
Diapositiva 1 - Altervista · La teoria umorale di Ippocrate fu ulteriormente supportata da Galeno,...
71
-
Upload
duongthien -
Category
Documents
-
view
219 -
download
0
Transcript of Diapositiva 1 - Altervista · La teoria umorale di Ippocrate fu ulteriormente supportata da Galeno,...





Da dove veniamo?
Dove andiamo?

Edwin Smith (1822-1906) Papyrus, ca. 1500 a.C. lungo circa 4,5 metri e largo 33 centimetri
Descrive 8 casi di tumori o ulcere della mammella che erano trattati con la cauterizzazione utilizzando una “punta di fuoco”
Galeno di Pergamo (129-216 d.C.)
La teoria umorale di Ippocrate fu ulteriormente supportata da Galeno, e ha dominato per tutto il Medioevo. Galeno attribuiva l’origine del tumore mammario ad una sorta di “melanconia morbosa” e consigliava il trattamento con diete specifiche.

Dal 476 d.C. la medicina diventa appannaggio quasi esclusivo dei religiosi, soprattutto di alcuni ordini monastici, in particolare benedettini. La malattia è considerata una punizione divina e quindi la sua guarigione può essere ottenuta non con le cure ma con le preghiere, dirette al Santo protettore: S. Agata per la mammella, S. Biagio per la gola, S. Lucia per gli occhi, ecc. Al più si può ricorrere a blande terapie dietetiche e fisiche, o all’erboristeria utilizzando estratti delle piante officinali.
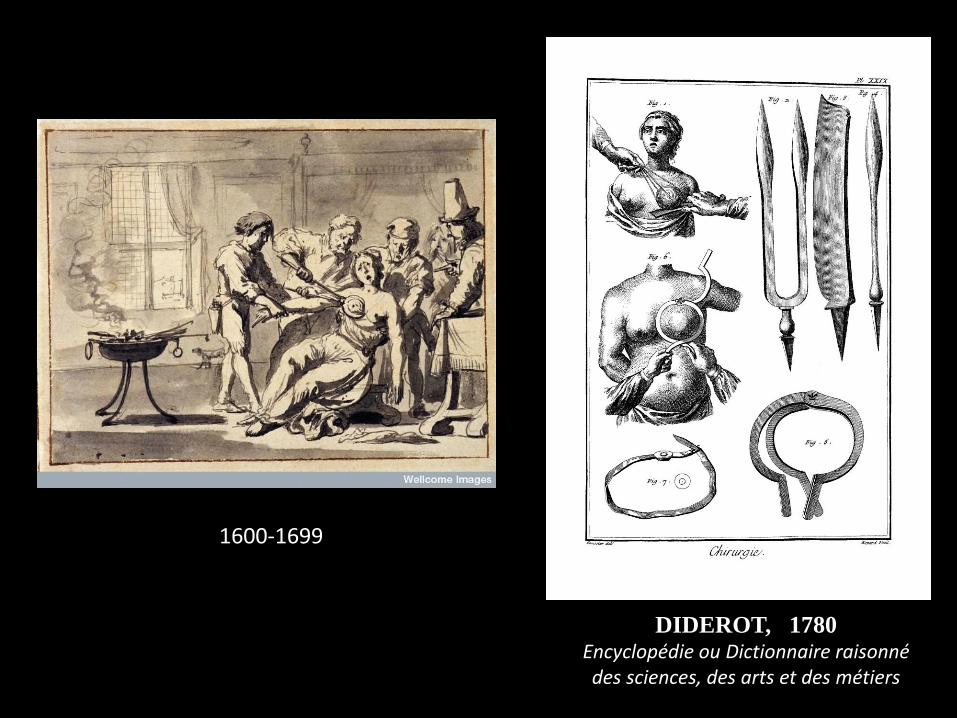
DIDEROT, 1780 Encyclopédie ou Dictionnaire raisonné des sciences, des arts et des métiers
1600-1699
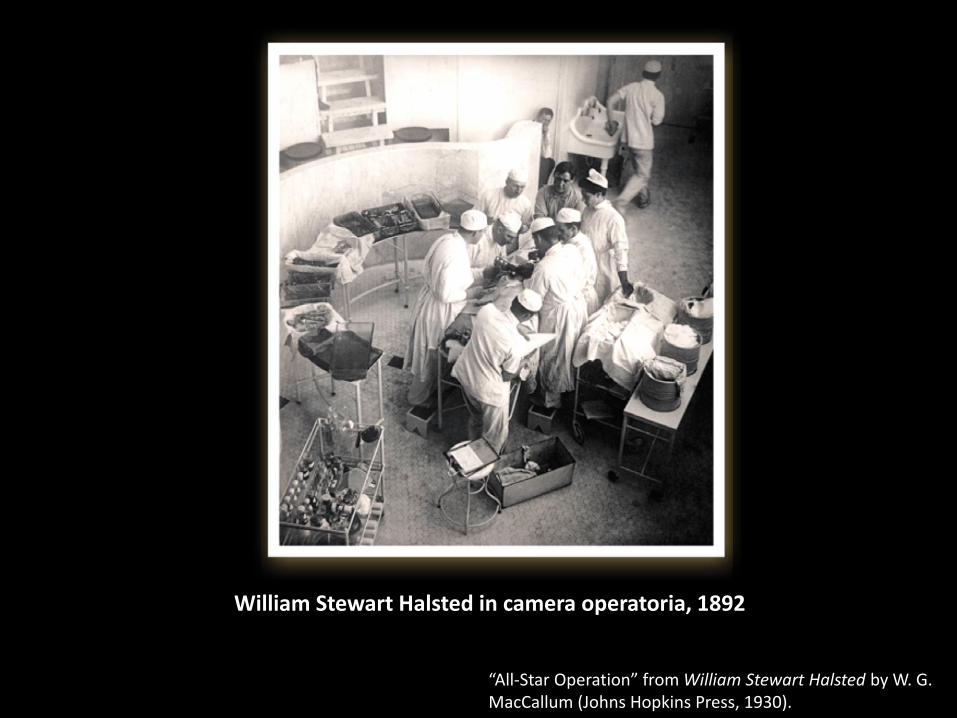
William Stewart Halsted in camera operatoria, 1892
“All-Star Operation” from William Stewart Halsted by W. G. MacCallum (Johns Hopkins Press, 1930).

Nel 1894 W. S. Halsted
pubblica i primi risultati ottenuti trattando il carcinoma della mammella con l’intervento di
MASTECTOMIA RADICALE
asportazione in blocco della mammella, dei muscoli pettorali e dei linfonodi ascellari
The Johns Hopkins Hosp. Rep.:
4, 297, 1894

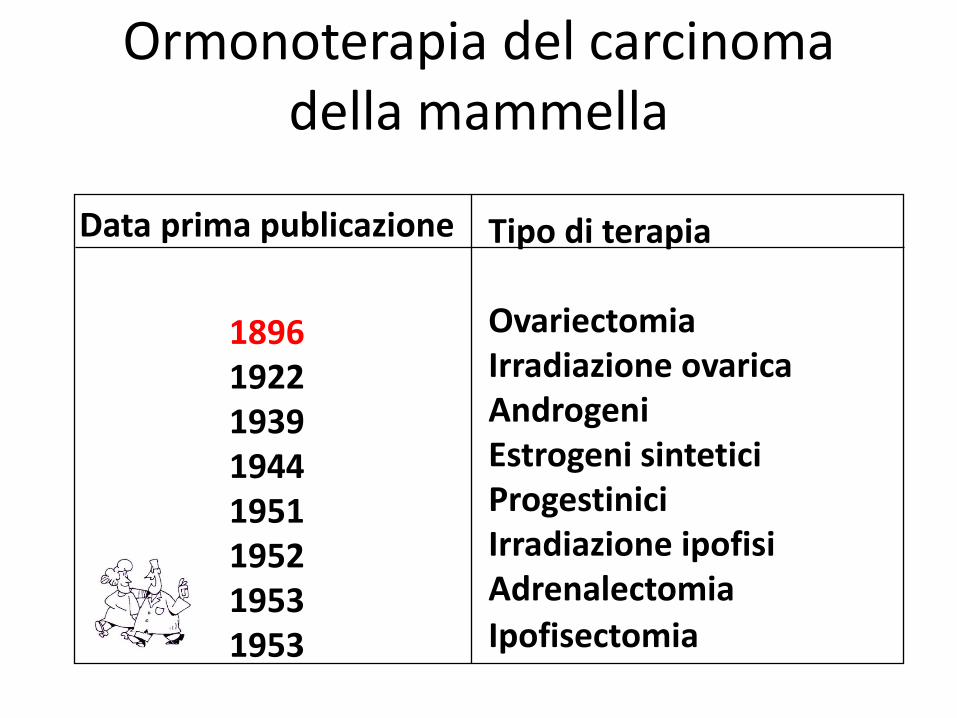
Ormonoterapia del carcinoma della mammella
Data prima publicazione
1896 1922 1939 1944 1951 1952 1953 1953
Tipo di terapia Ovariectomia Irradiazione ovarica Androgeni Estrogeni sintetici Progestinici Irradiazione ipofisi Adrenalectomia
Ipofisectomia

Sino agli anni ’60 Non era previsto alcuna terapia medica dopo l’intervento chirurgico di mastectomia radicale o radicale modificata
Storia della terapia medica del carcinoma della mammella

Intorno agli anni ‘70 si ebbe una svolta grazie alle
migliori conoscenze biologiche Affermazione della terapia medica, come terapia sistemica, ad integrazione della terapia chirurgica e della radioterapia come trattamenti loco-regionali
Storia della terapia medica del carcinoma della mammella

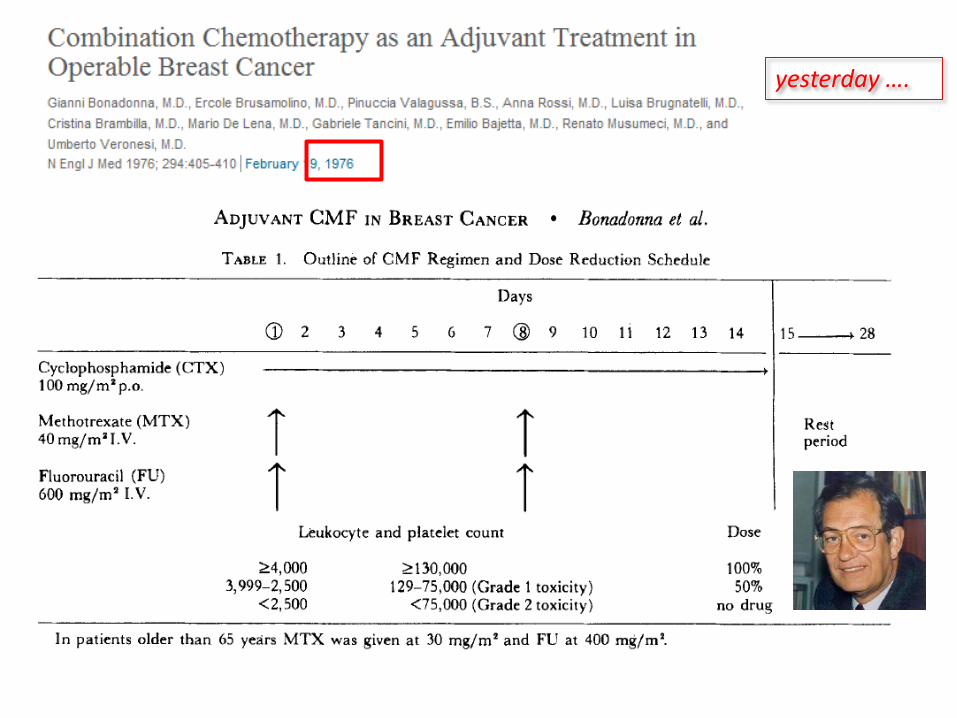
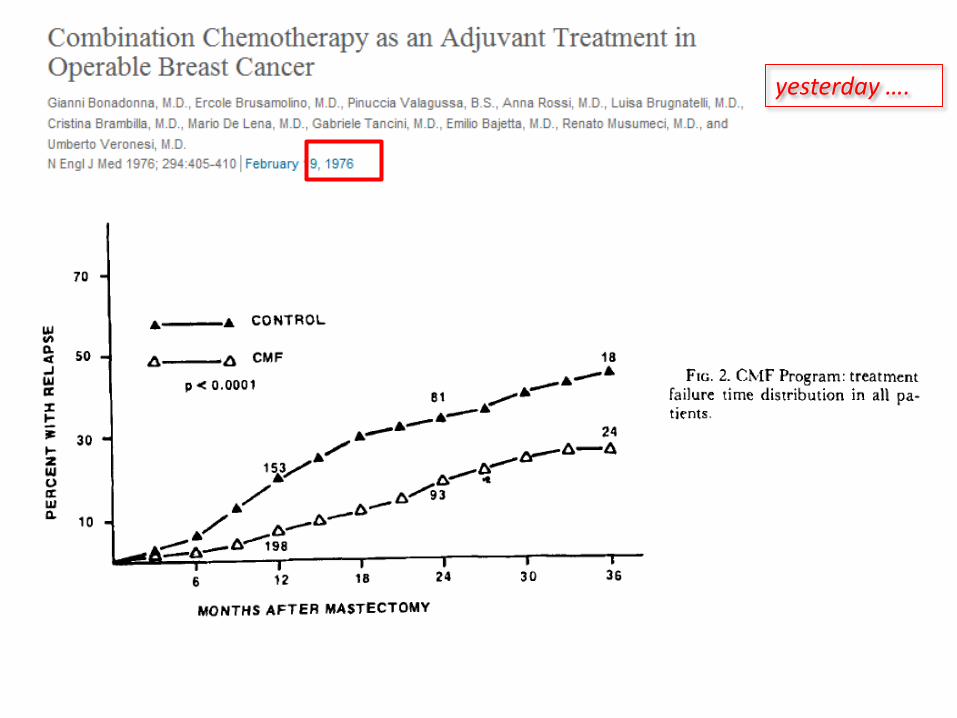
yesterday ….
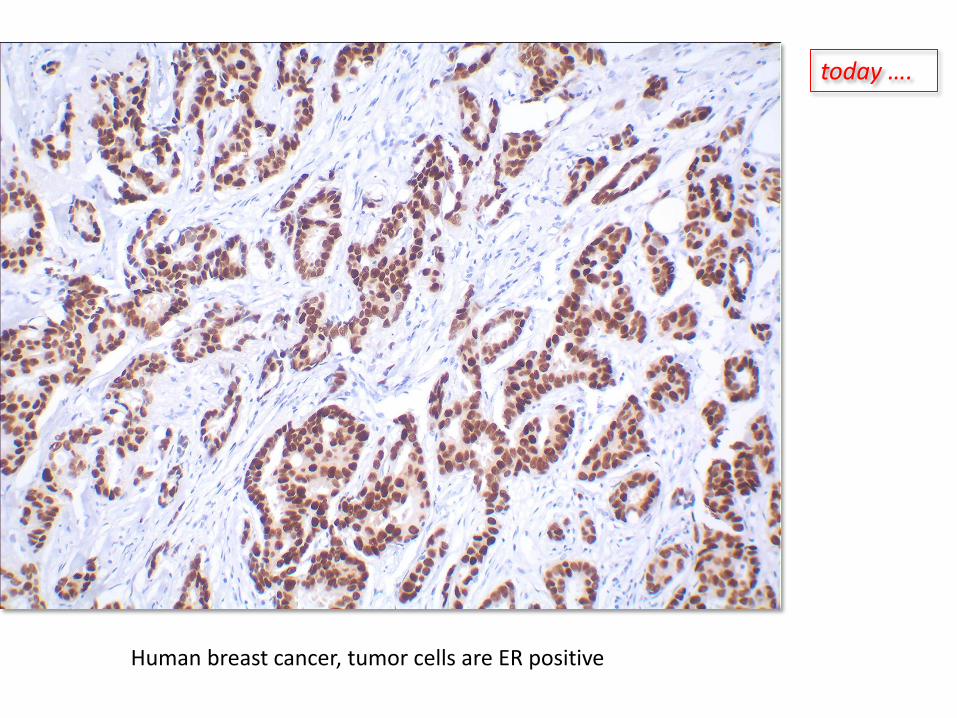
Human breast cancer, tumor cells are ER positive
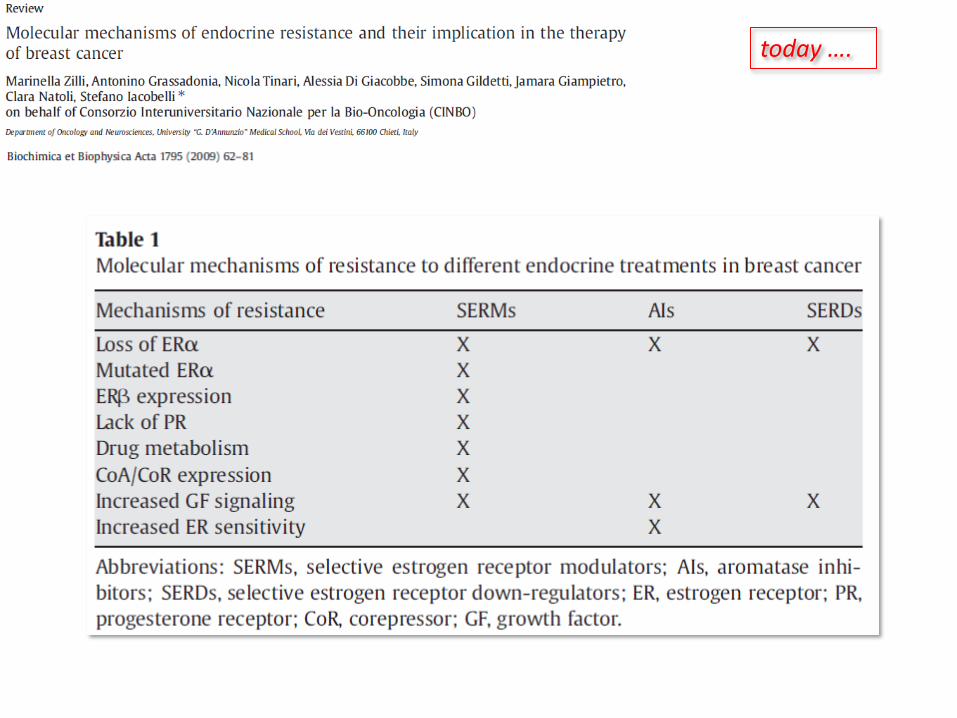
today ….

yesterday ….
today ….

yesterday ….
The Molecular Portrait Hypothesis
You can recognize the Mona Lisa by her smile and her nose and her eyes
and even her hands, but not by the sky or the trees

Breast Cancer: not one disease!
today ….
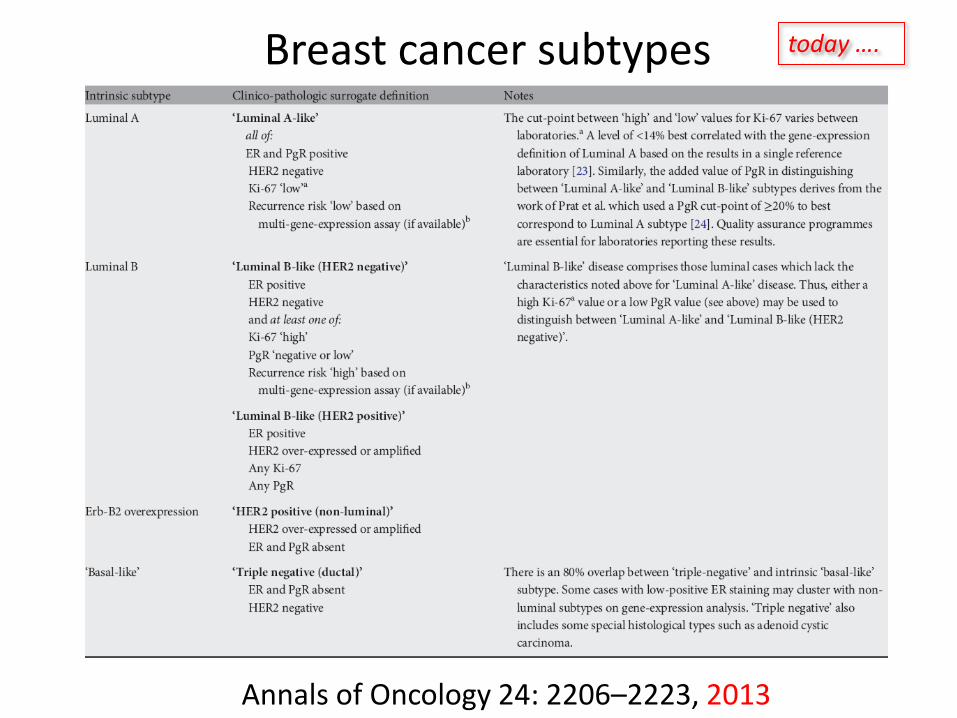
Annals of Oncology 24: 2206–2223, 2013
Breast cancer subtypes today ….

yesterday ….

yesterday ….

Annu Rev Med. 1975;26:353-63.
yesterday ….

Tamoxifen given for approximately five years after surgery to patients with early, estrogen-receptor-positive breast cancer is the current standard of care worldwide. This approach reduces the risk of death by about 25%, a reduction that translates into an absolute improvement in 10-year survival of more than 10% for patients N+ and 5% for patients N-
Early Breast Cancer
Trialists’Collaborative Group
Lancet, May 1998
yesterday ….

today ….

C. Palmieri et al. / Molecular and Cellular Endocrinology xxx (2013) xxx–xxx
Milestones in the development of treatment of HR-positive metastatic breast cancer
yesterday ….
yesterday ….
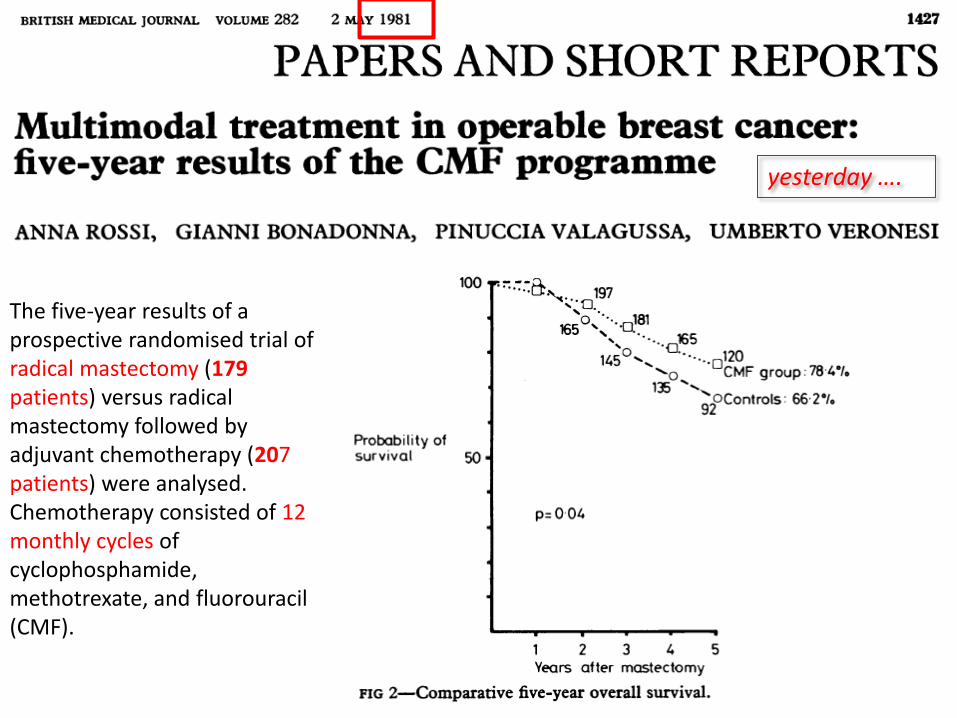
The five-year results of a prospective randomised trial of radical mastectomy (179 patients) versus radical mastectomy followed by adjuvant chemotherapy (207 patients) were analysed. Chemotherapy consisted of 12 monthly cycles of cyclophosphamide, methotrexate, and fluorouracil (CMF).
yesterday ….

CA Cancer J Clin 1986;36;42-47
For premenopausal women with positive nodes, regardless of hormone receptor status, treatment with established combination chemotherapy should become standard care.
For premenopausal women with negative nodes, adjuvant therapy is not generally recommended. For certain high-risk patients in this group, adjuvant chemotherapy should be considered.
For postmenopausal women with positive nodes and positive hormone receptor levels, tamoxifen is the treatment of choice.
For postmenopausal women with positive nodes and negative hormone receptor levels, chemotherapy may be considered but cannot be recommended as standard practice.
For postmenopausal women with negative nodes, regardless of hormone receptor levels, there is no indication for routine adjuvant treatment. For certain high-risk patients in this group, adjuvant therapy may be considered.
yesterday ….

today ….

St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013
Annals of Oncology 24: 2206–2223, 2013
today ….

HERA TRIAL DESIGN
Women with HER2 POSITIVE invasive
breast cancer IHC3+ or FISH+ centrally confirmed
Surgery + (neo)adjuvant chemotherapy (CT) radiotherapy
Stratification
Nodal status, adjuvant CT regimen, hormone receptor status and endocrine therapy, age,
region
Randomization
Trastuzumab
8 mg/kg 6 mg/kg
3 weekly x 2 years
Trastuzumab
8 mg/kg 6 mg/kg
3 weekly x 1 year
Observation
today ….
ASCO, Scientific Session, May 16, 2005

A 2008 Lifetime Television movie, directed by Dan Ireland, starring Harry Connick, Jr. The film is based on the true life story of Dr. Dennis Slamon.
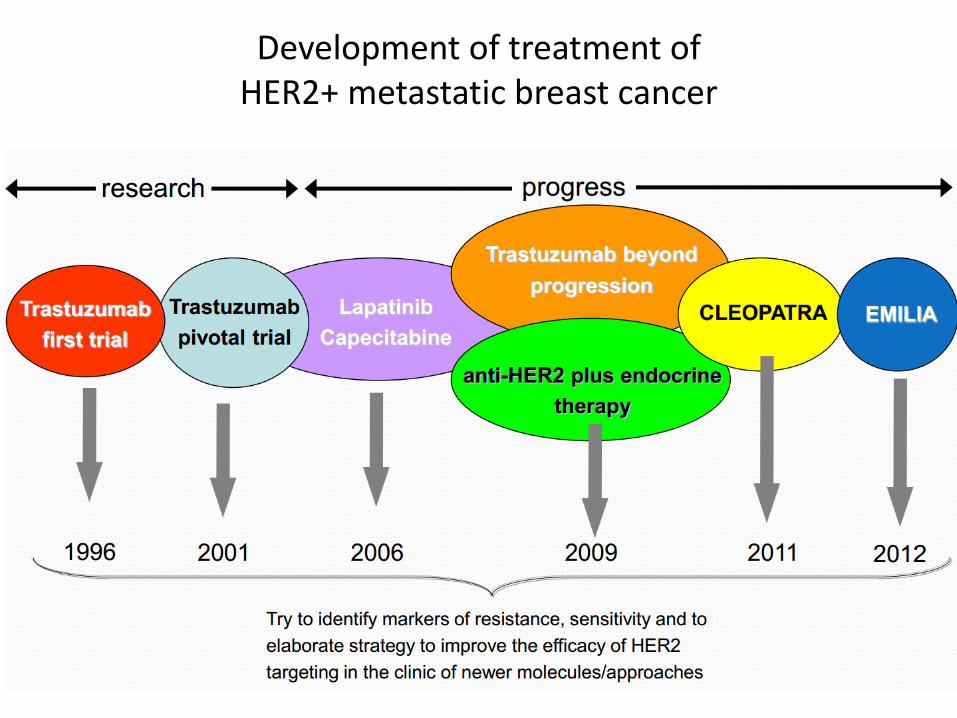
Development of treatment of HER2+ metastatic breast cancer

The light microscope remains the central cancer diagnostic tool for 400 years
Zacharias and Hans Jansen (ca 1595)
Modern microscope (ca 1995)

Today’s cancer diagnostic lab
Cellular Phenotyping Microscopy (histology/cytology) Immunohistochemistry Flow Cytometry
Genetic tests Cytogenetics Molecular Genetics Genotyping for specific mutations (PCR/RT-PCR) Minimal Residual Disease monitoring (CGH and SNP/LOH genotyping) (Gene Expression Profiling)

Genome Sequencing
Sanger (capillary) sequencing
2015 ? ~1day ?? $100
2005 ~3 years
~$ 20million
2010 ~1month
$9,500 (Illumina)
AM
L
Me
lanom
a
Sm
all-
cell
lung
Bre
ast
2008 ~4 months
~$ 1.5million
Lun
g (
NS
S)
Cancer Genomics
2000 ~10 years
~$ 3.5 billion
Myelo
ma
Hepato
ce
llula
r
CLL
Mo
use A
ML
Next generation sequencing

Diagnostic whole genome sequencing
Constitutional genome
Cancer genome
Compare
Clinical Report
Other diagnostic data
Somatic mutations Subclonal heterogeneity
Substitutions Indels
Copy number changes Translocations
Inherited mutations & polymorphisms
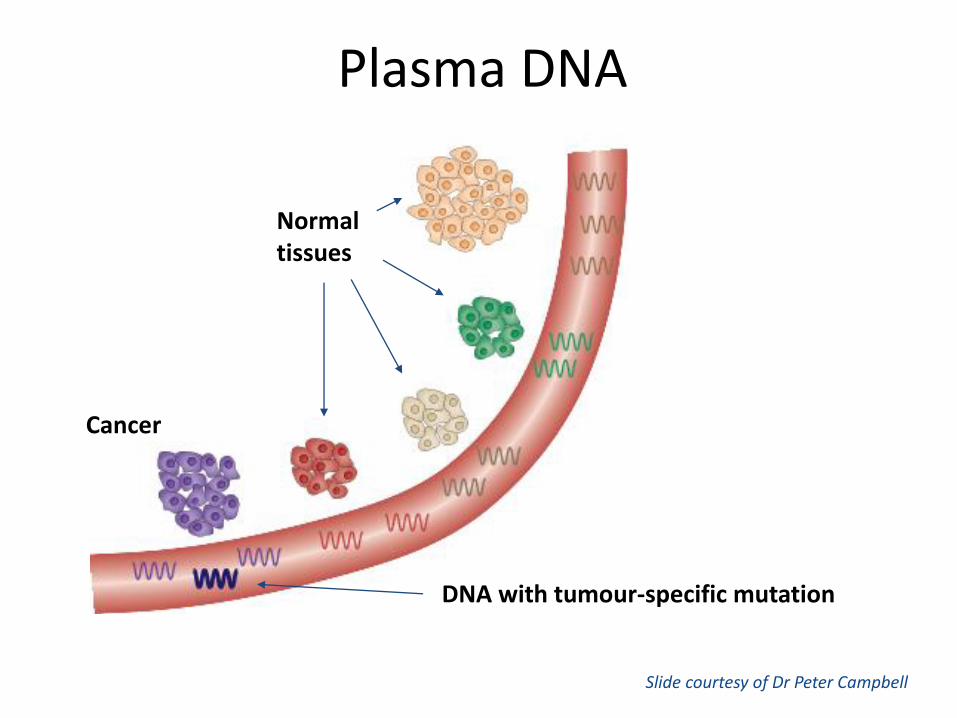
Cancer
Normal tissues
DNA with tumour-specific mutation
Plasma DNA
Slide courtesy of Dr Peter Campbell



Nuove opzioni terapeutiche
“terapie mirate” ovvero
la personalizzazione della cura


Triangolo Terapeutico
PAZIENTE
TUMORE FARMACO TERAPIA
RESISTENZA
INTERAZIONI FARMACO-TUMORE
INTERAZIONI OSPITE-TUMORE
INTERAZIONI FARMACO-OSPITE

Approccio multidisciplinare carcinoma della mammella
PAZIENTE
TUMORE FARMACO
Anatomia Patologica Biologia Molecolare Cardiologia Chirurgia Senologica Chirurgia Plastica Dermatologia Farmacia Genetica Medica Ginecologia Medicina di Base Medicina Nucleare Medicina di Laboratorio Medicina Palliativa Oncologia Medica Ortopedia Radiologia Radioterapia ………….

How breast cancer subtypes influence treatment
Turner N C , Jones A L BMJ 2008;337:bmj.a540


Breast cancer mortality has dropped by
nearly one-third since 1990

Akt
SOS
RAS
RAF
MEK
VEGF
MAPK P
P
P P
Receptor-specific
ligands
HER1, HER2,
HER3, or HER4
HER2
HER1
(EGFR)
HER2 HER4 HER3
Tyrosine kinase
domains
Plasma
membrane
PI3K
Cell proliferation
Cell survival
Cell mobility and invasiveness
Cytoplasm
Nucleus
Transcription
Signal Transduction Pathways by the HER Family
Ross JS, et al. The Oncologist. 2009;14:320-368.

Signal Transduction Pathways by estrogen receptors

A. Friedman and N. Perrimon, Cell 128, January 26, 2007
Pathway vs. Network signaling
Network “Chaotic”
Pathway “Newtonian”


Puglisi et al, Drugs 2012
Therapies targeting downstream HER2-pathways in clinical trial in breast cancer
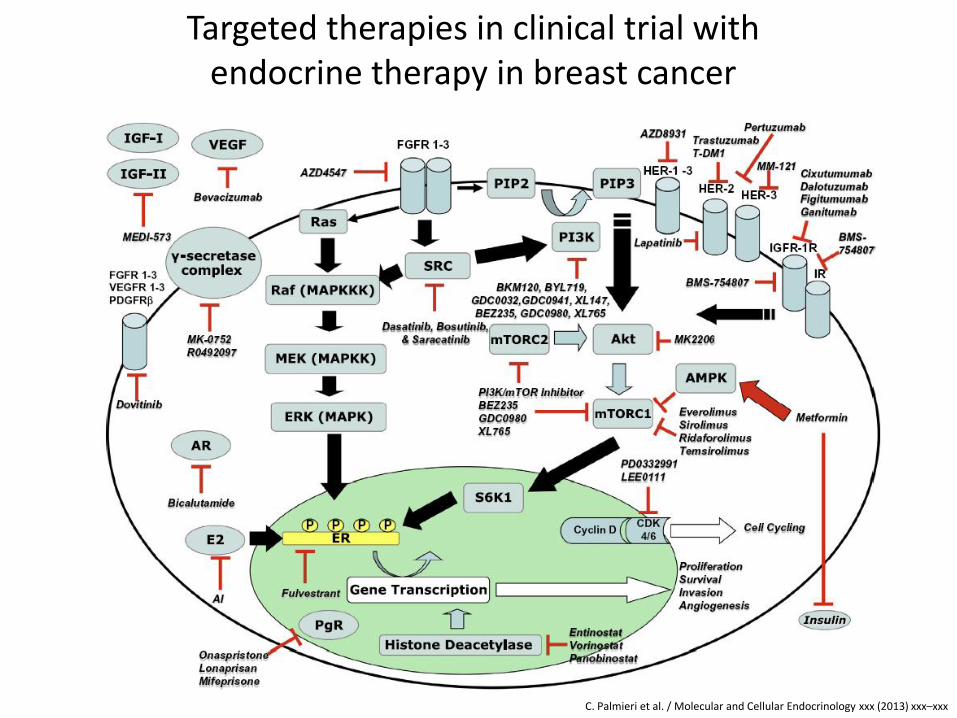
C. Palmieri et al. / Molecular and Cellular Endocrinology xxx (2013) xxx–xxx
Targeted therapies in clinical trial with endocrine therapy in breast cancer

The Future?
Cancer Patient
Surgery/Biopsy
Cancerous Tissue
Array Analysis
Tumor Fingerprint
Individualized Treatment

• Imaging
• Multiparametric/miniature testing of serum on a protein array
• Mass spectrometric serum/urine proteomic pattern generation
General Population
Screen-positive patients
Prevention; Effective Therapy
The Future?
Asymptomatic individuals
Predisposition to certain disease
Prevention (drugs; lifestyle) Surveillance
The Future?
Whole genome SNP analysis





















