Diagnostic and prognostic value of nucleolar organizer regions in normal epithelium, dysplasia, and...
9
2200 Diagnostic and Prognostic Value of Nucleolar Organizer Regions in Normal Epithelium, Dysplasia, and Squamous Cell Carcinoma of the Oral Cavity BACKGROUND. Nucleolar organizer regions (AgNORs) are associated with prolifera- Xin Xie, M.D. 1 tive activity and represent a diagnostic aid and prognostic marker in several neo- Ole Petter Fraas Clausen, M.D. 2 plastic entities. Jon Sudbo ¨, M.D. 3 METHODS. Sections from 51 T1-2 squamous cell carcinomas (SCC), 20 cases of Morten Boysen, M.D. 1 dysplasia, and 8 specimens with normal epithelium were evaluated by 2 AgNOR counting methods: 1) the mean number of AgNORs per nucleus (mAgNOR) and 1 Department of Otolaryngology, National Hos- pital, Oslo, Norway. 2) the percentages of nuclei with ú 1, ú 2, ú 3, and ú 4 AgNORs (pAgNOR ú 1, pAgNOR ú 2, pAgNOR ú 3, and pAgNOR ú 4, respectively). 2 Department of Pathology, National Hospital, RESULTS. Both mAgNOR and pAgNOR counts enabled significant discrimination Oslo, Norway. between normal epithelium and dysplasia (P õ 0.0003) and between dysplasia and 3 Department of Pathology, The Norwegian Ra- SCC (P õ 0.0001). For SCC, no correlation was found between AgNOR counts and diumhospital, University of Oslo, Oslo, Norway. clinical classification. Univariate analysis using the log rank test showed that the overall means for mAgNOR and pAgNORs correlated with the disease free period and survival time (P õ 0.0040). Patient age, gender, type of treatment, and T and N classification failed to predict the outcome. Multivariate analysis showed that pAgNOR ú 1 (cutoff level of 88%) was the best discriminator regarding the disease free period and survival time (P Å 0.0001 and P Å 0.0076, respectively). CONCLUSIONS. AgNOR enumeration, in particular pAgNOR ú 1, appears to be a useful tool in distinguishing between normal epithelium, dysplasia, and SCC of the oral cavity. In this study, AgNOR counts were strong prognostic markers for patients with SCC. Cancer 1997; 79:2200 – 8. q 1997 American Cancer Society. KEYWORDS: oral carcinoma, histopathology, squamous cell carcinoma, prognosis, nucleolar organizer regions. N Published in part in: Xie X, Boysen M. Prognos- ucleolar organizer regions (NORs) are loops of DNA on the short arms of acrocentric chromosomes that presumably are associ- tic value of two AgNOR quantification methods ated with ribosomal RNA activity, protein synthesis, and cell prolif- in glottic and oral carcinomas. In: Werner JA, eration. 1,2 By means of a one-step silver staining technique, the Lippert BM, Rudert HH. Head and neck cancer. Advances in basic research. Amsterdam: Else- NORs appear as black dots (AgNORs) that can be enumerated. 3 vier, 1996:453 – 8. Several investigations suggest that quantification of AgNORs is a valuable parameter in tumor pathology. Almost without exception Supported by the Norwegian Cancer Society and these studies showed that an increased number of AgNORs was the Anders Jahre Foundation. The authors wish associated with increased tumor aggressiveness, i.e., the mean num- to thank Anne Cromarty and Ruth Puntervold ber of AgNORs per nucleus was higher in malignant than in benign for excellent technical assistance. tissues, 4–6 higher in high grade than in low grade malignancies, 7–9 Address for reprints: M. Boysen, M.D., Depart- and higher in tumors with a poor prognosis compared with those ment of Otolaryngology, National Hospital, 0027 with a good prognosis. 10–18 These findings also pertain to squamous Oslo, Norway. cell carcinomas (SCC) of the oral cavity. 18,19 Recently, the authors introduced a new method for evaluation of Received September 30, 1996; revision received January 14, 1997; accepted January 14, 1997. AgNORs, the pAgNOR counting method, by which the percentages of q 1997 American Cancer Society / 7b57$$1094 05-05-97 13:41:08 cana W: Cancer
Transcript of Diagnostic and prognostic value of nucleolar organizer regions in normal epithelium, dysplasia, and...

2200
Diagnostic and Prognostic Value of NucleolarOrganizer Regions in Normal Epithelium, Dysplasia,and Squamous Cell Carcinoma of the Oral Cavity
BACKGROUND. Nucleolar organizer regions (AgNORs) are associated with prolifera-Xin Xie, M.D.1
tive activity and represent a diagnostic aid and prognostic marker in several neo-Ole Petter Fraas Clausen, M.D.2
plastic entities.Jon Sudbo, M.D.3
METHODS. Sections from 51 T1-2 squamous cell carcinomas (SCC), 20 cases ofMorten Boysen, M.D.1
dysplasia, and 8 specimens with normal epithelium were evaluated by 2 AgNOR
counting methods: 1) the mean number of AgNORs per nucleus (mAgNOR) and1 Department of Otolaryngology, National Hos-pital, Oslo, Norway. 2) the percentages of nuclei with ú 1, ú 2, ú 3, and ú 4 AgNORs (pAgNOR ú 1,
pAgNOR ú 2, pAgNOR ú 3, and pAgNOR ú 4, respectively).2 Department of Pathology, National Hospital,RESULTS. Both mAgNOR and pAgNOR counts enabled significant discriminationOslo, Norway.between normal epithelium and dysplasia (P õ 0.0003) and between dysplasia and
3 Department of Pathology, The Norwegian Ra-SCC (P õ 0.0001). For SCC, no correlation was found between AgNOR counts anddiumhospital, University of Oslo, Oslo, Norway.clinical classification. Univariate analysis using the log rank test showed that the
overall means for mAgNOR and pAgNORs correlated with the disease free period
and survival time (P õ 0.0040). Patient age, gender, type of treatment, and T and
N classification failed to predict the outcome. Multivariate analysis showed that
pAgNOR ú 1 (cutoff level of 88%) was the best discriminator regarding the disease
free period and survival time (P Å 0.0001 and P Å 0.0076, respectively).
CONCLUSIONS. AgNOR enumeration, in particular pAgNOR ú 1, appears to be a
useful tool in distinguishing between normal epithelium, dysplasia, and SCC of
the oral cavity. In this study, AgNOR counts were strong prognostic markers for
patients with SCC. Cancer 1997;79:2200–8. q 1997 American Cancer Society.
KEYWORDS: oral carcinoma, histopathology, squamous cell carcinoma, prognosis,nucleolar organizer regions.
NPublished in part in: Xie X, Boysen M. Prognos-ucleolar organizer regions (NORs) are loops of DNA on the shortarms of acrocentric chromosomes that presumably are associ-
tic value of two AgNOR quantification methodsated with ribosomal RNA activity, protein synthesis, and cell prolif-in glottic and oral carcinomas. In: Werner JA,eration.1,2 By means of a one-step silver staining technique, theLippert BM, Rudert HH. Head and neck cancer.
Advances in basic research. Amsterdam: Else- NORs appear as black dots (AgNORs) that can be enumerated.3
vier, 1996:453–8. Several investigations suggest that quantification of AgNORs is avaluable parameter in tumor pathology. Almost without exception
Supported by the Norwegian Cancer Society andthese studies showed that an increased number of AgNORs wasthe Anders Jahre Foundation. The authors wishassociated with increased tumor aggressiveness, i.e., the mean num-to thank Anne Cromarty and Ruth Puntervoldber of AgNORs per nucleus was higher in malignant than in benignfor excellent technical assistance.tissues,4 – 6 higher in high grade than in low grade malignancies,7 – 9
Address for reprints: M. Boysen, M.D., Depart- and higher in tumors with a poor prognosis compared with thosement of Otolaryngology, National Hospital, 0027 with a good prognosis.10 – 18 These findings also pertain to squamousOslo, Norway.
cell carcinomas (SCC) of the oral cavity.18,19
Recently, the authors introduced a new method for evaluation ofReceived September 30, 1996; revision receivedJanuary 14, 1997; accepted January 14, 1997. AgNORs, the pAgNOR counting method, by which the percentages of
q 1997 American Cancer Society
/ 7b57$$1094 05-05-97 13:41:08 cana W: Cancer

AgNOR in Oral Carcinoma/Xie et al. 2201
TABLE 1Treatment of 51 T1-2 Oral Squamous Cell Carcinomas According to the Site of the Primary Tumor
Radiotherapy Surgery andSite Surgery and surgery radiotherapy Radiotherapy Total
Tongue 2 14 5 3 24Gingiva 1 0 1 1 3Floor of mouth 0 2 11 1 14Buccal mucosa 3 6 1 0 10
Total 6 22 18 5 51
nuclei with more than one, more than two, more than patients with moderate dysplasias developed carcinomas2 to 4 years after the diagnosis of dysplasia.three, and more than four AgNORs were obtained.14
For glottic SCC this counting method appeared con-siderably better than mean AgNOR counts (mAgNOR) AgNOR Stainingin the discrimination of tumors with good and poor Two 4-mm sections were cut from the pretreatmentprognosis. This new counting method was also easier formalin fixed, paraffin embedded blocks. One sectionand quicker to perform than the conventional mAg- was stained with hematoxylin and eosin to verify theNOR counting. histopathologic diagnosis; the other was stained ac-
In this study, the authors tested both the mAgNOR cording to the method of Ploton et al.3 In brief, theand pAgNOR counting methods for their ability to dis- sections were dewaxed in xylene, and rehydratedcriminate between normal epithelium, dysplasia, and through graded ethanol to distilled, deionized water.oral SCC. For the clinical parameters of the carcino- The silver reaction was performed with a freshly pre-mas, mAgNOR and pAgNOR parameters were tested pared solution of 2 parts of 50% silver nitrate in dis-for their prognostic significance. tilled, deionized water and 1 part of 2% gelatin in 1%
formic acid for 45 minutes at room temperature (23C). After thorough washing, the sections were placedMATERIALS AND METHODSin 5% sodium thiosulfate, rinsed, and dehydratedThe material was comprised of formalin fixed, paraffinthrough graded alcohol to xylene and mounted. Theembedded pretreatment specimens from 51 retro-sections were stored in a dark cool place.spectively and randomly selected patients with T1 and
T2 oral SCC treated between 1983 and 1989. Therewere 17 females and 34 males ranging in age from 26 AgNOR Counting
In each section five fields were evaluated using a X100to 87 years (mean, 61 years). Fourteen patients had T1tumors and 37 patients had T2 tumors, and 44 were N0 oil immersion lens and an ocular grid with nine equi-
lateral squares. For carcinomas, the first field (upperand 7 were N1 (using the International Union AgainstCancer classification system of 1987). Clinical findings, left part of the section) was subjectively selected. The
subsequent fields were systematically chosen by mov-treatment, and follow-up were prospectively recorded.The mean follow-up time was 6 years (range, 3.5–9 ing the mechanical stage, with the coaxial controls, a
predetermined distance roughly proportional to theyears); no patient was lost to follow-up.Table 1 presents the treatment according to the overall size of the tumor area. Areas with necrosis,
pronounced inflammation, artificial damage, andsite of the tumors. Patients treated with surgery fol-lowed by radiotherapy received 50 grays (Gy) toward marked keratinization were avoided. For normal epi-
thelia and dysplasias, five fields covering the basal andthe primary site and the neck. For patients treatedwith radiotherapy alone or radiotherapy followed by adjacent parabasal layers were evaluated. By careful
focusing, all clearly distinguishable black dots withinsurgery the radiation dose was 66–70 Gy for the pri-mary tumor and 50–60 Gy for the neck. Sixteen pa- the nuclei were identified and counted. Black dots
within nucleoli or aggregated clusters were treated astients developed recurrences, 12 locally and 4 region-ally. Eleven patients died of their tumors. one AgNOR.
Two AgNOR counting methods were used: 1) theThe authors also included in this analysis 8 speci-mens with normal oral epithelium obtained from patients overall mAgNORs per nucleus was obtained by count-
ing the AgNOR dots in 20 nuclei within each of the 5treated for benign lesions and 20 specimens from patientswith dysplasia (10 mild and 10 moderate). Three of the fields; the counting started in the upper left square,
/ 7b57$$1094 05-05-97 13:41:08 cana W: Cancer

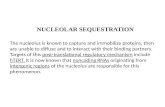
FIGURE 1. Silver-stained nucleolar organizer region (AgNOR)-stainedsections of paraffin embedded specimens from (A) normal oral mucosa,(B) epithelial dysplasia, and (C) squamous cell carcinoma (SCC). In normalepithelium, most of the nuclei had one to three AgNORs, whereas themajority of nuclei in SCCs exhibited more than four AgNORs. Dysplasiaspecimens show AgNOR counts between those of normal epithelium andSCCs. It should be stressed that careful focusing is necessary to discloseall AgNORs (original magnification, 1500).
/ 7b57$$1094 05-05-97 13:41:08 cana W: Cancer

AgNOR in Oral Carcinoma/Xie et al. 2203
StatisticsThe data were stored and analyzed by means of SAS6.10 software (SAS Institute, Cary, NC). The two-tailedStudent’s t test was used for comparison of groupmeans. The Kaplan-Meier method and log rank testwere used to screen the prognostic value of clinicaland AgNOR parameters in relation to the disease freeperiod and survival time. A case was censored if deathresulted from unrelated disease or, in analysis of thedisease free period, if death occurred in the absenceof disease recurrence. Parameters found to be prog-nostically significant by the univariate analysis werefurther analyzed by means of the Cox proportionalhazards regression model using the backward elimina-tion procedure. P valuesõ 0.05 were considered statis-tically significant. Log(-log) plots were used to checkthe assumption of proportional hazard rates in theCox model. Least square regression analysis was usedto test the reproducibility of both AgNOR countingmethods.
RESULTSFigure 1 presents the AgNOR staining of normal epi-thelium, dysplasia, and SCC and Figures 2 and 3 showthe distribution of mAgNOR and pAgNORs for all threetypes of tissue. The mean values for mAgNOR andpAgNOR parameters showed significant differencesbetween normal epithelium and dysplasias, and be-tween dysplasias and SCCs of the oral cavity (Table2).The three cases of dysplasia that progressed to SCCall had mAgNOR values above the mean for dysplasias.FIGURE 2. Mean silver-stained nucleolar organizer region counts (mAg-By chance, one of the cases with dysplasia that devel-NOR) distribution according to type of tissue. The bars indicate the meanoped into SCC was included in the series of SCC. Thisvalues. N: normal epithelium; D: dysplasia; CNF: squamous cell carcinomacase had the highest mAgNOR and pAgNOR ú 1 scorewithout failure; CF: squamous cell carcinoma with failure.of the dysplasias included in the analysis. Figure 4shows the frequency distribution of the number of
moving downward and then sideways; and 2) theAgNORs according to types of tissue. In normal epithe-
numbers of nuclei with 1, 2, 3, 4, and ú 4 AgNORslium, 70% of nuclei showed only 1 or 2 AgNORs. Con-
within all 9 squares in the 5 fields were counted. Fromversely, in SCCs,ú 60% of the nuclei hadú 4 AgNORs.
these figures, the percentages of nuclei with more thanDysplastic tissue showed a frequency distribution of
one, more than two, more than three, and more thanAgNORs ranging between that of normal epithelium
four AgNORs (pAgNOR ú 1, pAgNOR ú 2, pAgNOR úand SCCs.
3, and pAgNORú 4) were calculated. The time neededThe overall mAgNOR count for carcinomas was
for mAgNOR evaluation was approximately 45 minutes6.2 (range 4.7 – 11.3). Patients with counts below the
for each specimen. pAgNOR counts were less time-overall mean had a significantly longer disease free
consuming (approximately 20 minutes for each case).period and longer survival time compared with
The evaluation of nuclei with only 1 AgNOR took õ 2those with higher mAgNOR counts (Table 3). The
minutes per case. All the AgNOR counts were per-mean percentages for pAgNORs also correlated
formed by one of the authors (X.X.), who had nowith the disease free period and survival time. Table
knowledge of the clinical outcome.3 shows that 13 (pAgNOR ú 1 and pAgNOR ú 2) or14 (pAgNOR ú 3 and pAgNOR ú 4) of the 16 recur-Reproducibility
Two months after the completion of the evaluation, 8 rent cases and 10 of the 11 cases dead of diseasehad mean values above the overall mean for eachsections were randomly selected and recounted to test
the reproducibility of both AgNOR counting methods. of the pAgNOR parameters. Neither age, gender,
/ 7b57$$1094 05-05-97 13:41:08 cana W: Cancer

2204 CANCER June 1, 1997 / Volume 79 / Number 11
FIGURE 3. Percentage of nuclei with silver-stained nucleolar organizer regions (pAgNOR) frequency distribution according to type of epithelium.The bars indicate the mean values. N: normal oral epithelium; D: dysplasia; CNF: squamous cell carcinoma without failure; CF: squamous cellcarcinoma with failure; pAgNOR ú 1: percentage of nuclei with more than one AgNOR; pAgNOR ú 2: percentage of nuclei with more than twoAgNORs; pAgNOR ú 3: percentage of nuclei with more than three AgNORs; pAgNOR ú 4: percentage of nuclei with more than four AgNORs.
TABLE 2Overall Mean and Standard Deviation for Mean AgNOR Counts and Percentages of Nuclei with More than One, More than Two, More thanThree, and More than Four AgNORs in Normal Epithelium, Dysplasia, and Squamous Cell Carcinoma of the Oral Cavity
Type of tissue
Normal Dysplasia SCC
Parameters (n Å 8) P value (n Å 20) P value (n Å 51)
mAgNOR 2.3 { 0.4 õ 0.0001 3.8 { 0.8 0.0001 6.2 { 1.5pAgNOR ú 1 61 { 7 0.0003 77 { 3 0.0001 88 { 5pAgNOR ú 2 28 { 9 0.0001 58 { 7 õ 0.0001 78 { 9pAgNOR ú 3 12 { 5 õ 0.0001 42 { 11 õ 0.0001 69 { 11pAgNOR ú 4 5 { 3 0.0001 28 { 12 õ 0.0001 61 { 14
AgNOR: silver-stained nucleolar organizer regions; mAgNOR: mean silver-stained nucleolar organizer regions counts; pAgNOR ú 1: percentages of nuclei with more than one silver-stained nucleolar organizer
regions; pAgNOR ú 2: percentages of nuclei with more than two silver-stained nucleolar organizer regions; pAgNOR ú 3: more than three silver-stained nucleolar organizer regions; pAgNOR ú 4: percentages of
nuclei with more than four silver-stained nucleolar organizer regions.
type of treatment, nor T or N classification corre- Meier plots for the disease free period and survivaltime for pAgNOR ú1 with the mean cutoff level oflated with the clinical outcome. Multivariate analy-
sis revealed that pAgNOR ú 1 was the most notice- 88%. Improved discriminant function may be ob-tained by a posteriori selection of cut off levels, butable parameter in predicting the disease free period
and survival time (P Å 0.0001 and P Å 0.0076, re- this has not been tested further.Least square regression analysis regarding thespectively). Figures 5 and 6 present the Kaplan-
/ 7b57$$1094 05-05-97 13:41:08 cana W: Cancer

AgNOR in Oral Carcinoma/Xie et al. 2205
studies on head and neck SCC.15–18 Two studies onhead and neck SCC utilizing multivariate analysis inthe evaluation of the results showed that mean AgNORcounts were superior to clinical parameters in discrim-inating between prognostically poor and favorablecases.16,17
Two previous studies on oral SCC18,22 showedhigher overall mAgNOR counts (6.7 and 8.4, respec-tively) than in the current study. The study by Sano etal.18 included all T classifications. Both the observationthat laryngeal T3–4 tumors appear to have highermAgNOR counts than T1–2 tumors14 and methodo-logic problems such as the staining technique, varia-tion in section thickness, and the unambiguous identi-fication of all AgNOR dots may explain the diversityin mAgNOR counts. Therefore, mAgNOR counts ap-pear to be unsuitable for interstudy comparison untila standardized staining technique and counting pro-cedure has been established.
Mourad et al.23 introduced the pAgNOR methodin a study regarding DNA index and S-phase fraction.The authors modified this method by focusing on nu-clei with only a few AgNORs and used these parame-ters in the prognostication. This method has the ad-vantage that the time-consuming and tedious identi-fication of all AgNORs are avoided. When only a fewAgNORs are present in a nucleus, they are, as a rule,large and easily identifiable. The evaluation therebybecome easier and quicker to perform and there isFIGURE 4. Frequency distribution of nuclei with one, two, three, or fourno need for sophisticated equipment. Furthermore,
and more silver-stained nucleolar organizer regions (AgNORs) accordingpAgNOR counts are most likely less sensitive to varia-
to type of tissue. N: normal epithelium; D: dysplastic epithelium; C: squa-tions in section thickness and staining technique than
mous cell carcinoma.mean counts. With only one exception,14 previousstudies failed to present the reproducibility of the dataobtained. The current study showed a high degree of
reproducibility showed a coefficient of determina- intraobserver reproducibility for pAgNOR ú1. The re-tion (R2) Å 0.74, R2Å 0.88, R2Å 0.74, R2Å 0.66, and producibility for the remaining AgNOR parametersR2Å 0.58 for mAgNOR, pAgNOR ú 1, pAgNOR ú 2, might be improved by including more specimens, butpAgNOR ú 3, and pAgNOR ú 4, respectively. it is unlikely that the R2 level obtained for pAgNOR ú
1 could be reached.The findings of the current study show that pAg-DISCUSSION
The results of this study are in accordance with previ- NOR counts are more reliable in predicting the diseasefree period and survival than mAgNOR counts. Of theous studies and show that mAgNOR counts allow for
discrimination between normal epithelium and dys- pAgNORs, pAgNOR ú 1 emerged as the parameterwith the highest predictive power. The mean for pAg-plasias, and between dysplasias and SCC of the oral
cavity.20,21 It was an intriguing observation that the NOR ú 1 selected 13 of the 16 recurrences and 10 ofthe 11 deaths due to disease. No correlation was founddysplasia case that progressed to SCC had mAgNOR
counts exceeding the mean for dysplasia. This finding between T classification and prognosis in the currentstudy. Lymph node involvement is usually a significantindicates that mAgNOR counts may aid in establishing
the prognosis of a dysplastic lesion. Furthermore, it prognostic parameter in T1 and T2 oral SCC.24 Thisparameter did not predict the outcome in this serieswas found that mAgNOR counts allowed for discrimi-
nation between SCCs with favorable and unfavorable of patients, probably due to the fact that all those withregional metastases were N1.clinical courses. This observation is in agreement with
the authors’ previous study on glottic SCC14 and other Although the biologic significance of AgNOR re-
/ 7b57$$1094 05-05-97 13:41:08 cana W: Cancer

2206 CANCER June 1, 1997 / Volume 79 / Number 11
TABLE 3Univariate (Log Rank Test) Analysis for Clinical Parameters and Mean mAgNOR and pAgNORs with Regard to Disease Free Period (n Å 16) andSurvival Time for 51 Patients with T1-2 Squamous Cell Carcinoma of the Oral Cavity
Disease free period Survival time
No. of cases No. of Log rank No. of Log rankParameters Groups/cutoff level each group recurrences P value deaths P value
Age (yrs) ° 61 vs. ú 61 24/27 6/10 0.2812 5/6 0.7270Gender Females vs. males 17/34 5/11 0.6924 3/8 0.5559T class. T1 vs. T2 14/37 2/14 0.0982 2/9 0.3406N class. N0 vs. N/ 44/7 15/1 0.4278 10/1 0.7125Treatment Surgery or radiotherapy 11/40 3/13 0.7923 2/9 0.7752
vs. combinedmAgNOR ° 6.2 vs. ú 6.2 34/17 6/10 0.0037 3/8 0.0021pAgNOR ú 1 ° 88% vs. ú 88% 30/21 3/13 0.0001 1/10 0.0002pAgNOR ú 2 ° 78% vs. ú 78% 27/24 3/13 0.0002 1/10 0.0017pAgNOR ú 3 ° 69% vs. ú 69% 26/25 2/14 0.0005 1/10 0.0026pAgNOR ú 4 ° 61% vs. ú 61% 24/27 2/14 0.0023 1/10 0.0072
mAgNOR: mean silver-stained nucleolar organizer regions counts; pAgNOR: percentages of nuclei per silver-stained nucleolar organizer regions; class.: classification according to International Union Against
Cancer staging system; pAgNOR ú 1: percentage of nuclei with more than one silver-stained nucleolar organizer regions; pAgNOR ú 2: percentages of nuclei with more than two silver-stained nucleolar organizer
regions; pAgNOR ú 3: percentages of nuclei with more than three silver-stained nucleolar organizer regions; pAgNOR ú 4: percentages of nuclei with more than four silver-stained nucleolar organizer regions.
FIGURE 6. Survival time in relation to mean percentage of nuclei withFIGURE 5. Disease free period in relation to mean percentage of nucleisilver-stained nucleolar organizer regions (pAgNOR) ú 1 in 51 patientswith silver-stained nucleolar organizer regions (pAgNOR) ú 1 in 51 pa-with T1–2 oral squamous cell carcinomas (P Å 0.0002).tients with T1-2 oral squamous cell carcinomas (P õ 0.0001).
mains uncertain, the relationship between AgNOR over, studies on breast carcinomas and tumors of thebrain show that the percentage of nuclei with five orquantity and cell kinetics has been demonstrated in a
series of studies. Resting cells usually only have one more AgNORs correlated with the S-phase fraction andthe bromodeoxyuridine labeling index.23,31 TheseAgNOR dot.7,25–27 The number of AgNORs increases
from the early G1 phase to late S-/G2 phases.26,28 The findings indicate that the parameters pAgNOR ú 1 orpAgNOR ú 2 reflect the size of the growth fraction asnumber of AgNORs at any given stage in the cell cycle
appear to be inversely proportional to the cell cycle well as its proliferative activity. This is consistent withthe observation that high proliferative activity coin-time, i.e., the higher the amount of AgNOR, the shorter
the cell cycle time.29 In a study using double staining cides with poor prognosis.32
Several studies have tested the prognostic signifi-with AgNOR and Ki 67 (the latter being a marker forthe number of cells in the cycle) demonstrated that cance of other proliferative markers in head and neck
SCCs. The DNA content is the feature most extensivelythe number of AgNORs ranged from 2–12 in the Ki 67positive cells and 1–3 in Ki 67 negative cells.30 More- studied. Some of these studies show that aneuploidy
/ 7b57$$1094 05-05-97 13:41:08 cana W: Cancer

AgNOR in Oral Carcinoma/Xie et al. 2207
8. Malusardi G, Oldini C, Leopardi O. The quantitative study ofindicates an unfavorable prognosis,33–35 whereas oth-nucleolar organizers (AgNOR) in the diagnosis of laryngealers24,36 failed to demonstrate any correlation betweendysplasias and in the assessment of the prognosis in invasive
the ploidy pattern and prognosis. The reason for these carcinoma. Acta Otorhinolaryngol Ital 1992;12:3–12.conflicting results may be explained by the different 9. Egan M, Raafat F, Crocker J, Williams D. Comparative studymethods used in preparing the material and for evalu- of the degree of differentiation of neuroblastoma and mean
numbers of nucleolar organizer regions. J Clin Patholation (either flow or image cytometry) as well as a lack1988;41:527–31.of agreement as to the definitions regarding ploidy.
10. Kuratsu S, Aozasa K, Myoui A, Tsujimoto M, Ueda T, UchidaHowever, Munch-Wickland et al.37 demonstrated anA, et al. Prognostic significance of argyrophilic nucleolar or-
excellent discrimination between recurrent and non- ganizer staining in soft-tissue sarcomas. Int J Cancerrecurrent early glottic carcinomas, treated by irradia- 1991;48:211–4.tion, by combining hypertetraploidy and proliferating 11. Ofner D, Totsch M, Sandbichler P, Hallbrucker C, Margreiter
R, Mikuz G, et al.. Silver stained nucleolar organizer regioncell nuclear antigen. In addition, Ki 67 has been testedproteins (AgNORs) as a predictor of prognosis in colonicfor its possible prognostic significance, but no correla-cancer. J Pathol 1990;162:43–9.tion was demonstrated with regard to prognosis.38 His-
12. Kolar Z, Zabransky T, Mattler K, Zabransky E. Argyrophilictopathologic features, especially the grading of the nucleolar organizer regions in breast cancer: prognostic sig-deep invasive part of tumors, appear to be a promising nificance. Cesk Patol 1992;28:193–200.prognostic parameter.39,40 Although this method is 13. Delahunt B, Ribas JL, Nacey JN, Bethwaite PB. Nucleolar
organizer regions and prognosis in renal cell carcinoma. Jbased on the subjective evaluation of several histo-Pathol 1991;163:31–7.pathologic features, a reasonable intra- and interob-
14. Xie X, Stenersen TC, Clausen OPF, Boysen M. Nucleolar or-server reproducibility was achieved.ganizer regions and prognosis in glottic squamous cell carci-
The current study strongly suggests that both noma. Head Neck 1997;19:20–6.mAgNOR and pAgNOR counts allow discrimination 15. Morita M, Kuwano H, Matsuda H, Moriguchi S, Sugimachi K.between normal epithelium, dysplasia, and SCC of the Prognostic significance of argyrophilic nucleolar organizer
regions in esophageal carcinoma. Cancer Res 1991;51:5339–oral cavity. Furthermore, it appears that AgNOR41.counts may predict the progression of a dysplastic le-
16. Pich A, Pisani P, Kzengli M, Cappello N, Navone R. Argyro-sion to SCC. However, the most significant observationphilic nucleolar organizer region counts and prognosis in
was that AgNOR counts, in particular pAgNOR ú 1, pharyngeal carcinoma. Br J Cancer 1991;64:327–32.were strong indicators with regard to disease recur- 17. Bockmuhl U, Bockmuhl F, Dimmer V, Kunze KD. ‘‘Nucleolarrences and short survival in T1–2 SCC of the oral cav- organizer regions’’ as a factor for the prognosis of laryngeal
cancer? Laryngorhinootologie 1992;71:137–41.ity. Therefore, the authors believe that pAgNOR ú 118. Sano K, Takahashi H, Fujita S, Inokuchi T, Pe MB, Okabeshould be part of the routine histopathologic report
H, et al. Prognostic implication of silver-binding nucleolarof oral SCC.organizer regions (AgNORs) in oral squamous cell carci-noma. J Oral Pathol Med 1991;20:53–6.
REFERENCES 19. Schwint AE, Savino TM, Lanfranchi HE, Marschoff E, Cabrini1. Goodpasture C, Bloom SE. Visualization of nucleolar orga- RL, Itoiz ME. Nucleolar organizer regions in lining epithe-
nizer regions in mammalian chromosomes using silver lium adjacent to squamous cell carcinoma of human oralstaining. Chromosoma 1975;53:37–50. mucosa. Cancer 1994;73:2674–9.
2. Arden KC, Pathak S, Stettner S, Ritchie E. Differential silver- 20. Pillai KR, Sujathan K, Kannan S, Abraham EK, Mathew B,positive nucleolus organizer region activity in normal and Amma NS, et al. Argyrophilic nucleolar organizer regions inmalignant murine tissues. Cancer Genet Cytogenet 1989; the evaluation of tumour progression in the oral mucosa:37:55–60. correlation with tissue pathology. J Cancer Res Clin Oncol
3. Ploton D, Menager M, Jeannesson P, Himber G, Pigeon F, 1994;120:723–6.Adnet JJ. Improvement in the staining and in the visualiza-
21. Zoeller J, Flentje M, Sinn P, Born IA. Evaluation of AgNORtion of the argyrophilic proteins of the nucleolar organizerand Ki-67 antigen as cell kinetic parameters in oral dyspla-region at the optical level. Histochem J 1986;18:5–14.sias and carcinomas. Anal Cell Pathol 1994;7:77–88.4. Ayres JG, Crocker J, Skilbeck NQ. Differentiation of malig-
22. Warnakulasuriya KAAS, Johnson NW. Nucleolar organizernant from normal and reactive mesothelial cells by the arg-region (NOR) distribution as a diagnostic marker in oralyrophil technique for nucleolar organizer region associatedkeratosis, dysplasia and squamous cell carcinoma. J Oralproteins. Thorax 1988;43:366–70.Pathol Med 1993;22:77–81.5. Crocker J, Ayres JG, McGovern J. Nucleolar organizer regions
23. Mourad WA, Erkman-Balis B, Livingston S, Shoukri M, Coxin small cell carcinoma of the bronchus. Thorax 1987;CE, Nicosia SV, et al. Argyrophilic nucleolar organizer re-42:972–5.gions in breast carcinoma: correlation with DNA flow cytom-6. Hirsch SM, DuCanto J, Caldarelli DD, Hutchinson JC, Coonetry, histopathology, and lymph node status. Cancer 1992;JS. Nucleolar organizer regions in squamous cell carcinoma69:1739–44.of the head and neck. Laryngoscope 1992;102:39–44.
24. Tytor M, Franzen G, Olofsson J, Brunk U, Nordenskoøld B.7. Abe S, Ogura S, Kunikane H, Suko N, Watanabe N, NakajimaDNA content, malignancy grading and prognosis in T1 andI, et al. Nucleolar organizer regions in precancerous and
cancerous lesions of the bronchus. Cancer 1991;67:472–5. T2 oral cavity carcinomas. Br J Cancer 1987;56:647–52.
/ 7b57$$1094 05-05-97 13:41:08 cana W: Cancer

2208 CANCER June 1, 1997 / Volume 79 / Number 11
25. Mirre C, Knibiehler B. A re-evaluation of the relationships 33. Guo Y-C, DeSanto L, Osetinsky GV. Prognostic implicationsof nuclear DNA content in head and neck cancer. Otolaryn-between the fibrillar centres and the nucleolus-organizing
regions in reticulated nucleoli: ultrastructural organization, gol Head Neck Surg 1989;100:95–8.34. Truelson JM, Fisher SG, Beals TE, McClatchey KD, Wolf GT.number and distribution of the fibrillar centres in the nucle-
olus of the mouse Sertoli cell. J Cell Sci 1982;55:247–59. DNA content and histological growth pattern correlate withprognosis in patients with advanced squamous cell carci-26. Carbajo S, Orfao A, Vicente-Villardon JL, Carbajo-Perez E.
Expression of silver-stained nucleolar organizer regions is noma of the larynx. Cancer 1992;70:56–62.35. Walter MA, Peters GE, Peiper SC. Predicting radioresistancecoupled to cell cycle in rat thymic cells. Cytometry 1993;
14:46–52. in early glottic squamous cell carcinoma by DNA content.Ann Otol Rhinol Laryngol 1991;100:523–6.27. Jan-Mohamed RM, Armstrong SJ, Crocker J, Leyland MJ,
Hulten MA. The relationship between number of interphase 36. Bundgaard T, Sorensen FB, Gaihede M, Sogaard H, Over-gaard J. Stereologic, histopathologic, flow cytometric, andNORs and non-bearing chromosomes in non-Hodgkin’s
lymphoma. J Pathol 1989;158:3–7. clinical parameters in the prognostic evaluation of 74 pa-tients with intraoral squamous cell carcinomas. Cancer28. Ruschoff J, Fauser G, Knuchel R, Hofstadter F. AgNOR quan-
tification with special reference to staining patterns. Zen- 1992;70:1–13.37. Munch-Wikland E, Fernberg J-O, Kuylenstierna R, Lindholmtralbl Pathol 1994;140:23–30.
29. Brugal G. Interpretation of proliferation markers. In: J, Auer G. Proliferating cell nuclear antigen (PCNA) expres-sion and nuclear DNA content in predicting recurrence afterWied GL, Bartels PH, Rosenthal DL, Schenck U, editors.
Compendium on the computerized cytology and histol- radiotherapy of early glottic cancer. Eur J Cancer Oral Oncol1993;29B:75–9.ogy laboratory. Chicago: Chicago Tutorials of cytology,
1994:234 – 40. 38. Jones AS, Roland NJ, Caslin AW, Cooke TG, Cooke LD, For-ster G. A comparison of cellular proliferation markers in30. Mourad WA, Sneige N, Katz RL, Ordonez NG. Correlation of
two AgNOR counts with Ki-67 labelling index: a study in squamous cell carcinoma of the head and neck. J LaryngolOtol 1994;108:859–64.fine- needle aspirates of lymphoproliferative disorders and
breast carcinoma. Diagn Cytopathol 1994;10:113–9. 39. Bryne M, Koppang HS, Lilleng R, Kjaerheim A. Malignancygrading of the deep invasive margins of oral squamous cell31. Mourad WA, Connelly JH, Sembera DL, Atkinson EN, Bruner
JM. The correlation of two argyrophilic nucleolar organizer carcinomas has a high prognostic value. J Pathol 1992;166:375–81.region counting methods with bromodeoxyuridine-labeling
index: a study of metastatic tumors of the brain. Hum Pathol 40. Odell EW, Jani P, Sheriff M, Ahluwalia SM, Hibbert J, LevisonDA, et al. The prognostic value of individual histologic grad-1993;24:206–10.
32. Chauvel P, Courdi A, Gioanni J, Vallicioni J, Santini J, De- ing parameters in small lingual squamous cell carcinomas.The importance of the pattern of invasion. Cancer 1994;mard F. The labelling index: a prognostic factor in head and
neck carcinoma. Radiother Oncol 1989;14:231–7. 74:789–94.
/ 7b57$$1094 05-05-97 13:41:08 cana W: Cancer