DIFFUSION TENSOR IMAGING INVESTIGATIONS OF MILD … · Diffusion Tensor Imaging Investigations of...
71
DIFFUSION TENSOR IMAGING INVESTIGATIONS OF MILD BRAIN DAMAGE by Yuko Koshimori A thesis submitted in conformity with the requirements for the degree of Master‟s of Science Graduate Department of Rehabilitation Science University of Toronto © Copyright by Yuko Koshimori 2011
Transcript of DIFFUSION TENSOR IMAGING INVESTIGATIONS OF MILD … · Diffusion Tensor Imaging Investigations of...

DIFFUSION TENSOR IMAGING INVESTIGATIONS OF
MILD BRAIN DAMAGE
by
Yuko Koshimori
A thesis submitted in conformity with the requirements
for the degree of Master‟s of Science
Graduate Department of Rehabilitation Science
University of Toronto
© Copyright by Yuko Koshimori 2011

ii
Diffusion Tensor Imaging Investigations of Mild Brain Damage
Yuko Koshimori
Master‟s of Science
Graduate Department of Rehabilitation Science
University of Toronto
2011
Abstract
Diffusion tensor imaging (DTI) is a powerful tool to investigate subtle pathological changes in
the brain as it can provide microstructural and physiological information about white matter
tracts. Using this technology, we examined white matter changes secondary to traumatic brain
injury (TBI) and spinal cord injury (SCI) in two separate studies. Objective: (1) To examine the
utility of DTI for single case diagnosis of mild TBI. (2) To examine the sub-acute effects of SCI
on white matter tissue in the brains of individuals without direct injury to the brain. Methods:
DTI-derived fractional anisotropy (FA) in regions of interest (ROIs) were used as measures of
brain white matter integrity. Results: (1) The anterior limb of the internal capsule, and the genu
of the corpus callosum were sensitive and specific to mTBI. (2) SCI was associated with
changes in brain white matter: SCI patients showed significantly greater degree of hemispheric
FA asymmetry than control subjects in the superior corona radiata and posterior corona radiata.
Conclusions: (1) Our findings provide preliminary proof of principal evidence that DTI can be
used to diagnose mTBI in individual cases. (2) White matter changes are observed in the brains
of SCI patients without TBI; degree of hemispheric asymmetry may be a useful biomarker for
detecting subtle white matter changes.

iii
Acknowledgments
This thesis would not have been possible without the guidance and the help of people who
contributed and extended their valuable assistance in the preparation and completion of these
studies. First and foremost, I would like to thank Dr. Robin Green, my primary supervisor for
the invaluable learning opportunity, for the completions of enormous work as well as for her
encouragement and patient. I am also grateful for all the efforts provided by my committee
members. Thanks to Dr. Gary Turner for his tremendous support at each and every step of this
academic process, to Dr. Adrian Crawley for his generous help for the data analysis, and to Dr.
David Mikulis for his invaluable advice and expertise. I would also like to thank Dr. Cheryl
Bradbury for her assistance and cooperation for the projects. I am indebted to my current and
former lab members for their advice and kind support. Thanks to Diana Frasca, Danielle,
DeSouza, Areeba Adnan, Alexandra Arnold-Oatley, Kate Dupuis, Kadeen Jones, and Brenda
Colella. Last, but not least, I greatly appreciated the support, encouragement, and love of my
family in Japan and friends that allowed me to go through this process.

iv
Table of Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ii
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iii
Table of Contents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . iv
List of Tables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v
List of Figures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .vi
Chapter 1: General Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Chapter2: Diffusion tensor imaging for clinical diagnosis of mild traumatic brain injury . . . 13
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . .. . . . . . . . . . . . . . .. . 13
Introduction . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . 26
Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . 32
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Chapter 3: Reduced white matter integrity of the brain measured by diffusion tensor
imaging in patients with spinal cord injury . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . 35
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . 36
Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . 39
Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . 46
Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . 47
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
General Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . .. 51

v
List of Tables
Chapter 1
Table 1: Demographic and clinical characteristics of subjects . . . . . . . . . . . . . . . . . . . . . . . . . 22
Table 2: Mean FA values in right and left sides of 12 ROIs for younger and older control groups
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . 29
Table 3-1: The number of ROIs with FA values of > 3.0 SDs, 2.5 – 2.99 SDs, 2.0 - 2.49 SDs,
1.5 - 1.99 and 1.0 – 1.49 SDs below the age-stratified control mean for confirmed TBI patients .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Table 3-2: The number of ROIs with FA values of > 3.0 SDs, 2.5 – 2.99 SDs, 2.0 - 2.49 SDs,
1.5 - 1.99 and 1.0 – 1.49 SDs below the age-stratified control mean for TBI patients with normal
MRI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . 31
Table 3-3: The number of ROIs with FA values of > 3.0 SDs, 2.5 – 2.99 SDs, 2.0 - 2.49 SDs,
1.5 - 1.99 and 1.0 – 1.49 SDs below the age-stratified control mean for non-TBI patients . . .. .31
Chapter 2
Table 1: Demographic and clinical characteristics of subjects . . . . . . . . . . . . . . . . . . . .. . . . . . 42
Table 2: Mean asymmetric scores of controls as well as individual patients‟ asymmetric scores
and the standard deviations relative to control mean in the superior corona radiata and posterior
corona radiata . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . 47

vi
List of Figures
Chapter 1
Figure 1: A schematic image of myelinated axons . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . 7
Figure 2: Diffusion ellipsoid with its principal axes along the eigenvectors . . . . . . . .. . . . . . . . 8
Chapter 2
Figure1: White matter parcellation maps for FA analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Chapter 3
Figure 1: White matter parcellation maps for FA analysis . . . . . . . . . . . . . . . . .. . . . . . . . . . . . 45

1
CHAPTER 1: GENERAL INTRODUCTION
Clinical Diagnosis of Mild Traumatic Brain injury
Definition and Prevalence of Traumatic Brain Injury
Traumatic brain injury (TBI) refers to a sudden external insult to the brain, including
contact damage or the exertion of acceleration and deceleration forces, including rotational ones
(Alexander, 1995). Mild TBI (mTBI), representing 80% of all traumatic brain injuries
(Arciniegas, Held, & Wagner, 2002), is a brain injury for which the duration of lost or altered
consciousness is at the briefest end of the continuum.
The severity of TBI is typically classified by clinical indices that measure either
alterations to consciousness or the depth of unconsciousness. These include the Glasgow Coma
Scale score, duration of loss of consciousness, or duration of posttraumatic amnesia (Hannay,
Howieson, Loring, Fischer, & Lezak, 2004; Nuwer, Hovda, Schrader, & Vespa, 2005;
Povlishock & Katz, 2005; Saatman, et al., 2008; Smith, Meaney, & Shull, 2003). The Glasgow
Coma Scale is the most widely used measure (Moppett, 2007) and consists of an independent
assessment of motor responsiveness, verbal performance and eye opening, ranging from 3 (most
severe) to 15 (normal; Teasdale & Jennett, 1974). It is obtained readily at the scene of the
accident or in acute care. Posttraumatic amnesia refers to the period of time between trauma and
regaining normal continuous memory functioning (King, 1997). During this period, a patient is
unable to lay down new memories effectively, even though they may be fully conscious.
Posttraumatic amnesia is commonly measured with the Galveston Orientation and Amnesia
Test, which measures orientation and continuous memory (Bode, Heinemann, & Semik, 2000).
Loss of consciousness is defined as the absence of spontaneous or non-spontaneous (i.e., in
response to noxious stimuli) eye opening without ocular injury or oculomotor palsy (Gennarelli,

2
et al., 1982). Using these scales, mTBI is defined by the Glasgow Coma Scale scores of 13 to
15, loss of consciousness of 30 minutes or less, and/or posttraumatic amnesia of 24 hours or less
(American Congress of Rehabilitation Medicine, 1993), though definitions vary.
The prevalence of mTBI is high, with an annual worldwide incidence varying from 100
to 600 per 100,000 people (Cassidy, et al., 2004) and mTBI now widely recognized as a major
public health concern. MTBIs are most commonly sustained in contact sports, such as hockey,
football and boxing, moving vehicle accidents, falls, assaults and, exposure to bomb blasts
(Cassidy, et al., 2004; French & Parkinson, 2008; Mendez, Hurley, Lassonde, Zhang & Taber,
2005; Sosin, Sniezek, & Thurman, 1996; Stiell, et al., 2001). The incidence of mTBI shows a
bimodal distribution, with an elevation in younger adults, aged 15 to 24 years for which the
male to female ratio is 2:1 (Sosin, et al., 1996). A second peak occurs in older adults, due in
large part to falls and injuries, with a roughly even distribution between the sexes.
MTBI gives rise to a range of cognitive, somatic and emotional symptoms including
attention and memory problems; headache and dizziness; and symptoms of anxiety and
depression (Carroll, et al., 2004; Kelly & Rosenberg, 1997; King, 1997). Symptoms typically
resolve within a few weeks (Alexander, 1995; Iverson, 2005; Nuwer, et al., 2005). However,
approximately 30% of mTBI patients (Hofman, et al., 2001) have persisting symptoms several
months post-injury (Alexander, 1995; Kushner, 1998; Ingebrigsten, Waterloo, Marup-Jensen,
Attner, & Rommeret, 1998; Sterr, Herron, Hayward, & Montaldi, 2006) and after a year, 10 to
15% of mTBI patients still show significant symptoms (Alexander, 1995; Cierone & Kalmar,
1995; Dikmen, Machamer, Winn, & Temkin, 1995; Kushner, 1998; Nuwer, et al., 2005).
Better Diagnosis of MTBI: the Clinical Need
The exceedingly high rates of injury reported above are still thought to be an
underestimate of the true number of mTBI (Belanger, Vanderploeg, Curtiss, & Warden, 2007).

3
This is partly because conventional behavioural and neuroimaging tools used to assess mTBI,
such as neuropsychological assessment, CT and MRI, are not sufficiently sensitive to detect the
subtle neuropathological changes associated with mTBI. Thus, many mild traumatic brain
injuries are missed (Garnett, Blamire, Rajagopalan, Styles, & Cadoux-Hudson, 2000),
particularly when concomitant injuries have been sustained that consume the focus of medical
attention, such as spinal cord injury (SCI; Saboe, Reid, Davis, Warren, & Grace, 1991; Tolone,
Turkka, Salonen, Ahoniemi, & Alaranta, 2007) and crush injuries (Duhaime, Eppley, Margulies,
Heher, & Barlette, 1995).
The problem of missed diagnosis has important clinical implications. First, along with
headache, dizziness, and symptoms of anxiety and depression, mTBI gives rise to cognitive
symptoms such as attention and memory problems (Carroll, et al., 2004; Kelly & Posenberg,
1997; King, 1997). While these cognitive symptoms may be mild, they can still impede
functioning. Thus, a diagnosis of mTBI is needed to ensure withdrawal from activities that pose
a risk of harm to self or others, such as the operation of heavy machinery or participation in
contact sports. Diagnosis is also needed to ensure increased vigilance against a subsequent brain
injury, both in the short term - because of risk of second impact syndrome (Saunders &
Harbaugh, 1984) - and in the longer term, because of the putative cumulative impact of multiple
injuries (Nuwer, et al., 2005) including chronic traumatic encephalopathy (Le & Gean, 2009). A
diagnosis is also needed to ensure that clinical intervention ensues, where appropriate, given
evidence of improved outcomes with early intervention (Cicerone, et al., 2005; Miles,
Grossman, Johnson, Babb, Diller, et al., 2008; Till, Colella, Verwegen, & Green, 2008) and the
known deleterious impact of cognitive impairment on recovery from co-morbidities, such as
spinal cord injury (Bradbury, et al., 2008).

4
Neuropathology of MTBI
Postmortem and animal studies have shown that the primary neuropathology of mTBI is
microscopic axonal injury (Oppenheimer, 1968; Povlishock, Becker, Cheng, & Vaughan, 1983).
The microscopic axonal injury can occur in the absence of focal contusions, hemorrhage,
herniation or macroscopic axonal tearing (Povlishock, et al., 1983) or vascular injury
(Blumbergs, Scott, Mnanavis, Wainwright, et al., 1995; Oppenheimer, 1968; Povlishock, et al.,
1983).
Microscopic axonal damage of a traumatic nature (a.k.a. traumatic axonal injury;
Geddes, Whitwell, & Graham, 2000) is the result of shear, tensile and compressive strains
within the tissue that stretch and distort axon fibres (Gulani and Sundgren, 2006; Smith, et al.,
2003) rendering axons temporarily undulated and misaligned (Wolf, Stys, Lusardi, Meaney, &
Smith, 2001). The majority of them regain most of their pre-stretched orientation (Wolf, et al.,
2001), but calcium dysregulation can occur due to influx of extracellular calcium (Maxwell, et
al., 1999), activation of sodium channels (Wolf, et al., 2001) and/or mechanical damage to
channels (Buki & Povlishock, 2006). As a result, enzymes that degrade key structural proteins
become activated, destroying microtubules and neurofilaments, leading to focal axonal swelling
with accumulated proteins and organelles; axonal disconnection can occur under these
conditions, but not invariably (Buli & Povlishock, 2006; Maxwell, et al., 1991; Park, Bell, &
Baker, 2008).
Limits of Current Diagnostic Tools: CT and Conventional MRI Are Insensitive to the
Microscopic Neuropathology of MTBI
These microscopic changes, some of them biochemical, are notoriously difficult to
detect. Indeed, the limits of conventional imaging for mTBI have been widely reported (Hayes
& Dixon, 1994; Huisman, Sorensen, Hergan, Gonzalez, & Schaefer, 2003; Saatman, et al.,

5
2008). CT can reliably detect skull fractures and life-threatening intracranial hemorrhage
(Besenski, 2002; Hurley, McGowan, Arfanakis, & Taber, 2004; Le & Gean, 2009; Povlishock
& Katz, 2005), is relatively inexpensive (Hurley, et al., 2004) and can accommodate life-support
and monitoring equipment (Hurley, et al., 2004; Le & Gean, et al., 2009). However, the majority
of mTBI patients (with estimates ranging from 60 to 95%) show no visible abnormality on
intracranial CT (Borg, et al., 2004).
MRI is more sensitive to the neuropathology of mTBI than CT (Hurley, et al., 2004; Lee,
Wintermark, Gean, Ghajar, Manley, Mukherjee, et al., 2008; Mittl, et al., 1994; Saatman, et al.,
2008). In particular, T2*-weighted gradient recalled echo is highly sensitive to hemorrhagic
traumatic axonal injury while T2-weighted fluid attenuated inversion recovery is useful to detect
nonhemorrhagic traumatic axonal injury (Huisman, et al., 2003; Kinoshita, et al., 2005; Niogi &
Hukherjee, 2010). Nonetheless, the white matter lesions that are visualizable on fluid attenuated
inversion recovery are macroscopic (Niogi & Mukherjee, 2010) and thus mTBI lesions may not
be visualized.
Diffusion Tensor Imaging (DTI): A Promising Approach for MTBI Diagnosis
A relatively new magnetic resonance imaging technique, DTI, is showing promise for
the diagnosis of mTBI. There is a burgeoning literature demonstrating DTI differences between
patients with mTBI and healthy controls (Arafanakis, Haughton, Carew, Rogers, Dempsey, et
al., 2002; Inglese, et al., 2005; Kraus, Susmaras, Caughlin, Walker, Sweeney, et al., 2007;
Mayer, et al., 2010; Rutgers, Fillard, Parado, Tadie, Lasjaunias, et al., 2008; Rutgers, Toulgoat,
Cazejust, Fillard, Lasjaunias, et al., 2008). Some of these studies have also shown correlations
with neuropsychological assessments (Lipton, et al., 2009; Miles, et al., 2008).
Several studies have directly demonstrated the enhanced sensitivity of DTI to brain
injury relative to conventional MRI. For example, Niogi, et al. (2008b) demonstrated that the

6
number of white matter structures with microstructural injury detected by DTI was correlated
with impaired reaction time in mild TBI whereas the number of traumatic microbleeds detected
by conventional MRI sequences was unrelated to the cognitive function.
Brief overview of DTI
DTI is an MRI technique that can measure the preferred displacement of water
molecules in brain white matter (Le Bihan, 2006) allowing us to infer microstructual and
physiological information about white matter tracts (Mukherjee, Berman, Chung, Hess, &
Henry, 2008). The properties of DTI have been described in a number of reviews (Assaf &
Pasternak, 2008; Alexander, Lee, Lazar, & Field, 2007; Bammer, 2003; Le Bihan, et al., 2001;
Mukherjee, et al., 2008). In brief, water mobility in brain white matter is rather anisotropic,
reflecting non-equal, directional diffusivities (Basser, 1995; Pierpaoli & Basser, 1996; Watts,
Liston, Niogi, & Ulug, 2003). As most or all of the axons of the brain are tightly aligned in a
parallel fashion in white matter tracts, water diffuses over the long axis of the axons greater
compared to its displacement perpendicular to the axon. (See Figure 1; Chenevert, Pipe,
Williams, & Brungerg, 1999; Mac Donald, Dikranian, Song, Bayly, Holtzman, et al., 2007).

7
Figure 1. A schematic image of myelinated axons. Yellow dots represent water molecules. To
move perpendicular to the axons, water molecules must cross myelin sheath.
A diffusion tensor is a mathematical model of the three-dimensional pattern of diffusion
anisotropy (Alexander, et al., 2007; Mukherjee, et al., 2008). From the measured tensor, one can
calculate the principal diffusivities or eigenvalues, annotated 1, 2, and 3 in order of largest to
smallest magnitude of diffusivities (Neil, 2008; Nucifora, Verma, Lee, & Mehhem, 2007) as
well as eigenvectors (i.e., orientation; Pierpaoli & Basser, 1996) of the eigenvalues. The
eigenvector associated with the largest eigenvalue is oriented parallel to the fiber direction while
the two other eigenvectors are oriented perpendicular to it (Basser, Mattiello, & Le Bihan, 1994;
Neil, 2008). As illustrated below, diffusion ellipsoids are often used to visualize the concept of
the anisotropic diffusion (see Figure. 2; Mukherjee, et al., 2008; Neil, 2008).

8
Figure 2. Diffusion ellipsoid with its principal axes along the eigenvectors.
Quantifying Diffusion: Fractional Anisotropy (FA)
In DTI, the most common metric of diffusion (or anisotropy) is fractional anisotropy
(FA), representing the fraction of overall diffusion in a brain region that is anisotropic. Other
metrics include directionally-averaged mean diffusivity or apparent diffusion coefficient. FA is
a scalar rotationally invariant metric with values ranging from zero to one (Le Bihan, et al.,
2001). Rotationally invariant measures have values independent of the laboratory frame of
reference, of the direction of the applied diffusion gradients, and of the orientation of the tissue
structures within each voxel (Basser, et al., 1994). In general, FA has shown greater sensitivity
to mTBI than other diffusion metrics (but see Messe, et al., 2010; Zhang, Johnson, Pennell, Ray,
Sebastianelli, et al., 2010). Several studies have now reported abnormal FA values where
apparent diffusion coefficient and mean diffusivity values were in the normal range (Arfanakis,
et al., 2002; Bendlin, et al., 2008; Inglese, et al., 2005). Perhaps more importantly, FA has
shown greater correlations with the clinical sequelae of mTBI than other indices (Niogi,
Mukherjee, Ghajar, Johnson, Kolster, et al., 2008; Miles, et al., 2008; Wilde, et al., 2008). Taken
together, these findings suggest that DTI, and FA as a proxy measure for changes in white
matter integrity, may hold considerable potential for diagnosis of mTBI.
It should be noted that despite its potential, FA has limitations that must be taken into
consideration. Most studies have shown that mTBI subjects have reduced FA values relative to

9
uninjured controls. However, a few studies have reported higher FA mean values in patients.
Mechanisms of reduced FA include focal misalignments of the cytoskeletal network, change in
axolemmal permeability, axonal swelling and disconnection of axons (Arafanakis, et al., 2002;
Buki & Povlishock, 2006) followed by Wallerian degeneration (Griffin, et al., 1992; Povlishock
& Katz, 2005). Proposed mechanisms for increased FA include compressed intracellular spaces
due to cytotoxic edema (Mayer, et al., 2010; Wilde, et al., 2008) early injury or enhanced linear
arrangement of unaffected tracts late injury by a loss of crossing affected white matter tract or
compensatory alteration related to injury in other region (Lo, et al., 2009; Pierpaoli, et al., 2001).
Gaps in Research
Despite excellent promise, further research is needed before DTI will be ready for
clinical use. Most of the research to date employs group comparisons (Rutgers, et al., 2008a;
Lipton, et al., 2008; Lo, et al., 2009; Mayer, et al., 2010). However, for DTI to be used for
clinical purposes, we must be able to diagnose at the single case level. DTI has yet to be
validated for single case diagnosis.
Spinal Cord Injury and Effects on the Brain
Definition and Prevalence of Spinal Cord Injury
Spinal cord injury (SCI) results from mechanical injury to the spinal cord that disrupts
reciprocal connections from brain to body, giving rise to motor and sensory impairments
(Baptiste, Tighe, & Fehlings, 2009). These deficits can manifest in varying severities depending
on the anatomical levels (i.e., cervical, thoracic, lumbar or sacral). Loss of motor and/or sensory
function in the cervical segments of the spinal cord results in quadriplegia (tetraplegia). Damage

10
at the level of thoracic, lumbar or sacral segments of the spinal cord result in paraplegia
(Maynard, et al., 1997).
Injury severity can be classified as incomplete and complete injury (Maynard, et al.,
1997). This is typically determined by neurological examination of sensory and motor
functioning (Maynard, et al., 1997). The American Spinal Cord Injury Association impairment
scale is the most widely used scale with five categories ranging from complete injury (A), to
normal sensory and motor function (E). Incomplete injury is characterized by partially preserved
sensory and/or motor functions, while complete injury is defined by an absence of sensory and
motor function in the lowest sacral segment (Waters, Adkins & Yakura, 1991). However even in
complete injuries, nerve fibers that traverse the lesion epicenter may be spared at the time of the
primary mechanical traumatic event (Baptiste, et al., 2009).
The estimated incidence of traumatic SCI worldwide is approximately 13 to 52 cases per
million (Dryden, et al., 2003; O‟Connor & Murray, 2006). The mean age is in the third to fourth
decade and men are at three or four times greater risk of sustaining a traumatic SCI (Chiu, Lin,
Lam, Chu, Chiang, et al., 2010). The primary causes of traumatic SCI are the same as those for
TBI, namely traffic accidents and falls, accounting for the majority of cases. Injury at the
cervical level is most common, ranging from 41.6 % to 75% of injuries, followed by injury at
the thoracic level (16% to 36%) and injury at the lumbar level (9% to 17.6%).
Pathology within the spinal cord
Trauma to the vertebral column can cause injury to the cord from transient or fixed bone
displacement into the spinal canal compressing the spinal cord. Non-boney elements including
disc material and hematomas produced by the trauma can also compress the spinal cord (Sekhon
& Fehlings, 2001). Following the initial injury, the spinal cord undergoes a delayed cascade of
biochemical and cellular processes that involve a larger area of damage than the initial injury

11
(Baptiste, et al., 2009). SCI can cause two types of cell death, namely necrosis and apoptosis
(Hainx, Black, & Waxman, 2003; Koda, et al., 2002; Lee, et al., 2004; Shifman, Zhang, &
Selzer, 2008). Necrosis represents immediate cell death (Majno & Joris, 1995) while apoptosis
is a delayed process of cellular dysregulation ultimately leading to cell death. Cell death occurs
not only at lesion sites, but also remotely in neurons (Bradbury, King, Lucinda, Priestley, &
McMahon, 1998; Himes, Goldberger, & Tessler, 1994; Shibayama, Hattori, Himes, Murray &
Tessler, 1998), oligodendrocytes (Crowe, Bresnahan, Shuman, Masters, & Beattie, 1997; Koda,
et al., 2002), and microglia (Koda, et al., 2002).
Apoptotic cell death including oligodentrocytes was observed preferentially in the region
of the distal axonal segment of white matter tracts undergoing Wallerian degeneration in the
corticospinal tract as well as dorsal ascending tract (Warden, et al., 2001). Oligodendrocytes
appear to be particularly susceptible (Casha, Yu, & Fehlings, 2001; Emery, et al., 1998; Koda, et
al., 2002). Loss of oligodendrocytes due to apoptosis could result in demyelination of spared
axons, interfering with signal transduction (Shuman, Bresnahan, & Beattie, 1997), which
contributes to functional impairment (Crowe, et al., 1997; Li, Farooque, Holtz, & Olsson, 1999;
Warden, et al., 2001).
Pathology of the Brain Secondary to Spinal Cord Injury
Pathological changes are not confined to the spinal cord. The structural and functional
changes in the brain following SCI have been reported in both animal and human studies. For
example, animal models have demonstrated altered synaptic structures (Kim, Dai, McAtee,
Vicini, & Bregman, 2006), cell atrophy (Wannier, Schmidlin, Bloch, & Rouiller, 2005),
apoptotic cell death in the primary motor cortex (Hains, Black, & Waxman, 2003) as well as
functional reorganization in the primary somatosensory cortex (Endo, Spenger, Tominaga,
Brene, & Olson, 2007). In the human brain, reduced gray matter volume has been demonstrated

12
in the primary motor cortex and frontal areas (Wrigley, et al., 2009) and somatosensory and
posterior parietal cortices (Jurkiewicz, Crawley, Verrier, Fehlkings, & Mikulis, 2006) and
alterations in brain function have been reported in the motor and somatosensory cortices
(Jurkiewicz, et al., 2007; Mikulis, et al., 2002). To date, changes in gray matter structures have
been well studied.
On the contrary, axonal or white matter changes have been relatively unexplored. To our
knowledge, there have been six human studies that investigated white matter following SCI.
Two studies using the voxel-based morphometry methods failed to find significant changes in
white matter volume between healthy control and SCI patient groups. There are four studies that
used DTI to investigate changes in white matter integrity. Two studies found no significant
group differences between SCI patients and controls (Gustin, et al., 2009; Wei, et al., 2008)
while two other studies found abnormal FA values along the corticospinal tracts in the patient
group (Guleria, et al., 2008; Wrigley, et al., 2009). Thus, the effects of SCI on white matter are
equivocal and to be elucidated.

13
CHAPTER 2: DIFFUSION TENSOR IMAGING FOR
CLINICAL DIAGNOSIS OF MILD TBI
Abstract
Prevalence of mild TBI (mTBI) has reached epidemic proportions. However, reliable diagnosis
is limited by insensitivity of conventional neuroimaging to the neuropathology of mTBI:
microscopic white matter changes. Diffusion tensor imaging (DTI) has been shown to be more
sensitive to mTBI than conventional MRI in group studies. For clinical diagnosis it will be
important to determine whether DTI shows sensitivity and specificity for mTBI in individual
cases. To assess sensitivity we first examined a common DTI measure, fractional anisotropy
(FA), in mTBI predilection sites derived from the literature in two SCI patient groups: (1) five
with definitive TBI on neuroradiological report and (2) four whose TBI clinical indices (i.e.,
Glasglow Coma Sclae, posttraumatic amnesia, and loss of consciouness) suggest the presence of
mTBI, but whose conventional MRI findings were normal. To assess specificity, five additional
SCI patients who had no evidence of TBI on neuroradiological or clinical report were examined
for FA abnormalities. For each patient FA values were compared to a closely-matched, age-
stratified control group. We reported FA values of greater than 1.0 standard deviation below the
control mean in each ROI. The anterior limb of the internal capsule, and the genu of the corpus
callosum were sensitive and specific to mTBI. These preliminary data suggest that DTI may
have clinical relevance as a tool for diagnosing mTBI in SCI patients. Given the clinical
significance of mTBI, enhanced diagnosis will aid with prognosis and rehabilitation planning.

14
Introduction
Traumatic brain injury (TBI) refers to a blow to the head or the exertion of acceleration
and deceleration forces to the brain, with or without external skull impact. Approximately 80%
of TBIs are mild (Arciniegas, et al., 2002), which is defined typically as a Glasgow Coma Scale
score of 13 to 15, loss of consciousness of 30 minutes or less and posttraumatic amnesia of 24
hours or less (American Congress of Rehabilitation Medicine, 1993). MTBI has been associated
with a combination of cognitive, somatic, motor and emotional symptoms (Carroll, et al., 2004;
Kelly & Posenber, 1997; King, 1997). Increasingly referred to as an “epidemic” (Ellemberg,
Henry, Macciocchi, Guskiewicz, & Broglio, 2009), mTBI has a worldwide annual incidence
estimated at up to 600 per 100,000 people (Cassidy, et al., 2004).
The clinical manifestations of mTBI are not reliably detected using traditional
behavioural approaches, such as neuropsychological or clinical motor testing (Fait, McFadyen,
Swaine, & Cantin, 2009) or conventional neuroimaging (Hurley, et al., 2004: Lee, et al., 2008;
Mittl, et al., 1994; Saatman, et al., 2008). Consequently, clinicians tend to rely on subjective,
self-report measures of symptoms (King, Crawford, Wenden, Moss, & Wade, 1995; Randolph,
Millis, Barr, McCrea, Guskiewicz, et al., 2009). However, the objective verification of mTBI is
an important clinical gap, and represents a long-standing, and sometimes contentious area of
study (see Green, Koshimori, & Turner, 2010.)
One of the key diagnostic challenges is arguably the microscopic neuropathology of
mTBI. MTBI is associated with microscopic axonal (Oppenheimer, 1968; Povlishock, et, al.,
1983) and vascular injury (Bigler, 2004) that is well documented in post-mortem and animal
studies (Adams, Koyle, Ford, Gennarelli, Graham et al., 1989; Buki & Povlishock, 2006;
Maxwell, et al., 1999; Povlishock, Erb, & Astruc, 1992; Wolf, et al., 2001). Microscopic axonal
injury, in particular, can occur in the absence of macroscopic white matter tears (Povlishock, et

15
al 1983) or vascular damage (Blumbergs, et al, 1995) including petechial hemorrhage
(Oppenheimer, 1968; Povlishock, et al., 1983).
To overcome the issue of poor sensitivity with conventional neuroimaging methods, one
technique that is used increasingly in experimental settings is MRI diffusion tensor imaging
(DTI). DTI shows sensitivity to subtle white matter abnormalities by measuring the diffusion of
hydrogen nuclei contained in water molecules over time (Le Bihan, et al., 2006). Depending
upon the properties of the tissue environment, water diffusion will occur in an isotropic or
anisotropic fashion (i.e., with a preferred direction). Since most or all axons are tightly aligned
in a parallel fashion in white matter tracts, water shows a preferred diffusion pattern, moving
predominantly along the direction of the axons rather than perpendicular to them (Chenevert,
Brunberg, & Pipe, 1999; Mac Donald, Dikranian, Song, Bayly, Holtzman, et al., 2007;
Mukherjee, et al., 2008). This allows us to infer microstructural and physiological information
about the integrity of axonal fiber bundles (Basser, 1995).
Fractional anisotropy (FA), a scalar value between zero and one (A quantity which has
magnitude only, and has the same value in every coordinate system), is one of the most widely
used DTI indices of anisotropy (Alexander, Lee, Lazar, & Field, 2007). An FA value of zero
represents completely isotropic diffusion (i.e., random diffusion) whereas a value of one
represents completely anisotropic diffusion (Le Bihan, et al., 2001). When the integrity of white
matter is compromised, as may be the case in mTBI, FA values are reduced (Arfanakis et al.,
2002). Reduced FA values secondary to mTBI have been observed both acutely and during the
chronic phases of injury in a number of studies (Lipton, et al., 2009; Niogi, et al., 2008b; Rutger,
et al., 2008a; Rutgers, et al., 2008b). For examples of increased FA both early and later post-
injury, see Wilde et al. (2008), Mayer et al. (2010), and Lo, et al. (2009). Here, it is thought that
cytotoxic edema [early] and loss of damaged crossing tracts [later] can result in increased
anisotropic movement (Bhagat, et al., 2006; Field, Hasan, Jellison, Arfanakis, & Alexander,

16
2003; Green, et al., 2002; Lo, et al., 2009; Pierpaoli, et al, 2001). A comprehensive survey of the
diffusion imaging literature revealed that there are a number of brain regions that are
particularly susceptible to mTBI. These studies revealed abnormal FA values in the anterior
corona radiata (Maruta, Suh, Niogi, Mukherjee, & Ghajar, 2010; Niogi, et al., 2008b) and
superior corona radiata (Kraus, et al., 2007; Mayer, et al., 2010; Niogi, et al., 2008b); the genu
(Kumar, et al., 2009; Lipton, et al., 2008; Lo, et al., 2009; Niogi, et al., 2008b; Rutgers, et al.,
2008a) and splenium of the corpus callosum (Arfanakis, et al., 2002; Inglese, et al., 2005);
anterior and posterior limbs of the internal capsule (Arfanakis, et al., 2002; Inglese, et al., 2005;
Lipton, et al., 2008; Lo, et al., 2009); cingulum (Maruta, et al., 2010; Niogi, et al., 2008b,
Rutgers, et al., 2008b), superior longitudinal fasciculus (Kraus, et al., 2007); and uncinate
fascilus (Geary, Kraus, Pliskin, & Little, 2010; Mayor, et al., 2010; Niogi, et al., 2008b).
To date, the large majority of these DTI studies of mTBI have been group studies.
However, to objectively verify the presence of mTBI for clinical purposes, reliable identification
of mTBI in individual cases is needed. One study has shown promising findings in this regard
(Niogi, et al., 2008b). This study examined 34 chronic mTBI patients based on Glasgow Coma
Scale, loss of consciousness and posttraumatic amnesia findings who also reported at least one
postconcussive symptom. FA values of each patient were compared with the mean of 26 healthy
controls in 20 white matter structures using the ROI analysis. FA values with greater than 2.5
standard deviations below the control mean were considered abnormal. The study demonstrated
that (1) 85% of the patients had at least one injured ROI, (ten of whom had normal findings on
MRI sequences that are particularly sensitive to TBI, namely fluid-attenuated inversion recovery
and T2*-weighted gradient-recalled echo sequences; (2) none of the control subjects showed
deviations of 2.5 SDs or greater below the mean, and (3) the number of damaged white matter
structures, but not microbleeds was correlated with reaction times on an attention task.

17
Additionally, if DTI is to be a useful clinical tool, the sensitivity and specificity of the
method must be determined. Sensitivity refers to the ability of a diagnostic test to correctly
detect actual positives (i.e., diagnosing an mTBI when it is present). Specificity refers to the
ability of a test to correctly identify true negatives (i.e., a negative diagnosis of mTBI in an
uninjured person). The current proof-of-principal study aimed to identify those brain areas that
are maximally sensitive and specific to mTBI as a step towards the implementation of DTI for
single case diagnosis. We employed FA values given the ubiquity of their use and their
demonstrated sensitivity to mTBI.
The current study comprised three sets of examinations to investigate sensitivity and
specificity of DTI for mTBI. First, after identifying those brain regions that were most
susceptible to mTBI from prior research (see above), we examined the sensitivity of FA to
mTBI in these regions. The aim of this examination was to verify the sensitivity of mTBI
predilection sites to DTI using a sample of patients with unequivocal TBI (based on
microbleeds) with milder range of TBI indices (i.e., Glasgow Coma Scale, posttraumatic
amnesia, or loss of consciousness), and a very clean medical history; this was to ensure that
positive findings could not be attributed to other factors. This examination entailed the
individual comparison of patients with a definitive diagnosis of TBI to a normative sample of
age and education-matched controls.
The next step was to compare the FA values of four patients with mTBI to a normative
control sample. These patients had positive TBI clinical indices in the mild range, but showed
fully normal MRI scans (i.e., no microbleeds or no hyperintensities) on a protocol specifically
designed for TBI. Again, the group was carefully screened for co-morbidities that might
contaminate findings. The purpose of this examination was to identify those ROIs from the
previous examination that most robustly discriminated patients from controls.

18
Lastly, we assessed the specificity of the ROIs for mTBI. This was achieved by
examining the above ROIs in patients with fully normal MRI findings (neither microbleeds,
hyperintensities nor other spurious findings) and fully normal Glasgow Coma Scale, loss of
consciousness or post-traumatic amnesia. Here, the objective was to identify those ROIs that
would not show any (spurious) FA reductions compared to controls, that is, the ROIs that were
not only sensitive to mTBI, but also specific to it.
The patients examined in this study were drawn from a large sample of patients with
traumatic spinal cord injury who were therefore at elevated risk of mTBI. Therefore, we
excluded ROIs that might be affected by lost afferent projections from the spinal cord, including
the corticospinal or corticopontine tracts (Guleria, et al., 2008; Wrigley, et al., 2009).
Method
Subjects
Patients
Patients for the three examinations were selected from a sample of 82 patients
participating in a larger on-going study on the Spinal Cord Rehabilitation Program at Toronto
Rehabilitation Institute examining the prevalence of TBI in SCI between June 2006 and May
2009. Inclusion criteria for the current study were as follows: (1) 18 to 55 years of age; (2)
between two and six months post-injury; and, (3) able to provide informed consent. Exclusion
criteria were: (1) prior history of SCI, neurologic disorder, psychiatric illness or systemic illness
potentially affecting the brain (e.g., diabetes) and (2) drug dependence. Table 1 shows the
clinical and demographic information for participants in each of the three studies.
(I) Examining ROI sensitivity using patients with definitive TBI: microbleed patients.
This sub-group comprised five patients with microbleeds based on gradient-recalled echo T2*-
weighted images. Overall, patients in this group ranged in severity from an estimated moderate

19
to normal. A careful examination of the medical records and discussion with clinicians familiar
with the patients‟ medical histories indicated that some of the TBI clinical scores and findings
were tenuous due to post-injury medication and intubation, as well as alcohol at the time of
injury. Thus, we have reported here the clinical data along with some contextual details.
Patient One‟s clinical indices for TBI are ambiguous due to alcohol at scene of accident
and post-operative medication and surgeries. Nonetheless, there appears to be some degree of
posttraumatic amnesia and retrograde memory loss, the latter estimated at 5-15 minutes. She
also had positive CT of the brain. Patient Two was sleeping at the time of the accident, a motor
vehicle accident. He had a Glasgow Coma Scale of 15 in Emergency, but this was several hours
post-surgery and may be an underestimate of the severity of injury. There was loss of
consciousness at the scene of the accident. Patient Three had a Glasgow Coma Scale of 11 at the
scene of the motor vehicle accident; this rose quickly to 13 and then 15 at Emergency.
Posttraumatic amnesia was present, though of uncertain duration. In Emergency, CT and
conventional MRI were normal and he was diagnosed with mTBI in acute care. Patient four was
fully conscious at the scene of the accident and Glasgow Coma Scale was therefore not
completed. However, he had positive CT of the brain. In addition, there is no memory of the
accident, and therefore at least a brief period of post traumatic amnesia. Patient five had 5
minutes of loss of consciousness, a Glasgow Coma Scale of 15 at the hospital and some
retrograde memory loss. Posttraumatic amnesia could not be estimated due to post-surgical
medications. She had positive CT of the brain.
(II) Examining ROI sensitivity using patients with normal MRI and positive TBI indices.
This sub-group included four patients with normal conventional MRI (i.e., T1-weighted images,
T2-weighted fluid-attenuated inversion recovery images, and gradient-recalled echo T2*-
weighted images) and positive TBI indices. Again, medical records were carefully examined
and a discussion with a clinician familiar with patients‟ medical histories was carried out. By

20
design, this group was a milder TBI group than the previous group. All of the patients had
sustained a blow to the head in the context of their traumatic SCI. Patient Six was intoxicated at
the scene of the accident. However, some loss of consciousness is probable. At the scene of the
accident, Glasgow Coma Scale was 9, but this is invalidated by alcohol. At Emergency,
Glasgow Coma Scale was 14. Patient Seven had loss of consciousness of uncertain duration, but
a Glasgow Coma Scale of 15 by the time Emergency Services arrived. Admission diagnosis was
query mTBI. Patient Eight had a Glasgow Coma Scale score of 15, with one to two hours of
reported loss of consciousness; however, she had consumed alcohol prior to injury, which
confounds the estimate of loss of consciousness due to mTBI. Patient Nine had a Glasgow
Coma Scale score of 15, no posttraumatic amnesia and self-reported momentary loss of
consciousness.
(III) Examining ROI specificity using MRI and clinically negative patients. This sub-
group comprised five patients with no evidence of concomitant TBI. All had normal Glasgow
Coma Scale, and no loss of consciousness or posttraumatic amnesia. Other direct and indirect
indicators of TBI were also negative. These included: (1) evidence of blow to the head, (2)
positive findings on MRI T1-weighted images; T2-weighted fluid-attenuated inversion recovery
images and gradient-recalled echo T2*-weighted images; and, (3) circumstances of injury
compatible with acquired brain injury (e.g., hypoxia, acceleration/deceleration forces).
Control Subjects
Fifteen healthy control subjects were drawn from the local community of students, staff,
and family and friends of students and staff. Inclusion criteria and exclusion criteria were the
same as for patients, except for the injury criteria.
Control sub-groups. In order to match patients and controls as closely as possible, two
control groups were drawn from the 15 controls, a younger group (N=8) and an older group

21
(N=6). (See Table 1 for further details.) Each subject was compared to one of these two groups.
The gap in age between any patient and his/her respective normative group was no more than
eight years, and the gap in education was no more than six years.

22
Table 1
Demographic and Clinical Characteristics of Subjects
Groups Sex Age Years
of
Education
Injury
Type
Days
between
Injury and
MRI
Presence of TBI
indices (+/-)
Number of
microbleeds
Patient group
Microbleed
group
1 F 21 12 MVA 134 + 14
2 M 23 12 MVA 101 + N/A
3 M 51 12 MVA 147 + 2
4 M 51 15 Fall 62 + 2
5 F 41 14 Fall 68 + 3
Mean ± SD 37.4 ± 14.7 13 ± 1.4
Normal MRI/+
TBI indices
group
6 M 21 12 Fall 66 + 0
7 M 22 14 Sports 101 + 0
8 F 47 14 Fall 153 + 0
9 M 28 16 Sports 90 + 0
Mean ± SD 29.5 ± 12 14 ± 1.6
No TBI group
10 M 20 12 MVA 86 - 0
11 M 31 12 Fall 54 - 0
12 M 39 14 MVA 74 - 0
13 M 29 10 Fall 85 - 0
14 M 19 12 Fall 68 - 0
Mean ± SD 27.6 ± 8.3 12 ± 1.4
Control groups
Younger
controls
Mean ± SD (2F) 26.3 ± 4.5 15.1 ± 2
Older controls
Mean ± SD (1F) 43.3 ± 9 18.2 ± 2.1
F: female, M: male, MVA: motor vehicle accident

23
Materials
MRI protocol
Acquisition. Whole brain conventional MRI and DTI were acquired on a 3Tesla (3T)
General Electric Signa-EXCITE scanner (GE Healthcare, Waukesha, WI, USA) equipped with
an eight-channel head coil. DTI was acquired with diffusion-weighted spin-echo single-shot
echo planar imaging with diffusion encoding in 15 noncollinear directions. The sequence
parameters were as follows: TR = 10,000 ms; TE = 84 ms; field of view = 240 mm2; matrix =
128 x 128 mm; the number of slices = 45, slice thickness = 3 mm without gaps; b value = 1000
s/mm2. Parallel imaging was employed using the Array Spatial Sensitivity Encoding Technique
with an acceleration factor of 2. DTI for all subjects were acquired in the axial plane. One
additional image with no diffusion weighting was also acquired. The DTI scans were repeated
three times to increase signal to noise ratio. The total DTI acquisition time was approximately 8
minutes. The following conventional 3T MR sequences were acquired: (1) axial three-
dimensional (3D) inversion recovery fast spoiled gradient-recalled echo T1-weighted images
(TR = 7.9 ms, TE = 3.1 ms, TI = 450 ms, flip angle = 12º) with 220 mm2 field of view, 166 1.0-
mm contiguous partitions at a 256 x 256 matrix; (2) axial T2-weighted fluid-attenuated
inversion recovery images (TR = 8652, TE = 136.1 to 146, TI = 2250 ms) with 220 mm2 field of
view, 4 mm slice thickness, 28 slices, and 384 x 224 matrix (3) axial gradient-recalled echo
T2*-weighted images (TR = 600, TE =25, flip angle of 45º) with 220 mm2 filed of view, 45 or
46 slices, 3 mm slice thickness, and 384 x 224 matrix.
\
MRI Data Analysis
Evaluation of conventional MRI
The conventional MRI images were qualitatively evaluated by an experienced
neuroradiologist for TBI and other neurological findings. The radiologist was blinded to DTI

24
findings and clinical scores. The evaluation included classification of all visible lesions based on
their signal characteristics. Additionally, microbleeds in the five patients were located by
another experienced neuroradiologist (D.M.) who was blind to their initial MRI reports.
DTI processing
Imaging data were processed offline using FSL tools from the FMRIB software library
(FSL, http://www.fmrib.ox.ac.uk/; Smith, et al., 2004; Woolrich, et al., 2009). FMRIB‟s
diffusion toolbox was used to correct motion and eddy current distortion with b = 0 as reference.
An average set of DTI images was generated from the three sets of DTI data. Non-brain tissue
of the averaged DTI set was removed using brain extraction tool (Smith, 2002), and FA maps
were derived using DTIfit. The images from all subjects were nonlinearly transformed to a
standard space (Andersson, Jenkinson, & Smith, 2007a, 2007b) by normalizing them to a 1x1x1
mm common template, the International Consortium of Brain Mapping-DTI-81 (ICBM-DTI-81;
Mori, Wakana, Nagae-Poetscher, & van Zijl, 2005). ICMB-DTI-81 is white matter atlas in
sterotaxic coordinates based on DTI data from 81 healthy subjects (42 males and 39 females
with the mean age of 38.63 raging from 18 to 59 years; right-handed) and its white matter
parcellation maps include 50 manually segmented white matter structures. Consistent with
previous studies on the current topic (Arfanakis, et al., 2002; Bendlin, et al., 2008; Inglese, et
al., 2005), we chose FA as our primary diffusion measure.
Region of interest (ROI) analysis
The white matter parcellation maps were superimposed on normalized subject data
where 3D ROI analyses were performed for the calculation of FA values. The following white
matter structures were selected based on the literature review: genu of the corpus callosum,
splenium of the corpus callosum; anterior corona radiata; anterior limb of the internal capsule;
uncinate fasciculus; cingulum and superior longitudinal fasciculus. ROIs identified as possible

25
predilection sites in the literature, but which contained the corticospinal tracts were removed.
These were the posterior limb of the internal capsule and superior corona radiata due to possible
effects of SCI on the brain (Guleria, et al., 2008; Ramu, Herrera, Grill, Bockhorst, & Narayana,
2008; Wrigley, et al, 2009). The FA values in the right and left hemispheres of all the structures
were examined separately. Therefore, a total of 12 ROIs were investigated in Study 1 (Fig.1).
Design and Procedures
The design was retrospective, and utilized a series of single case analyses. Outcome
measures were FA values in ROI predilection sites. Of eighty-two patients eligible from the
larger study, the medical histories were carefully screened to identify factors that could
influence FA values (e.g., neurologic, psychotic, and systemic illnesses and drug dependence).
This reduced the sample to the 14 employed in the study.
Data Analysis
A case report analysis was conducted. Each case was compared with either the younger
or older control group depending on the age of the patient. FA values for each ROI for each
patient were classified relative to the normative controls: 1.0 to 1.49 standard deviations (SDs)
below the mean; 1.5 to 1.99 SDs below the mean; 2.0 to 2.49 SDs below the mean; and 2.5 to
2.99 SDs below the mean or 3.0 or more SDs below the mean. In addition, a chi square analysis
was run. Here, the frequencies of patients who had FA values of greater than 1.5 SDs below the
mean, which has an experimental false positive rate of 0.09, were compared between two
groups. The first group was the combined TBI groups, that is, the patient group with TBI
confirmed by structural lesions plus the patient group with no structural lesions, but positive
clinical indices for TBI. The second group was the “no TBI” group. The chi square analysis was
undertaken for all ROIs combined.

26
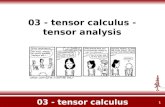
Figure 1. White matter parcellation maps for FA analysis. A. genu of corpus callosum; B.
splenium of corpus callosum; C. anterior limb of internal capsule; D. anterior corona radiata; E.
uncinate fasciculus; F. superior longitudinal fasciculus; G. cingulum
Results
Conventional MRI Findings
All subjects except those in the positive TBI group had normal findings on conventional
MRI. The second reading of microbleeds was in a good agreement with initial MRI reports in
terms of the number and locations of the microbleeds.
Control groups. FA values for each ROI for the control groups are presented in Table 2.
Individual Case Analyses
(I) Examining ROI sensitivity using patients with definitive TBI (microbleed patients).
Table 3-1 illustrates that in all of the predilection ROIs, FA values of greater than 1.0 SD below
A B C D
E F G

27
the control mean were observed in at least one patient with the exception of the splenium of the
corpus callosum.
Several ROIs showed robust findings. The left anterior limb of the internal capsule was
the most affected ROI, with two patients showing FA values of greater than 2.5 SDs below the
control mean and another with FA values between -1.5 and -1.99 SDs. The two patients with
severely reduced FA values in the left anterior limb of internal capsule also showed reduced FA
values in the right anterior limb of the internal capsule. The genu of the corpus callosum and the
right uncinate fasciculus were also robustly affected, with one patient showing FA values of
between -2.0 and -2.49 SDs, one showing FA values between -1.5 and -1.99 SDs, and another
showing FA values between -1.0 and -1.49 SDs. In the right cingulum, one patient had an FA
value of greater than 3.0 SDs below the control mean and two others had FA values of between
-1.0 and -1.49 SDs.
Table 3-1 also illustrates a number of areas that were less robustly affected. These
included the bilateral anterior corona radiata, bilateral superior longitudinal fasciculus, left
uncinate fasciculus and left cingulum.
This analysis enabled us to confirm the sensitivity of DTI to TBI in all areas identified in
the literature as mTBI predilection sites (some more sensitive than others) with the exception of
the splenium of the corpus callosum. As the splenium displayed no sensitivity to mTBI in the
above examination, it was not included in the next examination.
(II) Examining ROI sensitivity using patients with normal MRI and positive TBI indices.
Using this more mildly injured group of patients, we were able to identify those ROIs that
remained sensitive using DTI analysis. Table 3-2 illustrates that the genu of the corpus
callsoum, bilateral anterior limb of the internal capsule, anterior corona radiata, and uncinate
fasciculus, left superior longitudinal fasciculus and right cingulum all showed reduced FA
values in at least one patient from this group.

28
Again, the left anterior limb of the internal capsule was most robustly affected, with one
patient showing FA values of greater than 3 SDs below the control mean and two additional
patients showing FA values of between -2.0 and -2.49 SDs. These three patients also had FA
values of between -1.0 and -2.49 SDs in the right anterior limb of the internal capsule.
Regions also showing fairly marked sensitivity were the left uncinate fasciculus (in
which two patients had FA values between -2.0 and -2.49 SDs, and one patient had an FA value
of between -1.0 and -1.49 SDs), followed by the genu of the corpus callosum (with one patient
with an FA value of -2.0 and -2.49 SDs and another with a value in the -1.5 and -1.99 SDs
range). In the right anterior coronal radiata, one patient had an FA value of between -2.0 and -
2.49 SDs (this patient also had an equally reduced FA value in the left anterior corona radiata)
and a second patient had a FA value of -1.0 and -1.49 SDs. Regions more mildly affected were
the left superior longitudinal fasciculus, the right cingulum, and the right uncinate fasciculus.
(III) Examining ROI specificity using MRI and clinically negative patients. Table 3-3
illustrates that the genu of the corpus callosum as well as the right anterior limb of the internal
capsule and right anterior coronal radiata showed no FA reductions in any of the non-TBI
patients. Therefore, these regions showed not only sensitivity to mTBI, but also specificity.
Mild FA reductions (-1.0 and -1.49 SDs) were observed in the left anterior limb of the
internal capsule, left anterior corona radiata, and right cingulum in one patient, suggesting that
these areas might be somewhat less specific and that a higher threshold of FA value would be
needed to discriminate patients from controls in these regions. Even more substantive reductions
were observed in the left superior longitudinal fasciculus (-1.5 and -1.99 SDs) and the uncinate
fasciculus, including a reduction at greater than 3 SDs below the control mean in this region
bilaterally.

29
Chi-square Analysis
The combined TBI groups and the “no TBI” group were significantly different for the
frequencies of patients who had FA values of greater than 1.5 SDs below the control mean (p =
0.012).
Table 2
Mean FA values in Right and Left Sides of 12 ROIs for Younger and Older Control Groups
ROI Younger (N = 8) Older (N = 6)
Genu of corpus callosum 0.571 ± 0.022 0.552 ± 0.019
Splenium of corpus callosum 0.624 ± 0.013 0.604 ± 0.015
Left anterior limb of internal capsule 0.516 ± 0.013 0.505 ± 0.019
Right anterior limb of internal
capsule
0.526 ± 0.016 0.515 ± 0.022
Left anterior corona radiata 0.456 ± 0.031 0.423 ± 0.022
Right anterior corona radiata 0.458 ± 0.027 0.427 ± 0.025
Left cingulum 0.369 ± 0.037 0.378 ± 0.025
Right cingulum 0.388 ± 0.021 0.360 ± 0.016
Left uncinate fasciculus 0.400 ± 0.015 0.425 ± 0.023
Right uncinate fasciculus 0.427 ± 0.027 0.428 ± 0.034
Left superior longitudinal fasciculus 0.420 ± 0.017 0.400 ± 0.026
Right superior longitudinal fasciculus 0.435 ± 0.023 0.403 ± 0.026

30
Table 3-1
The Number of ROIs with FA Values of > 3.0 SDs, 2.5 - 2.99 SDs, 2.0 - 2.49 SDs, and 1.5 - 1.99 SDs, and 1.0 - 1.49 SDs Below the
Age-stratified Control Mean for Confirmed TBI Patients
TBI
Patie
nt
Genu
of CC
Spleniu
m of CC
ALIC_
R
ALIC_L ACR_
R
ACR_
L
UNC_
R
UNC_
L
SLF_R SLF_L CG_R CG_L
P1 2.0-
2.49
N/A 2.5-
2.99
> 3.0 N/A 2.0-
2.49
2.0-
2.49
2.5-
2.99
N/A 1.0-
1.49
P2 N/A N/A 1.5-1.99 1.0-
1.49
2.0-
2.49
> 3 1.5-
1.99
P3 1.5-
1.99
1.0-
1.49
1.5-
1.99
1.0-
1.49
P4
P5 1.5-
1.99
2.5-2.99 1.0-
1.49
Note. N/A: ROIs with microbleeds were excluded

31
Table 3-2
The Number of ROIs with FA Values of > 3.0 SDs, 2.5 - 2.99 SDs, 2.0 - 2.49 SDs, and 1.5 - 1.99 SDs, and 1.0 - 1.49 SDs Below the
Age-stratified Control Mean for TBI Patients with Normal MRI
TBI
Patient
Genu of
CC
ALIC_R ALIC_L ACR_R ACR_L UNC_R UNC_L SLF_R SLF_L CG_R CG_L
P6 1.5-1.99 2.0-2.49 > 3 1.0-1.49 2.0-2.49 1.0-1.49 1.0-1.49
P7 1.0-1.49 1.0-1.49
P8 2.0-2.49 1.0-1.49 2.0-2.49 2.0-2.49 2.0-2.49 1.0-1.49 1.0-1.49 1.0-1.49
P9 2.0-2.49 2.0-2.49 1.0-1.49 1.5-1.99
Table 3-3
The Number of ROIs with FA Values of > 3.0 SDs, 2.5 - 2.99 SDs, 2.0 - 2.49 SDs, and 1.5 - 1.99 SDs, and 1.0 - 1.49 SDs Below the
Age-stratified Control Mean for Non-TBI Patients
TBI
Patient
Genu of
CC
ALIC_R ALIC_L ACR_R ACR_L UNC_R UNC_L SLF_L CG_R
P10 1.5-1.99 1.5-1.99 1.0-1.49
P11 > 3 > 3
P12
P13 1.0-1.49 1.0-1.49
P14

32
Discussion
MTBI is a major public health concern given its high incidence and its clinical
consequences. However, the diagnosis of mTBI is challenging, in large part due to the
insensitivity of the current diagnostic neuroimaging tools for traumatic axonal injury, a
predominant neuropathology of mTBI. Several recent studies suggest that DTI holds promise
for the detection of microscopic axonal injury common in mTBI (Oppenheimer, 1968;
Povlishock, et al, 1983), illustrating its potential as clinical diagnostic tool. The current study
aimed to further examine the utility of DTI for the clinical diagnosis of mTBI.
Sensitivity
In the TBI groups, examinations I and II, FA values were reduced in the genu of the
corpus callosum, anterior limb of the internal capsule, anterior coronal radiate, uncinate
fasciculus, superior longitudinal fasciculus and cingulum. Among these regions, the anterior
limb of the internal capsule demonstrated highest sensitivity, with six of nine patients showing
reduced FA values. This finding is consistent with a small study examining five individual
mTBI cases (Arfanakis, et al., 2002) in which all of the five patients showed reduced FA values.
One group study that included 17 mTBI patients also found that the anterior limb of the internal
capsule was one of the most affected ROIs. This study used the whole brain analysis, and
patients in this study were normal on conventional MRI including T2-weighted fluid-attenuated
inversion recovery images, and gradient-recalled echo T2*-weighted images (Lipton, et al.,
2008).
Our findings of very reduced FA in the genu of the corpus callosum are also consistent
with previous group and frequency studies (Kumar, et al., 2009; Lipton, et al., 2008; Lo, et al.,
2009; Niogi, et al., 2008b; Rutgers, et al., 2008a). Consistent with other studies (Geary, et al.,

33
2010; Mayer, et al., 2010; Niogi, et al., 2008b), the uncinate fasciculus was also highly affected,
although as we discuss below, this region had low specificity for mTBI as well.
The anterior corona radiata was less affected in our sample. Previously, the anterior
corona radiata has shown mixed results. Niogi, et al (2008b) has shown that the anterior corona
radiata was the most affected ROI, with 41 % of the patients showing significantly reduced FA
values, including patients with normal conventional MRI. However, subsequent group studies
failed to find significant group differences in this region (Geary, et al., 2010; Little, et al., 2010).
As with the anterior corona radiata, the superior longitudinal fasciculus and cingulum were also
less sensitive to mTBI in our sample. Although an early group study reported that superior
longitudinal fasciculus was significantly affected by mTBI (Kraus, et al., 2007), subsequent
studies have failed to find significant group differences in the superior longitudinal fasciculus
(Little, et al., 2010; Mayer, et al., 2010). Previous studies showed that the cingulum was less
affected by mTBI compared with the ROIs mentioned above (Niogi, et al., 2008b, Rutgers, et
al., 2008b). Thus, our results were also consistent with these findings.
Specificity
Importantly, we demonstrated specificity of DTI findings in areas that demonstrated
good sensitivity. Using a threshold of 1.0 SD below controls, this included the genu of the
corpus callosum, the right anterior limb of the internal capsule and the right anterior coronal
radiata. For clinical purposes, a threshold of 1.0 SD may not effectively discriminate patients
from controls and a larger SD may be needed for greater specificity. Indeed, when we increased
the threshold to 1.5 SDs below controls, this increased the specificity of the left anterior limb of
the internal capsule and left anterior coronal radiata in addition to that of the three ROIs
mentioned above with only minimal effects on sensitivity in the main ROI predilection sites,
that is the genu of the corpus callosum and anterior limb of the internal capsule bilaterally.

34
Another factor of high importance is the variability of FA within ROIs. It is likely that
those predilection sites for mTBI with the smallest normative control standard deviations will
offer the maximal clinical utility for mTBI diagnosis.
Taken together, these results suggest that for clinical purposes, using an SD of 1.5 in the
genu of the corpus callosum and the anterior limb of the internal capsule
would provide optimum sensitivity and specificity. Ideally, we would employ an algorithm that
would allow us to combine ROIs, for example, one that could permit a higher threshold if only
one ROI was affected, but a lower threshold when two or three ROIs were affected.
Conclusion
The current study, employing a small sample of very carefully selected patients,
demonstrated robust sensitivity and specificity of DTI to mTBI for single case diagnosis of
mTBI. These preliminary data provide support for the clinical potential of DTI. Future research
including a larger sample size and controlling for other demographic variables that may impact
DTI values (such as sex and handedness) is needed to confirm the clinical utility of DTI for
mTBI.

35
CHAPTER 3: REDUCED WHITE MATTER INTEGRITY OF THE
BRIAN MEASURED BY DIFFUSION TENSOR IMAGING IN
PATIENTS WITH SPINAL CORD INJURY
Abstract
The primary objective of this study was to examine whether patients with traumatic spinal cord
injury (SCI) without concomitant TBI (TBI) showed changes in white matter integrity in the
brain at the sub-acute stage using diffusion tensor imaging (DTI). Eight traumatic SCI patients
without concomitant TBI and 15 age- and education-matched healthy control subjects were
included. DTI-derived absolute fractional anisotropy (FA) values as well as computed FA
hemispheric asymmetry scores were used as measures of brain white matter integrity. FA data in
the ROIs placed in the motor and sensory pathways were compared between healthy controls
and patients. FA absolute values did not show significant differences between the two groups
for any ROI. However, the patients demonstrated significantly greater degree of FA asymmetry
in the posterior corona radiata, F = 4.123, p = 0.032, and in the superior corona radiata, F =
3.991, p = 0.035, compared with age matched controls. These results were observed after
controlling for pre-morbid and co-existing medical conditions. Traumatic SCI patients without
concomitant TBI display altered white matter integrity in the brain at the sub-acute stage. FA
asymmetry scores are more sensitive than FA absolute values. Further research will be
necessary to confirm whether the FA asymmetry scores can serve as a potential biomarker of
brain abnormalities secondary to SCI.

36
Introduction
A number of studies over the past decade have documented the pathophysiologic
consequences of spinal cord injury (SCI) in the brain. Animal models have demonstrated altered
synaptic structures (Kim, et al., 2006), cell atrophy (Wannier, et al., 2005) apoptotic cell death
in the primary motor cortex (Hains, et al., 2003) as well as functional reorganization in the
primary somatosensory cortex (Endo, et al., 2007). In the human brain, structural and
functioning imaging studies have also revealed brain changes following SCI. Reduced gray
matter volume has been demonstrated in the primary motor cortex and frontal areas (Wrigley, et
al., 2009) and somatosensory and posterior parietal cortices (Jurkiewicz, et al., 2006), and
alterations in brain function have been reported in the motor and somatosensory cortices
(Jurkiewicz, et al., 2007; Mikulis, et al., 2002).
Most of the studies investigating the effects of SCI on the brain have examined gray
matter structures. Relatively few studies have investigated axonal or white matter changes, and
of these, findings have been equivocal. The earliest studies used voxel-based morphometry
methods and examined both gray and white matter; here, the authors observed no changes in
white (or gray) matter (Crawely, et al., 2004; Jurkiewicz, et al., 2006). A further four human
studies examined white matter changes after SCI using DTI (Guleria, et al., 2008; Gustin, et al.,
2010; Wei, et al., 2008; Wrigley, et al., 2009).
DTI methods can detect subtle changes in white matter such as axonal and myelin
damage (Buki & Povlishock, 2006) as well as changes in the extracellular matrix (Pierpaoli, et
al., 2001) and thus may be more sensitive than voxel-based morphometory to white matter
changes following SCI. Gustin et al. (2009) examined mean diffusivity in the entire brain, and
found no significant group differences between SCI patients and controls in white matter. Wei et
al. (2008) examined FA in three groups of patients: those with SCI and confirmed TBI, those
with SCI and no TBI, and a group of uninjured controls. Again, they found no differences

37
between the SCI-only group and controls.
In contrast, the studies of Guleria et al. (2008) and Wrigley et al. (2009) obtained
positive findings in white matter. Both studies observed changes in the corticospinal tract,
including the corona radiata, the posterior limb of the internal capsule, the pons and the
pyramids in addition to the cerebral peduncle (Guleria et al., 2008). Wrigley et al. (2009)
additionally found changes in frontal regions, including the primary motor cortex, and the
medial prefrontal and anterior cingulate cortices; parietal regions such as SI and precuneus
cortices, as well as the superior cerebellar cortex.
An alternative explanation for these positive findings, however, is the presence of TBI
(TBI). In studies examining brain changes in traumatic SCI patients, whereby an external insult
causes damage to the spinal cord (LaPlaca, Simon, Prado, & Cullen, 2007), one methodological
challenge is the presence of concomitant TBI (Iida, et al., 1999; Richards, Brown, Hagglund, et
al., 1988). For example, in the study examining the incidence of TBI in SCI, Tolonen et al.
(2007) found that 23 of 31 SCI patients had evidence of TBI. In some studies, TBI has been
associated in particular with cervical SCI (Go, Devivo, & Richards, 1995; Watanabe, Zafonte, &
Lairson, 1999).
The causes of SCI were not reported in the study by Wrigley et al. (2008). The patients
in the Guleria et al. (2008) study were traumatic SCI patients. The authors reported that their
patients showed no evidence of TBI on MRI. However, conventional MRI is known to display
limited sensitivity to traumatic axonal injury after brain injury (Hayes & Dixon, 1994; Saatman,
et al., 2008), and the study did not include T2* gradient-recalled echo or fluid attenuated
inversion recovery sequences, which are considered to be the most sensitive of the conventional
MRI protocols for traumatic axonal injury (Huisman, et al., 2003; Niogi & Mukherjee, 2010).
As well, patients in the study were at elevated risk of TBI because SCIs were at the cervical
level, and injuries were caused by motor vehicle accidents and falls, which are associated with

38
acceleration and deceleration forces, including rotational ones that are known to induce
traumatic axonal injury (Geddes, et al., 2000).
Considered together, it is difficult to conclusively rule out the presence of TBI in either
of the above studies, and as these studies obtained positive findings in regions that have also
shown positive findings in TBI studies, including the corona radiata (Guleria, et al., 2008;
Mayer, et al., 2010; Wrigley, et al., 2009), the posterior limb of the internal capsule (Guleria, et
al., 2008; Inglese, et al., 2005; Wrigley, et al., 2009), and the cerebral peduncle (Guleria, et al.,
2008; Rutgers, et al., 2008b), it is possible that the positive findings observed in these two
studies are attributable to TBI. Thus, further research into the question of white matter changes
following SCI is warranted.
The current study was designed to examine changes in white matter integrity after
traumatic SCI where the combination of clinical and neuroradiological information would
enable us to rule out concomitant TBI with some degree of confidence: We examined clinical
records detailing the precise mechanism and circumstances of injury to exclude patients in
which brain injury was possible. We also employed a conventional MRI protocol designed to
detect white matter pathology after TBI: T2*-weighted gradient-recalled echo, along with T1-
weighted spin echo and T2-weighted fluid-attenuated inversion recovery sequences.
We included in our study a somewhat novel approach to measuring FA abnormalities.
Previous studies have typically reported group-wise absolute differences in FA in a priori ROIs.
However, Guleria et al. (2008) also noted significant hemispheric differences in FA values in
SCI patients that were not present in controls. In another recent study, abnormal left-right
hippocampal volume differences were observed in a patient with TBI, even though each volume
on its own fell within the normal range (MacDonald, et al., 2008). These findings suggest that
the degree of asymmetry may be a useful index of neuropathology, particularly where brain
changes are subtle.

39
Thus, the study tested whether SCI would affect the white matter tracts of the brain in
sub-acute SCI patients. We hypothesized that (1) patients would show significantly reduced FA
values relative to controls in the selected ROIs, and (2) patients would show significantly
greater degree of asymmetries in the selected homologous ROIs. We compared absolute FA
values in a series of ROIs used in past studies and their degree of hemispheric asymmetry
between patients and matched controls and statistically controlled for potentially confounding
medical co-morbidities.
Methods
Subjects
SCI group
Patients were selected from a larger on-going study on the Spinal Cord Rehabilitation
Program at Toronto Rehabilitation Institute examining prevalence of TBI in SCI between June
2006 and May 2009. Inclusion criteria for the larger study were as follows: (1) 18 to 55 years of
age; (2) between about two and six months post-injury; and (3) able to provide informed
consent. There were 82 patients in the larger study. The following inclusion criteria were
additionally applied for the current study: no previous history of neurologic disease including
TBI and SCI; no extensive history of contact sports with high concussion risk, such as hockey,
football and boxing; and no evidence of concomitant TBI, operationalized as (1) normal
findings on MRI T2*-weighted gradient recalled echo and T2-weighted fluid-attenuated
inversion recovery imaging; (2) no loss of consciousness or posttraumatic amnesia at the time of
injury or thereafter (note that a recent study of mild TBI demonstrated that patients without loss
of consciousness or post-traumatic amnesia showed no differences from controls in FA at one-
month post-injury (Zhang, et al., 2010); and, (3) after a thorough chart review for each patient, a
consensus by two experienced neuropsychologists that circumstances of injury were not

40
compatible with acquired brain injury (e.g., no evidence of hypoxia, no injury with strong
acceleration/deceleration forces, with the exception of one patient who fell from 18 feet and
landed initially on his back, and subsequently hit his head). On the basis of these criteria, eight
patients (seven males) were included in the current study. Their demographic and clinical
characteristics are shown in Table 1.
Control group
A control group consisting of 15 healthy subjects (12 males) was drawn from the local
community (see Table 1). Inclusion criteria and exclusion criteria for the control subjects were
the same as those for the current study. Healthy control subjects with incidental signal
abnormalities on MRI were excluded from the study (N=4).
Materials
MRI Protocol
Acquisition. Whole brain conventional MRI and DTI were acquired on a 3Tesla (3T)
General Electric Signa-EXCITE scanner (GE Healthcare, Waukesha, WI, USA) equipped with
an eight-channel head coil. DTI was acquired with diffusion-weighted spin-echo single-shot
echo planar imaging with diffusion encoding in 15 noncolinear directions. The sequence
parameters were as follows: TR = 10,000 ms; TE = 84 ms; field of view = 240 mm2; matrix =
128 x 128 mm; the number of slices = 45, slice thickness = 3 mm without gaps; b value = 1000
s/mm2. Parallel imaging was employed using the Array Spatial Sensitivity Encoding Technique
with an acceleration factor of 2. DTI for all subjects were acquired in the axial plane. One
additional image with no diffusion weighting was also acquired. The DTI scans were repeated
three times to increase signal to noise ratio. The total DTI acquisition time was approximately 8
minutes. The following conventional 3T MR sequences were acquired: (1) axial three-

41
dimensional (3D) inversion recovery fast spoiled gradient-recalled echo T1-weighted images
(TR = 7.9 ms, TE = 3.1 ms, TI = 450 ms, flip angle = 12º) with 220 mm2 field of view, 166 1.0-
mm contiguous partitions at a 256 x 256 matrix; (2) axial T2-weighted fluid-attenuated
inversion recovery images (TR = 8652, TE = 136.1 to 146, TI = 2250 ms) with 220 mm2 field of
view, 4 mm slice thickness, 28 slices, and 384 x 224 matrix (3) axial gradient-recalled echo
T2*-weighted images (TR = 600, TE =25, flip angle of 45º) with 220 mm2 field of view, 45 or
46 slices, 3 mm slice thickness, and 384 x 224 matrix.

42
Table 1
Demographic and Clinical Characteristics of Subjects
Groups Sex Age Years
of
Education
Injury Type SCI
Level/
Severity
Days between
Injury and MRI
Medical Conditions Blow to
Head
Patients
Full SCI group
1 F 41 16 Fall T12/Inc 59 Bipolar disorder No
2 M 20 12 MVA C7/Inc 86 No
3 M 31 12 Fall T12/Inc 54 No
4 M 39 14 MVA T6/Inc 74 No
5 M 33 13 MVA C4,5/C 147 Migraine,
Depression,
Drug dependence
No
6 M 19 12 Fall T12/Inc 68 No
7 M 50 18 Fall T12/Inc 88 Impaired glucose
tolerance
Yes
8 M 29 10 Sports T12/Inc 85 No
Mean ± SD 30.6 ± 10.4 13.2 ± 2.3 87.6 ± 33.8
Controls
Mean ± SD 14 (3F) 32.5 ± 11.2 16.1 ± 2.6
F: female, M: male, MVA: motor vehicle accident, T: thoracic, C: cervical

43
MRI Data Analysis
Evaluation of conventional MRI
Conventional MRI images were qualitatively evaluated by an experienced
neuroradiologist (D. M.) blinded to DTI findings and clinical ratings. The evaluation included
classification of all visible lesions based on their signal characteristics.
DTI processing
Imaging data were processed offline using FSL tools from the FMRIB software library
(FSL, http://www.fmrib.ox.ac.uk/; Smith, et al., 2004; Woolrich, et al., 2009). FMRIB‟s
diffusion toolbox was used to correct motion and eddy current distortion with b = 0 as reference.
An average set of DTI images was generated from the three sets of DTI data. Non-brain tissue
of the averaged DTI set was removed using brain extraction tool (Smith, 2002), and FA maps
were derived using DTIfit. The images from all subjects were nonlinearly transformed to a
standard space (Andersson, et al., 2007a, 2007b) by normalizing them to a 1x1x1 mm common
template, the International Consortium of Brain Mapping-DTI-81 (ICBM-DTI-81; Mori, et al.,
2005). ICMB-DTI-81 is white matter atlas in sterotaxic coordinates based on DTI data from 81
healthy subjects (42 males and 39 females with the mean age of 38.63 raging from 18 to 59
years; right-handed) and its white matter parcellation maps include 50 manually segmented
white matter structures. Consistent with previous studies on the current topic (Guleria, et al.,
2008; Wrigley, et al., 2009), we chose FA as our primary diffusion measure.
Region of interest (ROI) analysis
The white matter parcellation maps were superimposed on normalized subject data
where 3D ROI analyses were performed for the calculation of FA values. The following white
matter structures were selected based on previous research investigating brain damage

44
secondary to SCI (Glueria, et al., 2008; Wrigley, et al., 2009): corona radiata including superior
corona radiata and posterior corona radiata; internal capsule including anterior limb of internal
capsule and posterior limb of internal capsule; and cerebral peduncle. The selected white matter
parcellation maps are displayed in Fig 1. Because we used the white matter parcellation maps
whose divisions of structures are arbitrary (Mori, et al., 2008), and there is no white matter
parcellation maps particularly for the genu of the internal capsule, we included the anterior limb
of the internal capsule. The FA values in the right and left hemispheres of all the structures were
examined separately, resulting in absolute FA scores in each of the 10 ROIs and 5 asymmetry
scores.

45
Figure 1. White matter parcellation maps for FA analysis. A. cerebral peduncle; B. anterior limb
of internal capsule; C. posterior limb of internal capsule; D. superior corona radiata; E. superior
corona radiata; F. posterior corona radiata; G. posterior corona radiata.
Statistical Analysis
Mean absolute FA values and mean computed FA asymmetry scores for each group for
each ROI were analyzed using multivariate analysis of covariance (MANCOVA), controlling
for the effects medical co-morbidities of the patients (see Table 1). FA hemispheric asymmetry
scores between the right and left homologous ROIs were calculated for each subject as follows:
FA asymmetry = (higher FA – lower FA)/[(higher FA + lower FA)/2]. This allowed us to test
for differences in FA asymmetry between our groups without regard for lateralization
differences (i.e. left greater than right or vice-versa).

46
Results
The two groups were matched on age (30.6 ± 10.4 vs 32.5 ± 11.2 years, p = 0.95).
However, they were significantly different on years of education (13 ± 2.3 vs 16 ± 2.6 years, p =
0.02). Note that post -hoc analyses showed that were no correlations between years of education
and FA values for the controls in any of the ROIs, with the exception of the left anterior limb of
internal capsule, r = -0.637, p = 0.048 in the controls, which indicated that higher education was
associated with lower FA values.
There was no significant difference in mean FA values observed between control and
patient groups for any ROI. Significant between-group differences were observed in the
hemispheric asymmetry scores in the superior corona radiata, F = 3.991, p = 0.035, and
posterior corona radiata, F = 4.123, p = 0.032. We additionally presented individual SCI
asymmetric data and their SDs relative to control mean in the superior corona ratidata and
posterior corona radiata (Table 2). Seven of the eight patients had asymmetry of greater than 1.0
SD relative to the control mean in either structure or both structures.

47
Table 2
Mean Asymmetric Scores (%) of Controls as well as Individual Patients’ Asymmetric Scores
(%) and the Standard Deviations Relative to Control Mean in the Superior Corona Radiata and
Posterior Corona Radiata
Superior corona radiata Posterior corona radiata
Control mean (%)
± SD 2.08 ± 1.65 3.51 ± 2.22
Patient Asymmetric
scores (%) SD relative to
control mean Asymmetric
scores (%) SD relative to
control mean
1 4.17 1 – 1.49 6.49 1 -1.49
2 6.30 2.5 – 2.99 11.18 > 3
3 1.55 3.11 4 4.63 1.5 – 1.99 4.86 5 9.45 > 3 3.59 6 2.27 6.57 1 – 1.49
7 2.31 10.43 > 3
8 3.84 1 – 1.49 7.10 1.5 – 1.99
Discussion
Brain FA is altered following SCI in patients without TBI
To our knowledge, this is the first study to demonstrate structural brain changes using
DTI methods in a group of traumatic SCI patients who were carefully screened for concomitant
TBI on clinical report and conventional neuroimaging. Our findings are consistent with previous
reports (Guleria, et al., 2008; Wrigley, et al., 2009), suggesting that SCI is associated with
changes in white matter integrity in the brain as measured using diffusion imaging methods. We
have extended previous research by using extensive clinical and imaging information to rule out
concomitant TBI and previous or co-morbid head injury as an alternative explanation for the
DTI changes.

48
FA asymmetry is a sensitive marker of brain changes following SCI
For group-wise comparisons of FA in a priori ROIs, we utilized a novel diffusion
imaging marker of brain damage following SCI: FA asymmetry. FA asymmetry was used to
characterize the relative differences between SCI and control groups in homologous ROIs.
Guleria and colleagues (2008) had previously observed FA asymmetry in a group of SCI
patients. In a related approach, hemispheric asymmetry in hippocampal volumes was
considered to be a marker of neuropathological change in TBI (MacDonald, et al., 2008). Here,
FA asymmetry proved more sensitive than absolute FA values for identifying brain changes in
SCI.
Contrary to the reports of Guleria et al. (2008) and Wrigley et al. (2009), we did not
observe differences on standard group-wise comparisons of FA in a priori ROIs. This is likely
attributable to differences in the composition of the SCI groups. While these previous studies
used only complete injury patients, our group was comprised of a majority (seven of eight) of
patients with incomplete injury. Thus variability in the localization and extent of FA reductions
would be greater in our sample, potentially obscuring group-wise differences. In contrast, a
relative measure of lateralized change in FA, as we have derived here, should be more sensitive
in this population. Indeed this was the case. These data suggest that FA asymmetry may be a
more sensitive marker of white matter changes in the brain following incomplete SCI injury.
Further large-scale, prospective studies will be needed to correlate FA asymmetry scores with
behavioral and functional data to confirm whether this marker has potential clinical utility as a
marker for brain changes in incomplete SCI.
We found significant group differences in the superior corona radiata and posterior
corona radiata. The significant finding in the superior corona radiata was consistent with both of
the previous studies (Guleria et al., 2008; Wrigley, et al., 2009). ROIs in the sensory pathway
including the posterior corona radiata were not examined by Guleria et al. (2008). Although

49
Wrigley, et al. (2009) did not report significant group difference in the posterior corona radiata
in particular, they reported abnormal FA values in primary sensory cortex and the precuneus,
suggesting that parietal regions adjacent to posterior corona radiata were affected. Consistent
with these data, gray matter atrophy was also reported by Jurkiewicz, et al. (2006) in primary
sensory and posterior parietal cortices. These findings suggest that posterior parietal cortices as
well as adjacent and underlying white matter may be impacted by SCI.
It was surprising that we did not observe any changes in the lower white matter
structures (i.e., posterior limb of the internal capsule and cerebral peduncle). This might be due
to the analysis method that we used. The FA values in smaller ROIs such as the posterior limb
of the internal capsule might have been confounded by the partial volume effect using the white
matter parcellation maps. Another possible explanation was that MRI data in patients tend to be
noisy in general resulting in greater asymmetries in those regions.
Conclusion
We have demonstrated white matter in the brain is altered following SCI, even in the
absence of clinical or conventional neuroimaging evidence of a TBI. Greater hemispheric
asymmetry using a standard measure of diffusion (FA) within the posterior corona radiata and
the superior corona radiata differentiated our „clean‟ SCI sample from a group of closely
matched control subjects. FA asymmetry appears to be a promising neural marker of structural
brain changes following incomplete SCI, even in the absence of standard clinical and
neuroradiological evidence of brain injury.
Future studies with larger samples of SCI patients, carefully screened for TBI, will be
necessary to characterize the behavioural and functional impact of structural brain changes
following SCI. Also, analysis methods such as the ROI analysis by manually placing
standardized circles, squares, or ovals over specific white matter (Nucifora, et al., 2007) or the

50
voxel-based analysis using the tract-based spatial statistics (Smith, Jenkinso, Johansen-Berg, et
al., 2006) may be used to reduce the partial volume effect.

51
CHAPTER 4: GENERAL DISCUSSION
DTI is a powerful tool to investigate subtle pathological changes in the brain as it can
provide microstructual and physiological information about white matter tracts (Mukherjee, et
al., 2008). Using this technology, we examined white matter changes secondary to TBI and SCI
in two separate studies. The purpose of the first study was to examine the utility of DTI for
single case diagnosis of mild TBI. This study employed people with SCI as a convenience
population, given the high prevalence of TBI in this clinical population. The second study
sought to examine the sub-acute effects of SCI on white matter tissue in the brains of individuals
without direct injury to the brain.
In the first study, we examined two groups of TBI patients at the mild end of the severity
spectrum (a total of nine patients), one group with TBI confirmed on imaging, the other – a
milder group – with normal MRI but positive TBI clinical indices (i.e., Glasgow Coma Scale,
posttraumatic amnesia, or loss of consciousness). The aim was to determine the brain regions
where DTI was maximally sensitive. We then examined a group of five patients from the same
larger sample, without any evidence of TBI (i.e., normal imaging and no positive TBI indices)
in order to demonstrate specificity of the DTI for the detection of mTBI in the maximally
sensitive ROIs. In an effort to ensure that any observed differences between groups were
attributable to mTBI and not the effects of aging, we included two age-stratified control groups
and each patient was examined using his/her closely age-matched group. We found that the
anterior limb of the internal capsule was highly sensitive and specific to mild TBI, followed by
the genu of the corpus callosum and to a lesser extent, the anterior coronal radiata. While the
uncinate fasciculus was sensitive to mTBI in our sample, this ROI was not specific. Our
findings provide preliminary proof of principal evidence that DTI can be used to sensitively and
specifically diagnose mTBI in individual cases.

52
In the second study, we examined brain white matter in eight patients with incomplete
sub-acute SCI who were carefully screened for concomitant TBI. We found that SCI was
associated with changes in brain white matter. More specifically, SCI patients showed
significantly greater hemispheric FA asymmetry than control subjects even though separate
examinations of right and left homologous structures showed no between-group differences. The
changes in white matter were observed in the superior corona radiata and posterior corona
radiata. This study was the first study to show white matter changes using the degree of
hemispheric FA asymmetry as an index in this population. The findings suggest that
hemispheric asymmetry may be a useful biomarker for detecting subtle white matter changes.
Key Limitations
MTBI Study
Niogi and Mukherjee (2010) have recently argued against the clinical utility of ROI-
based approach. Nonetheless, we argue that maximal sensitivity and specificity are most likely
to be attained by identifying patterns of FA change in a single region (i.e., a univariate
approach) or a constrained number of brain regions (i.e., a multi-variate approach) with known
susceptibility to damage from the mechanical forces in TBI (Besenski, 2002). However, before
DTI can be introduced clinically using this approach, its sensitivity and specificity will need to
be verified on a larger population than the one employed in this study.
Furthermore, as individual case analysis will require normative data, issues such as
feasibility, cost effectiveness, reproducibility (Bonekamp, et al., 2003; Mukherjee, Chung,
Berman, Hess, & Henry, 2008; Ozturk, et al., 2008; Pfefferbaum, Adalsteinsson, & Sullivan,
2003) as well as other technical challenges (Assaf & Pasternak, 2008) will need to be addressed.
It is likely that normative data will need to be collected separately for each platform using this
approach.

53
SCI Study
We carefully screened our patients to exclude concomitant TBI. However, there is no
gold standard for determining absence of mTBI. Further study may be required to replicate our
findings in SCI patients whose injury causes were unrelated to trauma or trauma that does not
cause TBI (e.g., blunt force to the spinal cord). In addition, functional data such as the American
Spinal Cord Injury Association scores coinciding with the time of brain scans were not obtained,
as this was not part of the larger study from which our patients were drawn. Prospective studies
will be needed to associate DTI findings and functional data.
Clinical Implications
Clinical diagnosis of mild TBI is needed in order to ensure that treatment or intervention
ensues, where necessary, as mTBI gives rise to a range of cognitive, somatic and emotional
symptoms. These include attention and memory problems; headache and dizziness; and
symptoms of anxiety and depression (Carroll, et al. 2004; Kelly & Rosenberg, 1997; King,
1997), which can be chronic in some patients (Alexander, 1995; Cicerone & Kalmar, 1995;
Dikmen, et al., 1986; Kushner, 1998; Nuwer, et al., 2005). Improved diagnosis can ensure that
patients withdraw from activities where cognitive impairment would elevate the risk of further
injury to self (Nuwer, et al., 2005; Saunders & Harbaugh, 1984) or others. In addition, objective
evidence of mTBI using DTI imaging can provide valuable data to adjudicate legal and
insurance issues for the patients.
In the SCI study, we observed only loss of white matter integrity in the brain after SCI.
Further research is needed to ascertain whether the changes to the white matter of the brain in
the current study have behavioural consequences. If negative behavioural consequences are
observed, then interventions to avert these secondary brain effects will need to be undertaken.

54
References
Adams, J. H., Doyle, D., Ford, I., Gennarelli, T. A., Graham, D. I., & McLellan, D. R. (1989).
Diffuse axonal injury in head injury: definition, diagnosis and grading. Histopathology,
15(1), 49-59.
Adams, J. H., Graham, D. I., Gennarelli, T. A., & Maxwell, W. L. (1991). Diffuse axonal injury
in non-missile head injury. J Neurol Neurosurg Psychiatry, 54(6), 481-483.
Agarwal, N., Port, J. D., Bazzocchi, M., & Renshaw, P. F. Update on the use of MR for
assessment and diagnosis of psychiatric diseases. Radiology, 255(1), 23-41.
Alexander, A. L., Lee, J. E., Lazar, M., & Field, A. S. (2007). Diffusion tensor imaging of the
brain. Neurotherapeutics, 4(3), 316-329.
Alexander, M. P. M. D. (1995). Mild TBI: Pathophysiology, natural history, and clinical
management. Neurology, 45(7), 1253-1260.
Andersson, M., Jenkinson, M., & Smith, S. (2007a). Non-linear optimisation. FMRIB technical
report TR07JA1 Retrieved 0922, 2010, from www.fmrib.ox.ac.uk/analysis/techrep
Andersson, M., Jenkinson, M., & Smith, S. (2007b). Non-linear registration. aka Spatial
normalization. FMRIB technical report TR07JA2 Retrieved 0922, 2010, from
www.fmrib.ox.ac.uk/analysis/techrep
Arciniegas, D. B., Held, K., & Wagner, P. (2002). Cognitive Impairment Following TBI. Curr
Treat Options Neurol, 4(1), 43-57.
Arfanakis, K., Haughton, V. M., Carew, J. D., Rogers, B. P., Dempsey, R. J., & Meyerand, M.
E. (2002). Diffusion tensor MR imaging in diffuse axonal injury. AJNR Am J
Neuroradiol, 23(5), 794-802.
Assaf, Y. & Pasternak, O. (2008). Diffusion tensor imaging (DTI)-based white matter mapping
in brain research: A review. J Mol Neuroci, 34, 51-61.
Bammer, R. (2003). Basic principles of diffusion-weighted imaging. Euro J Radiol, 45, 169-
184.
Baptiste, D. C., Tighe, A., & Fehlings, M. G. (2009). Spinal cord injury and neural repair: focus
on neuroregenerative approaches for spinal cord injury. Expert Opin Investig Drugs,
18(5), 663-673.
Basser, P. J. (1995). Inferring microstructural features and the physiological state of tissues from
diffusion-weighted images. NMR Biomed, 8(7-8), 333-344.
Basser, P. J., Mattiello, J., & Le Bihan, D. (1994). MR diffusion tensor spectroscopy and
imaging. Biophysical Journal, 66, 259-267.
Belanger, H. G., Vanderploeg, R. D., Curtiss, G., & Warden, D. L. (2007). Recent neuroimaging
techniques in mild TBI. J Neuropsychiatry Clin Neurosci, 19(1), 5-20.

55
Bendlin, B. B., Ries, M. L., Lazar, M., Alexander, A. L., Dempsey, R. J., Rowley, H. A., et al.
(2008). Longitudinal changes in patients with TBI assessed with diffusion-tensor and
volumetric imaging. Neuroimage, 42(2), 503-514.
Besenski, N. (2002). Traumatic injures: imaging of head injuries. Cur Radiol, 12, 1237-1252.
Bhagat, Y. A., Emery, D. J., Shuaib, A., Sher, F., Rizvi, N. H., Akhtar, N., et al. (2006). The
relationship between diffusion anisotropy and time of onset after stroke. J Cereb Blood
Flow Metab, 26(11), 1442-1450.
Bigler, E. D. (2004). Neuropsychological results and neuropathological findings at autopsy in a
case of mild TBI. J Int Neuropsychol Soc, 10, 794-806.
Blumbergs, P. C., Scott, G., Manavis, J., Wainwright, H., Simpson, D. A., & McLean, A. J.
(1995). Topography of axonal injury as defined by amyloid precursor protein and the
sector scoring method in mild and severe closed head injury. J Neurotrauma, 12(4), 565-
572.
Bode, R. K., Heinemann, A. W., & Semik, P. (2000). Measurement properties of the Galveston
Orientation and Amnesia Test (GOAT) and improvement patterns during inpatient
rehabilitation. J Head Trauma Rehabil, 15(1), 637-655.
Bonekamp, D., Nagae, L. M., Mahaveer, D., Matson, M., Abdalla, W. M. A., Barker, P. B., et
al. (2007). Diffusion tensor Imaging in children and adolescents : reproducibility
hemispheric, and age-related différences. NeuroImage, 34, 733-742.
Borg, J., Holm, L., Cassidy, J. D., Peloso, P. M., Carroll, L. J., von Holst, H., et al. (2004).
Diagnostic procedures in mild TBI: results of the WHO Collaborating Centre Task Force
on Mild TBI. J Rehabil Med(43 Suppl), 61-75.
Bradbury, E. J., King von R., Simmons, L. J., Priestley, J. V., & McMahon, S. B. (1998). NT-3
but not BDNF, prevents atrophy and death of axotomized spinal cord projection neurons.
Euro J Neurosci, 10, 3058-3068.
Bradbury, C. L., Wodchis, W. P., Mikulis, D. J., Pano, E. G., Hitzig, S. L., McGillivray, C. F.,
et al. (2008). TBI in patients with traumatic spinal cord injury: clinical and economic
consequences. Arch Phys Med Rehabil, 89(12 Suppl), S77-84.
Buki, A., & Povlishock, J. T. (2006). All roads lead to disconnection?--Traumatic axonal injury
revisited. Acta Neurochir (Wien), 148(2), 181-193; discussion 193-184.
Carroll, L. J., Cassidy, J. D., Peloso, P. M,, Borg, J., von Holst, H., Holm, L., Paniak, C., Pépin,
M; WHO Collaborating Centre Task Force on Mild TBI. (2004). Prognosis for mild
TBI: results of the WHO Collaborating Centre Task Force on mild TBI. J Rehabil Med,
43(Suppl), 84-105.
Casha, S. Yu, W., & Fehling, M. G. (2001). Oligodendroglial apoptosis occurs along
degenerating axons and is associated with FAS and p75 expression following spinal cord
injury in the rat. Neurosci, 103, 203-218.

56
Cassidy, J. D., Carroll, L. J., Peloso, P. M., Borg, J., von Holst, H., Holm, L., et al. (2004).
Incidence, risk factors and prevention of mild TBI: results of the WHO Collaborating
Centre Task Force on Mild TBI. J Rehabil Med(43 Suppl), 28-60.
Chenevert, T. L., Pipe, J. G., Williams, D. M., & Brunberg, J. A. (1991). Quantitative
measurement of tissue perfusion and diffusion in vivo. Magn Reson Med, 17(1), 197-
212.
Cicerone, K. D., Dahlberg, C., CCC-SLP, Malec, J. F, Langenbahn, D. M., Felicetti, T. Kneipp,
S., et al. (2005). Evidence-based cognitive rehabilitation: Updated review of the
literature from 1998 through 2002. Arch Phys Med Rehabil, 86, 1681-1692.
Cicerone, K. D. & Kalmar, K. (1995). Persistent postconcussion syndrome: The structure of
subjective complaints after mild TBI. J Head Trauma Rehab, 10, 1-17.
Chiu, W-T., Lin, H-C., Lam, C., Chu, S-F, Chiang, Y-S., Tsai, S-H. (2010). Epidemiology of
traumatic spinal cord injury: comparisons between developed and developing countries.
Asia-Pacific J Public Health, 22(1), 9-18.
Crawley, A. P., Jurkiewicz, M. T., Yim, A., Heyn, S., Verrier, M. C., Fehlings, M. G., et al.
(2004). Absence of localized grey matter volume changes in the motor cortex following
spinal cord injury. Brain Res, 1028(1), 19-25.
Crowe, M. J., Bresnahan, J. C., Shuman, S. L., Masters, J. N., & Beattie, M. S. (1997). Nat Med,
3(1), 73-76.
Dikmen, S., Machmer, J., Winn, R., & Temkin, N. (1995). Neuropsychological outcome at 1-
year post head injury. Neuropsychol, 9(1), 80-90.
Duhaime, A. C., Eppley, M., Margulies, S., Heher, K. L., & Bartlett, S. P. (1995). Crush injuries
to the head in children. Neurosurgery, 37(3), 401-406; discussion 407.
Ellemberg, D., Henry, L. C., Macciocchi, S. N., Guskiewicz, K. M., & Broglio, S. P. (2009).
Advances in sport concussion assessment: from behavioral to brain imaging measures. J
Neurotrauma, 26(12), 2365-2382.
Emery, E., Aldana, P., Bunge, M. B., Puckett, W., Srinivasan, A., Keane, R. W., et al. (1998).
Apoptosis after traumatic human spinal cord injury. J Neurogurg, 89, 911-920.
Endo, T., Spenger, C., Tominaga, T., Brene, S., & Olson, L. (2007). Cortical sensory map
rearrangement after spinal cord injury: fMRI responses linked to Nogo signalling. Brain,
130(Pt 11), 2951-2961.
Fait, P., McFadyen, B. J., Swaine, B., & Cantin, J. F. (2009). Alterations to locomotor
navigation in a complex environment at 7 and 30 days following a concussion in an elite
athlete. Brain Inj, 23(4), 362-369.
Field, A. S., Hasan, K., Jellison, B. J., Arfanakis, K., & Alexander, A. L. (2003). Diffusion
tensor imaging in an infant with traumatic brain swelling. AJNR Am J Neuroradiol,
24(7), 1461-1464.

57
French, L. M. & Parkinson, G.W. (2008). Assessing and treating veterans with TBI. J Clin
Psychol, 64(8). 1004-1013.
Garnett, M. R., Blamire, A. M., Rajagopalan, B., Styles, P., & Cadoux-Hudson, T. A. D. (2000).
Evidence for cellular damage in normal-appearing white matter correlates with injury
severity in patients following TBI: A magnetic resonance spectroscopy study. Brain,
123, 1403-1409.
Geary, E. K., Kraus, M. F., Pliskin, N. H., & Little, D. M. Verbal learning differences in chronic
mild TBI. J Int Neuropsychol Soc, 16(3), 506-516.
Geddes, J. F., Whitwell, H. L., & Graham, D. I. (2000). Traumatic axonal injury: practical
issues for diagnosis in medicolegal cases. Neuropathol Appl Neurobiol, 26(2), 105-116.
Gennarelli, T. A., Thibault, L. E., Adams, H. J., Graham, D. I., Thompson, C. J., & Marcincin,
R. P. (1982). Diffuse axonal injury and traumatic coma in the primate. Annals of
Neurology, 12(6), 564-574.
Go, B. K., Devivo, M. J., & Richards, J. S. (1995). The epidemiology of spinal cord injury. In S.
L. Stover, J. A. DeLisa & G. G. Whiteneck (Eds.), Spinal cord injury: clinical outcomes
from the model systems (pp. 21-51). Gaithersburg, MD: Aspen Publishers.
Granziera, C., DaSilva, A. F., Snyder, J., Tuch, D. S., & Hadjikhani, N. (2006). Anatomical
alterations of the visual motion processing network in migraine with and without aura.
PLoS Med, 3(10), e402
Green, H. A., Pena, A., Price, C. J., Warburton, E. A., Pickard, J. D., Carpenter, T. A., et al.
(2002). Increased anisotropy in acute stroke: a possible explanation. Stroke, 33(6), 1517-
1521.
Green, R., Koshimori, Y., & Turner, G. Research digest. Understanding the organic basis of
persistent complaints in mTBI: findings from functional and structural neuroimaging.
Neuropsychol Rehabil, 20(3), 471-478.
Griffin, J. W., George, R., Lobato, C., Tyor, W. R., Yan, L. C., & Glass, J. D. (1992).
Macrophage responses and myelin clearance during Wallerian degeneration: relevance
to immune-mediated demyelination. J Neuroimmunol, 40(2-3), 153-165.
Gulani, V. & Sundgren, P. C. (2006). Diffusion tensor magnetic resonance Imaging. J
Neuroophthalmol, 26(1), 51-60.
Guleria, S., Gupta, R. K., Saksena, S., Chandra, A., Srivastava, R. N., Husain, M., et al. (2008).
Retrograde Wallerian degeneration of cranial corticospinal tracts in cervical spinal cord
injury patients using diffusion tensor imaging. J Neurosci Res, 86(10), 2271-2280.
Gustin, S. M., Wrigley, P. J., Siddall, P. J., & Henderson, L. A. Brain anatomy changes
associated with persistent neuropathic pain following spinal cord injury. Cereb Cortex,
20(6), 1409-1419.

58
Hains, B. C., Black, J. A., & Waxman, S. G. (2003). Primary cortical motor neurons undergo
apoptosis after axotomizing spinal cord injury. J Comp Neurol, 462(3), 328-341.
Hannay, H. J., Howieson, D. B., Loring, D. W., et al. (2004). Neuropathology for
neuropsychologists. In M. D Lezak, D. B. Howieson, D. W. Loring (Eds.),
Neuropsychological Assessment (pp. 157-285). New York: Oxford University Press.
Hayes, R. L., & Dixon, C. E. (1994). Neurochemical changes in mild head injury. Semin Neurol,
14(1), 25-31.
Himes, B. T., Goldberger, M. E., & Tessler, A. (1994). Grafts of fetal central nervous system
tissue rescue axontomized Clarke‟s nucleus neurons in adult and neonatal operates. J
Comp Neurol, 339, 117-131.
Hofman, P. A., Stapert, S. Z., van Kroonenburgh, M. J., Jolles, J., de Kruijk, J., & Wilmink, J.
T. (2001). MR imaging, single-photon emission CT, and neurocognitive performance
after mild TBI. AJNR Am J Neuroradiol, 22(3), 441-449.
Huisman, T. A., Sorensen, A. G., Hergan, K., Gonzalez, R. G., & Schaefer, P. W. (2003).
Diffusion-weighted imaging for the evaluation of diffuse axonal injury in closed head
injury. J Comput Assist Tomogr, 27(1), 5-11.
Hurley, R. A., McGowan, J. C., Arfanakis, K., & Taber, K. H. (2004). Traumatic axonal injury:
novel insights into evolution and identification. J Neuropsychiatry Clin Neurosci, 16(1),
1-7.
Iida, H., Tachibana, S., Kitahara, T., Horiike, S., Ohwada, T., & Fujii, K. (1999). Association of
head trauma with cervical spine injury, spinal cord injury, or both. J Trauma, 46(3), 450-
452.
Ingebrigtsen, T., Waterloo, K., Marup-Jensen, S., Attner, E., & Rommer, B. (1998).
Quantification of post-concussion symptoms 3 months after minor head injury in 100
consecutive patients. J Neurol, 245, 609-612.
Inglese, M., Makani, S., Johnson, G., Cohen, B. A., Silver, J. A., Gonen, O., et al. (2005).
Diffuse axonal injury in mild TBI: a diffusion tensor imaging study. J Neurosurg,
103(2), 298-303.
Iverson, G. L. (2005). Outcome from mild TBI. Curr Opin Psychiatr, 18(3), 301-317.
Jurkiewicz, M. T., Crawley, A. P., Verrier, M. C., Fehlings, M. G., & Mikulis, D. J. (2006).
Somatosensory cortical atrophy after spinal cord injury: a voxel-based morphometry
study. Neurology, 66(5), 762-764.
Jurkiewicz, M. T., Mikulis, D. J., McIlroy, W. E., Fehlings, M. G., & Verrier, M. C. (2007).
Sensorimotor cortical plasticity during recovery following spinal cord injury: a
longitudinal fMRI study. Neurorehabil Neural Repair, 21(6), 527-538.
Kelly, J. P. & Rosenberg, J. H. (1997). Diagnosis and management of concussion in sports.
Neurology, 48(3), 575-580.

59
Kim, B. G., Dai, H. N., McAtee, M., Vicini, S., & Bregman, B. S. (2006). Remodeling of
synaptic structures in the motor cortex following spinal cord injury. Exp Neurol, 198(2),
401-415.
King, N. (1997). Mild head injury: Neuropathology, sequelae, measurement and recovery.
British Journal of Clinical Psychology, 36(2), 161-184.
King, N. S., Crawford, S., Wenden, F. J., Moss, N. E., & Wade, D. T. (1995). The Rivermead
Post Concussion Symptoms Questionnaire: a measure of symptoms commonly
experienced after head injury and its reliability. J Neurol, 242(9), 587-592.
Kinoshita, T., Moritani, T., Hiwatashi, Akio, Wang, H. Z., Shrier, D. A., Numaguchi, Y., &
Westesson, P-L. A. (2005). Conspicuity of diffuse axonal injury lesions on diffusion-
weighted MR imaging. Euro J Radiol 56, 5-11.
Koda, M., Murakami, M., Ino, H., Yoshinaga, K., Ikeda, O., Hashimoto, M., et al. (2002).
Brain-derived neurotrophic factor suppresses delayed apoptosis of oligodendrocytes after
spinal cord injury in rats. J Neurotrauma, 19(6), 777-785.
Kodl, C. T., Franc, D. T., Rao, J. P., Anderson, F. S., Thomas, W., Mueller, B. A., et al. (2008).
Diffusion tensor imaging identifies deficits in white matter microstructure in subjects
with type 1 diabetes that correlate with reduced neurocognitive function. Diabetes,
57(11), 3083-3089.
Kraus, M. F., Susmaras, T., Caughlin, B. P., Walker, C. J., Sweeney, J. A., & Little, D. M.
(2007). White matter integrity and cognition in chronic TBI: a diffusion tensor imaging
study. Brain, 130(Pt 10), 2508-2519.
Kumar, R., Gupta, R. K., Husain, M., Chaudhry, C., Srivastava, A., Saksena, S., et al. (2009).
Comparative evaluation of corpus callosum DTI metrics in acute mild and moderate
TBI: its correlation with neuropsychometric tests. Brain Inj, 23(7), 675-685.
Kushner, D. (1998). Mild TBI: Toward understanding manifestations and treatment. Arch Intern
Med, 158(15), 1617-1624.
LaPlaca, M. C., Simon, C. M., Prado, G. R., & Cullen, D. K. (2007). CNS injury biomechanics
and experimental models. Prog Brain Res, 161, 13-26.
Le, T. H., & Gean, A. D. (2009). Neuroimaging of TBI. Mt Sinai J Med, 76(2), 145-162.
Le Bihan, D. (2006). [From Brownian motion to mind imaging: diffusion MRI]. Bull Acad Natl
Med, 190(8), 1605-1627; discussion 1627.
Le Bihan, D., Mangin, J. F., Poupon, C., Clark, C. A., Pappata, S., Molko, N., et al. (2001).
Diffusion tensor imaging: concepts and applications. J Magn Reson Imaging, 13(4), 534-
546.
Lee, B. H., Lee, K. H., Kim, U. J., Yoon, D. H., Sohn, J-H., Choi, S. S. et al. (2004). Injury in
the spinal cord may produce cell death in the brain. Brain Res, 1020, 37-44.

60
Lee, H., Wintermark, M., Gean, A. D., Ghajar, J., Manley, G. T., & Mukherjee, P. (2008). Focal
lesions in acute mild TBI and neurocognitive outcome: CT versus 3T MRI. J
Neurotrauma, 25(9), 1049-1056.
Li, G. L., Farooque, M., Holtz, A., & Olsson, Y. (1999). Apoptosis of oligodendrocytes occurs
for long distances away from the primary injury after compression trauma to rat spinal
cord. Acta Neuropathol, 98(5). 473-480.
Little, D. M., Kraus, M. F., Joseph, J., Geary, E. K., Susmaras, T., Zhou, X. J., Pliskin, N.,
Gorelick, P. B. (2010). Thalamic integrity underlies executive dysfunction in TBI.
Neurology, 74, 558-564.
Lipton, M. L., Gellella, E., Lo, C., Gold, T., Ardekani, B. A., Shifteh, K., et al. (2008).
Multifocal white matter ultrastructural abnormalities in mild TBI with cognitive
disability: a voxel-wise analysis of diffusion tensor imaging. J Neurotrauma, 25(11),
1335-1342.
Lipton, M. L., Gulko, E., Zimmerman, M. E., Friedman, B. W., Kim, M., Gellella, E., et al.
(2009). Diffusion-tensor imaging implicates prefrontal axonal injury in executive
function impairment following very mild TBI. Radiology, 252(3), 816-824.
Lo, C., Shifteh, K., Gold, T., Bello, J. A., & Lipton, M. L. (2009). Diffusion tensor imaging
abnormalities in patients with mild TBI and neurocognitive impairment. J Comput Assist
Tomogr, 33(2), 293-297.
Mac Donald, C. L., Dikranian, K., Song, S. K., Bayly, P. V., Holtzman, D. M., & Brody, D. L.
(2007). Detection of traumatic axonal injury with diffusion tensor imaging in a mouse
model of TBI. Experimental Neurology, 205(1), 116-131.
MacDonald, C. L., Schwarze, N., Vaishnavi, S. N., Epstein, A. A., Snyder, A. Z., Raichle, M.
E., et al. (2008). Verbal memory deficit following TBI: assessment using advanced MRI
methods. Neurology, 71(15), 1199-1201.
Majno, G., & Joris, I. (1995). Apoptosis, oncosis, and necrosis. An overview of cell death. Am J
Pathol, 146(1), 3-15.
Maruta, J., Suh, M., Niogi, S. N., Mukherjee, P., & Ghajar, J. Visual tracking synchronization as
a metric for concussion screening. J Head Trauma Rehabil, 25(4), 293-305.
Maxwell, W. L., Irvine, A., Graham, Adams, J. H., Gennarelli, T. A., Tipperman, R., et al.
(1991). Focal axonal injury: the early axonal response to stretch. J Neurocytol, 20(3),
157-164.
Mayer, A. R., Ling, J., Mannell, M. V., Gasparovic, C., Phillips, J. P., Doezema, D., et al. A
prospective diffusion tensor imaging study in mild TBI. Neurology, 74(8), 643-650.
Maynard, F. M., Jr., Bracken, M. B., Creasey, G., Ditunno, J. F., Jr., Donovan, W. H., Ducker,
T. B., et al. (1997). International Standards for Neurological and Functional
Classification of Spinal Cord Injury. American Spinal Injury Association. Spinal Cord,
35(5), 266-274.

61
Mendez, C. Z., Hurley, R. A., Lassonde, M., Zhang, L., & Taber, K. H. (2005). Mild TBI:
neuroimaging of sports-related concussion. J Neuropsychiatry Clin Neurosci, 17(3), 297-
303.
Messe, A., Caplain, S., Paradot, G., Garrigue, D., Mineo, J-F., Ares, G. S., et al. (2010).
Diffusion tensor imaging and white matter lesions at the subacute stage in mild TBI with
persisitent neurobehavioral impairment. Hum Brain Mapp, [Epub ahead of print].
Moppett, I. K. (2007). TBI: assessment, resuscitation and early management. Br J Anaesth,
99(1), 18-31.
Mikulis, D. J., Jurkiewicz, M. T., McIlroy, W. E., Staines, W. R., Rickards, L., Kalsi-Ryan, S.,
et al. (2002). Adaptation in the motor cortex following cervical spinal cord injury.
Neurology, 58(5), 794-801.
Miles, L., Grossman, R. I., Johnson, G., Babb, J. S., Diller, L., & Inglese, M. (2008). Short-term
DTI predictors of cognitive dysfunction in mild TBI. Brain Inj, 22(2), 115-122.
Mittl, R. L., Grossman, R. I., Hiehle, J. F., Hurst, R. W., Kauder, D. R., Gennarelli, T. A., &
Alburger, G. W. (1994). Prevalence of MR evidence of diffuse axonal injury in patients
with mild head injury and normal head CT findings. AJNR, 15, 1583-1589.
Mori, S., Oishi, K., Jiang, H., Jiang, L., Li, X., Akhter, K., et al. (2008). Stereotaxic white
matter atlas based on diffusion tensor imaging in an ICBM template. Neuroimage, 40(2),
570-582.
Mori, S., Wakana, S., Nagae-Poetscher, L. M., & van Zijl, P. C. M. (2005). MRI atlas of human
white matter. Amsterdam, The Netherlands: Elsevier.
Mukherjee, P., Berman, J. I., Chung, S. W., Hess, C. P., & Henry, R. G. (2008). Diffusion
tensor MR imaging and fiber tractography: theoretic underpinnings. AJNR Am J
Neuroradiol, 29, 632-641.
Mukherjee, P., Chung, S. W., Berman, J. I., Hess, C. P., & Henry, R. G. (2008). Diffusion
tensor MR imaging and fiber tractography: technical considerations. AJNR Am J
Neuroradiol, 29(5), 843-852.
Neil, J. (2008). Diffusion imaging concepts for clinician. J Magn Reson Imaging, 27, 1-7.
Niogi, S. N., & Mukherjee, P. (2010). Diffusion tensor imaging of mild TBI. J Head Trauma
Rehabil, 25(4), 241-255.
Niogi, S. N., Mukherjee, P., Ghajar, J., Johnson, C. E., Kolster, R., Lee, H., et al. (2008a).
Structural dissociation of attentional control and memory in adults with and without mild
TBI. Brain, 131(Pt 12), 3209-3221.
Niogi, S. N., Mukherjee, P., Ghajar, J., Johnson, C., Kolster, R. A., Sarkar, R., et al. (2008b).
Extent of microstructural white matter injury in postconcussive syndrome correlates with
impaired cognitive reaction time: a 3T diffusion tensor imaging study of mild TBI. AJNR
Am J Neuroradiol, 29(5), 967-973.

62
Nucifora, P. G. P., Verma, R., Lee, S-K., & Melhem, E. R. (2007). Diffusion-tensor MR
imaging and tractography: exploring brain microstructure and connectivity. Radiology,
245(2), 367-384.
Nuwer, M. R., Hovda, D. A., Schrader, L. M., & Vespa, P. M. (2005). Routine and quantitative
EEG in mild TBI. Clin Neurophysiol, 116(9), 2001-2025.
O‟Connor, R. J. & Murray, P. C. (2006). Review of spinal cord injuries in Ireland. Spinal Cord.
44, 445-448.
Oppenheimer, D. R. (1968). Microscopic lesions in the brain following head injury. J Neurol
Neurosurg Psychiatry, 31(4), 299-306.
Ozturk, A., Sasson, A. D., Farrell, J. A., Landman, B. A., da Motta, A. C., Aralasmak, A., et al.
(2008). Regional differences in diffusion tensor imaging measurements: assessment of
intrarater and interrater variability. AJNR Am J Neuroradiol, 29(6), 1124-1127.
Pfefferbaum, A., Adalsteinsson, E., & Sullivan, E. V. (2003). Replicability of diffusion tensor
imaging measurements of fractional anisotropy and trace in brain. J Magn Reson
Imaging, 18(4), 427-433.
Pierpaoli, C., Barnett, A., Pajevic, S., Chen, R., Penix, L. R., Virta, A., et al. (2001). Water
diffusion changes in Wallerian degeneration and their dependence on white matter
architecture. Neuroimage, 13(6 Pt 1), 1174-1185.
Pierpaoli, C., & Basser, P. J. (1996). Toward a quantitative assessment of diffusion anisotropy.
Magn Reson Med, 36(6), 893-906.
Povlishock, J. T., Becker, D. P., Cheng, C. L., & Vaughan, G. W. (1983). Axonal change in
minor head injury. J Neuropathol Exp Neurol, 42(3), 225-242.
Povlishock, J. T., Erb, D. E., & Astruc, J. (1992). Axonal response to TBI: reactive axonal
change, deafferentation, and neuroplasticity. J Neurotrauma, 9 Suppl 1, S189-200.
Povlishock, J. T., & Katz, D. I. (2005). Update of neuropathology and neurological recovery
after TBI. J Head Trauma Rehabil, 20(1), 76-94.
Park, E., Bell, J. D., & Baker, A. J. (2008). TBI: Can the consequences be stopped? CMAJ,
178(9), 1163-1170.
Ramu, J., Herrea, J., Grill, R., Bockhorst, T., & Narayana, P. (2008). Brain fiber tract plasticity
in experimental spinal cord injury: diffusion tensor imaging. Exp Neurol, 212, 100-107.
Randolph, C., Millis, S., Barr, W. B., McCrea, M., Guskiewicz, K. M., Hammeke, T. A., &
Kelly, J. P. (2009). Concussion symptom inventory: an empirically derived scale for
monitoring resolution of symptoms following sport-related concussion. Arch Clin
Neuropsychol, 24(3), 219-229.
Richards, J. S., Brown, L., Hagglund, K., Bua, G., & Reeder, K. (1988). Spinal cord injury and
concomitant TBI: results of a longitudinal investigation. Am J Phys Med Rehabil, 67,
211-216.

63
Rutgers, D. R., Fillard, P., Paradot, G., Tadie, M., Lasjaunias, P., & Ducreux, D. (2008).
Diffusion tensor imaging characteristics of the corpus callosum in mild, moderate, and
severe TBI. AJNR Am J Neuroradiol, 29(9), 1730-1735.
Rutgers, D. R., Toulgoat, F., Cazejust, J., Fillard, P., Lasjaunias, P., & Ducreux, D. (2008).
White matter abnormalities in mild TBI: a diffusion tensor imaging study. AJNR Am J
Neuroradiol, 29(3), 514-519.
Saatman, K. E., Duhaime, A. C., Bullock, R., Maas, A. I., Valadka, A., Manley, G. T., et al.
(2008). Classification of TBI for targeted therapies. J Neurotrauma, 25(7), 719-738.
Saboe, L. A., Reid, D. C., Davis, L. A., Warren, S. A., & Grace, M. G. (1991). Spine trauma and
associated injuries. J Trauma, 31(1), 43-48.
Saunders, R. L., & Harbaugh, R. E. (1984). The second impact in catastrophic contact-sports
head trauma. JAMA, 252(4), 538-539.
Sekhon, L. H., & Fehlings, M. G. (2001). Epidemiology, demographics, and pathophysiology of
acute spinal cord injury. Spine (Phila Pa 1976), 26(24 Suppl), S2-12.
Shibayama, M., Hattori, B. T., Himes, M., Murray M., & Tessler, A. (1998). Neurotrophin-3
prevents death of axotomized Clarke‟s nucleus neurons in adult rats. J Comp Neurol,
390, 102-111.
Shifman, M. I., Zhang, G., & Selzer, M. E. (2008). Delayed death of identified reticulospinal
neurons after spinal cord injury in lampreys. J Comp Neurol, 510, 269-282.
Shuman, S. L., Bresnahan, J. C., Beattie, M. S. (1997). Apoptosis of microglia and
oligodendrocytes after spinal cord contusions in rats. J Neurosci Res, 50, 798-808.
Smith, S. M. (2002). Fast robust automated brain extraction. Hum Brain Mapp, 17(3), 143-155.
Smith, S. M., Jenkinson, M., Johansen-Berg, H., Rueckert, D., Nichols, T. E., Mackay, C. E.,
Watkins, K. E., Ciccarelli, O., Cader, M. Z., Matthews, P. M., & Behrens, T. E. J.
(2006). Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data.
NeuroImage, 31, 1487-1505.
Smith, S. M., Jenkinson, M., Woolrich, M. W., Beckmann, C. F., Behrens, T. E., Johansen-
Berg, H., et al. (2004). Advances in functional and structural MR image analysis and
implementation as FSL. Neuroimage, 23 Suppl 1, S208-219.
Smith, D. H., Meaney, D. F., Shull, W. H. (2003). Diffuse axonal injury in head trauma. J Head
Trauma Rehab, 18(4), 307-316.
Sosin, D. M., Sniezek, J. E., & Thurman, D. J. (1996). Incidence of mild and moderate brain
injury in the United States, 1991. Brain Inj, 10(1), 47-54.
Sterr, A., Herron, K. A., Hayward, C., & Montaldi, D. (2006). Are mind head injures as mild as
we thing? Neurobehavioral concomitants of chronic post-concussion syndrome. BMC
Neurology, 6(7).

64
Teasdale, G., & Jennett, B. (1974). Assessment of coma and impaired consciousness. A
practical scale. Lancet, 2(7872), 81-84.
The Mild TBI Committee of the Head Injury Interdisciplinary Special Interest Group of the
American Congress of Rehabilitation Medicine. (1993). Definition of mild TBI. J Head
Trauma Rehabil, 8, 86-87.
Till, C., Colella, B., Verwegen, J., & Green R. E. (2008). Postrecovery cognitive decline in
adults with TBI. Arch Phys Med Rehabil, 89(12 Suppl 2), S25-S34.
Tolonen, A., Turkka, J., Salonen, O., Ahoniemi, E., & Alaranta, H. (2007). TBI is under-
diagnosed in patients with spinal cord injury. J Rehabil Med, 39(8), 622-626.
Wannier, T., Schmidlin, E., Bloch, J., & Rouiller, E. M. (2005). A unilateral section of the
corticospinal tract at cervical level in primate does not lead to measurable cell loss in
motor cortex. J Neurotrauma, 22(6), 703-717.
Warden, P., Bamber, N. I., Li, H., Esposito, A., Ahmad, K. A., Hsu, C. Y., & Xu, X. M. (2001).
Delayed glial cell death following Wallerian degeneration in white matter tracts after
spinal cord dorsal column cordotomy in adult rats. Experimental Neurology, 168, 213-
224.
Watanabe, T. K., Zafonte, R. D., & Lairson, E. J. (1999). TBI Associated with Acute Spinal
Cord Injury: Risk Factors, Evaluation, and Outcomes. Topics in Spinal Cord Injury
Rehabilitation, 5(2), 83-90.
Waters, R. L., Adkins, R. H., & Yakura, J. S. (1991). Definition of complete spinal cord injury.
Paraplegia, 29(9), 573-581.
Watts, R., Liston, C., Niogi, S., & Ulug, A. M. (2003). Fiber tracking using magnetic resonance
diffusion tensor imaging and its applications to human brain development. Mental
Retardation and Developmental Disabilities, 9, 168-177.
Wei, C. W., Tharmakulasingam, J., Crawley, A., Kideckel, D. M., Mikulis, D. J., Bradbury, C.
L., et al. (2008). Use of diffusion-tensor imaging in traumatic spinal cord injury to
identify concomitant TBI. Arch Phys Med Rehabil, 89(12 Suppl), S85-91.
Wilde, E. A., McCauley, S. R., Hunter, J. V., Bigler, E. D., Chu, Z., Wang, Z. J., et al. (2008).
Diffusion tensor imaging of acute mild TBI in adolescents. Neurology, 70(12), 948-955.
Wolf, J. A., Stys, P. K., Lusardi, T., Meaney, D., & Smith, D. H. (2001). Traumatic axonal
injury induces calcium influx modulated by tetrodotoxin-sensitive sodium channels. J
Neurosci, 21(6), 1923-1930.
Woolrich, M. W., Jbabdi, S., Patenaude, B., Chappell, M., Makni, S., Behrens, T., et al. (2009).
Bayesian analysis of neuroimaging data in FSL. Neuroimage, 45(1 Suppl), S173-186.
Wrigley, P. J., Gustin, S. M., Macey, P. M., Nash, P. G., Gandevia, S. C., Macefield, V. G., et
al. (2009). Anatomical changes in human motor cortex and motor pathways following
complete thoracic spinal cord injury. Cereb Cortex, 19(1), 224-232.

65
Zhang, K., Johnson, B., Pennell, D., Ray, W., Sebastianelli, W., & Slobounov, S. Are functional
deficits in concussed individuals consistent with white matter structural alterations:
combined FMRI & DTI study. Exp Brain Res, 204(1), 57-70.