Diagnosis of Pneumothorax by Radiography and Ultrasonography … · CHEST Original Research...
24
DOI 10.1378/chest.10-2946 2011;140;859-866; Prepublished online May 5, 2011; Chest Wu Ding, Yuehong Shen, Jianxin Yang, Xiaojun He and Mao Zhang and Ultrasonography : A Meta-analysis Diagnosis of Pneumothorax by Radiography http://chestjournal.chestpubs.org/content/140/4/859.full.html services can be found online on the World Wide Web at: The online version of this article, along with updated information and 6.DC1.html http://chestjournal.chestpubs.org/content/suppl/2011/09/29/chest.10-294 Supplemental material related to this article is available at: ISSN:0012-3692 ) http://chestjournal.chestpubs.org/site/misc/reprints.xhtml ( written permission of the copyright holder. this article or PDF may be reproduced or distributed without the prior Dundee Road, Northbrook, IL 60062. All rights reserved. No part of Copyright2011by the American College of Chest Physicians, 3300 Physicians. It has been published monthly since 1935. is the official journal of the American College of Chest Chest © 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011 chestjournal.chestpubs.org Downloaded from
Transcript of Diagnosis of Pneumothorax by Radiography and Ultrasonography … · CHEST Original Research...

DOI 10.1378/chest.10-2946 2011;140;859-866; Prepublished online May 5, 2011;Chest
Wu Ding, Yuehong Shen, Jianxin Yang, Xiaojun He and Mao Zhang and Ultrasonography : A Meta-analysisDiagnosis of Pneumothorax by Radiography
http://chestjournal.chestpubs.org/content/140/4/859.full.html
services can be found online on the World Wide Web at: The online version of this article, along with updated information and
6.DC1.html http://chestjournal.chestpubs.org/content/suppl/2011/09/29/chest.10-294Supplemental material related to this article is available at:
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
written permission of the copyright holder.this article or PDF may be reproduced or distributed without the priorDundee Road, Northbrook, IL 60062. All rights reserved. No part of Copyright2011by the American College of Chest Physicians, 3300Physicians. It has been published monthly since 1935.
is the official journal of the American College of ChestChest
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

CHEST Original ResearchPULMONARY PROCEDURES
www.chestpubs.org CHEST / 140 / 4 / OCTOBER, 2011 859
Pneumothorax (PNX) frequently occurs in the ED and ICU, especially in patients with trauma and
those who are ventilated. Tension PNX is a very seri-ous condition that can potentially lead to cardiac arrest and requires early diagnosis and urgent treatment. A small or medium PNX generally is not life- threatening, but delays in diagnosis and treatment may result in progression of respiratory and circulatory compro-mise in unstable patients. The diagnosis of PNX gen-erally is confi rmed by chest radiography (CR), but CR has been demonstrated to be an insensitive and
unreliable examination. 1-4 Kirkpatrick and colleagues 5 evaluated the use of anterior-posterior supine CR with CT scanning for the diagnosis of PNX. In their study of 225 trauma patients, the sensitivity of CR
Objective: This study compares, by meta-analysis, the use of anterior-posterior chest radiography (CR) with transthoracic ultrasonography for the diagnosis of pneumothorax. Methods: English-language articles on the performance of CR and ultrasonography in the diag-nosis of a pneumothorax were selected. In eligible studies, data were recalculated, and the forest plots and summary receiver operating characteristic (sROC) curves were analyzed. Results: Pooled sensitivity and specifi city were 0.88 and 0.99, respectively, for ultrasonography, and 0.52 and 1.00, respectively, for CR. For ultrasonography performed by clinicians other than radiologists, pooled sensitivity and specifi city were 0.89 and 0.99, respectively. The sROC areas under the curve were compared, and no signifi cant differences between ultrasonography and CR were found. Meta-regression analysis implied that the operator is strongly associated with accu-racy (relative diagnostic OR, 0.21; 95% CI, 0.05-0.96; P 5 .0455). Conclusions: The meta-analysis indicated that bedside ultrasonography performed by clinicians had higher sensitivity and similar specifi city compared with CR in the diagnosis of pneumothorax, but the accuracy of ultrasonography in the diagnosis of pneumothorax depended on the skill of the operators. CHEST 2011; 140(4):859–866
Abbreviations: AUC 5 area under curve; CR 5 chest radiography; DOR 5 diagnostic OR; PNX 5 pneumothorax; QUADAS 5 the quality of diagnostic accuracy studies; sROC 5 summary receiver operating characteristic
Diagnosis of Pneumothorax by Radiography and Ultrasonography A Meta-analysis
Wu Ding , MM ; Yuehong Shen , MM ; Jianxin Yang , MM ; Xiaojun He , MM ; and Mao Zhang , MD
Manuscript received November 16, 2010; revision accepted March 13, 2011. Affi liations: From the Department of Emergency Medicine (Drs Ding, Yang, He, and Zhang), Second Affi liated Hospital, Zhejiang University, School of Medicine and Research Institute of Emergency Medicine, Zhejiang University; and Department of Burns (Dr Shen), Second Affi liated Hospital, Zhejiang University, Hangzhou, China. Funding/Support: The authors have reported to CHEST that no funding was received for this study .
For editorial comment see page 837
Correspondence to: Mao Zhang, MD, Department of Emergency Medicine, Second Affi liated Hospital, Zhejiang University, School of Medicine and Research Institute of Emergency Medicine, Zhejiang University, No 88, Jiefang Rd, Hangzhou, China; e-mail: [email protected] © 2011 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians ( http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.10-2946
was only 20.9%. CT scanning is considered the gold standard for detection of PNX. Sometimes, however, it is impractical to transfer a critically ill patient for
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

860 Original Research
standard that included clinical presentation and documentation of the escape or aspiration of intrapleural air at the time of drainage); (3) reporting of results in suffi cient detail to allow reconstruction of contingency tables of the raw data (ie, true-positive, true-negative, false-positive, and false-negative results); and (4) having diagnos-tic criteria for abnormal test results (eg, on ultrasonography, the disappearance of lung sliding; on CR, the appearance of air within the pleural space). Two of the authors (W. D. and Y. S.) indepen-dently reviewed the articles and ascertained the criteria for inclusion in the pooled data analysis, with disagreements resolved by discussion. Articles with the same authors were carefully inves-tigated, and some were excluded to avoid duplicate data analysis.
Quality of Study Reports
The quality of diagnostic accuracy studies (QUADAS) tool 18 (e-Table 1) was applied in our analysis to assess the quality of the studies included. The 14-item QUADAS tool assesses study design-related issues and the validity of the study results. Each item may be scored “yes” if reported, “no” if not reported, or “unclear” if no adequate information is available in the article to make an accurate judgment. We considered the quality items 1 (about the spectrum of patients), 4 (about the time period between reference standard and index test), 12 (whether the same clinical data were available when test results were interpreted as would be available when the test is used in practice), and 13 (whether uninterpretable/intermediate test results were reported) not relevant for our anal-ysis; thus, only the remaining 10 items were applied.
Data Extraction
In many of the studies included, hemithorax was used as the study unit for interpretation of the results instead of patient num-ber. Because the diagnosis of PNX in one lateral hemithorax has no relationship with the other side, and usually both hemitho-races must be examined to exclude PNX in one patient, we recon-structed some results as the number of hemithoraces. If there was no specifi c description, we recalculated one patient as two hemitho-races. For those postbiopsy, one biopsy specimen in one patient was counted as one hemithorax.
Data Analysis
We analyzed the forest plots and summary receiver operating characteristic (sROC) curves with freeware Meta-DiSc, version 1.4 software ( http://www.hrc.es/investigacion/metadisc_en.htm ; Ramon y Cajal Hospital; Madrid, Spain). The Spearman correla-tion coeffi cient between the logit of sensitivity and the logit of 1-specifi city was calculated to test the threshold/cutoff effect. Meta-DiSc allows users to test for heterogeneity (other than thresh-old effect) among various studies by statistical tests, including x 2 and Cochran Q . A low P value suggests the presence of heteroge-neity beyond what would be expected by chance alone. In addi-tion to these heterogeneity statistics, Meta-DiSc computes the inconsistency index ( I 2 ), which has been proposed as a measure to quantify the amount of heterogeneity.
Results
From the literature search, we retrieved 20 English-language articles eligible for analysis. The character-istics of the eligible articles are shown in Table 1 .
The details of the quality assessment are shown in e-Table 1. The eligible studies achieved most of the quality items. All 20 studies passed QUADAS items
CT scanning. The high doses of radiation in CT scan-ning also cannot be neglected.
Ultrasonography was fi rst used in the diagnosis of PNX in humans in 1987. 6 In recent years, some char-acteristic signs have been identifi ed for the diagnosis of PNX with ultrasonography, such as lung sliding, 7 comet tail artifacts, 8 the A line sign 8 and lung point. 9 Because lung ultrasonography can be performed easily and quickly at the bedside by intensivists, pneumolo-gists, and emergency physicians, it can be used in the diagnosis of PNX in ventilated patients, 7,10 in trauma patients, 11-13 and after lung biopsy. 14,15 The accuracy of ultrasonography in the detection of PNX varies across studies and is associated with the operator’s experi-ence. In the study by Sartori et al, 16 the sensitivity and specifi city were 100% for transthoracic ultra-sonography to detect PNX in 285 patients after lung biopsy. However, in another study, the sensitivity of ultrasonography was 58.9% and specifi city, 99.1%. Slater and colleagues 17 concluded that sometimes ultrasonography only could exclude but not confi -dently be used to diagnose PNX without the use of other imaging modalities.
Static and dynamic ultrasonography features of PNX have been identifi ed in a number of studies, but the contemporary diagnostic performance of ultra-sonography in the detection of PNX has not been well characterized. Should we use the thoracic sonographic examination in addition to the standard focused abdominal sonography for trauma examination in the ED, which is designated the extended focused abdominal sonography for trauma? 5 We undertook a meta-analysis of the published literature to compare the accuracy of ultrasonography and CR in the diag-nosis of PNX.
Materials and Methods
Study Design and Data Sources
A literature review and meta-analysis were conducted. Original articles published in English up to the end of October 2010 were searched in Medline, EMBASE, and the Cochrane Library. We used combinations of the following key words to identify all origi-nal articles in which ultrasonography, CR, or both were used in diagnosing PNX: (“ultrasound” or “sonography” or “ultrasonography” or “radiography” or “chest fi lm” or “chest radiograph”) and (“pneumothorax” or “aerothorax” or “aeropleura”) and (“sensitivity” and “specifi city”). New links displayed beside the abstracts were followed and retrieved. Bibliographies of retrieved articles were searched independently and checked for additional studies. No attempt was made to include unpublished data.
Study Selection
We selected articles for analysis that included the following criteria: (1) evaluation of the diagnostic performance of ultra-sonography, CR, or both for the detection of PNX; (2) comparison of imaging results with a gold standard (ie, CT scan or composite
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 140 / 4 / OCTOBER, 2011 861
Tabl
e 1—
Cha
ract
eris
tics
of
Eli
gib
le S
tudi
es
Us
CR
Stud
y O
rigi
nD
esig
nM
odal
ity a
Patie
nt T
ype
No.
a U
s O
pera
tor
Dia
gn C
rit b
TP
FP
FN
TN
TP
FP
FN
TN
Lic
hten
stei
n
and
Men
u 7 F
ranc
eN
RU
s, C
RC
ritic
ally
ill
148 c
NR
1 d 41
(100
)6
010
1 (9
4.4)
40 (9
3)0
341
(100
)
Hill
et a
l 19
Uni
ted
Stat
esR
etro
spec
tC
RTr
aum
a1,
684 c
107
(65.
6)0
561,
521
(100
)L
icht
enst
ein
et a
l 8 F
ranc
ePr
ospe
ctU
sC
ritic
ally
ill
184
NR
2 d,e,
f 41
(100
)5
013
8 (9
6.5)
Goo
dman
et a
l 20
Uni
ted
Kin
gdom
Pros
pect
CR
Post
biop
sy
416
(46.
2)0
728
(100
)L
icht
enst
ein
et a
l 9 F
ranc
ePr
ospe
ctU
s, C
RC
ritic
ally
ill
299
Inte
nsiv
ist
3 d,e,
f 66
(100
)11
022
2 (9
5.3)
60 (8
5.7)
010
58 (1
00)
Hol
mes
et a
l 21
Uni
ted
Stat
esPr
ospe
ctC
RTr
aum
a1,
076 c
13 (5
2)0
121,
051
(100
)R
owan
et a
l 22
Can
ada
Pros
pect
Us,
CR
Trau
ma
54 c
Rad
iolo
gist
2 f 11
(100
)1
042
(97.
7)4
(36.
4)0
743
(100
)K
irkp
atri
ck e
t al 5
Can
ada
NR
Us,
CR
Trau
ma
266
Trau
ma
surg
eon
2 f 21
(48.
8)3
2222
0 (9
8.7)
9 (2
0.9)
134
222
(99.
6)B
laiv
as e
t al 11
U
nite
d St
ates
Pros
pect
Us,
CR
Trau
ma
352 c
Em
erge
ncy
ph
ysic
ian
1 d 52
(98.
1)1
129
8 (9
9.7)
40 (7
5.5)
013
299
(100
)
Rei
ssig
and
Kro
egel
23
Ger
man
yPr
ospe
ctU
s, C
RPo
stbi
opsy
53
Pneu
mol
ogis
t3 d,
e,f
4 (1
00)
00
49 (1
00)
3 (7
5)0
149
(100
)
Chu
ng e
t al 24
K
orea
NR
Us,
CR
Post
biop
sy
97R
adio
logi
stN
R28
g (80
)3.
75 g
7 g 58
.25 g (
94)
16.5
g (47
.1)
3.75
g 18
.5 g
58.2
5 g (94
)B
all e
t al 1
Can
ada
Ret
rosp
ect
CR
Trau
ma
676 c
46 (4
4.7)
057
573
(100
)G
arof
alo
et a
l 25
Ital
yN
RU
s, C
RPo
stbi
opsy
18
4N
R3 f
44 (9
5.7)
02
138
(100
)19
(41.
3)0
2713
8 (1
00)
Zhan
g et
al 13
C
hina
Pros
pect
Us,
CR
Trau
ma
270 c
Em
erge
ncy
ph
ysic
ian
3 f 28
(87.
5)3
423
5 (9
8.7)
8 h (27
.6)
0 h 21
h 10
6 h (10
0)
Sold
ati e
t al 26
It
aly
Pros
pect
Us,
CR
Trau
ma
372 c
Em
erge
ncy
ph
ysic
ian
3 f 55
(98.
2)0
131
6 (1
00)
30 (5
3.6)
026
316
(100
)
Sart
ori e
t al 16
It
aly
Pros
pect
Us,
CR
Post
biop
sy
285
NR
3 f 8
(100
)0
027
7 (1
00)
7 (8
7.5)
01
277
(100
)So
ldat
i et a
l 12
Ital
yPr
ospe
ctU
s, C
RTr
aum
a21
8E
mer
genc
y
phys
icia
n3
23 (9
2)1
219
2 (9
9.5)
13 (5
2)0
1219
3 (1
00)
Bal
l et a
l 27
Uni
ted
Stat
esPr
ospe
ctC
RTr
aum
a81
0 c 26
(24.
3)0
8170
3 (1
00)
Bro
ok e
t al 28
Is
rael
Pros
pect
Us,
CR
Trau
ma
338
Rad
iolo
gist
2 f 20
(46.
5)3
2329
2 (9
9)7
(16.
3)0
3629
5 (1
00)
Gal
bois
et a
l 29
Fra
nce
Pros
pect
Us,
CR
Post
drai
nage
162
Inte
nsiv
ist
333
(100
)1
012
8 (9
9.2)
20 (6
0.6)
013
129
(100
)
Dat
a ar
e pr
esen
ted
as N
o. (%
), re
pres
entin
g th
e se
nsiti
vity
(TP)
and
the
spec
ifi ci
ty (T
N).
CR
5 ch
est r
adio
grap
hy; D
iagn
Cri
t 5 d
iagn
ostic
cri
teri
a; F
N 5
fals
e ne
gativ
e; F
P 5
fals
e po
sitiv
e; N
R 5
not
rep
orte
d;
Pros
pect
5 p
rosp
ectiv
e st
udy;
Ret
rosp
ect 5
retr
ospe
ctiv
e st
udy;
TN
5 tr
ue n
egat
ive;
TP
5 tr
ue p
ositi
ve; U
s 5 u
ltras
onog
raph
y. a I
n so
me
artic
les,
onl
y pa
rts
of th
e da
ta th
at fu
lfi lle
d th
e in
clus
ion
crite
ria
wer
e an
alyz
ed.
b Dia
gnos
tic c
rite
ria
of p
neum
otho
rax
by u
ltras
onog
raph
y co
ntai
ns th
e ab
senc
e of
lung
slid
ing
sign
, abs
ence
of c
omet
tail
sign
, and
the
pres
ence
of l
ung
poin
t. 1
5 th
e ab
senc
e of
lung
slid
ing
sign
; 2 5
the
abse
nce
of b
oth
lung
slid
ing
sign
and
com
et ta
il si
gn; 3
5 th
e ab
senc
e of
bot
h lu
ng s
lidin
g si
gn a
nd c
omet
tail
sign
and
the
seek
of l
ung
poin
t. c T
he d
ata
wer
e re
cons
truc
ted.
d Sel
ecte
d fo
r th
e su
bgro
up a
naly
ses:
dia
gnos
ing
pneu
mot
hora
x by
the
abse
nce
of lu
ng s
lidin
g si
gn.
e Sel
ecte
d fo
r th
e su
bgro
up a
naly
ses:
dia
gnos
ing
pneu
mot
hora
x by
the
abse
nce
of c
omet
tail
sign
. f S
elec
te fo
r th
e su
bgro
up a
naly
ses:
dia
gnos
ing
pneu
mot
hora
x by
the
abse
nce
of b
oth
lung
slid
ing
sign
and
com
et ta
il si
gn.
g The
dat
a ar
e th
e m
ean
valu
e of
the
four
obs
erve
rs’ n
umbe
rs.
h The
re w
as n
ot s
uffi c
ient
det
ail i
n th
e re
sults
to r
ecal
cula
te th
e da
ta p
er p
atie
nt a
s op
pose
d to
per
hem
ithor
ax; t
hus,
ori
gina
l dat
a of
the
artic
le w
ere
used
.
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

862 Original Research
Figure 1. Forest sensitivity, specifi city, diagnostic OR, and the sROC of ultrasonography. Inconsistency ( I 2 ) describes the percent-age of total variation across studies that is due to heterogeneity rather than to chance. I 2 can be readily calculated from basic results obtained from a typical meta-analysis as I 2 5 100% 3 ( Q 2 df )/ Q . Cochran Q is computed by summing the squared deviations of each study’s estimate from the overall meta-analytic estimate. The
t 2 statistic is a method for random-effects analysis, testing the heterogeneity other than threshold effect. AUC 5 area under the curve; df 5 degrees of freedom; sROC 5 summary receiver oper-ating characteristic.
2, 3, 8, and 9. The sample of 17 studies (85%) achieved verifi cation using the standard of diagnosis (item 5). QUADAS item 6 (patients received the same refer-ence standard regardless of the index test result) was reported in 75% of the studies. Item 7 (the refer-ence standard was independent of the index test) was achieved in 95% of the studies . Thirteen stud-ies (65%) reported on blinding in the results of the reference test (item 10), whereas six (30%) reported on blinding in the index test results (item 11). Of the nine studies withdrawn from the study, all had an explanation (item 14).
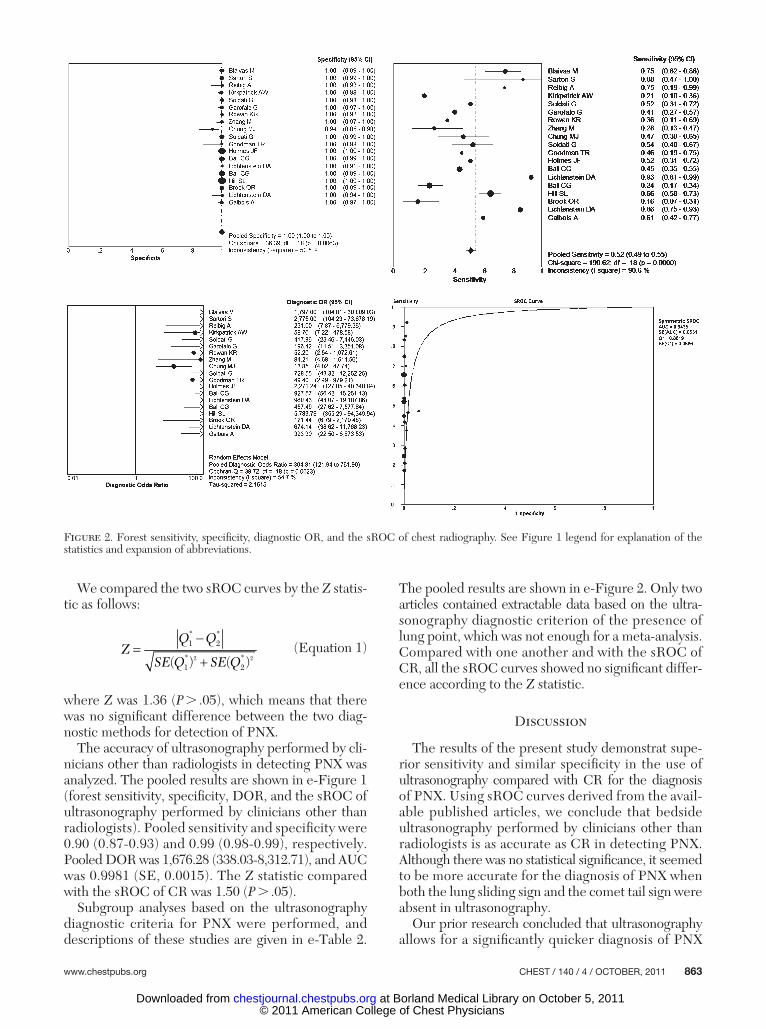
The pooled sensitivity, specifi city, diagnostic OR (DOR), and curves for detection of PNX with ultra-sonography and CR are shown in Figures 1 and 2 , respectively. Pooled sensitivity and specifi city were 0.88 (0.85-0.91) and 0.99 (0.98-0.99), respectively, for ultrasonography and 0.52 (0.49-0.55) and 1.00 (1.00-1.00), respectively, for CR. Pooled DOR was 993.05 (333.45-2,957.41), and sROC area under the curve (AUC) was 0.9961 (SE, 0.0023) for ultrasonog-raphy. For CR, the DOR was 304.81 (121.94-761.90), and sROC AUC, 0.9435 (SE, 0.0531).
The Spearman correlation coeffi cient between the log of sensitivity and log of 1-specifi city was 0.136 ( P 5 .629) for ultrasonography and 0.069 ( P 5 .778) for CR. The signifi cant x 2 P values, shown in the forest plots for each test, implied that there were causes of variations other than a cutoff effect. Possi-ble sources of heterogeneity across the studies were explored using meta-regression analysis with the fol-lowing covariates as predictor variables: study design (prospective vs retrospective), type of patient (eg, criti-cally ill, trauma), blinded test or not, ultrasonography diagnostic criteria, and operator. Results suggest that the operator is strongly associated with accuracy (relative DOR, 0.21; 95% CI, 0.05-0.96; P 5 .0455) ( Table 2 ). Subgroup analyses based on the ultra-sonography operator (clinicians other than radiolo-gists) were performed. In the x 2 test, pooled sensitivity was 79.93 ( P 5 .0000), and pooled specifi city was 26.71 ( P 5 .0004). The Cochran Q was 25.02 ( P 5 .0008) for DOR, which implied that heterogeneity resulted from factors other than the way a study was designed. We considered that the differences between the operators (their skill, experience, knowledge of chest ultrasonog raphy, etc) resulted in this heterogeneity, but there were no suffi cient details in the studies for us to make a classifi cation of the operators’ skills. The CR and ultrasonography modalities could be judged by their AUC.
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from
www.chestpubs.org CHEST / 140 / 4 / OCTOBER, 2011 863
We compared the two sROC curves by the Z statis-tic as follows:
2 2
1 2
1 2( ) ( )
Q QZ
SE Q SE Q
* *
* * (Equation 1)
where Z was 1.36 ( P . .05), which means that there was no signifi cant difference between the two diag-nostic methods for detection of PNX.
The accuracy of ultrasonography performed by cli-nicians other than radiologists in detecting PNX was analyzed. The pooled results are shown in e-Figure 1 (forest sensitivity, specifi city, DOR, and the sROC of ultrasonography performed by clinicians other than radiologists). Pooled sensitivity and specifi city were 0.90 (0.87-0.93) and 0.99 (0.98-0.99), respectively. Pooled DOR was 1,676.28 (338.03-8,312.71), and AUC was 0.9981 (SE, 0.0015). The Z statistic compared with the sROC of CR was 1.50 ( P . .05).
Subgroup analyses based on the ultrasonography diagnostic criteria for PNX were performed, and descriptions of these studies are given in e-Table 2.
The pooled results are shown in e-Figure 2. Only two articles contained extractable data based on the ultra-sonography diagnostic criterion of the presence of lung point, which was not enough for a meta-analysis. Compared with one another and with the sROC of CR, all the sROC curves showed no signifi cant differ-ence according to the Z statistic.
Discussion
The results of the present study demonstrat supe-rior sensitivity and similar specifi city in the use of ultrasonography compared with CR for the diagnosis of PNX. Using sROC curves derived from the avail-able published articles, we conclude that bedside ultrasonography performed by clinicians other than radiologists is as accurate as CR in detecting PNX. Although there was no statistical signifi cance, it seemed to be more accurate for the diagnosis of PNX when both the lung sliding sign and the comet tail sign were absent in ultrasonography.
Our prior research concluded that ultrasonography allows for a signifi cantly quicker diagnosis of PNX
Figure 2. Forest sensitivity, specifi city, diagnostic OR, and the sROC of chest radiography. See Figure 1 legend for explanation of the statistics and expansion of abbreviations.
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

864 Original Research
be made. The lung point is a specifi c sign that allows PNX to be confi rmed and the PNX volume to be determined, 30 but it is rarely found. The use of addi-tional ultrasonography signs, such as the seashore sign and power sliding, could improve the accuracy of the ultrasonography-based diagnosis of PNX, but there were not enough data for us to analyze these separately.
Despite its simplicity, security, and portability, ultrasonography has limitations in the diagnosis of PNX. It may not be appropriate for patients with sub cutaneous emphysema, adhesion of pleura, tho-racic dressings, pleural calcifi cations, or skin injury. Slater et al 17 concluded that patients with COPD commonly show signs on ultrasonography that mimic a PNX. Gillman et al 31 found the so-called “pseudo-lung point” sign by which the diagnosis of PNX should not be made and pockets of air could be missed on ultrasound. In a study by Chung and colleagues, 24
Table 2— Metaregression Analysis for Possible Sources of Heterogeneity
Variance Coeff Standard Error P Value RDOR 95% CI
Inverse variance weights 1 Cte 7.670 2.4070 .0129 … … S 0.322 0.2557 .2439 … … Design 1.091 1.0113 .3122 2.98 0.29-30.66 Patient 2 1.036 0.9913 .3265 0.35 0.04-3.49 Blind 1.332 1.6944 .4546 3.79 0.08-188.46 Diagnostic Criteria 0.168 0.7500 .8281 1.18 0.21-6.67 Operator 2 1.568 0.7330 .0648 0.21 0.04-1.13Inverse variance weights 2 Cte 8.070 1.3366 .0002 … … S 0.351 0.2276 .1578 … … Design 1.239 0.8480 .1779 3.45 0.51-23.52 Patient 2 1.190 0.8327 .1867 0.30 0.05-2.00 Blind 1.429 1.5401 .3777 4.17 0.13-136.03 Operator 2 1.613 0.6446 .0337 0.20 0.05-0.86Inverse variance weights 3 Cte 8.712 1.1164 .0000 … … S 0.253 0.1950 .2228 … … Design 1.549 0.7692 .0718 4.71 0.85-26.11 Patient 2 0.724 0.6473 .2895 0.48 0.11-2.05 Operator 2 1.836 0.5884 .0109 0.16 0.04-0.59Inverse variance weights 4 Cte 7.933 0.9033 .0000 … … S 0.182 0.2023 .3865 … … Design 1.286 0.8015 .1368 3.62 0.62-21.12 Operator 2 1.662 0.6079 .0194 0.19 0.05-0.72Inverse variance weights 5 Cte 8.705 0.8616 .0000 … … S 0.187 0.2310 .4330 … … Operator 2 1.550 0.6948 .0455 0.21 0.05-0.96Inverse variance weights 6 Cte 6.837 1.0165 .0000 … … S 0.295 0.2559 .2710 … … Design 0.874 1.0900 .4385 2.40 0.22-25.75
The RDOR (obtained by exponentiating the model coeffi cients) compared the DOR of studies of a given test that lacked a particular methodologic feature with those without the corresponding shortcomings in design. Coeff 5 coeffi cient; Cte 5 constant term in the equation; FPR 5 false-positive rate; RDOR 5 relative diagnostic OR; S 5 indicator of threshold (logit TPR 1 logit FPR); TPR 5 true-positive rate.
compared with CR and CT scanning. 13 The research of Sistrom and colleagues 15 showed that ultrasonog-raphy was not useful in estimating the volume of a PNX, but studies by Garofalo et al, 25 Soldati et al, 12 and ourselves 13 found the opposite. Although there was no statistical signifi cance, from our experience, we recommend that only if there is an absence of both the lung sliding sign and the comet tail sign can a diagnosis of PNX be made. The only part of normal lung visible on ultrasound is the pleura; the artifacts of normal pleura indicate the absence of a pneumothorax. Ultrasonography-based diag-nosis of PNX frequently is a “rule out” test. Thus, the presence of both the lung sliding sign and the comet tail sign could rule out PNX, but absence of the lung sliding sign or comet tail sign could not confi rm the existence of PNX. 30 In our experience, if one of these two signs is absent, the other sign must be carefully examined before a diagnosis of PNX can
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 140 / 4 / OCTOBER, 2011 865
Additional information: The e-Figures and e-Tables can be found in the Online Supplement at http://chestjournal.chestpubs.org/content/140/4/859/suppl/DC1.
References 1 . Ball CG , Kirkpatrick AW , Laupland KB , et al . Factors related
to the failure of radiographic recognition of occult posttrau-matic pneumothoraces . Am J Surg . 2005 ; 189 ( 5 ): 541 - 546 .
2 . Rankine JJ , Thomas AN , Fluechter D . Diagnosis of pneu-mothorax in critically ill adults . Postgrad Med J . 2000 ; 76 ( 897 ): 399 - 404 .
3 . Chiles C , Ravin CE . Radiographic recognition of pneumotho-rax in the intensive care unit . Crit Care Med . 1986 ; 14 ( 8 ): 677 - 680 .
4 . Tocino IM , Miller MH , Fairfax WR . Distribution of pneu-mothorax in the supine and semirecumbent critically ill adult . AJR Am J Roentgenol . 1985 ; 144 ( 5 ): 901 - 905 .
5 . Kirkpatrick AW , Sirois M , Laupland KB , et al . Hand-held tho-racic sonography for detecting post-traumatic pneumotho races: the Extended Focused Assessment with Sonography for Trauma (EFAST) . J Trauma . 2004 ; 57 ( 2 ): 288 - 295 .
6 . Wernecke K , Galanski M , Peters PE , Hansen J . Pneumothorax: evaluation by ultrasound—preliminary results . J Thorac Imaging . 1987 ; 2 ( 2 ): 76 - 78 .
7 . Lichtenstein DA , Menu Y . A bedside ultrasound sign ruling out pneumothorax in the critically ill. Lung sliding . Chest . 1995 ; 108 ( 5 ): 1345 - 1348 .
8 . Lichtenstein D , Mezière G , Biderman P , Gepner A . The comet-tail artifact: an ultrasound sign ruling out pneumotho-rax . Intensive Care Med . 1999 ; 25 ( 4 ): 383 - 388 .
9 . Lichtenstein D , Mezière G , Biderman P , Gepner A . The “lung point”: an ultrasound sign specifi c to pneumothorax . Intensive Care Med . 2000 ; 26 ( 10 ): 1434 - 1440 .
10 . Lichtenstein DA , Mezière G , Lascols N , et al . Ultrasound diagnosis of occult pneumothorax . Crit Care Med . 2005 ; 33 ( 6 ): 1231 - 1238 .
11 . Blaivas M , Lyon M , Duggal S . A prospective comparison of supine chest radiography and bedside ultrasound for the diagnosis of traumatic pneumothorax . Acad Emerg Med . 2005 ; 12 ( 9 ): 844 - 849 .
12 . Soldati G , Testa A , Sher S , Pignataro G , La Sala M , Silveri NG . Occult traumatic pneumothorax: diagnostic accuracy of lung ultrasonography in the emergency department . Chest . 2008 ; 133 ( 1 ): 204 - 211 .
13 . Zhang M , Liu ZH , Yang JX , et al . Rapid detection of pneu-mothorax by ultrasonography in patients with multiple trauma . Crit Care . 2006 ; 10 ( 4 ): R112 . Critical Care Web site. http://ccforum.com/content/10/4/R112 . Accessed August 20, 2009.
14 . Targhetta R , Bourgeois JM , Chavagneux R , Balmes P . Diagnosis of pneumothorax by ultrasound immediately after ultrasonically guided aspiration biopsy . Chest . 1992 ; 101 ( 3 ): 855 - 856 .
15 . Sistrom CL , Reiheld CT , Gay SB , Wallace KK . Detection and estimation of the volume of pneumothorax using real-time sonography: effi cacy determined by receiver operat-ing characteristic analysis . AJR Am J Roentgenol . 1996 ; 166 ( 2 ): 317 - 321 .
16 . Sartori S , Tombesi P , Trevisani L , Nielsen I , Tassinari D , Abbasciano V . Accuracy of transthoracic sonography in detection of pneumothorax after sonographically guided lung biopsy: prospective comparison with chest radiography . AJR Am J Roentgenol . 2007 ; 188 ( 1 ): 37 - 41 .
17 . Slater A , Goodwin M , Anderson KE , Gleeson FV . COPD can mimic the appearance of pneumothorax on thoracic ultrasound . Chest . 2006 ; 129 ( 3 ): 545 - 550 .
the accuracy of ultrasonography depended on the skill of the operator, and the diagnostic accuracy might be lower if ultrasonography was performed by an inexperienced clinician.
The present analysis has some limitations. We did not identify unpublished studies, and no attempt was made to include articles in other languages. From a traditional viewpoint, because air stops the progres-sion of the ultrasound beam, it might seem diffi cult to detect PNX with ultrasonography. Studies that concluded poor accuracy of ultrasonography or good accuracy of CR in the diagnosis of PNX might not have been published.
From the meta-analysis, the role of bedside ultra-sonography in detecting PNX is very promising. It would appear to be an attractive alternative to bed-side CR, especially in the emergency department, ICU, and other clinical situations where radiography is not available, such as in medical air transport and remote medical facilities. It has the potential to play a major role in the diagnosis of acute respiratory fail-ure, effectively acting as a visual stethoscope. 32
Conclusions
Clinician-performed ultrasonography is a reliable tool in the diagnosis of PNX. It has the advantage of portability, simplicity, rapidity, and higher sensitivity and similar specifi city compared with CR. Ultrasonog-raphy provides a useful adjunct for clinicians in treat-ing patients with multiple trauma or who are ventilated, but the accuracy of ultrasonography in the diagnosis of PNX depends on the skill of the operators.
Acknowledgments Author contributions: Dr Ding had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Dr Ding: contributed to the study design; data collection, analysis, and interpretation; preparation of the manuscript; and review and approval of the fi nal manuscript. Dr Shen: contributed to the data collection, analysis, and interpre-tation; preparation of the manuscript; and review and approval of the fi nal manuscript. Dr Yang: contributed to the preparation of the manuscript and review and approval of the fi nal manuscript. Dr He: contributed to the preparation of the manuscript and review and approval of the fi nal manuscript. Dr Zhang: contributed the study design, preparation of the manu-script, and review and approval of the fi nal manuscript. Financial/nonfi nancial disclosures: The authors have reported to CHEST that no potential confl icts of interest exist with any companies/organizations whose products or services may be dis-cussed in this article . Other contributions: This work was performed at the Department of Emergency Medicine, Second Affi liated Hospital, Zhejiang University, School of Medicine and Research Institute of Emergency Medicine, Zhejiang University, Hangzhou, China. We thank Dr Zhihai Liu, MD, for providing guidance on the study. We also thank all the relevant staff of the EDs for assisting in the imple-mentation of this study.
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

866 Original Research
25 . Garofalo G , Busso M , Perotto F , De Pascale A , Fava C . Ultra-sound diagnosis of pneumothorax . Radiol Med (Torino) . 2006 ; 111 ( 4 ): 516 - 525 .
26 . Soldati G , Testa A , Pignataro G , et al . The ultrasonographic deep sulcus sign in traumatic pneumothorax . Ultrasound Med Biol . 2006 ; 32 ( 8 ): 1157 - 1163 .
27 . Ball CG , Ranson K , Dente CJ , et al . Clinical predictors of occult pneumothoraces in severely injured blunt polytrauma patients: A prospective observational study . Injury . 2009 ; 40 ( 1 ): 44 - 47 .
28 . Brook OR , Beck-Razi N , Abadi S , et al . Sonographic detection of pneumothorax by radiology residents as part of extended focused assessment with sonography for trauma . J Ultrasound Med . 2009 ; 28 ( 6 ): 749 - 755 .
29 . Galbois A , Ait-Oufella H , Baudel JL , et al . Pleural ultrasound compared with chest radiographic detection of pneumotho-rax resolution after drainage . Chest . 2010 ; 138 ( 3 ): 648 - 655 .
30 . Lichtenstein DA . Ultrasound in the management of thoracic disease . Crit Care Med . 2007 ; 35 ( suppl 5 ): S250 - S261 .
31 . Gillman LM , Alkadi A , Kirkpatrick AW . The “pseudo-lung point” sign: all focal respiratory coupled alternating pleural patterns are not diagnostic of a pneumothorax . J Trauma . 2009 ; 67 ( 3 ): 672 - 673 .
32 . Lichtenstein D . Lung ultrasound in acute respiratory failure an introduction to the BLUE-protocol . Minerva Anestesiol . 2009 ; 75 ( 5 ): 313 - 317 .
18 . Whiting P , Rutjes AW , Reitsma JB , Bossuyt PM , Kleijnen J . The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews . BMC Med Res Methodol . 2003 ; 3 : 25 . BMC Web site. http://www.biomedcentral.com/1471-2288/3/25 . Accessed December 14, 2009.
19 . Hill SL , Edmisten T , Holtzman G , Wright A . The occult pneumothorax: an increasing diagnostic entity in trauma . Am Surg . 1999 ; 65 ( 3 ): 254 - 258 .
20 . Goodman TR , Traill ZC , Phillips AJ , Berger J , Gleeson FV . Ultrasound detection of pneumothorax . Clin Radiol . 1999 ; 54 ( 11 ): 736 - 739 .
21 . Holmes JF , Brant WE , Bogren HG , London KL , Kuppermann N . Prevalence and importance of pneumotho-races visualized on abdominal computed tomographic scan in children with blunt trauma . J Trauma . 2001 ; 50 ( 3 ): 516 - 520 .
22 . Rowan KR , Kirkpatrick AW , Liu D , Forkheim KE , Mayo JR , Nicolaou S . Traumatic pneumothorax detection with thoracic US: correlation with chest radiography and CT—initial expe-rience . Radiology . 2002 ; 225 ( 1 ): 210 - 214 .
23 . Reissig A , Kroegel C . Accuracy of transthoracic sonography in excluding post-interventional pneumothorax and hydro-pneumothorax. Comparison to chest radiography . Eur J Radiol . 2005 ; 53 ( 3 ): 463 - 470 .
24 . Chung MJ , Goo JM , Im JG , Cho JM , Cho SB , Kim SJ . Value of high-resolution ultrasound in detecting a pneumothorax . Eur Radiol . 2005 ; 15 ( 5 ): 930 - 935 .
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
1
Diagnosis of Pneumothorax by Radiography and Ultrasonography A Meta-analysis Wu Ding, MM, Yuehong Shen, MM, Jianxin Yang, MM, Xiaojun He,MM,and Mao Zhang,MD e‐Table1–Details of Quality Assessment by the QUADAS ToolStudy Ref Item2
Wereselectioncriteriaclearlydescribed?
Item3 Isthereferencestandardlikelytocorrectlyclassifythetargetcondition?
Item5Didthewholesamplereceiveverificationusingareferencestandardofdiagnosis?
Item6Didpatientsreceivethesamereferencestandardregardlessoftheindextestresult?
Item7Wasthereferencestandardindependentoftheindextest?
Item8Wastheexecutionoftheindextestdescribedinsufficientdetailtopermitreplicationofthetest?
Item9Wastheexecutionofthereferencestandarddescribedinsufficientdetailtopermititsreplication?
Item10Weretheindextestresultsinterpretedwithoutknowledgeoftheresultsofthereferencestandard?
Item11Werethereferencestandardresultsinterpretedwithoutknowledgeoftheresultsoftheindextest?
Item14Werewithdrawalsfromthestudyexplained?
LichtensteinDA(1995)
[7] Y Y Y Y Y Y Y Y U Y
HillSL(1999)
[24] Y Y Y Y Y Y Y U U *
LichtensteinDA(1999)
[8] Y Y Y Y Y Y Y Y U Y
GoodmanTR(1999)
[25] Y Y Y Y Y Y Y U Y *
LichtensteinDA(2000)
[9] Y Y Y Y Y Y Y Y U Y
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
2
HolmesJF(2001)
[26] Y Y Y Y Y Y Y Y Y *
RowanKR(2002)
[27] Y Y Y Y Y Y Y Y Y *
KirkpatrickAW(2004)
[5] Y Y Y Y Y Y Y U U Y
BlaivasM(2005)
[11] Y Y Y N Y Y Y Y Y Y
ReißigA(2005)
[28] Y Y N N N Y Y Y Y *
ChungMJ(2005)
[22] Y Y Y Y Y Y Y U U *
BallCG(2005)
[1] Y Y Y Y Y Y Y U U *
GarofaloG(2006)
[19] Y Y Y Y Y Y Y Y Y *
ZhangM(2006)
[13] Y Y Y N Y Y Y Y U Y
SoldatiG(2006)
[29] Y Y Y Y Y Y Y Y U Y
SartoriS(2007)
[16] Y Y N U Y Y Y Y N Y
SoldatiG(2008)
[12] Y Y Y Y Y Y Y N N Y
BallCG(2009)
[30] Y Y Y Y Y Y Y U U *
BrookOR(2009)
[31] Y Y Y Y Y Y Y Y U *
GalboisA(2010)
[32] Y Y N N Y Y Y Y U *
Y=Yes,N=No,U=Unclear,*=Donothavewithdrawals.
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
1
e-Figure 1.
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
2
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
3
e-Figure 1 . Forest sensi t ivi ty, speci f ic i ty, DOR and the sROC of Us performed by cl inicians
other than radiologists .
Df= the degrees of f reedom. Q= Cochran’s Q , AUC= area under the curve, SE= standard
error.Inconsistency (I 2 ) descr ibes the percentage of total variat ion across s tudies that is due to
heterogeneity rather than chance. I 2 can be readi ly calculated from basic results obtained
from a typical meta-analysis as I 2 = 100%× (Q − df)/Q . Cochran’s Q i s computed by summing
the squared deviat ions of each study’s est imate from the overal l meta-analyt ic est imate. The
Tau 2 s tat is t ic is a methods for random effects analysis , test ing the heterogeneity other than
threshold ef fect
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
1
e-Table 2A-Diagnosing Pneumothorax by the Absence of Lung-sliding Sign
Study
Ref
Design
US operator
Type of Patient TP FP FN TN
Lichtenstein DA (1995) [7] NR NR Critically Ill Patients 41 6 0 101
Lichtenstein DA (1999) [8] Prospective NR Critically Ill Patients 41 39 0 104
Lichtenstein DA (2000) [9] Prospective Intensivist Critically Ill Patients 66 51 0 182
Blaivas M (2005) [11] Prospective Emergency Physicians Trauma Patients 52 1 1 298
Reißig A (2005) [28] Prospective Pneumologists Post-biopsy Patients 4 0 0 49
e-Table 2B–Diagnosing Pneumothorax by the Absence of Comet-tail Sign
Study
Ref
Design
US operator
Type of Patient TP FP FN TN
Lichtenstein DA (1999) [8] Prospective NR Critically Ill Patients 41 56 0 87
Lichtenstein DA (2000) [9] Prospective Intensivist Critically Ill Patients 66 87 0 146
Reißig A (2005) [28] Prospective Pneumologist Post-biopsy Patients 4 2 0 47
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
2
e-Table 2C–Diagnosing Pneumothorax by the Absence of Both Lung-sliding Sign and Comet-tail Sign
Study
Ref
Design
US operator Type of Patient TP FP FN TN
Lichtenstein DA
(1999) [8] Prospective NR Critically Ill
Patients
41 5 0 138
Lichtenstein DA
(2000) [9] Prospective Intensivist Critically Ill
Patients
66 11 0 222
Rowan KR
(2002)
[27] Prospective Radiologists Traumatic
Patients
11 1 0 42
Kirkpatrick
AW(2004) [5] NR Trauma Surgeons Traumatic
Patients
21 3 22 220
Reißig A (2005) [28] Prospective Pneumologists Post-biopsy
Patients
4 0 0 49
Garofalo G
(2006)
[19] Prospective? NR Post-biopsy
Patients
44 0 2 138
Zhang M (2006) [13] Prospective Emergency
Physicians
Traumatic
Patients
28 3 4 235
Soldati G (2006) [29] Prospective Emergency
Physicians
Traumatic
Patients
55 0 1 316
Sartori S (2007) [16] Prospective NR Post-biopsy
Patients
8 0 0 277
Brook OR
(2009)
[31] Prospective Radiologists Traumatic
Patients
20 3 23 292
Galbois A
(2010)
[32] Prospective Intensivist Post-drainage
Patients
33 1 0 128
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
1
e-Figure 2A.
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
2
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
3
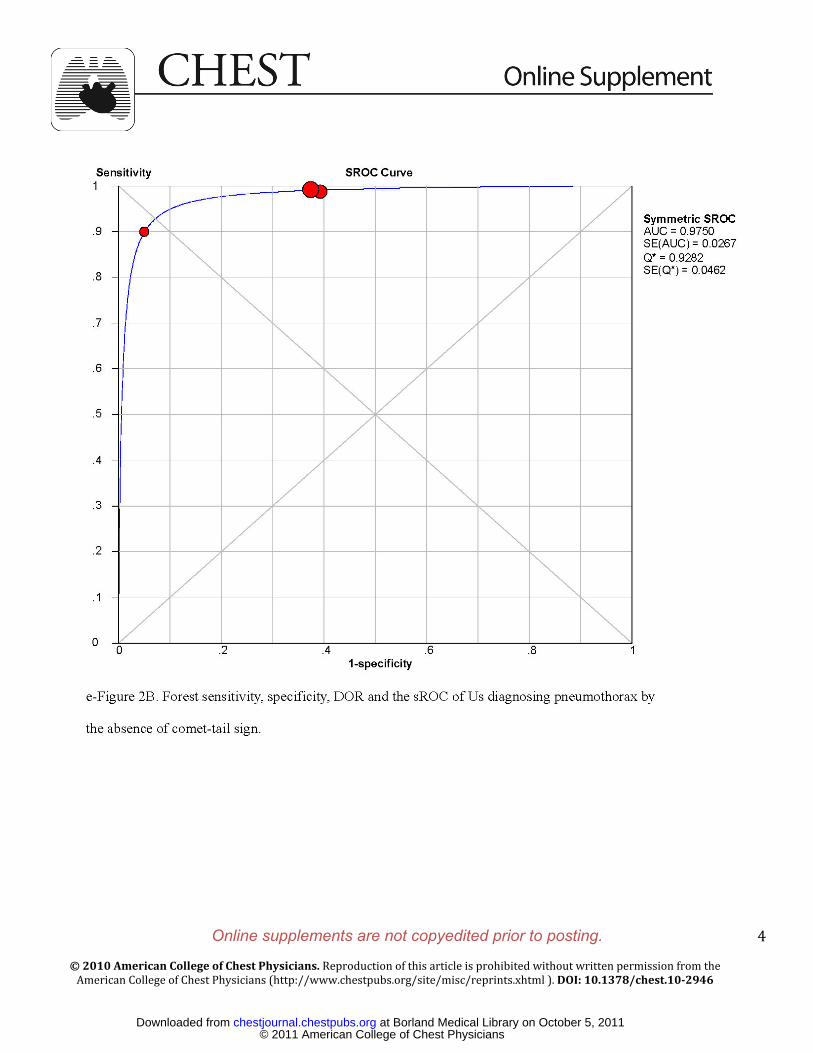
e-Figure 2B.
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from
Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
4
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
5
e-Figure 2C.
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
6
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

Online supplements are not copyedited prior to posting.
© 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.102946
7
e-Figure 2 . Forest resul ts of subgroup analyses based on the US diagnost ic cr i ter ia of PNX.
Df= the degrees of f reedom. Q= Cochran’s Q , AUC= area under the curve, SE= standard
error.Inconsistency (I 2 ) descr ibes the percentage of total variat ion across s tudies that is due to
heterogeneity rather than chance. I 2 can be readi ly calculated from basic results obtained
from a typical meta-analysis as I 2 = 100%× (Q − df)/Q . Cochran’s Q i s computed by summing
the squared deviat ions of each study’s est imate from the overal l meta-analyt ic est imate. The
Tau 2 s tat is t ic is a methods for random effects analysis , test ing the heterogeneity other than
threshold ef fect .
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from

DOI 10.1378/chest.10-2946; Prepublished online May 5, 2011; 2011;140; 859-866Chest
Wu Ding, Yuehong Shen, Jianxin Yang, Xiaojun He and Mao ZhangMeta-analysis
Diagnosis of Pneumothorax by Radiography and Ultrasonography : A
October 5, 2011This information is current as of
http://chestjournal.chestpubs.org/content/suppl/2011/09/29/chest.10-2946.DC1.html View e-supplements related to this article at:
Supplementary Material
http://chestjournal.chestpubs.org/content/140/4/859.full.htmlUpdated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/140/4/859.full.html#ref-list-1This article cites 30 articles, 11 of which can be accessed free at:
References
http://chestjournal.chestpubs.org/content/140/4/859.full.html#related-urlsThis article has been cited by 1 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlfound online at: Information about reproducing this article in parts (figures, tables) or in its entirety can bePermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
"Services" link to the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the
Citation Alerts
PowerPoint slide format. See any online figure for directions. articles can be downloaded for teaching purposes inCHESTFigures that appear in Images in PowerPoint format
© 2011 American College of Chest Physicians at Borland Medical Library on October 5, 2011chestjournal.chestpubs.orgDownloaded from