Diffusion-Weighted Intravoxel Incoherent Motion … Intravoxel Incoherent Motion Imaging of Renal...
9
Diffusion-Weighted Intravoxel Incoherent Motion Imaging of Renal Tumors With Histopathologic Correlation Hersh Chandarana, MD,* Stella K. Kang, MD,* Samson Wong, MD,* Henry Rusinek, PhD,* Jeff L. Zhang, PhD,Þ Shigeki Arizono, MD, PhD,þ William C. Huang, MD,§ Jonathan Melamed, MD,|| James S. Babb, PhD,* Edgar F. Suan, BS,* Vivian S. Lee, MD, PhD,Þ and Eric E. Sigmund, PhD* Purpose: The aim of this study was to use intravoxel incoherent motion diffusion-weighted imaging to discriminate subtypes of renal neoplasms and to assess agreement between intravoxel incoherent motion (perfusion fraction, f p ) and dynamic contrast-enhanced magnetic resonance imaging (MRI) metrics of tumor vascularity. Subjects and Methods: In this Health Insurance Portability and Account- ability ActYcompliant, institutional review boardYapproved prospective study, 26 patients were imaged at 1.5-T MRI using dynamic contrast-enhanced MRI with high temporal resolution and diffusion-weighted imaging using 8 b values (range, 0-800 s/mm 2 ). Perfusion fraction ( f p ), tissue diffusivity (D t ), and pseudodiffusivity (D p ) were calculated using biexponential fitting of the diffusion data. Apparent diffusion coefficient (ADC) was calculated with monoexponential fit using 3 b values of 0, 400, and 800 s/mm 2 . Dynamic contrast-enhanced data were processed with a semiquantitative method to generate model-free parameter cumulative initial area under the curve of gadolinium concentration at 60 seconds (CIAUC 60 ). Perfusion fraction, D t , D p , ADC, and CIAUC 60 were compared between different subtypes of renal lesions. Perfusion fraction was correlated with CIAUC 60 . Results: We examined 14 clear cell, 4 papillary, 5 chromophobe, and 3 cystic renal cell carcinomas (RCCs). Although f p had higher accuracy (area under the curve, 0.74) for a diagnosis of clear cell RCC compared with D t or ADC, the combination of f p and D t had the highest accuracy (area under the curve, 0.78). The combination of f p and D t diagnosed papillary RCC and cystic RCC with 100% accuracy, and clear cell RCC and chromophobe RCC, with 86.5% accuracy. There was significant strong correlation between f p and CIAUC 60 (r = 0.82; P G 0.001). Conclusion: Intravoxel incoherent motion parameters f p and D t can discrimi- nate renal tumor subtypes. Perfusion fraction demonstrates good correlation with CIAUC 60 and can assess degree of tumor vascularity without the use of exogenous contrast agent. Key Words: renal tumors, renal cancer, diffusion-weighted imaging, intravoxel incoherent, motion (IVIM); MRI (Invest Radiol 2012;47: 688Y696) D iffusion-weighted magnetic resonance imaging (DWI) derives image contrast from differences in the mobility (Brownian mo- tion) of water in tissues. Restriction of the random motion of water by the local microenvironment can be assessed either qualitatively or quantitatively. The decay of signal intensity (SI) as a function of in- creasing diffusion-weighting factor (or b value) is commonly ap- proximated by a monoexponential function to quantitatively assess restriction to the diffusion. The rate of decay is called the apparent diffusion coefficient (ADC) and can be mapped on a voxel-by-voxel basis as an ADC map. 1 Diffusion-weighted magnetic resonance imaging (MRI) is in- creasingly being used in the evaluation of renal lesions. Studies have shown lower ADC in malignant lesions compared to benign renal lesions. 2Y5 In addition, DWI has been used to examine renal cell carcinoma (RCC) subtypes. Clear cell RCCs (ccRCCs) account for approximately 70% of all RCCs and have relatively more aggressive behavior and worse prognosis compared with other subtypes. 6,7 Furthermore, ccRCC and papillary RCC (pRCC) respond differently to available targeted therapies in advanced disease. 8,9 These differ- ences in biologic behavior and response to targeted therapies under- score the need for accurately differentiating RCC subtypes. Higher ADCs in clear cell renal cell carcinomas (RCC) have been reported compared with papillary and chromophobe subtypes, 10 albeit with variable degree of overlap. Although most studies attribute the differences in ADC be- tween RCC subtypes to differences in the tissue cellularity and/or architecture, 3,4 it is important to realize that ADC measurements are influenced by tissue perfusion as well as the tissue cellularity. 11 The contribution of perfusion to the diffusion signal was elucidated by Le Bihan et al 12,13 in their pioneering work on intravoxel incoherent motion (IVIM). The blood flow in a randomly oriented microvascu- lature, referred to as pseudodiffusion, contributes to diffusion signal decay predominantly at low b values (G200 s/mm 2 ). Perfusion effects can be resolved from the true tissue diffusion by acquiring DWI with a sufficiently wide range of b values, followed by biexponential curve fit. Such analysis can resolve pseudodiffusivity (D p ) and tissue dif- fusivity (D t ) separately, along with their respective volume fractions f p and (1j f p ). 14Y23 Intravoxel incoherent motion provides a unique glimpse at tissue perfusion, without the use of exogenous contrast. Chandarana et al 24 demonstrated higher f p and lower D t in enhancing renal masses compared with benign nonenhancing lesions. Because RCC subtypes differ in degree of vascularity and cellularity/tumor architecture, dif- fusion MRI parameters f p /D p and D t , reflecting 2 distinct processes that contribute to ADC, may together provide more sensitive and specific characterization of renal lesions. Whereas f p was shown to be higher in gadolinium-enhancing lesions compared with nonenhancing lesions, 24 the relationship between f p and metrics of tumor perfusion from dynamic contrast- enhanced (DCE) MRI is not fully understood. Oncologic studies and clinical trials that use DCE MRI have sometimes expressed tumor perfusion using a semiquantitative parameter cumulative initial area under the curve (CIAUC). This parameter is a measure of the gado- linium concentration (mmol s j1 mL j1 ) obtained from the area under the gadolinium-enhancement signal intensity (SI) curve over the first 60 seconds (CIAUC 60 ) after intravenous injection of contrast. 25,26 The ORIGINAL ARTICLE 688 www.investigativeradiology.com Investigative Radiology & Volume 47, Number 12, December 2012 Received for publication April 29, 2012; and accepted for publication, after revision, July 4, 2012. From the *Department of Radiology, New York University Langone Medical Center, New York, NY; †Department of Radiology, University of Utah, Salt Lake City, UT; ‡Department of Radiology, Kobe City Medical Center General Hospital, Kobe, Japan; and Departments of §Urology and ||Pathology, New York Uni- versity Langone Medical Center, New York, NY. Conflicts of interest and sources of funding: This work partly supported by Ra- diologic Society of North America seed grant RSD0911 (2009Y2010). The authors report no conflicts of interest. Reprints: Hersh Chandarana, MD, New York University Langone Medical Center, Department of Radiology, 550 First Avenue, HCC 231, New York, NY 10016. E-mail: [email protected]. Copyright * 2012 by Lippincott Williams & Wilkins ISSN: 0020-9996/12/4712Y0688 Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Transcript of Diffusion-Weighted Intravoxel Incoherent Motion … Intravoxel Incoherent Motion Imaging of Renal...

Diffusion-Weighted Intravoxel Incoherent Motion Imagingof Renal Tumors With Histopathologic Correlation
Hersh Chandarana, MD,* Stella K. Kang, MD,* Samson Wong, MD,* Henry Rusinek, PhD,* Jeff L. Zhang, PhD,ÞShigeki Arizono, MD, PhD,þ William C. Huang, MD,§ Jonathan Melamed, MD,|| James S. Babb, PhD,*
Edgar F. Suan, BS,* Vivian S. Lee, MD, PhD,Þ and Eric E. Sigmund, PhD*
Purpose: The aim of this study was to use intravoxel incoherent motiondiffusion-weighted imaging to discriminate subtypes of renal neoplasms andto assess agreement between intravoxel incoherent motion (perfusion fraction,fp) and dynamic contrast-enhanced magnetic resonance imaging (MRI) metricsof tumor vascularity.Subjects and Methods: In this Health Insurance Portability and Account-ability ActYcompliant, institutional review boardYapproved prospective study,26 patients were imaged at 1.5-T MRI using dynamic contrast-enhancedMRI with high temporal resolution and diffusion-weighted imaging using8 b values (range, 0-800 s/mm2). Perfusion fraction ( fp), tissue diffusivity(Dt), and pseudodiffusivity (Dp) were calculated using biexponential fitting ofthe diffusion data. Apparent diffusion coefficient (ADC) was calculated withmonoexponential fit using 3 b values of 0, 400, and 800 s/mm2. Dynamiccontrast-enhanced data were processed with a semiquantitative method togenerate model-free parameter cumulative initial area under the curve ofgadolinium concentration at 60 seconds (CIAUC60). Perfusion fraction, Dt,Dp, ADC, and CIAUC60 were compared between different subtypes of renallesions. Perfusion fraction was correlated with CIAUC60.Results: We examined 14 clear cell, 4 papillary, 5 chromophobe, and 3 cysticrenal cell carcinomas (RCCs). Although fp had higher accuracy (area under thecurve, 0.74) for a diagnosis of clear cell RCC compared with Dt or ADC, thecombination of fp and Dt had the highest accuracy (area under the curve, 0.78).The combination of fp and Dt diagnosed papillary RCC and cystic RCC with100% accuracy, and clear cell RCC and chromophobe RCC, with 86.5%accuracy. There was significant strong correlation between fp and CIAUC60
(r = 0.82; P G 0.001).Conclusion: Intravoxel incoherent motion parameters fp and Dt can discrimi-nate renal tumor subtypes. Perfusion fraction demonstrates good correlationwith CIAUC60 and can assess degree of tumor vascularity without the use ofexogenous contrast agent.
KeyWords: renal tumors, renal cancer, diffusion-weighted imaging, intravoxelincoherent, motion (IVIM); MRI
(Invest Radiol 2012;47: 688Y696)
D iffusion-weighted magnetic resonance imaging (DWI) derivesimage contrast from differences in the mobility (Brownian mo-
tion) of water in tissues. Restriction of the random motion of water by
the local microenvironment can be assessed either qualitatively orquantitatively. The decay of signal intensity (SI) as a function of in-creasing diffusion-weighting factor (or b value) is commonly ap-proximated by a monoexponential function to quantitatively assessrestriction to the diffusion. The rate of decay is called the apparentdiffusion coefficient (ADC) and can be mapped on a voxel-by-voxelbasis as an ADC map.1
Diffusion-weighted magnetic resonance imaging (MRI) is in-creasingly being used in the evaluation of renal lesions. Studies haveshown lower ADC in malignant lesions compared to benign renallesions.2Y5 In addition, DWI has been used to examine renal cellcarcinoma (RCC) subtypes. Clear cell RCCs (ccRCCs) account forapproximately 70% of all RCCs and have relatively more aggressivebehavior and worse prognosis compared with other subtypes.6,7
Furthermore, ccRCC and papillary RCC (pRCC) respond differentlyto available targeted therapies in advanced disease.8,9 These differ-ences in biologic behavior and response to targeted therapies under-score the need for accurately differentiating RCC subtypes. HigherADCs in clear cell renal cell carcinomas (RCC) have been reportedcompared with papillary and chromophobe subtypes,10 albeit withvariable degree of overlap.
Although most studies attribute the differences in ADC be-tween RCC subtypes to differences in the tissue cellularity and/orarchitecture,3,4 it is important to realize that ADC measurements areinfluenced by tissue perfusion as well as the tissue cellularity.11 Thecontribution of perfusion to the diffusion signal was elucidated byLe Bihan et al12,13 in their pioneering work on intravoxel incoherentmotion (IVIM). The blood flow in a randomly oriented microvascu-lature, referred to as pseudodiffusion, contributes to diffusion signaldecay predominantly at low b values (G200 s/mm2). Perfusion effectscan be resolved from the true tissue diffusion by acquiring DWI witha sufficiently wide range of b values, followed by biexponential curvefit. Such analysis can resolve pseudodiffusivity (Dp) and tissue dif-fusivity (Dt) separately, along with their respective volume fractionsfp and (1j fp).14Y23
Intravoxel incoherent motion provides a unique glimpse attissue perfusion, without the use of exogenous contrast. Chandaranaet al24 demonstrated higher fp and lower Dt in enhancing renal massescompared with benign nonenhancing lesions. Because RCC subtypesdiffer in degree of vascularity and cellularity/tumor architecture, dif-fusionMRI parameters fp/Dp andDt, reflecting 2 distinct processes thatcontribute to ADC, may together provide more sensitive and specificcharacterization of renal lesions.
Whereas fp was shown to be higher in gadolinium-enhancinglesions compared with nonenhancing lesions,24 the relationshipbetween fp and metrics of tumor perfusion from dynamic contrast-enhanced (DCE) MRI is not fully understood. Oncologic studies andclinical trials that use DCE MRI have sometimes expressed tumorperfusion using a semiquantitative parameter cumulative initial areaunder the curve (CIAUC). This parameter is a measure of the gado-linium concentration (mmol sj1 mLj1) obtained from the area underthe gadolinium-enhancement signal intensity (SI) curve over the first60 seconds (CIAUC60) after intravenous injection of contrast.25,26 The
ORIGINAL ARTICLE
688 www.investigativeradiology.com Investigative Radiology & Volume 47, Number 12, December 2012
Received for publication April 29, 2012; and accepted for publication, after revision,July 4, 2012.
From the *Department of Radiology, NewYork University LangoneMedical Center,New York, NY; †Department of Radiology, University of Utah, Salt Lake City,UT; ‡Department of Radiology, Kobe City Medical Center General Hospital,Kobe, Japan; and Departments of §Urology and ||Pathology, New York Uni-versity Langone Medical Center, New York, NY.
Conflicts of interest and sources of funding: This work partly supported by Ra-diologic Society of North America seed grant RSD0911 (2009Y2010).
The authors report no conflicts of interest.Reprints: Hersh Chandarana, MD, New York University Langone Medical Center,
Department of Radiology, 550 First Avenue, HCC 231, New York, NY 10016.E-mail: [email protected].
Copyright * 2012 by Lippincott Williams & WilkinsISSN: 0020-9996/12/4712Y0688
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

CIAUC60 reflects the combined influence of blood volume, flow, andpermeability but is likely dominated by blood volume.
Given the promise of DWI in interrogating perfusion andvascular volume parameters with the advantage of not requiring ex-ogenous contrast material, our study had 2 goals:
1) to assess agreement between fp and the DCE MRI metric of tumorperfusion CIAUC60.
2) to use IVIM parameters to discriminate subtypes of renal neoplasm.
MATERIALS AND METHODS
Patient PopulationThis Health Insurance Portability and Accountability ActY
compliant, prospective, single-center study was performed afterobtaining approval from our institutional review board and informedpatient consent. Forty-one consecutive patients presenting for pre-operative imaging of renal lesions fromOctober 2009 to October 2011were recruited for this study. Two patients were excluded becausein one, no lesion was identified, and in the other, the lesion wassubcentimeter in size. Another four patients were excluded becausecomplete DCE and diffusion data were not available (because ofpatients’ inability to tolerate examination [n = 2] and of technical errors[n = 2]), and nine patients were excluded because these patients did notundergo surgery at our institution and no tumor histology was available.Twenty-six patients were included in the final cohort (mean age,57.7 years; range, 38Y75 years; 15 men with a mean age of 58.1 yearsand age range of 38Y72 years; 11 women with a mean age of 57.2 yearsand age rangeof 38Y75years). For this study, histopathologic slideswerere-reviewed by a board-certified pathologist with 19 years of experiencein genitourinary histopathology who rendered the diagnosis of RCCsubtype, using immunohistochemical stains when deemed necessary.
Magnetic Resonance ImagingMagnetic resonance imaging at 1.5 T (Magnetom Avanto,
maximumgradient strength 45 ofmT/m; SiemensMedical Solutions,Erlangen, Germany) was performed in all patients using torso phased-array coils. The routine renal protocol included the following breath-hold sequences: coronal and axial T2-weighted half-Fourier Acquisitionsingle-shot turbo spin-echo (HASTE), transverse T1-weighted gradientecho in-phase andopposed-phase, and transverse 3-dimensional (3D) T1-weighted fat-suppressed gradient echo (volume interpolated breath-holdexamination) precontrast and postcontrast acquisition in the cortico-medullary, nephrographic, and excretory phases of enhancement.The DWI and DCE acquisitions were performed before contrastadministration for volume interpolated breath-hold examinationacquisitions as detailed below.
Diffusion-Weighted ImagingTransverse respiratory-triggered twice-refocused spin echo,
bipolar gradient, single-shot echo planar DWI, with tridirectionaltrace-weighting diffusion gradients, was performed before contrastadministration.27 The following were used to acquire DWI: repetitiontime/echo time, 2700 to 4000/76 milliseconds; matrix, 192 � 144to 192; voxel size, 1.8 � 1.8 � 6 mm; 15 axial 6-mm slices with aninterslice gap of 0.6 mm; bandwidth, 1628 Hz/pix; parallel imagingfactor, 2; 8 b values (0, 50, 100, 150, 250, 400, 600, and 800 s/mm2)24;and 2 averages. Acquisition times ranged from 90 to 180 seconds,depending on the patient’s respiratory pattern.
Dynamic Contrast-Enhanced MRIDynamic contrast-enhanced MRI was performed with a 3D
volumetric T1-weighted gradient echo sequence using the view-sharingundersampling technique TWIST (time-resolved angiography withstochastic trajectories).28,29 Scanning startedwith a 5-second delay afterinitiation of intravenous contrast injection (but before the contrastreaching the abdominal structures) and continued for 4minutes. Using anautomated injector (Spectris; Medrad, Indianola, PA), 4 mL of gado-pentetate dimeglumine (Magnevist; Berlex Laboratories,Wayne, NJ) wasinjected intravenously, followed by 20 mL saline flush, both at a rate of2 mL/s. Image parameters were as follows: repetition time/echo time,2.33/0.77 milliseconds; flip angle, 12 degrees; slice thickness, 2.5 mm;matrix, 256� 180; voxel size, 2.4� 1.7� 2.5mm; bandwidth, 650Hz/pix; parallel imaging factor, 3; and 40 coronal slices acquired with eachmeasure. Total acquisition time for the initial full k-space acquisitionwas 5 seconds. TWISTacquisition updates 20% of central k-space area(A) and 20% of outer k-space lines (B) at a temporal resolution of1.2 seconds (28) for each repeat measurement. The initial 21 mea-sures were acquired at 1.2 seconds temporal resolution in a longbreath-hold (29 seconds), followed by 3 to 5 measures performed(acquisition time 8Y10 seconds) in a breath-hold every 30 seconds for4 minutes.
MRI Analysis
Diffusion-Weighted ImagingDiffusion-weighted imaging data in a DICOM format were trans-
ferred to a standard personal computer running an in-houseYdevelopedsoftware package (FireVoxel, http://files.nyu.edu/hr18/public).18,23,30
Two independent observers (with 5 years and 1 year of abdominalMRI experience) blinded to patient’s clinical information and tumorhistology segmented the entire lesion on the unweighted (b = 0) ac-quisition. This 3D region of interest (ROI) was propagated to the otherb-value images to derive integrated SI values for all the b values.
A biexponential model was used to describe the behavior of thediffusion-weighted signal S(b)14:
SðbÞ ¼ S0�fpexpð�bDpÞ þ ð1� fpÞexpð�bDtÞ
�ð1:1Þ
This model assumes (1) a vascular compartment, occupyinga fraction fp of the tissue volume and showing a pseudodiffusion
TABLE 1. Patient Demographics and Lesion Characteristics inRenal Cell Cancer Stratified by Histopathologic Subtype
ccRCC chRCC pRCC cyRCC
Number of lesions 14 5 4 3
Average size, cm 4.1 3.6 2.8 4.4
Range size, cm 1.5Y6.2 2.9Y6.3 2.0Y5.0 4.1Y5.1
Patient age, y, mean(range)
58 (38Y75) 62 (41Y73) 53 (42Y64) 57 (49Y69)
Sex distribution, F/M 6/8 2/3 0/4 3/0
ccRCC indicates clear cell; chRCC, chromophobe; cyRCC, cystic; pRCC,papillary.
TABLE 2. Diffusion and DCE Parameters in Renal Lesions Stratifiedby Histologic Subtype
ccRCC chRCC pRCC cyRCC
ADC, �10j3 mm2/s 2.2 T 0.4 1.9 T 0.3 1.0 T 0.2 2.6 T 0.1
Dt, �10j3 mm2/s 1.8 T 0.6 1.3 T 0.2 0.9 T 0.1 2.5 T 0.1
Dp, �10j3 mm2/s 19 T 13.5 14.7 T 9.8 18.8 T 12.0 20.7 T 14.2
fp 0.25 T 0.05 0.27 T 0.06 0.11 T 0.02 0.09 T 0.02
CIAUC60,mmol sj1 mLj1
9.94 T 2.55 12.19 T 3.02 2.56 T 0.80 1.86 T 0.98
Investigative Radiology & Volume 47, Number 12, December 2012 IVIM DWI in Evaluation of Renal Tumors
* 2012 Lippincott Williams & Wilkins www.investigativeradiology.com 689
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

coefficient Dp, and (2) a tissue compartment, occupying theremaining volume fraction (1j fp) and showing Dt. Both compart-ments are assumed to demonstrate exponential signal decay withdiffusion-weighting factor b. Although several non-Gaussian diffu-sion models apply to different tissue types and measurementregimes,31Y33 this bicompartmental model is deemed appropriate forcancerous tissue given the distinct prevalence and importance oftumor cellularity and vascularity.
An unconstrained fit of this biexponential model (Eq. 1.1) wasperformed to the integrated lesion SI decays to extract the 3 para-meters fp, Dp, and Dt. Apparent diffusion coefficient was calculatedwith monoexponential fit of SI at b = 0, 400, and 800 s/mm2 as inprevious studies.5,34
SðbÞ ¼ S0expð�b� ADCÞ ð1:2ÞParametric maps were also generated of each of these parameters
from voxel-wise fits to Eq. 1.1 (for fp, Dp, and Dt, using all b valueswhose signals exceeded background noise) or Eq. 1.2 (for ADC, usingb = 0, 400, and 800 s/mm2 and the same noise threshold) of all voxelsin the tumor ROI. These maps were qualitatively evaluated but werenot considered in the statistical analysis.
Dynamic Contrast-Enhanced MRITwo observers (with 4 and 2 years of abdominal MRI experi-
ence) independently analyzed DCEMRI data. Observers were blindedto patient’s clinical information, diffusion data, and tumor histology.The images were transferred to a personal computer runningFireVoxel software.
Targeted image coregistration was performed using normalizedmutual information as the voxel similarity measure.30 The entire tumorwas segmented on a postcontrast acquisition that best demonstrated thelesion, and this ROI was copied to the entire time series. Integrated lesionSI versus time course of the renal tumor was recorded and converted to
FIGURE 1. ADC (�10j3mm2/s) parametricmaps in representative cases of (A) chRCC, (B) ccRCC, (C) pRCC, and (D) cyRCC. PapillaryRCC had the lowest ADC, followed by chRCC and ccRCC, with cyRCC having the highest ADC. At the group level, there was nosignificant difference between chRCC and ccRCC.
TABLE 3. P values for Group comparison of DWI ParametersBetween RCC Subtypes
ADC Dt
fp Dp Chromophobe Papillary Cystic
Clear cell 0.08 0.006 G0.001 G0.001 G0.001 G0.001
0.799 0.728 G0.001 1.0 G0.001 0.993
Chromophobe G0.001 G0.001 G0.001 G0.001
G0.001 0.870 G0.001 0.806
Papillary G0.001 G0.001
0.094 0.993
Significant differences are highlighted in boldface. Key in upper left-handcorner indicates P values for each DWI parameter.
Chandarana et al Investigative Radiology & Volume 47, Number 12, December 2012
690 www.investigativeradiology.com * 2012 Lippincott Williams & Wilkins
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

gadolinium concentration using a phantom calibration method.35 Thearea under the concentration curve over the first minute, CIAUC60, wascomputed using the trapezoid approximation.
Statistical AnalysisTo assess interobserver agreement in DWI parameters, con-
cordance correlation coefficient (RC) and intraclass correlation co-efficient (ICC) were calculated for fp, Dt, Dp, ADC, and CIAUC60
measures provided by both observers.Renal lesions were compared in terms of each DWI (fp, Dt, Dp,
ADC) and DCE (CIAUC60 ) parameter using mixed-model analysisof variance. A separate mixed-model analysis was conducted for eachmeasure using that measure as the dependent variable. Each mixedmodel included lesion type and reader as fixed classification factors.The covariance structure was modeled by assuming observationsto be correlated only when acquired from the same patient and by
allowing the error variance to differ across lesion types. The Tukeyhonestly significant difference test was used to correct for multiplecomparisons when comparing lesion types. Logistic regression forcorrelated data was used to assess the ability of the imaging measures,alone and in combination, to discriminate ccRCC from other types ofcancers. To identify a threshold value that maximized the diagnosticaccuracy of detecting ccRCC, ROC analyses were used. Pearson rankcorrelations were used to characterize the association of fp withCIAUC60. Statistical significance was defined as P G 0.05. SAS 9.3(SAS Institute, Cary, NC) was used for all computations.
RESULTS
Patient and Lesion CharacteristicsA total of 26 lesions in 26 patientswere included in the final cohort
and were assessed with DWI and gadolinium-enhanced DCE MRI. All
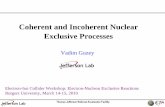
FIGURE 2. Biexponential fitting of the multi-b diffusionYweighted integrated lesion SI in representative cases demonstrates highperfusion fraction (fp) in vascular tumors (A) chRCC and (B) ccRCC and low fp in hypovascular (C) pRCC) and (D) cyRCC.
Investigative Radiology & Volume 47, Number 12, December 2012 IVIM DWI in Evaluation of Renal Tumors
* 2012 Lippincott Williams & Wilkins www.investigativeradiology.com 691
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

patients underwent surgery at our institution and, on histopathology, werefound to have diagnosis of clear cell (ccRCC, n = 4), papillary (pRCC,n = 4), chromophobe (chRCC, n = 5), and cystic (cyRCC, n = 3) subtypeof RCC (Table 1).
Interobserver AgreementThe RC for the DWI parameters ranged from 0.95 to 0.99,
and ICC ranged from 0.93 to 0.99. These results suggest excellentagreement between the 2 readers for all DWI measures. Similarly,both RC and ICC for CIAUC60 were 0.98, suggesting excellentagreement between the 2 readers.
DWI Results: Individual ParametersThe ADC, Dt, Dp, and fp of all lesions categorized by subtype
are shown in Tables 2 and 3, along with the results of group com-
parisons of each pair of lesion types for each parameter. Calculatedwith a monoexponential fit of b = 0, 400, and 800 s/mm2, ADC washighest in cyRCC 2.60 T 0.10 � 10j3 mm2/s) and lowest in pRCC(1.0 T 0.20 � 10j3 mm2/s). The clear cell and chromophobe RCCsubtypes hadADC values between that of cyRCC and pRCC (exampleparametric maps in Fig. 1). Although ADC was higher in clear cellcompared with chromophobe (2.20 T 0.40 � 10j3 mm2/s vs 1.90 T0.30 � 10j3 mm2/s), this difference did not reach statistical signifi-cance (P = 0.08). Using an ADC cutoff of greater than 1.85 � 10j3
mm2/s, ccRCC could be diagnosed with a sensitivity of 92.9%,specificity of 58.3%, and accuracy of 76.9%. The low specificity wasdue to the overlap in ADC values of clear cell with that of the cysticand chromophobe subtypes.
Similar trends were noted with Dt calculated from biexpo-nential fit (example fits in Fig. 2), which was highest in cyRCC (2.50 T0.10� 10j3 mm2/s) and lowest in pRCC (0.90 T 0.10� 10j3 mm2/s).
FIGURE 3. Dt (�10j3 mm2/s) parametric maps in representative cases of (A) chRCC (B), ccRCC (C), pRCC, and (D) cyRCC. At thegroup level, pRCC had the lowest Dt and cyRCC had the highest Dt. Chromophobe RCC had lower Dt compared with ccRCC, whichwas statistically significant.
TABLE 4. ROC Analysis for Multiple Parameters in Diagnosis of ccRCC
Measure Criterion AUC Sensitivity Specificity Accuracy
ADC, �10j3 mm2/s 90.00185 0.67 92.9% (26/28) 58.3% (14/24) 76.9% (40/52) (CI, 57.3Y89.2)
Dt, �10j3 mm2/s 90.00144 0.68 85.7% (24/28) 62.5% (15/24) 75.0% (39/52) (CI, 57.1Y87.1)
fp 90.16 0.74 100% (28/28) 62.5% (15/24) 82.7% (43/52) (CI, 65.6Y92.3)
CIAUC60, mmol sj1 mLj1 93.73 0.65 100% (28/28) 58.3% (14/24) 80.8% (42/52) (CI, 67.8Y90.4)
CI indicates confidence interval.
Chandarana et al Investigative Radiology & Volume 47, Number 12, December 2012
692 www.investigativeradiology.com * 2012 Lippincott Williams & Wilkins
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

The Dt of the clear cell and chromophobe subtypes were betweenthose of the pRCC and cyRCC (example parametric maps in Fig. 3).However, unlike ADC, Dt of the clear cell was significantly highercompared with the chromophobe subtype (1.80 T 0.60� 10j3 mm2/svs 1.30 T 0.20 � 10j3 mm2/s; P = 0.006). Dt demonstrated similar ac-curacy to that of ADC (Table 4) for a diagnosis of ccRCC (area underthe curve [AUC], 0.68 vs 0.67); withDt greater than 1.44� 10j3 mm2/s,ccRCC subtype could be diagnosed with a sensitivity of 85.7%, speci-ficity of 62.5%, and accuracy of 75%. Lower specificity was due tooverlap between ccRCC and that of chRCC and cyRCC.
Perfusion fraction fp obtained with biexponential fit (Fig. 2) hadthe highest accuracy for the diagnosis of ccRCC (AUC 0.74). Usingan fp cutoff grater than 0.16, the clear cell subtype could be diagnosedwith a sensitivity of 100%, specificity of 62.5%, and accuracy of82.7%. Representative fp parametric maps are shown in Figure 4.
The pseudodiffusion (Dp) rate was not significantly differentbetween different subtypes and had the lowest accuracy for detectionof ccRCC (AUC 0.53).
Multivariate Prediction ModelMultistep logistic regression identified fp and Dt as the opti-
mal 2 factors for the detection of ccRCC. The parameter fp wasa significant predictor of the clear cell subtype after adjusting for Dt
(P = 0.0016). Using the 2-factor model containing fp and Dt to dis-
criminate clear cell from all other subtypes (combined) achieved anAUC of 0.78 with a sensitivity of 92.9% (26/28) and a specificityof 79.2% (19/24).
Based on IVIM analysis, cyRCC and pRCC are hypovascular,with fp less than 0.16, unlike the other 2 subtypes. These 2 subtypescan be distinguished from each other based on Dt. Cystic RCC couldbe diagnosed with 100% accuracy using cutoffs of fp less than 0.16and Dt greater than 1.5� 10j3 mm2/s, and pRCC could be diagnosedwith 100% accuracy with cutoffs of fp less than 0.16 and Dt less than1.5 � 10j3 mm2/s. All ccRCC and chRCC had fp greater than 0.16.Using fp greater than 0.16 andDt greater than 1.5� 10j3 mm2/s, ccRCCcould be diagnosed with accuracy of 86.5%, and similarly, using cutoffsof fp greater than 0.16 and Dt less than 1.5 � 10j3 mm2/s, the chro-mophobe subtype could be diagnosed with 86.5% accuracy (Fig. 5).
DCE MeasurementThe more vascularized tumor types (ccRCC and chRCC)
demonstrate higher CIAUC60 compared with hypovascular pRCCand cyRCC (Tables 2 and 3). The CIAUC60 was higher in thechromophobe compared with the clear cell subtype (12.2 vs9.93 mmol sj1 mLj1), but this difference did not achieve statisti-cal significance (P = 0.165). Using a CIAUC60 cutoff of greaterthan 3.73 mmol sj1 mLj1, ccRCC could be diagnosed with asensitivity of 100%, specificity of 59.3%, and accuracy of 80.8%.
FIGURE 4. fp parametric maps in representative cases of (A) chRCC, (B) ccRCC, (C) pRCC, and (D) cyRCC. At the group level, ccRCCand chRCC are hypervascular, with fp greater than 0.16, whereas cyRCC and pRCC were hypovascular, with fp less than 0.16. Therewas no significant difference in fp between ccRCC and chRCC at the group level.
Investigative Radiology & Volume 47, Number 12, December 2012 IVIM DWI in Evaluation of Renal Tumors
* 2012 Lippincott Williams & Wilkins www.investigativeradiology.com 693
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

There was substantial significant (P G 0.0001) positive corre-lation between fp and CIAUC60 (r = 0.82) (Fig. 6).
DISCUSSIONRenal masses are increasingly discovered incidentally as use
of medical imaging rises.36,37 The incidental discovery of a renal neo-plasm can lead to a management dilemma because renal tumors havevariable natural history, growth rate, histopathologic features, and clinicalbehavior depending on their subtype.38,39 Differences in prognosis andevolving treatment paradigms based on tumor aggressiveness em-phasize the need for noninvasive tools to accurately differentiatebetween subtypes of RCC.
Studies have shown that DCE computed tomography and MRIcan noninvasively differentiate ccRCC from pRCC on the basis ofdegree of enhancement.40Y42 However, ccRCC and chRCC cannotalways be differentiated because they show overlap in the enhance-ment pattern. Moreover, most patients with renal tumors are elderly
individuals and may have renal dysfunction. For these patients, tech-niques such as DWI, which do not require exogenous contrast,are attractive alternatives. In this study, there was a high correlationbetween perfusion fraction fp and the DCE metric of tumor perfusionCIAUC60. Both fp and CIAUC60 were significantly higher in the clearcell and chromophobe subtypes, compared with the hypovascularpRCC and cyRCC. Furthermore, neither fp nor CIAUC60 showed sig-nificant difference between the clear cell and chromophobe subtypes.Thus, the information provided by fp was analogous to that obtainedfrom the DCE parameter CIAUC60.
Low ADC values have been shown to differentiate pRCC fromnon-pRCC subtypes in patients undergoing DWI at 1.5 Twith b valuesof 0, 400, and 800 s/mm2.5 In a study byWang et al,10 when DWI wasperformed at 3 Twith b values of 0 and 500 s/mm2, ccRCCs showed asignificantly higher mean ADC (1.849 � 10j3 mm2/s) than didthe papillary (1.087 � 10j3 mm2/sec) and chromophobe (1.307 �10j3 mm2/s) RCCs; however, the difference between pRCC andchRCC was not statistically significant. When ADC was calculated with
FIGURE 5. A, fp-Dt scatter plot of renal lesions. B, Diagnostic flowchart demonstrates the role of the combination of IVIM parametersfp and Dt in discriminating renal lesions by histologic subtype.
Chandarana et al Investigative Radiology & Volume 47, Number 12, December 2012
694 www.investigativeradiology.com * 2012 Lippincott Williams & Wilkins
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

b values of 0 and 800 s/mm2, the difference in ADC value betweenthe 3 subtypes was statistically significant.10 The higher accuracy ofADC calculated with a b value of 800 s/mm2 is understandable becauseit more closely proximates the true diffusion coefficient (Dt) calculatedin our study, which also significantly differentiated the RCC subtypes.However, in the study by Wang et al,10 contrast-enhanced imaging wasused to facilitate ROI placement to exclude area of necrosis or cysticdegeneration, and only a small portion of the tumor was sampled withan average ROI of 100 mm2. We, on the other hand, segmented theentire lesion on the b0 image, which circumvents the limitations ofsampling errors inherent to placing small ROIs or sampling bias fromrelying on contrast enhancement for ROI placement.
Selected recent studies have also recognized the limitations ofthe single ADC parameter in describing renal masses. Doganay et al43
and Erbay et al44 collected diffusion data at multiple b values inpatients with varied renal mass pathologies and demonstrated thatdifferentiation improves using ADCs at higher b values but did notexplicitly quantify IVIM parameters. Rheinheimer et al45 used theIVIM technique in a series of renal masses and found that the per-fusion fraction provided significant added value, particularly in thedifferentiation of clear cell from nonYclear cell neoplasm. However,in this study, authors did not evaluate the combination of fp and Dt indiscriminating RCC subtypes.
Substantial evidence is thus accruing in the literature that theoptimum application of DWI for renal tumor assessment should re-solve and quantify different contributions to ADC. The present studyusing the IVIM method was carried out from this perspective. Intra-voxel incoherent motion can simultaneously assess tumor vascularityand cellularity/architecture. The ability to explore both these metricsin our study showed higher accuracy when compared with ADC indiscriminating RCC subtypes.
Assessment of treatment response of metastatic RCC to anti-angiogenic drug therapy with DCE MRI has been performed in pre-clinical studies and in clinical trials.46,47 This powerful tool is not yetroutinely used in clinical practice, in part because it is technicallydifficult to perform and there is some controversy regarding appro-
priate pharmacokinetic models for assessment of RCC.48 We haveshown that the IVIM parameter of tumor vascularity fp is significantlycorrelated with the DCEmetric CIAUC60. This finding is most likely aresult of the dominant contribution of blood volume to the lattermetric. Given the vascular sensitivity of fp, an investigation of itsability to assess treatment response to antiangiogenic drug therapywithout the need for exogenous contrast is highly warranted. Intra-voxel incoherent motion DWI is relatively easy to perform and canbe added to any existing renal MRI protocol. Imaging vendors arepursuing online processing of IVIM data at the scanner to generatefp and Dt parametric maps, further facilitating the wider adoption ofIVIM in clinical practice. Parametric maps were qualitatively evalu-ated in this study but were not used for quantitative evaluation. Het-erogeneity at the edges of the fp andDt parametric maps (Figs. 3 and 4)may be related to partial volume averaging.
Several studies have shown that noncontrast MRImethods suchas arterial spin labeling (ASL) can also be used to assess treatmentresponse to antiangiogenic therapy in metastatic renal cancer.49Y51
Quantitation of perfusion with ASL is slightly more technically chal-lenging compared with calculation of perfusion fraction fp with IVIMDWI. However, future studies using a joint ASL-DWI encodingscheme, as previously reported in cerebral perfusion studies,52,53
may further illuminate the RCCmicroenvironment by probing bothintravascular and extravasational dynamics.
The limitations of our study include a relatively small numberof subjects. Although in this feasibility studywewere able to use IVIMparameters in discriminatingRCCsubtypeswith somedegree of overlapbetween chRCC and ccRCC, larger studies and more detailed lesionanalysis are required to assess diagnostic performance in accurately dis-criminating RCC subtypes. We compared fp with a model-free semi-quantitative parameter CIAUC60 instead of using a pharmacokineticmodel such as Toft’s model because its parameters’ interpretation mayvary with RCC subtype.48 For example, the commonly used transferconstant Ktrans may reflect vessel permeability in hypervascular tumorssuch as clear cell and chromophobe subtypes but may reflect bloodflow in hypovascular tumors such as pRCC and cyRCC. Finally, whereasthe IVIM sensitivities in renal lesions are expected to be general, thespecific mean values and discrimination thresholds in the current study(Dt = 1.5 � 10j3 mm2/s, fp = 0.16) may be unique to our particularprotocol. Estimations of IVIM parameters are known to dependsomewhat upon b-value selection,54Y56 relaxation weighting,57 andanalysis algorithm.58,59
Thus, a consistent protocol in any comparative study of lesionsubtypes is vital to achieving meaningful discriminatory power withIVIM biomarkers.
In conclusion, in this pilot study, we were able to demonstratethe feasibility of performing IVIM DWI and show the use of fp and Dt
in the assessment of renal tumor subtype. A combination of IVIM pa-rameters fp and Dt can discriminate renal tumor subtypes with accura-cy higher than that of monoexponential ADC. The parameter fpis correlated with the DCE metric of tumor vascularity CIAUC60
and can assess the degree of tumor vascularity without the use ofexogenous contrast agent. This study also suggests the potential ofIVIM for simultaneous assessment of multiple tumor microenvi-ronment properties.
REFERENCES1. Taouli B, Koh DM. Diffusion-weighted MR imaging of the liver. Radiology.
2010;254:47Y66.2. Zhang J, TehraniYM,WangL, et al. Renalmasses: characterizationwith diffusion-
weighted MR imagingVa preliminary experience. Radiology. 2008;247:458Y464.
3. Cova M, Squillaci E, Stacul F, et al. Diffusion-weighted MRI in the evaluationof renal lesions: preliminary results. Br J Radiol. 2004;77:851Y857.
4. Squillaci E, Manenti G, Di Stefano F, et al. Diffusion-weighted MR imagingin the evaluation of renal tumours. J Exp Clin Cancer Res. 2004;23:39Y45.
FIGURE 6. Correlation plot of IVIM perfusion parameter fp andDCEparameter CIAUC60 (mmol sj1mLj1) in renal lesions. Therewas a substantial significant (P G 0.0001) positive correlationbetween fp and CIAUC60 (r = 0.82).
Investigative Radiology & Volume 47, Number 12, December 2012 IVIM DWI in Evaluation of Renal Tumors
* 2012 Lippincott Williams & Wilkins www.investigativeradiology.com 695
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

5. Taouli B, Thakur RK, Mannelli L, et al. Renal lesions: characterization withdiffusion-weighted imaging versus contrast-enhanced MR imaging. Radiology.2009;251:398Y407.
6. Leibovich BC, Lohse CM, Crispen PL, et al. Histological subtype is an inde-pendent predictor of outcome for patients with renal cell carcinoma. J Urol.183:1309Y1315.
7. Teloken PE, Thompson RH, Tickoo SK, et al. Prognostic impact of histologicalsubtype on surgically treated localized renal cell carcinoma. J Urol. 2009;182:2132Y2136.
8. Escudier B, Eisen T, Stadler WM, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007;356:125Y134.
9. Chowdhury S, Choueiri TK. Recent advances in the systemic treatment ofmetastatic papillary renal cancer. Expert Rev Anticancer Ther. 2009;9:373Y379.
10. Wang H, Cheng L, Zhang X, et al. Renal cell carcinoma: diffusion-weightedMRimaging for subtype differentiation at 3.0 T. Radiology. 2010;257:135Y143.
11. Zhang L, Sigmund EE, Chandarana H, et al. Variability of renal apparent dif-fusion coefficient values: limitations of the mono-exponential model for dif-fusion quantification. Radiology. 2010;254:783Y792.
12. Le Bihan D, Breton E, Lallemand D, et al. Separation of diffusion and perfusionin intravoxel incoherent motion MR imaging. Radiology. 1988;168:497Y505.
13. Le Bihan D, Breton E, Lallemand D, et al. MR imaging of intravoxel incoherentmotions: application to diffusion and perfusion in neurologic disorders. Radi-ology. 1986;161:401Y407.
14. Luciani A, Vignaud A, Cavet M, et al. Liver cirrhosis: intravoxel incoherentmotion MR imagingVpilot study. Radiology. 2008;249:891Y899.
15. Callot V, Bennett E, DeckingUK, et al. In vivo study of microcirculation in caninemyocardium using the IVIM method. Magn Reson Med. 2003;50:531Y540.
16. Yao L, Sinha U. Imaging the microcirculatory proton fraction of muscle withdiffusion-weighted echo-planar imaging. Acad Radiol. 2000;7:27Y32.
17. Wirestam R, Borg M, Brockstedt S, et al. Perfusion-related parameters in intra-voxel incoherent motion MR imaging compared with CBV and CBF measuredby dynamic susceptibility-contrastMR technique.ActaRadiol. 2001;42:123Y128.
18. Patel J, Sigmund EE, Rusinek H, et al. Diagnosis of cirrhosis with intravoxelincoherent motion diffusion MRI and dynamic contrast-enhanced MRI aloneand in combination: preliminary experience. J Magn Reson Imaging. 2010;31:589Y600.
19. Klauss M, Lemke A, Grunberg K, et al. Intravoxel incoherent motion MRI forthe differentiation between mass forming chronic pancreatitis and pancreaticcarcinoma. Invest Radiol. 2011;46:57Y63.
20. Sigmund EE, Cho GY, Kim S, et al. Intravoxel incoherent motion imaging oftumor microenvironment in locally advanced breast cancer. Magn Reson Med.2011;65:1437Y1447.
21. Lemke A, Laun FB, Klauss M, et al. Differentiation of pancreas carcinomafrom healthy pancreatic tissue using multiple b-values comparison of apparentdiffusion coefficient and intravoxel incoherent motion derived parameters.Invest Radiol. 2009;44:769Y775.
22. SumiM, Van CauterenM, Sumi T, et al. Salivary gland tumors: use of intravoxelincoherent motion MR imaging for assessment of diffusion and perfusion forthe differentiation of benign from malignant tumors. Radiology. 2012;263:770Y777.
23. Sigmund EE, Vivier PH, Sui D, et al. Intravoxel incoherent motion anddiffusion-tensor imaging in renal tissue under hydration and furosemide flowchallenges. Radiology. 2012;263:758Y769.
24. Chandarana H, Lee VS, Hecht E, et al. Comparison of biexponential andmonoexponential model of diffusion weighted imaging in evaluation of renallesions: preliminary experience. Invest Radiol. 2011;46:285Y291.
25. Evelhoch JL, LoRusso PM, He Z, et al. Magnetic resonance imaging mea-surements of the response of murine and human tumors to the vascular-targetingagent ZD6126. Clin Cancer Res. 2004;10:3650Y3657.
26. Liu G, Rugo HS, Wilding G, et al. Dynamic contrast-enhanced magnetic res-onance imaging as a pharmacodynamic measure of response after acute dosingof AG-013736, an oral angiogenesis inhibitor, in patients with advanced solidtumors: results from a phase I study. J Clin Oncol. 2005;23:5464Y5473.
27. Reese TG, Heid O, Weisskoff RM, et al. Reduction of eddy-currentYinduceddistortion in diffusion MRI using a twice-refocused spin echo. Magn ResonMed. 2003;49:177Y182.
28. Song T, Laine AF, Chen Q, et al. Optimal k-space sampling for dynamic contrast-enhancedMRIwith an application toMR renography.MagnResonMed. 2009;61:1242Y1248.
29. Herrmann KH, Baltzer PA, Dietzel M, et al. Resolving arterial phase andtemporal enhancement characteristics in DCE MRM at high spatial resolutionwith TWIST acquisition. J Magn Reson Imaging. 2011;34:973Y982.
30. Mikheev A, Lee VS, Rusinek H. Targeted coregistration of abdominal DCEMRI. In Proceedings of the 19th Scientific Meeting ISMRM; May 7Y13, 2011;Montreal, Canada.
31. Wittsack HJ, Lanzman RS, Mathys C, et al. Statistical evaluation of diffusion-weighted imaging of the human kidney. Magn Reson Med. 2010;64:616Y622.
32. De Santis S, Gabrielli A, Bozzali M, et al. Anisotropic anomalous diffusionassessed in the human brain by scalar invariant indices. Magn Reson Med.2011;65:1043Y1052.
33. Jensen JH, Helpern JA. MRI quantification of non-Gaussian water diffusionby kurtosis analysis. NMR Biomed. 2010;23:698Y710.
34. Kim S, Jain M, Harris AB, et al. T1 hyperintense renal lesions: characterizationwith diffusion-weighted MR imaging versus contrast-enhanced MR imaging.Radiology. 2009;251:796Y807.
35. Bokacheva L, Rusinek H, Chen Q, et al. Quantitative determination of Gd-DTPA concentration in T1-weightedMR renography studies.Magn Reson Med.2007;57:1012Y1018.
36. Hock LM, Lynch J, Balaji KC. Increasing incidence of all stages of kidneycancer in the last 2 decades in the United States: an analysis of surveillance,epidemiology and end results program data. J Urol. 2002;167:57Y60.
37. ChowWH, Devesa SS, Warren JL, et al. Rising incidence of renal cell cancer inthe United States. JAMA. 1999;281:1628Y1631.
38. Lam JS, Shvarts O, Leppert JT, et al Renal cell carcinoma 2005: new frontiersin staging, prognostication and targeted molecular therapy. J Urol. 2005;173:1853Y1862.
39. Cheville JC, Lohse CM, Zincke H, et al. Comparisons of outcome and prog-nostic features among histologic subtypes of renal cell carcinoma. Am J SurgPathol. 2003;27:612Y624.
40. Sun MR, Ngo L, Genega EM, et al. Renal cell carcinoma: dynamic contrast-enhanced MR imaging for differentiation of tumor subtypesVcorrelation withpathologic findings. Radiology. 2009;250:793Y802.
41. Pedrosa I, Sun MR, Spencer M, et al. MR imaging of renal masses: correlationwith findings at surgery and pathologic analysis.Radiographics. 2008;28:985Y1003.
42. Herts BR, Coll DM, Novick AC, et al. Enhancement characteristics of papillaryrenal neoplasms revealed on triphasic helical CT of the kidneys. AJR Am JRoentgenol. 2002;178:367Y372.
43. Doganay S, Kocakoc E, Cicekci M, et al. Ability and utility of diffusion-weighted MRI with different b values in the evaluation of benign and malignantrenal lesions. Clin Radiol. 2011;66:420Y425.
44. Erbay G, Koc Z, Karadeli E, et al. Evaluation of malignant and benign renallesions using diffusion-weighted MRI with multiple b values. Acta Radiol.2012. doi:10.1258/ar.2011.110601.
45. Rheinheimer S, Stieltjes B, Schneider F, et al. Investigation of renal lesionsby diffusion-weighted magnetic resonance imaging applying intravoxel inco-herent motion-derived parametersVinitial experience. Eur J Radiol. 2012;81:310Y316.
46. Flaherty KT, Rosen MA, Heitjan DF, et al. Pilot study of DCE-MRI to predictprogression-free survival with sorafenib therapy in renal cell carcinoma.Cancer Biol Ther. 2008;7:496Y501.
47. Hillman GG, Singh-Gupta V, Zhang H, et al. Dynamic contrast-enhancedmagnetic resonance imaging of vascular changes induced by sunitinib in pap-illary renal cell carcinoma xenograft tumors. Neoplasia. 2009;11:910Y920.
48. Sourbron SP, Buckley DL. On the scope and interpretation of the Tofts modelsfor DCE-MRI. Magn Reson Med. 2011;66:735Y745.
49. De Bazelaire C, Rofsky NM, Duhamel G, et al. Arterial spin labeling bloodflow magnetic resonance imaging for characterization of metastatic renal cellcarcinoma. Acad Radiol. 2005;12:347Y357.
50. de Bazelaire C, Alsop DC, George D, et al. Magnetic resonance imaging-measured blood flow change after antiangiogenic therapy with PTK787/ZK222584 correlates with clinical outcome in metastatic renal carcinoma.Clin Cancer Res. 2008;14:5548Y5554.
51. Schor-Bardach R, Alsop DC, Pedrosa I, et al. Does arterial spin-labelingMR imagingYmeasured tumor perfusion correlate with renal cell cancer re-sponse to antiangiogenic therapy in a mouse model? Radiology. 2009;251:731Y742.
52. Kim T, Kim SG. Quantification of cerebral arterial blood volume usingarterial spin labeling with intravoxel incoherent motion-sensitive gradients.Magn Reson Med. 2006;55:1047Y1057.
53. Wang JJ, Fernandez-Seara MA, Wang SM, et al. When perfusion meets dif-fusion: in vivo measurement of water permeability in human brain. J CerebBlood Flow Met. 2007;27:839Y849.
54. Zhang JL, Sigmund EE, Rusinek H, et al. Optimization of b-value sampling fordiffusion-weighted imaging of the kidney. Magn Reson Med. 2012;67:89Y97.
55. Lemke A, Stieltjes B, Schad LR, et al. Toward an optimal distribution of b valuesfor intravoxel incoherent motion imaging. Magn Reson Imaging. 2011;29:766Y776.
56. Pang Y, Turkbey B, Bernardo M, et al. Intravoxel incoherent motion MR im-aging for prostate cancer: an evaluation of perfusion fraction and diffusioncoefficient derived from different b-value combinations [published online aheadof print]. Magn Reson Med. 2012.
57. Lemke A, Laun FB, Simon D, et al. An in vivo verification of the intravoxelincoherent motion effect in diffusion-weighted imaging of the abdomen. MagnReson Med. 2010;64:1580Y1585.
58. Mazaheri Y, Vargas HA, Akin O, et al. Reducing the influence of b-valueselection on diffusion-weighted imaging of the prostate: evaluation of arevised monoexponential model within a clinical setting. J Magn ResonImaging. 2012;35:660Y668.
59. Neil JJ, Bretthorst GL. On the use of Bayesian probability theory for analysisof exponential decay data: an example taken from intravoxel incoherent motionexperiments. Magn Reson Med. 1993;29:642Y647.
Chandarana et al Investigative Radiology & Volume 47, Number 12, December 2012
696 www.investigativeradiology.com * 2012 Lippincott Williams & Wilkins
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.