Ensuring Ensuring Competence Competence in Endoscopy in Endoscopy

Abstracts
group, although in no subjects was the manometry catheter gripped strongly. Insome cases the manometry catheter was gripped weakly, and in some casesincomplete peristalsis left a small but definite lumen . Peristalsis was not induced insome cases. The mean recorded peristaltic pressure was 28.0 � 25.6 mmHg. Therewas significant difference in mean pressure between volunteer and PPI-dependentGERD. Achalasia group: Endoscopically the absence of primary peristalsis wasrecognized induced by swallowing in all cases. Manometry also revealed absence ofcontractive waveform induced by swallowing. Conclusions: The use of TN-EGDmakes possible simultaneous manometry and endoscopic observation of theesophagus. This combination should prove useful in the screening evaluation ofesophageal peristaltic function
W1446
Development of Endoluminal Technique for Detection of
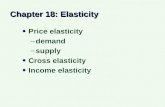
Elasticity in Gastrointestinal Tract During EndoscopyPhilip W. Chiu, Yongping Zheng, Yanping Huang, K. Ng Enders, Ka FaiTo, S.K. Kong, Aaron H. HoIntroduction: Current detection of early GI neoplasia relied on observation ofsubtle mucosal changes through endoscopy. Reports showed that the presence ofneoplasia will change the elasticity of GI lumen. We aimed to develop a novel deviceto measure tissue elasticity of gastrointestinal tract during endoscopic examination.MethodThis is an ex-vivo experiment to compare change in elasticity of gastric wallwith or without cancer. We obtained specimens from patients who underwentstandard D2 gastrectomy for carcinoma of stomach. These were tested for elasticityusing an indentation system. It consisted of two parts: one is to drive the indenterto load and unload the specimens, and the other is a sensor for collection ofchanges in elasticity. In the preliminary test, 3 cycles of loading and unloading witha range of 2 mm were induced. A pre-load force of about 0.1 N and a loading rangeof 0.7 mm were used for calculating the stiffness parameter. The stiffness parameterwas defined as regression of compression force to the tissue deformation in unit ofN/mm and only the loading stages were used due to tissue viscosity. Three testswere performed on the specimen and the average value was used as an indicator ofthe tissue properties. Results: The change between the force applied and thedetection of deformity of the gastrectomy specimen was shown in Figure 1. There isa significant difference in the deformity between cancerous and non-cancerousspecimens. The calculated stiffness of the specimen was t 1.34 � 0.17 for thecancerous part and 0.35 � 0.26 N/mm for the non-cancerous part. Conclusion: Theelasticity of the gastrointestinal lumen can be measured using an ex-vivoindentation system, and there is a significant difference in the stiffness measuredbetween cancerous and non-cancerous lesions. We will miniaturize the indentationsystem into a through-the-scope catheter so that in-vivo measurement ofgastrointestinal elasticity can be performed.
Relationship of force to deformity detected between normal gastric mucosa andgastric cancer
W1447
Multicenter Study of Interobserver Agreement in Describing
Capsule Endoscopy FindingsAlessandro Pezzoli, Renato Cannizzaro, Marco Pennazio,Emanuele Rondonotti, Ettore Bidoli, Laura Zancanella, Franco Cantoni,Giancarlo Caravelli, Raffaele Melina, Gaetano Iaquinto, Angela Alberani,Fausto Chilovi, Tino Casetti, Sergio GulliniBackground and Aim: Few studies have specifically addressed the interobserveragreement in describing the lesions identified during CE. The aim of our study is to
AB372 GASTROINTESTINAL ENDOSCOPY Volume 69, No. 5 : 2009
evaluate interobserver agreement in identification and interpretation CE findings.Materials and Methods: The study was a multicentre study. A group of 8 exspertendoscopists (more than 50 CE videos read) participated in the study. We choose tovisualise a short segment (20 seconds) of CE. An external author, non participant inthe reading of the tapes, prepared the cases to view that were recorded on DVD.This author was the only one to know the final diagnosis of such patients and he isconsidered as the ‘‘gold standard’’. The videos contained different lesions in 80% ofthe cases and the remaining 20% were negative. In order to obtain uniformity inacquisition, interpretation and reporting the results of CE examinations all readersused a validated standard terminology (CEST). Each endoscopist reported thepresence of any lesions in the segment observed and, if positive, described the size,colour, shape and the final diagnosis of the finding using the standardisedterminology. Interobserver agreement was assessed using kappa statistics,a measure of agreement that can be applied to different diagnostic categories.Results: Agreement for the ability to identify lesions showed moderate agreement(kappa 0.55, range between 0.39 to 0.92). The kappa for the presence of activebleeding was 0.58 (range between 0.34 to 0.98). For the shape of the lesionsagreement was moderate (k 0.50, range between 0.41 to 0.74). The colour of thelesion identified showed the same level of agreement (k 0.53, range between 0.47to 0.76). The size of the lesions was the category with worst agreement, with a kvalue of 0.37 (range from 0.24 to 0.58). Finally agreement for the diagnosis wassimilar to the other categories with a k level of 0.47 (range from 0.43 to 0.66).Conclusions: In the current study we found a moderate level of agreement forreading CE and this level is similar for the majority of the considered categories.This is the first CE agreement study in wich a enougth number of lesions forstatistical analysis was reviewed and all authors used CEST terminology forreporting CE findings.
W1448
Narrow Band Imaging to Detect and Differentiate Residual or
Recurrent Neoplastic Tissue During Real-Time EndoscopyJason N. Rogart, Harry R. Aslanian, Uzma D. SiddiquiBackground: There is little data on the prevalence of residual neoplastic tissue orthe rate of endoscopically detected recurrence in patients with prior surgical orendoscopic resection of advanced neoplasia. Narrow band imaging (NBI) isa relatively new technology which may facilitate the identification andcharacterization of dysplastic mucosal lesions. Aims: To compare standard whitelight (WL) with NBI for the detection, as well as the differentiation, of residual orrecurrent neoplastic tissue during real-time endoscopy. Methods: Patientsundergoing colonoscopy or upper endoscopy for surveillance of endoscopically orsurgically resected malignant lesions or advanced adenomas were recruitedprospectively. Two endoscopists with NBI experience using NBI performed allprocedures using Olympus 180 series endoscopes. When the region of priorresection was identified, it was examined first with WL (1.5� magnification setting)and the number of distinct lesions was recorded, as was the histologic prediction(neoplastic or non-neoplastic). The area was then reexamined with NBI and thefollowing recorded: number of additional lesions, whether lesions seen with WLappeared more extensive, and histologic prediction of all lesions based on NBIappearance. Each lesion was then either removed or biopsied for histologicevaluation. Results: 36 patients were enrolled: 22 post-polypectomy (14 colon, 7duodenum, 1 esophagus) and 14 post-surgical resection (10 colon, 2 esophagus, 2gastric). 47 lesions were identified, 13 of which were only seen with NBI. 17 (50%)of the lesions identified with WL appeared more extensive on NBI evaluation. In 10(28%) patients, 14 neoplastic lesions were detected (2 carcinoma, 1 adenoma withHGD, 2 serrated adenoma, 9 tubular adenoma) and 3 of these (21%) were detectedonly with NBI. The mean number of lesions per patient identified with WLþNBIwas 1.31, compared with 0.94 for WL alone (P!0.05). Of the 33 non-neoplasticlesions, 11 showed normal histology, 13 reactive/inflammatory changes, 2hyperplastic, and 7 prominent Brunners glands or lymphoglandular complex.Diagnostic accuracy for predicting histology was not significantly different for NBIcompared with WL (84% vs. 88%, P Z 0.59), however the sensitivity for neoplasticlesions showed a trend toward being higher with NBI (86% vs. 71%, P Z 0.24).Conclusions: A substantial number of patients undergoing surveillance endoscopyhad residual or recurrent neoplastic tissue identified at the prior resection site. Theadjunctive use of NBI should be considered, as NBI detected additional neoplasticlesions and demonstrated that lesions detected with WL were more extensive.
W1449
Colonoscopy Force Monitor (CFM)�: New Tool for Teaching,
Performance Assessment and Quality AssuranceArmen Sarvazyan, Louis Y. Korman, Sergey Tsuryupa, Brendan Corbin,Noune SarvazyanColonoscopy requires an examiner to inspect the colonic mucosal surface byapplying push/pull forces and torque to a colonoscope to maneuver through thecolon. Skilled endoscopists reach the cecum quickly, minimize pain and have highrates of polyp detection. Training programs are designed to impart and assess theseskills. The CFM� was designed to be a cost-effective tool for quantifyingmanipulation technique, examining maneuvers, and improving skills by using real-
www.giejournal.org