diabetes-ED
6
REVIEW Pathophysiology of diabetic erectile dysfunction: potential contribution of vasa nervorum and advanced glycation endproducts S Cellek 1 , NE Cameron 2 , MA Cotter 2 and A Muneer 3 Erectile dysfunction (ED) due to diabetes mellitus remains difficult to treat medically despite advances in pharmacotherapeutic approaches in the field. This unmet need has resulted in a recent re-focus on the pathophysiology, in order to understand the cellular and molecular mechanisms leading to ED in diabetes. Diabetes-induced ED is often resistant to PDE5 inhibitor treatment, thus there is a need to discover targets that may lead to novel approaches for a successful treatment. The aim of this brief review is to update the reader in some of the latest development on that front, with a particular focus on the role of impaired neuronal blood flow and the formation of advanced glycation endproducts. International Journal of Impotence Research (2013) 25, 1–6; doi:10.1038/ijir.2012.30; published online 23 August 2012 Keywords: advanced glycation endproducts; diabetes mellitus; erectile dysfunction; hypoxia; microvessel; nitric oxide; vasa nervorum INTRODUCTION Penile erection is the result of relaxation of smooth muscle in the cavernous body and associated blood vessels. 1 Smooth muscle relaxation is mediated primarily by nitric oxide (NO), which is a gaseous and labile mediator, yet one of the most potent endogenous smooth muscle relaxants. NO is synthesised by neuronal NO synthase (nNOS) in the autonomic postganglionic parasympathetic nerves (nitrergic nerves) 2,3 and by endothelial nitric oxide synthase in the endothelium lining the blood vessels and cavernosal sinusoids. Nerve impulses in response to sexual stimulus are carried from the spinal cord to the hypogastric plexus where the cell bodies of the nitrergic nerves are located. Once activated, the nitrergic neurones within the hypogastric plexus transmit action potential through their axons to the penile vasculature. These nitrergic axons then release high quantities of NO on to the nearby smooth muscle cells. NO diffuses rapidly into the smooth muscle cells, causing relaxation by increasing the intracellular concentrations of cGMP. The relaxation of the cavernosal and arterial smooth muscle results in an increase in blood flow into the penis. In turn, this causes shear stress on the endothelial lining, which promotes phosphorylation and prolonged activation of endothelial nitric oxide synthase leading to long-lasting release of NO from the endothelium to maintain the smooth muscle relaxation. 4 As the intracavernosal pressure reaches the level of the systemic arterial blood pressure, the subtunical venules are compressed, which results in a rigid erection. Diabetes mellitus is one of the predominant risk factors of erectile dysfunction (ED) and also one of the most difficult to treat. 5,6 Approximately 50% of diabetic men will suffer from ED within 10 years of the diagnosis. 7 ED presenting in these men is widely regarded as a manifestation of more systemic vascular disease and is likely to precede a coronary event by 5 years. 8,9 Combined with the prevalence of obesity and metabolic syndrome in these men, it is apparent that disease progression is likely to reduce the efficacy of conventional pharmacotherapeutic options for the treatment of ED in diabetic men. This has meant that diabetic men form a large group of patients undergoing end-stage treatment in the form of penile prosthesis surgery. Our knowledge regarding the pathophysiology of ED in diabetes has gradually increased since the 1990s. As NO is the main erectile mediator, the field has focussed on how diabetes alters the nitrergic and endothelial NO function. The aim of this paper is to update the reader with some of the latest development on that front, with a particular focus on the role of impaired neuronal blood flow, and the formation of advanced glycation end products. A NEED FOR TEMPORAL ANALYSIS The tone of penile vascular and cavernosal smooth muscle is regulated by vasodilators such as NO and vasoactive intestinal pep- tide, and by vasoconstrictors such as noradrenaline and endothelins. An imbalance in favour of the vasoconstrictors has been demon- strated in both type 1 and 2 diabetes. 9,10 Such an imbalance seems to be caused by several factors, all playing equal roles, such as decreased NO production from either nitrergic nerves or endothe- lium, 10 low responsiveness of the smooth muscle to vasodilators, 1 upregulation of the receptors for vasoconstrictor mediators such as endothelin 11 and increased vasoconstrictor production and/or release and hyper-responsiveness to vasoconstrictors. 12 It is important to study the progression of ED in a temporal fashion in order to gain a better understanding of the 1 Department of Translational Medicine, Cranfield Health, Cranfield University, Bedfordshire, UK; 2 School of Medical Sciences, University of Aberdeen, Aberdeen, UK and 3 Institute of Urology, University College London, London, UK. Correspondence: Dr S Cellek, Department of Translational Medicine, Cranfield Health, Cranfield University, Bedfordshire, MK43 0AL, UK. E-mail: s.cellek@cranfield.ac.uk Received 8 May 2012; revised 2 July 2012; accepted 20 July 2012; published online 23 August 2012 International Journal of Impotence Research (2013) 25, 1–6 & 2013 Macmillan Publishers Limited All rights reserved 0955-9930/13 www.nature.com/ijir
-
Upload
institute-for-the-study-of-urologic-diseases -
Category
Health & Medicine
-
view
526 -
download
0
description
Transcript of diabetes-ED

REVIEW
Pathophysiology of diabetic erectile dysfunction:potential contribution of vasa nervorum and advancedglycation endproductsS Cellek1, NE Cameron2, MA Cotter2 and A Muneer3
Erectile dysfunction (ED) due to diabetes mellitus remains difficult to treat medically despite advances in pharmacotherapeuticapproaches in the field. This unmet need has resulted in a recent re-focus on the pathophysiology, in order to understand thecellular and molecular mechanisms leading to ED in diabetes. Diabetes-induced ED is often resistant to PDE5 inhibitor treatment,thus there is a need to discover targets that may lead to novel approaches for a successful treatment. The aim of this brief review isto update the reader in some of the latest development on that front, with a particular focus on the role of impaired neuronal bloodflow and the formation of advanced glycation endproducts.
International Journal of Impotence Research (2013) 25, 1–6; doi:10.1038/ijir.2012.30; published online 23 August 2012
Keywords: advanced glycation endproducts; diabetes mellitus; erectile dysfunction; hypoxia; microvessel; nitric oxide; vasanervorum
INTRODUCTIONPenile erection is the result of relaxation of smooth muscle in thecavernous body and associated blood vessels.1 Smooth musclerelaxation is mediated primarily by nitric oxide (NO), which is agaseous and labile mediator, yet one of the most potentendogenous smooth muscle relaxants. NO is synthesised byneuronal NO synthase (nNOS) in the autonomic postganglionicparasympathetic nerves (nitrergic nerves)2,3 and by endothelialnitric oxide synthase in the endothelium lining the blood vesselsand cavernosal sinusoids. Nerve impulses in response to sexualstimulus are carried from the spinal cord to the hypogastric plexuswhere the cell bodies of the nitrergic nerves are located. Onceactivated, the nitrergic neurones within the hypogastric plexustransmit action potential through their axons to the penilevasculature. These nitrergic axons then release high quantities ofNO on to the nearby smooth muscle cells. NO diffuses rapidly intothe smooth muscle cells, causing relaxation by increasing theintracellular concentrations of cGMP. The relaxation of thecavernosal and arterial smooth muscle results in an increase inblood flow into the penis. In turn, this causes shear stress on theendothelial lining, which promotes phosphorylation andprolonged activation of endothelial nitric oxide synthase leadingto long-lasting release of NO from the endothelium to maintain thesmooth muscle relaxation.4 As the intracavernosal pressure reachesthe level of the systemic arterial blood pressure, the subtunicalvenules are compressed, which results in a rigid erection.
Diabetes mellitus is one of the predominant risk factors oferectile dysfunction (ED) and also one of the most difficult totreat.5,6 Approximately 50% of diabetic men will suffer from EDwithin 10 years of the diagnosis.7 ED presenting in these men iswidely regarded as a manifestation of more systemic vascular
disease and is likely to precede a coronary event by 5 years.8,9
Combined with the prevalence of obesity and metabolic syndromein these men, it is apparent that disease progression is likely toreduce the efficacy of conventional pharmacotherapeutic optionsfor the treatment of ED in diabetic men. This has meant thatdiabetic men form a large group of patients undergoing end-stagetreatment in the form of penile prosthesis surgery.
Our knowledge regarding the pathophysiology of ED indiabetes has gradually increased since the 1990s. As NO is themain erectile mediator, the field has focussed on how diabetesalters the nitrergic and endothelial NO function. The aim of thispaper is to update the reader with some of the latest developmenton that front, with a particular focus on the role of impairedneuronal blood flow, and the formation of advanced glycation endproducts.
A NEED FOR TEMPORAL ANALYSISThe tone of penile vascular and cavernosal smooth muscle isregulated by vasodilators such as NO and vasoactive intestinal pep-tide, and by vasoconstrictors such as noradrenaline and endothelins.An imbalance in favour of the vasoconstrictors has been demon-strated in both type 1 and 2 diabetes.9,10 Such an imbalance seemsto be caused by several factors, all playing equal roles, such asdecreased NO production from either nitrergic nerves or endothe-lium,10 low responsiveness of the smooth muscle to vasodilators,1
upregulation of the receptors for vasoconstrictor mediators such asendothelin11 and increased vasoconstrictor production and/orrelease and hyper-responsiveness to vasoconstrictors.12
It is important to study the progression of ED in a temporalfashion in order to gain a better understanding of the
1Department of Translational Medicine, Cranfield Health, Cranfield University, Bedfordshire, UK; 2School of Medical Sciences, University of Aberdeen, Aberdeen, UK and 3Instituteof Urology, University College London, London, UK. Correspondence: Dr S Cellek, Department of Translational Medicine, Cranfield Health, Cranfield University, Bedfordshire, MK430AL, UK.E-mail: [email protected] 8 May 2012; revised 2 July 2012; accepted 20 July 2012; published online 23 August 2012
International Journal of Impotence Research (2013) 25, 1–6& 2013 Macmillan Publishers Limited All rights reserved 0955-9930/13
www.nature.com/ijir

pathophysiology of the condition. Although such longitudinalstudies investigating the mechanisms at different time pointsof the disease are few,13 they provide invaluable information intoour understanding of diabetic ED. Similar longitudinal studiesfrom other fields within or outside the diabetes field14 also havebeen extremely useful in broadening our comprehension ofpathophysiological events.
THE STORY BEGINS WITH HYPERGLYCAEMIAAt the early stages of diabetes, before the patient has symptoms ofany complications such as ED and may not even be aware of theunderlying diagnosis and high blood glucose levels, there are twovery important factors that trigger the cascade of events: highblood glucose and low insulin (low insulin concentration in Type 1diabetes and low insulin action due to receptor resistance inType 2). The effect of high glucose on endothelial NO-dependentvasodilation has been debated: using isolated human blood vessels,high glucose concentrations have been shown to have varyingeffects on endothelial NO-dependent relaxations depending on thetype of the vascular bed.15,16 In humans, early reports have shownthat elevation of blood glucose concentrations does not affect theforearm blood flow.16,17 Later, it has been found that the reason forglucose-induced vasodilatation could be because of increasedinsulin levels as a direct response to glucose; insulin is knownto elicit vasodilation directly.17 When such studies were repeatedusing agents like octreotide to inhibit insulin secretion, henceremoving the influence of insulin on vasodilation, high glucoseconcentrations caused an acute and transient reduction inendothelium-dependent vasodilation.18–22 This has been attribu-ted to increased vasoconstrictor mediators22 and decreasedendothelial NO production23 as a direct response to hyper-glycaemia. Therefore we can deduce that acute and direct effectof hyperglycaemia could be a transient reduction in blood flow in ahealthy individual. In diabetic patients or individuals with impairedglucose tolerance, the recovery from reduced vasodilation has beenshown to be delayed.20,24
Although high glucose concentrations impair nitrergicfunction acutely and reversibly in vitro,24,25 ED occurs much laterin diabetic animal models.5,13,26–28 These observations have led theresearchers to conclude that endothelial dysfunction precedesnitrergic dysfunction. There seems to be a lag period betweenendothelial and ED; the latter coinciding with nitrergic dysfunction.In perspective, it takes a minimum of 4 weeks for a rat to developerectile and nitrergic dysfunction,13,27,28 whereas endothelialdysfunction can potentially develop in days as a directconsequence of hyperglycaemia, as mentioned above. So onequestion arising is: ‘What pathophysiological role could endothelialdysfunction play in the early stages of the development of ED?’.One potential answer comes from another area of the diabetesfield, the study of blood flow to peripheral nerves. Within days ofinduction of experimental diabetes, blood flow to major nervetrunks such as sciatic nerve has dropped.13,27,29–31 Recently such adramatic decrease in blood flow has also been shown in thesuperior cervical32 and in the major pelvic ganglia of diabetic rats.33
The latter is equivalent to hypogastric plexus in the human34 andcontains the cell bodies of the neurons that innervate theurogenital organs, including penis. Thus it is plausible that anearly decrease in blood flow to the ganglia in response to thediabetic state, including elevated glucose, may be the first steptriggering a series of events.
THE ROLE OF THE VASA NERVORUMThe ganglia where the cell bodies of the autonomic nerves arelocated are surrounded by small-diameter blood vessels (arteriolesand venules) known as vasa nervorum, which supply the bloodnecessary for the function of the neurons. All nerve trunks, from
large ones such as the sciatic nerve to small ones such as thecavernous nerve, have their own vasa nervorum. Earlier studieshave shown that vasa nervorum of the peripheral nerve trunks canbe divided into three groups: epineurial, perineurial andendoneurial.35 Epineurial and perineurial blood vessels form acomplex network known as the epineurial plexus.35 The epineurialplexus has prominent arteriovenous shunts, supplies theendoneurial vascular compartment and is innervated byautonomic nerves such as sympathetic and peptidergic nerves.36
However, such detailed information is not available for the vasanervorum of the autonomic ganglia, although ganglia have amuch greater metabolic demand than peripheral nerve trunk.35
Whether the vasa nervorum of autonomic ganglia can be dividedinto sub-compartments like in the peripheral nerve trunk is notknown. Moreover, details on the innervation of ganglion vasanervorum are sparse. We have recently shown that the rat majorpelvic ganglia are surrounded by numerous small diameter bloodvessels (20-120 mm), which are innervated by noradrenergic andnitrergic nerve fibres.37 A drop in blood flow by as much as 50% isobserved in the autonomic ganglia as early as 1 week afterdiabetes induction,32,33 although such an early decrease in bloodflow is not associated with ED initially. Thus drawing parallels withvasa nervorum in nerve trunks, it is likely that such a reduction inperfusion would cause ganglionic neurons to be exposed to ahypoxic environment.
CONSEQUENCES OF HYPOXIA IN AUTONOMIC GANGLIA ANDAXONSHypoxia can trigger several neuronal events both in the cell bodyand axon of the neuron: disturbances in membrane conductivity,impaired nerve conduction and action potential generation, anddecreased axonal transport. It is therefore not surprising thatnitrergic function in the isolated human corpus cavernosumdeteriorates in hypoxic conditions.38 However it should be notedthat the corpus cavernosum does not contain the neuronal cellbodies of the nitrergic nerves. To date, the effect of hypoxia onnitrergic neurons obtained either from human hypogastric plexusor rat major pelvic ganglia has not been studied. In the absence ofdirect evidence, inferences can be made from studies in otherparts of the peripheral and in the central nervous systems. Acutehypoxia or ischaemia alters the expression of endothelial nitricoxide synthase and nNOS in the blood vessels and centralneurons, respectively.39–45 In the nodose ganglion, which primarilyholds sensory neurons, acute hypoxia increases nNOS proteinexpression 2-4 folds.45 Upregulation of nNOS in the centralneurons is thought to be a compensatory mechanism to replenishthe blood flow by vasodilation and neovascularization. Whether asimilar phenomenon occurs in the autonomic ganglia remains tobe investigated.
Although acute hypoxia may increase nNOS expression transi-ently, nitrergic function deteriorates as the hypoxia is prolonged. Inchronic hypoxia models where animals were exposed to hypoxiafor extended periods, a significant decrease in nNOS expressionand NO production has been shown for nerves innervating thecerebral arteries46 and the central neurons.47 Interestingly chronicbladder outlet obstruction decreases nNOS expression in theintramural neurons of the bladder, which has been attributed to thechronic hypoxia caused by the urethral ligation.48,49 Althoughsympathetic neurons have received greater attention than nitrergicneurons within the ganglia, existing studies suggest that chronichypoxia causes a nitrergic–sympathetic imbalance in favour ofsympathetic system, which may contribute to conditions associatedwith chronic hypoxia such as hypertension and chronic respiratoryfailure.49
Acute and chronic hypoxia are associated with reduced nerveconduction velocity and neuronal action potential generation.50
In the central neurons, the reduction of nerve cell excitability
Vasa nervorum and AGEs in diabetic EDS Cellek et al
2
International Journal of Impotence Research (2013), 1 – 6 & 2013 Macmillan Publishers Limited

in hypoxia is primarily because of increased Kþ -conductance.Thus, the nerve cells are hyper-polarised and the input resistancereduced, causing higher threshold and reduction of synapticpotentials.51,52 In the peripheral nerves, hypoxia elicitedreductions in both sensory and motor conduction velocitiessimilar to those observed in diabetic animals.53
Another consequence of hypoxia on the central and peripheralnerves is a reduction in axonal (axoplasmic) transport. Theneurons transport the proteins, lipids, vesicles and organelles todistal parts of their axons via axonal transport. Considering that anaxon can be as long as 1-2 m (for example, in the sciatic nervetrunk) compared with its neuronal body (B10mm), an efficienttwo-way transport system akin to a very busy highway is requiredto meet the metabolic and functional needs of a neuron.Disruption of axonal transport can result in acute accumulationof proteins in the cell body, mitochondrial dysfunction in the distalparts of the nerve and loss of neuronal function which caneventually lead to axonal and/or neuronal degeneration. Diabetesis known to alter axonal transport.54 Rats exposed to hypoxia forup to 24 h have increased nNOS protein in the peripheralganglia.39 Interestingly, patients with chronic mountain sicknesswho suffer from ‘‘burning feet and hands’’ sensation at highaltitudes (low oxygen) exhibited mild sensory neuropathy whichwas attributed to the disruption of axonal transport.55 We havepreviously shown that nNOS protein is depleted in the axons andaccumulates in the autonomic ganglia of diabetic rats.13,14
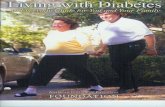
Overall it can be hypothesised that, hypoxia secondary todiabetes-induced dysfunction of vasa nervorum supplying thenerve trunks and ganglia alters neuronal electrophysiology andaxonal transport (Figure 1). Such effects can happen acutely andare often reversible as noted in both animal and human studiesmentioned above. For example, patients who return to loweraltitude after a trip in the mountains report improvement in their‘burning feet and hands’ symptoms within weeks.55
CONSEQUENCES OF NERVE DYSFUNCTION AND AXONALTRANSPORT DEFECTReduced conduction velocity develops in motor and sensorynerves within 2–3 weeks of diabetes induction in rats.29 Duringthis phase, there are no obvious structural alterations to thenerves and the deficit is largely reversible on the establishment of
normoglycaemia with insulin.56,57 A somewhat similarphenomenon can be observed in patients who were newlydiagnosed with Type 1 or 2 diabetes.58–61 Autonomic nervesfollow a similar pattern: nitrergic dysfunction, nNOS depletion inthe axons and accumulation in the ganglia can be reversed usinginsulin within the first 10 weeks of diabetes in rats, whereas thereis no loss of neurons.13,14 We have previously coined the term‘reversible phase’ followed by ‘a point of NO return’ (Figure 1).26
Thus, it is important to diagnose and start treatment within thefirst few years of human diabetes. The two largest trials in thediabetes field: The United Kingdom Prospective Diabetes Study(UKPDS62) and the Diabetes Control and Complications Trial(DCCT63) have answered the question of whether blood glucosecontrol is beneficial for people with diabetes with respect to thedevelopment of complications. It definitely is. Although improvedglycaemic control reduces the incidence of diabetic compli-cations,62,63 physiological levels of control are difficult to achieve.In addition, as diabetes duration increases, complications developand confounders such as chronic hypertension and dyslipidaemiacontribute to the complications, thus lessening the beneficialimpact of tight glycaemic control.64
HOW DO THE REVERSIBLE CHANGES BECOME IRREVERSIBLE?Data suggest that this could be because of several factors:Primarily, the ongoing impact of hypoxia and nerve dysfunction;secondarily, owing to the accumulation of advanced glycationendproducts (AGEs). AGEs are adducts formed on proteins andlipids following non-enzymatic glycation and oxidisation afterexposure to aldose sugars and their metabolites. Similar adductsmay be formed by lipid-oxidation products. AGEs are formednaturally in human body, and they are also ingested in food as aresult of cooking processes. They accumulate with age on long-lived proteins such as collagen. Diabetes is considered anaccelerated form of aging65 because of this elevated AGEaccumulation.66 In addition, it is becoming increasingly apparentthat relatively rapid intracellular AGE formation, primarily as aresult of increased methylglyoxal levels resulting from triosemetabolism, has marked effects in the pathophysiology of diabeticcomplications, including endothelial dysfunction.67–71
AGEs are implicated in the pathophysiology of both micro- andmacrovascular complications.72 They can induce oxidative stress in
DIABETES hyperglycemiadyslipidemia
Vasoconstrictionin vasa nervorum
Hypoxiain ganglia
Axonaltransport
defect
Nerveconduction
defect
nNOSaccumulationin cell body
nNOSdepletion at
nerveterminals
AGEs
Nitrergicdegeneration
Irreversibleerectile
dysfunction
TIME
ED symptoms
NOproduction
at nerveterminals �
Endothelial dysfunction in
the penis
Endothelial NOproduction in
penis �
Point ofno
return
reversible phase irreversible phase
Figure 1. The schematic representation of temporal effect of microvascular deficit and advanced glycation endproducts (AGEs) on erectilefunction with particular emphasis on nitrergic nerves.
Vasa nervorum and AGEs in diabetic EDS Cellek et al
3
& 2013 Macmillan Publishers Limited International Journal of Impotence Research (2013), 1 – 6

the cells either by binding to specific receptors (for example,receptor for AGEs), or as a result of their chemical reactions.73
AGEs have been shown to reduce endothelium-dependentvasorelaxation by altering the endothelial NO synthasesynthesis74,75 and have been associated with impairedendothelium-dependent vasodilation in Type 2 diabeticpatients.76 AGEs accumulate both in the penis77,78 and majorpelvic ganglia during diabetes.13,26,79 Exposure of humanneuroblastoma cells, which are differentiated into cholinergic-nitrergic phenotype to AGEs, induces apoptosis in a NO-dependent manner.79 It has also been demonstrated thatreceptor for AGEs expression is enhanced by ischaemia in theheart80 and brain.81 Although the effect of AGEs in combinationwith hypoxia have not been studied specifically in nitrergicneurons, it is plausible that under hypoxic conditions thedetrimental effect of AGEs may be enhanced. Thus, hypoxia,owing to microvascular defects in the ganglia, combined with thecytotoxic effects of accumulating AGEs might be specificallydetrimental to nitrergic neurons. The death of nitrergic neuronswould result in irreversible decrease in neuronal numbers in theganglia as those neurons are not able to replicate themselves orregenerate. Such a loss of neurons would inevitably push thepathology into the irreversible phase (Figure 1).
Studies with inhibitors of AGE formation, such as the reactivecarbonyl scavenger, aminoguanidine, have shown several bene-ficial effects in experimental diabetes. Thus, diabetic deficits inNO-mediated endothelium-dependent vasorelaxation were pre-vented, peripheral nerve conduction velocity and blood flow wasimproved, and several studies have shown prevention andreversal of ED in the early stages of diabetes.78,82–84 An AGE-breaker, ALT-711 (alagebrium) was also able to reverse the ED indiabetic rats.85 It should be noted that ALT-711 has beensuggested to have secondary effect on oxidative stress as it is ametal chelator compound.86 Nevertheless, the removal of alreadyformed AGEs from the body remains a potentially importanttherapeutic approach.
WHAT ARE THE TREATMENT OPTIONS WITHIN VASCULARHYPOTHESIS?As the hypoxia caused by microvascular deficit is the triggerleading to a series of events that eventually cause irreversibledamage (Figure 1), would the reversal of hypoxia be clinicallybeneficial? In diabetic patients who suffer from painfulperipheral neuropathy, PDE5 inhibitors have elicited acute reliefof pain87 this has been attributed to the vasodilator effect ofPDE5 inhibitors in the vasa nervorum supplying the nerves,although the situation here is complex to interpret as NO hasbeen implicated in pain processing.88 Similarly, PDE5 inhibitorshave been shown to be efficacious in relieving lower urinary tractsymptoms related to benign prostatic hyperplasia,89 which couldbe attributed to the vasodilator effect of PDE5 inhibitors in thevasa nervorum supplying the nerves and ganglia innervating theurinary bladder.
Cholesterol-lowering drugs such as statins,90,91 vasodilatorssuch as alpha-1 adrenoceptor antagonists, beta-2 adrenoceptoragonists,92–94 angiotensin-converting enzyme inhibitors,91,94–97
angiotensin receptor blockers,98 endopeptidase inhibitors99 andgene therapy such as vascular endothelial growth factor(VEGF100,101) have been shown to be beneficial in correctingnerve blood flow and function in diabetes in pre-clinical andclinical studies. Other approaches such as thiamine, PARPinhibitors and SOD/catalase mimetics to relieve the oxidativestress and restore endothelial function can also be of potentialbenefit to restore blood flow into the vasa nervorum.102 Novelvasodilator approaches specific to vasa nervorum may be ofpotential therapeutic value in the future.
CONCLUSIONSIt is highly plausible that a microvascular deficit in the vasanervorum of nerve trunks and ganglia is a major trigger for acascade of events that eventually lead to diabetic neuropathy andautonomic neuropathy. ED is a consequence of these events and ifnot treated early may become irreversible. Restoring diminishedblood flow to the vasa nervorum as early as possible beforeirreversible changes such as fibrosis and neuronal degenerationoccur should be a key aim of medical management of diabeticneuropathy. Clearly, we still have several challenges to meet:improving our understanding how the vasa nervorum tone isregulated by endothelial and neuronal mediators, and thedevelopment of non-invasive blood flow measurement techni-ques in human vasa nervorum to further test the validity of thishypothesis.
CONFLICT OF INTERESTThe authors declare no conflict of interest.
ACKNOWLEDGEMENTSThe authors wish to thank the European Society for Sexual Medicine (ESSM) forcontinuing support.
REFERENCES1 Gratzke C, Angulo J, Chitaley K, Dai YT, Kim NN, Paick JS et al. Anatomy,
physiology, and pathophysiology of erectile dysfunction. J Sex Med 2010; 7:445–475.
2 Moncada S, Higgs A, Furchgott R. International Union of PharmacologyNomenclature in Nitric Oxide Research. Pharmacol Rev 1997; 49: 137–142.
3 Cellek S. Let’s make NO mistake! Int J Impot Res 2005; 17: 388–389.4 Hurt KJ, Musicki B, Palese MA, Crone JK, Becker RE, Moriarity JL et al. Akt-
dependent phosphorylation of endothelial nitric-oxide synthase mediates penileerection. Proc Natl Acad Sci USA 2002; 99: 4061–4066.
5 Cameron NE, Cotter MA. Erectile dysfunction and diabetes mellitus: mechanisticconsiderations from studies in experimental models. Curr Diab Rev 2007; 3:149–158.
6 Chitaley K, Kupelian V, Subak L, Wessells H. Diabetes, obesity and erectiledysfunction: field overview and research priorities. J Urol 2009; 182: S45–S50.
7 Vinik AI, Erbas T. Recognizing and treating diabetic autonomic neuropathy.Cleve Clin J Med 2001; 68: 928–944.
8 Jackson G. Erectile dysfunction: a marker of silent coronary artery disease.Eur Heart J 2006; 27: 2613–2614.
9 Cellek S. Nitrergic-noradrenergic interaction in penile erection: a new insight intoerectile dysfunction. Drugs Today (Barc) 2000; 36: 135–146.
10 Toda N, Ayajiki K, Okamura T. Nitric oxide and penile erectile function. PharmacolTher 2005; 106: 233–266.
11 Ritchie R, Sullivan M. Endothelins & erectile dysfunction. Pharmacol Res 2011; 63:496–501.
12 Zhang XH, Melman A, Disanto ME. Update on corpus cavernosum smoothmuscle contractile pathways in erectile function: a role for testosterone? J SexMed 2011; 8: 1865–1879.
13 Cellek S, Foxwell NA, Moncada S. Two phases of nitrergic neuropathy in strep-tozotocin-induced diabetic rats. Diabetes 2003; 52: 2353–2362.
14 Cellek S, Anderson PN, Foxwell NA. Nitrergic neurodegeneration in cerebralarteries of streptozotocin-induced diabetic rats: a new insight into diabeticstroke. Diabetes 2005; 54: 212–219.
15 MacKenzie A, Cooper EJ, Dowell FJ. Differential effects of glucose on agonist-induced relaxations in human mesenteric and subcutaneous arteries. Br JPharmacol 2008; 153: 480–487.
16 Houben AJ, Schaper NC, de Haan CH, Huvers FC, Slaaf DW, de Leeuw PW et al.Local 24-h hyperglycemia does not affect endothelium-dependent or -inde-pendent vasoreactivity in humans. Am J Physiol 1996; 270: H2014–H2020.
17 Anderson EA, Hoffman RP, Balon TW, Sinkey CA, Mark AL. Hyperinsulinemiaproduces both sympathetic neural activation and vasodilation in normalhumans. J Clin Invest 1991; 87: 2246–2252.
18 Akbari CM, Saouaf R, Barnhill DF, Newman PA, LoGerfo FW, Veves A. Endo-thelium-dependent vasodilatation is impaired in both microcirculation andmacrocirculation during acute hyperglycemia. J Vasc Surg 1998; 28: 687–694.
Vasa nervorum and AGEs in diabetic EDS Cellek et al
4
International Journal of Impotence Research (2013), 1 – 6 & 2013 Macmillan Publishers Limited

19 Williams SB, Goldfine AB, Timimi FK, Ting HH, Roddy MA, Simonson DC et al.Acute hyperglycemia attenuates endothelium-dependent vasodilation inhumans in vivo. Circulation 1998; 97: 1695–1701.
20 Kawano H, Motoyama T, Hirashima O, Hirai N, Miyao Y, Sakamoto T et al.Hyperglycemia rapidly suppresses flow-mediated endothelium-dependentvasodilation of brachial artery. J Am Coll Cardiol 1999; 34: 146–154.
21 Title LM, Cummings PM, Giddens K, Nassar BA. Oral glucose loading acutelyattenuates endothelium-dependent vasodilation in healthy adults withoutdiabetes: an effect prevented by vitamins C and E. J Am Coll Cardiol 2000; 36:2185–2191.
22 Tesfamariam B, Brown ML, Deykin D, Cohen RA. Elevated glucose promotesgeneration of endothelium-derived vasoconstrictor prostanoids in rabbit aorta.J Clin Invest 1990; 85: 929–932.
23 Tesfamariam B, Brown ML, Cohen RA. Elevated glucose impairs endothelium-dependent relaxation by activating protein kinase C. J Clin Invest 1991; 87:1643–1648.
24 Way KJ, Reid JJ. Effect of diabetes and elevated glucose on nitric oxide-mediatedneurotransmission in rat anococcygeus muscle. Br J Pharmacol 1995; 115:409–414.
25 Utkan T, Yildiz F, Utkan NZ, Gacar N, Gocmez SS, Ulak G et al. Effects of diabetesand elevated glucose on nitrergic relaxations in the isolated duodenum of therat. Acta Diabetol 2009; 46: 295–301.
26 Cellek S. Point of NO return for nitrergic nerves in diabetes: a new insight intodiabetic complications. Curr Pharm Des 2004; 10: 3683–3695.
27 Ari G, Vardi Y, Finberg JP. Nitric oxide and penile erection in streptozotocin-diabetic rats. Clin Sci (Lond) 1999; 96: 365–371.
28 Vernet D, Cai L, Garban H, Babbitt ML, Murray FT, Rajfer J et al. Reductionof penile nitric oxide synthase in diabetic BB/WORdp (type I) andBBZ/WORdp (type II) rats with erectile dysfunction. Endocrinology 1995; 136:5709–5717.
29 Cameron NE, Cotter MA, Low PA. Nerve blood flow in early experimental dia-betes in rats: relation to conduction deficits. Am J Physiol 1991; 261: E1–E8.
30 Cameron NE, Eaton SE, Cotter MA, Tesfaye S. Vascular factors and metabolicinteractions in the pathogenesis of diabetic neuropathy. Diabetologia 2001; 44:1973–1988.
31 Coppey LJ, Davidson EP, Dunlap JA, Lund DD, Yorek MA. Slowing of motor nerveconduction velocity in streptozotocin-induced diabetic rats is preceded byimpaired vasodilation in arterioles that overlie the sciatic nerve. Int J Exp Diab Res2000; 1: 131–143.
32 Cameron NE, Cotter MA. Diabetes causes an early reduction in autonomicganglion blood flow in rats. J Diab Complications 2001; 15: 198–202.
33 Cameron NE, Cotter MA. Impaired corpus cavernosum responses to cavernousnerve stimulation in diabetic rats: effects of treatment with erythropoietin-delta.Autonom Neurosci 2009; 149: 24–25.
34 Dail WG. The pelvic plexus: innervation of pelvic and extrapelvic visceral tissues.Microsc Res Tech 1996; 35: 95–106.
35 Zochodne DW. Nerve and ganglion blood flow in diabetes: an appraisal. Int RevNeurobiol 2002; 50: 161–202.
36 Appenzeller O, Dhital KK, Cowen T, Burnstock G. The nerves to blood vesselssupplying blood to nerves: the innervation of vasa nervorum. Brain Res 1984;304: 383–386.
37 Cellek S, Smith S, Cameron NE, Cotter MA, Muneer A. Nitrergic innervation ofvasa nervorum supplying the major pelvic ganglion. J Sex Med 2011; 8: 407.
38 Muneer A, Cellek S, Dogan A, Kell PD, Ralph DJ, Minhas S. Investigation ofcavernosal smooth muscle dysfunction in low flow priapism using an in vitromodel. Int J Impot Res 2005; 17: 10–18.
39 Prabhakar NR, Pieramici SF, Premkumar DR, Kumar GK, Kalaria RN. Activation ofnitric oxide synthase gene expression by hypoxia in central and peripheralneurons. Brain Res Mol Brain Res 1996; 43: 341–346.
40 Prabhakar NR, Rao S, Premkumar D, Pieramici SF, Kumar GK, Kalaria RK. Reg-ulation of neuronal nitric oxide synthase gene expression by hypoxia. Role ofnitric oxide in respiratory adaptation to low pO2. Adv Exp Med Biol 1996; 410:345–348.
41 Phelan MW, Faller DV. Hypoxia decreases constitutive nitric oxide synthasetranscript and protein in cultured endothelial cells. J Cell Physiol 1996; 167:469–476.
42 Faller DV. Endothelial cell responses to hypoxic stress. Clin Exp Pharmacol Physiol1999; 26: 74–84.
43 Wei IH, Huang CC, Chang HM, Tseng CY, Tu HC, Wen CY et al. NeuronalNADPH-d/NOS expression in the nodose ganglion of severe hypoxic ratswith or without mild hypoxic preconditioning. J Chem Neuroanat 2005; 29:149–156.
44 Serrano J, Encinas JM, Fernandez AP, Rodrigo J, Martinez A. Effects of acutehypobaric hypoxia on the nitric oxide system of the rat cerebral cortex: pro-tective role of nitric oxide inhibitors. Neuroscience 2006; 142: 799–808.
45 Yamamoto Y, Henrich M, Snipes RL, Kummer W. Altered production of nitricoxide and reactive oxygen species in rat nodose ganglion neurons during acutehypoxia. Brain Res 2003; 961: 1–9.
46 Mbaku EM, Zhang L, Pearce WJ, Duckles SP, Buchholz J. Chronic hypoxia altersthe function of NOS nerves in cerebral arteries of near-term fetal and adultsheep. J Appl Physiol 2003; 94: 724–732.
47 Benesova P, Langmeier M, Betka J, Trojan S. Long-lasting changes in the densityof nitrergic neurons following kainic acid administration and chronic hypoxia.Physiol Res 2005; 54: 565–571.
48 Hu J, Chin CM, Png JC, Ng YK, Ling EA. The effect of chronic bladder outletobstruction on neuronal nitric oxide synthase expression in the intramuralganglia of the guinea pig bladder. J Urol 2004; 172: 1160–1165.
49 Prabhakar NR, Peng YJ, Jacono FJ, Kumar GK, Dick TE. Cardiovascular alterationsby chronic intermittent hypoxia: importance of carotid body chemoreflexes. ClinExp Pharmacol Physiol 2005; 32: 447–449.
50 Somjen GG, Aitken PG, Czeh G, Jing J, Young JN. Cellular physiology of hypoxiaof the mammalian central nervous system. Res Publ Assoc Res Nerv Ment Dis1993; 71: 51–65.
51 Leblond J, Krnjevic K. Hypoxic changes in hippocampal neurons. J Neurophysiol1989; 62: 1–14.
52 Schneider U, Quasthoff S, Mitrovic N, Grafe P. Hyperglycaemic hypoxia altersafter-potential and fast Kþ conductance of rat axons by cytoplasmic acidifica-tion. J Physiol 1993; 465: 679–697.
53 Hendriksen PH, Oey PL, Wieneke GH, van Huffelen AC, Gispen WH. Hypoxicneuropathy versus diabetic neuropathy. An electrophysiological study in rats.J Neurol Sci 1992; 110: 99–106.
54 Tomlinson DR, Mayer JH. Defects of axonal transport in diabetes mellitus--apossible contribution to the aetiology of diabetic neuropathy. J Auton Pharmacol1984; 4: 59–72.
55 Thomas PK, King RH, Feng SF. Muddle JR, Workman JM, Gamboa J, et al. Neuro-logical manifestations in chronic mountain sickness: the burning feet-burninghands syndrome. J Neurol Neurosurg Psychiatry 2000; 69: 447–452.
56 Greene DA, De Jesus PVJ, Winegrad AI. Effects of insulin and dietary myoinositolon impaired peripheral motor nerve conduction velocity in acute streptozotocindiabetes. J Clin Invest 1975; 55: 1326–1336.
57 Biessels GJ, Stevens EJ, Mahmood SJ, Gispen WH, Tomlinson DR. Insulin partiallyreverses deficits in peripheral nerve blood flow and conduction in experimentaldiabetes. J Neurol Sci 1996; 140: 12–20.
58 Ziegler D, Cicmir I, Mayer P, Wiefels K, Gries FA. The natural course of peripheraland autonomic neural function during the first two years after diagnosis of type1 diabetes. Klin Wochenschr 1988; 66: 1085–1092.
59 Ziegler D, Cicmir I, Mayer P, Wiefels K, Gries FA. Somatic and autonomic nervefunction during the first year after diagnosis of type 1 (insulin-dependent) dia-betes. Diab Res 1988; 7: 123–127.
60 Lehtinen JM, Niskanen L, Hyvonen K, Siitonen O, Uusitupa M. Nerve function andits determinants in patients with newly-diagnosed type 2 (non-insulin-depen-dent) diabetes mellitus and in control subjects--a 5-year follow-up. Diabetologia1993; 36: 68–72.
61 SoldersThalme G, Aguirre-Aquino B, Brandt M, Berg L, Persson U. A. Nerveconduction and autonomic nerve function in diabetic children. A 10-year follow-up study. Acta Paediatr 1997; 86: 361–366.
62 King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS):clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol1999; 48: 643–648.
63 The Diabetes Control and Complications Trial Research Group. The effect ofintensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329: 977–986.
64 Duckworth WC, Abraira C, Moritz TE, Davis SN, Emanuele N, Goldman S et al. Theduration of diabetes affects the response to intensive glucose control in type 2subjects: the VA Diabetes Trial. J Diab Complications 2011; 25: 355–361.
65 Kent S. Is diabetes a form of accelerated aging? Geriatrics 1976; 31: 140, 145,149-140, 145, 151.
66 Del TS, Basta G. An update on advanced glycation endproducts and atherosclerosis.Biofactors 2012.
67 Nishikawa T, Edelstein D, Brownlee M. The missing link: a single unifyingmechanism for diabetic complications. Kidney Int Suppl 2000; 77: S26–S30.
68 Brownlee M. The pathobiology of diabetic complications: a unifying mechanism.Diabetes 2005; 54: 1615–1625.
69 Berner AK, Brouwers O, Pringle R, Klaassen I, Colhoun L, McVicar C et al.Protection against methylglyoxal-derived AGEs by regulation of glyoxalase 1prevents retinal neuroglial and vasodegenerative pathology. Diabetologia 2012;55: 845–854.
70 Brouwers O, Niessen PM, Ferreira I, Miyata T, Scheffer PG, Teerlink T et al. Over-expression of glyoxalase-I reduces hyperglycemia-induced levels of advanced
Vasa nervorum and AGEs in diabetic EDS Cellek et al
5
& 2013 Macmillan Publishers Limited International Journal of Impotence Research (2013), 1 – 6

glycation end products and oxidative stress in diabetic rats. J Biol Chem 2011; 286:1374–1380.
71 Brouwers O, Niessen PM, Haenen G, Miyata T, Brownlee M, Stehouwer CD et al.Hyperglycaemia-induced impairment of endothelium-dependent vasorelaxationin rat mesenteric arteries is mediated by intracellular methylglyoxal levels in apathway dependent on oxidative stress. Diabetologia 2010; 53: 989–1000.
72 Giacco F, Brownlee M. Oxidative stress and diabetic complications. Circ Res 2010;107: 1058–1070.
73 Ramasamy R, Yan SF, Schmidt AM. Receptor for AGE (RAGE): signalingmechanisms in the pathogenesis of diabetes and its complications. Ann NY AcadSci 2011; 1243: 88–102.
74 Dhar A, Dhar I, Desai KM, Wu L. Methylglyoxal scavengers attenuate endothelialdysfunction induced by methylglyoxal and high concentrations of glucose.Br J Pharmacol 2010; 161: 1843–1856.
75 Dhar I, Dhar A, Wu L, Desai K. D-arginine attenuates methylglyoxal- and highglucose-induced endothelial dysfunction and oxidative stress by an eNOS-independent mechanism. J Pharmacol Exp Ther 2012.
76 Seals DR, Jablonski KL, Donato AJ. Aging and vascular endothelial function inhumans. Clin Sci (Lond) 2011; 120: 357–375.
77 Seftel AD, Vaziri ND, Ni Z, Razmjouei K, Fogarty J, Hampel N et al. Advancedglycation end products in human penis: elevation in diabetic tissue, siteof deposition, and possible effect through iNOS or eNOS. Urology 1997; 50:1016–1026.
78 Cartledge JJ, Eardley I, Morrison JF. Advanced glycation end-products areresponsible for the impairment of corpus cavernosal smooth muscle relaxationseen in diabetes. BJU Int 2001; 87: 402–407.
79 Cellek S, Qu W, Schmidt AM, Moncada S. Synergistic action of advanced glyca-tion end products and endogenous nitric oxide leads to neuronal apoptosisin vitro: a new insight into selective nitrergic neuropathy in diabetes. Diabeto-logia 2004; 47: 331–339.
80 Ramasamy R, Schmidt AM. Receptor for advanced glycation end products(RAGE) and implications for the pathophysiology of heart failure. Curr Heart FailRep 2012; 9: 107–116.
81 Ma L, Carter RJ, Morton AJ, Nicholson LF. RAGE is expressed in pyramidal cells ofthe hippocampus following moderate hypoxic-ischemic brain injury in rats. BrainRes 2003; 966: 167–174.
82 Cameron NE, Cotter MA, Robertson S. Rapid reversal of a motor nerve con-duction deficit in streptozotocin-diabetic rats by the angiotensin convertingenzyme inhibitor lisinopril. Acta Diabetol 1993; 30: 46–48.
83 Archibald V, Cotter MA, Keegan A, Cameron NE. Contraction and relaxation ofaortas from diabetic rats: effects of chronic anti-oxidant and aminoguanidinetreatments. Naunyn Schmiedebergs Arch Pharmacol 1996; 353: 584–591.
84 Usta MF, Bivalacqua TJ, Yang DY, Ramanitharan A, Sell DR, Viswanathan A et al.The protective effect of aminoguanidine on erectile function in streptozotocindiabetic rats. J Urol 2003; 170: 1437–1442.
85 Usta MF, Kendirci M, Gur S, Foxwell NA, Bivalacqua TJ, Cellek S et al. Thebreakdown of preformed advanced glycation end products reverses erectiledysfunction in streptozotocin-induced diabetic rats: preventive versus curativetreatment. J Sex Med 2006; 3: 242–250.
86 Sell DR, Monnier VM. Molecular basis of arterial stiffening: role of glycation.Gerontology 2012; 58: 227–237.
87 Hackett G. PDE5 inhibitors in diabetic peripheral neuropathy. Int J Clin Pract2006; 60: 1123–1126.
88 Miclescu A, Gordh T. Nitric oxide and pain: ’Something old, something new’.Acta Anaesthesiol Scand 2009; 53: 1107–1120.
89 Gacci M, Corona G, Salvi M, Vignozzi L, McVary KT, Kaplan SA et al. A systematicreview and meta-analysis on the use of phosphodiesterase 5 inhibitors alone orin combination with alpha-blockers for lower urinary tract symptoms due tobenign prostatic hyperplasia. Eur Urol 2012; 61: 994–1003.
90 Cameron N, Cotter M, Inkster M, Nangle M. Looking to the future: diabeticneuropathy and effects of rosuvastatin on neurovascular function in diabetesmodels. Diab Res Clin Pract 2003; 61(Suppl 1): S35–S39.
91 Ii M, Nishimura H, Kusano KF, Qin G, Yoon YS, Wecker A et al. Neuronal nitricoxide synthase mediates statin-induced restoration of vasa nervorum andreversal of diabetic neuropathy. Circulation 2005; 112: 93–102.
92 Cameron NE, Cotter MA, Ferguson K, Robertson S, Radcliffe MA. Effects ofchronic alpha-adrenergic receptor blockade on peripheral nerve conduction,hypoxic resistance, polyols, Na(þ )-K(þ )-ATPase activity, and vascular supply inSTZ-D rats. Diabetes 1991; 40: 1652–1658.
93 Cotter MA, Cameron NE. Correction of neurovascular deficits in diabetic rats bybeta2-adrenoceptor agonist and alpha1-adrenoceptor antagonist treatment:interactions with the nitric oxide system. Eur J Pharmacol 1998; 343: 217–223.
94 Reja A, Tesfaye S, Harris ND, Ward JD, Is ACE. inhibition with lisinopril helpful indiabetic neuropathy? Diabet Med 1995; 12: 307–309.
95 Malik RA. Can diabetic neuropathy be prevented by angiotensin-convertingenzyme inhibitors? Ann Med 2000; 32: 1–5.
96 Malik RA, Williamson S, Abbott C, Carrington AL, Iqbal J, Schady W et al. Effect ofangiotensin-converting-enzyme (ACE) inhibitor trandolapril on humandiabetic neuropathy: randomised double-blind controlled trial. Lancet 1998; 352:1978–1981.
97 Oltman CL, Davidson EP, Coppey LJ, Kleinschmidt TL, Lund DD, Yorek MA.Attenuation of vascular/neural dysfunction in Zucker rats treated with enalaprilor rosuvastatin. Obesity (Silver Spring) 2008; 16: 82–89.
98 Maxfield EK, Love A, Cotter MA, Cameron NE. Nerve function and regeneration indiabetic rats: effects of ZD-7155, an AT1 receptor antagonist. Am J Physiol 1995;269: E530–E537.
99 Oltman CL, Davidson EP, Coppey LJ, Kleinschmidt TL, Dake B, Yorek MA. Role ofthe effect of inhibition of neutral endopeptidase on vascular and neural com-plications in streptozotocin-induced diabetic rats. Eur J Pharmacol 2011; 650:556–562.
100 Ropper AH, Gorson KC, Gooch CL, Weinberg DH, Pieczek A, Ware JH et al.Vascular endothelial growth factor gene transfer for diabetic polyneuropathy: arandomized, double-blinded trial. Ann Neurol 2009; 65: 386–393.
101 Schratzberger P, Walter DH, Rittig K, Bahlmann FH, Pola R, Curry C et al. Reversalof experimental diabetic neuropathy by VEGF gene transfer. J Clin Invest 2001;107: 1083–1092.
102 Obrosova IG. Diabetes and the peripheral nerve. Biochim Biophys Acta 2009;1792: 931–940.
Vasa nervorum and AGEs in diabetic EDS Cellek et al
6
International Journal of Impotence Research (2013), 1 – 6 & 2013 Macmillan Publishers Limited