
Nitric Oxide in Pulmonary Processes: Role in Physiology and Pathophysiology of Lung Disease

1997;112;1091-1101 ChestK Wasserman
Diagnosing cardiovascular and lung pathophysiology from exercise gas exchange
This information is current as of January 11, 2006
http://www.chestjournal.orglocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
or distributed without the prior written permission of the copyright holder. ISSN: 0012-3692. Road, Northbrook IL 60062. All rights reserved. No part of this article or PDF may be reproducedmonthly since 1935. Copyright 2005 by the American College of Chest Physicians, 3300 Dundee CHEST is the official journal of the American College of Chest Physicians. It has been published
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

Diagnosing Cardiovascular and LungPathophysiology From Exercise GasExchange*
Karlman Wasserman, MD, PhD, FCCP
(CHEST 1997; 112:1091-1101)
Abbreviations: ATP5adenosine triphosphate; CAD5coronaryartery disease; C(a-v)O25arterial mixed venous O2 content dif-ference; CM5cardiomyopathy; COPD-A and COPD-S5physically active (COPD patient) and sedentary (COPDpatient), respectively; CPET5cardiopulmonary exercise test;HR5heart rate; IC5inspiratory capacity; LAT5lactic acidosis(anaerobic) threshold; MVV5maximum voluntary ventilation;PAD5peripheral arterial disease; PetCO25end-tidal Pco2;R5respiratory exchange ratio (V̇co2/V̇o2); RLD5restrictive lungdisease; V̇co25carbon dioxide output; V̇e5minute ventilation;V̇o25oxygen consumption; DV̇o2/DWR5increase in V̇o2 relativeto increase in work rate; Vd/Vt5physiologic dead space ventila-tion; V̇/Q̇5ventilation/perfusion ratio; Vt5tidal volume
E xercise testing with gas exchange measurements,added to monitoring of the ECG and BP, has
been used to evaluate patients with heart and lungdisease since the immediate post-World War IIboom in medical research. It was particularly stim-ulated by the development of right heart catheter-ization with the interest in measuring cardiac outputand stroke volume during exercise by the direct Fickmethod. However, it was not widely used for routineclinical diagnostic studies because it was time con-suming, technically difficult, and expensive. Therewas also a general lack of appreciation for theinformation that could be obtained from such mea-surements.
With the development of rapidly responding elec-tronic gas analyzers to replace the technically moredemanding chemical methods for the measurementof respiratory gases, and the development of flow-meters that could measure instantaneous flow andvolume, the stage was set to measure gas exchange atthe time of exercise testing. This greatly decreasedthe technical time and therefore the cost to do gasexchange measurements. However, the assimilationof the large amount of data obtained from these testswas laborious. When digital computers became avail-able, this problem was solved, since the large num-ber of measurements obtained and required to ad-
dress questions of cardiovascular and lung functioncould be reduced to a graphic display.
Because the cardiovascular and pulmonary sys-tems are assessed when gas exchange is measuredduring exercise, these tests are referred to as cardio-pulmonary exercise tests (CPETs). It is now possibleto do a CPET with complete graphing output readyfor interpretation in 15 min. In 1960, this required 2days of two technicians, and much time of postdoc-toral fellows who had the task of doing final calcula-tions and graphing. The gain in technology was alsotranslated into patient safety and comfort becausecontinuous measurement of function allowed exer-cise work rate to be progressively increased relativelyrapidly to maximum tolerance while simultaneouslyfollowing the physiologic responses. This replacedtests in which large-step increases in work rate of 3 to6 min in duration were used, the latter ostensibly toobtain steady-state measurements at each work level.Because of the vast gain in efficiency in measuringgas exchange and data processing, it became possibleto extend CPET into the routine of medical practice.
The purposes for which CPETs are currently beingapplied attest to its growing importance in medicine.They include the following: (1) determining the patho-physiology of exercise limitation, differential diagnosis,and severity of impairment in function; (2) evaluatingdisability; (3) individualizing prescription for exerciserehabilitation programs; (4) determining risk from ma-jor surgery; (5) estimating survival potential in patientcandidates for heart transplantation; and (6) determin-ing efficacy of treatment modalities in patients withcardiovascular and respiratory diseases. The latter isdone by following parameters of aerobic function withserial testing.
In this review, I shall address the use of exercisegas exchange in evaluating pathophysiology of theorgan systems involved in the coupling of external tocellular respiration. I shall refer repeatedly to Figure1 since it provides the interaction of the physiologicrequirements to perform exercise and how interrup-tion or alteration of the integrative response mightaffect cellular and external respiration.
The basic requirement to sustain muscular exerciseis an increase in cellular respiration for regeneration ofadenosine triphosphate (ATP). To support the increase
*From the Division of Respiratory and Critical Care Medicine,Harbor-UCLA Medical Center, Torrance, Calif.
Manuscript received March 7, 1997; accepted March 10.Reprint requests: Karlman Wasserman, MD, PhD, Division ofRespir and Crit Care Med - Box 405, Harbor-UCLA MedicalCenter, 1000 W Carson St, Torrance, CA 90502
CHEST / 112 / 4 / OCTOBER, 1997 1091
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

in cellular respiration, O2 and CO2 transport betweenthe cells and the external airway must match the rate ofcellular respiration except for transient lags allowed bythe capacitances in the transport system, O2 stores onthe venous side of the circulation, and small stores ofhigh-energy phosphate in the form of creatine phos-phate in the myocytes. The increase in O2 and CO2transport is a function of the skeletal muscles, periph-eral circulation, heart, pulmonary circulation, blood,lungs, and respiratory muscles. The latter provide theventilation needed to refresh the gas in the alveoli foradding O2 and removing CO2 from the blood flowingthrough the lungs. Any defect in this interactive systemcan cause exercise limitation.
Pathophysiologic questions appropriate for a phy-sician to ask when caring for a patient with exerciseintolerance because of exercise-induced dyspnea orfatigue are shown in Table 1. Using current tech-niques for making measurements and imposing anexercise stress, CPET provides an efficient way ofaddressing the questions posed. Examples of diseasestates that might be present with “yes” answers to theposed questions are also listed in Table 1. By iden-tifying the pathophysiology of exercise limitation, acorrect clinical diagnosis accounting for the patient’ssymptom(s) is possible.
Cardiopulmonary Exercise Testing
Which Ergometer?
To stress the cardiorespiratory gas transportsystem, exercise testing should involve large mus-
cle groups. Practical laboratory ergometers in-volving large muscle groups are the treadmilland cycle. Although normal untrained subjectscan achieve a maximum oxygen consumption(V̇o2max) on the treadmill that is about 10%higher than they can achieve on the cycle, thecycle ergometer has the major advantage that thework output performed by the patient is known.(The merits of each ergometer have been com-pared by Wasserman et al.1) This is of overwhelm-ing importance because considerably more infor-mation is learned from CPET about cardiovascularfunction and gas exchange when the external workperformed by the subject is known. Therefore,when the quantitative response to exercise isimportant in the patient evaluation, we prefer touse the cycle ergometer.
Some physicians seem to think that the cycle is moretaxing to the ill patient than walking on a treadmill. Thisis not the case when using the modern ergometers nowavailable. In the typical, nonobese adult, unloadedcycling at 60 rpm only doubles the resting metabolicrate. This is less cardiovascular stress than walking atzero grade at 2 mph on the treadmill, because the cyclesupports the weight of the patient. Reducing thecycling speed reduces the metabolic rate further. Be-cause the work rate increase is known, the normalincrease in V̇o2 is predictable. The ability to relate theincrease in V̇o2 to the increase in work rate can revealcritically important diagnostic information, such asidentifying whether the primary cause of the exerciselimitation is due to coronary blood flow or peripheral
Figure 1. Scheme depicting the coupling of external to cellular respiration. V̇a5ideal alveolarventilation/time; V̇d5physiologic dead space ventilation/time; V̇e5total ventilation measured duringexpiration/time; Q̇o25O2 consumption; Q̇co25CO2 production; V̇o25O2 uptake; V̇co25CO2 out-put; creat-PO45creatine phosphate; Pyr5pyruvate; Lac5lactate; Mito5mitochondria. See text fordescription of pathophysiologic states that interfere with the normal coupling of external to cellularrespiration.
1092 Reviews
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

blood flow in the patient with atherosclerosis. This willbe discussed under the heading of “Diagnosis of Exer-cise Pathophysiology.”
Which Protocol?
Because of the ability to monitor exercise gas ex-change continuously, breath by breath or over shortperiods, it is possible to use progressively increasingwork rate protocols, in which the total duration ofincreasing work rate exercise is only 8 to 12 min, fromthe lowest work rate to exhaustion. The work rate canbe increased under computer control, smoothly inramp pattern, or in small steps of 1-min duration.Diagnostically, nothing is lost from these non-steady-state, progressive exercise tests and there is consider-able gain by being able to determine the V̇o2 at whichthe lactic acidosis (anaerobic) threshold develops. Ad-ditionally, the increase in V̇o2 can be determined aswork rate is increased (DV̇o2/Dwork rate), a measure-ment of particular importance when evaluating thecardiovascular function of patients. A grade of workrate is selected to complete the increasing work rateperiod in the desired time, recognizing that V̇o2 willnormally increase 10 mL/min/W. The patient’s pre-dicted V̇o2max can be determined by referring toappropriate reference equations. (Multiple sourceswere reviewed by Wasserman et al.)2 While the patientincreases work rate to the maximum, he or she exer-cises at that level for a relatively short period. Thus,
recovery is fast and the exercise test could be repeatedat a different rate of increase, or with O2 breathing ifthe examining physician thinks it desirable for a morecomplete patient evaluation.
Data Display for the Medical Record
CPET studies in recent years have taught us thatdifferent defects in the coupling of external (air-way) to cellular (mitochondrial) respiration willaffect gas exchange in different ways. Thus, thepattern of gas exchange at the airway can be usedto diagnose pathophysiology and used to supportor refute the correctness of a clinical diagnosis.With an appropriate display of the data, it ispossible to determine, noninvasively, the func-tional status of the cardiovascular system, theventilatory system, and the uniformity of matchingventilation to perfusion. Because a graphic is mucheasier to read than a tabular data display, wetransformed the CPET data into graphs. To avoidreviewing and interrelating multiple pages ofgraphs and overburdening the medical record withpages of tedious data, we gradually evolved asingle page of nine strategically positioned graphs.These graphs contain 15 plots that systematicallyassess cardiovascular, ventilatory, ventilation-per-fusion matching, and the metabolic responses toexercise (Fig 2). Normal target values such as
Table 1—Questions Addressed by Cardiopulmonary Exercise Testing*
Question Example of Disorder Markers for Abnormality
1. Is exercise capacity reduced? Any disorder Maximum V̇o2 - panel 32. Is the metabolic requirement for exercise
increased?Obesity V̇o2-WR relationship - panel 3
3. Is exercise limited by impaired O2 flow? Due to ischemic, myopathic,valvular, congenital heartdisease?
ECG; LAT; DV̇o2/DWR; V̇o2/HR - panels 2,3,5
Due to pulmonary vasculardisease?
DV̇o2/DWR; LAT; V̇o2/HR; V̇e/V̇co2 - panels 2,3,5,6
Due to peripheral arterial disease? BP; DV̇o2/DWR;LAT - panels 3,5Due to anemia, hypoxemia, or
COHb?LAT; V̇o2/HR - panels 2,3,5
4. Is exercise limited by reduced ventilatorycapacity?
Lung; chest wall BR;ventilatory response - panels 1,7,9
5. Is there an abnormal degree of V̇/Q̇mismatching?
Lung; pulmonary circulation;heart failure
P(A-a)O2; P(a-et)CO2; Vd/Vt; V̇e/V̇co2 - panels 4,6,9
6. Is there a defect in muscle utilization ofO2 or substrate?
Muscle glycolytic or mitochondrialenzyme defect
LAT, R, V̇co2; HR vs V̇o2; lactate;lactate/pyruvate ratio - panels 3,8
7. Is exercise limited by a behavioralproblem?
Neurosis Breathing pattern - panels 7,8
8. Is work output reduced because of pooreffort?
Poor effort with secondary gain HRR;BR; peakR; P(A-a)O2; P(a-et)CO2 - panels2,5,7,8
*Maximum V̇o25highest O2 uptake measured; WR5work rate; BR (breathing reserve)5maximum voluntary ventilation-ventilation at maximumexercise; DV̇o2/DWR5increase in V̇o2 relative to increase in work rate; Vd/Vt5physiologic dead space/tidal volume ratio; P(A-a)O25alveolar-arterial Po2 difference; COHb5carboxyhemoglobin; P(a-et)CO25arterial-end tidal Pco2 difference; HRR (heart rate reserve)5predictedmaximum heart rate-maximum exercise heart rate; V̇e/V̇co25ventilatory equivalent for CO2; Peak R5peak gas exchange ratio.
CHEST / 112 / 4 / OCTOBER, 1997 1093
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

V̇o2max and maximum heart rate (HR) are dis-played on specific plots. Normal values for all themeasurements in the nine-panel graphic array,described by multiple groups for CPET, are sum-marized elsewhere.2
Evaluation of Systemic Function From the Nine-Panel Graphic Array
The questions that could be asked of exercise testsare shown in Table 1. The answer to the first
Figure 2. Nine-panel graphic array used to describe the cardiovascular, ventilatory, V̇/Q̇ matching, andmetabolic responses to exercise in the medical record. Study is from a 55-year-old male patient(modified from case 1 of reference 4). The responses are normal. The diagonal line drawn on panel 3is the normal rate of increase in V̇o2 for the work rate increase (10 mL/min/W). V̇e5minute ventilation;HR5heart rate; R5respiratory exchange ratio (V̇co2/V̇o2); PetO25end-tidal Po2; PetCO25end tidalPco2; PaO25arterial Po2; PaCO25arterial Pco2; MVV5maximal voluntary ventilation; IC5inspiratorycapacity; VC5vital capacity; watt5unit of power output (work rate).
1094 Reviews
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

question relating to exercise capacity is addressed inpanel 3 from the measurement of maximum (peak)V̇o2. If it is reduced, we ask if the reduction is due toa cardiovascular limitation (panels 2, 3, and 5),ventilatory limitation (panels 1, 3, 4, and 7), ventila-tion-perfusion mismatching (panels 3, 6, and 9), orabnormality in use of metabolic substrate (panels 3and 8). The nine graphs describe the followingphysiology.
Panel 1—Minute Ventilation (V̇E) vs Work Rate:This normally becomes curvilinear as work rate isincreased above the lactic acidosis (anaerobic)threshold (LAT) except when ventilatory work isexcessive, eg, some patients with obesity or lungdisease.
Panel 2—HR and V̇O2/HR (Equal to StrokeVolume3Arteriovenous O2 Difference) vs WorkRate: HR is high and V̇o2/HR is low for a given workrate in patients with certain cardiovascular defectsexcept when under rate control or b-adrenergicblockade.
Panel 3—V̇O2 and Carbon Dioxide Output (V̇CO2)vs Work Rate and Slope Showing Predicted Rate ofIncrease in V̇O2 for the Work Rate Increase (Diago-nal Line): This is the first panel to address because itgives global assessment of the presence of exerciselimitation. Increase in V̇o2 relative to work rate(DV̇o2/WR) is commonly abnormal in patients withcardiovascular disease, the pattern varying with thedefect as described below. V̇co2 increases above V̇o2after a lactic acidosis develops and continues toincrease steeply despite flattening of V̇o2.
Panel 4—V̇E vs V̇CO2: This is a linear relationshipuntil ventilatory compensation for metabolic acidosis(becomes steeper) or CO2 retention (becomes moreshallow) develops. The slope of the linear part issteep when the exercise physiologic dead space/tidalvolume ratio (Vd/Vt) is increased.
Panel 5—HR vs V̇O2 and V̇CO2 vs V̇O2: HR in-creases linearly with V̇o2 to the predicted maximumsin normal subjects. In patients with heart failure orpulmonary vascular disease, the increase may lose itslinearity with HR increasing progressively more rap-idly than V̇o2. Up to the LAT, V̇co2 increaseslinearly with V̇o2 with a slope of one, or slightly lessthan one. Then V̇co2 increases more rapidly, thesteepening of the slope depending on the rate ofbuffering of lactic acid. The breakpoint describes theLAT. It will be low in patients with poor cardiovas-cular function.
Panel 6—Ventilatory Equivalent for O2 and CO2
(V̇E/V̇O2 and V̇E/V̇CO2) vs Work Rate: V̇o2 decreasesto a nadir at the LAT. V̇co2 decreases to a nadir atthe ventilatory compensation point. Both values arehigh with pulmonary vascular occlusive disease.
Panel 7—VT vs V̇E: The patient’s vital capacity and
inspiratory capacity (IC) are shown on the Vt axis,and actually measured maximum voluntary ventila-tion (MVV) or FEV1 times 40 are shown on the V̇eaxis. With airflow limitation, maximal exercise V̇eapproximates the MVV. Thus, the breathing reserve(MVV-V̇e at maximal exercise) is approximately zero.The breathing reserve cannot be predicted fromresting pulmonary function measurements alone.With restrictive lung disease, Vt may approximatethe IC at low work rates and respiratory rate mayultimately increase above 50 or 60 breaths perminute.
Panel 8—Respiratory Exchange Ratio (V̇CO2/V̇O2)(R) vs Work Rate: This usually starts at approxi-mately 0.8 and increases to above 1.0 above the LAT,although these values may be lower after long fast-ing. Inability or failure to produce an exercise lacticacidosis would mitigate increase to values above 1.Acute hyperventilation at rest and low work rates, asreflected by a decreasing end-tidal Pco2 (PetCO2),yields an R .1.
Panel 9—PETCO2 and End-Tidal PO2 vs WorkRate: Low PetCO2 signals either hyperventilation orhigh ventilation/perfusion ratio (V̇/Q̇) mismatching.R (panel 8) reveals if hyperventilation is acute.Arterial blood gases or knowledge of plasma HCO3
2
differentiates chronic hyperventilation from V̇/Q̇ ab-normality. Arterial blood gases are plotted on thisgraph to detect the presence of high and low V̇/Q̇mismatching.
Poor effort is likely to be revealed by a high HRreserve (panel 2), high breathing reserve (panel 7),and a low R (panel 8) at end exercise. In addition, thepatient may elicit a chaotic breathing pattern (panel7) that may cause end-tidal Pco2 and Po2 to be quitevariable (panel 9), the latter most evident duringbreath-by-breath monitoring.
Fitting Physiologic Abnormality to Disease Entity
Table 1 describes disorders possible with a positiveanswer to each of the questions posed and identifiesthe panels of the nine-panel graphics array thataddress the question. Panel 3 is always the first panelto examine because of its ability to define if overallfunction is reduced. The internal relationships of thispanel are then reviewed, including the relationshipof V̇o2 and V̇co2 to work rate and each other. Theother panels are then systematically reviewed for thepurpose of evaluating cardiovascular, ventilatory,V̇/Q̇ matching, and metabolic abnormality. Panels 3,2, and 5 are characteristically abnormal with cardio-vascular disease. Lung and chest wall diseases com-monly cause abnormalities in panels 1 and 7. Whenlung and heart diseases are accompanied by V̇/Q̇abnormality, panels 4, 6, and 9 are affected. Panels 3
CHEST / 112 / 4 / OCTOBER, 1997 1095
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

and 8 are the metabolic plots and help address acutehyperventilation and adequacy of exercise effort.
Obesity, Cigarette Smoking, and AnemiaComplicate Interpretation
Three physiologic derangements, not usually con-sidered as diseases of the cardiorespiratory system,may contribute significantly to exercise intolerancedue to common cardiorespiratory disorders. Thesephysiologic derangements are (1) obesity, (2) ane-mia, and (3) carboxyhemoglobinemia secondary tocigarette smoking.
Obesity adds to the O2 and cardiac output cost ofexercise. It also restricts the ventilatory system andincreases the work of breathing. These factors be-come more marked as the V̇e requirement increases.
Anemia reduces the arterial O2 content and themaximal arteriovenous O2 difference. Therefore, toachieve a given V̇o2, a greater cardiac output isrequired than if anemia were not present. Also,because the O2 content of the arterial blood isreduced, the capillary Po2 decreases to its criticalvalue, inducing anaerobic metabolism and lacticacidosis to take place at a reduced work rate and V̇o2.
The increased carboxyhemoglobin of the heavycigarette smoker is about 10 to 12%. This not onlyreduces the arterial O2 content to a level that wouldbe found in patients with an arterial Po2 of about 50to 55 mm Hg, but also shifts the oxyhemoglobindissociation curve to the left making it more difficultfor O2 to dissociate from hemoglobin at a given Po2.Thus, the capillary Po2 would fall more rapidly to itscritical value, resulting in a lactic acidosis at areduced level of work.
The net effect of these complicating factors is thatthe amount of external work that the patient canperform is reduced. However, in obesity, the maxi-mal V̇o2 and LAT are normal or high. With anemiaand increased carboxyhemoglobinemia, the maximalV̇o2, LAT, and peak work rate may all be reduced.
Diagnosis of Exercise Pathophysiology
Exercise requires an increase in gas transportbetween the airway and mitochondria. Figure 1illustrates the physiologic mechanisms that must becoupled to achieve this gas exchange. Exercise limi-tation is caused by any disease state that disrupts thenormal gas exchange coupling.
Our approach to diagnosis of exercise pathophys-iology has been to use the nine-panel graphic arrayexemplified by Figure 2. We start with panel 3because it quantifies the peak V̇o2. We also start withthis panel because the pattern of increase in V̇o2 isoften abnormal in cardiovascular disorders, with the
abnormal pattern differing depending on the patho-physiologic condition. After reviewing the plots inpanel 3, the remaining panels are reviewed to eval-uate the physiologic state of coupling at each point inthe interactive process schematized in Figure 1.
A flow chart system has been developed to assistthe interpreter of exercise tests in selecting thedominant gas exchange pathophysiology limiting ex-ercise.3 Only the nine-panel graphic array for apatient with a normal response is presented herein(Fig 2). It is not possible in this format to discuss thedifferent features of all diseases known to interruptthe normal coupling of external to cellular respira-tion. Therefore, I have limited this analysis to thepathophysiology of three common cardiovasculardisorders, three common pulmonary disorders, andtwo disorders for which the diagnosis is uniquelymade by CPET. See the case presentations withnine-panel graphs in the article by Wasserman et al4for a more comprehensive presentation of examplesof cardiorespiratory diseases that impair exerciseperformance.
Differential Features in Exercise Gas Exchange inCoronary Artery Disease, Cardiomyopathy, andPeripheral Arterial Disease
In this section, the physiologic responses to CPETare contrasted in three different types of cardiovas-cular disease, including coronary artery disease(CAD), cardiomyopathy (CM), and peripheral arte-rial disease (PAD). It is important to distinguish therelative importance of the pathophysiology in thesethree conditions because they are commonly foundin the same patient. Knowing the limiting pathophys-iology would enable the patient’s physician to focuson the therapeutic modality most likely to relieve thepatient’s symptom(s).
Peak V̇O2 (Cardiac Output) and DV̇O2/DWR (Panel3): V̇o2 is equal to cardiac output times arterial-mixed venous O2 difference (C[a-v]O2). Cardiacoutput increases linearly with V̇o2 in normal subjectsand most heart failure patients with the same slope(approximately 6 L/min cardiac output per liter V̇o2)except for the most severe heart failure patients inwhom the slope is more shallow.5(p161,181) C(a-v)O2also increases approximately linearly with percent ofV̇o2max to the same peak value (approximately 80 to85% extraction) in heart disease patients5(p200) andnormal subjects6 alike. Therefore, V̇o2 becomes asurrogate measure of cardiac output and strokevolume provided the investigator knows the HR andfraction of the peak V̇o2 value.5(p200),6 While peakV̇o2 will be decreased below predicted in patientswith myocardial ischemia due to CAD, exerciselimitation due to CM, and claudication due to PAD,
1096 Reviews
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

the patterns of increase in V̇o2 and V̇co2 with workrate differ in all three cardiovascular conditions.
In CAD, the myocardial O2 supply may be ade-quate to support the O2 requirement at rest and lowwork rates. V̇o2 will increase linearly with work rateat a slope of about 10 mL/min/W, parallel to thediagonal line drawn with a slope of 10 mL/min/W onpanel 3 of Figure 2. V̇co2 will be slightly less thanV̇o2 and will increase in a similar pattern to V̇o2.However, when exercise drives up the myocardialwork as HR and BP increase, the myocardial O2 (andblood flow) requirement increases. Regions of themyocardium with limited ability to increase theirblood flow will be unable to contract. If a largeenough area of the myocardium is involved, strokevolume will decrease. As exercise work rate is in-creased, the falling stroke volume will prevent thecardiac output from sustaining its rate of increase. Atthat work rate, the slope of rise in V̇o2, the surrogatemeasure of cardiac output change, abruptly de-creases (Fig 3). In our experience, the ECG showselectrical evidence of myocardial ischemia at workrates soon after the abrupt change in DV̇o2/DWR(slope of increase in V̇o2 relative to work rateincrease) in patients with CAD. Chest pain is com-monly absent. The decrease in slope signals that therate of anaerobic ATP regeneration and lactate
accumulation is high in muscle. Reflecting thischange in source of ATP regeneration is an increasein V̇co2 relative to V̇o2, the difference being strikingsince V̇co2 continues to increase steeply, while V̇o2abruptly decreases its rate of rise (Fig 3).
In CM, DV̇o2/DWR commonly decreases as workrate increases when cardiac output fails to increaselinearly with work rate. The change is generallygradual rather than abrupt like that observed whenthe contracting myocardium becomes ischemic. Thedecreased DV̇o2/DWR signals that the rate of anaer-obic ATP regeneration and lactate accumulation ishigh. Reflecting this change in source of ATP regen-eration is the increase in V̇co2 relative to V̇o2, as inCAD. Thus, V̇co2 continues to increase steeply withwork rate in CM, as in CAD, but the pattern ofincrease in V̇o2 differs.
In PAD, V̇o2 increase will be linear but moreshallow than normal during the progressive exercisetest (Fig 4), because the high resistance of theconducting arteries leading to the exercising muscleprevents an appropriate increase in muscle perfusiondespite local hyperemia. The slow increase in V̇o2 isaccompanied by a slow increase in V̇co2 in contrastto patients with CAD and CM. In PAD, the slope ofV̇co2 vs work rate is usually more shallow than 10mL/min/W and similar to the V̇o2 vs work rate slope.This contrasts with that observed for CAD and CM
Figure 4. Panel 3 of a nine-panel graphic array of a 65-year-olddiabetic, cigarette-smoking man with exercise limitation second-ary to leg pain characteristic of claudication. ECG was normalduring exercise. V̇o2 and V̇co2 increase at a slower rate thannormal (diagonal line) showing that the aerobic response to theimposed work rate was increasing at an inappropriately low rate.Predicted V̇o2max is shown.
Figure 3. Panel 3 of a nine-panel graphic array of a 47-year-oldmale patient with nonanginal ischemic heart disease. ST segmentof ECG showed progressive down-sloping above 150 W reaching3 mm by the end of exercise in leads II and V4 by the end ofexercise. There was no chest pain. ECG changes resolved by 5min of recovery. There was no ectopy. Failure for V̇o2 to increasewith the slope of the diagonal line past 150 W, despite increasingwork rate, is evidence that cardiac output failed to increasenormally. Predicted V̇o2max is shown.
CHEST / 112 / 4 / OCTOBER, 1997 1097
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

patients in whom the V̇co2 vs work rate slope is .10mL/min/W. The reduced rate of CO2 output fromthe exercising muscle in PAD is likely due to theretention of much of the extra CO2 produced byanaerobic metabolism in the ischemic muscle alongwith lactate. Thus, the lactic acidosis cannot bereadily reflected in the lung gas exchange in contrastto that observed in CAD and CM patients.
LAT and Stroke Volume (Panel 5 and 2): In CAD,the LAT determined by the breakpoint in the plot ofV̇co2 vs V̇o2 (V-slope plot, panel 5) usually takesplace at the V̇o2 where there is myocardial ischemia,slowing the rate of V̇o2 increase with work rate. Thiscommonly takes place above the predicted lowerlimit of normal for LAT. Therefore, the LAT isusually normal in patients who develop myocardialischemia during exercise, unless functional myocar-dial ischemia develops with minimal exercise.
Concurrent with the reduction in DV̇o2/DWR inCAD is the steepening in HR vs V̇o2 instead of thelinear relationship usually observed with increasingwork rate (panel 5, Fig 2). The steepening of HRcomplements the decreasing stroke volume (reflect-ed by the abrupt reduction in rate of increase in V̇o2vs work rate) as work rate is increased above theLAT. Also the V̇o2/HR ratio (O2-pulse) (panel 2)does not increase normally above the work rate atwhich myocardial ischemia with dyskinesis occurs.Since the O2-pulse measures the product of strokevolume and C(a-v)O2, the unchanging O2-pulse sug-gests that the reduction in stroke volume is offset byan increasing C(a-v)O2.
In contrast to the CAD patient, the patient withsignificant CM will have a low LAT, depending onthe severity of the limitation in forward output (O2flow). The HR-V̇o2 relationship is steep but it rarelyreaches its predicted maximum because fatigue lim-its the patient. Thus, there is a significant HRreserve. The O2-pulse is low, but in contrast to CAD,the flattening in O2-pulse is less abrupt.
In PAD, as in all metabolic states in which ATP isregenerated anaerobically, lactic acid is produced.Since this acid is over 99% dissociated at the pH ofcells, it is almost totally buffered by HCO3
2 upon itsformation in the exercising muscle. This will result inincreased CO2 production relative to V̇o2. However,this is difficult to assess by the gas exchange methods(eg, V-slope) because much of this buffer-derivedCO2 is retained in the muscle due to the relativelylow blood flow through the ischemic limb. Conse-quently, an accurate assessment of the subject’s LATwould be difficult in patients limited by PAD.
The HR vs V̇o2 slope is linear in PAD, but thepeak predicted HR is not reached because exercisefatigue and leg pain develop before the centralcirculation is maximally stressed. Consequent to the
increased resistance to blood flow in the majorconducting vessels caused by obstructing atheroscle-rotic lesions and the nonlimiting cardiac outputresponse, marked BP increases take place at lowwork rates.
Breathing Reserve and Pattern (Panel 7): V̇e in-creases during exercise, predominantly by increasingVt at lower work rates and also increasing breathingrate at higher levels of exercise. There is nothingparticularly abnormal about the breathing pattern inthe CAD and PAD patient, and the maximumexercise ventilation is considerably below the MVV.However, the CM patient generally responds toexercise with a smaller Vt and greater breathingfrequency for a given exercise ventilation than nor-mal, the altered breathing pattern being moremarked, the worse the heart failure.7-10
V̇/Q̇ Mismatching (Panels 4, 6, and 9): Patientswith CAD with exercise myocardial ischemia and/orPAD manifestating claudication have normal unifor-mity in ventilation relative to perfusion. Thus, panels4, 6, and 9 are normal in these disorders. In contrast,patients with CM have a high V̇/Q̇ mismatchingabnormality. Therefore V̇e/V̇co2 is especially high inthese patients. Because of the high V̇/Q̇ lung units,PetCO2 will tend to be low, without evidence ofacute hyperventilation as can be deduced from anormal R (panel 8). The contribution of high V̇/Q̇lung units to overall ventilation results in a steepslope in the plot of V̇e vs V̇co2 (panel 4). Theabnormal steepness of the slope is primarily due to ahigh physiologic dead space ventilation (Vd/Vt) inthese patients. The more abnormal the heart func-tion, the steeper the slope.7,8,10
Differential Features in Exercise Gas Exchange inCOPDs, Sedentary and Physically Active, andRestrictive Lung Disease
In this section, I shall illustrate the gas exchangecharacteristics of three patients with different com-monly encountered lung disorders, a physically ac-tive COPD patient (COPD-A), a COPD patient whohas been sedentary (COPD-S), and a patient char-acterized by restrictive lung disease (RLD) as seen inpatients with idiopathic pulmonary fibrosis, connec-tive tissue disease, or sarcoidosis. In describing thesethree pulmonary conditions, I shall again refer toFigure 2 to illustrate how the pathophysiology ofeach condition alters the graphic description of thecardiovascular, ventilatory, V̇/Q̇, and metabolic re-sponses to exercise.
Peak V̇O2 (Cardiac Output) and DV̇O2/DWR (Panel3): The patterns of increase in V̇o2 and V̇co2 differ inthe three lung disorders that are the subject of discus-sion. In the COPD-A patient, V̇o2 will increase linearly
1098 Reviews
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from
with work rate at a slope of about 10 mL/min/W(parallel to the diagonal drawn on panel 3 of Fig 2).V̇co2 will be slightly less than V̇o2 and will increaseparallel to it, possibly never increasing above V̇o2,depending on the degree of airflow obstruction. Inother words, the patient, being physically active, doesnot develop a significant lactic acidosis before he isforced to stop exercise because of breathlessness fromventilatory limitation (panel 7).
In the COPD-S patient, V̇o2 will increase linearlyin the same fashion as in the COPD-A patientbecause forward output is not impaired by limitedheart function or pulmonary vascular resistance. Incontrast, V̇co2 will increase more steeply than V̇o2 ata relatively low work rate because the skeletal mus-cles of locomotion are deconditioned. Decondition-ing results in decreased muscle capillarity and moresparse mitochondrial density in muscle. These fac-tors define the surface area and diffusion distance inthe functional muscle unit and therefore dictate thecapillary Po2 needed to achieve the O2 flow fromblood to mitochondria. Detraining would cause a netincrease in lactate production in the active muscle ata higher capillary Po2 and lower V̇o2 than in thetrained state. The increase in V̇co2 and H1 causedby the lactic acidosis drives ventilation above that ofthe COPD-A patient. The presence of arterial hy-poxemia and/or increased carboxyhemoglobin willfurther disadvantage the O2 supply to the muscleduring exercise11 and cause V̇co2 to increase at astill-greater rate than V̇o2.
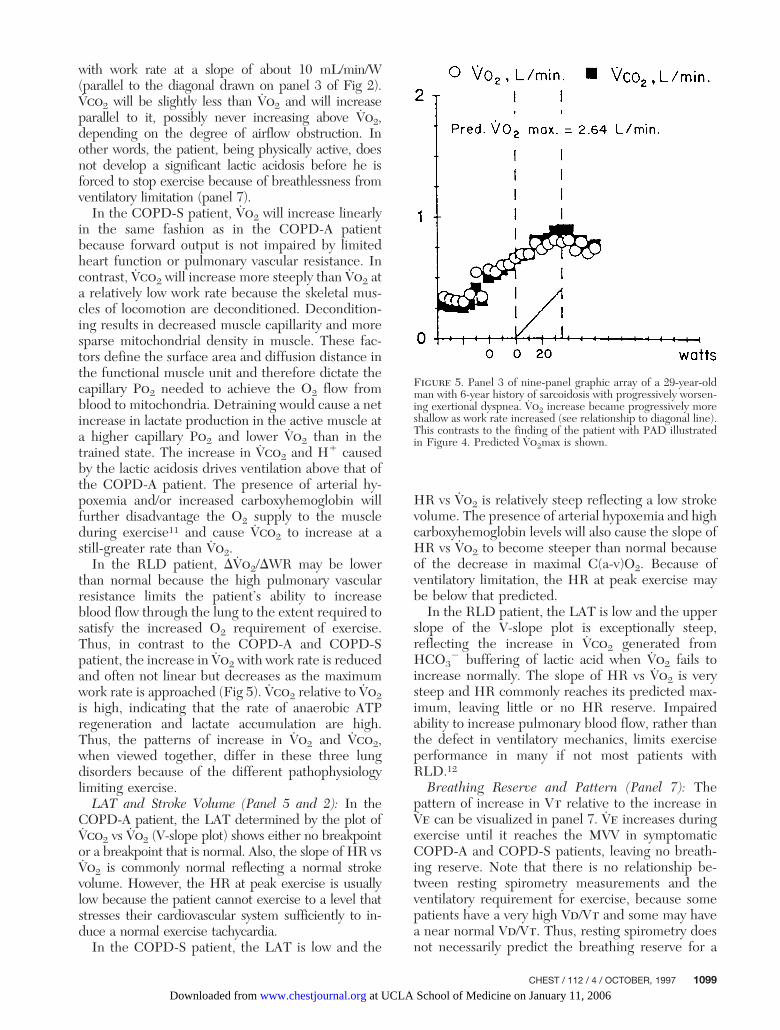
In the RLD patient, DV̇o2/DWR may be lowerthan normal because the high pulmonary vascularresistance limits the patient’s ability to increaseblood flow through the lung to the extent required tosatisfy the increased O2 requirement of exercise.Thus, in contrast to the COPD-A and COPD-Spatient, the increase in V̇o2 with work rate is reducedand often not linear but decreases as the maximumwork rate is approached (Fig 5). V̇co2 relative to V̇o2is high, indicating that the rate of anaerobic ATPregeneration and lactate accumulation are high.Thus, the patterns of increase in V̇o2 and V̇co2,when viewed together, differ in these three lungdisorders because of the different pathophysiologylimiting exercise.
LAT and Stroke Volume (Panel 5 and 2): In theCOPD-A patient, the LAT determined by the plot ofV̇co2 vs V̇o2 (V-slope plot) shows either no breakpointor a breakpoint that is normal. Also, the slope of HR vsV̇o2 is commonly normal reflecting a normal strokevolume. However, the HR at peak exercise is usuallylow because the patient cannot exercise to a level thatstresses their cardiovascular system sufficiently to in-duce a normal exercise tachycardia.
In the COPD-S patient, the LAT is low and the
HR vs V̇o2 is relatively steep reflecting a low strokevolume. The presence of arterial hypoxemia and highcarboxyhemoglobin levels will also cause the slope ofHR vs V̇o2 to become steeper than normal becauseof the decrease in maximal C(a-v)O2. Because ofventilatory limitation, the HR at peak exercise maybe below that predicted.
In the RLD patient, the LAT is low and the upperslope of the V-slope plot is exceptionally steep,reflecting the increase in V̇co2 generated fromHCO3
2 buffering of lactic acid when V̇o2 fails toincrease normally. The slope of HR vs V̇o2 is verysteep and HR commonly reaches its predicted max-imum, leaving little or no HR reserve. Impairedability to increase pulmonary blood flow, rather thanthe defect in ventilatory mechanics, limits exerciseperformance in many if not most patients withRLD.12
Breathing Reserve and Pattern (Panel 7): Thepattern of increase in Vt relative to the increase inV̇e can be visualized in panel 7. V̇e increases duringexercise until it reaches the MVV in symptomaticCOPD-A and COPD-S patients, leaving no breath-ing reserve. Note that there is no relationship be-tween resting spirometry measurements and theventilatory requirement for exercise, because somepatients have a very high Vd/Vt and some may havea near normal Vd/Vt. Thus, resting spirometry doesnot necessarily predict the breathing reserve for a
Figure 5. Panel 3 of nine-panel graphic array of a 29-year-oldman with 6-year history of sarcoidosis with progressively worsen-ing exertional dyspnea. V̇o2 increase became progressively moreshallow as work rate increased (see relationship to diagonal line).This contrasts to the finding of the patient with PAD illustratedin Figure 4. Predicted V̇o2max is shown.
CHEST / 112 / 4 / OCTOBER, 1997 1099
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

given level of exercise. In the COPD patient, Vtincreases predominantly at low work rates, and thenbreathing frequency increase becomes progressivelymore important. Vt generally remains below the IC,as is the case in normal subjects. In the RLD patient,Vt reaches its maximal value at a relatively lowexercise level. The upper limit for Vt increase isusually the IC. Thus, respiratory rate increase isusually greater in the RLD patient than in theCOPD patient.
V̇/Q̇ Mismatching (Panels 4, 6, and 9): Patientswith COPD generally have a modestly elevatedV̇e/V̇co2 at the LAT or maximum work rate becauseof mismatching of V̇/Q̇. The PetCO2 is low, reflect-ing the function of the high V̇/Q̇ lung units whichcompensate for the CO2 retention of the low V̇/Q̇lung units, the net effect usually being arterialeucapnia. In some patients with hypercapnia, V̇e/V̇co2 may be normal, with the overall hypoventila-tion masking the effect of high V̇/Q̇ lung units.However, some patients with COPD have a largeamount of pulmonary vascular occlusive disease.Thus, high V̇/Q̇ lung units (high Vd/Vt) make a largecontribution to overall ventilation. This forces venti-lation to be high for a given metabolic rate asreflected by an exceptionally high V̇e/V̇co2 (panel 6)and a steep slope of V̇e vs V̇co2 (panel 4). RLDpatients usually have a considerable loss of pulmo-nary capillary bed relative to loss of airways. Thisresults in a preponderance of high V̇/Q̇ lung units.Therefore, V̇e/V̇co2 is especially high in RLD pa-tients. Because of the high V̇/Q̇ lung units, PetCO2will tend to be low, without evidence of acutehyperventilation, as deduced from a normal R (panel8). The greater contribution of high V̇/Q̇ lung units tooverall ventilation, the steeper will be the plot of V̇evs V̇co2.
Diagnoses Uniquely Made by CardiopulmonaryExercise Testing
Severe Pulmonary Vascular Disease Without Pulmo-nary Hypertension: Most patients limited in exercisebecause of pulmonary vascular disease have short-ness of breath with exercise before they have theresting physical signs of pulmonary hypertension.Once the signs of pulmonary hypertension arepresent, the patient has occluded most of his or herfunctional pulmonary circulation, their clinical con-dition is quite tenuous, and the physician has lost theopportunity to perform simple diagnostic studies orintervene with specific treatment modalities. Thetest method that should be most sensitive in reveal-ing developing pulmonary vascular occlusive diseaseis CPET, because the patient’s symptoms are present
during exercise. While the pulmonary blood flowmay be adequate at rest, these patients have diffi-culty in increasing pulmonary blood flow appropri-ately in response to exercise, resulting in exercise-induced symptoms. During exercise, V̇o2 usuallyfails to continue to increase with a normal slope of 10mL/min/W, but the slope progressively decreases tothe point of fatigue when there may be no furtherrise (panel 3). The peak V̇o2 (panel 3) and LAT(panel 5) probably provide the best quantitation ofseverity of the illness. A steep HR response and lowO2-pulse will be evident in panel 5 and 2, respec-tively. Panel 6 would show a high value for V̇e/V̇co2at the LAT, reflecting decreased perfusion to venti-lated lung (high V̇/Q̇). Arterial blood gases displayedon panel 9 with end-tidal O2 and CO2 and calcula-tion of Vd/Vt would further characterize the abnor-mal physiologic state.
Foramen Ovale Patency With Development of aRight to Left Shunt During Exercise: The anatomybooks report that 25% of the population have a poten-tially patent foramen ovale. However, this is unimpor-tant unless such a person develops right atrial pressuresthat exceed left atrial pressures. The latter can developin patients with primary pulmonary vascular disease orpulmonary vascular disease secondary to lung disease.But even with these disorders and a potentially patentforamen ovale, the patient may not shunt venous rightatrial blood into the left atrium at rest, only duringexercise. If the increase in venous return during exer-cise exceeds the rate that the right ventricle can pumpblood into the pulmonary circulation, right ventricularend-diastolic and therefore right atrial pressure willincrease above the resting value. When right atrialpressure exceeds left atrial pressure during exercise,systemic venous blood can enter the left atrium causingrapid systemic arterial oxygen desaturation through apatent foramen ovale. This can take place despite anormal or near-normal arterial oxyhemoglobin satura-tion at rest. The exercise test repeated during 100% O2breathing with arterial blood sampling allows this diag-nosis to be confirmed. Panels 3, 4, 6, and 9 would beparticularly revealing of this diagnosis. Not only isCPET a specific test for this diagnosis, but it is a testwith minimal morbidity and relatively small cost.
Conclusion
Evidence has been presented showing how CPETcan be used, as a single method, to discriminate amongnonanginal myocardial ischemia, CM, and PAD as themajor pathophysiology limiting exercise in patients withcardiovascular disease. Similarly, CPET is the onlymethod that can discern if a given pulmonary functionimpairment limits exercise; it would also seem to be the
1100 Reviews
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

best noninvasive method to determine if a patient islikely to benefit from an exercise training programwhich can be expected to reduce the exercise-inducedlactic acidosis. It is also useful for defining the domi-nant disorder and directing therapy in patients withmultiple illnesses. In addition, it is uniquely valuable formaking some diagnoses such as the development of aright to left shunt during exercise, demonstrating thatpulmonary vascular occlusive disease is limiting exer-cise and detecting myocardial dyskinesis limiting exer-cise (increasing work rate and heart rate without anappropriate increase in V̇o2) in ischemic heart diseasepatients.
In summary, diseases of the cardiovascular systemand the lungs translate into abnormal gas exchangeduring exercise (Fig 1). There is also evidence thatpeak V̇o2 and the LAT may provide the best quan-titation of the degree of impairment in cardiovascu-lar function,13-15 and probably at the least cost.Therefore CPET, with measurements of gas ex-change, should play a major role in the evaluation ofpatients with cardiovascular and lung diseases whenthe cause of exercise intolerance due to dyspnea orfatigue is uncertain. Also, it is likely to be especiallyvaluable in determining the severity of functionallimitation. Patients with cardiovascular and/or pul-monary defects commonly go to their physicianbecause of exercise intolerance. Given the fact thatthe primary roles of the cardiovascular system andventilatory system are gas exchange between thecells and the air, it is remarkable that so few patientsundergo CPET before they undergo much moreexpensive imaging and invasive tests. It is importantfor physicians to appreciate that CPET is a powerfuldiagnostic tool with great decision-making value inguiding the management of patients with cardiovas-cular and lung diseases.
References1 Wasserman K, Hansen JE, Sue DY, et al. Protocols for
exercise testing. In: Principles of exercise testing and inter-
pretation. 2nd ed. Baltimore: Williams and Wilkins, 1994;95-111
2 Wasserman K, Hansen JE, Sue DY, et al. Normal values. In:Principles of exercise testing and interpretation. 2nd ed.Baltimore: Williams and Wilkins, 1994; 112-31
3 Wasserman K, Hansen JE, Sue DY, et al. Principles ofinterpretation. In: Principles of exercise testing and inter-pretation. 2nd ed. Baltimore: Williams and Wilkins, 1994;132-44
4 Wasserman K, Hansen J, Sue DY, et al. Case presentations.In: Principles of exercise testing and interpretation. 2nd ed.Baltimore: Williams and Wilkins, 1994; 145-431
5 Weber KT, Janicki JS. Cardiopulmonary exercise testing:physiologic principles and clinical applications. Philadelphia:WB Saunders, 1986; 161, 181, 200
6 Stringer WW, Hansen J, Wasserman K. Cardiac outputestimated noninvasively from oxygen uptake during exercise.J Appl Physiol 1997; 82:908-12
7 Sullivan MJ, Higginbotham MB, Cobb FR. Increased exer-cise ventilation in patients with chronic heart failure: intactventilatory control despite hemodynamic and pulmonaryabnormalities. Circulation 1988; 77:552-59
8 Metra M, Raccagni D, Carini G, et al. Ventilatory and arterialblood gas changes during exercise in heart failure. In: Was-serman K, ed. Exercise gas exchange in heart disease. Arr-monk, NY: Futura, 1996; 125-43
9 Kobayashi T, Itoh H, Kato K. The role of increased deadspace in the augmented ventilation of cardiac patients. In:Wasserman K, ed. Exercise gas exchange in heart disease.Arrmonk, NY: Futura, 1996; 45-156
10 Kleber F, Reindl I, Wernecke K, et al. Dyspnea in heartfailure. In: Wasserman K, ed. Exercise gas exchange in heartdisease. Arrmonk, NY: Futura, 1996; 95-108
11 Koike A, Weiler-Ravell D, McKenzie K, et al. Evidence thatthe metabolic acidosis threshold is the anaerobic threshold.J Appl Physiol 1990; 68:2521-26
12 Hansen JE, Wasserman K. Pathophysiology of activity limi-tation in patients with interstitial lung disease. Chest 1996;109:1566-76
13 Stevenson LW, Steimle AE, Fonarow G, et al. Improvementin exercise capacity of candidates awaiting heart transplanta-tion. J Am Coll Cardiol 1995; 25:153-70
14 Older P, Smith R, Courtney P, et al. Preoperative evaluationof cardiac failure and ischemia in elderly patients by cardio-pulmonary exercise testing. Chest 1993; 104:701-04
15 Stelken AM, Younis LT, Jennison SH, et al. Prognostic valueof cardiopulmonary exercise testing using percent achieved ofpredicted peak oxygen uptake for patients with ischemic anddilated cardiomyopathy. J Am Coll Cardiol 1996; 27:345-52
CHEST / 112 / 4 / OCTOBER, 1997 1101
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from

1997;112;1091-1101 ChestK Wasserman
Diagnosing cardiovascular and lung pathophysiology from exercise gas exchange
This information is current as of January 11, 2006
& ServicesUpdated Information
http://www.chestjournal.orgfigures, can be found at: Updated information and services, including high-resolution
Citations http://www.chestjournal.org#otherarticles
This article has been cited by 10 HighWire-hosted articles:
Permissions & Licensing
http://www.chestjournal.org/misc/reprints.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.chestjournal.org/misc/reprints.shtml
Information about ordering reprints can be found online:
Email alerting serviceup in the box at the top right corner of the online article. Receive free email alerts when new articles cite this article sign
Images in PowerPoint format
article figure for directions. teaching purposes in PowerPoint slide format. See any online Figures that appear in CHEST articles can be downloaded for
at UCLA School of Medicine on January 11, 2006 www.chestjournal.orgDownloaded from


















