Diagnostic difficulties with lesions of the oral mucosa · Diagnostic difficulties with lesions of...
69
School of Clinical Dentistry University of Sheffield Diagnostic difficulties with Diagnostic difficulties with lesions of the oral mucosa lesions of the oral mucosa Paul M Speight Paul M Speight Dept Oral & Maxillofacial Pathology Dept Oral & Maxillofacial Pathology University of Sheffield University of Sheffield BDIAP London, November 2010
Transcript of Diagnostic difficulties with lesions of the oral mucosa · Diagnostic difficulties with lesions of...
School of Clinical DentistryUniversity of Sheffield
Diagnostic difficulties with Diagnostic difficulties with lesions of the oral mucosalesions of the oral mucosa
Paul M SpeightPaul M Speight
Dept Oral & Maxillofacial PathologyDept Oral & Maxillofacial PathologyUniversity of SheffieldUniversity of Sheffield
BDIAPLondon, November 2010
AimAimTo provide an overview of some key problems in oral mucosal pathology
OutlineOutline
•To review oral potentially malignant lesions•To review grading schemes for epithelial dysplasia•To describe the clinico-pathological features of lesions which may be confused with cancer or precancer
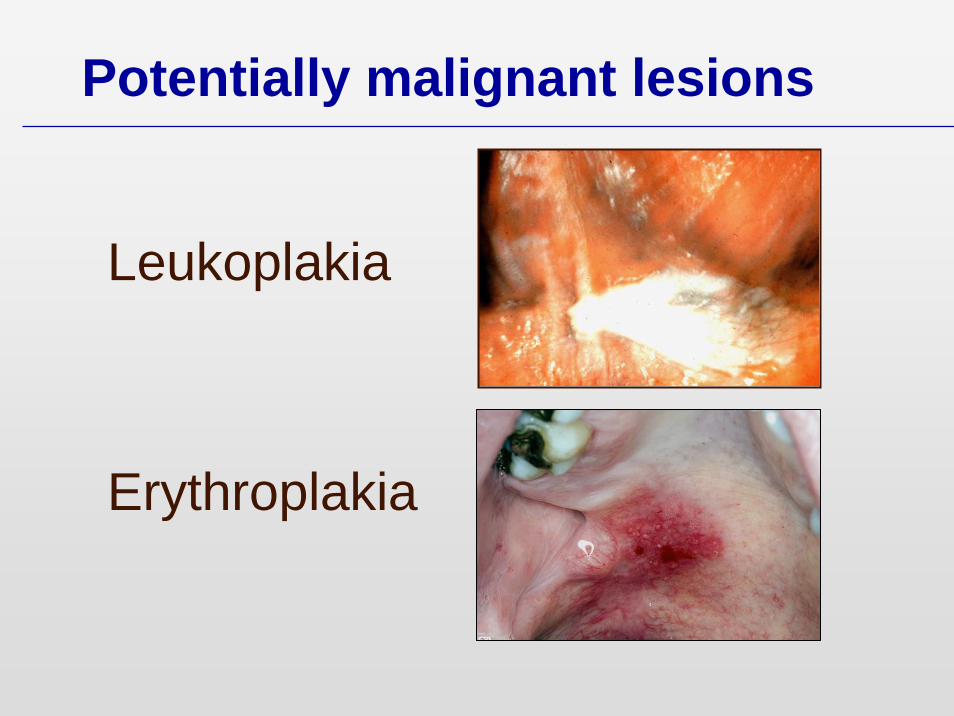
Leukoplakia
Erythroplakia
Potentially malignant lesions
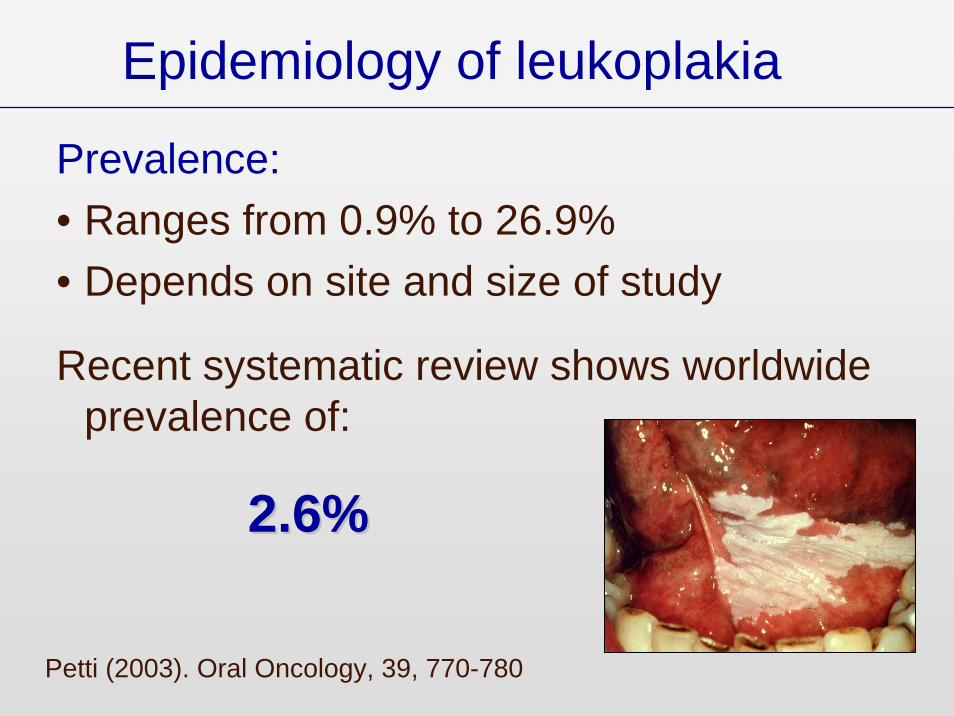
Epidemiology of leukoplakia
Prevalence:• Ranges from 0.9% to 26.9%• Depends on site and size of study
Recent systematic review shows worldwide prevalence of:
2.6%2.6%
Petti (2003). Oral Oncology, 39, 770-780

Leukoplakia• Homogeneous 1-5%• Non-homogeneous 20%
Erythroplakia 80%
PML and malignancy

Overal only about 5% become malignant
95% do not progress
Leukoplakia and malignancy
How do we identify this 5%?How do we identify this 5%?

Is epithelial dysplasia a useful marker of progression in oral potentially malignant lesions?
Epithelial dysplasiaEpithelial dysplasia

Leukoplakia - Histology
• Up to 80% show no dysplasia
• 20% - 50% show dysplasia
• 5% show carcinoma-in-Situ
• 5% are squamous cell carcinoma
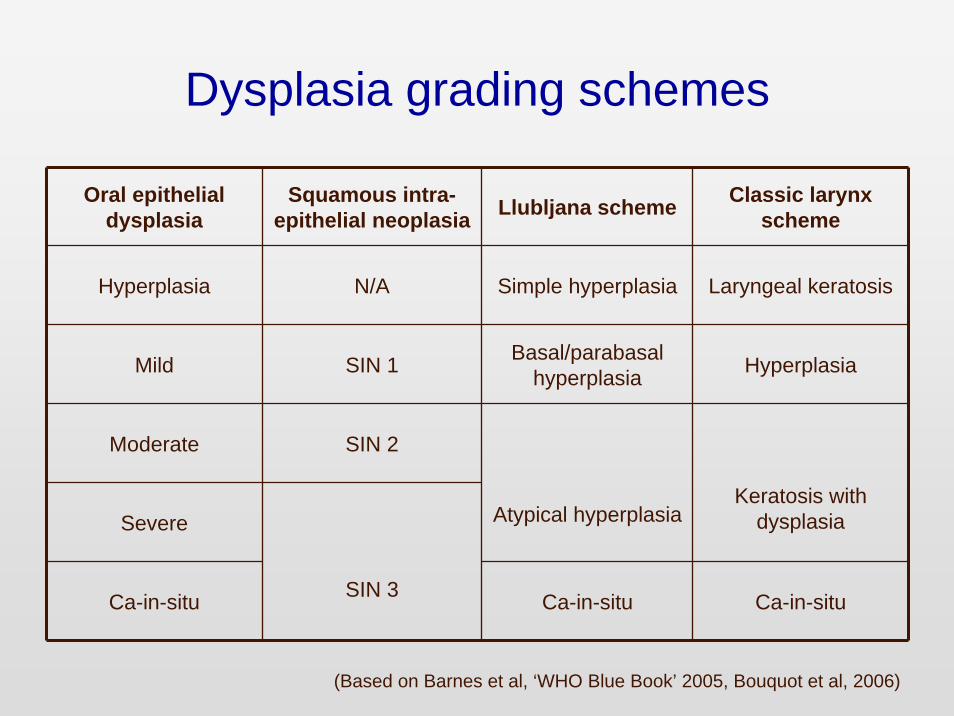
Dysplasia grading schemes
Oral epithelial dysplasia
Squamous intra-epithelial neoplasia Llubljana scheme Classic larynx
scheme
Hyperplasia N/A Simple hyperplasia Laryngeal keratosis
Mild SIN 1 Basal/parabasal hyperplasia Hyperplasia
Moderate SIN 2
Severe Atypical hyperplasiaKeratosis with
dysplasia
Ca-in-situ SIN 3 Ca-in-situ Ca-in-situ
(Based on Barnes et al, ‘WHO Blue Book’ 2005, Bouquot et al, 2006)

Grading of oral epithelial dysplasia
• Mild • Moderate• Severe• Carcinoma-in-situ
Grading is subjective based on a combination of cellular and architectural
features

Cellular changes:• Abnormal variation in nuclear size and shape
(anisonucleosis and pleomorphism)
• Abnormal variation in cell size and shape (anisocytosis and pleomorphism)
• Increased nuclear/cytoplasmic ratio
• Enlarged nuclei and cells
• Hyperchromatic nuclei
• Increased mitotic figures
• Abnormal mitotic figures (abnormal in shape or location)
• Increased number and size of nucleoli
Barnes L et al: 2005 WHO Classification
Architectural (Tissue) changes:• Loss of polarity
• Disordered maturation from basal to squamous cells
• Includes top-to-bottom change of carcinoma in situ
• Increased cellular density
• Basal cell hyperplasia
• Dyskeratosis (premature keratinization and keratin pearls deep in epithelium)
• Bulbous drop shaped rete pegs
• Secondary extensions (nodules) on rete tips
Barnes L et al: 2005 WHO Classification

Cellular changes
Pleomorphism of cells and nuclei

Cellular changes
Hyperchromatism & increased nuclear size and nuc/cyt ratio
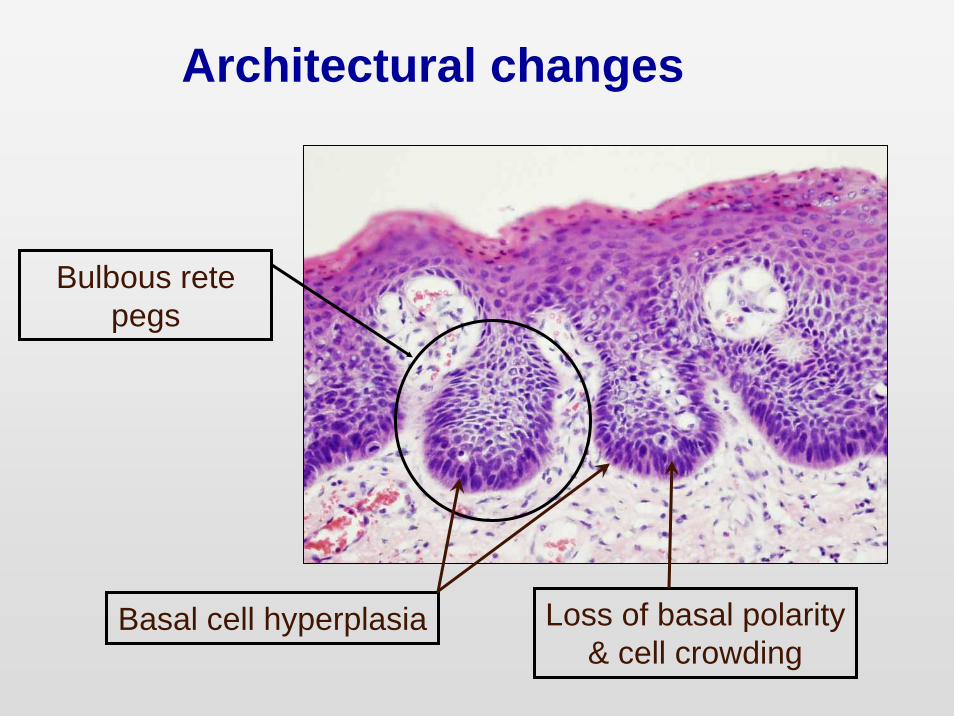
Architectural changes
Basal cell hyperplasia
Bulbous rete pegs
Loss of basal polarity& cell crowding
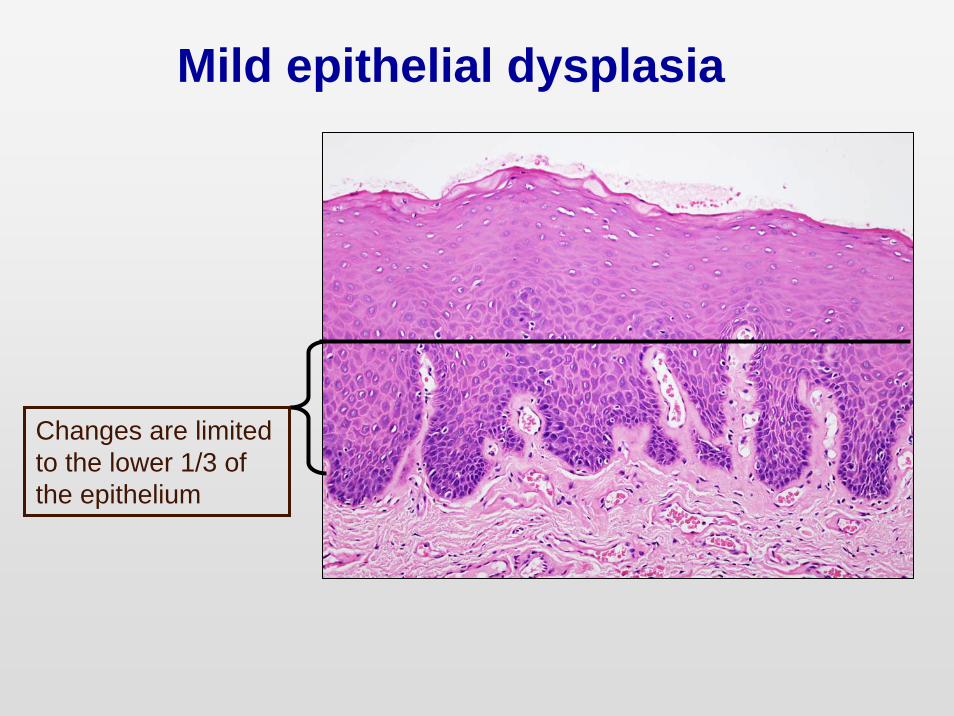
Mild epithelial dysplasia
Changes are limited to the lower 1/3 of the epithelium

Moderate epithelial dysplasia
Changes extend in to the middle 1/3 of the epithelium
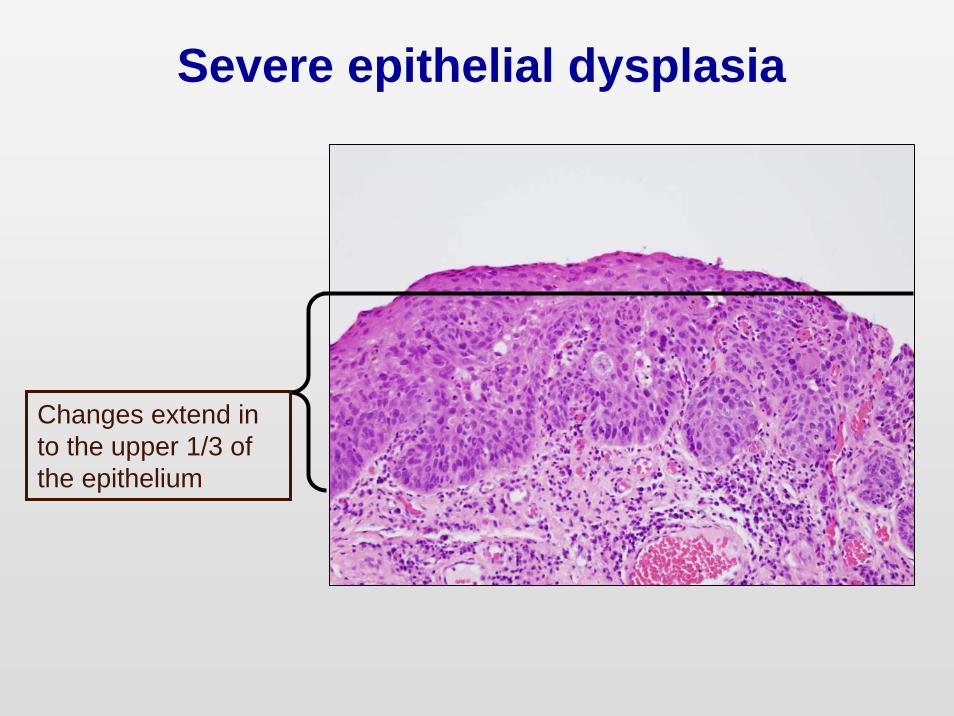
Severe epithelial dysplasia
Changes extend in to the upper 1/3 of the epithelium

Carcinoma-in-situ
Changes extend through the full thickness of the epithelium
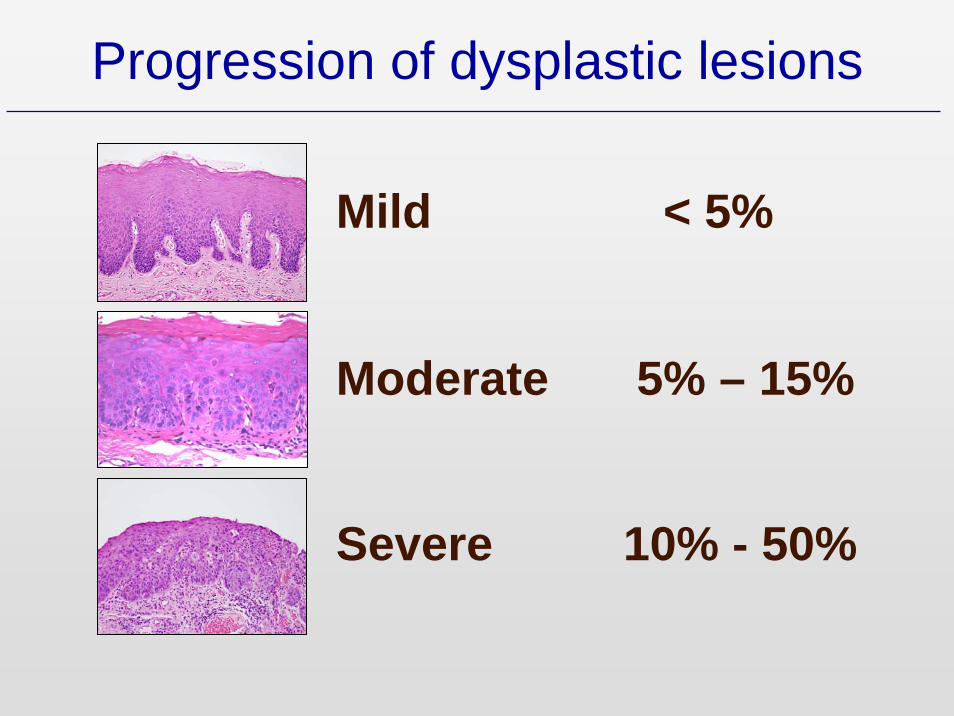
Progression of dysplastic lesions
Mild < 5%
Moderate 5% – 15%
Severe 10% - 50%
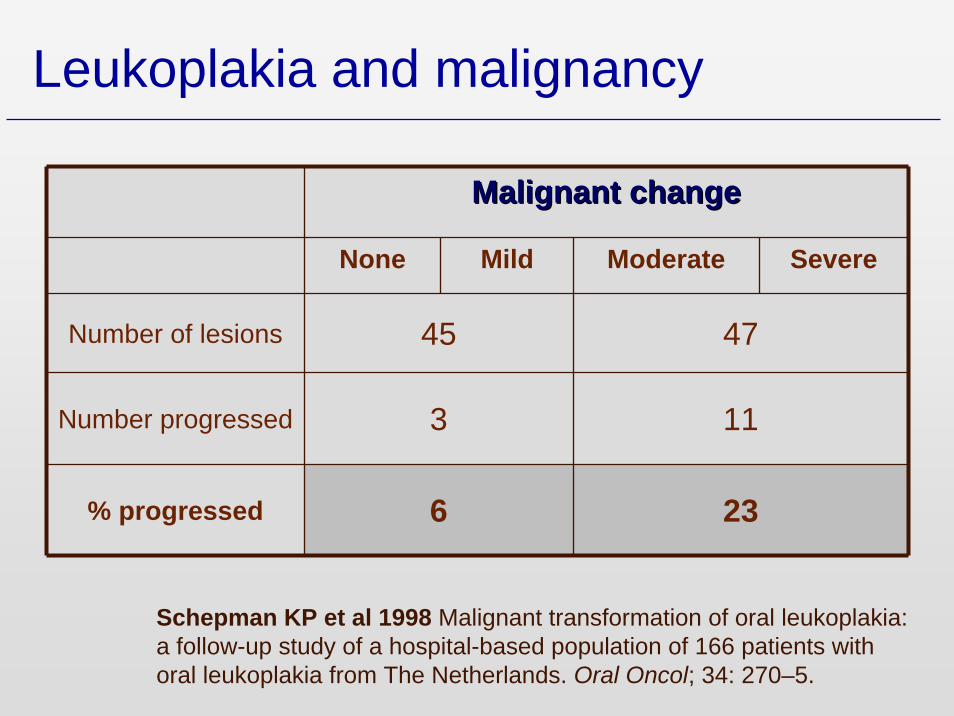
Leukoplakia and malignancy
Malignant changeMalignant change
None Mild Moderate Severe
Number of lesions 45 47
Number progressed 3 11
% progressed 6 23
Schepman KP et al 1998 Malignant transformation of oral leukoplakia: a follow-up study of a hospital-based population of 166 patients with oral leukoplakia from The Netherlands. Oral Oncol; 34: 270–5.
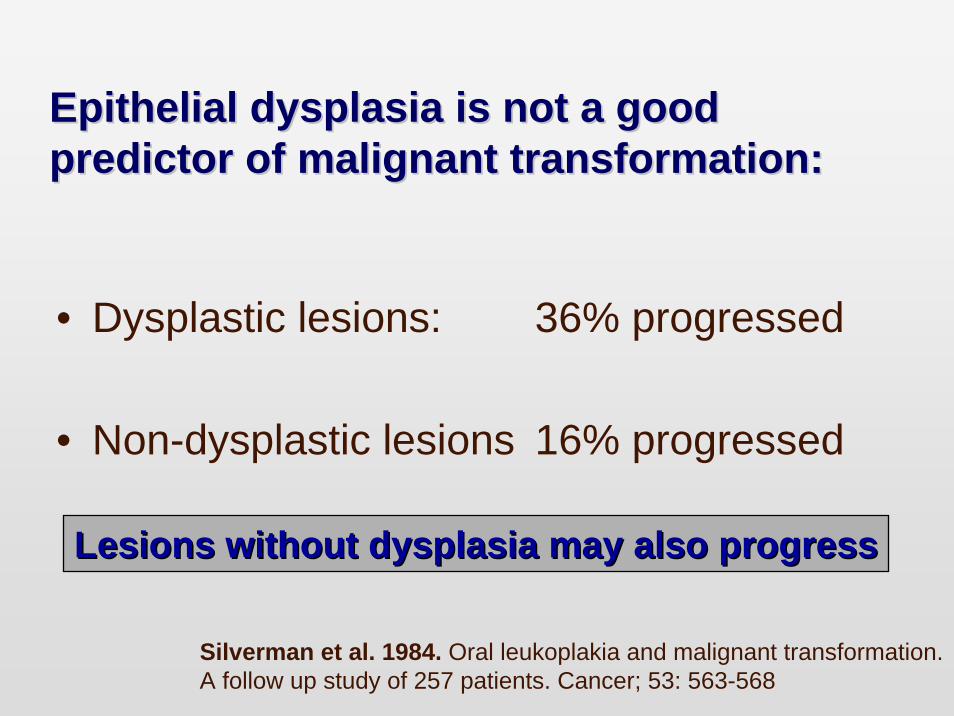
Epithelial dysplasia is not a good Epithelial dysplasia is not a good predictor of malignant transformation:predictor of malignant transformation:
• Dysplastic lesions: 36% progressed
• Non-dysplastic lesions 16% progressed
Silverman et al. 1984. Oral leukoplakia and malignant transformation. A follow up study of 257 patients. Cancer; 53: 563-568
Lesions without dysplasia may also progressLesions without dysplasia may also progress
Grading of oral epithelial dysplasia
Grading is subjective based on a combination of cellular and architectural features
Grading is regarded as unreliable

Inter-examiner variability in diagnosis
κs % agreementBrothwell et al, 2003 0.51 (0.42 - 0.58) 77 (75 – 85)
Karabulut et al, 1995 0.35 (0.27 - 0.45) 55 (49 – 69)
Abbey et al, 1995 0.46 (0.29 - 0.57) 82 (66 – 86)
K values calculated for presence/absence of dysplasia
Values show fair to moderate agreement only
• 68 cases
• 4 observers
• Calculated κs and for the 5 point scale and for the binary scale
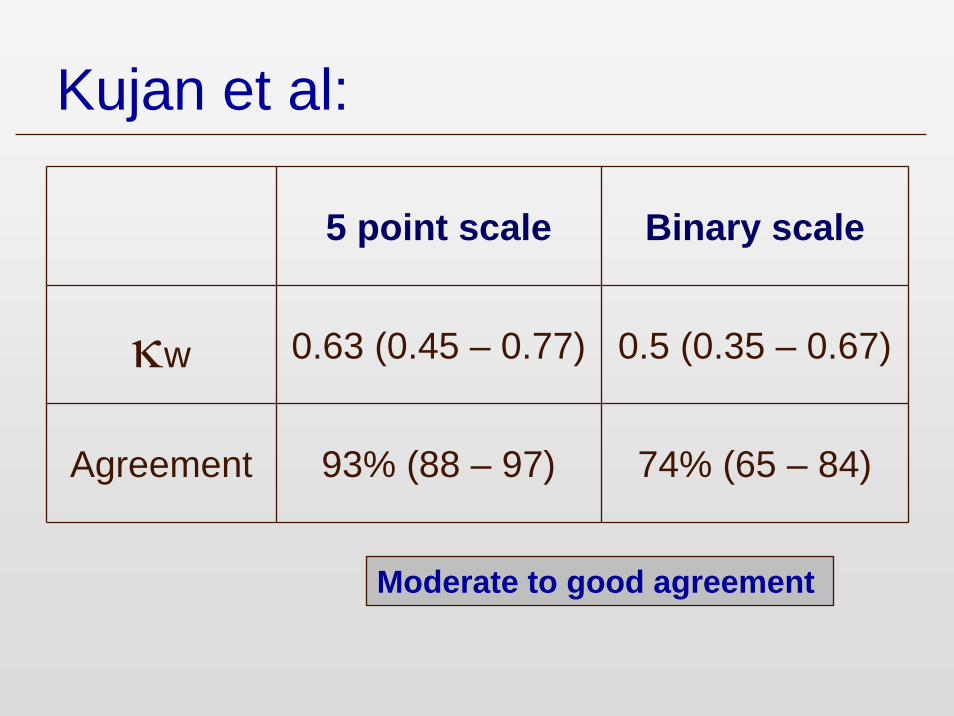
Kujan et al:
5 point scale Binary scale
κw 0.63 (0.45 – 0.77) 0.5 (0.35 – 0.67)
Agreement 93% (88 – 97) 74% (65 – 84)
Moderate to good agreement
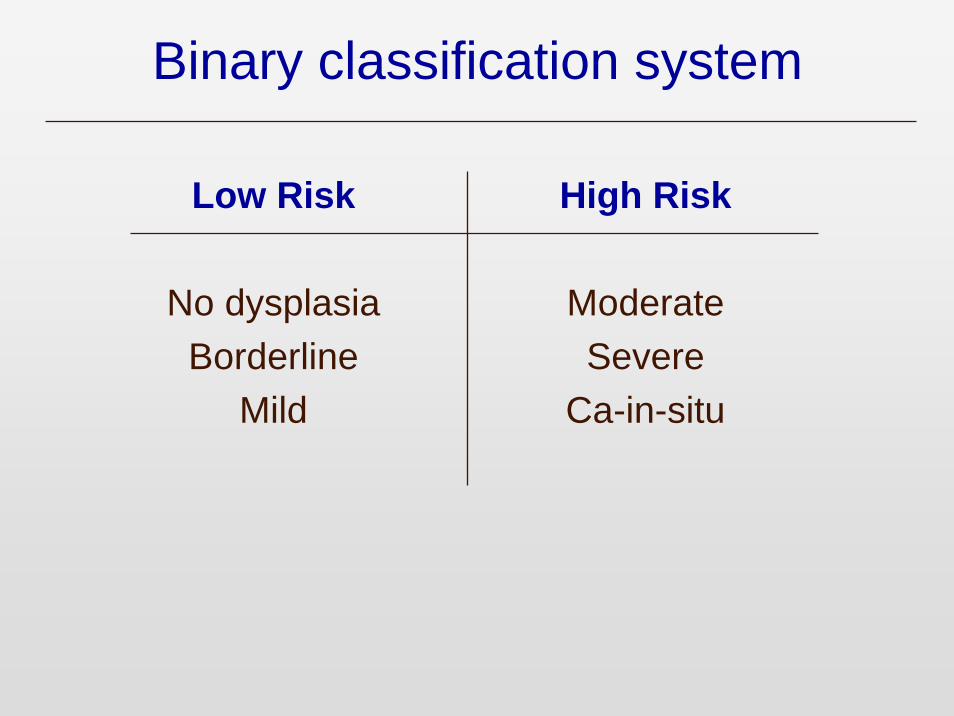
Binary classification system
Low Risk
No dysplasiaBorderline
Mild
High Risk
ModerateSevere
Ca-in-situ
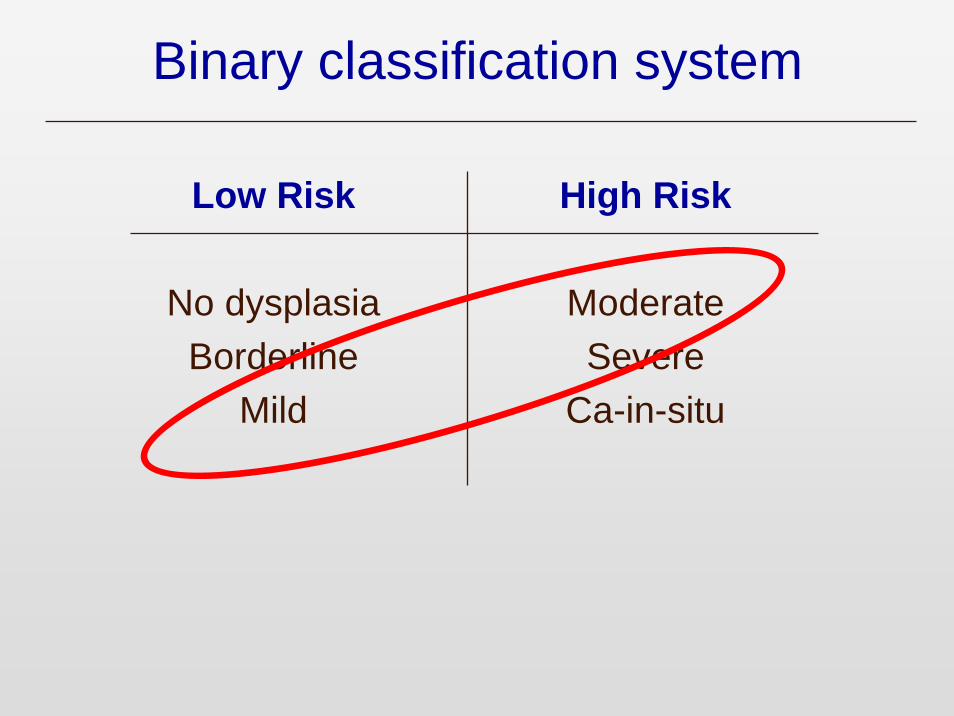
Binary classification system
Low Risk
No dysplasiaBorderline
Mild
High Risk
ModerateSevere
Ca-in-situ

Conclusions
• Epithelial dysplasia is still probably the best indicator of malignant progression in oral potentially malignant lesions
• BUT there are still major issues to be resolved:

Conclusions
There is a consensus that better tools are needed for the prediction of malignant progression in oral potentially malignant lesions
• Biomarkers• DNA ploidy analysis• Cytology

Bernard Ackerman:
“ The term dysplasia has never been defined in a lucid, comprehensible, repeatable way and ……….. has no place in the parlance of pathology”
Bernard Ackerman:
“ The term dysplasia has never been defined in a lucid, comprehensible, repeatable way and ……….. has no place in the parlance of no place in the parlance of pathologypathology”


• Reviewed 60 cases
• 10% progressed to SCC within 5 years



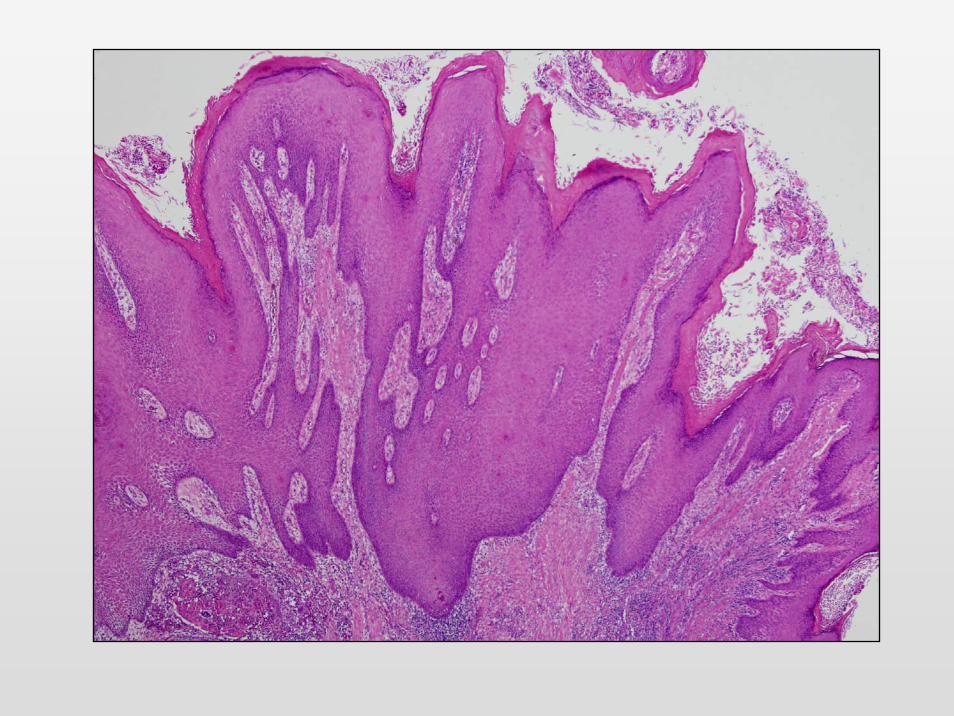
Proliferative verrucous leukoplakiaProliferative verrucous leukoplakia
A potentially malignant lesion
Characterised by• Multiple and recurrent white patches• Lesions persist and progress• Lesions are non-homogeneous:• Papillary or verruciform surface pattern• Cytologically bland


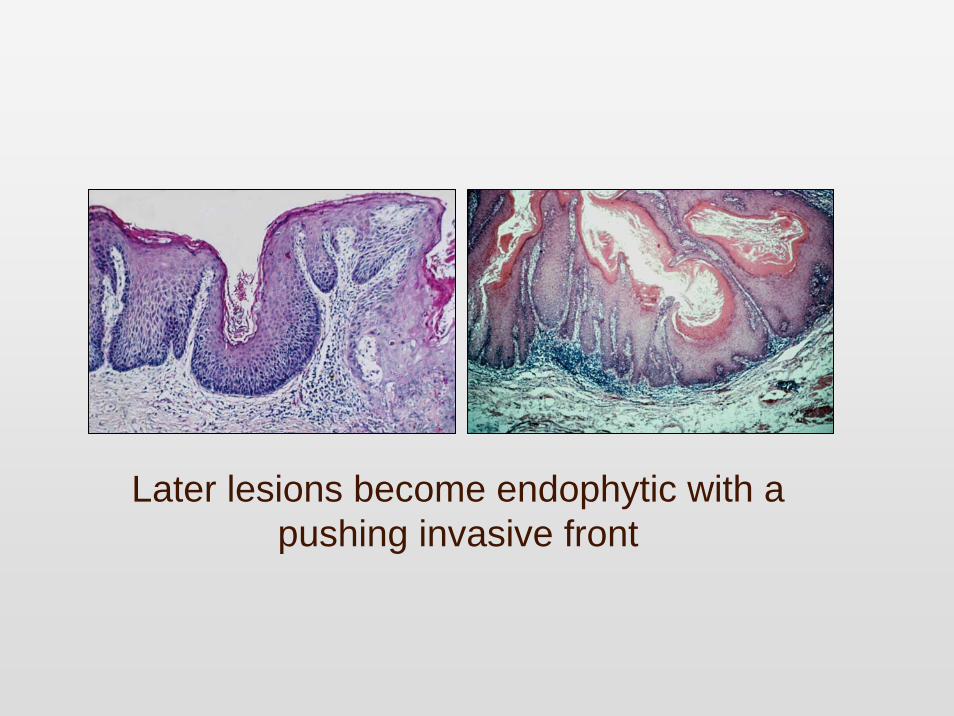
Later lesions become endophytic with a pushing invasive front
Proliferative verrucous leukoplakiaProliferative verrucous leukoplakia
Histology
• Start as flat hyperkeratotic lesions• Develop into hyperplasia with
papillary/verrucous surface• ‘Verruciform hyperplasia’• Usually exophytic
• Cytological atypia is minimal
Proliferative verrucous leukoplakiaProliferative verrucous leukoplakia
A potentially malignant lesion
• 70% - 100% become malignant• Progress to conventional squamous carcinoma
Diagnosis is retrospective and can only be made on the basis of a history of
recurrent and persistent lesions
Zakrzewska JM et al. 1996 Proliferative verrucous leukoplakia: a report of ten cases Oral Surg;82:396-40

Epithelial dysplasia ??
Problems in oral mucosal pathologyProblems in oral mucosal pathology
• Lesions which may be confused with cancer or precancer

Viral atypia (koilocytic dysplasia)
Fornatora et al. OOOE 1996; 82; 47

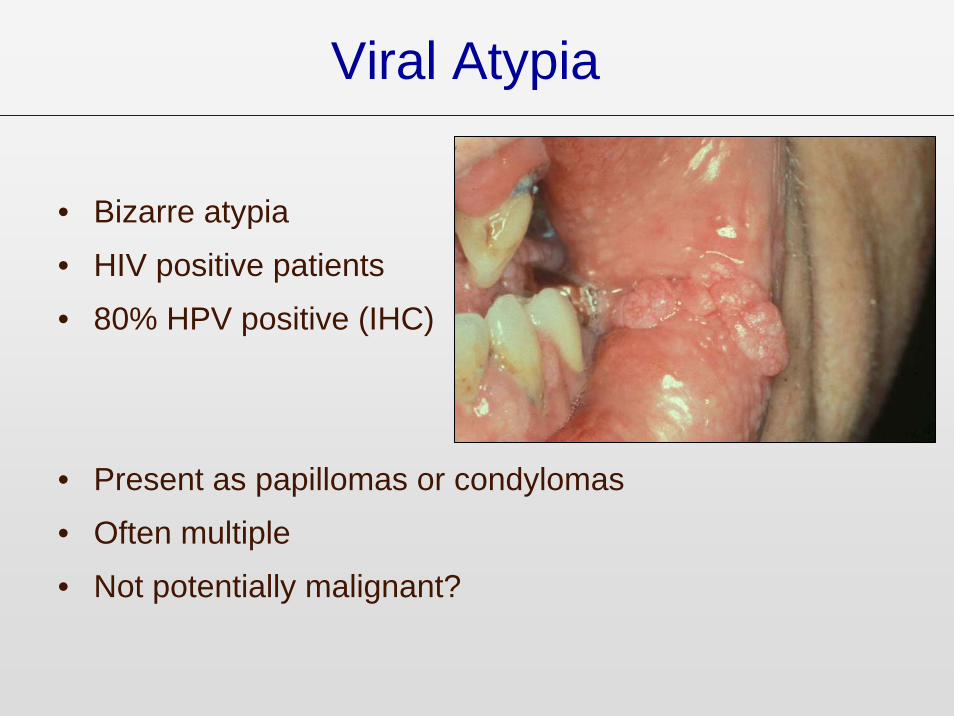
Viral Atypia
• Bizarre atypia
• HIV positive patients
• 80% HPV positive (IHC)
• Present as papillomas or condylomas
• Often multiple
• Not potentially malignant?

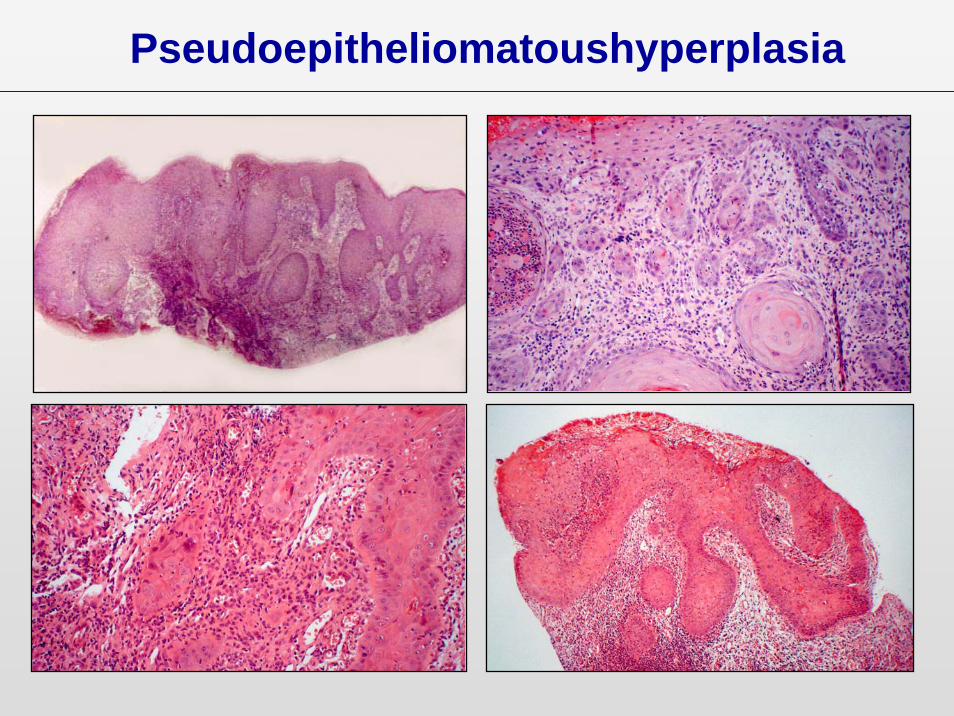
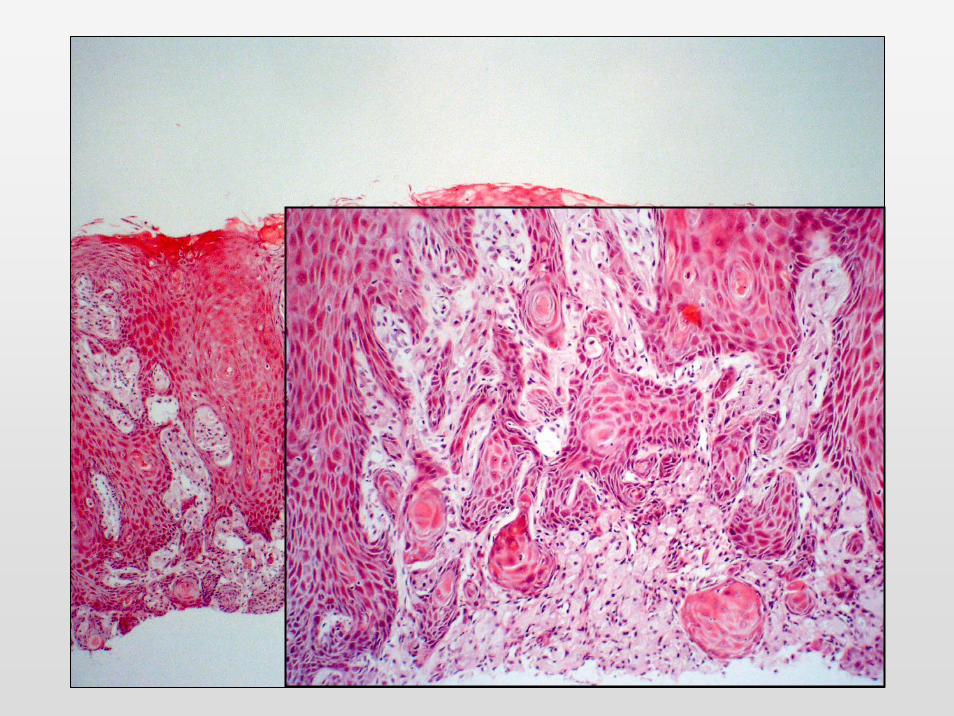
Pseudoepitheliomatoushyperplasia

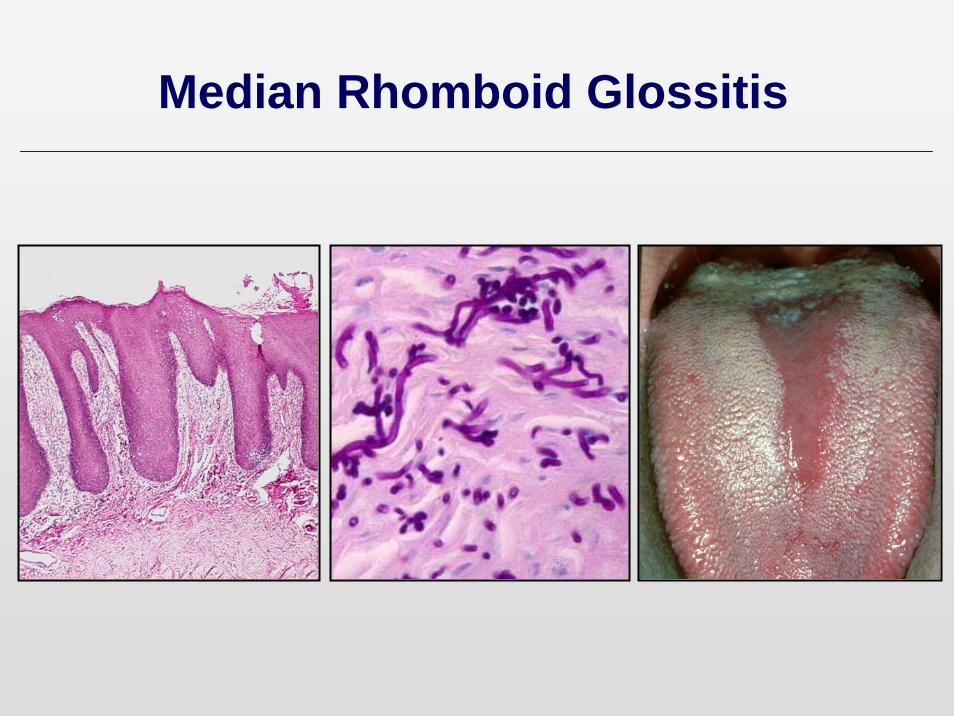
Median Rhomboid Glossitis

• Midline dorsum of tongue• Aetiolgy unclear• Associated with candida
infection• Pseudoepitheliomatous
hyperplasia common• Often mistaken clinically and
histologically for carcinoma• Presents at a site which is v rare
for malignancy
Median Rhomboid Glossitis
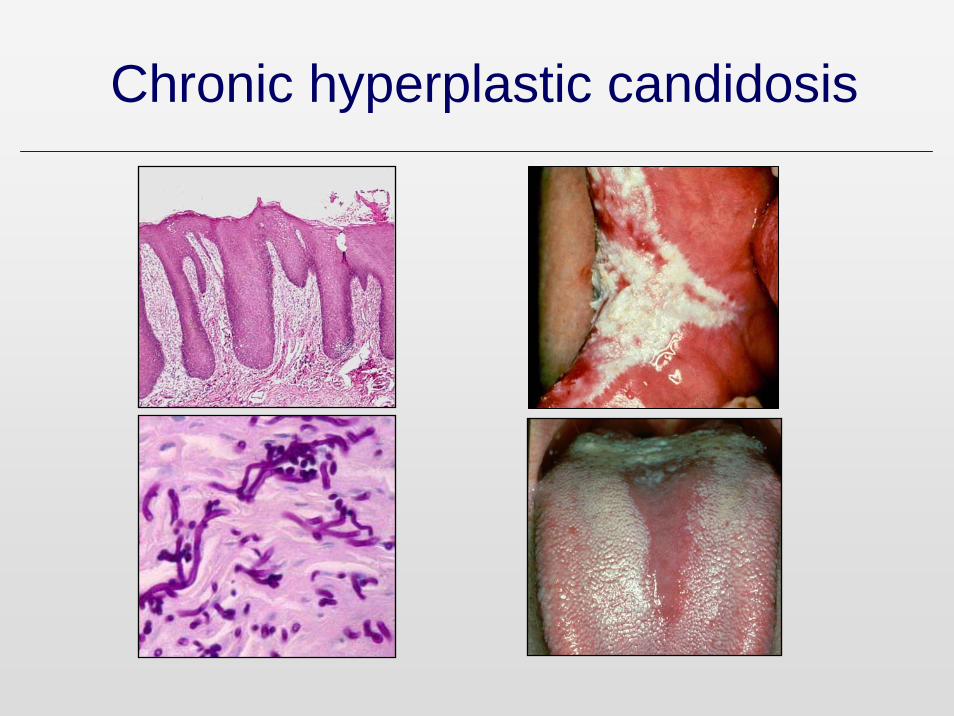
Chronic hyperplastic candidosis
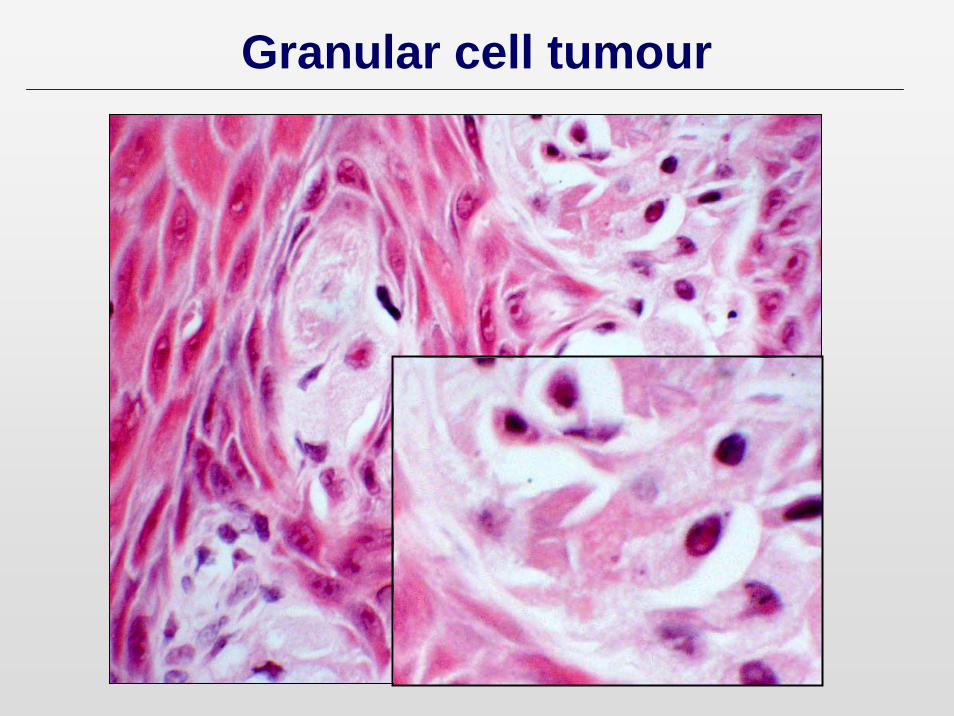
Granular cell tumour
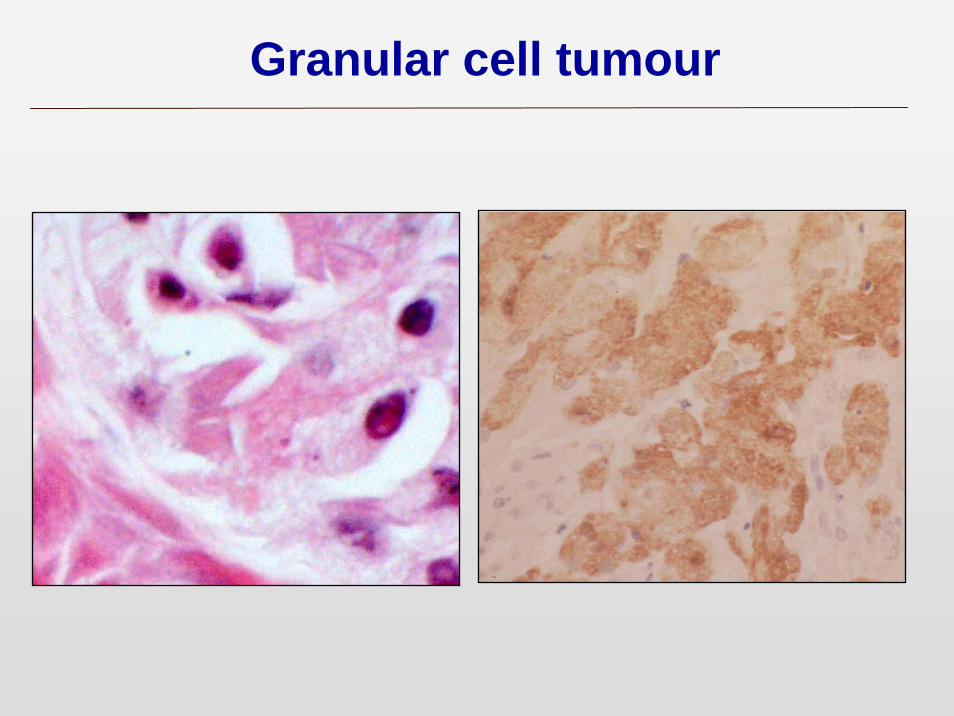
Granular cell tumour

• Benign and rarely recurs• May be multifocal • Of neural origin• S-100 positive granular cells
• Often in tongue• May be multiple lesions• Associated with pseudoepitheliomatous hyperplasia
Granular cell tumour
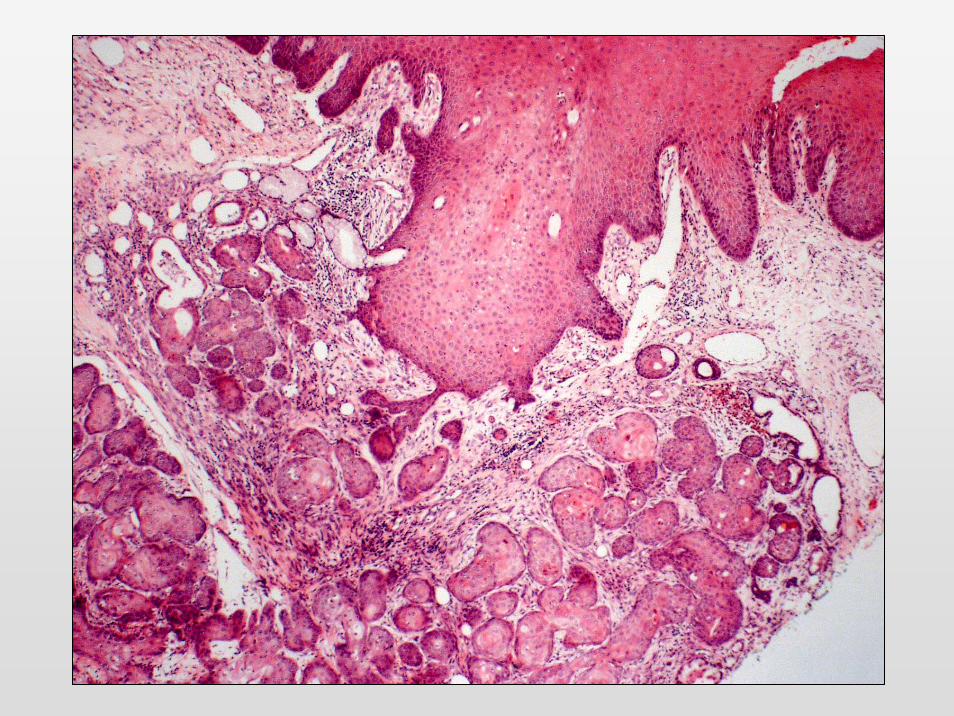

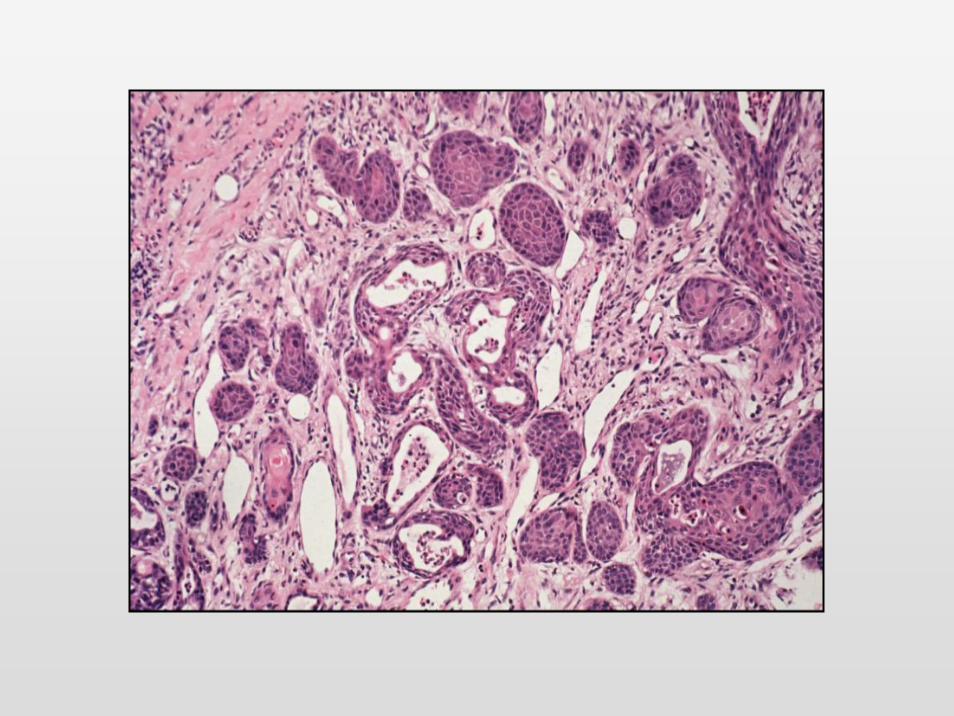
Necrotising sialometaplasia
• Benign inflammatory disease of glands of the palate and less commonly lips or other intraoral sites
• Clinically and microscopically resembles malignancy
Necrotising sialometaplasia
• Usually arises on the palate• Mean age 50 years• M:F 3:1• Appears as a ‘malignant’ ulcer• Aetiology unclear – traumatic?• Completely benign• Heals spontaneously 4 -10 weeks• Presents at a site which is rare for
malignancy
Necrotising sialometaplasia

Pictures courtesy of Prof John Eveson

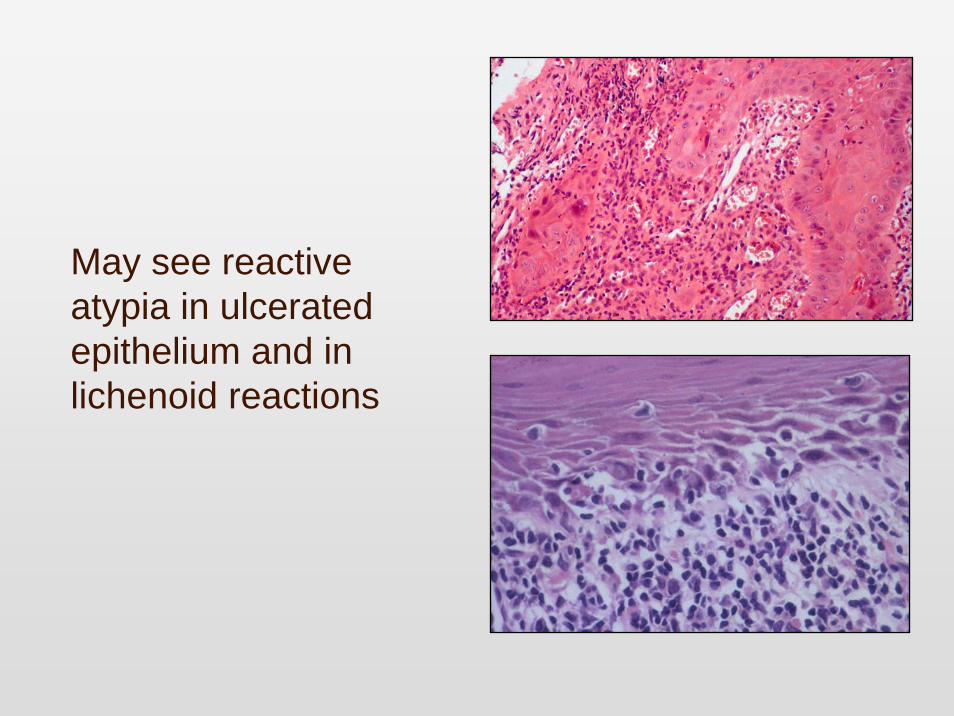
May see reactive atypia in ulcerated epithelium and in lichenoid reactions

Reactive atypia in infammatory lesionsReactive atypia in infammatory lesions

Summary
• Epithelial dysplasia is the best guide to potential progression of precursor lesions
• Grading is subjective• No molecular markers currently available• Overall only 5% of lesions progress• Care is needed in the interpretation of
atypia