
Diagnosis & management of nonvariceal upper gastrointestinal hemorrhage bleeding (nvugih-nvugib) ...
138
DR. WALEED KH. S. MAHROUS GASTROENTEROLOGY AND HEPATOLOGY CONSULTANT حروس م الد دخ وليWaleed Khalid Mahrous DR. W ALEED KH. S. MAHROUS GASTROEN TEROLOGY AND HEPATOLOGY CONSULTANT Diagnosis & Management of Nonvariceal Upper Gastrointestinal Hemorrhage - Bleeding (NVUGIH-NVUGIB) Guideline 2015
-
Upload
waleed-mahrous -
Category
Health & Medicine
-
view
1.169 -
download
0
Transcript of Diagnosis & management of nonvariceal upper gastrointestinal hemorrhage bleeding (nvugih-nvugib) ...

DR. WALEED KH. S. MAHROUSGASTROENTEROLOGY AND HEPATOLOGY
CONSULTANT
محروس خالد Waleed Khalid Mahrous وليد
DR. WALEED KH. S. MAHROUSGASTROENTEROLOGY AND HEPATOLOGY
CONSULTANT
Diagnosis & Management of Nonvariceal Upper Gastrointestinal Hemorrhage - Bleeding (NVUGIH-NVUGIB)
Guideline 2015

NVIGIH
Summary of Guideline statements and recommendations
محروس خالد Waleed Khalid Mahrous وليد
محروس خالد Waleed Khalid Mahrous وليد
Main Recommendations
Initial patient evaluation and hemodynamic
resuscitation
محروس خالد Waleed Khalid Mahrous وليد
Q

NVUGIH - MR1 - 1
ESGE recommends immediate assessment of hemodynamic status in patients who present with acute upper gastrointestinal hemorrhage (UGIH), with prompt intravascular volume replacement initially using crystalloid fluids if hemodynamic instability exists .
(strong recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

• 46 years old male with no comorbid disease
presented to emergency department (ED) at 8 pm with history of one day melena suggestive of acute upper gastrointestinal bleeding , the patient vitally
stable and Hb7.4 after initial resuscitation , on call GI teams booked the patient for early mooring EGD as first case of the duty work endoscopy .
• Which Transfusion Strategy Is Best for Acute Upper Gastrointestinal Bleeding in This Case ?
A - Transfuse at lest 1 U PRBC to keep Hb 7-9 B - Restrict Blood transfusion until Hb <7

• 46 years old male with no comorbid disease
presented to emergency department (ED) at 8 pm with history of one day melena suggestive of acute upper gastrointestinal bleeding , the patient vitally
stable and Hb7.4 after initial resuscitation , on call GI teams booked the patient for early mooring EGD as first case of the duty work endoscopy .
• Which Transfusion Strategy Is Best for Acute Upper Gastrointestinal Bleeding in This Case ?
A - Transfuse at lest 1 U PRBC to keep Hb 7-9
B - Restrict Blood transfusion until Hb <7

ESGE recommends a restrictive red blood cell transfusion strategy that aims for a target hemoglobin between 7 g/dL and 9 g/dL.
A higher target hemoglobin should be considered in patients with significant co-morbidity (e. g., ischemic cardiovascular disease) .
(strong recommendation, moderate quality evidence).
NVUGIH – MR2 - 2
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

• 46 years old male with no comorbid disease
presented to emergency department (ED) at 8 pm with history of one day melena suggestive of acute upper gastrointestinal bleeding , the patient vitally
stable and Hb7.4 after initial resuscitation , on call GI teams booked the patient for early mooring EGD as first case of the duty work endoscopy .
• Which Transfusion Strategy Is Best for Acute Upper Gastrointestinal Bleeding in This Case ?
A - Transfuse at lest 1 U PRBC to keep Hb 7-9

SURVIVAL IMPROVED WITH LOWER TRANSFUSION THRESHOLD IN ACUTE UPPER
INTESTINAL BLEEDS
• 1. A restrictive transfusion strategy (transfusion threshold at Hb=7) led to better outcomes in patients with upper gastrointestinal (UGI) bleeding.
• 2. This strategy reduced the risk of further bleeding, the need for rescue therapy, and the complication rate, all while improving the survival rate.

WHICH TRANSFUSION STRATEGY IS BEST FOR ACUTE UPPER GASTROINTESTINAL BLEEDING?
NEJM - Transfusion Strategies for Acute Upper Gastrointestinal Bleeding 2013• In the restrictive-strategy group, the hemoglobin
threshold for transfusion was 7 g per deciliter, with a target range for the post-transfusion hemoglobin level of 7 to 9 g per deciliter.
• In the liberal-strategy group, the hemoglobin threshold for transfusion was 9 g per deciliter, with a target range for the post-transfusion hemoglobin level of 9 to 11 g per deciliter.

• In both groups, 1 unit of red cells was transfused initially; the hemoglobin level was assessed after the transfusion, and an additional unit was transfused if the hemoglobin level was below the threshold value.

• The transfusion protocol was applied until the patient's discharge from the hospital or death.• The protocol allowed for a transfusion to
be administered any time symptoms or signs related to anemia developed, massive bleeding occurred during follow-up, or surgical intervention was required.
• Hemoglobin levels were measured after admission and again every 8 hours during the first 2 days and every day thereafter. • Hemoglobin levels were also assessed
when further bleeding was suspected.

• All the patients underwent emergency gastroscopy within the first 6 hours. • When endoscopic examination disclosed a
nonvariceal lesion with active arterial bleeding, a nonbleeding visible vessel, or an adherent clot, patients underwent endoscopic therapy with injection of adrenaline plus multipolar electrocoagulation or application of endoscopic clips.

• Patients with peptic ulcer received a continuous intravenous infusion of omeprazole (80 mg per 10-hour period after an initial bolus of 80 mg) for the first 72 hours.
CRITICISMS• In both groups (restrictive-strategy group & iberal-strategy
group) 1 unit of red cells was transfused initially .
• 1 unit of pRBCs was transfused up front in both groups. Therefore, there was no true conservative transfusion group. The study suggests that a transfusion threshold of Hgb 7 is superior, but cannot definitively answer the question as all patients in the study received a transfusion.
• (So do not miss to give at least 1U of pRBC initially and don't ignore the patient until Hb <7 without single blood transfusion , if the patient collapsed during your on call you will go directly to the court)

• All patients underwent emergent EGD within mean 5 hours of admission; therefore, it is unknown whether results would be similar in patients who do not receive endoscopic therapy as quickly as the patients in this trial.
• Upper endoscopies within 6 hours is unrealistic outside of a research setting.
• Whereas gastroscopy in the first 6 hours after admission is feasible in clinical research trials, time delays of more than 6 hours may routinely occur in general clinical practice, particularly for patients with low Rockall scores similar to our case her .
• Theoretically, patients treated with a restrictive transfusion strategy may have worse outcomes in the setting of delayed endoscopy with ongoing bleeding.
CRITICISMS

Main Recommendations
Risk stratification
محروس خالد Waleed Khalid Mahrous وليد

Q

A

NVUGIH - 3
ESGE recommends the use of a validated risk stratification tool to stratify patients into high and low risk groups.
Risk stratification can aid clinical decision making regarding timing of endoscopy and hospital discharge.
(strong recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد
محروس خالد Waleed Khalid Mahrous وليد

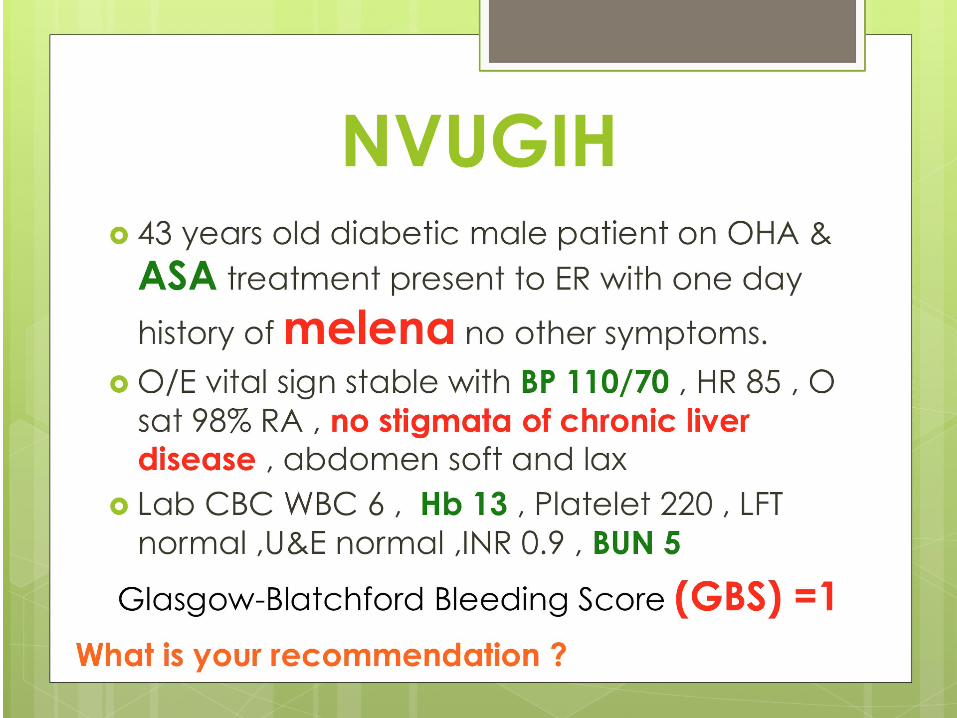
ESGE recommends the use of the Glasgow- Blatchford Score (GBS) for pre-endoscopy risk stratification.
Outpatients determined to be at very low risk, based upon a GBS score of 0 – 1, do not require early endoscopy nor hospital admission.
Discharged patients should be informed of the risk of recurrent bleeding and be advised to maintain contact with the discharging hospital
(strong recommendation, moderate quality evidence).
NVUGIH – MR3 - 4
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

Glasgow- Blatchford Score (GBS)

Main Recommendations
Pre-endoscopy management

NVUGIH – 5
For patients taking vitamin K antagonists (VKAs), ESGE recommends withholding the VKA and correcting coagulopathy while taking into account the patient's cardiovascular risk in consultation with a cardiologist.
In patients with hemodynamic instability, administration of vitamin K, supplemented with intravenous prothrombin complex concentrate (PCC) or fresh frozen plasma (FFP) if PCC is unavailable, is recommended .
(strong recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – 6
If the clinical situation allows, ESGE suggests an international normalized ratio (INR) value < 2.5 before performing endoscopy with or without endoscopic hemostasis .
(weak recommendation, moderate quality evidence).

NVUGIH – 7
ESGE recommends temporarily withholding new direct oral anticoagulants (DOACs) in patients with suspected acute NVUGIH in coordination/consultation with the local hematologist/cardiologist .
(strong recommendation, very low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – 8
For patients using antiplatelet agents, ESGE recommends the management algorithm detailed.
(strong recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015


Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding

Should we give a PPI IV before endoscopy in patients with
upper GI bleeding?
Yes No Probably Yes Probably No

Should we give a PPI IV before endoscopy in patients with
upper GI bleeding?
Yes (ESGE)No (SIGN, BSG , NICE)Probably Yes (ACG , ASGE)
Probably No

Interdiction
Experimental data suggest that acid suppression and increased pH are important in clot stabilisation and hence potentially in reducing rebleeding .

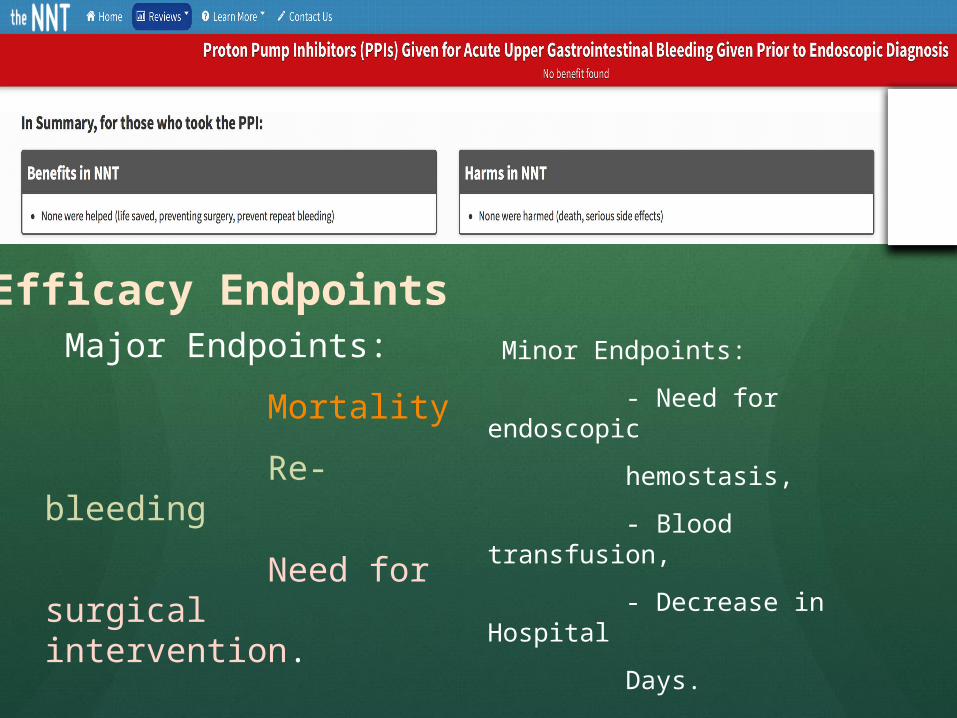
Major Endpoints: Mortality Re-bleeding Need for surgical intervention.
Minor Endpoints: - Need for endoscopic hemostasis, - Blood transfusion, - Decrease in Hospital Days.
Efficacy Endpoints

Also, a decrease in high risk stigmata on endoscopic evaluation may represent a clinically useful outcome if it reduced the need for hemostatic intervention.
A study showed that there was a 14% reduction in endoscopic hemostasis in the PPI group, with a number needed to treat to prevent one intervention of 7.
Efficacy Endpoints

Delaying definitive diagnosis and treatment,Direct cost to patient, Indirect cost (change in level of care, nursing
care, emergency department flow, etc.)Since 37-45% of undifferentiated upper GI
bleed is not from a peptic ulcer1,2 patients can be subject to unnecessary medications and cost.
Harm Endpoints:

Proton pump inhibitors Do not offer acid-suppression
drugs (proton pump inhibitors or H2-receptor antagonists) before endoscopy to patients with suspected non-variceal upper gastrointestinal bleeding.

Pre-endoscopic therapy with high-dose PPI may reduce the numbers of patients who require endoscopic therapy, but there is no evidence that it alters important clinical outcomes and there is insufficient evidence to support this practice.

A proton pump inhibitors should not be used prior to diagnosis by endoscopy in patients presenting with acute upper gastrointestinal bleeding.

PRE-ENDOSCOPIC MEDICAL THERAPY Proton pump inhibitor therapy
Recommendations.6. Pre-endoscopic intravenous proton pump inhibitor (PPI) (e.g., 80 mg bolus followed by 8 mg/h infusion) may be considered to decrease the proportion of patients who have higher risk stigmata of hemorrhage at endoscopy and who receive endoscopic therapy.

However, PPIs do not improve clinical outcomes such as further bleeding, surgery, or death (Conditional recommendation, high-quality evidence).

If endoscopy will be delayed or cannot be performed, intravenous PPI is recommended to reduce further bleeding (Conditional recommendation, moderate-quality evidence).

Before-procedure proton pump inhibitor therapy The role of proton pump inhibitor
(PPI) therapy in patients with suspected acute UGIB was systematically reviewed in a Cochrane meta-analysis that included 6 randomized controlled trials (RCT) published between 1992 and 2007.22

The analysis found that patients with nonvariceal UGIB administered intravenous PPI therapy prior to endoscopy did not experience any statistically significant differences in the outcomes of mortality, rebleeding, or progression to surgery compared with patients in the control group.

However, the analysis did show that before-procedure PPI therapy resulted in significantly reduced rates of high-risk stigmata identified on endoscopy (odds ratio [OR] 0.67; 95% confidence interval [CI], 0.54-0.84) and need for endoscopic therapy (OR 0.68; 95% CI, 0.50-0.93).

Therefore, intravenous PPI therapy is recommended for patients who are suspected of having acute UGIB.

Implications for Practice
PPI therapy is already widely initiated before endoscopy in patients with upper gastrointestinal bleeding.
The present analysis did not find significant improvement with PPI treatment for clinically important outcomes including rebleeding, surgery or mortality.

The reduced rate of serious endoscopic stigmata of bleeding found at endoscopy among patients given PPI therapy before endoscopy and the reduced requirement for endoscopic haemostatic treatment are of uncertain clinical significance.
However, PPI therapy may have a role if prompt endoscopy is not readily available.
Implications for Practice

Implications for Practice
Among such patients in whom PPI therapy is initiated before endoscopy, therapy can obviously be discontinued if endoscopy finds no evidence of bleeding or evidence of bleeding from an alternate source (for example, oesophageal or gastric varices).

ESGE recommends initiating high dose intravenous proton pump inhibitors (PPI), intravenous bolus followed by continuous infusion (80 mg then 8 mg/hour), in patients presenting with acute UGIH awaiting upper endoscopy.
However, PPI infusion should not delay the performance of early endoscopy
(strong recommendation, high quality evidence).
NVUGIH - MR4 - 9
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – 10
ESGE does not recommend the use of tranexamic acid in patients with NVUGIH .
(strong recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – 11
ESGE does not recommend the use of somatostatin, or its analogue octreotide, in patients with NVUGIH.
(strong recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

Erythromycin as a prokinetic treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding

YesNo Probably NoProbably Yes
Should we routinely administer erythromycin before
endoscopy in patients with upper GI bleeding?
Visibility during endoscopic hemostas
is

Should we routinely administer erythromycin before
endoscopy in patients with upper GI bleeding?
YesNo Probably NoProbably Yes

Answer : No , Probably not.
Among patients who present with UGIB, only a small percentage are likely to have a stomach full of blood necessitating gastric emptying before endoscopy.
Most guidelines do not recommend the routine use of erythromycin because there are no additional clinical benefits aside from improving endoscopic visibility and reducing the need for second-look EGDs.

Nevertheless, the use of erythromycin is recommended for patients who are suspected of having poor visibility due to the presence of large amounts of blood or clots in their stomachs.

However, there was no improvement in other clinical outcomes, such as duration of hospitalization, transfusion requirements, or surgery. Although the routine use of prokinetic agents is not recommended, use in patients with a high probability of having fresh blood or a clot in the stomach when undergoing endoscopy may result in a higher diagnostic yield. American Society for Gastrointestinal Endoscopy 2012

Promotility agents should not be used routinely before endoscopy to increase the diagnostic yield.
(Agree, 82. Grade: Moderate, 2b, “probably don’t do it”)
Although the use of preendoscopy promotility agents may improve diagnostic yield in selected patients with suspected blood in the stomach, they are not warranted for routine use in all patients who present with UGIB.
American College of Physicians 2010

Promotility agents are not promoted for routine use, but can be used to improve visualization in patients suspected to have large amounts of blood or food residue in the stomach.
2012 by the AGA Institute
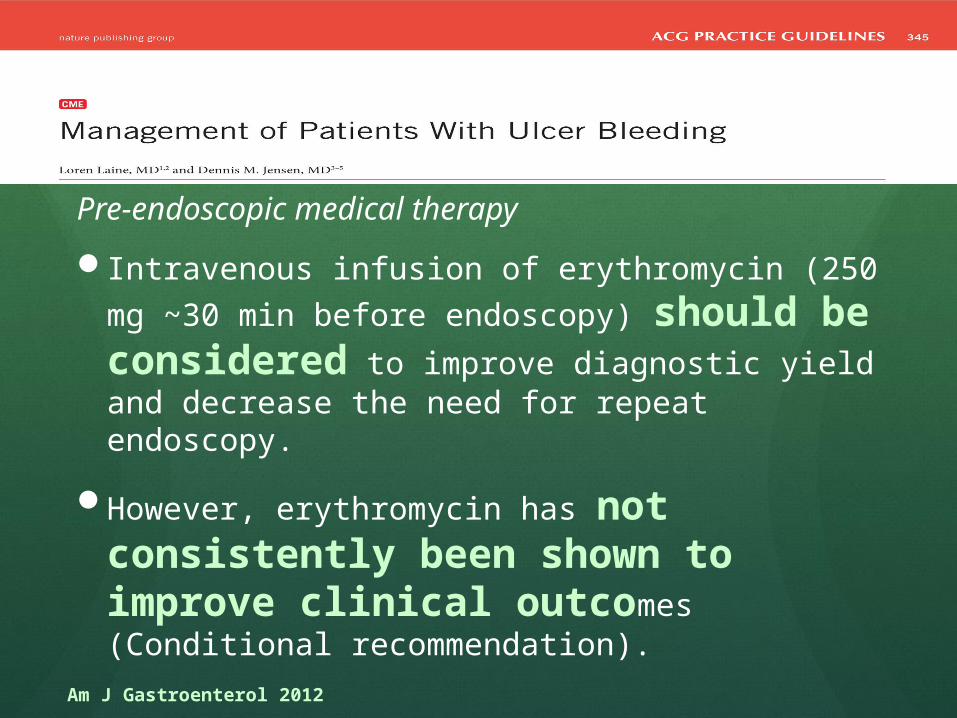
Pre-endoscopic medical therapy Intravenous infusion of erythromycin (250 mg
~30 min before endoscopy) should be considered to improve diagnostic yield and decrease the need for repeat endoscopy.
However, erythromycin has not consistently been shown to improve clinical outcomes (Conditional recommendation).
Am J Gastroenterol 2012

Visibility during endoscopic hemostasis
Based on the results of this study, we hope to develop guidelines on the use of prokinetics before emergency EGD that will assist in improving visibility during endoscopic hemostasis procedures.

NVUGIH – MR5 - 12
ESGE recommends intravenous erythromycin (single dose, 250 mg given 30 – 120 minutes prior to upper gastrointestinal [GI] endoscopy) in patients with clinically severe or ongoing active UGIH.
In selected patients, pre-endoscopic infusion of erythromycin significantly improves endoscopic visualization, reduces the need for second- look endoscopy, decreases the number of units of blood transfused, and reduces duration of hospital stay.
(strong recommendation, high quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

Is nasogastric tube lavage in patients with
acute upper GI bleeding indicated or
antiquated?
Why We Do What We Do: NG Tubes
محروس خالد Waleed Khalid Mahrous وليد

Nasogastric lavage (NGL) was once a standard initial procedure for all patients with acute gastrointestinal (GI) bleeding, but its use is now under debate.
Although some data suggest that patients with a bloody NGL are more likely to have severe bleeding, the test's presumed benefits — confirming an upper GI source of bleeding, clearing the stomach for better endoscopic visualization, and reducing the risk for aspiration — have not been tested.
Why We Do What We Do: NG Tubes
Nasogastric lavage (NGL) seems to be a logical procedure in the evaluation of patients with suspected upper GI bleeding, but does the evidence support the logic?
Most studies state that endoscopy should occur within 24 hours of presentation, but the optimal timing within the first 24 hours is unclear.
Rebleeding is the greatest predictor of mortality, and these patients benefit from aggressive, early endoscopic hemostatic therapy and/or surgery.
So what are the arguments for and against NGL?
To Lavage or Not to Lavage?

Is Nasogastric Lavage Beneficial for Acute
Gastrointestinal Bleeding ?
محروس خالد Waleed Khalid Mahrous وليد

Nasogastric (NG) lavage
Nasogastric (NG) lavage is an intuitively logical procedure for evaluation of stable patients without hematemesis suspected of having acute upper GI bleeding.
Indeed, a bloody NG aspirate is a good predictor of finding a high-risk lesion on upper endoscopy.
Patients undergoing NG lavage for suspected upper GI bleeding found that 45% of patients with a bloody aspirate had high-risk lesions on endoscopy versus 15% of those with only a clear or bilious aspirate.
Gastrointest Endosc. 2011 Nov;74(5):981-4. doi: 10.1016/j.gie.2011.07.007.

Nasogastric (NG) lavage
Prediction of high-risk lesions is important because it is those patients who have the worst outcomes and in whom early endoscopic therapy would be of most benefit.
Patients undergoing endoscopic therapy for high-risk lesions will be successfully managed in 80% to 90% of cases with control of active and prevention of further GI bleeding.
Rebleeding is the greatest predictor of poor outcomes including mortality.
Gastrointest Endosc. 2011 Nov;74(5):981-4. doi: 10.1016/j.gie.2011.07.007.

Nasogastric (NG) lavage
Studies suggests that finding red blood in the NG lavage predicts significant association with high-risk lesions and poor outcome vs. coffee ground.
So this studies demonstrates the benefit of a NG tube in risk stratification.
This studies suggests that early identification of high risk lesions by endoscopy decrease both re-bleeding rates and requirements for surgical intervention.

Nasogastric (NG) lavage
Studies shows that placement of a NGT tube, even with suggestion of a lower GI bleed can help localize the source of bleeding.
Studies shows that lavage through a NG tube can help clear the stomach contents of blood, allowing a more effective procedure during endoscopy.
From an endoscopic perspective, the fundus is typically the area of the stomach most likely to be obscured by retained blood in any bleeding scenario.

Nasogastric (NG) lavage
So, there is good evidence demonstrating that positive NG lavage tends to identify the presence of high-risk lesions found on subsequent endoscopy.
There is also evidence that endoscopic treatment of high-risk lesions decreases rebleeding and mortality.
So, if NG lavage identifies high-risk lesions, and endoscopic treatment of high-risk lesions decreases mortality, then patients who undergo NG lavage for their upper GI bleeds should have lower mortality, right?!!

Conclusion
ER feel that it is both helpful to the gastroenterologist, and more importantly, beneficial for the patient to place a NG tube and perform a lavage. The following should be reported to the gastroenterologist when you call them:Was bloody material spontaneously returned
upon placement of the tube.What was the color of the material that was
lavaged, bright blood red, maroon, clear with coffee-ground specks, etc.

Conclusion
If you find evidence of bleeding, please lavage at least 1-2 liters and tell us if the gastric contents clear of the bloody contents.
If there is no evidence of blood in the gastric contents, please continue to lavage until you see bilious material returned, so the gastroenterologist can be sure that you are sampling contents beyond the pylorus, a common site of peptic ulcers.

Can We Stop Placing NG Tubes?Can I simply avoid this procedure?
محروس خالد Waleed Khalid Mahrous وليد

Can We Stop Placing NG Tubes?
A negative NG lavage in an unstable patient with suspected Upper GI bleed does not rule out a bleed passed a closed pyloric sphincter, and a positive NG lavage (that clears) in a stable patient does not warrant more urgent EGD than an unstable patient.
It is common in my experience for GI docs to use lack of NGT, or negative or equivocal lavages as a way of delaying consultation till the morning.

Can We Stop Placing NG Tubes?
Incidentally, it is usually the least experienced member of the team (medical student) who is given the job of passing an NGT without adequate supervision.

Can We Stop Placing NG Tubes?
How good a diagnostic test is an NG tube? Usefulness and Validity of Diagnostic Nasogastric Aspiration in Patients Without Hematemesis.
Ann Emerg Med 2004 gives us a sensitivity of 42% and a specificity of 91%.
A 42% sensitivity stinks. So if you are doing this test to make sure that there is no upper GI bleeding, a negative test would not rule this out.
If you do get blood back then it is probably an upper GI bleed.
So the next obvious question is how does this change management?

One of the worst-tolerated procedures in Emergency Medicine - placement of the NG tube.
Unfortunately, when ER call GI fellow on-call for any upper GI bleeding, the first question is invariably - what did the NG lavage show?
محروس خالد Waleed Khalid Mahrous وليد

Patients who underwent NGL were more likely to have an endoscopy and to receive it sooner than other patients.
Lavage did not affect mortality, length of hospital stay, or the need for transfusions or surgery. Bloody aspirates were associated with high-risk lesions at endoscopy.
Conclude that NGL is associated with receiving early endoscopy and might be useful in triage but does not affect clinical outcomes.
محروس خالد Waleed Khalid Mahrous وليد

The procedure increased the likelihood of early endoscopy but not better patient outcomes, such as lower mortality.
Nasogastric tube insertion can be a traumatic experience to the patient. May traumatize the esophageal varices , mucosa and the gastric mucosa .
The trauma marks can act as confounders to the endoscopist

Comparison of patient and practitioner assessments of pain from commonly performed emergency department
procedures.
1. It is painful What they did:Prospective, observational study1,171 procedures, from the 15 most common procedures
performed in the EDPatients recorded a pain scoreWhat they found:The most painful procedure according to
patients was NG tube placement.NG tube placement was more painful than intubation,
abscess drainage, fracture reduction, and urethral catheterization.
Ann Emerg Med. 1999 Jun;33(6):652-8.

So, it has been rated the most painful procedure we perform on a patient.
There are many ways to lesson this pain like local or systemic analgesia but it still stinks for the patient.
The gagging and spitting are not great for the provider who is trying to keep the fragile patient doctor bond intact.
Comparison of patient and practitioner assessments of pain from commonly performed emergency department
procedures.

Conclusion
The most painful procedure for ED patients is NG tube placement.
Ann Emerg Med. 1999 Jun;33(6):652-8.

Erythromycin infusion or gastric lavage for upper gastrointestinal bleeding: a multicenter randomized
controlled trial.
2. NGL IS NOT the only way to get good visualization during endoscopy What they did:Prospective, randomized, multicenter study6 EDs, 253 patients with an upper GI bleed (UGIB)IV erythromycin (84 pts) vs NGT without erythromycin (85
pts) vs NGT with erythromycin (84 pts) for visualization during endoscopy
What they found:No difference in visualization between groupsNo difference in duration of endoscopic procedure,
rebleeding, need for 2nd endoscopy, number of transfused PRBCs, or mortality at 2, 7, and 30 days
Ann Emerg Med. 2011 Jun;57(6):582-9. doi: 10.1016/j.annemergmed.2011.01.001. Epub 2011 Feb 17.

Conclusion
In acute UGIB, administration of IV erythromycin provides satisfactory endoscopic visualization without need for a NGL.
Ann Emerg Med. 2011 Jun;57(6):582-9. doi: 10.1016/j.annemergmed.2011.01.001. Epub 2011 Feb 17.

Impact of nasogastric lavage on outcomes in acute GI bleeding
3. NGL DOES NOT improve mortality, length of stay, or transfusion requirements What they did:Retrospective analysis632 patients with GI bleeding to evaluate 30-day
mortality, mean hospital length of stay (LOS), and transfusion requirements.
What they found:No statistical difference in 30 day mortality, mean
LOS, or transfusion requirements.NGL was associated with earlier time to endoscopy.
Conclusion
NGL is associated with earlier performance of endoscopy, but NO difference in clinical outcomes.

The placement of a nasogastric tube should be considered in select patients who have suspected active UGIB.
The presence of bright red blood in a gastric aspirate can be useful in identifying patients with high-risk lesions, but is not as useful if coffee ground material or other findings are present without red blood.
It should be noted that the absence of blood in a gastric aspirate does not exclude the presence of active UGIB, because approximately 15% of patients with active bleeding can have a negative result for nasogastric lavage.
Because of these limitations, and the potential patient discomfort, use of a nasogastric tube remains controversial.
GASTROINTESTINAL ENDOSCOPY Volume 75, No. 6 : 2012

Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – ESGE GL 2015
In distinguishing upper from lower GI bleeding, nasogastric aspiration has low sensitivity 44% , high specificity 95% .
In identifying severe UGIH, its sensitivity and specificity are 77 % and 76%, respectively .
Clinical signs and laboratory findings (e.g., hemodynamic shock and hemoglobin < 8 g/dL) compared to nasogastric aspiration/lavage, had similar ability to identify severe UGIH .
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – ESGE GL 2015
Others have reported that nasogastric aspiration/lavage failed to assist clinicians in correctly predicting the need for endoscopic hemostasis, did not improve visualization of the stomach at endoscopy, or improve clinically relevant outcomes such as rebleeding, need for second-look endoscopy, or blood transfusion requirements.
It also should be noted that nasogastric aspiration/lavage is a very uncomfortable procedure that is not well tolerated or desired by patients.
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015



A3. Consider placement of a nasogastric tube in selected patients because the findings may have prognostic value.

Researchers argued here
Placement of a nasogastric tube for determining treatment of patients with upper gastrointestinal bleeding may be unnecessary since almost all these patients will eventually undergo an endoscopic procedure.
We found that the clinical judgment of the clinician was just about as good as a nasogastric tube examination - and didn't cause harm to the patient," .

"Since there is going to be an endoscopic follow-up to confirm the diagnosis and perform definitive treatment if necessary, there is no need to continue to torture our patients with nasogastric tube placement,”
Placement of nasogastric tubes cause pain and epistaxis in as many as 25% of patients undergoing the procedure; in another 10% of patients, the tube cannot be inserted due to some form of anatomic problem.
In the study ,pain, nasal bleeding, or nasogastric tube failure occurred in 35% patients assigned to that procedure.
Researchers argued here
Many patients refused to undergo the nasogastric tube placement." Those patients who refused were also followed as to their outcomes, and their clinical diagnosis turned out to be similar to the others.
Researchers argued here

FINAL THOUGHTS
So what should we say to our gastroenterology colleagues about NGL and UGIB? European Society of Gastrointestinal Endoscopy (ESGE) Guideline 2015
guidelines, and American College of Gastroenterology 2012 guidelines state NGL is not recommended in patients with UGIB for diagnosis, prognosis, visualization, or therapeutic effect . NG lavage DOES NOT help patients in the
emergency department with acute upper GI bleed and is an outdated practice.
It looks like there is no dilemma any longer.

ESGE does not recommend the routine use of nasogastric or orogastric aspiration/lavage in patients presenting with acute UGIH .
(strong recommendation, moderate quality evidence).
NVUGIH – MR6 - 13
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
NVUGIH – 14
In an effort to protect the patient's airway from potential aspiration of gastric contents, ESGE suggests endotracheal intubation prior to endoscopy in patients with ongoing active hematemesis, encephalopathy, or agitation .
(weak recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – 15
ESGE recommends adopting the following definitions regarding the timing of upper GI endoscopy in acute overt UGIH relative to patient presentation: very early < 12 hours, early ≤ 24 hours, and delayed > 24 hours.
(strong recommendation, moderate quality evidence).


Q

A

Following hemodynamic resuscitation, ESGE recommends early (≤24 hours) upper GI endoscopy.
Very early (<12 hours) upper GI endoscopy may be considered in patients with high risk clinical features, namely: hemodynamic instability (tachycardia, hypotension) that persists despite ongoing attempts at volume resuscitation; in hospital bloody emesis/nasogastric aspirate; or contraindication to the interruption of anticoagulation.
(strong recommendation, moderate quality evidence).
NVUGIH - MR7 - 16
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH - 17
ESGE recommends the availability of both an on-call GI endoscopist proficient in endoscopic hemostasis and on-call nursing staff with technical expertisein the use of endoscopic devices to allow performance of endoscopy on a 24 /7 basis .
(strong recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

Main Recommendations
Endoscopic therapy (peptic ulcer bleeding)

NVUGIH - 18
ESGE recommends the Forrest (F) classification be used in all patients with peptic ulcer hemorrhage in order to differentiate low and high risk endoscopic stigmata .
(strong recommendation, high quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH - MR8 - 19
ESGE recommends that peptic ulcers with spurting or oozing bleeding (Forrest classification Ia and Ib, respectively) or with a nonbleeding visible vessel (Forrest classification IIa) receive endoscopic hemostasis because these lesions are at high risk for persistent bleeding or rebleeding .
(strong recommendation, high quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – MR9 - 20
ESGE recommends that peptic ulcers with an adherent clot (Forrest classification IIb) be considered for endoscopic clot removal.
Once the clot is removed, any identified underlying active bleeding (Forrest classification Ia or Ib) or nonbleeding visible vessel (Forrest classification IIa) should receive endoscopic hemostasis.
(weak recommendation, moderate quality evidence). Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – MR10 - 21
In patients with peptic ulcers having a flat pigmented spot (Forrest classification IIc) or clean base (Forrest classification III), ESGE does not recommend endoscopic hemostasis as these stigmata present a low risk of recurrent bleeding.
In selected clinical settings, these patients may be discharged to home on standard PPI therapy, e. g., oral PPI once-daily .
(strong recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – 22
ESGE does not recommend the routine use of Doppler ultrasound or magnification endoscopy in the evaluation of endoscopic stigmata of peptic ulcer bleeding.
(strong recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
NVUGIH – MR11 – 23 - 24
For patients with actively bleeding ulcers (FIa, FIb), ESGE recommends combining epinephrine injection with a second hemostasis modality (contact thermal, mechanical therapy, or injection of a sclerosing agent).
ESGE recommends that epinephrine injection therapy not be used as endoscopic monotherapy.
(strong recommendation, high quality evidence). Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – 25
For patients with active NVUGIH bleeding not controlled by standard endoscopic hemostasis therapies, ESGE suggests the use of a topical hemostatic spray or over-the-scope clip as salvage endoscopic therapy.
(weak recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

Main Recommendations
Endoscopic therapy (Other causes of NVUGIH)
NVUGIH – 26
For patients with acid-related causes of NVUGIH different from peptic ulcers (e. g., erosive esophagitis, gastritis, duodenitis), ESGE recommends treatment with high dose PPI. Endoscopic hemostasis is usually not required and selected patients may be discharged early.
(strong recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – 27
ESGE recommends that patients with a Mallory – Weiss lesion that is actively bleeding receive endoscopic hemostasis.
There is currently inadequate evidence to recommend a specific endoscopic hemostasis modality.
Patients with a Mallory – Weiss lesion and no active bleeding can receive high dose PPI therapy alone.
(strong recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015

NVUGIH – 28
ESGE recommends that a Dieulafoy lesion receive endoscopic hemostasis using thermal, mechanical (hemoclip or band ligation), or combination therapy (dilute epinephrine injection combined with contact thermal or mechanical therapy).
(strong recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

NVUGIH – 29
In patients bleeding from upper GI angioectasias, ESGE recommends endoscopic hemostasis therapy.
However, there is currently inadequate evidence to recommend a specific endoscopic hemostasis modality.
(strong recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

NVUGIH – 30
In patients bleeding from upper GI neoplasia, ESGE recommends considering endoscopic hemostasis in order to avert urgent surgery and reduce blood transfusion requirements.
However, no currently available endoscopic treatment appears to have long-term efficacy.
(weak recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

NVUGIH – 30
Transcatheter angiographic embolization (TAE) or surgery should be considered if endoscopic treatment fails or is not technically feasible .
(strong recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

Main Recommendations
Post endoscopyEndoscopic Hemostasis
Management
محروس خالد Waleed Khalid Mahrous وليد
محروس خالد Waleed Khalid Mahrous وليد

NVUGIH – MR12 -31
ESGE recommends PPI therapy for patients who receive endoscopic hemostasis and for patients with adherent clot not receiving endoscopic hemostasis. PPI therapy should be high dose and administered as an intravenous bolus followed by continuous infusion (80 mg then 8 mg/hour) for 72 hours post endoscopy
(strong recommendation, high quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

NVUGIH – 32
ESGE suggests considering PPI therapy as intermittent intravenous bolus dosing (at least twice-daily) for 72 hours post endoscopy for patients who receive endoscopic hemostasis and for patients with adherent clot not receiving endoscopic hemostasis.
If the patient’s condition permits, high dose oral PPI may also be an option in those able to tolerate oral medications.
(weak recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

NVUGIH – MR13 – 33- 34
ESGE does not recommend routine second-look endoscopy as part of the management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH).
However, in patients with clinical evidence of rebleeding following successful initial endoscopic hemostasis, ESGE recommends repeat upper endoscopy with hemostasis if indicated.
In the case of failure of this second attempt at hemostasis, transcatheter angiographic embolization (TAE) or surgery should be considered .
(strong recommendation, high quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد
NVUGIH – MR14 - 35
In patients with NVUGIH secondary to peptic ulcer, ESGE recommends investigating for the presence of Helicobacter pylori in the acute setting with initiation of appropriate antibiotic therapy when H. pylori is detected.
Retesting for H. pylori should be performed in those patients with a negative test in the acute setting.
Documentation of successful H. pylori eradication is recommended .
(strong recommendation, high quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

NVUGIH – 36
ESGE recommends restarting anticoagulant therapy following NVUGIH in patients with an indication for long-term anticoagulation.
The timing for resumption of anticoagulation should be assessed on a patient by patient basis.
Resuming warfarin between 7 and 15 days following the bleeding event appears safe and effective in preventing thromboembolic complications for most patients.
Earlier resumption, within the first 7 days, may be indicated for patients at high thrombotic risk.
(strong recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

NVUGIH – 37
In patients receiving low dose aspirin for primary cardiovascular prophylaxis who develop peptic ulcer bleeding, ESGE recommends withholding aspirin, revaluating the risks/benefits of ongoing aspirin use in consultation with a cardiologist, and resuming low dose aspirin following ulcer healing or earlier if clinically indicated.
(strong recommendation, low quality evidence).
محروس خالد Waleed Khalid Mahrous وليد
NVUGIH – MR15 - 38
In patients receiving low dose aspirin for secondary cardiovascular prophylaxis who develop peptic ulcer bleeding, ESGE recommends aspirin be resumed immediately following index endoscopy if the risk of rebleeding is low (e. g., FIIc, FIII).
In patients with high risk peptic ulcer (FIa, FIb, FIIa, FIIb), early reintroduction of aspirin by day 3 after index endoscopy is recommended, provided that adequate hemostasis has been established .
(strong recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد
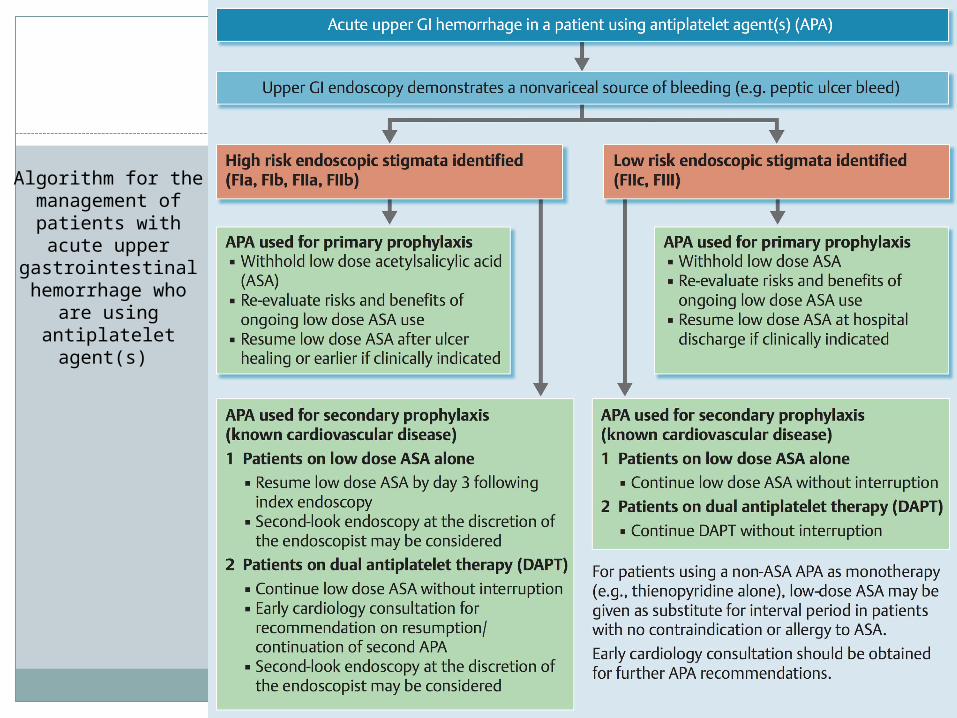
Algorithm for the management of
patients with acute upper
gastrointestinal hemorrhage who are
using antiplatelet agent(s)

NVUGIH – MR39
In patients receiving dual antiplatelet therapy (DAPT) who develop peptic ulcer bleeding, ESGE recommends continuing low dose aspirin therapy.
Early cardiology consultation should be obtained regarding the timing of resuming the second antiplatelet agent.
(strong recommendation, low quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد

NVUGIH – MR40
In patients requiring dual antiplatelet therapy (DAPT) and who have had NVUGIH, ESGE recommends the use of a PPI as co-therapy.
(strong recommendation, moderate quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015
محروس خالد Waleed Khalid Mahrous وليد


















![Acute Gastrointestinal Hemorrhage: Radiologic Diagnosis ... · bleeding are peptic ulcer disease, variceal bleeding, Mallory-Weisstear,vascularlesions,andneoplasms(Table1) [2]. Lower](https://static.fdocuments.net/doc/165x107/6021c6749b53ea1a471bc940/acute-gastrointestinal-hemorrhage-radiologic-diagnosis-bleeding-are-peptic.jpg)
![Delayed postoperative bleeding following lobectomy caused ......hemorrhage occur within 24 h of surgery and delayed bleeding is rare [24, ]. Early bleeding caused by staples in contact](https://static.fdocuments.net/doc/165x107/60c15026dd12a7739c41ba17/delayed-postoperative-bleeding-following-lobectomy-caused-hemorrhage-occur.jpg)