
Diagnosis and Treatment of Extraesophageal … and Treatment of Extraesophageal Reflux Disease ......
66
Diagnosis and Treatment of Extraesophageal Reflux Disease Rachel Rosen, MD Aerodigestive Center (ADC) Center for Motility and Functional Gastrointestinal Disorders
Transcript of Diagnosis and Treatment of Extraesophageal … and Treatment of Extraesophageal Reflux Disease ......

Diagnosis and Treatment ofExtraesophageal Reflux
DiseaseRachel Rosen, MD
Aerodigestive Center (ADC) Center for Motility and Functional
Gastrointestinal Disorders

Sinusitis 4.2%
Otitis 2.1%
Dental erosion 40.2°/o
Apparent lifethreatening event 20%Asthma 13.2%
Pneumonia 6.3%
Bronchiectasis 1%
General respiratorysymptoms 57.7%
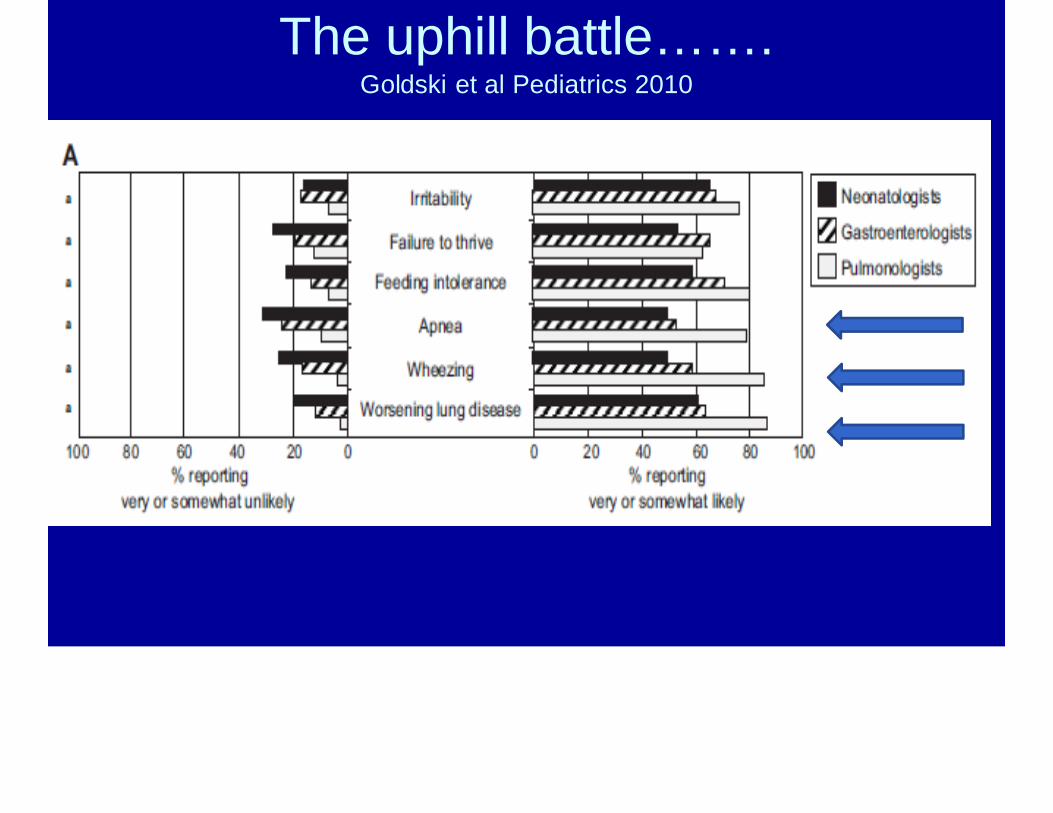
The uphill battle…….Goldski et al Pediatrics 2010

symptomsNelson et al J Med Economic 2009
Mechanisms of Reflux RelatedRespiratory Disease
• Neurally Mediated• Microaspiration
Making the diagnosis
• Total reflux burden? Acid vs. non-acid?• Symptom correlation?• Distal Reflux Burden?• Proximal Reflux burden?• Esophagitis?• Lung biomarkers?
pH probe
•Pharyngeal pH monitoring
•pH-MII
•Cough catheters
•Cough microphone
•Biomarkers
Pharyngeal pH Monitoring
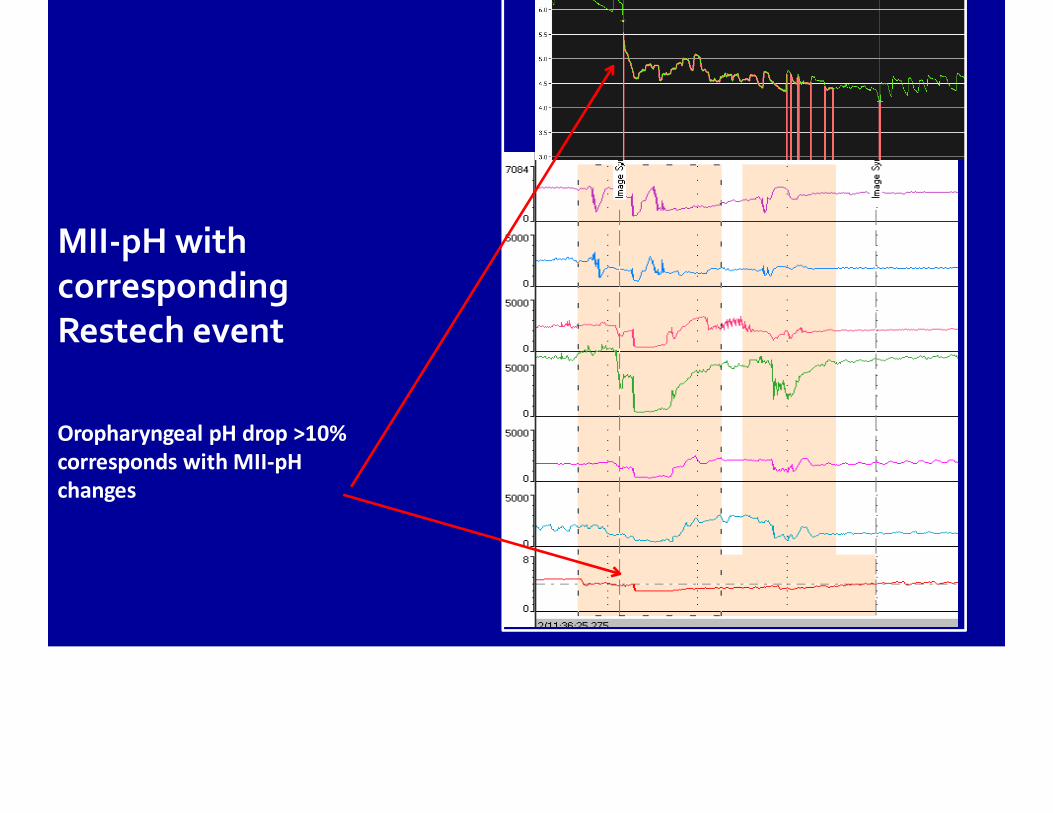
MII‐pHwith corresponding Restech event
Oropharyngeal pH drop >10% corresponds with MII‐pH changes
100
80
60
40
20
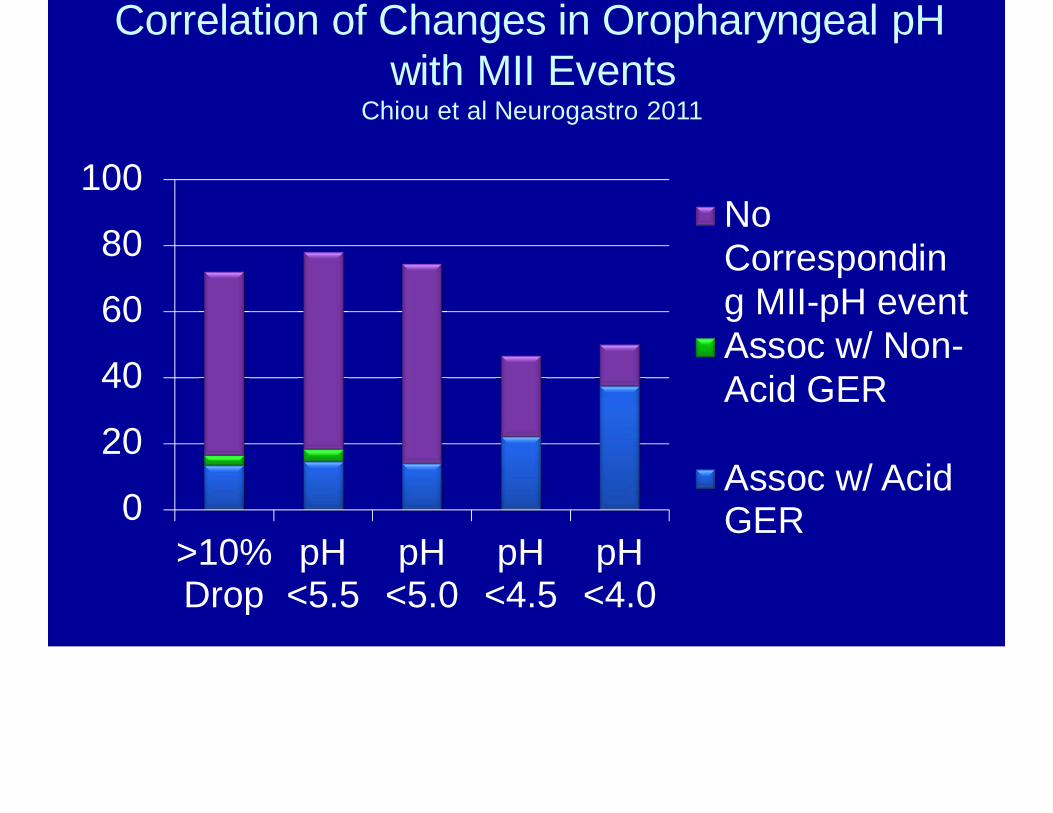
0>10% pHDrop <5.5
pH pH pH<5.0 <4.5 <4.0
No Corresponding MII-pH event Assoc w/ Non-Acid GER
Assoc w/ Acid GER
Correlation of Changes in Oropharyngeal pHwith MII Events
Chiou et al Neurogastro 2011
Multi Channel Intraluminal Impedance (MII)
• pH independent method of measuringreflux
• 7 sensors throughout the esophagus• 1 distal pH sensor• Advantages:
– Height of the refluxate,– Non-acid burden– Composition of reflux (liquid,gas)

Non Acid Reflux in PediatricsVandenplas et al Acta Paediatr. 2007
Percent of nonacid reflux episodes recorded(relative to total number of reflux episodes recorded)
Sifrim (n = 22) Rosen (n = 28) Mousa (n = 25) Wenzl (n = 22)
40 45 49 89
Del Buono (n =20) Corvaglia (n= 5)
69 78
Wenzl (n = 14) 55Condino (n = 24) 51
Condino (n =34) Lopez-Alonso (n= 21) Lopez-Alonso
(n = 7)
46 53 73
Del Buono (n = 16) 56Mattioli ( > 1 yr) (n = 50) 49Mattioli ( < 1 yr) (n = 50) 53
0 20 40 60 80 100
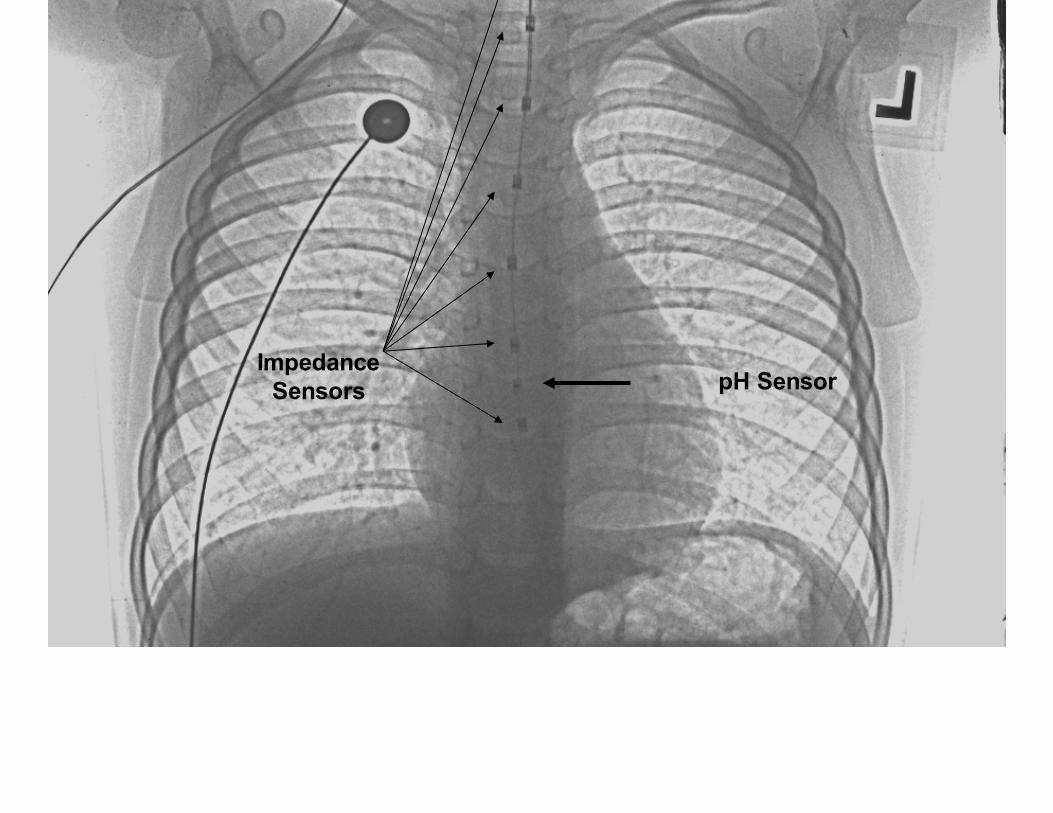
pH SensorImpedance
Sensors
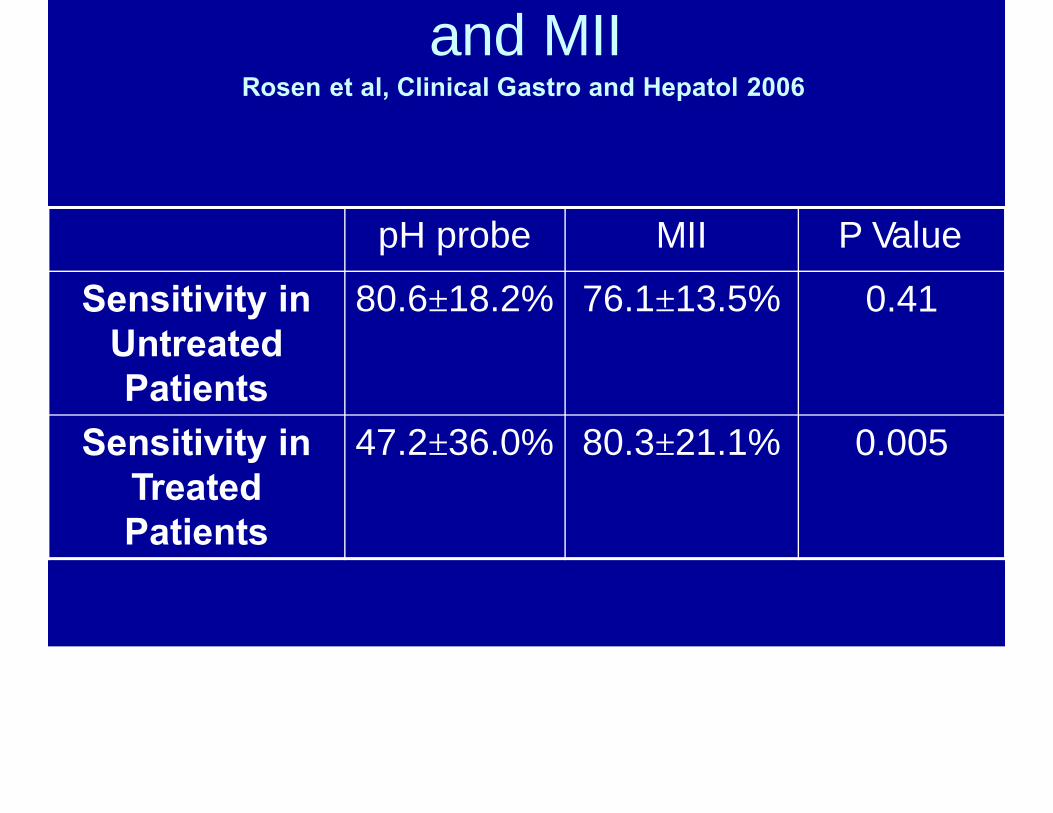
and MIIRosen et al, Clinical Gastro and Hepatol 2006
pH probe MII P Value
Sensitivity in Untreated Patients
80.6±18.2% 76.1±13.5% 0.41
Sensitivity in Treated Patients
47.2±36.0% 80.3±21.1% 0.005
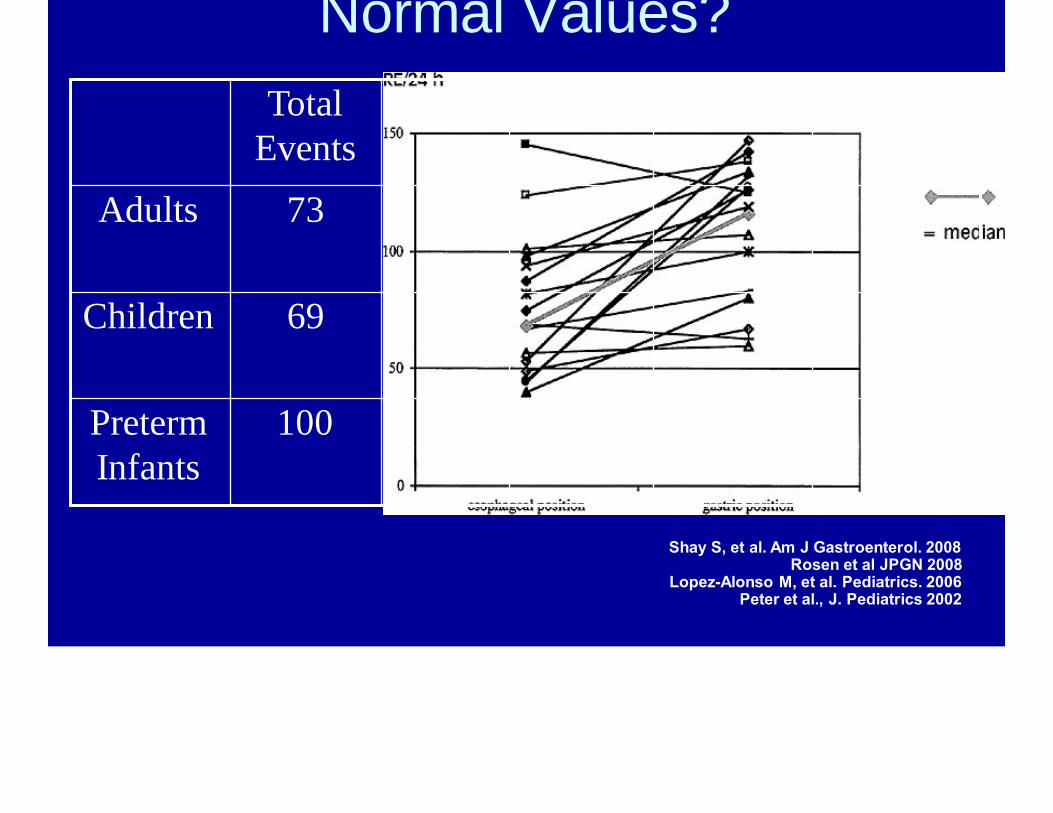
Normal Values?
Shay S, et al. Am J Gastroenterol. 2008Rosen et al JPGN 2008
Lopez-Alonso M, et al. Pediatrics. 2006 Peter et al., J. Pediatrics 2002
Acid Weakly Non- pH only Acid Acid
55 26 1 3
58 13 35
52 98
Total Events
Adults 73
Children 69
Preterm Infants
100
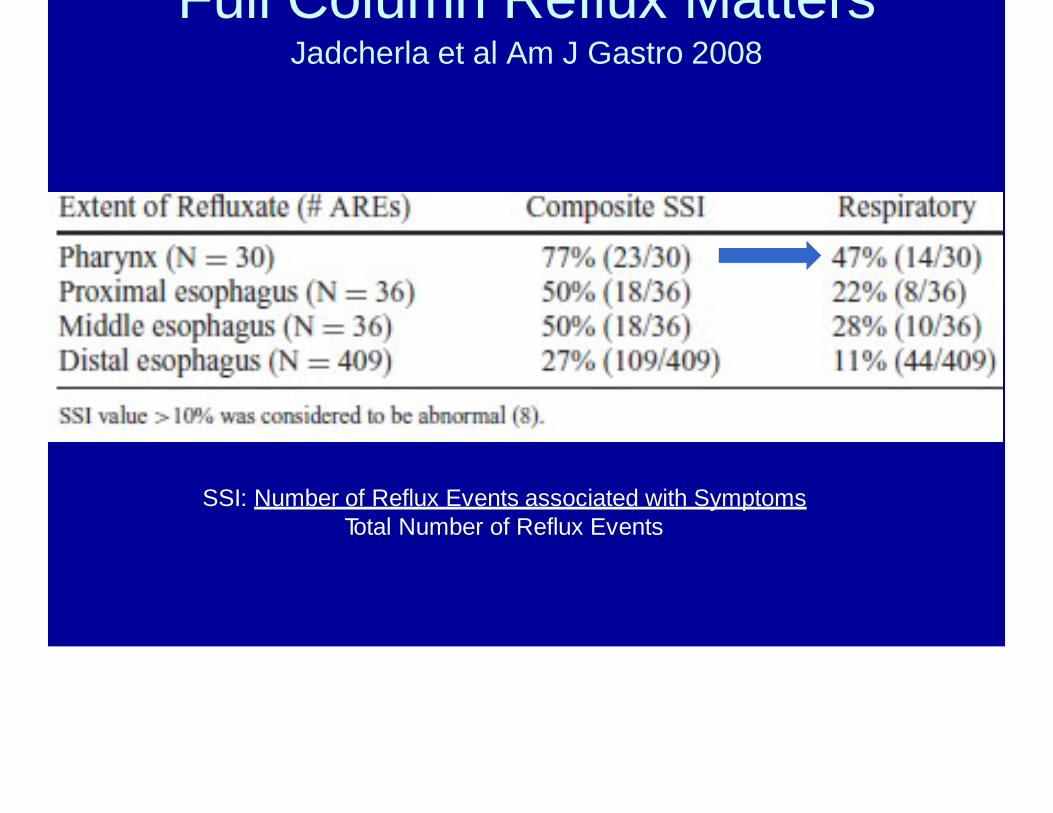
Full Column Reflux MattersJadcherla et al Am J Gastro 2008
SSI: Number of Reflux Events associated with SymptomsTotal Number of Reflux Events
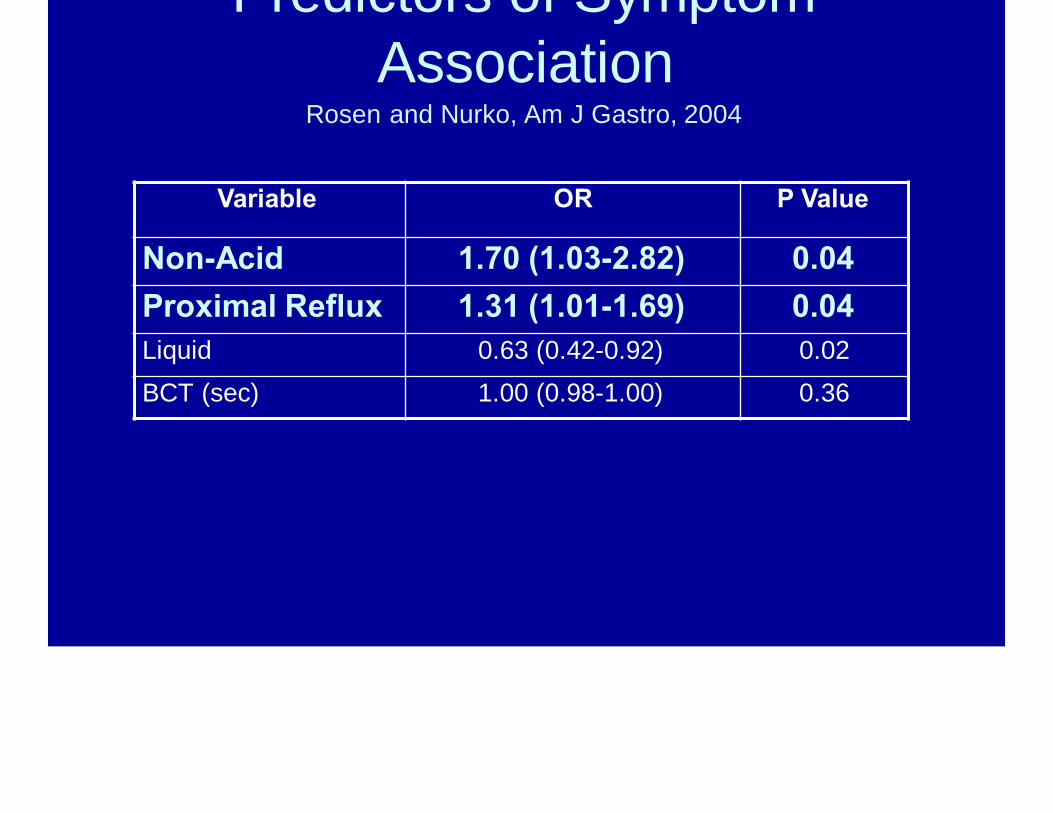
Predictors of SymptomAssociation
Rosen and Nurko, Am J Gastro, 2004
Variable OR P Value
Non-Acid 1.70 (1.03-2.82) 0.04Proximal Reflux 1.31 (1.01-1.69) 0.04Liquid 0.63 (0.42-0.92) 0.02BCT (sec) 1.00 (0.98-1.00) 0.36

p g pOutcome?
Rosen et al JPGN 2010
Improved (N=22)
Not Improved (N=12)
P value
# acid events 13 (5, 25) 18 (5, 72) 0.36# non-acid events 19 (10, 29) 15 (2, 23) 0.21# pH-only events 18 (8, 30) 16 (8, 24) 0.71% full column
reflux38±23 17±14 0.005
% time pH<4 7.9±7.7 13.7±13.8 0.12

p g gevaluation have abnormal testing by
EGD or pH-MIIRosen et al Peds Pulm 2014
7% have EoE

So much is unknown…
• How much full column reflux is too much?• How much full column reflux is too much in
the child that aspirates?• Can we treat full column reflux, other than
fundoplication?

Impedance: The nextgeneration…

30 sec
cough
peristalsis
pH
coughcough
Pres
sure
C
hann
els
Addition of manometry increases cough detectionby 100%
Sifrim, Gut 2005Rosen et al JPGN 2013

10000
lm0
10000
lm100
100
Pr0
0
pJOO
p Ro ...................................................................................................................................................................................................................................................................................................................................................................................................................·········································-·····································································································-································-···································································-································-·····································································································-··················
0
Sul>ine .................................................................................................................................................................................................................................................................................................................................................................................................................. .
I2/09 :53:30
I2/09 :54:00
I2/09:54:30
I2/09 :55:00

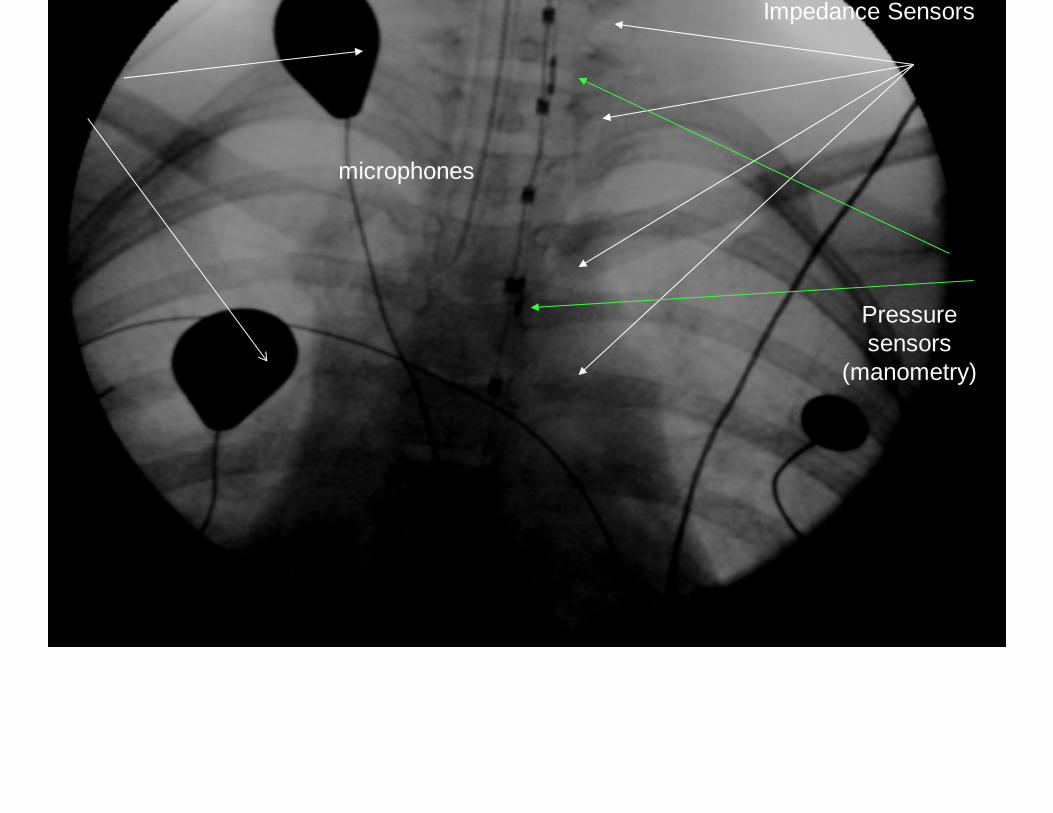
microphones
Impedance Sensors
Pressure sensors
(manometry)
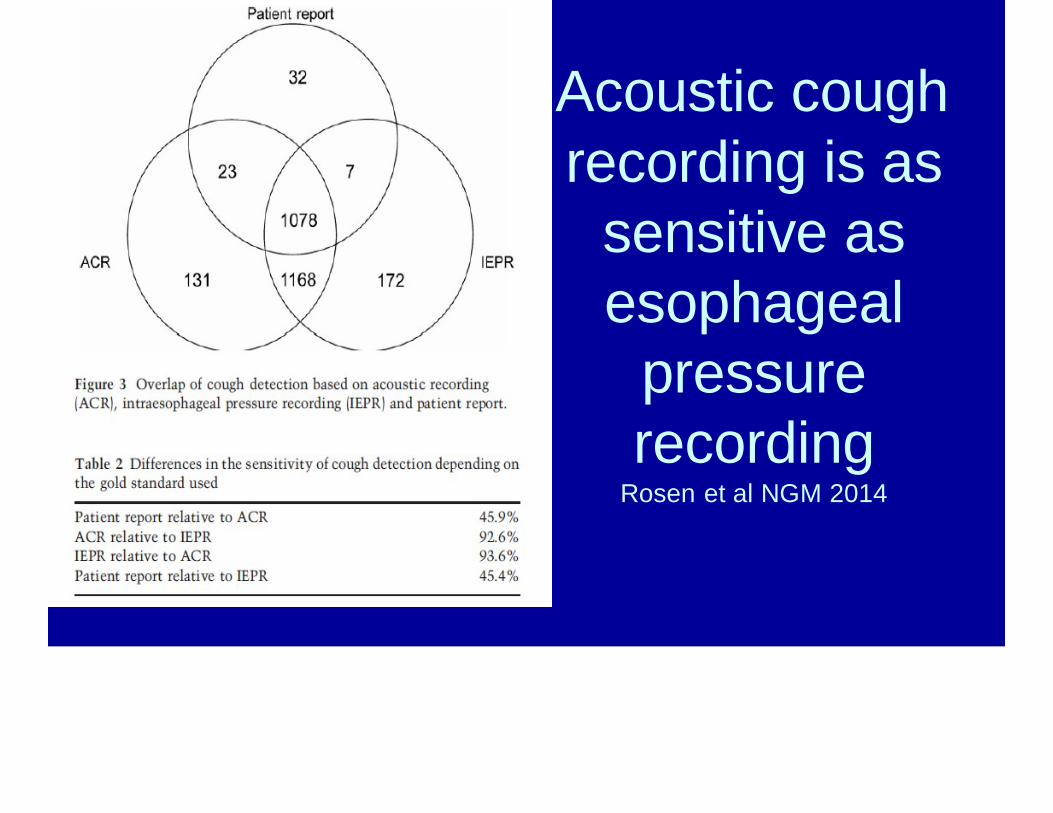
Acoustic coughrecording is as
sensitive as esophageal
pressurerecording
Rosen et al NGM 2014
to
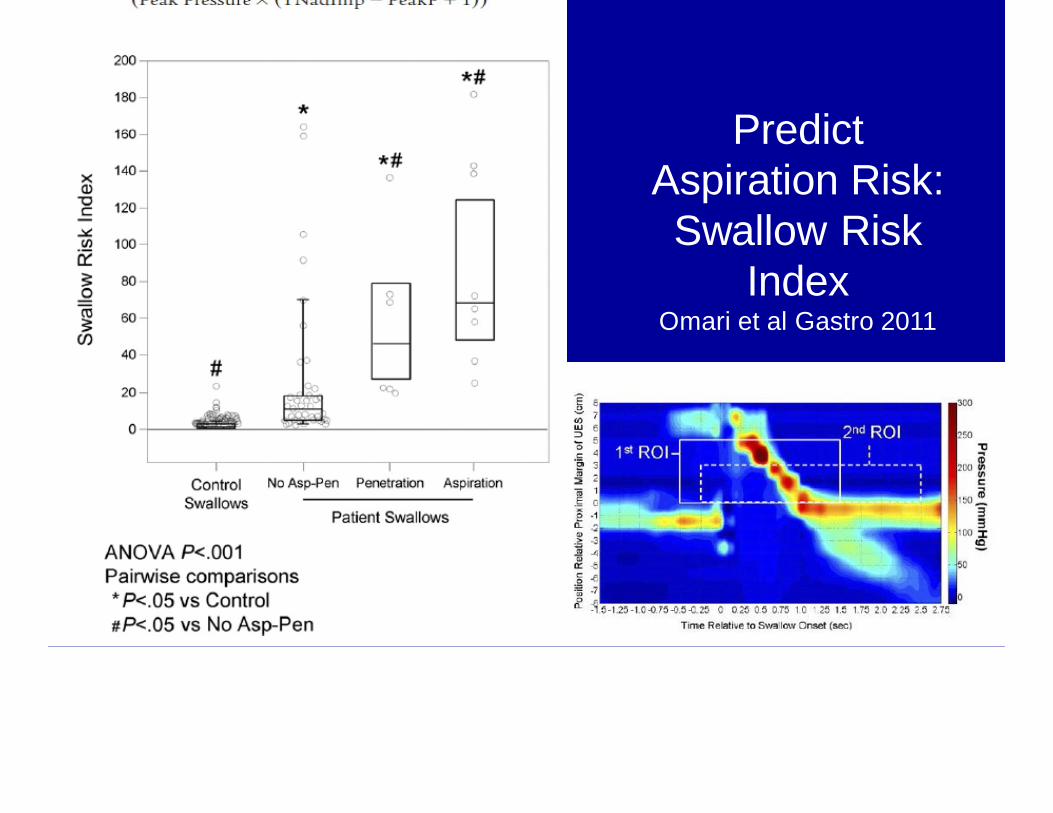
Predict Aspiration Risk:Swallow Risk
IndexOmari et al Gastro 2011

Biomarkers
• LLMI• Pepsin• Bile• Bacteria??
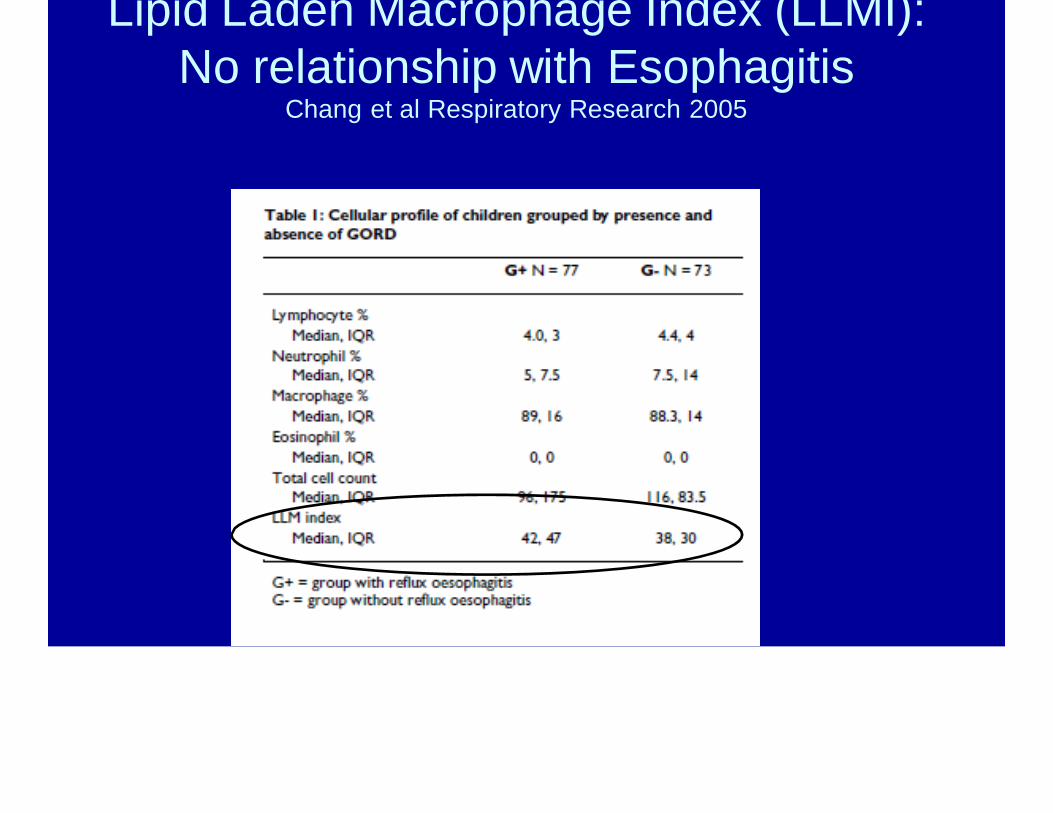
Lipid Laden Macrophage Index (LLMI): No relationship with Esophagitis
Chang et al Respiratory Research 2005
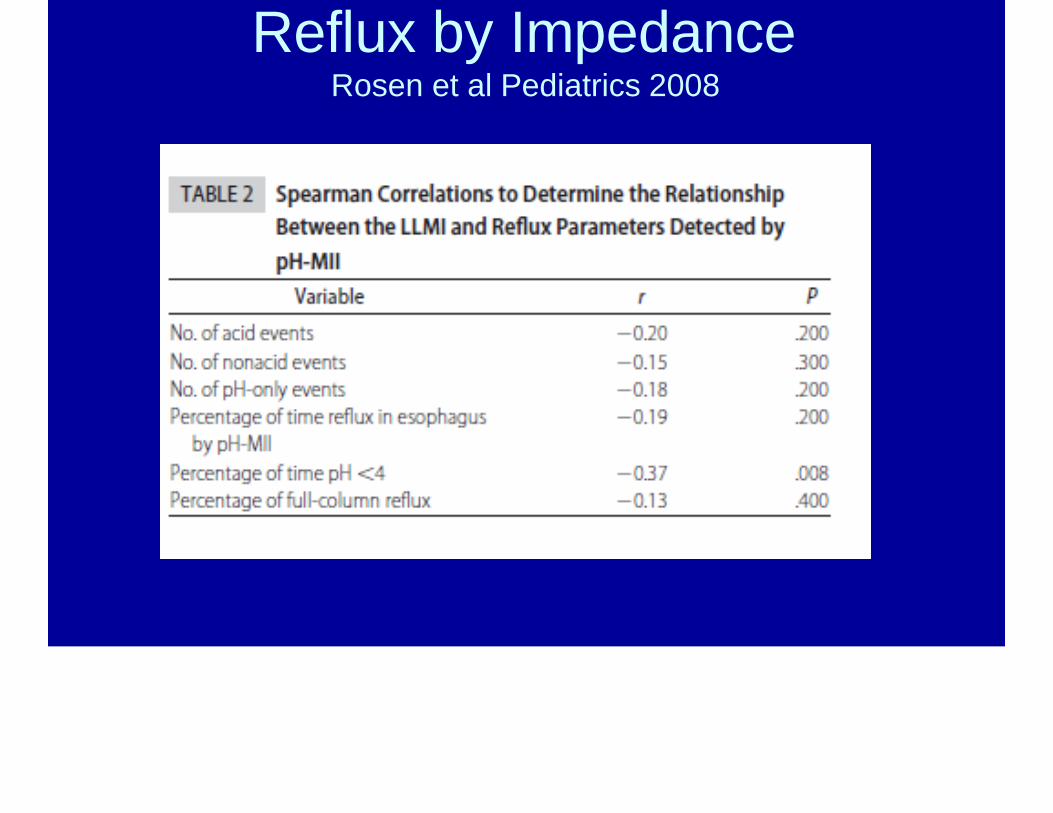
Reflux by ImpedanceRosen et al Pediatrics 2008

AspirationReiley et al Laryngoscope 2011

Pepsin in Patients With GERD
1Starosta V, et al. Chest. 2007
Pepsin Sensitivity and Specificity
• 63% sensitivity; 92%specificity if reflux indistal esophagus2
• 75% sensitivity; 91% specificity if reflux in the proximal esophagus2
Peps
inin
BAL
(n
g/m
L)1
2500
1500
500200
100
0
Reflux indexproximal ≥ 2%
Reflux indexproximal < 2%
Peps
inin
BAL
flu
id(n
g/m
L)1
0 25 50 75 100 125 150 175Number of proximal reflux episodes
r = 0.51
P < 0.0001
P = 0.034
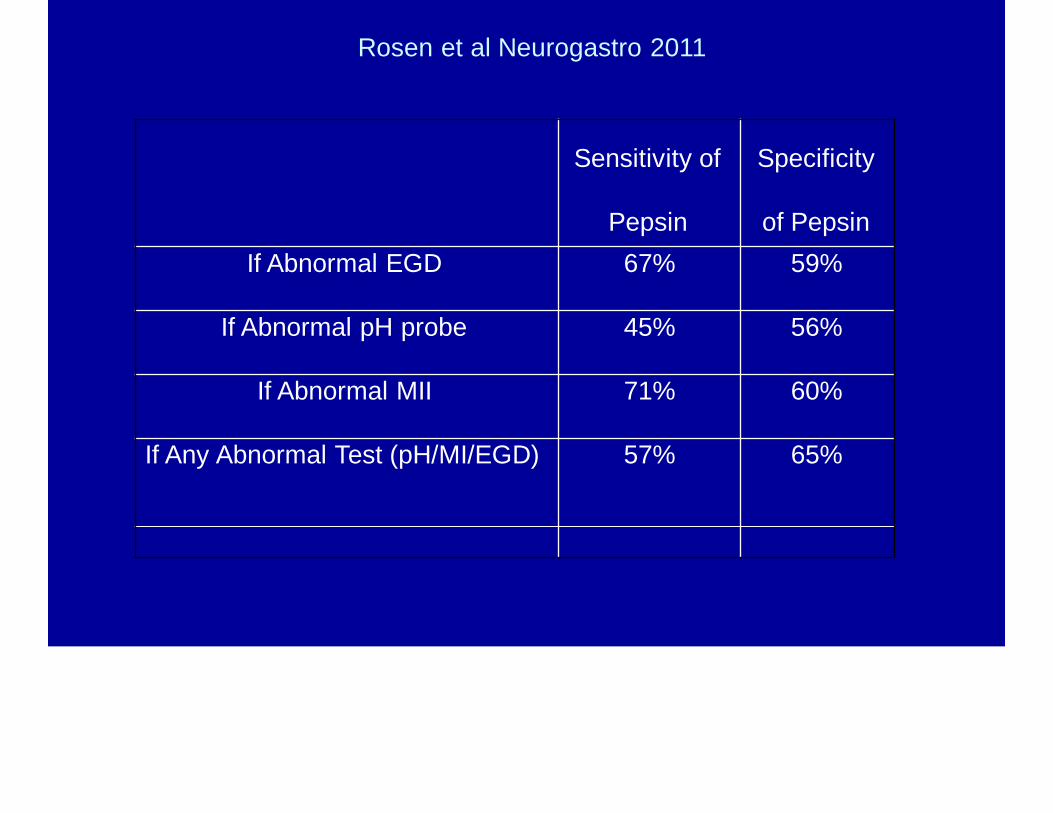
Rosen et al Neurogastro 2011
Sensitivity of
Pepsin
Specificity
of PepsinIf Abnormal EGD 67% 59%
If Abnormal pH probe 45% 56%
If Abnormal MII 71% 60%
If Any Abnormal Test (pH/MI/EGD) 57% 65%

Pepsin in the Lung and other ManifestationsRosen et al Neurogastro 2011
Pepsin Negative
n=28
Pepsin Positive
n=22
P Value
Ear Infections 11/28 3/19 0.4
Ear Tubes 4/28 5/22 0.4
Tonsillectomy 6/28 7/22 0.3
Sinus Infection 6/26 6/17 0.3
Pneumonia 6/26 8/19 0.4
Croup 5/27 4/20 0.9
Asthma 25/28 12/19 0.03
Cough 24/28 13/22 0.5
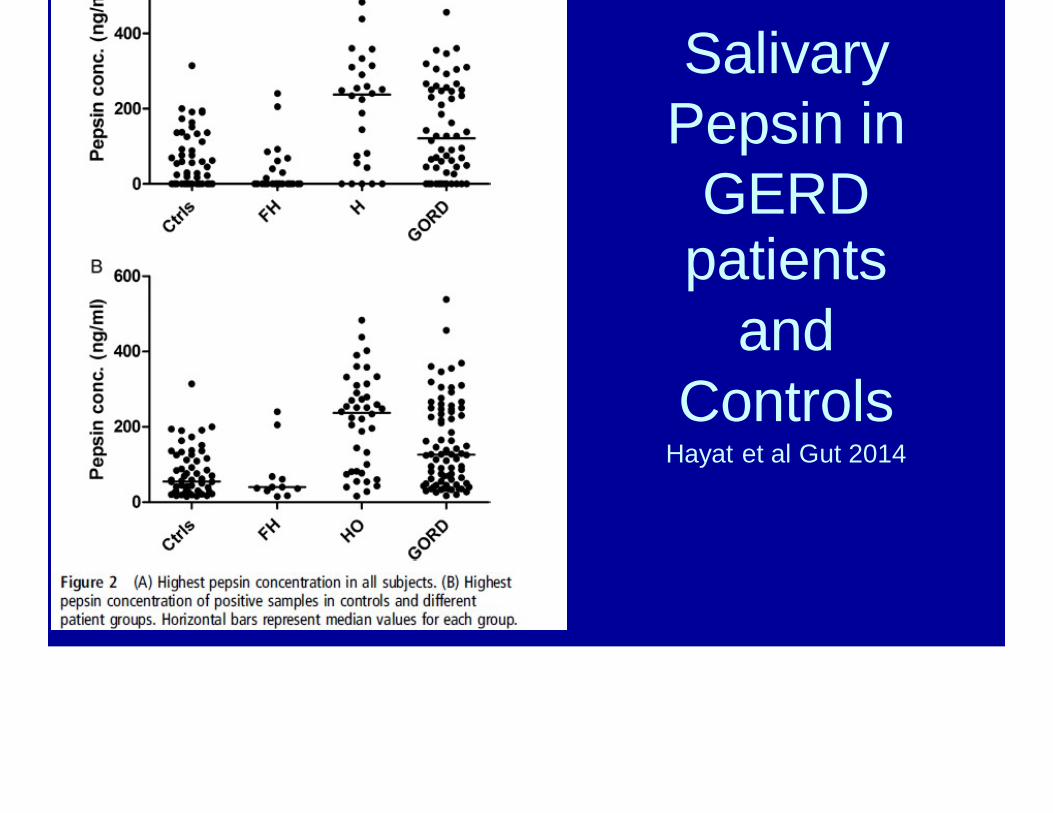
SalivaryPepsin in
GERDpatients
andControls
Hayat et al Gut 2014

pReflux Events
Blondeau et al J Heart Lung Transpl 2009
Bile in bronchoscopy fluid has been
associated with increased lung
rejection
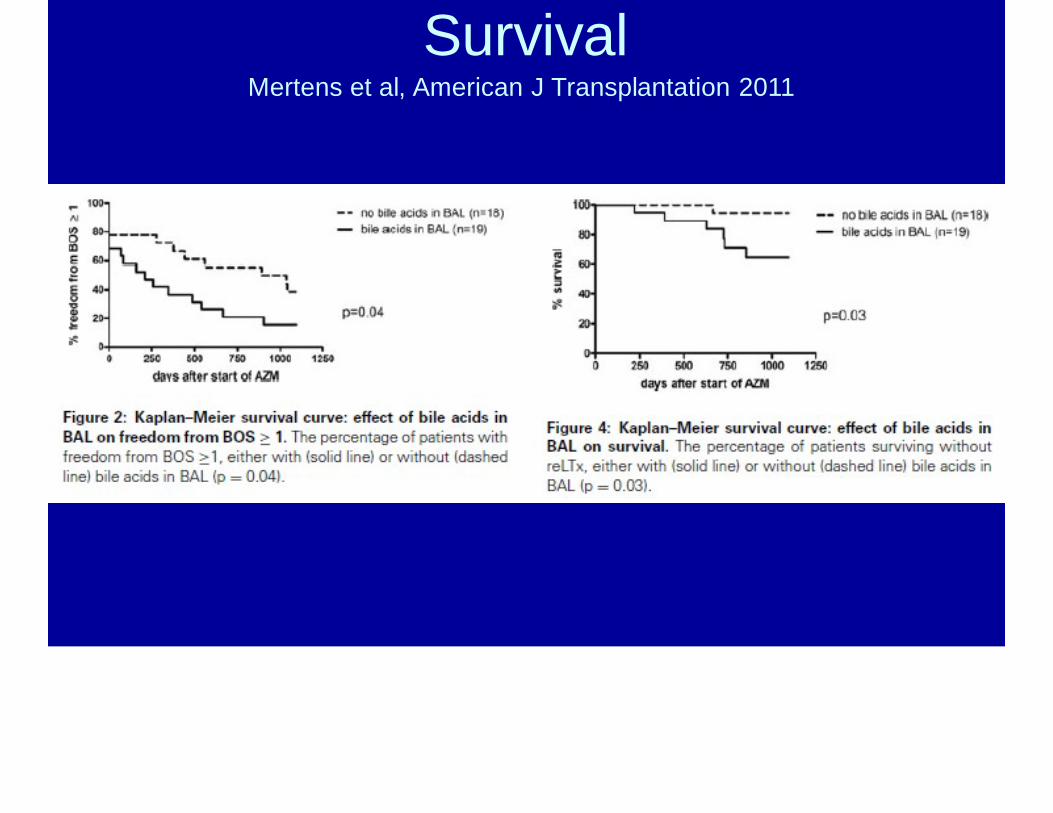
SurvivalMertens et al, American J Transplantation 2011
You made the diagnosis: Nowwhat?
Acid Suppression
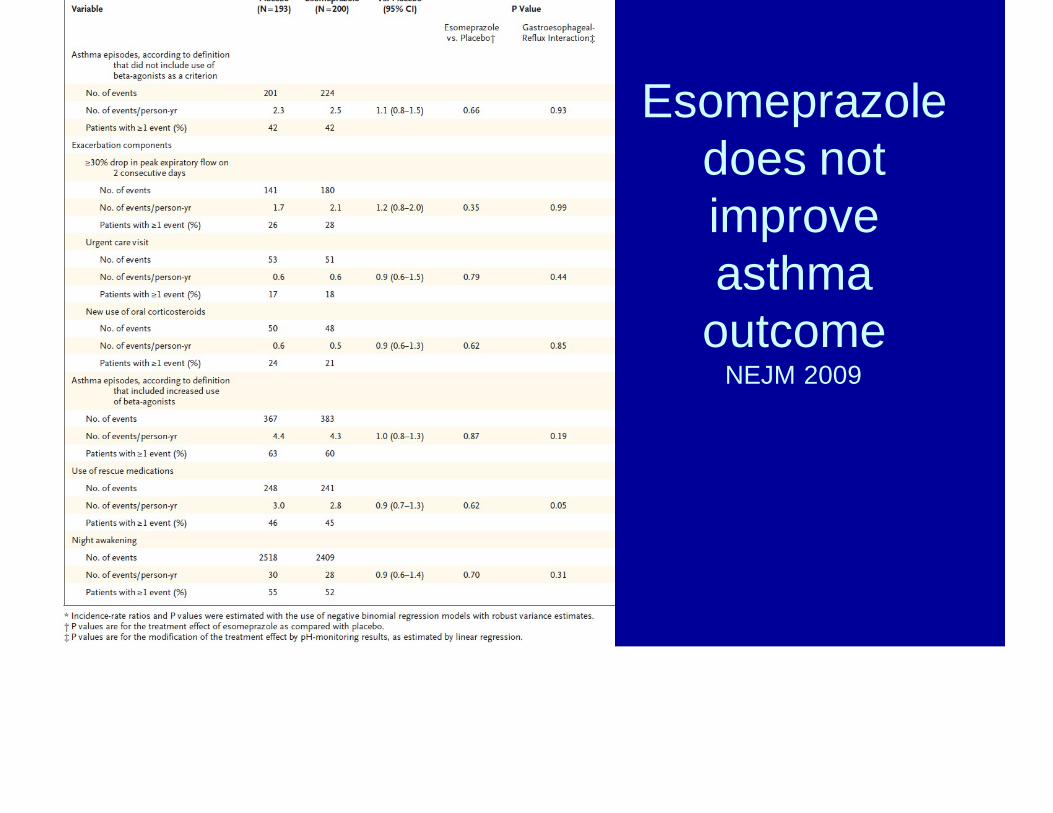
Esomeprazole does not improve asthma
outcomeNEJM 2009

RCT of Omeprazole in Treatment of AsthmaStordal et al Arch Dis Child 2005
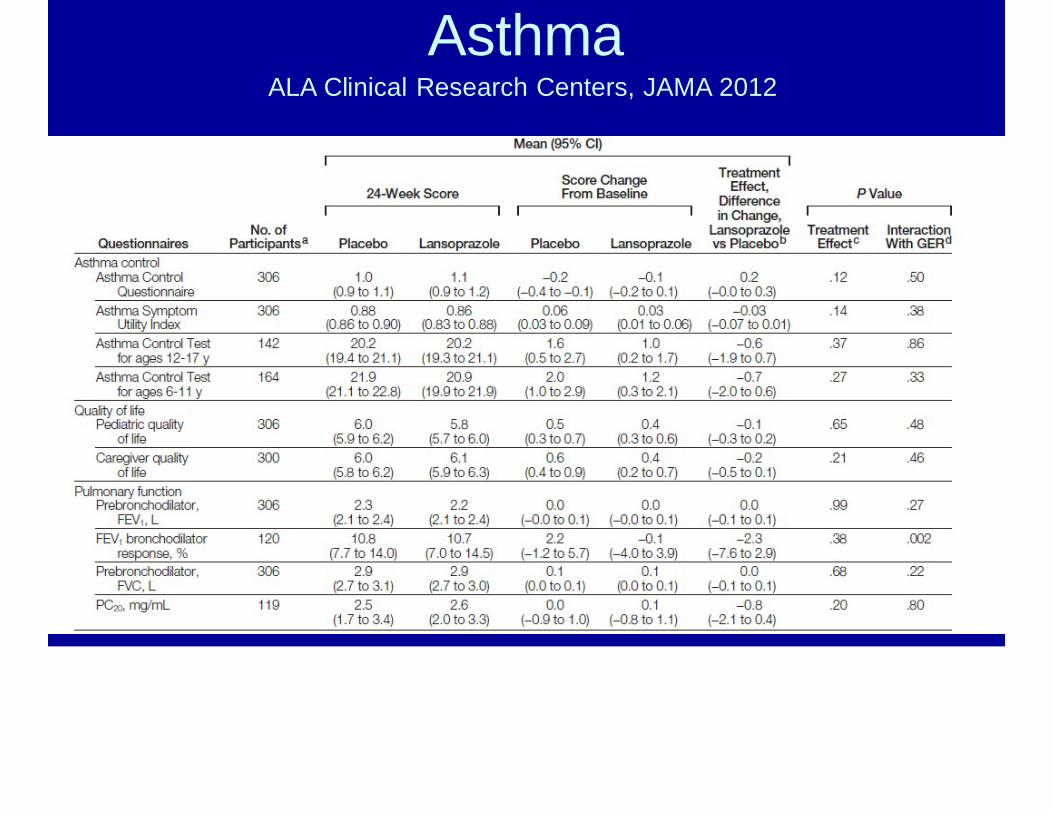
AsthmaALA Clinical Research Centers, JAMA 2012
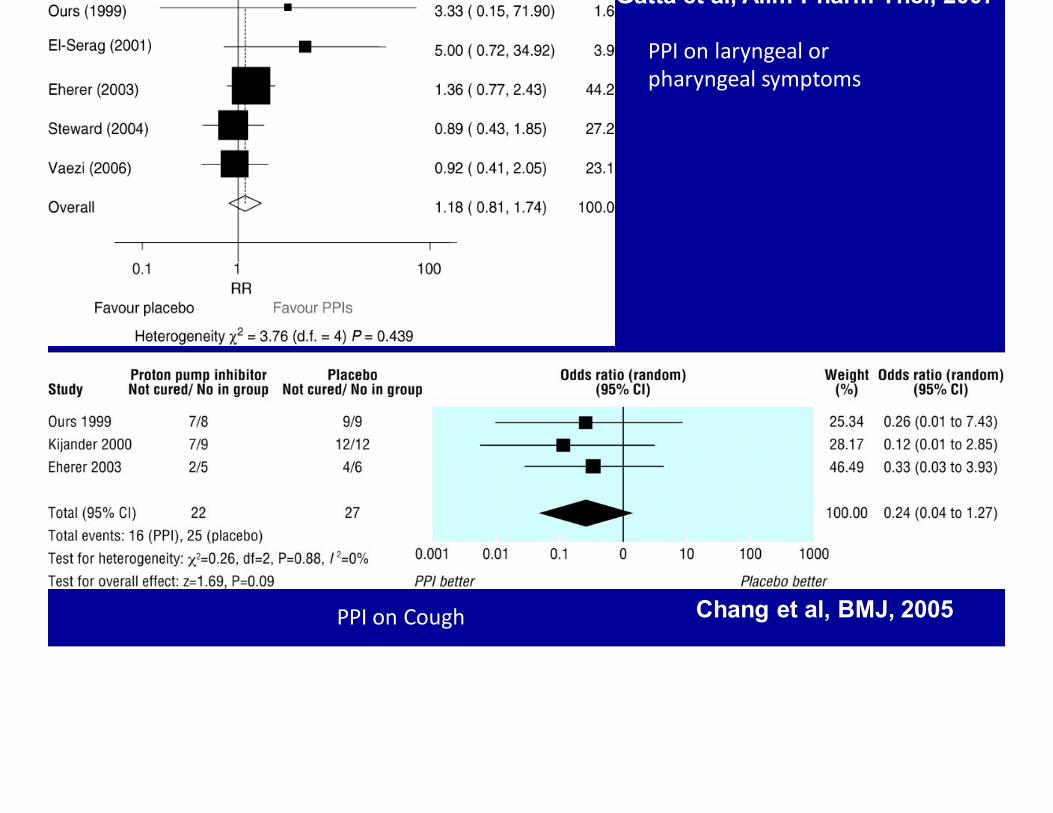
Chang et al, BMJ, 2005
Gatta et al, Alim Pharm Ther, 2007
PPI on laryngeal or pharyngeal symptoms
PPI on Cough
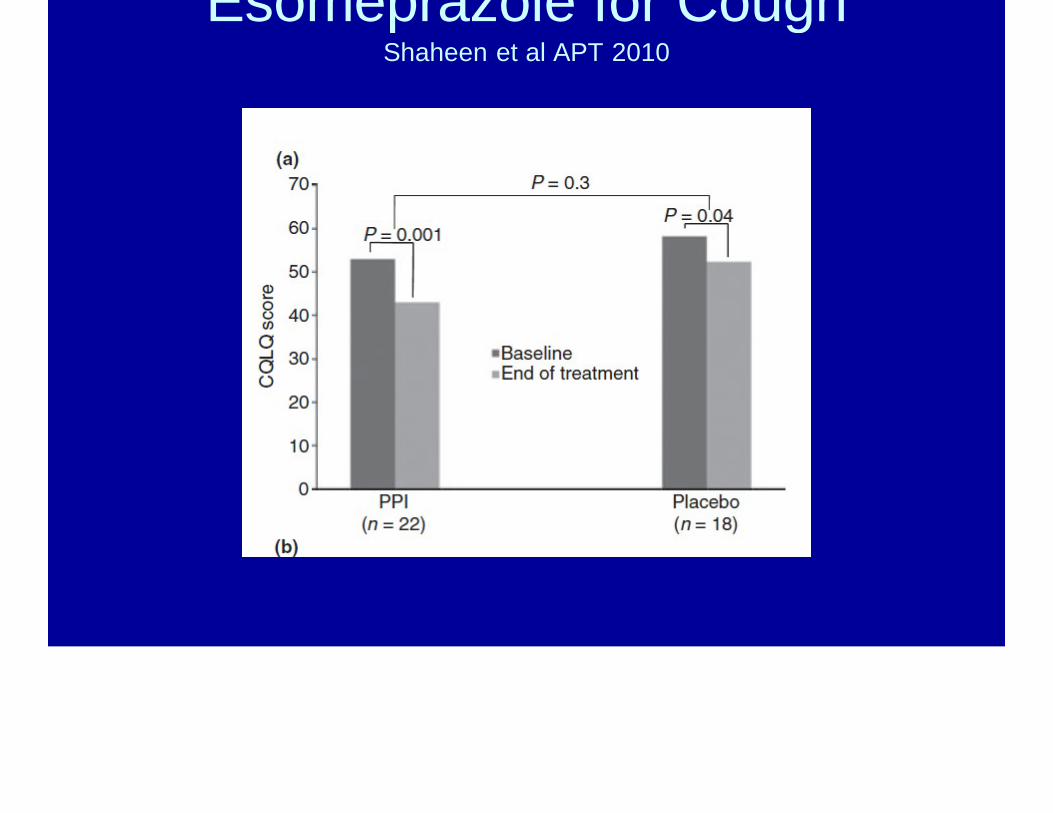
Esomeprazole for CoughShaheen et al APT 2010
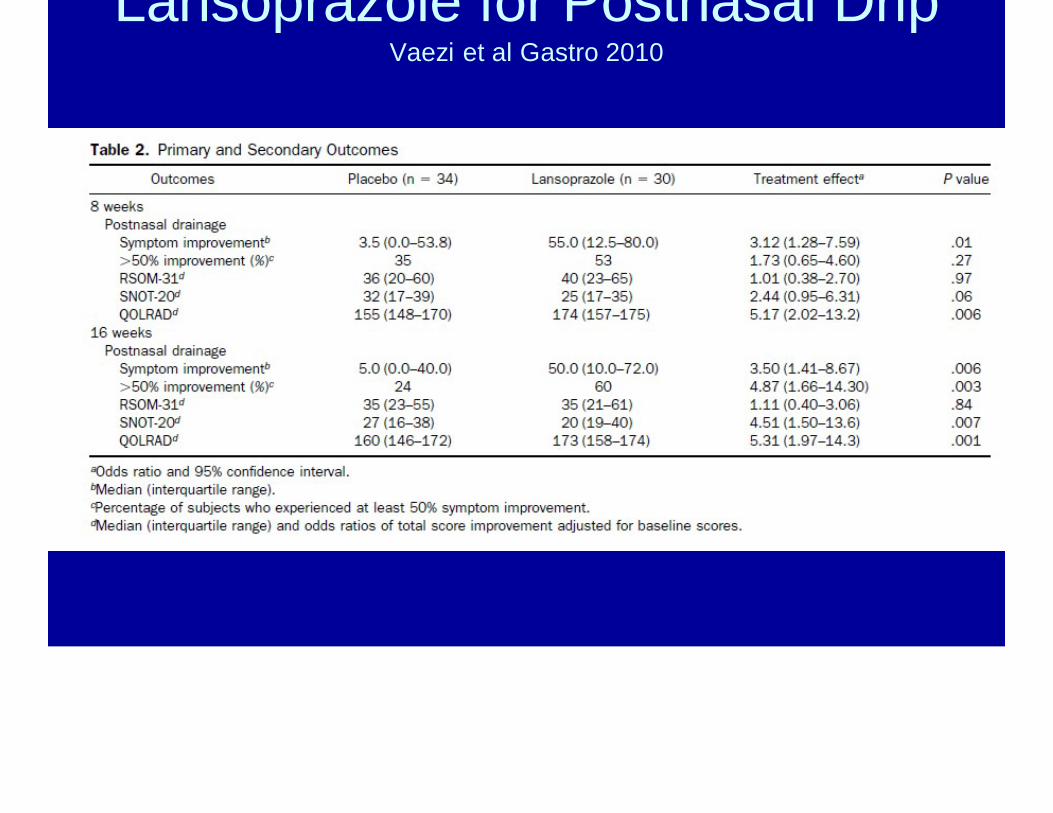
Lansoprazole for Postnasal DripVaezi et al Gastro 2010
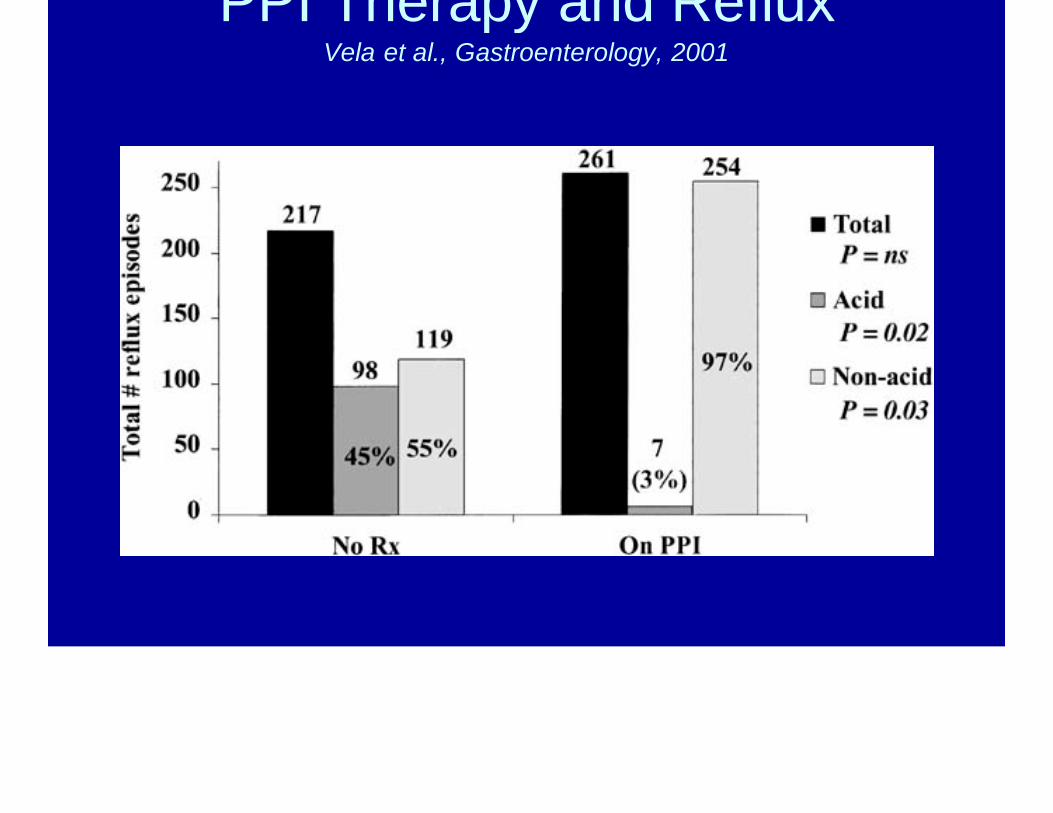
PPI Therapy and RefluxVela et al., Gastroenterology, 2001
Motility Agents

Reglan
Cisapride
Tagaserod
DomperIdone
Macrolides
• Increase antral contractility– Improvement in gastric emptying?– Improvement in reflux?
• Anti-inflammatory effect• Antimicrobial effect
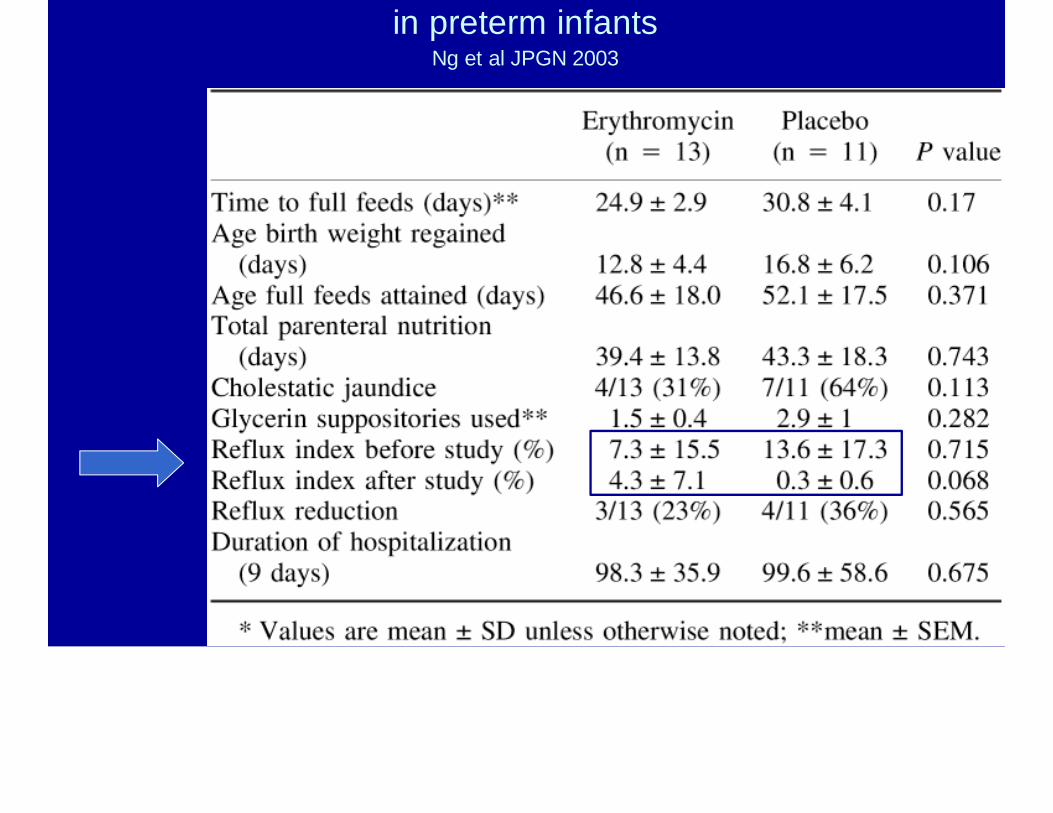
in preterm infantsNg et al JPGN 2003

RCT of Emycin (12.5 mg/kg/dose Q6)
Ng et al Gastro 2007
Prior efficacy data with conflicting results with feeding tolerance
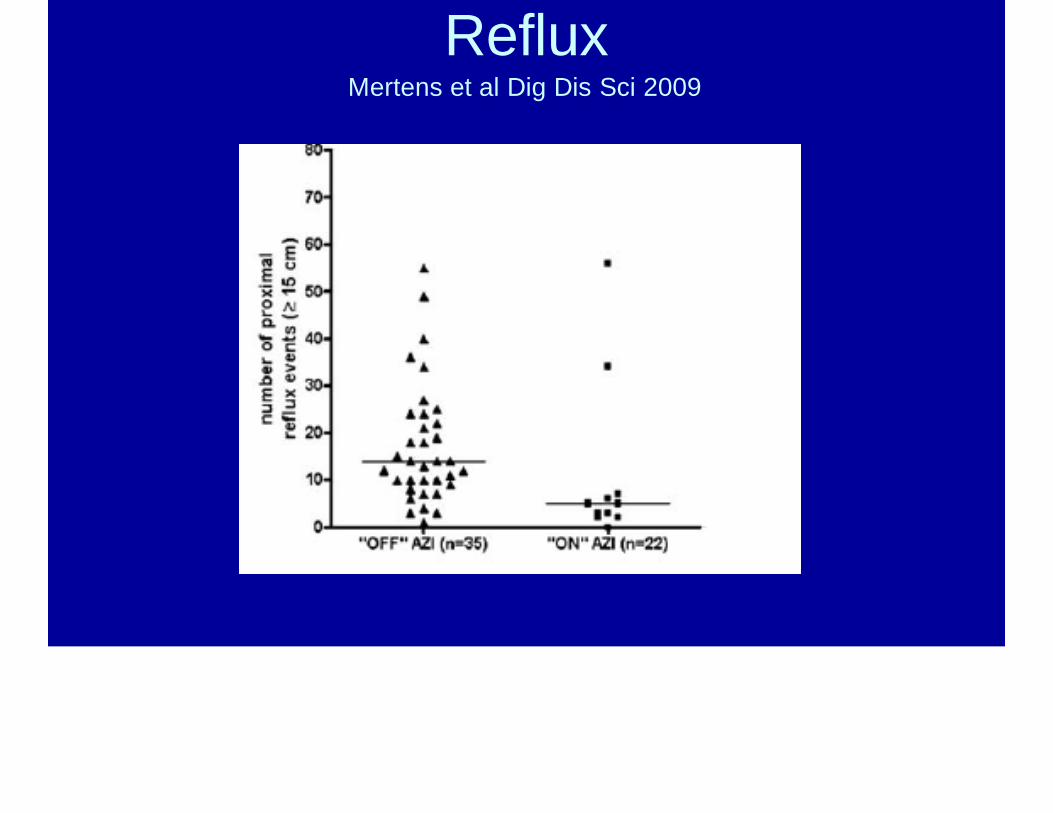
RefluxMertens et al Dig Dis Sci 2009
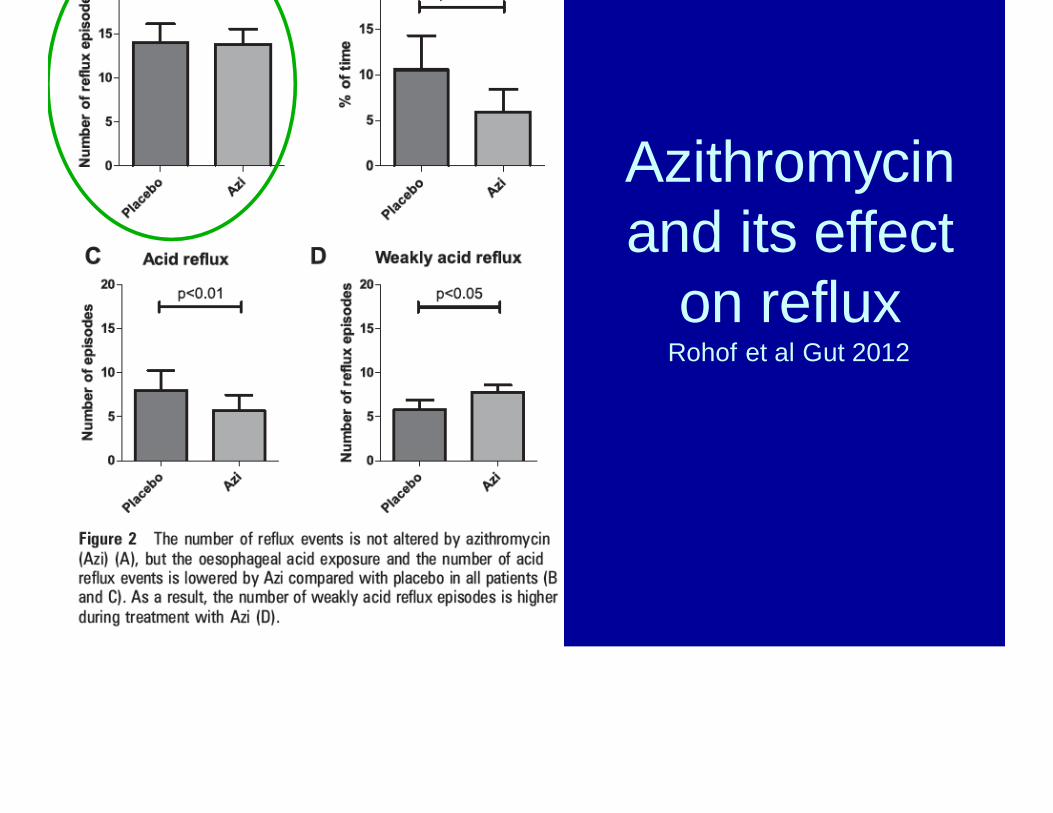
Azithromycin and its effect
on refluxRohof et al Gut 2012

InjuryWalkey and Weiner Chest 2011

Fundoplication
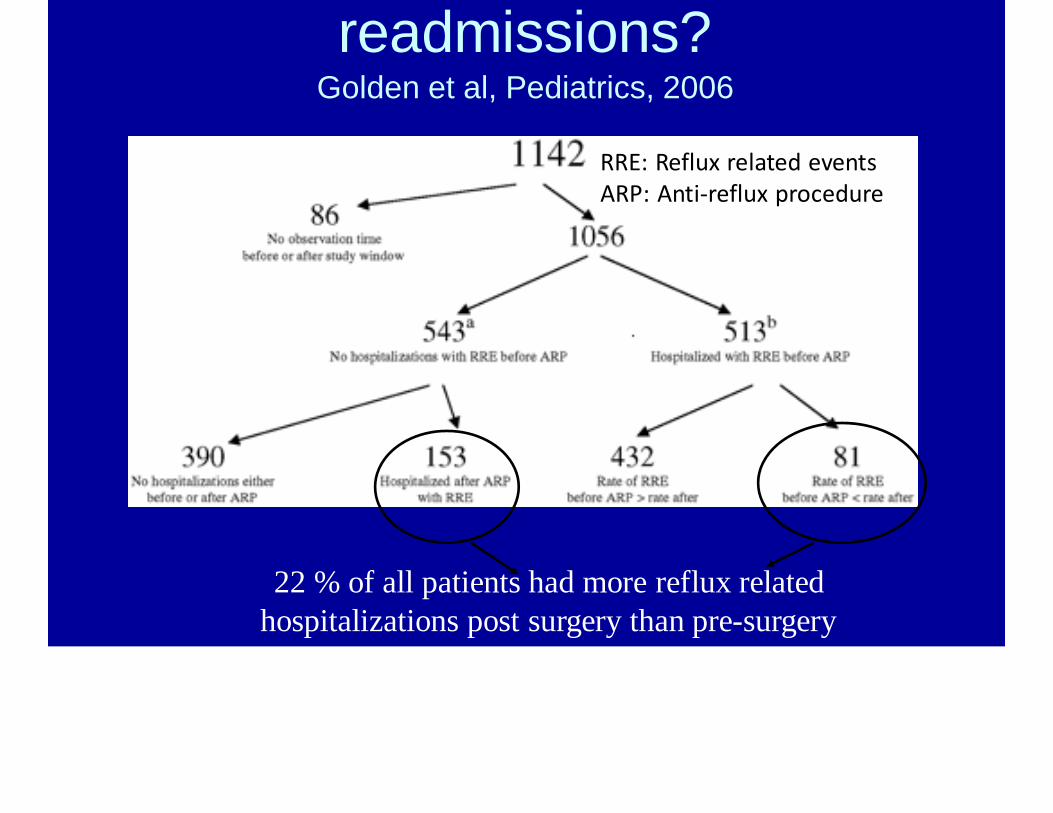
readmissions?Golden et al, Pediatrics, 2006
RRE: Reflux related eventsARP: Anti‐reflux procedure
22 % of all patients had more reflux related hospitalizations post surgery than pre-surgery
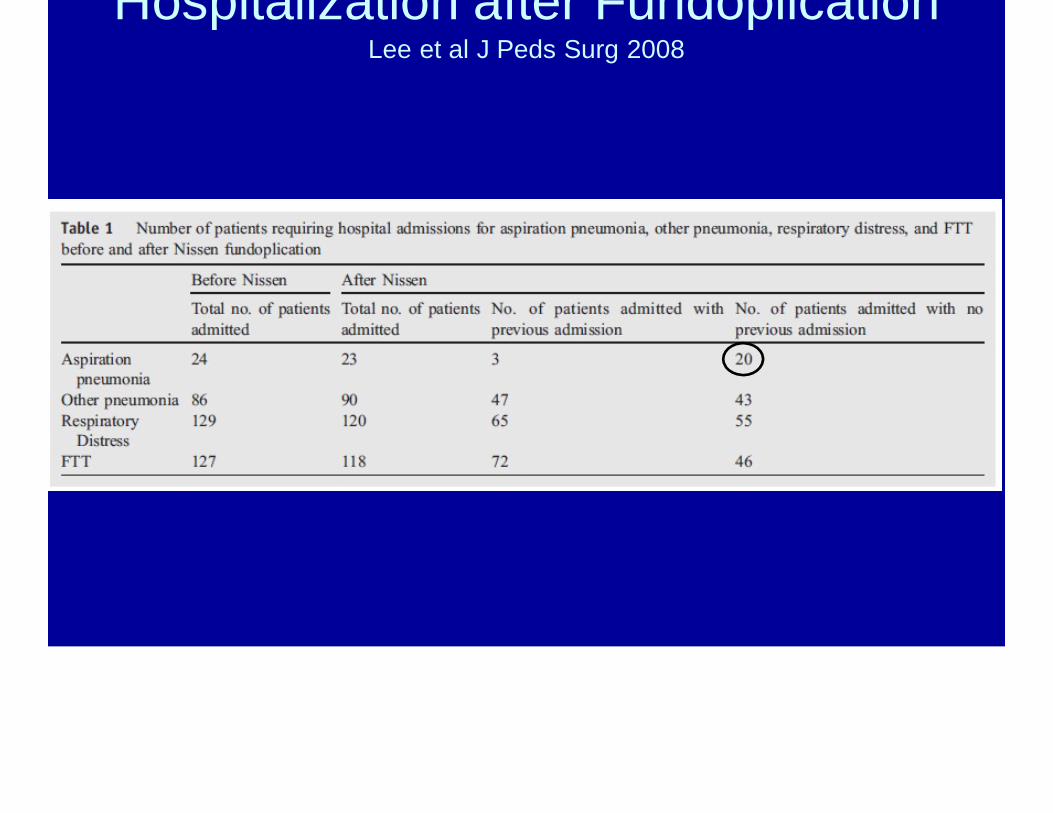
Hospitalization after FundoplicationLee et al J Peds Surg 2008
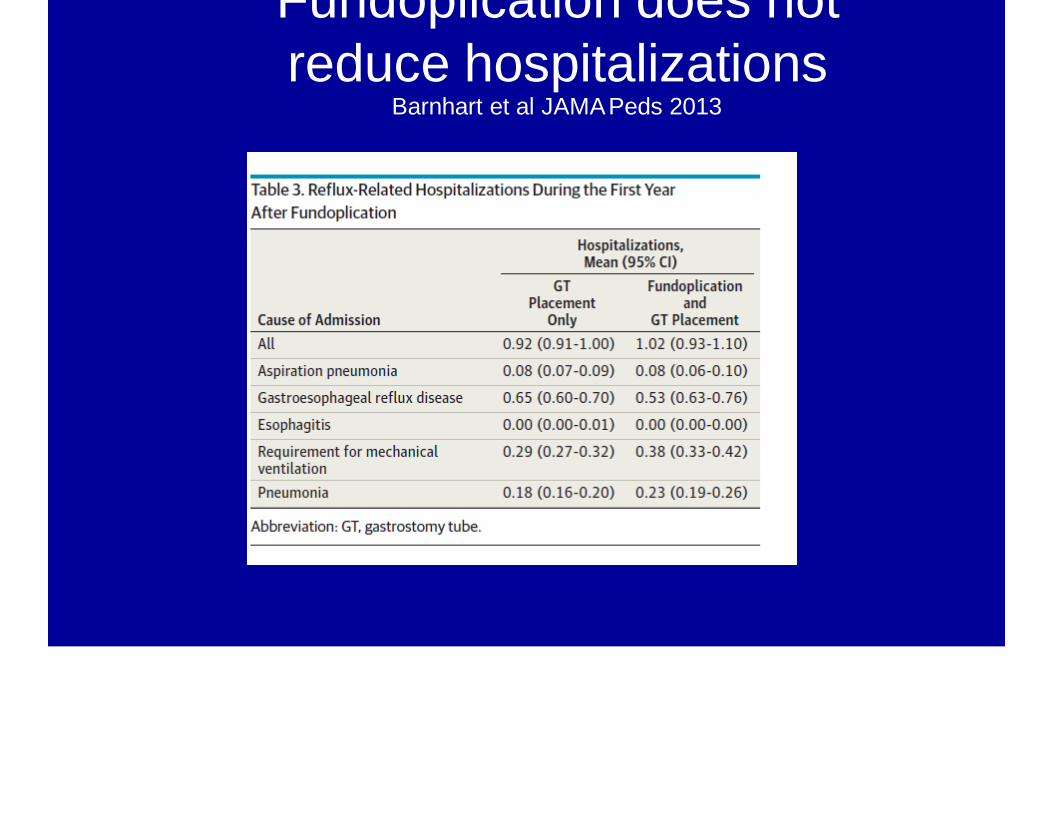
Fundoplication does not reduce hospitalizations
Barnhart et al JAMAPeds 2013
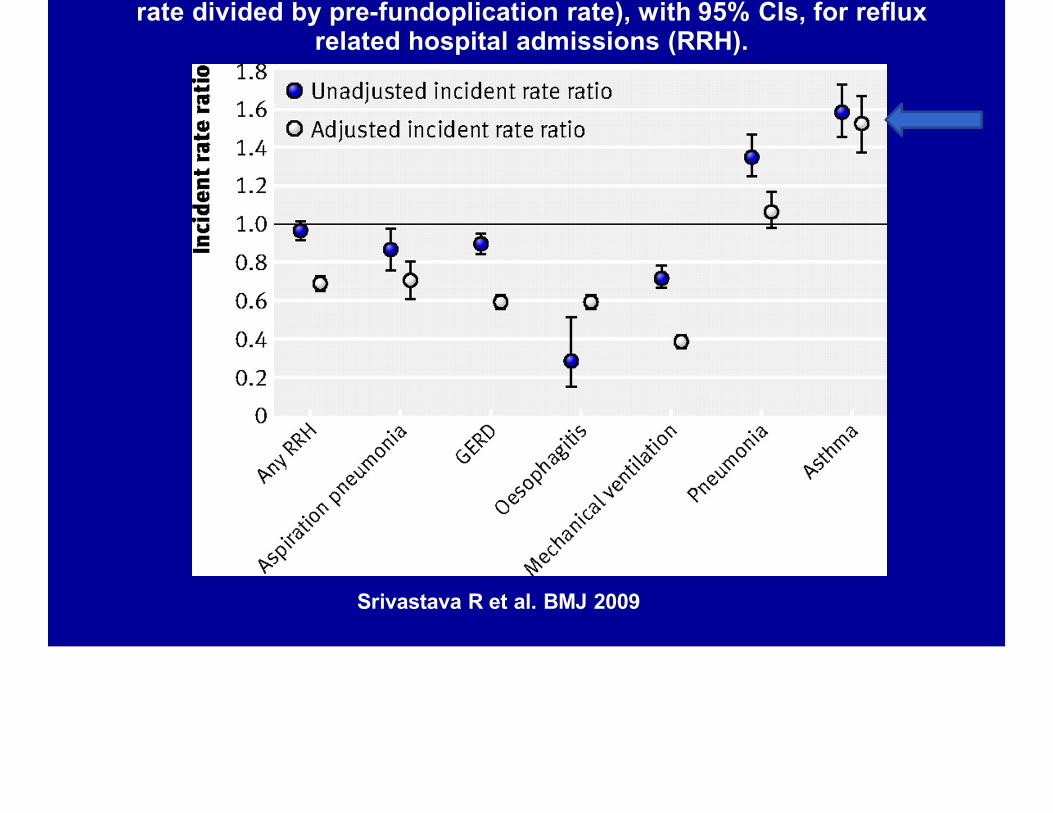
rate divided by pre-fundoplication rate), with 95% CIs, for refluxrelated hospital admissions (RRH).
Srivastava R et al. BMJ 2009

g yFrancis et al Laryngoscope 2011
Transpyloric Feeding
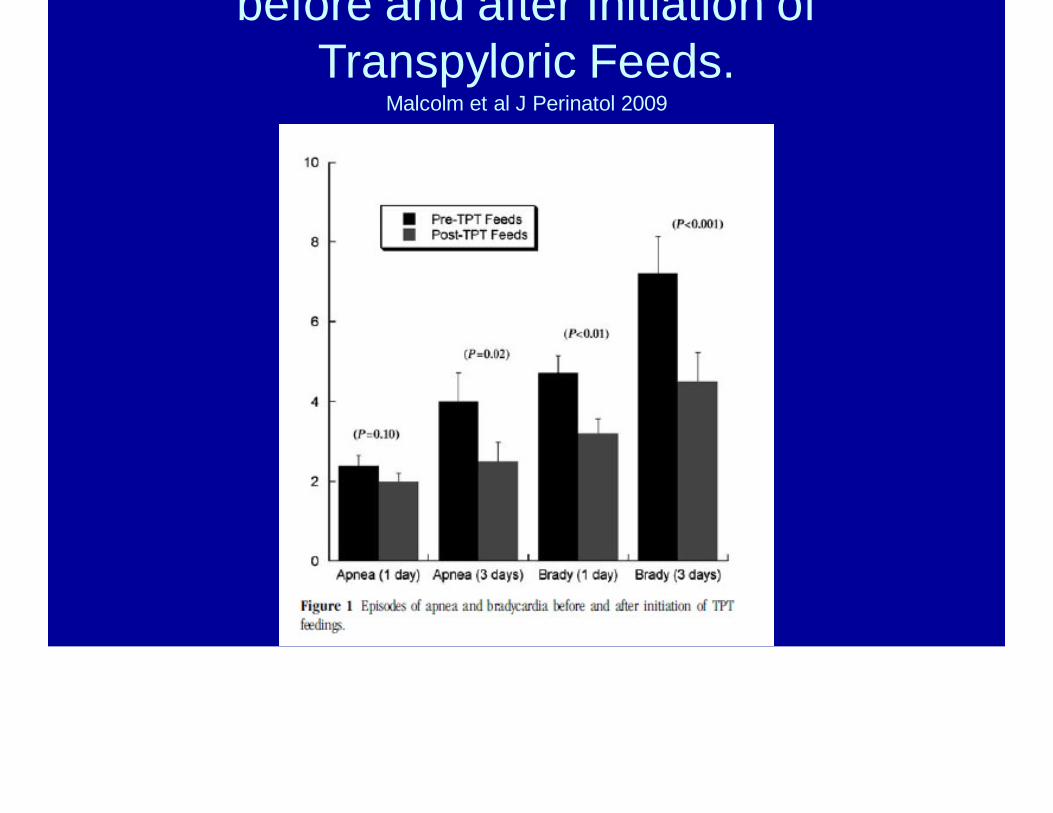
before and after Initiation of Transpyloric Feeds.
Malcolm et al J Perinatol 2009

pPneumonia free period
Sirvastava et al Pediatrics 2009

hour during feed (JF) and non-feed (NF) periods
Rosen et al, JPGN 2011
JF NF p Value
# Acid Events/hr 0.9±1.0 0.4±0.8 0.02
# Non-Acid Events/hr
1.3±1.3 0.7±1.1 0.04
# pH-Only Events/hr
0.5±0.8 0.3±0.6 0.3
# total MII/hr 2.2±1.4 1.1±1.2 0.003

.$i;lrv $ iN ,-S o l r . i ::.!1< : d o J11Po5mh: - i'd "-It i'-f'o
IO:lJ'I.I F":.,'111"'1..' \.' i1-:,1;- . ":1-. .r Jii"Joitl o.lil'li.:- lt.:.·; ,-1 r1:1 n Dl. l l ! ! . ln i . l
1NARNII\'"{; 1\/kiy c.aiJse ru1Jrin.J.1ing pulmoMIY e-dam . tock i h . ooirerOi.J$- 'I,J!Ier··.: . fi!"XII,Jrln:)ry ulCOillu f f'IC'. DtuL"Y 001 or $ ;:-t$ r•
mGII'hoid cme.m (41XC1J- !'.or u r I"ThOI:hGr in..lla\ )-
.-".'...HH
'...
--- J : l l i.
....,-.... :-. -._: .-:.-. -- t - •'!J-.... -=-"... a.. -::T tL.,:::; - -· ..........-·:--· s-· H- -... =-
f: ,)! -'=· .i'i ; ;
· - '='"?=.. ....
. - ::;: L•..--1
0r·""rH.•
-
...... ·_,:S... 2
.
'! ' .ill!.
:.;:.-
Made by retired rherd.Jlis-s l ivi lg a the""'11/hispe.ing ghs ..home lot" btlmooout AC..Ps
Reord.er by ca IIing 81))-661-5690 oronIine a1'Nw\•IJoocus. m
Summary
• Full column reflux matters• Acid suppression in the aerodigestive
patient requires thought and close followup
• Macrolides may be useful beyond their motility effect
• Fundoplication in the aerodigestive patientneeds thought (and a detailed consent)


















