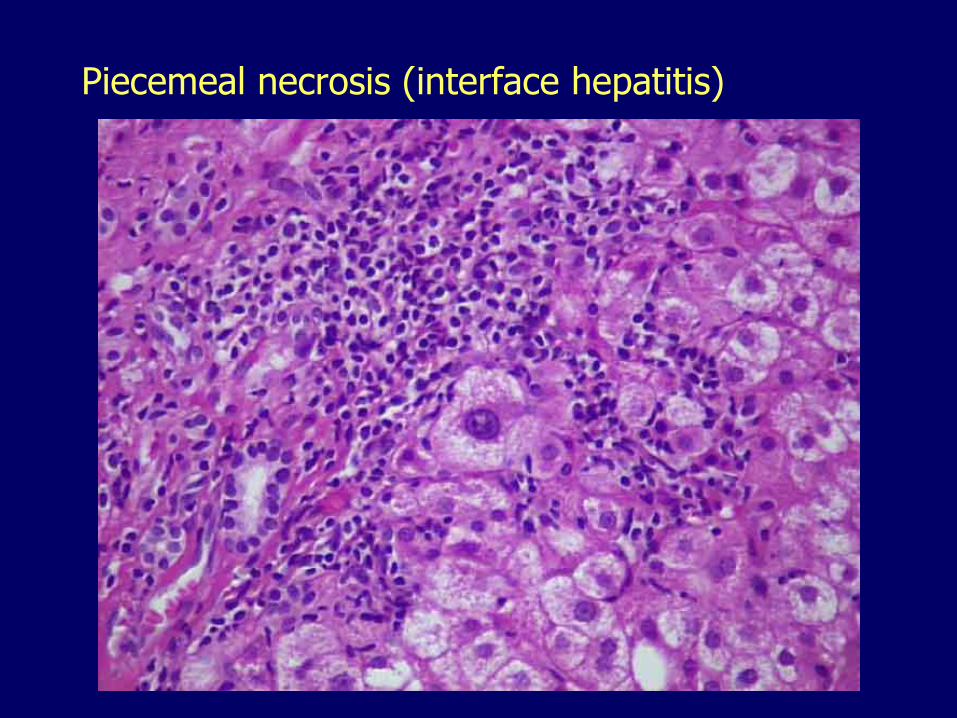
Piecemeal necrosis (interface hepatitis)
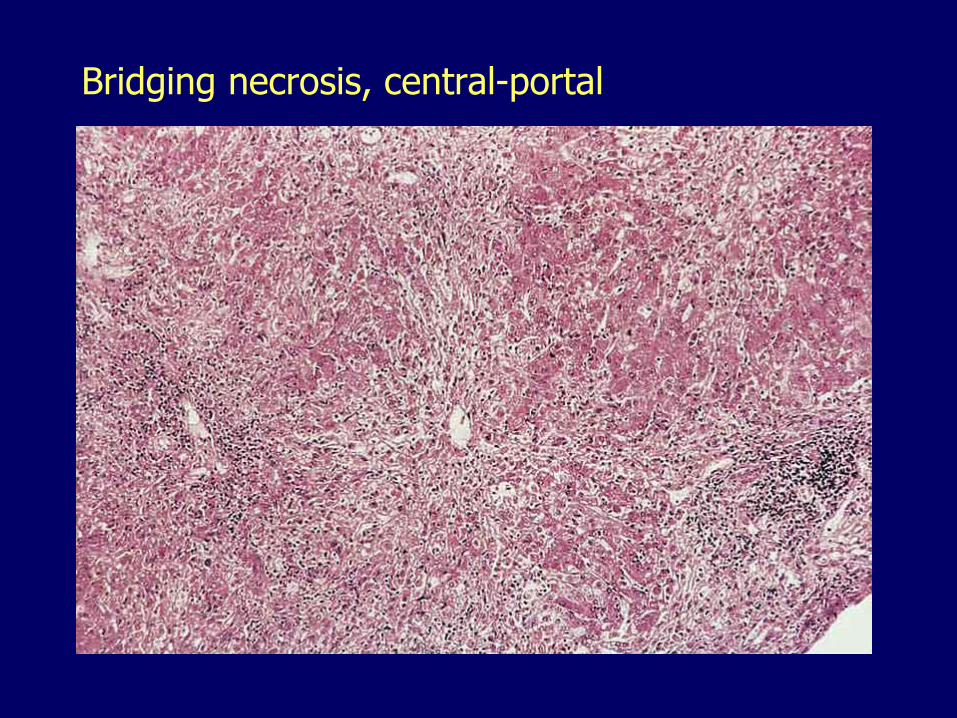
Bridging necrosis, central-portal
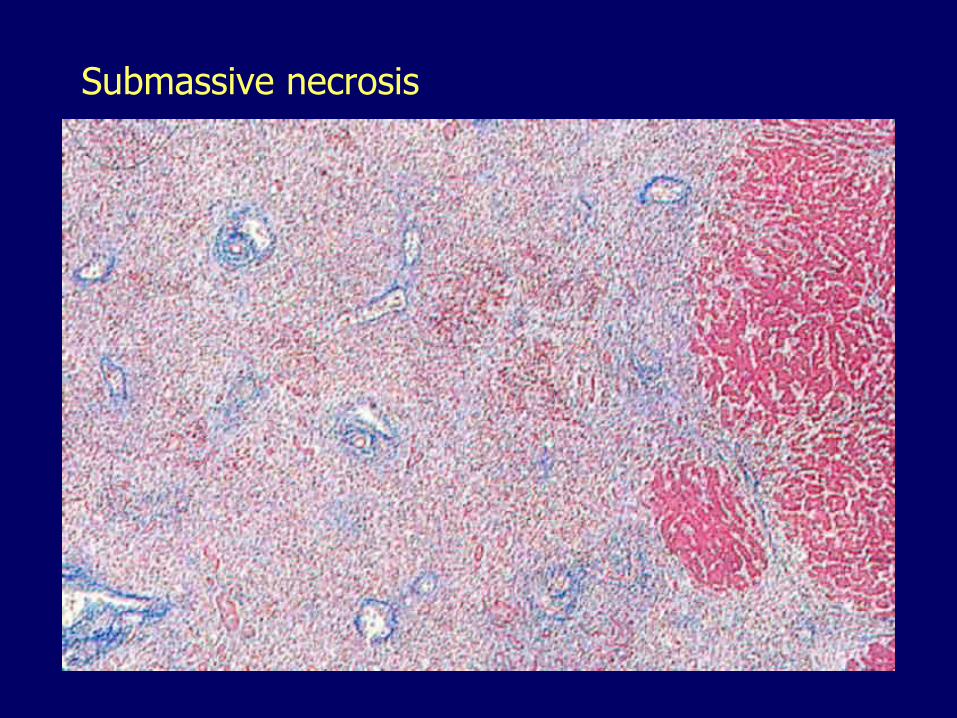
Submassive necrosis
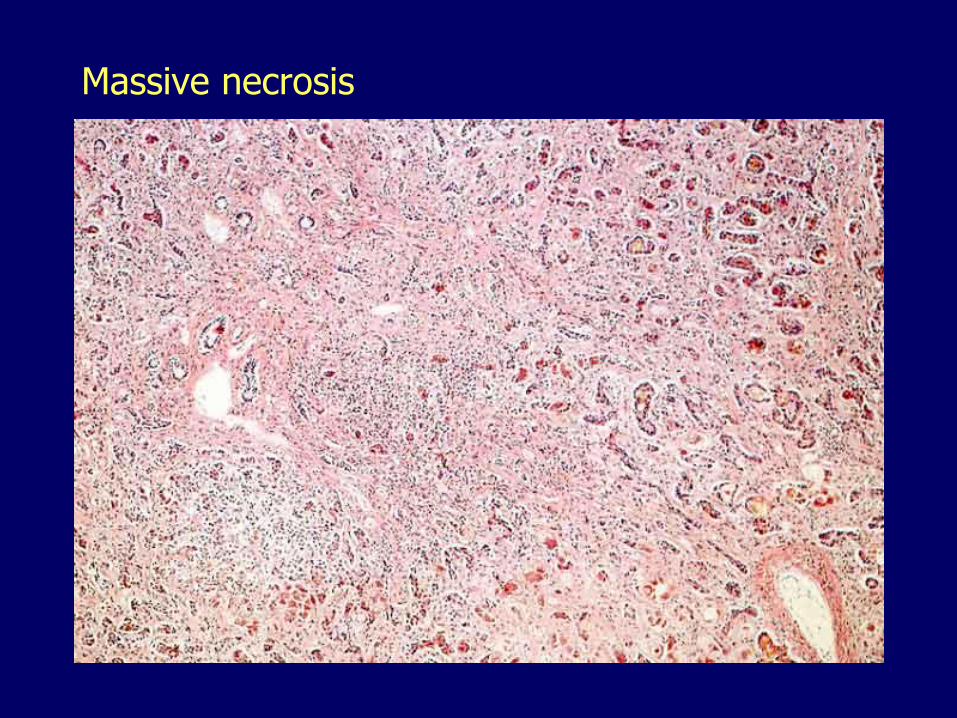
Massive necrosis
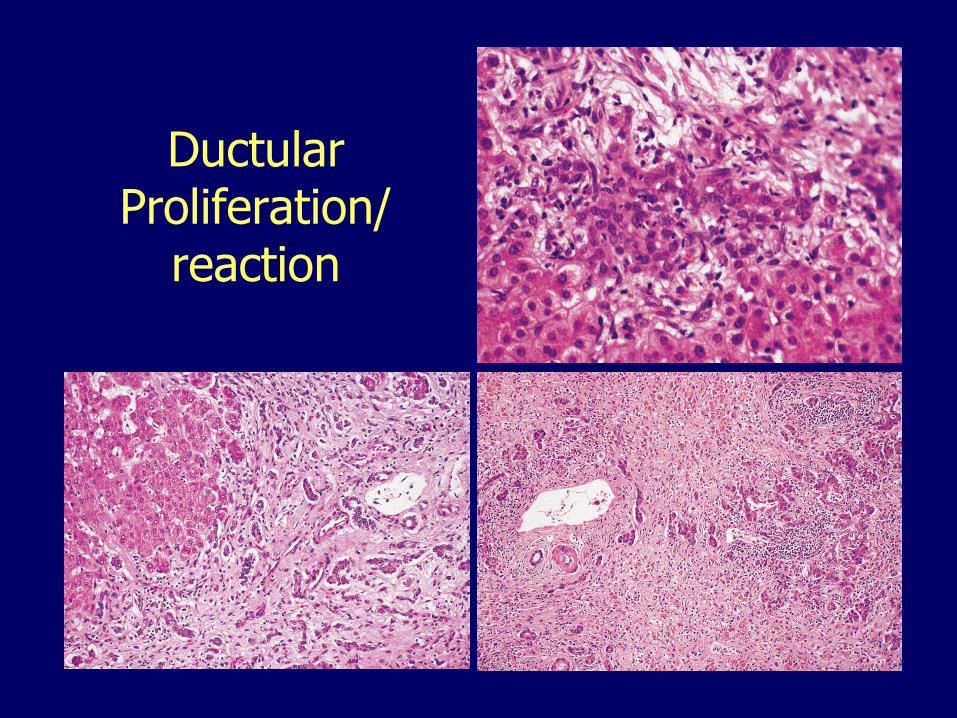
Ductular Proliferation/
reaction

Absence of fibrosis (trichrome stain)

Fibrosis, portal (trichrome stain)

Fibrosis, periportal (trichrome stain)
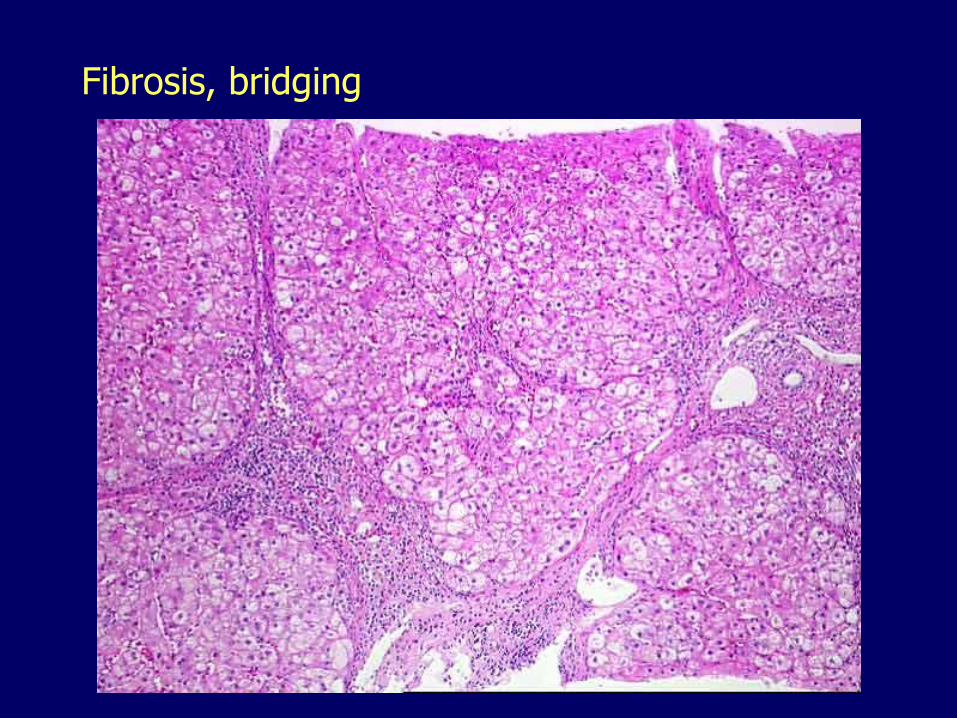
Fibrosis, bridging
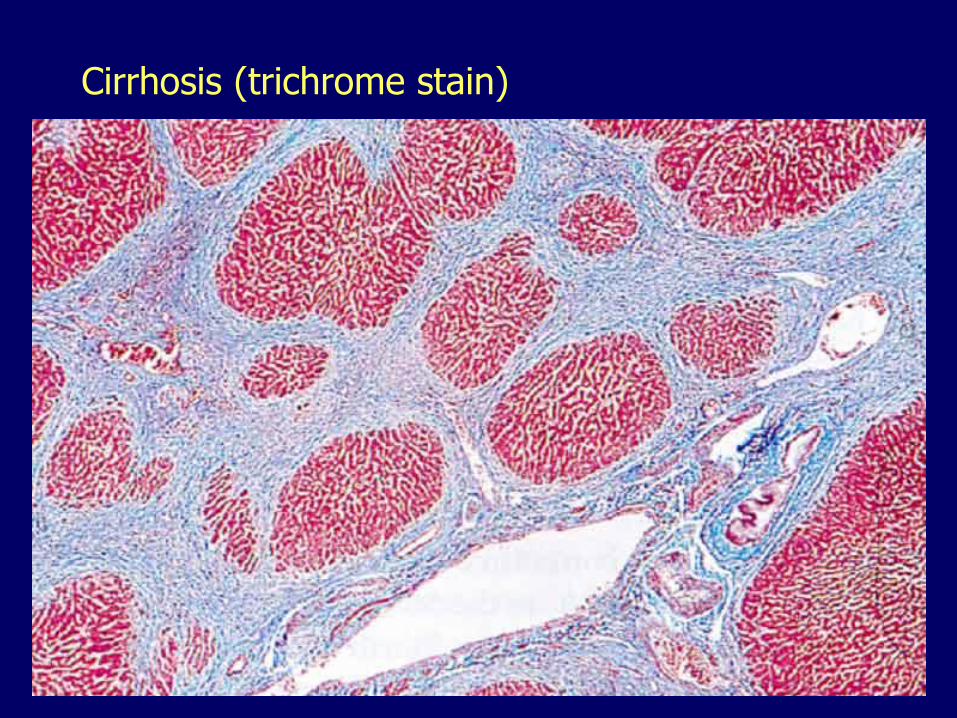
Cirrhosis (trichrome stain)
The liver 011. Functional reserve
2. Anatomic considerations
3. Patterns of injury
4. Cirrhosis5. Hyperbilirubinemias, cholestasis
6. Liver failure
Cirrhosis
A diffuse process characterized by:
– Fibrosis (broad bridging fibrous septa)
– Structurally abnormal, regenerative parenchymal nodules
– i.e., scarring and regeneration affecting the entire liver

Cirrhosis, macronodular

Cirrhosis, micronodular
Cirrhosis, pathogenesis Inflammation
Hepatocyte injury and regeneration
Transformation of stellate cells into myofibroblasts-like cells
Deposition of collagen in the space of Disse
Loss of sinusoidal fenestrations
Bridging fibrosis
Impaired exchange of nutrients, waste products
Impaired secretion of proteins
Vascular shunting (bypass through new vascular channels)
Cirrhosis, etiology– Alcoholic steatohepatitis
– Non-alcoholic steatohepatitis
– Viral• In the US mostly hepatitis C
• Worldwide mostly hepatitis B
– Primary biliary cirrhosis
– Autoimmune hepatitis
– Inherited disorders:• Primary hemochromatosis
• Wilson disease
• Alpha-1-antitrypsin deficiency
– Cryptogenic
Cirrhosis, outcome
May remain asymptomatic
– Functional reserve: 80% to 90%
“Constitutional” symptoms: anorexia, fatigue, weight loss
Portal hypertension
Overt liver failure
Hepatocellular carcinoma
Child-Pugh score
Used to assess the prognosis of cirrhosis
– Total bilirubin
– Albumin
– Prothrombin time/INR
– Ascites
– Encephalopathy
The liver 011. Functional reserve
2. Anatomic considerations
3. Patterns of injury
4. Cirrhosis
5. Liver failure6. Hyperbilirubinemias, cholestasis
Liver failure, etiology Massive necrosis (acute, fulminant, failure)
– Acetaminophen
– Other drugs/toxins
– Hepatitis (viral hepatitis A and B, autoimmune hepatitis)
Dysfunction without overt necrosis– Acute fatty liver (microvesicular steatosis)
• Reye syndrome
• Acute fatty liver of pregnancy
Decompensation of chronic liver disease– Chronic hepatitis and cirrhosis
• Alcoholic and non-alcoholic steatohepatitis, Hep C or B
Liver failure, manifestations
Jaundice
Liver may shrink
Hypoalbuminemia
– Peripheral edema
– Ascites
Coagulopathy
Hyperestrogenemia
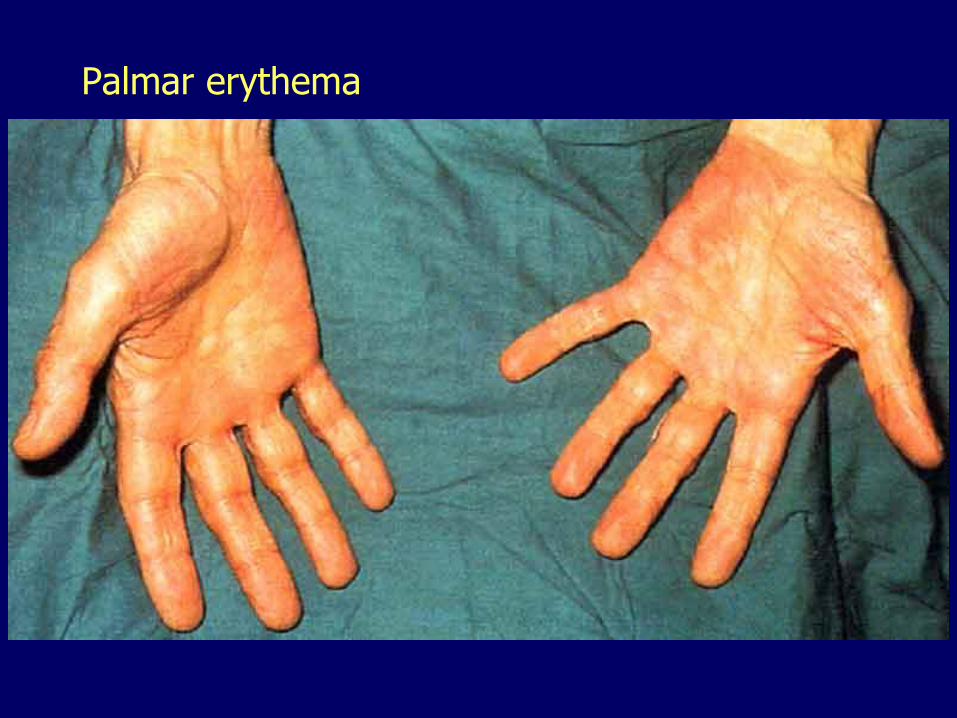
Palmar erythema
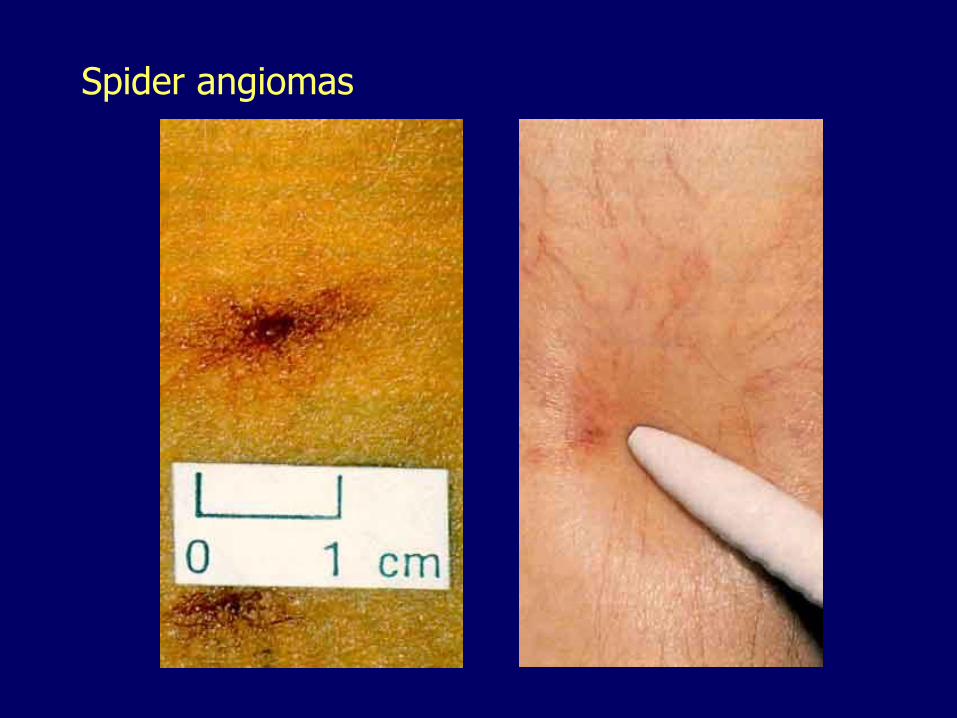
Spider angiomas
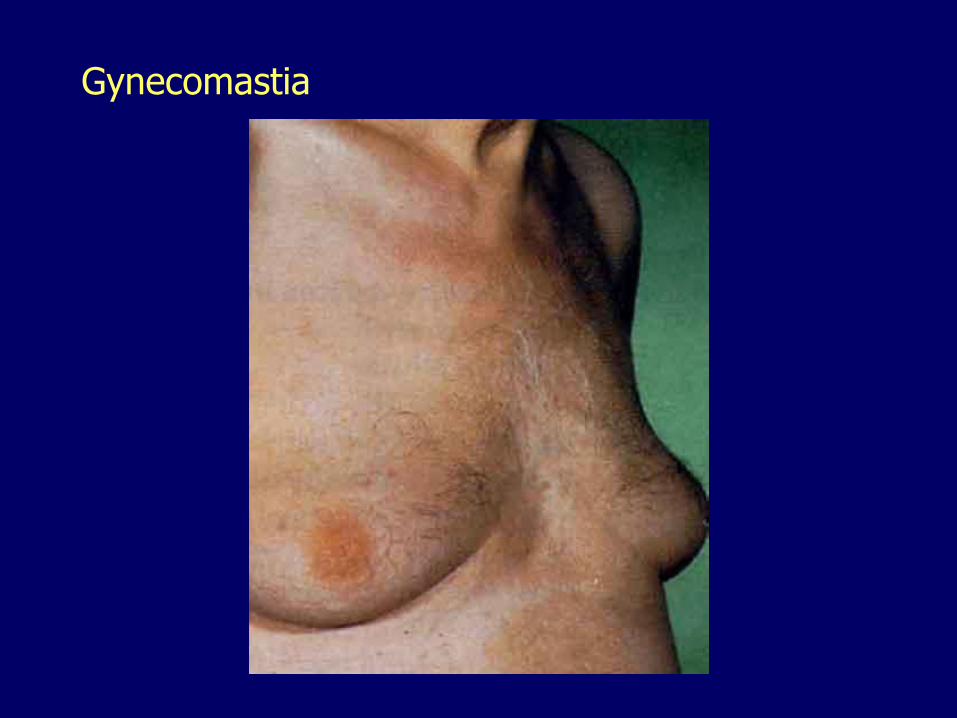
Gynecomastia
Liver failure, manifestations
Fetor hepaticus, accumulation of mercaptans (derived from methionine)
Hyperammonemia, hepatic encephalopathy
– Abnormal neurotransmission, brain edema
– Confusion, stupor, coma
– Rigidity, hyperreflexia, asterixis *
Liver failure, manifestations Cirrhosis and portal hypertension cause visceral
vasodilation, decrease vascular resistance
Initially compensated by increase in cardiac output
Disease progression causes decompensation
Two complications with high mortality:
– Renal failure (hepatorenal syndrome)
• Renal underperfusion
– Respiratory failure (hepatopulmonary syndrome)
• Ventilation-perfusion mismatch
The liver 011. Functional reserve
2. Anatomic considerations
3. Patterns of injury
4. Cirrhosis
5. Liver failure
6. Hyperbilirubinemias, cholestasis
– Bilirubin metabolism
– Unconjugated hyperbilirubinemia
– Conjugated hyperbilirubinemia
– Cholestasis
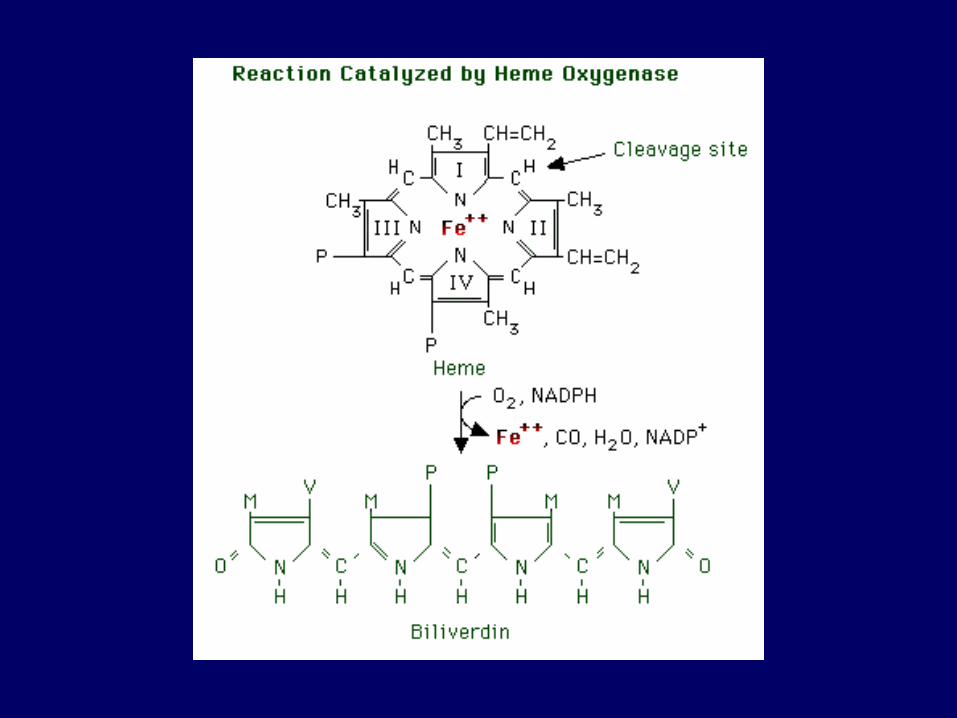
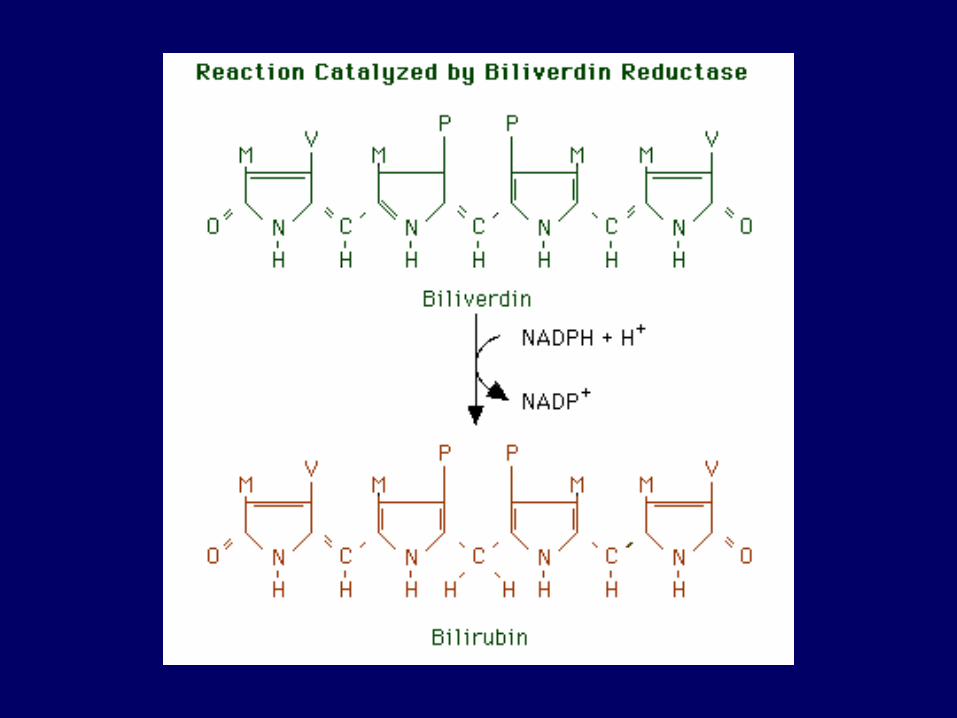
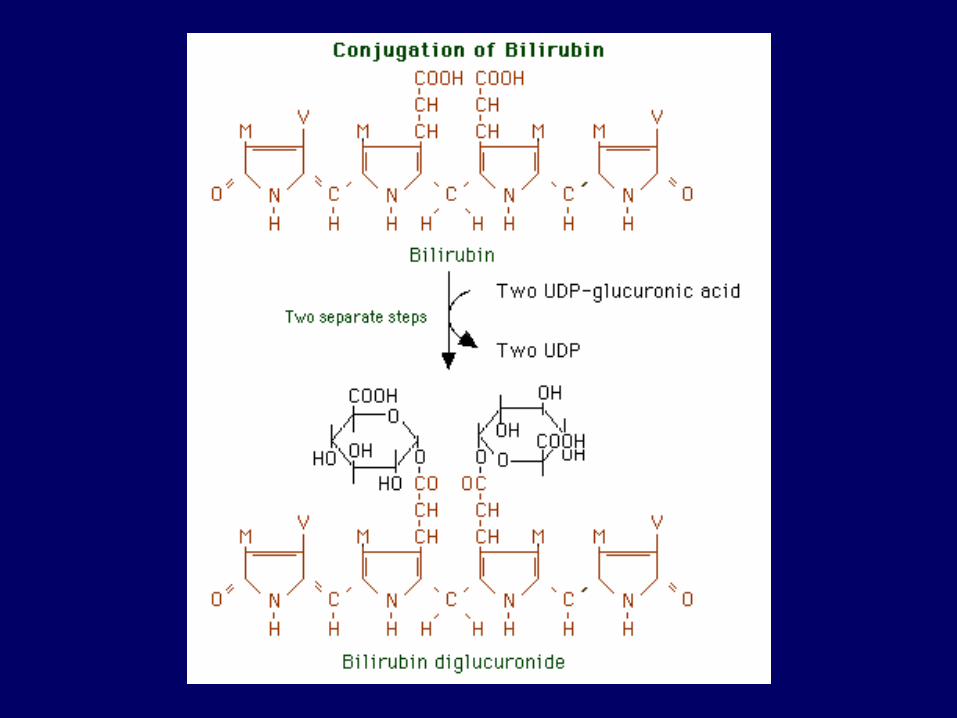
Bilirubin metabolism
– Bilirubin is derived from the prosthetic group heme• Hemoglobin
– Normal destruction of old erythrocytes by mononuclear phagocytic system, spleen
– Pathologic destruction of newly formed erythrocytes in the bone marrow(ineffective erythropoiesis: thalassemia, sideroblastic anemia, megaloblastic anemia)
• Other hemoproteins– Cytochromes, mostly in the liver
Unconjugated (indirect) bilirubin
Water-insoluble
– Tightly bound to albumin
– Not excreted in urine
– Potentially toxic
Hepatocyte carrier-mediated uptake
Conjugation: UDP-glucuronosyl transferase (UGT)
Conjugated (direct) bilirubin
Water-soluble
– Loosely bound to albumin
– Non-toxic
– Excreted in urine
– Actively excreted into the bile canaliculi
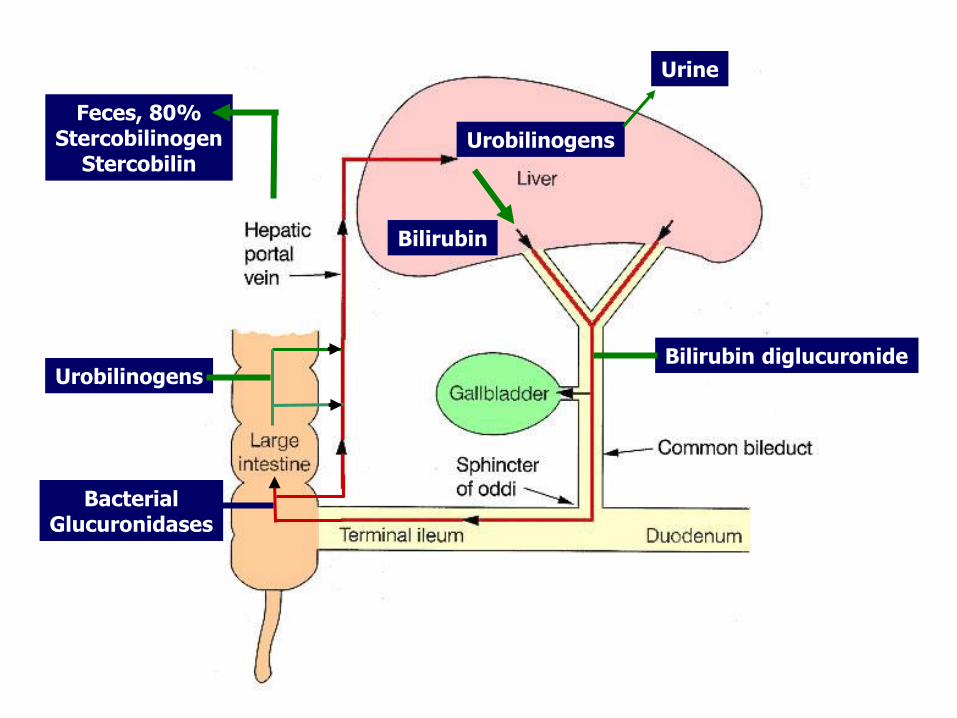
Bilirubin diglucuronide
BacterialGlucuronidases
Urobilinogens
Urobilinogens
Urine
Feces, 80%Stercobilinogen
Stercobilin
Bilirubin
Bilirubin
– Unconjugated (indirect) bilirubin
• Water-insoluble
• Tightly bound to albumin
• Not excreted in urine
• Potentially toxic
– Conjugated (direct) bilirubin
• Water-soluble
• Loosely bound to albumin
• Excreted in urine
• Not toxic

Jaundice, skin (bilirubin > 2.0-2.5 mg/dL)
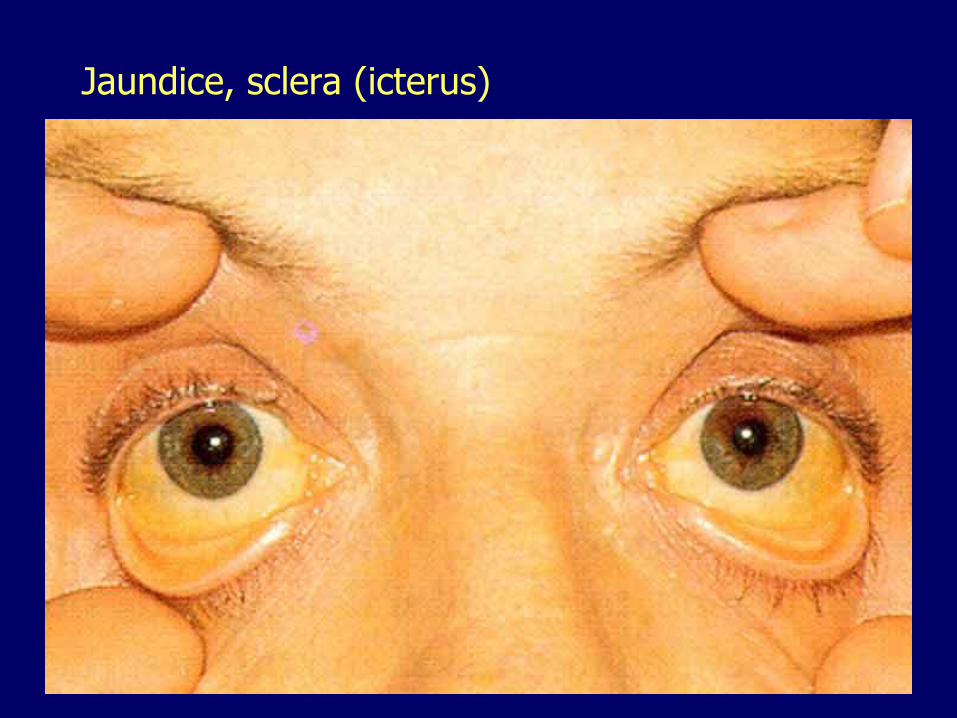
Jaundice, sclera (icterus)
Unconjugated (indirect) hyperbilirubinemia
– Excessive bilirubin production• Internal bleeding
• Hemolytic anemias
– Reduced uptake into the hepatocytes• Drugs
• Hepatocyte injury
– Impaired conjugation within the hepatocytes
• Hepatocyte injury
• Hereditary hyperbilirubinemia
• Physiologic jaundice of the newborn
Erythroblastosis fetalis
Hemolytic anemia of newborn– Rh-negative mother, antibodies to Rh-
positive fetal blood
Marked neonatal unconjugatedhyperbilirubinemia
Injury of basal ganglia, pons, cerebellum (kernicterus)– Lethargy, death
– Cerebral palsy, mental retardation, hearing loss
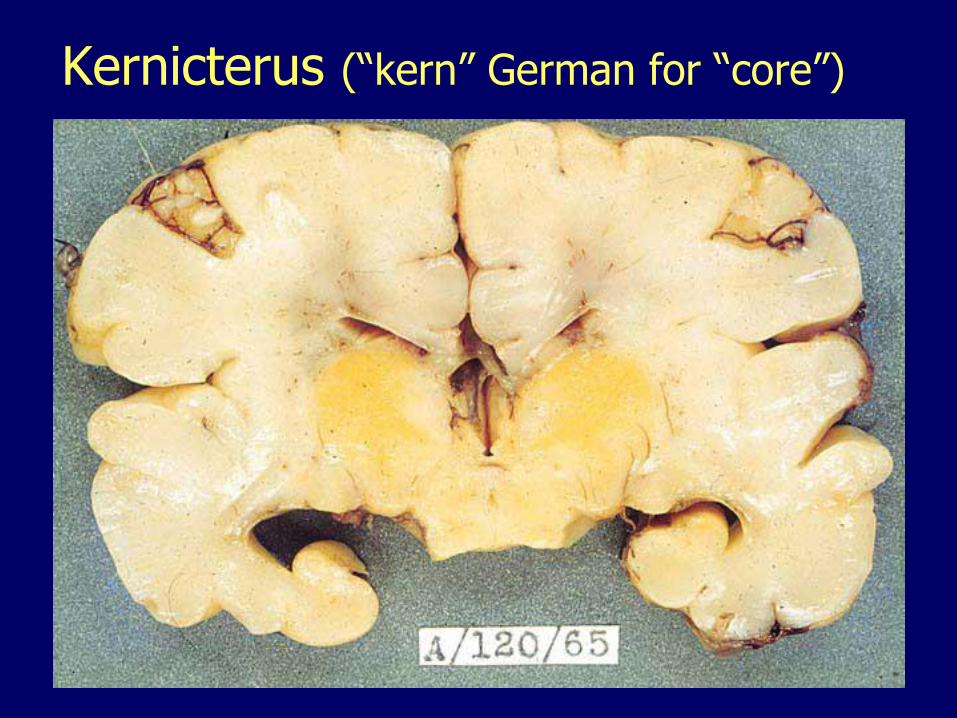
Kernicterus (“kern” German for “core”)
Neonatal jaundice (physiologic jaundice of the newborn)
Transient, mild unconjugatedhyperbilirubinemia
Immature conjugation of bilirubin
Jaundice in:• 60% of term infants
• 80% of prematures
– Visible, 2nd to 3rd day
– Disappears, 5th to 7th day
Neonatal jaundice (physiologic jaundice of the newborn)
Breast-fed infants greater frequency• Maternal milk inhibition of UGT
• Beta-glucuronidases in maternal milk
– Deconjugate bilirubin in the intestine
– Deconjugated bilirubin is readily reabsorbed (increased enterohepatic circulation)
• Neonates lack intestinal bacteria that normally catabolize bilirubin into urobilinogens, stercobilinogen, stercobilin, making more bilirubin available for reabsorption
Unconjugated hereditary hyperbilirubinemias
Impaired conjugation (UGT defect)
Crigler-Najjar type I• UGT is completely absent
• Fatal without liver transplantation
Crigler-Najjar type II• Markedly reduced UGT activity
• Nonfatal but risk of kernicterus
Gilbert syndrome• Reduced UGT activity (about 30% of normal levels)
• Common (6% of the population)
• Mild hyperbilirubinemia with fasting, stress
Conjugated (direct) hyperbilirubinemia
– Decreased hepatocellular excretion
• Hepatocellular injury
• Hereditary hyperbilirubinemia
– Cholestasis (arrest in the flow of bile)
Conjugated hereditary hyperbilirubinemias
Impaired bilirubin excretion
Jaundice, clinically inconsequential
Rotor syndrome
– Liver is not pigmented
Dubin-Johnson syndrome
– Liver is darkly pigmented (defect in a canalicular multi-specific organic anion transport protein –Mrp2, polymers of epinephrine accumulate)
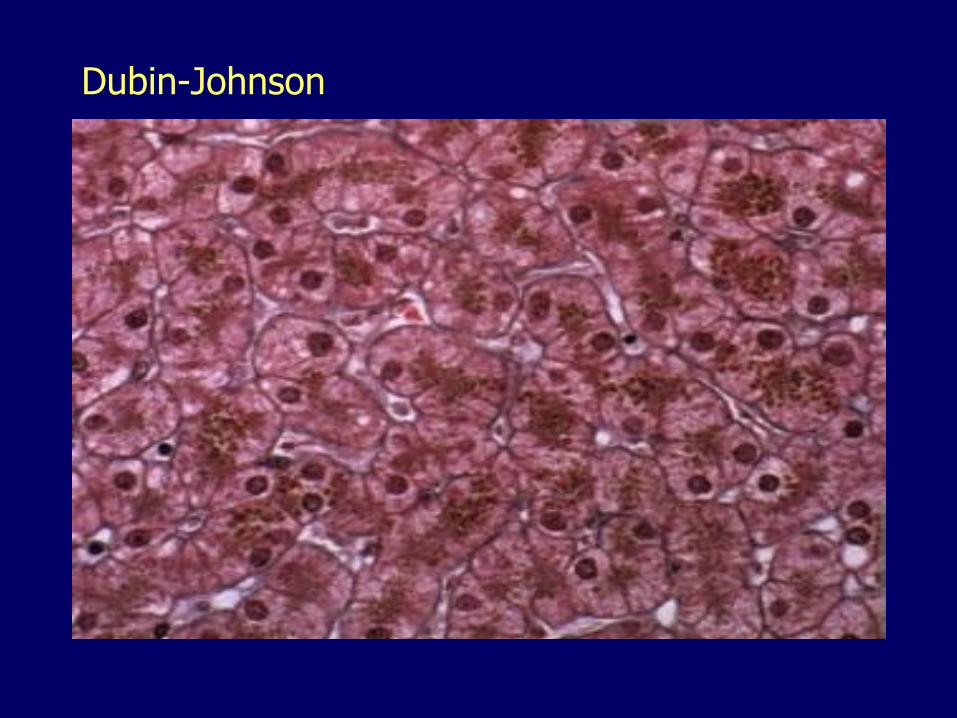
Dubin-Johnson
Cholestasis
Arrest in the flow of bile
Retention of bilirubin, bile acids and other solutes
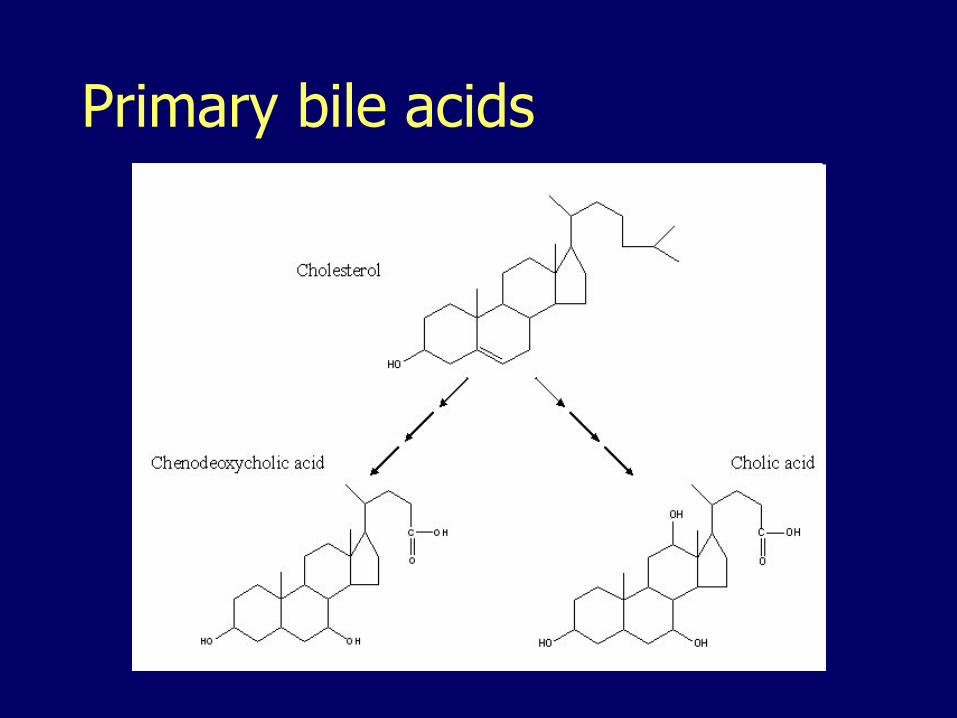
Primary bile acids
Bile acids
– Amphipathic, emulsify lipids, form micelles
– Role in
• Excretion of lipids from the liver
• Absorption of lipids from the intestine
– 95% are actively reabsorbed in the terminal ileum
– Reexcreted in the bile (enterohepatic circulation)
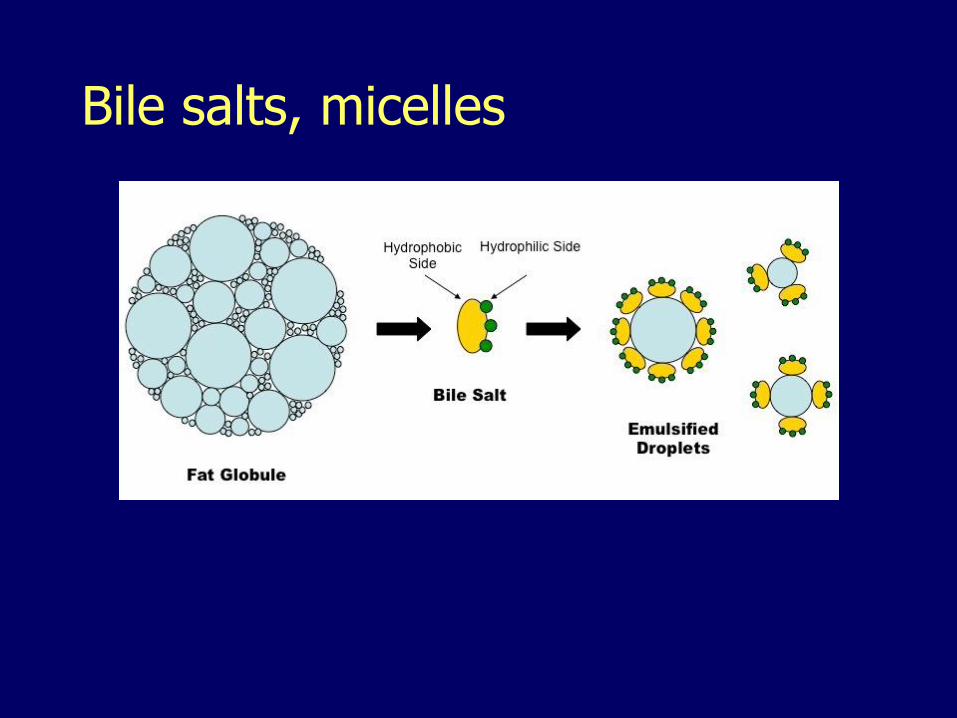
Bile salts, micelles
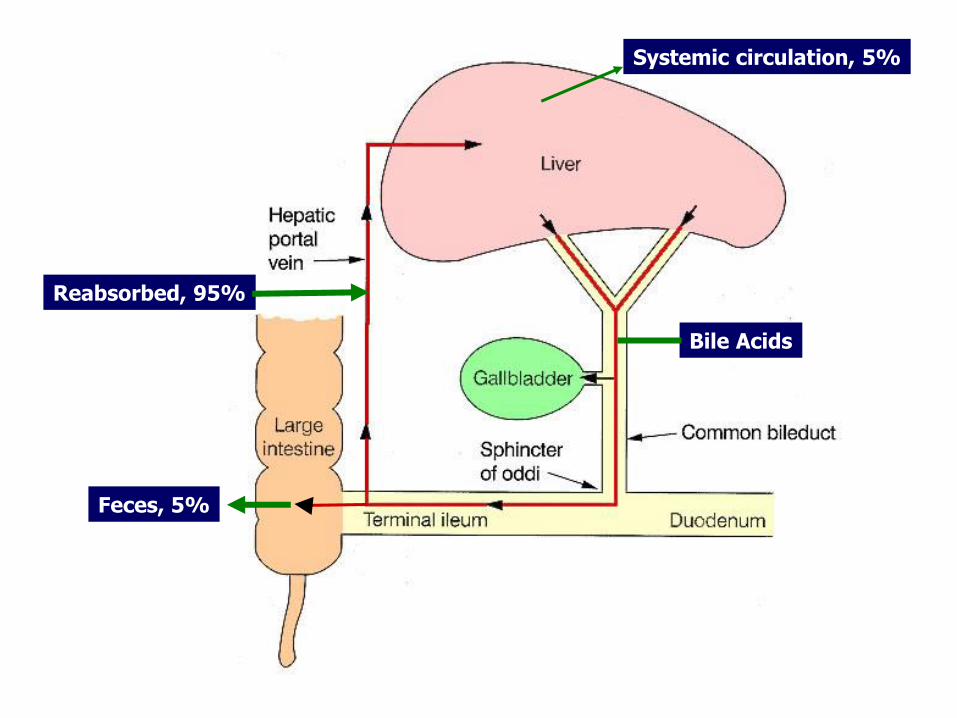
Bile Acids
Feces, 5%
Reabsorbed, 95%
Systemic circulation, 5%
Cholestasis, manifestations Conjugated hyperbilirubinemia
Elevated bile acids
Hypercholesterolemia
Elevated ALP, GGT
Malabsorption, fat-soluble vitamins (A, D, E and K)– Bleeding diathesis: impaired synthesis of vitamin-
K-dependent coagulation factors II, VII, IX and X
Steatorrhea, fat in feces
Acholia, pale stools
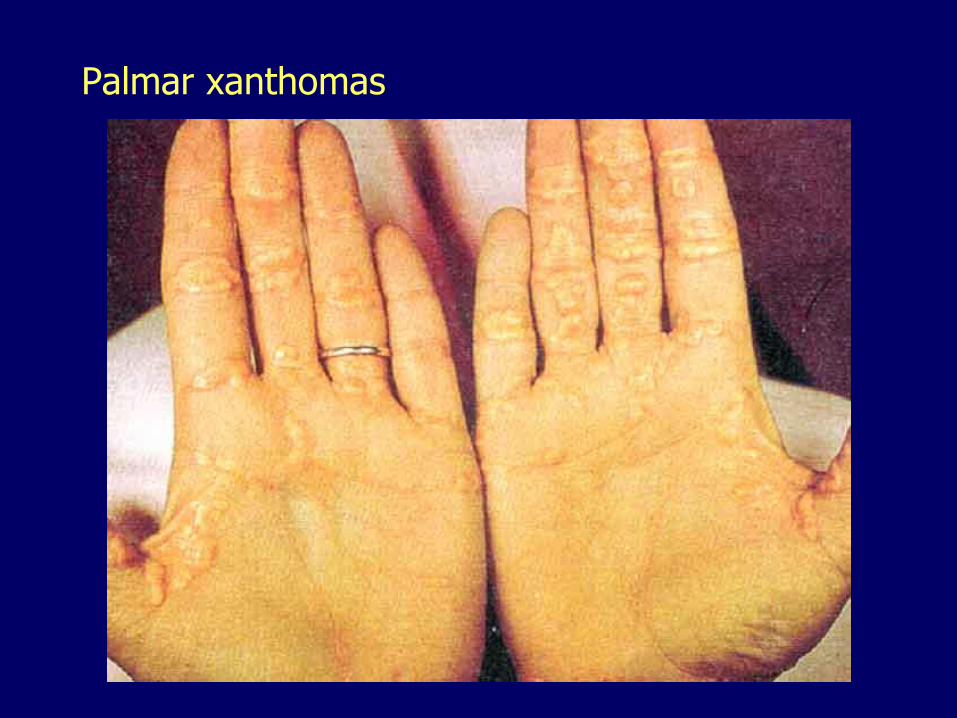
Palmar xanthomas
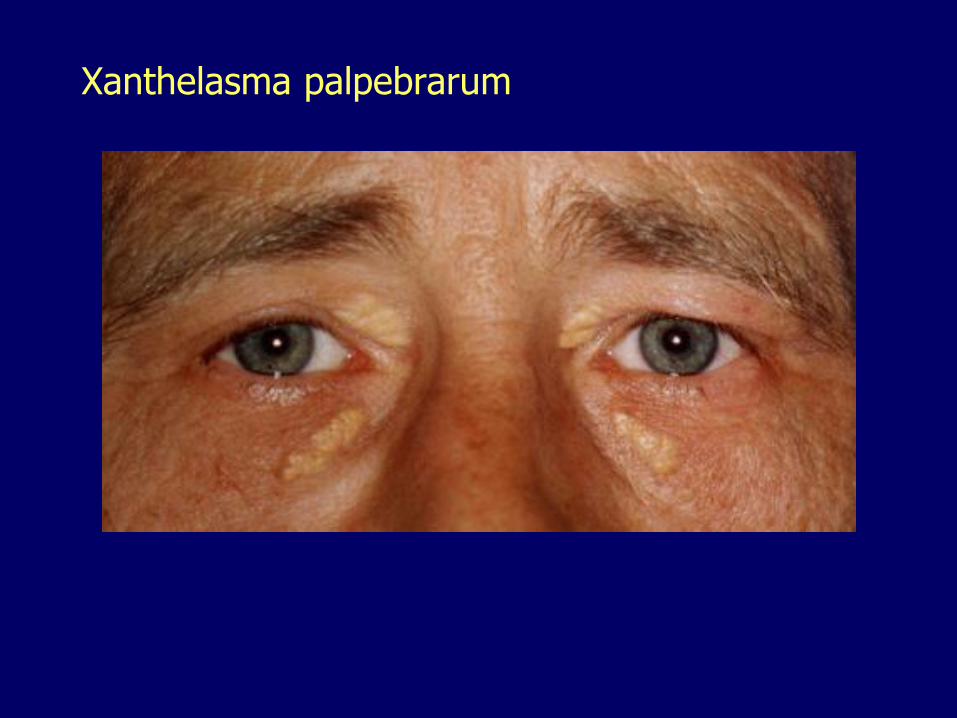
Xanthelasma palpebrarum
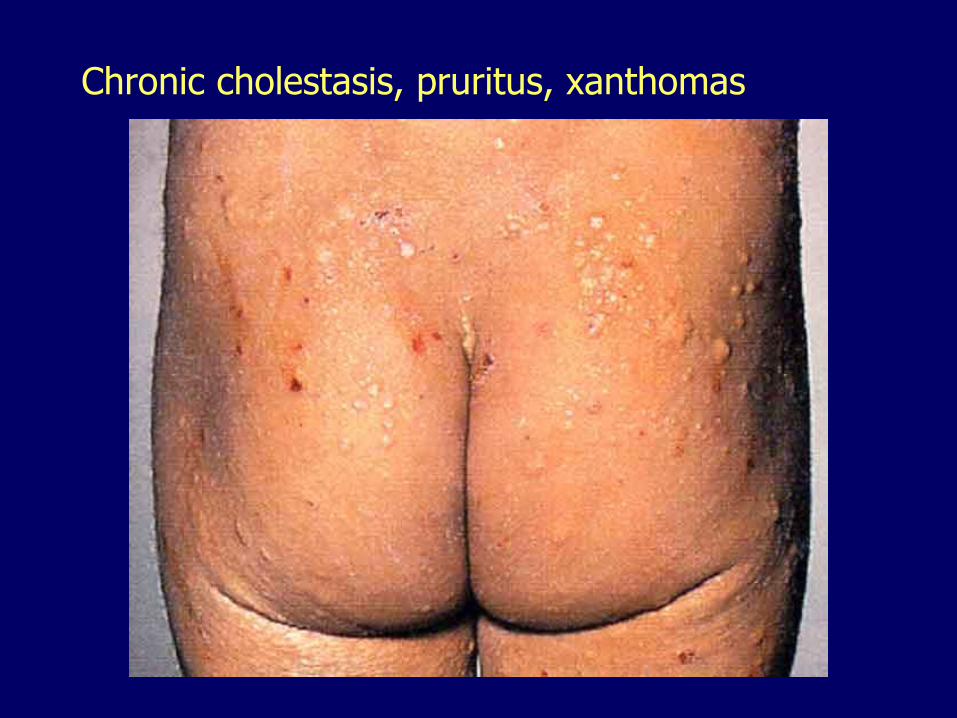
Chronic cholestasis, pruritus, xanthomas
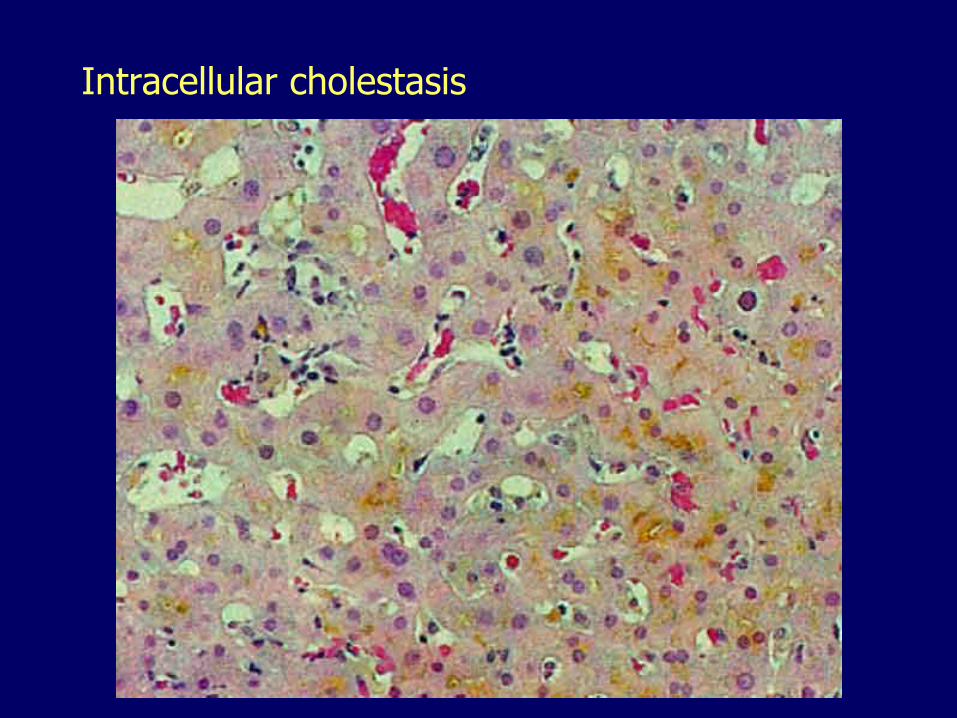
Intracellular cholestasis
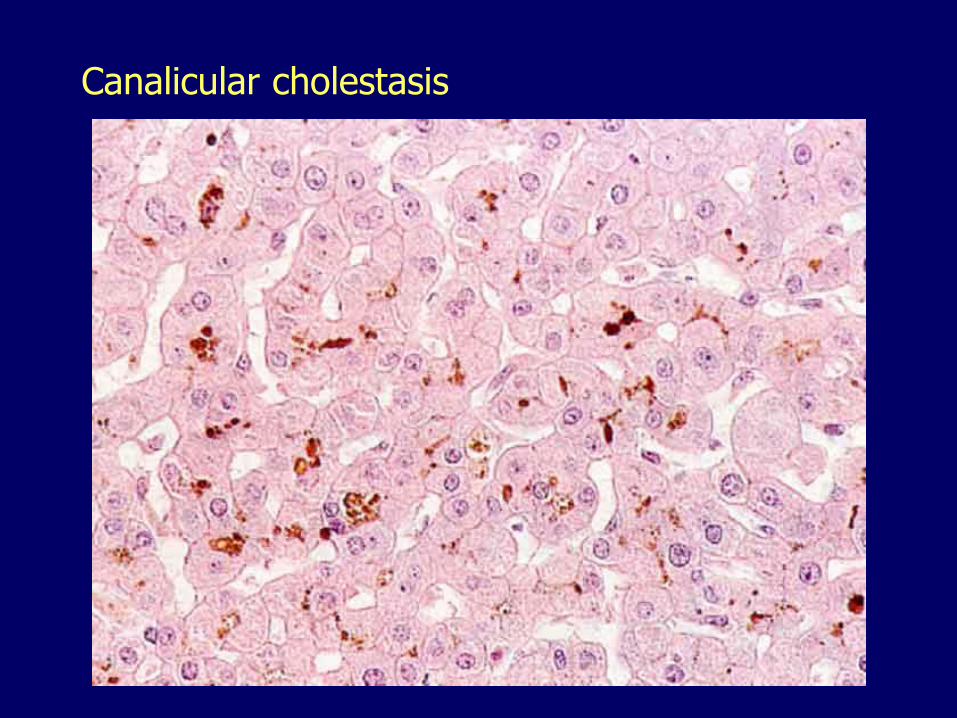
Canalicular cholestasis
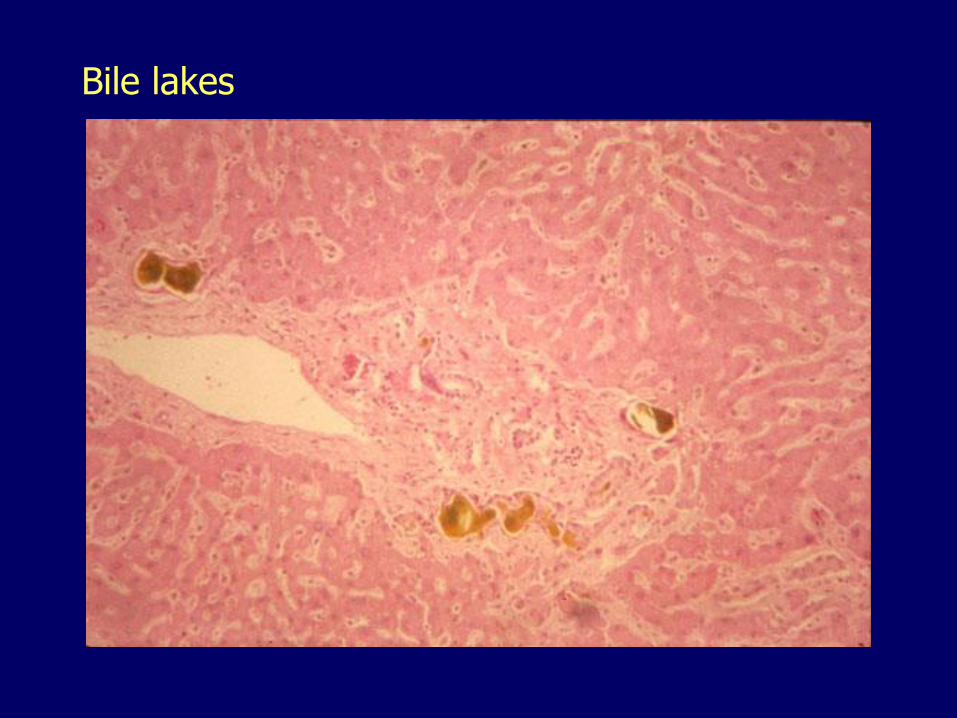
Bile lakes
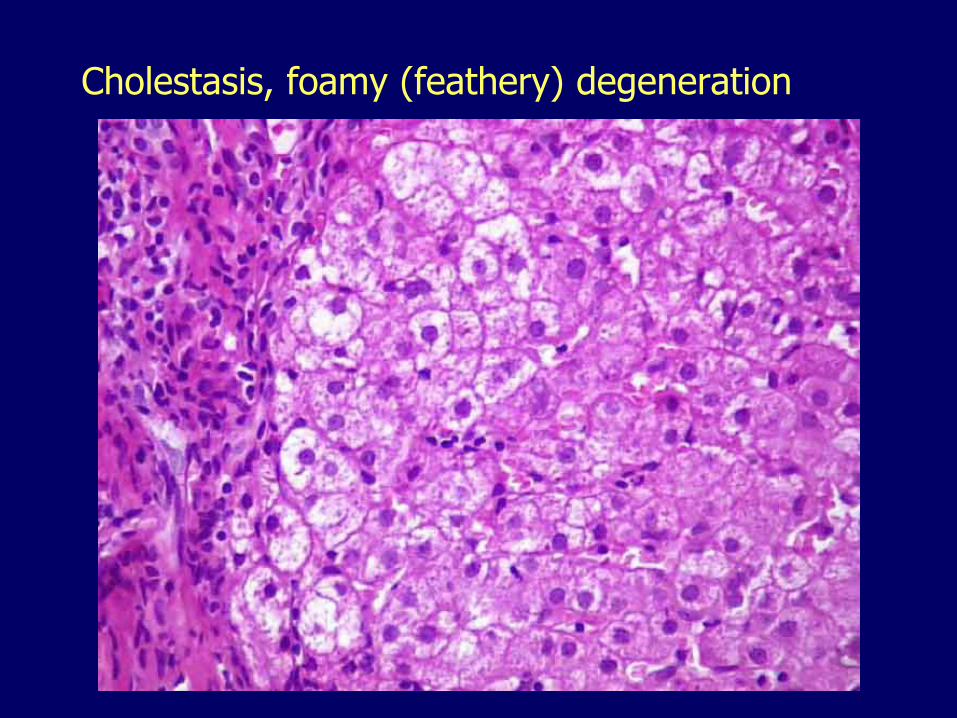
Cholestasis, foamy (feathery) degeneration
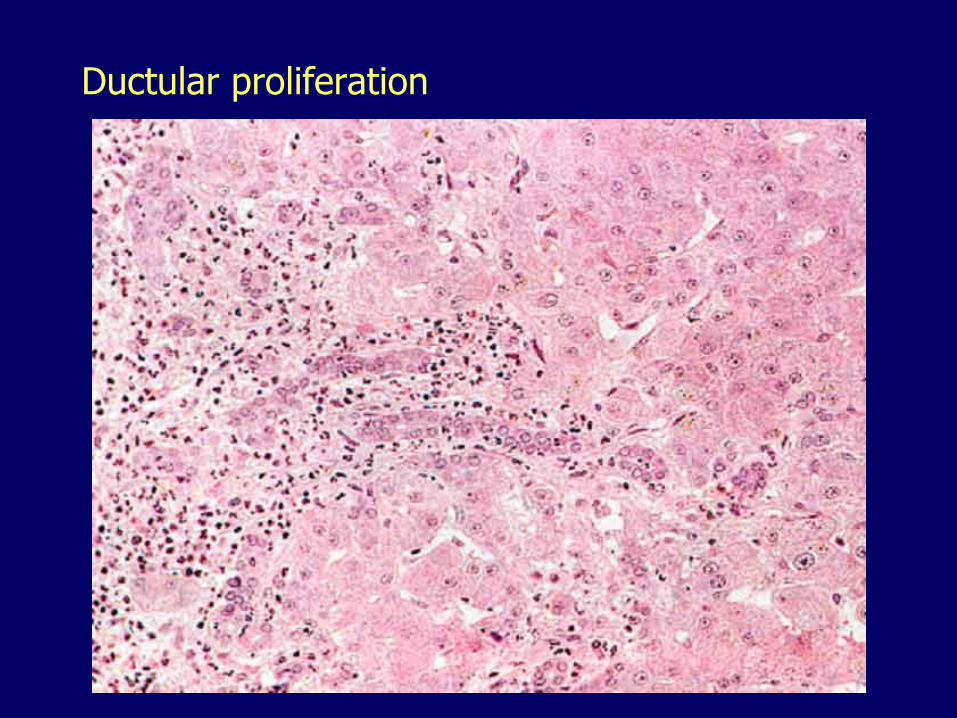
Ductular proliferation
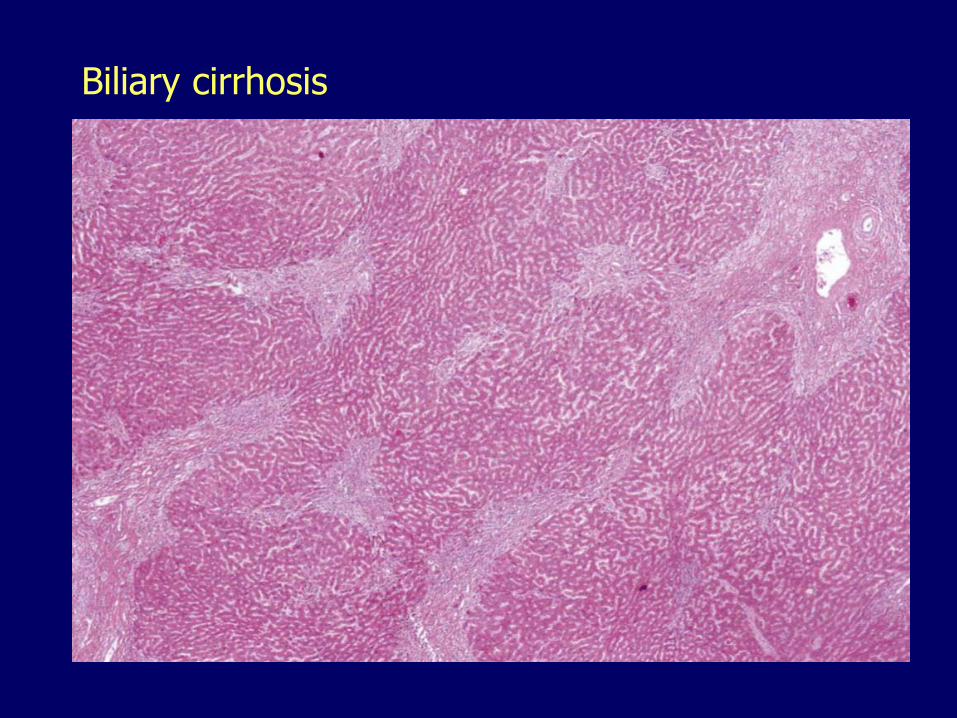
Biliary cirrhosis

Biliary cirrhosis
Cholestasis
Major causes:
– Obstructive
• Choledocholithiasis
• Cholangitis
• Primary biliary cirrhosis
• Primary sclerosing cholangitis
– Hepatocellular
• Drug-related
• Hepatitis
• Hereditary
Neonatal cholestasis Prolonged conjugated hyperbilirubinemia
Obstructive– Extrahepatic biliary atresia
– Choledochal cyst
Hepatocellular (neonatal hepatitis)– Congenital metabolic disorders
• Alpha-1-antitrypsin deficiency
• Tyrosinemia, Niemann-Pick, galactosemia…
– Infections• Cytomegalovirus, HIV, hepatitis viruses, bacteria…
– Endocrine disorders, toxins, drugs
– Idiopathic, 10-20% of cases

Neonatal cholestasis (obstructive)Bile ductular proliferation and portal fibrosis
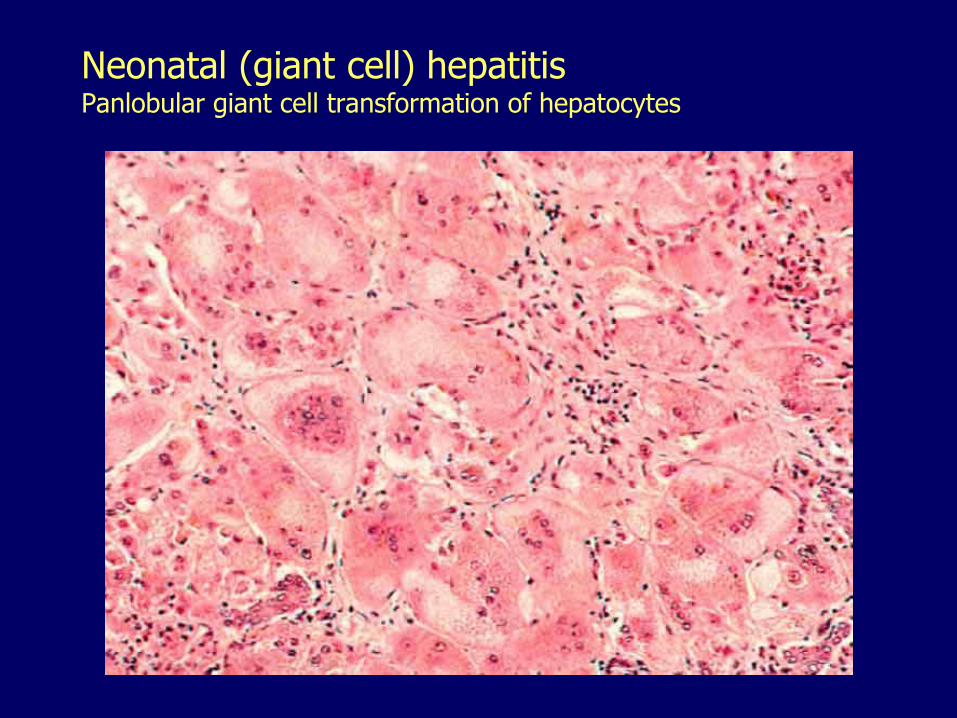
Neonatal (giant cell) hepatitisPanlobular giant cell transformation of hepatocytes
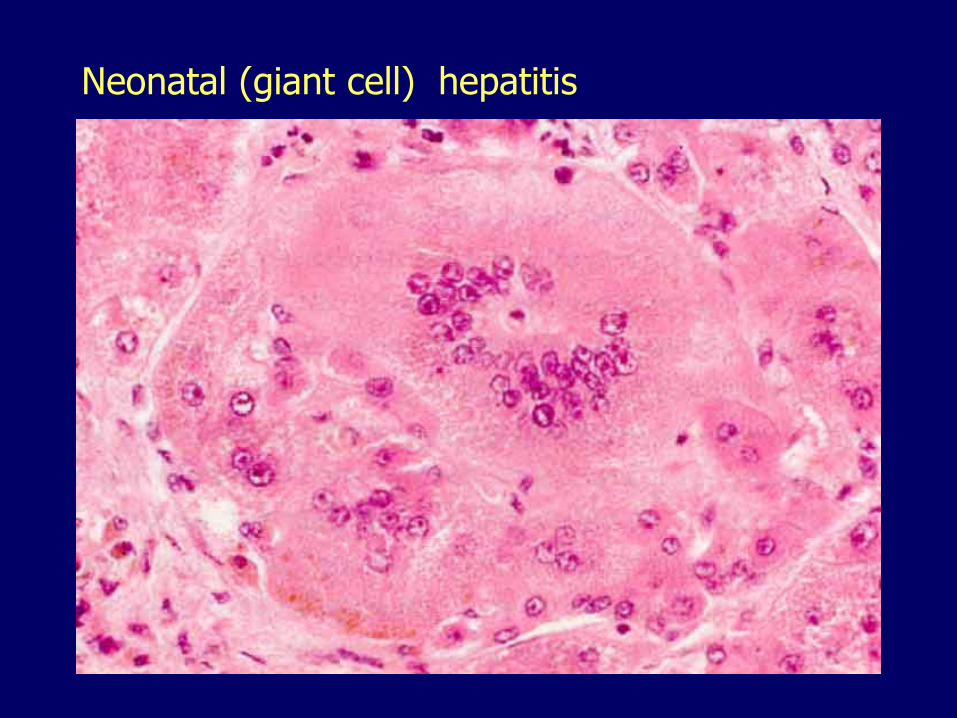
Neonatal (giant cell) hepatitis

















![arXiv:1705.03260v1 [cs.AI] 9 May 2017 · 2018. 10. 14. · Vegetables2 Normalized Log Size Vehicles1 Normalized Log Size Vehicles2 Normalized Log Size Weapons1 Normalized Log Size](https://static.fdocuments.net/doc/165x107/5ff2638300ded74c7a39596f/arxiv170503260v1-csai-9-may-2017-2018-10-14-vegetables2-normalized-log.jpg)