Diagnosis of Obstructive Jaundice
15
FROM THE UNIVERSITY OF CALIFORNIA, LOS ANGELES, SCHOOL OF MEDICINE Diagnosis of Obstructive Jaundice MODERATOR: JAMES S. CLARKE, M.D. DIScuSSANTS: PETER BARRETT, M.D., ERIC W. FONKALSRUD, M.D., JOHN N. JOHNSON, M.D., WILLIAM P. LONGMIRE, JR., M.D., MARTIN A. Pops, M.D., JOSEPH ROSCH, M.D., RICHARD J. STECKEL, M.D., AND MILO M. WEBBER, M.D. This is the edited transcription of an Interdepart- mental Clinical Case Conference arranged by the Department of Surgery, University of California, Los Angeles, School of Medicine. * The diagnosis of obstructive jaundice remains difficult yet vital, since operative decompression may relieve extrahepatic blockage, but opera- tion can only harm patients with intrahepatic block or parenchymal cell inflammation or necrosis. Three new diagnostic methods (liver scanning, angiography, and transiugular transhepatic cholangiography) are re- viewed, as is bilirubin metabolism, so important in the diagnosis of jaundice. Three clinical problems are discussed: extrahepatic obstruc- tion due to cancer of the pancreas, biliary atresia causing jaundice in the newborn, and the diffuse ductal obstruction known as sclerosing cholangitis. An accurate diagnosis can usually be made with standard diagnostic techniques, such as history, physical examination and biochemical tests, and, when appropriate, gastrointestinal x-ray studies, cholecystography and cholangiography, liver biopsy, observation of the patient's course, and the three new radiological approaches mentioned above. Extra- hepatic obstructive jaundice is an indication for surgical treatment, ex- cept perhaps in cases of sclerosing cholangitis. 44 MAY 1970 * 112 * 5
Transcript of Diagnosis of Obstructive Jaundice

FROM THE UNIVERSITY OF CALIFORNIA, LOS ANGELES, SCHOOL OF MEDICINE
Diagnosis of Obstructive JaundiceMODERATOR: JAMES S. CLARKE, M.D.
DIScuSSANTS: PETER BARRETT, M.D., ERIC W. FONKALSRUD, M.D., JOHN N. JOHNSON, M.D.,WILLIAM P. LONGMIRE, JR., M.D., MARTIN A. Pops, M.D., JOSEPH ROSCH, M.D.,
RICHARD J. STECKEL, M.D., AND MILO M. WEBBER, M.D.
This is the edited transcription of an Interdepart-mental Clinical Case Conference arranged by theDepartment of Surgery, University of California, LosAngeles, School of Medicine.
* The diagnosis of obstructive jaundice remains difficult yet vital, sinceoperative decompression may relieve extrahepatic blockage, but opera-tion can only harm patients with intrahepatic block or parenchymal cellinflammation or necrosis. Three new diagnostic methods (liver scanning,angiography, and transiugular transhepatic cholangiography) are re-viewed, as is bilirubin metabolism, so important in the diagnosis ofjaundice. Three clinical problems are discussed: extrahepatic obstruc-tion due to cancer of the pancreas, biliary atresia causing jaundice inthe newborn, and the diffuse ductal obstruction known as sclerosingcholangitis.
An accurate diagnosis can usually be made with standard diagnostictechniques, such as history, physical examination and biochemical tests,and, when appropriate, gastrointestinal x-ray studies, cholecystographyand cholangiography, liver biopsy, observation of the patient's course,and the three new radiological approaches mentioned above. Extra-hepatic obstructive jaundice is an indication for surgical treatment, ex-cept perhaps in cases of sclerosing cholangitis.
44 MAY 1970 * 112 * 5

DR. JOHN N. JOHNSON (Department of Medicine):The patient was a 24-year-old Caucasian malewelder who was admitted to UCLA on October 11,1966 with chief complaint of easy fatigability,weight loss, and some abdominal pain approxi-mately two and a half months before admission. Hehad been well until that time. These symptomswere progressive, and approximately two and a halfweeks before admission were accompanied bynausea, vomiting and the passing of light-coloredstools. About a week before admission the pa-tient's complexion became yellow and he noticeda lightening in the color of his stools and a deepyellow color in his urine.
His past history was relatively uncomplicated.On physical examination the positive findings in-cluded pronounced scleral icterus. The heart andlungs were within normal limits; the abdomen wassoft; the liver was palpable approximately 3.5 cmfrom the right costal margin and was very tender.No other masses or organomegaly were noted.Bowel sounds were normoactive. A stool wasnoted to be light-clay colored. There was noascites. With the exception of the jaundice, theremainder of physical examination was within nor-mal limits.
Leukocytes numbered 12,000 per cu mm, thehematocrit was 45, and hemoglobin was 15.4grams per ml. Other pertinent laboratory data in-cluded an alkaline phosphatase value of 21, bili-rubin of 7.4, SGOT of 240, SGPT of 272. Prothrom-bin time was 85 percent, heterophile 1:7, negativeANA. An upper gastrointestinal x-ray series sug-gested effacement of the second portion of theduodenum.The initial diagnosis was infectious hepatitis.
After an appropriate period of hospitalization, itbecame evident that the response was not of infec-tious hepatitis, but more suggestive of an obstruc-tive type of jaundice.On November 22, a transjugular cholangiogram
showed a dilated common bile duct. Because ofthis finding, an exploratory laparotomy was per-formed, and a hard tumor mass was found at thehead of the pancreas. The liver was noted to bestudded with metastatic lesions. Pathology reportverified adenocarcinoma of the pancreas.
Cholecystojejunostomy and jejunojejunostomywere performed, and the patient's postoperativecourse was uncomplicated. However, his enzymes
leprint reques to: Rment of Surgery, UCIA School of Medi.n. Center for the He Sciences. Los Angeles, Ca. 90024 (Dr.Clarkt).
continued to increase and bilirubin to rise. Hewas discharged in December of that year to anursing home.
DR. JAMES S. CLARKE (Department of Surgery):Moynihan said in 1926 that "no one living is in-fallible in the differential diagnosis of obstructivejaundice."8 Today, this statement stands as a ques-tion-is it still true, or only an interesting historicalrelic?By way of giving some perspective to the pre-
sentations which follow I wish to comment brieflyon the selectivity exercised in developing the pro-gram of this conference. Of the many ways of ap-proaching the diagnosis of a patient with jaundice,we have chosen only a few of the newer ones fordiscussion. While other methods, such as thehistory and physical examination, are still the cor-nerstone of accurate diagnosis, they cannot bereviewed in detail here. A history compatible withgallstones, cancer of the pancreas, a recent opera-tion on the biliary tract, alcoholism, recent bloodtransfusions, or ingestion of drugs known to causecholestatic jaundice would be of great help in thedifferential diagnosis of jaundice. Physical exam-ination is likewise of primary importance, espe-cially regarding the size of the liver and spleen, thepalpability of the gallbladder, and the stigmata ofcirrhosis of the liver. These aid in diagnosing andin the choice of proper tests for greater accuracyin the diagnosis.
Biochemical tests depend on the many syntheticand excretory functions of the liver and on therelease of enzymes that occurs during cell destruc-tion. Dr. Barrett will discuss those related to bili-rubin metabolism. Unfortunately, biochemicaltests are often confusing because of the mixtureof bile duct obstruction and damage to the livercells that is frequently the case in the jaundicedpatient.A liver biopsy specimen may be obtained at
operation under direct vision, or by the transcu-taneous route or a transjugular transhepatic route.The value and risks of obtaining specimens willnot be discussed today.
Radiological examination includes the well-established upper gastrointestinal series and oral orintravenous cholecystography and cholangiogra-phy. Because of current great interest in the newradiological methods, our presentations will coverliver scanning, angiography, and transjugular trans-hepatic cholangiography.
CALIFORNIA MEDICINE 45The Western Journal of Medicine

COOH
H2CH2
-CO2 +B6 c = o
.1N- ALA Synthetase CH2
NH2
-2H20
-ALA Dehydrose
8-AMINO-LE
COOH
CH2
lCN -.
C=O
C C2NH2
Chart 1.-The major steps in monopyrroleThe dots indicate the positions of the isotatoms when glycine-2.C1' is used as a precursoI
0F i
_ X
Uv'
1N-P.-N
-co
Hoe .-mothenyl oxygenoSe
X V P P M V
.;CH -J4 ;3 C Biliv rdin Reductose
H H H H
BILIRUBIN
Chart 2.-The major steps in hemoglobinIsotopic carbon atoms indicated by dots.
In addition to the case of cancer-dostructive jaundice presented by Dr. Joshall discuss two difficult problems in tobstructive jaundice: biliary atresia andcholangitis.
Bilirubin MetabolismIn Obstructive JaundiceDR. PETER BARRETT (Division of Gasogy): The presence of jaundice has attraiinterest for centuries, an interest rel
the fact that two of the four humours cGreek medicine were bile, yellow and blaour approach is a little more sophistiimany questions remain and one of the r
esting concerns the disposition of bilirustructive jaundice. It is well known tipresence of complete obstruction (whictient presented probably had) the serun
seldom exceeds 20 mg per 100 ml, yet it continuesto be produced at a normal or even increased rate.I will return to this aspect of bilirubin metabolismpresently.
In order to discuss bilirubin metabolism in thepresence of extrahepatic obstruction, it is first
EVULINIC ACID (8-ALA) necessary to review very briefly some aspects ofIOON normal bilirubin metabolism.
Charts 1 and 2 summarize the steps involvedin the production of bilirubin. Hemoglobin is the
7CH2 best known hemoprotein, but the heme moiety isNH2a critical portion of a variety of different enzymes,myoglobin, and the cytochromes. When these com-
biosynthesis. pounds are degraded, the iron is plucked from thetopic carbon cyclic molecule, and scission of the ring occurs at
the alpha bridge carbon position, resulting in therelease of carbon monoxide. It is worth empha-sizing that one mole of carbon monoxide is pro-duced for each mole of heme which is degraded,
Va&hwaglAin and the measurement of the rate of carbon mon-I-F... oxide production has proved to be a useful index
of heme turnover.m v Bilirubin is the major degradation product of
C-LIQ-ON heme in the body, and this pigment is rapidlyN NOm cleared from the serum by the liver. For example,f N lV if a tracer dose of CI4-bilirubin is given to a normalItC c person, less than 10 percent remains in the serum
P M at the end of four hours.1 Once the bilirubin entersBILIVERDIN the hepatocyte, it is probably bound to a specificmetabolism. protein during its journey to the endoplasmic re-ticulum, where conjugation of the molecule oc-
curs.4 Conjugated bilirubin is subsequently ex-creted into the bile canaliculus and then into the
erived ob- intestine.hnson, we The sequence of pathologic changes which oc-
hlerofie of cur in extrahepatic obstructive jaundice has beensclerosing well described. In a typical case, the initial changes
consist of cholestasis, inifitration of polymorpho-nuclear neutrophils and edema in the portal triads.With prolonged obstruction, the portal areas be-come enlarged with proliferating bile ducts, fibrous
,troenterol- tissue, inflammatory cells, and histiocytes. Bilected man's infarcts are pathognomonic of this condition, butilected by are relatively uncommon and therefore of little)f classical assistance in the differential diagnosis of jaundice.Lck. Today Using cytochemical techniques, an increasedcated, but amount of alkaline phosphatase has been demon-most inter- strated in the bile canaliculi shortly after the onsetibin in ob- of experimental obstruction, and the serum contentiat, in the of this enzyme begins to rise. It is of note thatch the pa- ligation of only one major hepatic bile duct willn bilirubin produce a rise in the serum alkaline phosphatase.
46 MAY 1970 * 112 * 5
ACTIVE SUCCINATE COOHH
CIHCOA-S-C = 0
GLYCINE HOOC-H2
NH2
COOH
COON CN2PORPHOBILINOGEN (PBG) IH2 CH2
c -c
C *CHCH2 N
HNH2

By contrast, in the presence of an otherwise normalliver, the same procedure will not lead to an eleva-tion of the serum bilirubin, for there is adequateclearance by the non-obstructed liver. This con-cept is essential for an understanding of the dis-parity between the serum alkaline phosphatase andbilirubin which may be observed in the presence offocal metastatic disease or in the occasional case ofblockage of the right or left hepatic duct by tumoror stone.'1The serum alkaline phosphatase determination
is very useful in the differential diagnosis of jaun-dice, but there is a moderate amount of overlapbetween parenchymal and obstructive diseasestates. Consequently, one cannot be dogmaticabout the presence or absence of obstruction onthe basis of this test alone.
In the presence of common bile duct obstruc-tion the intraductal pressure rises, and above alevel of 23 mm of mercury the production of bileceases and the serum bilirubin concentration beginsto rise. The precise pathway by which bilirubinreturns to the serum is still unsettled. It has beensuggested that conjugated bilirubin might makeits way from the bile canaliculus to the lymphaticsystem. However, experiments in dogs have shownthat, although there is a sharp rise in the thoracicduct bilirubin concentration immediately followingthe ligation of the common bile duct, this elevationpersists for only a few hours and then returns al-most to normal despite persistent obstruction.3This suggests that lymphatic outflow is not a sig-nificant pathway for the return of bilirubin fromthe liver to the serum. Two possibilities remain:The conjugated bilimbin may return to the serumdirectly from the hepatocyte or, alternatively, itmay be excreted into the bile canaliculus and thentravel between the cells back to the sinusoid. Thisissue must still be considered controversial.'4
Attempts have been made to differentiate paren-chymal from obstructive jaundice on the basis ofthe ratio of direct to indirect bilirubin (that is,conjugated to unconjugated bilimbin); however,the two fractions are generally found to rise to-gether in both types of jaundice and the ratiooffers no assistance in the differential diagnosis.2'The only situations in which this ratio is usefuloccur in patients with jaundice due to increasedbilirubin production, as in hemolytic anemia, or inpatients with metabolic defects such as Gilbert'ssyndrome, in which an elevation of the unconju-gated fraction of bilirubin predominates.
Bilirubinuria occurs in patients with obstructivejaundice. The excreted pigment is the conjugated,water-soluble fraction and is thought to be excretedchiefly by a process of glomerular ffltration.'9 How-ever, as the amount which can be measured in theurine in the presence of extrahepatic obstructionusually represents less than 20 percent of the dailybilirubin production, it is necessary to invokeother pathways and mechanisms for the disposalof the remaining 80 percent. This leaves us with aperplexing situation: In a patient with completeobstruction, the bilirubin cannot be delivered intothe gut, and only a small fraction can be found inthe urine.
Recent studies in mutant rats that cannot conju-gate and excrete bilirubin normally have shownthat, after the infusion of radioactive bilirubin,most of the radioactivity appears in the bile, butas unidentified water-soluble compounds; verylittle material can be identified as bilirubin itself.'5This demonstrates that alternate pathways of bili-rubin degradation are present, at least in thisspecies, and it is possible that similar mechanismsaccount for the disposition of bilirubin in the pres-ence of obstructive jaundice in man.
It has been proposed that alternate pathwaysfor bilirubin degradation occur in the endoplasmicreticulum, the site of many drug detoxification re-actions. In this regard it is of note that in jaun-diced patients the administration of glucocorticoids(compounds known to induce certain drug metab-olizing enzymes) usually results in a fall in theserum bilirubin concentration. The decrease in theserum bilirubin is most pronounced in patients withhepatitis, and this fact has been utilized as an aidin the differential diagnosis of parenchymal andobstructive jaundice. In practice, however, thereliability of this test is uncertain, and it is seldomused.
Further research will provide a better under-standing of the pathophysiology of obstructivejaundice and will allow improvement in the careof patients with this problem.
Angiography in Differential DiagnosisDRS. JOSEPH ROSCH* and RIcHARD J. STECKEL(Department of Radiology): Angiography is avaluable technique in the differential diagnosis ofobstructive jaundice.2 It gives detailed informationabout pathologic processes involving the liver and
*Visiting Professor, Docent of Charles University, Prague, Czecho-slovakia.
CALIFORNIA MEDICINE 47The Western Journal of Medicine

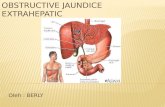
Figure 1.-Obstructive jaundice caused by pancreaticcarcinoma. Hepatic arteriography; tumor infiltration ofthe gastroduodenal artery (arrows) and small pancreaticbranches.
individual organs in the subhepatic area, and oftenresults in direct visualization of the lesion causingbiliary obstruction. It is useful in demonstratingtumors of the pancreas,7 gallbladder, bile ductsand liver (both primary and metastatic), andserves to differentiate them from non-neoplasticlesions. By determining the extent of a tumor andthe secondary involvement of surrounding organsand vessels, angiography also contributes greatlyto evaluation of tumor operability.
Selective studies of the celiac artery comple-mented by selective superior mesenteric studies, arethe basic examinations used.10 These proceduresresult in visualization of all organs in the upperabdomen and give a good impression of the portalcirculation in the venous phase of the angiogram.For better evaluation of individual organs and in-creased diagnostic accuracy, superselective arteri-ography should be performed in questionable cases.Direct hepatic artery injection gives a good surveyof the liver and gallbladder. Direct (superselec-tive) gastroduodenal, dorsal pancreatic or inferiorpancreaticoduodenal contrast injections are mostsuitable for diagnosis of disease in the pancreas orthe duodenal papilla.'2
Obstructive jaundice, whatever its cause, exhib-its certain typical angiographic changes in theliver as a result of the cholestasis: because of theenlarged intrahepatic bile ducts, the hepatic vascu-lar branches are narrowed and stretched, and theopacity of the liver in the capillary phase is irregu-lar, with ribbon-shaped negative defects.13 These
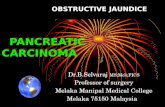
Figure 2.-Obstructive jaundice caused by carcinoma ofthe gallbladder spreading into the hepatic hilus. Superiormesenteric arteriography; arrows indicate tumor neovas-cularity occupying the entire gallbladder region and tu-mor infiltration of an aberrant hepatic artery.
liver changes, combined occasionally with faintvisualization of an enlarged gallbladder, are usuallythe only pathologic angiographic findings in caseswithout tumor. By contrast, biliary obstructioncaused by tumors exhibit certain additional angio-graphic changes, which are of crucial importance.
Pancreatic carcinoma (Figure 1) is diagnosedprincipally by tumor infiltration of vessels. Thesmaller pancreatic arteries are affected first. Theybecome irregular and narrowed with indented out-lines, and may even appear amputated. Later on,an enlarging tumor will also infiltrate the adjacentmajor vascular trunks-the gastroduodenal, hepat-ic and superior mesenteric arteries, and the portalvein. Tumor neovascularity is usually not striking,consisting only of very fine vessels, and neovascu-larity usually is absent in the scirrhous type ofcarcinoma. The infiltrative changes in the vesselsare of greatest importance in the differential diag-nosis: in inflammatory enlargement of the pan-creas, there is only displacement and mild deform-ity of the pancreatic branches or surroundingarterial trunks, but never signs of tumor invasionof the vessels.
Cancer of the duodenal papilla, particularly inits infiltrative form, also invades the nearbyarteries. Only the small branches of the pancre-aticoduodenal arcades are usually affected, ap-pearing irregularly narrowed or amputated. Super-selective injection techniques are essential forevaluating these small branches.
48 MAY 1970 * 112 * 5

Figure 4.-Obstructive jaundice caused by primary hep.Figure 3.-Obstructive jaundice caused by carcinoma of atoma. Celiac arteriography; extensive tumor neovascu-
the bile ducts in the liver hilus. Superior mesenteric ar- larity in the hepatic hilus (arrows); infiltration of rightteriography; tumor infiltration of the aberrant hepatic hepatic branch, displacement of enlarged left hepaticartery and its main branches in the hilus (arrows). branch.
Cancer of the gallbladder (Figure 2) exhibitstumor neovascularity as the main pathologic find-ing on angiography. The tumor vessels are irregu-lar and sometimes straightened, and in other casesare tortuous and may form "vascular lakes." Theyare supplied primarily by the cystic artery and itsbranches. In cases with tumor infiltration intosurrounding organs, the tumor vessels may acquireadditional supply from the intrahepatic, duodenalor right colic arteries. A large tumor usually in-vades the adjacent vascular trunks, and the hepaticartery and the portal vein are most often affected.
Cancer of the extrahepatic bile ducts (Figure 3)is diagnosed by tumor infiltration of adjacentarteries, with the proper hepatic artery and itsbifurcation usually affected. These arteries areirregularly narrowed and are often tortuous. Withhepatic spread of the tumor, similar infiltrativechanges are noted in the intrahepatic branchesclose to the liver hilus. There is also sometimesslight tumor neovascularity and tumor stainingaround the infiltrated vessels.
Primary hepatoma leading to obstructive jaun-dice (Figure 4) usually presents in a massive soli-tary form with perihilar localization. It is highlyvascular and supplied by an enlarged hepaticartery. The tumor vessels are large and tortuous,forming bizarre vascular networks. Arteriovenousshunts may also be present, with filling of irregularvascular lakes. There is prominent "tumor stain-ing," with the hepatoma becoming densely opaci-fied in the capillary phase. Portal vein thrombosis
is frequently visualized late in the angiogram, alongwith retrograde filling of a collateral venous circu-lation.
Liver metastases may have varying angiographicappearances, depending on their vascularity. Met-astases from hypernephromas, thyroid or islet-cellcarcinomas, hemangiosarcomas, and occasionallyeven colon carcinomas, may be highly vascular andmay present with many irregular tumor vessels inthe arterial phase, and with tumor "staining" ofthe metastatic deposits in the capillary phase ofhepatic angiography. The angiographic diagnosisof poorly vascular or avascular metastases is basedprincipally on deformity of the surrounding intra-hepatic branches, and on filling defects in the liverparenchyma visible in the capillary phase.
In summary, angiography aids preoperatively inthe differential diagnosis of obstructive jaundice ofneoplastic origin. It demonstrates the tumor aswell as its extent, and is of great assistance in evalu-ating potential operability.
Liver and Pancreatic Scanning
DR. MILO M. WEBBER (Department of Radiol-ogy): As far as definition of the images is con-cerned, what I have to show here is going to bea poor second to the radiographic procedures.However, the entire principle is relatively new and,I think, measured against radiography and the ad-vances we have seen in the past 60 or 70 yearsis equivalent to radiography back in the 1910s or
CALIFORNIA MEDICINE 49The Western Journal of Medicine

TABLE 1.-Liver Scanning AgentsAgent Tracer
Radiogold .Au198Rose bengal ..31Human serum albumin (microaggregates) ... I131Human serum albumin (microaggregates) .. Tc99mRadiotechnetium-sulfur colloid .Tc99mIndium colloid .In113
1920s. I think we have a long way to go, butthe future is there.Two procedures, liver scanning and pancreatic
scanning, were of special importance in the casepresented earlier. Before discussing them briefly,I would like to mention that liver scanning is in abroad sense a UCLA development, in that the firstpapers published on the subject were those of Dr.Stirrett and his associates back in the early 1950s.17The technique of scanning is different from the
technique of x-ray radiology in that the patienthimself, rather than an x-ray tube, is emitting thephotons. We attempt to make radioactive the partof the patient that we are interested in visualizing.In liver scanning we are limited to a few agents;Table 1 lists some of the most commonly used.Radiogold-198, in use throughout the world, islisted first. Rose bengal attracted originally a greatdeal of interest and is still used to some extent;in fact, it has a unique application (to be discussedlater) in cases of obstructive jaundice.The earliest liver scanning was done with serum
albumin tagged with radioiodine-131, not in aparticulate form at all, which collected to a minimalextent in areas of tumor activity.17 The type ofscan obtained in the early days was unsatisfactoryin comparison with what we are capable of obtain-ing today. Small particles of serum albumin,prepared by heating and shaking, when givenintravenously are concentrated by the reticulo-endothelial system throughout the liver and spleen.When the scan is made, the liver and the spleenare visualized. The albumin particles can be taggedwith radioiodine,18 as they are in most places, orwith radiotechnetium-99m, a relatively new tracerwhich permits the use of much more radioactivitywith much less radiation damage.
Radiotechnetium-99m-sulfur colloid is a rela-tively new agent which consists of small particlesof sulfur that include technetium sulfide; it is alsolocalized within the reticuloendothelial system ofthe liver.9 And, finally, Indium-l 13m, a new tracerwhich, like radiotechnetium-99m, has a very shorthalf-life (approximately 90 minutes), can be used
in large doses and yields many photons yet deliverslittle destructive irradiation to the patient.- Withthese two agents the scan images appear to havefine detail, and we see things that we were unableto see with the older types of scanning techniques.By the use of the techniques which involve up-
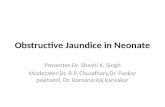
take of tracer within the reticuloendothelial systemwe see the collection of cells that represent theactive phagocytes of this system. Several patternscan be present in a normal person, and it is verydifficult to say that one pattern is normal and an-other abnormal. In fact, there are probably 15 orso usual patterns; of those most commonly seen,we have selected four, shown in Figure 5, whichrepresent what the liver scanning technique mightbe expected to show in a normal person.
Note that in some instances the left lobe is moreprominent than in others; in Figure SB it is almostseparate-in fact, in some cases an actual cleft canbe seen between the two lobes. The spleen showsup well at times, as in Figure SC, where it is muchmore apparent than in SA; the difference is due tothe agent used (technetium-sulfur suspension inSC, gold-198 in A). Another possible source ofconfusion is a Riedel's lobe extending from thetip of the right lobe.
In addition to the wide variation in the normalappearance of the liver, there is the problem ofloss of detail due to the patient's breathing duringthe many minutes needed to perform a scan. Thereis also a limit to the size of the lesion that can beseen in the liver scan: it must be at least 2 to 3 cmin diameter (depending upon its location withinthe liver) for it to be discerned with certainty. Ifthere are many small metastases scattered through-out the liver, we will be unable to see them. Onthe other hand, we can be sure to see large enoughmetastases, cysts or abscesses, even though wecannot really distinguish these processes from oneanother but see them all as areas of decreasedtracer uptake. If they are too small, however,we may easily miss them.
Figure 6 is a good example of what might beseen in a patient with a tumor at the head of thepancreas, as in the case here presented. Note alight area, rather large, extending up from the hilarregion of the liver, representing destruction offunctioning reticuloendothelial cells throughout theliver in the region of the porta hepatis.
Figure 7 also shows the possible result of atumor in the pancreas. The left lobe cannot beseen; its absence could represent that a tumor has
50 MAY 1970 * 112 * 5

Figure 5.-Commonly encountered scanning configurations of the normal liver and spleen. Note that the spleen isusually not seen clearly. A: Gold.198 scan. B, C, D: Technetium.sulfur suspension scans; note prominent left lobe in Band clearly visualized spleen in C.
involved and destroyed it, especially if the presenceof a mass in this region were confirmed radio-graphically or by physical examination.
Rose bengal can yield unique information forthe diagnosis of obstructive jaundice. Upon in-gestion, rose bengal is picked up by the paren-chymal cells of the liver, excreted in the gallblad-der, and then, if all is normal, passes out into thegastrointestinal tract to the duodenum. This ex-cretion sequence is prevented by an obstruction.The rose bengal will be picked up by the liver, ifthe liver still has this capacity, but then the agentwill gradually be released by the liver into thebloodstream, to be eventually excreted throughthe kidneys.
Figure 8 imlustrates the usefulness of the rosebengal liver scan. There is essentially no uptake oftechnetium-sulfur colloid (Figure 8A) in theKupfer cells of the liver. In the particular case
mustrated the liver function was so impaired be-cause of obstructive disease that most of the colloidis picked up in the spleen, the bone marrow, somein the liver, and some in the phagocytes of the lungs.Figure 8B shows a rose bengal scan in the samepatient. The tracer is picked up initially in theliver and in the gallbladder, which is seen clearly;much of the tracer is then passed into the gastro-intestinal tract, and a good deal of it can be seenin the bowel. This is a diseased liver, but there isno evidence of actual obstruction, although there isno question that the capacity to pick up a tracersuch as technetium-sulfur colloid is much impaired.
Pancreatic scanning, in practice since about1962, is based on the labeling of methionine (aprecursor to pancreatic enzymes) with radiose-lenium-75. An uptake in the pancreas (Figure 9)can be seen in about 50 percent of the cases giventhe labeled methionine. If an uptake looks rela-
CALIFORNIA MEDICINE 51The Western Journal of Medicine

Figure 6.-Liver scan (technetium-sulfur colloid) show-ing questionable area of decreased tracer uptake in thehilar region, representing destruction of functioning livertissue.
V
Figure 7.-Liver scan (technetium-sulfur colloid) show-ing destruction of the left lobe and of a portion of theright lobe due to malignancy.
tively normal in concentration and configuration(taking into account that we are in a very earlystage in the understanding of the variations of thepancreas in man) the chances are that the organ isnormal. On the other hand, failure to visualize itor the presence of areas of no uptake is a goodindication of some problem with the pancreas.This is not a widely accepted technique; I thinkit has promise for the future. Some investigatorshave claimed it to be as good as angiography ofthe pancreas, but that, of course, depends uponthe capability (and luck) of the person doing theangiography. Scanning is, however, nontraumaticand can be done with relative ease compared withcurrent angiographic techniques.
Figure 8.-A: Liver scan (technetium-sulfur colloid)showing no particulate uptake in the liver Kupfer cells,but only in the phagocytes of the spleen. B: Rose bengalscan on same patient, showing functioning of the paren-chymal cells and discharge of the tracer into the gastro-intestinal tract.
Transjugular TranshepaticCholangiography
DR. MARTIN A. Pops (Department of Medicine):To start with an oversimplification: in cases ofobstructive jaundice, the obstruction is surgicallyamenable where it resides exterior to the liver. Butthe clinical picture and laboratory tests can beidentical to those obtained in cases where it islocated within the liver, as it may be when cho-lestasis occurs secondary to infectious hepatitis oris caused by chlorpromazine or methyltestosterone.This has led in some instances to the mistaken per-formance of surgical operation in cases of choles-tatic viral hepatitis, with great risk to the patient.Thus it is important to determine whether patientswith apparent obstructive jaundice are surgicallytreatable.
52 MAY 1970 * 112 * 5

f V. -- #*,
Figure 9.-Scan of the pancreas done with Se'641abeledmethionine.
The oldest technique (and the one that we stillfavor when possible) is visualization of the biliarytree by intravenous cholangiography. This dependson hepatic conjugation and excretion of an iodideintroduced into the systemic circulation. Withjaundice, however, liver function may well be com-promised to the point where uptake and excretionof the opaque substance is suboptimal and visual-ization is not obtained. Direct cholangiographymay then be considered. Three techniques arenow in use.The first method is, of course, to operate on the
patient and do a cholangiogram at the operatingtable. Operative cholangiography has wide appli-cation, with obvious limitations. As our main topicis the preoperative evaluation of the jaundicedpatient, we shall proceed to consider the othertypes of direct cholangiography.
Transhepatic cholangiography involves the in-jection of a dye directly into the biliary tree afterlateral percutaneous puncture of the liver. Thecontrast agent fills the biliary system. In Figure 10,a gallstone totally occluding the common hepaticduct can be seen. The patient presented withjaundice and pruritus but no pain. The cholangio-gram proved that in her case jaundice was amen-able to surgical treatment.
Transhepatic cholangiography poses some prob-lems, and the reports dealing with this methodoften stress the need for immediate surgical inter-vention should obstruction be found. One recog-nized complication is leakage of bile back throughthe hepatic puncture site into the peritoneal cavity,with resultant bile peritonitis.The other reported complication of this pro-
Figure 10.-Transhepatic cholangiogram demonstratingtotal occlusion of the common hepatic duct by calculus(arrow).
cedure is hemoperitoneum. In performing trans-hepatic cholangiography the liver capsule is beingpunctured from the outside, so to speak. Havingcreated a situation where either bile or blood canextravasate into the peritoneal cavity, most personsexperienced with this method would like to be surethat the operating room is ready in case ductalobstruction is found.
At UCLA, Drs. W. N. Hanafee and M. Weinerhave recently devised a method of percutaneouscholangiography whereby the biliary system maybe opacified without the necessity of hepatic cap-sule puncture. They found that straight-line accessto the hepatic veins was obtainable by cannulationof the right internal jugular vein. A slightly curvedlong needle, adapted from trans-septal cardiaccatheterization, can be passed into the liver via itsvenous system and thence into the hepatic paren-chyma and finally into a biliary duct. The chancesof successful visualization are, of course, increasedif extrahepatic obstruction and secondary ductaldilatation are present. This technique may provide
CALIFORNIA MEDICINE 53The Western Journal of Medicine

an advantage over transhepatic cholangiographybecause the hepatic capsule is not punctured, there-by reducing or eliminating the risks of bile perito-nitis and hemoperitoneum. Our experience over thepast three years has tended to bear this out.
Figure 11 illustrates a transvenous (transjugu-lar) cholangiogram done by the technique just de-scribed. It shows a common duct stricture in aman who presented with jaundice six years aftercholecystectomy.
Figure 12 shows the radiographic studies in thecase presented by Dr. Johnson. The upper gastro-intestinal series shows some suggestive effacementand narrowing of the duodenal loop and someobliteration of the folds of the duodenum, sug-gesting a mass in the head of the pancreas. Thecholangiogram reveals an enormously dilated in-trahepatic ductal system. The arrow points to asharp cut-off which we have come to recognize ascharacteristic of tumor. As was noted earlier, onsurgical operation a fairly large carcinoma wasfound at the head of the pancreas.
Complications of transjugular cholangiographyhave included febrile episodes in several patientsfollowing the procedure and, in one case, frankGram-negative sepsis with death. The threat ofbacteremia and sepsis may be reduced by pre-procedural preparation of the patient with ap-propriate antibiotics such as ampicillin or tetra-cycline. It would seem wise to employ antibioticsin this way, especially if there is history of episodesof cholangitis.
In summary, then, we have a new technique ofdirect cholangiography which may be very usefulin diagnosis and planning of management for thepatient with apparent obstructive jaundice. Thecomplication of bile peritonitis and hemoperi-toneum can be avoided, thus eliminating the neces-sity for immediate operation. The risk of bac-teremia is probably the same or greater than withtranshepatic cholangiography.
Obstructive Jaundice in InfantsDR. ERic W. FONKALSRUD (Department of Sur-gery): Although carcinoma of the head of thepancreas and choledocholithiasis are unusual ininfants and children, jaundice is nonetheless acommon and serious problem in this age group.Of particular clinical importance (as in adults) isthe separation of obstructive from nonobstructivejaundice. Pathologic jaundice usually appearsduring the first 36 hours after birth. When jaundice
Figure 11.-Transjugular cholangiogram demonstratingsevere stricture of the common hepatic duct (arrow).
persists beyond the second week of life, the likeli-hood is greater that it is of the obstructive type.
Obstructive jaundice may be identified by meansof a combination of methods. The history andphysical examination may indicate the possibilityof the jaundice being caused by infection, isoim-munization, rubella, cystic fibrosis, or other non-obstructive conditions. The age at onset of thejaundice may be helpful in separating various typesof nonobstructive jaundice, as is shown in Table 2,in which conditions are classified by whether jaun-dice first appeared before or after the seventh dayof life. It seems that hepatitis in neonates is notan inflammatory condition similar to that in adults,but rather results from a congenital malformationof the hepatic cells.
Several conditions may produce nonobstructivejaundice in infants, with the onset of symptomsat various ages; these include conjugation de-ficiency, sepsis, concealed hemorrhage, galacto-semia, spherocytosis, drug toxicity, and hypoxia.Jaundice may occur during the first week or aslate as one or two months of age. Certain drugs
54 MAY 1970 * 112 * 5

Figure 12.-Left and center: Upper gastrointestinal series showing suggestive effacement of the duodenal loop. Right:Transjugular cholangiogram demonstrating pronounced dilatation of intrahepatic ductal system; cutoff by tumor aris-ing at the head of the pancreas is indicated by the arrow.
TABLE 2.-Caifying Characteristics ofNonobstructive Jaundice
Appears Under 7 Days of AgeIcterus neonatorumIsoimmunization (Rh and ABO)
Appears After 7 Days of AgeHepatitisToxoplasmosisCytomegalic inclusion diseaseCongenital syphilisFamilial nonhemolytic icterusCystic fibrosisPyloric stenosis
and sepsis may produce jaundice in an infantseveral months of age.
Various tests, such as the blood count, typing,Coombs' test, serology, urine galactose and exam-ination for cytomegalic inclusion bodies, may beof help in identifying these causes of nonobstruc-tive jaundice. Skull roentgenograms may identifytoxoplasmosis as the cause of jaundice. The find-ings that are most helpful in the recognition of ob-structive jaundice are acholic stools and biluria.An elevation in the direct serum bilirubin, ab-sence of urobilinogen in the urine, and absence of1131 rose bengal excretion into the intestine areconfirmatory evidence for the presence of ob-structive jaundice.
Several forms of obstructive jaundice may oc-cur in small infants. Congenital biliary atresia isthe most common type in neonates, the incidencebeing 1 in 2,000 to 3,000 births. This malforma-tion may be present in a variety of anatomical pat-terns, from atresia of the entire ductal system to
either extrahepatic or intrahepatic ductal atresia.In the most commonly encountered form of thisanomaly the extrahepatic ducts and gallbladderare atretic. In only a small number of infants doesthe intrahepatic ductal system empty into a dilatedproximal extrahepatic duct which communicateswith an atretic common bile duct. This is the onlyform of biliary atresia that may be corrected sur-gically by means of a choledochoenteric anasto-mosis, although the eventual prognosis dependsupon the degree of cirrhosis that develops beforeoperation.
Biliary hypoplasia is an uncommon malforma-tion in which either extrahepatic or intrahepaticbile ducts are narrowed in localized areas, pro-ducing partial ductal obstruction and jaundice,sometimes at an early age. This condition is be-lieved by many physicians to be a variant of giantcell hepatitis with narrow ducts. Many childrenwith biliary hypoplasia live until adolescence, al-though cirrhosis and portal hypertension usuallybecome evident and are progressive.
Choledochal cysts may become clinically symp-tomatic in infants as well as in children or adults.This congenital dilatation of the common bile ductproduces partial biliary obstruction with resultantintermittent jaundice, fever, pain, and usually anabdominal mass. Such cysts should be recognizedearly and drained internally before severe cirrhosisdevelops. This is one of the most readily cor-rectable forms of obstructive jaundice encounteredin pediatric patients.
Most children with biliary atresia die within
CALIFORNIA MEDICINE 55The Western Journal of Medicine

Figure 13.-Liver biopsy specimen from a 6-day-oldinfant with biliary atresia, showing moderate periportalfibrosis. This child subsequently underwent orthotopicliver homotransplantation and died with hepatic necrosisdue to arterial thrombosis three weeks after transplanta.tion.
the first two years of life (the average at 19months), regardless of the type of therapy. Oncethe diagnosis is suspected and substantiated by thelaboratory studies, a laparotomy with open liverbiopsy is recommended. If the liver is firm, nodularand dark green, characteristic of biliary cirrhosis,the incision is extended and a thorough explora-tion of the hepatoduodenal ligament is undertakenin search of a dilated proximal duct, either extra-hepatic or intrahepatic, which may be anastomosedto the small intestine. If the liver is soft, smoothand reddish brown, suggestive of hepatitis, a smallcatheter is placed into the gallbladder, and thewound is closed as quickly as possible to minimizethe duration of anesthesia. A cholecystogram andcholangiogram are then performed with the patientawake. A well-visualized complete extrahepaticductal system excludes the likelihood of biliaryatresia. If the ductal system is not visualized andbiopsy of a prepared speciman of liver is diagnosticof biliary atresia, laparotomy and extensive ex-ploration of the biliary ductal system are subse-quently performed. The importance of earlybiopsy and accurate identification of the occasionalsurgically correctable lesion early is emphasizedby the case illustrated in Figure 13, which showsmoderate cirrhosis in a specimen taken from aninfant with biliary atresia at six days of age.
Because of the almost uniformly poor prognosisof children with biliary atresia, several experi-
mental approaches have been studied to reducethe hyperbilirubinemia. The use of corticosteroidsand cholestyramine to reduce tbe serum bilirubin,which was mentioned earlier in discussion of themanagement of adults with jaundice, has been ofsome value in infants with jaundice. Clinical at-tempts to reduce the serum bilirubin which is inequilibrium with lymph by external draimage ofthoracic duct lymph have resulted in massiveprotein and fluid losses that make the procedureunfeasible for more than short periods. One childwith biliary atresia was kept alive for approxi-mately three months with the continued use ofthis treatment. At UCLA we have modified thisapproach by anastomosing the large lymphaticchannels in the hepatoduodenal ligament to anisolated loop of small intestine in five childrenwith biliary atresia, hoping to cause excretion ofexcess bilirubin and yet allow intestinal absorp-tion of proteins and fluid. Although these pro-cedures may lower the serum bilirubin temporarily,there is little evidence to suggest that the progres-sion of the biliary cirrhosis is altered, and deathusually occurs at approximately the same age aswhen the condition is untreated.
Perhaps the greatest hope for the future man-agement of children with biliary atresia rests inliver homotransplantation, which has become in-creasingly successful during the past several years,and has been used in three patients in this hospital.
Sclerosing CholangitisDR. WILLIAM P. LONGMIRE, JR. (Departmentof Surgery): Sclerosing cholangitis is, fortunately,a rare disease and no one has a wide experiencewith it from which to draw specific conclusions.One of the largest series reported in the literatureat this time concerns 42 cases collected by Warrenand his associates20 at the Lahey Clinic; the authorspoint out the almost uniformly unfavorable resultsof this disease.
There are two points that I would like to makein regard to this process, usually diagnosed at thetime of operation for jaundice of an obstructivetype in which a decided thickening and sclerosisof the wall of the common duct is found, a changethat occurs in the submucosal layer with pro-nounced periductal inflammatory reaction aboutit. The extent of the condition may vary from avery mild sort of process to one that almost com-pletely obliterates the lumen of the duct.
First, one must differentiate this process from
56 MAY 1970 * 112 * 5

a primary bile duct carcinoma, and this can pre-sent some major problems, primarily becausewhen performing a biopsy of the wall of thecommon duct the surgeon never likes to remove areally significant portion of the duct for fear ofcreating a permanent biliary fistula; hence thespecimen that the pathologist frequently receivesis not adequate to reach a definitive diagnosis.
Nevertheless, there are several points that canbe made with regard to this differential diagnosis.In the first place, when dealing with sclerosingcholedochitis, this is usually found to be a diffuseprocess that is apt to involve the entire extra-hepatic biliary system. Not infrequently, changeswill also be found inside the liver which are com-patible with a primary biliary cirrhosis, or whatwe refer to as cholangiolitic hepatitis (to be furtherdiscussed later or.) .On the other hand, in the case of carcinoma an
operative cholangiogram will demonstrate a morelocalized area of constriction, and above that pointof constriction a dilatation of the intrahepaticductal system or a dilatation of some portion ofthe extrahepatic system if the process is localizedto the lower portion of the duct. The point is thatthe sclerosing cholangitis is apt to be a diffuseprocess and the carcinoma apt to be localized,with dilatation above the point of obstruction inthe case of carcinoma, and no dilatation abovewith the cholangitis.As occasional exceptions to this, there are pa-
tients with a localized process, and these accountfor the rare case of sclerosing cholangitis in whichsome permanent cure may result.
In addition to this process alone, sclerosingcholangitis may also occur in combination withsome other systemic diseases. Not infrequently, itoccurs with ulcerative colitis, with retroperitonealfibrosis, with sclerosing fibrosis in other anatomicalsites; its relationship with these other diseases isnot clear.The other major point I would like to establish
is that this is probably the same process that weidentify as cholangiolitic hepatitis or primarybiliary cirrhosis, affecting in this case first or mostseverely the extrahepatic portion of the biliarytract.
Cholangiolitic hepatitis occurs typically in themost proximal portion of the biliary secretoryunit, while sclerosing cholangitis occurs more oftenin the major or extrahepatic ductal system. Theseprocesses frequently overlap. For example, in four
of the 28 cases of cholangiolitic hepatitis that wehave reported6 from this institution the patientwas thought to have a normal extrahepatic biliarytract at the time of the first exploration, but atsubsequent exploration, a year or more later, allfour were found to have extensive thickening andsclerosis of the extrahepatic system as the processseemed to extend. Turning the story around, practi-cally all the patients reported upon by Warren andhis associates20 eventually died of biliary cirrhosis,so that there was an extension of the process alongthis line.
In relation to this disease and ulcerative colitis,12 of the 42 patients in Warren's report hadulcerative colitis in association with the bile ductdisease. Two of these patients made an excellentrecovery, but ten did poorly, and five of them diedof the disease. In nine of these ten patients biliarycirrhosis developed.
Sherlock16 said that colectomy and antibioticsare of no benefit in the treatment of this particulartype of disease; we therefore feel that this is proba-bly not an infectious process but rather a systemicdisorder of some type, possibly related to an im-mune or an allergic phenomenon. It is associatedfrequently with other disease processes of similarnature. It follows a rather unfavorable course in amajority of instances, and the various treatmentsof prolonged biliary drainage are probably inef-fective in the majority of cases. Such treatment ispossibly contraindicated, inasmuch as is providesa means or an avenue for secondary infection toenter and extend up the biliary tract. The use ofsteroids may be of some value in the very earlycases if diagnosis can be made, and a short courseof therapy along this line may be tried.
DiscussionDR. CLARKE: We have a few minutes for ques-tions and discussion. First, I would like to saythat we are delighted to have Professor RichardWelbourn from Hammersmith with us this monthas a visiting professor in the Department of Sur-gery. I would like to invite Professor Welbourn tocomment if he wishes.
DR. RICHARD WELBOURN (Royal PostgraduateMedical School of London, Hammersmith, Eng-land): I have been fascinated to listen to thesepapers on the diagnosis of obstructive jaundice.The liver scanning interested me very much. It issomething which we, too, are doing; and, like you,
CALIFORNIA MEDICINE 57The Western Journal of Medicine

we are perhaps groping a bit in the early stages andnot knowing what particular appearances reallyindicate.The transjugular transhepatic cholangiography
I found particularly interesting. I had not heardabout this before. I shall certainly tell our radiol-ogists at home about this, and ask them if theycan help us, for it would be helpful in the type ofpatient on whom we now would have to do apuncture through the skin from the outside; andthese procedures, of course, have to be done on theway to the operating theater, and not all thesepatients may need operation.
DR. SHERMAN M. MELLINKOFF: I wonder if Icould ask Dr. Rosch if there is a characteristic ap-pearance of the angiogram in cholangiolitic hepa-titis or sclerosing cholangitis.
DR. ROsCH: There are changes secondary toperiportal infiltration, liver enlargement or liveratrophy, and cirrhosis; but there is no typicalangiographic appearance of sclerosing cholangitis.
DR. LONGMIRE: I would like to ask Dr. John-son why the bypass operation did not cure thejaundice in the case presented.
DR. JOHNSON: I could not tell from the chart. Ido not know.
DR. LONGMIRE: It seems to me that there mightbe two possibilities. One is that the gallbladder wasused in the decompression, and the tumor mayhave involved the junction between the cystic andthe common ducts, thereby obstructing the channelof decompression; such a tumor extension fre-quently occurs and is one of the reasons that acholecystojejunostomy is often not a satisfactoryoperation for decompression. The other explana-
tion would be that intrahepatic disease was soextensive that the patient's jaundice would not berelieved even though the extrahepatic ducts weredecompressed.
REFERENCES1. Barrett PVD, Berk PD, Menken M, et al: Bilirubin turnover
studies in normal and pathologic states using C"-bilirubin. Ann InternMed 68:355-377, 1968
2. Boijsen E, Reuter SR: Combined percutaneous transhepatic cho-langiography and angiography in the evaluation of obstructive jaundice.Amer J Roentgen 99:153-161, 1967
3. Bollman JL: Bile pigments in blood, lymph and bile, in thecourse of experimental bile stasis, In Brauer RW (Ed): Liver Function;A Symposium on Approaches to the Quantitative Descripton of LiverFunction. Washington DC, American Institute of Biological SciencesPublication No 4, 1958, pp 291-297
4. Gartner LM, Arias IM: Formation, transport, metabolism andexaetion of bilirubin. New Eng J Med 280:1339-1345, 1969
5. Goodwin DA, Stern HS, Wagner HN Jr, et al: A new radiophar-maceutical for liver scanning. Nucleonics 24(11):65, 68, 1966
6. Longmire WP Jr Joseph WL, Levin PM, et al: Diagnosis andtreatment of cholangioiidc hepatitis (primary biliary cirrhosis). AnnSurg 162:356-365. 1965
7. Lunderquist A: Angiography in carcinoma of the pancreas. ActaRadiol [Ther] (Stockholm) Suppl 235:1-143, 1965
8. Moyrnhan B: Abdominal Operations, Vol I (4th ed revised),Philadelphia, WB Saunders Company, 1926, p 528
9. Patton DD, Garcia EN, Webber MM: Simplified preparation oftechnetium 99m sulfide colloid for liver scanning. Amer JRoentgen97:880-885, 1966
10. Pollard JJ, Nebesar RA: Abdominal angiography. New Eng JMed 279:1093-1099, 1968
11. Posen S: Alkaline phosphatase. Ann Intern Med 67:183-203,1967
12. RUsch J: Roentgenology of the Spleen and Pancreas. Springfield,Charles C Thomas, Publisher, 1967
13. RBsch J, Grollman JH, Steckel RJ: Arteriography in the diag.nosis of gallbladder disease. Radiology 92:1485-1491, 1969
14. Rouiller C. J6Aquel A-M: Electron microscopy of the liver, InRouiller C (Ed): The Liver; Morphology, Biochemistry, Physiology;Vol I. New York, Academic Press, 1963, pp 195-264
15. Schmid R, Hammaker L: Metabolism and disposition of C14-bilirubin in congenital nonhemolytic jaundice. J Clin Invest 42:1720-1734, 1963
16. Sherlock S: Diseases of the Liver and Biliary System. (3rd edi-tion) Oxford, Blackwell Scientific Publications, 1963, p 353
17. Stirrett LA, Yuhl ET, Libby RL: The hepatic radioactivity sur-vey. Radiology 61 :930-934, 1953
18. Taplin GV, Johnson DE, Dore EK, et al: Suspensions ofradioalbumin aggregates for photoscanning the liver, spleen, lung andother organ. JNudMed5:259-275, 1964
19. Wallace DK, Owen EE: An evaluation of the mechanism ofbilirubin excretion by the human kidney. J Lab Clin Med 64:741-755,1964
20. Warren KW, Athanassiades S, Monge JI: Primary sclerosingcholangitis; a study of 42 cases. Amer J Surg 111:23-38, 1966
21. Zieve L, Hill E, Hanson M, et al: Normal and abnormal varia-tions and dinical significance of the one-minute and total serum bili-rubin determinations. J Lab ain Med 38:446469, 1951
58 MAY 1970 * 112 * 5