
Diagnosis, Treatment, and Prevention of Hemodialysis ... · In-Depth Review Diagnosis, Treatment,...
13
In-Depth Review Diagnosis, Treatment, and Prevention of Hemodialysis Emergencies Manish Saha and Michael Allon Abstract Given the high comorbidity in patients on hemodialysis and the complexity of the dialysis treatment, it is re- markable how rarely a life-threatening complication occurs during dialysis. The low rate of dialysis emergencies can be attributed to numerous safety features in modern dialysis machines; meticulous treatment and testing of the dialysate solution to prevent exposure to trace elements, toxins, and pathogens; adherence to detailed treatment protocols; and extensive training of dialysis staff to handle medical emergencies. Most hemodialysis emergencies can be attributed to human error. A smaller number are due to rare idiosyncratic reactions. In this review, we highlight major emergencies that may occur during hemodialysis treatments, describe their pathogenesis, offer measures to minimize them, and provide specific interventions to prevent catastrophic consequences on the rare occasions when such emergencies arise. These emergencies include dialysis disequilibrium syndrome, venous air embolism, hemolysis, venous needle dislodgement, vascular access hemorrhage, major allergic reactions to the dialyzer or treatment medications, and disruption or contamination of the dialysis water system. Finally, we de- scribe root cause analysis after a dialysis emergency has occurred to prevent a future recurrence. Clin J Am Soc Nephrol ▪: ccc–ccc, 2016. doi: 10.2215/CJN.05260516 Introduction There are currently approximately 400,000 patients with ESRD on maintenance hemodialysis (HD) in the United States (1). Each one receives dialysis at least thrice weekly (156 times per year) for a total of over 62 million dialysis sessions annually. Given the high comorbidity in patients on HD and the complexity of the dialysis treatment, it is remarkable how rarely a life-threatening complication occurs during dialysis. For example, a cardiac arrest occurs only seven times per 100,000 HD sessions (2). The low rate of major complications can be attributed to numerous safety features in modern dialysis machines; meticulous treatment and testing of the dialysate solution to pre- vent exposure to trace elements, toxins, and patho- gens; adherence to detailed treatment protocols; and extensive training of dialysis staff to handle medical emergencies. Most HD emergencies can be attributed to human error. A smaller number are due to rare idiosyncratic reactions. Ongoing dialysis staff train- ing is essential to both prevent human error as well as ensure prompt and effective interventions when complications happen. This review highlights major emergencies that may occur during HD treatments (Table 1), measures to minimize them, and specific interventions to prevent catastrophic consequences on the rare occasions when such complications arise. We have provided case re- ports to illustrate these emergencies in Supplemental Appendix. Complications related to more frequent HD are not addressed in this review. Intradialytic hypotension, a relatively common complication dur- ing dialysis, is also beyond the scope of this review but has been the subject of some recent comprehen- sive papers (3–6). Dialysis Disequilibrium Syndrome Dialysis disequilibrium syndrome (DDS) is a rare syndrome occurring in patients with severe azotemia undergoing their initial HD session. It is characterized by nausea, vomiting, headache, encephalopathy, and seizures (7,8). DDS is attributed to the faster decline of urea concentration in the blood than in the brain during the dialysis session. This lag (reverse urea ef- fect) creates an osmotic gradient that promotes net water shift from the blood into the brain, leading to cerebral edema and its associated manifestations (9,10). Rosen et al. (11) studied 10 patients with AKI (baseline BUN concentrations of 210–460 mg/dl) un- dergoing their initial HD session. They obtained con- current plasma and cerebrospinal fluid (CSF) samples before dialysis, immediately after dialysis, and 24 hours after dialysis. The CSF-to-plasma BUN ratio was 0.91 predialysis, 1.99 immediately after dialysis, and back to baseline 24 hours later. In animal models of uremia, the alteration in brain urea and other electrolytes concentrations does not completely account for the increase in brain osmolal- ity during rapid HD (12). Arieff et al. (12) suggested that generation of new solutes (“idiogenic osmoles”) in brain tissue accounted for brain edema during rapid HD. In contrast, Silver et al. (13) reported that retained urea in brain was sufficient to cause a change in brain water content in rapidly dialyzing animals. Moreover, the content of brain organic osmolytes Division of Nephrology, University of Alabama at Birmingham, Birmingham, Alabama Correspondence: Dr. Michael Allon, Division of Nephrology, PB, Room 226, 1530 Third Avenue South, Birmingham, AL 35294. Email: [email protected] www.cjasn.org Vol ▪ ▪▪▪, 2016 Copyright © 2016 by the American Society of Nephrology 1 . Published on November 9, 2016 as doi: 10.2215/CJN.05260516 CJASN ePress
Transcript of Diagnosis, Treatment, and Prevention of Hemodialysis ... · In-Depth Review Diagnosis, Treatment,...
In-Depth Review
Diagnosis, Treatment, and Prevention of HemodialysisEmergencies
Manish Saha and Michael Allon
AbstractGiven the high comorbidity in patients on hemodialysis and the complexity of the dialysis treatment, it is re-markable how rarely a life-threatening complication occurs during dialysis. The low rate of dialysis emergenciescan be attributed to numerous safety features inmodern dialysismachines;meticulous treatment and testing of thedialysate solution to prevent exposure to trace elements, toxins, and pathogens; adherence to detailed treatmentprotocols; and extensive training of dialysis staff to handle medical emergencies. Most hemodialysis emergenciescan be attributed to human error. A smaller number are due to rare idiosyncratic reactions. In this review, wehighlight major emergencies that may occur during hemodialysis treatments, describe their pathogenesis, offermeasures to minimize them, and provide specific interventions to prevent catastrophic consequences on the rareoccasions when such emergencies arise. These emergencies include dialysis disequilibrium syndrome, venous airembolism, hemolysis, venous needle dislodgement, vascular access hemorrhage, major allergic reactions to thedialyzer or treatment medications, and disruption or contamination of the dialysis water system. Finally, we de-scribe root cause analysis after a dialysis emergency has occurred to prevent a future recurrence.
Clin J Am Soc Nephrol ▪: ccc–ccc, 2016. doi: 10.2215/CJN.05260516
IntroductionThere are currently approximately 400,000 patientswith ESRD on maintenance hemodialysis (HD) in theUnited States (1). Each one receives dialysis at leastthrice weekly (156 times per year) for a total of over62 million dialysis sessions annually. Given the highcomorbidity in patients on HD and the complexity ofthe dialysis treatment, it is remarkable how rarely alife-threatening complication occurs during dialysis.For example, a cardiac arrest occurs only seven timesper 100,000 HD sessions (2). The low rate of majorcomplications can be attributed to numerous safetyfeatures in modern dialysis machines; meticuloustreatment and testing of the dialysate solution to pre-vent exposure to trace elements, toxins, and patho-gens; adherence to detailed treatment protocols; andextensive training of dialysis staff to handle medicalemergencies. Most HD emergencies can be attributedto human error. A smaller number are due to rareidiosyncratic reactions. Ongoing dialysis staff train-ing is essential to both prevent human error as wellas ensure prompt and effective interventions whencomplications happen.
This review highlights major emergencies that mayoccur during HD treatments (Table 1), measures tominimize them, and specific interventions to preventcatastrophic consequences on the rare occasions whensuch complications arise. We have provided case re-ports to illustrate these emergencies in SupplementalAppendix. Complications related to more frequentHD are not addressed in this review. Intradialytichypotension, a relatively common complication dur-ing dialysis, is also beyond the scope of this review
but has been the subject of some recent comprehen-sive papers (3–6).
Dialysis Disequilibrium SyndromeDialysis disequilibrium syndrome (DDS) is a rare
syndrome occurring in patients with severe azotemiaundergoing their initial HD session. It is characterizedby nausea, vomiting, headache, encephalopathy, andseizures (7,8). DDS is attributed to the faster declineof urea concentration in the blood than in the brainduring the dialysis session. This lag (reverse urea ef-fect) creates an osmotic gradient that promotes netwater shift from the blood into the brain, leading tocerebral edema and its associated manifestations(9,10). Rosen et al. (11) studied 10 patients with AKI(baseline BUN concentrations of 210–460 mg/dl) un-dergoing their initial HD session. They obtained con-current plasma and cerebrospinal fluid (CSF) samplesbefore dialysis, immediately after dialysis, and 24hours after dialysis. The CSF-to-plasma BUN ratiowas 0.91 predialysis, 1.99 immediately after dialysis,and back to baseline 24 hours later.In animal models of uremia, the alteration in brain
urea and other electrolytes concentrations does notcompletely account for the increase in brain osmolal-ity during rapid HD (12). Arieff et al. (12) suggestedthat generation of new solutes (“idiogenic osmoles”)in brain tissue accounted for brain edema duringrapid HD. In contrast, Silver et al. (13) reported thatretained urea in brain was sufficient to cause a changein brain water content in rapidly dialyzing animals.Moreover, the content of brain organic osmolytes
Division ofNephrology,University of Alabamaat Birmingham,Birmingham, Alabama
Correspondence:Dr. Michael Allon,Division ofNephrology, PB,Room 226, 1530 ThirdAvenue South,Birmingham, AL35294. Email:[email protected]
www.cjasn.org Vol ▪ ▪▪▪, 2016 Copyright © 2016 by the American Society of Nephrology 1
. Published on November 9, 2016 as doi: 10.2215/CJN.05260516CJASN ePress
(myoinosotol, glutamine, and taurine, etc.) did not increasein rapidly dialyzing animals (9,13,14). Idiogenic osmolesmay be generated in brain during acute azotemia as anadaptive response to increased plasma BUN to preventbrain cell shrinkage (15) but are probably not generatedduring rapid HD (9). Finally, in a CKD animal model,there was a decrease in brain urea transporters and anincrease in aquaporins (AQPs; AQP4 and AQP9), provid-ing a potential molecular mechanism for the reverse ureaeffect (16).The spectrum of DDS ranges from headache and rest-
lessness in mild forms to nausea, vomiting, and hyperten-sion in patients with moderate cases to seizures and comain patients with severe cases (7,17,18). There is no set BUNvalue above which patients predictably develop DDS.Both a high BUN level (.175 mg/dl) and its rapid declineare risk factors for DDS (7,18,19). Additional risk factorsinclude preexisting neurologic conditions, the first sessionof HD, hyponatremia, and liver disease (7,18,20). It is un-known whether the risk of DDS is similar in patients withadvanced CKD and those with AKI. Computed tomogra-phy or magnetic resonance may show cerebral edema inpatients with DDS.Several strategies may prevent DDS in patients with very
high serum BUN undergoing their first HD session (Table 2)(7,12,17). The most important measure is to slow the urea
removal rate. In a dog model of uremia, Arieff et al. (12)compared rapid and slow HD that achieved a similar re-duction in BUN. Rapid HD (100 minutes with a blood flowof 12 ml/kg per minute and a dialysate flow rate of 500ml/min) produced an elevated CSF pressure and seizures.In contrast, slower HD (200 minutes at 5 ml/kg per minuteblood flow rate and a dialysate flow rate of 500 ml/min)elevated the CSF pressure without causing seizures (12).Thus, a short HD session (2 hours) with a low blood flow(200 ml/min) and a urea reduction ratio goal of 0.4 is rec-ommended as the initial prescription for patients at risk forDDS (7,17). Continuous RRT (CRRT) may be considered inpatients at high risk for DDS, including those with intra-cranial mass or brain injury (20). Kidney Disease Improv-ing Global Outcomes recommends CRRT over intermittentdialysis for AKI in patients with brain injury/edema orelevated intracranial pressure (21).Port et al. (22) reported that a higher dialysate sodium
concentration (144–154 mmol/L) prevented DDS symp-toms. Each 1-mmol/L increase in serum sodium offsetthe osmotic effect of 12 mg/dl BUN. Thus, sodium mod-eling may be useful in preventing DDS during the initialHD sessions in patients at risk (22). Adding glucose orglycerol to the dialysate may also prevent DDS (23).Rodrigo et al. (24) studied patients on HD at risk for DDSby adding glucose to the dialysate or administering intrave-nous mannitol. Increasing the dialysate glucose concen-tration to 450 mg/dl contributed 2–3 mosM/kg H2O,whereas intravenous mannitol (1 g/kg) added 8.5–10mosM/kg H2O (24).
Air EmbolismVenous air embolism (VAE) during HD is thought to be
rare, but because signs and symptoms of air embolism maymimic other more common complications, careful vigilanceand high suspicion are required for the diagnosis. Airbubbles trapped in the systemic (pulmonary or cerebral)microcirculation may cause local ischemia, circulatoryarrest, activation of complement and coagulation sys-tem, localized inflammation, and vascular endothelial celldamage (25–27).
Table 1. Major dialysis emergencies
Type of Emergency Estimated Frequency, perMillion HD Sessions Refs.
Dialysis disequilibriumAir embolism 8.5–33 Tennankore et al. (31), Wong et al. (32)HemolysisVascular access hemorrhageVenous needle dislodgement 14–91 Tennankore et al. (31), Wong et al. (32), VA study (65),
Pennsylvania patient safety study (64)Allergic reaction 21–170 Villarroel and Ciarkowski (71), Daugirdas et al. (72),
Simon et al. (129)Cardiac arrest 70 Karnik et al. (2)Errors in following the HDprescription
HD, hemodialysis.
Table 2. Potential strategies to prevent dialysis disequilibriumsyndrome in high-risk patients
(1) Limit the first HD session to 2–2.5 h(2) Limit the blood flow to 200–250 ml/min(3) Sodium modeling or a high-sodium dialysate(4) Consider intravenous mannitol (1 g/kg)(5) Consider CRRT in patients at high risk for DDS
(traumatic brain injury, intracerebral hemorrhage,intracranial mass)
HD, hemodialysis; CRRT, continuous RRT; DDS, dialysis dis-equilibrium syndrome.
2 Clinical Journal of the American Society of Nephrology
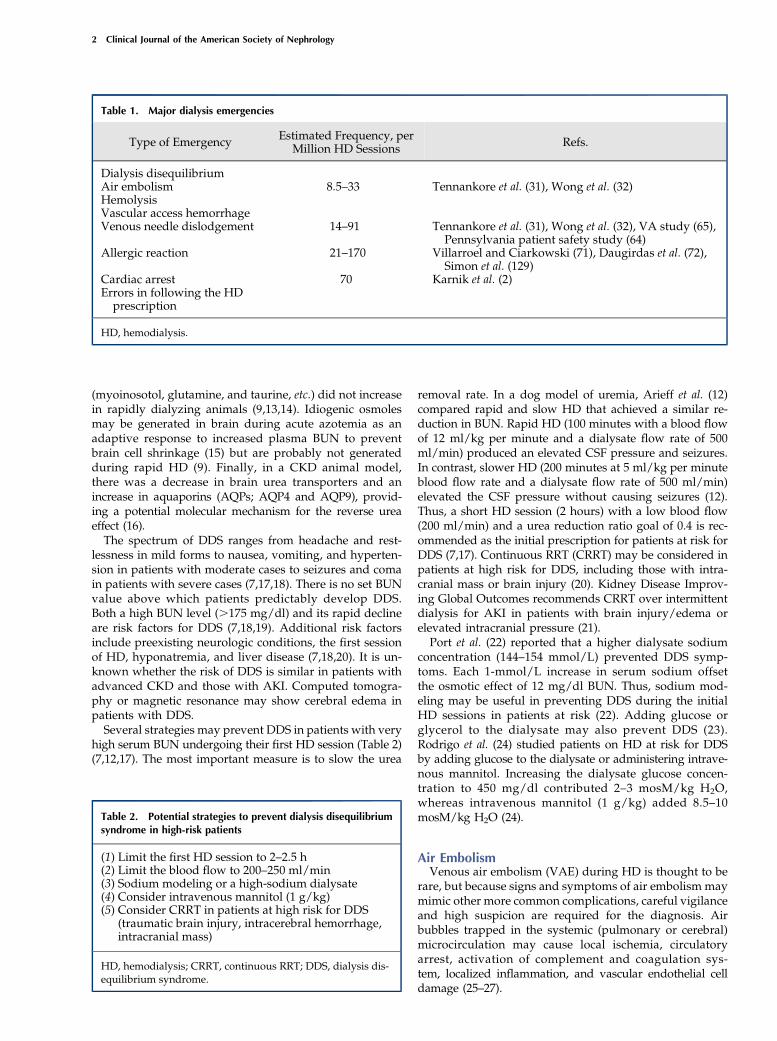
Owing to safeguards in the modern HD machine, symp-tomatic air embolism is exceedingly rare during HD. Airmay enter the extracorporeal HD circuit either as a re-sult of residual air trapped in the tubing or dialyzer dueto incomplete priming or because of a broken or loose luerconnection prepump (where the arterial pressure isnegative) (25,28–30) (Figure 1). Air entering the extracor-poreal circuit presents to the venous air trap placed distalto the dialyzer, immediately decreasing the blood level inthe chamber. The change in fluid level in this chamber isrecognized by a sensor that triggers an alarm and stops theblood pump. As a consequence of these technologic safe-guards, air embolism in the modern era results from hu-man error. In a retrospective cohort study of 202 patientson home HD, only six patients had suspected air embolismthat occurred during 183,603 dialysis sessions for an over-all incidence less than one episode per 30,000 dialysis ses-sions. These episodes were related to inadequate primingor lack of clamping of the catheter or tubing (31). Anotherstudy reported a single case of air embolism during
follow-up of 190 patients on home HD (approximately117,000 HD sessions) for an incidence of less than oneepisode per 100,000 HD sessions. This case resulted fromnot clamping the arterial line during disconnection, therebyallowing air to enter the tubing (32).Most microbubbles ,50 mm in diameter and many mi-
crobubbles between 50 and 200 mm pass through the ve-nous bubble catcher without triggering an alarm (33). Therate of microbubble formation is dependent on the bloodflow rate and negative arterial pressure. The total volumeof microbubbles during an HD session is a few milliliters, avolume insufficient to cause acute symptoms (34). The ve-nous air trap and air detector prevent infusion of largeramounts of air. If the air detector triggered an alarm forevery microbubble, HD would be regularly interrupted(28). Therefore, a safe limit of air infusion (0.1 ml/kgbody wt for bolus infusion and 0.03 ml/kg per minutefor continuous infusion) has been suggested (25,28).Measures to minimize the risk of air embolism include
avoidance of extremely high dialysis blood flow, keeping
Figure 1. | Venous air embolism may arise from 4 possible areas of air entry into the dialysis circuit. Schematic diagram of a hemodialysiscircuit depicting four possible areas of air entry. (1) A broken or loose luer connection between the arterial needle and the tubing can result in airentry, because this segment has negative intraluminal pressure. (2) A hole in the arterial tubing can suck air into the arterial line. (3) Air entry canoccur during administration of anticoagulation or saline. (4) Inadequate priming can result in air entry from the dialyzer or dialysis tubing. Acrack in the venous bloodline will not cause air entry due to the positive intraluminal pressure. Air entering the circuit presents to the venous airtrap and forms foam/bubble at the top of blood level. As soon as the blood level in the venous air trap chamber falls below the air detector level,it immediately triggers an alarm and stops blood flow. As a consequence, venous air embolism occurs due to human error.
Clin J Am Soc Nephrol ▪: ccc–ccc, ▪▪▪, 2016 Hemodialysis Emergencies, Saha et al. 3

the arterial luer lock tightened, adequately priming thedialyzer and tubing system before initiation of an HDsession, and maintenance of a high blood level in thevenous air catcher (29,35).Massive VAE manifests with chest pain, dyspnea, and
syncope. Cerebral air embolism may cause blurry vision,altered mental status, seizures, or ischemic stroke. Patientsmay develop hypotension and tachycardia due to rightventricular overload with involvement of the pulmonarycapillary bed (26,27,36). The degree of end organ damagedepends on the rate of air entry, volume of air, the pa-tient’s position, and underlying cardiac status. In dogs,rapid injection of 7.5 ml/kg air is lethal. In humans, a vol-ume of 100–300 ml air is considered fatal (37,38). A highclinical suspicion is required to diagnose VAE. PrecordialDoppler can detect 0.05 ml/kg air, whereas transesopha-geal echocardiogram can detect 0.02 ml/kg air (39). Com-puted tomography may detect air in suspected cases ofcerebral embolism.After VAE is suspected, the patient should be provided
with 100% oxygen (27). Aspiration of air may be attemptedif the catheter is still in place (26). Early studies suggestedthat the left lateral recumbent (LLR) position could pre-vent right ventricular failure by preventing outflow tractobstruction during air embolism by moving the air moresuperiorly in the right ventricle (40–42). Geissler et al. (43)and Mehlhorn et al. (44) studied the effect of injecting2.5 ml/kg air at a rate of 5 ml/s in dogs and concludedthat the LLR position did not provide hemodynamicadvantage over the supine position. Although traditionalteaching has been to maintain an LLR with head downposition for suspected VAE, the supine position has beenrecommended more recently (26). The supine position alsoprovides additional advantage of appropriate delivery ofoxygen and hemodynamic support, a critical part of thetreatment (26). An LLR position has been recommended byMuth and Shank (26) if aspiration of air is to be attemptedthrough an existing central venous catheter (CVC) forVAE (26,43).Air embolism may also occur during placement of an
HD CVC, accidental disconnection during its use, or at itsremoval. Vesely (45) reported 15 cases of air embolismoccurring during placement of 11,583 tunneled and non-tunneled CVCs (0.13%). All 15 cases occurred during in-sertion of tunneled CVCs; most patients had mild tomoderate symptoms, except one who died. Rinsing thecatheter, placing the patient in a supine position, andinserting the needle during expiration may prevent airembolism during CVC placement (46). A break in the cath-eter or accidental disconnection may also lead to fatal airembolism (47). During CVC removal, the patient should besupine, with catheter removal performed during exhala-tion or a Valsalva maneuver to increase intrathoracic pres-sure (46). An air-occlusive dressing should be in place for24 hours to prevent delayed air entry through the subcu-taneous track (48).
HemolysisRed blood cells (RBCs) undergo shear stress when they
circulate through the HD circuit, and are, therefore, at riskfor fragmentation. Additionally, blood osmotic changes,
dialysate contaminants, or hyperthermia may each enhancehemolysis (Table 3) (49–52). Because blood flow is higherat the center of a laminar flow than at the edges (wall) ofthe extracorporeal circuit, the RBC membrane is exposedto a differential force on two different sides, therebycausing a shear stress (51). The low degree of hemolysisthat typically occurs during HD is insufficient to produce ameasurable drop in hematocrit. More significant hemolysismay occur in cases of dialysate contamination with tracemetals (copper or zinc), disinfectant added to city water(chloramine), or nitrate (49,53). The normal starting dialy-sis blood flow with a new arteriovenous (AV) fistula is 250ml/min with a 17-gauge needle. In comparison, a dialysisblood flow of 500 ml/min can be delivered using a14-gauge needle without inducing hemolysis (54). Thepositive and negative pressures (approximately 1500 and2500 mmHg, respectively) sustained by RBCs in the ex-tracorporeal circuit usually do not cause any hemolysis(51). However, attempting a high dialysis blood flowwith a small gauge needle may induce hemolysis.Overheated dialysate may cause thermal injury and
hemolysis. A 1948 study by Ham et al. (55) showed changesin RBC morphology, osmotic fragility, and hemolysis attemperatures .47°C. In 1975, Berkes et al. (56) reportedon a patient with delayed hemolysis 48 hours after expo-sure to overheated dialysate of 50°C. Because modernHD machines trigger an alarm at dialysate temperature.39.5°C, hyperthermic hemolysis is rare (55,57). If theHD machine triggers an alarm for overheated dialysate,an appropriate stepwise protocol should be followed: re-sponding to the alarm, immediate cessation of dialysis,and informing concerned authorities and supervisor tofind the source of heated water (57). Jepson and Alonso(57) reported an issue with a valve system that led toheated dialysate of 39.8°C; no harm was caused to the pa-tient due to the attentiveness of the nurse who followed anappropriate protocol (57).Hemolysis due to osmotic changes and dialysate impu-
rities is also rare. Several investigators have reportedmechanical injury to RBCs caused by kinked dialysistubing (52,58). Sudden bends, turns, and the entry pointinto the dialyzer are additional vulnerable areas for kink-ing. A simultaneous decrease of .25 mmHg in both thearterial (prepump) and venous (postpump) pressuressuggests a severe postpump kinked tubing that may resultin hemolysis; this drop in pressure results from decreaseblood flow due to severe obstruction. Therefore, it essen-tial to use the length of tubing recommended by the man-ufacturer, monitor the arterial and venous dialysispressures, and avoid sudden bends in the tubing (59). Amultistate outbreak of hemolysis during HD led to thefinding of faulty blood tubing causing hemolysis. Narrow-ing of the blood tubing before its entry to the dialyzer ledto exposure of RBCs to increased pressure and consequenthemolysis (60).Patients with severe intradialytic hemolysis complain of
nausea, shortness of breath, abdominal/back pain, andchills and initially develop acute hypertension (61). Con-firmatory laboratory data include low serum haptoglobin,elevated lactate dehydrogenase, reduction in hematocrit,and pink serum. When hemolysis is suspected, the HDsession should be stopped immediately. Blood should
4 Clinical Journal of the American Society of Nephrology
not be returned from the extracorporeal circulation to thebloodstream due to the risk of precipitating severe hyper-kalemia by infusing potassium released from hemolyzed
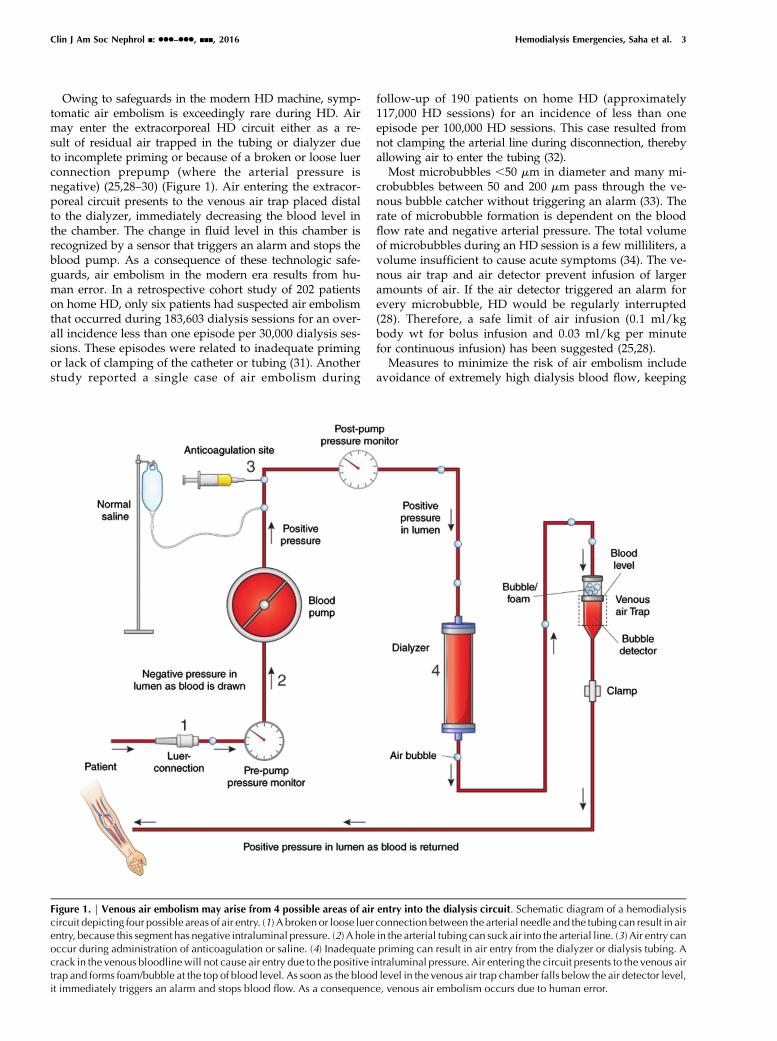
erythrocytes. If several patients develop hemolysis in a sin-gle dialysis unit, contamination of the dialysate, faultytubing, and altered dialysate osmolality should be suspec-ted. A systematic assessment of the potential causes isimperative to avoid recurrent hemolysis during a sub-sequent HD session (Figure 2). A root cause analysis(RCA) should be performed in each case, and every as-pect of the HD session should be well examined; bloodtubing and the needle system should be saved for futureinvestigation.
Venous Needle DislodgementVenous needle dislodgement (VND) is a rare but life-
threatening complication of HD. With a typical dialysisblood flow of 300–500 ml/min, hemorrhagic shock ensueswithin minutes (after loss of 30%–40% of total blood vol-ume) (62). The Veterans Administration National Centerfor Patient Safety reported 40 major hemorrhages due toVND or disconnection at the dialysis catheter site during2.5 million dialysis sessions or approximately one episodeper 60,000 HD sessions (63). Two large Canadian series ofpatients on home HD reported VND in one in 11,000 (31)
Table 3. Causes of hemolysis during hemodialysis
Dialysate relatedContamination with copper, zinc, nitrate, nitrite, andchloramine
Hypo-osmolar dialysateHyperthermia
Extracorporeal circuit relatedBlood pump malocclusionSingle–needle high–flow dialysisPartial occlusion of HD catheterKinked tubing, faulty blood tubing
Patient relatedSickle cell anemiaHereditary spherocytosisAutoimmune hemolysis
HD, hemodialysis.
Figure 2. | Schematic diagram illustrating an approach to evaluation of a suspected case of hemolysis during hemodialysis (HD) and its rootcause analysis to prevent future episodes. LDH, lactate dehydrogenase.
Clin J Am Soc Nephrol ▪: ccc–ccc, ▪▪▪, 2016 Hemodialysis Emergencies, Saha et al. 5

and one in 20,000 HD sessions (32). Data from Pennsylva-nia public safety reported 32 patients with VND during2.26 million HD session, for a frequency of about one in70,000 HD sessions (64).The major factors leading to needle dislodgement are
related to access care (improper taping of access tubing tothe skin, loose luer lock tubing connection, bloodlines notbeing looped loosely, or access site not being visible) andpatient factors (a confused patient pulling the needle outof the access) (65). An acute decrease in dialysis venouspressure should theoretically ensue rapidly after dislodge-ment of the venous needle from the access and trigger apressure alarm to alert the dialysis nurse. However, thevenous alarm monitor on HD machines is affected bynot only the intra-access pressure but also, the dialysisblood flow, blood viscosity, flow resistance of the extra-corporeal tubing, and the height difference between theaccess and venous drip chamber (66). In addition, the intra-access pressure is higher for grafts than fistulas (by 27/15mmHg) (67). Ideally, to ensure early detection of blood loss,the venous pressure alarm would be set 10 mmHg below thebaseline dialysis venous pressure. However, the venous pres-sure varies by 30–40 mmHg during a typical dialysis sessiondue to patient position (reclining versus sitting) and move-ment of the access extremity (66,68). To prevent triggeringmultiple false pressure alarms during each dialysis session,the pressure monitor is usually set below that threshold.As a consequence, the dialysis staff may have a false senseof security when, in fact, a substantial blood leak may occurbefore the venous pressure drops by 40 mmHg and triggersthe pressure alarm.Various sensors can detect blood leaks during VND.
Some were initially developed to detect moisture related toenuresis but later, used off label for detection of VND bysome dialysis units (65,66). Redsense, a device developedfor detection of blood leakage, has been Food and DrugAdministration cleared for in-center and home HD. It con-sists of an alarm unit connected by an optical fiber to asensor patch; the sensor patch has an absorbent patch inthe center. The patch is placed over the venous needle,with the absorbent area placed directly over the needleentry point. In the event of VND or significant blood leak-age, the blood comes in contact with the optical sensor thatis embedded within the patch and generates a continuousalarm (69). Ahlmén et al. (70) reported that Redsense cor-rectly alarmed in 92.5% of cases of blood leakage; whenthe patch was modified and placed closer to the venouspuncture site, the device functioned in 97.2% of all tests(70). Although blood sensors add substantially to the costof HD (Redsense costs about $550), they can be consideredfor additional safety in high-risk patients and patients onhome HD. However, sensors should never replace an ap-propriate stepwise protocol to prevent VND. This includesproper taping of access needle, adequate tightening ofluer lock at all connections, and ensuring that all blood-lines are loosely looped to prevent accidental dislodge-ment. The access site should always be examinedwhenever the venous pressure monitor suggests a dropin pressure, even if the blood leakage detector does notgenerate an alarm. The two most important measures aremaintaining the access site visible at all times and keep-ing high-risk patients close to the nurse’s station (65). A
detailed 12-step protocol, including taping techniques,assessment of risks for VND, and its prevention, is availableat https://www.annanurse.org/download/reference/journal/vndArticle.pdf (65).
Allergic Reaction during HDAn allergic or allergic-like reaction during HD must be
closely investigated, because re-exposure to the allergenmay result in worse signs and symptoms and a pooroutcome. A 1982–1983 survey documented 3.3 allergic re-actions per 1000 patient-years of dialysis with a hollowfiber dialyzer (71). Daugirdas et al. (72) reported 21 severeallergic reactions to dialyzers in 260,000 dialysis sessionsfor a frequency of approximately one episode in 12,000 HDsessions. These allergic reactions included four respiratoryarrests and one death. A patient may get an allergic reac-tion to the dialyzer itself or more commonly, the sterilizer(kills all micro-organisms, including bacterial spores),disinfectant (kills micro-organisms on the surface but notbacterial spores), heparin, or other medications infusedduring dialysis (antibiotics, blood, or iron) (73,74).Allergic reactions are classified as type A and type B
(75,76). Type A allergic reactions occur within 5–20 min-utes of HD initiation and present with pruritus, urticaria,bronchospasm, laryngeal edema, or anaphylactic shock.Type B reactions occur later in the dialysis session andare associated with less intense symptoms, such as chestand back pain. Type A reactions are mediated through IgE,whereas type B reactions are complement mediated (77).Earlier dialyzers were composed of cellulose (a cotton
derivative). Owing to their organic component, theyactivated the alternate complement cascade and wereconsidered bioincompatible (77,78). Subsequent modifica-tions that added acetate side chains to the cellulose (cellu-lose acetate, diacetate, and triacetate) reduced complementactivation, making the dialyzers more biocompatible. Atpresent, most United States dialysis centers use syntheticdialyzers, which are considered highly biocompatible, be-cause they only minimally activate complement (78). Syn-thetic dialyzers are composed of polymethylmethacrylate,polyether sulfone, polysulfone, or polyacrylonitrile (PAN)(78). Dialyzers are sterilized with chemicals (ethylene ox-ide), steam (heat), or radiation (g or b). Ethylene oxide hasfallen out of favor due to its propensity to attach to thepotting compound of the dialyzer and cause type A aller-gic reactions (79–82).Various mechanisms (Figure 3) have been proposed for
allergic and allergic-like reactions during HD dependingon the allergen (77,82–88). Ethylene oxide mediates ana-phylaxis through IgE-mediated hypersensitivity, whereasdialyzer components typically activate complement orbradykinin. Tielemans et al. (89) reported five cases of anaphy-lactoid reactions to acrylonitrile 69 (AN69) dialyzers occurringwithin minutes of HD initiation in patients on an angiotensin–converting enzyme inhibitor (ACEi). This reaction ismediated by bradykinin rather than IgE, histamine, orcomplement (89). The negatively charged moiety ofAN69 during contact phase with blood may activate Ha-geman factor (factor 12), leading to bradykinin formation.ACEi also inhibits kininase, an enzyme that inactivatesbradykinin, thereby further increasing plasma bradykinin
6 Clinical Journal of the American Society of Nephrology
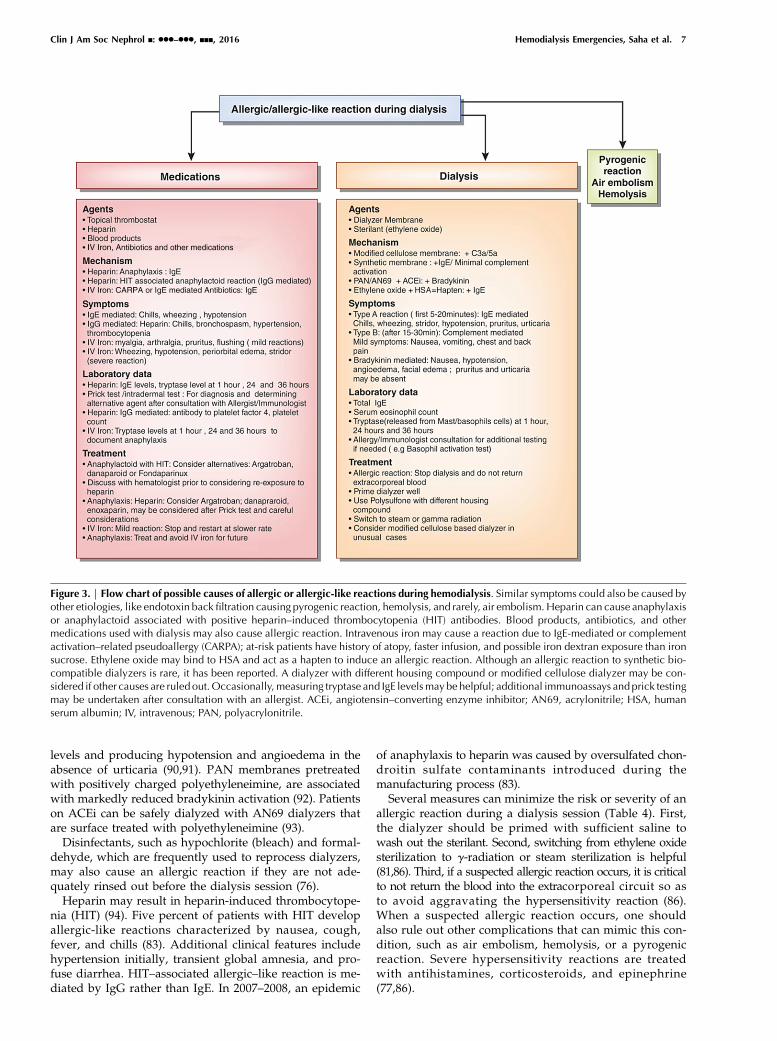
levels and producing hypotension and angioedema in theabsence of urticaria (90,91). PAN membranes pretreatedwith positively charged polyethyleneimine, are associatedwith markedly reduced bradykinin activation (92). Patientson ACEi can be safely dialyzed with AN69 dialyzers thatare surface treated with polyethyleneimine (93).Disinfectants, such as hypochlorite (bleach) and formal-
dehyde, which are frequently used to reprocess dialyzers,may also cause an allergic reaction if they are not ade-quately rinsed out before the dialysis session (76).Heparin may result in heparin-induced thrombocytope-
nia (HIT) (94). Five percent of patients with HIT developallergic-like reactions characterized by nausea, cough,fever, and chills (83). Additional clinical features includehypertension initially, transient global amnesia, and pro-fuse diarrhea. HIT–associated allergic–like reaction is me-diated by IgG rather than IgE. In 2007–2008, an epidemic
of anaphylaxis to heparin was caused by oversulfated chon-droitin sulfate contaminants introduced during themanufacturing process (83).Several measures can minimize the risk or severity of an
allergic reaction during a dialysis session (Table 4). First,the dialyzer should be primed with sufficient saline towash out the sterilant. Second, switching from ethylene oxidesterilization to g-radiation or steam sterilization is helpful(81,86). Third, if a suspected allergic reaction occurs, it is criticalto not return the blood into the extracorporeal circuit so asto avoid aggravating the hypersensitivity reaction (86).When a suspected allergic reaction occurs, one shouldalso rule out other complications that can mimic this con-dition, such as air embolism, hemolysis, or a pyrogenicreaction. Severe hypersensitivity reactions are treatedwith antihistamines, corticosteroids, and epinephrine(77,86).
Figure 3. | Flow chart of possible causes of allergic or allergic-like reactions during hemodialysis. Similar symptoms could also be caused byother etiologies, like endotoxin back filtration causing pyrogenic reaction, hemolysis, and rarely, air embolism. Heparin can cause anaphylaxisor anaphylactoid associated with positive heparin–induced thrombocytopenia (HIT) antibodies. Blood products, antibiotics, and othermedications used with dialysis may also cause allergic reaction. Intravenous iron may cause a reaction due to IgE-mediated or complementactivation–related pseudoallergy (CARPA); at-risk patients have history of atopy, faster infusion, and possible iron dextran exposure than ironsucrose. Ethylene oxide may bind to HSA and act as a hapten to induce an allergic reaction. Although an allergic reaction to synthetic bio-compatible dialyzers is rare, it has been reported. A dialyzer with different housing compound or modified cellulose dialyzer may be con-sidered if other causes are ruled out.Occasionally,measuring tryptase and IgE levelsmaybe helpful; additional immunoassays and prick testingmay be undertaken after consultation with an allergist. ACEi, angiotensin–converting enzyme inhibitor; AN69, acrylonitrile; HSA, humanserum albumin; IV, intravenous; PAN, polyacrylonitrile.
Clin J Am Soc Nephrol ▪: ccc–ccc, ▪▪▪, 2016 Hemodialysis Emergencies, Saha et al. 7

Adverse Reactions with Intravenous IronIntravenous iron, which is more efficacious than oral iron
in raising hemoglobin in the HD population, is adminis-tered to approximately 70% of patients on HD each month(95). Adverse drug events to intravenous iron were esti-mated at 94 per million intravenous doses in 1998–2000and decreased to 38 per million by 2001–2003 after aswitch to safer formulations (96,97). The rate of fatal ad-verse drug events was highest for higher molecular weightdextran (11.3 per million), intermediate for lower molecu-lar weight dextran (3.3 per million), and lowest for sodiumferric gluconate (0.9 per million) and iron sucrose (0.6 permillion). Wysowski et al. (98) reported that the mortalityrate between 2002 and 2006 was exceedingly low (0.06–0.32deaths per million doses of iron purchased).Minor adverse reactions can occur with any intravenous
iron preparation, but severe life–threatening reactions arerare. Minor symptoms, such as pruritus, flushing, mildchest discomfort, arthralgia, myalgia, and nausea, usuallyabate with cessation of the infusion; it can be restarted at alower rate after symptoms resolve (73,87). If patients de-velop urticaria, then infusion should be stopped, and thepatient should be observed. Restarting the infusion aftertreatment with steroids may be considered after symptomsresolve (99). A more severe reaction may present with se-vere chest pain, persistent hypotension, and cough, and itmay warrant stopping the infusion and treating with ste-roids and epinephrine. Premedication with steroids shouldbe considered in patients at high risk of developing a re-action: history of inflammatory arthritis, multiple drug al-lergies, or severe asthma (100,101). Diphenhydramineshould be avoided as a premedication, because it maycause symptoms similar to minor reactions and be falselyinterpreted as an adverse effect (102,103). A life-threateningreaction (stridor, wheezing, periorbital edema, or symptom-atic hypotension) to intravenous iron infusion precludes fu-ture iron infusion (99). Intravenous iron is contraindicated inthe first trimester of pregnancy and should be used withcaution during the second and third trimesters (87).
Emergencies Related to Dialysis Water SystemThis is a very brief review of the HD emergencies that can
arise due to water system issues. Several excellent reviewarticles provide greater detail (104–106). Acute loss of wa-ter in a dialysis unit is an emergency. It may be localizeddue to breakage in water pipes in the dialysis unit only orrepresent a hospital-wide problem. If it is localized todialysis units, immediate notification to concerned author-ities, nursing supervisor, and medical director shouldbe made. If water from other areas of the hospital can beused, then a portable reverse osmosis system can be used.
In case of more widespread loss of water, stepwise pro-tocol should be followed, including saving water, alertinghigher authorities, and communication with the city waterbody. Patients needing acute dialysis may be switched toalternative RRT, like CRRT, or transferred to a differentmedical facility (107).Patients on in-center HD are exposed to close to 200 L
water during an average dialysis session. With the dialysismembrane being the only barrier between the dialysate andblood, it is critical that municipal water undergo rigorouspurification before its use during dialysis. Each dialysisunit has its own water system for purification of municipalwater, protocol for sampling and monitoring, and man-agement to adhere to the guidelines for water quality set bythe American National Standards Institute/Association forthe Advancement of Medical Instrumentation (104).Pyrogenic reaction during a dialysis session may be due
to multiple causes, including infection from various sources;water/dialysate bacterial contamination should be consid-ered if there is cluster of similar events. Chloramine/chlorine is added to city water for decontamination; this levelof protection is abolished downstream of carbon tanks indialysis water systems, and thus, the reverse osmosis sys-tem, storage tank, and pipes are subjected to contamination(105,108,109). Dialysis units follow strict protocols to deliver
Table 4. Measures to minimize an allergic reaction to a dialyzer
(1) Prime the dialyzer well(2) Switch from ethylene oxide sterilization to g- or steam-sterilized dialyzer(3) In the event of a hypersensitivity reaction, do not return the blood, because this may aggravate the allergic reaction(4) Treat with antihistamines, corticosteroids, and epinephrine for a hypersensitivity reaction(5) Rule out other conditions that may simulate an allergic reaction (air embolism, hemolysis, pyrogenic reaction)
Figure 4. | An arteriovenous graft with evidence of thin shiny surface(arrow) and superficial ulceration (arrowhead) over a pseudoaneurysm.
8 Clinical Journal of the American Society of Nephrology
purified water for dialysis, including running water sys-tem, maintenance, disinfection process, and periodicchecks and evaluating with water cultures and endotoxinassays. Nonadherence to the protocol may result in watercontamination.Chloramine and chlorine are removed by primary and
secondary carbon tanks of the dialysis water system. Chlo-ramine may cause hemolysis and methemoglobinemia inpatients on dialysis due to exhaustion of carbon tanks orexcess load of chloramine in city water exceeding thecapacity of carbon tanks (49,108–111). Thus, total chlorine,which is the sum of free chlorine and bound chlorine (chlo-ramine), is measured from both carbon tanks every 4hours. The total chlorine level should be ,0.1 parts permillion (1 part per million 51 mg/L) (104,112).Methemoglobinemia usually manifests as cyanosis with
chocolate brown color blood in the tubing and saturationgap (113). In such cases, the oxygen saturation calculatedfrom arterial blood gas (PaO2$70 mmHg) is higher thanthat measured by pulse oximetry (SaO2#90%) (114,115).The diagnosis is confirmed by direct methemoglobinmeasurement.Hydrogen peroxide is commonly used for disinfection of
water storage tanks in hospitals. It is usually removed bycarbon filters but not by reverse osmosis. There have beenreports of hemolysis and methemoglobinemia from expo-sure of patients’ blood to hydrogen peroxide. This mayhappen if the potable water system does not have a carbonfilter or if the carbon tanks gets exhausted when largerquantities of chlorine/chloramine and hydrogen peroxidehave to be processed (113,116,117).
An outbreak of fluoride toxicity leading to severepruritus, headache, and cardiac arrest has been reported(118). It was found that an exhausted resin of deionizerwas releasing fluoride into the water. Fluoride (an anion)binds to calcium and magnesium and lowers their serumlevel. Additionally, it may cause hyperkalemia by its ac-tion on the sodium-potassium ATPase pump and indi-rectly cause efflux of potassium from cells (119).To prevent such complications, appropriate protocol
should always be followed. A periodic communication withthe city water body and hospital maintenance may preventadditional complications. A cluster of adverse symptoms orevents should prompt a thorough investigation.
Vascular Access HemorrhageHemorrhage from an AV access is an uncommon but
potentially fatal complication if it is not recognizedpromptly and acted on with an appropriate intervention.Most fatal vascular access hemorrhages occur outside of thedialysis facility, but occasionally, they rupture at thedialysis unit (120). Patients and their families should beeducated about the recognition and emergent manage-ment of a bleeding AV access. Pseudoaneurysm (PSA)is a false aneurysm, because it does not have all of thelayers of a vein, but it is rather composed of hematomaand fibrous tissue. It results from trauma and repeatedcannulation during HD. Aneurysms usually form at theoutflow vein/graft of an AV access and result from in-creasing dilation due to high blood flow and vasculardamage (121,122). Physical examination of an aneurysm
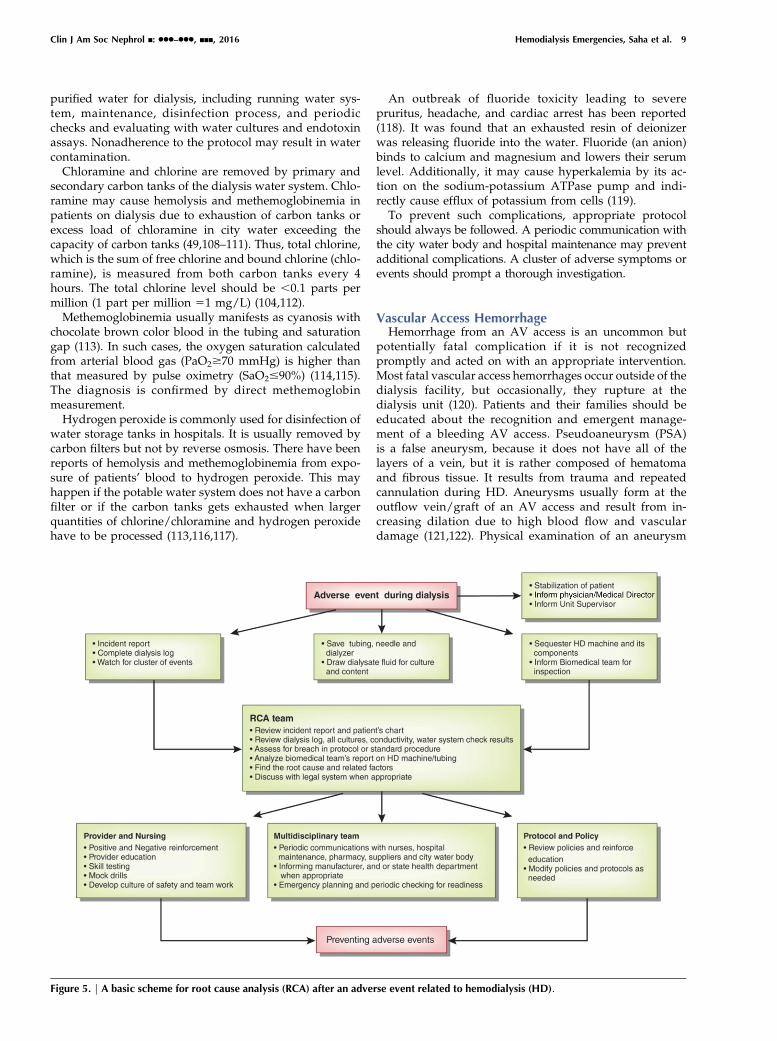
Figure 5. | A basic scheme for root cause analysis (RCA) after an adverse event related to hemodialysis (HD).
Clin J Am Soc Nephrol ▪: ccc–ccc, ▪▪▪, 2016 Hemodialysis Emergencies, Saha et al. 9

is the most important tool to determine the need for anintervention (Figure 4). Any rapidly enlarging PSA, evi-dence of outflow stenosis (arm elevation test—failure tocollapse, high-pitch bruit), thinning or ulceration of skinover the PSA, pulsatility, or evidence of infection shouldprompt urgent intervention (121,123). Proper cannulationtechniques may prevent PSA formation. Rope ladder tech-nique prevents aneurysm formation, whereas repeatedcannulation of the same area may promote aneurysmformation (123).If the aneurysm is stable without evidence of imminent
rupture (ulceration, thinning or shiny skin, or infection),then referral should be made for a fistulogram to evaluatefor potential underlying outflow stenosis. Angioplasty todecrease the intra-access pressure may prevent aneurysmformation or slow its growth.In the event of bleeding from vascular access site, direct
continuous pressure with a finger for 15–20 minutes isthe most effective method of controlling the bleeding. Inthe event of rupture of a PSA or aneurysm away fromdialysis unit or hospital, direct pressure with a finger atthe site of bleeding is the best method of controllingbleeding. Patients should be advised to continue holdingdirect pressure until emergency medical help arrives andavoid applying a tourniquet, towel, or BP cuff to theextremity (124).
RCAAny adverse event, whether it has occurred, has the
potential to occur, or was averted by appropriate in-tervention, requires a thorough investigation to identifyits root cause (125). All dialysis units must have proto-cols for reporting such events and taking appropriatemeasures toward RCA. The culture of safety in thehealth care field comes from education, following proto-cols, and a balance between staffing and work burden(126,127). There is often one main root cause leading toan adverse event and multiple other related factors; all ofthese factors should be evaluated. There are variousguidelines regarding performing an RCA, includingone by the Centers for Medicare and Medicaid Services(128).During an adverse event, patient safety andmanagement
of the adverse event are paramount. The nursing staff andother care providers should work as a team to achieve thatgoal rather than blaming each other or attempting to find acause. After the patient has been stabilized, additionalstepwise measures should be undertaken toward an RCA.This may start with an incident report completed bynursing staff. The nurses are encouraged to elaborate thesequence of events, including those related to the patient,surrounding environment, and the dialysis machine. Thedialysis log, including patient and machine vital measure-ments, should be completed. The HD machine, dialyzer,and tubing should be sequestered pending completion ofthe investigation. In an isolated event, like hemolysisduring HD, a stepwise protocol toward that event maybe considered (Figure 2). In other cases, a broader viewmay be more appropriate (Figure 5).The appropriate authorities, including the dialysis su-
pervisor, legal system, and hospital authorities, should
be informed of the complication. An RCA should beexhaustive and confidential. After a cause is found,appropriate measures should be implemented to preventa similar occurrence. These measures may include a changein policy or protocol, provider education, communicationamong different staff members and hospital personnel,multidisciplinary approach, and periodic mock drills andskills testing.
AcknowledgmentsThisworkwas supported, in part, byNational Institutes ofHealth
grant T32DK007545 (to M.S.).
DisclosuresNone.
References1. USRDS: US Renal Data System USRDS 2013 Annual Data
Report: Atlas of Chronic Kidney Disease and End-Stage RenalDisease in the United States, Vol. 2, Bethesda, MD, NationalInstitutes of Health, National Institute of Diabetes andDigestiveand Kidney Diseases, 2013
2. Karnik JA, Young BS, Lew NL, Herget M, Dubinsky C, LazarusJM, Chertow GM: Cardiac arrest and sudden death in dialysisunits. Kidney Int 60: 350–357, 2001
3. Agarwal R: How can we prevent intradialytic hypotension?Curr Opin Nephrol Hypertens 21: 593–599, 2012
4. Dheenan S, Henrich WL: Preventing dialysis hypotension: Acomparison of usual protective maneuvers. Kidney Int 59:1175–1181, 2001
5. Perazella MA: Pharmacologic options available to treat symp-tomatic intradialytic hypotension.Am J KidneyDis 38[Suppl 4]:S26–S36, 2001
6. Reilly RF: Attending rounds: A patient with intradialytic hypo-tension. Clin J Am Soc Nephrol 9: 798–803, 2014
7. Patel N, Dalal P, Panesar M: Dialysis disequilibrium syndrome:A narrative review. Semin Dial 21: 493–498, 2008
8. Arieff AI: Dialysis disequilibrium syndrome: Current conceptson pathogenesis and prevention. Kidney Int 45: 629–635, 1994
9. Silver SM, Sterns RH, HalperinML: Brain swelling after dialysis:Old urea or new osmoles? Am J Kidney Dis 28: 1–13, 1996
10. Kennedy AC, Linton AL, Eaton JC: Urea levels in cerebrospinalfluid after haemodialysis. Lancet 1: 410–411, 1962
11. Rosen SM, O’Connor K, Shaldon S: Haemodialysis disequilib-rium. BMJ 2: 672–675, 1964
12. Arieff AI, Massry SG, Barrientos A, Kleeman CR: Brain waterand electrolyte metabolism in uremia: Effects of slow and rapidhemodialysis. Kidney Int 4: 177–187, 1973
13. Silver SM, DeSimone JA Jr., Smith DA, Sterns RH: Dialysisdisequilibrium syndrome (DDS) in the rat: Role of the “reverseurea effect.” Kidney Int 42: 161–166, 1992
14. Silver SM: Cerebral edema after rapid dialysis is not caused byan increase in brain organic osmolytes. J Am Soc Nephrol 6:1600–1606, 1995
15. Trachtman H, Futterweit S, Tonidandel W, Gullans SR: The roleof organic osmolytes in the cerebral cell volume regulatoryresponse to acute and chronic renal failure. J Am SocNephrol 3:1913–1919, 1993
16. Trinh-Trang-Tan MM, Cartron JP, Bankir L: Molecular basisfor the dialysis disequilibrium syndrome: Altered aquaporinand urea transporter expression in the brain. Nephrol DialTransplant 20: 1984–1988, 2005
17. Zepeda-Orozco D, Quigley R: Dialysis disequilibrium syn-drome. Pediatr Nephrol 27: 2205–2211, 2012
18. Bagshaw SM, Peets AD, Hameed M, Boiteau PJ, Laupland KB,Doig CJ: Dialysis disequilibrium syndrome: Brain death fol-lowing hemodialysis for metabolic acidosis and acute renalfailure–a case report. BMC Nephrol 5: 9, 2004
19. Lopez-Almaraz E, Correa-Rotter R: Dialysis disequilibriumsyndrome and other treatment complications of extreme
10 Clinical Journal of the American Society of Nephrology
uremia: A rare occurrence yet not vanished. Hemodial Int 12:301–306, 2008
20. Esnault P, Lacroix G, Cungi PJ, D’Aranda E, Cotte J, Goutorbe P:Dialysis disequilibrium syndrome in neurointensive care unit:The benefit of intracranial pressure monitoring. Crit Care 16:472, 2012
21. Kidney Disease Improving Global Outcome: Clinical PracticeGuideline for Acute Kidney Injury, 2012. Available at: http://www.kdigo.org/clinical_practice_guidelines/pdf/KDIGO%20AKI%20Guideline.pdf. Accessed July 1, 2016
22. Port FK, Johnson WJ, Klass DW: Prevention of dialysis disequi-librium syndrome by use of high sodium concentration in thedialysate. Kidney Int 3: 327–333, 1973
23. Arieff AI, Lazarowitz VC, Guisado R: Experimental dialysisdisequilibrium syndrome: Prevention with glycerol. Kidney Int14: 270–278, 1978
24. Rodrigo F, Shideman J, McHugh R, Buselmeier T, Kjellstrand C:Osmolality changes during hemodialysis. Natural history,clinical correlations, and influence of dialysate glucose andintravenous mannitol. Ann Intern Med 86: 554–561, 1977
25. Barak M, Nakhoul F, Katz Y: Pathophysiology and clinical im-plications ofmicrobubbles during hemodialysis. SeminDial 21:232–238, 2008
26. Muth CM, Shank ES: Gas embolism. N Engl J Med 342: 476–482, 2000
27. vanHulst RA,Klein J, LachmannB:Gas embolism: Pathophysiologyand treatment. Clin Physiol Funct Imaging 23: 237–246, 2003
28. Polaschegg HD: Hemodialysis machine air detectors need notdetect microbubbles. Artif Organs 31: 911–912, 2007
29. Forsberg U, Jonsson P, Stegmayr C, Jonsson F, Nilsson B,Nilsson Ekdahl K, Stegmayr B: A high blood level in the venouschamber and a wet-stored dialyzer help to reduce exposure formicroemboli during hemodialysis. Hemodial Int 17: 612–617,2013
30. Riddick L, BrogdonBG: Fatal air embolismduring renal dialysis.Am J Forensic Med Pathol 33: 110–112, 2012
31. Tennankore KK, d’GamaC, Faratro R, Fung S,Wong E, Chan CT:Adverse technical events in home hemodialysis. Am J KidneyDis 65: 116–121, 2015
32. Wong B, Zimmerman D, Reintjes F, Courtney M, Klarenbach S,Dowling G, Pauly RP: Procedure-related serious adverse eventsamong home hemodialysis patients: A quality assurance per-spective. Am J Kidney Dis 63: 251–258, 2014
33. Keshavarzi G, Barber TJ, Yeoh G, Simmons A, Reizes JA:Two-dimensional computational analysis of microbubbles inhemodialysis. Artif Organs 37: E139–E144, 2013
34. Stegmayr B, ForsbergU, Jonsson P, Stegmayr C: The sensor in thevenous chamber does not prevent passage of air bubbles duringhemodialysis. Artif Organs 31: 162–166, 2007
35. Wagner S, Rode C, Wojke R, Canaud B: Observation of mi-crobubbles during standard dialysis treatments. Clin Kidney J 8:400–404, 2015
36. King MB, Harmon KR: Unusual forms of pulmonary embolism.Clin Chest Med 15: 561–580, 1994
37. Palmon SC, Moore LE, Lundberg J, Toung T: Venous air embo-lism: A review. J Clin Anesth 9: 251–257, 1997
38. Toung TJ, Rossberg MI, Hutchins GM: Volume of air in a lethalvenous air embolism. Anesthesiology 94: 360–361, 2001
39. Rossi UG, Torcia P, Rigamonti P, Colombo F, Giordano A,Gallieni M, Cariati M: Tunneled central venous catheter ex-change: Techniques to improve prevention of air embolism.J Vasc Access 17: 200–203, 2016
40. Durant TM, Long J, Oppenheimer MJ: Pulmonary (venous) airembolism. Am Heart J 33: 269–281, 1947
41. Oppenheimer MJ, Durant TM, Lynch P: Body position inrelation to venous air embolism and the associated car-diovascular-respiratory changes. Am J Med Sci 225: 362–373,1953
42. Durant TM,OppenheimerMJ, Lynch PR, AscanioG,WebberD:Body position in relation to venous air embolism: A roentgen-ologic study. Am J Med Sci 227: 509–520, 1954
43. Geissler HJ, Allen SJ, Mehlhorn U, Davis KL, Morris WP, ButlerBD: Effect of body repositioning after venous air embolism. Anechocardiographic study. Anesthesiology 86: 710–717, 1997
44. Mehlhorn U, Burke EJ, Butler BD, Davis KL, Katz J, Melamed E,Morris WP, Allen SJ: Body position does not affect the hemo-dynamic response to venous air embolism in dogs. AnesthAnalg 79: 734–739, 1994
45. Vesely TM: Air embolism during insertion of central venouscatheters. J Vasc Interv Radiol 12: 1291–1295, 2001
46. Feil M: Preventing central line air embolism. Am J Nurs 115:64–69, 2015
47. Halliday P, Anderson DN, Davidson AI, Page JG: Managementof cerebral air embolism secondary to a disconnected centralvenous catheter. Br J Surg 81: 71, 1994
48. Turnage WS, Harper JV: Venous air embolism occurring afterremoval of a central venous catheter. Anesth Analg 72:559–560, 1991
49. Junglee NA, Rahman SU, Wild M, Wilms A, Hirst S, Jibani M,Seale JR: When pure is not so pure: Chloramine-relatedhemolytic anemia in home hemodialysis patients. HemodialInt 14: 327–332, 2010
50. Yoon J, Thapa S, Chow RD, Jaar BG: Hemolysis as a rare butpotentially life-threatening complication of hemodialysis: Acase report. BMC Res Notes 7: 475, 2014
51. Polaschegg HD: Red blood cell damage from extracorporealcirculation in hemodialysis. Semin Dial 22: 524–531, 2009
52. Sweet SJ, McCarthy S, Steingart R, Callahan T: Hemolyticreactions mechanically induced by kinked hemodialysis lines.Am J Kidney Dis 27: 262–266, 1996
53. Manzler AD, Schreiner AW: Copper-induced acute hemolyticanemia. A new complication of hemodialysis. Ann Intern Med73: 409–412, 1970
54. Techert F, Techert S, Woo L, Beck W, Lebsanft H, Wizemann V:High blood flow rates with adjustment of needle diameter donot increase hemolysis during hemodialysis treatment. J VascAccess 8: 252–257, 2007
55. Ham TH, Shen SC, Fleming EM, Castle WB: Studies on thedestruction of red blood cells; thermal injury; action of heat incausing increased spheroidicity, osmotic and mechanical fra-gilities and hemolysis of erythrocytes; observations on themechanisms of destruction of such erythrocytes in dogs and in apatient with a fatal thermal burn. Blood 3: 373–403, 1948
56. Berkes SL, Kahn SI, Chazan JA, Garella S: Prolongedhemolysis from overheated dialysate. Ann Intern Med 83: 363–364, 1975
57. Jepson R, Alonso E: Overheated dialysate: A case study andreview. Nephrol Nurs J 36: 551–553, 2009
58. Gault MH, Duffett S, Purchase L, Murphy J: Hemodialysis in-travascular hemolysis and kinked blood lines. Nephron 62:267–271, 1992
59. Malinauskas RA: Decreased hemodialysis circuit pressuresindicating postpump tubing kinks: A retrospective investiga-tion of hemolysis in five patients. Hemodial Int 12: 383–393,2008
60. Duffy R, Tomashek K, Spangenberg M, Spry L, Dwyer D,Safranek TJ, Ying C, Portesi D, DivanH, Kobrenski J, ArduinoM,Tokars J, Jarvis W: Multistate outbreak of hemolysis in hemo-dialysis patients traced to faulty blood tubing sets.Kidney Int 57:1668–1674, 2000
61. Murcutt G: Guarding against hidden haemolysis during di-alysis: An overview. Summary of the EDTNA/ERCA Journal Clubdiscussion Spring 2007. J Ren Care 33: 191–195, 2007
62. Cherkas D: Traumatic hemorrhagic shock: Advances in fluidmanagement. Emerg Med Pract 13: 1–19, 2011
63. Bleeding Episodes during dialysis. Veterans Health Adminis-tration Warning System. Available at: http://www.patientsafety.va.gov/docs/alerts/BleedingEpisodesDuringDialysisAD09-02.pdf. Published 2008. Accessed July 1, 2016
64. Pennsylvania Patient Safety Authority: Hemodialysis Adminis-tration: Strategies to Ensure Safe Patient Care, 2010. Availableat: http://patientsafetyauthority.org/ADVISORIES/AdvisoryLibrary/2010/Sep7(3)/Pages/87.aspx. Accessed March 16, 2016
65. Axley B, Speranza-Reid J, Williams H: Venous needle dis-lodgement in patients on hemodialysis.NephrolNurs J 39: 435–445, 2012
66. Polaschegg HD: Venous needle dislodgement: The pitfalls ofvenous pressure measurement and possible alternatives, a re-view. J Ren Care 36: 41–48, 2010
Clin J Am Soc Nephrol ▪: ccc–ccc, ▪▪▪, 2016 Hemodialysis Emergencies, Saha et al. 11
67. Besarab A, Frinak S: The prevention of access failure: Pressuremonitoring. ASAIO J 44: 35–37, 1998
68. Ribitsch W, Schilcher G, Hafner-Giessauf H, Krisper P, HorinaJH, Rosenkranz AR, Schneditz D: Prevalence of detectablevenous pressure drops expected with venous needle dislodge-ment. Semin Dial 27: 507–511, 2014
69. Redsense Medical: How it works. Available at: http://www.redsensemedical.com/index.php/product/how-it-works.Accessed September 1, 2016
70. Ahlmen J, Gydell KH, Hadimeri H, Hernandez I, Rogland B,Strombom U: A new safety device for hemodialysis. HemodialInt 12: 264–267, 2008
71. Villarroel F, Ciarkowski AA: A survey on hypersensitivity reac-tions in hemodialysis. Artif Organs 9: 231–238, 1985
72. Daugirdas JT, Ing TS, Roxe DM, Ivanovich PT, Krumlovsky F,Popli S, McLaughlin MM: Severe anaphylactoid reactions tocuprammonium cellulose hemodialyzers. Arch Intern Med145: 489–494, 1985
73. Fishbane S: Safety in iron management. Am J Kidney Dis 41[Suppl]: 18–26, 2003
74. Centers for Disease Control and Prevention: Guideline forDisinfection and Sterilization in Healthcare Facilities, 2008.Available at: http://www.cdc.gov/hicpac/Disinfection_Sterilization/19_00glossary.html. Accessed May 1, 2016
75. Daugirdas JT, Ing TS: First-use reactions during hemodial-ysis: A definition of subtypes. Kidney Int Suppl 24: S37–S43,1988
76. Salem M, Ivanovich PT, Ing TS, Daugirdas JT: Adverse effects ofdialyzers manifesting during the dialysis session. Nephrol DialTransplant 9[Suppl 2]: 127–137, 1994
77. Sayeed K,Murdakes C, Spec A, Gashti C: Anaphylactic shock atthe beginning of hemodialysis. Semin Dial 29: 81–84, 2016
78. Boure T, Vanholder R: Which dialyser membrane to choose?Nephrol Dial Transplant 19: 293–296, 2004
79. Heegard KD, Tilley MA, Stewart IJ, Edgecombe HP, Lundy JB,Renz EM, Chung KK: Anaphylactoid reaction during first he-mofiltration with a PUREMA polysulfone membrane. Int J ArtifOrgans 36: 363–366, 2013
80. Ansorge W, Pelger M, Dietrich W, Baurmeister U: Ethyleneoxide in dialyzer rinsing fluid: Effect of rinsing technique, di-alyzer storage time, and potting compound. Artif Organs 11:118–122, 1987
81. Muller TF, Seitz M, Eckle I, Lange H, Kolb G: Biocompatibilitydifferences with respect to the dialyzer sterilization method.Nephron 78: 139–142, 1998
82. Dolovich J, Bell B: Allergy to a product(s) of ethylene oxide gas:Demonstration of IgE and IgG antibodies and hapten specificity.J Allergy Clin Immunol 62: 30–32, 1978
83. Warkentin TE, Greinacher A: Heparin-induced anaphylacticand anaphylactoid reactions: Two distinct but overlappingsyndromes. Expert Opin Drug Saf 8: 129–144, 2009
84. Shu KH, Kao TW, Chiang WC, Wu VC: A case of anaphylacticshock induced by FX60 polysulfone hemodialyzer but not F6-HPS polysulfone hemodialyzer. Hemodial Int 18: 841–845,2014
85. Santosa A, Tan SH, Cheng YK: Recurrent intradialytic heparininduced anaphylaxis: Workup and management. Asia Pac Al-lergy 3: 285–288, 2013
86. Ebo DG, Bosmans JL, Couttenye MM, Stevens WJ: Haemo-dialysis-associated anaphylactic and anaphylactoid reactions.Allergy 61: 211–220, 2006
87. Rampton D, Folkersen J, Fishbane S, Hedenus M, Howaldt S,Locatelli F, Patni S, Szebeni J, Weiss G: Hypersensitivity reac-tions to intravenous iron: Guidance for risk minimization andmanagement. Haematologica 99: 1671–1676, 2014
88. Ward RA: Ultrapure dialysate. Semin Dial 17: 489–497, 200489. Tielemans C, Madhoun P, Lenaers M, Schandene L, Goldman
M, Vanherweghem JL: Anaphylactoid reactions during hemo-dialysis on AN69 membranes in patients receiving ACE inhib-itors. Kidney Int 38: 982–984, 1990
90. Verresen L, Fink E, LemkeHD,VanrenterghemY: Bradykinin is amediator of anaphylactoid reactions during hemodialysis withAN69 membranes. Kidney Int 45: 1497–1503, 1994
91. Schulman G, Hakim R, Arias R, Silverberg M, Kaplan AP, ArbeitL: Bradykinin generation by dialysis membranes: Possible role
in anaphylactic reaction. J Am Soc Nephrol 3: 1563–1569,1993
92. Thomas M, Valette P, Mausset AL, Dejardin P: High molecularweight kininogen adsorption on hemodialysis membranes: In-fluence of pH and relationship with contact phase activation ofblood plasma. Influence of pre-treatment with poly(ethyl-eneimine). Int J Artif Organs 23: 20–26, 2000
93. Maheut H, Lacour F: Using AN69 ST membrane: A dialysiscentre experience. Nephrol Dial Transplant 16: 1519–1520,2001
94. Greinacher A: CLINICAL PRACTICE. Heparin-induced throm-bocytopenia. N Engl J Med 373: 252–261, 2015
95. TDOaPP Study: DOPPS Practice Monitor: Most Recent Trendsin US Hemodialysis Practice. Available at: http://www.dopps.org/dpm/DPMSlideBrowser.aspx. Accessed July 31, 2016
96. Chertow GM, Mason PD, Vaage-Nilsen O, Ahlmen J: On therelative safety of parenteral iron formulations. Nephrol DialTransplant 19: 1571–1575, 2004
97. ChertowGM,Mason PD, Vaage-NilsenO, Ahlmen J: Update onadverse drug events associated with parenteral iron. NephrolDial Transplant 21: 378–382, 2006
98. Wysowski DK, Swartz L, Borders-Hemphill BV, Goulding MR,Dormitzer C: Use of parenteral iron products and seriousanaphylactic-type reactions. Am J Hematol 85: 650–654, 2010
99. Macdougall IC, Bircher AJ, Eckardt KU, Obrador GT, PollockCA, Stenvinkel P, Swinkels DW, Wanner C, Weiss G, ChertowGM; Conference Participants: Iron management in chronickidney disease: Conclusions from a “Kidney Disease: Improv-ing Global Outcomes” (KDIGO) controversies conference.Kidney Int 89: 28–39, 2016
100. Auerbach M, Chaudhry M, Goldman H, Ballard H: Value ofmethylprednisolone in prevention of the arthralgia-myalgiasyndrome associated with the total dose infusion of irondextran: A double blind randomized trial. J Lab Clin Med 131:257–260, 1998
101. Cancado RD,Mu~nozM: Intravenous iron therapy:How far havewe come? Rev Bras Hematol Hemoter 33: 461–469, 2011
102. Auerbach M, Macdougall IC: Safety of intravenous iron for-mulations: Facts and folklore. Blood Transfus 12: 296–300,2014
103. Barton JC, Barton EH, Bertoli LF, Gothard CH, Sherrer JS: In-travenous iron dextran therapy in patients with iron deficiencyand normal renal function who failed to respond to or did nottolerate oral iron supplementation.Am JMed 109: 27–32, 2000
104. Kasparek T, Rodriguez OE: What medical directors need toknow about dialysis facility water management. Clin J Am SocNephrol 10: 1061–1071, 2015
105. Ward RA:Water processing for hemodialysis. Part I: A historicalperspective. Semin Dial 10: 26–31, 1997
106. Layman-Amato R, Curtis J, Payne GM: Water treatment for he-modialysis: An update. Nephrol Nurs J 40: 383–404, 2013
107. Centers for Medicare and Medicaid Services: Emergency pre-paredness for dialysis facilities. Available at: https://www.cms.gov/Medicare/End-Stage-Renal-Disease/ESRDNetworkOrgani-zations/downloads/emergencypreparednessforfacilities2.pdf.Accessed July 31, 2016
108. Fluck S, McKane W, Cairns T, Fairchild V, Lawrence A, Lee J,Murray D, PolpitiyeM, Palmer A, TaubeD: Chloramine-inducedhaemolysis presenting as erythropoietin resistance. NephrolDial Transplant 14: 1687–1691, 1999
109. Eaton JW, Kolpin CF, Swofford HS, Kjellstrand CM, Jacob HS:Chlorinated urbanwater: A cause of dialysis-induced hemolyticanemia. Science 181: 463–464, 1973
110. Davidovits M, Barak A, Cleper R, Krause I, Gamzo Z, EisensteinB: Methaemoglobinaemia and haemolysis associated with hy-drogen peroxide in a paediatric haemodialysis centre: Awarning note. Nephrol Dial Transplant 18: 2354–2358, 2003
111. de Torres JP, Strom JA, Jaber BL, Hendra KP: Hemodialysis-associated methemoglobinemia in acute renal failure. Am JKidney Dis 39: 1307–1309, 2002
112. de Oliveira RM, de los Santos CA, Antonello I, d’Avila D:Warning: An anemia outbreak due to chloramine exposure in aclean hemodialysis unit–an issue to be revisited. Ren Fail 31:81–83, 2009
12 Clinical Journal of the American Society of Nephrology
113. NewbiggingN, PeelW, Bell E, Isles C: Unexpected cyanosis in ahaemodialysis patient-did someone add hydrogen peroxide tothe dialysis water? NDT Plus 2: 158–160, 2009
114. Barker SJ, Tremper KK, Hyatt J: Effects of methemoglobinemiaon pulse oximetry and mixed venous oximetry. Anesthesiology70: 112–117, 1989
115. Guay J: Methemoglobinemia related to local anesthetics: Asummary of 242 episodes. Anesth Analg 108: 837–845, 2009
116. Hoenich NA: Disinfection of the hospital water supply: A hid-den risk to dialysis patients. Crit Care 13: 1007, 2009
117. Bek MJ, Laule S, Reichert-Junger C, Holtkamp R, Wiesner M,Keyl C: Methemoglobinemia in critically ill patients duringextended hemodialysis and simultaneous disinfection of thehospital water supply. Crit Care 13: R162, 2009
118. Arnow PM, Bland LA, Garcia-Houchins S, Fridkin S, Fellner SK:An outbreak of fatal fluoride intoxication in a long-term he-modialysis unit. Ann Intern Med 121: 339–344, 1994
119. Mohapatra M, Anand S, Mishra BK, Giles DE, Singh P: Reviewof fluoride removal from drinking water. J Environ Manage 91:67–77, 2009
120. Gill JR, Storck K, Kelly S: Fatal exsanguination from hemodialysisvascular access sites. Forensic Sci Med Pathol 8: 259–262, 2012
121. Georgiadis GS, Lazarides MK, Panagoutsos SA, Kantartzi KM,Lambidis CD, Staramos DN, Vargemezis VA: Surgical revisionof complicated false and true vascular access-related aneu-rysms. J Vasc Surg 47: 1284–1291, 2008
122. Pasklinsky G, Meisner RJ, Labropoulos N, Leon L, Gasparis AP,Landau D, Tassiopoulos AK, Pappas PJ: Management of trueaneurysms of hemodialysis access fistulas. J Vasc Surg 53:1291–1297, 2011
123. Saeed F, Kousar N, Sinnakirouchenan R, Ramalingam VS,Johnson PB, Holley JL: Blood loss through AV fistula: A casereport and literature review. Int J Nephrol 2011: 350870, 2011
124. Ball LK: Fatal vascular access hemorrhage: Reducing the odds.Nephrol Nurs J 40: 297–303, 2013
125. Kliger AS: Patient safety in the dialysis facility. Blood Purif 24:19–21, 2006
126. Thomas-Hawkins C, Flynn L, Clarke SP: Relationships betweenregistered nurse staffing, processes of nursing care, and nurse-reported patient outcomes in chronic hemodialysis units.Nephrol Nurs J 35: 123–130, 2008
127. Davis KK, Harris KG, Mahishi V, Bartholomew EG, Kenward K:Perceptions of culture of safety in hemodialysis centers.Nephrol Nurs J 43: 119–126, 2016
128. Centers for Medicare and Medicaid Services: Guidance forPerforming Root Cause Analysis with Performance Improve-ment projects, 2010. Available at: https://www.cms.gov/medicare/provider-enrollment-and-certification/qapi/downloads/guidanceforrca.pdf. Accessed July 31, 2016
129. Simon P, Potier J, Thebaud HE: Risk factors for acute hyper-sensitivity reactions in hemodialysis. Nephrologie 17:163–170, 1996
Published online ahead of print. Publication date available at www.cjasn.org.
This article contains supplemental material online at http://cjasn.asnjournals.org/lookup/suppl/doi:10.2215/CJN.05260516/-/DCSupplemental.
Clin J Am Soc Nephrol ▪: ccc–ccc, ▪▪▪, 2016 Hemodialysis Emergencies, Saha et al. 13
https://www.cms.gov/medicare/provider-enrollment-and-certification/qapi/downloads/guidanceforrca.pdf
https://www.cms.gov/medicare/provider-enrollment-and-certification/qapi/downloads/guidanceforrca.pdf


















