Diagnostic tests and assessment.
19
Although a large number of head trauma patients evidence significant alterations in the ability to taste and smell, quantitative assessment of their dysfunction is rarely performed. This is unfortunate, since such assessment is critical for establishingthe validity of the complaint, characterizingthe specific nature of the problem, objectively monitoring changes in function over time, including those resulting from medical interventions or treatments,detecting malingering, and establishingcompensation for disability. In this article, a discussionof the theory and methods for objectively testing the senses of taste and smell is presented, along with a number of examples of the application of various chemosensorytests in the clinical selling. D ECREASED ABlLI1Y to taste or smell is common in individuals who have suf- fered head injury. Indeed, in a recent study of 750 consecutive patients presenting to the University of Pennsylvania Smell and Taste Center with chemosensory dysfunction, nearly 20% had olfactory dysfunction as a re- sult of head trauma.t Although most trauma patients who complain of decreased taste function are, in fact, experiencing decreased flavor sensation as the result of loss of olfac- tory stimulation via the retronasal route;-s subtle alterations in the ability to perceive sweet, sour, bitter, and salty stimuli can be detected in a number of these individuals using modem psychophysical taste tests.1.4.6.7 This article discusses practical and theo- retical issues related to the clinical assess- ment of taste and smell and provides the practitioner with information helpful in pa- tient assessment. First, procedures for pre- senting olfactory and gustatory stimuli are described. Next, the concepts of test reliabil- Richard L Doty, PhD Director Smell and Taste Center Hospital of the University of Pennsylvania Associate Professor Department of Otorhinolaryngology Head and Neck SU'8ery School of Medicine UnivetSity of Pennsylvania Philadelphia, Pennsylvania This ~rk was supported by Grant No. POl DC 00161 from the National Institute on Deafness and Other Com- munication Disorders and Grant No. ROl AG 08148 from the National Institute on Aging. J Head Trauma Rebabill992;7(1):47-65 @ 1992 Aspen Publishers, Inc. 47
Transcript of Diagnostic tests and assessment.

Although a large number of head trauma patients evidence significant alterations in the ability to tasteand smell, quantitative assessment of their dysfunction is rarely performed. This is unfortunate, sincesuch assessment is critical for establishing the validity of the complaint, characterizing the specific natureof the problem, objectively monitoring changes in function over time, including those resulting frommedical interventions or treatments, detecting malingering, and establishing compensation for disability.In this article, a discussion of the theory and methods for objectively testing the senses of taste and smellis presented, along with a number of examples of the application of various chemosensory tests in theclinical selling.
D ECREASED ABlLI1Y to taste or smell iscommon in individuals who have suf-
fered head injury. Indeed, in a recent studyof 750 consecutive patients presenting to theUniversity of Pennsylvania Smell and TasteCenter with chemosensory dysfunction,nearly 20% had olfactory dysfunction as a re-sult of head trauma.t Although most traumapatients who complain of decreased tastefunction are, in fact, experiencing decreasedflavor sensation as the result of loss of olfac-tory stimulation via the retronasal route;-ssubtle alterations in the ability to perceivesweet, sour, bitter, and salty stimuli can bedetected in a number of these individualsusing modem psychophysical taste tests.1.4.6.7
This article discusses practical and theo-retical issues related to the clinical assess-ment of taste and smell and provides thepractitioner with information helpful in pa-tient assessment. First, procedures for pre-senting olfactory and gustatory stimuli aredescribed. Next, the concepts of test reliabil-
Richard L Doty, PhDDirectorSmell and Taste CenterHospital of the University of PennsylvaniaAssociate Professor
Department of OtorhinolaryngologyHead and Neck SU'8erySchool of Medicine
UnivetSity of PennsylvaniaPhiladelphia, Pennsylvania
This ~rk was supported by Grant No. POl DC 00161from the National Institute on Deafness and Other Com-munication Disorders and Grant No. ROl AG 08148
from the National Institute on Aging.
J Head Trauma Rebabill992;7(1):47-65
@ 1992 Aspen Publishers, Inc.
47

48 JOURNAL OF HEAD TRAUMA REHABILrI'A11ON/MARCH 1992
ity and validity are discussed, with the goalof sensitizing the reader to their importancein chemosensory evaluation. Psychophysicalmethods used to measure taste and smellfunction are then described, followed by adiscussion of the utility of unilateral and bi-lateral testing procedures and strategies fordetecting malingering. Finally, the psycho-metric properties of currently available tests,including the degree to which they measureindependent components of chemosensa-tion, are reviewed.
The first six of these are illustrated in Figs 1and 2. The strengths and weaknesses of mostof these stimulus-presentation proceduresare discussed elsewhere.18,20-23
IA
STIMULUS CONfROL ANDPRESENTAnoN
iD
Fig 1. Procedures for presenting odorants to sub-jects for assessment. (a) An early draw-tube olfac-tometer of Zwaardemaker. Later models allowedmixtures to be presented from several paralleltubes. (b) Sniff bottle. (c) Squeeze bottle. (d)Perfumist's strip. (e) Sniff ports on a rotating tableconnected to the University of Pennsylvania's Dy-namic Air-Dilution Olfactometer. Reprinted withpermission from Doty RL. Psychophysical mea-surement of human odor perception. In: Laing
DG, Doty RL, Breipohl B, eds. The Human Senseof Smell. Berlin, Germany: Springer-Verlag, 1991.@ 1991 by Springer-Verlag.
Many types of equipment have been de-scribed for presenting chemosensory stimulito patients. Fortunately, the exact number ofmolecules entering the nose or reaching thetaste buds need not be known for a clinicaltest to be useful, so long as the stimuli arepresented in a reliable manner and normsare available to establish whether the ob-tained responses are normal or abnormal.Thus, accurate clinical assessment of chemo-sensory function can be made using surpris-
ingly simple stimulus-presentation equip-ment coupled with sound psychophysical
procedures.In the case of olfaction, equipment tradi-
tionally used to present stimuli to patientsincludes
.the draw-tube olfactometer of Zwaarde-
maker,8.glass sniff bottles,9.10.glass rods, wooden sticks, or strips of
blotter paper dipped in various concen-trations of odorants 11.121
.plastic squeeze bottles,I'.I~
.air-dilution olfactometers (which can be
very complex),1S-17.microencapsulated "scratch and sniff'
odorized strips,I8 and.bottles from which blasts of saturated air
are presented.19
49Diagnostic Tests and Assessment
.small amounts of stimulus solutionpipet ted to the selected areas,1
.Q-tip application of stimulus solution,26and
.microampere levels of current (usuallyanodal) applied to the tongue surface(termed electrogustometry).27
Intravenous administration of odorantsand tastants can also be used to produce no-ticeable chemosensory sensations. This pro-cedure has been used primarily in Japan forclinically assessing olfactory function (seeTakagi23 for review). The clinical paradigm isto inject thiamine propyldisulfide (Alinamin)slowly into the median cubital vein and torecord the duration and latency of the onsetof a garlic-like sensation experienced by thepatient. The degree to which the sensation isdue to exposure of the receptors to odorizedlung air or diffusion of the stimulus from na-sal capillaries to olfactory receptors is un-known, although studies using tracheoto-mized rats and turtles suggest that bothprobably occur and that the phenomenon isreceptor mediated.28
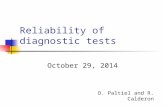
Fig 2. A subject sniffing an odorant released froma microencapsulated strip of the University ofPennsylvania Smell Identification Test, a widelyused modern clinical test. This 40-odorant testconsists of four lO-page booklets. Each page con-tains a different "scratch and snifF scented stripand an associated multiple-choice question. Thestimuli are released using a pencil tip.
TEST REIJABn.rrY AND VAUDOY:BASIC CONSmERAnONS
The utility of a sensory test depends uponthe degree to which it is reliable (consistent,dependable, or stable) and valid (accuratelymeasures what it portends to measure). Re-lated to its validity are its sensitivity (ability todetect abnormalities when present) andspecificity (ability to detect abnormalitieswith a minimum of false positives). Althoughempirical indices of these characteristics areavailable for a number of medical andpsychologic tests, this is unfortunately notthe case for the vast majority of chemo-sensory tests.
A test's reliability can be determined inseveral ways. First, and most commonly, thesame test is administered on two occasionsto a group of subjects and a correlation coef-
Gustatory stimuli are usually presented indeionized water. "Whole-mouth" proceduresrequire the patient to sip a small amount ofstimulus solution from a paper cup, swishthe solution in the mouth, and expectorate.6,7Rinsing with deionized or spring water be-tween trials eliminates residuals.24 "Regional"testing of the anterior tongue (chordatympani branch of cranial nerve [CN] VII),posterior tongue (CN IX), and in some in-stances, the palate (greater superficial petro-sal branch of CN VII) can be performed inthe clinic using
.small pieces of filter paper soaked instimulus solution,25

JOURNAL OF HEAD TRAUMA REHABILrrA'nON/MARCH 199250
ability is a necessary but not sufficient condi-tion for validity .
Three concepts related to a test's validityhave been particularly emphasized by epide-miologists: (1) sensitivity, (2) specificity, and(3) positive predictive value.~ A test's sensi-tivity reflects the proportion of individualswithin a population who have a particulardisorder (eg, anosmia) that score positivelyon the test (in effect, the "hit rate" of the test).A test's specificity reflects the proportion ofpersons without the disorder who have anegative test result (in effect, the "correct re-jection" rate of the test); whereas the test'spositive predictive value is the proportion ofall positive tests that are true positives.
aJNICAL TESTS OF OIEMOSENSORYFUNcnON
Numerous tests of chemosensory functionhave been developed over the years (for re-views, see21-23.'I-36). A subset of these tests hasmade its way into the clinic, where time is ata premium and the use of complex stimulus-presentation equipment is not practical. Suchtests can be divided into two types: (I)psychophysical and (2) psychophysiologic.In the latter category are stimulus-inducedcortical-evoked potentials and autonomicmeasures of reactivity, such as changes inheart rate. Only psychophysical tests are de-scribed in this article; the reader is referred tothe literature on taste- and odor-evoked po-tentials and to the literature on autonomicchanges associated with odorant stimula-tion.21-23.'5-36
Detection- and recognition-thresholdtests
ficient is computed (termed the test-retest re-ltablllly coefficient or the coefficient of stabil-ity). Second, in cases where parallel forms ofa test are available, the two forms are admin-istered, and a correlation coefficient com-puted. Third, subsections of some types oftests (eg, a multiple-item odor identificationtest) can be correlated with one another togive an estimate of the test's stability .In thiscase, the single test is viewed as consisting ofparallel forms, and the resulting correlationcoefficient is termed the spllt-balf reltabllllycoefflclent. Since reliability is a function oftest length, a mathematical correction for testlength must be applied to the correlationcoefficient obtained in this way to obtain thecorrect reliability coefficient for the full test.29
In practice, a number of types of validityhave been defined, some of which are diffi-cult to quantify .The most common types ofvalidity described in test measurementtheory are content validity (the degree towhich a test is made up of items, odorants,tastants, etc relevant to the task at hand) andcrlterlon-related validity (the degree towhich a test correlates with criteria known tobe associated with the trait to be measured).Criterion-related validity can be subdividedinto two classes, depending on whether thecriterion information is: (1) available immedi-ately (concurrent validity) or (2) later (pre-dtctlve valtdlty). An example of concurrentvalidity would be the situation in which anew olfactory test is administered to a groupof people known to have differing degrees ofolfactory abilities, as measured by anothertype of test, and a correlation is determinedbetween the new test and the other criterionmeasure or measures.
It is important to realize that a test can behighly reliable but not valid, since reliabilityis influenced by only unsystematic (ie, ran-dom) sources of error, whereas validity is in-fluenced by both systematic (ie, directional)and unsystematic sources of error. Thus, reli-
The most popular class of procedures usedto assess chemosensory function establishesan operational measure of the lowest con-centration of a stimulus discernible to a sub-

51Diagnostic Tests and Assessment
sition between detection and no detection isdetermined to provide an estimate of thresh-old concentration. Forced-choice responsesare required on each trial. In the singlestaircase method (a variant of the method oflimits technique),~0.~1 the stimulus concentra-tion is increased, following trials on which asubject fails to detect the stimulus, and de-creased, following trials where correct de-tection occurs.
An example of a clinical use of the methodof limits-threshold procedure is provided byCain.~2 This investigator used specially con-structed 60-mL glass sniff bottles to present,in a two-alternative forced-choice situation,either diluent (water) or odorant (n-butanoldissolved in water) to 43 patients with vary-ing degrees of olfactory dysfunction usingfour repeated ascending series. Testing wasperformed for each nasal chamber sepa-rately. This procedure, which took approxi-mately half an hour per patient, was found toclearly discern between anosmic, hyposmic,and normosmic subjects and demonstratedthat olfactory dysfunction is typically bilat-eral.
An example of the use of a modified two.alternative forced-choice staircase procedurecomes from a study of patients with earlyAlzheimer's disease.~' In this study, a trialconsisted of the presentation of two 100-mLglass sniff bottles to the subject in rapid suc-cession. One contained 20 mL of a givenconcentration of phenyl ethyl alcohol (PEA)dissolved in USP-grade light mineral oil,whereas the other contained mineral oilalone. The subject's task was simply to reportwhich stimulus was strongest. The first trialcommenced at the -6.50 log Oiquid volume/volume) concentration step. If a miss oc-curred on any trial before five successiveblank/odorant pairs were completed, thenext trial began at the concentration one logstep higher. When five consecutive correcttrials occurred at a given concentration, the
ject, that is, the absolute threshold measure.In the case of olfaction, a qualitative odorsensation is rarely perceived at very lowodorant concentrations (eg, "rose-like"), andsubjects only experience the faint presenceof something. The lowest concentrationwhere such a presence is noted is termed thedetection threshold, whereas the lowest con-centration where odor quality is discernibleis the recognition threshold. 11 is now com-mon on a detection-threshold task to ask asubject to indicate, on a given trial, which oftwo or more stimuli (eg, an odorant and oneor more blanks) smells strongest (the forced-choice procedure), rather than to present justthe odor stimulus and ask whether it is per-ceived or not. Forced-choice procedures areless susceptible to response biases (ie, theconservatism or liberalism in reporting thepresence of an odor under uncertain condi-tions) and are more accurate and reliablethan non-forced-choice procedures."
Recognition thresholds can be obtained ina manner similar to detection thresholds byhaving the patient indicate the lowest con-centration at which the tal'get odor or tastequality is perceived. Unfortunately, criterionbiases are difficult, if not impossible, to con-trol in recognition threshold paradigms.Thus, even in a forced-choice situation,guesses are not randomly distributed amongalternatives, thereby biasing the thresholdvalue. The classic example of this is in tastepsychophysics, where there is a tendency forsome subjects to report "sour" more oftenthan the other primary qualities when nostimulus is clearly discernible, resulting in aspuriously low sour-taste recognition-thresh-old measure.38.39
Two threshold procedures have receivedthe widest usage in the clinic: (1) the ascend-ing method of limits and (2) the single stair-case. In the ascending method of limits,stimuli are presented sequentially from lowto high concentrations, and the point oftran-

JOURNAL OF HEAD TRAUMA REHABIUTA11ON/MARCH 199252
ject over time are obtained. For these andother reasons, they are not discussed in de-tail here.
Difference-threshold tests
In classic psychophysics, the concentra-tion by which a stimulus must be changed tomake it perceptibly stronger or weaker istermed a just noticeable difference OND).According to Weber's law,so the size of theincrement in odorant concentration (~1) re-ql,lired to produce a JND increases as thecomparison concentration (1) increases, withthe ratio being a constant; that is, ~l/ I = K
Although K, in fact, is rarely a constant (be-ing influenced by the size of I at extremes ofthe continuum and by such factors as thestimulus used),'1 it is a rough index of a sen-sory system's sensitivity; the smaller the Kvalue, the greater the sensory discrimination.
Eichenbaum et a149 devised a relativelybrief clinical test to assess the discriminationability of a group of neurologically normalsubjects and the famous patient HM (whoseamygdala, uncus, and anterior two-thirds ofthe hippocampus and parahippocampal gy-rus had been removed bilaterally to controlcerebral seizures).sl In this test, 10 binarydilutions (in water) of each of 4 stimuli (ac-etone, ethanol, almond extract, and lemonextract) were used. Subjects were initiallypresented with the highest and lowest con-centrations of a given odorant and were re-quired to choose the stronger stimulus. Suc-cessively stronger stimuli were paired withthe strongest stimulus until, on the last of the10 trials, the 2 samples were identical. Thedifference threshold was defined as the low-est concentration for which discriminationup to and including that dilution was error-less.
staircase was "reversed," and the subsequentpair of trials was presented at a concentration0.5 log step lower. However, from this pointon, only one or two trials were presented ateach step (ie, if the first trial was missed, thesecond was not given, and the staircase wasmoved to the next higher 0.5 log step con-centration). If both trials were correct, thestaircase was moved down one 0.5 log-unitstep. The geometric mean of the last four ofseven staircase-reversal points was used asthe threshold estimate. Compared to age-matched control subjects, the Alzheimer'sdisease patients had significantly higherthreshold values.
It should be noted that threshold valuesproduced by the aforementioned staircaseprocedure are not mathematically equivalentto those produced by most other methodssince, after the initial reversal point, two cor-rect trials are required for the staircase to de-scend and only one incorrect trial is requiredfor the staircase to ascend. As discussed byWetherill and Levitt,« the threshold concen-tration determined by this method representsthe value chosen correctly by the subject 71%of the time.
Signa1-detection tests
Signal-detection theory is an approach tosensory measurement that differs radicallyfrom the approach used in threshold testing,in that it does not accept the classic conceptof a threshold and focuses on the importanceof subject expectancies and rewards in influ-encing the detection decision. Unlike classicthreshold procedures, methods based on thistheory provide a measure of response bias,as well as a measure of sensitivity theoreti-cally unconfounded by response bias.45However, with rare exception,46-49 sensitivityprocedures based on signal-detection theoryhave found little applicability in the clinicalsetting, since they require large numbers oftrials and are most applicable in studieswhere repeated measures on the same sub-
Suprathreshold-scaling procedures
Odors and tastes can be described in termsof a number of psychologic attributes, in-cluding strength, pleasantness, and quality.
Diagnostic Tests and Assessment 53
Since sensation magnitude varies as a func-tion of stimulus concentration, ratings orother measures of stimulus intensity haveproved useful in evaluating taste and smellfunction. In general, the intensity of a stimu-Ius is related to the number of neurons thatare recruited and the frequency at whichthey fire;sz therefore, perceived intensity ispresumed to be a sensitive index of the ex-tent of neural damage in afferent pathways.Suprathreshold tests have an advantage overthreshold tests in that they are often brief andeasy to administer; furthermore, they are lesssusceptible to subtle stimulus contaminationthat can occur at low odorant and tastantconcentrations.
Although psychophysicists and psychome-tricians seek to develop psychologic scaleswith ruler-like properties (ie, where dis-tances along the scale can be thought of asratios and a true zero point is present), thedegree to which they have been successful inthe chemosensory sciences is debatable. Forthe purposes of clinical testing, however, theexact form of underlying psychologic scalesis not particularly important, so long as re-sponses on standardized scaling tasks are re-liable and can differentiate among personswith various degrees of dysfunction. Thus,the fact that judgments of the intensity ofboth odors and tastes are relative and influ-enced by contextual factors (eg, a moder-ately intense odor is judged as more intensewhen presented with weak comparisonstimuli than when presented with strongcomparison stimuli)s3 is not of great concernin the development or administration of aclinical test, so long as the test and the test-taking procedures are standardized.
Rating scales are widely used to assess therelative amount of a psychologic attributeperceived by a subject. In chemosensory as-sessment, two types are popular: (1) categoryscales, where the subject signifies the relativeamount of a sensation by indicating which ofa series of discrete categories best describes
the sensation, and (2) /ine sca/es (also termedvisua/ analog or graphic sca/es), where themagnitude of the sensation is signified byplacing a mark along a line that has descrip-tors (termed "anchors") located at its ex-tremes (eg, very weak-very strong). Thereader is referred elsewhere to discussionsregarding the optimal number of categoriesand other theoretic aspects of ratingscales.29.31.54
Intensity matching procedures have alsobeen used in clinical studies. Since intra-moda/ intensity matching procedures havenever been used in a clinical context for ei-ther taste or smell assessment, only cross-moda/ intensity matching procedures areconsidered here.
In cross-modal matching, the relative mag-nitude of the sensory attribute is signified foreach member of a stimulus set by using someother sensory modality or cognitive domain.A key distinction between this procedureand rating-scale procedures is that the sub-ject or patient attempts to estimate the ratiorelations among the intensities of the differ-ent concentrations of stimuli that are pre-sented, without being constrained by catego-ries or a short response line. Continuacommonly used in this task include distance(eg, pulling a tape measure a distance pro-portionate to the odor's intensity) and num-ber (eg, assigning numbers proportionate tothe odor's intensity), the latter procedure be-ing termed magnitude estimation.55.56 Whensubjects judge intensities of sensations fromtwo or more modalities on a single commonscale, the procedure is termed the method ofmagnitude matching. Since magnitude esti-mation and magnitude matching are amongthe most commonly used cross-modal
matching procedures, they are discussed indetail here.
In magnitude estimation, the patient orsubject assigns numbers relative to the mag-nitude of the sensations. For example, if thenumber 50 is used to indicate the intensitv of

JOURNAL OF HEAD TRAUMA REHABILrrAnON/MARCH 199254
one concentration of a tastant, a concentra-tion that tastes 4 times as intense would beassigned the number 200. If another concen-tration is perceived to be half as strong as theinitial stimulus, it would be assigned thevalue 25. The examinee can assign any rangeof numbers to the stimuli, so long as theyreflect the relative magnitudes of the per-ceived intensities. In some cases, a standardfor which a number has been preassigned(often the middle stimulus of the series) ispresented to the subject in an effort to makethe responses more reliable. In other cases,this is not done (the "free-modulus"method), and the individual is free to chooseany number system desired, so long as thenumbers are made proportional to the mag-nitude of the attribute. For example, one pa-tient may choose to assign the first stimulusthe number 200, whereas another maychoose to assign this same stimulus the num-ber 10. If a second stimulus is perceived tobe 10 times stronger than the first by each ofthese individuals, the first one would assignthe number 2000, whereas the second onewould assign the number 100. The importantpoint is that the absolute value of the numberis not important, only the ratios between thenumbers.
Intensity magnitude estimation data aremost commonly analyzed by plotting the log-magnitude estimates on the ordinate and thelog-odorant concentrations on the abscissaand fitting the best-fit line to the data usinglinear regression. The resulting function, logp= nlog 0+log k (where p= perceived inten-sity , k = the y intercept, g = stimulus concen-tration, and n = the slope), can be repre-sented in its exponential form as a powerfunction, p = k0n, where the exponent n isthe slope of the function on the log-log plotIn olfaction, n varies in magnitude from odorto odor but is generally less than one, reflect-ing a negatively accelerated function on lin-ear-Iinear coordinates. As discussed else-
where, modifications have been made tothese equations in attempts to take into ac-count threshold sensitivity and adapta-tion.'1'S7
It is important to note that magnitude esti-mation, perhaps more so than a number ofother sensory procedures, can be biased orinfluenced in systematic ways by proceduraland subject factors.'I'SS The task is compara-tively complex in that accurate responses toa stimulus require a good memory for theprior stimulus and, ideally, for a number ofthe stimuli that are being judged. If too muchtime lapses between the presentation ofstimuli, the memory of the prior stimulusfades. On the other hand, if the trials arespaced too closely together, adaptation candistort the relationship. There is evidencethat not all subjects consistently provide ratioestimates of the stimuli, and a number do notunderstand the concept of producing ra-tios.59.60 Furthermore, the magnitude of theexponent is dependent upon the choice ofthe stimulus scale (ie, the units in which thestimulus concentration is expressed), al-though in olfaction this is probably of minorconsequence.61 However, these and otherpotential shortcomings need not hinder theuse of this procedure clinically, so long asthe instructions, test procedures, and teststimuli are carefully standardized and moni-tored, and reliable responses are obtained.Nevertheless, comparative assessments ofnine-point rating scales, line scales, mag-nitude estimation scales, and a hybrid ofcategory and line scales suggest that, for rela-tively untrained or mathematically unsophis-ticated subjects, category scales and linescales may be superior to magnitude estima-tion when such factors as variability, reliabil-ity, and ease-of-use are considered.62.6'
Although investigators typically view theslope of the magnitude estimation function(on log-log coordinates) as a key indicant ofsensory function. this is not the case with the

55Diagnostic Tests and Assessment
two sides of the tongue were similar, theywere combined. As shown in Fig 3, it is ap-parent that the tip" of the tongue is signifi-cantly more sensitive than the other areas toelectrical stimulation, as evidenced both bythe slope and the absolute position of thepsychophysical functions.
Quality-discrimination tests
The most straightforward chemosensoryquality-discrimination test requires individu-als to decide whether two stimuli have thesam~ or different quality. In the case ofodors, a series of same-odorant and differ-ent-odorant pairs are presented, and themeasure of discrimination is calculated as theproportion of pairs that are correctly differ-entiated.46.48 Variants on this theme include
fii::!?:-
~Ci5zw1-~wz
~
intercept and other parameters associatedwith the function's position relative to theordinate. The intercept is not independent ofthe slope and, more importantly, is depen-dent upon differences in the use of numbers
by subjects.The method of magnitude matching, un-
like that of magnitude estimation, providesinformation about the perceived overall in-tensity of stimuli from the absolute positionof the magnitude estimation function andcorrects, to some degree, for differencesamong subjects in number usage (for a dis-cussion of strengths and weakness of thisprocedure, see Marks et al~). In the mostcommon application of this method, judg-ments of the intensity of sensations from twomodalities (eg, loudness, odor intensity) aremade on a common magnitude estimationscale.6s Under the assumption that subjectsexperience stimuli on one of the continua(eg, loudness) in a similar manner, one canassume that differences among their loud-ness ratings reflect differences in number us-age. The odor intensity continuum can thenbe adjusted accordingly. Such normalizationallows, theoretically, for a direct comparisonof scale values across subjects; thus, if theadjusted odor intensity magnitude value for 1subject is 10 and another subject is 20 at thesame concentration level, the 2nd subject ispresumed to experience twice the odor in-tensity as the Ist subject.
An example of cross-modal matching in astudy of electric taste is presented by Salataet al.66 In this study, 12 subjects estimated,during the same test sessions, the intensity ofone-second duration white-noise pulses (at1000 Hz ranging from 40 to 60 dB SPL in 5 dB
increments) presented binaurally and half-second electric current pulses (40, 64, 100,160, and 250 microamperes) delivered to thetongue tip, anterior tongue side, posteriortongue side, the posterior medial tongue,and the soft palate. Since the data from the
Fig 3. Intensity magnitude estimates (converted toa tone level) versus the electrical current appliedto each of five tongue and palate areas. Data
points represent means (:!:SEM) of 12 subjects.Reprinted with permission from Salata JA, DotyRL, Raj JM. Differential sensitivity of tongue areasand palate to electrical stimulation: A supra-threshold cross-modal matching study. ChemSens. 1991;16:483-489. <e 1991 by Oxford Univer-sity Press.

56 JOURNAL OF HEAD TRAUMA REHABIIJTA11ON/MARCH 1992
type of test uses the number of correct re-sponses in a series of several such presenta-tions as the test score.
A variant on this theme is the stimulus-matching task, in which a set of stimuli areprovided and the patient is required to matchthe stimuli, one by one, to those of a set ofidentical stimuli. Abraham and Matha 70 pro-
vide an example of this test, in which fourodorants are contained in eight vials (two vi-als per odor), and the patient is asked to pairup the equivalent two-vial containers. Thenumber of pairs correctly matched on eachof two administrations of the test is used asthe test score. If a discrepancy arises in thetwo tests, a third administration is given, andthe data are averaged to provide the finalscore.
tests in which a stimulus differs from a set ofother stimuli that, in turn, are equivalent, andthe task is to select the "odd" stimulus (eg,the so-called triangle test).67
Another form of discrimination test, whichis defined primarily in terms of how the dataare analyzed, derives from a proceduretermed multidtmenstonal scaltng (MDS). Inthis procedure, ratings are made for all pos-sible pairs of stimuli on a line scale anchoredwith descriptors like "completely different"versus "exactly the same," and the resultingvalues are subjected to correlational analysis.This correlation matrix is then subjected to analgorithm that places the stimuli in spacerelative to their perceived similarities.68 Theprocess is akin to constructing a map of acountry from a list of distances available be-tween the cities of that country. Clinically,persons with poor discrimination abilities failto discern differences and similarities amongstimuli, as illustrated by multidimensionalspaces that have no distinct or reliable group-ings. Because MDS is comparatively timeconsuming, and statistical procedures forcomparing one person's MDS space to an-other's (or to a norm) are poorly worked out,it has not received wide clinical application.
Quality-identiflcation tests
Quality-recognition tests
Two general classes of quality-recognitiontests can be envisioned. In the first class, aseries of odorants or tastants are presented,and the subject is simply asked on each pre-sentation whether or not a stimulus is recog-nized. Identification is not required. Thisrelatively crude procedure, which is analo-gous to testing vision by shining a flashlightin the eye and asking the examinee if lightwas seen, is unfortunately one of the mostcommon tests used by medical practitionersto ascertain CN I function.69 In the secondclass, a patient is presented with a "target"stimulus and is subsequently asked to selectthe target from a larger set of stimuli. This
Among the most popular procedures forassessing taste and smell function are thosethat require stimulus-quality identification.Such tests can be divided into three majortypes: (1) naming tests, (2) yes/no identifica-tion tests, and (3) multiple-cboice identifica-tion tests. The respective responses required,on a given trial, in these three types of testsare
.to provide a name for the stimulus;
.to signify whether or not the stimulussmells like an object named by the ex-aminer (eg, does this smell like a rose?);and
.to identify the stimulus from a list ofnames.
Odor-naming tests, although they havebeen used clinically,7I have limited useful-ness, since many normal individuals havedifficulty in naming or identifying even famil-iar odors without cues. This problem is lessacute in taste-naming tests, although a con-siderable proportion of individuals in thegeneral population exhibit sour-bitter andbitter-salty confusions.72
Diagnosttc Tests and Assessment 57
clinical settings (see also Koster81). In thistest, each of 10 stimuli are presented to apatient in counterbalanced order 10 timesapiece. The response alternatives are thenames of the 10 stimuli: (1) ammonia, (2)Clorox, (3) licorice, (4) mothballs, (5) pep-permint, (6) roses, (7) turpentine, (8) vanilla,(9) Vicks vap9r rub, and (10) vinegar. Nofeedback is given to the examinee concern-ing the correctness or incorrectness of theresponses. The data are presented as the per-centage of responses given to each alterna-tive for each odorant and displayed in a rec-tangular matrix (stimuli making up rows andresponse alternatives making up equivalentlyordered columns). Responses that fall alongthe negative diagonal represent correct re-sponses, whereas those that fall away fromthe diagonal represent "confusions." Thepercentage of responses that are correctserves as the primary test measure, althoughWrigQt argues that the "off-diagonal" re-sponses (confusions) may provide meaning-ful clinical information.
Memory tests
A basic odor or taste-recognition memorytest requires a subject to taste or smell astimulus (termed the target or inspectionstimulus) and then to select, after an intervalof time (eg, 30 seconds), that stimulus from aset of foils. Repeated trials are often per-formed at one or more retention intervals foreach of several stimuli. In an effort to mini-mize the rehearsal of verbal labels for delayintervals longer than 10 seconds, the exam-inee is sometimes asked to perform an unre-lated task, such as counting backwards, dur-ing the retention period. The proportion oftrials where correct performance occurs iscommonly used as the test measure.
An example of a clinical application of anodor recognition task is described by jones,Moskowitz, and Butters.82 These authors pre-sented 20 pairs of odorants at 2 delay inter-
Yes/no identification tests require a patientonly to report whether or not each of a set ofstimuli smells (or tastes) like a particular sub-stance named by the experimenter. Two tri-als with each stimulus are usually given, withthe correct alternative provided on one trialand an incorrect one on the other (eg, lemonodor is presented and the subject is asked onone trial whether the odor smells like lemonand on another trial whether the odor smellslike peppermint). Although this test requiresthe subject to keep the percept in memorylong enough to compare it with the targetword (which, of course, must also be re-called from memory), some of its proponentsargue that it is less influenced by cognitiveand memory demands than multiple-choiceidentification tests (see following).73 How-ever, since chance performance on this typeof test is 50% compared to 25% on a 4-alter-native multiple-choice identification test, itsrange of discriminability is lower and, there-fore, more trials are needed to obtain thesame statistical power.
A number of multiple-choice odor-identifi-cation tests have been described in the clini-cal literature.18,31,71,74-76 These tests are con-ceptually similar and, in the few cases thathave been examined, strongly corre-lated.75.77,78 The most widely used of thesetests (the University of Pennsylvania SmellIdentification Test or UPSIT, commerciallytermed the Smell Identification TestTM,Sensonics, Inc, Haddonfield, NJ)l8.79$) exam-ines the ability of subjects to identify, fromsets of 4 descriptors, each of 40 "scratch andsniff' odorants (Fig 2). The number of correctitems out of 40 serves as the test measure;this value is compared to norms and a per-centile rank is determined, depending uponthe age and gender of the patient.79 This testhas several unique features, including ame-nability to self-administration and a meansfor detecting malingering.
Wright75 has recently developed an odoridentification confusion matrix applicable to

JOURNAL OF HEAD TRAUMA REHABILn'A11ON/MARCH 199258
vals (0 and 30 seconds) to 14 alcoholicKorsakofrs psychosis patients, 14 alcoholiccontrols, and 14 nonalcoholic controls. On agiven trial, the task of each subject was toreport whether the second stimulus of a pairof odors was the same or different than thefirst. In the 3O-second delay interval, the sub-jects counted backwards by 3s from a 3-digitnumber given by the experimenter after thepresentation of the first stimulus of the pair.The Korsakofrs psychosis patients per-formed significantly more poorly than didthe control groups at both the 0- and 30-sec-ond retention Intervals.
Campbell and Gregson83 developed a testof short-term odor memory in which a pa-tient was given four odors in a row andasked if the fourth odor, which was the sameas one of the first three, was equivalent to thefirst, second, or third presented odorant. Nodelay interval, per se, was defined betweenthe presentation of the stimuli, but presum-ably the trials were presented soon after oneanother. Seven 3-odor combinations of12 in-spection stimuli were given. If patients haddifficulty with this task, they were then giventwo-odor combinations. The test score valuewas the number of odors that were consis-tently recognized by the subject. This test hasbeen shown to be sensitive to deficits ob-served in schizophrenia,83 Kallmann's syn-drome,73 and Korsakoff's psychosis.71
OnlER CONSmERAnONS
Unilateral and bilateral olfactory testing
occasions when unilateral olfactory testing isof considerable value, for example in headinjury and the detection of rare tumors.84 Acomplete workup of a patient should includeunilateral, as well as bilateral, olfactory test-
ing.Unilateral testing is straightforward. Al-
though it is possible to present a stimulus toone naris and obtain unilateral stimulation,the possibility of the crossing of odorant tothe contralateral side within the nasopharynxupon exhalation cannot be excluded. Thus, itis prudent to close the contralateral nariswithout distorting the septum (eg, by using apiece of MicrofoamTM tape [3M Corporation,Minneapolis, Minn] cut to fit tightly over theborders of the naris).8S This precaution servesto make it difficult for air to enter the blockednasal chamber via the retronasal route.
Furukawa et al86 report that 7 of 94 patientsthey examined evidenced significant unilat-eral threshold deficits, despite the fact thatnone evidenced a deficit on bilateral testing.A similar phenomenon was observed in 6 of12 patients who had received brain surgery.A recent assessment of 82 consecutivenonanosmic patients presenting to our centerwith chemosensory dysfunction found 14 (ie,17%) whose unilateral detection thresholdswere discrepant from one another by at least3 orders of magnitude (Doty , unpublisheddata). Interestingly, 9 of these 14 individualsappeared to be anosmic on one side of thenose, even though only 3 had bilateral detec-tion-threshold values that were consideredabnormal.
Removal of temporal lobe tissue for con-trol of intractable seizure activity typicallyproduces greater olfactory dysfunction onthe side ipsilateral to the operation, reflectingthe fact that most olfactory projections fromthe olfactory bulb are ipsilateral.87 Interest-ingly, head injuries that produce damage tothe right hemisphere sometimes result in uni-lateral neglect to the left side of the body that
Most patients evidence olfactory dysfunc-tion bilaterally.77 When unilateral losses arepresent, they often go unnoticed and appearto be of little significance to the patient. Sincebilateral testing requires less time and resultsin the detection or clinically meaningful defi-cits, it is often selected for assessing olfactoryfunction. However, there are a number of

59Dtagnostic Tests and Assessment
chance alone, on approximately 50% of thestimulus trials. However, malingerers oftenavoid the correct response more often thanexpected on the basis of chance and, for thisreason, can be detected. This is well illus-trated in olfaction by responses to the UPSIT.Since this is a four-alternative forced-choicetest, one would expect that approximately25% of the test items (ie, 10) should be cor-rectly answered, on average, by an anosmic.The probability of scoring 5 or less on theUPSIT and not having at least some ability tosmell is less than 5 in 100. The probability ofscoring zero on the UPSIT and having nosense of smell is approximately 1 in 100,000.
is also expressed in olfactory perception.Given the olfactory system's large ipsilateralprojections from the bulb, Bellas et al88 rea-soned that if a sensory loss were responsiblefor the problem, it should occur on the right,rather than the left, side of the nose. On theother hand, if the problem is a cognitive one,the loss should be on the left, rather than onthe right. These authors simultaneously pre-sented different odorants to the two nostrilsof 15 patients with this syndrome and foundthat the recognized odorant was the one pre-sented to the right nostril, supporting the no-tion that unilateral neglect was due to acognitive, rather than sensory , dysfunction.
Detection of malingering PSYalOMETRIC PROPERTIES OFCIJNICAL CJ.IEMOSENSORY TESTS
Malingering on chemosensory tasks is notuncommon, largely because considerablecompensation can be available in accidentcases for alterations in the ability to taste orsmell. It is frequently suggested in the medi-cal literature that if a patient cannot readilyperceive the vapors from an irritating sub-stance presented to the nose, the patient ismalingering.89 However, this is not a surefiremeans for detecting malingering. Thus, indi-vi~uals who, on other grounds, are believedto be feigning anosmia usually have difficultyin denying experiencing the effects of am-monia or other irritants, particularly sincethese stimuli often produce eye watering,coughing, and reflexive responses that aremanifested overtly. Furthermore, there ap-pears to be considerable variability in tri-geminal responsiveness to such stimuliwithin the normal population.
A more valid approach for detecting ma-lingering is to examine response strategies ofpatients on forced-choice tests. For example,in a taste-threshold test in which a blank anda taste stimulus are presented in random or-der on each trial, an individual with no abil-ity to detect the stimuli should be correct, by
As indicated in the first section of this ar-ticle, an effective clinical test must be reliableand valid. A consummate test battery wouldbe made up of tests that measure differentaspects of the function of a sensory system,ideally ones that reflect the location and de-gree of the physical pathology itself. How-ever, despite the large number of olfactoryand gustatory clinical tests that have beendevised, there are only a handful of tests forwhich reliability or validity information isavailable. With the exception of grossly lo-calizing pathologies via regional tongue test-ing or unilateral olfactory testing, there ispresently no convincing evidence that thephysical location of an olfactory or gustatorypathology can be established solely on thebasis of psychophysical testing. Neverthe-less, most of the olfactory and gustatory testsavailable today have demonstrable clinicalutility , and research is progressing in thisfield.
It is well documented that forced-choiceodor identification tests, such as the UPSIT,the Connecticut Chemosensory Clinical Re-search Center's odor identification test, and

JOURNAL OF HEAD TRAUMA REHABILrrA11ON/MARCH 199260
Wright's confusion matrix test, evidence highreliability (eg, both the test-retest and split-half rs of the UPSIT are above 0.90).90 Sinceolfactory detection threshold values varyconsiderably among individuals and evi-dence considerable day-to-day fluctuationswithin the same individuals,91 one might ex-pect their reliability to be suspect. However,with noticeable exceptions,92 this appearsnot to be the case. Thus, in a study of 40subjects, Koelega93 reported test-retest reli-ability coefficients (Spearman r) for a four-alternative forced-choice n-amyl acetatethreshold test to be 0.65, 0.51, and 0.59 forbilateral, right nostril, and left nostril presen-tations, respectively. More recently, in astudy of 32 subjects ranging in age from 22 to59 years, Cain and Gent94 established correla-tions between the left and right sides of thenose for detection threshold values of buta-no1, phenyl ethyl methyl carbinol (PEMEC),isoamyl butyrate, and pyridine. The high cor-
relations (0.68, 0.96, 0.86, 0.83, respectively)were interpreted as reflecting split-half reli-ability coefficients. Recently, we evaluatedthe test-retest reliability of 10 olfactory testsin the same set of 57 subjects aged 24 to 84years.78 Included in this evaluation were fourdetection threshold tests (the PEA single-staircase threshold, the butanol single seriesascending method of limits threshold [BTJ,the PEMEC single-ascending method of limitsthreshold, and the Japanese T&T olfactom-eter-threshold series [T&TD. Most of the ol-factory tests, including the threshold tests,evidenced relatively high test-retest reliabilitycoefficients (ie, coefficients >0.65). A factoranalysis of the correlations among the testssupported the notion that most of the testsevaluated measure, in large part, a commonsensory domain.78.9s Whether this is true forsubject samples containing individuals witholfactory dysfunction as a result of definedclinical conditions, such as those arising from
head injury or degenerative diseases, is notknown.
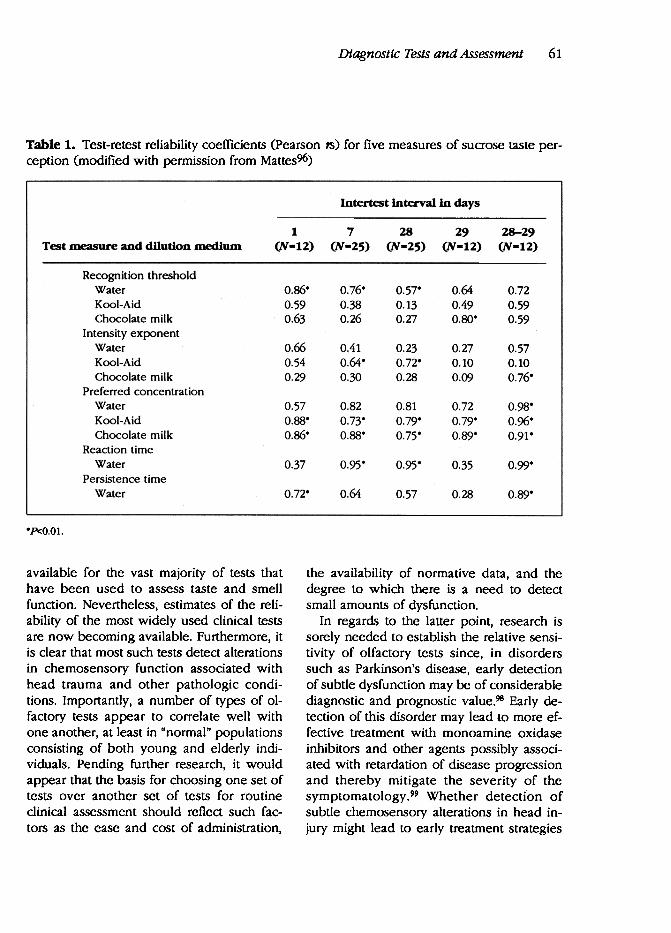
The literature on gustatory testing suggeststhat, as in the case of olfaction, considerableintra individual variability is present. In a rela-tively extensive study of 12- to 25-year-olds,Mattes96 assessed, over a 29-day period, test-retest reliabilities of five measures of sucrosetaste perception. These measures includedsweet recognition thresholds, exponents ofpower functions fit to suprathreshold inten-sity magnitude estimates, the most preferredsucrose concentration, reaction times to theonset of a sweet sensation following sucrosepresentation to the tongue, and the durationof such a sweet sensation. Tests were con-ducted separately for sucrose solutions dis-solved in three different media: (1) water, (2)cherry Kool-Aid, and (3) chocolate milk. Ascan be seen in Table 1, the threshold andpreference measures were more reliable thanthe magnitude estimation measures. Al-though the reaction time measure was quitereliable for some test intervals, it is notknown to what extent the high-reliability co-efficient is simply a reflection of the reliabil-ity of reaction times, per se.
As noted in a recent review of the epide-miology of olfactory dysfunction,97 formalstudies on the comparative sensitivity, speci-ficity, and positive predictive value ofchemosensory tests do not exist. Thus, whileit is clear from the present review that a num-ber of chemosensory tests are highly reliable,research is still needed to establish their rela-tive efficacy.
. . .
In the present article, both theoretical andpractical aspects of psychophysical chemo-sensory testing have been presented. It isapparent that basic psychometric parameterssuch as test reliability and validity are not
61Diagnostic Tests and Assessment
Table 1. Test-retest reliability coefficients (Pearson 18) for five measures of sucrose taste per-ception (modified with permission from Mattes96)
Intertest interval in days
1
(N-12)
7(N-25)
28(N-2S>
29
(N-12)
28-29
(N-12)Test ~ure and dilution medium
0.86.
0.59
0.63
0.76.
0.38
0.26
0.64
0.49
0.80°
0.57.
0.13
0.27
0.720.590.59
0.660.540.29
0.410.64.0.30
0.23
0.72.
0.28
0.270.100.09
0.57
0.10
0.76.
0.57
0.88.
0.86.
0.82
0.73"
0.88"
0.81
0.79.
0.75.
0.72
0.79.
0.89.
0.98.
0.96.
0.91.
Recognition thresholdWaterKooi-AidChocolate milk
IntensityexponentWaterKooI-AidChocolate milk
Preferred concentrationWaterKooI-AidChocolate milk
Reaction timeWater
Persistence timeWater
0.37 0.95. 0.95. 0.35 0.99.
0.72. 0.64 0.57 0.28 0.89.
.P<O.Ol.
available for the vast majority of tests thathave been used to assess taste and smellfunction. Nevertheless, estimates of the reli-ability of the most widely used clinical testsare now becoming available. Furthermore, itis clear that most such tests detect alterationsin chemosensory function associated withhead trauma and other pathologic condi-tions. Importantly, a number of types of ol-factory tests appear to correlate well withone another, at least in "normal" populationsconsisting of both young and elderly indi-viduals. Pending further research, it wouldappear that the basis for choosing one set oftests over another set of tests for routineclinical assessment should reflect such fac-tors as the ease and cost of administration,
the availability of normative data, and thedegree to which there is a need to detectsmall amounts of dysfunction.
In regards to the laner point, research issorely needed to establish the relative sensi-tivity of olfactory tests since, in disorderssuch as Parkinson's disease, early detectionof subtle dysfuncti9n may be of considerablediagnostic and prognostic value.98 Early de-tection of this disorder may lead to more ef-fective treatment with monoamine oxidaseinhibitors and other agents possibly assod-ated with retardation of disease progressionand thereby mitigate the severity of thesymptomatology.99 Whether detection ofsubtle chemosensory alterations in head in-jury might lead to early treatment strategies

62 JOURNAL OF HEAD TRAUMA REHABII.rrAnON/MARCH 1992
in order to minimize damage to the olfactorysystem and other neural pathways is notpresently known, but it is certainly a possibil-
ity.
are available at specialized smell and tastecenters located at university medical centers.Chemosensory tests can be of particularvalue in head injury, since they can provide aquantitative assessment of sensory impair-ment, establish the validity of chemosensorycomplaints, detect malingering, and objec-tively monitor changes during rehabilitation.
Health care professionals should be awareof the variety of diagnostic tests available forthe assessment of taste and smell function. Anumber of the tests discussed in this article
REFERENCES
13. ArnooreJE, Oilman BG. Practical test kits for quan-titatively evaluating the sense of smell. Rbi110logy.
1983;21:49-54.14. Cain WS, Gent JP, Goodspeed RB, Leonard G.
Evaluation of olfactory dysfunction in the Con-necticut Chemosensory Clinical Researd1 Center.
Laryngosc!¥Je. 1988;98:83-88.15. Punter PH. Measurement of human olfactory
thresholds for several groups of structurally relatedcompounds. Gbem Sens.1983;7:215-235.
16. Doty RL, Deems DA, Frye R, Pelberg R, Shapiro A.
Olfactory sensitivity, nasal resistance, and auto-nomic function in the multiple chemical sensitivi-ties (MCS) syndrome. Arcb Otolaryngol Head Neck
Su76'.1988;114:1422-1427.17. Kobal G, Hummel C. Cerebral d1emosensory
evoked potentials elicited by d1emical stimulationof the human olfactory and respiratory nasal mu-cosa. Electroencepbalogr Glin Neuropbysiol.
1988;71:241-250.18. Doty RL, Shaman P, Dann M. Development of the
University of Pennsylvania Smell IdentificationTest: A standardized microencapsulated test of ol-
factory function. Pbysiol Bebav. 1984;32:489-502.19. Elsberg CA, Levy I. The sense of smell: I. A new
and simple method of quantitative olfactometry.Bull Neurollnst NY. 1935;4:5-19.
20. Doty RL. A review of olfactory dysfunctions inman. AmJOtolaryngol. 1979;1:57-79.
21. Wenzel B. Techniques in olfactometry. PsycbolBull. 1948;45:231-246.
2? Zwaardemaker H. L'Odorat. Paris, France: Doin,
1925.23. Takagi SF. Human Olfaction. Tokyo. Japan: Tokyo
Press, 1989.24. O'Mahony M. The interstimulus interval for taste:
I. The efficiency of expectoration and mouth-rinsing in clearing the mouth of salt residuals. Per-
ception.1972;1:209-215.
1. Deems DA, DOly RL, Settle RG, Moore-Gillon V,
Shaman P, Mester AF, Kimmelman CP, BrightmanVJ , Snow JB Jr. Smell and taste disorders, a study of750 patients from the University of PennsylvaniaSmell and Taste Center. Arch Otolaryngol Head
N«:kSurg.I991;117:519-528.2. Burdach K, Doty RL. Retronasal flavor perception:
Influences of mouth movements, swallowing, and
spitting. Physiol Behav.1987;41:353-3S6.3. Mozell MM, Smith BP, Smith PE, Sullivan RL Jr,
Swender P. Nasal chemoreception in flavor identi-fication. Arch Otolaryngol.I969;90:131-137.
4. Smith DV. Taste and smell dysfunction. In:Paparella MM, Shumrick DA, Gluckman JL,Meyerhoff WL, eds. Otolaryngology, III. 3rd ed.Philadelphia, Pa: Saunders; 1991.
5. Stevens JC, Cain WS. Smelling via the mouth: Effect
of aging. Percept Psychophys. 1986;40:142-146.6. Banoshuk LM, GentJ, CatalanOlto FA, Goodspeed
RB. Clinical evaluation of taste. Amer J
Otolaryngol. 1983;4 :257-260.7. Harris H, Kalmus H. The measurement of taste
sensitivity to phenylthiourea (PTC). Ann Eugenics.
1949;15:24-31.8. Zwaardemaker H. The sense of smell. Acta Oto-
Laryngo11927;11 :3-15.9. Cheesman GH, Townsend MJ. Funher experiments
on the olfactory thresholds of pure chemical sub-stances, using the "sniff-bottle method." Q J Exp
psychol. 1956;8:8-14.10. Doty RL, Gregor T, Settle RG. Influences of
intertrial interval and sniff-bottle volume on thephenyl ethyl alcohol olfactory detection threshold.
ChemSens.1986;11:259-264.11. Semb G. The detectability of the odor of butanol.
Percept Psychophys. 1968;4:335-340.12. ToyOla B, Kitamura T, Takagi SF. Olfactory D':Sor-
ders-Olfactometry and Therapy. Tokyo, Japan:
Igaku-Shoin; 1978.

Diagnostic Tests and Assessment 63
25. Collings V. Human taste response as a function oflocus of stimulation on the tongue and soft palate.Percept Psycbophys. 1974;16:169-174.
26. Banoshuk LM, Desnoyers S, Hudson C, et al.Tasting on localized areas. NY Acad Sci.1987;510:166-168.
27. Frank ME, Hettinger TP, Hemess MS, Pfaffmann c.Evaluation of taste function by electrogustometry.In: Meiselman HL, Rivlin RS, eds. Clinical Mea-surement of Taste and Smell. New York, NY:MacmilJan; 1986:187-199.
28. MaruniakJA, Silver WL, Moulton DG. Olfactory reoceptors respond to blood-bome odorants. BrainRes. 1983;265:312-316.
29. GuilfordJP. psychometric methods. New York, NY:McGraw-Hill; 1954.
30. Schwartz BS. The epidemiology of olfactory dys-function. In: Laing DG, Doty RL, Breipohl B, eds.The Human Sense of Smell. Berlin, Germany:Springer-Verlag; 1991.
31. Doty RL. Olfactory system. In: Getchell TV, DotyRL, Bartoshuk LM, Snow JBJr, eds. Smell and Tastein Health and Disease. New York, NY: RavenPress; 1991-.
32. Miller IJ Jr, Banoshuk LM. Taste perception, tastebud distribution, and spatial relationships. In:Getchell TV, Doty RL, Banoshuk LM, Snow JB Jr,eds. Smell and Taste in Health and Disease. NewYork, NY: Raven Press; 1991.
33. Kobal G, Hummel T. Olfactory evoked potentialsin humans. In: Getchell TV, Doty RL, BartoshukLM, Snow JBJr, eds. Smell and Taste in Health andDisease. New York, NY: Raven Press; 1991.
34. Plattig KH. Gustatory evoked brain potentials inhumans. In: Getchell TV, Doty RL, Bartoshuk LM,Snow JB Jr, eds. Smell and Taste in Health andDisease. New York, NY: Raven Press; 1991.
35. Frank ME, Smith DV. Electrogustometry: A simpleway to test taste. In: Getchell TV, Doty RL,Bartoshuk LM, Snow JR Jr, eds. Smell and Taste inHealth and Disease. New York, NY: Raven Press;1991.
36. Moncrieff RW. The Chemical Senses. London, Eng:Leonard Hill; 1967.
37. Blackwell HR. Psychophysical thresholds: Experi-mental studies of methods of measurement. Bul-letin of the Engineering Research Institute. No 36,Ann Arbor, Mich: University of Michigan Press;1953.
38. O'Mahony M. Gustatory responses to nongustatorystimuli. Perception. 1983;12:627-633.
39. Wejffenbach JM. Taste-quality recognition andforced-choice response. Percept Psychophys.1983;33:251-254.
40. C0rnsweet TN. The staircase-method inpsychophysics. Am] psychol. 1962;75:485-491.
41. Deems DA, Doty RL Age-related changes in thephenyl ethyl alcohol odor detection threshold.Trans Pa Acad Ophlbalmol Otolaryngol.1987;39:64~50.
42. Cain WS. Sumner's "on testing the sense of smell"rev~ited. Yale] BiolMed.1982;55:51S-519.
43. Doty RL, Reyes P, Gregor T. Presence of both odoridentification and detection deficits in Alzheimer'sd~ease. Brain Res BuU.1987;18:597-600.
44. Wetherill GB, Levitt H. Sequential estimation ofpoints on a psychometric function. Brit] Math Statpsychol. 1965;18:1-9.
45. Tanner WP Jr, SwetsJA. A decision-making theoryof visual detection. psychol Rev. 1954;61:401-409.
46, O'Mahony M. Short-cut signal detection measure-ments for sensory analys~. ] Food Sci. 1979;44:302-303.
47. O'Mahony M, Gardner L, Long D, Heintz C,Thompson B, Davies M. Salt taste detection: An R-index approach to signal-detection measurements.
Perception. 1979;8:497-506.48. Potter H, Butters N. An assessment of olfactory
deficits in patients with damage to prefrontal cor-tex. Neu1qJsychologia. 1980;18:621-628.
49. Eichenbaum H, Morton TH, Potter H, Corkin C.Selective olfactory deficits in case HM. Brain.1983;106:459-472.
50. Weber EH. De pulsu, resorptione, auditu et tactu:Annotationes anatomicae et physiologicae.Leipzig, Germany: Koehier; 1834.
51. Scoville WB, Dunsmore RH, Liberson WT, HendryCE, Pepe A. Observations on medial temporallobectomy and uncotomy in the treatment of psy-choiic states. psychiatry Treatment. 1953;31:347-369.
52. Drake B, Johansson B, Yon Sydow D, Doving KB.Quantitative psychophysical and electrophysi-ological data on some odorous compounds. Scand] psychol. 1969;10:89-96.
53. Helson H. Adaptation-Level Theory: An Experi-mental and Systematic Approach to Bebavior. NewYork, NY: Harper & Row; 1964.
54. Anderson NH. Functional measurement andpsychophysical judgment. Psychol Rev.1970;77:15}-170.
55. Berglund B, Berglund U, Ekman G, Engen T. Indi-vidual psychophysical functions for 28 odorants.Percept Psycbophys. 1971 ;9:379-384.
56. Stevens ss. The psychophysics of sensory func-tion. In: Rosenblith WA, ed. Sensory Communica-tion. Cambridge, Mass: M rr Press, 1961.
57. Overbosch P. A theoretical model for perceived in-

64 JOURNAL OF HEAD TRAUMA REHABIUTAnON/MARcH 1992
tensity in human taste and smell as a function oftime. Chem Sens.1986;11:31S-329.
58. Marks LE. Sensory Processes. New York, NY: Aca-demic, 1974.
59. Moskowitz H. Magnitude estimation: Notes onwhat, how, when, and why to use it. J Food Qual-
ity.1977;3:19S-227.60. Baird JC, l.ewis C, Romer D. Relative frequencies
of numerical responses in ratio estimation. Perceptpsycbopbys.1970;8:358-362.
61. Myers At. Psychophysical scaling and scales ofphysical stimulus measurement. Psychol Bull.1982;92:203-214.
62. Lawless fIT, Malone GT. The discrimination effi-ciency of common scaling methods. J Sens Studies.1986; 1 :85-98.
63. Lawless fIT, Malone GT. A comparison of ratingscales: Sensitivity, replicates, and relative measure-ment. J Sens Studies 1986;1:155-174.
64. Marks LE, Stevens JC, Bartoshuk LM, Gent JF,Rifkin B, Stone VK. Magnitude matching: The mea-surement of taste and smell. Chem Sens.1988;13:63-87.
65. Marks LE, Szczesiul R, Ohlott P. On the cross-modal perception of intensity. J Exp Psychol.1988;12:517-534.
66. SalataJA, Doty RL, RajJM. Differential sensitivity oftongue areas and palate to electrical stimulation: Asuprathreshold cross-modal matching study. ChemSens.I99I;16:483-489.
67. FrijtersJER, Kooistra A, Vereijken PF. Tables of d'for the triangular method and the 3-AFC signal de-tection performance. Percept Psychophys.1980;27:176-178.
68. Schiffrnan SS, Reynolds Ml, Young FW. Introduc-tion to Multidimensional Scaling: Theory, Methods,and Applications. Orlando, Fla: Academic Press,1981.
69. Surnner D. On testing the sense of smell. Lancet.1962;ii:895-897.
70. Abraham A, Matha KV. The effect of right temporallobe lesions on matching of smells.Neu't¥1sychologia. 1983;21 :277-281.
71. Gregson RAM, Free Ml, Abbott MW. Olfaction inKorsakoffs, alcoholics and normals. Br J Clin
psycbol.1981;20:3-10.72. O'Mahony M, Thompson B. Taste quality descrip-
tions: Can the subject's response be affected bymentioning taste words in the instructions. ChemSens Flav. 1977;2:283-298.
73. Corwin J. Olfactory identification in hemodialysis:Acute and chronic effects on discrimination andresponse bias. Neu't¥1SYChologia.1989;27:513-522.
74. Cain WS. Gent 1, Catalanotto FA. Goodspeed RB.
Clinical evaluation of olfaction. Amer j
Otolaryngol. 1983;4:252-256.75. Wright HN. Characterization of olfactory dysfunc-
tion. Arch Otolaryngol Head Neck Surg.
1987;113:163-168.76. WoodJB, Harkins SW. Effects of age, stimulus se-
lection, and retrieval environment on odor identifi-cation. j Gerontol. 1987;42:584-588.
77. Cain WS, Rabin RD. Comparability of tWo tests ofolfactory functioning. Chem Sens. 1989;14:479-
485.78. Doty RL, Smith R, McKeown D, Raj J. A compari-
son of tests of olfactory function: Factor analysisand reliability studies. Chem Senses. 1992. Submit-ted for publication.
79. Doty RL. The Smell IdentifICation Test7JI Adminis-tration Manual. 2nd ed. Haddonfield, NJ:
Sensonics; 1989.80. Doty RL, Shaman P, Applebaum SL, Giberson R,
Sikorsky L, Rosenberg L. Smell identification abil-ity: Changes with age. Science. 1984;226:1441-
1443.81. Koster EP. Human psychophysics in olfaction. In:
Moulton DG, Turk A,JohnstonJW Jr, eds. Methodsin Olfactory Research. New York, NY: Academic
Press; 1975:345-374.82. Jones BP, Moskowitz HR, Butters N. Olfactory dis-
crimination in alcoholic Korsakoff patients.
Neuropsychologia.1975;13:173-179.83. Campbell IM, Gregson RAM. Olfactory short-term
memory in normal, schizophrenic, and brain dam-aged cases. Austj psychol. 1972;24:179-185.
84. Doty RL. A review of olfactory dysfunctions inman. AmjOtolaryngol. 1979;1:57-79.
85. Doty RL, Stern MB, Pfeiffer C, Gollomp SM, HurtigHI. Bilateral olfactory dysfunction in early stagemedicated and unmedicated idiopathicParkinson's disease. j Neurol Neurosurg Psychiatry.1992. In press.
86. Furukawa M, Kamide M, Miwa T, Umeda R. Impor-tance of unilateral examination on olfactometry.Auris Nasus Larynx. 1988;15:113-116.
87. Eskenazi B, Cain WS, Novelly RA, Mattson R. Odorperception in temporal lobe epilepsy patients withand without temporal lobectomy. Neuropsycho-
Iogia.1966;24:553-562.88. Bellas DN, Novelly RA, Eskenazi B, Wasserstein J.
The nature of unilateral neglect in the olfactory
sensory system. Neuropsycbologia. 1988;26:45-52.89. Griffith IP. Abnormalities of taste and smell. Prac-
titioner.1976;217:907-913.90. Doty RL, Agrawal U, Frye R. Evaluation of the in-
ternal consistency reliability of the fractionatedand whole Universitv of Pennsvlvania Smell

65Diagnostic Tests and Assessment
97. Schwartz BS. The epidemiology of olfactory dys-function. In: I.aing DG, Doty RL, Breipohl B, eds.The Human Sense of Smell. Berlin, Ger: Springer-Verlag, 1991.
98. Doty RL, Deems D, Stellar S. Olfactory dysfunctionin Parkinson's disease: A general deficit unrelatedto neurologic signs, disease stage, or disease du-ration. Neurology. 1988;38:1237-1244.
99. I.angston JW, Koller WC. The next frontier inParkinson's disease: Presymptornatic detection.Neurology. 1991;41Csuppl 2):5-7.
100. Doty RL. Psychophysical measurement of humanodor perception. In: I.aing DG, Doty RL, BreipohlB, eds. The Human Sense of Smell. Berlin, Ger-many: Springer-Verlag, 1991.
Identification Test. Percept Psycbopbys. 1989;45:
381-384.91. Stevens JC, Cain WS, Burke RJ. Variability of olfac-
tory thresholds. Gbem Sens. 1988;13:643-Q53.92. Heywood PG, Costanzo RM. Identifying
normosmics: A comparison of two populations.Amer jOtolaryngol.1986;7:194-199.
93. Koelega HS. Olfaction and sensory asymmetry.Gbem Sens Flav. 1979;4:89-95.
94. Cain WS, Gent JF. Olfactory sensitivity: Reliability,generality, and association with aging. j Exp
psycbol.I991;17:382-391.95. Yoshida M. Correlation analysis of detection
threshold data for "standard test" odors. Bull Fac-ully Sci Eng Gbuo Univ. 1984;27:343-353.
96. Mattes RD. Reliability of psychophysical measuresof gustatory function. Percept Psycbopbys.
1988;43:107-114.