Diabetes Management in Hospital Orlando, May 31, 2003 Paul C. Davidson, MD, FACE Atlanta Diabetes...
59
Diabetes Management in Hospital Orlando, May 31, 2003 Paul C. Davidson, MD, FACE Atlanta Diabetes Associates Atlanta, Georgia
Transcript of Diabetes Management in Hospital Orlando, May 31, 2003 Paul C. Davidson, MD, FACE Atlanta Diabetes...

Diabetes Management in Hospital
Orlando, May 31, 2003
Paul C. Davidson, MD, FACE
Atlanta Diabetes Associates
Atlanta, Georgia

Diabetes in Hospitalized Patients
• 6 Million US Hospitalizations
15% of Admissions
• 24 Million Hospital Days
20% of All Hospital Days
• 36% First Diagnosed in Hospital 66% No Documentation by Physician 27% Labeled Hyperglycemia
2% Diagnosis on Face Sheet

Diabetes in Hospitalized Patients1997 Costs
•$$23,500 Each Diabetes Patient vs.23,500 Each Diabetes Patient vs. $12,200 for Non-Diabetes Patient$12,200 for Non-Diabetes Patient
•60% of All Diabetes-Related Costs60% of All Diabetes-Related Costs
•Only 5% DKA, HHNKCOnly 5% DKA, HHNKC
•48% Diabetes Complications48% Diabetes Complications
•52% Other Conditions52% Other Conditions

Impairment of Phagocytic Function Bybee, 1964
Short, Transient Hyperglycemia
Abnormalities in granulocyte
adherence, chemotaxis, phagocytosis,
bacterocidal function. Bybee, 1964; Hill, 1974;
Chase, 1981; Rosenberg, 1990
Effects of HyperglycemiaInfectious Disease

Global PerspectivesEffect of Underlying DiabetesImpact of Acute Diabetic State
Stress ResponseCounter Regulatory Hormones
Epinephrine, Glucagon, Cortisol, GH Glucose Toxicity
Increased Glucose, FFA, KetonesAcidosis: Lactic or KetosisMechanism of Progressive Insulin Resistance
Diabetes in Hospitalized Patients Diabetes in Hospitalized Patients ..
PathophysiologyPathophysiology

Role of Insulin and Glucose in Acute MI
Insulin Anti-inflammatory
– Acute Reduction CRP Anti-thrombotic
– Profibrinolytic
• Suppresses PAI-1 Suppresses FFA
– Preserve Endothlium Suppresses MMPs
– Prevents Rupture
Glucose
Pro-inflammatory
Pro-thrombotic
Induces MMPs (Matrix Matalloproteinases)
– Mediates Plaque Rupture
Dandona Diab Care 2003

Detriments:Decreased AppetiteMeals Held or DelayedDecreased ActivityOral Agents StoppedInsulin HeldSliding Scale Insulin
Only for Extreme BGs Benefit: Detecting Hyperglycemia
Effects of Hospitalization
on Diabetes Management

Missed Opportunities:
To Reduce Hospital Morbidity and
Mortality
To Initiate Interventions to Delay
Long-term Complications
Diabetes in Hospitalized Patients Diabetes in Hospitalized Patients ..
Failure to Treat Hyperglycemia

Diabetes in Hospitalized Diabetes in Hospitalized
Patients .Patients . Psychology Psychology
Patients expect good glycemic control as part of Patients expect good glycemic control as part of
hospital carehospital care
They strive for recommended goals at homeThey strive for recommended goals at home
Difficult to understand staff’s casual approach to Difficult to understand staff’s casual approach to
BG’s >150BG’s >150

Diabetes in Hospitalized Diabetes in Hospitalized Patients . Patients .
Clinical RisksClinical Risks
• High-risk for Bacterial Infection– Surgery– Catheters– Intravenous Access– Anesthesia
• Problems with wound healing
• Problems with tissue and organ perfusion

Infections in Diabetes
One BG >220 mg/dl results in 5.8 times increase in nosocomial infection rate
Two hours hyperglycemia results in impaired WBC function for weeks
Pomposelli, New England Deaconess, J Parenteral and Enteral Nutrition 22:77-81,1998

Side Effects of BG >200 mg/dl Side Effects of BG >200 mg/dl
Reduced Intravascular VolumeReduced Intravascular Volume
DehydrationDehydration
Electrolyte FluxesElectrolyte Fluxes
Impaired WBC FunctionImpaired WBC Function
Immunoglobulin InactivationImmunoglobulin Inactivation
Complement DisablingComplement Disabling
Increased Collagenase, Decreased Wound Increased Collagenase, Decreased Wound CollagenCollagen

Evidence for Immediate Benefit of Evidence for Immediate Benefit of Normoglycemia in Hospitalized PatientsNormoglycemia in Hospitalized Patients
Numerous Publications on in Vitro EvidenceNumerous Publications on in Vitro Evidence
– Neutrophil DysfunctionNeutrophil Dysfunction
– Complement InhibitionComplement Inhibition
– Altered Redox State (Pseudohypoxia)Altered Redox State (Pseudohypoxia)
– Glucose Rich Edema as Culture MediaGlucose Rich Edema as Culture Media
Recent Outcome Studies Supporting Good Glucose Control in Hospital Recent Outcome Studies Supporting Good Glucose Control in Hospital SettingSetting
Reduction in CRPReduction in CRP

Open Heart Surgery in DiabetesPortland St. Vincent Medical Center
Control Group
N=968
1987-1991
SubQ Insulin q 4 h
Goal 200 mg/dl
Standard Deviation 36
All Mean BG’s <200 47%
Study Group
N=1499
1991-1997
IV Insulin
Goal 150-200 mg/dl
Standard Deviation 26
All Mean BG’s <200 84%
Furnary et al, The 34th Meeting of The Society of Thoracic Surgeons New Orleans, LA January 26, 1998

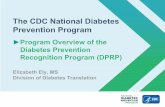
170180190200210220230240250
DOS POD 1 POD 2 POD 3
SQI
CII
Open Heart Surgery in DiabetesPortland St. Vincent Medical Center Perioperative Blood Glucose
Furnary et al, The 34th Meeting of The Society of Thoracic Surgeons New Orleans, LA January 26, 1998

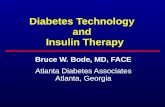
Incidence of DSWI: 1987-1997
0.0%
1.0%
2.0%
3.0%
4.0%
87 88 89 90 91 92 93 94 95 96 97
Year
DS
WI DM Pts.
Non-DM
CII
Furnary, et al, The 34th Meeting of The Society of Thoracic Surgeons New Orleans, LA January 26, 1998

Open Heart Surgery in DiabetesOpen Heart Surgery in DiabetesPortland CII ProtocolPortland CII Protocol
MortalityMortality AllAll (99/2467) 4.0%(99/2467) 4.0%
SQI SQI 6.1% 6.1%
CIICII 3.0% 3.0%
DSWIDSWI 19.0% 19.0%
No DSWI 3.8%No DSWI 3.8%
Recent ExperienceRecent Experience
1994-1997 DSWI as in non-diabetics1994-1997 DSWI as in non-diabetics
1996-7 No DSWI in last 15 mo.1996-7 No DSWI in last 15 mo.

Open Heart Surgery in DiabetesJohn Hopkins
24.3% with infections
BG divided into quartiles Relative Odds
Q1 121-206 20.1%
Q2 207-229 21.6% 1.17
Q3 230-252 29.8% 1.86*
Q4 252-352 25.7% 1.72*
Golden SH Diabetes Care 22: 1408, 1999 * P < 0.01

Admission glucose values >108 mg/dl
IV Insulin with Bypass Surgery
Hospital mortality identical
Diabetics and Non-diabetics (1.75%
vs. 1.71%)
Usual Diabetic Mortality 50% Higher
CABG in DiabetesKalin 1998

DIGAMI StudyDiabetes, Insulin Glucose Infusion in Acute Myocardial Infarction
Acute MI With BG > 200 mg/dl Intensive Insulin Treatment IV Insulin For > 24 Hours Four Insulin Injections/Day For > 3 Months Reduced Risk of Mortality By:
28% Over 3.4 Years
51% in Those Not Previous Diagnosed
Malmberg BMJ 1997;314:1512Malmberg BMJ 1997;314:1512

Cardiovascular RiskMortality After MI Reduced by Insulin Therapy in the DIGAMI Study
Malmberg, et al. BMJ. 1997;314:1512-1515.
All Subjects
(N = 620)Risk reduction (28%)
P = .011
Standard treatment
0
.3
.2
.4
.7
.1
.5
.6
0 1Years of Follow-up
2 3 4 5
Low-risk and Not Previously on Insulin
(N = 272)Risk reduction (51%)
P = .0004
IV Insulin 48 hours, then 4 injections daily
0
.3
.2
.4
.7
.1
.5
.6
0 1Years of Follow-up
2 3 4 5
6-11

623 Hyperglycemic Patients
Mortality and Stroke Severity
Increase Linearly with BG
BG >144 mg/dl in First 24 Hours
Double Mortality Risk
Stroke in Diabetes
Weir

Diabetes with Steroid TherapyPiedmont Hospital
1998
Problem Noted by DRC Case Managers
– Frequency of Hyperglycemia in “Non-Diabetic” Patients
– Prevalence Among Steroid Treated
– No Systematic Plan of Response
– Frequency of Discharge “Out-of-Control”
The Dark Side of CorticosteroidsThe Dark Side of Corticosteroids

Diabetes with Steroid TherapyPiedmont Hospital1998
N ot Tes ted0 %
N ot Trea ted0 %
U n con tro lled B G6 3 %
1 2 % o f To ta l
C on tro lled B G3 7 %
Trea ted1 0 0 %
B G > 2 0 01 0 0 %
C on tro lled B G0 %
B G Tes ted1 0 0 %
K n ow n D iab e tes1 9 %
N ot Tes ted2 6 %
2 1 % o f To ta l
N o t Trea ted2 3 %
7 % o f To ta l
U n con tro lled B G8 0 %
1 9 % o f To ta l
C on tro lled B G2 0 %
Trea ted7 7 %
B G > 2 0 05 2 %
C on tro lled B G4 8 %
B G Tes ted7 4 %
N o R ecord ed D iab e tes8 1 %
P atien ts R ece ivin g > 5 0 m g m P red n ison e E q u iva len t in O n e D ay6 6 3 1 ou t o f 2 5 ,3 0 9 A d m iss ion s
Chart Review by Terry Kaplan RNChart Review by Terry Kaplan RN

Diabetes with Steroid TherapyPiedmont Hospital1998
Controlled41%
Not Tested21%
Not Treated7%
Uncontrolled31%
Opportunity for Improvement 59%

Classical Diabetes ManagementTypical A1c 9%
The daily dosage of insulin is divided
– 2/3 in the morning and 1/3 in the evening.
– Two thirds NPH and 1/3 Regular.
Results
– 70/30 Insulin
• (The insulin for the retarded)
– No Patients to Goal!

Sliding Scale Insulin
Five Units for Each Plus on bid Urine TestingTable of BG Ranges and R DosesCorrection Bolus Formula
–(BG-Target BG) / CF
No Benefit When Used Without Basal InsulinThree Times More Hyperglycemia Compared to Standing Dose NPHQueale, 1997

ICU Survival
1548 Patients (mostly OHS pts.)
All with BG >200 mg/dl
Randomized into two groups
– Maintained on IV insulin
– Conventional group (BG 180-200)
– Intensive group (BG 80-110)
Conventional Group had 1.74 X mortality
Van den Berghe et al, NEJM 2001;345(19):1359

ICU Survival
Conventional Intensive
Mean AM BG 153 103
% Receiving Insulin 39% 100%
BG < 40 mg/dl 6 39
Van den Berghe et al, NEJM 2001;345(19):1359
No serious hypoglycemic events

ICU Survival
Intensive Therapy (80 to 110 mg/dL) resulted in:
34% reduction in mortality
46% reduction in sepsis
41% reduction in dialysis
50% reduction in blood transfusion
44% reduction in polyneuropathy
Van den Berghe et al, NEJM 2001;345(19):1359

ICU IV Insulin Protocol
Arterial BG q 1-2 hrs
If > 100 mg/dl, 2 U/h If > 200 mg/dl, 4 U/h
If > 140 mg/dl, increase by 1 – 2 U/h
If 121 to 140 mg/dl, increase by 0.5 – 1 U/h
If 111 to 120 mg/dl, increase by 0.1 – 0.5 U/h
If 81 to 110 mg/dl, no change
If 61 to 80 mg/dl, change back to prior rate
Van den Berghe et al, NEJM 2001;345(19):1359

Methods For Managing Hospitalized Persons with Diabetes
Continuous Variable Rate IV Insulin Drip
Major Surgery, NPO, Unstable, MI, DKA, Hyperglycemia, Steroids, Gastroparesis, Delivery, etc
Basal / Bolus Therapy (MDI)

Continuous Variable Rate IV Insulin Davidson 1982
Mix Drip with 125 units Regular Insulin in 250 cc NS
Starting Rate: Units / hour = (BG – 60) x 0.02
Check glucose hourly and adjust
Change Multiplier to keep in desired range
– 100 to 140 mg/dl

Continuous Variable Rate IV Insulin
Adjust Multiplier to obtain glucose in target range
If BG not decreasing > 50 mg/dL and > 140 mg/dL, increase by 0.01
If BG < 100 mg/dL, decrease by 0.01
If BG 100 to 140 mg/dL, no change in Multiplier If BG is < 80 mg/dL, Give D50 cc = (100 – BG) x 0.4 Give continuous rate of Glucose in IVF’s Once eating, continue drip till 2 hour post SQ
insulin

Glucommander
Invented in 1984 Davidson and Steed
Based on 17 Year Experience with a Computer Based Algorithm for the Administration of IV Insulin
Developed for Marketing by MiniMed and Roche
GMS System
Shelved Pending FDA Approval of IV Use of Insulin
Useful and Safe for Any Application of IV Insulin

Glucommander
Computer Based Algorithm for IV Insulin
Invented by Davidson and Steed in 1984
17 Year Experience
Developed for Marketing by MiniMed and Roche
GMS System
Shelved Pending FDA Approval of IV Insulin
Useful and Safe for Any Application of IV Insulin

Glucose Management System

Glucommander .
Summary of PerformanceGlucose Averages for 3404 Patients
Glu
cose
mg
m/d
l
Hours
50
Pe
rce
nti
les
90
10

Glucommander . Effectiveness
Initial blood glucose
– Median 292 mg/dl
– Range 181-1,568 Time to achieve glucose < 180 mg/dl
– Median 3 hours
– Range 0.3 - 19.7 Time to achieve first of three consecutive glucose results between 60 -
180 mg/dL
– Median 3. 1 hours
– Range 0.3 - 22.5

GlucommanderPrinciples
0123456789
10
0 100 200 300 400 500
Insu
lin
Un
its
/ H
ou
r
Glucosemgm / dl

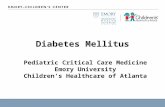
GlucommanderComparsion to Other Systems
0123456789
10
0 100 200 300 400 500
Insu
lin
Un
its
/ H
ou
r
Glucosemgm / dl
Glucommander
ADA
MARKS
FURNEY
METCHICK
VAN DEN BERGHE
IV DRIP

Hospital Diabetes PlanHospital Diabetes Plan
NPO Pathway For All Diabetes PatientsNPO Pathway For All Diabetes Patients
Finger Stick BG ac qid on ALL AdmissionsFinger Stick BG ac qid on ALL Admissions
Check All Steroid Treated PatientsCheck All Steroid Treated Patients
Diagnose DiabetesDiagnose Diabetes
FBG >126 mg/dlFBG >126 mg/dl
Any BG >200 mg/dlAny BG >200 mg/dl
Paul Davidson MDPaul Davidson MDAtlanta Diabetes AssociatesAtlanta Diabetes Associates

Hospital Diabetes PlanHospital Diabetes Plan
Document Diagnosis in ChartDocument Diagnosis in Chart
Hyperglycemia Is Diabetes Until Proven OtherwiseHyperglycemia Is Diabetes Until Proven Otherwise
Bring to All Physician’s AttentionBring to All Physician’s Attention
Note on Problem List and Face SheetNote on Problem List and Face Sheet
Check Hemoglobin A1CCheck Hemoglobin A1C
Hold Metformin; Hold TZD with CHF, Liver DysfunctionHold Metformin; Hold TZD with CHF, Liver Dysfunction
Use Insulin in All Hospitalized Persons with Diabetes Use Insulin in All Hospitalized Persons with Diabetes Continue for Course of Hospitalization
Paul Davidson MDAtlanta Diabetes Associates

Hospital Diabetes PlanHospital Diabetes Plan
Get Diabetes Education ConsultGet Diabetes Education Consult
Instruct Patient in Monitoring and RecordingInstruct Patient in Monitoring and Recording
See That Patient Has Meter on DischargeSee That Patient Has Meter on Discharge
Decide on Case Specific Program for DischargeDecide on Case Specific Program for Discharge
Arrange Early F/U with PCPArrange Early F/U with PCP
Paul Davidson MDAtlanta Diabetes Associates

Hospital Diabetes PlanHospital Diabetes Plan
Follow National Guidelines For Endocrinology Consults
– Any Type 1
– Any Hypoglycemia Requiring Intervention
– DKA or HHNC
– Patient on Insulin Pump
– Pregnant Diabetic
– Glucocorticoid Therapy in Diabetes
– Progressive Diabetic Complications
– HbA1c >8%, Microalbuminuria >30 mg,LDL >130, HDL <35, TG >400 mg/dl

Treat Any Patient With BG > 150 With InsulinTreat Any Patient With BG > 150 With Insulin
– Treat Any BG >150 with Rapid-acting Insulin Treat Any BG >150 with Rapid-acting Insulin (BG-100) / (7000 / wt #) (BG-100) / (7000 / wt #)
– Treat Any Recurrent BG >200 with IV InsulinTreat Any Recurrent BG >200 with IV Insulin
If More than 0.5 u/hr IV Insulin Required with Normal If More than 0.5 u/hr IV Insulin Required with Normal BG Start Long Acting InsulinBG Start Long Acting Insulin
Protocol for Insulin in Hospitalized PatientProtocol for Insulin in Hospitalized Patient

• Prescription for insulin therapy includes:
• Basal Insulin (BI)
• Carbohydrate-to-Insulin Ratio (CIR)
• Correction Factor (CF)
•1600 Records from Pump Patients Studied
•Data from 182 best-controlled pump patients
• Analyzed for optimum parameters
•Resulting formulae used as model for others
• The Accurate Insulin Management (AIM) formulae
The Accurate Insulin Management (AIM) Formulae

RESULTS
Accurate Insulin Management
(AIM) formulaeCarbohydrate-to-Insulin Ratio:
CIR=2.8*BW#/TDDCorrection Factor:
CF=1700/TDDBasal Insulin:
Basal=0.48*TDD

0
50
100
150
200
250
300
0 50 100 150 200
Total Daily Dose of Insulin (TDD)
Bo
dy
We
igh
t in
lbs
125
100
75
50
25
Co
r rection
Facto
r
25 20 15 12 10 9 8 7 6 5
Carbohydrate to Insulin Ratio
CF Curve
AIM Nomogram
Davidson et al Diab Tech Ther 2003 Vol 5 No 2
( CIR = 2.8 Wt / TDD )( C
F =
17
00
/ TD
D )
Intial Dosing: Plot BW and 25 CIR for BI Plot BW and 12 CIR for TDD
Plot BW and TDDfor CIRPlot TDD and CF curve for CFFollow-up Dosing: Change CF as above Change CIR by 20% toward CIRAIM
4
3
2

Protocol for Insulin in Hospitalized PatientProtocol for Insulin in Hospitalized Patient
Daily Total: Pre-Admission or Weight (#) x 0.24 uDaily Total: Pre-Admission or Weight (#) x 0.24 u
– 50 % as Glargine (Basal) 50 % as Glargine (Basal)
• Split as q 12 DosesSplit as q 12 Doses
– 50% as Rapid-acting Insulin (Bolus)50% as Rapid-acting Insulin (Bolus)
• Give in Proportion to CHO Eaten, CIR 12Give in Proportion to CHO Eaten, CIR 12 BG >150: (BG-100) / CFBG >150: (BG-100) / CF
– CF = 7000 / Wt(#) CF = 7000 / Wt(#) Do Not Use Sliding Scale As Only InsulinDo Not Use Sliding Scale As Only Insulin Do Not Hold Insulin When BG Normal

Protocol for Insulin in Hospitalized PatientProtocol for Insulin in Hospitalized Patient
Treatment of HypoglycemiaTreatment of Hypoglycemia
Any BG <80 mg/dl: D50 = (100-BG) x 0.4 ml IVAny BG <80 mg/dl: D50 = (100-BG) x 0.4 ml IV
Do Not Hold Insulin When BG NormalDo Not Hold Insulin When BG Normal

20
40
60
80
100
120
140
160
Glu
cose
Correction of Hypoglycemia with Glucose100-BG X 0.2 Grams
Before After
Richardson Diabetes 1999 50:A200
100-BG X 0.15 Grams

Hospital Diabetes PlanHospital Diabetes PlanConclusionsConclusions
Any BG >200 mg/dl Is Diabetes (Fasting >126 mg/dl)Any BG >200 mg/dl Is Diabetes (Fasting >126 mg/dl)
Most Diabetes Is Type 2Most Diabetes Is Type 2
All DM patients Must Self-Monitor BG’s and RecordAll DM patients Must Self-Monitor BG’s and Record
No BG >150 mg/dl Should Go UntreatedNo BG >150 mg/dl Should Go Untreated
Most Hospitalized DM Patients Should Be on InsulinMost Hospitalized DM Patients Should Be on Insulin
IV Insulin is Most Effective, Efficient, Safest Rx in Acute Illness IV Insulin is Most Effective, Efficient, Safest Rx in Acute Illness (Glucommander)(Glucommander)

Hospital Diabetes PlanHospital Diabetes Plan Conclusions 2
Switch to Basal Insulin Glargine– IV Hourly Dose X 24 / 2
DC IV Glucose Feed and Give Rapid Acting Insulin p.c.
– One Unit Per 12 Grams CHO BG ac tid, hs, 3 am
– Correct with Rapid Insulin• (BG - 100) / 7000 / BW#
Type 2 Diabetics Are Resistant to Insulin Reactions
Treat Insulin Reactions in Hospital With IV Glucose
Do Not Be Hold Insulin for Normal BG, i.e. 80-120
HbA1c Values >7% Indicates Sub-optimal Care

Hospital Diabetes PlanHospital Diabetes Plan Conclusions 3
Discharge Plan For BG Control
The Physician of Record Is the Link Between the Best
Diabetes Care and the Patient
Use Available Diabetes Resources
Diabetes Educators
Dietiticians
Endocrinologists

The Paradigm for the MilleniumThe Paradigm for the MilleniumHyperglycemia: A “Mortal” SinHyperglycemia: A “Mortal” Sin
A blood glucose over 200 in a hospitalized patient A blood glucose over 200 in a hospitalized patient causes increased morbidity and mortality.causes increased morbidity and mortality.
In the 21st Century In the 21st Century
Neglecting BG >200 Neglecting BG >200
Is MalpracticeIs Malpractice

Conclusion
All hospital patients should have normal glucose

Insulin
The agent we have
to control glucose
only
most powerfulpowerful

QUESTIONS
For a copy or viewing of these slides, contact
WWW.adaendo.com