DIABETES UPDATE NON INSULIN THERAPY - ACP · DIABETES UPDATE – NON INSULIN THERAPY FOCUS ON:...
60
DIABETES UPDATE – NON INSULIN THERAPY FOCUS ON: INCRETIN THERAPY (DPP41, GLP1-RA) & SGLT2 INHIBITORS American College of Physicians (ACP) Northern California Chapter Scientific Meeting Walnut Creek (2017) Jaiwant Rangi, MD, FACE
Transcript of DIABETES UPDATE NON INSULIN THERAPY - ACP · DIABETES UPDATE – NON INSULIN THERAPY FOCUS ON:...

DIABETES UPDATE – NON INSULIN THERAPY FOCUS ON: INCRETIN THERAPY (DPP41, GLP1-RA) & SGLT2 INHIBITORS
American College of Physicians (ACP)
Northern California Chapter Scientific Meeting
Walnut Creek (2017)
Jaiwant Rangi, MD, FACE

Disclosures
Consultant and Speaker for Sanofi,
Boehringer- Ingelheim, Astra Zeneca, Dexcom,
AbbVie and Jannsen

Available Drugs for the Treatment
of Type 2 Diabetes Mellitus- 2017

Non-Insulin Agents Available for
Treatment of Type 2 Diabetes Class Primary Mechanism of Action Agent Available as
ALPHA GLUCOSIDASE
INHIBITORS
Delay carbohydrate absorption
from intestine
Acarbose Precose or generic
Miglitol Glyset
AMYLIN
ANALOGUES
Decrease glucagon secretion
Slow gastric emptying
Increase satiety
Pramlintide Symlin
BIGUANIDES
Decrease HGP
Increase glucose uptake in
muscle
Metformin Glucophage or generic
BILE ACID SEQUESTRANTS
Decrease absorption / HGP?
Increase incretin levels? Colesevelam WelChol
DPP-4 INHIBITORS
Increase glucose-dependent
insulin secretion
Decrease glucagon secretion
Alogliptin Nesina
Linagliptin Tradjenta
Saxagliptin Onglyza
Sitagliptin Januvia
DOPAMINE
AGONISTS
Activates dopaminergic
receptors Bromocriptine Cycloset

Non-Insulin Agents Available
for Treatment of Type 2
Diabetes Class Primary Mechanism of Action Agent Available as
GLINIDES Increase insulin secretion Nateglinide Starlix or generic
Repaglinide Prandin
GLP-1 RECEPTOR AGONISTS
Increase glucose-dependent
insulin secretion
Decrease glucagon secretion
Slow gastric emptying
Increase satiety
Exenatide Byetta
Exenatide XR Bydureon
Liraglutide Victoza
Albiglutide
Tanzeum
Dulaglutide Trulicity
Lixisenatide Lyxumia *
SGLT2 INHIBITORS Increase urinary excretion of
glucose
Dapagliflozin Farxiga
Canagliflozin Invokana
Empagliflozin Jardiance
Iprafliflozin Suglat
SULFONYLUREAS Increase insulin secretion
Glimepiride Amaryl or generic
Glipizide Glucotrol or generic
Glyburide Diaeta, Glynase, Micronase, or generic
THIAZOLIDINEDIONES (TZD’S)
Increase glucose uptake in
muscle and fat
Decrease HGP
Pioglitazone Actos
Rosiglitazone Avandia

Combination Agents Available for the Treatment of
Type 2 Diabetes
Class Added Agent Available as
DPP4i + SGLT2i Saxagliptin/Empagliflozin Glyxambi
METFORMIN + DPP-4 INHIBITOR Alogliptin Kazano
Linagliptin Jentadueto
Saxagliptin Kombiglyze XR
Sitagliptin Janumet
METFORMIN + GLINIDE Repaglinide Prandimet
METFORMIN + SGLT2 INHIBITORS Canagliflozin Invokamet Dapagliflozin Xigduo Empagliflozin Synjardy
METFORMIN + SULFONYLUREA Glipizide Metaglip and generic
Glyburide Glucovance and generic
METFORMIN + THIAZOLIDINEDIONE Pioglitazone Actoplus Met
Rosiglitazone Avandamet
TZD + DPP-4 INHIBITOR Pioglitazone + alogliptin Oseni
TZD + SULFONYLUREA Pioglitazone + glimepiride Duetact
Rosiglitazone + glimepiride Avandaryl

Updated Metformin – CKD Prescribing Guidelines (April 2016)
Obtain eGFR before starting metformin and annually, more frequently in
those at risk for renal impairment (e.g., elderly).
Metformin contraindicated in patients with an eGFR <30
Starting metformin in patients with an eGFR between 30-45 not
recommended
If eGFR falls <45, assess the benefits and risks of continuing
treatment. D/C if eGFR falls <30
Hold metformin at the time of / before iodinated contrast procedure if
eGFR 30-60; if H/o Liver disease, Alcoholism, or Heart failure; or if
Intra-arterial contrast. Recheck eGFR 48 hrs after procedure and restart
if renal function stable
http://www.fda.gov/Drugs/DrugSafety/ucm493244.htm (accessed 4-8-16)



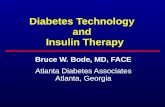
Hyperglycemia
β α
Treatment based on pathophysiology
INSULIN
RESISTANCE
↑glucose reabsorption
↓insulin 50-80%
at diagnosis
↑Hepatic glucose
production
Decreased
incretin effect
and faster carb
absorption
Neurotransmitter
dysfunction
Decreased glucose
uptake
DeFranzo R, et al. Diabetes Care, Volume 36, Supplement 2, August 2013 S127-138
Islet- α cell
↑ glucagon
secretion
Lipolysis
increased
DPP IV inhibitors
GLP-1 agonists
Sulfonylureas
Meglitinides
Insulin GLP-1 agonists
SGLT-2
inhibitors
TZDs
Insulin Insulin
TZDs
GLP-agonists
DPP IV inhibitors
Metformin

Incretin Based Therapy
GLP-1 receptor agonists (injectable therapies) Exenatide
Liraglutide
Dulaglitide
Abiglutide
DPP-4 inhibitors (oral therapies) Sitagliptin
Saxagliptin
Linagliptin, Alogliptin

DPP – 4 Inhibitor's DIPEPTIDYL PEPTIDASE 4 INHIBITORS (GLIPTINS)


DPP-4 Inhibitors Alogliptin, Linagliptin, Saxagliptin, Sitagliptin
Mechanism Inhibit enzymatic degradation of GLP-1 and GIP; glucose-dependent
Efficacy Decrease A1C levels 0.6%–0.9%
Dosing Once daily
Side effects Headaches, nasopharyngitis
Main risk Viral infection; long-term safety unknown
Rosenstock J, et al. Curr Opin Endocrinol Diabetes Obes. 2007;14:98-107. Nathan DM, et al. Diabetes Care. 2008;31:173-175.
A1C = glycated hemoglobin; GIP = gastric inhibitory polypeptide; GLP-1 = glucagon-like peptide-1

DPP-4 Inhibitors
FDA-Approved
Agents
Alogliptin
Linagliptin
Saxagliptin
Sitagliptin
Key Features
Oral administration
Increase endogenous GLP-1
and GIP levels
Increase glucose-dependent
insulin secretion
Suppress glucagon production

Monotherapy Add-on to Metformin Add-on to SU
Alo1 Lin2 Sax3 Sit4 Alo5 Lin6 Sax7 Sit8 Alo9 Lin10,* Sax11 Sit12,†
Baseline A1C (%) 7.9 8.0 8.0 7.5 8.1 8.2 8.6 8.4 7.8 7.9 8.5 8.3
Glucose Control with DPP-4 Inhibitors
-0.57 -0.5 -0.53
-0.69 -0.64 -0.62 -0.65
-0.83 -0.72
-0.67 -0.65 -0.74
-1
-0.8
-0.6
-0.4
-0.2
0
Placebo-Adjusted Change from Baseline
(Not Head-to-Head Trials)
*SU + metformin. †With or without metformin. ‡Absolute change from baseline (active-controlled trial).
1. DeFronzo RA, et al. Diabetes Care. 2008;31:2315–2317. 2. Del Prato S, et al. Diabetes Obes Metab. 2011;13:258-267.
3. Rosenstock J, et al. Curr Med Res Opin. 2009;25:2401-2411. 4. Nauck MA, et al. Diabetes Obes Metab. 2007;9:194-205. 5. Nauck MA, et al. Int
J Clin Pract. 2009;63:46-55. 6. Taskinen MR, et al. Diabetes Obes Metab. 2011;13:65-74. 7. DeFronzo RA, et al. Diabetes Care. 2009;32:1649-1655.
8. Charbonnel B, et al. Diabetes Care. 2006;29:2638-2643. 9. Pratley RE, et al. Diabetes Obes Metab. 2009;11:167-176. 10. Owens DR, et al.
Diabet Med. 2011;28:1352-61. 11. Chacra AR, et al. Int J Clin Pract. 2009;63:1395-1406. 12. Hermansen K, et al. Diabetes Obes Metab. 2007;9:733-745.
Pla
ce
bo
-ad
just
e
d
A1
C (
%)
‡

Monotherapy Add-on to Metformin Add-on to SU
Alo1 Lin2 Sax3 Sit4 Alo5 Lin6 Sax7 Sit8 Alo9 Lin10,* Sax11 Sit12,†
Weight Change with DPP-4 Inhibitors
-0.22 -0.3
0.68
-0.4
0.27
-0.1
-0.87
0.8
-1.5
0.8
-2
-1.5
-1
-0.5
0
0.5
1
Absolute Change from Baseline
(Not Head-to-Head Trials)
NR, value not reported.
*SU + metformin. †With or without metformin.
1. DeFronzo RA, et al. Diabetes Care. 2008;31:2315–2317. 2. Del Prato S, et al. Diabetes Obes Metab. 2011;13:258-267.
3. Rosenstock J, et al. Curr Med Res Opin. 2009;25:2401-2411. 4. Nauck MA, et al. Diabetes Obes Metab. 2007;9:194-205. 5. Nauck MA, et al. Int
J Clin Pract. 2009;63:46-55. 6. Taskinen MR, et al. Diabetes Obes Metab. 2011;13:65-74. 7. DeFronzo RA, et al. Diabetes Care. 2009;32:1649-1655.
8. Charbonnel B, et al. Diabetes Care. 2006;29:2638-2643. 9. Pratley RE, et al. Diabetes Obes Metab. 2009;11:167-176. 10. Owens DR, et al.
Diabet Med. 2011;28:1352-61. 11. Chacra AR, et al. Int J Clin Pract. 2009;63:1395-1406. 12. Hermansen K, et al. Diabetes Obes Metab.
2007;9:733-745.
W
eig
ht
(kg
)
NR NR

Monotherapy Add-on to Metformin Add-on to SU
Alo1 Lin2 Sax3 Sit4 Alo5 Lin6 Sax7 Sit8 Alo9 Lin10,* Sax11 Sit12,†
Hypoglycemia with DPP-4 Inhibitors
1.5 0
9.6
0.3 0.6
22.7
5.2 5.2
14.6
4.9
1.3
12.2
0
5
10
15
20
25
Percentage of Patients Reporting Hypoglycemia
(Not Head-to-Head Trials)
NR, value not reported.
*SU + metformin. †With or without metformin.
1. DeFronzo RA, et al. Diabetes Care. 2008;31:2315–2317. 2. Del Prato S, et al. Diabetes Obes Metab. 2011;13:258-267.
3. Rosenstock J, et al. Curr Med Res Opin. 2009;25:2401-2411. 4. Nauck MA, et al. Diabetes Obes Metab. 2007;9:194-205. 5. Nauck MA, et
al. Int J Clin Pract. 2009;63:46-55. 6. Taskinen MR, et al. Diabetes Obes Metab. 2011;13:65-74. 7. DeFronzo RA, et al. Diabetes Care.
2009;32:1649-1655. 8. Charbonnel B, et al. Diabetes Care. 2006;29:2638-2643. 9. Pratley RE, et al. Diabetes Obes Metab. 2009;11:167-176.
10. Owens DR, et al. Diabet Med. 2011;28:1352-61. 11. Chacra AR, et al. Int J Clin Pract. 2009;63:1395-1406. 12. Hermansen K, et al.
Diabetes Obes Metab. 2007;9:733-745.
Pa
tie
nts
(%
)

Incidence of Selected Adverse Events
with Sitagliptin: Pooled Data
Adverse Event Incidence per 100 patient-years Difference (95% CI)
Sitagliptin 100 mg Nonexposed
Constipation 2.6 1.9 0.8 (0.1, 1.4)
Diarrhea 6.9 9.6 -2.3 (-3.6, -1.0)
Headache 5.8 5.6 0.4 (-0.7, 1.4)
Nasopharyngitis 7.7 7.0 0.9 (-0.3, 2.1)
Pancreatitis 0.08 0.10 -0.02 (-0.20, 0.14)
Rash 1.3 0.9 0.4 (-0.1, 0.8)
Upper respiratory tract infection
8.6 9.0 -0.3 (-1.6, 1.0)
Williams-Herman D, et al. BMC Endocr Disord. 2010;10(7) . http://www.biomedcentral.com/1472-6823/10/7.
Engel SS, et al. Int J Clin Pract. 2010;64:984-990.

GLP-1's GLUCAGON LIKE PEPTIDE –1 INHIBITOR'S

GLP-1 Receptor Agonists
FDA-Approved Agents
Albiglutide
Dulaglutide
Exenatide
Exenatide ER
Liraglutide
Key Features
Injectable administration
Mimic action of native GLP-1
Increase glucose-dependent insulin
secretion
Suppress glucagon production
Slow gastric emptying
ER, extended release; GLP-1, glucagon-like peptide 1.
Garber AJ, et al. Endocr Pract. 2013;19(suppl 2):1-48.

Gastroenterology 2007 132, 2131-2157DOI: (10.1053/j.gastro.2007.03.054
Anti-diabetic Activities of GLP-1

Monotherapy Add-on to Metformin Add-on to SU
Alb1 Dul2 Exe3 Exe ER4
Lir5 Alb6 Dul7 Exe8 Exe ER9
Lir10 Alb11,* Exe12 Exe ER13,†
Lir14
Baseline A1C (%)
8.1 7.6 7.8 8.5 8.3 8.1 8.1 8.2 8.6 8.4 8.2 8.6 8.3 8.5
Glucose Control with
GLP-1 Receptor Agonists
-1.0 -0.9
-0.8 -0.8
-1.4
-1.0
-0.7 -0.9
-1.5 -1.5 -1.5 -1.4
-1.1
-1.5
-2
-1.5
-1
-0.5
0
Placebo-Adjusted Change from Baseline
(Not Head-to-Head Trials)
*Metformin with or without SU or TZD. †Metformin with or without SU. ‡Absolute change from baseline (active-controlled trial).
1. Tanzeum (albiglutide) injection prescribing information. Research Triangle Park, NC: GlaxoSmithKline; 2014.
2. Umpierrez G, et al. Diabetes Care. 2014;37:2168-2176. 3. Moretto TJ, et al. Clin Ther. 2008;30:1448-1460. 4. Russell-Jones D, et al.
Diabetes Care. 2012;35:252-258. 5. Garber A, et al. Lancet. 2009;373:473-481. 6. Ahrén B, et al. Diabetes Care. 2014;37:2141-2148. 7.
Dungan KM, et al. Lancet. 2014;384:1349-1357. 8. DeFronzo RA et al. Diabetes Care. 2005;28:1092-1100. 9. Bergenstal RM, et al. Lancet.
2010;376:431-439. 10. Pratley RE, et al. Lancet. 2010;375:1447-1456. 11. Pratley RE, et al. Lancet Diabetes Endocrinol. 2014;2:289-297. 12.
Buse JB, et al. Diabetes Care. 2004;27:2628-2635. 13. Diamant M, et al. Lancet. 2010;375:2234-2243. 14. Marre M, et al. Diabet Med.
2009;26:268-278.
Pla
ce
bo
-ad
just
e
d
A1C
(%
)
‡

Monotherapy Add-on to Metformin Add-on to SU
Alb1 Dul2 Exe3 Exe ER4
Lir5 Alb6 Dul7 Exe8 Exe ER9
Lir10 Alb11,* Exe12 Exe ER13,†
Lir14
Weight Change with GLP-1
Receptor Agonists
-0.9 -1.2
-0.6
-2.3 -2.6
-1.6
-3.1 -2.8
-2.6
-2 -2.3
-0.2
-2.5
-3.4 -4
-3
-2
-1
0
*Metformin with or without SU or TZD. †Metformin with or without SU.
1. Tanzeum (albiglutide) injection prescribing information. Research Triangle Park, NC: GlaxoSmithKline; 2014.
2. Umpierrez G, et al. Diabetes Care. 2014;37:2168-2176. 3. Moretto TJ, et al. Clin Ther. 2008;30:1448-1460. 4. Russell-Jones D, et al.
Diabetes Care. 2012;35:252-258. 5. Garber A, et al. Lancet. 2009;373:473-481. 6. Ahrén B, et al. Diabetes Care. 2014;37:2141-2148. 7.
Dungan KM, et al. Lancet. 2014;384:1349-1357. 8. DeFronzo RA et al. Diabetes Care. 2005;28:1092-1100. 9. Bergenstal RM, et al.
Lancet. 2010;376:431-439. 10. Pratley RE, et al. Lancet. 2010;375:1447-1456. 11. Pratley RE, et al. Lancet Diabetes Endocrinol.
2014;2:289-297. 12. Buse JB, et al. Diabetes Care. 2004;27:2628-2635. 13. Diamant M, et al. Lancet. 2010;375:2234-2243. 14. Marre M,
et al. Diabet Med. 2009;26:268-278.
W
eig
ht
(kg
)
Absolute Change from Baseline
(Not Head-to-Head Trials)

Blood Pressure Changes with Liraglutide
Monotherapy vs
Glimepiride
52 Weeks1
Add-on to
Metformin
26 Weeks2
Add-on to
Metformin
26 Weeks3
Add-on to
Sulfonylurea
26 Weeks4,5
Add-on to
Met + TZD
26 Weeks6
Add-on to
Met + SU
26 Weeks7
N 746 1091 665 1041 821 581
Treatment† Glim Lir Met Glim +
Met
Lir+ Met
Sit+ Met
Lir+ Met
SU Rosi + SU
Lir+ SU
Rosi + Met
Lir+ Rosi+ Met
Met+ SU
Glar+ Met+
SU
Lir+ Met+
SU
*P<0.05 vs comparator.
†All liraglutide dosages shown are 1.8 mg QD.
1. Garber A, et al. Lancet. 2009;373:473-481. 2. Nauck M, et al. Diabetes Care. 2009;32:84-90.
3. Pratley RE, et al. Lancet. 2010;375:1447-1456. 4. Marre M, et al. Diabet Med. 2009;26:268-278.
5. Colagiuri S, et al. Diabetes. 2008;57(suppl 2): Abstr. 554-P. 6. Zinman B, et al. Diabetes Care.
2009;32:1224-1230. 7. Russell-Jones D, et al. Diabetologia. 2009;52:2046-2055
-1.8 -2.3
-0.7
0.4
-0.9 -0.9 -1.1
0.5
-3.6
-2.3
-0.7
-2.8
-5.6
-4.0
-6
-5
-4
-3
-2
-1
0
1
S
ysto
lic B
P
(mm
Hg)
*
*
*
*

Monotherapy Add-on to Metformin Add-on to SU
Alb1 Dul2 Exe3 Exe ER4
Lir5 Alb6 Dul7 Exe8 Exe ER9
Lir10 Alb11,* Exe12 Exe ER13,†
Lir14
Hypoglycemia with GLP-1 Receptor Agonists
0 3
10.4 12.3
9
36
4.0 5.0
13.0
5.2 1
8.1 8
3
0
10
20
30
40
*Metformin with or without SU or TZD. †Metformin with or without SU.
1. Nauck M, et al. Diabetes. 2013;62(suppl 2): Abstr. 55-LB. 2. Umpierrez G, et al. Diabetes Care. 2014;37:2168-2176. 3. Moretto TJ,
et al. Clin Ther. 2008;30:1448-1460. 4. Russell-Jones D, et al. Diabetes Care. 2012;35:252-258. 5. Garber A, et al. Lancet.
2009;373:473-481. 6. Ahrén B, et al. Diabetes Care. 2014;37:2141-2148. 7. Dungan KM, et al. Lancet. 2014;384:1349-1357. 8.
DeFronzo RA et al. Diabetes Care. 2005;28:1092-1100. 9. Bergenstal RM, et al. Lancet. 2010;376:431-439. 10. Pratley RE, et al.
Lancet. 2010;375:1447-1456. 11. Pratley RE, et al. Lancet Diabetes Endocrinol. 2014;2:289-297. 12. Buse JB, et al. Diabetes Care.
2004;27:2628-2635. 13. Diamant M, et al. Lancet. 2010;375:2234-2243. 14. Marre M, et al. Diabet Med. 2009;26:268-278.
Percentage of Patients Reporting Hypoglycemia
(Not Head-to-Head Trials) P
atie
nts
(%
)

Safety Considerations
with GLP1 Receptor Agonists
GI adverse
events
• Common • Usually dose dependent and transient • Usually reduced with dose titration
Pancreatitis
• Pancreatitis has been reported with postmarketing use of some of incretin agents, although no causal relationship has been established
• Extensive review by FDA of studies involving >80,000 patients has not uncovered reliable evidence of increased pancreatic risk with incretins vs other agents
• Labeling for all incretins states these agents should be immediately discontinued if pancreatitis is suspected
• Labeling for GLP-1 receptor agonists suggests consideration of other therapies for patients with a history of pancreatitis
Pancreatic
cancer
• Extensive review by FDA of studies involving >80,000 patients has not uncovered reliable evidence of increased pancreatic risk with incretins vs other agents
• Further assessments required from long duration-controlled studies or epidemiological databases
Medullary
thyroid
cancer
• Animal data showed an increased incidence of C-cell tumors with liraglutide and exenatide ER treatment, but confirmatory population studies are lacking
• Labeling for liraglutide and exenatide ER: • Patients should be counseled regarding medullary thyroid carcinoma and the signs/symptoms
of thyroid tumors • Contraindicated in patients with personal/family history of MTC or multiple endocrine neoplasia
syndrome type 2
Renal
impairment
• Renal Impairment has been reported postmarketing, usually in association with nausea, vomiting,
diarrhea, or dehydration. Use caution when initiating or escalating doses in patients with renal
impairment. Exenatide is contraindicated in patients with severe renal insufficiency or ESRD
ER, extended release.
Garber AJ, et al. Endocr Pract. 2013;19(suppl 2):1-48.
ADA/EASD/IDF statement concerning the use of incretin therapy and pancreatic disease [news release]. Alexandria, VA: American
Diabetes Association, European Association for the Study of Diabetes, International Diabetes Federation; June 28, 2013.
http://www.diabetes.org/newsroom/press-releases/2013/recommendations-for.html.

SGLT-2 Inhibitors SODIUM GLUCOSE CO-TRANSPORTER 2 INHIBITOR'S

SGLT2 Inhibitors Canagliflozin, Dapagliflozin, Empagliflozin
Invokana [Package Insert] Janssen Pharmaceuticals, Inc. Titusville, NJ.; Lavalle-gonzález FJ, Januszewicz A, Davidson J, et al.
Diabetologia. 2013; Stenlöf K, Cefalu WT, Kim KA, et al. Diabetes Obes Metab. 2013;15(4):372-82; Burki TK. Lancet. 2012;379(9815):507.
Mechanism Inhibits sodium-glucose transport protein subtype 2 (SGLT2) which is responsible for at least 90% of glucose reabsorption in the kidney causing blood glucose is eliminated in the urine
Efficacy Modest (HbA1C 0.8-1.1%)
Advantages
Insulin-independent glucose reduction, Low risk of hypoglycemia,
Weight loss (to 4% BW), Blood pressure-lowering
Disadvantages
Osmotic diuresis causing Polyuria and lightheadedness, Bacterial
urinary tract infections (≈5%), Fungal genital infections (≈10%),
Increased LDL cholesterol, Hyperkalemia (canagliflozin), Bladder
cancer concerns (dapagliflozin)
Contraindications History of genital fungal infections, caution in chronic kidney
disease

SGLT2 Inhibitors Promote Urinary Glucose
Excretion
SGLT2 mediates most (≈ 90%) glucose reabsorption from the proximal renal tubular lumen back into the circulation
SGLT2 inhibitors lower the
threshold at which glucose is excreted, leading to Increased urinary glucose
excretion Decreased return of
glucose to circulation Decreased blood glucose
levels
Bowman’s
capsule
Return
to
circulation
Urinary excretion
Glucose
SGLT2
Proximal
renal
tubule

Sodium-glucose co-transporter 2 inhibitors
(SGLT2)
Benefits:
Weight loss
Improved systolic BP
A1c reduction
Other effects
Increase LDL
Increase risk of yeast infections
Not recommended in over 75 y/o
Canagliflozin (Invokana 100 & 300 mg)
GFR>45 mL/min/1.73m²
Dapaglifozin (Farxiga 5 & 10 mg QD)
GFR>60
Empagliflozin (Jardiance 10 & 25 mg)
GFR>45

Glucose Control with SGLT2 Inhibitors
Placebo-Adjusted Change from Baseline
(Not Head-to-Head Trials)
*Absolute change from baseline (active-controlled trial).
1. Stenlof K, et al. Diabetes Obes Metab. 2013;15:372-382. 2. Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224. 3. Roden M, et al.
Lancet Diabetes Endocrinol. 2013;1:208-219. 4. Cefalu WT, et al. Lancet. 2013;382:941-950. 5. Nauck MA, et al. Diabetes Care.
2011;34:2015-2022. 6. Haring HU, et al. Diabetes Care. 2014;37:1650-1659. 7. Yale J-F, et al. Diabetes Obes Metab. 2013;15:463-473. 8.
Wilding JPH, et al. Ann Intern Med. 2012;156:405-415. 9. Rosenstock J, et al. Diabetes Care. 2014;37:1815-1823.
Monotherapy Add-on to Metformin Add-on to Insulin +/- OAs
Can1 Dap2 Emp3 Can4 Dap5 Emp6 Can7 Dap8 Emp9
Baseline A1C
(%)
8.1 7.8 7.9 8.1 8.2 7.9 8.2 8.6 8.3
Pla
ce
bo
-ad
just
ed
A1
C (
%)
*
*
-1.2
-0.9
-0.4
-0.66 -0.52 -0.57
-0.86
-0.64
-0.46
-1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0

Weight Change with SGLT2 Inhibitors
Absolute Change from Baseline
(Not Head-to-Head Trials)
Monotherapy Add-on to Metformin Add-on to Insulin +/- OAs
Can1 Dap2 Emp3 Can4 Dap5 Emp6 Can7 Dap8 Emp9
-3.4
-4.0
-1.4
-3.2 -3.2
-1.6
-2.48 -2.46 -2.04
-4.5
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
1. Stenlof K, et al. Diabetes Obes Metab. 2013;15:372-382. 2. Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224. 3. Roden M, et al.
Lancet Diabetes Endocrinol. 2013;1:208-219. 4. Cefalu WT, et al. Lancet. 2013;382:941-950. 5. Nauck MA, et al. Diabetes Care.
2011;34:2015-2022. 6. Haring HU, et al. Diabetes Care. 2014;37:1650-1659. 7. Yale J-F, et al. Diabetes Obes Metab. 2013;15:463-473. 8.
Wilding JPH, et al. Ann Intern Med. 2012;156:405-415. 9. Rosenstock J, et al. Diabetes Care. 2014;37:1815-1823.
W
eig
ht
(kg
)

Overseas phase III clinical study - A metformin combination study (D1690C00012)
Changes in body composition from the baseline (24 and 102 weeks after start of treatment)
Bolinder J. et al.: Diabetes Obes Metab. 16(2): 159-169, 2014
-5.0
-4.5
-4.0
-3.5
-2.0
-1.5
-0.5
Ch
an
ge
(24 Weeks)
Placebo + MET
(n=86)
Farxiga 10 mg + MET
(n=83)
(102 Weeks)
Placebo + MET
(n=71)
Total lean tissue mass
Total fat mass
0.0
-1.0
-2.5
-3.0
Farxiga 10 mg + MET
(n=66)
-0.65
-0.40
-2.16
-1.00
-1.46
-0.90 -2.80
-1.30
(kg)
Subjects: Patients with type 2 diabetes mellitus poorly controlled as to blood glucose by uncombined metformin (MET) therapy [182 patients included in safety analysis; 180 patients included in efficacy analysis (FAS)]
Methods: A randomized, double-blind, placebo-controlled, multicenter, parallel-group comparative study. Subjects were allocated at random to the Forxiga 10 mg + MET group and the placebo + MET group. Once daily treatment (combined with MET 1,500 mg/day) in the morning was continued for 102 weeks, and mean adjusted change in body composition at 24 and 102 weeks after the start of treatment was analyzed.
Safety: The incidence of adverse reactions was 19.8% (18/91) in the Forxiga 10 mg + MET group and 14.3% (13/91) in the placebo + MET group.
Adjusted mean change (95% CI)
FAS
(including data after hyperglycemia rescue therapy) MET: Metformin
Note) The starting dose level of Forxiga Tablet in Japan is 5 mg/day. Before use, reference to the latest package insert is needed.

Blood Pressure Changes with SGLT2 Inhibitors
Absolute Change from Baseline (Not Head-to-Head Trials)
1. Stenlof K, et al. Diabetes Obes Metab. 2013;15:372-382. 2. Ferrannini E, et al. Diabetes Care.
2010;33:2217-2224. 3. Roden M, et al. Lancet Diabetes Endocrinol. 2013;1:208-219. 4. Cefalu WT, et al.
Lancet. 2013;382:941-950. 5. Nauck MA, et al. Diabetes Care. 2011;34:2015-2022. 6. Haring HU, et al.
Diabetes Care. 2014;37:1650-1659. 7. Yale J-F, et al. Diabetes Obes Metab. 2013;15:463-473. 8. Wilding JPH, et al. Ann Intern Med. 2012;156:405-415. 9. Rosenstock J, et al. Diabetes Care. 2014;37:1815-1823.
Monotherapy Add-on to Metformin Add-on to Insulin +/- OAs
Can1 Dap2 Emp3 Can4 Dap5 Emp6 Can7 Dap8 Emp9
-5.0 -4.6
-6.4
-3.6 -4.3
-6.7
-5.0 -5.2
-3.8
-8
-7
-6
-5
-4
-3
-2
-1
0
S
yst
olic
BP
(m
mH
g)

Hypoglycemia with SGLT2 Inhibitors
Percentage of Patients Reporting Hypoglycemia
(Not Head-to-Head Trials)
1. Stenlof K, et al. Diabetes Obes Metab. 2013;15:372-382. 2. Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224. 3. Roden M, et al.
Lancet Diabetes Endocrinol. 2013;1:208-219. 4. Cefalu WT, et al. Lancet. 2013;382:941-950. 5. Nauck MA, et al. Diabetes Care.
2011;34:2015-2022. 6. Haring HU, et al. Diabetes Care. 2014;37:1650-1659. 7. Yale J-F, et al. Diabetes Obes Metab. 2013;15:463-473. 8.
Wilding JPH, et al. Ann Intern Med. 2012;156:405-415. 9. Rosenstock J, et al. Diabetes Care. 2014;37:1815-1823.
Monotherapy Add-on to Metformin Add-on to Insulin +/- OAs
Can1 Dap2 Emp3 Can4 Dap5 Emp6 Can7 Dap8 Emp9
3.0 5.0
51.2
2.9 3.4
53.6
1.4
58.2
0
10
20
30
40
50
60
70
Pa
tie
nts
(%
)
<1

Safety Considerations with SGLT2 Inhibitors
Genitourinary infection
Increased incidence; patients should be monitored and treated if necessary
Increased LDL-C Small increases in LDL-C have been observed in clinical trials
Bladder cancer
Increased incidence of bladder cancers in patients receiving dapagliflozin
Dapagliflozin labeling recommends not using in patients with active bladder cancer and should be used with caution in patients with a history of bladder cancer
Renal impairment Monitor kidney function during therapy, especially in patients with GFR <60 mL/min/1.73 m2
Garber AJ, et al. Endocr Pract. 2013;19(suppl 2):1-48.
Farxiga (dapagliflozin) prescribing information. Princeton, NJ: Bristol-Meyers Squibb Company. 2014.
Invokana (canagliflozin) prescribing information. Titusville, NJ: Janssen Pharmaceuticals, Inc. 2014.

Time course of eGFR (meta-analysis)
Changes in eGFR
4 8 16 24 37 50 1 63 76 89 102 (Week) BL
Number of patients
Placebo (n=1,955) C
ha
ng
e fro
m b
ase
lin
e in
eG
FR
(mL/min/1.73 m2)
2,026
1,955
1,697
1,629
1,655
1,570
1,777
1,671
1,600
1,513
1,663
1,558
Forxiga 10 mg
Placebo
712
605
692
585
656
551
627
521
10
15
5
0
-5
-10
-15
Farxiga 10 mg (n=2,026)
Baseline
Mean (mL/min/1.73 m2)
Placebo
Forxiga 10 mg 81.0
80.7
EMDAC data <http://www.fda.gov/downloads/advisorycommittees/committeesmeetingmaterials/drugs/endocrinologicandmetabolicdrugsadvisorycommittee/ucm
378079.pdf>
Note) The starting dose level of Forxiga Tablet in Japan is 5 mg/day. Before use, reference to the latest package insert is needed.
Subjects/Methods: Meta-analysis of the combined subjects of Phase IIb/III studies conducted across the world (including Japan and Asia) (30-MU:
data cut off on November 15, 2012)

Prescribing Information Comparison* CANAGLIFLOZIN DAPAGLIFLOZIN EMPAGLIFLOZIN
Dosing • 100 mg once daily
before first meal
• 300 mg if eGFR ≥60 mL/min/1.73m2
• 5 or 10 mg once daily in morning, with
or without food
• 10 or 25 mg once daily in morning,
with or without food
Contraindications Severe renal impairment, ESRD, dialysis
• Do not initiate if eGFR
<45 mL/min/1.73m2
Severe renal impairment, ESRD, dialysis
• Do not initiate if eGFR
<60 mL/min/1.73m2
Severe renal impairment, ESRD, dialysis
• Do not initiate if eGFR
<45 mL/min/1.73m2
Warnings and
Precautions
• Hypotension
• Impaired renal function
• Hyperkalemia
• Hypoglycemia: concomitant insulin or
secretagogues
• Genital mycotic infections
• Hypersensitivity reactions
• LDL-C increases
• Hypotension
• Impaired renal function
• Hypoglycemia: concomitant insulin or
secretagogues
• Genital mycotic infections
• Bladder cancer imbalance
• LDL-C increases
• Hypotension
• Impaired renal function
• Hypoglycemia: concomitant insulin or
secretagogues
• Genital mycotic infections
• Urinary tract infections
• LDL-C increases
Key Adverse Events
(>5% incidence)
• Female genital mycotic infections
• Urinary tract infections
• Increased urination
• Female genital mycotic infections
• Nasopharyngitis
• Urinary tract infections
• Female genital mycotic infections
• Urinary tract infections
Differences are bold and in red.
*Accurate comparison of SGLT2 inhibitors requires head-to-head studies, which have not yet been conducted.
Farxiga (dapagliflozin) prescribing information. Princeton, NJ: Bristol-Meyers Squibb Company. 2014.
Invokana (canagliflozin) prescribing information. Titusville, NJ: Janssen Pharmaceuticals, Inc. 2014.

Combination options (Basal Insulin and GLP-1 Agonists) for
the treatment of Type 2 diabetes
Xultophy (Degludec / Liraglutide)
Administered once daily by sc injection,
It is supplied as a 3ml prefilled pen containing 100 units/3.6mg insulin Degludec/liraglutide per ml;
The proportion of patients reaching target HbA1c was higher with Xultophy than with insulin degludec or
liraglutide
Adverse effects are typical of the component drugs, with a lower incidence of gastrointestinal effects but
less weight loss than Liraglutide
Soliqua (Glargine U-100 and Lixisenetide) LixiLan, single-injection fixed-ratio combination of GLP1-RA & Analog Basal Insulin- Lixisenatide (Lyxumia) &
Glargine (Lantus)
24-week, double-blind trial, 495 patients with type 2 diabetes inadequately controlled with Insulin Glargine
and Metformin (mean HbA1C 8.4 percent) were randomly assigned to the addition of Lixisenatide or
placebo
The reduction in A1C was significantly greater in the Lixisenatide group (-0.6 versus -0.3 percent)

CVOT's CARDIOVASCULAR OUTCOME TRIALS

Study SAVOR EXAMINE TECOS CAROLINA CARMELIN
A
DPP4-i saxaglip
tin
alogliptin sitaglipti
n
linagliptin linagliptin
Comparat
or
placebo placebo placebo sulfonylurea placebo
N 16,500 5,400 14,000 6,000 8,300
Results 2013 2013 June
2015
2017 2017 Study LEADER ELIXA SUSTAIN 6 EXSCEL REWIN
D
FREEDOM
GLP1-
RA
liraglutide lixisenatid
e
semaglutide exenatide
LR
Dulaglutide ITCA-
650
Comparat
or
placebo placebo placebo placebo Placebo
Placebo
N 16,500 14,000 6,000 5,400 8,300 4000+
Results 2016 2015 2016 2018 2019 2015
Study EMPA-REG CANVAS DECLARE NCT01986881
SGLT-2-i empaglifozin canagliflozin dapagliflozin ertugliflozin
Comparat
or
placebo placebo placebo placebo
N 7300 4300 22,200 3900
Results Sept 2015 2017 2019 2020
Large Non-Insulin CVOTs in T2DM
✓ ✓
✓
✓
POSITIVE

PROactive Study
>5,000 patients in 19 European countries involving over 320 investigators
Investigated effect of insulin resistance on CV morbidity and mortality in patients
with T2DM
Investigated Pioglitazone’s ability to prevent the progression of macrovascular
disease
PROspective Actos Clinical Trial In macroVascular Events (PROactive) results. http://www.proactive-results.com/html/about_the_study.htm Accessed February 2011.
CV = cardiovascular; T2DM = type 2 diabetes mellitus
All-cause mortality
Stroke
Leg revascularization
Non-fatal MI (including silent)
Major leg amputation
(above the ankle)
Acute coronary syndrome
Cardiac intervention
The primary endpoint was time to first occurrence of any of the following
events from time of randomization:

Dormandy JA, et al. Lancet. 2005;366:1279-1285.
Time to Fatal/Nonfatal MI
(excluding silent MI)
PROactive results Web site. Available at
http://www.proactive results.com
/html/analysis.htm. October 10, 2006.
Placebo
PIO
Ka
pla
n-M
eie
r Ev
en
t R
ate
(35/1230)
(54/1215)
HR 95% CI
P value
PIO vs placebo 0.63 0.41, 0.97 .035 2445 2397 2351 2308 2265 2222 406(139) N at
Risk: l 0
l 6
l 12
l 18
l 24
l 30
l 36
Time From Randomization (mo)
.0–
.01–
.03–
.04–
.05–
.06–
.02–
CV=cardiovascular; ACS=acute coronary syndromes; MI=myocardial infarction
The official PROspective Actos Clinical Trial In macroVascular Events
(PROactive) results website. Available at http://www.proactive-
results.com/html/analysis.htm.
Time to ACS
Time From Randomization (mo)
Ka
pla
n-M
eie
r Ev
en
t R
ate
.02–
.04–
.06–
.08–
.10–
.0–
0 6
12 18 24 30 36
2445 2387 2337 2293 2245 2199 399(139) N at
Risk:
HR 95% CI P value
0.72 0.52, 0.99 .045
Placebo
PIO (65/1230)
(88/1215)
PIO vs placebo
l
l
l
l
l
l
l
l
l
PROactive Study, Secondary Endpoints Pioglitazone Had No Significant Effect on Primary Composite CV Endpoints
Benefit Seen in Select Secondary Endpoints

Pioglitazone after Ischemic Stroke or Transient Ischemic Attack Primary Outcome
Kernan WN et al. N Engl J Med 2016;374:1321-1331

Pioglitazone after Ischemic Stroke or TIA Primary and Secondary Outcomes
Kernan WN et al. N Engl J Med 2016;374:1321-1331

EMPA-REG Clinical Outcomes with Empagliflozin
EMPA-REG OUTCOME Pooled Analysis
(N=7020)
*CV death, nonfatal MI (excluding silent MI), or nonfatal stroke; †CV death, nonfatal MI (excluding silent MI), nonfatal stroke, and hospitalization for unstable
angina.
CI, confidence interval; CV, cardiovascular; HF, heart failure; HR, hazard ratio; MI, myocardial infarction.
Zinman B, et al. N Engl J Med. 2015;373:2117-2128.
0.00 0.50 1.00 1.50
Hazard ratio (95%
CI) P value
Primary composite endpoint* 0.86 (0.74-0.99) 0.04
Secondary composite endpoint† 0.89 (0.78-1.01) 0.08
Death from any cause 0.68 (0.57-0.82) <0.001
CV death 0.62 (0.49-0.77) <0.001
Fatal or nonfatal MI 0.87 (0.70-1.09) 0.23
Hospitalization for HF 0.65 (0.50-0.85) 0.002
Hospitalization for HF or CV death 0.66 (0.55-0.79) <0.001
Favors empagliflozin
14%
36%
34%
32%
35%

CVOT- Empa-Reg Trial
Cum
ula
tive in
cid
ence fu
nctio
n. H
R, h
azard
ratio
HR 0.62 (95% CI 0.49, 0.77)
p<0.0001

Number needed to treat (NNT) to prevent one death
across landmark trials in patients with high CV risk
1. 4
S in
vestig
ato
r. Lancet 1
994; 3
44: 1
383
-89,
http
://ww
w.tria
lresults
cente
r.org
/stu
dy2590
-4S
.htm
;
2. H
OP
E in
vestig
ato
r N E
ngl J
Med 2
000;3
42:1
45
-53,
http
://ww
w.tria
lresults
cente
r.org
/stu
dy2606
-HO
PE
.htm
Simvastatin1
for 5.4 years
High CV risk 5% diabetes, 26% hypertension
1994 2000 2015
Pre-statin era
High CV risk 38% diabetes, 46% hypertension
Ramipril2
for 5 years
Pre-ACEi/ARB era
<29% statin
Empagliflozin for 3 years
T2DM with high CV risk 92% hypertension
>80% ACEi/ARB
>75% statin

LEADER (Liraglutide)- Primary outcome CV death, non-fatal myocardial infarction, or non-fatal stroke
The primary composite outcome in the time-to-event analysis was the first occurrence of death from cardiovascular causes, non-fatal myocardial infarction, or non-fatal stroke. The cumulative incidences were estimated with the use of the Kaplan–Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI: confidence interval; CV: cardiovascular; HR: hazard ratio.
Presented at the American Diabetes Association 76th Scientific Sessions, Session 3-CT-SY24. June 13 2016, New Orleans, LA, USA.

LEADER Trial Primary and secondary CV Outcomes
*Hazard ratios and p-values were estimated with the use of a Cox proportional-hazards model with treatment as a covariate. †The primary composite outcome in the time-to-event analysis consisted of the first occurrence of death from cardiovascular causes (181 patients in the liraglutide group vs. 227 in the placebo
group), non-fatal (including silent) myocardial infarction (275 vs. 304), or non-fatal stroke (152 vs. 163). The p-value is for superiority. ‡The expanded composite outcome included death from
cardiovascular causes, non-fatal myocardial infarction, non-fatal stroke, coronary revascularization, or hospitalization for unstable angina pectoris or heart failure.
§This analysis was not prespecified. CI: confidence interval; CV: cardiovascular; UAP: unstable angina pectoris.
Presented at the American Diabetes Association 76th Scientific Sessions, Session 3-CT-SY24. June 13 2016, New Orleans, LA, USA.

LEADER Trial: Time to first renal event Macroalbuminuria, doubling of serum creatinine, ESRD, renal death
The cumulative incidences were estimated with the use of the Kaplan–Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI: confidence interval; ESRD: end-stage renal disease; HR: hazard ratio.
Presented at the American Diabetes Association 76th Scientific Sessions, Session 3-CT-SY24. June 13 2016, New Orleans, LA, USA.

LEADER TRIAL: NNT to treat to prevent one…
CV: cardiovascular; MACE: major adverse cardiovascular event.
Presented at the American Diabetes Association 76th Scientific Sessions, Session 3-CT-SY24. June 13 2016, New Orleans, LA, USA.

CANVAS: Canagliflozin and Cardiovascular and
Renal Events in Type 2 Diabetes
Compared with patients taking placebo, patients taking Canagliflozin had lower
A1C levels (mean difference -0.58 percent) and reductions in weight and systolic and diastolic blood pressure
After a mean follow-up of 3.6 years, the primary outcome, a composite of death
from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke,
occurred in fewer patients in the Canagliflozin group (26.9 vs. 31.5 patients per 1000
patient-years,
The rate of hospitalization for heart failure was lower in the canagliflozin group (5.5
versus 8.7 patients per 1000 patient-years in the placebo group, HR 0.67, 95% CI 0.52-
0.87)
Progression of albuminuria (a secondary endpoint) occurred less frequently in the Canagliflozin group (89.4 versus 128.7 participants per 1000 patient-years in the
placebo group, HR 0.73, 95% CI 0.67-0.79)

CANVAS and CANVAS -R
Adverse reactions were consistent with the previously reported risks associated
with canagliflozin except for an increased risk of amputation
Amputation incidence 5.9 and 2.8 per 1000 patient-years for patients taking
canagliflozin and placebo, respectively, in the first trial, and 7.5 and 4.2 per
1000 patient-years, respectively, in the second trial
Patients were followed for a mean 5.7 and 2.1 years, respectively
Amputations were primarily at the level of the toe or metatarsal
Patients with a history of prior amputation, peripheral vascular disease, and
neuropathy were at highest risk for amputation

Summary: CVOT's of SGLT-2 Inhibitors
The large cardiovascular benefit of Empagliflozin and Canagliflozin while
impressive, was in a very high-risk population with established CVD at baseline
Benefit in patients taking Canagliflozin must be balanced with the increased risk of
amputations
The difference in glycemia between the treatment groups was minimal,
suggesting that extra-glycemic effects of the drugs were responsible for the CVD
outcome
It is unknown whether Empagliflozin, Canagliflozin, or other SGLT2 inhibitors, will have similar CVD effects in the majority of persons with type 2 diabetes who do
not have overt CVD
Wait for DECLARE (with Dapagliflozin)

Look beyond your patient's HbA1c DIABETES TECHNOLOGY: CGMS, INSULIN PUMPS AND OTHER OPTIONS

Look Beyond Your Patient's HbA1c

Summary: DM Contemporary Care
Identify individual treatment goals
Institute personalized comprehensive care for people with diabetes
Start intensive lifestyle modification for glycemic control while concomitantly starting
medications
Choose medications based on safety, efficacy and characteristics
Monitor every three months intensify/advance treatment as needed
Per the AACE Algorithm Consider GLP1 RA and SGLT- 2 Inhibitors as first options with
metformin based on safety efficacy in reducing glucose and positive effect on CV
risk parameters especially weight and blood pressure

THANK YOU