Differentiated Service Delivery for People Displaced by ...
14
Differentiated Service Delivery for People Displaced by Violence & Emergencies in Northern Nigeria Dr. Olawale Fadare Technical Director | RISE Nigeria ICAP at Columbia University 8 th December 2020
Transcript of Differentiated Service Delivery for People Displaced by ...

Differentiated Service Delivery for People Displaced by Violence & Emergencies in Northern Nigeria
Dr. Olawale FadareTechnical Director | RISE Nigeria
ICAP at Columbia University 8th December 2020

Presentation Outline
• RISE Nigeria Program• Security situation update: Adamawa & Niger States• Impact on ART services delivered through DSD• Innovative strategies measures to ensure uninterrupted DSD in FY20• Novel initiatives targeting displaced populations in FY21
The CQUIN Project 4th Annual Meeting | December 7-10, 2020 2

RISE Program Implementation In Nigeria
The CQUIN Project 4th Annual Meeting | December 7-10, 2020 3
30 Local Government Areas 90 Health Facilities
Supported4 SupportedStates

Security Situation Update: Adamawa & Niger States
The CQUIN Project 4th Annual Meeting | December 7-10, 2020 4
NIGER STATE:Tx_Curr = 21,800 (RISE = 10,015)(~17% of RISE Tx_Curr in security prone areas) Security Report:• Responsible – bandits, marauding
herdsmen• Recurring cases since 2014/15
with escalation in 2019/20• Est. mortalities = est. 750
Other Factors:• Largest state (landmass) in Nigeria• Very poor road network• Movement restrictions and hike in
transport costs due to COVID19
ADAMAWA STATE:Tx_Curr = 26,292 (RISE = 8,980)(~60% of RISE Tx_Curr are in high-risk areas)Security Report:• Responsible – Boko Haram, Ansaru,
ISWA• Earliest cases in 2010/2011• Est. mortalities = est. 20,000 in
Adamawa/Borno axis
Other Factors:• Extensive border with Cameroon
(relatively safer)• Poor road network• Movement restrictions and hike in
transport costs due to COVID19
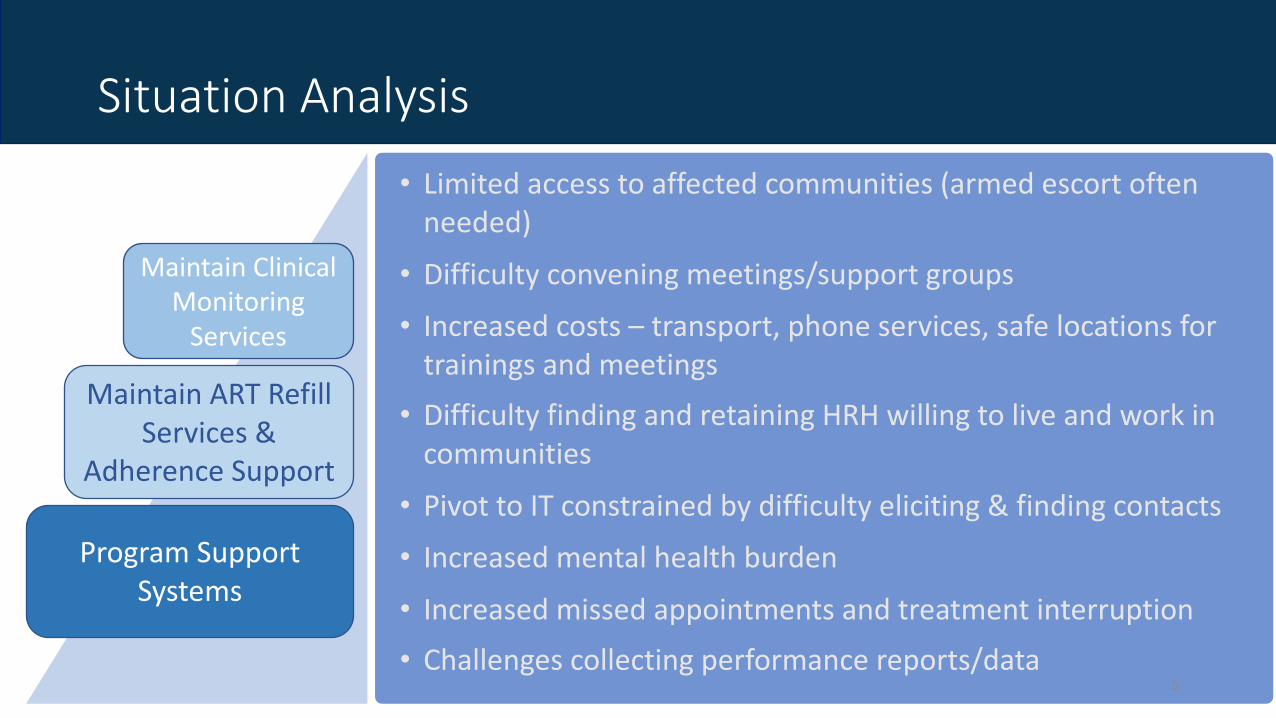
Situation Analysis
• Limited access to affected communities (armed escort often needed)
• Difficulty convening meetings/support groups
• Increased costs – transport, phone services, safe locations for trainings and meetings• Difficulty finding and retaining HRH willing to live and work in
communities
• Pivot to IT constrained by difficulty eliciting & finding contacts
• Increased mental health burden
• Increased missed appointments and treatment interruption
• Challenges collecting performance reports/data5
Maintain ART Refill Services &
Adherence Support
Maintain Clinical Monitoring
Services
Program Support Systems

RISE Nigeria: Analysis of Reasons for LTFU
1280
890
694
316 308
106 92 88 35 26 25 20 19 16 16 7 5 4 2 2
32%
23%
18%8%
8%3% 2% 2% 1% 1% 1% 1% 0% 0% 0% 0% 0% 0% 0%
0%0%
5%
10%
15%
20%
25%
30%
35%
0
200
400
600
800
1000
1200
1400
Distance
/economic r
easons
Forgo
t appointm
nent
Travelin
g/busy
with w
ork
Spirit
ual/cultu
ral belie
fs
Lack
of family
support
Hard drugs
Pill burden
Stigma
Waiting t
ime at
clinic
Domestic V
iolence
Side effe
cts of d
rugs
Alcohol
Others (N
ot Specif
ied)
Unsure how to
take
drugs
Shari
ng drugs
Conduct of s
taff c
linic
Health/death of re
lative/fa
mily
Receiving d
rugs fro
m…
Taking herbs
Non disclosure/ f
ear to disc
lose/self…
Community ART clients
Clients in employmentSingle Clients
10 – 24-year-olds
Clients enrolled in facilities
Clients not resident in LGAs
of treatment site
Vulnerability Profile
Clients enrolled in Private Facilities
80% of Reasons for LTFU
Related to impact of insecurity

The CQUIN Project 4th Annual Meeting | December 7-10, 2020 7
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct Nov Dec Jan Feb Mar Apr May Jun< 3 Months 3 - 5 Months 6 Months+
MMD transition among children and adolescents (0 - 19 years)
16%
30%
77%81%
71%
80%85%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
0
200
400
600
800
1000
1200
1400
1600
1800
May 22 May 29 Jun 5 Jun 12 June 19 Jun 26 July 03
VL Samples Collected
# Eligible # VL Collected Gap % Uptake
Weekly VL Collection and Viremia Clinic Enrollment (0-19 yrs)

The CQUIN Project 4th Annual Meeting | December 7-10, 2020 8
Viral Load Suppression: Q1 vs Q3 (0 – 24 years)
100%
43% 42%53%
64%70%
100%
51%57%
71%77%
84%
0%8%
15% 18%13% 14%
0%
20%
40%
60%
80%
100%
120%
<1 1 - 4 5 - 9 10 - 14 15 - 19 20 - 24
VL Suppression
Quarter 1 Quarter 3 Change in Suppression
Supporting Unsuppressed Adult Clients (Viremia Clinic & EAC Profile)
EAC boosted by virtual (phone) counselling using standardized
scripts

Key Strategies:
Strategic response to maintain DSD rested on:
• Open communication with high-risk locations
• Security training & low profile field operations
• Deploying ad hoc personnel to access high risk locations (including collaboration with trusted community and religious leaders)
• Regular, multi-channel data review systems (Zoom, phone, WhatsApp, SMS)
The CQUIN Project 4th Annual Meeting | December 7-10, 2020 9

The CQUIN Project 4th Annual Meeting | December 7-10, 2020
Innovative Strategies to Ensure Uninterrupted DSD
HIV Retention
• “Menu” approach - patients choose from different pickup options
• Structured adherence support (remote adherence calendar & scripts for adherence support)
• MMD for longer ART refills (>90% of patients on MMD3 and MMD6)
• “ARV frontloading” for patients with upcoming appointments if a crisis is anticipated
• Strengthening orthodox and unorthodox clinic settings for ART pickup
HIV Viral Load Monitoring
• Optimized sample collection through:• Phlebotomists embedded in
community teams• DSD model for VL (during home visits,
unsupported clinical platforms)• PPEs and training on COVID19
prevention• Sample storage and logistic systems • Digital technology for VL result
transmission
HIV Case Finding
• Index testing communicated as best practice for case finding (low prevalence in both states)
• Train community embedded ad hoc teams to drive Index HTS
• GIS-guided HTS that focused on high prevalence facilities and communities

Planned Initiatives Targeting Displaced Populations for FY21
•PEPFAR-driven inter-agency ARV delivery network• Safe Zones to facilitate deliveries during insurgencies• Backup ARV pickup centers guided by geo-spatial analysis• Religious leaders to deliver ARVs to insurgent controlled or
militarized locations
The CQUIN Project 4th Annual Meeting | December 7-10, 2020 11

The CQUIN Project 4th Annual Meeting | December 7-10, 2020 12
“One thing that has helped us is the integrated model we applied…….We worked as a team, and every contact with the patient, whether by a lab scientist or case manager, was an opportunity to provide services and build capacity“.
~ Friday Abbah(Lab Advisor, ICAP Nigeria)

This presentation was made possible with support from the U.S. President's Emergency Plan for AIDS Relief, through the United States Agency for International Development funded RISE program, under the terms of the cooperative agreement
7200AA19CA00003. The contents are the responsibility of the RISE program and do not necessarily reflect the views of USAID or the United States Government.

The CQUIN Project 4th Annual Meeting | December 7-10, 2020 14
Thank You For Listening