
Diagnostic distinction anencephaly and amnion...
7
I Med Genet 1994;31:823-829 Original articles Diagnostic distinction between anencephaly and amnion rupture sequence based on skeletal analysis Jean W Keeling, Inger Kjar Royal Hospital for Sick Children, Edinburgh, UK J W Keeling Department of Orthodontics, School of Dentistry, Faculty of Health Sciences, University of Copenhagen, 20 Norre Alle, DK- 2200 Copenhagen N, Denmark I Kjter Correspondence to Dr Kjar. Received 2 June 1994 Accepted for publication 6 July 1994 Abstract The axial skeletal development of eight second trimester aborted fetuses, clin- ically diagnosed as amnion rupture se- quence with cranial involvement, was examined radiographically and hi- stologically. Three of the eight fetuses showed axial skeletal malformation in the spine and the craniofacial skeleton cor- responding to the malformations seen in anencephaly. These are vertebral body malformations, consisting of double cor- pora and of osseous malformations in the components of the cranial base, the corpus of the occipital bone, and the postsphenoid bone. These types of malformation, which have previously been described, are loc- ated along the original course of the no- tochord. The findings show that it is possible by means of radiography of the axial skeleton to distinguish between anencephalic fe- tuses which become secondarily involved in amnion rupture and fetuses which were initially normally developed. The method supplements detailed fetal examination and provides important information for genetic counselling. (37 Med Genet 1994;31:823-829) The amniotic band disruption complex or early amnion rupture sequence is characterised by a variety of combinations of fetal disruption, often involving different body regions, which are usually asymmetrical. Tissue bands, some- times running to the placental membranes are often, but not universally, observed particularly in the more mature fetus. A disrupted fetal part may be firmly adherent to placental membranes over a wide area.l" Theories about the aetiology and pa- thogenesis of this sequence are many and are discussed later. They do, however, underlie a major diagnostic problem, particularly when the cephalic region is involved. Seeds et al' drew attention to misdiagnosis and in- appropriate counselling and mentioned cranial defects as a potential source of confusion. Hughes and Benzie6 and Urich and Herrick7 cited amnion disruption as a cause of anen- Types of anomaly seen in amnion rupture sequence Fetuses* GA Fig Postmortem external examination Postmortem axial radiography Diagnosis No Craniofacial Trunk Limbs Amniotic band Cranial base Vertebral bodies Case 1 22 9 Meracrania, as Normal Bilateral talipes Head Normal, s Normal, s ARS Case 2 17 8 Meracrania, as Normal Small short Hands, feet Malformed Normal, s ARS Abnormal facial fingers, as sphenoid corpus clefts, as Toes curled up, (not anenceph Eye malf, as as type), s Vestigial big toe, as Case 3 15 1, 3 Holocrania, facial Imperforate anus Right arm absent Not seen Malformed Double vertebral Anencephaly cleft, ear, eye, Right leg red, (anenceph type), bodies and ARS as left white as and s (anenceph type), as and s Case 4 18 4A, 5 Meracrania, as Kyphoscoliosis Vestigial right arm Head, abdomen Normal, s Normal, s but ARS Abdominal Deformed lower torqued wall defect limbs, as Case 5 14 Meracrania, s Normal Normal Vertex Normal, s Normal, s ARS Case 6 17 4B, 6 Anencephalic Thoracic Bilateral talipes Head, abdomen Malformed Double vertebral Anencephaly facies, rachischisis (anenceph bodies and ARS protuberant Abdominal wall type), s (anenceph type), orbits, s defect s, but torqued Case 7 16 4C, 7 Holocrania, s Thoracolumbar Normal Abdomen Malformed Double vertebral Anencephaly rachischisis (anenceph bodies and ARS Omphalocele type), s (anenceph type), s, but torqued Case 8 16 Holocrania, as Abdominal wall Amputations and Hands, feet, Malformed Normal, s but ARS defect deformities of abdominal wall sphenoid corpus torqued extremities (not anenceph type), s * Fetuses are listed chronologically. GA = gestational age (wk). ARS = amnion rupture sequence. s = symmetry; as = asymmetry. 823 on 12 May 2018 by guest. Protected by copyright. http://jmg.bmj.com/ J Med Genet: first published as 10.1136/jmg.31.11.823 on 1 November 1994. Downloaded from
Transcript of Diagnostic distinction anencephaly and amnion...

I Med Genet 1994;31:823-829
Original articles
Diagnostic distinction between anencephaly andamnion rupture sequence based on skeletalanalysis
Jean W Keeling, Inger Kjar
Royal Hospital forSick Children,Edinburgh, UKJ W Keeling
Department ofOrthodontics, Schoolof Dentistry, Facultyof Health Sciences,University ofCopenhagen,20 Norre Alle, DK-2200 Copenhagen N,DenmarkI Kjter
Correspondence toDr Kjar.
Received 2 June 1994Accepted for publication6 July 1994
AbstractThe axial skeletal development of eightsecond trimester aborted fetuses, clin-ically diagnosed as amnion rupture se-
quence with cranial involvement, wasexamined radiographically and hi-stologically. Three of the eight fetusesshowed axial skeletal malformation in thespine and the craniofacial skeleton cor-responding to the malformations seen inanencephaly. These are vertebral bodymalformations, consisting of double cor-
pora and of osseous malformations in thecomponents ofthe cranial base, the corpusofthe occipital bone, and the postsphenoidbone. These types of malformation, whichhave previously been described, are loc-ated along the original course of the no-
tochord.The findings show that it is possible by
means ofradiography of the axial skeletonto distinguish between anencephalic fe-tuses which become secondarily involvedin amnion rupture and fetuses which were
initially normally developed. The methodsupplements detailed fetal examination
and provides important information forgenetic counselling.
(37 Med Genet 1994;31:823-829)
The amniotic band disruption complex or earlyamnion rupture sequence is characterised by a
variety of combinations of fetal disruption,often involving different body regions, whichare usually asymmetrical. Tissue bands, some-times running to the placental membranes are
often, but not universally, observed particularlyin the more mature fetus. A disrupted fetal partmay be firmly adherent to placental membranesover a wide area.l"
Theories about the aetiology and pa-thogenesis of this sequence are many and are
discussed later. They do, however, underlie a
major diagnostic problem, particularly whenthe cephalic region is involved. Seeds et al'drew attention to misdiagnosis and in-appropriate counselling and mentioned cranialdefects as a potential source of confusion.Hughes and Benzie6 and Urich and Herrick7cited amnion disruption as a cause of anen-
Types of anomaly seen in amnion rupture sequence
Fetuses* GA Fig Postmortem external examination Postmortem axial radiography DiagnosisNo
Craniofacial Trunk Limbs Amniotic band Cranial base Vertebral bodies
Case 1 22 9 Meracrania, as Normal Bilateral talipes Head Normal, s Normal, s ARSCase 2 17 8 Meracrania, as Normal Small short Hands, feet Malformed Normal, s ARS
Abnormal facial fingers, as sphenoid corpusclefts, as Toes curled up, (not anenceph
Eye malf, as as type), sVestigial big toe,
asCase 3 15 1, 3 Holocrania, facial Imperforate anus Right arm absent Not seen Malformed Double vertebral Anencephaly
cleft, ear, eye, Right leg red, (anenceph type), bodies and ARSas left white as and s (anenceph type),
as and sCase 4 18 4A, 5 Meracrania, as Kyphoscoliosis Vestigial right arm Head, abdomen Normal, s Normal, s but ARS
Abdominal Deformed lower torquedwall defect limbs, as
Case 5 14 Meracrania, s Normal Normal Vertex Normal, s Normal, s ARSCase 6 17 4B, 6 Anencephalic Thoracic Bilateral talipes Head, abdomen Malformed Double vertebral Anencephaly
facies, rachischisis (anenceph bodies and ARSprotuberant Abdominal wall type), s (anenceph type),orbits, s defect s, but torqued
Case 7 16 4C, 7 Holocrania, s Thoracolumbar Normal Abdomen Malformed Double vertebral Anencephalyrachischisis (anenceph bodies and ARS
Omphalocele type), s (anenceph type),s, but torqued
Case 8 16 Holocrania, as Abdominal wall Amputations and Hands, feet, Malformed Normal, s but ARSdefect deformities of abdominal wall sphenoid corpus torqued
extremities (not anencephtype), s
* Fetuses are listed chronologically. GA = gestational age (wk). ARS = amnion rupture sequence. s = symmetry; as = asymmetry.
823
on 12 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.31.11.823 on 1 Novem
ber 1994. Dow
nloaded from

Keeling, Kjar
In our experience, doubt about the dis-tinction between primary defects of cranialneural tube closure which subsequently adhereto the placental amnion and defects owing tosubsequent disruption of the normally closedcranial portion of the neural tube may persisteven after detailed fetal examination.The purpose of the present investigation is
to analyse the axial skeleton, comprising thespine and the craniofacial skeleton, in a group offetuses clinically diagnosed as amnion rupturesequence, by comparing the findings to normalskeletal patterns and to skeletal patterns re-cently described in a group of anencephalicfetuses.'01' The axial skeletons in anencephalyshowed characteristic malformations along theoriginal course of the notochord, which involvethe vertebral bodies, the basilar part of theoccipital bone, and the postsphenoid bone,supporting the pituitary gland. Four types ofradiographical and histological craniofacial de-
Figure 1 Schematic drawing indicating the axial skeletonand the central nervous system in a midsagittal tissueblock from a normal human fetus (14-16 weeks'gestation). The vertical arrow, p, indicates the pituitarygland in the sella turcica, and the oblique arrow, f, thecentral area in the frontal bone. Arrow n indicates theoriginal course of the notochord. Solid black areas showthe para-axialfy derived skeleton involved in anencephalicmalformation. Dotted bones show the neural crest derivedskeleton, sometimes malformed in anencephaly. 0
a
I
V_
V L
Figure 2 Drawings of radiographs of the midline craniofacial bcfetuses at different states of skeletal development. Stage A correspcgestation and stage B to 16 to 23 weeks. V= vertical projection. JFa, Fm, and Fp =fiontal proections of anterior, middle, and posmidsagittal tissue segment, respectively.
Fa Fm Fp
mes in two normal
onds to 14 to 16 weeks'L=lateral projection.terior parts of the
cephaly and pointed out the implications forcounselling. Goldstein and Filly8 stressed thesymmetry of the ultrasound abnormality inanencephaly as an important diagnostic featureofprimary neural tube defect, but as distinctionmay be very difficult9 detailed fetal examinationshould always be performed after terminationfor fetal anomaly.
Figure 3 Three human fetuses with placenta. Clinicaldiagnoses offetuses: amnion rupture sequence. (A)Gestational age 18 weeks. For radiographic examination,see fig 5. (B) Gestational age 17 weeks. For radiographicexamination, see fig 6. (C) Gestational age 16 weeks. Forradiographic examination, see fig 7. The external clinicalcharacteristics of the three fetuses do not permit distinctionbetween fetuses originally affected by anencephaly andsecondarily by amnion rupture sequence and fetuses onlyaffected by amnion rupture sequence.
n
0
824
a
on 12 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.31.11.823 on 1 Novem
ber 1994. Dow
nloaded from

Anencephaly and amnion rupture sequence
Figure 4 Radiographs offetus shown in fig 3A. (A) Whole body radiograph. (B)Lateral radiograph of midsagittal cranial structures showing normal structures of thebasilar part of the occipital bone (o) and of the postsphenoid bone component (sp). (C)Frontal radiograph ofposterior cranial base segment (Fp segment) indicating occipitaland sphenoid bone components, same as in (B). The radiographs show normal spinecontour with a pronounced curvature and normal cranial base bony component,indicating a normal fetus affected by amnion rupture sequence.
viations in anencephaly have previously beendescribed." These are deformed/normal con-
tours, cleft palate, short nasal septum, andmultilocular ethmoid cartilage malformation.The goal is to assess the validity of skeletalinvestigations as a contribution to the im-provement of genetic counselling in amnionrupture sequence.
Material and methodsFETUSESThe series comprised eight human fetuses withdiagnosed amion rupture sequence from legallyapproved therapeutic abortions. The fetuses
were derived from a consecutive series of abor-ted fetuses examined during 1987 to 1989at the Department of Histopathology, JohnRadcliffe Hospital, Oxford, UK. The main dataconcerning age and necropsy are shown inthe table. Foot lengths were between 14 and39mm, corresponding to gestational ages be-tween approximately 14 and 22 weeks.From the time of routine diagnostic ex-
amination until the present investigation, thefetuses were kept fixed in 10% buffered form-alin.
RADIOGRAPHYWhole body radiographs in frontal and lateralprojections were first taken. Tissue was thendissected for further radiological analysis. Thisincluded a midsagittal tissue block of the cra-nium and the entire spine (fig 1). The sec-tioning was done from the interior side of thecranial base by letting two sagittal incisionstouch the lateral borders of the foramen mag-num. The incisions continued on both sides ofthe often extremely curved and torqued spine tothe very caudal end. The interjacent midsagittalsegment was radiographed in frontal and lateralprojections before and after being stretchedout.The midsagittal tissue block of the cranial
base was separated from the spine and dividedby means oftwo frontal sections into three partsof equal fronto-occipital dimensions: anterior(Fa), middle (Fm), and posterior (Fp). Theseblocks were examined in lateral and frontalprojection (fig 2). The following distinctionswere made: notochordal axial skeleton: the ver-tebral bodies of the spine and the Fp segment,constituting the axial skeleton posterior to thesella turcica; craniofacial skeleton: Fa and Fmsegment, constituting the axial skeleton an-terior to the sella turcica.A Grenz ray radiographic apparatus, Hewlett
Packard, Faxitron Series 43805 N x ray systemwas used with Kodak X-Omat film. The tissuewas placed directly on the film envelope. De-pending on the size of the specimen, the tubevoltage varied between 20 and 60kV, and theexposure time from 10 to 60 seconds at 2-8 to3-0mA.From the radiographs, enlarged paper copies
and drawings of the ossified tissue were madeand used for the detailed analysis. Similar ra-diographs and outline drawings from a series ofnormal fetuses with corresponding gestationalage, foot length, and general skeletal de-velopment (assessed by counting the numberof ossified bones in hand and foot'2) were usedas controls. 3 Two normal developmental stagesin the spine'4 and two stages in the cranialbase and craniofacial skeleton""'9 covered thematerial under study.
HISTOLOGYAfter radiography, the Fa and Fm tissue blockswere embedded in paraffin, cut frontally into5 gm sections, and stained with toluidine blueat pH 7. Tissue from a series of normal fetusesof corresponding gestational age was used forcontrol purposes.
825
on 12 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.31.11.823 on 1 Novem
ber 1994. Dow
nloaded from

Keeling, Kjar
Figure 6 Radiographs offetus shown in fig 3C. (A)Lateral radiograph of whole body. (B) Frontal radiographof cervical and upper thoracic part of the spine indicatingthe existence of double vertebral bodies. (C) Lateralradiograph of midsagittal cranial structures indicatingmalformed basilar part of occipital bone (o). (D) Frontalradiographs of anterior, middle, and posterior segments ofthe midsagittal craniofacial segment indicating normalbony contours in front of the malformed sphenoid body(sp). The spine and the bony contours in the cranial baseindicate that the fetus is presumably anencephalic,secondarily affected by amnion rupture sequence.
Figure S Radiographs offetus shown in fig 3B. (A) Lateral radiograph of the wholebody. (B) Lateral radiograph of midsagittal axial tissue segment including the spine andcranial components. (C) Frontal radiograph of stretched spine and cranial basemidsagittal segtnent showing double vertebral bodies in the cervical and upper thoracicregions. (D), (E) Frontal radiographs of tissue segments from the midsagittal cranial baseshowing the postsphenoid bone component (sp) and the basilar part of the occipital bone(o). Both bony structures are malformed. The spine and the bony contours in the cranialbase indicate that the fetus is presumably anencephalic, secondarily affected by amnionrupture sequence.
ResultsThe morphological abnormalities and postnatalaxial radiography of all fetuses are set out inthe table.The analysis of the spine and the craniofacial
skeleton showed that three of the eight fetusesshowed a skeletal developmental pattern ident-ical to that observed in anencephaly. Thesethree fetuses are shown in figs 3B, 3C, 5, 6, 7,and 8.
NOTOCHORDAL AXIAL SKELETONIt was a characteristic finding in the threefetuses with an anencephalic ossification pat-tern that double or malformed vertebral bodiesoccurred in the spine and, corresponding tothis pattern in the spine, the basilar parts ofthe occipital bone (Fp segment) are short inthe craniocaudal dimension. In all three casesmalformations were also seen in the region ofthe rostral end of the notochord, in post-sphenoid bone, supporting the pituitary gland.The five fetuses without an anencephalic
ossification pattern showed a normal os-sification pattern in the spine, as illustrated infigs 4 and 9, and a normal appearance of thebasilar part of the occipital bone (Fp segment),illustrated in figs 4, 9, and 10. The post-sphenoid bone appeared normal in two cases(figs 4 and 10) and had a horseshoe shape,open anteriorly, in one case (fig 9). This typeof malformation was never observed in anen-cephaly.The five fetuses not showing anencephalic
malformations in the spinal skeleton, oftenshowed severely distorted spines (fig 8).
CRANIOFACIAL SKELETONIn five cases external asymmetry of the cranio-facial structures was recorded. Three cases ap-peared to be symmetrical in externalcraniofacial appearance. In the present in-vestigation one of the three fetuses with ananencephalic axial ossification pattern showedasymmetrical multilocular ethmoid cartilage(fig 8), and the remaining fetuses showed sym-metrical craniofacial skeletal morphologythough disrupted contours.The cleft in the palate and lip of one fetus
(fig 9) was a mucosa covered, midsagittallylocated furrow, seemingly caused by distortion.There was no resemblance to developmentallyrelated cleft lip, which occurs parasagittally,
826
on 12 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.31.11.823 on 1 Novem
ber 1994. Dow
nloaded from
Anencephaly and amnion rupture sequence
.,gp
U-
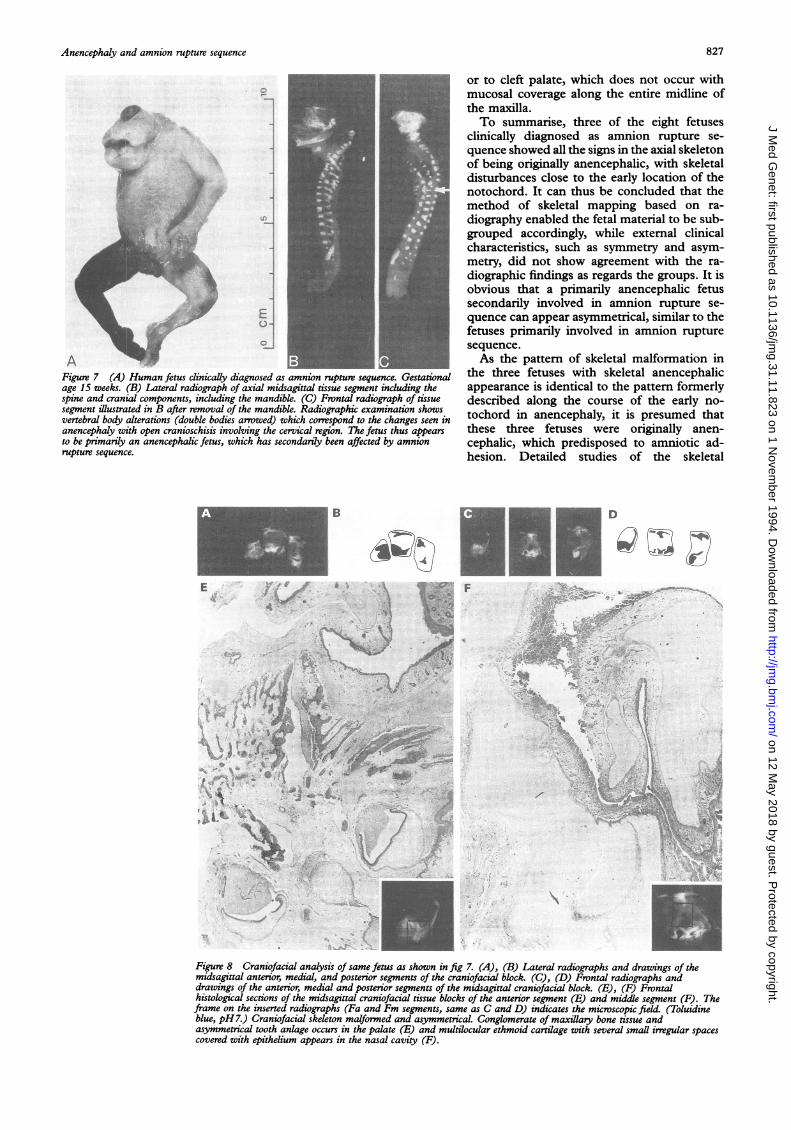
AFigure 7 (A) Human fetus clinicaly diagnosed as amnion rupture sequence. Gestationalage 15 weeks. (B) Lateral radiograph of axial midsagittal tissue segment induding thespine and cranial components, including the mandible. (C) Frontal radiograph of tissuesegment illustrated in B after removal of the mandible. Radiographic examination showsvertebral body alterations (double bodies arrowed) which correspond to the changes seen inanencephaly with open cranioschisis involving the cervical region. The fetus thus appearsto be primarily an anencephalic fetus, which has secondardy been affected by amnionrupture sequence.
B
E
p, tv
N.,
1.C5a .
or to cleft palate, which does not occur withmucosal coverage along the entire midline ofthe maxilla.To summarise, three of the eight fetuses
clinically diagnosed as amnion rupture se-quence showed all the signs in the axial skeletonof being originally anencephalic, with skeletaldisturbances close to the early location of thenotochord. It can thus be concluded that themethod of skeletal mapping based on ra-diography enabled the fetal material to be sub-grouped accordingly, while external clinicalcharacteristics, such as symmetry and asym-metry, did not show agreement with the ra-diographic findings as regards the groups. It isobvious that a primarily anencephalic fetussecondarily involved in amnion rupture se-quence can appear asymmetrical, similar to thefetuses primarily involved in amnion rupturesequence.As the pattern of skeletal malformation in
the three fetuses with skeletal anencephalicappearance is identical to the pattern formerlydescribed along the course of the early no-tochord in anencephaly, it is presumed thatthese three fetuses were originally anen-cephalic, which predisposed to amniotic ad-hesion. Detailed studies of the skeletal
D
4 - s>
Pi ^* gJ '/
Figure 8 Craniofacial analysis of same fetus as shown in fig 7. (A), (B) Lateral radiographs and drawings of themidsagittal anterior, medial, and posterior segments of the craniofacial block. (C), (D) Frontal radiographs anddrawings of the anterior, medial and posterior segments of the midsagittal craniofacial block. (E), (F) Frontalhistological sections of the midsagittal craniofacial tissue blocks of the anterior segment (E) and middle segment (F). Theframe on the inserted radiographs (Fa and Fm segments, same as C and D) indicates the microscopic field. (Toluidineblue, pH7.) Craniofacial skeleton malformed and asymmetrical. Conglomerate of maxillaty bone tissue andasymmetrical tooth anlage occurs in the palate (E) and multilocular ethmoid cartilage with several small irregular spacescovered with epithelium appears in the nasal cavity (F).
827
..i
I-1
'.*i,.-J4 lf.
Ark
i...
k-,41w-". -4
on 12 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.31.11.823 on 1 Novem
ber 1994. Dow
nloaded from

828
Figure 9 Human fetus with amnion rupture sequence.Gestational age 17 weeks. (A) Facial appearance. (B)Lateral radiograph of axial midsagittal segment includingthe spine and cranial components. Nornal appearance ofspine and basilar part of the occipital bone (o). (C)Frontal radiograph of segment in (B) after removal of themandible. The posterior part of the sphenoid bone (sp)appears horseshoe shaped, a malformation pattern notnormally occurring in anencephaly. The fetus appears tobe a normal human fetus secondarily affected by amnionrupture sequence.
development of fetuses with amnion rupturesequence, based on a larger number of cases,may clarify the situation further.
DiscussionEarly theories about the pathogenesis ofamnionrupture sequence attempted to explain all ob-served abnormalities through a single mech-anism. Streeter' discounted a causal role for theamniotic bands or strings and proposed a prim-ary germline defect within the developing em-bryo. Torpin2 considered that early rupture ofthe amniotic membrane resulted in the de-velopment ofmesodermal bands which effectedthe asymmetrical disruptions. This theory wassupported by the infrequency of anomalies inthe affected fetus away from regions of surfacedisruption and its occurrence in families withinherited connective tissue disorders.20 It wassuggested that the timing of amnion rupturemight explain the wide variation of distributionand severity of abnormalities.3 More recent re-views have drawn attention to familial cases2'and the presence of internal structural defects,some of which might be explained by vasculardisruption22 and suggest that amniotic bands are
a late event in the process. It is important to notethat physical manipulation ofthe gestational sacduring chorionic villus sampling can producevascular disruption in the embryo.23 Lockwoodet al24 suggested that amniotic bands are alwayssecondary and may complicate embryonic orfetal disruption from any cause provided that itaffects cutaneous integrity. Donnai and Winter25moved back towards Streeter' and postulatedthat a human homologue of the mouse mutantdisorganisation (DS) gene might explain somecases of amniotic disruption, drawing parallelsbetween abnormalities observed in these miceand some of the human fetuses. This mousemodel exhibits both asymmetrical limb defectsand exencephaly,2"28 while complex ham-artomas are frequently present both close to thebody surface and within body cavities. Lowergenitourinary malformations are frequent andthoracoschisis and gastroschisis are occasionalfindings. Hummel27 gives no indication of thenumber ofanimals with multiple abnormalities,although this is clearly seen from her il-lustrations. In the more recent study28 the ma-jority (88.5%) of abnormal mice had only asingle anomaly, 10% had two, and 1.4% hadthree separate anomalies, whereas multiple de-fects involving different body areas are usual inhuman ARS. The disorganisation mutationmodel would be more convincing if familialcases, in the absence of conditions which mightbe expected to predispose to amnion rupture,were observed more frequently. Bamforth29 alsosupported Streeter' and suggested that the ab-normal neuropore closure and consequent er-rors in migration of cephalic neural crest tissueexplain most of the observed defects. Mo-
Figure 10 Human fetus with amnion rupture sequence.Gestational age 22 weeks. (A) Appearance of neck. (B)Lateral radiograph of axial midsagittal segment of cranialcomponents. The basilar part of the occipital bone (o) andthe postsphenoid bone (sp) appear normal. (c) Frontalradiograph of postsphenoid bone (sp) and occipital bone(o) shown in B. The radiographs indicate that this is anormal human fetus secondarily affected by amnionrupture sequence.
Keeling, Kjcer
FIFF,
on 12 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.31.11.823 on 1 Novem
ber 1994. Dow
nloaded from

Anencephaly and amnion nupture sequence
ermann et al"0 considered that the Streeter' andTorpin2 theories are not mutually exclusive, thatconfusion has been compounded by lumpingtogether the more severe defects, best explainedby Streeter based hypotheses and the localised,often peripheral disruptions which are morelikely to result from local amnion disruption,2just because both groups involve adherence toplacental membranes. Yang3' had observed thesame confusion and suggested that cases oflimb-body wall complex be removed from con-
sideration ofamnion rupture sequence. He sug-gested that histological examination of theplacenta enabled the distinction to be made.
Systematic mapping of the axial skeletalcomponents in fetuses with amnion rupturesequence, as performed in the presentinvestigation, does notseem to havebeen carriedout before. The axial skeletal tissue is assumedto reflect the condition ofthe notochord, knownto be involved in neural tube closure and alsoin the formation of sclerodermal tissue.32 Thus,radiography ofthe axial skeleton seems valuablein evaluating anencephalic conditions resultingfrom malfunction of the notochord.The method described seems also to be valid
in timing the onset of malformation, since a
fetus with a normal spine has inevitably been ex-
posed to amniotic band disturbance in the axialskeleton later than a fetus with types of mal-formations such as double vertebral bodies(without ossification in the notochord region),which can be traced back to the very early failurein notochordal induction ofthe para-axial scler-oderm. This condition cannot arise later, afterthe vertebral bodies have been formed normallyby bone encircling the notochord.Timing has been recognised as an important
element in evaluating the pathogenesis.' 2133 34 Itis generally agreed that the earlier the amnioticbands form during gestation, the greater thelikelihood of associated abnormalities. In thepresent report, it is obvious that the latest eventto interfere with fetal craniofacial developmentmust be the one in the fetus illustrated in fig10. In this case it is to be supposed that thesphenoid bone had formed normally, beforedisruption. This is not the case in fig 9, wheredevelopment ofthe sphenoid bone is abnormal.This bone normally forms at 14 weeks of gest-ation, which is later than the onset of os-sification of the occipital bone.6"1719 Thedisruption of craniofacial bones is also de-pendent on local interactions.
Further studies of the axial skeleton in am-nion rupture sequence fetuses with cranial in-volvement are needed to confirm the findingsof this small study. It is important in geneticcounselling to be able to distinguish primaryanencephaly from secondary disruption.4 Wesuggest that analysis of the axial skeleton beincluded in the diagnostic examination of am-nion rupture fetuses. The observations ofDonnai and Wmter,25 and the observation offamilial cases2' and internal malformations22underline the need for detailed fetal ex-amination and careful history taking and a morecautious approach to parental counselling thanhas perhaps been the case in the recent past.
This investigation was supported by grants 12-9762, 12-0405,and 12-0885 from the Danish Medical Research Council, andby gants from the Danish Dental Association (FUT).
1 Streeter GL. Focal deficiencies in fetal tissues and theirrelation to intrauterine amputations. Contrib EmbryolCarnegie Inst 1930;22:1-44.
2 Torpin R. Amniochorionic mesoblastic fibrous strings andamnionic bands. Am Jf Obstet Gynecol 1965;91:65-75.
3 Higginbottom MC, Jones KL, Hall BD, Smith DW. Theamniotic band disruption complex: timing of amnioticrupture and variable spectra of consequent defects. JPediatr 1979;95:544-9.
4 Keeling JW, Boyd PA. Congenital malformations, prenataldiagnosis and fetal examination. In: Keeling JW, ed. Fetaland neonatal pathology. 2nd ed. Chapter 4. London:Springer-Verlag, 1993.
5 Seeds JW, Cefalo RC, Herbert WNP. Amniotic band syn-drome. Am Jf Obstet Gynecol 1982;144:243-8.
6 Hughes RM, Benzie RJ. Amniotic band syndrome causingfetal head deformity. Prenat Diagn 1984;4:447-50.
7 Urich H, Herrick MK. The amniotic band syndrome as acause of anencephaly. Report of a case. Acta Neuropathol1985;67: 190-4.
8 Goldstein RB, Filly RA. Prenatal diagnosis of anencephaly:spectrum ofsonographic appearances and distinction fromthe amniotic band syndrome. Am Jf Roentgenol 1988;151:547-50.
9 Harrington BJ, Horger EO, Edwards JG. A counselingdilemma involving anencephaly, acrania and amnioticbands. Genet Counsel 1992;3: 183-6.
10 Kjalr I, Keeling JW, Graem N. The midline maxillofacialskeleton in human anencephalic fetuses. Cleft PalateCraniofac J 1994;31:250-6.
11 Kjar I, Keeling JW, Graem N. Cranial base and vertebralcolumn in human anencephalic fetuses. J Craniofac GenetDev Biol (in press).
12 Kjer I. Skeletal maturation of the human fetus assessedradiographically on the basis of ossification sequences inthe hand and foot. Am J Phys Anthropol 1974;40:257-76.
13 Kjzr I, Graem N. Simple autopsy method for analysis ofcomplex fetal cranial malformations. Pediatr Pathol 1990;10:717-27.
14 Kjaer I, Kj:er TW, Graem N. Ossification sequence of oc-cipital bone and vertebrae in human fetuses. Jf CraniofacGenet Dev Biol 1993;13:83-8.
15 Kjzr I. Prenatal skeletal maturation of the human maxilla.Jf Craniofac Genet Dev Biol 1989;9:257-64.
16 Kjer I. Radiographic determination of prenatal basicranialossification. J7 Craniofac Genet Dev Biol 1990;10: 113-23.
17 Kjoer I. Ossification of the human fetal basicranium. JCraniofac Genet Dev Biol 1990;10:29-38.
18 Kjar I. Prenatal human cranial development evaluated oncoronal plane radiographs. J Craniofac Genet Dev Biol1990;10:339-51.
19 Kjaer I. New methods of analyzing bone growth and bonematuration of the human fetal cranium. In: Dixon AD,Sarnat GB, Hoyte DAN, eds. Fundamentals ofbone growth:methodology and applications. Boca Raton: CRC Press,1990: 51-60.
20 Young ID, Lindenbaum RH, Thompson EM, Pembrey ME.Amniotic bands in connective tissue disorders. Arch DisChild 1985;60:1061-3.
21 Hunter AGW. Carpenter BF. Implications of malformationsnot due to amniotic bands in the amniotic band sequence.Am JMed Genet 1986;24:691-700.
22 Van Allen MI, Curry C, Gallagher L. Limb body wall com-plex. I. Pathogenesis. AmJfMed Genet 1987;28:529-48.
23 Quintero RA, Romero R, Mahoney MJ, Vecchio M, HoldenJ, Hobbins J. Fetal haemorrhagic lesions after chorionicvillous sampling. Lancet 1992;339:193.
24 Lockwood C, Ghidini A, Romero R, Hobbins JC. Amnioticband syndrome: reevaluation of its pathogenesis. Am JObstet Gynecol 1989;160:1030-3.
25 Donnai D, Winter RM. Disorganisation: a model for 'earlyamnion rupture'? J Med Genet 1989;26:421-5.
26 Hummel KP. The inheritance and expression of dis-organization, an unusual mutation in the mouse. J ExpZool 1985;137:389-423.
27 Hummel KP. Developmental anomalies in mice resultingfrom action of the gene, disorganisation, a semi-dominantlethal. Pediatrics 1959;23:212-21.
28 Crosby JL, Varnum DS, Nadeau JH. Two-hit model forsporadic congenital anomalies in mice with the dis-organization mutation. Am JfHum Genet 1993;52:866-74.
29 Bamforth JS. Amniotic band sequence: Streeter's hypothesisreexamined. Am J Med Genet 1992;44:280-7.
30 MoermanP,FrynsJP, Vandenberghe K, LauwerynsJM. Con-strictive amniotic bands, amniotic adhesions, and limb-body wall complex: discrete disruption sequences with pa-thogenetic overlap. AmJrMed Genet 1992;42:470-9.
31 Yang SS, ADAM sequence and innocent amniotic band:manifestations of early amnion rupture. Am J Med Genet1990;37:562-8.
32 Kjaer I. The prenatal axial skeleton as marker of normal andpathological development of the human central nervoussystem. In: Lou HC, Greisen G, Larsen JF, eds. Brainlesions in the newborn. Hypoxic and haemodynamic pa-thogenesis. Copenhagen: Munksgaard, 1994: 124-35.
33 Heifetz SA. Strangulation of the umbilical cord by amnioticbands: report of 6 cases and literature review. PediatrPathol 1984;2:285-304.
34 Miller MT, Deutsch TA, Cronin C, Keys CL. Amnioticbands as a cause of ocular anomalies. Am J Ophthalmol1 987;104:270-9.
829
on 12 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.31.11.823 on 1 Novem
ber 1994. Dow
nloaded from


















