
Diagnosis and Treatment of Velopharyngeal Insufficiency · blowing, and whistling) and nonpneumatic...
20
CLINICAL CASE A 4-year-old boy presented for evaluation of his “abnormal voice.” His mother reports that since he has been able to speak he has never made clear “s” and “p” sounds. She reports that to most people he is unintelli- gible. She is seeking options for therapy, but currently lives on a Caribbean island with minimal access to speech services or surgi- cal care. The child has no other medical problems, feeds well, and has no previous surgical history. His examination shows a healthy energetic boy with no evidence of craniofacial dysmorphisms. However, he demonstrates markedly hypernasal speech. Fiberoptic examination demonstrates a short palate with decent lateral wall motion. Nasometry is consistent with marked nasal air escape. Given his anatomic deficit, sur- gical management was offered. In discuss- ing the potential risks and benefits of each surgical option with his mother, she pro- vided additional history that suggested he might have some degree of sleep apnea. She gave support to the notion that, were he to develop worse sleep apnea postoperatively, there would be no access on the island to anyone with expertise in diagnosing and managing such a condition. Given the his- tory, a sphincter pharyngoplasty was offered in place of a posterior pharyngeal flap. The child underwent surgery uneventfully and noticed immediate improvement. Six months later his results were maintained. INTRODUCTION The complex neuromuscular functions that regulate human speech are not limited to the larynx. The sphincteric interaction of the palate (velum) within the pharynx is criti- cal to the production of intelligible speech. Velopharyngeal insufficiency (VPI), or the inability to effectively seal the nasopharynx, 16 Diagnosis and Treatment of Velopharyngeal Insufficiency Matthew T. Brigger Jean E. Ashland Christopher J. Hartnick 16_HartBose_225-244 11/14/09 11:31 AM Page 225
Transcript of Diagnosis and Treatment of Velopharyngeal Insufficiency · blowing, and whistling) and nonpneumatic...

CLINICAL CASE
A 4-year-old boy presented for evaluation ofhis “abnormal voice.” His mother reportsthat since he has been able to speak he hasnever made clear “s” and “p” sounds. Shereports that to most people he is unintelli-gible. She is seeking options for therapy, butcurrently lives on a Caribbean island withminimal access to speech services or surgi-cal care. The child has no other medicalproblems, feeds well, and has no previoussurgical history. His examination shows ahealthy energetic boy with no evidence ofcraniofacial dysmorphisms. However, hedemonstrates markedly hypernasal speech.Fiberoptic examination demonstrates a shortpalate with decent lateral wall motion.Nasometry is consistent with marked nasalair escape. Given his anatomic deficit, sur-gical management was offered. In discuss-ing the potential risks and benefits of eachsurgical option with his mother, she pro-
vided additional history that suggested hemight have some degree of sleep apnea. Shegave support to the notion that, were he todevelop worse sleep apnea postoperatively,there would be no access on the island toanyone with expertise in diagnosing andmanaging such a condition. Given the his-tory, a sphincter pharyngoplasty was offeredin place of a posterior pharyngeal flap. Thechild underwent surgery uneventfully andnoticed immediate improvement. Six monthslater his results were maintained.
INTRODUCTION
The complex neuromuscular functions thatregulate human speech are not limited tothe larynx.The sphincteric interaction of thepalate (velum) within the pharynx is criti-cal to the production of intelligible speech.Velopharyngeal insufficiency (VPI), or theinability to effectively seal the nasopharynx,
16Diagnosis and Treatment of
Velopharyngeal Insufficiency
Matthew T. BriggerJean E. Ashland
Christopher J. Hartnick
16_HartBose_225-244 11/14/09 11:31 AM Page 225

results in loss of resonant control of speechand in some cases, optimal intraoral pressureto achieve orally directed speech sounds.Given that the nasopharynx is effectivelyclosed during the vast majority of speech,this can significantly impact speech intelli-gibility. A lack of speech intelligibility hasan obvious detrimental effect to affectedchildren, but even mild cases of VPI canalter a child’s effective communication andtheir well-being as speech provides a bridgeto the people around us. The etiology ofVPI varies from residual speech patternsafter cleft palate repair to congenital anom-alies of the soft palate (eg, shortness, sub-mucous cleft) as well as weakness or motorplanning difficulties.1 Subsequently, theapproaches to assessment and interventionare variable and often need to be tailored tothe individual child.
SEMANTICS
Terminology used within the VPI literatureis limited by redundancy and inconsistencies.In addition to velopharyngeal insufficiency,commonly used terms include velopharyn-geal dysfunction, velopharyngeal inade-quacy, and velopharyngeal incompetence.These terms are often used interchangeably.When specific terminology is used, varia-tions of the classification introduced by Trostin 1981 seem to be the most common.2 Inthe classification, an all encompassing termvelopharyngeal inadequacy is used to de-scribe velopharyngeal mislearning (faultylearning of articulation patterns), velopha-ryngeal incompetence (neurologic dysfunc-tion leading to impaired motor control ofthe palate), and velopharyngeal insufficiency(an anatomic deficiency of insufficient tis-sue for closure). A similar, widely used allencompassing term is velopharyngeal dys-
function (VPD).3 For the purposes of thischapter, VPI is used to connote velopharyn-geal inadequacy.
PERTINENT ANATOMY
A brief review of anatomy is requisite tounderstanding the problem of VPI and thepotential implications regarding evaluationand treatment. In general terms, the velo-pharyngeal port is a sphincter that regulatesairflow through the nasopharynx. The de-gree of regulation manifests in the produc-tion (or lack thereof) of nasal resonance.In simple terms, six muscles constitute thesphincter. These include the levator velipalatini, tensor veli palatini, palatoglossus,palatopharyngeus, muscular uvula, and supe-rior pharyngeal constrictor. All except forthe superior constrictor comprise the softpalate, also known as the velum. Anatomi-cally, the soft palate is located at the poste-rior aspect of the maxilla protruding fromthe hard palate.The Latin term velum refersto a “ship’s sail” and connotes the flat sheet-like shape of the soft palate as it protrudesposteriorly. By separating the oropharynxfrom the nasopharynx, the palate has bothan oral and nasal surface.
Regarding the musculature, motor con-trol is primarily mediated through branchesof cranial nerve X except for the tensor velipalatini which is innervated by a motorbranch of cranial nerve V. The paired leva-tor palatini serve as the primary musclemass of the soft palate and form a sling sus-pended from the skull base.4 The muscleserves to elevate the palate in a posteriordirection. This motion is counteracted bythe action of the palatoglossus (anteriortonsillar pillar) and the palatopharyngeus(posterior tonsillar pillar). Although the lev-ator veli palatini provides the muscular
226 CLINICAL MANAGEMENT OF CHILDREN’S VOICE DISORDERS
16_HartBose_225-244 11/14/09 11:31 AM Page 226

mass of the velum, the tensor veli palatinicontributes the majority of the fibrous com-ponent referred to as the palatal aponeuro-sis.4 The primary action of the tensor velipalatini is to facilitate middle ear aerationand overall has a minimal effect on velopha-ryngeal closure.5 The muscular uvula tensesthe palate as well as providing a bulge onthe posterior nasal surface of the palatewhich has been postulated to be instrumen-tal in tight velopharyngeal closure.6 Thesuperior pharyngeal constrictor serves toprovide lateral wall motion of the nasophar-ynx to close the velopharyngeal port.7 Addi-tionally, it may contribute to the presenceof Passavant’s ridge, a transverse mucosalbulge along the posterior pharyngeal wallnoted in 20% of the population.8
From a functional standpoint, an inter-esting distinction is made between the phys-iology involved in closing the nasopharynxduring swallowing versus speech exercises.A common situation is seen when childrenhave evidence of severe VPI with speech,but exhibit no nasal regurgitation duringswallowing. Shprintzen and colleagues clas-sified differences in pneumatic (speech,blowing, and whistling) and nonpneumatic(gagging and swallowing) closure mecha-nisms based on videofluoroscopic findings.7
Furthermore, an electromyographic (EMG)study of levator function during speech,blowing, and swallowing suggests that dif-ferent muscle types are activated during swal-lowing exercises as compared to speechand blowing exercises.9 By determining themean power frequencies of EMG signals,Nohara et al. concluded that pneumaticactivities tend to activate slow-twitch motorunits while swallowing tends to trigger fasttwitch motor units.9 This work is corrobo-rated by the hypothesis that the humanpharyngeal constrictors possess a subspe-cialized slow twitch inner layer of musclefibers that appears to be related to speech
and respiration.10 Ultimately the complexneuromuscular interaction and subspecial-ization of muscle fibers highlights theimportance of approaching VPI as morethan a simple anatomic deficit and realizingthat the manifestations of VPI can resultfrom a variety of insults.
Closure Patterns
The relatively simplistic discussion of themusculature involved in velopharyngealclosure described above fails to reveal thehigh degree of coordination, complexity,and variation involved. The sum motion isone in which the palate elevates posteriorlyand contacts the pharyngeal wall circumfer-entially. On a lateral view, the palate appearsto flex like a knee due to the bulge of theuvula maximizing contact with the poste-rior pharyngeal wall (Fig 16–1).11 Perhaps a
DIAGNOSIS AND TREATMENT OF VELOPHARYNGEAL INSUFFICIENCY 227
Fig 16–1. Lateral fluoroscopic view demon-strating “kneelike” contact between palateand posterior pharyngeal wall.
16_HartBose_225-244 11/14/09 11:31 AM Page 227

better way to look at velopharyngeal anat-omy is through closure patterns. In 1973,Skolnick and associates used videofluoros-copy to delineate four patterns of velopha-ryngeal closure.12 The most commonlyobserved pattern is the situation in whichthe posterior surface of the velum comesinto broad apposition with the posteriorpharyngeal wall in the absence of lateral pha-ryngeal wall motion. Two circular patternsof closure are described.The first pattern in-volves a combination of lateral wall motionand posterior velar movement to achievevelopharyngeal closure.A secondary circularpattern with posterior pharyngeal motion(Passavant’s ridge) is described. However,this motion pattern must be interpreted withcaution as Passavant’s ridge does not alwayscorrespond to the level of closure.The leastcommon closure pattern is referred to assagittal and demonstrates minimal velarmovement combined with medial apposi-tion of the lateral pharyngeal walls. An
assessment of closure patterns is instrumen-tal in characterizing the nature and locationof the velopharyngeal air escape. Suchknowledge is critical in selecting operativeprocedures to effectively seal the gap.
Normal Versus Abnormal Speech
Etiology and Pathophysiology
VPI is most commonly seen in childrenwith associated craniofacial developmentalanomalies of which cleft palate is the mostcommon. Despite successful palatoplasty,post repair prevalence of VPI has beenreported to be 20 to 50%.11,13 A special caseis the submucosal (occult) cleft palate. Inthis situation, no overt cleft is seen, but afailure of the midline fusion of the velarmuscles is present often manifesting as abifid uvula, hard palate notch, or a bluishline of a visible diastasis (Fig 16–2). The
228 CLINICAL MANAGEMENT OF CHILDREN’S VOICE DISORDERS
A B
Fig 16–2. Submucous cleft with bifid uvula. A. Intraoral view. B. Intranasal view, note midlinegroove.
16_HartBose_225-244 11/14/09 11:31 AM Page 228

majority of these children will have nospeech deficits during their lifetime.14 How-ever, a subset will present with VPI oftenafter adenotonsillar surgery. In a review of126 children with VPI after adenoidectomy,26% were noted to have a previously uniden-tified submucosal cleft palate or bifid uvula.15
In a different study, 55% of children withVPI in the absence of an overt bony cleftwere noted to have a submucous cleft onendoscopic examination.16
Associated Syndromes
Over 200 syndromes have been describedwhere cleft palate is a reported manifesta-tion. Any such syndrome can be associatedwith VPI. Of special note is velocardiofacialsyndrome which typically does not manifestan overt palatal cleft. The syndrome wasfirst described in 1977 by Shprintzen andcolleagues.17 The syndrome has a wide spec-trum of phenotypes including congenital
cardiac anomalies, VPI, and characteristicfacial dysmorphisms.18 The prevalence in theUnited States is estimated to be 1:2000.18
The difficulty lies in the wide variability ofpresentations and propensity to be under-diagnosed. Proper diagnosis is essential inthat patients with VCFS must be screenedfor potentially lethal cardiac anomalies.From a surgical standpoint, there have beena number of reports of carotid artery medi-alization which may possibly represent hazardous surgical anatomy (Fig 16–3).19,20
Additionally, surgical outcomes for VPI havebeen reported to be inferior to the resultsachieved in children without VCFS.21
Postadenoidectomy
VPI manifesting after adenoidectomy is rel-atively rare and generally of short duration,with most cases resolving within 6 weeks.Given the bulk of adenoid tissue, many chil-dren produce velopharyngeal closure by
DIAGNOSIS AND TREATMENT OF VELOPHARYNGEAL INSUFFICIENCY 229
Fig 16–3. Computed tomography demonstrating carotid arterymedialization.
16_HartBose_225-244 11/14/09 11:31 AM Page 229

approximating the velum to their adenoidpad. In most children, removal of the ade-noid pad is of no consequence because theirvelum has adequate length to reach the pos-terior pharyngeal wall. However, in selectchildren, the new dynamics of velopharyn-geal closure do not allow adequate apposi-tion. Permanent VPI after adenoidectomyrequiring intervention is reported to occur inapproximately 1:1500 adenoidectomies.22,23
In retrospect,many children have suggestionsof marginal velopharyngeal competenceincluding physical stigmata of a submucosalcleft, preoperative hypernasality or regurgita-tion (Table 16–1). In a review of 23 childrenwith VPI after adenoidectomy, 14 childrenwere found to carry the VCFS genotype.24 Insituations where an adenoidectomy appearsto be indicated in a child with features con-cerning for marginal velopharyngeal com-petence, a superior pole adenoidectomy canbe performed in which the inferior aspectof the adenoid pad is maintained to preventthe development of VPI.
Other Causes
VPI has been noted in a variety of other set-tings.Any surgery that involves orthognathicmaxillary advancement (often performed inchildren with craniofacial abnormalities) bydefinition puts a child at risk for developing
VPI. Hypertrophied tonsils have been asso-ciated with clinical VPI and resolution hasbeen documented after tonsillectomy.25 Addi-tionally, neuromuscular disorders resultingin poor control of pharyngeal musculaturecan result in hypernasality and dysarthria.
DIAGNOSTIC EVALUATION
As delineated above, VPI represents a com-plex problem with a variety of manifesta-tions. The degree of complexity mandates amultidisciplinary approach to the diagnosisand treatment of affected children. Oftenthese children are best served in the settingof a tertiary care referral center with coor-dinated access to speech pathologists, sur-geons, dentists, audiologists, and socialworkers.
History
Evaluation of a child with suspected VPIstarts by simply listening with a keen ear.Although children are often referred forgrossly abnormal speech, a great deal canbe learned by listening to the child speak.Using standard phrases weighted with sibi-lants and plosives will help to uncover theextent of VPI. A comprehensive history isimperative for all children. Particular empha-sis on any developmental anomalies, pastmedical history and past surgical historymay yield clues to syndromic associationsor other problems that can be seen in thesetting of VPI. Eliciting any history of hear-ing loss or other anomalies that potentiallyincrease the child’s communication difficul-ties is essential. A developmental and psy-chological history is useful in determiningthe extent of disability imparted by thecommunication difficulties.
230 CLINICAL MANAGEMENT OF CHILDREN’S VOICE DISORDERS
Table 16–1. Physical Examination Findings fora Submucosal Cleft Palate
Prevention of Postadenoidectomy VPI:Recognize the Signs of a SubmucosalCleft
bifid uvula
hard palate notch
bluish line of a visible diastasis
16_HartBose_225-244 11/14/09 11:31 AM Page 230

Physical Examination
A comprehensive physical examination isrequisite in all children with VPI.All childrenmust be assessed for the presence of syn-dromic stigmata, craniofacial dysmorphismsand the presence of cardiac abnormalities.A thorough head and neck examinationincludes an assessment of the middle earstatus.An oral exam is performed to identifythe presence of a cleft and status of repair.As described below, flexible nasopharyngos-copy has proven to be a well tolerated andinvaluable tool in examining and formulat-ing a treatment plan for these children.
A further note on orofacial examina-tion is necessary at this point.The completeevaluation consists of close intraoral exam-ination with attention to oromotor skills, theocclusal and dental status as well as directvisualization and palpation of the velum.Facial examination during speech in rela-tion to characteristic grimaces and gesturesare often noted.
Perceptual Evaluation
Several perceptual evaluation scales havebeen developed and validated. One of themost commonly used is that of McWilliamsand Phillips which is sometimes referred toas the Pittsburgh Weighted Speech Scale.26
This weighted scale rates five componentsof speech including nasal emission, facialgrimace, nasality, phonation, and articula-tion (Fig 16–4). Points are assigned for eachsubgroup and summed to give an overallscore that can be used to track outcomes.
Nasometry
Nasometry is based on the measurement of nasal acoustic energy within speech.27
A headset with two directional microphones(nasal and oral) is connected through a converter to a computer. The child beingevaluated wears the headset and voices stan-dardized passages.A nasalence score relatingthe nasal acoustic energy as related to thetotal acoustic energy is displayed graphicallyon the computer screen and a nasalencescore is generated. The score is then com-pared to normative data, such as with theMacKay-Kummer Simplified NasometricAssessment Procedures (SNAP) test.28 Addi-tionally, nasometry can be useful in therapyin the form of biofeedback as discussedbelow.
Assessment of Velopharyngeal Closure
Flexible Nasapharyngoscopy
Flexible nasopharyngoscopy has becomeindispensable in the evaluation of childrenwith VPI. The development of high-qualitysmall-caliber flexible endoscopes permitsexcellent visualization in most children.Theflexible endoscope is passed transnasally to a position in the posterior nasal cavityallowing a complete view of the velum andnasopharynx. Children of all ages can be eval-uated anatomically; however, it is generallyaround age six that children can cooperateand perform comprehensive volitional vocal-izing tasks for a complete evaluation. Flexiblenasopharyngoscopy provides an excellentview of the nasal surface of the palate andmay provide the only sign of a submucouscleft palate as described above.Additionally,flexible nasopharyngoscopy allows an exam-ination of the larynx, which may uncoveradditional pathologies associated with com-pensatory measures, such as vocal nodules,that may have developed in response to the VPI.
DIAGNOSIS AND TREATMENT OF VELOPHARYNGEAL INSUFFICIENCY 231
16_HartBose_225-244 11/14/09 11:31 AM Page 231

232
Fig 16–4. Perceptual weighted speech score used at Massachusetts General Hospital.Adapted from McWilliams and Phillips.26
16_HartBose_225-244 11/14/09 11:31 AM Page 232
Multiview Fluoroscopy
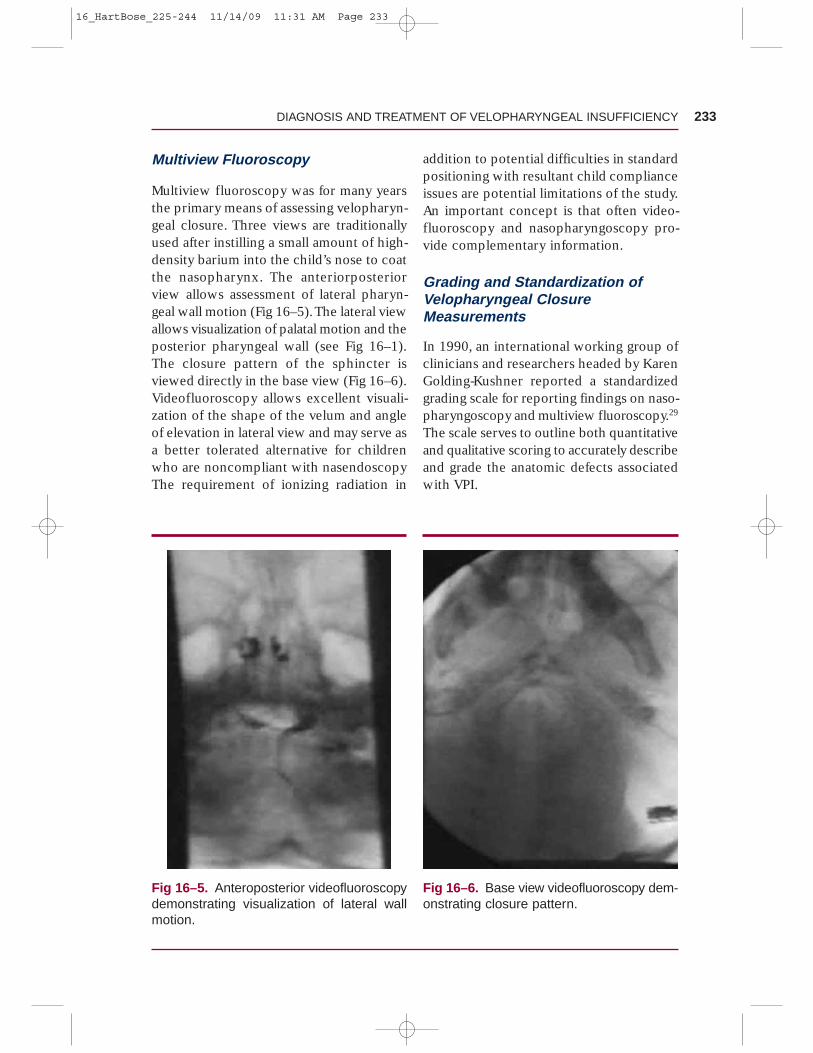
Multiview fluoroscopy was for many yearsthe primary means of assessing velopharyn-geal closure. Three views are traditionallyused after instilling a small amount of high-density barium into the child’s nose to coatthe nasopharynx. The anteriorposteriorview allows assessment of lateral pharyn-geal wall motion (Fig 16–5).The lateral viewallows visualization of palatal motion and theposterior pharyngeal wall (see Fig 16–1).The closure pattern of the sphincter isviewed directly in the base view (Fig 16–6).Videofluoroscopy allows excellent visuali-zation of the shape of the velum and angleof elevation in lateral view and may serve asa better tolerated alternative for childrenwho are noncompliant with nasendoscopyThe requirement of ionizing radiation in
addition to potential difficulties in standardpositioning with resultant child complianceissues are potential limitations of the study.An important concept is that often video-fluoroscopy and nasopharyngoscopy pro-vide complementary information.
Grading and Standardization ofVelopharyngeal ClosureMeasurements
In 1990, an international working group ofclinicians and researchers headed by KarenGolding-Kushner reported a standardizedgrading scale for reporting findings on naso-pharyngoscopy and multiview fluoroscopy.29
The scale serves to outline both quantitativeand qualitative scoring to accurately describeand grade the anatomic defects associatedwith VPI.
DIAGNOSIS AND TREATMENT OF VELOPHARYNGEAL INSUFFICIENCY 233
Fig 16–5. Anteroposterior videofluoroscopydemonstrating visualization of lateral wallmotion.
Fig 16–6. Base view videofluoroscopy dem-onstrating closure pattern.
16_HartBose_225-244 11/14/09 11:31 AM Page 233

Nasopharyngoscopy, MultiviewFluoroscopy, or Both?
Over time, much has been written aboutthe merits and disadvantages of both naso-pharyngoscopy and multiview fluoroscopy.Both are used to accurately assess velopha-ryngeal anatomy to assist in developing atreatment plan, particularly surgical meth-ods. Nasopharyngoscopy allows an excellentview of velopharyngeal closure patterns, butcan be limited by optical distortion and tol-erance by the child undergoing the exam.Multiview fluoroscopy allows an excellentview of lateral wall motion as well as clo-sure patterns. As stated above, the closurepatterns of the velopharynx were initiallydescribed based on fluoroscopic studies.Difficulties arise in interpreting anatomicfindings in the presence of multiple shad-ows. Additionally, postsurgical examinationparticularly in the setting of a pharyngealflap is quite difficult with fluoroscopy, butis easily visualized directly with nasopharyn-goscopy. A recent review suggests that bothmodalities provide complementary data,but that nasopharyngoscopy may provide ahigher correlation with VPI severity.30 Cur-rently, our practice is to perform flexiblenasopharyngoscopy on all children to visu-alize anatomy and assist in surgical planningand proceed to multiview fluoroscopy inchildren where additional information mayprove useful, particularly in children undersix years of age who have limited coopera-tion for a functional endoscopic assessment.
TREATMENT: BASIC TENETS
Prior to surgical repair of a cleft palate orprimary VPI, a speech-language pathologistwith specialized training can help guide par-ents to elicit sound play with their infant,
expand consonant repertoires, and to min-imize patterns of glottal stops.
As language and speech emerge for thetoddler and preschool age child, it is impor-tant to discern if speech errors are develop-mental, obligatory, or compensatory. Whenchildren with cleft or noncleft velopharyn-geal problems display articulation errorsand resonance abnormalities, the develop-mentally appropriate articulation issues areaddressed first. It is important to remediatethese developmental speech errors as wellas establish accurate placement of the artic-ulators and manner of production (eg, frica-tive versus stop consonants), even whenthe anatomy prohibits the ability to achievean orally produced sound. This is especiallytrue for children under four years of agewith a cleft palate who are often too youngfor consideration of a secondary surgery.
Behavioral therapy with a speech-language pathologist can be helpful in mildVPI and phoneme specific VPI. Speech/resonance therapy is not indicated when:(a) nasal emissions are present in all non-nasalconsonants with subsequent hypernasalityrelated to a short or poor moving palate orexcessively deep pharynx, (b) nasal air lossrelated to a palatal fistula, or (c) articulationerrors related to severe dental malocclu-sions that require physical management.31,32
Speech/resonance therapy cannot workagainst atypical anatomy and if attemptedmay cause undue frustration to the child.
Perhaps the primary concern for everychild, parent, and VPI surgeon is to avoidoperating when a child has a functionalspeech abnormality that can be masking aswhat appears to be VPI secondary to ana-tomic deficit. A thorough evaluation by aspeech and language pathologist is often nec-essary to accurately diagnose such disorderspreoperatively.As described below, compre-hensive therapy often involves much morethan simply filling the anatomic defect.
234 CLINICAL MANAGEMENT OF CHILDREN’S VOICE DISORDERS
16_HartBose_225-244 11/14/09 11:31 AM Page 234

Speech Therapy:Resonance Therapy
Resonance therapy is helpful in certain con-ditions: mild velopharyngeal dysfunctionthat results in inconsistent nasal air emis-sions related to articulation errors and inthe postoperative period.33,34 Short-termspeech therapy preoperatively is helpful toestablish accurate patterns so that the childcan experience maximum success followingsurgery. Also, speech therapy may be con-sidered for young children with a repairedcleft palate who are too young for second-ary surgery but who have either difficultieswith accurate articulation placement orhave compensatory strategies considered asspeech errors, such as glottal stops.34 Treat-ment approaches generally include estab-lishing auditory discrimination of nasal andnon-nasal speech productions, maximizingoral airflow for non-nasal speech sounds,facilitating accurate articulation placement,production, and manner; and diminishingdeviant compensatory speech patterns, suchas glottal stops. Approaches may includearticulation strategies to foster oral airflow,such as a prolonged plosive sound “t” toglide into a sibilant “s,” whispered speechwith initial sounds “h” or “w” paired with lowfront vowels (eg, “haha” or “wah wah”).32,35
Low resistance blowing toys can be helpfulfor the concept of oral airflow, but shouldnot be used to “strengthen” the palate mus-cle as research does not support that an“exercise model” results in improved palatemotion.36,37 Other approaches that may helpwith improved resonance balance include:vowel prolongation, increased mouth open-ing, and increased vocal loudness. In addi-tion, visual and auditory feedback in therapycan offer additional modalities to help thechild see or hear the degree of nasal airescape. Feedback can be seen via foggingon a nasal mirror, use of a SeeScape® device
which uses a nasal tip to capture nasal air-flow and provides the visual correlation ofan object moving up a tube to reflect degreeof flow, the new Oral and Nasal Listener®
device with connected dual stethoscopesto provide auditory feedback, or a computerprogram using a nasometer to display nasalairflow in graphic form.35,38
Of note, resonance therapy will not behelpful for moderate to severe VPI whenthe physical ability of the palate to achieveclosure during speech is not possible. Thiswould include unintelligible speech relatedto hypernasality and velopharyngeal incom-petence, inability to achieve non-nasal con-sonants because of nasal air leakage andpoor intraoral pressure.39
Obturators and Prostheses
In some children, the use of a dental appli-ance to serve as a palatal lift or nasopharyn-geal obturator may serve as a useful therapyalternative. Palatal lifts serve to elevate theneurogenic palate that has reduced motionor decreased accurate timing of soft palateelevation to achieve VP closure. Generallysuch children will have adequate velar length,but poor muscle tone. In contrast, speechbulbs or obturators are fashioned to fill theopen space or gap between the soft palateand posterior pharyngeal wall in cases ofinsufficient palatal length (Fig 16–7). Thelateral and posterior walls of the pharynx canthen close against the obturator.40 Ideally, aspeech appliance (either lift or bulb) providesthe closure between the soft palate andpharyngeal wall to remediate nasal emissionsand/or hypernasality associated with VPI.41,42
In general, prosthetic management of VPI is not generally a first-line approach due tocompliance issues and the need for adequatestable dentition.40 However, such devicescan be useful when secondary surgical
DIAGNOSIS AND TREATMENT OF VELOPHARYNGEAL INSUFFICIENCY 235
16_HartBose_225-244 11/14/09 11:31 AM Page 235

management, such as a pharyngeal flap, iscontraindicated as in the case of a childwith potential surgical comorbidities suchas severe obstructive sleep apnea or cardiacanomalies. The devices can often serve as a temporary approach until surgery can becompleted, or to offer insight if surgery willbe beneficial.43
A team approach for speech applianceselection and fitting is useful. In general, theteam should consist of a speech languagepathologist, dental specialist, and orthodon-tist or prosthodontist to maximize successfuloutcomes.43 Some studies have documentedimproved VP muscle function following useof speech appliances in electromyographymeasures, such as increased activiation sig-nal of the levator veli palatini muscle.41
Careful selection of patients is requisitefor success. Potential candidates includechildren with wide clefts in whom a lack ofavailable tissue may compromise potentialrepair techniques, children with significantneuromuscular deficits of the soft palate orwhen surgery is contraindicated or delayedfor any reason.44 In general, the limitations ofsuch devices are realized through noncom-pliance. Extensive dental caries precludesthe use of such devices as well.44
Surgical Treatment
Surgical treatment is the cornerstone ofeffective therapy for the anatomic defectassociated with VPI. A variety of techniqueshave been developed over time to addressthe various configurations of closure patternsand degree of difficulties experienced byindividual children. Most surgeons acceptthat a basic tenet of VPI surgery is that pro-cedures must be tailored to the specific dif-ficulty and anatomic deficiency present ineach child.
The timing of such procedures dependson a variety of factors including age at diag-nosis, etiology of VPI, access to trained ther-apists and neurocognitive development. Ingeneral, as discussed above, adequate diag-nosis of VPI often does not occur until thechild is approximately 3 to 4 years of age.Once diagnosed, most surgical procedurescan be safely performed in children as youngas 3 years old. A special note regardingselection of procedure type is the presenceof baseline obstructive sleep apnea. As pro-cedures designed to address VPI constrictthe nasopharyngeal airway by definition, thetheoretical possibility of exacerbating orintroducing obstructive sleep apnea mustbe considered.
Posterior Pharyngeal Flap
Efforts to lessen the nasal emission of VPIwere first described by Passavant in 1865when he reported adhesion of the softpalate to the posterior pharyngeal wall.45
This was subsequently followed in 1875when Schoenborn described the inferiorlybased posterior pharyngeal flap followedby his introduction of a superior based flap10 years later.46 The procedure has subse-quently undergone numerous modificationssince that time, but the principle remainsthe same.The goal of a posterior pharyngeal
236 CLINICAL MANAGEMENT OF CHILDREN’S VOICE DISORDERS
Fig 16–7. Velopharyngeal obturator (photocourtesy of Dr. Matthew Jackson).
16_HartBose_225-244 11/14/09 11:31 AM Page 236

flap is to effectively obturate the nasophar-ynx with a biologic obturator. The proce-dure involves creating a flap of tissue fromthe posterior pharyngeal wall that is raisedfrom an inferior point superiorly where itremains attached to the posterior pharynx.The elevated inferior aspect is subsequentlysecured to the nasal surface of the softpalate. This can be accomplished eitherwith or without splitting the soft palate.Once completed, the central region of thenasopharynx is obturated by the tissue,whereas lateral ports for air escape remainopen to allow an attenuated degree of nasaltransmission (Fig 16–8).
The development of the procedure overtime has placed attention to the proper con-struction of the lateral ports. A prevailingconcept is that children with some degreeof lateral wall motion may benefit mostfrom a pharyngeal flap as the existing lat-eral wall motion may be used to control therelease of air through the ports.47
Sphincter Pharyngoplasty
In distinction to the static obturator createdby a pharyngeal flap, the sphincter pharyn-goplasty operation was developed in an
effort to recreate a dynamic sphincter. Firstintroduced in 1950 by Hynes with furthermodifications by Orticochea, Jackson, andothers, the sphincter pharyngoplasty involveselevating two lateral superiorly based flapsfrom the region of the posterior tonsillarpillars.48–50 A transverse incision is made inthe posterior pharyngeal wall mucosa, andthe flaps are rotated 90 degrees and subse-quently inset into the transverse incisionpotentially placing dynamic muscle (palato-phayngeus) into an orientation to create adynamic sphincteric effect (Fig 16–9).A studycomparing pre and postoperative operativevideofluoroscopy suggested that there issome degree of dynamism after sphincterpharyngoplasty, but that it is difficult toquantify.51 Ultimately, sphincter pharyngo-plasty is generally pursued in the setting of achild with adynamic lateral pharyngeal walls.
Posterior Wall Augmentation
In some children with a mild to moderatedegree of VPI and a clearly evident smallvelopharyngeal gap, posterior pharyngealwall augmentation may provide significantspeech improvement.The concept involvesplacing the augmentation material in a loca-tion that allows adequate velopharyngealclosure by displacing the posterior pharyn-geal wall anteriorly to allow contact with thesoft palate. A variety of materials have beenadvocated including cartilage, fat, fascia,paraffin, silicone, acellular dermis, polytetra-fluoroethylene, and calcium hydroxylap-atite (CaHA).4,52–56 Placement methods haveincluded direct incision over the pharyn-geal mucosa, transcervical approaches, andinjection. Teflon is associated with an un-clear safety profile and migration leading toa sharp decrease in its use in recent years.4
Recently, our center has had a favorableexperience with CaHA which serves as astable, easily placed injectable augmentation
DIAGNOSIS AND TREATMENT OF VELOPHARYNGEAL INSUFFICIENCY 237
Fig 16–8. Postoperative endoscopic view ofa superior based pharyngeal flap.
16_HartBose_225-244 11/14/09 11:31 AM Page 237

agent (Fig 16–10).56 To date, we have usedCaHA augmentation in 12 patients. Eightchildren demonstrated success defined asnormalized nasometry and improved per-ceptual scores at 3 months. Four childrenhave been followed for over 24 months andhave demonstrated sustained success.Threeof the 4 failures occurred very early in ourexperience and it became evident that thetechnique is both operator and patientdependent. From a technique standpoint, amimimum of 2 to 3 mL of CaHA must beinjected. This is performed under directvisualization using a 120-degree endoscopewith a soft palate retractor. Of note, wehave had no cases of CaHA migration. Inour experience, older children with mild tomoderate VPI with a clear anatomic deficitseem to benefit most from the procedure.
An alternative method of posteriorwall augmentation is elevating a superiorlybased posterior pharyngeal wall flap androlling it onto itself instead of attaching it tothe soft palate as in typical pharyngeal flapsurgery. This creates a mound of tissue thatultimately scars and provides for a contactpoint in the soft palate. Patient selection iscritical as this method is only appropriatein children with small gaps. A particularadvantage with injection methods is theability to precisely locate the area of defi-ciency and to endoscopically target onlythe area that requires treatment.
Palatoplasty Methods
In some children, the configuration of theirpalate or previous surgeries may make palato-
238 CLINICAL MANAGEMENT OF CHILDREN’S VOICE DISORDERS
A B
Fig 16–9. A. Transverse mucosal incision and elevation of superiorly based lateral flaps.B. Flaps rotated 90 degrees and inset on posterior pharyngeal wall.
16_HartBose_225-244 11/14/09 11:31 AM Page 238

plasty techniques more useful. In particular,children with submucous cleft palate or con-genitally short palate and associated VPI maybenefit from a palatal lengthening proceduresuch as a Furlow palatoplasty or V-Y push-
back palatoplasty. Both of these methodsserve to effectively lengthen the soft palate.The Furlow method involves using opposingZ-plasties whereas the V-Y method uses softtissue elevated from the hard palate.
DIAGNOSIS AND TREATMENT OF VELOPHARYNGEAL INSUFFICIENCY 239
A B
C D
Fig 16–10. Posterior pharyngeal wall augmentation with injectable calcium hydroxylapatiteviewed with 120-degree endoscope placed transorally viewing superiorly into nasopharynx.A. Prior to injection. B. Needle in place. C. During injection. D. Post injection.
16_HartBose_225-244 11/14/09 11:31 AM Page 239

Special Case: Unilateral Deficits
Special consideration must be given in thesetting of VPI in children with unilateraldeficits as is commonly seen with hemifacialmicrosomia or unilateral neurologic injury.57
In these children, the anatomic defect resultsin a unilateral escape of air on the affectedside. Surgical therapy can be accomplishedwith unilateral sphincter pharynoplastytechniques, offset superior based pharyn-geal flaps or possibly directed posteriorwall augmentation.57,58 The decision on thebest procedure is dictated by the child’sanatomy, underlying features and the expe-rience of the surgeon. The situation clearlydemonstrates the need to address VPI on anindividual case by case basis.
Tonsillectomy
A rarely described, but clinically importantcause of VPI is obstructed velar closure sec-ondary to hypertrophic tonsils.Tonsillectomycan be curative in such children.25 In suchchildren examination will demonstrate sig-nificant tonsillar hypertrophy, but confirma-tion requires an endoscopic or fluoroscopicexamination to determine the presence ofthe velopharyngeal gap and to visualize therole that the tonsils play in contributing tothe overall gap dimensions.
Surgical Outcomes
Each of the described methods has beenshown to be effective in representative caseseries. Definitions of success vary and theheterogeneity of the problem leads to pre-operative characteristics that are not uniformin studies addressing surgical outcomes. Ingeneral, success rates described as resolu-tion of VPI vary from 62 to 98% with mostaccounts being in the realm of 75% resolu-
tion.58–67 Of note, several studies have lookedto differentiate success rates between pha-ryngeal flaps and sphincter pharyngoplasty.Unfortunately, the relative rarity of the prob-lem coupled with different techniques amongdifferent surgeons clouds the literature. Anunderpowered multicenter trial in 2005suggested that outcomes were similar.68
Perhaps a greater concern might be therisk of complications between the variousprocedures. Moderate to severe bleedingseen after both pharyngeal flap surgery andsphincter pharyngoplasty is generally rare,but may occasionally require transfusion.As described above, prudence in detectingmedialized carotid arteries is requisite inchildren with velocardiofacial syndrome.Complications associated with posterior wallaugmentation procedures are related to thematerial used. Extrusion, infection, resorp-tion and migration are all possibilities andoccur at varying rates.Our material of choice,calcium hydroxylapatite, has not demon-strated any such complications to date.56
The development of obstructive sleepapnea is likely one of the most worrisomecomplications associated with the surgicalmanagement of VPI. Obstructive sleepapnea is almost exclusively seen in pharyn-geal flap surgery and several postoperativedeaths have been reported.69,70 Recentattention to the subject has suggested thatcareful preoperative airway evaluation andconsideration of preoperative tonsillectomymay be useful in preventing untoward outcomes.60
When considering patient selectionfor various procedures, a certain degree oftailoring is necessary. A combination of thechild’s anatomy, neurocognitive develop-ment, social situation, and access to therapycoupled with the surgeon’s experience areall factors in selecting the appropriate pro-cedure for each child.
240 CLINICAL MANAGEMENT OF CHILDREN’S VOICE DISORDERS
16_HartBose_225-244 11/14/09 11:31 AM Page 240

FUTURE DIRECTIONS
The management of velopharyngeal insuffi-ciency continues to be an evolving field.Recent advances in evaluation include thewidespread use and acceptance of nasalendoscopy. Of recent note, the utility ofmagnetic resonance imaging (MRI) as anevaluation tool has emerged as stronger mag-nets and imaging algorithms have allowed thedevelopment of cine MRI sequences whichprovide high-resolution detailed velopharyn-geal movement visualized without ionizingradiation.71 Further developments in surgi-cal technique including the novel materialsfor posterior wall augmentation as well asalternative procedures such as cerclagepharyngoplasty and creation of a palatopha-ryngeal sling have been described and rep-resent exciting advances in the field.56,72,73
CONCLUSIONS
Overall, the evaluation and management ofVPI remains both challenging and reward-ing.The heterogeneity of the problem leadsto a wide variety of manifestations and ther-apies.The care of these children requires anindividualized approach to each patient ina multidisciplinary fashion. Fortunately, giventhe opportunity, most children can ultimatelyachieve intelligible speech and experienceminimal vocal disability over the long term.
REFERENCES
1. Johns DF, Rohrich RJ, Awada M. Velopharyn-geal incompetence: a guide for clinical evaluation. Plast Reconstr Surg. 2003;112:1890–1897; quiz 1898, 1982.
2. Trost JE. Articulatory additions to the classi-cal description of the speech of persons withcleft palate. Cleft Palate J. 1981;18:193–203.
3. Kummer AW. Velopharyngeal dysfunction(VPD) and resonance disorders. In: CleftPalate and Craniofacial Anomalies: TheEffects on Speech and Resonance. San Diego,CA: Singular; 2001:145–176.
4. Willging JP, Cotton RT. Velopharyngealinsufficiency. In Bluestone CD, Stool SE,Alper CM, eds. Pediatric Otolaryngology.4th ed. Philadelphia, PA: Saunders; 2003:1789–1799.
5. Kamerer DB, Rood SR. The tensor tympani,stapedius, and tensor veli palatini muscles—an electromyographic study. Otolaryngol-ogy. 1978;86:416–421.
6. Azzam NA, Kuehn DP. The morphology ofmusculus uvulae. Cleft Palate J. 1977;14:78–87.
7. Shprintzen RJ, McCall GN, Skolnick ML, et al.Selective movement of the lateral aspects ofthe pharyngeal walls during velopharyngealclosure for speech, blowing, and whistlingin normals. Cleft Palate J. 1975;12:51–58.
8. Dickson DR, Dickson WM. Velopharyngealanatomy. J Speech Hear Res. 1972;15:372–381.
9. Nohara K, Kotani Y, Ojima M, et al. Powerspectra analysis of levator veli palatini mus-cle electromyogram during velopharyngealclosure for swallowing, speech, and blow-ing. Dysphagia. 2007;22:135–139.
10. Mu L, Sanders I. Neuromuscular specializa-tions within human pharyngeal constrictormuscles. Ann Otol Rhinol Laryngol. 2007;116:604–617.
11. Kummer AW. Anatomy and Physiology: Theorofacial structures and velopharyngealvalve. In: Cleft Palate and CraniofacialAnomalies: The Effects on Speech and Res-onance. San Diego, CA: Singular; 2001:3–32.
12. Skolnick ML, Mc CG, Barnes M. The sphinc-teric mechanism of velopharyngeal closure.Cleft Palate J. 1973;10:286–305.
13. Morris HL.Velopharyngeal competence andprimary cleft palate surgery,1960–1971: a crit-ical review. Cleft Palate J. 1973;10:62–71.
DIAGNOSIS AND TREATMENT OF VELOPHARYNGEAL INSUFFICIENCY 241
16_HartBose_225-244 11/14/09 11:31 AM Page 241

14. McWilliams BJ. Submucous clefts of thepalate: how likely are they to be sympto-matic? Cleft Palate Craniofac J. 1991;28:247–249; discussion 250–251.
15. Witzel MA, Rich RH, Margar-Bacal F, et al.Velopharyngeal insufficiency after ade-noidectomy: an 8-year review. Int J PediatrOtorhinolaryngol. 1986;11:15–20.
16. Trier WC. Velopharyngeal incompetency inthe absence of overt cleft palate: anatomicand surgical considerations. Cleft Palate J.1983;20:209–217.
17. Shprintzen RJ, Goldberg RB, Lewin ML, etal. A new syndrome involving cleft palate,cardiac anomalies, typical facies, and learn-ing disabilities: velo-cardio-facial syndrome.Cleft Palate J. 1978;15:56–62.
18. Robin NH, Shprintzen RJ. Defining the clin-ical spectrum of deletion 22q11.2. J Pediatr.2005;147:90–96.
19. MacKenzie-Stepner K, Witzel MA, StringerDA, et al. Abnormal carotid arteries in the velocardiofacial syndrome: a report of three cases. Plast Reconstr Surg. 1987;80:347–351.
20. D’Antonio LD, Marsh JL. Abnormal carotidarteries in the velocardiofacial syndrome.Plast Reconstr Surg. 1987;80:471–472.
21. Butts SC, Tatum SA 3rd, Mortelliti AJ, et al.Velo-cardio-facial syndrome: the pediatricotolaryngologist’s perspective. Curr OpinOtolaryngol Head Neck Surg. 2005;13:371–375.
22. Gibb AG. Hypernasality (rhinolalia aperta)following tonsil and adenoid removal. JLaryngol Otol. 1958;72:433–451.
23. Skolnick ML.Velopharyngeal function in cleftpalate. Clin Plast Surg. 1975;2:285–297.
24. Perkins JA, Lewis CW, Gruss JS, et al. Furlowpalatoplasty for management of velopha-ryngeal insufficiency: a prospective study of148 consecutive patients. Plast ReconstrSurg. 2005;116:72–80; discussion 81–84.
25. Kummer AW, Billmire DA, Myer CM 3rd.Hypertrophic tonsils: the effect on resonanceand velopharyngeal closure. Plast ReconstrSurg. 1993;91:608–611.
26. McWilliams BJ, Phillips BJ. In: VelopharyngealIncompetence: Audio Seminars in Speech
Pathology. Philadelphia, PA: WB Saunders;1979.
27. Kummer AW. Nasometry. In: Cleft Palateand Craniofacial Anomalies: The Effectson Speech and Resonance. San Diego, CA:Singular; 2001; 311–330.
28. MacKay I, Kummer A. Simplified nasometricassessment procedures. The MacKay-Kum-mer SNAP Test. Lincoln, NJ: Kay ElemtricsCorporation; 1994.
29. Golding-Kushner KJ, Argamaso RV, CottonRT, et al. Standardization for the reporting ofnasopharyngoscopy and multiview video-fluoroscopy: a report from an InternationalWorking Group. Cleft Palate J. 1990;27:337–247; discussion 47–48.
30. Lam DJ, Starr JR, Perkins JA, et al. A compar-ison of nasendoscopy and multiview video-fluoroscopy in assessing velopharyngealinsufficiency. Otolaryngol Head Neck Surg.2006;134:394–402.
31. Peterson-Falzone S, Trost-Cardamone J, Kar-nell M, et al. Articulation therapy for school-age children. In: The Clinician’s Guide toTreating Cleft Palate Speech. St. Louis, MO:Mosby; 2005:124–160.
32. Golding-Kushner KJ. Therapy techniquesfor cleft palate speech and related disorders.In Golding-Kushner KJ, ed. Therapy Tech-niques for Cleft Palate Speech and RelatedDisorders. San Diego, CA: Singular; 2001.
33. Smith BE, Kuehn DP. Speech evaluation ofvelopharyngeal dysfunction. J CraniofacSurg. 2007;18:251–261; quiz 266–267.
34. Rudnick EF, Sie KC. Velopharyngeal insuffi-ciency: current concepts in diagnosis andmanagement. Curr Opin Otolaryngol HeadNeck Surg. 2008;16:530–535.
35. Kummer AW. Cleft Palate and CraniofacialAnomalies: Effects on Speech and Reso-nance. 2nd ed. San Diego, CA: Singular/Thomas Learning; 2008.
36. Ruscello D. Considerations for behavioraltreatment of velopharyngeal closure forspeech. In Bzoch KR, ed. CommunicativeDisorders Related to Cleft Lip and Palate.Austin, TX: Pro-Ed; 2004:763–796.
37. Kummer AW, Marty-Grames L, Jones DL, et al.Response to “Velopharyngeal dysfunction:
242 CLINICAL MANAGEMENT OF CHILDREN’S VOICE DISORDERS
16_HartBose_225-244 11/14/09 11:31 AM Page 242

speech characteristics, variable etiologies,evaluation techniques, and differential treat-ments” by Dworkin, Marunick, and Krouse,October 2004. Lang Speech Hear Serv Sch.2006;37:236–238; author reply 239–243.
38. Retrieved 11/22/08 from http://www.superduperinc.com/products/view.aspx?pid=ONL22 .
39. Retrieved 11/22/2008 from http://www.choa.org/default.aspx?id=762 .
40. Willging JP. Velopharyngeal insufficiency.Curr Opin Otolaryngol Head Neck Surg.2003;11:452–455.
41. Tachimura T, Nohara K, Wada T. Effect ofplacement of a speech appliance on levatorveli palatini muscle activity during speech.Cleft Palate Craniofac J. 2000;37:478–482.
42. Dworkin JP, Marunick MT, Krouse JH. Velo-pharyngeal dysfunction: speech characteris-tics, variable etiologies, evaluation techniques,and differential treatments.Lang Speech HearServ Sch. 2004;35:333–352.
43. Sell D, Mars M, Worrell E. Process and out-come study of multidisciplinary prosthetictreatment for velopharyngeal dysfunction. IntJ Lang Commun Disord. 2006;41:495–511.
44. Kumar S, Hedge V. Prosthodontics in velo-pharyngeal insufficiency. J Ind ProsthodontSoc. 2007;7:12–16.
45. Passavant G. Ueber die Beseitigung dernaselnden Sprache bei angeborenen Spaltendes harten und weichen Gaumens. ArchKlin Chir. 1865;6:333–349.
46. Schoenborn D.Vorstellung eines Falles staph-yloplastik. Verhandlungen der DeutschenGesellschaft fur Chirurgie. 1886;15:57.
47. Cotton RT, Quattromani F. Lateral defects invelopharyngeal insufficiency. Diagnosis andtreatment. Arch Otolaryngol. 1977;103:90–93.
48. Hynes W. Pharyngoplasty by muscle trans-plantation. Br J Plast Surg. 1950;3:128–135.
49. Orticochea M. Construction of a dynamicmuscle sphincter in cleft palates. PlastReconstr Surg. 1968;41:323–327.
50. Jackson IT. Sphincter pharyngoplasty. ClinPlast Surg. 1985;12:711–717.
51. Witt PD, Marsh JL,Arlis H, et al. Quantificationof dynamic velopharyngeal port excursion
following sphincter pharyngoplasty. PlastReconstr Surg. 1998;101:1205–1211.
52. Lando RL. [Transplant of cadaveric cartilageinto the posterior pharyngeal wall in treat-ment of cleft palate.] Stomatologiia (Mosk).1950;4:38–39.
53. Hagerty RF, Hill MJ. Cartilage pharyngo-plasty in cleft palate patients. Surg GynecolObstet. 1961;112:350–356.
54. Bluestone CD, Musgrave RH, McWilliams BJ,et al. Teflon injection pharyngoplasty. CleftPalate J. 1968;5:19–22.
55. Blocksma R. Correction of velopharyngealinsufficiency by Silastic pharyngeal implant.Plast Reconstr Surg. 1963;31:268–274.
56. Sipp JA, Ashland J, Hartnick CJ. Injectionpharyngoplasty with calcium hydroxyapatitefor treatment of velopalatal insufficiency.Arch Otolaryngol Head Neck Surg. 2008;134:268–271.
57. Funayama E, Igawa HH, Nishizawa N, et al.Velopharyngeal insufficiency in hemifacialmicrosomia: analysis of correlated factors.Otolaryngol Head Neck Surg. 2007;136:33–37.
58. Argamaso RV, Levandowski GJ, Golding-Kushner KJ, et al. Treatment of asymmetricvelopharyngeal insufficiency with skewedpharyngeal flap. Cleft Palate Craniofac J.1994;31:287–294.
59. Armour A, Fischbach S, Klaiman P, et al.Does velopharyngeal closure pattern affectthe success of pharyngeal flap pharyngo-plasty? Plast Reconstr Surg. 2005;115:45–52;discussion 53.
60. Chegar BE, Shprintzen RJ, Curtis MS, et al.Pharyngeal flap and obstructive apnea:maximizing speech outcome while limitingcomplications. Arch Facial Plast Surg.2007;9:252–259.
61. de Serres LM, Deleyiannis FW, Eblen LE,et al. Results with sphincter pharyngoplastyand pharyngeal flap. Int J Pediatr Otorhino-laryngol. 1999;48:17–25.
62. Lendrum J, Dhar BK. The Orticocheadynamic pharyngoplasty. Br J Plast Surg.1984;37:160–168.
63. Meek MF, Coert JH, Hofer SO, et al.Short-term and long-term results of speech
DIAGNOSIS AND TREATMENT OF VELOPHARYNGEAL INSUFFICIENCY 243
16_HartBose_225-244 11/14/09 11:31 AM Page 243

improvement after surgery for velopharyn-geal insufficiency with pharyngeal flaps inpatients younger and older than 6 years old:10-year experience. Ann Plast Surg. 2003;50:13–17.
64. Pryor LS, Lehman J, Parker MG, et al. Out-comes in pharyngoplasty: a 10-year experi-ence. Cleft Palate Craniofac J. 2006;43:222–225.
65. Seagle MB, Mazaheri MK, Dixon-Wood VL,et al. Evaluation and treatment of velopha-ryngeal insufficiency: the University ofFlorida experience. Ann Plast Surg. 2002;48:464–470.
66. Sie KC, Chen EY. Management of velo-pharyngeal insufficiency: development of a protocol and modifications of sphincterpharyngoplasty. Fac Plast Surg. 2007;23:128–139.
67. Sie KC, Tampakopoulou DA, de Serres LM,et al. Sphincter pharyngoplasty: speech out-come and complications. Laryngoscope.1998;108:1211–1217.
68. Abyholm F, D’Antonio L, Davidson Ward SL,et al. Pharyngeal flap and sphincterplasty
for velopharyngeal insufficiency have equaloutcome at 1 year postoperatively: results ofa randomized trial. Cleft Palate Craniofac J.2005;42:501–511.
69. Sloan GM. Posterior pharyngeal flap andsphincter pharyngoplasty: the state of theart. Cleft Palate Craniofac J. 2000;37:112–122.
70. Kravath RE, Pollak CP, Borowiecki B, et al.Obstructive sleep apnea and death associatedwith surgical correction of velopharyngealincompetence. J Pediatr. 1980;96:645–648.
71. Sato-Wakabayashi M, Inoue-Arai MS, Ono T,et al. Combined fMRI and MRI movie in theevaluation of articulation in subjects withand without cleft lip and palate. Cleft PalateCraniofac J. 2008;45:309–314.
72. Ragab A. Cerclage sphincter pharyngoplasty:a new technique for velopharyngeal insuffi-ciency. Int J Pediatr Otorhinolaryngol.2007;71:793–800.
73. Abdel-Aziz M. Palatopharyngeal sling: a newtechnique in treatment of velopharyngealinsufficiency. Int J Pediatr Otorhinolaryn-gol. 2008;72:173–177.
244 CLINICAL MANAGEMENT OF CHILDREN’S VOICE DISORDERS
16_HartBose_225-244 11/14/09 11:31 AM Page 244



![Videofluoroscopic Swallowing Studies[1]](https://static.fdocuments.net/doc/165x107/577cc0d51a28aba711914509/videofluoroscopic-swallowing-studies1.jpg)














