Different patterns of structural luteolysis in the human corpus luteum ...
10
Human Reproduction vol.15 no.10 pp.2119–2128, 2000 Different patterns of structural luteolysis in the human corpus luteum of menstruation Concepcio ´n Morales 1 , Lourdes Garcı ´a-Pardo 1 , Carlos Reymundo 1 , Carmen Bellido 2 , Jose ´ Eugenio Sa ´nchez-Criado 2 and Francisco Gayta ´n 2,3 Departments of 1 Pathology and 2 Cell Biology, Physiology and Immunology, Faculty of Medicine, University of Co ´rdoba, Co ´rdoba, Spain 3 To whom correspondence should be addressed at: Department of Cell Biology, Physiology and Immunology, Faculty of Medicine, University of Co ´rdoba, 14004-Co ´rdoba, Spain. E-mail: fi[email protected] Structural luteolysis is a complex process responsible for the elimination of the corpus luteum (CL). The aim of this study was to analyse the luteolytic process of the CL of menstruation. For this, we have morphologically studied 654 ovaries from 340 cycling women. Apoptotic cells were observed almost exclusively during the perimenstrual period and were extremely scarce at advanced stages of involution. Steroidogenic luteal cells surviving to the perimenstrual apoptotic wave underwent characteristic degenerative changes, consisting of intense cytoplasmic vacuolation, expression of macrophage markers and accumulation of lipofuscin pigment, and they persisted for long periods of time. Accumulation of corpora albicantia (CA) was observed in only 25% of a subset of 168 women, whereas 28% showed involuting CL without hyalinization, consisting of clusters of pigment-filled cells, and 46.4% showed ovaries with a mixture of CA and involuting CL without hyalinization or involuting CL with intermediate features. Evolution of the CL towards CA seemed to be related to the presence of a large, blood-filled cavity. The data from this study suggested that different patterns of structural luteolysis exist during CL involution, and that the final fate of the involuting CL is dependent on the presence of a large, central, blood-filled cavity. Key words: apoptosis/cell death/corpus albicans/corpus luteum/ structural luteolysis Introduction In non-fertile cycles, the demise of the corpus luteum (CL) occurs in two phases. First, the CL loses the ability to produce progesterone, which is referred to as functional luteolysis. This is necessary to allow the development of new follicles, providing new opportunities for fertilization, and it occurs by day 22–24 of the menstrual cycle (Niswender and Nett, 1988; Baird, 1991; Stouffer and Brannian, 1993). Second, the functionally inactive CL should be removed to avoid © European Society of Human Reproduction and Embryology 2119 accumulation of non-functional luteal tissue within the ovary. This is referred to as structural luteolysis, and it begins after the decrease in progesterone secretion, although complete deletion of the CL takes several cycles (Balboni, 1983; Nicosia, 1983; Stouffer and Brannian, 1993). Structural luteolysis has received relatively little attention, although this process is important for ovarian tissue homeo- stasis. In the absence of structural luteolysis, non-functional tissue would accumulate within the ovaries. The mechanisms ultimately responsible for the structural regression of the CL are poorly understood. Recently, apoptosis has been considered as the mechanism responsible for structural luteolysis. How- ever, previous reports on the abundance of apoptotic cells in regressing CL are controversial. The reported proportions of luteal cells undergoing apoptosis ranged from only scattered cells in only some specimens (Funayama et al., 1996) to all luteal cells (Yuan and Giudice, 1997), and affected both granulosa- and theca-lutein cells (Shikone et al., 1996) or only granulosa-lutein cells (Yuan and Giudice, 1997). In addition, previous studies focusing on the role of apoptosis in CL regression (Rodger et al., 1995; Funayama et al., 1996; Shikone et al., 1996; Yuan and Giudice, 1997) have been limited to the late luteal phase and early regression. However, degenerat- ing CL beyond ovulation in the next cycle have not been studied. It is generally assumed that CL involution gives rise to corpora albicantia (CA) through fibrosis and hyalinization of luteal tissue (Balboni, 1983; Scully et al., 1998). However, observation of different ovaries indicates that the abundance of CA is highly variable among normally cycling women. This is difficult to explain if CA formation is the only way to eliminate non-functional luteal tissue. Alterations of CL regression could be involved in different pathological conditions. About 10% of climacteric women showed Halban’s disease (Bukovsky et al., 1996), characterized by persistence of the CL, i.e. a lack of CL regression. On the other hand, premature CL regression may account for some cases of CL insufficiency (i.e. luteal phase defect; Hinney et al., 1996). Knowledge of the mechanisms responsible for the elimination of luteal tissue would contribute to the understanding of these alterations of CL disappearance. The objective of this study was to analyse the process of structural luteolysis in cycling women. Materials and methods Tissue samples Tissue samples were obtained from the files of the Department of Pathology of the University of Cordoba. A total of 654 ovaries
Transcript of Different patterns of structural luteolysis in the human corpus luteum ...

Human Reproduction vol.15 no.10 pp.2119–2128, 2000
Different patterns of structural luteolysis in the humancorpus luteum of menstruation
Concepcion Morales1, Lourdes Garcıa-Pardo1,Carlos Reymundo1, Carmen Bellido2,Jose Eugenio Sanchez-Criado2 andFrancisco Gaytan2,3
Departments of 1Pathology and 2Cell Biology, Physiology andImmunology, Faculty of Medicine, University of Cordoba, Cordoba,Spain3To whom correspondence should be addressed at: Department ofCell Biology, Physiology and Immunology, Faculty of Medicine,University of Cordoba, 14004-Cordoba, Spain.E-mail: [email protected]
Structural luteolysis is a complex process responsible forthe elimination of the corpus luteum (CL). The aim of thisstudy was to analyse the luteolytic process of the CL ofmenstruation. For this, we have morphologically studied654 ovaries from 340 cycling women. Apoptotic cells wereobserved almost exclusively during the perimenstrualperiod and were extremely scarce at advanced stagesof involution. Steroidogenic luteal cells surviving to theperimenstrual apoptotic wave underwent characteristicdegenerative changes, consisting of intense cytoplasmicvacuolation, expression of macrophage markers andaccumulation of lipofuscin pigment, and they persisted forlong periods of time. Accumulation of corpora albicantia(CA) was observed in only 25% of a subset of 168 women,whereas 28% showed involuting CL without hyalinization,consisting of clusters of pigment-filled cells, and 46.4%showed ovaries with a mixture of CA and involuting CLwithout hyalinization or involuting CL with intermediatefeatures. Evolution of the CL towards CA seemed to berelated to the presence of a large, blood-filled cavity. Thedata from this study suggested that different patterns ofstructural luteolysis exist during CL involution, and thatthe final fate of the involuting CL is dependent on thepresence of a large, central, blood-filled cavity.Key words: apoptosis/cell death/corpus albicans/corpus luteum/structural luteolysis
Introduction
In non-fertile cycles, the demise of the corpus luteum (CL)occurs in two phases. First, the CL loses the ability to produceprogesterone, which is referred to as functional luteolysis.This is necessary to allow the development of new follicles,providing new opportunities for fertilization, and it occurs byday 22–24 of the menstrual cycle (Niswender and Nett,1988; Baird, 1991; Stouffer and Brannian, 1993). Second,the functionally inactive CL should be removed to avoid
© European Society of Human Reproduction and Embryology 2119
accumulation of non-functional luteal tissue within the ovary.This is referred to as structural luteolysis, and it begins afterthe decrease in progesterone secretion, although completedeletion of the CL takes several cycles (Balboni, 1983; Nicosia,1983; Stouffer and Brannian, 1993).
Structural luteolysis has received relatively little attention,although this process is important for ovarian tissue homeo-stasis. In the absence of structural luteolysis, non-functionaltissue would accumulate within the ovaries. The mechanismsultimately responsible for the structural regression of the CLare poorly understood. Recently, apoptosis has been consideredas the mechanism responsible for structural luteolysis. How-ever, previous reports on the abundance of apoptotic cells inregressing CL are controversial. The reported proportions ofluteal cells undergoing apoptosis ranged from only scatteredcells in only some specimens (Funayama et al., 1996) to allluteal cells (Yuan and Giudice, 1997), and affected bothgranulosa- and theca-lutein cells (Shikone et al., 1996) or onlygranulosa-lutein cells (Yuan and Giudice, 1997). In addition,previous studies focusing on the role of apoptosis in CLregression (Rodger et al., 1995; Funayama et al., 1996; Shikoneet al., 1996; Yuan and Giudice, 1997) have been limited tothe late luteal phase and early regression. However, degenerat-ing CL beyond ovulation in the next cycle have not beenstudied.
It is generally assumed that CL involution gives rise tocorpora albicantia (CA) through fibrosis and hyalinization ofluteal tissue (Balboni, 1983; Scully et al., 1998). However,observation of different ovaries indicates that the abundanceof CA is highly variable among normally cycling women. Thisis difficult to explain if CA formation is the only way toeliminate non-functional luteal tissue.
Alterations of CL regression could be involved in differentpathological conditions. About 10% of climacteric womenshowed Halban’s disease (Bukovsky et al., 1996), characterizedby persistence of the CL, i.e. a lack of CL regression. On theother hand, premature CL regression may account for somecases of CL insufficiency (i.e. luteal phase defect; Hinneyet al., 1996). Knowledge of the mechanisms responsiblefor the elimination of luteal tissue would contribute to theunderstanding of these alterations of CL disappearance.
The objective of this study was to analyse the process ofstructural luteolysis in cycling women.
Materials and methods
Tissue samples
Tissue samples were obtained from the files of the Department ofPathology of the University of Cordoba. A total of 654 ovaries

C.Morales et al.
belonging to 340 women (64% in the luteal phase and 36% in thefollicular phase; age range 19 to 48 years) was studied morpho-logically. Most tissue samples corresponded to hysterectomized andbilaterally salpingo-oophorectomized women due to uterine lesions.Patients did not show ovarian pathology, nor were they under-going hormonal treatment, and showed normal menstrual cycles.Normal cyclicity was confirmed by the presence of a CL of thecurrent cycle (luteal phase), or an early regressing CL of the precedingcycle (follicular phase). The day of the cycle was assigned byconsidering the menstrual history, and dating of the endometrium(Dallenbach-Hellweg, 1971) and corpus luteum (Corner, 1956).
The standard cycle was considered to be 28 days. CL were classifiedin the following phases: (i) functional CL (FCL) from the date ofovulation to day 24 of the first cycle; (ii) regressing CL (RCL), fromday 25 of the first cycle to the date of ovulation in the next (second)cycle; and (iii) involuting CL (ICL), from day 15 of the second cycleonward. For the purposes of this study the dating of only two specificcycle points was necessary. Days 24–25 of the standard cycle(corresponding to the transition from FCL to RCL) were recognizedby CL histology [general shrinkage of the granulosa-lutein layer,presence of scattered apoptotic nuclei and vacuolated granulosa-lutein cells (GLC) showing CD68 immunostaining], endometrialcharacteristics (presence of prominent spiral arteries and pre-decidualization around these arteries or beneath the epithelium,corresponding to days 23–25 of the standard cycle) and a compatiblemenstrual history, corresponding to the late luteal phase. Days14–15 of the standard cycle (corresponding to the transition fromRCL to ICL) were recognized by the presence in the ovary of a just-ruptured follicle or a newly formed, still unluteinized CL, togetherwith compatible endometrial dating and menstrual history. CA wereconsidered to be present when only hyalinized material lacking lutealtissue was visible.
The following tissue compartments were considered in the CL: (i)luteal tissue, corresponding to the granulosa-lutein layer, togetherwith theca-lutein areas; (ii) inner boundary tissue (IBT), whichcorresponded to the connective tissue lining the inner aspect of theluteal tissue; and (iii) central cavity, that was filled with blood andfollicular fluid remnants and surrounded by the IBT.
Sections of the CL were stained with haematoxylin and eosin, orthe AFIP method for lipofuscin (Johnson, 1992).
Immunohistochemistry
Immunohistochemistry was performed on routinely neutral-buffered,formaldehyde-fixed, paraffin-embedded tissues. Sections (5 µm) wereplaced on poly-L-lysine-coated slides and, after dewaxing and rehydra-tion in a graded series of ethanol, were incubated in 2% hydrogenperoxide in methanol for 30 min, to inhibit endogenous peroxidase.Monoclonal antibodies against CD68 antigen (Dako Diagnostica,Seville, Spain) as a macrophage marker (Bukovsky et al., 1995, 1996;Suzuki et al., 1998), CD34 antigen (Novocastra Laboratories Ltd,Barcelona, Spain) as an endothelial cell marker (Ito et al., 1995;Gaytan et al., 1999), Ki-67 antigen (Concepta, Barcelona, Spain) asa marker of proliferating cells (Hall and Levison, 1990) and anti-human muscle actin (HHF35, Enzo Diagnostic Inc., New York,USA; Tsukada et al., 1987) were used. Sections destined to beimmunostained for Ki-67 were predigested in 0.1% (w/v) trypsin(Difco, Detroit, MI, USA) in phosphate-buffered saline (PBS)containing 0.1% (w/v) sodium chloride for 20 min at 37°C. Afterwashing in distilled water, these sections, as well as those destinedto be stained for the CD68 and CD34 antigens were immersed in10 mmol/l citrate buffer and submitted to antigen retrieval in amicrowave oven (2�5 min at 700 W). Afterwards, the sections wereallowed to cool at room temperature, washed in PBS, blocked with
2120
normal rabbit serum, and incubated overnight with the primaryantibodies (anti-CD68 1:400; anti-CD34 1:25; anti-Ki67 pre-diluted,anti-actin 1:300). The sections were then processed by the avidin–biotin peroxidase complex (ABC) method, following previouslydescribed procedures (Gaytan et al., 1997).
Negative control sections were run by incubating sections withnon-immune serum or PBS instead of the first antibody. Positivecontrols were provided by non-luteal ovarian tissues (i.e. atreticfollicles for macrophages, medullary blood vessels for endothelium,proliferating cells in healthy growing follicles for Ki-67 and smoothmuscle of the arterial wall for actin). Sections were counterstainedwith haematoxylin.
Quantitative studies
The total number of cases (i.e. 340 women, 654 ovaries) was usedfor morphological evaluation. For quantitative studies, 168 women(in which both ovaries and two blocks per ovary were available)were selected. At least five non-consecutive equatorial sections (at50 µm intervals) from each block were scored and the ovaries wereclassified into the following types: (i) CA(–), with absence of CA,and showing only involuting CL without or with minute hyalinizedareas; (ii) CA(�), containing abundant large CA; or (iii) mixed,containing both CA and involuting CL without hyalinization or CLwith intermediate features, showing an asymmetrical distribution ofhyalinized and non-hyalinized areas. To test the hypothesis thatfolding of the CL was associated with the luteolytic pattern, 62 ofthese 168 women who were in the luteal phase and showing adequatesections of the CL of the current cycle were selected. The CL of thecurrent cycle was classified as: (i) folded, when luteal tissue showeda festooned contour, limiting a usually small cavity; or (ii) unfoldedor irregularly folded, when the luteal tissue showed a smooth contourin the whole or large areas of the CL section. In all cases, the CLwas evaluated only when a central section of the CL was present.The zone of the CL adjacent to the point of rupture was not considered,because unfolding was common in this area in most CL.
Statistical analysis was performed by the χ2 test with Yates’correction.
Results
Morphological changes during structural luteolysis occurredin all CL compartments. Although structural luteolysis wasassessed by observation of static tissue sections, indirectconclusions about the progression of the luteolytic processwere easily derived from this material. The observation ofcorpora lutea at different stages of the luteolytic process indifferent ovaries allowed us to establish a correspondencebetween the age of the CL and the morphological changes inthe luteal tissue. In addition, the presence in the same ovary(or pair of ovaries) of several generations of corpora lutea(one cycle-old difference) provided also valuable data forrelating changes in luteal tissue to CL age, avoiding individualvariability. For greater clarity, changes in the different compart-ments will be described separately.
Changes in luteal tissue
Morphological changes during the luteal phase of the currentcycle have been described elsewhere (Gaytan et al., 1998,1999). Briefly, steroidogenic luteal cells reached full luteiniz-ation by day 19 and abundant macrophages, showing dendritic

Human luteolysis
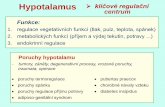
Figure 1. Expression of the macrophage marker CD68 bymacrophages (arrows) showing dendritic features in a functionalcorpus luteum (CL) (A), by scattered granulosa-lutein cells (arrows)in a regressing CL (B) and by all granulosa-lutein cells but not bytheca-lutein cells in an involuting CL (C). G � granulosa-luteinlayer; T � theca-lutein areas. A–C all printed at the samemagnification. Scale bar in (A) � 100 µm.
features (Figures 1A and 2B), were observed in the granulosa-lutein layer. Clear morphological signs of structural luteolysiswere not evident before day 25 of the cycle. In regressing CL,increasing regressive changes were apparent. There was ageneral shrinkage of the luteal tissue, due to the decrease inthe volume of the GLC, as previously reported (Gaytan et al.,1998, 1999). Apoptotic cells, characterized by condensedchromatin, shrunken eosinophilic cytoplasm and fragmentationinto clusters of apoptotic bodies at advanced stages, wereobserved (Figure 2A) in both theca-lutein and granulosa-luteinareas during the perimenstrual period, from a few days beforeto a few days after menstruation. Apoptotic cells were scarceduring the late follicular phase of the second cycle, andwere only occasionally found from day 14 of the secondcycle onward.
From day 25 of the first cycle onward, isolated GLC showedhighly vacuolated cytoplasm and strong immunostaining for
2121
the macrophage marker CD68 (Figure 1B). GLC showingthese features were more abundant during the follicular phaseof the second cycle, and were found scattered among non-vacuolated, non-CD68-expressing GLC throughout thegranulosa-lutein layer. In involuting CL, the above-describedchanges affected the totality of the granulosa-lutein layer. AllGLC became vacuolated and showed intense CD68 immuno-staining (Figure 1C). Theca-lutein cells did not show CD68immunostaining, although they were also vacuolated. Duringthe luteal phase of the second cycle, GLC were highlyvacuolated, whereas the expression of CD68 was fainter(Figure 2C). These cells showed small nuclei and light-stainedcytoplasm with haematoxylin and eosin, but did not showchromatin condensation or other apoptotic features. Duringadvanced involution (in subsequent cycles) vacuolated GLCshowed accumulation of lipofuscin pigment (Figures 2D and3A), as indicated by their specific staining by the AFIPmethod for lipofuscin (Figure 3C). In some cases, cytoplasmicmembranes separating adjacent cells were apparently disruptedand images suggestive of syncytia formation were observed(Figure 2C). Clusters of pigment-filled (Figure 3A), CD68-expressing (Figure 3B) cells were found scattered in theovarian stroma and surrounding young CA (Figure 5E). Insome cases, the intercellular areas of the luteal tissue ininvoluting CL, showed intense eosinophilia, homogeneousappearance, and became hyalinized, entrapping pigment-filledcells (Figure 3D). Even at advanced stages of involution,blood vessels were present within involuting luteal tissue.Proliferating (Ki67-immunostained) cells were abundant duringthe first stages of CL development, but were only occasionallyfound in regressing and involuting CL.
Changes in the inner boundary tissue (IBT)
The IBT appeared in functional CL, from day 18 onward,lining the inner border of the luteal tissue. In sections immuno-stained with anti-actin antibodies, connective tissue cells inthe IBT showed intense cytoplasmic immunoreactivity(Figure 4B). These actin-containing cells did not correspondto vascular or perivascular cells, since blood vessels didnot invade the IBT, as shown by immunostaining with theendothelial cell marker CD34 (Figure 4A). In regressing CL,a wide band of actin-containing cells was observed lining thecentral cavity. The IBT was more prominent in those CLdisplaying a large blood-filled central cavity, whereas in well-folded CL the IBT from opposite foldings made contact andthe small central cavity was filled with loose connectivetissue, containing actin-immunostained cells. In involuting CL,progressive hyalinization of the IBT was observed (Figure5A–C). In young CA, an external zone containing fibroblast-like, actin-immunostained (Figures 4D and 5D) cells wasevident, surrounding a central area lacking (or with onlyoccasional) cells. In more mature CA, actin-containing cellswere observed deeper into the CA (Figure 4E), and were foundthroughout the section in old CA (Figure 4F). Proliferatingcells were extremely scarce.
Changes in the central cavity
The central cavity was highly variable in size among differentCL. This cavity was filled with blood shortly after ovulation.

C.Morales et al.
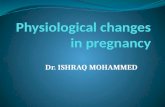
Figure 2. Changes in luteal tissue during structural luteolysis and involution. (A) Apoptotic cells (arrows) in a perimenstrual corpus luteum(CL). (B) Macrophages (arrows) immunostained for CD68, showing dendritic features in a functional CL. (C) Vacuolization and faintexpression of CD68 (arrows) by granulosa-lutein cells in an involuting CL. (D) Accumulation of lipofuscin pigments in granulosa-luteincells (arrows) during advanced involution. A–D all printed at the same magnification. Scale bar in (D) � 25 µm.
Figure 3. Remnants of luteal tissue (LT) at advanced corpus luteum (CL) involution. Clusters of pigment-filled cells (A), expressingCD68 (B), that are specifically stained for lipofuscin (C). The boundaries of the clusters are indicated by arrowheads. (D) Hyalinizationof the intercellular areas (stars) in a luteal tissue remnant. Scale bar in A (applies also to B) � 60 µm; scale bar in C (applies alsoto D) � 50 µm.
The central blood clot was more dense in older corpora lutea,but successive haemorrhage occurred during the luteal phaseof the first cycle and the follicular phase of the second cycle.In those CL displaying a large, blood-filled cavity, the centralblood clot was not invaded by connective tissue of blood
2122
vessels (Figure 5A–C). In advanced regressing and involutingCL, the central blood clot showed a homogeneous appearanceand intense eosinophilia that was suggestive of hyalinization(Figure 5A–C). This was first seen at the outer aspect of thecentral cavity, and throughout the central cavity in advanced

Human luteolysis
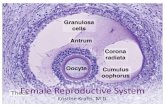
Figure 4. Micrographs from corpus luteum (CL) sections immunostained for the endothelial cell marker CD34 (A) or actin (B–F). (A)Functional CL. Blood vessels (arrows) are present in the luteal tissue (LT), but do not invade the inner boundary tissue (stars). (B, C) Actin-containing cells are present in large blood vessels (short arrows) in the luteal tissue (LT), and in the inner boundary tissue (long arrows) inboth functional (B) and involuting (C) CL. In young corpora albicantia (D), actin-containing cells (arrows) are present in the peripheral zone(PZ) and absent in the central zone (CZ). Actin-containing cells are found deeper in the CA at more advanced stages (E) and throughout thesection in old CA (F). Scale bar in B (applies also to A) � 100 µm; scale bar in C (applies also to D–F) � 60 µm.
involuting CL. White blood cells were abundant in the centralcavity in functional CL, but were almost absent in involutingCL. Macrophages containing haemosiderin were rarelyobserved in the central cavity, and were found almostexclusively in CL containing a small cavity. In some cases, acentral empty area—probably due to retraction of the centralblood clot—was observed. In young CA, a central hyalinizedzone was found which lacked myofibroblasts and bloodvessels (Figure 5D). Old CA appeared as lobulated structurescontaining abundant actin-immunostained cells, and wereconsiderably shrunken.
General evolution of the CL during structural luteolysis
The data obtained from this study suggested that the differentluteolytic patterns observed were dependent on the existenceof structural differences among different CL. Under thishypothesis, the final fate of an involuting CL seemed to bedependent on the presence or absence of a large, blood-filledcavity. In those CL displaying a small cavity with minimalhaemorrhage, the cavity was usually filled with looseconnective tissue derived from the IBT from opposite foldings.Involution of these CL seemed to give rise to scattered
2123
remnants of pigment-filled GLC (Figures 3A–C and 6A), orto small scars with some entrapped pigment-filled luteal cells,but typical CA seemed not to develop.
Alternatively, some CL showed a large, blood-filled cavity.In these cases, progressive hyalinization of the central bloodclot was observed, and this material seemed to constitute thebulk of the CA. In young CA, several layers (Figure 5C andD) were distinguishable: (i) a central hyalinized zone, that wasdisorganized and showed absence or extremely low numbersof cells and absence of blood vessel remnants, probably derivedfrom the central blood clot; (ii) a mid zone of well-organizedhyalinized tissue, containing myofibroblasts, and probablyderived from the IBT; and (iii) in some cases, an external zoneof hyalinized tissue containing fibroblasts and blood vesselremnants, that was probably derived from hyalinization ofintercellular areas of the involuting luteal tissue. In old CA,however, distinction among the different zones was notpossible, due to the progressive invasion of the CA byperipheral actin-containing cells. Many CA were observed inCA(�) ovaries; this indicated that these structures persist forlong periods of time before final resorption.
Involuting CL displaying intermediate features between the

C.Morales et al.
Figure 5. Evolution of the inner boundary tissue and central cavity during corpus luteum (CL) regression and involution. (A–C) Progressiveloss of luteal tissue (LT), hyalinization of the inner boundary tissue (double-arrows) and of the central cavity (C). Hyalinization of thecentral blood clot was first evident at the periphery (stars). (D, E) In young corpora albicantia, a peripheral zone (PZ) containing cells, and acentral zone (CZ) as well as remnants of luteal tissue (arrows) surrounding hyalinized areas (HA) can be observed. Scale bar in C (appliesalso to A and B) � 50 µm; scale bar in E (applies also to D) � 40 µm.
above-described modes of involution were also found (Figure6C). In these cases asymmetrical CA (consisting of zones ofpigment-filled cells) as well as areas of hyalinization wereobserved. In some cases, these involuting CL showed an emptycavity containing fresh blood and haemosiderin-containingmacrophages.
Large variations with respect to the number and size of CAwere found among the ovaries from regularly cycling women.From the quantitative study of a subset of 168 cases, wedetermined that some women (corresponding to 28.5%;n � 48), had CA(–) ovaries showing involuting CL andabsence of CA, and only small scars or clusters of pigment-filled cells remaining after CL effacement. In contrast, somewomen (corresponding to 25.1%; n � 42) had CA(�) ovaries,showing high numbers of large CA at different stages ofinvolution. In these ovaries, considerable distortion of largeantral follicles and newly formed CL was observed, and alarge proportion of the ovarian volume was occupied by CA.Finally, the majority of women (corresponding to 46.4%;n � 78) had mixed ovaries that showed a mixture of bothtypes of CL involution, or involuting CL with intermediatefeatures, with wide hyalinized areas together with areas lackinghyalinization. No differences were found between the twoovaries in individual women for CA(�) and CA(–) types.
The relationship between the degree of folding of the CL
2124
of the current cycle (Figure 7) and the luteolytic pattern forwomen with CA(�) and CA(–) ovaries is shown in Table I.There was a significant (P � 0.001) association between thedegree of folding of the new CL and the luteolytic pattern. Inwomen lacking CA [CA(–)], the CL of the current cycle wasfolded in 84.2% of cases, whereas in women containingabundant CA [CA(�)], the CL of the current cycle wasunfolded or irregularly folded in 83.3% of cases.
Discussion
The mechanisms responsible for luteal cell disappearanceduring structural luteolysis are not well known. During recentyears, the possible role of apoptosis as a mechanism for lutealcell disappearance has received considerable attention, sincethis type of cell death could suggest a time-programmedmechanism for the cyclical removal of non-functional lutealtissue (Rodger et al., 1995; Funayama et al., 1996; Shikoneet al., 1996; Yuan and Giudice, 1997).
In this study, dying luteal cells showing the characteristicmorphological features of apoptosis were almost exclusivelyobserved at the beginning of CL regression, and were veryscarce in involuting CL, when luteal cells were still abundant.Apoptotic cells were recognized on the basis of theirmorphological features. The morphological characteristics of

Human luteolysis
Figure 6. Different luteolytic patterns. Involuting corpus luteum(CL) lacking hyalinization (A), consisting of clusters of lutealtissue (LT), corpora albicantia (asterisks) in different stages ofinvolution (B) and involuting CL showing intermediate features(C), consisting of clusters of pigment-filled cells (arrows),intermingled with hyalinized areas (stars). Scale bar in C (appliesalso to A) � 100 µm; scale bar in B � 130 µm.
apoptotic cells are highly specific to this type of cell death(Searle et al., 1982; Wyllie, 1986). Previous studies comparingdetection of apoptotic cells by morphological criteria and3�-end-labelling methods demonstrated that cells exhibitingapoptotic morphological features contained fragmented DNA(Young et al., 1997; Gaytan et al., 1998). The amount ofapoptosis evaluated by the two different techniques wasequivalent in both rat (Gaytan et al., 1998) and primate (Younget al., 1997) species. This indicates that careful morphologicalevaluation is a useful, simple and rapid method for the detectionof apoptosis.
Large differences in the number of apoptotic cells duringstructural luteolysis have been reported, ranging from onlyscattered apoptotic nuclei (Funayama et al., 1996) to thepractical totality of luteal cells (Shikone et al., 1996; Yuanand Giudice, 1997). Although the reasons for thesediscrepancies are not known, it is clear that most luteal cellscannot undergo apoptosis at early stages of structural luteolysis,
2125
Figure 7. Corpus luteum (CL) of the current cycle. (A) A well-folded CL, in which the boundaries of the granulosa-lutein layerhave been highlighted with dashed lines, and (B) an unfolded CL.(C) Theca- (T) and granulosa- (G) lutein cells can be observed athigher magnification. LT � luteal tissue. The inner zone isindicated by asterisks. Scale bars: (A, B) � 100 µm; (C) � 30 µm.
Table I. Relationship between the luteolytic pattern and the degree offolding of the corpus luteum (CL) in ovarian tissues taken from 62 normalcycling women
Luteolytic pattern CL of the current cycle
Folded Unfolded
Corpus albicans (–) 32 (84.2) 6 (15.8)Corpus albicans (�) 4 (16.6) 20 (83.3)
Values in parentheses are percentages.P � 0.001 (χ2 with Yates’ correction � 24.86 for n � 62).
since luteal tissue persisted for several cycles. Studies in themarmoset monkey (Young et al., 1997) indicated that apoptosiswas relatively abundant at the beginning of the follicular phaseof the next cycle, and decreased thereafter, which agrees withdata obtained in the present study.
Indeed, the data of this study suggested that in the humanCL, apoptosis represents an initial and probably important stepin structural luteolysis. However, most steroidogenic luteal

C.Morales et al.
cells seemed to survive to the perimenstrual apoptotic wave.Thereafter, the remaining luteal cells underwent slowdegenerative changes [consisting of extreme cytoplasmicvacuolation, expression of lysosome-associated antigens(CD68) and accumulation of lipofuscin pigments and, in somecases, apparent cytoplasmic membrane disruption and syncytiaformation] and persisted for long periods of time. Changessimilar to those described in this study have been reportedrecently (Young et al., 1997; Fraser et al., 1999) duringluteolysis in the marmoset monkey. Vacuolation and apparentsyncytia formation have been also reported in the regressingCL of sheep (Sawyer, 1995), while cytoplasmic vacuolationand autophagia have also been described in developing tissues(Clarke, 1990). The expression of the lysosome marker CD68reported here, in accordance with previous studies (Bukovskyet al., 1995, 1996), as well as the increased numbers ofphagolysosomes reported in steroidogenic cells during luteo-lysis (Sawyer, 1995), are suggestive of the existence ofautophagic activity. Furthermore, the accumulation of lipo-fuscin pigments in the remaining luteal cells also agrees withan autophagic model of cell degeneration. Lipofuscin is aninsoluble pigment that represents the accumulation ofindigestible material in lysosomes after autophagy (Yeldandiet al., 1996). A previous study (Quatacker, 1971), alsosuggested that cells within the regressing CL correspondedto granulosa cells with autophagocytic capabilities. Whetherpigment-filled cells are finally removed by apoptosis isunknown. If apoptosis is the mechanism responsible for thedisappearance of luteal cell remnants, it should happen at avery low rate, probably below the limits of detection by tissuesection assessment.
Expression of CD68 was observed in isolated GLC at thelate luteal stage, and GLC expressing CD68 became moreabundant during the follicular phase of the next cycle. Expres-sion of several macrophage markers by GLC has been reportedpreviously (Best et al., 1996; Bukovsky et al., 1996; Gaytanet al., 1998) in the regressing CL. In this study, generalizedexpression of CD68 in the whole granulosa-lutein layer wascoincident with generalized vacuolation of GLC and with theexpected date of ovulation in the second cycle. In fact, whena CL of the previous cycle showing generalized vacuolationand expression of CD68 was present, a newly formed CL wasfound in the same or in the contralateral ovary. This suggeststhat pre-ovulatory hormone surges are involved in theregressive changes observed at this time in the CL of theprevious cycle. In cycling rats, the pre-ovulatory hormonesurges on the evening of prooestrus links ovulation to theinduction of regressive changes in the CL of the previouscycle (Gaytan et al,. 1997). Although regressive changes inthe human CL were already present from the late lutealphase, generalized vacuolation and CD68 expression seemedto represent a specific step in structural luteolysis. Changes inthe CL associated with the next ovulation are characteristicenough to recognize this stage of the cycle by observation ofthe CL of the previous cycle.
It is generally agreed that the final fate of the CL is theformation of a CA, and that the CA arises through hyalinizationof collagen produced by the connective tissue that replaces
2126
luteal tissue and invades the central cavity during luteolysis(Balboni, 1983; Scully et al., 1996). However, the observationsof this study did not support this view. First, the absence ofCA in about 28% of regularly cycling women indicated thatCA formation is not the only luteolytic pathway. Second, onlya small part of the CA seemed to be formed by hyalinizationof the IBT and in some cases, by hyalinization of the interstitialareas of the luteal tissue. The bulk of the CA seemed to beformed through hyalinization of the central blood clot. Hyalineis a descriptive term applied to any homogeneous, eosinophilicmaterial that is produced by a multitude of mechanisms. Insome cases, extracellular hyaline is composed of precipitatedplasma proteins (Cotran et al., 1989), which agrees with theproposed origin of CA hyaline in this study. Under thishypothesis, only CL displaying a large blood-filled cavity giverise to large typical CA. Several lines of evidence support thisview: (i) Resorption of the central blood clot was not observedat any stage of CL involution; macrophages that would benecessary to eliminate the central coagulum, and becomehaemosiderin-containing cells, were rarely observed ininvoluting CL. (ii) Replacement of the central blood clot byconnective (collagen-synthesizing) tissue was not observed;connective tissue cells were almost exclusively found ininvoluting CL lacking a central cavity and seemed to corre-spond to the IBT from opposite foldings, and proliferativeactivity was extremely scarce in the IBT throughout CLinvolution. (iii) Hyalinization-like changes, such as intenseeosinophilia and the acquisition of a homogeneous appearance,were observed in the central blood clot during CL involution.(iv) The existence in young CA of an external zone containingactin-immunostained cells (i.e. myofibroblasts), probablyderived from the IBT, surrounding a central hyalinized arealacking cells. The presence of a band of actin-containing cellssurrounding the CA suggested that progressive contraction ofthe CA could be due to the presence of this outer band ofcontractile cells. These data suggest that only CL displayinga large blood-filled cavity give rise to CA, whereas if therewas no central blood-filled cavity or it was minimal, typicalCA did not develop. Mixed involuting CL were probablyderived from CL showing a small blood-filled cavity. Sinceresorption of CA seems to take years, CA are over-representedin ovarian sections with respect to non-hyalinized involutingCL.
Large variations among CL within the same ovary, as wellas among women, with respect to the presence and numbersof CA, were observed in regularly cycling women of similarage. These differences ranged from ovaries lacking CA andcontaining only involuting CL without (or with minimal)hyalinization, to ovaries containing large numbers of CA ofdifferent sizes, corresponding to different stages of evolution.This indicated that alternative luteolytic patterns (involvingdevelopment of CA or not) may account for the eliminationof non-functional luteal tissue in the human ovary. Theexistence of differences among different corpora lutea withinthe same ovary (mixed ovaries that were present in 46.4% ofwomen) indicated that the luteolytic pattern was dependent onthe characteristics of each particular CL. On the other hand,the existence of women showing exclusively a particular

Human luteolysis
luteolytic pattern [25% CA(�) and 28.5% CA(–)] indicatedthe existence of an individual tendency to follow a specificluteolytic pathway. Only CL displaying a large blood-filledcavity seemed to give rise to large CA. However, the causefor the presence of a large blood-filled cavity in some CL isnot clear. A possibility is that variations in the collapse of thepost-ovulatory follicle are responsible for the accumulation ofblood. This was also suggested by the existence of a statisticallysignificant association between unfolding of the newly formedCL and the luteolytic pattern. However, the presence ofunfolded luteal tissue could be either a cause or a consequenceof the presence of a large central blood clot. Therefore, acause-and-effect relationship cannot be established from thedata presented in this study.
The unfolded/irregularly folded CL considered in this study,and characterized by a well-luteinized wall surrounding ablood-filled cavity and a prominent IBT, are usually referredto as CL cysts (Clement, 1989; Scully et al., 1996). Most ofthem contained folded and unfolded areas, and the site offollicular rupture was observed. The existence of luteinizedunruptured follicles (LUF) has been reported, mostly associatedwith ovarian stimulation (Coetsier and Dhont, 1996) or endo-metriosis (Kaya and Oral, 1999). The presence of LUF innormally cycling women seems to be a sporadic and infrequentphenomenon (Kerin et al., 1983), that cannot account for theabundance of CA reported in this study [CA(�) 25% ofwomen and mixed ovaries 46.5% of women]. However, itcannot be ruled out that some blood-containing unfolded CLcorresponded to LUF. Furthermore, the lack of collapse of thepost-ovulatory follicle has been achieved experimentally inewes after immunization against inhibin-related peptides(Russell et al., 1995), even in the presence of follicle rupture.This suggests that follicle collapse is not only due to folliclerupture, but also depends on complex tissue remodellingprocesses.
In summary, luteal cells surviving to the perimenstrualapoptotic wave underwent progressive degenerative changes,characterized by extreme vacuolation, expression of macro-phage markers and accumulation of lipofuscin pigments. Thepattern of structural luteolysis (formation of a CA or not)seemed to be determined shortly after ovulation, dependingon the presence or absence of a large, blood-filled central cavity.
AcknowledgementsThe authors are very grateful to J.Molina, P.Cano and E.Tarradasfor their technical assistance. This work was supported by grantsPM98-0167, APC98-0148 and 1FD97-1065-CO3-03.
ReferencesBaird, D.T. (1991) The ovarian cycle. In Hillier, S.G. (ed.), Ovarian
Endocrinology. Blackwell Scientific Publications, Oxford, pp. 1–24.Balboni, G.C. (1983) Structural changes: ovulation and luteal phase. In Serra,
G.B. (ed.), The Ovary. Raven Press, New York, pp. 123–141.Best, C.L., Pudney, J., Welch, W.R. et al. (1996) Localization and
characterization of white blood cell populations within the human ovarythroughout the menstrual cycle and menopause. Hum. Reprod., 11, 790–797.
2127
Bukovsky, A., Caudle, M.R., Keenan, J.A. et al. (1995) Is corpus luteumregression an immune-mediated event? Localization of immune systemcomponents and luteinizing hormone receptor in human corpora lutea. Biol.Reprod., 53, 1373–1384.
Bukovsky, A., Caudle, M.R., Keenan, J.A. et al. (1996) Is irregular regressionof corpora lutea in climacteric women caused by age-induced alterations inthe ‘tissue control system’? Am. J. Reprod. Immunol., 36, 327–341.
Clarke, P.G.H. (1990) Developmental cell death: morphological diversity andmultiple mechanisms. Anat. Embryol., 181, 195–213.
Clement, P.P. (1989) Non-neoplastic lesions of the ovary. In Kurman, R.J.(ed.), Blaunstein’s Pathology of the Female Genital Tract. Springer-Verlag,New York, pp. 471–515.
Coetsier, T. and Dhont, M. (1996) Complete and partial luteinized unrupturedfollicles syndrome after ovarian stimulation with clomiphene citrate/humanmenopausal gonadotrophin/human chorionic gonadotrophin. Hum. Reprod.,11, 583–587.
Corner, G.W., Jr (1956) The histological dating of the human corpus luteumof menstruation. Am. J. Anat., 98, 377–392.
Cotran, R.S., Kumar, V. and Robbins, S.L. (1989) Cell injury and adaptation.In Cotran, R.S., Kumar, V. and Robbins, S.L. (eds), Pathologic Basis ofDisease, W.B. Saunders Co., Philadelphia, pp. 1–38.
Dallenbach-Hellweg, G. (1971) Histopathology of the Endometrium. Springer-Verlag, Berlin, pp. 20–76.
Fraser, H.L., Lunno, S.F., Harrison, D.J. et al. (1999) Luteal regression in theprimate: different forms of cell death during natural and gonadotropin-releasing hormone antagonist or prostaglandin analogue-induced luteolysis.Biol. Reprod., 61, 1468–1479.
Funayama, Y., Sasano, H., Suzuki, T. et al. (1996) Cell turnover in normalcycling human ovary. J. Clin. Endocrinol. Metab., 81, 828–834.
Gaytan, F., Morales, C., Bellido, C. et al. (1997) Role of prolactin in theregulation of macrophages and in the proliferative activity of vascular cellsin newly formed and regressing rat corpora lutea. Biol. Reprod., 57, 478–486.
Gaytan, F., Morales, C., Garcıa-Pardo, L. et al. (1998) Macrophages, cellproliferation, and cell death in the human menstrual corpus luteum. Biol.Reprod., 59, 417–425.
Gaytan, F., Morales, C., Garcıa-Pardo, L. et al. (1999) A quantitative studyof changes in the human corpus luteum microvasculature during themenstrual cycle. Biol. Reprod., 60, 914–919.
Hall, P.A. and Levison, D.A. (1990) Assessment of cell proliferation inhistological material. J. Clin. Pathol., 43, 184–192.
Hinney, B., Henze, C., Kuhn, W. et al. (1996) The corpus luteum insufficiency:a multifactorial disease. J. Clin. Endocrinol. Metab., 81, 565–570.
Ito, A., Nomura, S., Hirota, S. et al. (1995) Enhanced expression of CD34messenger RNA by developing endothelial cells of mice. Lab. Invest., 72,532–538.
Johnson, F.B. (1992) Pigments and minerals. In Prophet, E.B., Mills, B.,Arrington, J.B. and Sokin, L.H. (eds), Laboratory Methods inHistopathology. Armed Forces Institute of Pathology, Washington, DC,pp. 183–199.
Kaya, H. and Oral, B. (1999) Effect of ovarian involvement on the frequencyof luteinized unruptured follicle in endometriosis. Gynecol. Obstet. Invest.,48, 123–126.
Kerin, J.F., Kirby, C., Morris, D. et al. (1983) Incidence of the luteinizedunruptured phenomenon in cycling women. Fertil. Steril., 40, 620–626.
Nicosia, S.V. (1983) Morphological changes of the human ovary throughoutlife. In Serra, G.B. (ed.), The Ovary. Raven Press, New York, pp. 57–81.
Niswender, G.D. and Nett, T.M. (1988) The corpus luteum and its control. InKnobil, E. and Neill, J.D. (eds), The Physiology of Reproduction. RavenPress, New York, pp. 489–526.
Quatacker, J.R. (1971) Formation of autophagic vacuoles during human corpusluteum involution. Z. Zellforsch., 122, 479–487.
Rodger, F.E., Fraser, H.M., Duncan, W.C. et al. (1995) Immunolocalizationof bcl-2 in the human corpus luteum. Mol. Hum. Reprod., 1, 1566–1570.
Russell, D.L., Salamonsen, L.A. and Findlay, J.K. (1995) Immunizationagainst the N-terminal peptide of the inhibin α43-subunit (αN) disruptstissue remodeling and the increase in matrix metalloproteinase-2 duringovulation. Endocrinology, 136, 3657–3664.
Sawyer, H.R. (1995) Structural and functional properties of the corpus luteumof pregnancy. In Scaranuzzi, R.J., Nancarrow, C.D. and Doberska, C. (eds),Reproduction in Domestic Ruminants III. J. Reprod. Fertil., Dorset, 97–110.
Scully, R.E., Young, R.H. and Clement, P.B. (1996) Ovarian structure andfunction. In Rosai, J. and Skin, L.H. (eds), Tumors of the Ovary,Maldeveloped gonads, Fallopian tube and Broad ligament. Armed ForcesInstitute of Pathology, Washington, DC, pp. 1–212.

C.Morales et al.
Searle, J., Kerr, J.F.R. and Bishop, C.J. (1982) Necrosis and apoptosis: distinctmodes of cell death with fundamentally different significance. In Sommers,S. and Rosen, P.P. (eds), Pathology Annual. Appleton-Century-Crofts,Norwalk, pp. 229–260.
Shikone, T., Yamoto, M., Kokawa, K. et al. (1996) Apoptosis of humancorpora lutea during cyclic luteal regression and early pregnancy. J. Clin.Endocrinol. Metab., 81, 2376–2380.
Stouffer, R.L. and Brannian, J.D. (1993) The function and regulation of cellpopulations composing the corpus luteum of the ovarian cycle. In Adashi,E.Y. and Leung, P.C.K. (eds), The Ovary. Raven Press, New York,pp. 245–259.
Suzuki, T., Sasano, H., Takaya, R. et al. (1998) Leukocytes in normal-cyclinghuman ovaries: immunohistochemical distribution and characterization.Hum. Reprod., 13, 2186–2191.
Tsukada, T., Gordon, D., Ross, R. et al. (1987) HHF35, a muscle-actin-specific monoclonal antibody. I. Immunohistochemical and biochemicalcharacterization. Am. J. Pathol., 126, 51–60.
Wyllie, A.H. (1986) What is apoptosis? Histopathology, 10, 995–998.Yeldandi, A.V., Kaufman, D.G. and Reddy, J.K. (1996) Cell injury and cellular
adaptations. In Damjanov, I. and Linder, J. (eds), Anderson’s Pathology.Mosby, London, pp. 357–371.
Young, F.M., Illingworth, P.J., Lunn, S.F. et al. (1997) Cell death during lutealregression in the marmoset monkey (Callithrix jacchus). J. Reprod. Fertil.,111, 109–119.
Yuan, W. and Giudice, L.C. (1997) Programmed cell death in human ovaryis a function of follicle and corpus luteum status. J. Clin. Endocrinol.Metab., 82, 3148–3155.
Received on March 10, 2000; accepted on June 22, 2000
2128