
Developmental programming therapies to reverse …/media/Files/Activity Files... · reverse...
43
Associate Professor Mark Vickers, Liggins Institute and Gravida: National Centre for Growth and Development, University of Auckland, New Zealand. Developmental programming – therapies to reverse metabolic disturbances
-
Upload
hoangnguyet -
Category
Documents
-
view
225 -
download
1
Transcript of Developmental programming therapies to reverse …/media/Files/Activity Files... · reverse...
Associate Professor Mark Vickers, Liggins Institute and Gravida: National Centre for Growth and Development, University of Auckland, New Zealand.
Developmental programming – therapies to reverse metabolic disturbances
Introduction
• well-established that alterations in
the early life environment increase risk
for obesity and metabolic and
cardiovascular disorders in offspring
• not a single cause but complex
multifactorial process
• while the underlying mechanisms are being elucidated, little is known about
interventions early in life to diminish
the incidence and severity of later disease
• Most evidence to date is derived from experimental models with limited translation
What interventions ? • Dietary
• lipids, pre-/probiotics, taurine, vitamins, polyphenols, methyl donors etc…
• Pharmacologic • Leptin, growth hormone, melatonin, GLP-1 analogs, nuclear receptor agonists etc…
• Behavioral/lifestyle • Exercise, counselling etc…
When to intervene ? • Pre-conception, pregnancy, lactation, early infancy/childhood
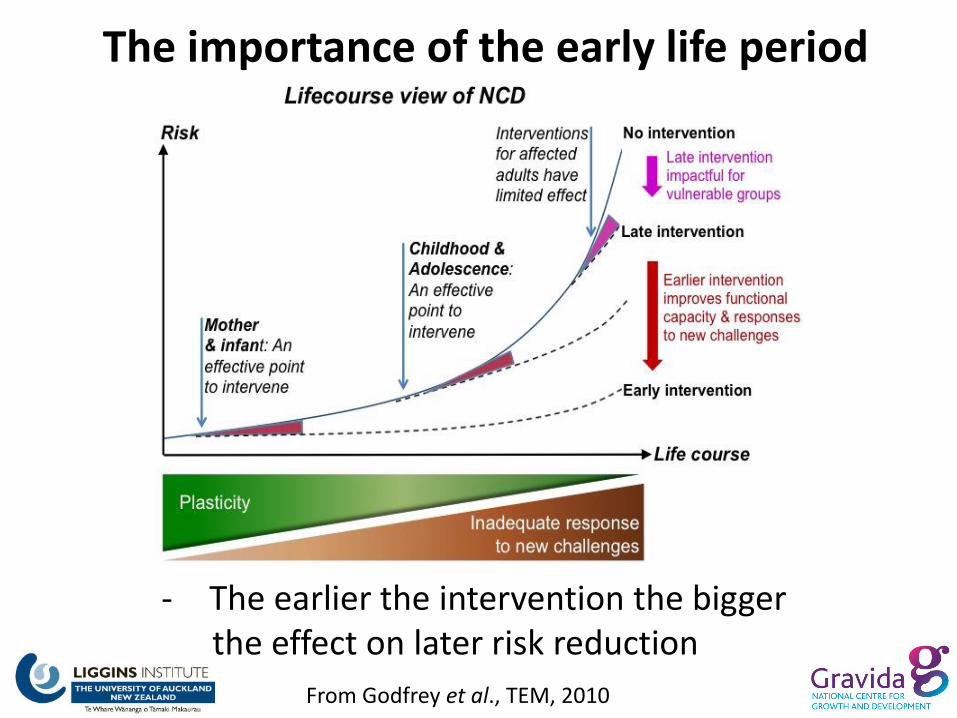
From Godfrey et al., TEM, 2010
- The earlier the intervention the bigger the effect on later risk reduction
The importance of the early life period
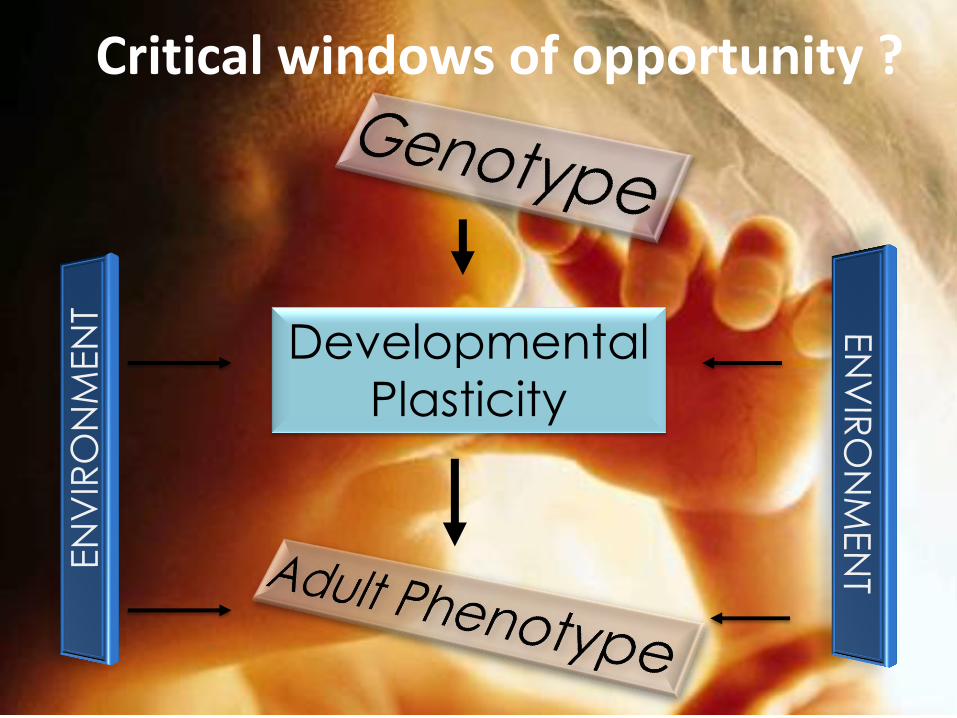
Developmental
Plasticity
Critical windows of opportunity ?
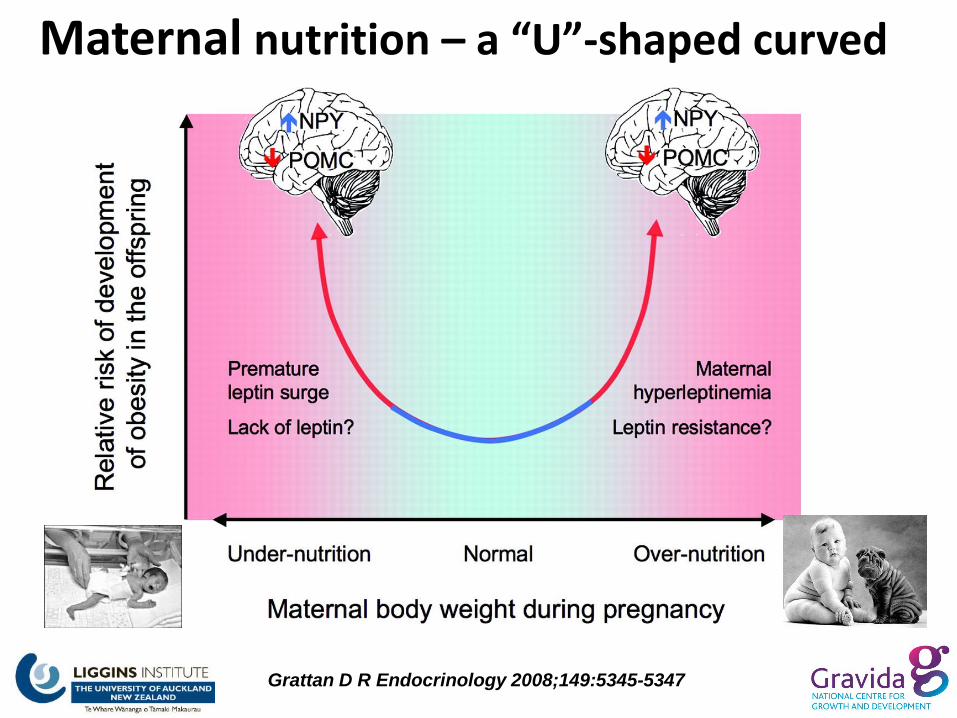
Maternal nutrition – a “U”-shaped curved
Grattan D R Endocrinology 2008;149:5345-5347

Interventions in programming: Evidence from pre-clinical models
Control
Supplements e.g. Folic acid
Low protein
High fat
Undernutrition High salt
Pre-clinical models of early life nutritional manipulation
High sugar
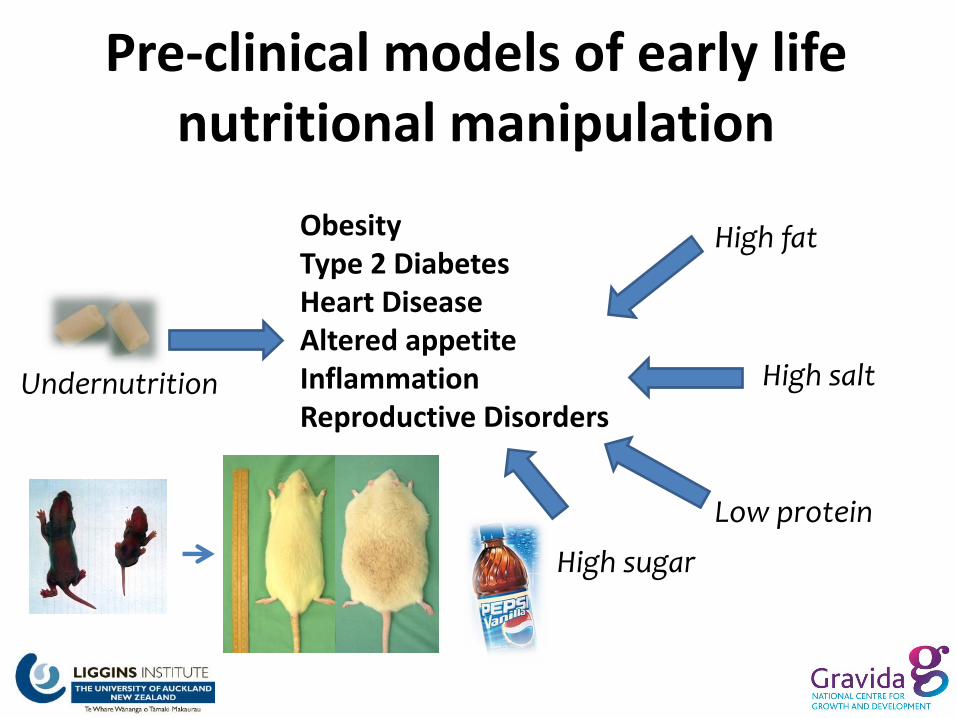
Pre-clinical models of early life nutritional manipulation
Low protein
High fat
Undernutrition
High sugar
High salt
Obesity Type 2 Diabetes Heart Disease Altered appetite Inflammation Reproductive Disorders
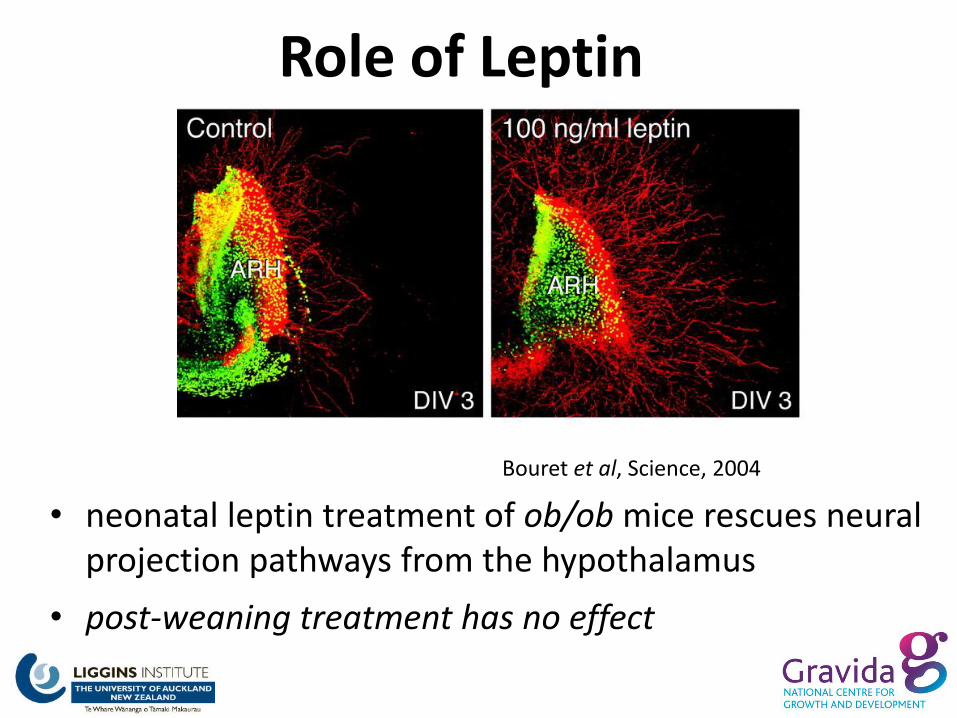
Role of Leptin
• neonatal leptin treatment of ob/ob mice rescues neural projection pathways from the hypothalamus
• post-weaning treatment has no effect
Bouret et al, Science, 2004

Control Saline Control Leptin UN Leptin
UN Saline
Leptin as an intervention ?
• The effects appeared permanent and were specific to offspring of maternally undernourished offspring
- has been repeated in numerous other models/species including effects on hypothalamic neuropeptides
- of note, leptin is present in breast milk but is not in infant formula
- we know that the effects of neonatal leptin treatment are dependent upon prior maternal nutritional status and gender
- leptin treatment to male neonates of normal pregnancies can elicit an adverse metabolic phenotype in later life
Vickers et al, 2005, 2008 Endocrinology, Gluckman et al, 2007, PNAS
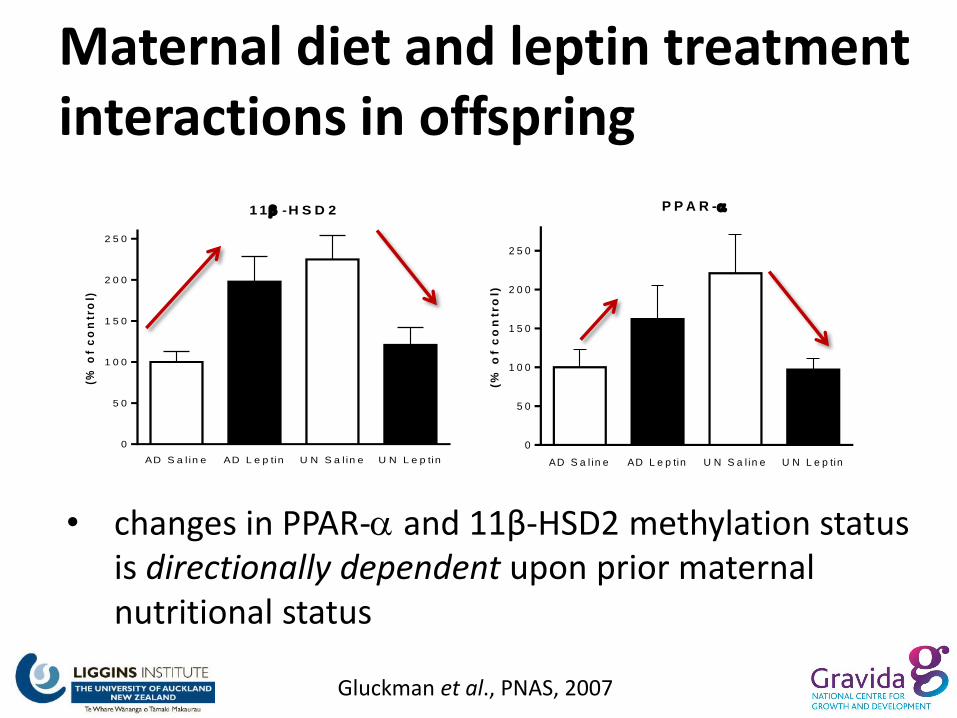
Maternal diet and leptin treatment interactions in offspring
• changes in PPAR- and 11β-HSD2 methylation status is directionally dependent upon prior maternal nutritional status
Gluckman et al., PNAS, 2007
P P A R -
AD S a l in e AD L e p tin U N S a l in e U N L e p tin
0
5 0
1 0 0
1 5 0
2 0 0
2 5 0
(% o
f c
on
tro
l)
1 1 -H S D 2
AD S a l in e AD L e p tin U N S a l in e U N L e p tin
0
5 0
1 0 0
1 5 0
2 0 0
2 5 0
(% o
f c
on
tro
l)
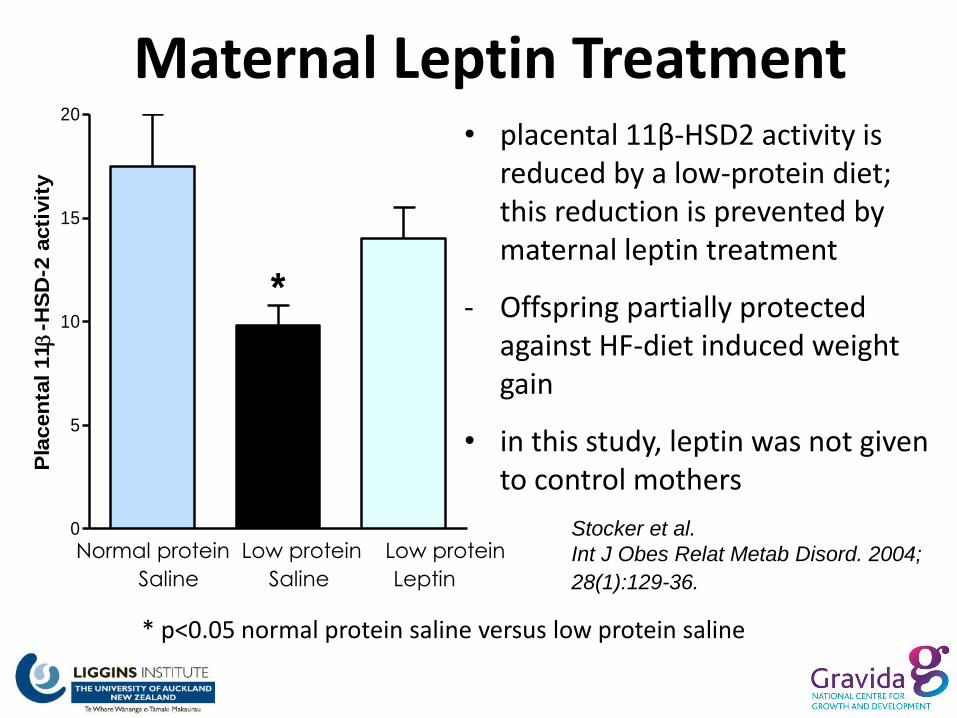
Maternal Leptin Treatment
0
5
10
15
20
*
Pla
cen
tal 11
-HS
D-2
acti
vit
y
Stocker et al.
Int J Obes Relat Metab Disord. 2004;
28(1):129-36.
* p<0.05 normal protein saline versus low protein saline
Normal protein Low protein Low protein
Saline Saline Leptin
• placental 11β-HSD2 activity is reduced by a low-protein diet; this reduction is prevented by maternal leptin treatment
- Offspring partially protected against HF-diet induced weight gain
• in this study, leptin was not given to control mothers

C o n t ro l V E H C o n t ro l E X-4 IU G R V E H IU G R E X-4
0 .0
2 .5
5 .0
7 .5
1 0 .0
1 2 .5
p < 0 .0 0 6 p < 0 .0 0 1 7
be
ta-c
ell
ma
ss
(m
g)
B e ta -c e ll m a s s
• Exendin 4 (GLP-1 analog) • normalisation of -cell mass and proliferation • reverses epigenetic modifications to pancreatic and
duodenal homeobox 1 (Pdx1)
Stoffers et al, Diabetes, 52: 737
Neonatal Exendin 4
Is le t P D X -1 p ro m o te r m e th y la t io n
me
thy
lati
on
(%
)
C o n tr o l V EH C o n tr o l EX -4 IU GR V EH IU GR EX -4
0
2 5
5 0
7 5
1 0 0
*
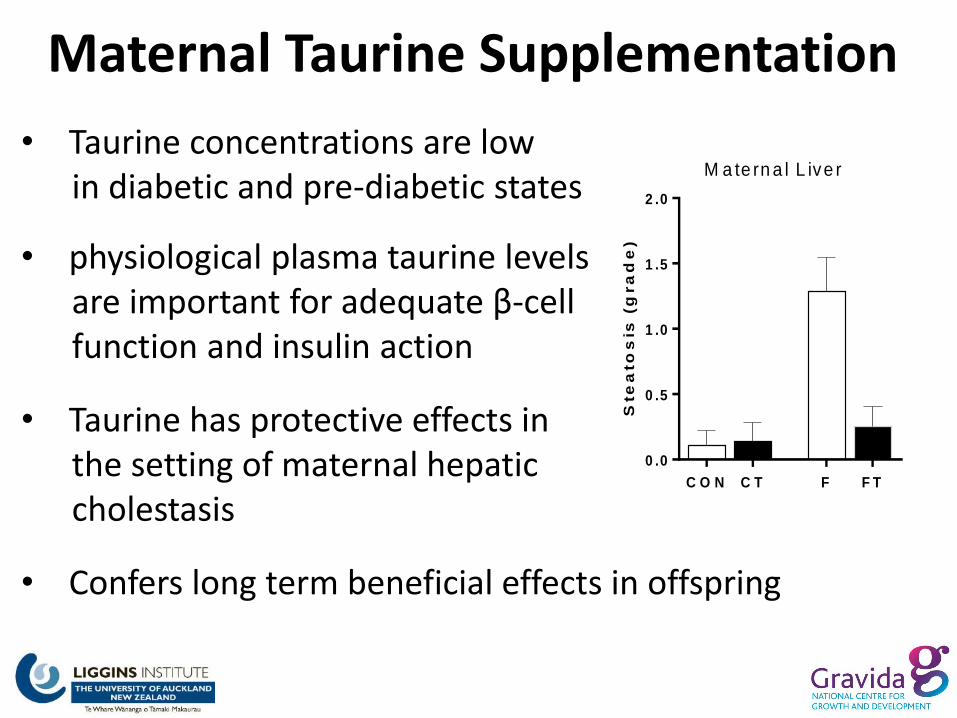
• Taurine concentrations are low in diabetic and pre-diabetic states
• physiological plasma taurine levels are important for adequate β-cell function and insulin action
• Taurine has protective effects in the setting of maternal hepatic cholestasis
• Confers long term beneficial effects in offspring
Maternal Taurine Supplementation
Ste
ato
sis
(g
ra
de
)
C O N C T F F T
0 .0
0 .5
1 .0
1 .5
2 .0
M a te rn a l L ive r

Maternal Taurine Supplementation
• fructose supplemented mothers are hyperinsulinemic compared to control mothers with increases in inflammatory markers
• these effects are normalised with maternal taurine supplementation
M a te rn a l P la s m a In s u lin
C o n t C o n t - T a u Fr F r - T a u
0 .0
0 .5
1 .0
1 .5
2 .0
2 .5
3 .0
*
Ins
uli
n (
ng
/ml)
Fructose-fed mothers
M a te rn a l P la s m a IL -1 B
C o n tr o l C o n tr o l + Ta u r in e F R F R + Ta u r in e
0
1 0
2 0
3 0
4 0
5 0
6 0
*
pg
/ml
Vickers, Li et al (J. Nutr. Biochem. 2014)
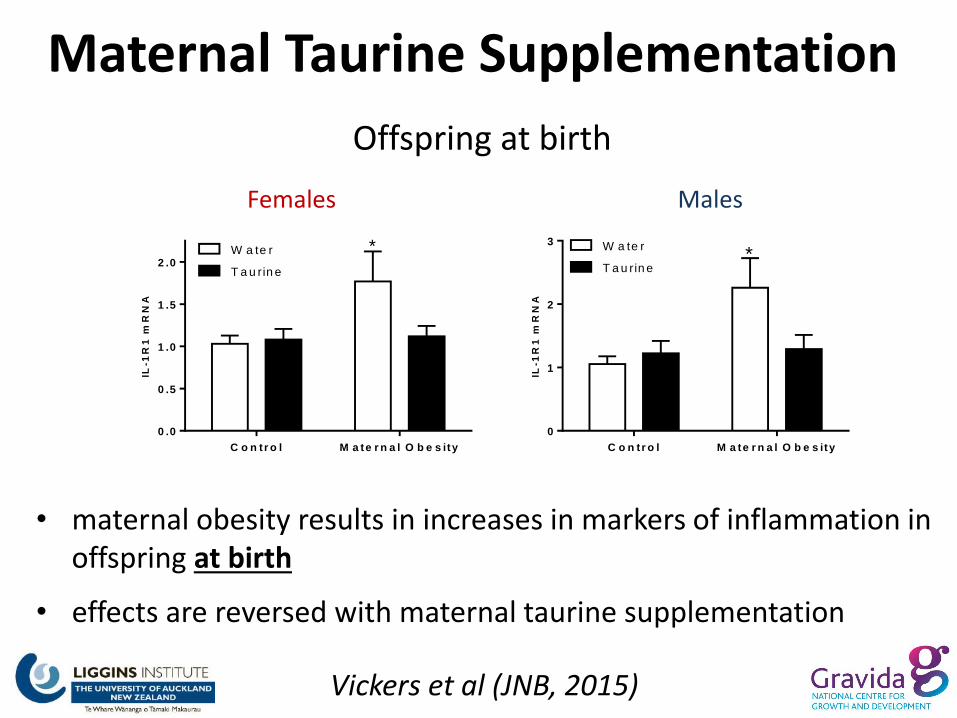
Vickers et al (JNB, 2015)
• maternal obesity results in increases in markers of inflammation in offspring at birth
• effects are reversed with maternal taurine supplementation
C o n tr o l M a te r n a l O b e s ity
0 .0
0 .5
1 .0
1 .5
2 .0W a te r
T a u rin e
*
IL-1
R1
mR
NA
C o n tr o l M a te r n a l O b e s ity
0
1
2
3 W a te r
T a u rin e*
IL-1
R1
mR
NA
Offspring at birth
Females Males
Maternal Taurine Supplementation
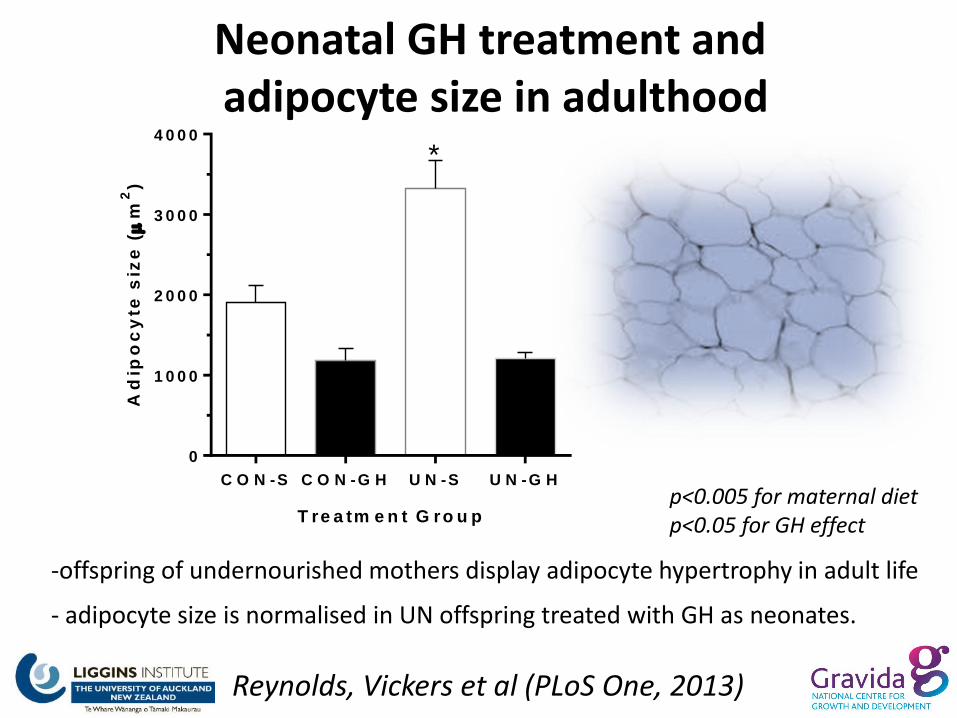
Neonatal GH treatment and adipocyte size in adulthood
-offspring of undernourished mothers display adipocyte hypertrophy in adult life
- adipocyte size is normalised in UN offspring treated with GH as neonates.
T re a tm e n t G ro u p
Ad
ipo
cy
te s
ize
(
m2
)
C O N -S C O N -G H U N -S U N -G H
0
1 0 0 0
2 0 0 0
3 0 0 0
4 0 0 0
*
p<0.005 for maternal diet p<0.05 for GH effect
Reynolds, Vickers et al (PLoS One, 2013)
S y s to lic B P
C o n t C o n t + G H U N U N + G H
1 0 0
1 1 0
1 2 0
1 3 0
1 4 0
1 5 0 *
mm
Hg
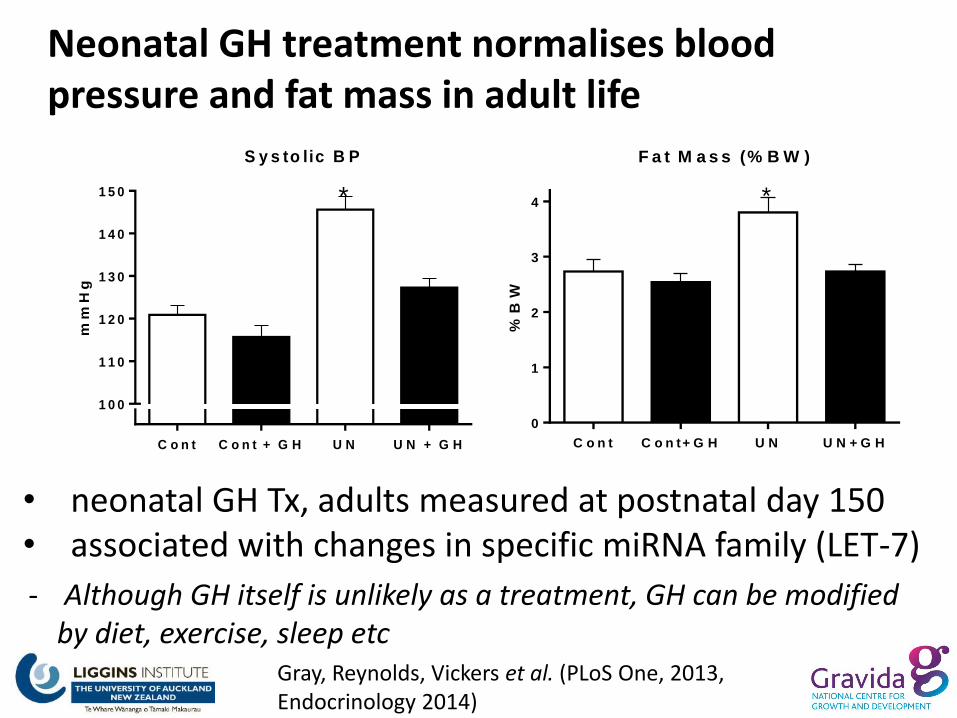
Gray, Reynolds, Vickers et al. (PLoS One, 2013, Endocrinology 2014)
Neonatal GH treatment normalises blood pressure and fat mass in adult life
• neonatal GH Tx, adults measured at postnatal day 150 • associated with changes in specific miRNA family (LET-7)
F a t M a s s (% B W )
%B
W
C o n t C o n t+ G H U N U N + G H
0
1
2
3
4 *
- Although GH itself is unlikely as a treatment, GH can be modified by diet, exercise, sleep etc
0 .0
0 .1
0 .2
0 .3
HO
MA
IR
We
an
lin
g M
ale
*
C O N C L A H F H F C L A
H F : N S
C L A : P < 0 .0 1
In te ra c t io n : p < 0 .0 5
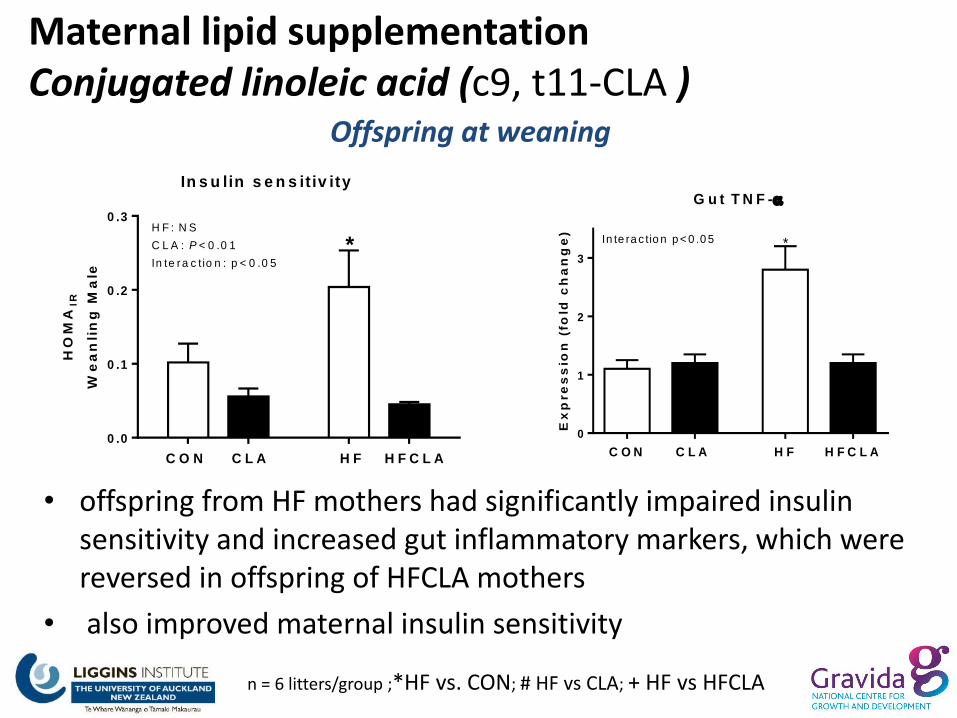
In s u lin s e n s it iv ity
n = 6 litters/group ;*HF vs. CON; # HF vs CLA; + HF vs HFCLA
• offspring from HF mothers had significantly impaired insulin sensitivity and increased gut inflammatory markers, which were reversed in offspring of HFCLA mothers
• also improved maternal insulin sensitivity
Offspring at weaning
G u t T N F -
Ex
pre
ss
ion
(fo
ld c
ha
ng
e)
C O N C L A H F H F C L A
0
1
2
3
*In te ra c tio n p < 0 .0 5
Maternal lipid supplementation Conjugated linoleic acid (c9, t11-CLA )
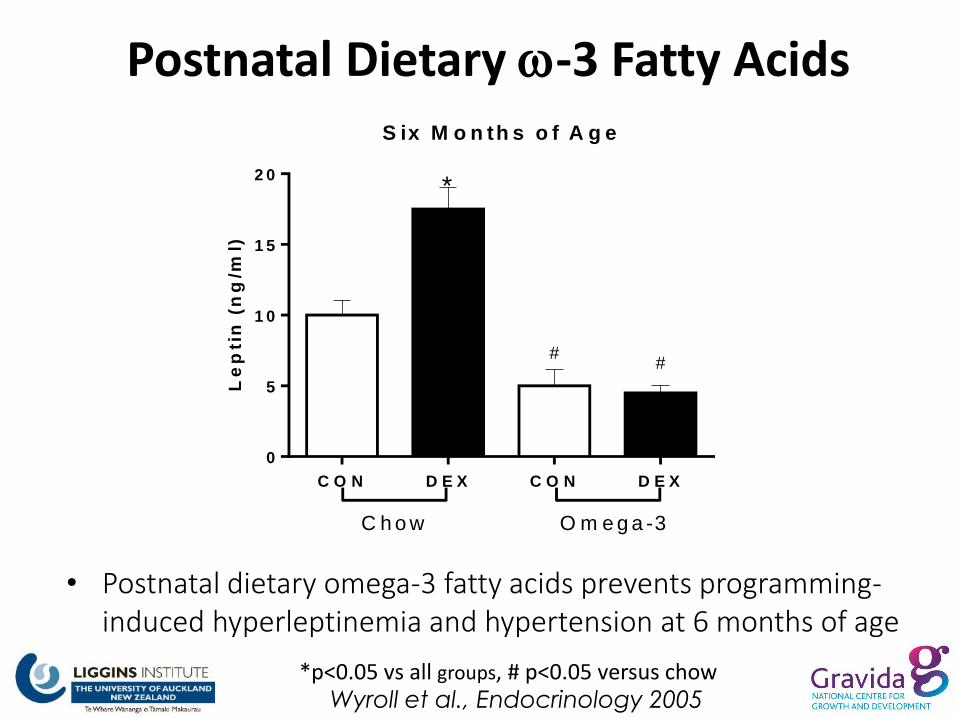
• Postnatal dietary omega-3 fatty acids prevents programming-induced hyperleptinemia and hypertension at 6 months of age
Wyroll et al., Endocrinology 2005
Postnatal Dietary -3 Fatty Acids S ix M o n th s o f A g e
Le
pti
n (
ng
/ml)
C O N D E X C O N D E X
0
5
1 0
1 5
2 0
C h o w O m e g a -3
*
##
*p<0.05 vs all groups, # p<0.05 versus chow
Maternal Vitamin D status
- role in controlling placental inflammation and insulin sensitivity
- pre-pregnancy obesity predicts poor vitamin D status in mothers and their neonates
- Vitamin D deficiency in pregnancy can result in insulin resistance, altered inflammatory profiles and increased risk of early postnatal obesity in offspring1,2
- impact of supplements on outcomes related to adiposity are conflicting
(1Morales E, Int J. Obesity, 2015, 2Zhang H, Diabetologia, 2014)
Folic acid1
Glycine2
Choline3
Mixed supplements4
Maternal supplementation improves metabolic and cardiovascular outcomes in offspring following both undernutrition and maternal obesity
1. Torrens et al., (2006) 2. Jackson et al., (2002) 3. Vickers et al., (2012) 3. Carlin et al., (2013)
Dietary methyl donors
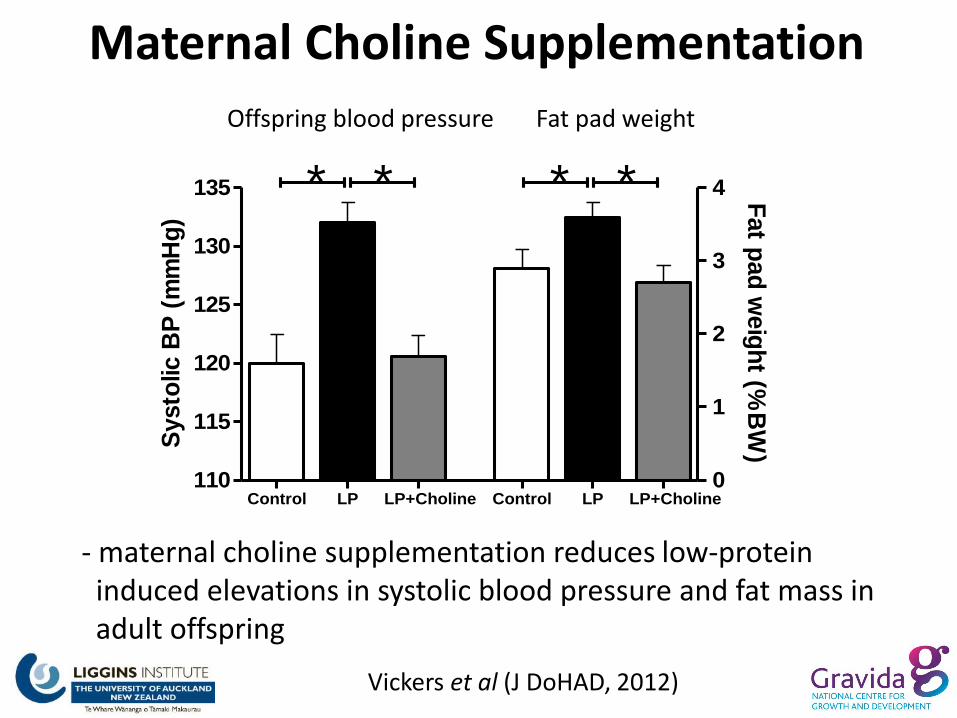
Maternal Choline Supplementation
- maternal choline supplementation reduces low-protein induced elevations in systolic blood pressure and fat mass in adult offspring
Control LP LP+Choline Control LP LP+Choline110
115
120
125
130
135
0
1
2
3
4****S
ysto
lic B
P (
mm
Hg
)
Fat p
ad
weig
ht (%
BW
)
Offspring blood pressure Fat pad weight
Vickers et al (J DoHAD, 2012)
Exercise/Lifestyle Interventions • Physical activity has the potential to mitigate against the increased obesity observed in “programmed” offspring during two critical windows
- maternal exercise prior to and during pregnancy
- exercise during childhood for those at risk of “programmed” obesity
• Recent early feeding practices intervention study reported no change in prevalence of overweight/obesity
Siebel et al, Clin Exp Pharm. Physiol 2012, Daniels et al., Pediatrics, 2013

Exercise as an intervention
1Miles JL, Endocrinology 2008, 2Santos M, Am J Phys. 2015 3Sun B, Am J Physiol. 2013, 4Hopkins S, JCEM, 2010
• Early exercise can reduce adiposity in experimental models of both maternal undernutrition and maternal obesity1,2
• Effects mediated in part by improved central leptin sensitivity3
• Dependent on type and duration - moderate exercise in normal pregnancy can lead to a significant decrease in birth weight4
Control non-exercised Control exercised UN non-exercised UN exercised
Age (days)
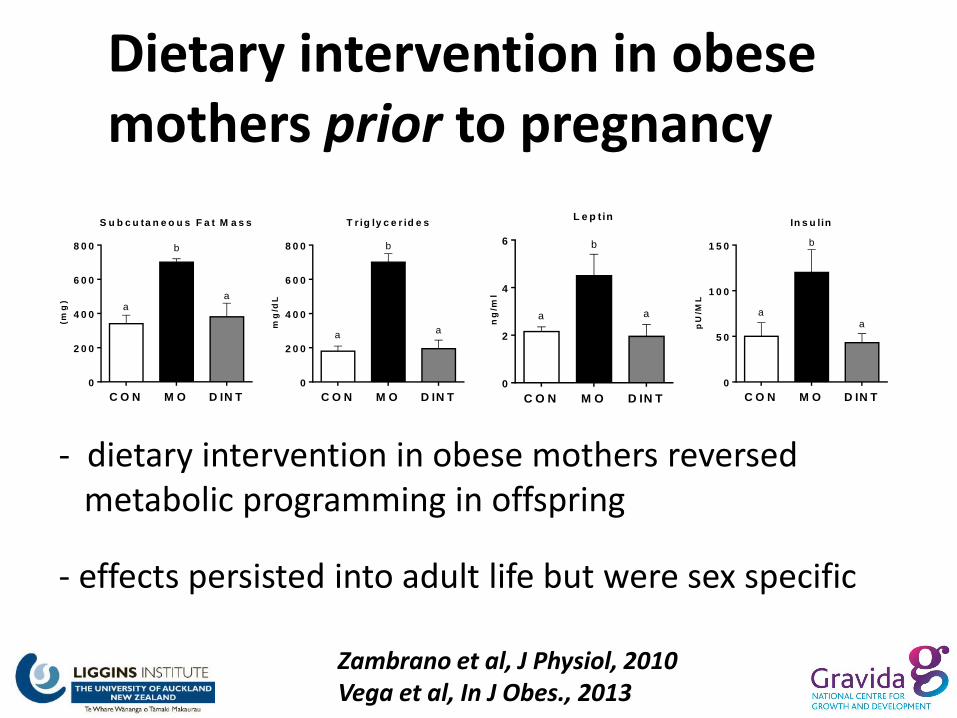
Dietary intervention in obese mothers prior to pregnancy
Zambrano et al, J Physiol, 2010 Vega et al, In J Obes., 2013
- dietary intervention in obese mothers reversed metabolic programming in offspring
- effects persisted into adult life but were sex specific
S u b c u ta n e o u s F a t M a s s
(mg
)
C O N M O D IN T
0
2 0 0
4 0 0
6 0 0
8 0 0
aa
b
T r ig ly c e r id e s
mg
/dL
C O N M O D IN T
0
2 0 0
4 0 0
6 0 0
8 0 0
aa
b
L e p t in
ng
/ml
C O N M O D IN T
0
2
4
6
aa
b
In s u lin
pU
/ML
C O N M O D IN T
0
5 0
1 0 0
1 5 0
aa
b
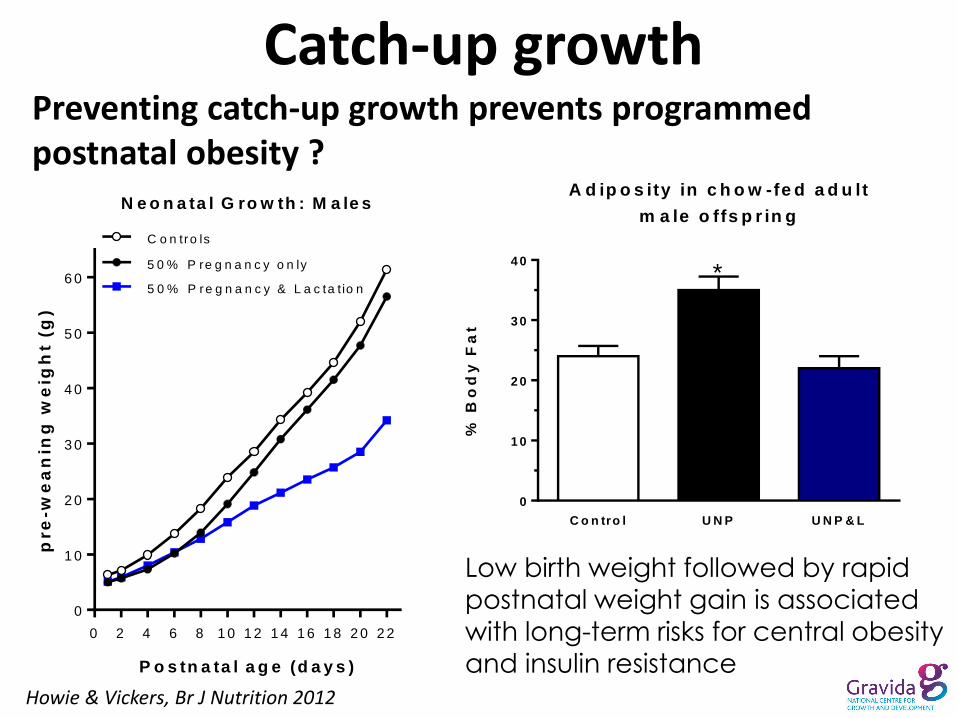
Preventing catch-up growth prevents programmed postnatal obesity ?
A d ip o s ity in c h o w -fe d a d u lt
m a le o ffs p r in g
C o n tro l U N P U N P & L
0
1 0
2 0
3 0
4 0
% B
od
y F
at
*
Howie & Vickers, Br J Nutrition 2012
Catch-up growth
Low birth weight followed by rapid
postnatal weight gain is associated with long-term risks for central obesity
and insulin resistance
N e o n a ta l G ro w th : M a le s
0 2 4 6 8 1 0 1 2 1 4 1 6 1 8 2 0 2 2
0
1 0
2 0
3 0
4 0
5 0
6 0
C o n tro ls
5 0 % P re g n a n c y o n ly
5 0 % P re g n a n c y & L a c ta t io n
P o s tn a ta l a g e (d a y s )
pre
-we
an
ing
we
igh
t (g
)

Maternal Obesity and Omega-3/DHA • as an anti-inflammatory - obesity and pregnancy are low-grade inflammatory states that increase the risk of fetal adiposity in the short term and metabolic syndrome in the long term
• maternal-fetal PUFA status is associated with lower infant adiposity - offspring born to mothers with recommended quantity of DHA during pregnancy are 30% less likely to have excessive body fat
• DHA supplementation in women with overweight/obesity results in infants with lower adiposity at birth (Donahue, 2011)
• DHA supplements in last half of pregnancy led to greater gestation length and increased infant size (Carlson et al, Am J Clin Nutr. 2013)
• differences across reported studies may simply relate to doses, sources and potential oxidation of n-3 PUFAs
Pre-/Probiotics - administration of certain probiotics and/or prebiotics during the perinatal and postnatal period may be a potential prophylactic therapy for obesity and metabolic disease - early gut microbiota modulation with probiotics may modify the growth pattern of the child by restraining excessive weight gain during the first years of life - supplementation of infant formula with prebiotic oligosaccharides to compensate for the lack of some of the complex molecules naturally present in human milk?
Thum et al., J Nutr., 2012, 142(11) Luoto et al., Int J. Obesity, 2010, 34(10)

• potential that interventions in setting of “intact” systems may lead to adverse outcomes
• how best to identify those “at risk” of programmed disorders ? – tailored approach, metabolic markers
• sex-specific effects e.g. maternal methyl-deficient diets can result in metabolic disturbances in male, but not female, rat offspring
Who and when to target for intervention ? • Predictive biomarkers –
• Importance of large biobanks • E.g. cord blood methylation of RXR-α and later childhood adiposity • Predominantly associative
• Biomarkers in populations often have a wide range and within this range, individuals can behave quite differently
• What are the trade-offs ? i.e. epimutations that are likely associated with later negative health outcomes
e.g. maternal methyl donor supplementation can lead to a reduction in fatty liver but increased adipose tissue storage in offspring when later exposed to a HF diet
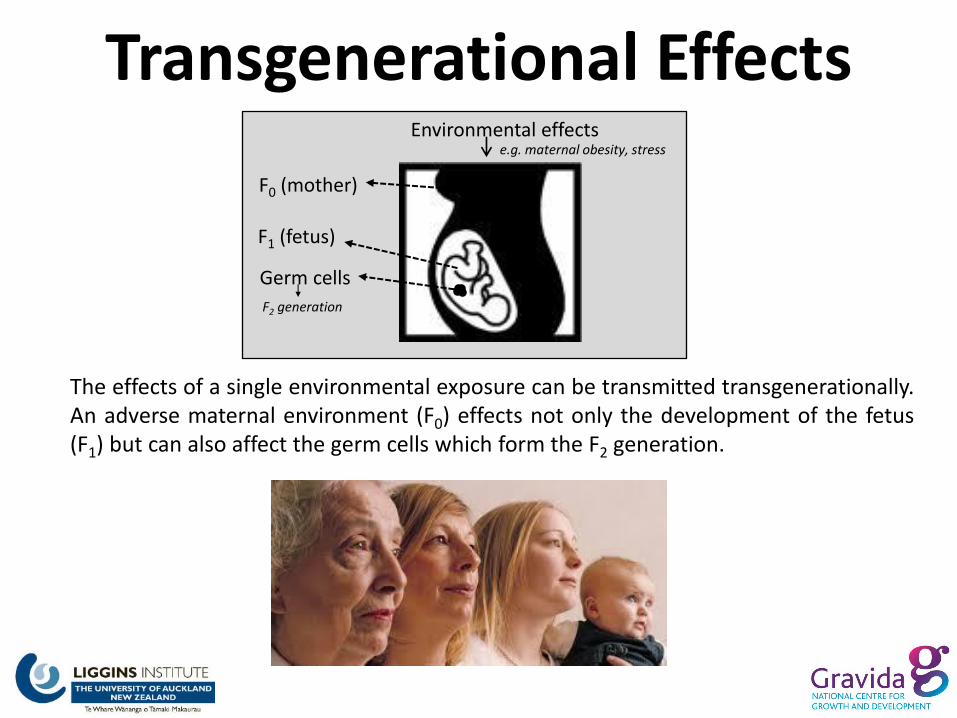
Transgenerational Effects
F0 (mother)
F1 (fetus)
Germ cells
F2 generation
Environmental effects e.g. maternal obesity, stress
The effects of a single environmental exposure can be transmitted transgenerationally. An adverse maternal environment (F0) effects not only the development of the fetus (F1) but can also affect the germ cells which form the F2 generation.
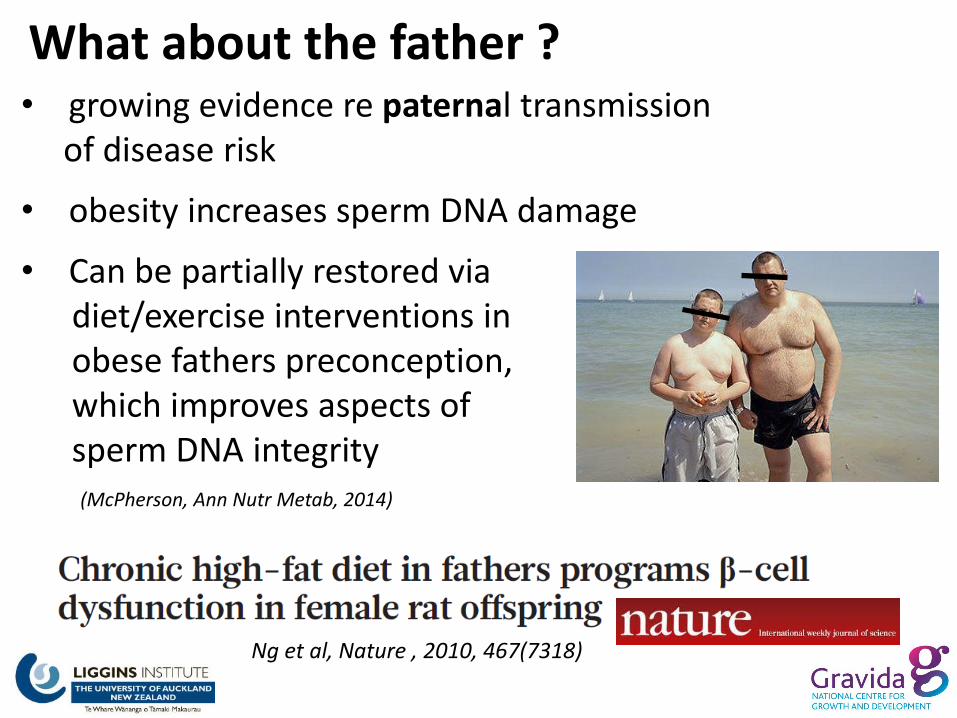
What about the father ? • growing evidence re paternal transmission of disease risk
• obesity increases sperm DNA damage
• Can be partially restored via diet/exercise interventions in obese fathers preconception, which improves aspects of sperm DNA integrity (McPherson, Ann Nutr Metab, 2014)
Ng et al, Nature , 2010, 467(7318)
Discussion - the early life period of developmental plasticity offers the
most effective avenue for intervention
- although reversal has been shown in a number of experimental models (maternal and neonatal), direct translation to the clinic may prove difficult but will inform on possible intervention strategies

Acknowledgements Deborah Sloboda Peter Gluckman Bernhard Breier Clare Reynolds Clint Gray Minglan Li Angelica Bernal Rachna Patel Claudia Harrison
Kelliher Trust
Friends of the Liggins Trust
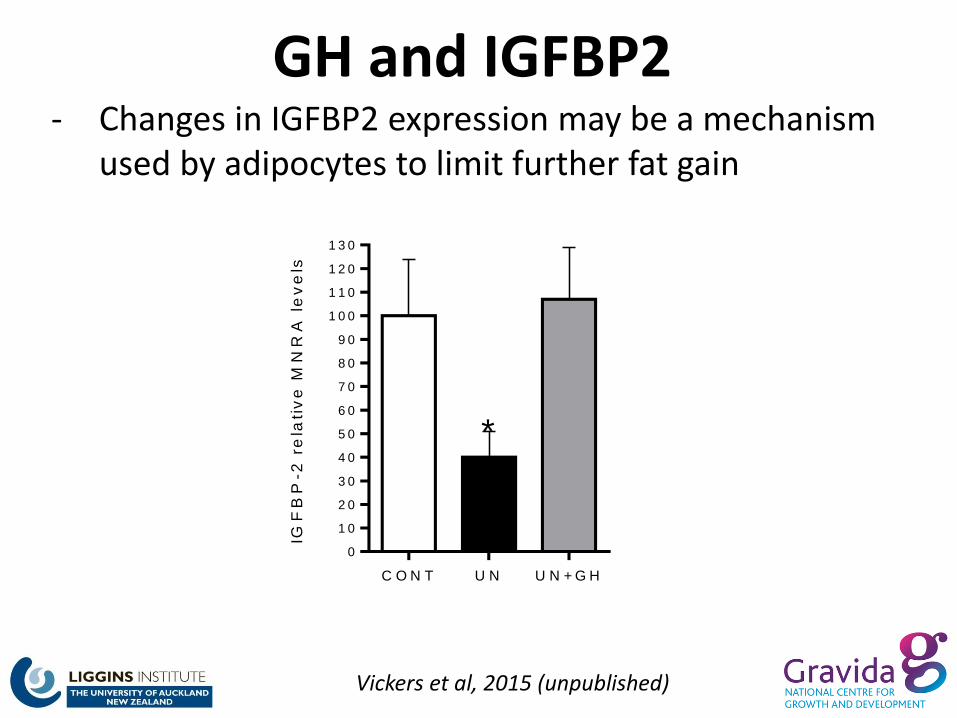
GH and IGFBP2
C O N T U N U N + G H
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
1 1 0
1 2 0
1 3 0
IGF
BP
-2 r
ela
tiv
e M
NR
A l
ev
els
*
Vickers et al, 2015 (unpublished)
- Changes in IGFBP2 expression may be a mechanism used by adipocytes to limit further fat gain
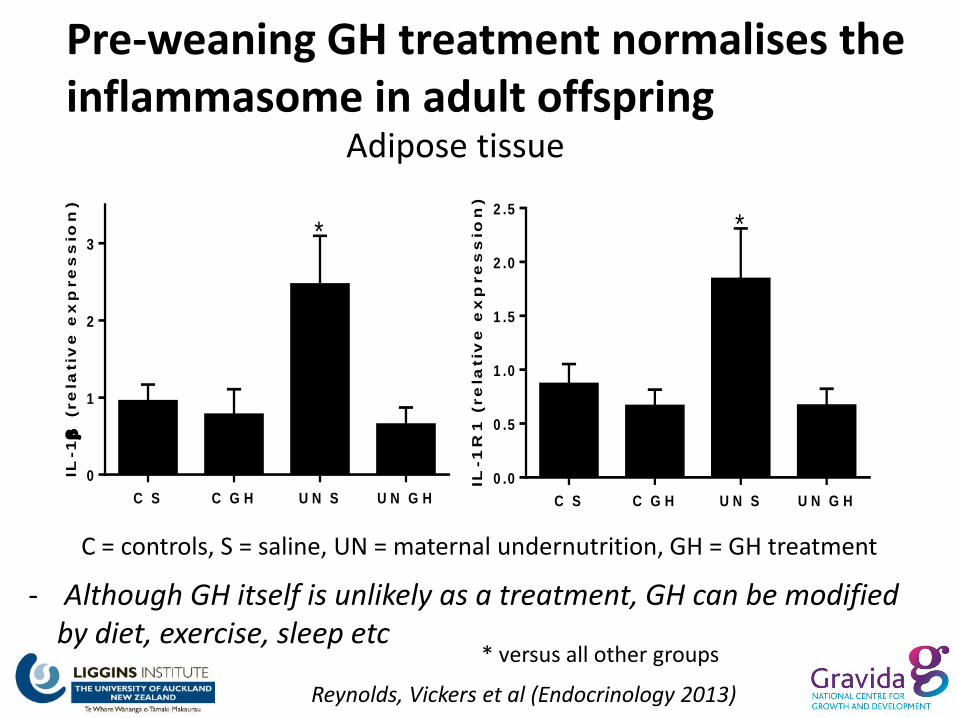
Pre-weaning GH treatment normalises the inflammasome in adult offspring
C S C G H U N S U N G H
0
1
2
3*
IL-1
(re
lativ
e e
xp
re
ss
ion
)
Adipose tissue
C S C G H U N S U N G H
0 .0
0 .5
1 .0
1 .5
2 .0
2 .5
*
IL-1
R1
(re
lativ
e e
xp
re
ss
ion
)
C = controls, S = saline, UN = maternal undernutrition, GH = GH treatment
Reynolds, Vickers et al (Endocrinology 2013)
* versus all other groups
- Although GH itself is unlikely as a treatment, GH can be modified by diet, exercise, sleep etc
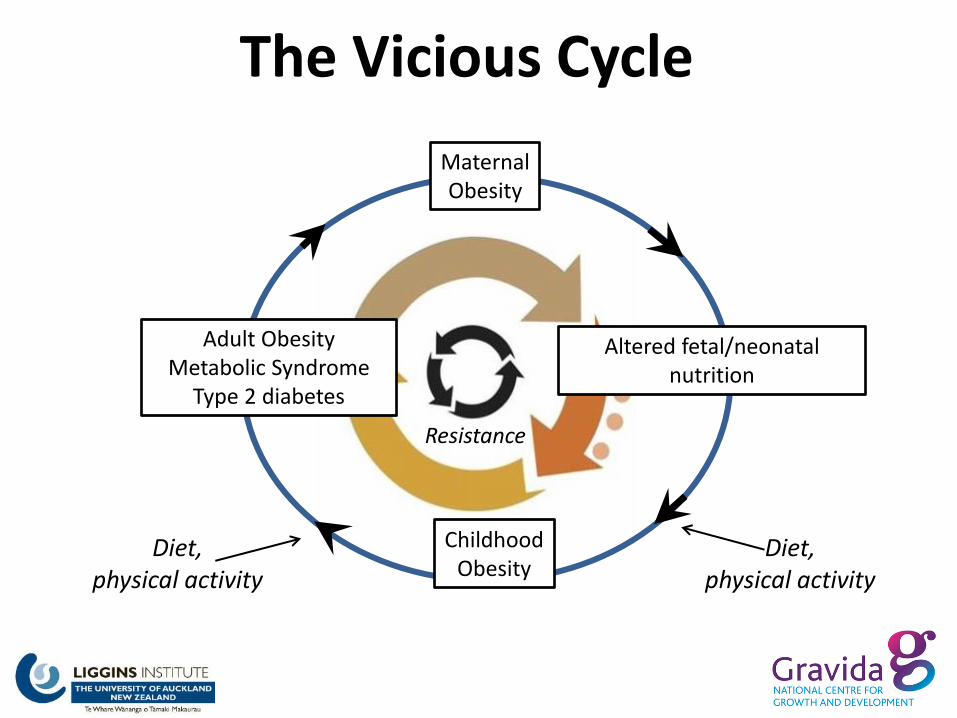
Maternal Obesity
Altered fetal/neonatal nutrition
Childhood Obesity
Adult Obesity Metabolic Syndrome
Type 2 diabetes
Diet, physical activity
Diet, physical activity
The Vicious Cycle
Resistance
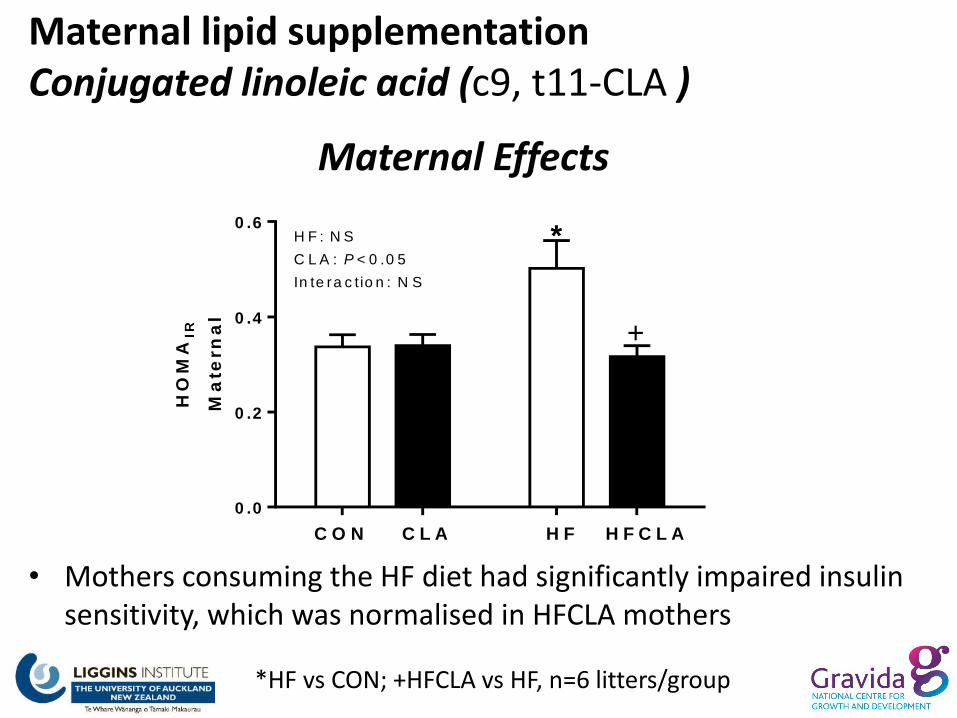
Maternal Effects
0 .0
0 .2
0 .4
0 .6
HO
MA
IR
Ma
tern
al
+
*H F : N S
C L A : P < 0 .0 5
In te ra c t io n : N S
C O N C L A H F H F C L A
• Mothers consuming the HF diet had significantly impaired insulin sensitivity, which was normalised in HFCLA mothers
*HF vs CON; +HFCLA vs HF, n=6 litters/group
Maternal lipid supplementation Conjugated linoleic acid (c9, t11-CLA )
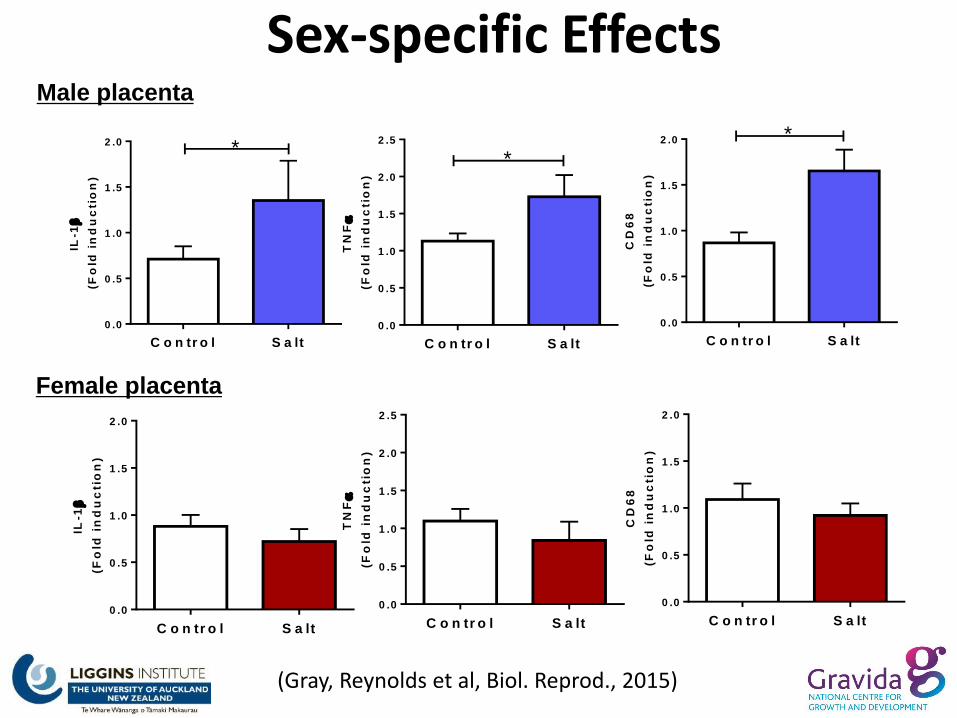
Sex-specific Effects Male placenta
Female placenta
IL-1
(Fo
ld i
nd
uc
tio
n)
C o n tr o l S a lt
0 .0
0 .5
1 .0
1 .5
2 .0 *
IL-1
(Fo
ld i
nd
uc
tio
n)
C o n tr o l S a lt
0 .0
0 .5
1 .0
1 .5
2 .0
TN
F
(Fo
ld i
nd
uc
tio
n)
C o n tr o l S a lt
0 .0
0 .5
1 .0
1 .5
2 .0
2 .5
*
TN
F
(Fo
ld i
nd
uc
tio
n)
C o n tr o l S a lt
0 .0
0 .5
1 .0
1 .5
2 .0
2 .5
CD
68
(Fo
ld i
nd
uc
tio
n)
C o n tr o l S a lt
0 .0
0 .5
1 .0
1 .5
2 .0 *
CD
68
(Fo
ld i
nd
uc
tio
n)
C o n tr o l S a lt
0 .0
0 .5
1 .0
1 .5
2 .0
(Gray, Reynolds et al, Biol. Reprod., 2015)