
Diagnosis and Treatment of Hepatocellular...
12
Diagnosis and Treatment of Hepatocellular Carcinoma Hashem B. El–Serag* Jorge A. Marrero ‡ Lenhard Rudolph K. Rajender Reddy § *Section of Gastroenterology and Hepatology, Baylor College of Medicine, Houston, Texas; ‡ Division of Gastroenterology, University of Michigan, Ann Arbor, Michigan; and § Division of Gastroenterology and Hepatology, University of Pennsylvania, Philadelphia, Pennsylvania and Institute of Molecular Medicine and Max- Planck-Research Group on Stem Cell Aging, University of Ulm, Ulm, Germany The diagnosis and treatment of hepatocellular carci- noma (HCC) have witnessed major changes over the past decade. Until the early 1990s, HCC was a rela- tively rare malignancy, typically diagnosed at an ad- vanced stage in a symptomatic patient, and there were no known effective palliative or therapeutic options. However, the rising incidence of HCC in several re- gions around the world coupled with emerging evi- dence for efficacy of screening in high-risk patients, liver transplantation as a curative option in select patients, ability to make definitive diagnosis using high-resolution imaging of the liver, less dependency on obtaining tissue diagnosis, and proven efficacy of transarterial chemoembolization and sorafenib as palliative therapy have improved the outlook for HCC patients. In this article, we present a summary of the most recent information on screening, diagnosis, staging, and different treatment modalities of HCC, as well as our recommended management approach. Diagnosis of Hepatocellular Carcinoma C irrhosis is the strongest and the most common known risk factor for hepatocellular carcinoma (HCC), particularly cirrhosis related to hepatitis C virus (HCV) and hepatitis B virus (HBV) infections. 1–3 In addi- tion, HBV acquired in the perinatal period and early childhood is associated with increased risk of HCC even in the absence of cirrhosis. Clinical Features Patients with HCC present with one or more of several clinical features including right upper quadrant pain, weight loss, and/or worsening liver enzymes in a patient known to have cirrhosis. Rare presenting features include acute abdominal catastrophe from rupture of HCC with intraabdominal bleeding or extra hepatic man- ifestations (eg, hypercalcemia, hypoglycemia, thyrotoxi- cosis). 4,5 Anemia is present in more than half of cases, although rarely erythrocytosis can be seen because of extrarenal synthesis of erythropoeitin. 6 In addition to signs of cirrhosis (eg, jaundice, palmar erythema, gyneco- mastia) and portal hypertension (eg, ascites, varices), a hepatic bruit could be detected in 10%–20% of patients with HCC. 7 With the increased awareness of HCC, more asymptomatic patients are being diagnosed as part of active surveillance. Unfortunately, the majority of pa- tients still presents with signs and symptoms suggestive of liver decompensation and/or tumor spread. HCC Screening HCC screening is recommended in high-risk pa- tients (Table 1). In a randomized controlled trial of nearly 19,000 HBV-infected patients in China, it was shown that HCC surveillance with testing of serum -fetoprotein (AFP) and performance of abdominal ultrasound (US) at repeated 6-month intervals improves survival. 8,9 Al- though adherence to surveillance was relatively low (60%), a 37% reduction in HCC-related mortality was reported. A similar, randomized clinical trial study in China, however, reported that surveillance for HCC is not beneficial in the absence of curative therapies after the cancer was diagnosed. 10 In addition, several nonrandom- ized trials, as well as observational studies, have observed a survival benefit in those identified with small and early tumors. 11 AFP and liver US are the most widely used tools for HCC surveillance. Based on the estimated HCC doubling time, the recommended surveillance interval is 6 months, Abbreviations used in this paper: AFP, -fetoprotein; HCC, hepato- cellular carcinoma; BCLC, Barcelona-Clinic Liver Cancer; CTP, Child- Turcotte-Pugh; LDLT, living donor liver transplantation; OTL, orthotopic liver transplantation; PEI, percutaneous ethanol injection; RFA, radio- frequency ablation; TACE, transarterial chemoembolization; UNOS, United Network for Organ Sharing; US, ultrasound. © 2008 by the AGA Institute 0016-5085/08/$34.00 doi:10.1053/j.gastro.2008.02.090 GASTROENTEROLOGY 2008;134:1752–1763
Transcript of Diagnosis and Treatment of Hepatocellular...

D
*MP
TnptvnHgdlphotpHtsa
C((tci
sppiHic
GASTROENTEROLOGY 2008;134:1752–1763
iagnosis and Treatment of Hepatocellular Carcinoma
Hashem B. El–Serag* Jorge A. Marrero‡ Lenhard Rudolph� K. Rajender Reddy§
Section of Gastroenterology and Hepatology, Baylor College of Medicine, Houston, Texas; ‡Division of Gastroenterology, University of Michigan, Ann Arbor,ichigan; and §Division of Gastroenterology and Hepatology, University of Pennsylvania, Philadelphia, Pennsylvania and �Institute of Molecular Medicine and Max-
lanck-Research Group on Stem Cell Aging, University of Ulm, Ulm, Germanyaesmhwaato
t1H(rt(rCbciat
Ht
cTlfU
he diagnosis and treatment of hepatocellular carci-oma (HCC) have witnessed major changes over theast decade. Until the early 1990s, HCC was a rela-
ively rare malignancy, typically diagnosed at an ad-anced stage in a symptomatic patient, and there wereo known effective palliative or therapeutic options.owever, the rising incidence of HCC in several re-
ions around the world coupled with emerging evi-ence for efficacy of screening in high-risk patients,
iver transplantation as a curative option in selectatients, ability to make definitive diagnosis usingigh-resolution imaging of the liver, less dependencyn obtaining tissue diagnosis, and proven efficacy ofransarterial chemoembolization and sorafenib asalliative therapy have improved the outlook forCC patients. In this article, we present a summary of
he most recent information on screening, diagnosis,taging, and different treatment modalities of HCC,s well as our recommended management approach.
Diagnosis of Hepatocellular Carcinomairrhosis is the strongest and the most commonknown risk factor for hepatocellular carcinoma
HCC), particularly cirrhosis related to hepatitis C virusHCV) and hepatitis B virus (HBV) infections.1–3 In addi-ion, HBV acquired in the perinatal period and earlyhildhood is associated with increased risk of HCC evenn the absence of cirrhosis.
Clinical FeaturesPatients with HCC present with one or more of
everal clinical features including right upper quadrantain, weight loss, and/or worsening liver enzymes in aatient known to have cirrhosis. Rare presenting features
nclude acute abdominal catastrophe from rupture ofCC with intraabdominal bleeding or extra hepatic man-
festations (eg, hypercalcemia, hypoglycemia, thyrotoxi-
osis).4,5 Anemia is present in more than half of cases,lthough rarely erythrocytosis can be seen because ofxtrarenal synthesis of erythropoeitin.6 In addition toigns of cirrhosis (eg, jaundice, palmar erythema, gyneco-
astia) and portal hypertension (eg, ascites, varices), aepatic bruit could be detected in 10%–20% of patientsith HCC.7 With the increased awareness of HCC, moresymptomatic patients are being diagnosed as part ofctive surveillance. Unfortunately, the majority of pa-ients still presents with signs and symptoms suggestivef liver decompensation and/or tumor spread.
HCC ScreeningHCC screening is recommended in high-risk pa-
ients (Table 1). In a randomized controlled trial of nearly9,000 HBV-infected patients in China, it was shown thatCC surveillance with testing of serum �-fetoprotein
AFP) and performance of abdominal ultrasound (US) atepeated 6-month intervals improves survival.8,9 Al-hough adherence to surveillance was relatively low�60%), a 37% reduction in HCC-related mortality waseported. A similar, randomized clinical trial study inhina, however, reported that surveillance for HCC is noteneficial in the absence of curative therapies after theancer was diagnosed.10 In addition, several nonrandom-zed trials, as well as observational studies, have observed
survival benefit in those identified with small and earlyumors.11
AFP and liver US are the most widely used tools forCC surveillance. Based on the estimated HCC doubling
ime, the recommended surveillance interval is 6 months,
Abbreviations used in this paper: AFP, �-fetoprotein; HCC, hepato-ellular carcinoma; BCLC, Barcelona-Clinic Liver Cancer; CTP, Child-urcotte-Pugh; LDLT, living donor liver transplantation; OTL, orthotopiciver transplantation; PEI, percutaneous ethanol injection; RFA, radio-requency ablation; TACE, transarterial chemoembolization; UNOS,nited Network for Organ Sharing; US, ultrasound.
© 2008 by the AGA Institute0016-5085/08/$34.00
doi:10.1053/j.gastro.2008.02.090

aTepssuAoiseeacat
utgcgsdtwpet
6papsy
c
ithmasfnbthdai7anb4Mgipapat
hslbpn
oiatoewfamb
wcpaov
T
H
N
May 2008 DIAGNOSIS AND TREATMENT OF HCC 1753
lthough a 1-year interval may be equally effective.8,12,13
he performance of US depends on the experience of thexaminer, the technology used, the body habitus, theresence of cirrhosis, and the size of the tumor. Recenttudies generally indicate a �60% sensitivity, and �90%pecificity.14 The sensitivity of US to detect tumor nod-les in cirrhotic livers is particularly low.15–17 The serumFP level of 20 ng/mL commonly used as the upper limitf normal18,19 has low sensitivity (25% to 65%) for detect-
ng HCC and is therefore considered inadequate as theole screening test. Patients with chronic liver disease,specially those with a high degree of hepatocyte regen-ration (eg, HCV), can express elevated serum AFP in thebsence of malignancy.20,21 Other tests such as des-�arboxy prothrombin and lectin-bound AFP (AFP-L3) arevailable, but there are no reliable prospective data onheir effectiveness in HCC screening.
The cost-effectiveness of HCC surveillance strategiessing both AFP and US have been evaluated in retrospec-ive studies as well as mathematical models,1,8 –10,14 andenerally reported surveillance for HCC in patients withompensated cirrhosis might be associated with a modestain in quality adjusted life years at acceptable costs. Onetudy also reported that the effectiveness of surveillanceepends mostly on the outcomes and costs of HCCreatments.22 In patients undergoing HCC screeninghile awaiting liver transplantation, screening with com-uterized tomography (CT) is associated with the great-st gain in life expectancy and is possibly cost-effective inhis setting.23
Therefore, current guidelines advocate the use of US at–12 months frequency to screen for HCC in high-riskatients. The use of AFP alone is strongly discouraged,nd its use in addition to US is controversial. High-riskatients include virtually all patients with cirrhosis andome HBV-infected patients irrespective of cirrhosis (�40ears in men and �50 years in women).8
Diagnostic ImagingOnce a screening test is abnormal or there is a
able 1. Groups in Whom HCC Screening and SurveillanceIs Recommended
epatitis B carriers (HBsAg positive)Asian males �40 yAsian females �50 yAll cirrhotic hepatitis B carriersFamily history of HCCAfricans over age 20 y
onhepatitis B cirrhosisHepatitis CAlcoholic cirrhosisGenetic hemochromatosisPrimary biliary cirrhosisPossibly: �1-antitrypsin deficiency, nonalcoholic steatohepatitis,
autoimmune hepatitis
linical suspicion that a patient may have HCC, imaging s
s very important for the diagnosis and staging of thisumor. The most reliable diagnostic tests are triple-phaseelical CT and triple-phase dynamic contrast enhancedagnetic resonance imaging (MRI),24,25 whereas hepatic
ngiography has fallen out of favor in most practiceettings. HCC derives its blood supply predominantlyrom the hepatic artery, whereas the remainder of theontumorous liver receives both arterial and portallood. The hallmark of HCC during CT scan or MRI ishe presence of arterial enhancement followed by delayedypointensity of the tumor in the portal venous andelayed phases, ie, washout26 (Figure 1). The presence ofrterial enhancement followed by washout has a sensitiv-ty and specificity of 90% and 95%, respectively. However,1% of patients with HCC will have arterial enhancementnd washout on more than one test, whereas the rest doot have these features and, therefore, will require liveriopsy for the diagnosis of HCC. There have been at leaststudies that have compared the accuracy of CT andRI for HCC diagnosis, using the explanted liver as the
old standard.27–30 These show that MRI is slightly bettern the characterization and diagnosis of HCC when com-ared with CT scan (Table 2). The performance of CTnd MRI is affected by the size of the lesions. For exam-le, in tumors larger than 2 cm, MRI is reported to haven accuracy �90%; however, in tumors smaller than 2 cm,his level is reduced to 33%.31
Currently, AFP serum levels above 200 ng/mL areighly specific for HCC diagnosis in patients with cirrho-is and coinciding radiologic evidence of focal hepaticesions.8 However, the sensitivity of AFP is much lowerecause it has been reported that only one third ofatients with HCC have AFP levels higher than 100g/mL.32,33
Diagnostic Approach to HCCA diagnostic approach to HCC has been devel-
ped based on the literature and expert consensus andncorporates serology, cytohistology, and radiologic char-cteristics.8,34 Diagnosis of HCC can be confidently es-ablished if (1) a focal hepatic mass �2 cm is identifiedn one imaging technique wherein characteristic contrastnhancement features on the arterial phase with venousashout on an MRI or CT can be demonstrated; (2) a
ocal hepatic mass with atypical imaging findings (norterial enhancement with washout), or a focal hepaticass detected in a noncirrhotic liver, should undergo a
iopsy.Noninvasive diagnosis of HCC is best limited to patients
ith cirrhosis and to patients with a focal hepatic mass �2m. On the other hand, the recommended diagnostic ap-roach for tumors �2 cm or tumors that do not meetbove criteria8 is such that (1), when nodules within 1–2 cmn screening of a cirrhotic liver are typical of HCC (hyper-ascular with washout) on 2 imaging modalities, the lesion
hould be treated as HCC. In an atypical lesion where the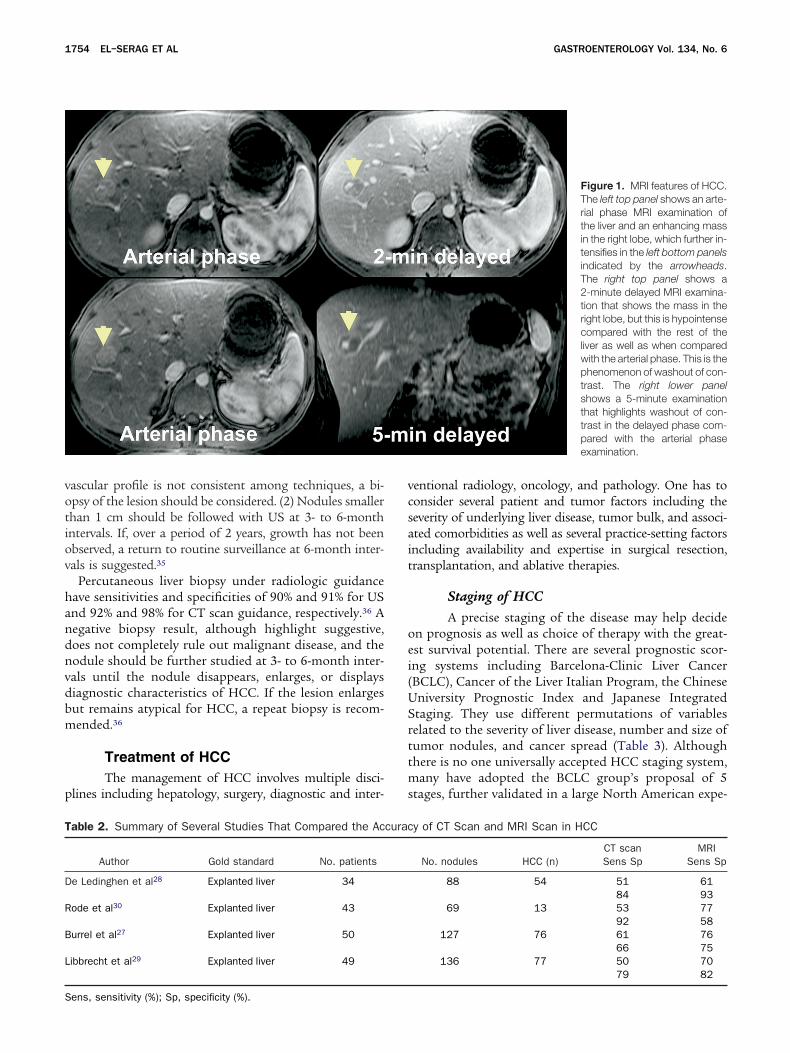
votiov
handnvdbm
p
vcsait
oei(USrttms
T
D
R
B
L
S
1754 EL–SERAG ET AL GASTROENTEROLOGY Vol. 134, No. 6
ascular profile is not consistent among techniques, a bi-psy of the lesion should be considered. (2) Nodules smallerhan 1 cm should be followed with US at 3- to 6-monthntervals. If, over a period of 2 years, growth has not beenbserved, a return to routine surveillance at 6-month inter-als is suggested.35
Percutaneous liver biopsy under radiologic guidanceave sensitivities and specificities of 90% and 91% for USnd 92% and 98% for CT scan guidance, respectively.36 Aegative biopsy result, although highlight suggestive,oes not completely rule out malignant disease, and theodule should be further studied at 3- to 6-month inter-als until the nodule disappears, enlarges, or displaysiagnostic characteristics of HCC. If the lesion enlargesut remains atypical for HCC, a repeat biopsy is recom-ended.36
Treatment of HCCThe management of HCC involves multiple disci-
lines including hepatology, surgery, diagnostic and inter-
able 2. Summary of Several Studies That Compared the Ac
Author Gold standard No. patients
e Ledinghen et al28 Explanted liver 34
ode et al30 Explanted liver 43
urrel et al27 Explanted liver 50
ibbrecht et al29 Explanted liver 49
ens, sensitivity (%); Sp, specificity (%).
entional radiology, oncology, and pathology. One has toonsider several patient and tumor factors including theeverity of underlying liver disease, tumor bulk, and associ-ted comorbidities as well as several practice-setting factorsncluding availability and expertise in surgical resection,ransplantation, and ablative therapies.
Staging of HCCA precise staging of the disease may help decide
n prognosis as well as choice of therapy with the great-st survival potential. There are several prognostic scor-ng systems including Barcelona-Clinic Liver CancerBCLC), Cancer of the Liver Italian Program, the Chineseniversity Prognostic Index and Japanese Integratedtaging. They use different permutations of variableselated to the severity of liver disease, number and size ofumor nodules, and cancer spread (Table 3). Althoughhere is no one universally accepted HCC staging system,
any have adopted the BCLC group’s proposal of 5tages, further validated in a large North American expe-
Figure 1. MRI features of HCC.The left top panel shows an arte-rial phase MRI examination ofthe liver and an enhancing massin the right lobe, which further in-tensifies in the left bottom panelsindicated by the arrowheads.The right top panel shows a2-minute delayed MRI examina-tion that shows the mass in theright lobe, but this is hypointensecompared with the rest of theliver as well as when comparedwith the arterial phase. This is thephenomenon of washout of con-trast. The right lower panelshows a 5-minute examinationthat highlights washout of con-trast in the delayed phase com-pared with the arterial phaseexamination.
y of CT Scan and MRI Scan in HCC
No. nodules HCC (n)CT scanSens Sp
MRISens Sp
88 54 51 6184 93
69 13 53 7792 58
127 76 61 7666 75
136 77 50 7079 82
curac

rclastaprttimiiwtsup
caHwCtdste
ltettfis
T
TABS
EBPAA
Cra
b ints o
May 2008 DIAGNOSIS AND TREATMENT OF HCC 1755
ience.37,38 The BCLC staging and prognostic system ac-ounts for variables related to tumor stage, physical andiver functional status, and cancer-related symptoms andlso provides a link to a treatment algorithm. Patients intage A can undergo resection, transplantation, or abla-ion. Child–Turcotte–Pugh (CTP) class, which providesn assessment of the synthetic function, may serve com-lementary to the BCLC staging in providing a moreefined treatment algorithm.39 The Okuda classificationakes into account radiologic tumor size and liver func-ion (ascites, total serum bilirubin, and serum albumin)s helpful in identifying patients with advanced HCC but
ay be less adequate for staging patients with early orntermediate stage disease. Another commonly used stag-ng system is the Cancer of the Liver Italian Program,21,40
hich uses a mathematical score based on the CTP,umor morphology, AFP, and presence of vascular inva-ion; however, it does not adequately assess populationsndergoing radical therapies, such as resection or trans-
able 3. Several Commonly Used Staging Systems for HCC
Okuda
Negative:
umor size �50% of liverscites Absentilirubin �3 mg/dLerum albumin �3 g/dL
Child–Turco
1 Point: 2 P
ncephalopathy None Grailirubin (mg/dL) �2 2T/INR �1.7 1.71scites None Conlbumin (g/L) �35 28
BCLC Staging and corr
Stage: PS: Tumor stage:
A1 0 SingleA2 0 SingleA3 0 SingleA4 0 3 � �3 cmB 0 �5 cm or multinodularC 1–2 Vascular invasionD 3–4 Any stage
CLIP
Points: CTP: Tumor morph
0 A Uninodular �501 B Multinodular �502 C Massive �50%
LIP, Cancer of the Liver Italian Program; PH, portal hypertension; PSatio.Median survival without therapy: Stage I: 8.3 years, Stage II: 2 yearThe median survival is 36, 22, 9, 7, and 3 months for total CLIP po
lantation. m
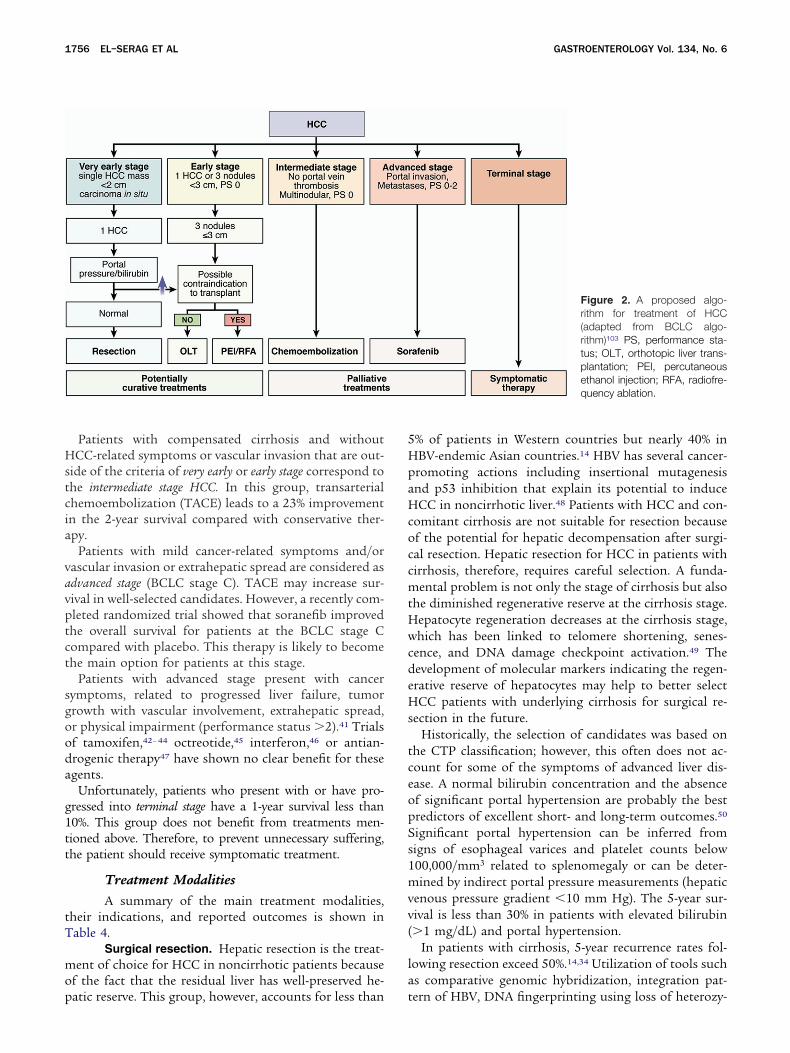
Despite some degree of overlap, several stages of HCCan be identified, and each has different clinical featuress well as treatment and prognosis (Figure 2). Very earlyCC is currently very difficult to diagnose, presentingith a single HCC lesion �2 cm. Affected patients haveTP class A, display no signs or symptoms, and the
umor displays no vascular invasion. Resection and ra-iofrequency ablation (RFA) likely offer similar 5-yearurvival rates. The choice of therapy depends on theumor location, degree of portal hypertension, and pres-nce of medical comorbidities.
Patients presenting as early stage HCC exhibit preservediver function (CTP A and B) with a solitary HCC or upo 3 nodules, each �3 cm in size. These patients can beffectively treated by resection, liver transplantation (or-hotopic liver transplantation [OLT]), or ablation withhe possibility of long-term cure, with 5-year survivalgures up to 75%. The choice of therapy is dictated by theeverity of the liver function, portal hypertension, and
ginga
Positive: Stage:
�50% of liver I: No positive factorsPresent II: 1–2 positive factors
�3 mg/dL III: 3–4 positive factors�3 g/dL
ugh (CTP)
: 3 Points: Class:
II Grade III–IV A 5–6 pts�3 B 7–9 pts
0 �2.20 C 10–15 ptsd Refractory
�28
n with Okuda Staging
da: pH: Bilirubin: Classification:
I No Normal Very earlyI Yes Normal EarlyI Yes AlteredII Yes AlteredII IntermediateII AdvancedII Terminal
ingb
: AFP:Portal vein
thrombosis:
iver �400 ng/dL Noliver �400 ng/dL Yeser
ormance status; PT, prothrombin time; INR, international normalized
ge III: 0.7 years.f 0, 1, 2, 3, and 4 to 6, respectively.
Sta
tte–P
oints
de I––3–2.2trolle–35
elatio
Oku
I–I–I–I
Stag
ology
% of l% ofof liv
, perf
s, Sta
edical comorbidities.
Hstcia
vavptct
sgooda
g1tt
tT
mop
5HpaHcoccmtHwcdeHs
tceopSs1mvv(
la
1756 EL–SERAG ET AL GASTROENTEROLOGY Vol. 134, No. 6
Patients with compensated cirrhosis and withoutCC-related symptoms or vascular invasion that are out-
ide of the criteria of very early or early stage correspond tohe intermediate stage HCC. In this group, transarterialhemoembolization (TACE) leads to a 23% improvementn the 2-year survival compared with conservative ther-py.
Patients with mild cancer-related symptoms and/orascular invasion or extrahepatic spread are considered asdvanced stage (BCLC stage C). TACE may increase sur-ival in well-selected candidates. However, a recently com-leted randomized trial showed that soranefib improvedhe overall survival for patients at the BCLC stage Compared with placebo. This therapy is likely to becomehe main option for patients at this stage.
Patients with advanced stage present with cancerymptoms, related to progressed liver failure, tumorrowth with vascular involvement, extrahepatic spread,r physical impairment (performance status �2).41 Trialsf tamoxifen,42– 44 octreotide,45 interferon,46 or antian-rogenic therapy47 have shown no clear benefit for thesegents.
Unfortunately, patients who present with or have pro-ressed into terminal stage have a 1-year survival less than0%. This group does not benefit from treatments men-ioned above. Therefore, to prevent unnecessary suffering,he patient should receive symptomatic treatment.
Treatment ModalitiesA summary of the main treatment modalities,
heir indications, and reported outcomes is shown inable 4.
Surgical resection. Hepatic resection is the treat-ent of choice for HCC in noncirrhotic patients because
f the fact that the residual liver has well-preserved he-
atic reserve. This group, however, accounts for less than t% of patients in Western countries but nearly 40% inBV-endemic Asian countries.14 HBV has several cancer-romoting actions including insertional mutagenesisnd p53 inhibition that explain its potential to induceCC in noncirrhotic liver.48 Patients with HCC and con-
omitant cirrhosis are not suitable for resection becausef the potential for hepatic decompensation after surgi-al resection. Hepatic resection for HCC in patients withirrhosis, therefore, requires careful selection. A funda-ental problem is not only the stage of cirrhosis but also
he diminished regenerative reserve at the cirrhosis stage.epatocyte regeneration decreases at the cirrhosis stage,hich has been linked to telomere shortening, senes-
ence, and DNA damage checkpoint activation.49 Theevelopment of molecular markers indicating the regen-rative reserve of hepatocytes may help to better selectCC patients with underlying cirrhosis for surgical re-
ection in the future.Historically, the selection of candidates was based on
he CTP classification; however, this often does not ac-ount for some of the symptoms of advanced liver dis-ase. A normal bilirubin concentration and the absencef significant portal hypertension are probably the bestredictors of excellent short- and long-term outcomes.50
ignificant portal hypertension can be inferred fromigns of esophageal varices and platelet counts below00,000/mm3 related to splenomegaly or can be deter-ined by indirect portal pressure measurements (hepatic
enous pressure gradient �10 mm Hg). The 5-year sur-ival is less than 30% in patients with elevated bilirubin�1 mg/dL) and portal hypertension.
In patients with cirrhosis, 5-year recurrence rates fol-owing resection exceed 50%.14,34 Utilization of tools suchs comparative genomic hybridization, integration pat-
Figure 2. A proposed algo-rithm for treatment of HCC(adapted from BCLC algo-rithm)103 PS, performance sta-tus; OLT, orthotopic liver trans-plantation; PEI, percutaneousethanol injection; RFA, radiofre-quency ablation.
ern of HBV, DNA fingerprinting using loss of heterozy-

gttn
rvTeaptSh1tbbracmrw
tsrllm
cilprfallbCsigtH
Sa(eaHtaairpf
T
S
T
R
P
T
NmA
May 2008 DIAGNOSIS AND TREATMENT OF HCC 1757
osity assays, or DNA microarray has allowed researcherso determine that 60% to 70% of recurrences correspondo intrahepatic metastases and that 30% to 40% are deovo tumors.51–53
Several variables affect the risk of recurrence followingesection: these include tumor size, number of tumors,ascular invasion, and the width of the resection margin.he recommended upper limit of tumor size for consid-ration of resection has been argued, noting that there issignificant difference in the 5-year recurrence rates in
atients with tumors �5 cm that is considerably greaterhan those with �5 cm (43% vs 32%, respectively).54
imilarly, multinodular tumors have been determined toave an increased tendency to recur.55 A large study of000 HCC patients reported a 5-year survival after resec-ion of single tumors to be 57% and 3 or more nodules toe 26%.56 Resectable tumor-free margins vary on a case-y-case basis to balance tumor removal to reduce recur-ence with preservation functioning liver parenchyma tollow survival. A recent prospective randomized trialompared wide (�2 cm) and narrow (�1 cm) resectionargins for solitary HCC.57 Although recurrence rates
emained high in both groups, the overall survival ratesere higher for the wide margin group.
Liver transplantation. Liver transplantation, inheory, is the optimal therapeutic option for HCC; itimultaneously removes the tumor and underlying cir-hosis thus minimizing the risk of HCC recurrence. Ear-ier selection criteria for liver transplantation were broad,eading to poor results with recurrence rates of approxi-
able 4. Summary of Therapeutic Modalities for HCC and Th
Treatment Survival
urgical resection 1 y: 97%3 y: 84%5 y: 26%–57%
ransplantation (LT) 1 y: 91%2 y: 75%5 y (MILAN): �70%5 y (extended): �50
adiofrequency ablation (RFA) 1 y: 90%3 y: 74%5 y: 40%–50%
ercutaneous ethanol injection (PEI) 1 y: 85%3 y: 50%5 y: 40%–50%
ransarterial chemoembolization (TACE) 1 y: 82%2 y: 63%
OTE. The 1-year survival rates are reported from different studiesodalities.E, adverse events; OLT, orthotopic liver transplantation.
ately 50% and 5-year survival rates of �40%.58,59 The e
urrently recommended United Network for Organ Shar-ng (UNOS) criteria (1 lesion �5 cm or maximum 3esions �3 cm in diameter) have shown tremendousromise, with reported 5-year survival rates of �70% andecurrence rates of �15%.59 – 61 The tumor burden criteriaor transplantation for HCC as established by the UNOSre largely accepted. Expanded selection criteria (a singleesion of �6.5 cm or up to 3 lesions, none of which arearger than 4.0 cm, with a maximum combined tumorulk of �8.0 cm), have been proposed by University ofalifornia in San Francisco.62 Liver transplantation in
uch candidates has been associated with outcomes sim-lar to those who are within the UNOS criteria. However,iven the large number of HCC cases considered for liverransplantation, the struggle is to keep a balance betweenCC and non-HCC recipients.The UNOS oversees liver allocation in the United
tates. Based on the radiologic diagnosis of the numbernd size of lesions, Model for End-Stage Liver DiseaseMELD) exception points are awarded for HCC, with thexpectation that liver transplantation is accomplished in
reasonable period of time. The exception points forCC are based on the 3-month pretransplantation mor-
ality rates. For solitary lesions �2 cm and �5 cm, as wells up to 3 lesions, each �3 cm, patients currently receiveMELD score of 22, unless their calculated MELD score
s otherwise greater. For each 3-month interval that theyemain on the wait list, a greater number of exceptionoints are awarded based on an expected increase of 10%or the 3-month pretransplantation mortality rate (eg,
utcomes
Special issues
Choice of therapy for patients without cirrhosis (low morbidity)5%–15% of HCC patients eligibleRight hepatectomy has higher risk than left hepatectomyPre/postresection adjunct therapy not recommendedCurative treatment for chronic disease and HCCMELD exception points for HCCEffective corresponding to UNOS criteria (1 tumor �5 cm; up
to 3 tumors �3 cmLiver donor LT considered for HCC progression outside MILAN
criteriaUCSF criteria not implemented in current MELD exception
allocation policyEffect is more predictable in all tumor sizes than following PEISuperior to PEI in larger tumors; equivalent in small tumorsRequires fewer treatment sessionsEarly HCC patients not suitable to resection or OLT or RFA not
available or contraindicatedHighly effective for small HCC (�2 cm)Low rate of AEsNonsurgical patients with large/multifocal HCC w/o vascular
invasion or extrahepatic spread
thus may not be used to compare directly the different therapeutic
eir O
%
and
xtension No. 1: 25 points for 25% mortality; extension
NeetHtft
cDdhacTetpnOaiop
ststaameirttitttTi
cfrmOaa
ta
Hctacfworsnat
c3se
P5irLa4rpttrty4gbtdlamcspOm
tnrrRwr
1758 EL–SERAG ET AL GASTROENTEROLOGY Vol. 134, No. 6
o. 2: 28 points for 35% mortality, . . .). The challengesncountered in HCC pertain to the degree of MELDxception points that should be assigned to HCC pa-ients so that the number of transplantations done forCC patients are reasonable relative to other indications,
hat there is an acceptable and comparable mortalityrom all indications while awaiting transplantation, andhat the outcomes are similar after transplantation.
The role of downstaging of tumors that are outside ofonventional UNOS criteria for OLT has been explored.ownstaging is HCC-directed therapy that aims at re-ucing the size and/or number of HCC lesions. Studiesave shown that successful tumor downstaging can bechieved in up to 70% of the patients treated in a proto-ol with one or more therapeutic modalities includingACE, radiofrequency ablation (RFA), or percutaneousthanol injection (PEI). Subsequently, successful liverransplantation was accomplished in nearly half of theseatients.63,64 Although encouraging, longer follow-up iseeded to assess further the risk of HCC recurrence afterLT before downstaging can be recommended and
dopted. The role of salvage liver transplantation afternitial resection of HCC is less clear. Overall, suboptimalutcomes have been observed with this strategy com-ared with primary liver transplantation for HCC.65
Given the shortage of donors and in attempts tohorten the waiting time for cadaveric liver transplanta-ion, living donor liver transplantation (LDLT) has beenhown to be an alternative to cadaveric liver transplanta-ion, with approximately 3000 cases done worldwide forll indications. LDLT is a complex procedure that isssociated with a morbidity of 20%– 40% and a donorortality of 0.3%– 0.5%.66,67 With that, consideration of
thical, societal, and legal issues are vital to successfulmplementation of LDLT for HCC treatment. A recentetrospective analysis of a United States experience notedhat the disease-free survival following LDLT was lowerhan that of cadaveric liver transplantation. LDLT recip-ents had a higher rate of HCC recurrence within 3 yearshan deceased donor OLT recipients, 30% vs 0%, respec-ively. However, there was no difference in mortality orhe combined outcome of mortality or recurrence.68
hus, the role of LDLT, particularly for those outside ofdeal criteria, needs further evaluation.
Percutaneous ablation. Minimally invasive per-utaneous treatments are the best treatment alternativesor early HCC patients who are not eligible for surgicalesection or transplantation. The most widely utilized
ethods to induce tumor necrosis are PEI and RFA.ther, less utilized methods include the injection of
cetic acid, boiling saline, cryotherapy, microwave ther-py, and laser therapy.8,58,69
PEI consists of injecting absolute ethanol directly intohe HCC lesions. PEI performed under US guidance
chieves complete tumor necrosis in 70%– 80% of solitary aCC �3 cm24 and in almost 100% in tumors less than 2m. Tumor necrosis is less likely to be achieved in largeumors; 70% necrosis is reported for tumors between 2nd 3 cm and 50% necrosis for HCC between 3 and 5m.70 –72 It is a well-tolerated, inexpensive procedure withew adverse effects. In nonrandomized studies of patientsith small HCC, PEI has been shown to carry the sameverall survival and recurrence-free survival as surgicalesection.73,74 In a large series of 3225 patients witholitary tumors �3 cm reported by Ryu et al,75 there wereo significant differences in survival between resectionnd PEI. The best survival for PEI has been shown forumors �3 cm and �3 lesions.75
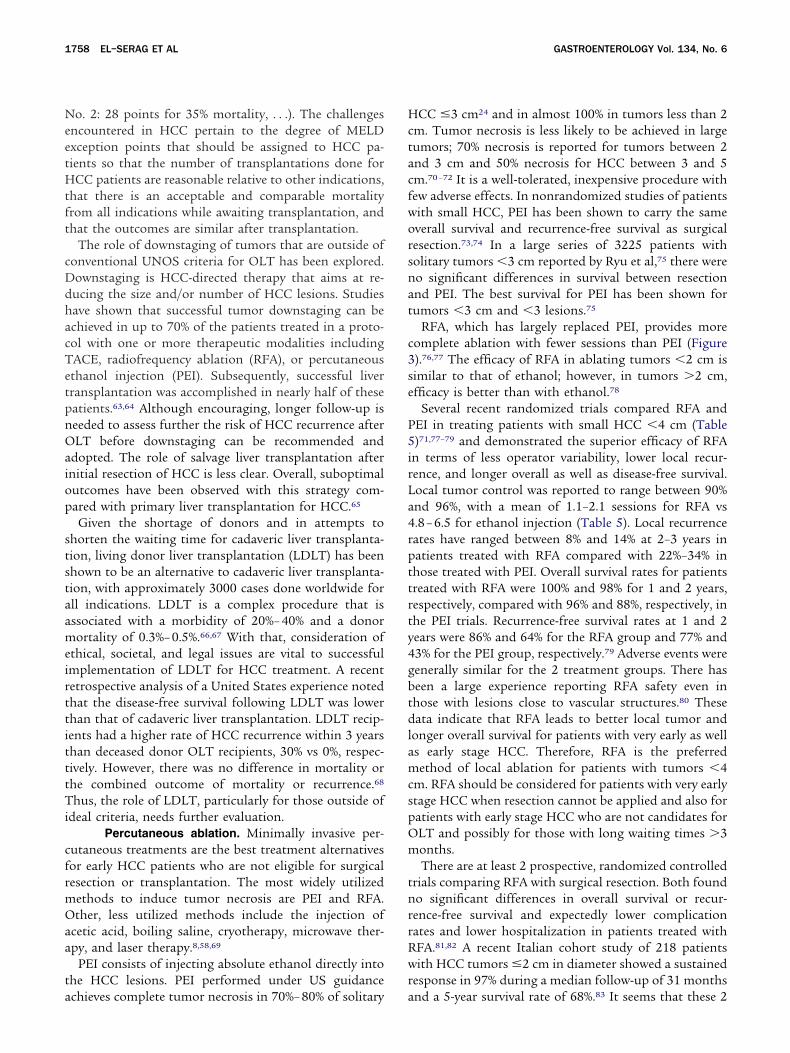
RFA, which has largely replaced PEI, provides moreomplete ablation with fewer sessions than PEI (Figure).76,77 The efficacy of RFA in ablating tumors �2 cm isimilar to that of ethanol; however, in tumors �2 cm,fficacy is better than with ethanol.78
Several recent randomized trials compared RFA andEI in treating patients with small HCC �4 cm (Table)71,77–79 and demonstrated the superior efficacy of RFA
n terms of less operator variability, lower local recur-ence, and longer overall as well as disease-free survival.ocal tumor control was reported to range between 90%nd 96%, with a mean of 1.1–2.1 sessions for RFA vs.8 – 6.5 for ethanol injection (Table 5). Local recurrenceates have ranged between 8% and 14% at 2–3 years inatients treated with RFA compared with 22%–34% inhose treated with PEI. Overall survival rates for patientsreated with RFA were 100% and 98% for 1 and 2 years,espectively, compared with 96% and 88%, respectively, inhe PEI trials. Recurrence-free survival rates at 1 and 2ears were 86% and 64% for the RFA group and 77% and3% for the PEI group, respectively.79 Adverse events wereenerally similar for the 2 treatment groups. There haseen a large experience reporting RFA safety even inhose with lesions close to vascular structures.80 Theseata indicate that RFA leads to better local tumor and
onger overall survival for patients with very early as wells early stage HCC. Therefore, RFA is the preferredethod of local ablation for patients with tumors �4
m. RFA should be considered for patients with very earlytage HCC when resection cannot be applied and also foratients with early stage HCC who are not candidates forLT and possibly for those with long waiting times �3onths.There are at least 2 prospective, randomized controlled
rials comparing RFA with surgical resection. Both foundo significant differences in overall survival or recur-ence-free survival and expectedly lower complicationates and lower hospitalization in patients treated withFA.81,82 A recent Italian cohort study of 218 patientsith HCC tumors �2 cm in diameter showed a sustained
esponse in 97% during a median follow-up of 31 months
nd a 5-year survival rate of 68%.83 It seems that these 2
pafpt
TiticwHwsr
1a
nbwda
taratcA
Ft
T
LL
LS
NmP
May 2008 DIAGNOSIS AND TREATMENT OF HCC 1759
rocedures offer similar efficacy, and the choice of ther-py for very early stage HCC should depend on candidacyor surgery in terms of performance status, severity ofortal hypertension, and feasibility of RFA in terms ofumor location.
Transarterial embolization/chemoembolization.ACE may offer palliative benefits for patients with
ntermediate stage HCC with 5-year survival rates afterreatment exceeding 50%. TACE has been shown tomprove survival in patients outside of the early stageriteria, especially in those who have not presentedith cancer-related symptoms or vascular invasion.69
owever, its safe and effective use is limited to patientsith preserved liver function, absence of extrahepatic
pread or vascular invasion, and no significant cancer-elated symptoms. A European study revealed that only
igure 3. Percutaneous abla-ion of HCC using radiofrequency.
able 5. Summary of Several Studies That Compared PEI an
ne
Author N Tumor size PEI
ivraghi et al71 86 �3 cm 80encioni et al79 102 Milan criteria 82
in et al78 157 �4 cm 88hiina et al77 232 Milan criteria
OTE. The 1-year survival rates are reported from different studiesodalities.
EI, percutaneous ethanol injection; RFA, radiofrequency ablation.2% of the 903 patients evaluated for HCC were suit-ble for TACE.84
The basis of embolization is to induce ischemic tumorecrosis via acute arterial occlusion. Embolization maye done alone (transarterial embolization) or combinedith selective intraarterial chemotherapy (TACE) such asoxorubicin, mitomycin, or cisplatin and a contrastgent, lipiodol.
TACE induces extensive tumor necrosis in 30% to upo 50% of those treated patients, but with fewer than 2%chieving a complete response.84 A meta-analysis of 7andomized controlled trials comparing in that meta-nalysis, arterial embolization and/or chemoemboliza-ion as a primary treatment for HCC in comparison withonservative management and/or suboptimal therapies.85
rterial embolization improved 2-year survival compared
A for HCC Treatment
pleterate (%)
Sessions(average number)
RFA PEI RFA Survival difference
90 4.8 1.2 No91 5.4 1.1 Yes
Recurrence free96 6.5 1.6 Yes
A 6.4 2.1 Yes
thus may not be used to compare directly the different therapeutic
d RF
Comcrosis
N
and

w0
wssitTt
atiptpT
ipfciidt
ecitehi
ea
IttG
ceprLhruCp
iv2p1ptsatwcmriirf
�iioadHr
istcut
cwdftecntbU2at4lrv
1760 EL–SERAG ET AL GASTROENTEROLOGY Vol. 134, No. 6
ith that in control subjects (odds ratio, 0.53; 95% CI:.32– 0.89).
In a large, prospective cohort study of 8510 patientsho received TACE for unresectable HCC, the median
urvival was 34 months with 1-, 2-, 3-, 5-, and 7-yearurvivals of 82%, 47%, 26%, and 16%, respectively.86 Theres currently little data to guide the choice of the chemo-herapeutic agent or the retreatment schedule for TACE.he current evidence does not support the use of transar-
erial embolization without chemotherapeutic agent.Transarterial embolization/TACE are associated with
dverse events in approximately 10% of treated patients;hese events include ischemic cholecystitis, nausea, vom-ting, bone marrow depression, and abdominal pain.58 Aostembolization syndrome is reported in �50% of pa-ients treated with TACE and includes fever, abdominalain, and moderate degree of intestinal obstruction.reatment-related mortality is less than 5%.TACE is clearly the first-line therapy for patients at the
ntermediate stage who exceed the criteria for liver trans-lantation (Figure 2). In addition, TACE can be per-ormed in patients at the early stage in whom RFAannot be performed because of tumor location (proxim-ty to a gallbladder, biliary tree, or blood vessel) or med-cal comorbidities. TACE is also the first-line therapy forownstaging tumors that exceed the criteria forransplantation.64
Other options. Radionuclide Yttrium-90, a pure �mitter, is a form of hepatic artery-directed therapy. Mi-rospheres of approximately 25 �m in diameter contain-ng Yttrium-90 are lodged via a catheter insertion intohe lobar or segmental level of either hepatic artery andmit local radiation with limited exposure to adjacentealthy tissue.87 Currently, there are no data to suggest
ts superiority over ablative therapies.
Molecular TherapiesThere are a growing number of clinical studies
valuating the efficacy of molecular therapies in HCC,lone or in combination with classical chemotherapy.
Angiogenesis inhibitors. Several studies (phase I,I, and III) are underway. Positive results have been ob-ained for therapies using Bevacizumab (vascular endo-helial growth factor inhibitor) in combination withemcitabine and Oxalliplatin.
Growth-receptor signaling. Studies have beenonducted targeting platelet-derived growth factor receptor,ndothelial growth factor receptor, Raf, and other signalingathways controlling cell proliferation. Positive results wereeported for the use of Nexavar (Bayer Healthcare AG,everkusen, Germany) (sorafenib), an oral multikinase in-ibitor, in patients with HCC. A phase III double-blind,andomized, placebo-controlled trial was designed to eval-ate Nexavar in patients with advanced HCC (BCLC stage) who had no prior systemic therapy. Six hundred two
atients were randomized and enrolled at sites in the Amer- scas, Europe, and Australia/New Zealand. The overall sur-ival (46.3 weeks, 95% CI: 40.9–57.9, vs 34.4 weeks, 95% CI:9.4–39.4, respectively, P � .058) and time to symptomrogression (24 weeks, 95% CI: 18–30, vs 12 weeks, 95% CI:1.7–17.1, respectively, P � .007) were significantly longer inatients administered Nexavar vs those patients adminis-ered placebo.88 Approximately 83% of the patients in theorafenib trial had portal vein invasion and were classifieds Barcelona stage C, with 20% having extrahepatic metas-ases. The 17% without portal vein invasion were patientsho did not respond to TACE and were classified as Bar-
elona stage B in the study. Most patients had mild tooderate performance status. Therefore, it is reasonable to
ecommend sorafenib for patients with advanced stage orntermediate stage HCC with portal vein thrombosis. Prom-sing results89 on progression-free survival have also beeneported for Erlotinib, an inhibitor of endothelial growthactor receptor signalling.90
Telomerase inhibition. Telomerase is active in90% of human HCC, and it appears to be necessary for the
mmortal proliferation capacity of HCCs.49 Preclinical stud-es show that telomerase inhibition can impair proliferationf human HCC in nude mice.91 Phase I/II clinical studiesre currently underway in patients with lymphoma. In ad-ition to the above approaches, antibody treatment againstCC surface markers have been reported to lower recur-
ence rates after liver transplantation.92
Another important factor to improve future therapiesn HCC is the development of new markers to improvecreening of cirrhosis patients for early lesions,93 selec-ion of HCC patients that could benefit from surgery orhemotherapy,94 –97 or diagnosis of HCC.98 However, thetility of these tests remains unproven and will have to beested in translational and clinical studies.
HCC Treatment: Effectiveness vs EfficacyPopulation-based studies in the United States indi-
ate that the overall 1- and 3-year survival rates for patientsith HCC are approximately 20% and 5%, respectively (me-ian survival of 8 months).99 These figures accommodateor a 20% improvement in survival that was observed be-ween 1987 and 2001. To make a positive impact on theffectiveness of treating HCC, several steps have to be suc-essfully accomplished so that more patients can be diag-osed at an early stage and receive timely potentially cura-ive therapy. However, there seems to be a serious chasmetween efficacy and effectiveness of treatment of HCC.100 Anited States population-based study reported that, in963 patients 65 years and older diagnosed between 1992nd 1999 with HCC, only 13% received potentially curativeherapy (transplant, 0.9%; resection, 8.2%; local ablation,.1%). Furthermore, only 34% of 513 patients with single
esions and 34% of 143 patients with lesions �3.0 cmeceived potentially curative therapy. There were geographicariations in the management of HCC that are at least as
ignificant as clinical and tumor-related features in deter-
mUaHywgpptoPpcTcc
lfp
Hoisoams
May 2008 DIAGNOSIS AND TREATMENT OF HCC 1761
ining the extent and type of HCC therapy.101 Anothernited States population-based study of 1156 patients di-
gnosed between 1998 and 2002 with small nonmetastaticCC in the United States found that liver transplantation
ielded excellent overall survival, but only 21% of patientsith localized HCC received a transplant. Marked geo-raphic and racial variations were seen in the use of trans-lantation for HCC after controlling for other tumor andatient-related variables. For example, 25% of white pa-ients, 21% of Hispanic patients, 17% of Asians patients, andnly 13% of African-American patients received a transplant.atients with HCC were 2.2 times less likely to get a trans-lant in the South and 3.3 times less likely in the Northeastompared with patients in the Western United States.102
ransplantation patients with nonmetastatic HCC have ex-ellent long-term survival, and this has been shown in singleenter as well as population-based studies.
In summary, the evidence indicates marked underuti-ization of these interventions. Underutilization seems toollow some disturbing patterns in relation to ethnicity,overty, and gender.Several steps have to be taken to improve effectiveness of
CC therapy. These include provider and patient educationn risk factors for HCC and methods of diagnosis, increas-
ng the number of patients diagnosed in early or very earlytage by better implementation of screening programs andptimizing screened patients for curative therapy (eg, drugnd alcohol rehabilitation), improving access to specializedultidisciplinary treatment, and utilization of a validated
taging system.
References
1. Chen TH, Chen CJ, Yen MF, et al. Ultrasound screening and riskfactors for death from hepatocellular carcinoma in a high-riskgroup in Taiwan. Int J Cancer 2002;98:257–261.
2. Tsukuma H, Hiyama T, Tanaka S, et al. Risk factors for hepato-cellular carcinoma among patients with chronic liver disease.N Engl J Med 1993;328:1797–1801.
3. Velazquez RF, Rodriguez M, Navascues CA, et al. Prospectiveanalysis of risk factors for hepatocellular carcinoma in patientswith liver cirrhosis. Hepatology 2003;37:520–527.
4. Choi BG, Park SH, Byun JY, et al. The findings of rupturedhepatocellular carcinoma on helical CT. Br J Radiol 2001;74:142–146.
5. Eastman RC, Carson RE, Orloff DG, et al. Glucose utilization ina patient with hepatoma and hypoglycemia. Assessment by apositron emission tomography. J Clin Invest 1992;89:1958–1963.
6. Sakisaka S, Watanabe M, Tateishi H, et al. Erythropoietin pro-duction in hepatocellular carcinoma cells associated with poly-cythemia: immunohistochemical evidence. Hepatology 1993;18:1357–1362.
7. Kew M. Tumors of the liver. In: Zakim D, Boyer T, eds. Hepatol-ogy: A textbook of liver disease. Philadelphia: WB SaundersCompany, 1996:1513.
8. Bruix J, Sherman M. Management of hepatocellular carcinoma.Hepatology 2005;42:1208–1236.
9. Zhang BH, Yang BH, Tang ZY. Randomized controlled trial ofscreening for hepatocellular carcinoma. J Cancer Res Clin Oncol
2004;130:417–422.10. Chen JG, Parkin DM, Chen QG, et al. Screening for liver cancer:results of a randomised controlled trial in Qidong, China. J MedScreen 2003;10:204–209.
11. Wong LL, Limm WM, Severino R, et al. Improved survival withscreening for hepatocellular carcinoma. Liver Transpl 2000;6:320–325.
12. Trevisani F, De NS, Rapaccini G, et al. Semiannual and annualsurveillance of cirrhotic patients for hepatocellular carcinoma:effects on cancer stage and patient survival (Italian experience).Am J Gastroenterol 2002;97:734–744.
13. Zhang B, Yang B. Combined �-fetoprotein testing and ultra-sonography as a screening test for primary liver cancer. J MedScreen 1999;6:108–110.
14. Bolondi L, Sofia S, Siringo S, et al. Surveillance programme ofcirrhotic patients for early diagnosis and treatment of hepato-cellular carcinoma: a cost effectiveness analysis. Gut 2001;48:251–259.
15. Collier J, Sherman M. Screening for hepatocellular carcinoma.Hepatology 1998;27:273–278.
16. Kim CK, Lim JH, Lee WJ. Detection of hepatocellular carcinomasand dysplastic nodules in cirrhotic liver: accuracy of ultrasonog-raphy in transplant patients. J Ultrasound Med 2001;20:99–104.
17. Trevisani F, D’Intino PE, Morselli-Labate AM, et al. Serum �-fe-toprotein for diagnosis of hepatocellular carcinoma in patientswith chronic liver disease: influence of HBsAg and anti-HCVstatus. J Hepatol 2001;34:570–575.
18. Sherman M, Peltekian KM, Lee C. Screening for hepatocellularcarcinoma in chronic carriers of hepatitis B virus: incidence andprevalence of hepatocellular carcinoma in a North Americanurban population. Hepatology 1995;22:432–438.
19. Trevisani F, D’Intino PE, Caraceni P, et al. Etiologic factors andclinical presentation of hepatocellular carcinoma. Differencesbetween cirrhotic and noncirrhotic Italian patients. Cancer1995;75:2220–2232.
20. Bayati N, Silverman AL, Gordon SC. Serum �-fetoprotein levelsand liver histology in patients with chronic hepatitis C. Am JGastroenterol 1998;93:2452–2456.
21. Franca AV, Elias JJ, Lima BL, et al. Diagnosis, staging andtreatment of hepatocellular carcinoma. Braz J Med Biol Res2004;37:1689–1705.
22. Patel D, Terrault NA, Yao FY, et al. Cost-effectiveness of hepa-tocellular carcinoma surveillance in patients with hepatitis Cvirus-related cirrhosis. Clin Gastroenterol Hepatol 2005;3:75–84.
23. Saab S, Ly D, Nieto J, et al. Hepatocellular carcinoma screeningin patients waiting for liver transplantation: a decision analyticmodel. Liver Transpl 2003;9:672–681.
24. Choi D, Kim SH, Lim JH, et al. Detection of hepatocellularcarcinoma: combined T2-weighted and dynamic gadolinium-en-hanced MRI versus combined CT during arterial portography andCT hepatic arteriography. J Comput Assist Tomogr 2001;25:777–785.
25. Arguedas MR, Chen VK, Eloubeidi MA, et al. Screening forhepatocellular carcinoma in patients with hepatitis C cirrhosis:a cost-utility analysis. Am J Gastroenterol 2003;98:679–690.
26. Marrero JA, Hussain HK, Nghiem HV, et al. Improving the predictionof hepatocellular carcinoma in cirrhotic patients with an arterially-enhancing liver mass. Liver Transpl 2005;11:281–289.
27. Burrel M, Llovet JM, Ayuso C, et al. MRI angiography is superiorto helical CT for detection of HCC prior to liver transplantation:an explant correlation. Hepatology 2003;38:1034–1042.
28. de Ledinghen V, Laharie D, Lecesne R, et al. Detection ofnodules in liver cirrhosis: spiral computed tomography or mag-netic resonance imaging? A prospective study of 88 nodules in
34 patients. Eur J Gastroenterol Hepatol 2002;14:159–165.
1762 EL–SERAG ET AL GASTROENTEROLOGY Vol. 134, No. 6
29. Libbrecht L, Bielen D, Verslype C, et al. Focal lesions in cirrhoticexplant livers: pathological evaluation and accuracy of pretrans-plantation imaging examinations. Liver Transpl 2002;8:749–761.
30. Rode A, Bancel B, Douek P, et al. Small nodule detection incirrhotic livers: evaluation with US, spiral CT, and MRI andcorrelation with pathologic examination of explanted liver.J Comput Assist Tomogr 2001;25:327–336.
31. Ebara M, Ohto M, Watanabe Y, et al. Diagnosis of small hepa-tocellular carcinoma: correlation of MR imaging and tumor his-tologic studies. Radiology 1986;159:371–377.
32. Ebara M, Ohto M, Kondo F. Strategy for early diagnosis ofhepatocellular carcinoma (HCC). Ann Acad Med Singapore1989;18:83–89.
33. Torzilli G, Minagawa M, Takayama T, et al. Accurate preopera-tive evaluation of liver mass lesions without fine-needle biopsy.Hepatology 1999;30:889–893.
34. Bruix J, Sherman M, Llovet JM, et al. Clinical management ofhepatocellular carcinoma. Conclusions of the Barcelona-2000EASL conference. European Association for the Study of theLiver. J Hepatol 2001;35:421–430.
35. Byrnes V, Shi H, Kiryu S, et al. The clinical outcome of small(�20 mm) arterially enhancing nodules on MRI in the cirrhoticliver. Am J Gastroenterol 2007;102:1654–1659.
36. Durand F, Regimbeau JM, Belghiti J, et al. Assessment of thebenefits and risks of percutaneous biopsy before surgical resec-tion of hepatocellular carcinoma. J Hepatol 2001;35:254–258.
37. Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma:the BCLC staging classification. Semin Liver Dis 1999;19:329–338.
38. Marrero JA, Fontana RJ, Barrat A, et al. Prognosis of hepatocel-lular carcinoma: comparison of 7 staging systems in an Ameri-can cohort. Hepatology 2005;41:707–716.
39. Levy I, Sherman M. Staging of hepatocellular carcinoma: as-sessment of the CLIP, Okuda, and Child-Pugh staging systemsin a cohort of 257 patients in Toronto. Gut 2002;50:881–885.
40. Prospective validation of the CLIP score: a new prognostic sys-tem for patients with cirrhosis and hepatocellular carcinoma.The Cancer of the Liver Italian Program (CLIP) Investigators.Hepatology 2000;31:840–845.
41. Conill C, Verger E, Salamero M. Performance status assess-ment in cancer patients. Cancer 1990;65:1864–1866.
42. Tamoxifen in treatment of hepatocellular carcinoma: a random-ised controlled trial. CLIP Group (Cancer of the Liver ItalianProgramme). Lancet 1998;352:17–20.
43. Castells A, Bruix J, Bru C, et al. Treatment of hepatocellularcarcinoma with tamoxifen: a double-blind placebo-controlledtrial in 120 patients. Gastroenterology 1995;109:917–922.
44. Farinati F. Tamoxifen treatment in hepatocellular carcinoma.Gastroenterology 1996;111:272–274.
45. Yuen MF, Poon RT, Lai CL, et al. A randomized placebo-con-trolled study of long-acting octreotide for the treatment of ad-vanced hepatocellular carcinoma. Hepatology 2002;36:687–691.
46. Llovet JM, Sala M, Castells L, et al. Randomized controlled trialof interferon treatment for advanced hepatocellular carcinoma.Hepatology 2000;31:54–58.
47. Grimaldi C, Bleiberg H, Gay F, et al. Evaluation of antiandrogentherapy in unresectable hepatocellular carcinoma: results of aEuropean Organization for Research and Treatment of Cancermulticentric double-blind trial. J Clin Oncol 1998;16:411–417.
48. Dewantoro O, Gani RA, Akbar N. Hepatocarcinogenesis in viralhepatitis B infection: the role of HBx and p53. Acta Med Indones2006;38:154–159.
49. El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiol-ogy and molecular carcinogenesis. Gastroenterology 2007;132:
2557–2576.50. Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgicaltreatment for early hepatocellular carcinoma: resection versustransplantation. Hepatology 1999;30:1434–1440.
51. Chen YJ, Yeh SH, Chen JT, et al. Chromosomal changes andclonality relationship between primary and recurrent hepatocel-lular carcinoma. Gastroenterology 2000;119:431–440.
52. Finkelstein SD, Marsh W, Demetris AJ, et al. Microdissection-based allelotyping discriminates de novo tumor from intrahe-patic spread in hepatocellular carcinoma. Hepatology 2003;37:871–879.
53. Ng IO, Guan XY, Poon RT, et al. Determination of the molecularrelationship between multiple tumour nodules in hepatocellularcarcinoma differentiates multicentric origin from intrahepaticmetastasis. J Pathol 2003;199:345–353.
54. Vauthey JN, Lauwers GY, Esnaola NF, et al. Simplified stagingfor hepatocellular carcinoma. J Clin Oncol 2002;20:1527–1536.
55. Zhou XD, Tang ZY, Yang BH, et al. Experience of 1000 patientswho underwent hepatectomy for small hepatocellular carci-noma. Cancer 2001;91:1479–1486.
56. Ikai I, Arii S, Kojiro M, et al. Reevaluation of prognostic factorsfor survival after liver resection in patients with hepatocellularcarcinoma in a Japanese nationwide survey. Cancer 2004;101:796–802.
57. Shi M, Guo RP, Lin XJ, et al. Partial hepatectomy with wideversus narrow resection margin for solitary hepatocellular car-cinoma: a prospective randomized trial. Ann Surg 2007;245:36–43.
58. Bruix J, Hessheimer AJ, Forner A, et al. New aspects of diagno-sis and therapy of hepatocellular carcinoma. Oncogene 2006;25:3848–3856.
59. Sala M, Varela M, Bruix J. Selection of candidates with HCC fortransplantation in the MELD era. Liver Transpl 2004;10(Suppl2):S4–S9.
60. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation forthe treatment of small hepatocellular carcinomas in patientswith cirrhosis. N Engl J Med 1996;334:693–699.
61. Shetty K, Timmins K, Brensinger C, et al. Liver transplantationfor hepatocellular carcinoma validation of present selectioncriteria in predicting outcome. Liver Transpl 2004;10:911–918.
62. Yao FY, Ferrell L, Bass NM, et al. Liver transplantation forhepatocellular carcinoma: expansion of the tumor size limitsdoes not adversely impact survival. Hepatology 2001;33:1394–1403.
63. Margarit C, Escartin A, Castells L, et al. Resection for hepato-cellular carcinoma is a good option in Child-Turcotte-Pugh classA patients with cirrhosis who are eligible for liver transplanta-tion. Liver Transpl 2005;11:1242–1251.
64. Yao FY, Hirose R, LaBerge JM, et al. A prospective study ondownstaging of hepatocellular carcinoma prior to liver transplan-tation. Liver Transpl 2005;11:1505–1514.
65. Adam R, Azoulay D, Castaing D, et al. Liver resection as a bridgeto transplantation for hepatocellular carcinoma on cirrhosis: areasonable strategy? Ann Surg 2003;238:508–518.
66. Lo CM, Fan ST, Liu CL, et al. The role and limitation of livingdonor liver transplantation for hepatocellular carcinoma. LiverTranspl 2004;10:440–447.
67. Trotter JF, Wachs M, Everson GT, et al. Adult-to-adult transplan-tation of the right hepatic lobe from a living donor. N Engl J Med2002;346:1074–1082.
68. Fisher RA, Kulik LM, Freise CE, et al. Hepatocellular carcinomarecurrence and death following living and deceased donor livertransplantation. Am J Transplant 2007;7:1601–1608.
69. Ringe B, Pichlmayr R, Wittekind C, et al. Surgical treatment ofhepatocellular carcinoma: experience with liver resection andtransplantation in 198 patients. World J Surg 1991;15:270–
285.
1
1
1
1
Sc
May 2008 DIAGNOSIS AND TREATMENT OF HCC 1763
70. Ishii H, Okada S, Nose H, et al. Local recurrence of hepatocel-lular carcinoma after percutaneous ethanol injection. Cancer1996;77:1792–1796.
71. Livraghi T, Bolondi L, Lazzaroni S, et al. Percutaneous ethanolinjection in the treatment of hepatocellular carcinoma in cirrho-sis. A study on 207 patients. Cancer 1992;69:925–929.
72. Vilana R, Bruix J, Bru C, et al. Tumor size determines the efficacyof percutaneous ethanol injection for the treatment of smallhepatocellular carcinoma. Hepatology 1992;16:353–357.
73. Livraghi T, Bolondi L, Buscarini L, et al. No treatment, resectionand ethanol injection in hepatocellular carcinoma: a retrospec-tive analysis of survival in 391 patients with cirrhosis. ItalianCooperative HCC Study Group. J Hepatol 1995;22:522–526.
74. Yamamoto J, Okada S, Shimada K, et al. Treatment strategy forsmall hepatocellular carcinoma: comparison of long-term re-sults after percutaneous ethanol injection therapy and surgicalresection. Hepatology 2001;34:707–713.
75. Ryu M, Shimamura Y, Kinoshita T, et al. Therapeutic results ofresection, transcatheter arterial embolization and percutaneoustranshepatic ethanol injection in 3225 patients with hepatocel-lular carcinoma: a retrospective multicenter study. Jpn J ClinOncol 1997;27:251–257.
76. Livraghi T, Goldberg SN, Lazzaroni S, et al. Small hepatocellularcarcinoma: treatment with radio-frequency ablation versus eth-anol injection. Radiology 1999;210:655–661.
77. Shiina S, Teratani T, Obi S, et al. A randomized controlled trial ofradiofrequency ablation with ethanol injection for small hepato-cellular carcinoma. Gastroenterology 2005;129:122–130.
78. Lin SM, Lin CJ, Lin CC, et al. Radiofrequency ablation improvesprognosis compared with ethanol injection for hepatocellularcarcinoma �4 cm. Gastroenterology 2004;127:1714–1723.
79. Lencioni RA, Allgaier HP, Cioni D, et al. Small hepatocellularcarcinoma in cirrhosis: randomized comparison of radio-fre-quency thermal ablation versus percutaneous ethanol injection.Radiology 2003;228:235–240.
80. Teratani T, Yoshida H, Shiina S, et al. Radiofrequency ablationfor hepatocellular carcinoma in so-called high-risk locations.Hepatology 2006;43:1101–1108.
81. Liu DQ, Lu MD, Tan JF, et al. Microwave coagulation at differenttemperatures for hepatocellular carcinoma management: effi-cacy evaluation by enzyme histochemical staining. Nan Fang YiKe Da Xue Xue Bao 2006;26:1149–1151.
82. Chen MS, Li JQ, Zheng Y, et al. A prospective randomized trialcomparing percutaneous local ablative therapy and partial hep-atectomy for small hepatocellular carcinoma. Ann Surg 2006;243:321–328.
83. Livraghi T, Meloni F, Di SM, et al. Sustained complete responseand complications rates after radiofrequency ablation of veryearly hepatocellular carcinoma in cirrhosis: is resection still thetreatment of choice? Hepatology 2008;47:82–89.
84. Llovet JM, Real MI, Montana X, et al. Arterial embolisation orchemoembolisation versus symptomatic treatment in patientswith unresectable hepatocellular carcinoma: a randomised con-trolled trial. Lancet 2002;359:1734–1739.
85. Bruix J, Sala M, Llovet JM. Chemoembolization for hepatocellu-lar carcinoma. Gastroenterology 2004;127(Suppl 1):S179–S188.
86. Llovet JM, Bruix J. Systematic review of randomized trials forunresectable hepatocellular carcinoma: chemoembolization im-proves survival. Hepatology 2003;37:429–442.
87. Kulik LM, Atassi B, van Holsbeek L, et al. Yttrium-90 micro-
spheres (TheraSphere) treatment of unresectable hepatocellu- (lar carcinoma: downstaging to resection, RFA and bridge totransplantation. J Surg Oncol 2006;94:572–586.
88. Llovet J. Sorafenib improves survival in advanced hepatocellularcarcinoma (HCC): results of a phase III randomized placebo-controlled trial (SHARP trial). J Clin Oncol 2007;25(18S [June20 Suppl]):LBA1.
89. Hampton T. Cancer drug trials show modest benefit: drugstarget liver, gastric, head and neck cancers. JAMA 2007;298:273–275.
90. Philip PA, Mahoney MR, Allmer C, et al. Phase II study ofErlotinib (OSI-774) in patients with advanced hepatocellularcancer. J Clin Oncol 2005;23:6657–6663.
91. Djojosubroto MW, Chin AC, Go N, et al. Telomerase antagonistsGRN163 and GRN163L inhibit tumor growth and increase che-mosensitivity of human hepatoma. Hepatology 2005;42:1127–1136.
92. Xu J, Shen ZY, Chen XG, et al. A randomized controlled trial ofLicartin for preventing hepatoma recurrence after liver trans-plantation. Hepatology 2007;45:269–276.
93. Quaglia A, McStay M, Stoeber K, et al. Novel markers of cellkinetics to evaluate progression from cirrhosis to hepatocellularcarcinoma. Liver Int 2006;26:424–432.
94. Fiorentino M, Altimari A, Ravaioli M, et al. Predictive value ofbiological markers for hepatocellular carcinoma patients treatedwith orthotopic liver transplantation. Clin Cancer Res 2004;10:1789–1795.
95. Ho MC, Lin JJ, Chen CN, et al. A gene expression profile forvascular invasion can predict the recurrence after resection ofhepatocellular carcinoma: a microarray approach. Ann Surg On-col 2006;13:1474–1484.
96. Hoshida Y, Moriyama M, Otsuka M, et al. Gene expressionsassociated with chemosensitivity in human hepatoma cells.Hepatogastroenterology 2007;54:489–492.
97. Tateishi R, Shiina S, Yoshida H, et al. Prediction of recurrence ofhepatocellular carcinoma after curative ablation using threetumor markers. Hepatology 2006;44:1518–1527.
98. Llovet JM, Chen Y, Wurmbach E, et al. A molecular signature todiscriminate dysplastic nodules from early hepatocellular carci-noma in HCV cirrhosis. Gastroenterology 2006;131:1758–1767.
99. Davila JA, El-Serag HB. Racial differences in survival of hepato-cellular carcinoma in the United States: a population-basedstudy. Clin Gastroenterol Hepatol 2006;4:104–110.
00. El-Serag HB. Translational research: the study of communityeffectiveness in digestive and liver disorders. Gastroenterology2007;132:8–10.
01. El-Serag HB, Siegel AB, Davila JA, et al. Treatment and out-comes of treating of hepatocellular carcinoma among Medicarerecipients in the United States: a population-based study.J Hepatol 2006;44:158–166.
02. Siegel AB, McBride RB, El-Serag HB, et al. Racial disparities inutilization of liver transplantation for hepatocellular carcinomain the United States, 1998–2002. Am J Gastroenterol 2008;103:120–127.
03. Bruix J, Castells A, Bosch J, et al. Surgical resection of hepa-tocellular carcinoma in cirrhotic patients: prognostic value ofpreoperative portal pressure. Gastroenterology 1996;111:1018–1022.
Received December 19, 2007. Accepted February 25, 2008.Address requests for reprints to: Hashem B. El-Serag, MD, MPH,
ection of Gastroenterology and Hepatology, Baylor College of Medi-ine, Houston, Texas 77030. e-mail: [email protected]; fax:
713) 748 7359.

















