
dIffereNTIATINg cArdIAc froM NoN cArdIAc syMPToMs
44
The Journal of the Irish Practice Nurses Association Issue 3 Volume 5 May/June 2012 Are your patients at risk? Pneumococcal Disease Vaccinate your at-risk patients and those 65 years and over against serious pneumococcal disease. 09/11 IR00094c age 65+ chronic lung, heart or renal disease weakened immune system other at-risk groups** smoker diabetes infant* v i s i t o n e i n s e v e n . i e Marketing authorisation holder: Sanofi Pasteur MSD Limited, Block A, Second Floor, Cookstown Court, Old Belgard Road, Tallaght, Dublin 24. Marketing authorisation number: PA 544/21/3 Legal category: POM Information about adverse event reporting can be found at www.imb.ie. Adverse events and inadvertent vaccination during pregnancy should also be reported to Sanofi Pasteur MSD by calling 00 44 1628 785291. * All infants are offered immunisation against pneumococcal disease as part of the National Immunisation Programme. ** See Immunisation Guidelines for Ireland www.immunisation.ie € 1000 IPNA AWARD 2012 SMOKING CESSATION TREOIR – SERVICE FOR UNMARRIED PARENTS IPNA CONFERENCE 2012 PICTURE GALLERY FROM 2011 DIFFERENTIATING CARDIAC FROM NON CARDIAC SYMPTOMS Lisa Browne DIABETES CARE IN GENERAL PRACTICE Katie Murphy EATING DISORDERS – THE DIETITIAN’S ROLE IN A CAMHS SETTING Joanne Corbett
Transcript of dIffereNTIATINg cArdIAc froM NoN cArdIAc syMPToMs
The Journal of the Irish Practice Nurses AssociationIssue 3 Volume 5 May/June 2012
Are your patients at risk?
Pneumococcal DiseaseVaccinate your at-risk patients and those 65 years and over against serious pneumococcal disease.
09/11 IR00094c
age 65+
chronic lung, heart or renal
disease
weakenedimmunesystem
other at-risk groups**smoker
diabetes
infant*
Vaccinate your at-risk patients and those 65 years
v is i t one inseven. ie
Marketing authorisation holder: Sanofi Pasteur MSD Limited, Block A, Second Floor, Cookstown Court, Old Belgard Road, Tallaght, Dublin 24. Marketing authorisation number: PA 544/21/3 Legal category: POM
Information about adverse event reporting can be found at www.imb.ie. Adverse events and inadvertent vaccination during pregnancy should also be reported to Sanofi Pasteur MSD by calling 00 44 1628 785291.
* All infants are offered immunisation against pneumococcal disease as part of the National Immunisation Programme.** See Immunisation Guidelines for Ireland www.immunisation.ie
€1000 IPNA AwArd 2012 sMokINg cessATIoN
TreoIr – servIce for uNMArrIed PAreNTs
IPNA coNfereNce 2012PIcTure gAllery froM 2011
dIffereNTIATINg cArdIAc froM NoN cArdIAc
syMPToMs Lisa BrownedIAbeTes cAre IN
geNerAl PrAcTIceKatie Murphy
eATINg dIsorders – The dIeTITIAN’s role IN A cAMhs seTTINgJoanne Corbett
Centrum Pregnancy Care is a specially formulated multivitamin-multimineral range for women planning a baby and for pregnant and breastfeeding mums. Containing 19 vitamins and minerals, including Folic Acid and Calcium, Centrum Pregnancy Care has been developed by the experts at Centrum to help support the nutritional needs of you and your baby.
For more information ask at your local pharmacy or visit: www.centrum.ie
Pfizer Consumer Healthcare, Citywest, Dublin 24. * Trade Mark.
www.centrum.ie
NEWNutritional support for you and your baby
1
editorial
clinical nurse specialists – “cupboard nurses”?
I recently read the findings from a study on the role of the practice nurse which was carried out in UCC (McCarthy, Cornally, Moran, 2011, Room for expansion in role of practice nurse, Forum, November 2011). Whilst I was heartened by most of the findings, one or two thorny issues came to the fore. In relation to the clinical nurse specialist and advanced nurse practitioner roles, one GP described “serious subspecialisation of practice nurses should
be discouraged or they will become cupboard nurses like many of their hospital colleagues”. It is my understanding that GPs fought, not that long ago, to have general practice created as a speciality within medicine so why not have clinical nurse specialists/advanced nurse practitioners in general practice? The title does not denote that the role is confined to a specific speciality such as respiratory, diabetes, dermatology etc. It denotes that the role is positioned in a clinical area in the community and outside the hospital arena and because of its very nature, it denotes a generalised role which provides a service to the practice population. There has been many a debate within the nursing literature about generalist versus specialist roles and how can a nurse be a specialist in a generalist role?
Our clinical nurse specialist colleagues in hospital are highly skilled, expert and accessible. They make our jobs a lot easier as they are a reliable and accurate source of information. For practice nurses, the hospital based CNS is the primary contact source when we have a query about a patient and they assist us greatly in the care of many of our patients. They always know our patients and can provide us with up to date specialist knowledge about the patient’s condition. To describe these highly skilled, knowledgeable and expert nurses as “cupboard nurses” is nothing but insulting.
While the study supports the development of the CNS and ANP role in general practice, I wonder how this might evolve. Within the clinical care programmes, there is a shift in the model of care from secondary care to primary care and for many people with chronic illness; primary care is the appropriate place to access the required services. There is a wealth of skills and expertise amongst practice nurses to provide such services but whether practice nurses will be supported and encouraged to change the direction and focus of their work will be the crux. Or will we see our clinical nurse specialist colleagues changing the focus and direction of their work so that they will be providing services in the community with reduced time in the hospital setting? It is an exciting and challenging time for practice nurses and clinical nurse specialists in terms of what the future may hold. We should embrace it and maybe, for some of us it will provide us with a career opportunity that will be challenging and rewarding and worthy of out skills and expertise.
Ruth Morrow
Abbreviated Prescribing Information: Please refer to the Summary of Product Characteristics before prescribing. Presentation: Lexapro® tablets 5 mg, 10 mg, 15 mg and 20 mg containing escitalopram (as oxalate). Indications: Treatment of major depressive episodes.Panic disorder with or without agoraphobia. Social Anxiety Disorder. Generalised Anxiety Disorder. Obsessive Compulsive Disorder. Dosage: Major depressive episodes Adults: Usual dosage is 10 mg once daily. The dose may be increased to a maximum of 20 mg/day. PanicDisorder with or without agoraphobia: An initial dose of 5 mg is recommended for the first week before increasing the dose to 10 mg/day. The dose may be further increased, up to a maximum of 20 mg/day. Social Anxiety Disorder: Usual dosage is 10 mg once daily. Thedose may subsequently be decreased to 5 mg or increased to a maximum of 20 mg/day. Generalised Anxiety Disorder: Initial dosage is 10 mg once daily. The dose may subsequently be increased to a maximum of 20 mg/day. Obsessive Compulsive Disorder: Initialdosage is 10 mg once daily. The dose may be increased to a maximum of 20 mg daily. Elderly (>65 yrs): Initial dosage is 5 mg once daily. Depending on individual patient response the dose may be increased to 10 mg daily. The efficacy of Lexapro in social anxiety disorderhas not been studied in elderly patients. Children and adolescents (<18 years): Not recommended. Poor metabolisers of CYP2C19: In known poor metabolisers of CYP2C19, 5 mg/day Lexapro is recommended for the first 2 weeks, the dose can be increased to 10 mgafter assessment. Reduced hepatic function: In mild/moderately impaired hepatic function an initial dose of 5 mg/day for the first two weeks of treatment is recommended, the dose may be increased to 10 mg/day. Caution and extra careful dose titration advised inpatients with severely reduced hepatic function. Reduced renal function: Dosage adjustment is not necessary in patients with mild or moderate renal impairment. Caution is advised in patients with severely reduced renal function (CLcr<30 ml/min). Contraindications:Hypersensitivity to escitalopram or to any of the excipients. Concomitant treatment with a nonselective, irreversible monoamine oxidase inhibitor (MAOI). Concomitant treatment with reversible MAO-A inhibitors e.g. moclobemide or reversible non-selective MAO-inhibitorse.g. linezolid. (Lexapro may be started 14 days after discontinuing treatment with an irreversible MAOI. At least 7 days should elapse after discontinuing Lexapro treatment, before starting a non-selective irreversible MAOI). Lexapro is contraindicated together with medicinalproducts that are known to prolong the QT interval and in patients with known QT interval prolongation or congenital long QT syndrome. Fertility, Pregnancy & Lactation: Lexapro should not be used during pregnancy unless clearly necessary. Neonates should be observedif maternal use of Lexapro continues into the later stages of pregnancy, particularly the third trimester. Abrupt discontinuation should be avoided during pregnancy. Use of SSRIs during pregnancy may increase the risk of persistent pulmonary hypertension (PPHN) in thenewborn. Refer to the full prescribing information for a list of serotonergic or discontinuation symptoms, which may occur in the neonate after maternal SSRI/SNRI use in later stages of pregnancy. Breast-feeding is not recommended during treatment. Precautions: Patientsshould be cautioned about the potential risk to their ability to drive a car and operate machinery. No pharmacokinetic or pharmacodynamic interactions are expected with concomitant alcohol intake, however the combination is not advised. Insulin and/or oral hypoglycaemicdosage may need to be adjusted in diabetics. Hyponatraemia has been observed rarely with SSRI use, caution is required in patients at risk of hyponatraemia. Caution is advised with coadministration of ECT and in patients with a history of mania/hypomania. Caution isadvised with concomitant use of oral anticoagulants, products affecting platelet function and in patients with known bleeding tendencies. Avoid in patients with unstable epilepsy & monitor patients with controlled epilepsy. Discontinue if patient develops seizures or if thereis an increase in seizure frequency. Caution is advised with concomitant use of serotonergic compounds. Stop treatment immediately if patient develops serotonin syndrome. Use at a low starting dose for panic disorders. Avoid abrupt discontinuation. Gradual discontinuationby dose tapering is advised. As with all SSRIs it is advisable to closely monitor patients for suicide and self-harm risk in the first few weeks of treatment and until significant remission occurs. The use of SSRIs/SNRIs has been associated with the development of akathisia,increasing the dose in these patients may be detrimental. Caution is advised in patients with coronary heart disease. As Lexapro has been found to cause a dose-dependent prolongation of the QT interval, caution is advised for patients with risk factors such as female gender,pre-existing QT interval prolongation, significant bradycardia, recent acute myocardial infarction, uncompensated heart failure, hypokalaemia, hypomagnesaemia or other cardiac diseases. Consider an ECG review before starting Lexapro in patients with stable cardiac disease.If signs of cardiac arrhythmia occur during treatment with Lexapro, the treatment should be withdrawn and an ECG perfomed. Drug Interactions: MAO inhibitors (see Contraindications), advise caution in use with irreversible selective MAO-B inhibitors (selegiline). Medicinalproducts that prolong the QT interval (see Contraindications). Caution in use with lithium, tryptophan, serotonergic medicinal products or with products capable of lowering the seizure threshold. Avoid concomitant use with St. John’s Wort. Caution is advised with co-administration of drugs metabolised by enzymes CYP2C19, CYP3A4 and CYP2D6. Co-administration with CYP2C19 inhibitors, and general enzyme inhibitors e.g. cimetidine may require reduction of the Lexapro dose. Lexapro is an inhibitor of CYP2D6, caution is advisedwith concomitant use of drugs (particularly those with a narrow therapeutic index) mainly metabolized by CYP2D6. Caution is advised with concomitant use of oral anti-coagulants, medicinal products known to affect platelet function and non-steroidal anti-inflammatorydrugs (NSAIDs). Adverse Events: Adverse reactions are most frequent during the first or second week of treatment and usually decrease in intensity and frequency with continued treatment. Frequencies are not placebo-corrected. Very Common (≥1/10): Nausea. Common(≥1/100 to <1/10): Weight increased, insomnia, somnolence, dizziness, paraesthesia, tremor, sinusitis, yawning, diarrhoea, constipation, vomiting, dry mouth, sweating increased, arthralgia, myalgia, decreased and increased appetite, fatigue, pyrexia, ejaculation disorder,impotence, anxiety, restlessness, abnormal dreams, male & female libido decreased, female anorgasmia. Uncommon (≥1/1,000 to <1/100): weight decreased, tachycardia, taste disturbance, sleep disorder, syncope, mydriasis, visual disturbance, tinnitus, epistaxis, gastrointestinalhaemorrhages (incl. rectal), urticaria, alopecia, rash, pruritus, oedema, metrorrhagia, menorrhagia, bruxism, agitation, nervousness, panic attack, confusional state. Rare (≥1/10,000 to <1/1,000): Bradycardia, serotonin syndrome, anaphylactic reaction, aggression, depersonalisation,hallucination. Not known (cannot be estimated from the available data): Liver function test abnormal, thrombocytopenia, dyskinesia, movement disorder, convulsion, urinary retention, ecchymosis, angioedemas, inappropriate ADH secretion, hyponatraemia, orthostatichypotension, hepatitis, galactorrhoea, male priapism, mania, suicidal ideation, suicidal behaviour, psychomotor restlessness, akathisia, anorexia, ECG QT prolonged and ventricular arrhythmia including Torsadede Pointes. Others: discontinuation symptoms (SSRIs/SNRIs), increased risk of bone fractures (patients ≥50 years) (SSRIs/TCAs). Overdose: Clinical data on escitalopram overdose is limited and many casesinvolve concomitant overdoses with other drugs. Doses between 400-800 mg of Lexapro alone have been taken without any severe symptoms. Symptoms seen in reported overdose of Lexapro mainly relateto the central nervous system, the gastrointestinal system, the cardiovascular system and electrolyte/fluid balance conditions. There is no specific antidote. Treatment is symptomatic and supportive withmonitoring of cardiac and vital signs. In case of overdose ECG monitoring is advised in patients using concomitant medications that prolong the QT interval, in patients with altered metabolism (e.g. liverimpairment) and in those with congestive heart failure and bradyarrhythmias. Gastric lavage and the use of activated charcoal should be considered. Legal Category: POM. Product Licence Holder: H. LundbeckA/S, Ottiliavej 9, DK-2500 Valby, Copenhagen, Denmark. PA Numbers: 5 mg PA805/2/1; 10 mg PA805/2/2; 15 mg PA805/2/3; 20 mg PA805/2/4. Further information is available upon request from Lundbeck(Ireland) Ltd., 7 Riverwalk, Citywest Business Campus, Citywest, Dublin 24. ‘Lexapro’ is a registered trademark ® 2002 Lundbeck Ltd. Date of preparation: January 2012. Reference: 1. Combined IMS Hospitaland IRLP Unit Sales Data (YTD/Dec/2011).
So many symptoms...
The No.1 prescribed anti-depressant in Ireland 1
LX2/1/12
Treat the coreof depression
withLexapro®
07482 Lexapro Ads_07482 Lexapro IP 20/02/2012 10:54 Page 1
3
Issue 5 Volume 2 september / october2009
ContentsThe Journal of the Irish Practice Nurses Association
Nursing in General Practice is published by GreenCross Publishing, 7 Adelaide Court, Adelaide Road, Dublin 2. Tel: 4189799 Fax: 4789449Email: [email protected]
EDITORMaura Henderson
CONSUlTING EDITORSDarina lane and Ruth Morrow
COMMISSIONING EDITORJudith leavy
DESIGNERBarbara Vasic
PUBlISHERSGraham CookeMaura Henderson
DisclaimerThe views expressed in Nursing in General Practice are not necessarily those of the publishers, editor or editorial advisory board. While the publishers, editor and editorial advisory board have taken every care with regard to accuracy of editorial and advertisement contributions, they cannot be held responsible for any errors or omissions contained.
Issue 3 Volume 5 May/June 2012
*GreenCross Publishing was established in 2007 and is jointly owned by Graham Cooke and Maura Henderson.
© Copyright GreenCross Publishing 2012The contents of Nursing in General Practice are protected by copyright. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form by any means – electronic, mechanical or photocopy recording or otherwise – whole or in part, in any form whatsoever for advertising or promotional purposes without the prior written permission of the editor or publishers
1 edITorIAl
4 News
11 brANch News
IPNA coNfereNce
14 PIcTure gAllery froM 2011
15 IPNA coNfereNce 2012
€1000 IPNA AwArd
16 sMokINg cessATIoN
clINIcAl revIew
18 dIffereNTIATINg cArdIAc froM NoN cArdIAc syMPToMs Assessment and risk stratification of patients presenting with the most common cardiac symptom
lisa browne
21 dIAbeTes cAre IN geNerAl PrAcTIce Integrated care ensures the highest standard of
patient care katie Murphy
eThIcs
30 TreoIr – servIce for uNMArrIed PAreNTs
IN PrAcTIce
32 eATINg dIsorders – The dIeTITIAN’s role IN A cAMhs seTTINg Management of child and adolescent anorexia
nervosa in a specialist CAMHS in-patient unit setting. Joanne corbett
AbsTrAcTs
36 MeN’s heAlTh
38 ProducTs
41 crossword
Abbreviated Prescribing Information: Please refer to the Summary of Product Characteristics before prescribing. Presentation: Lexapro® tablets 5 mg, 10 mg, 15 mg and 20 mg containing escitalopram (as oxalate). Indications: Treatment of major depressive episodes.Panic disorder with or without agoraphobia. Social Anxiety Disorder. Generalised Anxiety Disorder. Obsessive Compulsive Disorder. Dosage: Major depressive episodes Adults: Usual dosage is 10 mg once daily. The dose may be increased to a maximum of 20 mg/day. PanicDisorder with or without agoraphobia: An initial dose of 5 mg is recommended for the first week before increasing the dose to 10 mg/day. The dose may be further increased, up to a maximum of 20 mg/day. Social Anxiety Disorder: Usual dosage is 10 mg once daily. Thedose may subsequently be decreased to 5 mg or increased to a maximum of 20 mg/day. Generalised Anxiety Disorder: Initial dosage is 10 mg once daily. The dose may subsequently be increased to a maximum of 20 mg/day. Obsessive Compulsive Disorder: Initialdosage is 10 mg once daily. The dose may be increased to a maximum of 20 mg daily. Elderly (>65 yrs): Initial dosage is 5 mg once daily. Depending on individual patient response the dose may be increased to 10 mg daily. The efficacy of Lexapro in social anxiety disorderhas not been studied in elderly patients. Children and adolescents (<18 years): Not recommended. Poor metabolisers of CYP2C19: In known poor metabolisers of CYP2C19, 5 mg/day Lexapro is recommended for the first 2 weeks, the dose can be increased to 10 mgafter assessment. Reduced hepatic function: In mild/moderately impaired hepatic function an initial dose of 5 mg/day for the first two weeks of treatment is recommended, the dose may be increased to 10 mg/day. Caution and extra careful dose titration advised inpatients with severely reduced hepatic function. Reduced renal function: Dosage adjustment is not necessary in patients with mild or moderate renal impairment. Caution is advised in patients with severely reduced renal function (CLcr<30 ml/min). Contraindications:Hypersensitivity to escitalopram or to any of the excipients. Concomitant treatment with a nonselective, irreversible monoamine oxidase inhibitor (MAOI). Concomitant treatment with reversible MAO-A inhibitors e.g. moclobemide or reversible non-selective MAO-inhibitorse.g. linezolid. (Lexapro may be started 14 days after discontinuing treatment with an irreversible MAOI. At least 7 days should elapse after discontinuing Lexapro treatment, before starting a non-selective irreversible MAOI). Lexapro is contraindicated together with medicinalproducts that are known to prolong the QT interval and in patients with known QT interval prolongation or congenital long QT syndrome. Fertility, Pregnancy & Lactation: Lexapro should not be used during pregnancy unless clearly necessary. Neonates should be observedif maternal use of Lexapro continues into the later stages of pregnancy, particularly the third trimester. Abrupt discontinuation should be avoided during pregnancy. Use of SSRIs during pregnancy may increase the risk of persistent pulmonary hypertension (PPHN) in thenewborn. Refer to the full prescribing information for a list of serotonergic or discontinuation symptoms, which may occur in the neonate after maternal SSRI/SNRI use in later stages of pregnancy. Breast-feeding is not recommended during treatment. Precautions: Patientsshould be cautioned about the potential risk to their ability to drive a car and operate machinery. No pharmacokinetic or pharmacodynamic interactions are expected with concomitant alcohol intake, however the combination is not advised. Insulin and/or oral hypoglycaemicdosage may need to be adjusted in diabetics. Hyponatraemia has been observed rarely with SSRI use, caution is required in patients at risk of hyponatraemia. Caution is advised with coadministration of ECT and in patients with a history of mania/hypomania. Caution isadvised with concomitant use of oral anticoagulants, products affecting platelet function and in patients with known bleeding tendencies. Avoid in patients with unstable epilepsy & monitor patients with controlled epilepsy. Discontinue if patient develops seizures or if thereis an increase in seizure frequency. Caution is advised with concomitant use of serotonergic compounds. Stop treatment immediately if patient develops serotonin syndrome. Use at a low starting dose for panic disorders. Avoid abrupt discontinuation. Gradual discontinuationby dose tapering is advised. As with all SSRIs it is advisable to closely monitor patients for suicide and self-harm risk in the first few weeks of treatment and until significant remission occurs. The use of SSRIs/SNRIs has been associated with the development of akathisia,increasing the dose in these patients may be detrimental. Caution is advised in patients with coronary heart disease. As Lexapro has been found to cause a dose-dependent prolongation of the QT interval, caution is advised for patients with risk factors such as female gender,pre-existing QT interval prolongation, significant bradycardia, recent acute myocardial infarction, uncompensated heart failure, hypokalaemia, hypomagnesaemia or other cardiac diseases. Consider an ECG review before starting Lexapro in patients with stable cardiac disease.If signs of cardiac arrhythmia occur during treatment with Lexapro, the treatment should be withdrawn and an ECG perfomed. Drug Interactions: MAO inhibitors (see Contraindications), advise caution in use with irreversible selective MAO-B inhibitors (selegiline). Medicinalproducts that prolong the QT interval (see Contraindications). Caution in use with lithium, tryptophan, serotonergic medicinal products or with products capable of lowering the seizure threshold. Avoid concomitant use with St. John’s Wort. Caution is advised with co-administration of drugs metabolised by enzymes CYP2C19, CYP3A4 and CYP2D6. Co-administration with CYP2C19 inhibitors, and general enzyme inhibitors e.g. cimetidine may require reduction of the Lexapro dose. Lexapro is an inhibitor of CYP2D6, caution is advisedwith concomitant use of drugs (particularly those with a narrow therapeutic index) mainly metabolized by CYP2D6. Caution is advised with concomitant use of oral anti-coagulants, medicinal products known to affect platelet function and non-steroidal anti-inflammatorydrugs (NSAIDs). Adverse Events: Adverse reactions are most frequent during the first or second week of treatment and usually decrease in intensity and frequency with continued treatment. Frequencies are not placebo-corrected. Very Common (≥1/10): Nausea. Common(≥1/100 to <1/10): Weight increased, insomnia, somnolence, dizziness, paraesthesia, tremor, sinusitis, yawning, diarrhoea, constipation, vomiting, dry mouth, sweating increased, arthralgia, myalgia, decreased and increased appetite, fatigue, pyrexia, ejaculation disorder,impotence, anxiety, restlessness, abnormal dreams, male & female libido decreased, female anorgasmia. Uncommon (≥1/1,000 to <1/100): weight decreased, tachycardia, taste disturbance, sleep disorder, syncope, mydriasis, visual disturbance, tinnitus, epistaxis, gastrointestinalhaemorrhages (incl. rectal), urticaria, alopecia, rash, pruritus, oedema, metrorrhagia, menorrhagia, bruxism, agitation, nervousness, panic attack, confusional state. Rare (≥1/10,000 to <1/1,000): Bradycardia, serotonin syndrome, anaphylactic reaction, aggression, depersonalisation,hallucination. Not known (cannot be estimated from the available data): Liver function test abnormal, thrombocytopenia, dyskinesia, movement disorder, convulsion, urinary retention, ecchymosis, angioedemas, inappropriate ADH secretion, hyponatraemia, orthostatichypotension, hepatitis, galactorrhoea, male priapism, mania, suicidal ideation, suicidal behaviour, psychomotor restlessness, akathisia, anorexia, ECG QT prolonged and ventricular arrhythmia including Torsadede Pointes. Others: discontinuation symptoms (SSRIs/SNRIs), increased risk of bone fractures (patients ≥50 years) (SSRIs/TCAs). Overdose: Clinical data on escitalopram overdose is limited and many casesinvolve concomitant overdoses with other drugs. Doses between 400-800 mg of Lexapro alone have been taken without any severe symptoms. Symptoms seen in reported overdose of Lexapro mainly relateto the central nervous system, the gastrointestinal system, the cardiovascular system and electrolyte/fluid balance conditions. There is no specific antidote. Treatment is symptomatic and supportive withmonitoring of cardiac and vital signs. In case of overdose ECG monitoring is advised in patients using concomitant medications that prolong the QT interval, in patients with altered metabolism (e.g. liverimpairment) and in those with congestive heart failure and bradyarrhythmias. Gastric lavage and the use of activated charcoal should be considered. Legal Category: POM. Product Licence Holder: H. LundbeckA/S, Ottiliavej 9, DK-2500 Valby, Copenhagen, Denmark. PA Numbers: 5 mg PA805/2/1; 10 mg PA805/2/2; 15 mg PA805/2/3; 20 mg PA805/2/4. Further information is available upon request from Lundbeck(Ireland) Ltd., 7 Riverwalk, Citywest Business Campus, Citywest, Dublin 24. ‘Lexapro’ is a registered trademark ® 2002 Lundbeck Ltd. Date of preparation: January 2012. Reference: 1. Combined IMS Hospitaland IRLP Unit Sales Data (YTD/Dec/2011).
So many symptoms...
The No.1 prescribed anti-depressant in Ireland 1
LX2/1/12
Treat the coreof depression
withLexapro®
07482 Lexapro Ads_07482 Lexapro IP 20/02/2012 10:54 Page 1
4
newsNEC NEWS
IPNA AwArds 2012The following educational awards are offered to members this year:• Practice Nurse of the Year Award – closing date 31st July
2012.• Clinical Award (based on Smoking Cessation) – see
elsewhere in this issue for the case study and closing date.• Educational Bursary – closing date 31st July 2012• Valerie Mangan IPNA loyalty Award – closing date 31st July
2012Details of all awards are available on the IPNA website
(Grants and Awards page)
Nec MeeTINgs 2012 Wednesday 5th September 2012, Ashling Hotel, Parkgate Street, Dublin 8.
Friday 5th October 2012, Tullamore Court Hotel.Agendas will be emailed to all NEC Reps before each
meeting.
IPNA coNfereNce/AgM 2012The 2012 IPNA Annual Educational Conference and AGM will be held on Friday 5th and Saturday 6th October 2012 in the Tullamore Court Hotel. The programme is now available for members to view on the Events page of the IPNA website. Exhibitors who require information can e-mail [email protected]
IPNA Is Now oN TwITTerTo complement existing IPNA communication channels, the IPNA now has a Twitter account. If you have a Twitter account you can follow the handle @PracticeNurses to receive IPNA news, reminders and useful information directly to your timeline.
IPNA websITeThe IPNA website, www.irishpracticenurses.ie is updated constantly, so please log-in regularly to get the latest news on study days, new posts in the Discussion boards and more…
lisa Nolan, Tel: 042-9692403 e-mail: [email protected]
Attending the victrelis launch were dr shay keating, Nurse barbara hynes, Niamh lavin, clinical Nurse co-ordinator and dr Akin Akinwonmi, Msd.
victrelis: a new era in hepatitis c treatment
Legal Category: Prescription Medicine
Product Authorisation Holder: Organon Ireland Limited, P.O. Box 2857, Drynam Road, Swords, Co. Dublin, Ireland. Further information is available on www.medicines.ie or on request from: MSD, Pelham House, South County Business Park, Leopardstown, Dublin 18.
© Merck Sharp & Dohme Limited 2011. All rights reserved.
Date of review: January 2012
Date of preparation: January 2012
Pelham House, South County Business Park, Leopardstown, Dublin 18. 01-1
4-W
OMN
-102
3512
-000
0

5
news
Nurses, midwives now able to provide faster and more effective pain relief
Changes to the Misuse of Drugs Regulations mean that appropriately qualified nurses and pharmacists will now be able to prescribe controlled drugs like morphine, diamorphine and prescription-strength co-codamol, the Government announced recently. This means that:• Up to 20,000 nurses and midwives, and 1,500 pharmacists who
are qualified as ‘independent prescribers’ will now be able to prescribe controlled drugs where it is clinically appropriate and within their professional competence. This makes the best use of their skills and helps patients get faster and more effective care.
• Nurses and pharmacists will also now be able to mix a controlled drug with another medicine for patients who need drugs intravenously. This will ensure faster treatment, especially for those who need urgent pain relief in A&E and palliative care settings.
• They will also now be able to supply or administer morphine and diamorphine under Patient Group Directions, for urgent treatment of very sick or critically injured groups of patients.Most prescriptions for controlled drugs will be to reduce pain
and suffering of emergency patients in A&E, or those nearing the end of their life. These patients will now no longer have to wait for a doctor to sign a prescription, which means they will be able to receive urgent pain relief more quickly. Nurses and pharmacists will also now be able to prescribe controlled drugs in community pain clinics for patients with long-term conditions such as arthritis.
Chief Nursing Officer, Professor Dame Chris Beasley, said:“These changes will help deliver faster and more effective care, making it easier for patients to get the medicines they need, without compromising safety.
“Enabling appropriately qualified nurses and pharmacists to prescribe and mix those controlled drugs they are competent to use, for example in palliative care, completes the changes made over recent years to ensure we make the best use of these highly trained professionals’ skills, for the benefit of patients.”
valerie Mangan Prize 2012 – open to all active IPNA members
This annual award was launched in 2006 in memory of our friend and colleague Valerie Mangan (R.I.P.).
Valerie was a very active member of the IPNA, and felt strongly that members should attend their local branch meetings so that the association would continue to grow and develop as a strong body of practice nurse professionals. The format of the award was developed in consultation with Valerie’s family and is as follows:
The names of all IPNA members who attended at least six branch educational meetings between September 2011 and summer 2012 will be sent to the NEC before the closing date below and the draw will take place during the 2012 IPNA Annual Educational Conference.
The winner will receive an educational bursary of €1,000 (from IPNA) and an engraved statuette (from Valerie’s family) in recognition of their attendance at all of their branch meetings.
Each branch should e-mail the names of all members who attended at least six branch meetings between Sept 2011 and summer 2012 to: [email protected]
Closing date strictly 31st July 2012*.
*due to time constraints any names sent after that date will not be included in the draw.
Cerazette® 75 microgram film-coated tabletsDesogestrelAbbreviAted PresCribing informAtion(refer to summary of Product Characteristics before prescribing)PresentAtion: One sachet containing 1 strip of 28 tablets, each tablet containing 75mcg desogestrel. Uses: Contraception. dosAge: One tablet daily at about the same time. There is no pill-free week between strips. ContrAindiCAtions: Known or suspected pregnancy, active venous thromboembolic disorder, presence or history of severe hepatic disease with current abnormal liver function tests, known or suspec-ted sex-steroid sensitive malignancies, undiagnosed vaginal bleeding, hypersensitivity to any ingredients. PreCAUtions And WArnings: Women currently using combined oral contraceptives (COCs) have a slightly increased risk of having breast cancer diagnosed. The risk in users of progestogen only pills is possibly of similar magnitude to COCs. This risk is low compared to the risk of getting breast cancer ever in life. The increased risk in COC users may be due to an earlier diagnosis, biological effects of the pill, or a combination of both. Refer to a specialist if acute or ch ronic disturbances of liver function occur. Epidemiological studies have associated the use of COCs with an increased incidence of venous thromboembolism (VTE, deep venous thrombosis and pulmonary embolism). It is unclear whether desogestrel used alone carries the same risk. Discontinue in the event of a thrombosis. Consider stopping prior to long term immobilisation due to surgery or illness. Caution patients with a history of thromboembolic disorders. Consider discontinuation if hypertension develops. Benefit/risk assessment should be made in women with liver cancer. Monitor patients with diabetes during the first months of use. Effects on bone density are unknown. Despite the fact that Cerazette consistently inhibits ovulation, ectopic pregnancy should be taken into account in the differential diagnosis if the woman gets amenorrhoea or abdominal pain. Chloasma may occasionally occur. Cerazette contains less than 65mg lactose, and therefore should not be administered to patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency, or glucose-galactose malabsorption. Use in PregnAnCY And LACtAtion: Not recommended during pregnancy. Cerazette does not influence the production or quality of breast milk. Small amounts of the metabolite etonogestrel are excreted with the milk. Limited long term follow-up data (up to 2.5 yrs) on children who were breast-fed do not indicate any differences compared to those whose mother used a copper IUD. However development and growth of the nursing infant should be carefully observed. interACtions: Interactions may lead to breakthrough bleeding and contraceptive failure. This may be seen with enzyme inducers such as hydantoins, barbiturates, primidone, carbamazepine, rifampicin, oxcarbazepine, topiramate, rifabutin, felbamate, ritonavir, nelfinavir, griseofulvin and products containing St John’s Wort. Reduced absorption of etonogestrel may be seen with medical charcoal. Hormonal contraceptives may interfere with metabolism of other drugs, and therefore increase or decrease their plasma or tissue concentrations. Adverse reACtions: Refer to SmPC for full details. Common: irregular bleeding, amenorrhoea, headache, weight gain, breast pain, nausea, acne, mood changes, decreased libido. Breast discharge may also occur. Other less common and rarely reported side effects are listed on the SmPC. overdose: No serious ef-fects have been reported. Symptoms may include nausea, vomiting and in young girls, slight vaginal bleeding. Treatment should be symptomatic.Legal Category: Prescription Only Medicine. Product Licence number: PA 61/27/1. Product Licence Holder: Organon (Ireland) Limited, P.O. Box 2857, Drynam Road, Swords, Co. Dublin, Ireland. date of revision of Prescribing information: July 2009. date of preparation: June 2011. Cerazette/API/1RL/07-09/1. references: 1. Cerazette Summary of Product Characteristics: www.medicines.ie 2. Data on file. Kenilworth, NJ: Schering Corporation.
Full prescribing information is available on www.medicines.ie or on request.
06-1
2-CE
R-20
11-IR
L-46
11-J
Because oestrogen may not be right for many women,
Consider Cerazette®, an oestrogen-free solution1
99% effective12-hr intake window
oestrogen
1 solution+
Pelham House, South County Business Park, Leopardstown, Dublin 18, Ireland
#1globally prescribed oestrogen-free
contraceptive for more than 1 million
women per year2
www.talkoptions.ie
3035_Cerazette_AD_297_105_v.indd 1 14/07/2011 18:09
6
newsCall for submission of papers
3rd International conference on survivors of rape
8-10 November 2012
The closing date for submission of papers is coming up shortly.
If you are planning on presenting a paper for ICSoR 2012, please submit your 250 word abstract using this link http://icsor.org/site/view/10/
The organisers are particularly interested in exploring issues surrounding:
• How to create and sustain effective multiagency working• New approaches to identifying and meeting survivor needs• Responding to survivors of rape’s medical and forensic
needs• Effective and ethical recording and use of data on
prevalence, perpetrators and survivors of rape• The role of those responding to survivors of rape in primary
prevention,• The role of alcohol in rape• Supporting a survivor of rape engaging in the criminal
justice process.
Registration for ICSoR 2012 will open shortly.Early registration before June 30th will cost €280. Registration from June 30th-October 26th will cost €330.
For more informationwww.icsor.org
Launch of the Centre for Practice and Healthcare Innovation at TCD School of Nursing
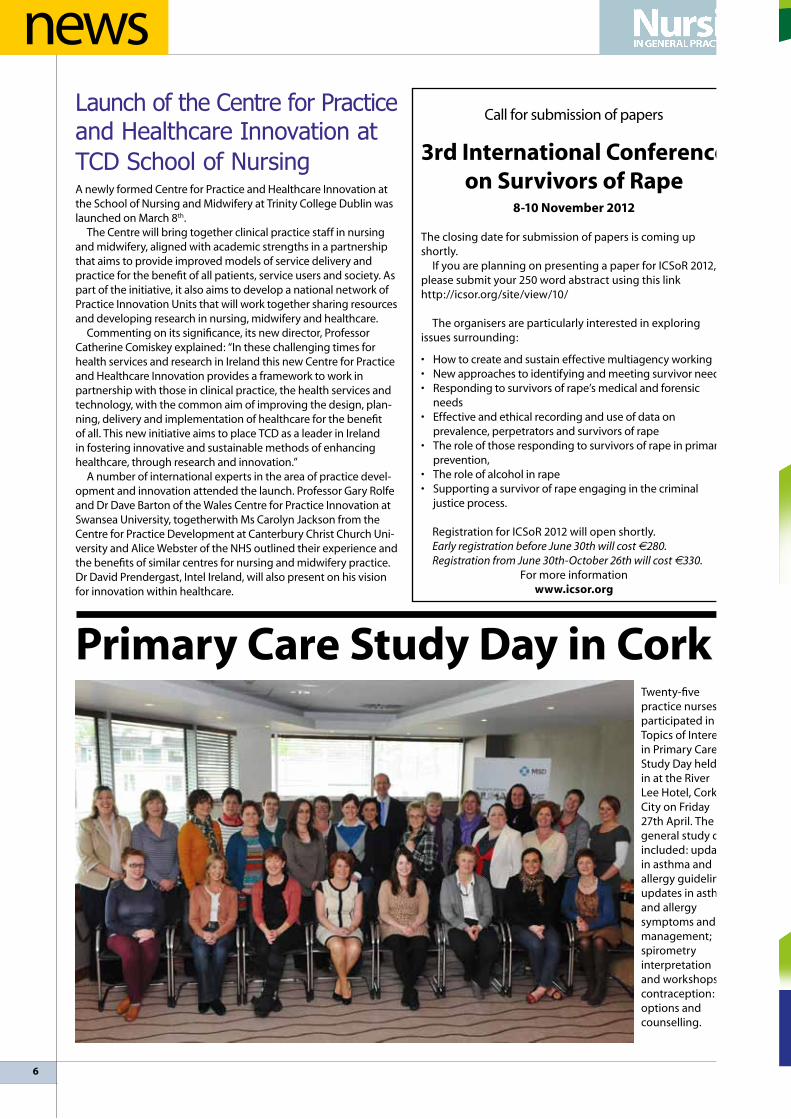
Primary care study day in corkTwenty-five practice nurses participated in the Topics of Interest in Primary Care Study Day held in at the River lee Hotel, Cork City on Friday 27th April. The general study day included: updates in asthma and allergy guidelines; updates in asthma and allergy symptoms and management; spirometry interpretation and workshops; contraception: options and counselling.
A newly formed Centre for Practice and Healthcare Innovation at the School of Nursing and Midwifery at Trinity College Dublin was launched on March 8th.
The Centre will bring together clinical practice staff in nursing and midwifery, aligned with academic strengths in a partnership that aims to provide improved models of service delivery and practice for the benefit of all patients, service users and society. As part of the initiative, it also aims to develop a national network of Practice Innovation Units that will work together sharing resources and developing research in nursing, midwifery and healthcare.
Commenting on its significance, its new director, Professor Catherine Comiskey explained: “In these challenging times for health services and research in Ireland this new Centre for Practice and Healthcare Innovation provides a framework to work in partnership with those in clinical practice, the health services and technology, with the common aim of improving the design, plan-ning, delivery and implementation of healthcare for the benefit of all. This new initiative aims to place TCD as a leader in Ireland in fostering innovative and sustainable methods of enhancing healthcare, through research and innovation.”
A number of international experts in the area of practice devel-opment and innovation attended the launch. Professor Gary Rolfe and Dr Dave Barton of the Wales Centre for Practice Innovation at Swansea University, togetherwith Ms Carolyn Jackson from the Centre for Practice Development at Canterbury Christ Church Uni-versity and Alice Webster of the NHS outlined their experience and the benefits of similar centres for nursing and midwifery practice. Dr David Prendergast, Intel Ireland, will also present on his vision for innovation within healthcare.

8
news
One in eight Irish men will get melanoma
At the launch of May Melanoma Awareness Month, which this year focused on men’s susceptibility to skin cancer, were: Dr Patrick Ormond, Consultant Dermatologist, Dr James Reilly, Minister for Health and Julienne Curran, Medical Relations Manager, la Roche-Posay
Management of Type 2 diabetes and coPd in primary care meeting
Attending the type 2 meeting sponsored by Novatis were Dr Sarah Keane, Co. Wexford, Dr Elaine Murphy, Cork City and Dr Sarah Duggan, Mallow, Co. Cork.
CHY 17932 www.irishpracticenurses.ie
tel: 042-9692403 SMS text to: 087-1304115
e-mail: [email protected]
The IPNA is offering a €1,000 educational bursary for members
who are undertaking or have undertaken a research project or clinical audit in the area of practice nursing. This can be any initiative in practice nursing –
clinical, educational or practice management – within the past 2 years.
THE WINNING ENTRY WILL BE FEATURED IN “NURSING IN GENERAL PRACTICE” AND ON THE IPNA WEBSITE – www.irishpracticenurses.ie
THE WINNER WILL ALSO BE ASKED TO PRESENT THEIR FINDINGS AT THE 2012
IPNA ANNUAL EDUCATIONAL CONFERENCE.
To enter, e-mail an abstract of 500 words to: [email protected]
Please include your contact details and details of any other funding/sponsorship you have received for this study if applicable.
Kindly supported by an unrestricted educational grant from Allen & Hanburys/GSK
Call for cradle to grave strategy for people with autism The current approach to the provision of equity of access to care and intervention in helping people with autism in Ireland is no longer appropriate or sustainable according to Executive Director of Irish Society for Autism, and co-founder and former President of World Autism Organisation, Dr Pat Matthews.
Speaking at the launch of a ground-breaking new book entitled ‘Charter of Rights for People with Autism: “Reflections” and Personal Experiences’, to mark World Autism Awareness Day he said “there are deficiencies in the existing model in Ireland. We need a new ‘cradle to the grave’ strategy and framework for the future development of a comprehensive and appropriate structure for education and support of people with autism in Ireland, people who are hitherto a marginalised and misunderstood population. I hope this book of reflections serves to create a new discourse about autism in Ireland and internationally and contributes to the development of a culture of dignity, care and respect for individuals whose lives are directly affected by the condition.”
The book contains 19 different people’s reflections on the 19 points of the European Charter of Rights for Persons with Autism. The chapters have been written by a diverse range of contribu-tors, including medical experts in the field, individuals with autism, advocates and family members whose lives have been directly affected by the condition. The book is being launched in Ireland first, before being published around the world through the World Autism Organisation network. The Charter of Rights for People with Autism, which was co-authored by Dr Pat Matthews, was passed by the Eu-ropean Parliament in 1996. It is a major contributor internationally to creating a greater understanding of the complexities of autism and the difficulties that people with autism experience on a daily basis.
The book was compiled and edited by Dr. Pat Matthews and Tara Matthews MSc. of the Irish Society for Autism. A paperback edition is available in all good book shops and on the publishers website www.originalwriting.ie priced at €15. All proceeds from the sale of the publication will go directly to the Irish Society for Autism and the World Autism Organisation. For further information go to www.autism.ie

9
news
Model gets tagged and tries out for heart charityModel Rachel Wallace was onside to launch the 2012 tagrugby.ie season and new charity partnership with the Irish Heart Foundation. The Irish Tag Rugby Association wants to get hearts pumping on pitches around Ireland and raise vital funds for the national charity fighting heart disease and stroke. With more than 15,000 players, ITRA saw a natural match with the IHF promoting Tag Rugby as a fun way to get active and raising money towards the charity’s physical activity programmes in schools, workplaces and communities.
Top female tag rugby champion Eimear Flannery who also works in the Irish Heart Foundation’s Health Promotion department said: “Adults should be active at a moderate intensity for at least 30 minutes, 5 days a week. However, half of Irish adults are not meeting this recommendation and are not active enough for heart health. Tag rugby is a great way to become more active and the great thing is it caters for all levels of fitness so you don’t have to be very sporty to start. Plus it offers great social interaction for men and women and it’s plenty of fun. By signing up for the new season, players will not only keep their hearts happy, but they will be supporting a good cause as well.” Register now on www.itra.ie
dr honor Nicholl – educator of the yearDr Honor Nicholl from The School of Nursing and Midwifery at Trin-ity College Dublin (TCD) has been named as International ‘Educator of the Year’ for her work in the area of children’s palliative care.
On the 29th March, the International Journal of Palliative Nursing (IJPN) partnered with Macmillan Cancer Support to host the IJPN Awards and celebrate achievement and excellence in all aspects of palliative care internationally.
At an event in london, Dr Honor Nicholl, Assistant Professor in the School of Nursing and Midwifery, was announced as joint winner of the ‘Educator of the Year’ category in recognition of her influence and commitment to education in the area of children’s palliative care.
An estimated 1,400 children are living with life-limiting condi-tions in Ireland. There are about 350 child deaths each year - the majority in the first year of life. The government launched Pallia-tive Care for Children with life-limiting Conditions in Ireland - A National Policy in 2010.
Dr Nicholl developed the first interdisciplinary children’s pallia-tive care education programme in Ireland with the aid of funding from the Irish Hospice Foundation (IHF). The judges were particu-larly impressed with how Dr Nicholl responded to National Policy and had made determined efforts to ensure key stakeholders were involved in curriculum development and programme delivery.
Dr Nicholl stated: “I am very grateful to the project team and my colleagues in the School of Nursing and Midwifery for their support as well as the Irish Hospice Foundation which supported the development the children’s palliative care programme. It is very important that national policy for children with palliative needs is fulfilled so that children and their families’ needs are met. This requires a sound basis on which to plan all aspects of care.”

10
news
Asthma & Allergy Study Day, Aisling Hotel, Dublin on 20 April 2012
fitness telephone for older people in corkA free telephone support line getting Cork’s older people more active has gone live in Cork. The Go for Life FitLine (1800 303 545) gives people the help and support they need to get off the couch and to start feeling great.
Fitline gets its inspiration from the Smoker Quit line. A caller signs up to get calls from Fitline and, with that little bit of advice and encouragement over the phone, they start to get more active. The line is staffed by volunteer mentors from Cork who are trained to listen, encourage and motivate. This initiative is supported by the HSE South Health Promotion Department and Cork Sports Partnership.
“What’s new and exciting about Go for Life FitLine is that the volunteer mentors making the calls are ordinary older adults from the local area who have themselves been through the ups and downs of trying to be active” said Mary Harkin, Go for life’s Programme Manager. “Having the support of the HSE South Health Promotion Department and Cork’s lSP has been very important to us”.
Sheelagh Broderick, Health Promotion Officer with the HSE South said “This initiative is a great addition to all of the other physical activity programmes we have in place within the city and county. There are lots of older people active in Cork, but we all know someone who might need that little extra nudge to get them involved. The mentors on the Go for life Fitline are wonderful and they’re like a good friend – they can praise you when things go well and encourage you to keep going when your motivation is low. Healthy habits take time to develop but Fitline will stay with you until you’re happy with your progress.”
The Go for life Fitline is already in place in Co louth, South Dublin, Wicklow, Meath and Fingal and the results are very positive. So much so that the World Health Organisation recently endorsed the Go for life Fitline as a great way to encourage and motivate people to be active.
People can call the Go for life Fitline on free phone 1800 303 545 for further information or go to www.ageandopportunity.ie
Dentists welcome GAA move on gumshields
The Irish Dental Association recently welcomed the decision by the GAA to make it compulsory for players to wear mouth guards in football games and training.
At the weekend GAA Congress passed a motion making it mandatory for juvenile players up to minor grade to wear mouth guards from the start of 2013. The rule will come into effect for senior players from the start of 2014.
While some senior inter-county players have already expressed reservations about the rule, Dr Maurice Quirke of the Irish Dental Association has urged all players, parents and coaches to support it fully.
‘Anybody who is playing contact sports without a mouth guard is being irresponsible. It’s like going on a motorbike without a helmet. I would urge all players to protect their teeth from injury by using a gumshield immediately. Players are important role models for children so it is particularly important that they back the move’ Dr Quirke said.
IDA figures indicate Ireland has one of the highest rates of sport-related oral injuries in the EU, with one third of all adult dental injuries being sports-related. In many sports such as rugby and hockey the wearing of gumshields is the norm with nearly all clubs adhering strictly to a ‘no gumshield – no game’ rule. The IDA believes parents and coaches in particular will have a key role to play in ensuring a similar situation pertains in gaelic football for young players.
Dr Quirke, who is based in New Ross, Co Wexford, said that some players were put off by ill fitting gumshields and it was important to ensure the mouth guard was as good a fit as possible.
The Irish Dental Association believes the gumshield rule should also apply to hurling and it is hopeful the GAA will introduce a similar measure for that sport in the near future.
11
News for IPNA br ANches couNtry wIde regional news
cArlow
KATE ATTRIDE
The second official meeting of the newly formed Carlow branch of the IPNA was held in Teach Dolmen, Tullow St, Carlow on Mon 26th March. The meeting was sponsored by MSD. Presentation and talk was given by Dr Deirdre lundy on women’s health with an update on contraception. The meeting was well attended by practice nurses and Nurses from Caredoc.
New members wishing to join can contact Kate on 086 3598363.The next meeting, which will be on COPD, will take place on Tuesday 15th May. The meeting is sponsored by Novartis and the talk will be given by Kate Walsh, Respiratory Nurse Specialist, from St luke’s Hospital Kilkenny.
The NEC meeting is on Wednesday 2nd May in Dublin and Nurse liz Carroll will obtain a report from this meeting. The IPNA AGM will be held on 5/6th October in Tullamore Court Hotel and is hosted by the Cavan/Monaghan branch. An IPNA education bursary of €1000 euro is available. Each branch can nominate one nurse: members are encouraged to put names forward for this.
cAvAN/MoNAghAN
PATRICIA JENKINS
Our meeting in March was sponsored by Elaine O’Shaughnessy from Cow & Gate. Ms Clodagh Dolan, a community pharmacist, discussed various relevant topics and answered any questions that we had in relation to over-the-counter medications.
In April, Mr Turlough Farnan, ENT consultant at Monaghan General Hospital, gave us an update on services that they provide for children and adults. He provides a clinic one day a week which is funded by CAWT. There are plans for a second ENT consultant to start soon. Although there are long waiting lists, Mr Farnan will see patients at short notice if a GP contacts him directly. Mr Farnan stressed that it is best practice to refer patients with any swellings or lumps around the neck or face to an ENT consultant rather than a surgical or medical consultant. The meeting was kindly sponsored by Teresa O‘Regan from GSK. Both of these meetings were held in Errigal House Hotel and was very well attended by members. Winny McCabe, INO rep. discussed with us the importance of checking that our employers have medical insurance paid for practice nurses, as it should never be assumed that it is being paid.
The preparations for this year’s IPNA’s AGM is well underway and we hope that as many nurses as possible will attend this year’s conference in Tullamore in October 2012.
cork
ElAINE GOGGIN
We had our last meeting on April 25th, Guest speaker, Una O’Neill, Diabetes CNS, gave a very informative talk on diabetic neuropathy including assessment and clinical guidelines. There was a good attendance and the topic was well received. Thanks to Elaine Dineen, Eli lilly, for sponsorship of the meeting.
The topic for our March meeting was Parkinson’s disease and Alison Cashell, Parkinson’s Nurse, gave a very relevant overview. This was kindly sponsored by the Parkinson’s Society of Ireland. Our next meeting will be held at Rochestown Park Hotel on May 23rd when the focus will be on RAST testing.
Members are also completing the Asthma Society’s elearning course and practical demonstrations are being held in the next couple of months. Some members also attended an information afternoon on childhood obesity, organised by the Health Promotion Unit; this was found to be very relevant and beneficial.
We would like to thank our members for their continued support and welcome new members.
doNegAl
BRIDGET BREEN
Our first spring meeting in February 2012 held in the Station House Hotel was sponsored by Chris Kenny from Johnson & Johnson, Smoking Cessation Officer, Fiona Boyle, gave a very intensive talk on her role in helping people to give up the dreaded weed. In March, Kevin O’Donnell, for Astra Zenica sponsored our meeting. Patricia Mclaughlin, Respiratory Nurse Specialist, gave a demonstration on inhaler technique etc. This was well timed as some of the practice nurses are doing the on-line asthma course that the Asthma Society are making available free of charge. April 25th saw us all back in the Raddison for a very interesting and engaging overview of dementia given by Grace Kelly. She maintained the audiences attention throughout the talk and answered numerous questions from the floor. Brian Horkan from lundbeck kindly sponsored the evening. To finish off the evening, Elsie, lorraine and Helen, our hardworking outgoing officers were presented with a voucher and crystal bowl, engraved with the IPNA logo, in recognition of their time spent at the helm during which, amongst all their other duties they organised the AGM in 2010, which was a great success. Well done girls We have big boots to fill! Next meeting in the Raddison , May 22nd.
Finally we would like to extend sympathy to our colleague, Kathy Taffee and her family, on the untimely death of her father, Hugh Duffy which occurred recently at his home in Ballybofey. Ar dheis de go raibh sè.

12
News for IPNA br ANches couNtry wIderegional news
NorTh dublIN
lIZ HEAlY
This year has been busy with our monthly meeting. January was sponsored by Movicol; the rep gave us an insight into its use and paediatric dosages. February’s speaker was from Yakult. Deirdre’s talk was very informative, explaining the research behind the benefits of probiotics. Our speaker for March was our community tissue viability nurse – Fiona. Her presentation showed us the different groups of dressing and when and how to use them. She has kindly offered anyone who would like to attend one of her clinics to contact her.
Our most recent meeting was kindly sponsored by AstraZeneca. The guest speaker was Ruth lunnon from Headway. Her talk was very interesting and gave us all information on services available in different types of acquired brain injury.
Our meeting in May will be the last meeting organised by the present committee, as myself, Brid Buckley and Siobhan Moore will be stepping down and a new committee will be voted in at our AGM in September. I would like to say that I have enjoyed the last two years and have made some good friends in Siobhan and Brid.
Finally, congratulations to Johanna Walsh, Siobhan Moore and Niamh Byrne on the birth of their respective babies.
kerry
JOANIE MURPHY
Hi to all from the Kerry Branch. Our March meeting took place in the Carlton Hotel Tralee on Wednesday 21st March. It was sponsored by GSK, our Rep was Richard Hayes and our guest speaker was louise Mannion. louise is the scientific adviser for GSK and she gave us a very informative talk on the topic of travel vaccines. Richard also gave us an update on the drug Prolia. We had our next meeting on Wednesday 18th April and the Carlton was the venue yet again. Elaine Dineen and Flor O’leary from lilly and Boehringer Ingelheim sponsored our meeting on the night. Dr James Ryan, endocrinologist, from the Bon Secour Hospital, Tralee spoke to us about type 2 diabetes and the most recent and up-to-date medicines avaliable to treat this condition. Our next meeting which will be our last one before the summer is being held in Killarney and will be on Wednesday 23rd May in the Malton Hotel.
I hope everyone will have a very enjoyable summer and that the sun will shine.
kIlkeNNy
lEONIE FINNEGAN
We have had two very interesting educational updates since our last local news update. Our March educational and networking opportunity was sponsored by Novo Nordisk with Aine McGrath, Senior Diabetic Care Specialist. Aine gave a brief overview on Victoza, the once daily non-insulin injectable medication that may help improve blood glucose levels in adults with type 2 diabetes.
Following on, lisa Hennessy, Diabetic Nurse Educator then introduced us to MERIT the diabetes education programme designed for primary care professionals. This modular programme is tailored to fit the needs of a busy primary care practice and has been developed by Novo Nordisk, using a team of medical writers and reviewed by a panel of GPs. lisa is available to come to any practice and will provide a flexible classroom based education course designed to provide delegates with the theory required to support diabetes management. A minimum requirement for this is one GP and one PN.
We can only welcome such initiatives, which will serve to improve management of patients with type 2 diabetes in primary care. This will assist in improving the outcome for diabetic patients in our care, as potential complications are identified and managed effectively. A timely reminder too, from Patricia McQuillan, that we have the upcoming Diabetes Care Programme on 10 May 2012 with further dates following for Kilkenny/Carlow area. Useful supports available are: NICE guidelines on diabetes, while the HSE has approved the appointments of 3 podiatrists in the South East and we welcome Sian Stokes, who will be Waterford based.
Our second meeting, in April, was sponsored by Galderma, though local Rep. Maria Mc Elwee and was dermatology based. Fiona Reid nurse specialist travelled from England to educate and update on fungal infections and childhood eczema. We were treated to a lecture on both areas and updated on diagnosis, treatment options and current practice and advice. Both topics were extremely relevant to all attending and an interactive and lively session resulted, with questions, queries and debate, halted only by time. We are already looking forward to the next educational dermatology session with Fiona.
Our final meeting this term will be on May 23rd in Pembroke Hotel, Kilkenny sponsored by MSD and our guest speaker is Dr Melanie O’Reilly, on Women’s Health matters to include fertility and observations at smear taking. We would encourage all our members to attend and always look forward to welcoming new members also. We are grateful to and wish to thank all our reps and the pharmaceutical companies for their on-going support, for education and networking in our branch throughout the year and look forward to the next term. We wish each of you and all of us, a healthy, calm and sun-filled summer!
13
News for IPNA br ANches couNtry wIde regional news
wIcklow
MARY FINNEGAN
We held an excellent educational meeting on Monday 16th April, in Bray. The topic was the Prevention and Management of Diabetic Foot Care Complications. This was presented as a mini course, and carried ABA Category 1 certification. The course was facilitated by Ms Una O’ Neill, Diabetic Foot Care Nurse, with Ashfield Healthcare, who sponsored the course on behalf of Ely lilly. The course was well attended with half of our current members present, and consisted of both theoretical and practical content, involving the participation of all the nurses present, and their feet! It was a very interesting and helpful course, and very worthwhile doing. Una is also happy to provide further training in our surgeries, or visit to advise at any stage.
Our final meeting before the ‘summer’ break will be on Monday 28th May at 8pm in Wilton Hotel (formerly Ramada) Bray. It is hoped to have a talk on hypercholesterolaemia (TBC). At the April meeting, about 10 members requested an up to date BlS +AED course, as their current certs run out shortly. The plan is to arrange this for the nurses, within next few weeks.
As I write this on the last day of April, the wind is howling, the rain is pouring down, and it is so cold! But hopefully, by the time you read this, we might be at the start of some good summer weather (and sincerely hope that the sun and warm days of March, were not all we get this year!)= look forward to seeing you all at the May meeting, before we take our summer break. Branch meetings will resume again in September, and a reminder that the Annual Conference will be held in Tullamore the first weekend in October. Start planning your weekend away now! Hopefully, we will have several members from Wicklow attending the conference.
Finally, I just want to say a big thank you to all Wicklow Branch members who have attended meetings since last September. Your support, and enthusiasm is great, and it has been wonderful to see our attendance numbers steady, averaging out at 22-25 per meeting. This has been very encouraging, and is keeping your branch alive! Also many thanks to the hard working officers, especially the NEC and INMO reps who attend meetings in their time off, on our behalf, and of course our excellent Treasurer and Secretary. My job as Chair, is so much easier with the excellent support of these four lovely ladies!
Thank you to all and hope you all have a happy, healthy, safe summer.
Practice nurserequired
Practice nurse required for a busy long established practice in Dublin 15. Modern and fully computerised. Initially 2 sessions per week approximately 8 hours in total.
Previous experience: venepuncture, cervical smears, vaccinations, antenatal care. General practice experience an advantage.
Please forward your CV to Julianne O’Brien Gill Email: [email protected]
Part time practice nurserequired
Three mornings and 1 afternoon per week in a fully computerised practice in Kilmacud/Stillorgan, Co Dublin. Previous experience in a similar role desirable as the practice offers a full range of services including phlebotomy, childahood/travel vaccinations, CervicalCheck and cyrotherapy. Good IT skills essential.
Forward CV plus covering note to [email protected]
Practice nurserequired
Glasnevin family practice seeks practice nurse to work as part of our team commencing July 2012. Duties include phlebotomy, childhood immunisations, cervical screening, travel vaccinations etc.
Please e-mail CV to [email protected].
educATIoN seMINAr
Palliative care in the communitykeynote speaker:
Professor Catriona Kennedy, Department of Nursing and Midwifery, University of limerick
29th May 2012 at 19:00 Dept of Nursing & Midwifery, Health Sciences Building
Please register to attend Email: [email protected]

Picture gallery
14
IPNA Conference 2011
A look back at the 2011 IPNA conferenceThe IPNA South Tipperary host branch would like to thank most sincerely all who attended, presented, sponsored and helped in any way with the running of the conference in 2011. Thanks to all those Practice Nurses who attended, for their enthusiasm and support, ensuring the resounding success of our national educational conference.
eileen brennan, bernie bourke, Tara bourke, Mary hunter, south Tipperary at registration desk.
National chair 2012, roisin
doogue with vice-chair,
siobhan Jordan.
siobhan Jordan, south Tipperary, orla loftus-Moran, IPNA National chair 2011, Pierce finegan IcgP, and Judy hayes, south Tipperary.
siobhan Jordan, host branch chair, orla loftus-Moran, National chair, eileen brennan PN, cNs general Practice rNP, with lisa Nolan, Administrator IPNA.
Presentation to winners of the inaugural
pharmaceutical award voted by
the delegates. Tina breen,
Promed (corporate
sponsor of the conference),
with Judy hayes.
felicity keenan, south Tipperary
host branch, presenting
cheque from proceeds
of raffle to susie brock,
cystic fibrosis Association.
recipients of the valarie Mangan Award.

15
IPNA Conference 2012
2012 IPNA National conferenceThis year’s IPNA National Educational Conference & AGM will take place in The Tullamore Court Hotel on the 5th and 6th October 2012. This annual conference has proven to be a firm favourite with practice nurses – both IPNA members and non-members. The conference aims to deliver high quality up-to-date evidence based workshops and presentations, and also provides a forum for colleagues and friends to meet and socialize.
The Tullamore Court Hotel is a beautiful centrally located venue with high class conference facilities. This year’s conference will hosted by the Cavan Monaghan Branch IPNA, and is open to all Practice Nurses both members and non-members of IPNA to attend.
Registration will take place between 2.00 and 4.30pm on Friday 5th, viewing of the pharmaceutical exhibition will continue until 4.45pm to allow you plenty of time to visit the stands at your leisure.
On Friday afternoon we have three workshops which will take place between 5.00 and 6.30pm, delegates may choose two out of the following three workshops to attend, Ear care and Syringing, Diabetic Foot Assessment and Caring for Patients on Warfarin therapy. There will be a half hour break before the evening events start with the Conference Gala Dinner at 7.00pm followed by the keynote speaker Dr Tony O’Sullivan (GP in Irishtown, Dublin) will give a talk on living with Diabetes. At 8.30pm the presentation of three awards, the Research Bursary Award, the Clinical Award and the Practice Nurse of the Year 2012, will take place.
Saturday the 6th October will commence at 8.30am with viewing of the Pharmaceutical Exhibition until 10.00am. Followed by the first speaker Dr Deirdre lundy (GP in Bray, Co. Wicklow) who will give a talk Menopause and HRT. At 10.45am Ms Susan McKenna (CNS in Renal in Cavan General Hospital) will give a talk on Chronic Renal Disease with a break at 11.30am for refreshments and Pharmaceutical Exhibition viewing until 12.30pm. Ms Martina Carolan (CNS Rheumatology in Navan) will give the final talk of the morning on Rheumatoid Arthritis.
Before lunch, presentation of the Valerie Mangan IPNA loyalty Award for Practice Nurses who have attended six or more branch meetings during the year, will be made. The pharmaceutical award will be presented to the exhibit that the nurses voted best presentation and information relevant to primary care. The AGM will follow lunch at 2.30pm.
All Practice Nurses wishing to join us should register using the IPNA web site where the registration form and details can be downloaded. For IPNA members registering on or before 11th August the cost will be €75, after this date the conference fee is €90. For any IPNA member wishing to attend on Saturday, the fee is only €60. For non-members wishing to attend the conference the fee is €120.
All delegates wishing to reserve accommodation should contact the Tullamore Court Hotel directly; the venue has been blocked booked on a first come first served basis.
looking forward to seeing you all there and wishing the Cavan Monaghan Conference the best of luck in their endeavours.
Judy Hayes, PRO IPNA
01-1
4-W
OMN
-102
3212
-000
1
NXT®
Getting pregnant may be in her plans one day.Just not today.
Pelham House, South County Business Park, Leopardstown, Dublin 18, Ireland
Legal Category: Prescription Medicine Marketing Authorisation Number: PA 61/28/1. Marketing Authorisation Holder: Organon Ireland Limited, P.O. Box 2857, Drynam Road, Swords, Co. Dublin, Ireland.Please refer to the full SPC text before prescribing this product.Date of review: January 2012.Further information is available on www.medicines.ie or on request from: MSD Pelham House, South County Business Park, Leopardstown, Dublin 18.
www.talkoptions.ie
16
IPNA clinical award 2012
IPNA Clinical Award 2012 (Smoking Cessation)The IPNA and Nursing in General Practice are delighted to announce the IPNA Clinical Award 2012, kindly supported by an unrestricted educational grant from Pfizer. This year the award is focused on Smoking Cessation and the winner will receive an educational bursary of €1,000.
how To eNTer Below is a case study accompanied by a set of questions that must be answered within the word limit of 1,500. Please e-mail your completed answers, along with your name, An Bord Altranais PIN and full contact details to [email protected]
Closing date for receipt of entries is Friday 10th August 2012. The winner will be notified by telephone before the conference. The result will be announced and Certificate and Award will be presented to the winner at the IPNA Annual Educational Conference in Tullamore on 5th October 2012 if they are in attendance. The winner will also be announced on the IPNA website after the conference and the winning entry will be published in a later issue of Nursing in General Practice.
rules• Entrants must be on the current register of An Bord Altranais in either the RGN or PHN divisions. The Bord Altranais PIN must
accompany each entry for verification.• Entrants must be a current member of the Irish Practice Nurses Association.• Entrants must answer all questions.• Word limit for entries is 1,500.• Entrants must submit their entry on or before the closing date.• Joint entries will not be accepted.• The judges’ decision is final and no correspondence will be entered into.
Kindly supported by an educational grant from Pfizer
cAse sTudySarah is a 61 year old lady who has recently been investigated at her local general hospital for episodes of tachycardia and chest tightness which she has experienced intermittently over the past six months. Sarah has a positive family history for coronary heart disease, her other cardiovascular risk factors include raised cholesterol; currently smoking 20 cigarettes per day.
Sarah has recently had a gastroscopy which indicated gastric inflammation and has been commenced on medication with good effect.
Sarah’s cardiac investigations, including the Echo cardiograph, exercise stress test and 24 hour holter monitor reports, are within normal limits. During her visit to the hospital Sarah has been told she needs to stop smoking.
MedicationAtorvastatin 20mgs od.Omeprazole 20mgs od.
Sarah has returned today to her own GP to obtain the outstanding results of her recent blood tests and would like to receive information and assistance to stop smoking.
Questions.
1. Outline the principles of brief intervention in smoking cessation?
2. Explain the Model of Behaviour Change (cycle of change)?
3. How you would apply these principles to effectively support Sarah in her smoking cessation attempt?
4. Considering the constituents of tobacco, explain the health risks associated with tobacco use and the major disease associated with smoking?
5. Outline how smoking adversely effects the cardiovascular/circulatory system.
6. What are the immediate and longer term benefits associated with stopping smoking?
7. Explain the Fagerstrom score and outline how we can use this tool to evaluate person nicotine dependence?
8. Identify the pharmacological therapies available to assist in smoking cessation and outline their efficacy?
9. What are the perceived barriers to smoking cessation education being delivered in a primary care setting?
10. What systems do you think could be introduced to overcome such barriers?
18
clinical review
Chest pain, dyspnoea, palpitations and syncope are the most common symptoms experienced by patients with cardiovascular disease. These symptoms are not unique to cardiac disease and are also frequently caused by relatively benign
conditions including musculoskeletal injuries, respiratory tract infections or simple faints. Caution must always be exercised when dealing with such symptoms, because in a small yet significant percentage of people they are a warning of a potentially life-threatening cardiac event. Differentiating the benign from the more serious is often clinically challenging.
In the majority of cases, particularly in rural areas, the GP or primary care centre is the first point of contact for patients. It is in this arena that the seriousness of the presenting symptom must be determined. Critical to this assessment is the clinical history. A carefully performed and properly interpreted clinical history and physical examination will provide clinicians with sufficient information to accurately risk-stratify patients.
When considering whether a symptom is cardiac in origin, the clinician should determine the individual’s probability of having cardiac disease. There is empirical evidence to support the association between hypertension, hypercholesterolaemia, cigarette smoking, diabetes, obesity, age and family history with an increased probability of disease occurrence. In the case of coronary heart disease, the more risk factors a person has, the more likely they are to develop the disease. A second variable worth considering is the patient’s exercise tolerance. Myocardial function is closely related to exercise and many cardiac symptoms are exacerbated by exercise. Specific attention should therefore be placed upon the relationship between symptoms and functional capacity.
symptomsCoronary heart disease is still ranked as one of the biggest killers in Ireland and chest pain is its cardinal symptom. Despite this prevalence the majority of chest pain presentations are non-cardiac in origin. Knowledge of main features of different causes of pain will assist clinicians in differentiating the benign from the serious.
cardiac chest pain Angina, or cardiac chest pain. is a product of myocardial ischaemia, which occurs when there is an imbalance between coronary blood flow and myocardial oxygen demand. In the
majority of cases this is caused by a fixed obstruction (plaque) in the artery or, in the case of a myocardial infarction, the formation of a blood clot on an area of ruptured plaque.
Cardiac chest pain is typically described as ‘tightness’, ‘pressure’ or ‘squeezing’ in nature, and it may radiate to the arms or neck. It is often associated with dyspnoea, nausea and diaphoresis. Stable angina is typically predictable, brought on by exertion and is always relieved with rest. Angina that accelerates in severity or frequency or that occurs at rest or with minimal activity is termed ‘unstable angina’ and often signifies critical coronary disease. Unstable symptoms warrant prompt hospital treatment. Prolonged cardiac chest pain, i.e. greater than 20 minutes in duration should make clinicians suspicious of myocardial infarction where thrombus partially or totally occludes the coronary artery. This condition should be treated as a cardiac emergency and referred to hospital by ambulance.
It should be noted that not all patients with cardiac ischaemia present with typical chest pain – for some the presentation is vague and atypical. This sub-group may describe symptoms such as epigastric fullness, profound lethargy or left arm heaviness. Women, the elderly and persons with diabetes are more likely to experience atypical symptoms.
Cardiac pain can often be differentiated from non-cardiac pain by simple assessment or questioning techniques. Chest pain exacerbated by inspiration or coughing is more likely to be respiratory in origin, whereas chest pain reproduced by movement and associated with chest wall tenderness is more likely to have a musculoskeletal aetiology. Intermittent darts of pain lasting seconds, or constant pain lasting days weeks or months is unlikely to have a cardiogenic origin. Knowledge of discriminating factors together with an assessment of the patient’s probability of having coronary disease can be invaluable in guiding clinical decision–making.
shortness of breathDyspnoea, shortness of breath, is a common symptom and indeed most of us will experience it on occasion. Clinicians must be able to differentiate appropriate from inappropriate dyspnoea. It is normal for a person to feel breathless after running up flights of stairs, and inappropriate for someone to be breathless after walking short distances or at rest. Once we have clarified the dyspnoea as inappropriate, we should then attempt to identify the causative pathology. Typically
differentiating cardiac from non cardiac symptoms This paper focusses on the assessment and risk stratification of patients presenting with the most common cardiac symptoms in a primary care setting.
lIsA browNe, ADVANCED NURSE PRACTITIONER, ACUTE CARDIOlOGY UNIT, MATER MISERICORDIAE UNIVERSITY HOSPITAl
19
clinical review
dyspnoea is caused by either a pulmonary or a cardiac cause. Cardiac dyspnoea occurs primarily due to pulmonary venous congestion, occurring when the heart’s pumping action has become weakened. When left atrial pressure rises as seen in aortic and mitral valve disease or in left ventricular dysfunction, the pulmonary veins become distended and the bronchial walls become congested and oedematous. As pulmonary venous pressure rises further lung tissue becomes stiffer due to interstitial oedema, this impedes lung inflation causing dyspnoea. As the condition worsens, fluid engorges the alveoli resulting in pulmonary oedema.1 This type of dyspnoea is often worsened by lying flat (orthopnoea) or may wake the patient from sleep (paroxysmal nocturnal dyspnoea). Although cardiac dyspnoea may occur acutely (flash pulmonary oedema), it is more commonly a gradually worsening process. Acute onset dyspnoea should make one consider other causes such as pulmonary emboli or pneumothorax. Whatever the underlying cause, acute onset dyspnoea warrants acute assessment.
Cardiac dyspnoea may also be ischaemic in origin. Some patients experience exertional dyspnoea as an anginal equivalent. This is caused by left ventricular dysfunction occurring due to myocardial ischaemia, which typically subsides with rest. This variant of angina is more common in women, the elderly or those with diabetes.
Palpitations Palpitations are a common symptom and are often a benign awareness of one’s heart beat. Normally the heart beats in a regular rhythm, though occasionally extra or premature ectopic beats occur that disturb the regularity of the rhythm. The majority of these are benign and occur in structurally normal hearts. Indeed most people will experience some sort of fluttering or awareness of their heart rhythm in their lifetime. These symptoms may be particularly prevalent during times of emotional stress, after excessive alcohol consumption, or drinking caffeine-rich products. For the most part these symptoms resolve themselves; they can however be a source of significant anxiety for patients particularly if they are ongoing. Patients should be advised that identifying the stimulant and reducing its consumption may reduce the frequency of the events.
Irregular or very rapid heart beats may occur in patients with or without structural heart disease. Atrial fibrillation (AF) is the most common cardiac arrhythmia with a prevalence approximated at 1% of the population; this rate increases exponentially with age, reaching up to 9% in octogenarians.2 While AF may be well-tolerated from a symptomatic viewpoint it is an important cause of cardiovascular mortality and morbidity. AF increases the risk of clot formation within the left atrium, which may subsequently embolise into the systemic circulation causing an ischaemic stroke. In patients with non-valvular atrial fibrillation, the risk of ischaemic stroke averages 5% per year.3 A diagnosis of AF should be suspected when the apex or radial pulse is irregular and should be confirmed with an ECG.
Occasionally palpitations are symptomatic of a more serious cardiac arrhythmia such as ventricular tachycardia. This potentially life-threatening arrhythmia is usually seen in patients with underlying heart disease. In this arrhythmia the heart rate may approach or even exceed 200 beats per minute; this is usually associated with profound symptoms including chest pain and dyspnoea, leading to full cardiovascular collapse and cardiac arrest. In general, palpitations associated with symptoms of chest pain, dyspnoea, dizziness or syncope indicate cardiac compromise and therefore warrant acute assessment.
syncopeSyncope is defined as “transient loss of consciousness due to transient global cerebral hypoperfusion”4 and is usually associated with a fall. There are numerous causes ranging from a simple faint (vaso-vagal syncope) to more serious causes including obstructive cardiac lesions (aortic stenosis) or cardiac arrhythmias (sinus arrest, heart blocks or ventricular tachycardia). The key to differentiating cardiogenic from non-cardiogenic syncope is the history and physical examination, paying particular attention to prodromal features, duration of unconsciousness and the presence or absence of seizure activity. It is often essential to obtain a witness’ account of events. Cardiogenic syncope is typically very transient (seconds), without warning, though the patient rapidly recovers. Assessment of patient activity immediately prior to the event is often helpful. Activities such as prolonged standing may suggest a vasovagal cause – syncope occurring immediately after standing suggests orthostatic hypotension while loss of consciousness occurring while lying or with exertion is more likely to be cardiac. Prolonged loss of consciousness associated with seizure-like activity, tongue-biting and incontinence is unlikely to be a syncopal episodes; such features are more typical of a neurological focus.
conclusion The importance of identifying cardiac symptoms early cannot be over-emphasized, as most of the treatments for acute cardiac dysfunction are time dependant. Several discriminating factors as mentioned above could assist clinicians to differentiate cardiac from non-cardiac symptoms. Using this information together with a comprehensive clinical history should provide clinicians with sufficient information to accurately risk-stratify their patients. In cases of uncertainty particularly in patients with significant risk factors for cardiac disease one is always best taking the cautious route and referring the patients for further evaluation.
references1. Gray H. et al (2008) lecture Notes – Cardiology. 5th ed. Blackwell Publishing.
Southampton, UK.2. Fuster V. et al. ACC/AHA/ESC (2006) Guidelines for the management of patients
with atrial fibrillation. Journal of American College of Cardiology. 48: 854-9063. Medi C. et al. Atrial Fibrillation (2007) MJA, 186 (4) 197-202 4. European Society of Cardiology (2009) Guidelines for the diagnosis and
management of syncope (version 2009). European Heart Journal. 30 2631-2671
The importance of identifying cardiac symptoms early cannot be over-emphasized, as most of the treatments for acute cardiac dysfunction are time dependant.

Powerful glucose reductions to help get patients to goal1,a
For patients not adequately controlled on metformin alone,
(sitagliptin/metformin)
Glucose reductions at 24 weeks
PPGFPGJANUMET 50/1000 mg twice daily
HbA1c primary end point
–2.1%
–3.9 mmol/L – 6.5 mmol/L(n=180; mean
baseline 10.9 mmol/L; P≤0.001)(n=152; mean
baseline 15.9 mmol/L; P≤0.001)
vs placebo(n=178;
mean baseline 8.8%; P≤0.001)
All-patients-treated population.
Additional HbA1c results at 24 weeks1,a
• 1.3% placebo-adjusted HbA1c reduction with metformin 1000 mg twice daily (n=177; mean baseline 8.7%; P≤0.001)
• 1.6% placebo-adjusted HbA1c reduction with JANUMET™ (sitagliptin/metformin, MSD) 50/500 mg twice daily (n=183; mean baseline 8.8%; P≤0.001)
• 1.0% placebo-adjusted HbA1c reduction with metformin 500 mg twice daily (n=178; mean baseline 8.9%; P≤0.001)
• 0.8% placebo-adjusted HbA1c reduction with sitagliptin 100 mg once daily (n=175; mean baseline 8.9%; P≤0.001)
JANUMET: Powerful efficacy
to help get patients to goal1
As an adjunct to diet and exercise, For patients uncontrolled on metformin alone2
In combination with a glitazone or sulfonylurea2
In combination with insulin2
✔
✔
✔
07-1
2-JM
T-20
11-IR
L-47
07-J
JANUVIA® Sitagliptin JANUMET® Sitagliptin/metformin hydrochlorideABRIDGED PRESCRIBING INFORMATION Refer to Summary of Product Characteristics (SmPC) before prescribing PRESENTATION Januvia® 100 mg film-coated tablet containing 100 mg of sitagliptin. Janumet® 50 mg/850 mg and 50 mg/1000 mg tablets each contain-ing 50 mg sitagliptin and 850 mg or 1000 mg metformin hydrochloride. USES For patients with type 2 diabetes mellitus Januvia is indi-cated to improve glycaemic control: as monotherapy • in patients inadequately controlled by diet and exercise alone and for whom metformin is inappropriate due to contraindications or intolerance as dual oral therapy in combination with • metformin when diet and exercise plus metformin alone do not provide adequate glycaemic control • a sulphonylurea when diet and exercise plus maximal tolerated dose of a sulphonylurea alone do not provide adequate glycaemic control and when metformin is inappropriate due to con-tra-indications or intolerance • a PPARγ agonist (i.e. a thiazolidinedione) when use of a PPARγ agonist is appropriate and when diet and exercise plus the PPARγ agonist alone do not provide adequate glycaemic control as triple oral therapy in combination with • a sulphonylurea and metformin when diet and exercise plus dual therapy with these agents do not provide adequate glycaemic control. • a PPARγ agonist and metformin when use of a PPARγ agonist is appropriate and when diet and exercise plus dual therapy with these agents do not provide adequate glycaemic control. Januvia is also indicated as add-on to insulin (with or without metformin) when diet and exercise plus stable dosage of insulin do not provide adequate glycaemic control. Janumet: as an adjunct to diet and exercise to improve glycaemic control in patients inadequately controlled on their maximal tolerated dose of metformin alone or those already being treated with the combination of sitagliptin and metformin. • in combination with a sulphonylurea (i.e., triple combination therapy) as an adjunct to diet and exercise in patients inadequately controlled on their maximal tolerated dose of metformin and a sulphonylu-rea. • as triple combination therapy with a PPARγ agonist (i.e., a thiazolidinedione) as an adjunct to diet and exercise in patients inad-equately controlled on their maximal tolerated dose of metformin and a PPARγ agonist. • as add-on to insulin (i.e., triple combination therapy) as an adjunct to diet and exercise to improve glycaemic control in patients when stable dosage of insulin and metformin alone do not provide adequate glycaemic control. DOSAGE AND ADMINISTRATION Januvia - One 100 mg tablet once daily, with or without food. Janumet - The dose of antihyperglycaemic therapy with Janumet should be individualised on the basis of the patient’s current regimen, effectiveness, and tolerability while not exceeding the maximum recommended daily dose of 100 mg sitagliptin. For patients not adequately controlled on metformin alone, the usual starting dose of Janumet should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) plus the dose of metformin already being taken. For patients switching from co-administration of sitag-liptin and metformin, Janumet should be initiated at the dose of sitagliptin and metformin already being taken. For patients inadequate-ly controlled on dual combination therapy with the maximal tolerated dose of metformin and a sulphonylurea or with maximal tolerated dose of metformin and a PPARγ agonist or with maximal tolerated dose of metformin and insulin, the dose of Janumet should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) and a dose of metformin similar to the dose already being taken. All patients should continue their diet with an adequate distribution of carbohydrate intake during the day. Overweight patients should continue their energy-restricted diet. Januvia and Janumet - In combination with a sulphonylurea or with insulin, consider a lower dose of sulphonylurea or insulin, to reduce risk of hypoglycaemia. Renal impairment: See Precautions. Hepatic impairment: For Janu-via only - no dosage adjustment necessary for patients with mild to moderate hepatic impairment. Januvia has not been studied in patients with severe hepatic impairment. For Janumet only – do not use. Elderly < 75 years: For Januvia only - no dosage adjustment necessary. For Janumet only - use with caution as age increases. Monitoring of renal function is necessary to aid prevention of met-formin-associated lactic acidosis. Elderly ≥ 75 years: Exercise care as there are limited safety data in this population. Children: not recommended below 18 years of age. CONTRA-INDICATIONS For Januvia - Hypersensitivity to active substance or excipients. For Janumet - Hypersensitivity. Diabetic ketoacidosis and diabetic pre-coma. Moderate and severe renal impairment (creatinine clear-ance < 60 ml/min). Acute conditions with the potential to alter renal function such as dehydration, severe infection, shock. Intravascu-lar administration of iodinated contrast agents. Acute or chronic disease which may cause tissue hypoxia such as cardiac or respira-tory failure, recent myocardial infarction, shock. Hepatic impairment. Acute alcohol intoxication, alcoholism. Lactation. PRECAUTIONS For Januvia and Janumet - General: do not use in patients with type 1 diabetes or for diabetic ketoacidosis. Pancreatitis: Post-market-ing experience - spontaneously reported adverse reactions of acute pancreatitis. Inform patients of the symptom of acute pancreati-tis: persistent, severe abdominal pain. Resolution of pancreatitis has been observed after discontinuation of sitagliptin, but very rare cases of necrotizing or haemorrhagic pancreatitis and/or death have been reported. If pancreatitis is suspected, Januvia or Janumet and other potentially suspect medicinal products should be discontinued. Hypoglycaemia when used with other anti-hyperglycaemic agents: Rates of hypoglycaemia reported with sitagliptin were generally similar to rates in patients taking placebo. When sitagliptin was added to a sulphonylurea or to insulin, the incidence of hypoglycaemia was increased over that of placebo; therefore consider a lower dose of sulphonylurea or insulin to reduce the risk of hypoglycaemia when administering Janumet or Januvia. Hypersensitivity reactions: Serious hypersensitivity reactions have been reported, including anaphylaxis, angioedema, and exfoliative skin conditions including Stevens-Johnson syndrome. Onset occurred within the first 3 months after initiation of treatment with some reports occur-ring after the first dose. If suspected, discontinue Januvia or Janumet. For Januvia only - As experience is limited, patients with moderate or severe renal impairment should not be treated with Januvia. For Janumet only - Lactic acidosis and renal function: a very rare, but serious, metabolic complication can occur due to metformin accumulation. Cases in patients on metformin have occurred primarily in diabetic patients with significant renal failure. Reduce incidence by assessing other associated risk factors. If suspected, discontinue treatment and hospitalise patient immediately. If changes in clinical status of patients with previously controlled type 2 diabetes occurs, evaluate promptly for evidence of ketoacidosis or lactic acidosis in any patient with type 2 diabetes previously well
controlled on Janumet who develops laboratory abnormalities or clinical illness (especially vague and poorly defined illness). If aci-dosis of either form occurs, stop Janumet immediately and initiate corrective measures.Determine serum creatinine concentrations regularly, i.e. at least once a year in patients with normal renal function and at least two to four times a year in patients with serum creatinine levels at or above the upper limit of normal and in elderly patients. Decreased renal function in elderly patients is frequent and asymptomatic. Exercise special caution where renal function may become impaired, e.g. when initiating antihypertensive or diu-retic therapy or when starting treatment with a non-steroidal anti-inflammatory drug (NSAID). Surgery: due to metformin hydrochlo-ride content of Janumet, discontinue treatment 48 hours before elective surgery with general, spinal or epidural anaesthesia. Do not resume earlier than 48 hours afterwards and only after renal function is normal. DRUG INTERACTIONS For Janumet only - Alcohol: avoid alcohol and medicinal products containing alcohol due to risk of lactic acidosis. Cationic agents that are eliminated by renal tubular secretion (e.g., cimetidine): these may interact with metformin by competing for common renal tubular transport systems. Consider close monitoring of glycaemic control, dose adjustment within the recommended posology and changes in diabetic treat-ment when these agents are co-administered. Iodinated contrast agents in radiological studies: intravascular administration of these agents may lead to renal failure, resulting in metformin accumulation and a risk of lactic acidosis. Discontinue Janumet prior to, or at the time of the test and do not reinstitute until 48 hours afterwards, and only after renal function is found to be normal. Combination requiring precautions for use: glucocorticoids (given by systemic and local routes) beta-2-agonists, and diuretics have intrinsic hyper-glycaemic activity. Inform the patient and perform more frequent blood glucose monitoring, especially at the beginning of treatment. If necessary, adjust dose of the anti-hyperglycaemic medicine during therapy with, or on discontinuation of the other medicine. ACE-inhibitors: as these may decrease the blood glucose levels, if necessary, adjust dose of the antihyperglycaemic during therapy with, or on discontinuation of the other medicine. For Januvia and Janumet - Low risk of clinically meaningful interactions with metformin and ciclosporin. Meaningful interactions would not be expected with other p-glycoprotein inhibitors. The primary enzyme responsible for the limited metabolism of sitagliptin is CYP3A4, with contribution from CYP2C8. Digoxin: sitagliptin had a small effect on plasma digoxin concentrations, and may be a mild inhibitor of p-glycoprotein in vivo. No dosage adjustment of digoxin is recommended, but monitor patients at risk of digoxin toxicity if the two are used together.Pregnancy and lactation: Do not use during pregnancy or breast-feeding. SIDE EFFECTS Refer to SmPC for complete information on side effects There have been no therapeutic clinical trials con-ducted with Janumet tablets however Janumet is bioequivalent to co-administered sitagliptin and metformin. Sitagliptin only: In stud-ies of sitagliptin 100 mg alone compared to placebo, adverse reactions considered as drug-related reported in patients treated with sitagliptin in excess (> 0.2 % and difference > 1 patient) of that in patients receiving placebo are headache, hypoglycaemia, constipa-tion, and dizziness. Also, adverse experiences reported regardless of causal relationship to medication and more commonly in pa-tients treated with sitagliptin included upper respiratory tract infection, nasopharyngitis, osteoarthritis and pain in extremity. Met-formin only: Clinical Trial Data and Post-marketing data: Very common (≥ 1/10): gastro-intestinal disorders; Common (≥ 1/100 to < 1/10): metallic taste; Very rare (< 1/10,000): urticaria, erythema; pruritis; lactic acidosis; vitamin B12 deficiency; liver function disorders, hepatitis. Sitagliptin with metformin: Common: nausea; Uncommon: somnolence; upper abdominal pain, diarrhoea, blood glucose de-creased, anorexia, weight decreased. Sitagliptin with a sulphonylurea: Common: hypoglycaemia. Sitagliptin with metformin and a sulphonylurea: Very common: hypoglycaemia; Common: constipation. Sitagliptin with a PPARγ agent (pioglitazone): Common: hypogly-caemia, flatulence, peripheral oedema. Sitagliptin with a PPARγ agent (rosiglitazone) and metformin: Common: headache, diarrhoea, vomiting, hypoglycaemia, peripheral oedema. Sitagliptin with insulin with/ without metformin: Common: headache, hypoglycaemia, influenza; Uncommon: dry mouth, constipation. Sitagliptin with metformin and insulin: very common: hypoglycaemia; uncommon: headache and dry mouth. Post-marketing experience additional side effects have been reported (frequency not known): hypersensi-tivity reactions, including anaphylaxis, angioedema, rash, urticaria, cutaneous vasculitis and exfoliative skin conditions including Stevens-Johnson syndrome (see precautions); acute pancreatitis, including fatal and non-fatal haemorrhagic and necrotizing pan-creatitis (see precautions); impaired renal function, including acute renal failure (sometimes requiring dialysis); vomiting. PACKAGE QUANTITIES Januvia 100 mg film-coated tablets 28 tablets Janumet 50mg/850mg and 50mg/1000mg film-coated tablets 56 tablets Marketing Authorisation Number Januvia 100 mg: EU/1/07/383/014 Janumet 50 mg/850 mg: EU/1/08/455/003 Janumet 50 mg/1000 mg: EU/1/08/455/010 Marketing Authorisation Holder Merck Sharp & Dohme Limited, Hertford Road, Hoddesdon, Hertfordshire EN11 9BU, UK POM Date of review of prescribing information: June 2011 © Merck Sharp & Dohme Limited,2011. All rights reserved. API.COM-BINED JANUMET/JANUVIA.JUN11.IRLReferences: 1. Goldstein BJ, Feinglos MN, Lunceford JK, et al; for the sitagliptin 036 study group. Effect of initial combination therapywith sitagliptin, a dipeptidyl peptidase-4 inhibitor, and metformin on glycemic control in patients with type 2 diabetes. Diabetes Care.2007;30(8):1979–1987. 2. Janumet SPC available at www.medicines.ie. a A randomized, double-blind, placebo-controlled, parallel-group study evaluating the combination of sitagliptin + metformin ad-
ministered as separate 50/850-mg or 50/1000-mg tablets compared with either agent alone in 1091 patients with type 2 diabetes inadequately controlled on diet and exercise (HbA1c ≥7.5% to ≤11%).1 FPG=fasting plasma glucose; PPG=postprandial glucose.
Further information is available on request from from MSD, Pelham House, South County Business Park, Leopardstown, Dublin 18 or from www.medicines.ie.
Copyright © 2010 Merck Sharp & Dohme Corp., a subsidiary of MSD, Pelham House, South County Business Park, Leopardstown, Dublin 18, Ireland. All rights reserved.
3089_JMT_A4_Ad_July2011.indd 1 14/07/2011 16:16
21
clinical review
Powerful glucose reductions to help get patients to goal1,a
For patients not adequately controlled on metformin alone,
(sitagliptin/metformin)
Glucose reductions at 24 weeks
PPGFPGJANUMET 50/1000 mg twice daily
HbA1c primary end point
–2.1%
–3.9 mmol/L – 6.5 mmol/L(n=180; mean
baseline 10.9 mmol/L; P≤0.001)(n=152; mean
baseline 15.9 mmol/L; P≤0.001)
vs placebo(n=178;
mean baseline 8.8%; P≤0.001)
All-patients-treated population.
Additional HbA1c results at 24 weeks1,a
• 1.3% placebo-adjusted HbA1c reduction with metformin 1000 mg twice daily (n=177; mean baseline 8.7%; P≤0.001)
• 1.6% placebo-adjusted HbA1c reduction with JANUMET™ (sitagliptin/metformin, MSD) 50/500 mg twice daily (n=183; mean baseline 8.8%; P≤0.001)
• 1.0% placebo-adjusted HbA1c reduction with metformin 500 mg twice daily (n=178; mean baseline 8.9%; P≤0.001)
• 0.8% placebo-adjusted HbA1c reduction with sitagliptin 100 mg once daily (n=175; mean baseline 8.9%; P≤0.001)
JANUMET: Powerful efficacy
to help get patients to goal1
As an adjunct to diet and exercise, For patients uncontrolled on metformin alone2
In combination with a glitazone or sulfonylurea2
In combination with insulin2
✔
✔
✔
07-1
2-JM
T-20
11-IR
L-47
07-J
JANUVIA® Sitagliptin JANUMET® Sitagliptin/metformin hydrochlorideABRIDGED PRESCRIBING INFORMATION Refer to Summary of Product Characteristics (SmPC) before prescribing PRESENTATION Januvia® 100 mg film-coated tablet containing 100 mg of sitagliptin. Janumet® 50 mg/850 mg and 50 mg/1000 mg tablets each contain-ing 50 mg sitagliptin and 850 mg or 1000 mg metformin hydrochloride. USES For patients with type 2 diabetes mellitus Januvia is indi-cated to improve glycaemic control: as monotherapy • in patients inadequately controlled by diet and exercise alone and for whom metformin is inappropriate due to contraindications or intolerance as dual oral therapy in combination with • metformin when diet and exercise plus metformin alone do not provide adequate glycaemic control • a sulphonylurea when diet and exercise plus maximal tolerated dose of a sulphonylurea alone do not provide adequate glycaemic control and when metformin is inappropriate due to con-tra-indications or intolerance • a PPARγ agonist (i.e. a thiazolidinedione) when use of a PPARγ agonist is appropriate and when diet and exercise plus the PPARγ agonist alone do not provide adequate glycaemic control as triple oral therapy in combination with • a sulphonylurea and metformin when diet and exercise plus dual therapy with these agents do not provide adequate glycaemic control. • a PPARγ agonist and metformin when use of a PPARγ agonist is appropriate and when diet and exercise plus dual therapy with these agents do not provide adequate glycaemic control. Januvia is also indicated as add-on to insulin (with or without metformin) when diet and exercise plus stable dosage of insulin do not provide adequate glycaemic control. Janumet: as an adjunct to diet and exercise to improve glycaemic control in patients inadequately controlled on their maximal tolerated dose of metformin alone or those already being treated with the combination of sitagliptin and metformin. • in combination with a sulphonylurea (i.e., triple combination therapy) as an adjunct to diet and exercise in patients inadequately controlled on their maximal tolerated dose of metformin and a sulphonylu-rea. • as triple combination therapy with a PPARγ agonist (i.e., a thiazolidinedione) as an adjunct to diet and exercise in patients inad-equately controlled on their maximal tolerated dose of metformin and a PPARγ agonist. • as add-on to insulin (i.e., triple combination therapy) as an adjunct to diet and exercise to improve glycaemic control in patients when stable dosage of insulin and metformin alone do not provide adequate glycaemic control. DOSAGE AND ADMINISTRATION Januvia - One 100 mg tablet once daily, with or without food. Janumet - The dose of antihyperglycaemic therapy with Janumet should be individualised on the basis of the patient’s current regimen, effectiveness, and tolerability while not exceeding the maximum recommended daily dose of 100 mg sitagliptin. For patients not adequately controlled on metformin alone, the usual starting dose of Janumet should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) plus the dose of metformin already being taken. For patients switching from co-administration of sitag-liptin and metformin, Janumet should be initiated at the dose of sitagliptin and metformin already being taken. For patients inadequate-ly controlled on dual combination therapy with the maximal tolerated dose of metformin and a sulphonylurea or with maximal tolerated dose of metformin and a PPARγ agonist or with maximal tolerated dose of metformin and insulin, the dose of Janumet should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) and a dose of metformin similar to the dose already being taken. All patients should continue their diet with an adequate distribution of carbohydrate intake during the day. Overweight patients should continue their energy-restricted diet. Januvia and Janumet - In combination with a sulphonylurea or with insulin, consider a lower dose of sulphonylurea or insulin, to reduce risk of hypoglycaemia. Renal impairment: See Precautions. Hepatic impairment: For Janu-via only - no dosage adjustment necessary for patients with mild to moderate hepatic impairment. Januvia has not been studied in patients with severe hepatic impairment. For Janumet only – do not use. Elderly < 75 years: For Januvia only - no dosage adjustment necessary. For Janumet only - use with caution as age increases. Monitoring of renal function is necessary to aid prevention of met-formin-associated lactic acidosis. Elderly ≥ 75 years: Exercise care as there are limited safety data in this population. Children: not recommended below 18 years of age. CONTRA-INDICATIONS For Januvia - Hypersensitivity to active substance or excipients. For Janumet - Hypersensitivity. Diabetic ketoacidosis and diabetic pre-coma. Moderate and severe renal impairment (creatinine clear-ance < 60 ml/min). Acute conditions with the potential to alter renal function such as dehydration, severe infection, shock. Intravascu-lar administration of iodinated contrast agents. Acute or chronic disease which may cause tissue hypoxia such as cardiac or respira-tory failure, recent myocardial infarction, shock. Hepatic impairment. Acute alcohol intoxication, alcoholism. Lactation. PRECAUTIONS For Januvia and Janumet - General: do not use in patients with type 1 diabetes or for diabetic ketoacidosis. Pancreatitis: Post-market-ing experience - spontaneously reported adverse reactions of acute pancreatitis. Inform patients of the symptom of acute pancreati-tis: persistent, severe abdominal pain. Resolution of pancreatitis has been observed after discontinuation of sitagliptin, but very rare cases of necrotizing or haemorrhagic pancreatitis and/or death have been reported. If pancreatitis is suspected, Januvia or Janumet and other potentially suspect medicinal products should be discontinued. Hypoglycaemia when used with other anti-hyperglycaemic agents: Rates of hypoglycaemia reported with sitagliptin were generally similar to rates in patients taking placebo. When sitagliptin was added to a sulphonylurea or to insulin, the incidence of hypoglycaemia was increased over that of placebo; therefore consider a lower dose of sulphonylurea or insulin to reduce the risk of hypoglycaemia when administering Janumet or Januvia. Hypersensitivity reactions: Serious hypersensitivity reactions have been reported, including anaphylaxis, angioedema, and exfoliative skin conditions including Stevens-Johnson syndrome. Onset occurred within the first 3 months after initiation of treatment with some reports occur-ring after the first dose. If suspected, discontinue Januvia or Janumet. For Januvia only - As experience is limited, patients with moderate or severe renal impairment should not be treated with Januvia. For Janumet only - Lactic acidosis and renal function: a very rare, but serious, metabolic complication can occur due to metformin accumulation. Cases in patients on metformin have occurred primarily in diabetic patients with significant renal failure. Reduce incidence by assessing other associated risk factors. If suspected, discontinue treatment and hospitalise patient immediately. If changes in clinical status of patients with previously controlled type 2 diabetes occurs, evaluate promptly for evidence of ketoacidosis or lactic acidosis in any patient with type 2 diabetes previously well
controlled on Janumet who develops laboratory abnormalities or clinical illness (especially vague and poorly defined illness). If aci-dosis of either form occurs, stop Janumet immediately and initiate corrective measures.Determine serum creatinine concentrations regularly, i.e. at least once a year in patients with normal renal function and at least two to four times a year in patients with serum creatinine levels at or above the upper limit of normal and in elderly patients. Decreased renal function in elderly patients is frequent and asymptomatic. Exercise special caution where renal function may become impaired, e.g. when initiating antihypertensive or diu-retic therapy or when starting treatment with a non-steroidal anti-inflammatory drug (NSAID). Surgery: due to metformin hydrochlo-ride content of Janumet, discontinue treatment 48 hours before elective surgery with general, spinal or epidural anaesthesia. Do not resume earlier than 48 hours afterwards and only after renal function is normal. DRUG INTERACTIONS For Janumet only - Alcohol: avoid alcohol and medicinal products containing alcohol due to risk of lactic acidosis. Cationic agents that are eliminated by renal tubular secretion (e.g., cimetidine): these may interact with metformin by competing for common renal tubular transport systems. Consider close monitoring of glycaemic control, dose adjustment within the recommended posology and changes in diabetic treat-ment when these agents are co-administered. Iodinated contrast agents in radiological studies: intravascular administration of these agents may lead to renal failure, resulting in metformin accumulation and a risk of lactic acidosis. Discontinue Janumet prior to, or at the time of the test and do not reinstitute until 48 hours afterwards, and only after renal function is found to be normal. Combination requiring precautions for use: glucocorticoids (given by systemic and local routes) beta-2-agonists, and diuretics have intrinsic hyper-glycaemic activity. Inform the patient and perform more frequent blood glucose monitoring, especially at the beginning of treatment. If necessary, adjust dose of the anti-hyperglycaemic medicine during therapy with, or on discontinuation of the other medicine. ACE-inhibitors: as these may decrease the blood glucose levels, if necessary, adjust dose of the antihyperglycaemic during therapy with, or on discontinuation of the other medicine. For Januvia and Janumet - Low risk of clinically meaningful interactions with metformin and ciclosporin. Meaningful interactions would not be expected with other p-glycoprotein inhibitors. The primary enzyme responsible for the limited metabolism of sitagliptin is CYP3A4, with contribution from CYP2C8. Digoxin: sitagliptin had a small effect on plasma digoxin concentrations, and may be a mild inhibitor of p-glycoprotein in vivo. No dosage adjustment of digoxin is recommended, but monitor patients at risk of digoxin toxicity if the two are used together.Pregnancy and lactation: Do not use during pregnancy or breast-feeding. SIDE EFFECTS Refer to SmPC for complete information on side effects There have been no therapeutic clinical trials con-ducted with Janumet tablets however Janumet is bioequivalent to co-administered sitagliptin and metformin. Sitagliptin only: In stud-ies of sitagliptin 100 mg alone compared to placebo, adverse reactions considered as drug-related reported in patients treated with sitagliptin in excess (> 0.2 % and difference > 1 patient) of that in patients receiving placebo are headache, hypoglycaemia, constipa-tion, and dizziness. Also, adverse experiences reported regardless of causal relationship to medication and more commonly in pa-tients treated with sitagliptin included upper respiratory tract infection, nasopharyngitis, osteoarthritis and pain in extremity. Met-formin only: Clinical Trial Data and Post-marketing data: Very common (≥ 1/10): gastro-intestinal disorders; Common (≥ 1/100 to < 1/10): metallic taste; Very rare (< 1/10,000): urticaria, erythema; pruritis; lactic acidosis; vitamin B12 deficiency; liver function disorders, hepatitis. Sitagliptin with metformin: Common: nausea; Uncommon: somnolence; upper abdominal pain, diarrhoea, blood glucose de-creased, anorexia, weight decreased. Sitagliptin with a sulphonylurea: Common: hypoglycaemia. Sitagliptin with metformin and a sulphonylurea: Very common: hypoglycaemia; Common: constipation. Sitagliptin with a PPARγ agent (pioglitazone): Common: hypogly-caemia, flatulence, peripheral oedema. Sitagliptin with a PPARγ agent (rosiglitazone) and metformin: Common: headache, diarrhoea, vomiting, hypoglycaemia, peripheral oedema. Sitagliptin with insulin with/ without metformin: Common: headache, hypoglycaemia, influenza; Uncommon: dry mouth, constipation. Sitagliptin with metformin and insulin: very common: hypoglycaemia; uncommon: headache and dry mouth. Post-marketing experience additional side effects have been reported (frequency not known): hypersensi-tivity reactions, including anaphylaxis, angioedema, rash, urticaria, cutaneous vasculitis and exfoliative skin conditions including Stevens-Johnson syndrome (see precautions); acute pancreatitis, including fatal and non-fatal haemorrhagic and necrotizing pan-creatitis (see precautions); impaired renal function, including acute renal failure (sometimes requiring dialysis); vomiting. PACKAGE QUANTITIES Januvia 100 mg film-coated tablets 28 tablets Janumet 50mg/850mg and 50mg/1000mg film-coated tablets 56 tablets Marketing Authorisation Number Januvia 100 mg: EU/1/07/383/014 Janumet 50 mg/850 mg: EU/1/08/455/003 Janumet 50 mg/1000 mg: EU/1/08/455/010 Marketing Authorisation Holder Merck Sharp & Dohme Limited, Hertford Road, Hoddesdon, Hertfordshire EN11 9BU, UK POM Date of review of prescribing information: June 2011 © Merck Sharp & Dohme Limited,2011. All rights reserved. API.COM-BINED JANUMET/JANUVIA.JUN11.IRLReferences: 1. Goldstein BJ, Feinglos MN, Lunceford JK, et al; for the sitagliptin 036 study group. Effect of initial combination therapywith sitagliptin, a dipeptidyl peptidase-4 inhibitor, and metformin on glycemic control in patients with type 2 diabetes. Diabetes Care.2007;30(8):1979–1987. 2. Janumet SPC available at www.medicines.ie. a A randomized, double-blind, placebo-controlled, parallel-group study evaluating the combination of sitagliptin + metformin ad-
ministered as separate 50/850-mg or 50/1000-mg tablets compared with either agent alone in 1091 patients with type 2 diabetes inadequately controlled on diet and exercise (HbA1c ≥7.5% to ≤11%).1 FPG=fasting plasma glucose; PPG=postprandial glucose.
Further information is available on request from from MSD, Pelham House, South County Business Park, Leopardstown, Dublin 18 or from www.medicines.ie.
Copyright © 2010 Merck Sharp & Dohme Corp., a subsidiary of MSD, Pelham House, South County Business Park, Leopardstown, Dublin 18, Ireland. All rights reserved.
3089_JMT_A4_Ad_July2011.indd 1 14/07/2011 16:16
Diabetes is the fifth leading cause of death in the world and is increasingly being described as an epidemic.1 The Institute of Public Health (IPH), estimated that just over 140,000 people had diabetes in 2007 (4.5% of the population; type 1
and type 2 combined). This figure is expected to rise to over 190,000 adults (5.2% of the population) by 2015. The rising problem of obesity, a more sedentary lifestyle and an ageing population are just some of the reasons for the projected increase internationally and nationally in the number of people with diabetes.2,3,4 Having established that diabetes is a serious illness what can the Irish health service and more particularly what can we in general practice do about it?
National diabetes clinical care diabetes ProgrammeIn 1989 Ireland signed up to the WHO’s St Vincent Declaration: we agreed to deploy resources for the prevention, identification and treatment of diabetes and particularly its complications: blindness, renal failure, amputation, coronary artery disease and stroke. The Irish St Vincent Task Force reported an uneven distribution of resources – individuals working in isolation with pockets of excellent care. They recommended that we adopt a planned, integrated, and structured approach to diabetes care and that the health service provide the resources to deliver
on our commitment made in 1989. Now over 20 years later we have a National Diabetes Clinical Care Diabetes Programme which has set as its aim to: ‘save the lives, eyes and limbs of patients with diabetes’. The objective of the programme is that everyone with diabetes should access a structured programme which covers all aspects of their diabetic care. The projected result of investing in integrated care, will be a reduction in overall bed days by 40,000 per year; reduction in mortality by 10% and reduction in morbidity (Reduce; blindness by 40%, amputations by 40%, cardiovascular events by 20%). The National Diabetes Programme prioritised the National Retinopathy Screening Programme and Foot Care in 2011. The next priority is progressing integrated care – with the majority of the care of type 2 diabetes being delivered in primary care i.e. the appropriate care in the appropriate setting.
Integrated careIntegrated care is a model of care which makes best use of available resources, fully utilising the clinical skills of GPs and Practice Nurses, with patient care pathways agreed between primary and secondary care. Integrated care ensures that patients have access to the care they need when they need it. By supporting structured diabetes care in the primary care setting, secondary care will have the capacity to review
diabetes care in general practiceIntegrated care is a model of care which makes best use of available resources, fully utilising the clinical skills of practice nurses
kATIe MurPhy, DIGP DIABETES NURSE FACIlITATOR, DEPT OF GENERAl PRACTICE, lANCASTER HAll, UCC

IEBDR00036 ©2011 AMYLIN PHARMACEUTICALS, INC. AND LILLY, LLC. September 2011ALL RIGHTS RESERVED.BYDUREON is a registered trade mark and BYDUREON By Your Side is a trade mark of Amylin Pharmaceuticals, Inc. Further information is available in the SPC
BYDUREON® (EXENATIDE) REPUBLIC OF IRELAND ABBREVIATED PRESCRIBING INFORMATIONPresentation: Exenatide 2mg powder and solvent for prolonged-release suspension for injection. Each single-dose kit contains one vial of 2mg exenatide and one pre-filled syringe of 0.65ml solvent. Uses: Bydureon is indicated for treatment of Type 2 diabetes mellitus in combination with metformin, sulphonylureas, thiazolidinediones, or combinations of metformin and a sulphonylurea or metformin and a thiazolidinedione, in adults who have not achieved adequate glycaemic control on maximally tolerated doses of these oral therapies. Dosage and Administration: The recommended dose is 2mg once weekly, on the same day each week. Each dose should be administered in the abdomen, thigh, or the back of the upper arm as a subcutaneous injection immediately after suspension of the powder in the solvent. Instructions on the suspension and administration of Bydureon can be found in the ‘Instructions for the User’ provided in the carton and must be followed carefully by the patient. Appropriate training is recommended for non-healthcare professionals administering the product. Patients switching from exenatide twice daily (Byetta) to Bydureon may experience transient elevations in blood glucose concentrations, which generally improve within the first two weeks after initiation of therapy. When Bydureon is added to existing metformin and/or thiazolidinedione therapy, the current dose of metformin and/or thiazolidinedione can be continued. When Bydureon is added to sulphonylurea therapy, a reduction in the dose of sulphonylurea should be considered to reduce the risk of hypoglycaemia. Blood glucose self-monitoring may be necessary to adjust the dose of sulphonylurea. If a different antidiabetic treatment is started after the discontinuation of Bydureon, consideration should be given to the prolonged release of Bydureon. Elderly: No dose adjustment is required based on age. Consideration should be given to the patient’s renal function. Renal or hepatic impairment: No dosage adjustment is necessary in patients with mild renal impairment (creatinine clearance 50-80ml/min) or hepatic impairment. Not recommended in patients with moderate renal impairment (creatinine clearance 30-50ml/min), severe renal impairment (creatinine clearance <30ml/min), or end-stage renal disease. Paediatric population: The safety and efficacy in children and adolescents aged under 18 years have not yet been established. No data are available. Contra-indications: Hypersensitivity to the active substance or to any of the excipients. Warnings and Special Precautions: Should not be used in
patients with Type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis. Must not be administered by intravenous or intramuscular injection. Not recommended for use in patients with moderate or severe renal impairment or end-stage renal disease. There have been rare, spontaneously reported events of altered renal function with exenatide, including increased serum creatinine, renal impairment, worsened chronic renal failure, and acute renal failure, sometimes requiring haemodialysis. Some of these occurred in patients experiencing events that may affect hydration and/or receiving medicinal products known to affect renal function/hydration status, including angiotensin converting enzymes inhibitors, angiotensin-II antagonists, non-steroidal anti-inflammatory medicinal products, and diuretics. Not recommended in patients with severe gastro-intestinal disease. There have been rare, spontaneously reported events of acute pancreatitis. Patients should be informed of the characteristic symptom of acute pancreatitis: persistent, severe abdominal pain. Resolution of pancreatitis has been observed with supportive treatment, but very rare cases of necrotizing or haemorrhagic pancreatitis and/or death have been reported. If pancreatitis is suspected, Bydureon and other potentially suspect medicinal products should be discontinued. Treatment with Bydureon should not be resumed after pancreatitis has been diagnosed. The concurrent use of Bydureon with insulin, D-phenylalanine derivatives (meglitinides), alpha-glucosidase inhibitors, dipeptidyl peptidase-4 inhibitors, or other GLP-1 receptor agonists has not been studied. The concurrent use of Bydureon and exenatide twice daily (Byetta) has not been studied and is not recommended. The risk of hypoglycaemia was increased when Bydureon was used in combination with a sulphonylurea in clinical trials. Furthermore, patients on a sulphonylurea combination, with mild renal impairment, had an increased incidence of hypoglycaemia compared to patients with normal renal function. To reduce the risk of hypoglycaemia associated with the use of a sulphonylurea, reduction in the dose of sulphonylurea should be considered. Rapid weight loss (>1.5 kg per week) has been reported in patients treated with exenatide. Weight loss of this rate may have harmful consequences. There have been some reported cases of increased INR, sometimes associated with bleeding, with concomitant use of warfarin and exenatide. After discontinuation, the effect of Bydureon may continue as plasma levels of exenatide decline over 10 weeks. Choice of other medicinal products and dose selection should be considered accordingly until exenatide levels decline. Interactions: The following interaction studies
were conducted using 10 micrograms exenatide twice daily, but not exenatide once weekly: HMG CoA reductase inhibitors: Lovastatin AUC and Cmax were decreased and Tmax was delayed when exenatide (10μg BD) was administered concomitantly with a single dose of lovastatin (40mg). Concomitant use of exenatide twice daily and HMG CoA reductase inhibitors was not associated with consistent changes in lipid profiles. Lipid profiles should be monitored as appropriate. Warfarin: Tmax was delayed when warfarin was administered 35 min after exenatide twice daily. No clinically relevant effects on Cmax or AUC were observed. Increased INR has been reported during concomitant use of warfarin and exenatide twice daily. INR should be monitored during initiation of Bydureon therapy in patients on warfarin and/or cumarol derivatives. Digoxin and lisinopril: A delay in Tmax was observed in interaction studies between digoxin or lisinopril and exenatide twice daily. No clinically relevant effects on Cmax or AUC were observed. Fertility, Pregnancy, and Lactation: Women of childbearing potential should use contraception during treatment with Bydureon. Bydureon should be discontinued at least 3 months before a planned pregnancy. Bydureon should not be used during pregnancy and the use of insulin is recommended. Bydureon should not be used during breast-feeding. Driving, etc: No studies on the effects on the ability to drive and use machines have been performed. When Bydureon is used in combination with a sulphonylurea, avoid hypoglycaemia while driving and using machines. Undesirable Effects: Adverse Reactions Reported From Clinical Studies.Very common: Hypoglycaemia (with a sulphonylurea), constipation, diarrhoea, nausea, vomiting, injection site pruritus, injection site nodules. Common: Decreased appetite, dizziness, headache, abdominal distention, abdominal pain, dyspepsia, eructation, flatulence, gastro-oesophageal reflux, fatigue, injection site erythema, injection site rash, somnolence. Rapid weight loss has been reported with Bydureon. Patients may develop anti-exenatide antibodies following treatment with Bydureon. These patients tend to have more injection site reactions (eg, skin redness, itching). Acute pancreatitis and acute renal failure have been reported rarely and anaphylactic reaction has been reported very rarely in spontaneous post-marketing reports with exenatide twice daily. For full details of these and other side-effects, please see the Summary of Product Characteristics, which is available at http://www.medicines.ie/. Legal Category: POM. Marketing Authorisation Number and Holder: EU/1/11/696/001. Eli Lilly Nederland BV, Grootslag 1-5, NL-3991 RA Houten, The Netherlands. Date of Preparation or Last Review June 2011. Full Prescribing Information is Available From: Eli Lilly and Company Limited, Lilly House, Priestley Road, Basingstoke, Hampshire, RG24 9NL. Telephone: Basingstoke (01256) 315 000. E-mail: [email protected] or Eli Lilly and Company (Ireland) Limited, Hyde House, 65 Adelaide Road, Dublin 2, Republic of Ireland, Telephone: Dublin (01) 661 4377. E-mail: [email protected]. BYDUREON® (exenatide) is a registered trademark of Amylin Pharmaceuticals, Inc. References: 1. BYDUREON summary of product characteristics. 2. Duration 6 press release. Available at: https://investor.lilly.com/releasedetail2.cfm?ReleaseID=554248 3. Taylor et al. BMC Endocrine Disorders 2011, 11:9, http://www.biomedcentral. com/1472-6823/11/9
•Mean HbA1C reduction between 1.3% and 1.9%1,2
•Sustained HbA1C reduction of 1.5% at 2years3
•Sustained weight loss of 2.4kg at 2years3*
NEW
Mon
day
Tuesda
y
Wed
nesday
Thursday
Friday
Saturday
Sund
ay
BYDUREON the first and only therapy to provide continuous glycaemic control with aonce weekly injection1
BYDUREON is indicated for treatment of type 2 diabetes mellitus in combination with metformin, sulphonylurea, thiazolidinedione, or combinations of metformin and sulphonylurea or metformin and thiazolidinedione, in adults who have not achieved
adequate glycaemic control on maximally tolerated doses of these oral therapies
*Rapid weight loss at a rate of > 1.5kg per week has been reported in patients treated with exenatide. Weight loss of this rate may have harmful consequences.1
*BYDUREON is not indicated for the management of obesity, and weight change was a secondary endpoint in clinical trials.
IE_BYD_Journal_Ad_FP.indd 1 05/10/2011 15:36
23
clinical review
IEBDR00036 ©2011 AMYLIN PHARMACEUTICALS, INC. AND LILLY, LLC. September 2011ALL RIGHTS RESERVED.BYDUREON is a registered trade mark and BYDUREON By Your Side is a trade mark of Amylin Pharmaceuticals, Inc. Further information is available in the SPC
BYDUREON® (EXENATIDE) REPUBLIC OF IRELAND ABBREVIATED PRESCRIBING INFORMATIONPresentation: Exenatide 2mg powder and solvent for prolonged-release suspension for injection. Each single-dose kit contains one vial of 2mg exenatide and one pre-filled syringe of 0.65ml solvent. Uses: Bydureon is indicated for treatment of Type 2 diabetes mellitus in combination with metformin, sulphonylureas, thiazolidinediones, or combinations of metformin and a sulphonylurea or metformin and a thiazolidinedione, in adults who have not achieved adequate glycaemic control on maximally tolerated doses of these oral therapies. Dosage and Administration: The recommended dose is 2mg once weekly, on the same day each week. Each dose should be administered in the abdomen, thigh, or the back of the upper arm as a subcutaneous injection immediately after suspension of the powder in the solvent. Instructions on the suspension and administration of Bydureon can be found in the ‘Instructions for the User’ provided in the carton and must be followed carefully by the patient. Appropriate training is recommended for non-healthcare professionals administering the product. Patients switching from exenatide twice daily (Byetta) to Bydureon may experience transient elevations in blood glucose concentrations, which generally improve within the first two weeks after initiation of therapy. When Bydureon is added to existing metformin and/or thiazolidinedione therapy, the current dose of metformin and/or thiazolidinedione can be continued. When Bydureon is added to sulphonylurea therapy, a reduction in the dose of sulphonylurea should be considered to reduce the risk of hypoglycaemia. Blood glucose self-monitoring may be necessary to adjust the dose of sulphonylurea. If a different antidiabetic treatment is started after the discontinuation of Bydureon, consideration should be given to the prolonged release of Bydureon. Elderly: No dose adjustment is required based on age. Consideration should be given to the patient’s renal function. Renal or hepatic impairment: No dosage adjustment is necessary in patients with mild renal impairment (creatinine clearance 50-80ml/min) or hepatic impairment. Not recommended in patients with moderate renal impairment (creatinine clearance 30-50ml/min), severe renal impairment (creatinine clearance <30ml/min), or end-stage renal disease. Paediatric population: The safety and efficacy in children and adolescents aged under 18 years have not yet been established. No data are available. Contra-indications: Hypersensitivity to the active substance or to any of the excipients. Warnings and Special Precautions: Should not be used in
patients with Type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis. Must not be administered by intravenous or intramuscular injection. Not recommended for use in patients with moderate or severe renal impairment or end-stage renal disease. There have been rare, spontaneously reported events of altered renal function with exenatide, including increased serum creatinine, renal impairment, worsened chronic renal failure, and acute renal failure, sometimes requiring haemodialysis. Some of these occurred in patients experiencing events that may affect hydration and/or receiving medicinal products known to affect renal function/hydration status, including angiotensin converting enzymes inhibitors, angiotensin-II antagonists, non-steroidal anti-inflammatory medicinal products, and diuretics. Not recommended in patients with severe gastro-intestinal disease. There have been rare, spontaneously reported events of acute pancreatitis. Patients should be informed of the characteristic symptom of acute pancreatitis: persistent, severe abdominal pain. Resolution of pancreatitis has been observed with supportive treatment, but very rare cases of necrotizing or haemorrhagic pancreatitis and/or death have been reported. If pancreatitis is suspected, Bydureon and other potentially suspect medicinal products should be discontinued. Treatment with Bydureon should not be resumed after pancreatitis has been diagnosed. The concurrent use of Bydureon with insulin, D-phenylalanine derivatives (meglitinides), alpha-glucosidase inhibitors, dipeptidyl peptidase-4 inhibitors, or other GLP-1 receptor agonists has not been studied. The concurrent use of Bydureon and exenatide twice daily (Byetta) has not been studied and is not recommended. The risk of hypoglycaemia was increased when Bydureon was used in combination with a sulphonylurea in clinical trials. Furthermore, patients on a sulphonylurea combination, with mild renal impairment, had an increased incidence of hypoglycaemia compared to patients with normal renal function. To reduce the risk of hypoglycaemia associated with the use of a sulphonylurea, reduction in the dose of sulphonylurea should be considered. Rapid weight loss (>1.5 kg per week) has been reported in patients treated with exenatide. Weight loss of this rate may have harmful consequences. There have been some reported cases of increased INR, sometimes associated with bleeding, with concomitant use of warfarin and exenatide. After discontinuation, the effect of Bydureon may continue as plasma levels of exenatide decline over 10 weeks. Choice of other medicinal products and dose selection should be considered accordingly until exenatide levels decline. Interactions: The following interaction studies
were conducted using 10 micrograms exenatide twice daily, but not exenatide once weekly: HMG CoA reductase inhibitors: Lovastatin AUC and Cmax were decreased and Tmax was delayed when exenatide (10μg BD) was administered concomitantly with a single dose of lovastatin (40mg). Concomitant use of exenatide twice daily and HMG CoA reductase inhibitors was not associated with consistent changes in lipid profiles. Lipid profiles should be monitored as appropriate. Warfarin: Tmax was delayed when warfarin was administered 35 min after exenatide twice daily. No clinically relevant effects on Cmax or AUC were observed. Increased INR has been reported during concomitant use of warfarin and exenatide twice daily. INR should be monitored during initiation of Bydureon therapy in patients on warfarin and/or cumarol derivatives. Digoxin and lisinopril: A delay in Tmax was observed in interaction studies between digoxin or lisinopril and exenatide twice daily. No clinically relevant effects on Cmax or AUC were observed. Fertility, Pregnancy, and Lactation: Women of childbearing potential should use contraception during treatment with Bydureon. Bydureon should be discontinued at least 3 months before a planned pregnancy. Bydureon should not be used during pregnancy and the use of insulin is recommended. Bydureon should not be used during breast-feeding. Driving, etc: No studies on the effects on the ability to drive and use machines have been performed. When Bydureon is used in combination with a sulphonylurea, avoid hypoglycaemia while driving and using machines. Undesirable Effects: Adverse Reactions Reported From Clinical Studies.Very common: Hypoglycaemia (with a sulphonylurea), constipation, diarrhoea, nausea, vomiting, injection site pruritus, injection site nodules. Common: Decreased appetite, dizziness, headache, abdominal distention, abdominal pain, dyspepsia, eructation, flatulence, gastro-oesophageal reflux, fatigue, injection site erythema, injection site rash, somnolence. Rapid weight loss has been reported with Bydureon. Patients may develop anti-exenatide antibodies following treatment with Bydureon. These patients tend to have more injection site reactions (eg, skin redness, itching). Acute pancreatitis and acute renal failure have been reported rarely and anaphylactic reaction has been reported very rarely in spontaneous post-marketing reports with exenatide twice daily. For full details of these and other side-effects, please see the Summary of Product Characteristics, which is available at http://www.medicines.ie/. Legal Category: POM. Marketing Authorisation Number and Holder: EU/1/11/696/001. Eli Lilly Nederland BV, Grootslag 1-5, NL-3991 RA Houten, The Netherlands. Date of Preparation or Last Review June 2011. Full Prescribing Information is Available From: Eli Lilly and Company Limited, Lilly House, Priestley Road, Basingstoke, Hampshire, RG24 9NL. Telephone: Basingstoke (01256) 315 000. E-mail: [email protected] or Eli Lilly and Company (Ireland) Limited, Hyde House, 65 Adelaide Road, Dublin 2, Republic of Ireland, Telephone: Dublin (01) 661 4377. E-mail: [email protected]. BYDUREON® (exenatide) is a registered trademark of Amylin Pharmaceuticals, Inc. References: 1. BYDUREON summary of product characteristics. 2. Duration 6 press release. Available at: https://investor.lilly.com/releasedetail2.cfm?ReleaseID=554248 3. Taylor et al. BMC Endocrine Disorders 2011, 11:9, http://www.biomedcentral. com/1472-6823/11/9
•Mean HbA1C reduction between 1.3% and 1.9%1,2
•Sustained HbA1C reduction of 1.5% at 2years3
•Sustained weight loss of 2.4kg at 2years3*
NEW
Mon
day
Tuesda
y
Wed
nesday
Thursday
Friday
Saturday
Sund
ay
BYDUREON the first and only therapy to provide continuous glycaemic control with aonce weekly injection1
BYDUREON is indicated for treatment of type 2 diabetes mellitus in combination with metformin, sulphonylurea, thiazolidinedione, or combinations of metformin and sulphonylurea or metformin and thiazolidinedione, in adults who have not achieved
adequate glycaemic control on maximally tolerated doses of these oral therapies
*Rapid weight loss at a rate of > 1.5kg per week has been reported in patients treated with exenatide. Weight loss of this rate may have harmful consequences.1
*BYDUREON is not indicated for the management of obesity, and weight change was a secondary endpoint in clinical trials.
IE_BYD_Journal_Ad_FP.indd 1 05/10/2011 15:36
patients requiring specialist intervention quickly. Adopting a structured approach to care delivery involves creating practice registers, adherence to evidence based guidelines, allocation of protected time, regular patient follow-up, ongoing audit and feedback, and continuing professional education.2,5
Routine integrated care involves the patient, GP, practice nurse, endocrinlogist, clinical nurse specialist in diabetes, dietitian, ophthalmologist and podiatrist. All patients with type 2 diabetes should have access to specialist services such as retinopathy screening, endocrinology, vascular, cardiology, nephrology and psychology as needed. An annual and comprehensive review is regarded as the crucial element of integrated diabetes care.
Research proves that interventions at key stages can make a difference (see Table 1).
Table 1
The Impact of Intervention at key stages in diabetes (Source: Audit Commission UK 2000)Prevention Up to half of all new cases could, in theory, be prevented by reducing rates of obesity
early diagnosis Up to half of all people with diabetes already have serious complications when diagnosed.
People with diabetes• Structured programmes of care increase the level of self-
management.• Surveillance and early intervention prevents/reduces
complications.• Good blood glucose control can reduce kidney damage
by one-third.• Good blood pressure control can reduce strokes by one-
third.• Eye screening and treatment can reduce blindness by half.• Footcare can reduce foot complications by two-thirds.
diabetes – active case findingIt is estimated that the average time from the onset of type 2 diabetes to diagnosis is 7 years as patients are initially asymptomatic, therefore patients often have complications of diabetes on diagnosis.2 This will continue if we in general practice do not screen our practice population to detect diabetes early and prevent the onset of complications. If primary care are not actively case finding patients with diabetes, as per targeted screening guidelines2 patients will continue to be diagnosed when they present with a complication e.g. MI. Diagnosis is made as per 2008 Guidelines.2
who to screen• Family Hx. 1st degree rel. type 2 diabetes• Hx. gestational diabetes• Baby >4.1kg/9lbs or Hx gestational diabetes• Obese patients – BMI >25/inactive lifestyle• Symptoms polydipsia/polyuria • Recurrent candidiasis, skin or urine infections• Hypertensive, hypercholesterolaemia • Established arterial disease – IHD, CVA, PVD• >45 year olds• Polycystic ovarian disease, patients on long term steroids• Ethnicity – Asian, African, African/American• ? when taking bloods offer to do random blood sugar
creating a diabetes registerUnless you know who your patients with diabetes are you cannot recall them for review appointments. Create registers of patients with diabetes: type 1, type 2. Many GP software systems facilitate drug searches of diabetes medications and glucose test strips. www.hse.ie has notes on creating diabetes registers for several software systems, or ask your software provider to assist you. Practices who are not computerised can create a manual register of patients with diabetes – Cardex file or ledger. Once you have created the register, each member of the practice team has a responsibility to maintain it by entering all newly diagnosed patients.
Pre-diabetesWhen screening for diabetes you will also diagnose patients with impaired fasting glucose and impaired glucose tolerance. These patients have the same cardiovascular risk as those with diabetes, so should be followed up to reduce cardiovascular risk factors (diet, exercise, smoking, BP, lipids). 5% per year will progress to type 2 diabetes: this can be reduced by 60% with lifestyle modification.2 They should attend for an annual glucose tolerance test to ensure that they have not progressed to a diagnosis of diabetes. Creating a register of patients with pre-diabetes will facilitate recall for annual review.
Adherence to evidence based guidelinesA Practical Guide to Integrated Type 2 Diabetes Care (Harkins, 2008) has the current guidelines for management of type 2 diabetes and can be downloaded from www.hse.ie
These guidelines are very user friendly and should be available for reference in every practice. The HSE West Diabetes Manual is also very helpful. I suggest laminating page 1 – type 2 diabetes at a glance – is a useful desk top quick reference tool. In DiGP we have Harkins 2008 Protocol for the Management of Microalbuminuria ( pg 37) on the back of this.
evidence for target bP and hbA1cThe UK Prospective Diabetes Study (UKPDS, 1998)6, a landmark study in type 2 diabetes, demonstrated that lower HbA1c (aim <7%= 53) is associated with less complications, also any reduction was advantageous. This validates the efforts of patients who struggle to make small reductions in HbA1c. Also good BP control (target <140/85) was as important as glycaemic control with 24% reduction in all complications of diabetes and 44% reduction in stroke. A 10 year follow-up of UKPDS study group (2008) still showed reduced cardiovascular risk of 25% for every 1% reduction in HbA1c. Both the original intervention group and control group show increased HbA1c which demonstrates that type 2 diabetes is a progressive disease. Investigators have concluded that early control of hyperglycaemia provides future cardiovascular protection. This further reinforces the role for primary care in early diagnosis and good glycaemic control. Unlike early glycaemic control, benefit from BP control is not maintained over time, therefore good blood pressure control must be continued if benefits are to be sustained. The findings of the ACCORD study showed a previously unrecognised risk of intensive glucose lowering (target HbAic 6%= 42) of high risk patients with established type 2 diabetes. In light of these findings the UK and USA recommend target is HbA1c of 6.5-7%. At recent conferences there has been discussion of less stringent targets in the elderly.
Targets to prevent complications:• BP <130/80 (>65 yr old <140/80)• HbA1c < 42 (6.5%)

Mean reductions in HbA1c: up to 1.50% (16 mmol/mol)1
Mean reductions in weight: up to 3.7 kg1
Improvements in SBP* from baseline1
Improvements in beta-cell function1
*SBP = Systolic Blood Pressure
...to help your patients with type 2 diabetes achieve:1
Abbreviated Prescribing InformationVictoza® 6 mg/ml solution for injection in pre-filled pen (liraglutide) Pleaserefer to the Summary of Product Characteristics for full information. Victoza® 2 x 3ml pre-filled pens. Victoza® 3 x 3 ml pre-filled pens. 1 ml of solution contains6 mg of liraglutide. Indication: Treatment of adults with type 2 diabetes mellitus incombination with metformin or a sulphonylurea, in patients with insufficient glycaemiccontrol despite maximal tolerated dose of metformin or sulphonylurea monotherapy;or in combination with metformin and a sulphonylurea, or metformin and athiazolidinedione in patients with insufficient glycaemic control despite dual therapy.Dosage: Victoza® is administered once daily by subcutaneous injection and can beadministered at any time independent of meals however, it is preferable that Victoza®
is injected around the same time of the day. Victoza® should not be administeredintravenously or intramuscularly. Recommended starting dose is 0.6 mg daily. Afterat least one week, the dose should be increased to a maintenance dose of 1.2 mg.Based on clinical response, after at least one week the dose can be increased to 1.8mg to further improve glycaemic control in some patients. Daily doses higher than1.8 mg are not recommended. When used with existing metformin therapy or incombination with metformin and thiazolidinedione therapy, the current dose ofmetformin and thiazolidinedione can continue unchanged. When added to existingsulphonylurea therapy or in combination with metformin and sulphonylureas, areduction in the dose of sulphonylurea may be necessary to reduce the risk ofhypoglycaemia. Victoza® can be used in the elderly (>65 years old) without doseadjustment but therapeutic experience in patients ≥75 years of age is limited. Nodose adjustment is required for patients with mild renal impairment (creatinineclearance 60-90 ml/min). Due to lack of therapeutic experience Victoza® is not to berecommended for use in patients with moderate (creatinine clearance of 30-59ml/min) and severe renal impairment (creatinine clearance below 30 ml/min), patientswith end stage renal disease, patients with hepatic impairment and children below18 years of age. Contraindications: Hypersensitivity to the active substance or anyof the excipients. Warnings and Precautions for use: Victoza® should not be usedin patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis.Victoza® is not a substitute for insulin. Addition of liraglutide in patients alreadytreated with insulin has not been evaluated and is therefore not recommended.
Limited experience in patients with congestive heart failure New York HeartAssociation (NYHA) class I-II and no experience in patients with NYHA class III-IV.Due to limited experience Victoza® is not recommended for patients withinflammatory bowel disease and diabetic gastroparesis. Victoza® is associated withtransient gastrointestinal adverse reactions, including nausea, vomiting and diarrhoea.GLP-1 analogues have been associated with pancreatitis; patients should be informedof symptoms of acute pancreatitis: persistent, severe abdominal pain. If pancreatitissuspected, Victoza® and other suspect medicinal products should be discontinued.Thyroid adverse events, including increased blood calcitonin, goitre and thyroidneoplasm reported in clinical trials particularly in patients with pre-existing thyroiddisease. Risk of hypoglycaemia in combination with sulphonylureas; lowered by dosereduction of sulphonylurea. Signs and symptoms of dehydration, including renalimpairment and acute renal failure reported with Victoza®. Patients should be advisedof potential risk of dehydration in relation to gastrointestinal side effects and takeprecautions to avoid fluid depletion. No studies on the effects on the ability to driveand use machines performed. Patients should be advised to take precautions to avoidhypoglycaemia while driving and using machines, in particular when Victoza® is usedin combination with a sulphonylurea. Substances added to Victoza® may causedegradation; in the absence of compatibility studies Victoza® must not be mixed withother medicinal products. Fertility, pregnancy and lactation: Victoza® shouldnot be used during pregnancy or during breast feeding. If a patient wishes to becomepregnant, or pregnancy occurs, treatment with Victoza® should be discontinued; useof insulin is recommended instead. Apart from a slight decrease in number of liveimplants, animal studies did not indicate direct harmful effects with respect to fertility.Undesirable effects: During clinical trials with Victoza® the most frequentlyobserved adverse reactions which varied according to the combination used(sulphonylurea, metformin or a thiazolidinedione) were: Very common: nausea,diarrhoea, headache when used in combination with metformin. Hypoglycaemia,nausea and diarrhoea when used with metformin and a sulphonylurea. Nausea,diarrhoea and vomiting when used with metformin and a thiazolidinedione; Common:anorexia, appetite decreased, dizziness, vomiting, dyspepsia, gastritis and injectionsite reactions when used in combination with metformin. Nasopharyngitis,hypoglycaemia, anorexia, nausea, diarrhoea, vomiting, dyspepsia, constipation,
abdominal discomfort, injection site reactions when used in combination with asulphonylurea. Bronchitis, anorexia, headache, vomiting, dyspepsia, abdominal painupper, constipation, toothache when used with metformin and a sulphonylurea.Nasopharyngitis, hypoglycaemia, anorexia, appetite decreased, headache, dyspepsia,constipation, flatulance, abdominal distension, gastroesophageal reflux disease,gastroenteritis viral, fatigue, pyrexia, injection site reactions when used withmetformin and a thiazolidinedione. Gastrointestinal adverse reactions are morefrequent at start of therapy but are usually transient. Very few hypoglycaemic episodesobserved other than with sulphonylureas. Patients >70 years or with mild renalimpairment (creatinine clearance 60-90 ml/min) may experience more gastrointestinaleffects. Consistent with medicinal products containing proteins/peptides, patientsmay develop anti-liraglutide antibodies following treatment but this has not beenassociated with reduced efficacy of Victoza®. Few cases reported of angioedema(0.05%) and acute pancreatitis (<0.2%). Injection site reactions usually mild. Thyroidneoplasms, increased blood calcitonin and goitres are the most frequent reportedthyroid adverse events – rates per 1000 subjects years of exposure were 6.8, 10.9and 5.4 of liraglutide treated patients in comparison with 6.4, 10.7 and 2.1 of placebotreated and 2.4, 6.0 and 1.8 of total comparator treated. The Summary of ProductCharacteristics should be consulted for a full list of side effects. Overdose: In theevent of overdose, appropriate supportive treatment should be initiated according tothe patient’s clinical signs and symptoms. MA numbers: Victoza® 2 x 3ml pre-filledpens EU/1/09/529/002. Victoza® 3 x 3ml pre-filled pens EU/1/09/529/003. LegalCategory: POM. For complete prescribing information please refer to The Summaryof Product Characteristics which is available on www.medicines.ie or by email [email protected] or from Medical department, Novo Nordisk Limited, 3-4 UpperPembroke Street, Dublin 2, Ireland; www.novonordisk.ie. Date created: Dec 2011.Victoza® is a trademark of Novo Nordisk A/S.
Information about adverse event reporting is available at www.imb.ie. Adverse events should be reported to the Novo Nordisk Medical department:
Tel: 1850 665 665.
Victoza® and the Apis bull logo are registered trademarks of Novo Nordisk A/S.
Date of preparation: January 2012. IR/LR/0112/0012
1. Pratley R et al. One year of liraglutide treatment offers sustained and more effective glycaemic control and weight reduction compared with sitagliptin, both incombination with metformin, in patients with type 2 diabetes: a randomised, parallel-group, open-label trial. Int J Clin Pract 2011;65(4):397-407
Further Information is available from: Novo Nordisk Limited
3/4 Upper Pembroke StreetDublin 2, IrelandTel: 01 678 5989 Fax: 01 676 3259
Lo Call: 1850 665 665www.novonordisk.ie
Victoza A4 Con Spring 2012(1):Layout 1 21/02/2012 14:01 Page 1
25
clinical review
Mean reductions in HbA1c: up to 1.50% (16 mmol/mol)1
Mean reductions in weight: up to 3.7 kg1
Improvements in SBP* from baseline1
Improvements in beta-cell function1
*SBP = Systolic Blood Pressure
...to help your patients with type 2 diabetes achieve:1
Abbreviated Prescribing InformationVictoza® 6 mg/ml solution for injection in pre-filled pen (liraglutide) Pleaserefer to the Summary of Product Characteristics for full information. Victoza® 2 x 3ml pre-filled pens. Victoza® 3 x 3 ml pre-filled pens. 1 ml of solution contains6 mg of liraglutide. Indication: Treatment of adults with type 2 diabetes mellitus incombination with metformin or a sulphonylurea, in patients with insufficient glycaemiccontrol despite maximal tolerated dose of metformin or sulphonylurea monotherapy;or in combination with metformin and a sulphonylurea, or metformin and athiazolidinedione in patients with insufficient glycaemic control despite dual therapy.Dosage: Victoza® is administered once daily by subcutaneous injection and can beadministered at any time independent of meals however, it is preferable that Victoza®
is injected around the same time of the day. Victoza® should not be administeredintravenously or intramuscularly. Recommended starting dose is 0.6 mg daily. Afterat least one week, the dose should be increased to a maintenance dose of 1.2 mg.Based on clinical response, after at least one week the dose can be increased to 1.8mg to further improve glycaemic control in some patients. Daily doses higher than1.8 mg are not recommended. When used with existing metformin therapy or incombination with metformin and thiazolidinedione therapy, the current dose ofmetformin and thiazolidinedione can continue unchanged. When added to existingsulphonylurea therapy or in combination with metformin and sulphonylureas, areduction in the dose of sulphonylurea may be necessary to reduce the risk ofhypoglycaemia. Victoza® can be used in the elderly (>65 years old) without doseadjustment but therapeutic experience in patients ≥75 years of age is limited. Nodose adjustment is required for patients with mild renal impairment (creatinineclearance 60-90 ml/min). Due to lack of therapeutic experience Victoza® is not to berecommended for use in patients with moderate (creatinine clearance of 30-59ml/min) and severe renal impairment (creatinine clearance below 30 ml/min), patientswith end stage renal disease, patients with hepatic impairment and children below18 years of age. Contraindications: Hypersensitivity to the active substance or anyof the excipients. Warnings and Precautions for use: Victoza® should not be usedin patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis.Victoza® is not a substitute for insulin. Addition of liraglutide in patients alreadytreated with insulin has not been evaluated and is therefore not recommended.
Limited experience in patients with congestive heart failure New York HeartAssociation (NYHA) class I-II and no experience in patients with NYHA class III-IV.Due to limited experience Victoza® is not recommended for patients withinflammatory bowel disease and diabetic gastroparesis. Victoza® is associated withtransient gastrointestinal adverse reactions, including nausea, vomiting and diarrhoea.GLP-1 analogues have been associated with pancreatitis; patients should be informedof symptoms of acute pancreatitis: persistent, severe abdominal pain. If pancreatitissuspected, Victoza® and other suspect medicinal products should be discontinued.Thyroid adverse events, including increased blood calcitonin, goitre and thyroidneoplasm reported in clinical trials particularly in patients with pre-existing thyroiddisease. Risk of hypoglycaemia in combination with sulphonylureas; lowered by dosereduction of sulphonylurea. Signs and symptoms of dehydration, including renalimpairment and acute renal failure reported with Victoza®. Patients should be advisedof potential risk of dehydration in relation to gastrointestinal side effects and takeprecautions to avoid fluid depletion. No studies on the effects on the ability to driveand use machines performed. Patients should be advised to take precautions to avoidhypoglycaemia while driving and using machines, in particular when Victoza® is usedin combination with a sulphonylurea. Substances added to Victoza® may causedegradation; in the absence of compatibility studies Victoza® must not be mixed withother medicinal products. Fertility, pregnancy and lactation: Victoza® shouldnot be used during pregnancy or during breast feeding. If a patient wishes to becomepregnant, or pregnancy occurs, treatment with Victoza® should be discontinued; useof insulin is recommended instead. Apart from a slight decrease in number of liveimplants, animal studies did not indicate direct harmful effects with respect to fertility.Undesirable effects: During clinical trials with Victoza® the most frequentlyobserved adverse reactions which varied according to the combination used(sulphonylurea, metformin or a thiazolidinedione) were: Very common: nausea,diarrhoea, headache when used in combination with metformin. Hypoglycaemia,nausea and diarrhoea when used with metformin and a sulphonylurea. Nausea,diarrhoea and vomiting when used with metformin and a thiazolidinedione; Common:anorexia, appetite decreased, dizziness, vomiting, dyspepsia, gastritis and injectionsite reactions when used in combination with metformin. Nasopharyngitis,hypoglycaemia, anorexia, nausea, diarrhoea, vomiting, dyspepsia, constipation,
abdominal discomfort, injection site reactions when used in combination with asulphonylurea. Bronchitis, anorexia, headache, vomiting, dyspepsia, abdominal painupper, constipation, toothache when used with metformin and a sulphonylurea.Nasopharyngitis, hypoglycaemia, anorexia, appetite decreased, headache, dyspepsia,constipation, flatulance, abdominal distension, gastroesophageal reflux disease,gastroenteritis viral, fatigue, pyrexia, injection site reactions when used withmetformin and a thiazolidinedione. Gastrointestinal adverse reactions are morefrequent at start of therapy but are usually transient. Very few hypoglycaemic episodesobserved other than with sulphonylureas. Patients >70 years or with mild renalimpairment (creatinine clearance 60-90 ml/min) may experience more gastrointestinaleffects. Consistent with medicinal products containing proteins/peptides, patientsmay develop anti-liraglutide antibodies following treatment but this has not beenassociated with reduced efficacy of Victoza®. Few cases reported of angioedema(0.05%) and acute pancreatitis (<0.2%). Injection site reactions usually mild. Thyroidneoplasms, increased blood calcitonin and goitres are the most frequent reportedthyroid adverse events – rates per 1000 subjects years of exposure were 6.8, 10.9and 5.4 of liraglutide treated patients in comparison with 6.4, 10.7 and 2.1 of placebotreated and 2.4, 6.0 and 1.8 of total comparator treated. The Summary of ProductCharacteristics should be consulted for a full list of side effects. Overdose: In theevent of overdose, appropriate supportive treatment should be initiated according tothe patient’s clinical signs and symptoms. MA numbers: Victoza® 2 x 3ml pre-filledpens EU/1/09/529/002. Victoza® 3 x 3ml pre-filled pens EU/1/09/529/003. LegalCategory: POM. For complete prescribing information please refer to The Summaryof Product Characteristics which is available on www.medicines.ie or by email [email protected] or from Medical department, Novo Nordisk Limited, 3-4 UpperPembroke Street, Dublin 2, Ireland; www.novonordisk.ie. Date created: Dec 2011.Victoza® is a trademark of Novo Nordisk A/S.
Information about adverse event reporting is available at www.imb.ie. Adverse events should be reported to the Novo Nordisk Medical department:
Tel: 1850 665 665.
Victoza® and the Apis bull logo are registered trademarks of Novo Nordisk A/S.
Date of preparation: January 2012. IR/LR/0112/0012
1. Pratley R et al. One year of liraglutide treatment offers sustained and more effective glycaemic control and weight reduction compared with sitagliptin, both incombination with metformin, in patients with type 2 diabetes: a randomised, parallel-group, open-label trial. Int J Clin Pract 2011;65(4):397-407
Further Information is available from: Novo Nordisk Limited
3/4 Upper Pembroke StreetDublin 2, IrelandTel: 01 678 5989 Fax: 01 676 3259
Lo Call: 1850 665 665www.novonordisk.ie
Victoza A4 Con Spring 2012(1):Layout 1 21/02/2012 14:01 Page 1
• Chol<4.5, lDl<2.5,HDl>1.2,Trigly<1.7 • No smoking• BMI 19-25, Waist Circ-m<94cm f<80cm• Exercise – >30 minutes at least 5 days per week (150 min/
mod, 90min/vigorous)
regular patient follow-upThe 2008 Guidelines2 recommend that patients attend for review of their diabetes every 3-6 months. The practice protocol for recall may be that you advise the patient when their next review is due and the onus is on the patient to make the appointment. Actually giving the patient a return appointment increases attendance; as patients may go to the desk on the way out and there is a queue so the return appointment is not made. Your protocol could include follow up of those who do not attend, either by phone call/text or recall letter.
Having the diagnosis of diabetes clearly visible on the patient’s file facilitates opportunistic reminders to attend for diabetic review, when the patient attends for other reasons. Having a formal recall system means that you can be confident the patient has been invited for their diabetes review, that they haven’t been lost to follow-up because they were not aware it was necessary. Patient empowerment hugely facilitates diabetes care, as a patient who is aware of what is required for self management will seek the required care even when it is not offered. It is essential to explore the patient’s attitude and health beliefs around diabetes as eliciting these at the outset can provide an opportunity for you to address fears and correct any misinformation. If someone’s only experience of diabetes has been associated with amputations, the fear generated by this can be a huge barrier to involvement with self-management.
It is essential to provide ‘protected time’ for a diabetes review, as opportunistic reviews in a routine appointment time is insufficient for a comprehensive review. The diabetic review appointment usually takes 20 to 30 minutes. Protected time can be a longer appointment time or the practice may choose to provide a dedicated diabetes clinic.
Investigations• HbA1c• Fasting lipid profile• Full blood count• Microalbuminuria• Serum creatinine• Serum iron• Serum transferrin• Thyroid function Tests• 12-lead ECG• Provision of education and psychological support:
explain, advise, follow-up.
organisation of careEncourage the patient to join an integrated care programme if available in your practice. This usually involves the patient signing a consent form.
Add the patient to practice register and give follow-up appointment.
The patient should attend for retinopathy screening, podiatrist – if not categorised as low risk as per screening protocol – and a dietitian.
Consider the need for review by diabetic nurse specialist.Set up a management plan for the control of glycaemia, lipid
levels and blood pressure with defined targets appropriate for
the individual patient as outlined later in this guideline.Identify lifestyle issues that need to be addressed.Issue the patient with glucose monitor and instruct in its use.
regular review includes Recent life-events/new symptoms
1. New difficulties in self-management of diabetes2. Self-monitored results; discussion of their meaning3. Dietary behaviours, physical activity and smoking4. Diabetes education, skills and foot care5. Blood glucose, lipid and blood pressure therapy and results6. Other medical conditions and therapy affecting diabetes7. Psychological, lifestyle and social aspects8. Arterial/foot risk factors identified at annual review9. Complications and other problems identified at annual
review.
Annual reviewAlong with all of the areas monitored at regular review, the annual review also includes surveillance of the following:
symptoms: ischaemic heart disease, peripheral vascular disease – neuropathy, erectile dysfunction. All patients with
symptoms that might reflect vascular disease, particularly ischaemic heart disease, should be investigated.
feet: footwear, deformity/joint rigidity, poor skin condition, ischaemia, ulceration, absent pulses, sensory impairment.
eyes: visual acuity and retinal review by ophthalmologist/retinal screening programme.
kidney: renal damage, albumin excretion and serum creatinine.
Arterial risk: blood glucose, blood pressure, blood lipids, and smoking status.
Attendance: podiatry, dietician and other as indicated.Integrated care mandates joint care at primary and
secondary levels. As outlined above a review of the patient in the DiabetesCentre should take place at 1-2 yearly intervals. This interval should be agreed locally.• BP/WT/HT/BMI/Waist Circ• F.HX/Medication hx and current meds• Medical Hx • Complications. Ask re-claudication as patient may not elicit
this information• Smoking status• Physical activity• Diet• Foot assessment. If low risk as per screening guidelines
(Harkins 2008)• Arrange retinopathy screening appointment• Knowledge assessment.
health Promotion empowerment ModelPatients are empowered when they have:• The knowledge to make informed decisions.• The support and resources to implement change.• A partnership relationship with their healthcare professional.
refer to:• Retinopathy screening • Podiatrist – community if foot screen not low risk• Dietitian – community• Structured Pt. Ed. – XPERT/CODE/Desmond• Endocrinologist (Not practical to refer all patients with type
2 diabetes)• Individual management plan: control blood sugar, lipids, BP,
lifestyle modification.
26
clinical review
follow up appointment• Newly diagnosed patient may need to be seen weekly x4
or monthly x3 then every 3 months x1yr. This needs to be individually tailored.
• lifestyle modification is the cornerstone of treatment and as the patient is responsible for 95% of his/her treatment, self management education is vital.
social and emotional well being• Build knowledge, skills and confidence• Explore worries – existing knowledge of diabetes and its
complications.• Explore feelings – failure/self blame – if associated with
obesity, may feel self inflicted.• Feeling helpless and alone.• Overwhelmed by the burden of chronic disease – almost a
grief reaction.• Explore feelings of depression.
home blood sugar monitoring• Necessary if patient is on insulin.• Some evidence suggests not associated with improved
control in type 2 if not on insulin.• Most treatment decisions are made on HbA1c results not
home BS readings.• Time spent teaching monitor use may be better spent on
other aspects of diabetes education.• Beneficial if patient is adjusting diet according to readings
(pre-prandial BS<6, 2hr PP BS<8).• Offer only as an integral part of self-management. Discuss its
purpose and agree how it should be interpreted and acted upon.
Patient education • What is diabetes• Complications of diabetes• Diet/exercise/Wweight control/alcohol• Aims of diabetes care• Eye and foot care• Discuss self-monitoring• Allowances/lTI Scheme/GMS/DFI• Medications – uses and side effects, mention insulin• Hypoglycaemia• Hyperglycaemia• Sick days
• Employment/insurance/driving issues• Flu and pneumonia vaccine
structured Patient educationGroup Education• DESMOND – Diabetes EducationaAnd Self Management for
Ongoing and Newly Diagnosed – Type 2. 6-10 people, 8 hour programme.
• XPERT-Expert Patient Education versus Routine Treatment – type 2. 2 hours x 6weeks.
• CODE-Community Oriented Diabetes Education – type 2. 2hour x 4 weeks, follow-up 6 months.
• DAFNE – Dose Adjustment For Normal Eating – type 1. Group (4-6) 5 Day course.
• Berger – type 1. 3 day course.
Dietary advise• Healthy eating, not a special restrictive diet – use food
pyramid.• Regular meals based on high fibre starchy foods.• NB portion sizes.• Food and drinks low in sugar.• low in fat and salt.• 5 portions fruit/veg per day.• Alcohol – 3 units/day men, 2 units women with some alcohol
free days.• No diabetic products – expensive and unnecessary.• Watch weight – calories to match activity.• Note if not on meds associated with hypoglycaemia no need
to pre-load with calories before exercising.
Physical activity• 30 min per day, note 3x10 min spread over the day is
beneficial.• Housework/stairs/gardening.• GP exercise referral scheme. • Resistance e xercise – armchair programme.• Walking groups/walking buddy.• Find activity that suits patients interest and lifestyle –
increase gradually. If patient enjoys the activity more likely to sustain it long-term.
• Patient should be able to talk while doing activity and not be out of breath.
• Appropriate footwear. Check feet after activity for blisters.• If on insulin check BS before activity.
Exercise 3 times a week for 6 months reduction in HbA1cAerobic exercise only – 0.51% Resistance training with weights. – 0.38% Both types of exercise – 0.96%
Sigal RJ. et al. Ann Int Med 2007;147:357-69.
Comparison with some oral hypoglycaemic agents• Glitazone (Actos)
Reduce HbA1c by 0.8-1%• GlP-1 analogues (Byetta, Victoza)
Reduce HbA1c by 1%• DPP4 Inhibitors (Januvia, Onglyza):
Reduce HbA1c by 0.5-1%JAMA 2007;298:194-206
Cardiovascular fitness• Patients who were fit had 1/3 the risk of non-fit subjects even
if they had a high BMI.
having the diagnosis of diabetes clearly visible on the patient’s file facilitates opportunistic reminders to attend for diabetic review, when the patient attends for other reasons.
Dat
e o
f p
rep
arat
ion:
Ap
ril 2
011
IE.G
LA.1
0.03
.01
Abbreviated Prescribing InformationLantus® 100 Units/ml solution for injection (insulin glargine).Presentation: 1 glass vial/pack containing 10ml solution (1,000 U insulin glargine, equivalent to 36.4mg) or 5 glass cartridges/pack each containing 3ml solution (300 U insulin glargine, equivalent to 10.92mg) or packs of 5 OptiSet® pens each containing 3ml solution (300 U insulin glargine, equivalent to 10.92mg) or packs of 5 Solostar® pens each containing 3ml solution (300 U insulin glargine, equivalent to 10.92mg). (Excipients: zinc chloride, m-cresol, glycerol, hydrochloric acid, sodium hydroxide and water for injection). Indications: Treatment of adults, adolescents and children of 6 years or above with diabetes mellitus, where treatment with insulin is required. Dosage and Administration: Lantus contains insulin glargine, an insulin analogue, and has a prolonged duration of action. Lantus should be administered subcutaneously once daily at the same time each day and the dose should be individually adjusted. Elderly population (≥ 65 years old): Progressive deterioration of renal function may lead to a steady decrease in insulin requirements. Renal impairment: Insulin requirements may be diminished due to reduced insulin metabolism. Hepatic impairment: Insulin requirements may be diminished due to reduced capacity for gluconeogenesis and reduced insulin metabolism. Paediatric population: Safety and efficacy of Lantus have been established in adolescents and children of 6 years and above. In children (aged 6 years or above), only evening administration has been studied. Due to limited experience on the efficacy and safety of Lantus in children below the age of 6 years, Lantus should only be used in this age group under careful medical supervision. Close metabolic monitoring is recommended during transition from other insulins to Lantus and in circumstances that increase susceptibility to hypo- or hyperglycaemia. Lantus must not be mixed with other insulins or diluted. Mixing or diluting can change its time/action profile and mixing can cause precipitation. Contraindications: Hypersensitivity to insulin glargine or to any of the excipients. Precautions and Warnings: Lantus is not the insulin of choice for treatment of diabetic ketoacidosis. In case of insufficient glucose control or a tendency to hypo/hyperglycaemic episodes, all relevant factors must be reviewed before dose adjustment is considered. Insulin administration may cause insulin antibodies to form. In rare cases, these insulin antibodies may necessitate adjustment of the insulin dose in order to correct a tendency to hyper- or hypoglycaemia. Particular caution should be exercised, and intensified blood monitoring is advisable, for patients in whom hypoglycaemic episodes might be of clinical relevance and in those with intercurrent illness, where dose adjustments may be required. Warning signs of hypoglycaemia may be changed, less pronounced or absent in certain risk groups, including patients in whom: glycaemic control is markedly improved; hypoglycaemia develops gradually; an autonomic neuropathy is present; or elderly patients. Prolonged effect of subcutaneous Lantus may delay recovery from hypoglycaemia. Adherence of the patient to the dosage and dietary regimen, correct insulin administration and awareness of hypoglycaemia symptoms are essential to reduce the risk of hypoglycaemia. Cardiac failure has been reported when pioglitazone was used in combination with insulin; especially in patients with risk factors for heart failure. Observe for signs and symptoms of heart failure (weight gain and oedema) if pioglitazone is used with Lantus. Discontinue pioglitazone if symptoms of cardiac deterioration occur. Interactions: Substances that may enhance the blood glucose-lowering effect and increase susceptibility to hypoglycaemia include oral antidiabetic medicinal products, ACE inhibitors, disopyramide, fibrates, fluoxetine, MAO inhibitors, pentoxifylline, propoxyphene, salicylates and sulfonamide antibiotics. Substances that may reduce the blood glucose-lowering effect include corticosteroids, danazol, diazoxide, diuretics, glucagon, isoniazid, oestrogens and progestogens, phenothiazine derivatives, somatropin, sympa-thomimetic medicinal products (e.g. epinephrine [adrenaline], salbutamol, terbutaline), thyroid hormones, atypical antipsychotic medicinal products (e.g. clozapine and olanzapine) and protease inhibitors. Beta-blockers, clonidine, lithium salts or alcohol may potentiate or weaken the blood glucose-lowering effect of insulin. Under the influence of sympatholytic medicinal products, the signs of adrenergic counter-regulation may be reduced or absent. Fertility, Pregnancy and Lactation: Pregnancy: For insulin glargine no clinical data on exposed pregnancies from controlled clinical trials are available. A moderate amount of data on pregnant women exposed to marketed insulin glargine indicate no adverse effects of insulin glargine on pregnancy and no malformative nor feto/neonatal toxicity. Animal data do not indicate reproductive toxicity. The use of Lantus may be considered during pregnancy, if necessary. Breastfeeding: It is unknown whether insulin glargine is excreted in human milk. No metabolic effects of ingested insulin glargine on the breastfed newborn/infant are anticipated since insulin glargine as a peptide is digested into aminoacids in the human gastrointestinal tract. Breastfeeding women may require adjustments in insulin dose and diet. Fertility: Animal studies do not indicate direct harmful effects with respect to fertility. Effects on ability to drive and use machines: The patient’s ability to concentrate and react may be impaired as a result of hypo/hyperglycaemia or, for example, as a result of visual impairment. Patients should be advised to take precautions to avoid hypoglycaemia whilst driving or operating machinery. Adverse Reactions: Hypoglycaemia, in general the most frequent adverse reaction of insulin therapy, may occur if the insulin dose is too high in relation to the insulin requirement. Metabolism and nutrition disorders: Very Common (≥ 1/10): Hypoglycaemia. Skin and subcutaneous tissue disorders: Common (≥ 1/100 to <1/10): Lipohypertrophy. General disorders and administration site conditions: Common: Injection site reactions such as: redness, itching, pain, itching hives, swelling or inflammation. Paediatric Population (≤18 years): relatively more frequent injection site reactions, injection site pain and skin reactions (rash, urticaria) were received from post marketing surveillance. Please refer to the Summary of Product Characteristics (SPC) for complete list of adverse reactions. Overdose may lead to severe and sometimes prolonged and life-threatening hypoglycaemia. Mild episodes can usually be treated with oral carbohydrates. More severe episodes may be treated with intramuscular/subcutaneous glucagon or concentrated intravenous glucose. Pharmaceutical Precautions: Store unopened cartridges/vials/OptiSet/ Solostar pens at 2°C–8°C. Do not freeze. Once opened, do not store above 25°C and use within 4 weeks. Once in use, do not refrigerate OptiPen® Pro pen (containing cartridge), vial, OptiSet or Solostar pens. Legal Category: POM. Marketing Authorisation Numbers: Lantus 100 U/ml solution for injection in a cartridge (5 cartridges/pack): EU/1/00/134/006, Lantus 100 U/ml solution for injection in a 10ml vial (1 vial/pack) EU/1/00/134/012, Lantus 100 U/ml OptiSet solution for injection (5 pens) EU/1/00/134/010, Lantus 100 Units/ml solution for injection in a pre-filled pen (Solostar® 5 pens) EU/1/00/134/033. Marketing Authorisation Holder: sanofi-aventis Deutschland GmbH, D-65926 Frankfurt am Main, Germany. Please refer to SPC which can be found on IPHA @ http://www.medicines.ie/ before prescribing. For further information contact [email protected] or Medical Information Department, sanofi-aventis Ireland Ltd., 18 Riverwalk, National Digital Park, Citywest Business Campus, Dublin 24. Ph.: 01 403 5600.Information about adverse event reporting can be found at www.imb.ieAdverse events should be reported to the sanofi-aventis Drug Safety DepartmentDate of Revision: March 2011
1. Porcellati F et al, Diabetes Care Vol 30; No 10; 2447 - 2452 October 2007. 2. Lantus SPC.
Effective, right from the start
24-hourpeakless efficacy1,2
28
clinical review
• Men with BMI of <27 who were unfit had 2/3 greater risk of cardiovascular event.Blair, SN 1997
Weight management10% weight loss results in:
• 15% reduction in HbA1c• 10mmhg reduction systolic BP• 20mmhg reduction diastolic BP• 10% reduction cholesterol• 30% reduction in triglyceridesJung RT, 1997 British Medical Bulletin 53:307-21
Weight management• Patients with BM1 >30 non-smoker• Patients with BM1 >30 smoke have similar life expectancy.Blair, SN 1997
Addressing obesity and smoking cessationReview appointment• Review 3-6 monthly.• Discuss self management issues.• Explore what aspects of dabetes the patient is ready to
address.• BP/diet/physical activity/alcohol/smoking/weight control.
(Target may be not to increase weight)• Results – HbA1c, FlP, Renal profile.• Agree targets – short-term/achievable.• Ongoing education.• Social impact of diabetes.• Psychological impact of chronic illness.
Annual review• In shared care annual review occurs in OPD
As for regular review and the following:• Symptoms – IHD, Neuropathy, Erectile dysfunction (50%
males with diabetes), claudication.• Feet-footwear, skin condition/integrity, pulses, sensation.• Eyes – annual retinal screening.• Kidneys – urea/Creat/eGFR/ urine microalb. (if no
proteinuria).
• ?attending podiatrist/dietitian.Categorise as per Foot Assessment Protocol: low/mod/high/
active disease. Refer as per screening protocol Harkins (2008).
MicroalbuminuriaPredictor for retinopathy and cardiovascular disease
• Reversible damage.• Improve glycaemic+BP control.• Start ace inhibitor or angiotension reception blocker even if
normotensive to delay the progression to macroalbuminuria.
Albumin Creatinine Ratio (ACR)• Normal <2.5 – repeat annually• Microalbuminuria: 2.5-25 repeat x 3 over 6 months • 2 out of 3 positive = nephropathy• >25 macroalbuminuria (Proteinuria)
Exclude UTI.
key points • Practice nurse ideally placed for primary prevention in
childhood – Healthy diet/physical activity.• Targeted case finding in general p ractice – early
detection.• Clearly document diagnosis of diabetes in patient
file – even if not involved in delivering diabetes care. Opportunistically check patient is attending for regular review.
• If delivering diabetes care – register, review, recall. • lifestyle factors: healthy diet/exercise/smoking
cessation.
resources Diabetes Federation of Ireland – www.diabetesireland.ie. Patient information booklets, membership form, Structured Patient education Programme – CODE. Smoking Cessation/Physical Activity/leaflets – HSE Health Promotion Unit. Community Podiatry.Community Dietitian, Structured Pt. Ed. XPERT Programme.
references1. Roglic G, Unwin N, Bennett P, Mathers C, Tuomilehto J, NagS, et al. The
burden of mortalit attributable to diabetes. Diabetes Care2005;28(9):2130-5.2. Harkins V. A Practical Guide to Integrated Type 2 Diabetes Care. In: Irish
College of General Practitioners, Health Service Executive, Irish Endocrine Society, editors. Dublin: Health Service Executive; 2008.
3. Wild S, Roglic G, Green A, Sicree R, King H. Global Prevalence of Diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care2004 May 1, 2004;27(5):1047-53.
4. Zimmet P, Alberti K, Shaw J, Oakley W. Global and societal implications of the diabetes epidemic. Nature2001;414:782-7.
5. Olivarius N, Beck-Nielsen H, Andreasen A, Horder M, Pedersen P. Randomised controlled trial of structured personal care of type 2 diabetes mellitus. BMJ2001;323(7319):970-5.
6. UKPDS. UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonyureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes. lancet1998;352(9131):837-53.
7. Murphy K, Mc Hugh S, O’Keeffe J, Moran J. Diabetes Interest Group Audit Report; Dec 2007 – May 2008. 2009.
8. Murphy K, Mc Hugh S, Moran J. Diabetes In General Practice Audit Report; Jun 2009 – May 2010. 2011.
It is essential to provide ‘protected time’ for a diabetes review, as opportunistic reviews in a routine appointment time is insufficient for a comprehensive review.
*IMPORTANT CHANGE: Prostap Dual Chamber Syringe (DCS) is replacing Prostap, so it’s necessary for prescriptions to reflect this change of name. A video demonstrating
the five steps of administration can be viewed at www.ProstateCancerUpdate.ie
Needle shown is not actual size
*
come as standardWhen it comes to the treatment of prostate cancer,look no further than Prostap DCS
Prescribing InformationPROSTAP *SR DCS, 3.75mg / PROSTAP *3 DCS, 11.25mg powder and solventfor prolonged-release suspension for injection in pre-filled syringe; LeuprorelinAcetate 1 month / 3 month Depot Injection Before prescribing PROSTAP SRDCS/PROSTAP 3 DCS, please refer to the full Summary of Product Characteristics(SmPC). PRESENTATION: Powder and solvent for prolonged- release suspension forinjection in pre-filled syringe (Dual Chamber Syringe); PROSTAP SR DCS Powder:Contains 3.75mg of leuprorelin acetate. PROSTAP 3 DCS Powder: Contains 11.25mgof leuprorelin acetate. INDICATIONS: PROSTAP SR DCS and PROSTAP 3 DCS:Management of prostatic carcinoma for which suppression of testosterone is indicated.Management of oestrogen dependent gynaecological disorders including themanagement of pain and lesions associated with endometriosis. Preoperativemanagement of uterine fibroids to reduce their size and associated bleeding.PROSTAP SR DCS is also indicated for: Endometrial preparation prior to intrauterinesurgical procedures including endometrial ablation or resection. DOSAGE ANDADMINISTRATION: Male adults: PROSTAP SR DCS: 3.75mg administered as a singlesubcutaneous or intramuscular injection every month. PROSTAP 3 DCS: 11.25mgadministered as a single subcutaneous or intramuscular injection every 3 months. Donot discontinue when remission or improvement occurs. Response to therapy shouldbe monitored clinically. Female adults: Treatment should be initiated during the first5 days of the menstrual cycle. PROSTAP SR DCS: 3.75mg administered as a singlesubcutaneous or intramuscular injection every month for a period of 6 months(endometriosis), for a maximum of 6 months (uterine fibrosis). Vary the injection siteperiodically. PROSTAP 3 DCS: 11.25mg administered as a single subcutaneous orintramuscular injection every 3 months: For a period of 6 months (endometriosis), fora maximum of 6 months (uterine fibroids). Vary the injection site periodically. Elderly:
As for adults. Children: Use in children not established. CONTRAINDICATIONS:Hypersensitivity to any of the ingredients or to synthetic GnRH or GnRH derivatives.Men: Use in patients insensitive to endocrine therapy or post-orchidectomy. Women:Use in women who are or may become pregnant, in women who are breastfeedingor who have undiagnosed abnormal vaginal bleeding. PRECAUTIONS ANDWARNINGS: Development or aggravation of diabetes may occur, therefore diabeticpatients may require more frequent monitoring of blood glucose. Hepatic dysfunctionand jaundice with elevated liver enzyme levels have been reported. Therefore, closeobservation should be made and appropriate measures taken if necessary. Spinalfracture, paralysis, hypotension and worsening of depression have been reported.Men: Should only be used under the direction of a clinician having appropriatefacilities for monitoring response to treatment. Testosterone should fall to castratelevels within 6 weeks; failure to do so requires reassessment. Initial transient rise inlevels of testosterone may be associated with tumour “flare” manifesting as systemicor neurological symptoms. Patients at risk of ureteric obstruction or spinal compressionshould be carefully considered and monitored during initial weeks of treatment. Ananti-androgen may be administered to reduce the risk of “flare” (see section 4.4 ofthe SmPC). Any urological or neurological complications which occur should betreated by appropriate specific measures. Women: Menstruation should stop duringtreatment; therefore the patient should notify her physician if regular menstruationpersists.Spotting/breakthrough bleeding may occur with PROSTAP SR DCS andPROSTAP 3 DCS treatment. An increase in clinical signs and symptoms may beobserved during the initial days of therapy as sex steroids temporarily rise abovebaseline. In the case of uterine fibroids, it is mandatory to confirm the diagnosis offibroids and exclude ovarian mass, before therapy is instituted. May cause an increasein uterine cervical resistance. The induced hypo-oestrogenic state results in a clinically
significant loss in bone density over the course of treatment, some of which may notbe reversible. The generally accepted level of bone loss with LHRH analogues suchas PROSTAP is 5%. During one 6 month treatment period, this bone loss should notbe important. In patients with major risk factors for decreased bone mineral contentsuch as chronic alcohol and/or tobacco use, strong family history of osteoporosis, orchronic use of drugs that can reduce bone mass, therapy may pose an additional risk.Treatment options for vasomotor symptoms and bone mineral density loss should beconsidered. In the treatment of endometriosis, the addition of HRT (an oestrogen andprogestogen) has been shown to reduce bone mineral density loss and vasomotorsymptoms. SIDE EFFECTS: Refer to section 4.8 of the SmPC in relation to other sideeffects Serious: Pituitary apoplexy, anaphylactic reactions, alteration of glucosetolerance which may affect diabetic control. Common: Weight gain, anorexia,depression (occasionally severe), headache, hot flushes, nausea, vomiting, muscleweakness, arthralgia, impotence, decreased libido, orchiatrophy, gynaecomastia,irritation at the injection site, sweating, fatigue, peripheral oedema, insomnia,parasthesia, increases in liver function test values (usually transient). Men: If tumourflare occurs, symptoms and signs due to disease may exacerbate e.g. bone pain andurinary obstruction, which should subside on continuation of therapy. Women:Adverse events occurring most frequently with PROSTAP SR DCS and PROSTAP 3DCS are associated with hypo-oestrogenism. The induced hypo-oestrogenic stateresults in a loss in bone density over the course of treatment, some of which may notbe reversible (see Precautions and Warnings). In women who have submucous fibroidsthere have been reports of severe bleeding following the administration of PROSTAPSR DCS and PROSTAP 3 DCS as a consequence of the acute degeneration of thefibroids. Patients should be warned of the possibility of abnormal bleeding or pain incase earlier surgical intervention is required. LEGAL CATEGORY: POM. PACKAGE
QUANTITIES: PROSTAP SR DCS: One dual chamber pre-filled syringe containing3.75mg leuprorelin acetate powder in the front chamber and 1ml of Sterile Solvent inthe rear chamber. One 25 gauge needle, one syringe plunger and one injection siteswab are included in a single injection pack. PROSTAP 3 DCS: One dual chamber pre-filled syringe containing 11.25mg leuprorelin acetate powder in the front chamberand 1ml of Sterile Solvent in the rear chamber. One 23 gauge needle, one syringeplunger and one injection site swab are included in a single injection pack. PRODUCTAUTHORISATION NUMBER: PROSTAP SR DCS PA 1547/3/3; PROSTAP 3 DCS PA1547/3/4. PRODUCT AUTHORISATION HOLDER: Takeda UK Limited, Takeda House,Mercury Park, Wooburn Green, High Wycombe, Bucks. HP10 0HH, UK. DATE OFPREPARATION: May 2011. Full prescribing information is available on request from:Takeda UK Limited, Takeda House, Mercury Park, Wooburn Green, High Wycombe,Bucks. HP10 0HH, UK. Tel: +44 1628 537900 * Trade mark of Takeda PS110525.
Date of preparation: August 2011 PT110703
Adverse events should be reported to the Pharmacovigilance Unit at the Irish Medicines Board
(IMB) ([email protected]). Information about adverse event reporting
can be found on the IMB website (www.imb.ie). Adverse events should also be reported to
Takeda UK Ltd. on +44 1628 537900.
PRI132 rocket ad AW_Layout 1 23/08/2011 12:22 Page 1

30
ethics
Treoir, the Irish word for direction or guidance, operates the National Specialist Information Service for Unmarried Parents and those working with them, including general practice nurses. All the information you need when working with unmarried families can
be obtained from Treoir at loCall 1890 252 084.
legal status of unmarried fathersAccording to the Central Statistics Office1 in 2010 over 44% of first births in Ireland were to unmarried parents and approximately 50% of births to unmarried parents were to couples living together. Unmarried parents and professionals are often misinformed about the legal position of parents who are not married to each other. For instance, the commonly held belief that having the (unmarried) father’s name on his child’s birth certificate gives the father legal rights in respect of his child.
If the father is not a legal guardian of his child:• he cannot give consent to medical treatment for his child.• he has no right to medical information on his child.• he has no right to visit his child in hospital without the
mother’s consent.• he has no right to information about his child from school
without the mother’s consent.• he has no right to have a say in his child’s religion. • his child can be taken out of the country without his consent.
Treoir’s major challenge is to alert parents to the fact that unmarried fathers do not have any automatic rights to their children and that they can take action to remedy the situation by becoming joint guardians with the mother. This can be done by agreement through signing the statutory declaration (SI No 5 of 1998). If the mother does not agree, the father can apply to court for his guardianship rights. It is often only when the relationship deteriorates, or ends, that the issue of guardianship arises. Typically, in these situations, fathers are left with no option but to go to the local district court to seek their guardianship rights.
Medical consentThe issue of medical consent for non-emergency treatment and services for children of unmarried parents can be very confusing. However, the Guidelines issued by the Health Service Executive (HSE) in 20091 state that “only parents who are guardians...can give consent on behalf of their children”. The Guidelines state that at the point of referral the names of any legal guardian(s) of a child should be requested and recorded. Therefore, it is essential for general practice nurses to request and record the names of any legal guardian of a child. Where the parents are married to each other, both are automatically guardians of their children. As mentioned above, where parents are not married to each other, only the mother is automatically a guardian of her child.
Can unmarried parents consent to medical treatment?Irish general practice nurses provide an invaluable service to a wide population from newborns to the elderly. As a consequence it is crucial that they have an extensive range of up-to-date information available to them. In this article Treoir focuses on key issues relevant to single pregnant women, unmarried parents and those involved with them.
31
ethics
young parentsIn situations where the parent is under 18 years of age and the child needs non-emergency treatment, it is uncertain whether or not minor parents can consent to treatment for their child since minors are deemed to be legally incompetent to give consent. However, the HSE guidelines state that in law, the unmarried mother of a child is the sole legal guardian and her wishes, providing she is competent to understand the proposed treatment, are to be taken into account.
The HSE guidelines go on to say that it would be prudent practice to attempt to:• obtain the consent of an appropriate next of kin who is
competent to consent and which consent is in the best interests of the child
• include all parties in the consent process including the parent
• ensure that if the next of kin does give consent that their signature and name is recorded on the consent form and
• ensure that such situations are recorded in detail in the patient’s medical record/notes
• in case of doubt/uncertainty, it is recommended that healthcare providers seek further legal advice.
dNA testingTreoir’s National Information Service often receives queries about how to get a DNA test to establish paternity. It is very important for the child to have accurate information on her/his parentage, not only for identity reasons but also for their medical history. It may be necessary to establish paternity, where paternity is in doubt, in order to pursue child maintenance or to support a case for access and guardianship. The court hearing these proceedings may order that the parents involved undergo paternity testing before an order can be made.
In Ireland there are many services available for DNA testing. Some of these are listed on Treoir’s ‘Establishing Paternity’
information leaflet, which is downloadable from www.treoir.ie. The testing service will take samples from the mother, the child and alleged father or can arrange for a sample kit to be sent out to a nominated GP. The processing of all the samples is carried out by accredited laboratories overseas, usually in England, and results can be provided within two to three weeks.
About TreoirTreoir is committed to providing a comprehensive information service to unmarried parents and those professionals involved with them. To this end Treoir has developed a range of support services including a comprehensive website, www.treoir.ie, which contains information relevant to unmarried parents on their legal rights; social welfare entitlements; co-habiting parents; shared parenting; representing yourself in court and much more. Treoir’s confidential phone service (loCall 1890 252 084) is extremely popular because it provides a unique opportunity for clients to receive up-to-date information on a one-to-one basis from highly experienced and empathetic information officers.
In addition, Treoir produces a number of useful publications including the ‘Information Pack for Unmarried Parents’, ‘Young Parents Survival Guide’, ‘Being There for Them’ (for grandparents) and a series of information leaflets on such topics as DNA testing, guardianship, access, shared parenting, birth registration, passports etc. In addition Treoir circulates a regular E-mail Bulletin containing all the latest news on issues affecting unmarried parents to over 1,000 subscribers. Email [email protected] to have your name added to the list.
Information workshops are provided to groups of professionals working with unmarried parents and to parents themselves. Workshops can be tailored to meet the particular needs of a group. Topics covered include legal rights of unmarried parents, the new laws for co-habitants, shared parenting and social welfare issues.
for further information contact:TREOIR14 Gandon House, lower Mayor Street, IFSC, Dublin 1loCall: 1890 252 084 Phone: 00353 1 6700 120 [email protected] informed: follow us in Facebook and Twitter.HSE Children and Family Services , Staff Guidelines for Obtaining Consent for Non Emergency Treatment/Services from Parents of Children and Young People Under the Age of 18 years. Children and Families Document (Ref C+F 2/2009)
references:1. www.cso.ie
In situations where the parent is under 18 years of age and the child needs non-emergency treatment, it is uncertain whether or not minor parents can consent to treatment for their child since minors are deemed to be legally incompetent to give consent.
32
in practice
Eating disorders – the dietitian’s role in a CAMHS settingThis article focuses on the dietetic management of child and adolescent anorexia nervosa in a specialist CAMHS in-patient unit setting.
JoANNe corbeTT, SENIOR DIETITIAN, EIST lINN CAMHS IN-PATIENT UNIT, HSE SOUTH, BESSBOROUGH, BlACKROCK, CORK
Child and Adolescent Mental Health Services (CAMHS) provide a service to young people under 18 years (and their families) with severe emotional and behavioural disorders where there is a likelihood of mental illness. Young people are referred by
their GP/primary care team to the local community CAMHS multidisciplinary team for assessment and intervention/treatment. Referrals include eating disorders, psychosis, anxiety and depression, obsessive compulsive disorder and attention deficit hyperactivity disorder. More severe and complex cases may be referred by the Community CAMHS teams onto their regional specialist CAMHS in-patient unit for admission.
effects of edEating disorders such as anorexia nervosa (AN), bulimia nervosa (BN) and ‘atypical’ versions or ‘eating disorders not otherwise specified’ (EDNOS) are insidious mental illnesses with morbid fear of weight gain at their core.1
With AN, characteristic dietary restriction may or may not be augmented by self-induced vomiting, laxatives, excessive exer-cise, and/or diuretics. The physical deterioration associated with malnutrition affects every system in the body, with symptoms that include amenorrhoea, arrhythmia, bradycardia, hypoten-sion and hypothermia. Adolescence is already a nutritionally vulnerable time with increased requirements for nutrients to fuel maturation. The normal dramatic physical development of teenage years is therefore halted in its tracks, with significant
impact on growth, bone health, body composition, hormonal function and consequences for later health if illness is protracted or severe. Starvation also severely affects normal teenage emo-tional, psychosocial and cognitive development. The cognitive effects of malnutrition include anxiety, self-isolation, obsessional behaviours, perfectionism and total rigidity around food.
bulimia nervosaBulimia nervosa (BN), like AN, arises from initial attempts to restrict food. Bulimia often evolves from a pre-existing anorexia, or can develop by itself. Attempts at restriction are interspersed with regular secretive binges and subsequent compensatory behaviours (self-induced vomiting, laxatives, diuretics, exercise or fasting). Bulimia often stays hidden because of its secretive nature, and also because weight tends to stay within normal ranges. While AN can present in children as young as 8 years of age, BN is more commonly seen in older adolescents from 14 years.
AN and BN and ‘atypical’ versions/EDNOS, are characterised by a core psychopathology where self-evaluation is based on weight and shape and its control. However, clinically significant eating disturbance can occur in young people without any underlying preoccupation with weight and shape. The research team at Great Ormond Street Hospital have identified a number of such eating difficulties in children. These include ‘food avoidance emotional disorder’, ‘restrictive eating’, ’functional dysphagia’ and ‘pervasive refusal syndrome’2.
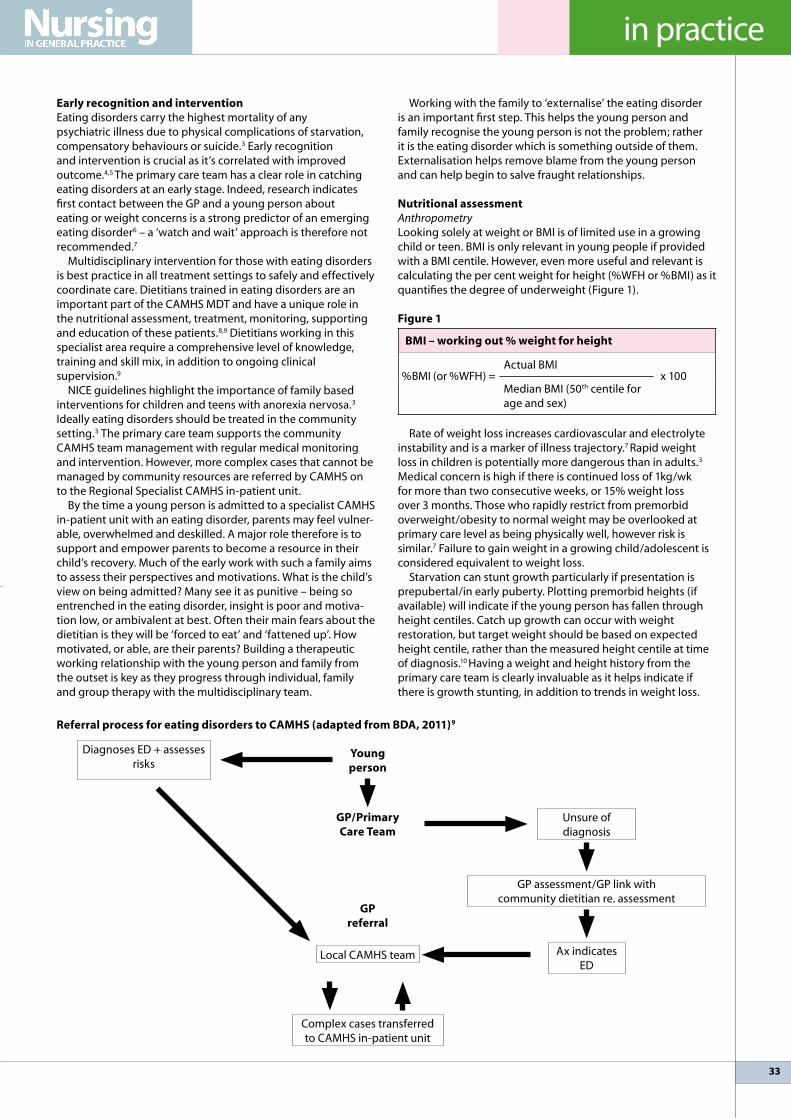
33
in practice
referral process for eating disorders to cAMhs (adapted from bdA, 2011)9
early recognition and interventionEating disorders carry the highest mortality of any psychiatric illness due to physical complications of starvation, compensatory behaviours or suicide.3 Early recognition and intervention is crucial as it’s correlated with improved outcome.4,5 The primary care team has a clear role in catching eating disorders at an early stage. Indeed, research indicates first contact between the GP and a young person about eating or weight concerns is a strong predictor of an emerging eating disorder6 – a ‘watch and wait’ approach is therefore not recommended.7
Multidisciplinary intervention for those with eating disorders is best practice in all treatment settings to safely and effectively coordinate care. Dietitians trained in eating disorders are an important part of the CAMHS MDT and have a unique role in the nutritional assessment, treatment, monitoring, supporting and education of these patients.8,9 Dietitians working in this specialist area require a comprehensive level of knowledge, training and skill mix, in addition to ongoing clinical supervision.9
NICE guidelines highlight the importance of family based interventions for children and teens with anorexia nervosa.3 Ideally eating disorders should be treated in the community setting.3 The primary care team supports the community CAMHS team management with regular medical monitoring and intervention. However, more complex cases that cannot be managed by community resources are referred by CAMHS on to the Regional Specialist CAMHS in-patient unit.
By the time a young person is admitted to a specialist CAMHS in-patient unit with an eating disorder, parents may feel vulner-able, overwhelmed and deskilled. A major role therefore is to support and empower parents to become a resource in their child’s recovery. Much of the early work with such a family aims to assess their perspectives and motivations. What is the child’s view on being admitted? Many see it as punitive – being so entrenched in the eating disorder, insight is poor and motiva-tion low, or ambivalent at best. Often their main fears about the dietitian is they will be ‘forced to eat’ and ‘fattened up’. How motivated, or able, are their parents? Building a therapeutic working relationship with the young person and family from the outset is key as they progress through individual, family and group therapy with the multidisciplinary team.
Working with the family to ‘externalise’ the eating disorder is an important first step. This helps the young person and family recognise the young person is not the problem; rather it is the eating disorder which is something outside of them. Externalisation helps remove blame from the young person and can help begin to salve fraught relationships.
Nutritional assessment Anthropometrylooking solely at weight or BMI is of limited use in a growing child or teen. BMI is only relevant in young people if provided with a BMI centile. However, even more useful and relevant is calculating the per cent weight for height (%WFH or %BMI) as it quantifies the degree of underweight (Figure 1).
figure 1
bMI – working out % weight for height
%BMI (or %WFH) = Actual BMI
x 100Median BMI (50th centile for age and sex)
Rate of weight loss increases cardiovascular and electrolyte instability and is a marker of illness trajectory.7 Rapid weight loss in children is potentially more dangerous than in adults.3
Medical concern is high if there is continued loss of 1kg/wk for more than two consecutive weeks, or 15% weight loss over 3 months. Those who rapidly restrict from premorbid overweight/obesity to normal weight may be overlooked at primary care level as being physically well, however risk is similar.7 Failure to gain weight in a growing child/adolescent is considered equivalent to weight loss.
Starvation can stunt growth particularly if presentation is prepubertal/in early puberty. Plotting premorbid heights (if available) will indicate if the young person has fallen through height centiles. Catch up growth can occur with weight restoration, but target weight should be based on expected height centile, rather than the measured height centile at time of diagnosis.10 Having a weight and height history from the primary care team is clearly invaluable as it helps indicate if there is growth stunting, in addition to trends in weight loss.
Diagnoses ED + assesses risks
young person
Unsure of diagnosis
gP/Primary care Team
gP referral
local CAMHS team
Complex cases transferred to CAMHS in-patient unit
Ax indicates ED
GP assessment/GP link with community dietitian re. assessment
34
in practice
BloodsThe nutritional assessment takes into account blood results (including FBC, U+Es, lFTs, TFTs, iron status, vitamin B12, inflammatory markers and coeliac screen).
Clinical assessmentClinical effects of malnutrition are noted, including endocrine status – whether there is primary or secondary amenorrhoea. Cardiovascular changes are often the earliest and most severe medical complications noted in ED – bradycardia, orthostatic heart rate and blood pressure changes may indicate need for admission to an acute paediatric ward for monitoring.
Compensatory behavioursAssessment of ‘compensatory behaviours’ such as self induced vomiting, compulsive or excessive exercise, laxatives or diuretics is key. Parents are a key source of information about their child when carrying out the nutritional assessment, with regards to compensatory behaviours, and daily dietary habits.
DietDiet assessment takes a detailed look at current daily intake for:• estimation of caloric intake versus requirements.• information around ‘food rules’ (e.g. having a set daily
calorie/fat gram limit or only allowing certain ‘safe’ foods). • maladaptive eating behaviours and rituals (e.g. excessive use
of condiments or cutting food into tiny pieces). It’s important to ascertain whether claims of being
vegetarian, having strong food ‘dislikes’ or ‘allergies’ existed premorbidly, or are part of the eating disorder. Working collaboratively with the family, it is useful to get a picture of how meals at home were prior to the eating disorder, and the family attitudes and beliefs around food, weight and dieting. Parents can also shed light on how the family’s eating habits may have changed as their child’s eating disorder took hold.
The nutritional assessment contributes to the medical risk assessment, including assessment of risk of re-feeding syndrome (Figure 2), and the decision as to whether a young person needs to be transferred to an acute paediatric ward for monitoring. In addition the assessment gleans broader information around family dynamics in the context of food and nutrition beliefs and attitudes, which is relevant to the ongoing family work.
figure 2
re-feeding syndrome
Re-feeding syndrome refers to the severe shifts in fluid and electrolytes that can occur with rapid re-feeding in a malnourished individual. Re-feeding syndrome can result in cardiovascular, neurological and haematological complications, and may be fatal. *Junior MARSIPAN (draft report)7 provides guidelines for management anorexia nervosa in <18yrs. They highlight those most at risk of re-feeding syndrome as young people with: • very low % weight for height• minimal or no nutritional intake for more than a few (3-4)
days• weight loss of over 15% in the last 3 months• abnormal electrolytes prior to re-feeding• ECG abnormalities• active co-morbidities (e.g. diabetes, infections)
Nutritional managementMeal planningDevelopment of the meal plan is collaborative; however, medical risk may determine how directive the re-feeding process needs to be and how much room there is for choice and negotiation.11 Meal plans should accommodate the usual family diet and the child’s premorbid likes and dislikes (sometimes it is necessary to agree to a limit to 3 dislikes). Initial meal plans start at a lower calorie level, for both physiological and psychological reasons. Psychologically, a person with a restrictive ED will be extremely agitated and distressed at the idea of having to switch to normal portions overnight. Physiological reasons for re-feeding slowly include avoiding ‘re-feeding syndrome’ if there is risk, but also to manage digestive discomfort. Malnutrition results in slowed gut peristalsis and gastric motility, resulting in early satiety, bloating and constipation, resulting in further restriction. There is no evidence to support use of prokinetic drugs.12 Rather, gradually building up to normal portions helps as digestive function normalises with ongoing re-feeding and weight restoration. Intake is gradually increased every 2-3 days until the person has built up to their required intake for the process of weight regain catch-up growth and development.
A multivitamin and mineral supplement is charted to supplement diet in the initial stages, and thiamine may be added if risk of re-feeding syndrome has been identified.
Recommended rate of weight regainNICE guidelines3 recommend a weight regain rate of 0.5kg per week in a community setting, and 0.5-1.0kg per week in an in-patient setting. Weight fluctuations in the first 7-10 days of re-feeding are due to fluid shifts rather than real weight changes. As weight is a proxy measurement of progress it is important to be aware of the methods the young person may employ to falsify their weight, such as water loading/hiding weights.
Meal coachingMeal coaching is an effective behavioural technique carried out by nursing staff on the unit to support a return to normal eating behaviour at meal times. Once the initial re-feeding period is underway and medical risk managed, work begins with parents/carers to give them with skills and confidence to take charge of their child’s re-feeding and weight restoration once at home.
Those who rapidly restrict from premorbid overweight/obesity to normal weight may be overlooked at primary care level as being physically well, however risk is similar.
35
in practice
Nutrition psycho-educationProviding information to parents around physiological, cognitive and emotional effects associated with starvation is important, to highlight the severe and serious nature of this illness and mobilise them as a resource in their child’s recovery.
Physical activityRecommended physical activity levels are based on medical, psychological and nutritional status. Total rest may be required during the initial stages of re-feeding, with physical activity built up gradually to normal healthy levels as appropriate.
Setting a target healthy weight rangeNutritional treatment aims focus on supporting completion of puberty and growth. While there is lack of consensus regarding the setting of target weight, 95 – 105% weight for height (%BMI) is a good starting point. 95% approximates the weight needed to return to normal growth, endocrine status (and menstruation) and bone health for most young people. However, the target healthy weight range becomes a moving goalpost as height increases over time. Weight targets and energy requirements should therefore be readjusted every 3 to 6 months to account for growth.13 This is challenging for the young person as they try to come to terms with a new physical state with continued growth, unlike adult cases who are returning to their premorbid healthy state.
ongoing MdT treatmentOnce medical risk has resolved, weight restoration is progressing well, and the family ready, the next phase of treatment begins, where parents are supported in helping their child take back more control of their eating. At this point, the young person is cognitively more open and able for individual psychological work and family therapy. This phase often rolls out as the young person goes back to home and to the care of their community CAMHS team. Dietitian input at this point can focus on nutrition psycho-education to tackle core maladaptive beliefs and attitudes about food, weight, self-concept and control. The final phase of this family approach tends to begin when the young person is able to keep their weight above approx. 95% of what it should be for their height and therapy moves on to focus on the development of a healthy adolescent identity. Dietetic input at this stage may include supporting
the young person towards eating intuitively, away from the scaffolding of meal plan. (Note – the team approach used will vary as appropriate to the young person and their family).
summaryEating disorders are complex conditions and can be fatal. Age of onset is generally during adolescence. The primary care team has a clear role in identifying eating disorders at an early stage – early recognition and intervention is associated with improved outcome. Multidisciplinary management of eating disorders is essential. Information from the primary care team such as premorbid weights and heights, medical history, history of onset of weight and shape concerns and morbid trends in medical parameters is invaluable for subsequent nutritional assessment and management of these children in a CAMHS setting.
helpful resources for working with ed
1. Practical, evidence based resources for health professionals working with eating disorders available to download from the Institute of Psychiatry, Kings College london website (www.eatingresearch.com), including the following (not an exhaustive list): • A Guide to the Medical Risk Assessment for Eating
Disorders • Restoring regular eating• The SCOFF questionnaire• Maudsley Body Mass Index Table• Maudsley Nutritional Health Over Time Chart• A GP’s Guide to Eating Disorders • Medical complications of anorexia nervosa
2. MARSIPAN: Management of Really Sick Patients with Anorexia Nervosa14
3. Junior MARSIPAN: Management of Really Sick Patients under 18 with Anorexia Nervosa – draft report7
references1. Nicholls D, Hudson l and Mahomed F. Managing Anorexia Nervosa. Arch Dis
Child. 2011; 96(10): 977-982.2. Nicholls D, Chater R and lask B. Children into DSM don’t go: a comparison
of classification systems for eating disorders in childhood and early adolescence. Int J Eat Disord. 2000; 28 (3): 317-324.
3. National Institute of Clinical Excellence. Eating Disorders: full national guidelines; 2004. www.nice.org.uk
4. Van Son GE, Van Hoeken D, Van Furth EF, Donker GA, Hoek HW. Course and outcome of eating disorders in primary care based cohort. Int J Eat Disord. 2010; 43: 130-138.
5. American Academy of Pediatrics, Committeee on Adolescence. Identifying and treating eating disorders. Pediatrics. 2003; 111: 204-211.
6. lask B, Bryant-Waugh R, Wright F, Campbell M, Willoughby K and Waller G. Family physician consultation patterns indicate high risk for early-onset anorexia nervosa. Int J Eat Disord. 2005; 38(3):269-272.
7. Nicholls D. Junior MARSIPAN: Management of Really Sick Patients under 18 with Anorexia Nervosa. Royal College of Psychiatrists. DRAFT report. 2010 (http://sites.google.com/site/marsipannini/newsandupdates/consultationperiodbeginsforjuniormarsipanreport
8. Rowel D, Nolan G, O’Donnell M. Eating Disorders – Best Practice Guidelines for Dietitians. HSE West; 2008.
9. British Dietetic Association. Dietitians working with Patients with Eating Disorders – Position Statement. Produced by the BDA Mental Health Group; 2011.
10. Modan-Moses D, Yaroslavsky A, Novikov I, Segev S, Toledano A, Miterany E and Stein D. Stunting of Growth as a Major Feature of Anorexia Nervosa in Male Adolescents. Pediatrics. 2003; 111: 270.
11. Hart M. Nutrition and Refeeding. In: lask B, Bryant-Waugh R, Editors. Eating Disorders in Childhood and Adolescence. 3rd ed. UK: Routledge; 2007.
12. Pinhas l, Steinegger CM and Katzman DK. Clinical Assessment and Physical Complications. In: lask B, Bryant-Waugh R, Editors. Eating Disorders in Childhood and Adolescence. 3rd ed. UK: Routledge; 2007.
13. American Dietetic Association. Nutrition Intervention in the Treatment of Eating Disorders. J Am Diet Assoc. 2011; 111 (8): 1236 – 1241.
14. Robinson P. MARSIPAN: Management of Really Sick Patients with Anorexia Nervosa. Royal College of Psychiatrists. College Report; 2010.
building a therapeutic working relationship with the young person and family from the outset is key as they progress through individual, family and group therapy with the multidisciplinary team
36
abstracts
Clinicopathological predictors of systemic progression and prostate cancer mortality in patients with a positive surgical margin at radical prostatectomy
boorjian sA, Tollefson Mk,
rangel lJ et al. Prostate Cancer
Prostatic Dis 2012; 15 (1): 56 – 62.
A recent study carried out by a group based in the Department of Urology at the Mayo Clinic, Minnesota, US, has found that tumour variables are the primary determinants of cancer death in men with prostate cancer.
Although a positive surgical margin (PSM) at radical prostatectomy (RRP) has been consistently linked to an increased risk of biochemical recurrence, the impact of margin status on patient survival continues to be debated. This study evaluated long-term outcomes of patients with a PSM at RRP and determined predictors of systemic progression (SP) and mortality in these men.
The group reviewed their institutional registry of 16,749 patients who underwent RRP between 1990 and 2008 to identify 2,895 patients with a PSM. Median follow-up was 10.6 years. Postoperative survival was estimated using the Kaplan–Meier method. Cox proportional hazard regression models were used to analyse clinic-pathological variables associated with SP and death from prostate cancer.
A 15-year SP-free and cancer-specific survival was 90 and 93 per cent, respectively. On multivari-ate analysis, higher tumour volume, increased pathological Gleason score and advanced pathological tumour stage were associated with significantly increased risks of SP and death from prostate cancer, whereas number and location of PSM did not predict mortality.
From these results study authors concluded that the risks of SP and prostate cancer death in patients with a PSM remain low on long-term follow-up. Tumour variables are the primary determinants of can-cer death. They added that these results should be considered when evaluating patients with a PSM for adjuvant therapy.
Usefulness of electromyography of the cavernous corpora (CC EMG) in the diagnosis of arterial erectile dysfunction
virseda-chamorro M, lopez-garcia-
Moreno AM, salinas-casado J
et al. International Journal
of Impotence Research 2012;
advance online publication, 3 May 2012; doi:10.1038/
ijir.2012.10.
A Spanish study has recently confirmed that due to high specificity the use of electromyography of the corpora cavernosa (CC EMG) as a diagnostic screening tool is very effective in patients with erectile dysfunction.
EMG of the corporea cavernosa is able to record the activity of the erectile tissue during erection, and has thus been used as a diagnostic technique in patients with erectile dysfunction (ED). This study examined the usefulness of the technique in the diagnosis of ED.
A cross sectional study was carried out of 35 males with a men age of 48.5 years (S.D = 11.34), referred to a Spanish centre with ED for over one year. The patients underwent CC EMG and a penile Doppler ultrasound investigation followed by 20µg of prostaglandin E1 (PGE1). The patients were divided into three groups according to their response to the intracavermous injection of PGE1: Group 1 (adequate erection and reduction/suppression of EMG activity); Group 2 (insufficient erection and per-sistence of EMG activity) and Group 3 (insufficient erection and reduction/suppression of EMG activity).
Patient classification according to response to the intracavernous injection of PGE1 was as follows: Group 1: six patients (17%), Group 2: 18 patients (51%), and Group 3: 11 patients (31%). Patients were diagnosed with arterial insufficiency according to Doppler ultrasound (systolic arterial peak velocity <30mm s(-1) in both arteries) were significantly older thatn those without damage (54.5 versus 41.8 years, respectively; S.D = 11.12). The patients in Group 3 showed a significantly lower maximum systolic velocity in both arteries that the subjects in Group 2. likewise, a statistically significant relationship was observed between the diagnoses of arterial insufficiency and patient classification in Group 3. The confirmation of insufficient erection associated with reduction/suppression of EMG activity showed a sensitivity of 66.7 per cent (confidence interval between 50 and 84%) and a specificity of 92.9 Per cent (confidence interval of 84 and 100%) in the diagnosis of arterial ED.
The study authors concluded that owing to the high specificity of CC EMG response to the injection of PGE1, this test is considered useful as a screening technique in the diagnosis of arterial ED.
FoCUs on: MEn’s HEALTH
Think Choice
CIALIS* (TADALAFIL) REPUBLIC OF IRELAND ABBREVIATED PRESCRIBING INFORMATION Presentation Tablets 2.5mg, 5mg, 10mg, or 20mg of tadalafil. Also contains lactose. Uses Treatment of erectile dysfunction in adult males. Dosage and Administration Adult men: The recommended dose is 10mg orally, taken at least 30 minutes prior to sexual activity. In those patients in whom tadalafil 10mg does not produce an adequate effect, 20mg might be tried. Maximum dosing frequency, once per day. 10mg or 20mg tadalafil is not recommended for continuous daily use. In patients who anticipate a frequent use of Cialis (ie, at least twice weekly), a once daily regimen with the lowest doses of Cialis might be considered. The recommended dose is 5mg taken once a day at approximately the same time of day. The dose may be decreased to 2.5mg once a day based on individual tolerability. The appropriateness of continued use of the daily regimen should be reassessed periodically. Elderly: Dosage adjustment not required. Impaired renal or hepatic function: In patients with severe renal impairment the maximum recommended dose is 10mg. Once a day dosing of Cialis is not recommended in patients with severe renal impairment. In men with hepatic impairment the recommended dose is 10mg. There are no available data about the administration of doses higher than 10mg of tadalafil to patients with hepatic impairment. There is limited clinical data on the safety of Cialis in patients with severe hepatic impairment; if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Once a day dosing has not been evaluated in patients with hepatic impairment; therefore, if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Diabetes: Dosage adjustment not required. Use in children and adolescents: Cialis should not be used in individuals below 18 years of age. Not indicated for use by women. In clinical trials, Cialis demonstrated improvement in patients’ erectile function and the ability to have successful sexual intercourse up to 36 hours following dosing. Contra-indications Known hypersensitivity to any ingredient. Patients using any form of organic nitrates. In men with cardiac disease for whom sexual activity is inadvisable. Physicians should consider the potential cardiac risk of sexual activity in patients with pre-existing cardiovascular disease. Patients with myocardial infarction within the last 90 days, patients with unstable angina or angina occurring during sexual intercourse, patients with New York Heart Association class 2 or greater heart failure in the last 6 months, patients with uncontrolled arrhythmias, hypotension (<90/50mmHg), or uncontrolled hypertension, patients with a stroke within the last 6 months. Cialis is contra-indicated in patients who have loss of vision in one eye because of non-arteritic anterior ischaemic optic neuropathy (NAION), regardless of whether this episode was in connection or not with previous PDE5 inhibitor exposure. Warnings and Special Precautions Prior to any treatment for erectile dysfunction, physicians should consider the cardiovascular status of their patients, since there is a degree of cardiac risk associated with sexual activity. Tadalafil has vasodilator properties, resulting in mild and transient decreases in blood pressure. It augments the hypotensive effect of nitrates. Tadalafil (2.5mg and 5mg): In patients receiving concomitant antihypertensive medicines, tadalafil may induce a blood pressure decrease. When initiating daily treatment with tadalafil, appropriate clinical considerations should be given to a possible dose adjustment of the antihypertensive therapy. Serious cardiovascular events were reported either post-marketing and/or in clinical trials. Although most of the patients in whom these events have been observed had pre-existing cardiovascular risk factors, it is not possible to determine whether these events are related directly to these risk factors, to Cialis, to sexual activity, or to a combination of these or other factors. Visual defects and cases of NAION have been reported in connection with the intake of Cialis and other PDE5 inhibitors. In case of sudden visual defect, patients should be advised to stop taking Cialis and consult a physician immediately. Due to increased tadalafil exposure (AUC), limited clinical experience, and the lack of ability to influence clearance by dialysis, once a day dosing of Cialis is not recommended in patients with severe renal impairment. There is limited clinical data on the safety of single-dose administration of tadalafil in patients with severe hepatic insufficiency (Child-Pugh class C); if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Use with caution in patients who have conditions that might predispose them to priapism, or in patients with anatomical deformation of the penis. Patients who experience erections lasting 4 hours or more should be instructed to seek medical assistance. If priapism is not treated immediately, penile tissue damage and permanent loss of potency may result. It is not known if Cialis is effective in patients who have undergone pelvic surgery or radical non-nerve-sparing prostatectomy. Cialis should not be administered to patients with hereditary problems of galactose intolerance, the Lapp lactase deficiency, or glucose-galactose malabsorption. In patients who are taking alpha1-blockers, concomitant administration of Cialis may lead to symptomatic hypotension in some patients. The combination of tadalafil and doxazosin is not recommended. Caution should be exercised when prescribing Cialis to patients using potent CYP3A4 inhibitors (ritonavir, saquinavir, ketoconazole, itraconazole, and erythromycin) as increased tadalafil exposure (AUC) has been observed if the drugs are combined. The safety and efficacy of combinations of tadalafil and other PDE5 inhibitors or other treatments for erectile dysfunction have not been studied. Patients should be informed not to take Cialis with such combinations. Pregnancy and Lactation Not indicated for use by women. There are limited data from the use of tadalafil in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition, or postnatal development. As a precautionary measure, it is preferable to avoid the use of Cialis during pregnancy. Available pharmacodynamic/toxicological data in animals have shown excretion of tadalafil in milk. A risk to the suckling child cannot be excluded. Cialis should not be used during breast-feeding. Driving, etc No studies on the effect on the ability to drive and use machines have been performed. Although the frequency of reports of dizziness in placebo and tadalafil arms in clinical trials was similar, patients should be aware of how they react to Cialis before driving or operating machinery. Undesirable Effects Very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), and not known (events not reported in registration trials cannot be estimated from post-marketing spontaneous reports). Very common: Headache. Common: Dizziness, flushing, dyspepsia, nasal congestion, back pain, myalgia. Uncommon: Hypersensitivity reactions, blurred vision, sensations described as eye pain, tachycardia, palpitations, hypotension (more commonly reported when tadalafil is given to patients who are already taking antihypertensive agents), hypertension, abdominal pain, gastro-oesophageal reflux, rash, hyperhidrosis (sweating), chest pain(1). Rare: Stroke(1) (including haemorrhagic events), syncope, transient ischaemic attacks(1), migraine(3), visual field defect, swelling of eyelids, conjunctival hyperaemia, myocardial infarction, urticaria, Stevens-Johnson syndrome(3), exfoliative dermatitis(3), prolonged erections, priapism(3), facial oedema(3), seizures, transient amnesia, NAION(3), retinal vascular occlusion(3), sudden hearing loss(2), unstable angina pectoris(3), ventricular arrhythmia(3), epistaxis, sudden cardiac death(1, 3). (1)Most of the patients in whom these events have been reported had pre-existing cardiovascular risk factors. (2)Sudden decrease or loss of hearing has been reported in a small number of post-marketing and clinical trial cases with the use of all PDE5 inhibitors, including tadalafil. (3)Post-marketing surveillance reported adverse reactions not observed in placebo-controlled clinical trials. Adverse reactions reported with tadalafil were transient, and generally mild or moderate. Adverse reaction data are limited in patients >75 years. A slightly higher incidence of ECG abnormalities, primarily sinus bradycardia, has been reported in patients treated with tadalafil once a day as compared with placebo. Most of these ECG abnormalities were not associated with adverse reactions. For full details of these and other side-effects, please see the Summary of Product Characteristics, which is available at http://www.medicines.ie/. Legal Category POM Marketing Authorisation Numbers and Holder EU/1/02/237/001 EU/1/02/237/002 EU/1/02/237/003 EU/1/02/237/004 EU/1/02/237/005 EU/1/02/237/006 EU/1/02/237/007 EU/1/02/237/008. Eli Lilly Nederland BV, Grootslag 1-5 3991, RA Houten, The Netherlands. Date of Preparation or Last Review March 2011. Full Prescribing Information is Available From Eli Lilly and Company Limited Lilly House, Priestley Road Basingstoke, Hampshire, RG24 9NL. Telephone: Basingstoke (01256) 315 000 E-mail: [email protected] or Eli Lilly and Company (Ireland) Limited Hyde House, 65 Adelaide Road, Dublin 2, Republic of Ireland. Telephone: Dublin (01) 661 4377. E-mail: [email protected]. *CIALIS (tadalafil) is a trademark of Eli Lilly and Company. Reference 1. Cialis Summary of Product Characteristics. Eli Lilly and Company Limited.
Date of Preparation: April 2012. IECLS00208
can offer couples the freedom to choose whenthe time is right for them1
38
product news
Torvacol (Atorvastatin) 10mg, 20mg, 40mg and 80mg Clonmel Healthcarehas announced the launch of Torvacol (Atorvastatin) 10mg, 20mg, 40mg and 80mg Film-coated tablets.
Torvacol (Atorvastatin) 10mg, 20mg, 40mg and 80mg are indicated for:• Adjunct to diet in primary hypercholesterolaemia, including
familial hypercholesterolaemia or combined hyperlipidaemia • Adjunct to other lipid-lowering treatments in adults with
homozygous, familial hypercholesterolaemia, or if such treatments are unavailable
• Prevents cardiovascular events in adult patients at high risk, as an adjunct to correction of other risk factors 1
Torvacol Film-coated tablets are available in a 28 pack. Full prescribing information for Torvacol is available on
request or go to www.clonmel-health.ie . This Product is subject to medical prescription. Torvacol is GMS reimbursable as of 7th May 2012.
Please contact Clonmel Healthcare on 01-6204000 if you require any additional information on Torvacol.
dermatological skincare for mature skin with linactyl, ProXylane and both UVB and UVA protection. Substiane [+] UV has proven results for firmer, more toned and radiant skin.
Substiane [+] UV is targeted at women aged 55 years+ including those with sensitive skin.
These women, with mature skin report the following skin concerns: loss of firmness, wrinkles, brown spots and dryness.
Substiane contains ProXylane 5% which replenishes the skin’s support cells environment, while linactyl 4% helps
regain substance and density. Substiane’s SPF 15 & UVA PPD 9 helps
protect from daily harmful elements.In 2011 la Roche-Posay discovered that
skin contains two distinct fibroblasts: dormant fibroblasts – found deep within the epidermis and active fibroblasts – found in the upper dermis.
The dermis of young skin is filled with a great number of fibroblasts which produce more synthesis molecules than degradation molecules, ensuring that collagen fibres and proteins keep regenerating.
In mature skin, fibroblasts are less plentiful and less active. They produce more degradation molecules than synthesis molecules causing collagen fibres to break and the structure of the skin to sag.
To effectively take action on mature skin ageing, la Roche Posay developed ProXylane. an infinitely small and naturally derived molecule capable of acting at the very heart of living tissues. It is a sugar-protein hybrid made from xylose, which stimulates the production of molecules responsible for defending the skin against water loss. By penetrating the extra-cellular matrix that supports skin structure, ProXylane can restore and replenish skin’s overall health and suppleness.
Substiance also contains linactyl, an exclusive anti-ageing reversive active ingredient which reactivates the skin support cells to reverse the dynamics of ageing. It inhibits the production of proteins responsible for mature skin degradation.
Skin regains intense comfort, is firmer, more toned and radiant. Day after day, features are lifted, skin’s facial support structure is reinforced and the face is re-profiled.
Candist (Candesartan) 4mg, 8mg and 16mgClonmel Healthcare has announced the launch of Candist (Can-desartan) 4mg, 8mg and 16mg tablets.
Candist (Candesartan) 4mg, 8mg and 16mg are indicated for:• Treatment of essential hypertension in adults• Treatment of adult patients with heart failure and impaired left
ventricular systolic function (left ventricular ejection fraction ≤ 40%) as add-on therapy to Angiotensin Converting Enzyme (ACE) inhibitors or when ACE inhibitors are not tolerated. Candist tablets are available in a 28 pack. Full prescribing information for Candist is available on request
or go to www.clonmel-health.ie. This product is subject to medi-cal prescription. Candist is GMS reimbursable from 1st May 2012.
Also available is Candist Plus (Candesartan cilexetil/Hydrochlo-rothiazide) 16mg/12.5mg tablets 28 pack. Candist Plus is GMS reimbursable from 1st May 2012.
Candist and Candist Plus are the Clonmel brands of Candesar-tan Cilexetil and Candesartan Cilexetil/Hydrochlorothiazide.
Please contact Clonmel Healthcare on 01-6204000 if you re-quire any additional information on Candist and Candist Plus.
New Substiane [+] UV – anti-ageing care for mature skin Developed by sensitive skin specialists la Roche-Posay, Substiane [+] UV is the first

39
product news
A.Menarini Pharmaceuticals Ireland ltd. and Daiichi-Sankyo Ireland ltd have announce dthe launch of Konverge Plus, the first triple combination anti-hypertensive to contain the angiotensin II receptor antagonist, olmesartan.
Konverge Plus, is indicated for the treatment of essential hypertension, as a substitution therapy in adult patients whose blood pressure is adequately controlled on the combination of olmesartan medoxomil, amlodipine and hydrochlorothiazide, taken as a dual-component (olmesartan medoxomil and amlodipine or olmesartan medoxomil and hydrochlorothiazide) and a single-component formulation (hydrochlorothiazide or amlodipine).
Speaking at a recent meeting on hypertension at the Royal College of Physicians, Prof Eoin O’Brien, Professor of Molecular Pharmacology at the Conway Institute of Biomolecular and Biomedical Research at UCD, explained:
“Apart from accurate ambulatory blood pressure measurement, we also need therapeutic assistance to help us control blood pressure. Faced with the need to not only lower mean blood pressure but also to reduce blood pressure variability and the fact that the majority of patients with hypertension will require two or more dugs to obtain blood pressure control, we can now resort to what I have termed the ‘flexipill’.
“The flexibility of Konverge Plus means that we only have to give the patient one tablet and yet we have the ability to use the many permutations of this ‘flexipill’, which allows us to use lower doses of three drugs so as to minimise side-effects and improve compliance,” he concluded.
Patient compliance to BP medication is an issue in overall blood pressure management, as less than half of patients on treatment has their blood pressure controlled. However, through the use of a combination therapy, such as Konverge Plus, compliance to anti-hypertensive therapy increases as pill burden decreases. Research has also shown that compliance is associated with more effective blood pressure control.
There are five presentations of Konverge Plus, all of which are currently obtainable on the GMS.
• Konverge Plus 20mg/5mg/12.5mg film-coated tablets • Konverge Plus 40 mg/5 mg/12.5 mg film-coated tablets • Konverge Plus 40 mg/10 mg/12.5 mg film-coated tablets • Konverge Plus 40mg/5mg/25mg film-coated tablets• Konverge Plus 40mg/10mg/25mg film-coated tablets
For more information on Konverge Plus, please contact A.Menarini Pharmaceuticals Ireland Ltd at email: [email protected] or call (01) 2846744.
Servier has announced that the company’s heart rate lowering agent, Procoralan (ivabradine), the first selective If channel inhibitor, has received European Approval for the treatment of patients with chronic heart failure.
The decision to authorise this new indication for Procoralan followed the review of data from the SHIfT trial, the largest-ever morbi-mortality study of treatments for chronic heart failure. It demonstrated that Procoralan significantly reduced the risk of death (-26%) and hospitalisation for heart failure (-26%), and improved the quality of life of people living with the disease. In patients with a heart rate of 75 beats per minute (bpm), or above, for whom Procoralan is now indicated the reduction in all-cause mortality was highly significant (-17%).
In brief, SHIfT (Systolic Heart failure treatment with the If inhibitor ivabradine Trial) was a randomised, double-blind placebo controlled study involving 6,505 people in 37 countries, which set out to evaluate whether the addition of Procoralan, to optimal guideline-based treatment, improves cardiovascular outcomes in patients with moderate to severe chronic heart failure, reduced left ventricular ejection fraction and heart rate of 70 bpm or above.
SHIfT reported that Procoralan reduced the risk of hospitalisation due to worsening heart failure by over a quarter (26%, p<0.0001) and the likelihood of death from heart failure by the same amount (26%, p=0.014). Despite the
fact that patients were already well treated, in line with current best practice, these benefits were seen in just three months of treatment with Procoralan.
SHIFT also reported that the higher the heart rate the higher the risk and therefore the greater the benefit of heart rate reduction. Indeed these benefits are impressive in patients with a heart rate >75 bpm; Procoralan significantly reduced the risk of cardiovascular death by 17% (p=0.0166) and all cause death by 17 %(p=0.0109).
Furthermore, the results of a SHIfT sub-study (of 1,944 patients) revealed for the first time a direct link between heart rate reduction with Procoralan and an improvement in health-related quality of life (HQol), as measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ). By one year, the study showed that patients with lower KCCQ scores (equating to a lower HQol) were at an increased risk of a cardiovascular event. Procoralan was shown to improve HQol in heart failure patients. Improvements in clinical summary score and overall summary score were greater in the patients with the greatest reductions in heart rate and this was more marked in the Procoralan group. Practically speaking, this means that patients with heart failure who received Procoralan were able to participate in a greater number of everyday activities, considerably changing their day to day life, which has been clearly altered by the disease.
Procoralan receives European approval for use in heart failure
New triple hypertensive therapy available – Konverge

40
product news
Zoely, an innovative oral contraceptive pill now available in Ireland
MSD recently announced that Zoely (nomegestrol acetate/17-beta estradiol) is now available in Ireland for the prevention of pregnancy.
“Zoely is the latest addition to the MSD portfolio of contracep-tive and fertility products which are manufactured at MSD Swords for worldwide distribution. The launch further reinforces MSD’s longstanding commitment to providing women with greater choice in contraceptive options,” added Tony Pusic, Plant Manager at MSD Swords, North County Dublin.
Zoely, a Guaranteed Irish product is a combined oral contracep-tive pill containing an innovative monophasic combination of two hormones; nomegestrol acetate, a highly selective progesterone-derived progestin, with a 46 hour half life, and 17-beta estradiol, an oestrogen that is structurally identical to the one naturally present in a woman’s body.
It was shown to be more than 99% effective in preventing preg-nancy when used as directed and results in short, light withdrawal bleeds. The median number of withdrawal bleeding and spotting days with Zoely is 3 to 4 days, while the median number of bleeding days is 2.² This innovative combination pill will be made available to women in a 24 day active and 4 day placebo dosing regimen. ¹
Welcoming the launch of Zoely, Dr Mary O’Flynn, General Practi-tioner, Mallow, Co. Cork, with specialist interest in female health said, “Millions of women worldwide have benefited from using the pill since its introduction just over 50 years ago.
Although we have seen continual advancements in the pill since then, the introduction of Zoely, with its innovative combination of hormones, this is the first time we’ve had a contraceptive pill with an oestrogen identical to the one produced in a woman’s own body making this new contraceptive pill an attractive option for Irish women.”
In the clinical trial performed in the European Union, 1,587 women, 1,315 of whom were aged 18-35, were treated with Zoely for up to 13 consecutive cycles. ² The Pearl Index for women aged 18-35, including method and user failure, was calculated as 0.38 (upper limit 95% confidence interval 0.97). The Pearl Index calculation was based on pregnancies that occurred after the onset of treatment and within two days after the last pill intake.
Zelboraf for the treatment of people with deadly form of skin cancer
Roche has announced that the European Commission has approved Zelboraf (vemurafenib) as a monotherapy for the treatment of adult patients with BRAF V600 mutation-positive unresectable or metastatic melanoma, a very aggressive form of skin cancer. Zelboraf is designed to target and inhibit mutated forms of the BRAF protein found in about half of all cases of melanoma. “This approval is important news for people with BRAF mutation-positive metastatic melanoma as Zelboraf significantly improves patient survival and exemplifies the benefits that Roche’s personalized approach to medicine can provide for patients, physicians and society,” said Dr. John Bolodeoku, Interim Medical Director, Roche Products (Ireland) ltd.
Welcoming the announcement, the leading oncologist Dr Paul Donnellan, Consultant Medical Oncologist at University College Hospital Galway said: “I am delighted to hear that Vemurafenib has received its European licence and look forward to its availability in Ireland. Vemurafenib is the first targeted therapy to show efficacy in the treatments of Metastatic malignant melanoma with response rates that are truly phenomenal (53%) and a definite improvement in otherwise-dismal survival. As a bonus, treatment is oral and without the usual chemotherapy or immunotherapy-type side effects. This treatment will be a major boon to the 40% or so of my patients with Metastatic malignant melanoma whose tumours are BRAF mutated. We look forward to participating in the on-going global safety studies which will provide access to Zelboraf for patients with BRAF V600 mutation-positive metastatic melanoma”.
In pivotal clinical trials, Zelboraf is proven to improve patient survival in both previously untreated and previously treated people with unresectable or metastatic melanoma who tested positive for BRAF V600 mutations using the Roche cobas 4800 BRAF V600 Mutation Test.• In the pre-specified interim analysis of the phase III
trial (BRIM3), the risk of death was reduced by 63 per cent (median follow-up of 3.8 months for patients in the vemurafenib group and 2.3 months for those in the dacarbazine group) for people who received Zelboraf compared to those who received standard first-line treatment (hazard ratio [HR]=0.37, p<0.0001).1
• In a post-hoc analysis of BRIM3 data with a longer follow up compared to previous analyses, including cross-over of patients from the placebo to the active treatment arm, Zelboraf significantly improved survival over standard first-line treatment by providing a median overall survival (OS) of 13.2 months compared to 9.6 months for chemotherapy (hazard ratio [HR]=0.62)
Naraverg – name changeTeva Pharmaceuticals Ireland would like to announce the following name change: Naramerg (naratriptan) Film Coated Tabs 2.5mg has changed to Naraverg™ (naratriptan) Film Coated Tabs 2.5mg. Packs sizes are available in 6’s and 12.
Seropia (Quetiapine) 25mg, 100mg, 200mg and 300mg
Clonmel Healthcare has announced the launch of Seropia (Que-tiapine) 25mg, 100mg, 200mg and 300mg film-coated tablets.
Seropia (Quetiapine) 25mg, 100mg, 200mg and 300mg are indicated for:• Treatment of schizophrenia• Treatment of moderate to severe manic episodes• Treatment of major depressive episodes in bipolar disorder
Seropia Film-coated tablets are available in a 60 pack. Full prescribing information for Seropia is available on request
or go to www.clonmel-health.ie . This Product is subject to medi-cal prescription. Seropia is GMS reimbursable from 1st April 2012.
Please contact Clonmel Healthcare on 01-6204000 if you require any additional information on Seropia.
Seropia is the Clonmel brand of Quetiapine.
41
crossword
Name:
Address:
Email:
Congratulations to the winner of last month’s crossword, Colette Gibbons, Killadoon, louisurgh, Co Mayo.
Please send your answers to the Editor, Nursing in General Practice, GreenCross Publishing, 7 Adelaide Court, Adeliade Road, Dublin 2. Closing date for entries: 1 July 2012.Winner will receive v50. Please note: the winners’ cheques will be sent out within 45 days.
Caltrate is a trademark. PA 172/38/1. Full prescribing information available from Pfizer Consumer Healthcare ltd., 9 Riverwalk, National Digital Park, Citywest Business Campus, Dublin 24 or from www.medicines.ie
ANswers To lAsT MoNTh’s crosswordAcross: 1 Scurvy, 4 Ufos, 8 Pea, 9 Rostrum, 10 Ribs, 11 Uncle, 14 In may, 16 lice, 18 Gastric, 20 lab, 21 Rope, 22 Impale. down: 1 Sept, 2 Uranium, 3 Virus, 5 Fir, 6 Summer, 7 Esau, 12 Cochlea, 13 Finger, 15 Yard, 16 locum, 17 Able, 19 Sap.
Across1 Uncontrolled blaze is quite big (7)4 Moral difference concerning back teeth (5)7 Ancient discovery by confused char in CIA (7)8 Behave stealthily for public relations with a night
bird! (5)9 What a heart might do if one were to steal up
unexpectedly (7)10 Change of efts is compensating (6)12 Disregard nothing in a troublesome reign (6)15 This may qualify one to get ten with a broken tile (7)17 Three. Odd that it’s used by anaesthetists as a
number! (5)19 It alone explodes into a sense of euphoria (7)20 Give way to triangular road-sign (5)21 Bloodsuckers used by medics of old (7)
dowN1 Claps confusedly on ones head (5)2 It is read with feeling! (7)3 Get away in a broken-down Espace (6)4 Decoration in domed alcove (5)5 lob a mug awkwardly to produce back pain (7)6 Re-live around the east to mitigate dicomfort (7)10 Ties boy in a knot for being overweight (7)11 Would ague fit this description of weariness? (7)13 Weapon requiring a safety pin! (7)14 Uncover a broken lever (6)16 ‘lukewarm’ in Israelite pidgin English (5)18 Jewellery going around Saturn? (5)
1 2 3 4 5 6
7
8 9
10 11 12 13
14
15 16 17 18
19
2120

Calcium and/or vitamin D deficiency in the elderly can lead to lossof muscle tone and increased risk of falls and osteoporotic fractures.1-5
Calcichew-D3 Forte is indicated for the treatment and prevention of calcium and vitamin D deficiency.6
CALCICHEW-D3 FORTE CHEWABLE TABLETS PRESCRIBINGINFORMATION(Please refer to full Summary of Product Characteristics whenprescribing)Presentation: Chewable tablet containing 1250mg calcium carbonate(equivalent to 500mg of elemental calcium) plus 400IU colecalciferol(equivalent to 10 micrograms vitamin D3). Uses: Prevention andtreatment of vitamin D/calcium deficiency. Supplementation of vitaminD and calcium as an adjunct to specific therapy for osteoporosis, inpregnancy, in established vitamin D dependent osteomalacia and inother situations requiring therapeutic supplementation of malnutrition.Dosage and administration: Oral (suck or chew). Adults and elderly:Two tablets daily. Children: Not intended for use in children. Hepaticimpairment: No dose adjustment required. Renal impairment: Shouldnot be used in patients with severe renal impairment.Contraindications: Diseases and/or conditions resulting inhypercalcaemia and/or hypercalciuria, severe renal impairment, renalstones, hypervitaminosis D, hypersensitivity to ingredient(s)Precautions: Monitor serum calcium and creatinine levels,particularly in patients on cardiac glycosides or diuretics and inpatients with high tendency to calculus formation. Use with caution inpatients with impaired renal function. Take into account risk of softtissue calcification. Avoid in patients with phenylketonuria or sugar
intolerance. Prescribe with caution in patients with sarcoidosis. Usewith caution in immobilised patients. Additional doses of calcium orvitamin D should only be taken under close medical supervision.Interactions: Tetracyclines (take 2 hours before, or 4 to 6 hours afterCalcichew-D3 Forte), bisphosphonates or sodium fluoride (take 3hours before Calcichew-D3 Forte), Quinolone antibiotics (take twohours before or after), levothyroxine (take four hours before or after),thiazide diuretics, corticosteroids, cardiac glycosides, ion exchangeresins (cholestyramine), laxatives (paraffin oil). Calcichew-D3 Forteshould not be taken within 2 hours of eating foods high in oxalic acid(e.g. spinach and rhubarb) or phytic acid (e.g. whole cereals). Sideeffects: Hypercalcaemia, hypercalciuria, constipation, dyspepsia,flatulence, nausea, abdominal pain, diarrhoea, pruritus, rash, urticaria.Very rarely (usually only seen on overdose) milk-alkali syndrome. Usein pregnancy and lactation: Can be used in case of calcium andvitamin D deficiency. Daily intake in pregnancy should not exceed1500mg calcium and 600IU colecalciferol (15 micrograms vitamin D3).Avoid overdose as permanent hypercalcaemia affects developingfoetus. Calcium and vitamin D3 pass into breast milk so consider thiswhen giving additional vitamin D to the child. Pharmaceuticalprecautions: Do not store above 30°C. Keep container tightly closedto protect from moisture. Legal category: Pharmacy product.Product Authorisation No: 535/1/3. Product Authorisation holder:
Shire Pharmaceuticals Ltd., Hampshire International Business Park,Chineham, Basingstoke, Hampshire RG24 8EP UK. Distributed inRepublic of Ireland by: Cahill May Roberts, P.O. Box 1090, Chapelizod,Dublin 20, Republic of Ireland. Further information is available onrequest. Date of revision: May 2011CALCICHEW is a registered trademark of Shire Pharmaceuticals Ltd inthe Republic of Ireland.
Adverse events should be reported to the Pharmacovigilance Unit at theIrish Medicines Board (IMB) ([email protected]).Information about adverse event reporting can be found on the IMBwebsite (www.imb.ie). Adverse events may also be reported to ShirePharmaceuticals Ltd on +44 1256 894000.
References: 1. Perez-Lopez FR. Maturitas 2007;58: 117-137. 2. Dawson-Hughes B & Bischoff-Ferrari HA. J Bone Miner Res 2007; 22: S2; v59-v63.3. Lin JT & Lane JM. Phys Med Rehabil Clin N Am 2005; 16: 109-128.4. Heaney RP. Endocrinol Metab Clin North Am 1998; 27(2): 255-265.5. Hunter DJ & Sambrook PN. Arthritis Res 2000; 2(6): 441-445.6. Calcichew-D3 Forte. Summary of Product Characteristics. May 2011. 7. MIMS July 2011. 8. MAT IMS data June 2011
Date of preparation: August 2011 Item Code: IRE/CDF/11/0002a
Their strength is our forte
Costs
40% le
ss tha
n
neares
t com
petito
r7Ireland's No.1Calcium supplement8(according to IMS unit sales data June 2011)HELP PROTECT
THE FRAGILE ELDERLY
Calcichew Ad A4 D4:Layout 1 09/09/2011 12:41 Page 1


















