Diet and Stress Reduction in Advanced Prostate Cancer GORDON A. SAXE, MD, PhD UNIVERSITY OF...
46
Diet and Stress Reduction in Advanced Prostate Cancer GORDON A. SAXE, MD, PhD UNIVERSITY OF CALIFORNIA, SAN DIEGO Rebecca and John Moores UCSD Cancer Center Dept. of Family and Preventive Medicin
-
Upload
reginald-lamb -
Category
Documents
-
view
217 -
download
0
Transcript of Diet and Stress Reduction in Advanced Prostate Cancer GORDON A. SAXE, MD, PhD UNIVERSITY OF...

Diet and Stress Reductionin Advanced Prostate Cancer
Diet and Stress Reductionin Advanced Prostate Cancer
GORDON A. SAXE, MD, PhD
UNIVERSITY OF CALIFORNIA, SAN DIEGO
Rebecca and John Moores UCSD Cancer Center
Dept. of Family and Preventive Medicine

Primary Research Question:Primary Research Question: Primary Research Question:Primary Research Question:
Can healthy dietary change, reinforced by stress reduction, slow or stop the progression of advanced prostate cancer?

RationaleRationale RationaleRationale
Prostate cancer is the most commonly occurring cancer (other than skin cancer) among men in the U.S.
In 1995, there were 244,000 new cases and 44,000 deaths from prostate cancer in the U.S.

RationaleRationale RationaleRationale
One in six men in the U.S. will develop invasive prostate cancer in his lifetime.
One in four African-American men will develop invasive prostate cancer.

RationaleRationale RationaleRationale
Following initial treatment, one in three patients will have a biochemical recurrence (marked by a rising PSA) within 10 years.
Biochemical recurrence implies that there is microscopic evidence of cancer that has spread beyond the prostate.

RationaleRationale RationaleRationale
One third of those with a biochemical recurrence will develop clinical evidence of metastatic disease within the subsequent five years.
No curative therapy exists for metastatic prostate cancer.

RationaleRationale RationaleRationale
Hormonal therapy can induce partial or complete remission and palliate symptoms.
However, its effects are only temporary, lasting an average of 18 – 24 months.

RationaleRationale RationaleRationale
Hormone therapy is also accompanied by unpleasant side-effects such as hot flashes, fatigue, impotence, gynecomastia, osteoporosis, and muscle loss.
As a result, patients with rising PSA after surgery tend to feel anxious and helpless in the face of their illness, a condition referred to as “PSA anxiety.”

RationaleRationale RationaleRationale
Risk factors for prostate cancer:
Male gender Age Heredity (genetic polymorphisms) Vasectomy Race Diet

International VariationInternational Variation
ChinaChina 1.3 1.3 perper 100,000 100,000
SwedenSweden 55.3 55.3 perper 100,000 100,000
United StatesUnited States 102.1 102.1 perper 100,000 100,000

RationaleRationale RationaleRationale
Epidemiological and laboratory evidence has associated specific dietary intakes with prostate cancer incidence, mortality, and possibly even disease progression:
Meat Dairy food Saturated fat

RationaleRationale RationaleRationale
Other dietary factors appear to be protective:
Whole grains Vegetables, especially cabbage family Tomatoes and other lycopene-rich foods Vitamin E, Selenium, and Zinc Green tea Soy foods (?)

RationaleRationale RationaleRationale
However, it is critical to promote stress reduction along with dietary change:
A major change in eating habits can be quite stressful.
Many of these patients are already suffering from “PSA anxiety.”
Stress reduction (such as meditation and yoga) may help patients to focus and make better dietary selections.

Primary Research QuestionPrimary Research Question Primary Research QuestionPrimary Research Question
Can healthy dietary change, reinforced by stress reduction, slow or stop the progression of advanced prostate cancer?

DefinitionsDefinitions DefinitionsDefinitions
Healthy dietary change: increased whole grains and vegetables, decreased saturated fat
Stress reduction: meditation, yoga, social support, mild exercise
Advanced prostate cancer: rising PSA on serial PSA tests after post-surgical PSA nadir

Findings from our Pilot StudyFindings from our Pilot Study Findings from our Pilot StudyFindings from our Pilot Study
“Can Diet in Conjunction with Stress Reduction Affect the Rate of Increase in Prostate Specific Antigen after Biochemical Recurrence of Prostate Cancer?”
Saxe GA, Hebert JR, Kabat-Zinn J, et al
Journal of Urology, 166(12): 2202-7, Dec., 2001

MethodsMethods MethodsMethods
Small non-randomized pilot study
Subjects (N=10) were men who had undergone radical prostatectomy and had subsequent rising PSA on serial tests
Pre/post study design with each subject serving as his own control

MethodsMethods MethodsMethods
Pre- vs. post-intervention rates of PSA increase and doubling times were compared.
Data also gathered on diet, physical activity, and body weight

InterventionIntervention InterventionIntervention
Group-based intervention consisting of a series of 12 weekly classes, with each class lasting 3-4 hours
Subjects were asked to be accompanied by a support person, preferably someone with whom they shared meals.

InterventionIntervention InterventionIntervention
Each class included a cooking demonstration, hands-on training in prostate-healthy meal preparation, and a didactic presentation on diet and health.
Classes also included formal instruction and practice in meditation and yoga (with subjects asked to practice daily at home).

ResultsResults ResultsResults
Signed rank test found significant reduction in the rate of PSA increase for the group as a whole (p=.01).

Results Results
Pre Post
Mean Slope 0.124
[0.076 - 0.173]
0.031
[0.012 - 0.075]
MedianDoubling Time 6.5 months
[3.7 - 10.1]
17.7 months
[7.8 -
95% C.I.
95% C.I.

ResultsResults ResultsResults
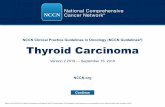
Eight out of ten subjects showed a decrease in their rates of PSA increase.

LogPSA
Subject #
-.3
-.2
-.1
0
.1
Change in PSA Slope
1 2 3 4 5 6 7 8 9 10
Figure 1. Change in PSA slopes (pre-study – post-study) by subject

ResultsResults ResultsResults
Three subjects had absolute reductions in their PSA levels.

Log
PSA
Subject #
1
0
-.1
.1
.2
.3
Pre-studySlope
Post-studySlope
2 3 4 5 6 7 8 9 10
Figure 2. PSA slopes, paired (pre-studyvs. post-study), by subject

Change in
PSA Slope
(log PSA)
Change in Fiber Intake (g/day)
-20.00 0.00 20.00 40.00
-0.30
-0.20
-0.10
0.00
0.10
Figure 3. Change in fiber intake as apredictor of change in PSA slope
Spearman = -.73, p=.02

Change in
PSA Slope
(log PSA)
Change in Exercise Level (mins./ day)
0.00 70.00 140.00
-0.30
-0.20
-0.10
0.00
0.10
Figure 4. Change in exercise level as apredictor of change in PSA slope
Spearman’s = -.60, p=.04

Change in
PSA Slope
(log PSA)
Change in Body Mass Index (kg/m2)
Spearman’s = .60, p=.04
-4.00 -3.00 -2.00 -1.00 0.00
-0.30
-0.20
-0.10
0.00
0.10
Figure 5. Change in body mass index asa predictor of change in PSA slope

ConclusionsConclusions ConclusionsConclusions
In this small sample we saw a significant reduction in the rate of increase in PSA in men with biochemically recurrent prostate cancer.
Major changes in diet and lifestyle were feasible in a relatively short period of time.

ConclusionsConclusions ConclusionsConclusions
An intervention of this type may provide a means for men with recurrent prostate cancer to slow the progression of their disease without adverse side effects while simultaneously improving their well being and quality of life.
These PSA results are promising and warrant further investigation through a larger multi-arm, randomized trial.

Current ResearchCurrent Research Current ResearchCurrent Research
“Diet and Stress Reduction in Recurrent Prostate Cancer”
Gordon A. Saxe, MD, PhD
Cheryl L. Rock, PhD, RD
Dan Mercola, MD, PhD
Carol Salem, MD

Differences with Pilot StudyDifferences with Pilot StudyDifferences with Pilot StudyDifferences with Pilot Study
Randomized trial (pilot was pre-post design)
Larger sample size (N=50)
Longer intervention period (6 months vs. 4)
More funding!!

Study DesignStudy DesignStudy DesignStudy Design
Subjects randomized to intervention or control status
Intervention subjects receive program similar to subjects in pilot study
Control subjects asked to maintain usual diet for 6 months and undergo same monitoring as those in intervention

Eligibility CriteriaEligibility CriteriaEligibility CriteriaEligibility Criteria
Biopsy-confirmed prostate cancer
Primary therapy consisting of surgery or radiation treatment
Rising PSA, documented on a minimum of three serial tests within a 12-month period, after achieving post-treatment nadir

Eligibility CriteriaEligibility CriteriaEligibility CriteriaEligibility Criteria
No use of hormone therapy within the last 12 months
No competing health conditions that would limit participation
Age 18 or older

MonitoringMonitoringMonitoringMonitoring
Occurs at baseline, 3 months, and 6 months post-baseline
Body weight assessment
Blood draws for PSA, plasma carotenoids, and other biomarkers of tumor metastasis

QuestionnairesQuestionnairesQuestionnairesQuestionnaires
Identifying and demographic data
Food frequency questionnaire
Physical activity recall

QuestionnairesQuestionnairesQuestionnairesQuestionnaires
Spielberg Anxiety Scale
Diet-related quality of life
FACT-P
SF-36

Data AnalysisData AnalysisData AnalysisData Analysis
Primary analysis will test the hypothesis that subjects in the intervention group will have a lower rate of increase in PSA than control subjects over the course of the 6-month intervention period
We will also test differences in mean PSA rates and doubling times between intervention and control subjects

Data Analysis:Data Analysis:Data Analysis:Data Analysis:
We will also examine:We will also examine:
– The effect of the intervention on quality of life
– Changes in other biomarkers of tumor metastasis
– Degree of dietary and lifestyle change by men in the intervention.

Eligibility CriteriaEligibility CriteriaEligibility CriteriaEligibility Criteria
Biopsy-confirmed prostate cancer
Primary therapy consisting of surgery or radiation treatment
Rising PSA, documented on a minimum of three serial tests within a 12-month period, after achieving post-treatment nadir

Eligibility CriteriaEligibility CriteriaEligibility CriteriaEligibility Criteria
No use of of hormone therapy within the last 12 months
No competing health conditions that would limit participation
Age 18 or greater

Contact Information:Contact Information: Contact Information:Contact Information:
GORDON A. SAXE, MD, PhD
UNIVERSITY OF CALIFORNIA, SAN DIEGO
Rebecca and John Moores UCSD Cancer Center
Dept. of Family and Preventive Medicine
Tel. (858) 622-1731, ext. 2233
Email: [email protected]

Sample Size ConsiderationsSample Size ConsiderationsSample Size ConsiderationsSample Size Considerations
N = 50 subjects (25 intervention, 25 control)
Based on following assumptions:
– Two-sided t-test– Mean PSA doubling time will increase by 100%
(from 245 days to 490 days) (pilot = 937 days)– Standard deviation = 227 days (same as pilot)– Alpha = .05– Study power = 80%– Dropout rate < 40%

Data AnalysisData AnalysisData AnalysisData Analysis
PSA doubling time is defined as:
PSA-DT = (ln2 [0.639]/slope)