Did the KDOKI–CKD Classification Corresponds to the Clinical ...
110
The National Kidney Foundation –KDIGO guidelines ( 2002-2013 KI Supl 3) Chronic Kidney Disease (CKD) Classification System CKD1 CKD2 CKD3 CKD4 CKD5 Kidney dammage : proteinuria, hematuria, sediment….imaging
Transcript of Did the KDOKI–CKD Classification Corresponds to the Clinical ...
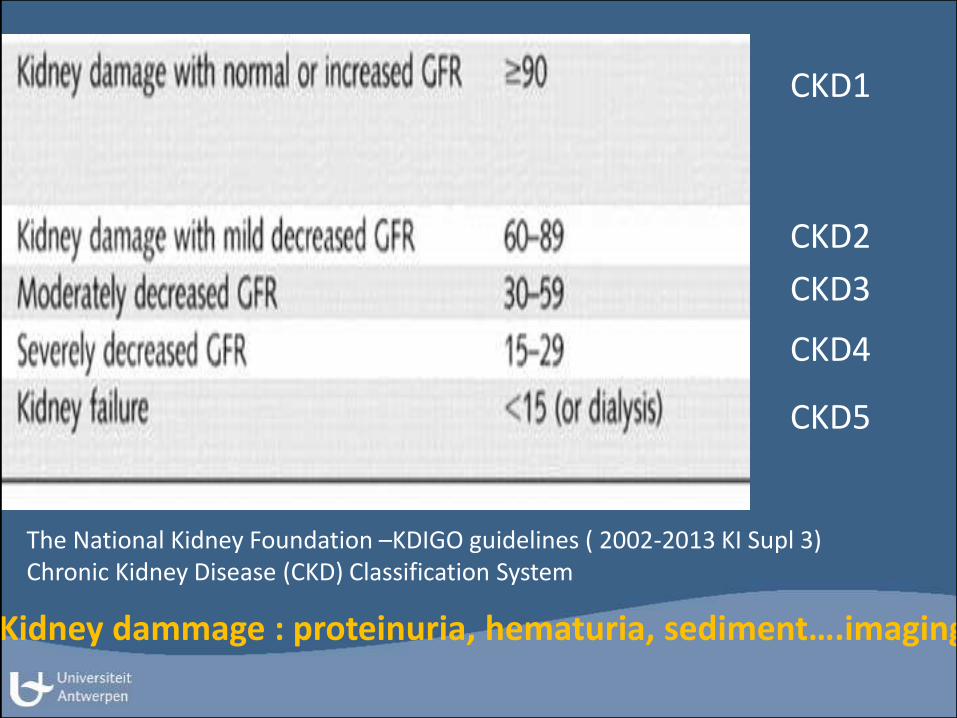
The National Kidney Foundation –KDIGO guidelines ( 2002-2013 KI Supl 3)Chronic Kidney Disease (CKD) Classification System
CKD1
CKD2
CKD3
CKD4
CKD5
Kidney dammage : proteinuria, hematuria, sediment….imaging

Chronic kidney disease awareness, prevalence, and
trends among U.S. adults, 1999 to 2000
Coresh J et al: JASN 16: 180-188, 2005

Hallan S J Jasn , 17 , 2275 , 2006
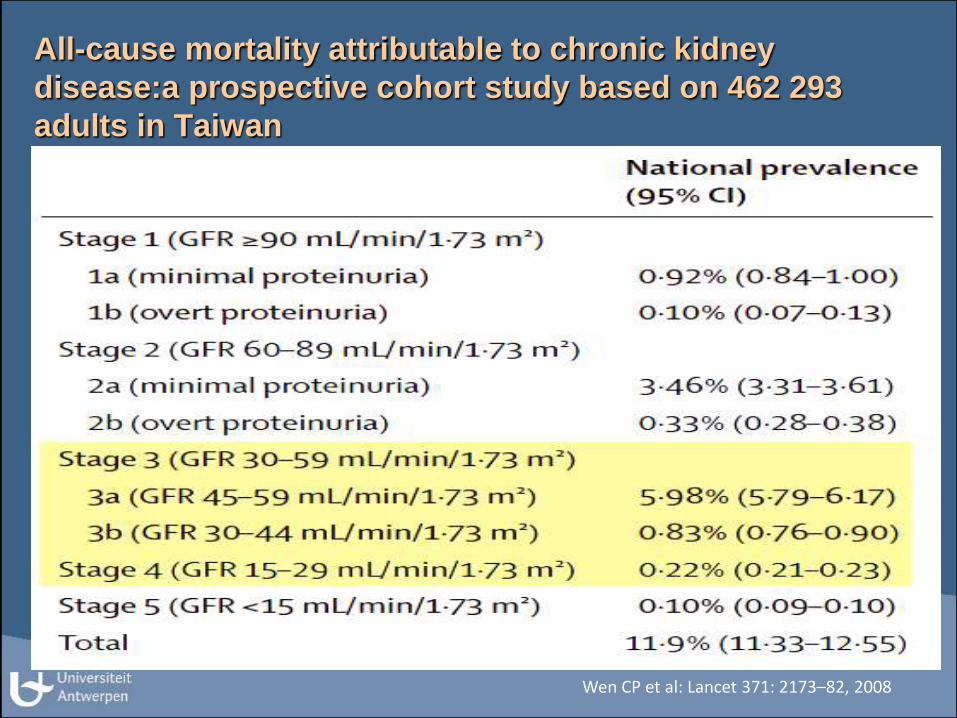
All-cause mortality attributable to chronic kidney
disease:a prospective cohort study based on 462 293
adults in Taiwan
Wen CP et al: Lancet 371: 2173–82, 2008

Prevalence of chronic kidney disease in China:
a cross-sectional survey
Zhang L et al: Lancet 379: 815–822, 2012

CKD IN MOROCCO: Early detection and intervention project
Prevalence of CKD in different studies around the
world according to the KDIGO staging guidelines.
CKD 1 and 2 GFR <90 , GFR 90-60 ml/min 1.73m2 AND
albuminuria
CKD 3-4-5 GFR < 60, 30 , 15 ml/min 1.73m2
• 1988-1994 1999-2000 Number
US adults 8.8% 9.4% 19,000,000JASN 2005
Taiwan 11.9% 2,000,000Wen,.. Lancet 2008 (11.3 – 12.5)
Mainland China 10.8% 140,000,000Zhang,.. Lancet 2012 (10.2 – 11.3)
Maremar 2.9-5.1% 750,000( 2014) manus (2015)
Single eGFR and no confirmed proteinuria exept Maremar

ESTIMATED PREVALENCE 3-42 (%)
20
McCullough et al N.D.T. 2012

An example of partnership
Maremar
“Maladies rénales au Maroc””

MAREMAR: Four main objectives
• To estimate the prevalence of CKD, hypertension obesitas ,diabetes in a representative randomized sample of the adult population of Morocco (26—70 years of age)
• To identify subjects at risk to develop CKD,
• To identify health related habits associated with an increased risk to develop CKD,
• To establish an intervention program for a follow-up period of 5 years.

Measurements:
• estimated Glomerular Filtration Rate (eGFR)
using the MDRD equation (Modification of Diet in Renal Disease)
• serum creatinine (Scr) using a methodology traceable to the Scr
reference system (NIST) (GC-IDMS). Quality control /monthly,in
case of hemolysis a new sample was analysed,chronicity
• microproteinuria (mPR) mild,using the Hemocue method and
nephelometry (quaility control), dipstick = > +
• macroproteinuria (MPR) overt, using dipstick (++ or more)
• on two morning midstream urine samples over 2-3 weeks
• fasting glycemia
NIST= National Institute of Standards and Technology
IDMS= isotope dilution mass spectrometry
transport systemfrom H.C. to lab within hours
KDIGO guidelines

CKD IN MOROCCO: Early detection and intervention project
Time schedule
• Jan – May 2008: discussion of the protocol (Ben Gharbi, M Elseviers, M DE Broe)
• June – Aug 2008: negotiation of the contract
• October 2008:
• ethical committee: approval of protocol
• official approval of the release of voters by Min. of Internal affairs,
Pasha of Khemmisset
• order for dipsticks, BP measurement, devices (Hemocue…)
• hardware – software
• 28 November 2008: Meeting in Marrakech of Internal Steering Committee
• Mid December 2008: training sessions of health care personnel
• January 2009: Pilot study in Khemisset
• February 2009: Start of the study in Khemisset
• May 2009: Start of the study in El JadidaVoters list

Based on this sample size, (10.000, 9%of adult population of the 2 towns) we expect to recruit:between 200 and 800 CKD patients (2-8% of screened population) with signs of renal impairment, needing further clinical investigations and appropriate treatment (28)between 2000 and 3000 patients (20-30% of screened population) with pathological findings (hypertension, diabetes and/or microalbuminuria) at risk to develop CKD, to whom a preventive treatment for 5 years (based on a prevalence of 20% hypertension and 6% diabetes in Morocco with or without microalbuminuria (29) ) will be offered.
between 1000 and 2000 subjects (10-20% of screened population) with two or more health related habits increasing the risk for the development of renal impairment, that will be invited for a new screening after 1, 3 and 5 years (29, 33-37))
With a total sample size of 10 000 participants, the 95% confidence interval for the observed prevalence of CKD will be lower than 1%. This means that, even with a CKD prevalence of e.g. 7,5%, we will be able to state with 95% confidence that the real prevalence will be not lower than 7% and not higher than 8%.

Sampling
KHEMISSET EL JADIDA
105 088 144 440 Population
26 – 70 years
Stratified random sample (9% of eligible people)
Sampling
5 000
46 553 67 309
5 000
Recruitment
Voters list
Period of six months

Sampling
5 health centers of screening/city in two cities
(40 subjects/week x25 weeks = 1000 /health center )
Stratified randomized
sample , voters list
1000 participants / centre
in total 10 health centers,
(HC) = 10,000 subjects
Sex
Age
M F
25-40 y N N
40-55 y N N
55-70 y N N
VOTERS LIST
• First list obtained after one year of negotiations was useless.(1999)
• Missing,wrong adressess
• Second updated list was given after the elections of 2009
• Second list turned out to be usefull

Centre de Santé Khemisset

Organization, training & monitoring
• 19 official meetings
• 10 education meetings, workshops and training sessions
• 38 local visits
• 88 people involved at different levels

Screening1st visit (Investigations)
Dipstick
Albuminuria
Glycemia
Creatininemia3X sitting
Understanding is essential

Screening2nd visit (1 week)
Confirmation of pathological findings
Dipstick > +
Microalbuminuria > 20mg/l
SAP>140 mmHg and/or DAP> 90 mmHg

illitaration rate: 30%
How to perform a midstream urine sample
Dirk De Weerdt

CKD IN MOROCCO: Early detection and intervention project
Recruitment: response rates
Response rates during the different phases of the Maremar recruitment procedure
Total number : n= 10524
at first visit

Recruitment
KHEMISSET EL JADIDA
Age KHEMISSET EL JADIDA Total26 – 40 years 1 832 1 674 3 50641 – 55 years 1 910 1 779 3 68956 – 70 years 1 725 1 604 3 329Total 5 467 5 507 10 524
07 December 2009 to 16 June 2010 17 May 2010 to 18 March 2011

Prevalence of hypertension(SAP ≥ 140 mmHg and/or DAP ≥ 90 mmHg)
16.7%
39.2%
20.3%
7.2%
0 10 20 30 40
All
56 - 70 years
41 - 55 years
26 - 40 years
%
Correction: based on the demographic structure of the populationHypertension confirmed in 1003/1458 cases

9
18,5
27,7
18,2
1,7
5,6
12,8
6,6
0,31,5
5,8
2,44,1
10,4
21,8
11,9
0
5
10
15
20
25
30
Stage I Stage II Stage III Systolic
26-40 years
41-55 years
56-70 years
All
Prevalence of hypertension stages by age (%)

Prevalence of obesity (BMI ≥ 30 kg/m²)
23.2%
25.9%
28.1%
18.3%
0 5 10 15 20 25 30
All
56 - 70 years
41 - 55 years
26 - 40 years
%

45,1
32,9
29,7
24,2
72,6
58,1
53,5
36,4
16
6,3
4,6
11,3
0 10 20 30 40 50 60 70 801, 2
or 3W
aist >
104
M, 8
0 FW
-H ra
tio >
1 M
, 0,8
5 F
BMI >
30
Male
Female
All
Prevalence of obesity markers
Health outcomes : no difference between men and woman

Prevalence of hyperglycemia ≥ 1.26g/l
13.8%
27.4%
18.2%
6.3%
0 5 10 15 20 25 30
All
56 - 70 years
41 - 55 years
26 - 40 years
%
Mean glycemia was 1.13 g/l (SD 0.49).
Corrected prevalence of glycemia between 1.00-1.25 g/l was 30.3%

Prevalences observed in the study population ,total group(n=10524), males (5122) , females (5402).

CKD IN MOROCCO: Early detection and intervention project
eGFR(MDRD) in the adult population of Morocco:
Gaussian distribution of three age categories
85.8% 13.7% 0.3% 0.3% 0%
70.2% 28.5% 0.9% 0.2% 0.1%
51.2% 42.1% 5.8% 0.4% 0.4%
CKD IN MOROCCO: Early detection and intervention project
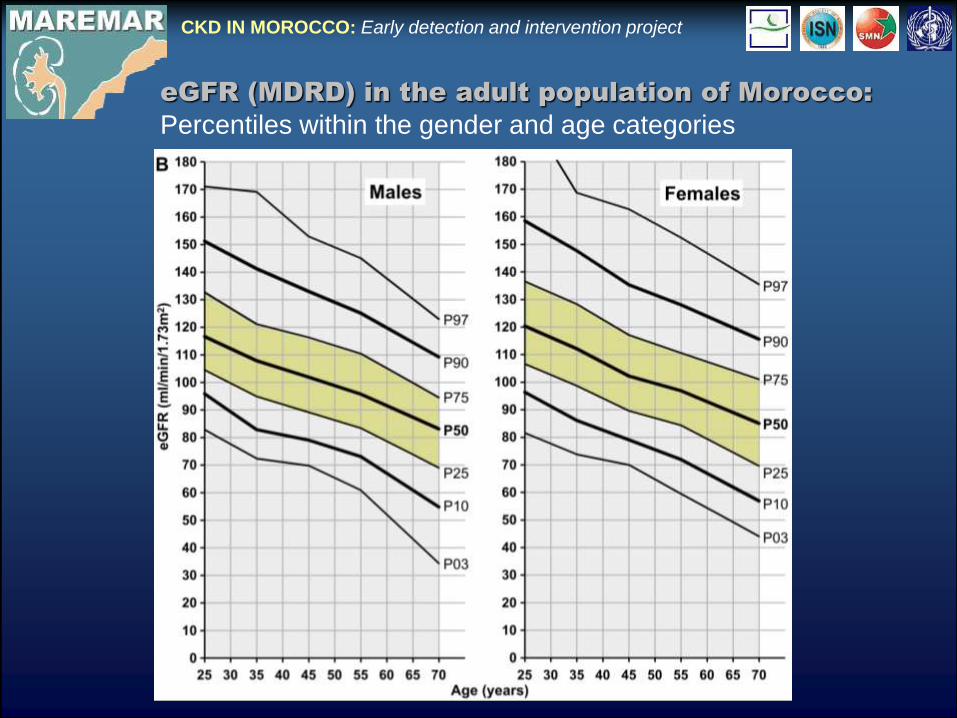
eGFR (MDRD) in the adult population of Morocco:
Percentiles within the gender and age categories


CKD IN MOROCCO: Early detection and intervention project
dipstick + = 67.2%; dipstick +/++ = 28.6% FALSE POSITIVE RESULTSfever, exercice, smoking,obesity,medication (Rosuvastatin),diet
KDIGO classification of eGFR and confirmed proteiniuria (mild, overt)

CKD IN MOROCCO: Early detection and intervention project
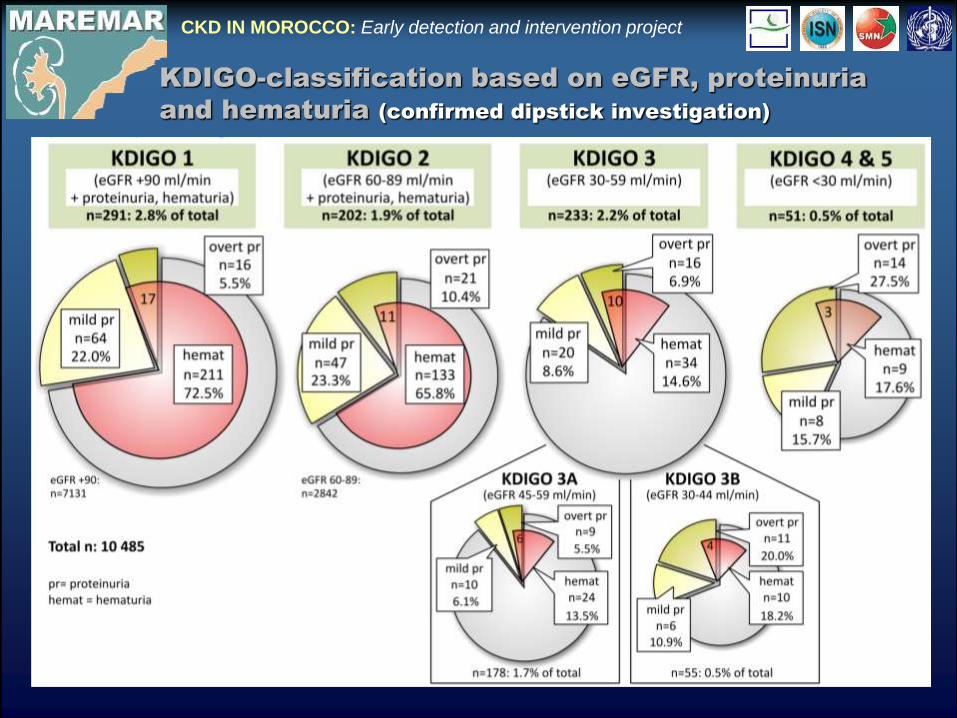
KDIGO-classification based on eGFR, proteinuria and
hematuria (confirmed dipstick investigation)

Changes in excretion of creatinine, plasma creatinine and creatinine clearance in healthy individuals at different ages
Stewart Cameron J & Macias-Nunez JF: 'Renal function in the elderly'in: Oxford Textbook of Clinical Nephrology, Oxford Med Publ 1998, pp 78-91
Percentiles of estimated GFR by age
Coresh et al: JASN 2005 : 16 , 180
eGFR-MDRD for men
Wetzels et al Kidney Int 2007 , 72, 632-637
Fall of GFR with age
Ferrari P. et al., NDT ; 2009 24, 1828
Interpretation of creatinine clearance
Elseviers MM, M E De Broe et al:. Lancet 1: 457,1987
N =12.000

CKD IN MOROCCO: Early detection and intervention project
CKD 1-2: n=153Total group eGFR >60: n=4971
CKD 1-2: n=260Total group eGFR >60: n=5269
eGFR – age (MDRD formula)
Overdiagnosed
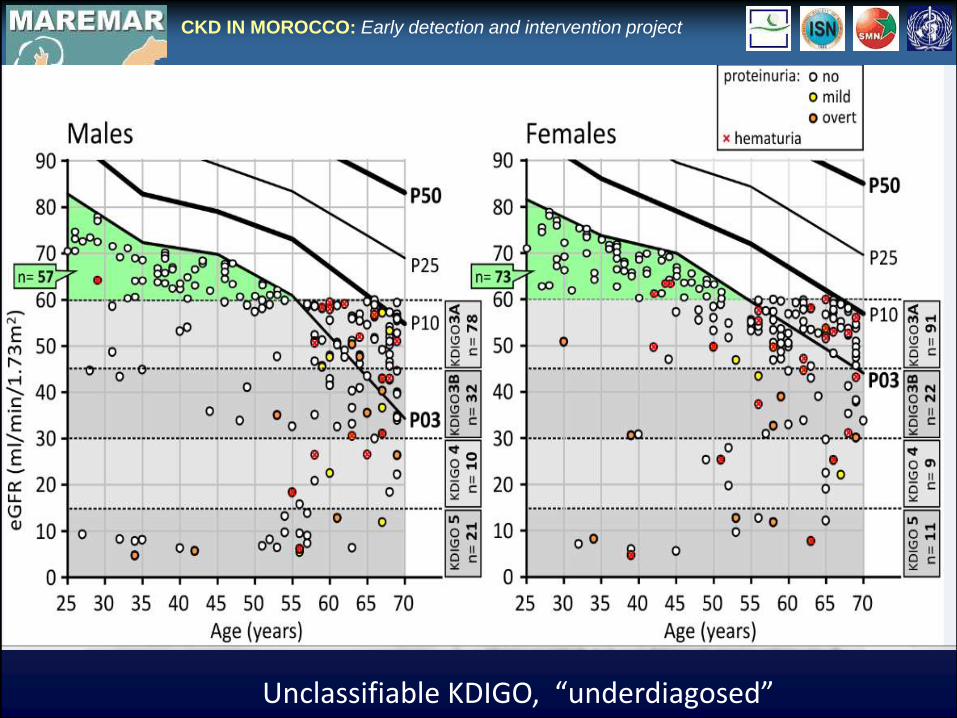
CKD IN MOROCCO: Early detection and intervention project
Unclassifiable KDIGO, “underdiagosed”

CKD 3, 4, 5,4 ,5
CKD1=44.9CKD2=52.8CKD3=60.3CKD4=60.6CKD5=49.2
AGE
Dutch population
Arab-Berber population
Wetzels et al Kidn InternWetzels et al Kidn. Intern 2007


Maremar manuscript submitted august 2015

Prevalence of CKD in different studies around the world according to the
KDIGO staging guidelines.
CKD 1 and 2 GFR <90 , GFR 90-60 ml/min 1.73m2 AND albuminuria
CKD 3-4-5 GFR < 60, 30 , 15 ml/min 1.73m2
• 1988-1994 1999-2000 Number
US adults 8.8% 9.4% 19,000,000JASN 2005
Taiwan 11.9% 2,000,000Wen,.. Lancet 2008 (11.3 – 12.5)
Mainland China 10.8% 140,000,000Zhang,.. Lancet 2012 (10.2 – 11.3)
Maremar 2.9-5.1% 750,000( 2014) manus (2015)
Single eGFR and no confirmed proteinuria exept Maremar

CKD IN MOROCCO: Early detection and intervention project
Belgium
Demography and CRF
Morocco
Prevalence of CRFeGFR< 60 ml/min/1.73m2
56-70y 6.6%
41-55y 1.3%
26-40y 0.5%
4.7%
population pyramids
1.6%

CKD IN MOROCCO: Early detection and intervention project
Low prevalence of CKD in Maremar
The second reason is the “overdiagnosing” due to investigation of proteinuria limited to the first screening time. Indeed in most published reports, dealing with epidemiology of CKD, confirmation of the proteinuria was not performed even in the those considered as of good quality
False positivity of urine analysis dipstick + 67;5%dipstick ++/+++ 28.7%
Many factors can influence protein/albumin excretion such as obesity, age, gender, distant inflammation, high blood pressure, remote infection and drug use (Rosuvastatine)
The third reason of “overdiagnosis” is : the MDRD equation has been demonstrated to systematically under-estimate to a certain extend renal function in healthy individuals

Proteinuria Dipstick Analysis• Confirmed False Positives
• First visit => + n= 513 (4.9%) 206 (1.9%)
• mild n= 408 (3.9% ) 139 (1.6%) 67.2%
• overt n= 105 (1.0%) 67 (0.3%) 28.7%
• False positive results using dipstick proteinuria : 59,8% in our study
population , mainly mild proteinuria
• Many factors however can influence protein/albumin excretion such as
obesity, age, gender, distant inflammation, high blood pressure, remote
infection and drug use (Rosuvastatin), excercise.
• Hooi LS, Ong LM, Ahmad G, Bavanandan S, Ahmad NA, Naidu BM. A population-based study
measuring the prevalence of chronic kidney disease among adults in West Malaysia. Kidney Int.
2013;84(5):1034-40. [PMID: 23760287] doi: 10.1038/ki.2013.220 :55% false + )• Qaseem A, Wilt TJ, Cooke M, Denberg TD. The paucity of evidence supporting screening for
stages 1-3 CKD in asymptomatic patients with or without risk factors. Clin J Am SocNephrol.
2014;9(11):1993-5. [PMID: 25237074] doi: 10.2215/CJN.02940314

CKD IN MOROCCO: Early detection and intervention project
McCullough et al N.D.T. 2012
Summary of the prevalence of CKD reported in high quality
studies (%; 95% CI)
nine best studies

Chronicity of eGFR measurement
False positives:CKD 3A: 32.2%CKD 3B: 7.4%
Clear improvement of accuracy

CKD IN MOROCCO: Early detection and intervention project
Assessment of CKD
CKD assessment based on eGFR
with proteinuria with proteinuria
and/or hematuria
1 eGFR ,+ unconfirmed proteinuria/hematuria 7.0% 14.0%
2 eGFR + confirmed proteinuria 4.2% 7.4%
3 Chronicity eGFR + conf. proteinuria/hematuria
(KDIGO 2013)3.9% 6.7%
3+ correction for total populations 2.9% 5.1%
Mild or overt proteinuria at first visit (n=513): 4.9% of study population
A false positive result was found in 67.2% of the subjects with mild proteinuria (+) and decreased substantially to 28.7% in subjects with overt (++/++++) proteinuria.mild or overt proteinuria at first visit: n= 513 4.9% of study populationconfirmed mild or overt proteinuria: n= 206 1.9% of study population
Chronicity of eGFR: The vast majority (75%) of false positives found in the subjects with CKD3A 32.2% had an eGFR exceeding 60ml/min/1.72m2.

CKD IN MOROCCO: Early detection and intervention project
Prevalence of CKD stages 1 to 4 as mean and
SD of 6 studies according to the KDOQI criteria
Prevalence rate of stage 3 is many times more common than CKD 4/5, suggesting that stage 3 CKD is not simply a stage in the evolution of CKD. It’s a stage that seldom progresses to kidney failure.
KDOQI CKD in our study: 6.6% corrected : 5.1%without hematuria : 3.9% corrected : 2.9%

LIMITATIONS of CKD DEFINITION in KDOQ - KDIGO
• Single absolute eGFR criterion unadjusted for normal decline in GFR
with age ,sex , leads to high prevalence of “false positive CKD and false
negatives “whenever used for diagnosis and treatment
• eGFR 60 -45 ml/mi/1.73m2 without proteinuria are not at greater risk of
CVD compared with eGFR greater than 60 ml/min and proteinuria
• Majority of living related or non related donors will be excluded ( are in
the US) when <60 ml/min is used as criterion of CKD
• Association of decreased and declining e GFR and increased risk of
CVD is steeper and more robust when eGFR is less than 45ml/min
(CKD 3b) and is GREATLY magnified by the presence of
PROTEINURIA
• In stage 3 of CKD representing almost 40-55% of the CKD population
the number that will PROGRESS to ESRD is estimated (measured) at
only 0.15 –0.2 % per year over 10-25 years. The vast majority of
these patients are younger that 60 years of age

Measures to Define Chronic Kidney Disease (CKD)
• A higher absolute risk and lower relative MORTALITY
risk in older versus younger adults with SIMILAR
levels of eGFR means that survival is generally more
limited at older ages and varies less as a funtion of
eGFR. O’Hare 2013
• FALSE NEGATIVES and FALSE POSITIVES
• Young and middle –aged adults with an eGFR of 60-74
ml/min/1.73m2 but WITHOUT proteinuria and whose life
expectancy is probably substantially shorter than those with
higher levels of eGFR , will NOT meet the criteria for CKD ,
whereas a large number of older adults with eGFR levels slightly
below 60ml/min/1.73m2 and no proteinuria , whose life
expectancy is probably similar to those with higher levels of
eGFR , WILL meet the criteria.
• O’Hare JAMA April 2013

REVISION of the CKD 3 definition in the KDOQI guidelines
• We favor to include the presence of kidney dammage as
manifested from an elevated albuminuria in stage CKD3 .
• Stage 1 and 2 CKD subjects with elevated albuminuria with a
fairly normal eGFR have a WORSE prognosis than the present
CKD3 subjects without elevated albuminuria.
• P De Jong ,R Gansevoort NDT, 23; 1092; 2008
• The risk of developing a CV event was NOT increased in subjects with
stage 3CKD without increasd albuminuria . In stage 3CKD subjects with
albuminuria was the CV risk elevated. P De Jong ,R Gansevoort NDT, 23; 1092; 2008
•
• For a given level of kidney function older adults have a clearly LOWER
risk of ESRD compared with younger adults
• M Tamura , W Winkelmayer JAMA June 2012 vol 307,

CONCLUSIONSMaremar demonstates that the choice of an arbritrary single threshold of eGFR for classifying CKD3-5 inevitably leads to “over-diagnosis “( false positives) of CKD in the elderly, particularly in those without proteinuria ,hematuria , hypertension. It also leads to “under-diagnosis” (false negatives ) of CKD in younger individuals with an eGFR above 60ml/min/1.73m2 and below the 3th percentile of their age and gender category
The use of a 3th percentile eGFR level as cut –off based on age and gender specific reference values of eGFR of the Moroccan population allows the detection of these false positives and negatives.
Lack of confirmation of increased proteinuria and absence of demonstration of ‘chronicity’ of
the decreased eGFR found at inclusion are the main reasons for the important inflation of the prevalence of CKD in the literature
Maremar demonstrates that the combination of population screening encompassing four different major health problems in the same screening procedure, using the correct methodologies and procedures, combined with a prevention and follow up program results in a clinically and scientifically relevant program.

Mohammed Ben Gharbi, Monique Elseviers, Mohammed Zamd

Pieter Bruegel (Antwerpen 1525-1569) The Blind leading the Blind

McCullough et al N.D.T. 27; 1812 ; 2012
MAREMAR : O O O, Proteinuria , confirmedHematuria , confirmed

MaReMar Baseline results, update December 2014
2014
Prevalences
Corrected prevalence according to the Moroccan population distribution:
x 0.78 (41-55y) and x 0,29 (56-70y)
Hypertension: confirmed BPsyst>140 or BPdiast>90
Diabetes: fasting glycemia>1,25
Obesitas: BMI>30
Proteinuria and Hematuria: confirmed dipstick analysis >= one cross positive
In case only confirmed proteinuria is taken into account KDOQI CKD : 3.0%
Observed
prevalence
Corrected
prevalence
26-40y 41-55y 56-70y
n=10524 n=3506 n=3689 n=3329
Hypertension 21,9% 7,2% 20,3% 39,2% 16,7%
Diabetes 16,8% 6,2% 17,8% 26,7% 13,4%
Obesitas 24,2% 18,3% 28,2% 25,9% 23,2%
KDOQI CKD 6,6% 3,0% 5,3% 12,0% 5,1%
eGFR<60 2,7% 0,5% 1,3% 6,6% 1.6%
Proteinuria 1,6% 0,9% 1,2% 2,7% 1,3%
Hematuria 3,4% 1,9% 3,3% 5,2% 2,4%
Observed prevalence
according to age


MDRD 4 variable equation for estimating eGFR from gender, age, ethnicity and plasma creatinine
MDRD equation:[1] Estimated GFR (ml/min/1.73m2) = 186 x (Creat / 88.4)-1.154 x (Age)-0.203 x (0.742 if female) x (1.210 if black)
http://www.patient.co.uk/doctor/estimated-glomerular-filtration-rate-gfr-calculator

CKD IN MOROCCO: Early detection and intervention project
CKD: Etiologies

The progression of chronic kidney disease: A 10-year population-based study
of the effects of genderand age
BO Eriksen and OC Ingebretsen Kidn Intern 2006; 69 ; 375 .
• The different prognoses of CKD stage 3 in identifiable subgroups make it
difficult to establish guidelines with a general approach to these patients.
• A patient with stable GFR may need more attention to an increased risk of
• cardiovascular disease, whereas patients with progressiev disease must also
be prepared for RRT.
• The present National Kidney Foundation Kidney Disease Outcomes
• Quality Initiative guidelines do not incorporate different approaches to
subgroups of the CKD population, presumably because the evidence base
has been lacking.This should be changed.
• Proteinuria is known to be associated with progressive disease.
• Although included in the definition of stages 1 and 2, definitions of the more
advanced stages have been made without taking proteinuria into account.
This needs to be reconsidered.

Using a single threshold GFR value, in the absence of any additional information such as urinary protein concentration, for the definition of CKD (Chronic Kidney Disease) is creating a huge number of false positives which among the “’Western “ populations goes up to 50% and according to recent papers even higher.
This leads to excessive futile use of health care resources.This puts a wrong label of a serious disease on individuals who will never consult a nephrologist or be treated by renal replacement techiques and will die of CV diseases.
Such a uncorrect CKD label has many untoward and undesirable effects , such as unnecessary anxiety , unneeded additional investigations and loss of insurabillity
It creates a non-negligible number of false negatives at younger ages. Younger individuals who are in urgent need to be seen by a nephrologist. We all known how silent a renal disease may progress and early detection is of paramount importance..
CKD IN MOROCCO: Early detection and intervention project
“Reduced/ impaired kidney function “ would be established by the finding of an eGFR less than fifth (or less) percentile for healty individuals of similar age, gender, and ancestry without proteinuria/hematuria.
CKD has the same definition plus the presence of dipstick positivity or increased ACR and or “renal” hematuria

LIMITATIONS of CKD DEFINITION in KDOQ - KDIGO
• Single absolute eGFR criterion unadjusted for normal decline in GFR
with age ,sex , leads to high prevalence of “false “ positive CKD and
false negatives whenever used for diagnosis and treatment
• eGFR 60 -45 ml/mi/1.73m2 without proteinuria are not at greater risk of
CVD compared with eGFR greater than 60 ml/min and proteinuria
• Majority of living related or non related donors will be excluded ( are in
the US) when <60 ml/min is used as criterion of CKD
• Association of decreased and declining e GFR and increased risk of
CVD is steeper and more robust when eGFR is less than 45ml/min
(CKD 3b) and is GREATLY magnified by the presence of
PROTEINURIA
• In stage 3 of CKD representing almost 40-55% of the CKD population
the number that will PROGRESS to ESRD is estimated (measured) at
only 0.15 –0.2 % per year over 10-25 years. The vast majority of
these patients are younger that 60 years of age
SCREEN or NOT to SCREEN the GENERAL ADULT POPULATION
• Maremar found 16.7 hypertension; 13.4% diabetes type 2; 23.3% of obesitas and 5.1% of KDOQI CKD in the general adult population (25-70 years of age) in Morocco .More than 50% of the subjects were unaware of their diseases
• Subjects with one of these diseases or CKD stage were followed up and appropriate treatment was installed if necessary
• The results of Maremar have been implemented in the teaching program of the faculties of medicine in the country at master and post graduate level .
• At institutional level the Maremar model (kidney, hypertension, diabetes, CV diseases screening ) is planned to be implemented in the “centres de santé “ throughout the country.
• Screening of the adult population in Morocco within the frame of the methodology used in Maremar was highly relevant

CONCLUSIONS
MAREMAR is a prevalence study of hypertension, diabetes,obesitas KDIGO
CKD of a randomized ,stratified , representative sample of the adult
population of Morocco.
The relative low level of KDIGO CKD prevalence in Morocco has to do with the
structure of the population pyramid and the fact that, in contrast with our
study, almost all prevalence studies have NOT confirmed proteinuria-
hematuria and NOT proven the chronicity of the CKD stage (false positives)
The CKD3a group without proteinuria ( 30% of CKD population) should be
renamed ‘impaired kidney function’(IKF) and NOT CKD . Dose adaptation in
prescribing nephrotoxic drug.

CONCLUSIONS
eGFR percentiles within gender- age categories, and NOT a SINGLE threshold GFR value, should be used. Improved accuracy and much less false+ and -
Screening for hypertension , diabetes, obesitas, and KDIGO CKD linked to a diagnostic –therapeutic follow up and implementation into the CV of the medical schools, makes screening of the adult population highly relevant.
There is a need for other quality studies on the prevalence of CKD using the appropriate methodologies and confirmation of the findings in time according to the KDIGO guidelines (confirmation of proteinuria. , hematuria…. , chronicity of CKD)

Urinary analysis
Blood analysis & drugs
Analyzers
Equipment & software
Printing
Workload
Meetings & Training
NB: not included expertise, workload, supervision and travel costs
of principal investigators who are involved on a voluntary basis.
Financial aspects Phase of recruitment and screening

Steering Committee
- A. Belghiti Alaoui- R. Bayahia
- M. Benghanem Gharbi
- A. Bitane
- M. De Broe
- E. El Haroudi
- O. Elmenzhi
- B. Ramdani
- S.S. Youssef
Scientific Committee
- M. De Broe
- M. Benghanem Gharbi- M. Arrayhani
- R. Bayahia
- A. Belghiti Alaoui
- N. Benahadi
- S.S. El Khayat
- O. Elmenzhi
- M. Elseviers - B. Ramdani
- E. Trabelssi
- M. Zamd
Who is who
Docters, nurses , administrative personnel of the health centers

Sarlingyi, Burma

Maremar poster ASN 2012 eGFR
Whether early identification and treatment of subjectswith “reduced” levels of GFR within the normal range for their age/gender, but without any other manifestations of kidney disease, will reduce the subsequent risk of cardiovascular events or progression to end-stage-renal disease is
currently unproven
Screening for CKD with eGFR. Doubts and DangersRichard J. Glassock and Christopher WinearlsClin J Am Soc Nephrol 3: 1563–1568, 2008

Gansevoort et al 2012 Lancet

MaReMar Baseline results, February 2012
Renal failure
Khemisset El Jadida
numbers corrected %
age 26-40 0,2% 1,0% 19/3487 19/3487 0,5%
age 41-55 1,3% 1.2% 47/3678 37/2869 1,3%
age 56-70 5,9% 7.4% 220/3320 64/963 6,6%
TOTAL 2,4% 3.1% 286/10485 120/7319 1.6%
TOTAL
RENAL FAILURE (GFR<60)
Correction: based on the demographic structure of the adult population (25-70years)
n= 29.608.009 , 50.1% female
Age 41-55: correction factor 0.78 (size of this population is only 78% of group 1)
Age 56-70: correction factor 0.29 (size of this population is only 29% of group 1)
(magic KDOQI number)

Definition of CKD
One or more of the following symptoms: - eGFR (MDRD) < 60 ml/min/1.73 m² , (confirmed)- Macroalbuminuria ≥ 200 mg/L, (confirmed)- Diabetes type I with microalbuminuria between
20-199 mg/L (confirmed)- Dipstick investigation showing more than one
cross positive (after confirmation) for proteins or blood. (confirmed)

Conclusion
• MaReMar generated, for the first time in Morocco, quantitative and scientifically correct information on the prevalence of CKD Hypertension, Obesitas, Diabetes, Risk Habits
• This information is highly relevant for future national health strategies.

z
Ishani et al JASN 2006, 17, 1444-1452
prot ++/+++
prot +
eGFR <60ml/mn
eGFR 60-75 ml/m

LIMITATIONS of CKD DEFINITION in KDOQ - KDIGO
• Single absolute eGFR criterion unadjusted for normal decline in GFR
with age ,sex ,will lead to high prevalence of “false “ positive CKD
whenever used for diagnosis and treatment
• eGFR below 60 ml/min without proteinuria are not at greater risk of CVD
compared with eGFR greater than 60 ml/min
• Majority of living related or non related donors will be excluded ( are in
the US) when <60 ml/min is udsed as criterion of CKD
• Association of decreased and declining e GFR and increased risk of
CVD is steeper and more robust when eGFR is less than 45ml/min
(CKD 3b) and is GREATLY magnified by the presence of
PROTEINURIA
• In stage 3 of CKD representing almost 40-55% of the CKD population
the number that will PROGRESS to ESRD is estimated (measured) at
only 0.15 –0.2 % per year over 10-25 years. The vast majority of
these patients are younger that 60 years of age
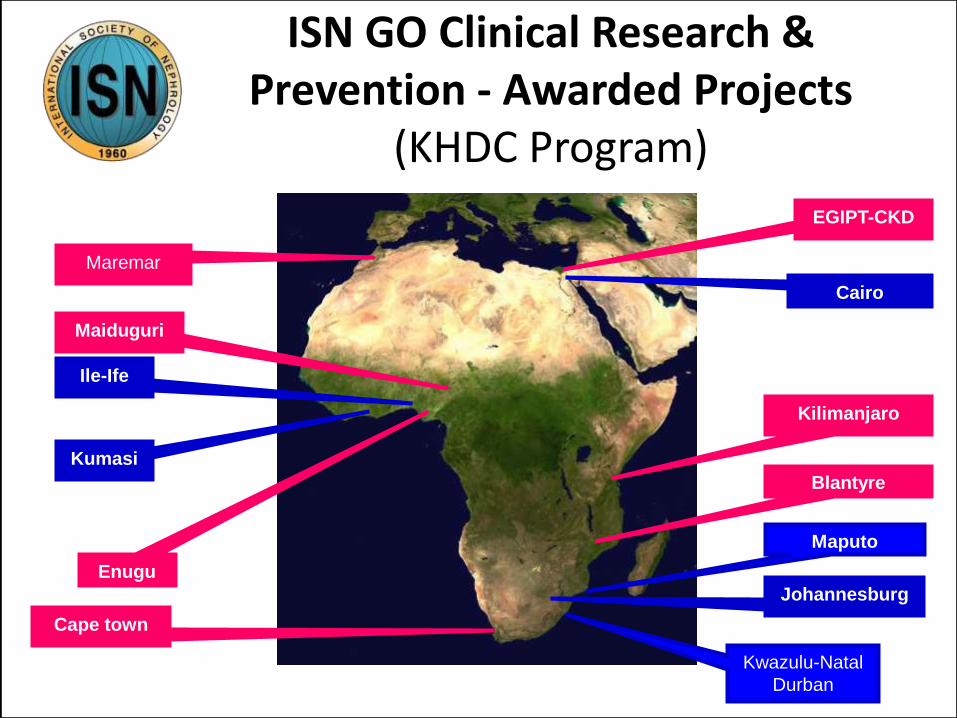
ISN GO Clinical Research & Prevention - Awarded Projects
(KHDC Program)
Maremar
EGIPT-CKD
Enugu
Maiduguri
Kwazulu-Natal
Durban
Maputo
Cape town
Blantyre
Cairo
Ile-Ife
Kumasi
Kilimanjaro
Johannesburg

MaReMar Baseline results, February 2012
Renal function:
DOQi and dipstick positive
GFRdoqi
90 plus 60-89 30-59 15-29 15 min Total
% % % % % %
albumine no albuminuria 68,84 27,41 2,00 0,13 0,22 98,60
macroalbuminuria 0,53 0,49 0,24 0,05 0,09 1,40
Total 69,38 27,90 2,24 0,18 0,31 100,00
number 7274 2925 235 19 32 10 485
GFRdoqi and macroalbuminuria (confirmed dipstick >= ++)

MaReMar Baseline results, February 2012
Pre-diabetes and diabetes
Khemisset El Jadida
numbers corrected %
age 26-40 20,9% 33,5% 939/3490 939/3490 26,9%
age 41-55 30,2% 36,0% 1214/3679 947/2870 33,0%
age 56-70 33,6% 35,7% 1149/3320 333/963 34,6%
TOTAL 28,2% 35,1% 3302/10489 2219/7323 30,3%
Khemisset El Jadida
numbers corrected %
age 26-40 5,9% 6,8% 221/3490 221/3490 6,3%
age 41-55 16,4% 20,1% 669/3679 522/2870 18,2%
age 56-70 23,8% 31,2% 909/3320 264/963 27,4%
TOTAL 15,2% 19,2% 1799/10489 1007/7323 13,8%
PREDIABETES (glycemie 1-1.24)
TOTAL
TOTAL
DIABETES (glycemie>1.25)
Correction: based on the demographic structure of the population
Age 41-55: correction factor 0.78 (size of this population is only 78% of group 1)
Age 56-70: correction factor 0.29 (size of this population is only 29% of group 1)
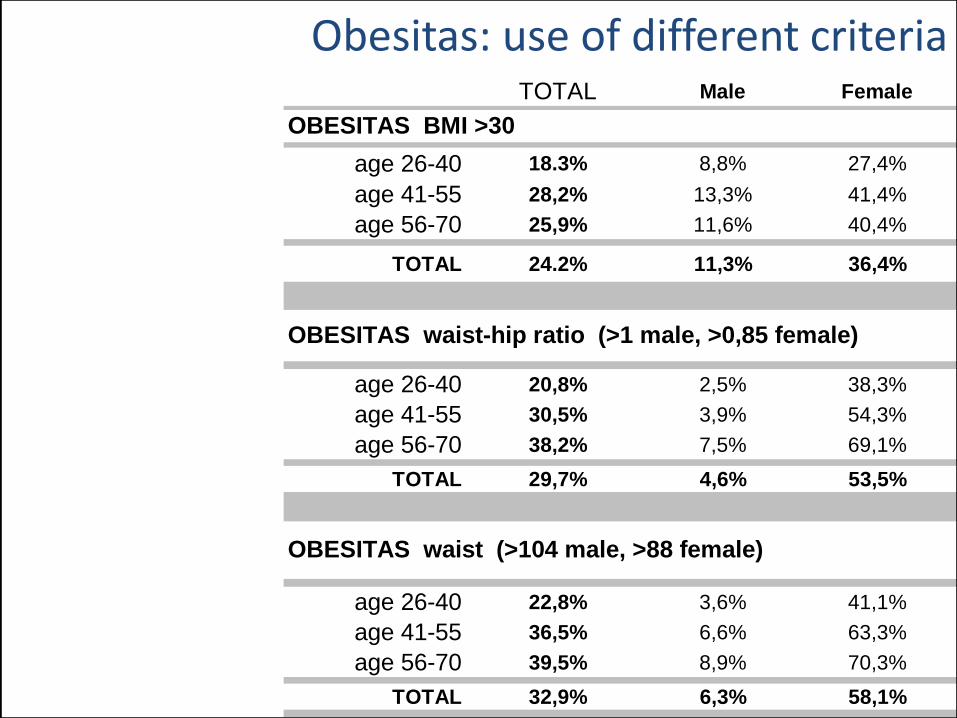
Obesitas: use of different criteriaTOTAL Male Female
age 26-40 18.3% 8,8% 27,4%
age 41-55 28,2% 13,3% 41,4%
age 56-70 25,9% 11,6% 40,4%
TOTAL 24.2% 11,3% 36,4%
age 26-40 20,8% 2,5% 38,3%
age 41-55 30,5% 3,9% 54,3%
age 56-70 38,2% 7,5% 69,1%
TOTAL 29,7% 4,6% 53,5%
age 26-40 22,8% 3,6% 41,1%
age 41-55 36,5% 6,6% 63,3%
age 56-70 39,5% 8,9% 70,3%
TOTAL 32,9% 6,3% 58,1%
OBESITAS waist-hip ratio (>1 male, >0,85 female)
OBESITAS waist (>104 male, >88 female)
OBESITAS BMI >30

SCREEN or NOT to SCREEN the GENERAL ADULT POPULATION
• Maremar found 16.7 hypertension, 13.4% diabetes type 2, 23.3% of
obesitas and 5.1% of KDOQI CKD in the general adult population (25-70
years of age) in Morocco .More than 50% of the subjects were unaware
of their diseases
• Subjects with one of these diseases or CKD stage were followed up and
appropriate treatment was installed if necessary
• The results of Maremar have been implemented in the teaching program
of the faculties of medicine in the country at master and post graduate
level .
• At institutional level the Maremar model (kidney, hypertension, diabetes,
CV diseases screening ) is planned to be implemented in the “centres
de santé “ throughout the country.
• Screening of the adult population in Morocco within the frame of the
methodology used in Maremar was highly relevant

Screening for CKD with eGFR. Doubts and Dangers
Richard J. Glassock and Christopher Winearls
Clin J Am Soc Nephrol 3: 1563–1568, 2008
• Whether early identification and treatment of subjects
• with “reduced” levels of GFR within the normal range
for their age/gender, but without any other
manifestations of kidney disease, will reduce the
subsequent risk of cardiovascular events or
progression to end-stage-renal disease is
• currently unproven

MaReMar Baseline results, revision Augustus 2014
Tabel Hematuria
HematuriaDipstick:
FirstInvestigation
N=10 430
ConfirmedHematuriaN=10 430
0 9509 (91,2%)
+ 593 (5,7%) 216 (2,0%)
++ 245 (2,3%) 123 (1,2%)
+++ 83 (0,8%) 20 (0,2%)
Hematuria>= +
921 (8,8%) 359 (3,4%)
MaReMar Baseline results, revision Augustus 2014
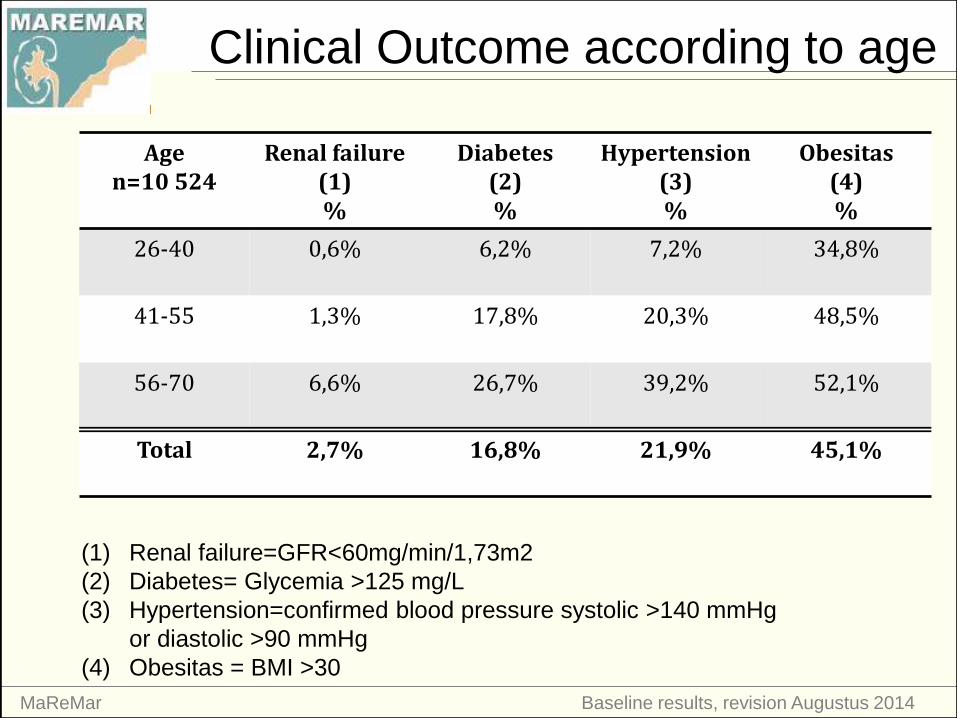
Clinical Outcome according to age
Agen=10 524
Renal failure (1)%
Diabetes(2)%
Hypertension(3)%
Obesitas(4)%
26-40 0,6% 6,2% 7,2% 34,8%
41-55 1,3% 17,8% 20,3% 48,5%
56-70 6,6% 26,7% 39,2% 52,1%
Total 2,7% 16,8% 21,9% 45,1%
(1) Renal failure=GFR<60mg/min/1,73m2
(2) Diabetes= Glycemia >125 mg/L
(3) Hypertension=confirmed blood pressure systolic >140 mmHg
or diastolic >90 mmHg
(4) Obesitas = BMI >30

MaReMar Baseline results, revision Augustus 2014
Renal Failure
GFRdoqi
90 plus 60-89 30-59 <30 Total
% % % % %
albumine no proteinuria (n=10088) 98,90 97,60 86,80 66,70 98,40
mild proteinuria (n=101) 0,80 1,60 6,80 7,80 1,00
overt proteinuria (n=63) 0,30 0,80 6,40 25,50 0,60
Total 69,6 27,7 2,2 0,5 100,00
number 7131 2842 228 51 10252
GFRdoqi and proteinuria (confirmed dipstick investigation)
Nieuwe figuur aangevraagd (zoals screen 83)
op basis van deze algemene cijfers

MaReMar Baseline results, revision Augustus 2014
Hypertension and proteinuria
No hypertension:
0,8% mild and 0,3% overt proteinuria (confirmed)
Hypertension:
1,6% mild and 1,7% overt proteinuria (confirmed)







MaReMar Baseline results, update Maart 2015
Age and gender per CKD class
CKD n %
age
mean (SD)
Gender
% M/F
NO CKD 9788 93,4 46,9 (11,9) 49-51
90 plus 245 2,3 48,6 (11,4) 36-64
60-89 168 1,6 55,3 (10,0) 39-61
45-59 178 1,7 60,7 (7,5) 49-51
30-44 55 ,5 60,2 (10,2) 60-40
15-29 19 ,2 60,8 (6,7) 53-47
min 15 32 ,3 49,2 (11,3) 66-34
total 10485 100,0 47,5 (12,0) 49-51

Follow-up CKD3 subjects KhemissetJanuary 2010 – January 2014

Follow-up CKD3 subjects KhemissetJanuary 2010 – January 2014

Follow-up CKD3 subjects KhemissetJanuary 2010 – January 2014


Comparison Hemocue - Nephelometry (UZA)
University of Antwerp, Laboratory of Pathophysiology

2. Sample size calculation
In November 2004, the population of the two towns, was as follows:El Jadida: Total : 144,440 inhabitants ; 26-70 years old: 67,309 Khemisset: Total 105,088 inhabitants ; 26-70 years old: 46,553
A total of 113,862 subjects are eligible to participate in the screening program.
Recruitment will be performed in a period of 6 months based on the assumption that 8 subjects will be screened per working day in each of the 5 health care area’s per town, making a total of 40 subjects per area per week. Recruitment during 25 weeks will result in 1000 subjects per area multiplied by 5 area’s in each town giving a total sample size of 2x 5000 (10,000)participants (approximately 9% of the eligible population). Sampling will take into account that a non-response rate between 20 and 40% can be expected.

MaReMar Baseline results, revision Augustus 2014

CKD IN MOROCCO: Early detection and intervention project
eGFR – age (MDRD formula)

Recrutement




Mohammed Ben Gharbi, Monique Elseviers, Mohammed Zamd

Steering Committee
- A. Belghiti Alaoui- R. Bayahia
- M. Benghanem Gharbi
- A. Bitane
- M. De Broe
- E. El Haroudi
- O. Elmenzhi
- B. Ramdani
- S.S. Youssef
Scientific Committee
- M. De Broe
- M. Benghanem Gharbi- M. Arrayhani
- R. Bayahia
- A. Belghiti Alaoui
- N. Benahadi
- S.S. El Khayat
- O. Elmenzhi
- M. Elseviers - B. Ramdani
- E. Trabelssi
- M. Zamd
Who is who

Table 2: Prevalences according to age categories and adult population of Morocco.
Observed
prevalence
Observed prevalence according to age Corrected prevalence according to the Moroccan
population
26-40y 41-55y 56-70y
n=10,524 n=3506 n=3689 n=3329 95% CI
Hypertension 21.9% 7.2% 20.3% 39.2% 16.7% 16.0-17.4
Diabetes 16.8% 6.2% 17.8% 26.7% 13.4% 12.8-14.1
Obesitas 24.2% 18.3% 28.2% 25.9% 23.2% 22.4-24.0
CKD 6.7% 3.0% 5.3% 12.0% 5.1% 4.7-5.5
eGFR<60 2.7% 0.5% 1.3% 6.6% 1.6% 1.4-1.8
Proteinuria 1.6% 0.9% 1.2% 2.7% 1.3% 1.1-1.5
Hematuria 3.4% 1.9% 3.3% 5.2% 2.4% 2.1-2.7
Corrected prevalence according to the Moroccan population distribution: x 0.78 (41-55y) and x 0,29 (56-70y)
Hypertension: confirmed BP syst>140 mmHg or BPdiast>90mmHG
Diabetes: glycemia>1,25g/l
Obesitas: BMI>30
Proteinuria and hematuria: confirmed => one cross positive

MaReMar Baseline results, revision Augustus 2014

CKD IN MOROCCO: Early detection and intervention project
CONCLUSIONSMaremar demonstates that the choice of an arbritrary single threshold of eGFR for classifying CKD3-5 inevitably leads to “over-diagnosis “( false positives) of CKD in the elderly, particularly in those without proteinuria ,hematuria , hypertension. It also leads to “under-diagnosis” (false negatives ) of CKD in younger individuals with an eGFR above 60ml/min/1.73m2 and below the 3th percentile of their age and gender category
The use of a 3th percentile eGFR level as cut –off based on age and gender specific reference values of eGFR of the Moroccan population allows the detection of these false positives and negatives.Lack of confirmation of increased proteinuria and absence of demonstration of ‘chronicity’ of the decreased eGFR found at inclusion are the main reasons for the important inflation of the prevalence of CKD in the literature
Maremar demonstrates that the combination of population screening encompassing four different major health problems in the same screening procedure, using the correct methodologies and procedures, combined with a prevention and follow up program results in a clinically and scientifically relevant program.
CKD IN MOROCCO: Early detection and intervention project
KDIGO-classification based on eGFR, proteinuria
and hematuria (confirmed dipstick investigation)