Development and Applications of Varieties of Bioactive...
49
4 Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System Samit Kumar Nandi 1 , Biswanath Kundu 2 and Someswar Datta 2 1 Department of Veterinary Surgery and Radiology, West Bengal University of Animal and Fishery Sciences, Kolkata, 2 Bioceramics and Coating Division, Central Glass and Ceramic Research Institute, Kolkata, India 1. Introduction Bioactive glass is composed mainly of silica, sodium oxide, calcium oxide and phosphates. The bone-bonding reaction results from a series of reactions in the glass and its surface (Hench & Wilson, 1984). When granules of bioactive glass are inserted into bone defects, ions are released in body fluids and precipitate into a bone-like apatite on the surface, promoting the adhesion and proliferation of osteogenic cells (Ohtsuki et al., 1991; Neo et al., 1993) which is partially replaced by bone after long time implantation (Neo et al., 1994). The ion leaching phenomenon involves the exchange of monovalent cations from the glass, such as Na+ or K+, with H3O+ from the solution, and thus causes an increase in the pH of the solution. It is known that osteoblasts prefer a slightly alkaline medium (Ramp et al., 1994; Kaysinger & Ramp, 1998), but it is also known that severe changes in pH can inhibit osteoblast activity and cause cell necrosis or apoptosis (Brandao-burch et al., 2005; Frick et al., 1997; El-ghannam et al., 1997). Bioactive glass with a macroporous structure has the properties of large surface areas, which are favourable for bone integration. The behaviour of bioactive glass is dependent on the composition of the glass (Brink, 1997; Brink et al., 1997), the surrounding pH, the temperature, and the surface layers on the glass (Andersson et al., 1988; Gatti & Zaffe, 1991). The porosity provides a scaffold on which newly-formed bone can be deposited after vascular in growth and osteoblast differentiation. The porosity of bioglass is also beneficial for resorption and bioactivity (De Aza et al., 2003). In push-out tests the strength of the chemical bond between bioactive glass and the host tissue has been measured to be at least ten times higher than the contact osteogenesis (Anderson et al., 1992). Its high modulus and brittle nature makes its applications limited, but it has been used in combination with poly-methylmethacrylate to form bioactive bone cement and with metal implants as a coating to form a calcium-deficient carbonated calcium phosphate layer. Certain bioactive glass are strong enough to function in stress-bearing sites in the head and www.intechopen.com
Transcript of Development and Applications of Varieties of Bioactive...

4
Development and Applications of Varieties of Bioactive Glass Compositions in
Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery
and as Drug Delivery System
Samit Kumar Nandi1, Biswanath Kundu2 and Someswar Datta2 1Department of Veterinary Surgery and Radiology, West Bengal
University of Animal and Fishery Sciences, Kolkata, 2Bioceramics and Coating Division, Central Glass
and Ceramic Research Institute, Kolkata, India
1. Introduction
Bioactive glass is composed mainly of silica, sodium oxide, calcium oxide and phosphates. The bone-bonding reaction results from a series of reactions in the glass and its surface (Hench & Wilson, 1984). When granules of bioactive glass are inserted into bone defects, ions are released in body fluids and precipitate into a bone-like apatite on the surface, promoting the adhesion and proliferation of osteogenic cells (Ohtsuki et al., 1991; Neo et al., 1993) which is partially replaced by bone after long time implantation (Neo et al., 1994). The ion leaching phenomenon involves the exchange of monovalent cations from the glass, such as Na+ or K+, with H3O+ from the solution, and thus causes an increase in the pH of the solution. It is known that osteoblasts prefer a slightly alkaline medium (Ramp et al., 1994; Kaysinger & Ramp, 1998), but it is also known that severe changes in pH can inhibit osteoblast activity and cause cell necrosis or apoptosis (Brandao-burch et al., 2005; Frick et al., 1997; El-ghannam et al., 1997). Bioactive glass with a macroporous structure has the properties of large surface areas, which are favourable for bone integration. The behaviour of bioactive glass is dependent on the composition of the glass (Brink, 1997; Brink et al., 1997), the surrounding pH, the temperature, and the surface layers on the glass (Andersson et al., 1988; Gatti & Zaffe, 1991). The porosity provides a scaffold on which newly-formed bone can be deposited after vascular in growth and osteoblast differentiation. The porosity of bioglass is also beneficial for resorption and bioactivity (De Aza et al., 2003). In push-out tests the strength of the chemical bond between bioactive glass and the host tissue has been measured to be at least ten times higher than the contact osteogenesis (Anderson et al., 1992). Its high modulus and brittle nature makes its applications limited, but it has been used in combination with poly-methylmethacrylate to form bioactive bone cement and with metal implants as a coating to form a calcium-deficient carbonated calcium phosphate layer. Certain bioactive glass are strong enough to function in stress-bearing sites in the head and
www.intechopen.com

Biomaterials Applications for Nanomedicine
70
neck (e.g., mandible replacement); however, such implants cannot be easily contoured in the operating room, and screws cannot be easily placed into bioactive glass blocks because they defy drilling and have a tendency to fragment during creation of screw holes.
2. Bioactive glass materials
Legendary Prof. L. L. Hench of University of Florida, USA discovered in 1969 that some compositions of glasses can bond chemically with bone when implanted to living tissues. Many researchers later on discovered some other ceramics, glass-ceramics and composites also have the same property (De Groot, 1983, 1988; De Groot et al., 1990; De Groot & LeGeros, 1988; Ducheyne et al., 1980; Gross et al., 1988; Gross and Strunz, 1985; Hench, 1987, 1988; Hench & Ethridge, 1982; Hench et al., 1971; Hench & Wilson, 1984; Holand et al., 1985; Hulbert et al., 1987; Jarcho, 1981; Kitsugi et al., 1989; Kokubo et al., 1986; Kokubo et al., 1982; Nakamura et al., 1985; Wilson et al., 1981; Yamamuro et al., 1990b; Yamamuro et al., 1988; Yoshii et al., 1988). He defined these glasses as ‘bioactive glass’ and since then it has been used mostly as a reconstructive material for damaged hard tissues such as bone (Hench, 2006; Hench et al., 1971). Some more specialized compositions of bioactive glass will bond to soft tissues and bone (Wilson & Nolletti, 1990; Wilson et al., 1981; Yamamuro et al., 1990a). General characteristics of these bioactive glasses are a time-dependent, kinetic modification of the surface that occurs when implanted in vivo (Gross et al., 1988; Hench, 1988), the surface forms biologically active hydroxycarbonate apatite (HCA) layer providing bonding interface with tissues. The advantage is that it is possible to design this glass to get a controlled rate of degradation and bonding to the tissue. The HCA phase that forms on these implants is very similar chemically and structurally to the mineral phase in bone and thus responsible for interfacial bonding. These bioactive materials develop an adherent interface with tissues that resists significant mechanical forces. In some cases this interfacial strength of adhesion is equivalent to or greater than the cohesive strength of the implant material or the tissue bonded to bioactive implant. The rapid reaction at the surface leads to a fast bonding with the living tissues, but, due to the mainly two-dimensional structure of the glass network, the mechanical properties are relatively low. It may be noted that small changes in the composition can lead to very different properties and thus has added advantage of its versatility in contact with different living tissues, on range of properties depending on the implantation site of the prosthesis. Certain compositional range of bioactive glass containing SiO2, Na2O, CaO, and P2O5 like ordinary soda-lime-silica glasses in specific proportions shows bonding to bone (Table 1).Three key compositional features of these glasses distinguish them from traditional Na2O-CaO-SiO2 glasses: (1) less than 60 mol. % SiO2, (2) high-Na2O and high-CaO content, and (3) high-CaO/P2O5 ratio. As known, SiO2/Al2O3 act as glass network former, CaO/MgO/P2O5 is the network modifier and Na2O/K2O is the fluxing agent. These compositional features made the surface highly reactive when exposed to aqueous medium. Very popular 45S5 bioactive silica glasses are based upon 45 wt. % SiO2, S as the network former, and a 5 to 1 molar ratio of Ca to P. Glasses with very lower molar ratios of Ca to P (in the form of CaO and P2O5) do not bond to bone (Hench and Paschall, 1973). Different substitutions in the 45S5 compositions of 5-15 wt. % B2O3 for SiO2, or 12.5 wt. % CaF2 for CaO or crystallizing the various bioactive glass compositions to form glass-ceramics were found to have no measurable effect on the ability of the material to form a bone bond (Hench & Paschall, 1973). But, addition of small 3 wt. % Al2O3 to the 45S5 formula prevents bonding
www.intechopen.com

Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
71
Sl. No.
Name of the composition
All are in weight %
SiO2 P2O5 CaOCa
(PO3)2 CaF2 MgO MgF2 Na2O K2O Al2O3 B2O3
Ta2O5
/TiO2
1. 45S5 Bioglass ®
(Hench et al., 1971)
45 6 24.5 - - - - 24.5 - - - -
2.
45S5.4F Bioglass ® (Hench et al., 1986; Hench et
al., 1971)
45 6 14.7 - 9.8 - - 24.5 - - - -
3.
45B15S5 Bioglass ® (Hench and Paschall, 1974; Hench et al.,
1975)
30 6 24.5 - - - - 24.5 - - 15 -
4. 52S4.6 Bioglass ®
(Hench and Clark, 1982)
52 6 21 - - - - 21 - - - -
5. 55S4.3 Bioglass ®
(Hench and Clark, 1982)
55 6 19.5 - - - - 19.5 - - - -
6. KGC Ceravital ®
(Gross et al., 1988)
46.2 - 20.2 25.5 - 2.9 - 4.8 0.4 - - -
7. KGS Ceravital ®
(Gross et al., 1988)
46 - 33 16 - - - 5 - - - -
8. KGy213 Ceravital
® (Gross et al., 1988)
38 - 31 13.5 - - - 4 - 7 - 6.5
9. A/W glass-
ceramic (Kokubo et al., 1986)
34.2 16.3 44.9 - 0.5 4.6 - - - - - -
10. MB glass-ceramic
(Holand et al., 1985)
19-52 4-24 9-3 - - 5-15 - 3-5 3-5 12-33 - -
11. S45P7
(Andersson et al., 1988)
45 7 22 - - - - 24 - - 2 -
12. S53P4 (Zehnder
et al., 2004) 53 4 20 - - - - 23 - - - -
13. 13-93 (Fu et al.,
2008) 53 4 20 - - 5 - 6 12 - - -
14. 4-Mar (Zhang et
al., 2008) 50.5 1 22.5 - - 6 - 5 15 - - -
15. 18-04 (Zhang et
al., 2008) 54.5 4 20 - - 4.5 - 15 - - 2 -
16. 23-04 (Zhang et
al., 2008) 56.25 1 20 - - 4.5 - 5 11.25 - 2 -
17. H2-02 (Munukka
et al., 2008) 53 2 22 - - 4.5 - 6 11 0.5 1 -
www.intechopen.com

Biomaterials Applications for Nanomedicine
72
Sl. No.
Name of the composition
All are in mole %
SiO2 P2O5 CaOCa
(PO3)2 CaF2 MgO MgF2 Na2O K2O Al2O3 B2O3
Ta2
O5/ TiO2
ZnO
18. CEL-2 (Vitale-
Brovarone et al., 2009)
45 3 26 - - 7 - 15 4 - - - -
19. 55S (Loty et al.,
2001) 55 4 41 - - - - - - - - - -
20. H (Linati et al.,
2005) 46.2 2.6 26.9 - - - - 24.3 - - - - -
21. HZ5 (Linati et al.,
2005) 44.4 2.5 25.9 - - - - 23.4 - - - - 3.8
22. HZ10 (Linati et
al., 2005) 42.5 2.4 4.8 - - - - 22.5 - - - - 7.8
23. HZ20 (Linati et
al., 2005) 38.8 2.2 22.6 - - - - 20.5 - - - - 15.9
Table 1. Different compositions of bioactive glass materials
(Andersson et al., 1990; Greenspan & Hench, 1976; Gross et al., 1988; Gross and Strunz, 1985; Hench & Clark, 1982; Hench & Paschall, 1973). Gross and co-workers found that a range of low-alkali (0-5 wt. %), bioactive silica glass-ceramics (Ceravital ®) also bond to bone (Gross et al., 1981; Gross et al., 1988; Gross et al., 1986a; Gross et al., 1986b; Gross & Strunz, 1985; 1980). Also small additions of Al2O3, Ta2O5, TiO2, Sb2O3 or ZrO2 inhibit bone bonding (Table 1). A two-phase silica-phosphate glass-ceramic composed of apatite (Ca10(PO4)6(OH1F2)) and wollastonite (CaO.SiO2) crystals (termed A/W glass-ceramic by the Kyoto University team, Japan) and a residual SiO2 glassy matrix, also bonds with bone with very high interfacial bond strength (Kitsugi et al., 1989; Kokubo et al., 1986; Kokubo et al., 1982; Nakamura et al., 1985; Yamamuro et al., 1988; Yoshii et al., 1988). But, addition of A12O3 or TiO2 to the A/W glass-ceramic inhibits bone bonding, while a second phosphate phase, -whitlockite (3CaO.P2O5) does not. Multiphase machinable bioactive silica phosphate glass-ceramic containing phlogopite ((Na,K)Mg3(AlSi3Ol0)F2), mica and apatite crystals, developed by the Freidrich Schiller University, Jena, Germany, bonds to bone despite presence of alumina in the composition (Holand et al., 1985). A13+ ions incorporated within the crystal phase did not alter the surface reaction kinetics of the material (Vogel et al., 1990). Some other compositions of bioactive glass have been developed at Abo Akademi, Turku, Finland, for coating onto dental alloys (Andersson et al., 1988; Andersson et al., 1990; Kangasniemi & Yti-Urpo, 1990). Prof. Hench has recently published the history leading to the development of bioactive glass from the discovery of classical 45S5 Bioglass® composition to successful clinical applications and tissue engineering (Hench, 2006). High amounts of Na2O and CaO as well as relatively high CaO/P2O5 ratio make the glass surface highly reactive in physiological environments (Hench, 1991). Other bioactive glass compositions developed over few years contain no sodium or have additional elements incorporated in the silicate network such as fluorine (Vitale-Brovarone et al., 2008), magnesium (Vitale-Brovarone et al., 2005; Vitale-Brovarone et al., 2007), strontium (Gentleman et al., 2010; O'Donnell & Hill, 2010; Pan et al., 2010), iron (Hsi et al., 2007), silver (Balamurugan et al., 2008; Bellantone et al., 2002; Blaker et al., 2004;
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
73
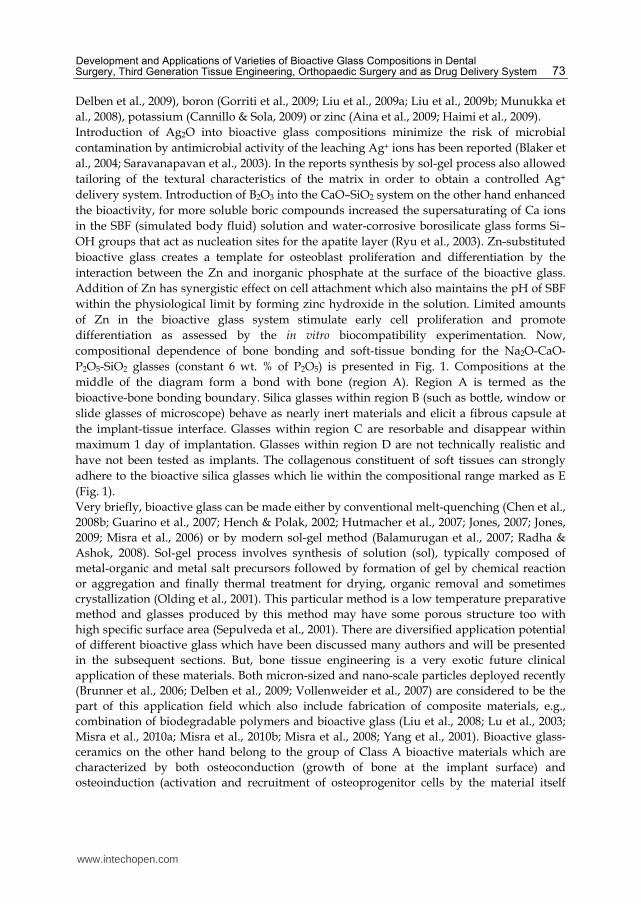
Delben et al., 2009), boron (Gorriti et al., 2009; Liu et al., 2009a; Liu et al., 2009b; Munukka et al., 2008), potassium (Cannillo & Sola, 2009) or zinc (Aina et al., 2009; Haimi et al., 2009). Introduction of Ag2O into bioactive glass compositions minimize the risk of microbial contamination by antimicrobial activity of the leaching Ag+ ions has been reported (Blaker et al., 2004; Saravanapavan et al., 2003). In the reports synthesis by sol-gel process also allowed tailoring of the textural characteristics of the matrix in order to obtain a controlled Ag+ delivery system. Introduction of B2O3 into the CaO–SiO2 system on the other hand enhanced the bioactivity, for more soluble boric compounds increased the supersaturating of Ca ions in the SBF (simulated body fluid) solution and water-corrosive borosilicate glass forms Si–OH groups that act as nucleation sites for the apatite layer (Ryu et al., 2003). Zn-substituted bioactive glass creates a template for osteoblast proliferation and differentiation by the interaction between the Zn and inorganic phosphate at the surface of the bioactive glass. Addition of Zn has synergistic effect on cell attachment which also maintains the pH of SBF within the physiological limit by forming zinc hydroxide in the solution. Limited amounts of Zn in the bioactive glass system stimulate early cell proliferation and promote differentiation as assessed by the in vitro biocompatibility experimentation. Now, compositional dependence of bone bonding and soft-tissue bonding for the Na2O-CaO-P2O5-SiO2 glasses (constant 6 wt. % of P2O5) is presented in Fig. 1. Compositions at the middle of the diagram form a bond with bone (region A). Region A is termed as the bioactive-bone bonding boundary. Silica glasses within region B (such as bottle, window or slide glasses of microscope) behave as nearly inert materials and elicit a fibrous capsule at the implant-tissue interface. Glasses within region C are resorbable and disappear within maximum 1 day of implantation. Glasses within region D are not technically realistic and have not been tested as implants. The collagenous constituent of soft tissues can strongly adhere to the bioactive silica glasses which lie within the compositional range marked as E (Fig. 1). Very briefly, bioactive glass can be made either by conventional melt-quenching (Chen et al., 2008b; Guarino et al., 2007; Hench & Polak, 2002; Hutmacher et al., 2007; Jones, 2007; Jones, 2009; Misra et al., 2006) or by modern sol-gel method (Balamurugan et al., 2007; Radha & Ashok, 2008). Sol-gel process involves synthesis of solution (sol), typically composed of metal-organic and metal salt precursors followed by formation of gel by chemical reaction or aggregation and finally thermal treatment for drying, organic removal and sometimes crystallization (Olding et al., 2001). This particular method is a low temperature preparative method and glasses produced by this method may have some porous structure too with high specific surface area (Sepulveda et al., 2001). There are diversified application potential of different bioactive glass which have been discussed many authors and will be presented in the subsequent sections. But, bone tissue engineering is a very exotic future clinical application of these materials. Both micron-sized and nano-scale particles deployed recently (Brunner et al., 2006; Delben et al., 2009; Vollenweider et al., 2007) are considered to be the part of this application field which also include fabrication of composite materials, e.g., combination of biodegradable polymers and bioactive glass (Liu et al., 2008; Lu et al., 2003; Misra et al., 2010a; Misra et al., 2010b; Misra et al., 2008; Yang et al., 2001). Bioactive glass-ceramics on the other hand belong to the group of Class A bioactive materials which are characterized by both osteoconduction (growth of bone at the implant surface) and osteoinduction (activation and recruitment of osteoprogenitor cells by the material itself
www.intechopen.com
Biomaterials Applications for Nanomedicine
74
stimulating bone growth on the surface of the material) (Hench, 2006; Hench, 1998; Jones, 2007; Thompson & Hench, 1998). In contrast, Class B bioactive materials exhibit only osteoconductivity. A recent review summarizing research on Ca-Si-based ceramics is also available (Wu, 2009). As far as bioactive glass-ceramics are concerned, these are partially crystallized glasses produced by heating the parent bioactive glass above its crystallization temperature, usually at about 610-630o C (Boccaccini, 2005; Boccaccini et al., 2007; Brunner et al., 2006; Jones, 2007). Glass-ceramics obtained by a sintering process, it is found that during the incidence of crystallization and densification, the microstructure of the parent glass shrinks, porosity is reduced and the solid structure gains mechanical strength (Thompson & Hench, 1998). But, brittleness and low fracture toughness remain a major problem of these materials. The limited strength and low fracture toughness (i.e., resistance to fracture crack propagation) of bioactive glass has so far prevented their use for load-bearing implants (Boccaccini, 2005; Hench, 2006; Thompson & Hench, 1998; Thompson, 2005). Subsequently, the repair and regeneration of large bone defects at load-bearing anatomical sites remains a clinical/orthopedic challenge (Fu et al., 2010; Kanczler & Oreffo, 2008).
Fig. 1. Compositional dependence of bone bonding and soft tissue bonding of bioactive glass and glass ceramics. All compositions in region A have a constant 6 wt. % of P2O5. A-WGC (apatite-wollastonite glass-ceramic) has higher P2O5 content (Table 1). Region E (soft tissue boding) is inside the dashed line where IB>8 [* 45S5 Bioglass ®, ▲ Ceravital®, ● 55S4.3 Bioglass ®, and (---) soft-tissue bonding; IB=100/t0.5bb, where t0.5bb is the time to have more than 50% of the implant surface bonded to the bone and IB is bioactivity index, i.e. the level of bioactivity of a specific material can be related to the time for more than 50% of the interface to be bonded (Hench, 1988; Hench, 1991)]
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
75
2.1 Reaction kinetics
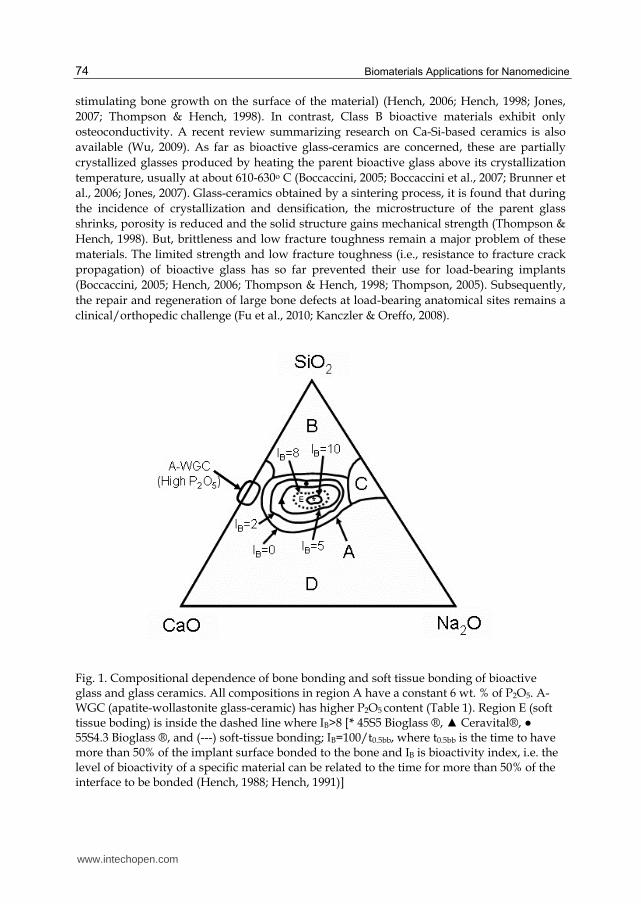
When a bioactive glass is immersed in an aqueous solution, like SBF (simulated body fluid) or TBS (tris buffer solution), there are three distinguishing reactions could be identified (Andersson et al., 1992; Hench, 1991, 1996, 1998; Hench & Andersson, 1993) (Fig. 2):
Fig. 2. Sequence of interfacial reactions kinetics involved in forming a bond between bone and a bioactive glass [modified after (Hench, 1998) and (Gerhardt & Boccaccini, 2010)].
1. Leaching and formation of silanols: Glass network releases alkali or alkaline earth elements exchanging cations with H+ or H3O+ cations proceeding from the solution. These modifying ions lead to high values of the interfacial pH, usually more than 7.4.
2. Dissolution of the glass network: -Si-O-Si-O-Si- bonds break through the action of hydroxyl ions. Breakdown of the silica network releases locally silicic acid [Si(OH)4]. If there is more than 60% of silica, the dissolution rate decreases as this increases the number of bridging oxygens in the structure of the glass. The hydrated silica (Si-OH) formed on the glass surface by these reactions undergoes rearrangement by polycondensation of neighboring silanols, resulting in a silica rich gel layer.
3. Precipitation: Calcium and phosphate ions released from the glass together with those from solution form a calcium-phosphate rich layer (CaP) on the surface. This phosphate is initially amorphous, then crystallizes to a hydroxycarbonate apatite (HCA) structure by incorporating carbonate anions from solution within the amorphous CaP phase. The mechanism of nucleation and growth of HCA appears to be the same in vivo and in vitro and is accelerated by the presence of hydrated silica. These stages do not depend on the presence of the tissue and they are observed in distilled water as well as SBF or tris-buffer solution. The following additional series of reactions is needed to get a bond with the tissue:
4. Absorption of biological moieties in the SiO2-HCA layer 5. Action of macrophages
www.intechopen.com
Biomaterials Applications for Nanomedicine
76
6. Attachment of stem cells 7. Differentiation of stem cells 8. Generation of matrix 9. Mineralisation of matrix This model as proposed by Prof. Hench is widely accepted but has some limitations too. As for example the first stage of the reaction relies on the rapid exchange of the Na+ ions released from the glass with the protons of the solution, although bioactive glass have been produced without sodium. The index as given in Fig. 1 is also not predictive of the influence of the silica mole fraction on the reactivity of the glass. Some parameters like network connectivity based on the inorganic polymer model for glasses could be considered to describe the behavior of a bioactive glass (Bovo, 2007). The closer the glass composition to the boundary of Fig. 1, the slower is the bonding rate. Usually, the thickness of the bonding zone is proportional to IB. As the thickness of this zone increases, the failure strength decreases. Further, it was found that if they break after implantation and the broken surfaces stay in contact with SBF, they may self-repair fusing themselves through their apatite surface layers (Bovo, 2007). Again, bioactive glass produced by Ebisawa et al. with a molecular formula of CaO.SiO2 (Ebisawa et al., 1990) could not account for the bioactivity, the model of which proposed by Prof. Hench (Hill, 1996). Concepts such as cross-link density or network connectivity can be applied to describe their structure if silicate glasses are considered to be inorganic polymers of silicon cross-linked by oxygen (Ray, 1978). The network connectivity of a glass is defined as the average number of additional cross-linking bonds (more than two) for elements other than oxygen that form the network backbone. The calculation of network connectivity of a glass network is based on the relative numbers of network-forming oxide species (those which contribute “bridging” or cross-linking oxygen species) and network-modifying species (those which result in the formation of “non-bridging” species) present (Wallace et al., 1999). The network connectivity of a glass can be used to predict various physical properties of the glass, including its solubility (Hill, 1996). The silicate structural units in a glass of low network connectivity are probably of low molecular mass and are capable of going into solution. Thus, glass solubility increases as network connectivity is reduced. So, glasses of low network connectivity are potentially bioactive (Wallace et al., 1999). Lockyer et al. determined the effect of substituting sodium oxide for calcium oxide on some glass properties (Lockyer et al., 1995). Most studies on bioactive glass systems have been carried out on a weight per cent basis. But, mole per cent substitutions are known to have more significance on a structural level. Weight percent basis has the effect of hiding the composition-property relationships of bioactive glass as there is no account taken of the degree of disruption of the glass network (Lockyer et al., 1995; Strnad, 1992). Fig. 3 represents a highly disrupted glass network. It can be seen that for every mole of calcium oxide removed from the glass network, one mole of sodium oxide must be added in order to maintain the same number of non-bridging oxygen species and, thus the same network connectivity value. So, a substitution on weight per cent basis produces a change in the relative number of non-bridging oxygen species and bridging oxygen species, with consequent change in network connectivity. Work carried out by Wallace et al. uses the concepts of network connectivity for the purposes of designing bioactive glass compositions for control of the physical, chemical and biological properties of bioactive glass (Wallace et al., 1999).
www.intechopen.com

Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
77
Fig. 3. Representation of glass structure (Wallace et al., 1999)
2.2 Fabrication
Properties of bioactive glass and glass-ceramics are dependent on fabrication methods and the heat-treatment used. Many scaffold fabrication techniques have been reported in the literature, e.g., foam replication methods, salt or sugar leaching, thermally induced phase separation, microsphere emulsification sintering, electrospinning for nano-fibrous structures, computer aided rapid prototyping techniques (Yang et al., 2002; Yun et al., 2007), textile and foam coating methods (De Diego et al., 2000; Francis et al., 2010; Mohamad Yunos et al., 2008) and biomimetic approach (Oliveira et al., 2003; Taboas et al., 2003). All of these methods were done to optimize the structure, properties and mechanical integrity of scaffolds. The design and incorporation of nano-topographic features on the scaffold surface architecture, in order to mimic the nanostructure of natural bone, is also becoming a significant area of research in bone tissue engineering (Berry et al., 2006; Jones, 2009; Stevens & George, 2005; Webster & Ahn, 2007). Also, comprehensive reviews of the general state-of-the art in scaffold manufacturing and optimization are available (Boccaccini & Blaker, 2005; Guarino et al., 2007; Hutmacher et al., 2007; Mohamad Yunos et al., 2008; Rezwan et al., 2006; Yang et al., 2001). Pores of bioactive glass and glass-ceramics could be formed by the addition of suitable porogens, such as polymeric materials and foaming agents (Karlsson et al., 2000). Rainer et al. prepared bioactive glass foams for mimicking bone tissue engineering scaffolds using in situ foaming of bioactive glass-loaded polyurethane foam (Rainer et al., 2008). Inspired by this fabrication technique, the bioactive materials were prepared with three-dimensional processing and showed promising applications in reconstructive surgery tailored to each single patient. Polyethylene glycol 4000 (HO(C2H4O)-nH) with particles sizes of 5-500 μm was used as foaming agent for preparing porous bioactive glass ceramic (Lin et al., 1991). This group has also reported the compatibility of porous bioactive glass ceramic with animal tissues. The microstructures of the implant were distributed uniformly in the material, which provided channels for bone in-growth and improved the microscopic bioresorption. Organic polymers were found to be an alternate attractive choice for generating desired pores and porosity due to the complete degradation at temperatures above 600° C. These organic polymers are abundant in natural environment, also available as biomass such as dry and wet woods and crops. This can be obtained from wastes in many related industries too such as food processing and wood finishing manufactures (Sooksaen et al., 2008). It was reported that textural properties (pore size, pore volume, pore structure) of biomaterials may have complex influences on the development of the apatite layer in bioactive glass. Increasing the specific surface area and pore volume of bioactive glass may greatly accelerate the apatite formation and therefore enhance the bioactive behavior (Vallet-Regí et al., 2003).
www.intechopen.com
Biomaterials Applications for Nanomedicine
78
Sl. No. Glass composition or system Reference Fabrication method
adopted
Particle size of starting glass
powder
1 45S5 (Ochoa et al.,
2009) Polymer foam
replication< 5 μm
2 SiO2-CaO-CaF2-Na2O-K2O-
P2O5-MgO
(Vitale-Brovarone et
al., 2008)
Polymer foam replication
< 32 μm
3 SiO2-P2O5-CaO-MgO-Na2O-
K2O
(Vitale-Brovarone et
al., 2009b; Vitale-
Brovarone et al., 2007)
Polymer foam replication
< 30 μm
4 SiO2-P2O5-CaO-MgO-Na2O-
K2O(Renghini et
al., 2009)Polymer foam
replication-do-
5 45S5 (Chen et al.,
2008a)Polymer foam
replication10-20 μm
6 SiO2-Na2O-CaO-MgO (Vitale-
Brovarone et al., 2005)
Starch consolidation < 100 μm
7 SiO2-P2O5-B2O3-CaO-MgO-
K2O-Na2O (Moimas et al.,
2006)
Compaction and sintering of melt-spun
fibers
75 μm (fibre diameter)
8 SiO2-CaO-Na2O-K2O-P2O5-
MgO-CaF2
(Baino et al., 2009)
Polymer porogen bakeout
< 106 μm
9 45S5 (Boccaccini et
al., 2007)Polymer foam
replication20-50 μm
10 SiO2-Na2O-K2O-MgO-CaO-
P2O5
(Fu et al., 2007)
Slip casting 255-325 μm
11 SiO2-Na2O-K2O-MgO-CaO-
P2O5
(Fu et al., 2008)
Polymer foam replication
< 5-10 μm
12 SiO2-Na2O-K2O-MgO-CaO-
P2O5
(Fu et al., 2010)
Freeze casting < 5 μm
13 SiO2-CaO-K2O (Vitale
Brovarone et al., 2006)
Polymer porogen burn-off
< 106 μm
14 SiO2-TiO2-B2O3-P2O5-CaO-
MgO-K2O-Na2O (Haimi et al.,
2009)
Compaction and sintering of melt-spun
fibers
75 μm (fibre diameter)
15 45S5 (Deb et al.,
2010) Polymer porogen
bakeout45-90 μm
16 45S5 (Bretcanu et
al., 2008)Polymer foam
replication< 5 μm
17 SiO2-Na2O-K2O-MgO-CaO-
P2O5; 45S5 (Brown et al.,
2008)
Densification andsintering of melt-spun
fibers
25-40 μm (fibre diameter)
www.intechopen.com

Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
79
18 45S5 (Chen et al.,
2006b)Polymer foam
replication≈ 5 μm
19 45S5 (Chen et al.,
2006a)Polymer foam
replication5-10 μm
20 45S5 (Chen et al.,
2007) Polymer foam
replication≈ 10 μm
21 SiO2-P2O5-CaO-MgO-Na2O-
K2O
(Vitale-Brovarone et
al., 2010)
Polymer burn-off, foam replication
Not applicable
22 45S5 (Vargas et al.,
2009) Polymer foam
replication< 5 μm
23 SiO2-Na2O-CaO-P2O5-B2O3-
TiO2
(Ghosh et al., 2008)
Polymer porogen bakeout
Not applicable
24 SiO2-Na2O-CaO-P2O5-B2O3-
TiO2
(Nandi et al., 2009)
Polymer porogen bakeout
Not applicable
25 SiO2-CaO-P2O5-Al2O3 (Mahmood et
al., 2001)Manual free-forming of melt- spun fibers
8-30 μm (fibre diameter)
26 SiO2-CaO-Na2O-P2O5-K2O-
MgO-B2O3
(Mantsos et al., 2009)
Polymer foam replication
Not applicable
27 SiO2-CaO-Na2O-K2O-MgO-
P2O5-B2O3 (Miguel et al.,
2010)
Densification andsintering of melt-spun
fibers
75 μm (fibre diameter)
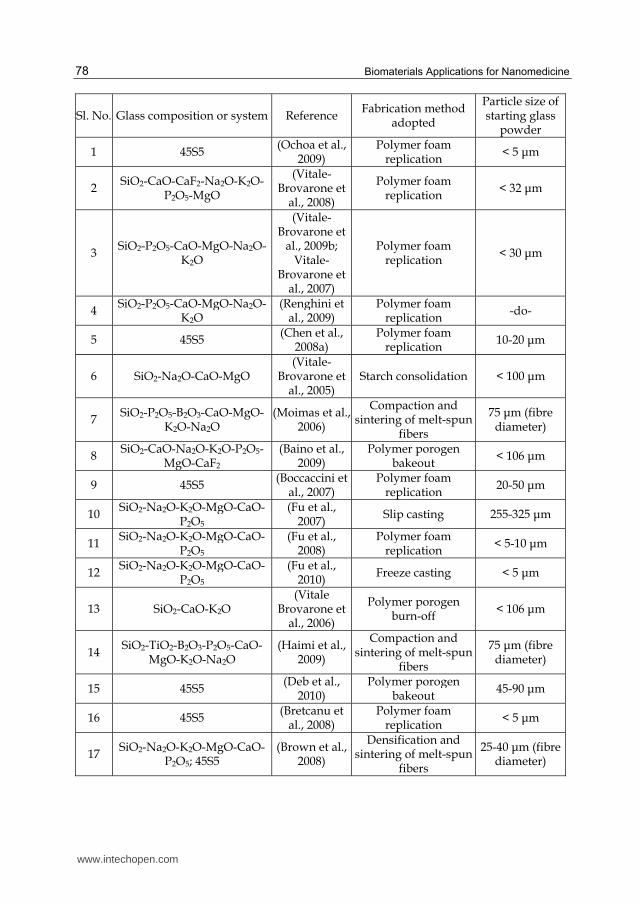
Table 2. Summary of recent studies performed on silicate bioactive glass-ceramic scaffolds
2.3 Clinical relevance
For bioactive glass-ceramics, recent developments related to bone tissue engineering scaffolds have been used to remove the gap of load-bearing large bone defects by inter-playing between architectures and components carefully designed from comprehensive levels, i.e., from the macro-, meso-, micrometer down to the nanometer scale (Deville et al., 2006), including both multifunctional bioactive glass composite structures and advanced bioactive glass-ceramic scaffolds exhibiting oriented microstructures, controlled porosity and directional mechanical properties (Baino et al., 2009; Bretcanu et al., 2008; Fu et al., 2010; Fu et al., 2008; Vitale-Brovarone et al., 2010). As summarized in Table 2 [reproduced from (Gerhardt & Boccaccini, 2010)], most of the studies have mainly investigated the mechanical properties, in vitro and cell biological behavior of glass-ceramic scaffolds (Baino et al., 2009; Boccaccini et al., 2007; Bretcanu et al., 2008; Brown et al., 2008; Chen et al., 2007; Chen et al., 2006a; Chen et al., 2008a; Chen et al., 2006b; Deb et al., 2010; Fu et al., 2010; Fu et al., 2007; Fu et al., 2008; Ghosh et al., 2008; Haimi et al., 2009; Klein et al., 2009; Kohlhauser et al., 2009; Mahmood et al., 2001; Mantsos et al., 2009; Miguel et al., 2010; Moimas et al., 2006; Nandi et al., 2009; Ochoa et al., 2009; Renghini et al., 2009; Vargas et al., 2009; Vitale-Brovarone et al., 2009a; Vitale-Brovarone et al., 2010; Vitale-Brovarone et al., 2009b; Vitale-Brovarone et al., 2008; Vitale-Brovarone et al., 2004; Vitale-Brovarone et al., 2005; Vitale-Brovarone et al., 2007; Vitale Brovarone et al., 2006). Scaffolds with compressive strength (Baino et al., 2009; Fu et al., 2010) and elastic modulus values (Fu et al., 2010; Fu et al., 2008) in magnitudes far above that of cancellous bone and close to the lower limit of cortical bone have been realized.
www.intechopen.com

Biomaterials Applications for Nanomedicine
80
3. Bioactive glass in dental surgery and cranio-maxillofacial augmentation
The increasing need for biomedical devices, required to face dysfunctions of natural tissues and organs caused by traumatic events, diseases and simple ageing, has drawn attention onto new materials that could be able to positively interact with the human body. Biomaterials play a significant role in dental, craniofacial and maxillofacial reconstruction. Their ever-increasing ease of use, long ‘shelf-life’ and safety enables them to be used efficiently and play an important role in reducing operating times (Gosain & Persing, 1999; Chim & Gosain, 2009). The ideal biomaterial in such reconstruction should be biocompatible with surrounding tissue without elucidating a foreign body reaction, radiolucent, easily shaped or molded, strong enough to endure trauma, stable over time, able to maintain volume, and osteoactive (Gosain & Persing, 1999; Damien & Parsons, 1991; Costantino et al., 1992; Jackson & Yavuzer, 2000; Gosain, 2003). Abnormality of the craniofacial skeleton may bring in from various causes, including tumor resection, severe infection, trauma, or congenital deformity. Restoring appropriate contour and support in the cranio-orbital region following loss or removal of bone may be quite challenging to the Craniofacial and Neurosurgeons. Since the late 1800’s when Muller described using calvarial bone grafts for reconstruction, they have remained the gold standard [Muller, 1890]. Autologous bone grafting provides a rich amount of native tissue that has a high possibility of osseous integration with little risk of rejection or infection long-term, in addition to safety and security (Manson et al., 1986). Although autogenous bone is the ideal material to primarily reconstruct large skull bone defects (Barone & Jimenez, 1997; Goodrich et al., 1992; Weber et al., 1987), it has some drawbacks in reconstruction including donor site morbidity, prolonged operating times, limited availability, and difficulty to contour (Nickell et al., 1972; Whitaker et al., 1979; Jackson et al., 1983). In the pediatric surgery, bone grafts may be relatively easily contoured and curved while, in adults, it is often difficult to achieve the precise three dimensional contours normally found in the cranio-orbital region (Ducic, 2001). Research was then initiated by reconstructive surgeons to find alternative means of reconstruction with alloplasts. In reality, alloplast reconstruction of the calvarium dates back to the year 2000 B. C. in ancient Peru when a gold plate was used to disguise a trephination defect (Grana et al., 1954). Since then, various alloplasts have been used in craniofacial reconstruction. The most commonly utilized material has been methylmethacrylate. Although, it suffers from several potential drawbacks including lack of osseointegration, secondary infection, plate fracture, erosion of the underlying recipient bone, necrosis of surrounding tissues during setting as it forms during an exothermic reaction with temperatures reaching 110° C, and difficulty shaping once polymerization occurs (Ducic , 2002; Costantino et al., 2000; Smith et al., 1999). In the past century, other metallic materials, such as silver, tantalum, stainless steel or titanium and calcium phosphate based materials like hydroxyapatite cement, calcium orthophosphate cements, porous granular hydroxyapatite, marine coral-based calcium carbonate were used for reconstruction purposes. The present endeavor deals with the application of bioactive glass based material in dental, craniofacial and maxillofacial reconstruction. Bioactive glass (BG) is biocompatible, osteoconductive, form a strong bond with living tissue via the formation of a hydroxyapatite layer on their surface (Meffert et al., 1985; Schepers et al., 1991; Hench et al., 1971) and have been used to repair hard tissues in a variety of craniofacial, maxillofacial, and periodontal applications (Hench, 1991). It has also been established that BG has good mechanical properties and a higher bioactivity in comparison to hydroxyapatite (Mardare et al., 2003; Ghosh et al., 2008)
www.intechopen.com

Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
81
BG particulate, for example, is used in a variety of dental procedures (Shapoff et. al., 1997), and many BG compositions can be formed into scaffolds for tissue engineering (Jones et al., 2007). Surface reactivity, however, is not their only mechanism of action as BG also releases ions that promote the osteoblast phenotype (Effah Kaufmann et al., 2000; Jell et al., 2008). In vitro studies have established that BG stimulates osteoprogenitors to differentiate to mature osteoblasts that produce bone-like nodules (Tsigkou et al., 2007; 2009). Bioactive glass was used in dentistry as a bioactive material in endosseous ridge maintenance implants (ERMI) as early as in 1986. Dicor® was the first glass-ceramic that allowed the manufacture of inlays and crowns where the major crystalline phase in the glass ceramic was mica (Grossman, 1991). A new glass-ceramic was developed by sol-gel technique having resemblance with commercial leucite based fluorapatite dental glass-ceramic. The produced material has prospective application in dental restorations and it is anticipated to exhibit better control of composition, microstructure and properties due to the intrinsic advantages of the sol-gel preparation method (Chatzistavrou et al., 2009). Recent studies indicated that rhenanite glass-ceramics can be utilized in dentistry (Holand et al., 2006). In a study, bioactive glass coated titanium alloy dental implants were compared with hydroxyapatite implants in human jaw bone and observed that bioactive glass coated implants were as equally successful as hydroxyapatite in achieving osseointegration and supporting final restorations (Mistry et al., 2011). Bioglass was mixed with phosphoric acid and irradiated with CO(2) laser could occlude the dentinal tubule orifices with calcium-phosphate crystals where the application of CO(2) laser potentially improved the mechanical organization of these crystals (Bakry et al., 2011). In another study, radio-opaque nanosized bioactive glass was used for root canal application particularly for dressing or filling material (Mohn et al., 2010). A modified bioglass formula was used as a pulp capping agent where the incidence of properly positioned dentin bridge formation was higher and the incidence of extruded dentin bridge formation was reduced (Stanley et al., 2001). A new treatment for localized aggressive periodontitis using enamel matrix proteins and bioactive glass resulted in the successful treatment of intrabony defects (Miliauskaite et al., 2007; Zietek et al., 1998). Bioactive glass was used in the treatment of intrabony defects in patients with generalized aggressive periodontitis (Mengel et al., 2006), in patients with moderate to advanced periodontitis with excellent outcome in mandibular molar Class II furcations (Yukna et al., 2001), molar furcation invasions (Anderegg et al., 1999), periodontal intrabony defects (Zamet et al., 1997) and in experimental periodontal wound healing in animal model (Karatzas et al., 1999). The effects of a recombinant mouse amelogenin (rM179) on the growth of apatite crystals nucleated on a bioactive glass (45S5 type Bioglass) surface were investigated with a view to gaining a better understanding of the role of amelogenin protein in tooth enamel formation and of its potential application in the design of novel enamel-like biomaterials (Wen et al., 1999). A fibre-reinforced bioglass composite is a promising material for dental applications where fibre significantly increases strength and toughness (Gheysen et al., 1983). PerioGlas, a silicate-based synthetic biomaterial was used for regeneration of peri-implant infrabony defects where new bone eventually reaches the implant, and osseointegration occurs with incorporation of the PerioGlas particles (Johnson et al., 1997). Bioactive glass has been used in cranio-maxillofacial reconstruction especially on the repair of periodontal and alveolar ridge defects (Quinones & Lovelace, 1997; Han et al., 2002; Sy, 2002; Throndson & Sexton, 2002; Norton & Wilson, 2002; Knapp et al., 2003) although its use is also extended for successful reconstruction of other areas of the head and neck (Scotchford et al., 2011). Bioactive glass has been utilized for the repair of orbital floor
www.intechopen.com

Biomaterials Applications for Nanomedicine
82
fractures with maintenance of globe position (Kinnunen et al., 2000; Aitasalo et al., 2001) and elevation of the floor of the maxillary sinus floor (Tadjoedin et al., 2002) in combination with autogenous iliac bone. Bioactive glass particles (Nova Bone, Porex Surgical) mixed with autogenous bone particles has also been used to cranial vault reconstruction (Gosain, 2003), in clinical studies in the treatment of cystic defects, ridge augmentations, apical resections, extraction sites, periodontal osseous defects and sinus lifts and augmentation (Furusawa T, Mizunuma, 1997; Low et al., 1997; Lovelace et al., 1998; Galindo-Moreno et al., 2008; Klongnoi et al., 2006). Bioactive glass posed some complications when used as a ceramic implant for contour restoration of the facial skeleton.
4. Bioglass as bone graft substitute
The management of fractures remains an incessant challenge for trauma and orthopedic surgeons. Although, majority of fractures heal uncomplicated, 5–10% of patients meet problems due to bone defects or impaired fracture healing, or a combination of both (Einhorn, 1995). Bone grafts fill voids and offer support, and therefore may augment the biological repair of the defect. Bone grafting is a widespread surgical procedure, carried out in approximately 10% of all skeletal reconstructive surgery cases (Schnettler & Markgraf, 1997). Bone healing differs from any other soft tissue since it heals through the generation of new bone rather than by forming fibrotic tissue. Osteogenesis, osteoinduction, osteoconduction and adequate blood and nutrient supply are the four critical elements of bone regeneration along with the final bonding between host bone and grafting material which is called osteointegration (Hing, 2004). Osteoprogenitor cells living within the donor graft, may survive during transplantation, could potentially proliferate and differentiate to osteblasts and eventually to osteocytes which represent the ‘‘osteogenic’’ potential of the graft (Cypher & Grossman, 1996; Giannoudis et al., 2005). ‘‘Osteoinduction’’ conversely is the stimulation and activation of host mesenchymal stem cells from the surrounding tissue, which differentiate into bone-forming osteoblasts. This process is mediated by a cascade of signals and the activations of several extra and intracellular receptors the most important of which belong to the TGF-beta superfamily (Urist, 1965; Cypher & Grossman, 1996). Osteoconduction describes the facilitation and orientation of blood-vessel and the creation of the new Haversian systems into the bone scaffold [Burchardt, 1983; Constantino & Freidman, 1994]. At last, ‘‘osteointegration’’ describes the surface bonding between the host bone and the grafting material (Constantino & Freidman, 1994). The most desirable form of bone substitute is the autologous bone graft for their superior osteoconduction, ease of incorporation, lack of immunological reactions, contains living bone cells that offer osteogenesis and growth factors that stimulate osteoinduction (Cypher & Grossman, 1996; Naber et al., 1972; Marciani et al., 1977). However, massive replacements of bone are not easily achieved by bone autografts as autogenous bone is limited in availability, and may result in the donar site morbidity (Mankin et al., 1976). Moreover, harvesting the autograft requires an additional surgery at the donar site that can result in its own 8–39% risk of complications, such as inflammation, risk of extensive blood loss infection, nerve and urethral injury, pelvic instability, cosmetic disadvantages and chronic pain (Banwart et al., 1995; Constantino & Freidman, 1994; Patka et al., 1998; Younger & Chapman, 1989; Summers & Eisenstein, 1989; Ross et al., 2000; Seiler & Johnson, 2000;
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
83
Skaggs et al., 2000). Furthermore, autografting is normally not recommended for elderly or pediatric patients or for patients with malignant or infectious disease (Bridwell et al., 1994; Gau et al., 1991; McCarthy et al., 1986). An allograft is preferred in some cases but the possible immune response and disease transmission may be detrimental for the recipient (Asselmeier et al., 1993; Stevenson & Horowitz, 1992; Chapman et al., 1997; Gazdag et al., 1995), so their use is suboptimal. Despite the benefits of autografts and allografts, the limitations of each have necessitated the pursuit of alternatives biomaterials. The ideal bone composite material with composition and mechanical properties equivalent to that of bone should have adequate biocompatibility, tailorable biodegradability, ability to initiate osteogenesis; in short, the graft should closely mimic the natural bone. Biodegradability together with biocompatibility and suitable mechanical properties are found only in a small group of materials. The aim of the present chapter was to provide a comprehensive overview of literature data of bioactive glass as bone substitutes for use in trauma and orthopedic surgery. Bioactive glasses exhibit osteoinductive and osteoconductive properties (Giannoudis et al., 2005) and can be manufactured into microspheres, fibers and porous implants. They are bioactive, as they interact with the body. Bioactivity depends upon the SiO2 content; the bonding between bone and glass is most excellent if the bioactive glass contains 45–52% SiO2 (Valimaki & Aro, 2006). The combination of hydroxyapatite with bioglass result in better composite bioactivity and biocompatibility compared to hydroxyapatite alone (Cholewa-Kowalska et al., 2009). They have significantly greater mechanical strength when compared to calcium phosphate preparations. After contact with body fluids, a silicate- rich layer is formed leading to mechanical strong graft–bone bonding. Above this, a hydroxyapatite layer will form, which directs new bone formation together with protein absorption. The extracellular proteins magnetize macrophages, mesenchymal stem cells and osteoprogenitor cells. Consequently, the osteoprogenitor cells proliferate into matrix-producing osteoblasts (Valimaki & Aro, 2006; Hench & Paschall, 1973). Mechanical properties of bioactive glass are not optimal, and therefore other ceramic components are sometimes added to the bioactive glass for reinforcement. Mechanical capability and biological absorbability of SiO(2)-CaO bioactive glass may also be improved by incorporating Na(2)O into bioactive glass, which can result in the formation of a hard yet biodegradable crystalline phase from bioactive glass when sintered by sol-gel process (Chen et al., 2010). In another study, mechanical properties of potassium fluorrichterite (KNaCaMg(5)Si(8)O(22)F(2)) glass-ceramics may be improved by either increasing the concentration of calcium (GC5) or by the addition of P(2)O(5) (GP2) that has potential as a load bearing bioceramic for fabrication of medical devices intended for skeletal tissue repair (Bhakta et al., 2010; Bandyopadhyay-Ghosh et al., 2010). A new porous bioactive glass has been developed by foaming with rice husks and sintering at 1050 degrees C for 1 hour that provides sufficient mechanical support temporarily while maintaining bioactivity, and that can biodegrade at later stages is achievable with the developed 45S5 bioglass-derived scaffolds (Wu et al., 2009). In experimental cancellous bone defects in rat models, bioactive glass was found biocompatible, and the filler effect was greater with bioactive glass than with autogenous bone (Heikkila et al., 1995). Bioglass was found to trigger new bone formation by allogenic demineralized bone matrix, and the biocompatibility of the glass was verified by the absence of adverse cellular reactions (Erdemli et al., 2010; Pajamaki et al., 1993a, 1993b).
www.intechopen.com

Biomaterials Applications for Nanomedicine
84
Biocompatibility and osteogenesis of biomimetic bioglass-collagen composite scaffolds alone and in combination with phosphatidylserine were also studied and confirmed that the composite scaffolds fulfill the basic requirements of bone tissue engineering scaffold and have the potential to be applied in orthopedic and reconstructive surgery (Marelli et al., 2010; Xu et al., 2011). Addition of hyaluronic acid and mesenchymal stem cell in the aforesaid scaffold further enhanced the healing of the bone defect (Xu et al., 2010). Bone-bonding response significantly enhanced with the micro-roughening of the bioactive glass surface, but the glass composition affected the intensity of the response (Itala et al., 2003). Bioactive glass have shown no or only mild inflammatory responses in the surrounding tissue in histological in vivo studies and in 6 months, the glass fiber scaffolds are completely resorbed (Moimas et al., 2006). In an experimental critical size bone defect model in goat, porous bioactive glass promoted bone formation over the extension of the defect and offers interesting potential for orthopedic reconstructive procedures (Nandi et al., 2009). Bioglass has been investigated extensively in bone tissue engineering but there has been relatively little previous research on its application to soft-tissue engineering. In a study, bioactive glass incorporated into scaffold was able to increase neovascularization that is extremely beneficial during the engineering of larger soft-tissue constructs (Day et al., 2004). Irrespective of soft and hard tissue healing necessitates enhanced neovascularization which can be induced by localized low concentration bioglass delivery and may offer an alternative approach to costly growth factors and their potential side-effects in bone regeneration (Leu et al., 2009). The first reports on clinical applications of bioactive glass materialize in the 1980s (Reck, 1981). Screw augmentation with bioactive glass was evaluated in 37 Weber type B ankle fractures with no information of screw loosening within a period of 2 years (Andreassen et al., 2004). Bioactive glass have been clinically used in vertebroplasty (Middleton et al., 2008; Palussiere et al., 2005), treatment of an unstable distal radius fracture (Smit et al., 2005), tympanoplastic reconstruction (Reck, 1983), as filling material in benign tumour surgery (Heikkila et al., 1995), for reconstruction of defects in facial bones [Suominen & Kinnunen, 1996], for treatment of periodontal bone defects (Villaca et al., 2005; Leonetti et al., 2000), in obliteration of frontal sinuses (Suonpaa et al., 1997; Peltola et al., 2000a, 2000b), in repairing orbital floor fractures (Kinnunen et al., 2000; Aitasalo et al., 2001), in lumbar fusion (Ido et al., 2000), reconstruction of the maxillary sinus (Scala et al., 2007), in cementless metal-backed acetabular cups (Hedia et al., 2006) and for reconstruction of the iliac crest defect after bone graft harvesting (Asano et al., 1994). The combination of a thermoplastic, viscous carrier with a granular bioglass scaffold allowed for the delivery of allergenic mesenchymal stem cells in a clinically manageable form that enhanced bone formation at early stages of canine alveolar repair (Mylonas et al., 2007).
5. Bioactive glass in drug delivery system
In recent years wide spread research has been initiated with new advanced drug delivery systems with better drug control and prolonged action. The drug delivery process is of paramount importance in assuring that a certain molecule will reach without decomposition or secondary reactions at the right place to perform its task with efficiency. The drug is introduced as part of an inert matrix, from which it should be released in a controlled way and where it should be distributed uniformly. Smart delivery systems that can be utilized
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
85
for the delivery of antibiotics, insulin, anti-inflammatory drugs, anticancer drugs, hormones and vaccines are yet to be developed, which are responsive to normal physiological process. Significant consideration is paid on the use of microspheres as carriers for proteins and drugs. The main benefit of microspheres over the more traditional macroporous block orthopaedic scaffolds is that microspheres possess not only better drug-delivery properties, but also the potential to fill the bone defects with irregular and complex shapes and sizes (Wu et al., 2004). The interstitial space between the particles of the microspheres is imperative for effective and functional bone regeneration (Malafaya et al., 2008; Luciani et al., 2008; Hsu et al., 1999), as they permit for both bone and vascular ingrowths. Several difficulties are encountered when macromolecules are incorporated in polymer devices e.g. protein drugs when impregnated may denature within the polymer matrix causing a loss of biological activity and probable changes in immunogenicity (Langer, 1990a, 1980b). This may happen due to degradation of the drug by the solvents or the temperature involved in the fabrication of the polymeric devices. Presently, ceramics have gained major recognition as bone substitute materials in dentistry and medicine as ceramics are biocompatible, resorbable and porous, attempts have been made to exploit them as delivery systems for drugs, chemicals and biologicals (Bajpai & Benghuzzi, 1988; Bajpai, 1994; Lasserre & Bajpai, 1998).
5.1 Drug delivery of antibiotics for treatment of osteomyelitis Treatment of orthopaedic infections with antibacterial agents by oral or intravenous route often leads the clinicians to be distrustful about patient outcome (Walenkamp, 1997); as the condition is frequently associated with poor vascular perfusion accompanied by infection of the surrounding tissue (Mader et al., 1993). Subsequent to surgical debridement, it is essential to maintain a highly effective concentration of the antibiotic in the infected area for a sufficient period of time (usually 4–6 weeks) to allow the healing process to complete (Kanellakopoulou & Giamarellos-Bourboulis, 2000). Treatment of osteomyelitis with local biodegradable antibiotic delivery systems has become a common practice in orthopaedic surgery. Biodegradable implants could provide high local bactericidal concentrations in tissue for the prolonged time needed to completely eradicate the infection and the likelihood to match the rate of implant biodegradability according to the type of infection treated (Kanellakopoulou & Giamarellos-Bourboulis, 2000). Biodegradation also makes surgical removal of the implant unnecessary. The implant can also be used initially to obliterate the dead space and, eventually to guide its repair. Porous block of bioactive glass has been studied for drug delivery applications of antibiotics for treatment of osteomyelitis in animal model (Nandi et al., 2009; Kundu et al., 2011). The glass ceramic block exists in two forms: one with porosity of 20-30 % and the other of 70 %. Excellent results were observed in infected arthroplasty after 2 years of treatment and the implanted material triggered osteogenesis so as to produce a complete radiological replacement of the osseous defect (Kawanabe et al., 1998). It has been observed that locally produced pure or bioglass reinforced plaster of Paris, hydroxyapatite and sodium alginate with cephazoline antibiotic are promising biomaterials for treatment of osteomyelitis and mainly because of economical reasons and availability, may be an alternative in clinical practice, especially for developing countries (Heybeli et al., 2003). Glass reinforced hydroxyapatite with sodium ampicillin, a broad spectrum antibiotic has been successfully applied for treatment of periodontitis (Queiroz et al., 2001). Gentamicin sulfate impregnated bioactive SiO2-CaO-P2O5 glass implants are good carriers for local gentamicin release into
www.intechopen.com

Biomaterials Applications for Nanomedicine
86
the local osseous tissue, where they show excellent biocompatibility and bone integration. Moreover, these implants are able to promote bone growth during the resorption process (Mes eguer-Olmo et al., 2006; Arcos et al., 2001). Antimicrobial activity of bioactive glass (BG) as a controlled release device for tetracycline hydrochloride and an inclusion complex formed by tetracycline and b-cyclodextrin has been investigated in mice model where there is prolonged period of release of antibiotic due to presence of cyclodextrin. It has been observed that there was an initial burst of 12%, followed by a sustained release over 80 days and a total release of 22–25%. (Dominguesa et al., 2004). The effectiveness of a degradable and bioactive borate glass has been compared with the clinically used calcium sulfate in the treatment of osteomyelitis of rabbits, as a carrier for vancomycin and proved to have excellent biocompatibility and to be very effective in eradicating osteomyelitis and simultaneously stimulating bone regeneration, avoiding the disadvantages of vancomycin loaded calcium sulphate (Zongping et al., 2009). Chitosan-bonded mixture of borate bioactive glass particles with teicoplanin (antibiotic) combining sustained drug release with the ability to support new bone ingrowth, could provide a method for treating chronic osteomyelitis in vitro and in vivo (Wei-Tao et al., 2010; Xin et al., 2010). In another study, well-ordered mesoporous bioactive glass impregnated with gentamycin has been carried out in vitro as a bioactive drug release system for preparation of bone implant materials vis-à-vis treatment of osteomyelitis (Xia & Chang, 2006; Zhu & Kaskel, 2009). Mesoporous bioactive glass (MBGs) with different compositions impregnated tetracycline has been prepared and their drug release behaviors have been studied (Zhao et al., 2008). Recently, an unique multifunctional bioactive composite scaffold mainly 45S5 Bioglass-based glass–ceramic scaffolds has been investigated with the potential to enhance cell attachment and to provide controlled delivery of gentamicin for bone tissue engineering (Francis et al., 2010). Composite materials composed of borate bioactive glass and chitosan (designated BGC) were investigated in vitro and in vivo as a new delivery system for teicoplanin in the treatment of chronic osteomyelitis induced by methicillin-resistant Staphylococcus aureus (MRSA) and demonstrated that this system is effective in treating chronic osteomyelitis by providing a sustained release of teicoplanin, in addition to participating in bone regeneration (Jia et al., 2010).
5.2 Bioactive glass delivery of growth factors
Bone regeneration is a coordinated cascade of events regulated by several hormones, cytokines and growth factors (Carano & Filvaroff, 2003; El-Ghannam, 2005; Hsiong & Mooney, 2000). Bioactive glass is regarded as high-potential scaffolds due to their osteoconductive properties (Thomas et al., 2005). The bone bonding ability is based on the chemical reactivity of the bioactive glass in which silicon bonds are broken and finally a CaP-rich layer is deposited on top of the glass which crystallizes to hydroxycarbonate apatite (HCA). To improve the biodegradability of this implant, porosity is introduced (Karageorgiou & Kaplan, 2005) which also helps to bone ingrowth, though pore sizes should be large enough. This porosity is occasionally called macroporosity while the bioglass implants can encompass a micro or nanoporosity of their own. Interconnectivity of the pores is of paramount necessity for tissue engineered bone constructs which implies generation of overlapping pore connection into the scaffolds. In bone tissue engineering growth factors are also introduced to accelerate tissue ingrowth. However, due to variation in potency and efficacy of individual growth factors, each study claimed different levels of bone healing. Growth factors like bone morphogenic protein-2&7 (BMP-2&7), transforming growth factor
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
87
(TGF-β), basic fibroblast growth factor (bFGF), insulin like growth factor-1&2 (IGF-1&2) and vascular endothelial growth factor (VEGF) are commonly introduced into these scaffolds due to their osteoinductive properties and vascularization (Seeherman & Wozney, 2005; Ginebra et al., 2006; Jansen et al., 2005). This increases the clinical significant amount high above normal values inside the human body and increases the cost of a single implant considerably, therefore diminishing a possible use of the material. The most appropriate technique for growth factor delivery is still under debate. Bioactive glass stimulates fibroblasts to secrete significantly increased amounts of angiogenic growth factors and can induce infiltration of a significantly increased number of blood vessels into tissue engineering scaffolds (Day, 2005; Day et al., 2004). Therefore it has a number of potential applications in therapeutic angiogenesis (Keshaw et al., 2005). PLGA polymeric system coated bioactive glass with VEGF has been investigated in the rat critical-sized defect with resultant enhanced angiogenesis and additive bone healing effects (Leach et al., 2006). An additional study in which BMP-4 and VEGF were concertedly delivered confirmed that combination of two growth factors promoted greater bone formation as compared to single factor treatment group (Huang et al., 2005). These results delineate a promising approach to enhance bone healing in hypovascularized defects that commonly occur after removal of bone tumors by radiation therapy. Sol-gel silica-based porous glass (xerogel) was used as a novel carrier material for recombinant human transforming growth factor-β1 (TGF-β1) and is capable of eliciting bone tissue reactivity that may serve as an effective bone graft material for the repair of osseous defects (Nicoll et al., 1997). A delivery system consisting of collagen Type I gel, Recombinant human BMP-2 (rhBMP-2) and 45S5 Bioglass microspheres seem to be a promising system for bone regeneration (Bergeron et al., 2007). Bovine bone morphogenetic protein has been delivered in bioactive glass on demineralized bone matrix grafts in the rat muscular pouch with effective outcome (Pajamaki et al., 1993).
6. Bioglass as coating of implants
In the present days, metallic materials gained considerable dimension as medical and dental devices due to their mechanical properties (Roessler et al., 2002). Implants are usually prepared of metals such as titanium alloys, cobalt alloys and SS 316L (García et al., 2004). The need to diminish costs in public health services has constrained the use of SS as the most economical option for orthopedic implants (Meinert et al., 1998; Fathi et al., 2003), because of its comparative low cost, ease of fabrication, ready availability and reasonable corrosion resistance. However, this material is prone to localized attack in long term use due to the hostile biological effects (Yılmaz et al., 2005). Besides, the corrosion of the metallic implants is imperative because it could adversely affect the biocompatibility and the mechanical integrity. Large concentrations of metallic cations coming from the implant can result in biologically unwanted reactions and might lead to the mechanical failure of the implant. Titanium and Ti-alloys are commonly used materials for in vivo applications, due to their good physical and mechanical properties such as low density, high corrosion resistance and mechanical resistance. Nevertheless, titanium and other alloying metal ions as aluminium and vanadium, release from the implants being accumulated in the nearby tissues, due to the aggressive action of the biological fluids (Hodgson et al., 2002; Zaffe et al., 2003; Yue et al., 2002; Finet et al., 2000; Milosev et al., 2000). The lack of interaction with the biological environment prevents the implant from integrating with the surrounding hard tissue.
www.intechopen.com
Biomaterials Applications for Nanomedicine
88
The perfection of the interface between bone and orthopaedic or dental implants is still considered as a challenge because the formation and maintenance of viable bone closely apposed to the surface of biomaterials are indispensable for the stability and clinical success of non-cemented orthopaedic/dental implants. It has been addressed to create a suitable environment where the natural biological potential for bone functional regeneration can be encouraged and maximized (Carlsson et al., 1994; Wennerberg et al., 1996; Larsson et al., 1996; Buser et al., 1998). Implant osseointegration depends on various factors viz. surface structure, biomechanical factors and biological response (Carlsson et al., 1994; Chappard et al., 1999). At the present time, osseointergation is defined not only as the absence of a fibrous layer around the implant with an active response in terms of integration to host bone, but also as a chemical (bonding osteogenesis) or physico-chemical (connective tissue osteogenesis) bond between implant and bone (Branemårk et al., 1983; Albrektsson, 1993) which in turn, depends on the biomineralization into the surrounding tissue. Biomineralization is normally happens when the bony injury or normal bone tissue in cellular level takes place. The process starts with the osteolysis through the osteoclastic cells from the vicinity as well as from the systemic source. This is instantaneously followed by formation of a protein-rich matrix in the localized area (injury site) which ultimately being mineralized with the inorganic ions viz. calcium and phosphorous from the serum and the localized tissues. Once the nucleation of bone formation takes place at a very faster rate (approx. 10 days), then routinely further bone formation with the incorporation of above-mentioned inorganic ions are found from the serum (Weiner, 1986). Further, implant loosening/migration is an unanswered complication associated with internal fixation. This problem may be overcome by modifying the implant/bone interface for improved osseous integration. Improved osseous integration may be obtained by the use of hydroxyapatite (HAp), b-tri calcium phosphate (b-TCP) and their composite coatings as nominally HAp to enhance the osteoconductivity of metallic implant (Thomas et al., 1987; Filiaggi, et al., 1991; Rivero et al., 1988). These coatings have been shown to promote osseointegration by stimulating bone growth onto the surface (Dey et al., 2011). Apart from calcium phosphate coating of metallic implants, extensive research has been initiated with bioglass as coatings for metallic implants because of their controlled surface reactivity and good bone bonding ability (Hench and Andersson, 1993; Hench, 1993; Ferraris et al., 1996). These coatings accomplish two purposes: improving the osseointegration of the implants, and shielding the metal against corrosion from the body fluids and the tissue from the corrosion products of the alloys. Unfortunately, most of the attempts to coat metallic implants with bioactive glass have had poor success. The explanation behind is due to poor adhesion of the coating and/or degradation of the glass properties during the coating procedure (typically enameling, or flame or plasma spray coating) (Hench & Andersson, 1993). Bioactive glass can be used to coat titanium alloys by different methods such as conventional enamelling, sputtering techniques, vacuum plasma spray and subsonic thermal spraying technique (STS) (Ferraris et al., 1996; Verné et al., 2000; Jana et al., 1995; Gomez-Vega et al., 2000; Li et al., 2007). These implants can offer several advantages, in terms of the high mechanical properties of the metallic substrate combined with the bioactivity of the coating aside from good protection of the substrate from corrosion. Bioactive glass and nanohydroxyapatite (BG-nHA) on titanium-alloy orthopaedic implants and surrounding bone tissue in vivo was evaluated and observed that these coatings could enhance the osteointegration of orthopaedic implant (Xie et al., 2010). Bioglass coating of the three-dimensional Ti scaffolds by the radio frequency magnetron sputtering technique
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
89
determines an in vitro increase of the bone matrix elaboration and may potentially have a clinical benefit (Saino et al., 2010). Biocompatible yttrium-stabilized zirconia (YSZ) in the form of nanoparticles and bioactive Bioglass (45S5) in the form of microparticles were used to coat Ti6Al4V substrates by electrophoretic deposition with potential applications in the orthopedics (Radice et al., 2007). Fluorapatite glass LG112 can be used as a sputtered glass coating on roughened surfaces of Ti6Al4V for possible future use for medical implants (Bibby et al., 2005). However, the Ti-alloys used in the fabrication of prosthetic implants are very reactive, and the glass/metal reactions that occur during firing are unfavorable to adhesion and bioactivity. Thus, coating titanium with bioactive glass is challenging. Besides, tremendous care should be taken in storing and/or shipping HA- or BG-coated Ti6A14V implants due to loss of bonding strength in low and high humidity (Chern et al., 1993). Bioactive glass comprising of SiO2-Na2O-K2O-CaO-MgO-P2O5 system has been formulated to coat orthopedic metallic implants by enameling and now have been utilized for coatings on commercial dental implants approximately 100 µm thick (Lopez-Esteban et al., 2003). Due to the peculiar softening properties of these materials, bioactive glass and glass-ceramics do imply a good alternative to hydroxyapatite, commonly used as bioactive coating on metallic prostheses in order to improve their adhesion to the bone. Further, bioglass coated implants exhibited greater bone ingrowth compared to hydroxyapatite coated and control implants in animal model and they maintained their mechanical integrity over time (Wheeler et al., 2001). In a study, multilayered bioactive glass-ceramic coatings on a Ti6Al4V alloy screws was conducted for dental applications with layers of controlled thickness (Verné et al., 2004). A biocompatible composite implant system was developed by coating bioglass onto cobalt-chromium alloy substrates where thin, adherent bioglass coating provides the ability of bonding directly to bone, while the underlying metal substrate gives the composite implants adequate strength to be used in load bearing applications (Lacefield & Hench, 1986). Improvement of the alumina/bone interface in Alumina on alumina total hip arthroplasty can be done by coating with sol-gel derived bioactive glass (Hamadouche et al., 2000). Polyurethane (PUR) and polyurethane/poly(d, l-lactide) acid (PUR/PDLLA) based scaffolds coated with Bioglass particles have potential to be used as bioactive, biodegradable scaffolds in bone tissue engineering (Bil et al., 2007).
7. Bioactive glasses’ in biomolecular engineering with special referencing to third generation biomaterials
Third generation biomaterials should be biocompatible, resorbable, and also bioactive eliciting specific cellular responses at the molecular level (Hench & Polak, 2002). Three-dimensional porous structures that stimulate cells’ invasion, attachment and proliferation, as well as functionalized surfaces with peptide sequences that mimic the ECM components so as to trigger specific cell responses are being developed (Agrawal & Ray, 2001; Hutmacher et al., 1996; Temenoff & Mikos, 2000). Tissue engineering applications and development of third generation biomaterials emerged at the same time. Tissue engineering is the promising therapeutic approach that combines cells onto resorbable scaffolds for in situ tissues regeneration and has emerged as an alternative potential solution to tissue transplantation and grafting. Tissue engineering is a multidisciplinary field that applies principles of life sciences and engineering towards the development of biological substitutes employing three fundamental “tools”, namely cells, scaffolds and growth factors (GFs) for the restoration, maintenance or improvement of
www.intechopen.com
Biomaterials Applications for Nanomedicine
90
tissue form and function (Langer & Vacanti, 1993). The common limitations associated with the application of allografts, autografts and xenografts include donor site insufficiency, rejection, diseases transfer, harvesting costs and post-operative morbidity (Fernyhough et al., 1992; Banwart et al., 1995; Goulet et al., 1997). Tissue engineering and regenerative medicine has made a new horizon in repairing and restoring organs and tissues using the natural signaling pathways and components such as stem cells, growth factors and peptide sequences among others, in amalgamation with synthetic scaffolds (Hardouin et al., 2000). Apart from the basic tissue engineering triad (cells, signaling and scaffold), angiogenesis and nutrients delivery should be taken into account as they both play vital role to stimulate tissue regeneration. Although tissue engineering emerged as a very dazzling option to overcome many existing problems related to the current use of autografts, allografts and xenografts, its implementation as part of a routine treatment for tissue replacement is controversial. Despite such limitations, tissue engineering is a very promising approach that opens newer vista of study and research in the field of regenerative medicine. Scaffolds of three-dimensional porous structures need to achieve the following criteria in order to be used in tissue engineering [Spaans et al., 2000; Boccaccini et al., 2008]. must be biocompatible and bio-resorbable at a controllable degradation and resorption
rate as well as provide the control over the appropriation must possess well defined microstructure with an interconnected porous network,
formed by a combination of macro and micro pores to allow proper tissue ingrowth, vascularization and nutrient delivery.
must have proper mechanical properties to regenerate bone tissue in load-bearing sites. must keep its structural integrity during the first stages of the new bone formation. The amalgamation of bioactivity and biodegradability is most likely the pertinent characteristics that include third-generation biomaterials. The bioactivation of surfaces with specific biomolecules is an influential means that allows cell guidance and stimulation towards a particular response. The endeavor is to mimic the ECM environment and function in the developed scaffold by coupling specific cues in its surface. Thus, cell behavior including adhesion, migration, proliferation and differentiation into a particular lineage will be influenced by the biomolecules attached to the material surface. In addition, pore distribution, interconnectivity and size are of paramount significance in order to assurance of proper cell proliferation and migration, as well as tissue vascularization and diffusion of nutrients. The concept of using bioactive glass substrates as templates for in vitro synthesis of bone tissue for transplantation by assessing the osteogenic potential has been investigated (Xynos et al., 2000; Phan et al., 2003; Chen et al., 2008; Brown et al., 2008) and confirmed that Bioglass scaffolds have potential as osteoconductive tissue engineering substrates for maintenance and normal functioning of bone tissue (Bretcanu et al., 2009). Human primary osteoblast-like cells cultured in contact with different bioactive glass suggested that bioglass not only induces osteogenic differentiation of human primary osteoblast-like cells, but can also increase collagen synthesis and release. The newly formulated bioactive gel-glass seems to have potential applications for tissue engineering, inducing increased collagen synthesis (Bosetti et al., 2003; Jones et al., 2007). Bone marrow is a combination of hematopoietic, vascular, stromal and mesenchymal cells capable of skeletal repair/regeneration with the ability of bone marrow cells to differentiate into osteoblasts and osteoclasts which is imperative in tissue regeneration during fracture healing, or for successful osteointegration of implanted prostheses, and in bone remodelling. Bone marrow cell culture systems with
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
91
bioactive glass seem to be useful and induce osteogenic differentiation and cell mineralization (Bosetti & Cannas, 2005). In another study, bioglass granules in combination with expanded periosteal cells in culture were investigated in rabbit large calvarial defects with increased ossification (Moreira-Gonzalez et al., 2005). Bioresorbable and bioactive tissue engineering composite scaffolds based on bioactive glass (45S5 Bioglass(R)) particles and macroporous poly(DL-lactide) (PDLLA) and polylactide-co-glycolide (PLAGA) with osteoblasts (HOBs) cells have tremendous potential as scaffolds for guided bone regeneration (Roether et al., 2002; Lu et al., 2005; Yang et al., 2006; ), for intervertebral disc tissue repair (Wilda & Gough, 2006; Helen & Gough, 2008). In another study, the cellular response of fetal osteoblasts to bioactive resorbable composite films consisting of a poly-D,L-lactide (PDLLA) matrix and bioactive glass 45S5 particles in the absence of osteogenic factors stimulates osteoblast differentiation and mineralization of the extracellular matrix, demonstrating the osteoinductive capacity of the composite (Tsigkou et al., 2007). Revision cases of total hip implants are complicated by the considerable amount of bone loss. New materials and/or approaches are desirable to provide stability to the site, stimulate bone formation, and eventually lead to fully functional bone tissue. Porous bioactive glass have been developed as scaffolds for bone tissue engineering. The incorporation of tissue-engineered constructs utilizing these scaffolds seeded with osteoprogenitor cells or culture expanded to form bonelike tissue on the scaffold prior to implantation has been conducted in large, cortical bone defects in the rat (Livingston et al., 2002). Bioglass-incorporated alginate hydrogels encapsulated with murine embryonic stem cells have potential implications and applications for tissue engineering where bioglass substrates could be used for the production of bioengineered bone both in vitro and in vivo and bioglass-incorporated alginate hydrogels can be injected directly into the defect area (Zhang et al., 2009). One of the major factors in the therapeutic accomplishment of bone tissue engineered scaffolds is the capacity of the construct to vascularise after implantation. For improving vascularization, porous bioactive glass-ceramic construct combination of co-culture human umbilical vein endothelial cells (HUVECS) with human osteoblasts (HOBS) may promote vascularization and facilitate tissue regeneration (Deb et al., 2010).
8. Conclusion
During the past decades, there has been a major breakthrough in development of biomedical materials including various ceramic materials for bone and dental repair as well as implantable drug delivery systems. Both increases in life expectancy and the social obligations to provide a better quality of life appeared to be the vital factors to this development. Significant attention has been paid towards the use of synthetic graft materials in bone tissue and dental repair and development of new implant technologies has led to the design concept of novel bioactive materials. Bioactive glass inducing active biomineralization in vivo have been a high demand in the development of clinical regenerative medicine. Originally, it was thought for bone repair and bone regeneration via tissue engineering (TE), but eventually has become a very attractive biomaterials of choice having implications in: dental, maxillofacial and ear implants, drug delivery system, injectable for treatment of enuresis, to activate genes for maintaining the health of tissues as they age, third generation TE scaffolds for soft connective tissue regeneration and repair,
www.intechopen.com

Biomaterials Applications for Nanomedicine
92
hybrid inorganic/organic bioactive scaffolds, anti-microbial effect for wound dressing, molecular modeling of the interaction of surface sites with amino acids, coating of metallic implants, effective carriers of growth factors, bioactive peptides etc.. In the coming future, bioactive glass may be explored by the scientists/researchers/clinicians in a better way and dimension for wellbeing of human kind.
9. References
Agrawal, CM. & Ray, RB. (2001). Biodegradable polymeric scaffolds for musculoskeletal tissue engineering. Journal of Biomedical Materials Research, 55(2): 141-150
Aina, V., Malavasi, G., Fiorio Pla, A., Munaron, L. & Morterra, C. (2009) 'Zinc-containing bioactive glasses: Surface reactivity and behaviour towards endothelial cells', Acta
Biomaterialia, 5(4): 1211-1222. Aitasalo, K., Kinnunen, I., Palmgren, J. & Varpula, M. (2001). Repair of orbital floor fractures
with bioactive glass implants. J. Oral. Maxillofac. Surg., 59(12):1390-1395. Albrektsson, T. (1993). On long-term maintenance of the osseointegrated response.
Australian Pros. J., 7: 15-24. Anderegg, C.R., Alexander, D.C. & Freidman, M. (1999). A bioactive glass particulate in the
treatment of molar furcation invasions. J. Periodontol., 70(4):384-7. Anderson, O.H., Liu, G., Kangasniemi, K. & Juhanoja, J. (1992). Evaluation of the acceptance
of glass in bone. Journal of Materials Science: Materials in Medicine, 3(2):145-150. Andersson, O.H., Karlsson, K.H., Kangasniemi, K. & Xli-Urpo, A. (1988). Models for
physical properties and bioactivity of phosphate opal glasses. Glastechnische
Berichte, 61(10):300-305. Andersson, Ö.H., Liu, G., Kangasniemi, K. & Juhanoja, J. (1992) 'Evaluation of the
acceptance of glass in bone', Journal of Materials Science: Materials in Medicine, 3(2): 145-150.
Andersson, Ö.H., Liu, G., Karlsson, K.H., Niemi, L., Miettinen, J. & Juhanoja, J. (1990) 'In vivo behaviour of glasses in the SiO2-Na2O-CaO-P2O5-Al2O3-B2O3 system', Journal of
Materials Science: Materials in Medicine, 1(4): 219-227. Andreassen, G.S., Hoiness, P.R., Skraamm, I., Granlund, O. & Engebretsen, L. (2004). Use of
a synthetic bone void filler to augment screws in osteopenic ankle fracture fixation. Arch. Orthop. Trauma. Surg., 124:161–5.
Arcos, D., Ragel, CV. & Vallet-Regí, M. (2001). Bioactivity in glass/PMMA composites used as drug delivery system. Biomaterials, 22(7): 701-708
Asano, S., Kaneda, K., Satoh, S., Abumi, K., Hashimoto, T. & Fujiya, M. (1994). Reconstruction of an iliac crest defect with a bioactive ceramic prosthesis. Eur. Spine
J., 3(1):39-44. Asselmeier, M.A., Caspari, R.B. & Bottenfield, S. (1993). A review of allograft processing and
sterilization techniques and their role in transmission of the human immunodeficiency virus. Am. J. Sports Med., 21:170–5.
Baino, F., Verné, E. & Vitale-Brovarone, C. (2009) '3-D high-strength glass-ceramic scaffolds containing fluoroapatite for load-bearing bone portions replacement', Materials
Science and Engineering: C, 29(6): 2055-2062.
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
93
Bajpai, PK. (1994). Using ceramics as drug delivery devices. Biomedical Engineering -
Applications, Basis and Communications, 6(4): 64-70. Bajpai, PK. & Benghuzzi HA. (1988). Ceramic systems for long-term delivery of chemicals
and biologicals. Journal of Biomedical Materials Research, 22(12): 1245-1266. Bakry, A.S., Takahashi, H., Otsuki, M., Sadr, A., Yamashita, K. & Tagami, J. (2011). CO2 laser
improves 45S5 bioglass interaction with dentin. J. Dent. Res., 90(2):246-50. Balamurugan, A., Balossier, G., Laurent-Maquin, D., Pina, S., Rebelo, A.H.S., Faure, J. &
Ferreira, J.M.F. (2008) 'An in vitro biological and anti-bacterial study on a sol-gel derived silver-incorporated bioglass system', Dental Materials, 24(10): 1343-1351.
Balamurugan, A., Balossier, G., Michel, J., Kannan, S., Benhayoune, H., Rebelo, A.H.S. & Ferreira, J.M.F. (2007) 'Sol gel derived SiO2-CaO-MgO-P2O5 bioglass system - Preparation and in vitro characterization', Journal of Biomedical Materials Research
Part B: Applied Biomaterials, 83B(2): 546-553. Bandyopadhyay-Ghosh, S., Faria, P.E., Johnson, A., Felipucci, D.N., Reaney, I.M., Salata,
L.A., Brook, I.M. & Hatton, P.V. (2010). Osteoconductivity of modified fluorcanasite glass-ceramics for bone tissue augmentation and repair. J. Biomed. Mater. Res. A., 94(3):760-8.
Banwart, JC., Asher, MA. & Hassanein, RS. (1995). Iliac crest bone graft harvest donor site morbidity. A statistical evaluation. Spine, 20(9): 1055-1060.
Barone, C.M. & Jimenez, D.F. (1997). Split-thickness calvarial grafts in young children. The
Journal of craniofacial surgery, 8(1):43-47. Bellantone, M., Williams, H.D. & Hench, L.L. (2002). 'Broad-Spectrum Bactericidal Activity
of Ag2O-Doped Bioactive Glass', Antimicrob. Agents Chemother., 46(6): 1940-1945. Bergeron, E., Marquis, ME., Chrétien, I. & Faucheux, N. (2007). Differentiation of
preosteoblasts using a delivery system with BMPs and bioactive glass microspheres. J. Mater. Sci. Mater. Med. 18(2): 255-63.
Berry, C.C., Dalby, M.J., Oreffo, R.O.C., McCloy, D. & Affrosman, S. (2006) 'The interaction of human bone marrow cells with nanotopographical features in three dimensional constructs', Journal of Biomedical Materials Research Part A, 79A(2): 431-439.
Bhakta, S., Pattanayak, D.K., Takadama, H., Kokubo, T., Miller, C.A., Mirsaneh, M., Reaney, I.M., Brook, I., van Noort, R. & Hatton, P.V. (2010). Prediction of osteoconductive activity of modified potassium fluorrichterite glass-ceramics by immersion in simulated body fluid. J. Mater. Sci. Mater. Med., 21(11):2979-88.
Bibby, JK., Bubb, NL., Wood DJ. & Mummery, PM. (2005). Fluorapatite-mullite glass sputter coated Ti6Al4V for biomedical applications. J. Mater. Sci. Mater. Med., 16(5): 379-85.
Bil, M., Ryszkowska, J., Roether, JA., Bretcanu, O. & Boccaccini, AR. (2007). Bioactivity of polyurethane-based scaffolds coated with Bioglass. Biomed. Mater., 2(2): 93-101.
Blaker, J.J., Nazhat, S.N. & Boccaccini, A.R. (2004) 'Development and characterisation of silver-doped bioactive glass-coated sutures for tissue engineering and wound healing applications', Biomaterials, 25(7-8): 1319-29.
Boccaccini, A.R. (2005) 'Ceramics', in Hench, L.L. & Jones, J.R. (Eds.): Biomaterials, Artificial
Organs and Tissue Engineering, Woodhead Publishing Limited CRC Press, Cambridge, U. K., pp. 26-36.
www.intechopen.com
Biomaterials Applications for Nanomedicine
94
Boccaccini, A.R. & Blaker, J.J. (2005). 'Bioactive composite materials for tissue engineering scaffolds', Expert Review of Medical Devices, Vol. 2, No. 3, pp. 303-317.
Boccaccini, A.R., Chen, Q., Lefebvre, L., Gremillard, L. & Chevalier, J. (2007) 'Sintering, crystallisation and biodegradation behaviour of Bioglass (R)-derived glass-ceramics', Faraday Discussions, 136: 27-44.
Boccaccini, AR., Roelher, JA., Hench, LL., Maquet, V. & Jérome, RA. (2008). Composites approach to tissue engineering. 26th Annual Conference on Composites, Advanced Ceramics, Materials, and Structures: B: Ceramic Engineering and Science
Proceedings, 23(4): 805-816. Bosetti, M. & Cannas, M. (2005). The effect of bioactive glasses on bone marrow stromal cells
differentiation. Biomaterials, 26(18): 3873-9. Bosetti, M., Zanardi, L., Hench, L. & Cannas, M. (2003). Type I collagen production by
osteoblast-like cells cultured in contact with different bioactive glasses. J. Biomed.
Mater. Res. A., 64(1): 189-95. Bovo, N. (2007) 'Structure-properties relationships in bioactive glasses for PAA-based
polyalkenoate cements': Departament de Ciència dels Materials i Enginyeria
Metallúrgica, Universitat Politècnica de Catalunya, Barcelona, Spain. Brandao-Burch, A., Utting, JC., Orriss, IR. & Arnett, TR. (2005). Acidosis inhibits bone
formation by osteoblasts in vitro by preventing mineralisation. Calcified Tissue
International, 77: 167-174. Branemårk, PI., Adell, R., Albrektsson, T., Lekholm, U., Lundkvist, S. & Rockler, B. (1983).
Osseointegrated titanium fixtures in the treatment of endentulosness. Biomaterials, 4: 25-28.
Bretcanu, O., Misra, S., Roy, I., Renghini, C., Fiori, F., Boccaccini, AR. & Salih, V. (2009). In vitro biocompatibility of 45S5 Bioglass-derived glass-ceramic scaffolds coated with poly(3-hydroxybutyrate). J. Tissue Eng. Regen. Med., 3(2): 139-48.
Bretcanu, O., Samaille, C. & Boccaccini, A. (2008) 'Simple methods to fabricate Bioglass andlt;sup>®</sup>-derived glass–ceramic scaffolds exhibiting porosity gradient', Journal of Materials Science, 43(12): 4127-4134.
Bridwell, KH., O’Brien, MF., Lenke, LG., Baldus, C. & Blanke, K. (1994). Posterior spinal fusion supplemented with only allograft bone in paralytic scoliosis. Does it work? Spine, 19: 2658—66.
Brink, M. (1997). The influence of alkali & alkaline earths on the working range for bioactive glasses. Journal of biomedical materials research, 36(1):109-117.
Brink, M., Turunen, T., Happonen, R.P. & Yli-Urpo, A. (1997). Compositional dependence of bioactivity of glasses in the system Na2O-K2O-MgO-CaO-B2O3-P2O5-SiO2. Journal
of biomedical materials research, 37(1):114-121. Brown, R.F., Day, D.E., Day, T.E., Jung, S., Rahaman, M.N. & Fu, Q. (2008) 'Growth and
differentiation of osteoblastic cells on 13-93 bioactive glass fibers and scaffolds', Acta Biomaterialia, Vol. 4(2): 387-396.
Brunner, T.J., Grass, R.N. & Stark, W.J. (2006) 'Glass and bioglass nanopowders by flame synthesis', Chemical Communications, 13: 1384-1386.
Burchardt, H. (1983). The biology of bone graft repair. Clin. Orthop. Relat. Res., 174: 28–42.
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
95
Buser, D., Nydegger, T., Hirt, HP., Cochran, DL. & Nolte, LP. (1998). Removal torque values of titanium implants in the maxilla of miniature pigs. Int. J. Oral Maxillofac.
Implants, 13: 611-619. Cannillo, V. & Sola, A. (2009) 'Potassium-based composition for a bioactive glass', Ceramics
International, 35(8): 3389-3393. Carano, RA. & Filvaroff, EH. (2003). Angiogenesis and bone repair, Drug Discov. Today 8:
980–989. Carlsson, L., Regner, L., Johansson, C., Gottlander, M. & Herberts, P. (1994). Bone response
to hydroxyapatite-coated and commercially pure titanium implants in the human arthritic knee. J. Orthop. Res., 12: 274-285.
Chapman, M.W., Bucholz, R. & Cornell, C. (1997). Treatment of acute fracture with collagen-calcium phosphate graft material. J. Bone Joint Surg., 79-A: 143-147.
Chappard, D., Aguado, E., Huré, G., Grizon, F. & Basle, MF. (1999). The early remodeling phases around titanium implants: a histomorphometric assessment of bone quality in a 3- and 6-month study in sheep. Int. J. Oral. Maxillofac. Implants, 14: 189-196.
Chatzistavrou, X., Hatzistavrou, E., Kantiranis, N., Papadopoulou, L., Kontonasaki, E., Chrissafis, K., Petros, K., Konstantinos, M., Paraskevopoulos, A. & Boccaccini, R. (2009). Novel glass-ceramics for dental application by sol-gel technique. Key
Engineering Materials, 396-398: 153-156. Chen, Q., Rezwan, K., Armitage, D., Nazhat, S. & Boccaccini, A. (2006a) 'The surface
functionalization of 45S5 Bioglass (R)-based glass-ceramic scaffolds and its impact on bioactivity', Journal of Materials Science: Materials in Medicine, 17(11): 979-987.
Chen, Q.Z., Efthymiou, A., Salih, V. & Boccaccini, A.R. (2008a) 'Bioglass®-derived glass–ceramic scaffolds: Study of cell proliferation and scaffold degradation in vitro', Journal of Biomedical Materials Research Part A, 84A (4): 1049-1060.
Chen, Q.Z., Li, Y., Jin, L.Y., Quinn, J.M. & Komesaroff, PA. (2010). A new sol-gel process for producing Na(2)O-containing bioactive glass ceramics. Acta Biomater., 6(10):4143-53.
Chen, Q.-Z., Rezwan, K., Françon, V., Armitage, D., Nazhat, S.N., Jones, F.H. & Boccaccini, A.R. (2007) 'Surface functionalization of Bioglass®-derived porous scaffolds', Acta
Biomaterialia, 3(4): 551-562. Chen, Q.Z., Thompson, I.D. & Boccaccini, A.R. (2006b). '45S5 Bioglass®-derived glass-
ceramic scaffolds for bone tissue engineering', Biomaterials, 27(11): 2414-2425. Chen, X., Meng, Y., Li, Y. & Zhao, N. (2008b). 'Investigation on bio-mineralization of melt
and sol-gel derived bioactive glasses', Applied Surface Science, 255(2): 562-564. Chern, LJ., Liu, ML. & Ju, CP. (1993). Environmental effect on bond strength of plasma-
sprayed hydroxyapatite/bioactive glass composite coatings. Technical note. Dent.
Mater., 9(4): 286-7. Chim, H. & Gosain, A.K. (2009). Biomaterials in craniofacial surgery: experimental studies
and clinical application. The Journal of craniofacial surgery, 20(1):29-33. Cholewa-Kowalska, K., Kokoszka, J., Laczka, M., Niedźwiedzki, L., Madej, W. & Osyczka,
A.M. (2009). Gel-derived bioglass as a compound of hydroxyapatite composites. Biomed. Mater., 4(5):055007.
www.intechopen.com
Biomaterials Applications for Nanomedicine
96
Constantino, P.D. & Freidman, C.D. (1994). Synthetic bone graft substitutes. Otolaryngol.
Clin. North Am., 27: 1037—73. Costantino, P.D., Friedman, C.D., Jones, K., Chow, L.C. & Sisson, G.A. (1992). Experimental
hydroxyapatite cement cranioplasty. Plastic and reconstructive surgery, 90(2):174-185. Costantino, PD., Chaplin, JM., Wolpoe, ME., Catalano, PJ., Sen, C., Bederson, JB. &
Govindaraj, S. (2000). Applications of fast-setting hydroxyapatite cement: cranioplasty. Otolaryngol Head Neck Surg., 123(4): 409-412.
Cypher, T.J. (1996). Grossman JP. Biological principles of bone graft healing. J. Foot Ankle
Surg., 35: 413–7. Damien, C.J. & Parsons, J.R. (1991). Bone graft and bone graft substitutes: a review of current
technology and applications. J. Appl. Biomater., 2(3):187-208. Day, R.M., Boccaccini, A.R., Shurey, S., Roether, J.A., Forbes, A., Hench, L.L. & Gabe, S.M.
(2004). Assessment of polyglycolic acid mesh and bioactive glass for soft-tissue engineering scaffolds. Biomaterials, 25(27):5857-66.
Day, RM. (2005). Bioglasss stimulates the secretion of angiogenic growth factors and angiogenesis. Tissue Eng., 11(5-6): 768-77.
Day, RM., Boccaccini, AR., Shurey, S., Roether, JA., Forbes, A., Hench, LL. & Gabe, SM. (2004). Assessment of polyglycolic acid mesh and bioactive glass for soft tissue engineering scaffolds. Biomaterials, 25 (27): 5857–66.
De Aza, P.N., Luklinska, Z.B., Santos, C., Guitian, F. & De Aza, S. (2003). Mechanism of bone-like formation on a bioactive implant in vivo. Biomaterials, 24(8):1437-1445.
De Diego, M.A., Coleman, N.J. & Hench, L.L. (2000). 'Tensile properties of bioactive fibers for tissue engineering applications', Journal of Biomedical Materials Research, 53(3): 199-203.
De Groot, K. (1983). Bioceramics of Calcium Phosphate. CRC Press, Boca Raton, FL. De Groot, K. (1988). 'Effect of porosity and physico-chemical properties on the stability,
resorption and strength of calcium phosphate ceramics', in Ducheyne, P. & Lemons, J. (Eds.): Bioceramics: Material Characteristics Versus In Vivo Behaviour, Annals of New York Academy of Sciences, New York.
De Groot, K. & LeGeros, R.Z. (1988) 'Significance of porosity and physical chemistry of calcium phosphate ceramics', in Ducheyne, P. & Lemons, J. (Eds.): Bioceramics:
Material Charactersitics Versus In Vivo Behaviour, Annals of New York Academy of Sciences, New York, pp. 268-277.
De Groot, K., Klein, C.P.A.T., Wolke, J.G.C. & De Blieck-Hogervorst, J. (1990) 'Chemistry of calcium phosphate bioceramics', in Yamamuro, T., Hench, L.L. & Wilson, J. (Eds.): Handbook of Bioactice Ceramics, CRC Press, Boca Raton, FL, pp. 3-15.
Deb, S., Mandegaran, R. & Di Silvio, L. (2010) 'A porous scaffold for bone tissue engineering/45S5 Bioglass and lt;supandgt;®and lt;/supandgt; derived porous scaffolds for co-culturing osteoblasts and endothelial cells', Journal of Materials
Science: Materials in Medicine, 21(3): 893-905. Delben, J., Pimentel, O., Coelho, M., Candelorio, P., Furini, L., Alencar dos Santos, F.b., de
Vicente, F.b. & Delben, A. (2009) 'Synthesis and thermal properties of nanoparticles of bioactive glasses containing silver', Journal of Thermal Analysis and Calorimetry, 97(2): 433-436.
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
97
Deville, S., Saiz, E., Nalla, R.K. & Tomsia, A.P. (2006) 'Freezing as a Path to Build Complex Composites', Science, 311(5760): 515-518.
Dey, A., Nandi, SK., Kundu, B., Kumar, C., Mukherjee, P., Roy, S., Mukhopadhyay, AK., Sinha, MK. & Basu, D. (2011). Evaluation of hydroxyapatite and β-tri calcium phosphate microplasma spray coated pin intra-medullary for bone repair in a rabbit model. Ceramic International, 37 (4): 1377-1391
Dominguesa, ZR., Cortes, ME., Gomes, TA., Diniz, HF., Freitas, CS. Gomes, JB., Faria, AMC. & Sinisterra, RD. (2004). Bioactive glass as a drug delivery system of tetracycline and tetracycline associated with b-cyclodextrin. Biomaterials, 25 (2004): 327–333
Ducheyne, P., Hench, L.L., Kagan, A., 2nd, Martens, M., Bursens, A. & Mulier, J.C. (1980) 'Effect of hydroxyapatite impregnation on skeletal bonding of porous coated implants', J. Biomed. Mate.r Res., 14(3): 225-37.
Ducic, Y. (2001). Three-dimensional alloplastic orbital reconstruction in skull base surgery. The Laryngoscope, 111(7):1306-1312.
Ducic, Y. (2002). Titanium mesh and hydroxyapatite cement cranioplasty: a report of 20 cases. J. Oral Maxillofac. Surg., 60(3):272-276.
Ebisawa, Y., Kokubo, T., Ohura, K. & Yamamuro, T. (1990) 'Bioactivity of CaO·SiO2-based glasses: In vitro evaluation', Journal of Materials Science: Materials in Medicine, 1(4): 239-244.
Effah Kaufmann, E.A., Ducheyne, P. & Shapiro, I.M. (2000). Evaluation of osteoblast response to porous bioactive glass (45S5) substrates by RT-PCR analysis. Tissue
Eng., 6(1):19–28. Einhorn, T.A. (1995). Enhancement of fracture-healing. J. Bone Joint Surg. Am., 77:940–56. El-Ghannam, A. (2005). Bone reconstruction: from bioceramics to tissue engineering, Expert
Rev. Med. Devices, 2: 87–101. El-Ghannam, A., Ducheyne, P. & Shapiro, IM. (1997a). Formation of surface reaction
products on bioactive glass and their effects on the expresssion of the osteoblastic phenotype and the deposition of mineralized extracellular matrix. Biomaterials, 18: 295-303.
Erdemli, O., Captug, O., Bilgili, H., Orhan, D., Tezcaner, A. & Keskin, D. (2010). In vitro and in vivo evaluation of the effects of demineralized bone matrix or calcium sulfate addition to polycaprolactone-bioglass composites. J. Mater. Sci. Mater. Med., 21(1):295-308.
Fathi, MH., Salehi, M., Saatchi, A., Mortazavi, V. & Moosavi, SB. (2003). In vitro corrosion behavior of bioceramic, metallic, and bioceramic-metallic coated stainless steel dental implants. Dent. Mater., 19(3): 188-198.
Fernyhough, JC., Schimandle, JJ., Weigel, MC., Edwards, CC. & Levine, AM. (1992). Chronic donor site pain complicating bone graft harvesting from the posterior iliac crest for spinal fusion. Spine, 17(12): 1474-1480.
Ferraris, M., Rabajoli, P., Brossa, F. & Paracchini, L. (1996). Vacuum plasma spray deposition of titanium particle/glass-ceramic matrix biocomposites. Journal of the American
Ceramic Society, 79(6): 1515-1520.
www.intechopen.com
Biomaterials Applications for Nanomedicine
98
Filiaggi, M., Pilliar, RM. & Coombs, NA. (1991). Characterization of the interface in the plasma-sprayed HA coating/Ti-6AI-4V implant system. Journal of Biomedical
Materials Research, 25: 1211-29. Finet, B., Weber, G. & Cloots, R. (2000). Titanium release from dental implants: An in vivo
study on sheep. Materials Letters, 43(4):159-165. Francis, L., Meng, D., Knowles, J.C., Roy, I. & Boccaccini, A.R. (2010) 'Multi-functional
P(3HB) microsphere/45S5 Bioglass®-based composite scaffolds for bone tissue engineering', Acta. Biomaterialia, 6(7): 2773-2786.
Frick, KK., Jiang, L., & Bushinsky, DA. (1997). Acute metabolic acidosis inhibits the induction of osteoblastic egr-1 and type 1 collagen. Am. J. Physiol. (Cell Physiol.), 272: C1450-C1456
Fu, Q., Rahaman, M.N., Bal, B.S. & Brown, R.F. (2010) 'Preparation and in vitro evaluation of bioactive glass (13–93) scaffolds with oriented microstructures for repair and regeneration of load-bearing bones', Journal of Biomedical Materials Research Part A, 93A (4): 1380-1390.
Fu, Q., Rahaman, M.N., Bal, B.S., Huang, W. & Day, D.E. (2007) 'Preparation and bioactive characteristics of a porous 13–93 glass, and fabrication into the articulating surface of a proximal tibia', Journal of Biomedical Materials Research Part A, 82A (1): 222-229.
Fu, Q., Rahaman, M.N., Sonny Bal, B., Brown, R.F. & Day, D.E. (2008) 'Mechanical and in vitro performance of 13-93 bioactive glass scaffolds prepared by a polymer foam replication technique', Acta Biomaterialia, 4(6): 1854-1864.
Furusawa, T. & Mizunuma, K. (1997). Osteoconductive properties and efficacy of resorbable bioactive glass as a bone-grafting material. Implant dentistry, 6(2):93-101.
Galindo-Moreno, P., Avila, G., Fernández-Barbero, J.E., Mesa, F., O'Valle-Ravassa, F. & Wang, H.L. (2008). Clinical and histologic comparison of two different composite grafts for sinus augmentation: a pilot clinical trial. Clin. Oral. Implants Res., 19(8):755-9.
García, C., Ceré, S. & Durán, A. (2004). Bioactive coatings prepared by sol-gel on stainless steel 316L. Journal of Non-Crystalline Solids, 348: 218-224
Gatti, A.M. & Zaffe, D. (1991). Short-term behaviour of two similar active glasses used as granules in the repair of bone defects. Biomaterials, 12(5):497-504.
Gau, YL., Lonstein, JE., Winter, RB., Koop, S. & Denis, F. (1991). Luque—Galveston procedure for correction and stabilization of neuromuscular scoliosis and pelvic obliquity: a review of 68 patients. J. Spinal Disord. 4: 399—410.
Gazdag, A.R., Lane, J.M., Glaser, D. & Forster, R.A. (1995). Alternatives to autogenous bone graft: efficacy and indications. J. Am. Acad. Orthop. Surg., 3: 1-8.
Gentleman, E., Fredholm, Y.C., Jell, G., Lotfibakhshaiesh, N., O'Donnell, M.D., Hill, R.G. & Stevens, M.M. (2010) 'The effects of strontium-substituted bioactive glasses on osteoblasts and osteoclasts in vitro', Biomaterials, 31(14): 3949-3956.
Gerhardt, LC. & Boccaccini, A.R. (2010) 'Bioactive glass and glass-ceramic scaffolds for bone tissue engineering', Materials, 3(7): 3867-3910.
Gheysen, G., Ducheyne, P., Hench, L.L. & de Meester, P. (1983). Bioglass composites: a potential material for dental application. Biomaterials, 4(2):81-4.
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
99
Ghosh, SK., Nandi, SK., Kundu, B., Datta, S., De, DK., Roy, SK. & Basu, D. (2008) 'In vivo response of porous hydroxyapatite and β-tricalcium phosphate prepared by aqueous solution combustion method and comparison with bioglass scaffolds', Journal of Biomedical Materials Research Part B: Applied Biomaterials, 86B (1): 217-227.
Giannoudis, P.V. (2005). Dinopoulos H, Tsiridis E. Bone substitutes: an update. Injury, 36(Suppl. 3): S20–7.
Ginebra, MP., Traykova, T. & Planell, JA. (2006). Calcium phosphate cements as bone drug delivery systems: a review, J. Control. Release., 113: 102–110.
Gomez-Vega, JM., Saiz, E., Tomsia, AP., Marshall, GW. & Marshall, SJ. (2000). Bioactive glass coatings with hydroxyapatite and Bioglass particles on Ti-based implants. 1. Processing. Biomaterials, 21(2): 105-111.
Goodrich, J.T., Argamaso, R. & Hall, C.D. (1992). Split-thickness bone grafts in complex craniofacial reconstructions. Pediatric neurosurgery, 18(4):195-201.
Gorriti, MF., López, JMP., Boccaccini, AR., Audisio, C. & Gorustovich, A.A. (2009) 'In vitro Study of the Antibacterial Activity of Bioactive Glass-ceramic Scaffolds', Advanced
Engineering Materials, 11(7): 67-B70. Gosain, A.K. (2003). Biomaterials in facial reconstruction. Operative Techniques in Plastic and
Reconstructive Surgery, 9(1):23-30. Gosain, A.K. & Persing, J.A. (1999). Biomaterials in the face: benefits and risks. The Journal of
craniofacial surgery, 10(5):404-414. Goulet, JA., Senunas, LE., DeSilva, GL. & Greenfield, ML. (1997). Autogenous iliac crest
bone graft. Complications and functional assessment. Clinical Orthopaedics and
Related Research, 339: 76-81. Grana, F., Rocca, ED. & Grana, L. (1954). Las trepanaciones craneanas en el Peru en a epoca
prehispanica. Lima, Peru: Imprenta Santa Maria, Greenspan, DC. & Hench, LL. (1976). 'Chemical and mechanical behavior of bioglass-coated
alumina', J Biomed Mater Res, 10(4): 503-9. Gross, U. & Strunz, V. (1985) 'The interface of various glasses and glass ceramics with a
bony implantation bed', J Biomed Mater Res, Vol. 19, No. 3, pp. 251-71. Gross, U., Brandes, J., Strunz, V., Bab, I. & Sela, J. (1981) 'The ultrastructure of the interface
between a glass ceramic and bone', J Biomed Mater Res, Vol. 15, No. 3, pp. 291-305. Gross, U., Kinne, R., Schmitz, H.J. & Strunz, V. (1988) 'The response of bone to surface active
glass/glass-ceramics', CRC Critical Reviews on Biocompatibility, Vol. 4, p. 2. Gross, U., Roggendorf, W., Schmitz, H.J. & Strunz, V. (1986a) 'Testing procedures for surface
reactive biomaterials', in Christel, P., Meunier, A. & Lee, A.J.C. (Eds.): Biological and
Biomechanical Performance of Biomaterials, Elsevier, Amsterdam, Netherlands, p. 367. Gross, U., Schmitz, H.J., Strunz, V., Schuppan, D. & Termine, J. (1986b) 'Proteins at the
interface of bone-bonding and non-bonding glass-ceramics': Transaction of the
Twelfth Annual Meeting of the Society for Biomaterials, Society for Biomaterials, Algonquin, IL, p. 98.
Gross, U.M. & Strunz, V. (1980) 'The anchoring of glass ceramics of different solubility in the femur of the rat', J Biomed Mater Res, Vol. 14, No. 5, pp. 607-18.
Grossman, D.G. (1991). In: International Symposium on Computer Restorations, IL: Quintessenz, Chicago, p. 103.
www.intechopen.com
Biomaterials Applications for Nanomedicine
100
Guarino, V., Causa, F. & Ambrosio, L. (2007) 'Bioactive scaffolds for bone and ligament tissue', Expert Review of Medical Devices, Vol. 4, pp. 405-418.
Haimi, S., Gorianc, G., Moimas, L., Lindroos, B., Huhtala, H., Räty, S., Kuokkanen, H., Sándor, G.K., Schmid, C., Miettinen, S. & Suuronen, R. (2009) 'Characterization of zinc-releasing three-dimensional bioactive glass scaffolds and their effect on human adipose stem cell proliferation and osteogenic differentiation', Acta Biomaterialia, Vol. 5, No. 8, pp. 3122-3131.
Hamadouche, M., Meunier, A., Greenspan, DC., Blanchat, C., Zhong, JP., La Torre, GP. & Sedel, L. (2000). Bioactivity of sol-gel bioactive glass coated alumina implants. J.
Biomed. Mater. Res. 52(2): 422-9. Han, J., Meng, H. & Xu, L. (2002). Clinical evaluation of bioactive glass in the treatment of
periodontal intrabony defects. Zhonghua kou qiang yi xue za zhi = Zhonghua kouqiang
yixue zazhi = Chinese journal of stomatology, 37(3):225-227. Hardouin, P., Anselme, K., Flautre, B., Bianchi, F., Bascoulenguet, G. & Bouxin, B. (2000).
Tissue engineering and skeletal diseases. Joint Bone Spine, 67(5): 419-424. Hedia, H.S., El-Midany, T.T., Shabara, M.A. & Fouda, N. (2006). Design optimization of
cementless metal-backed cup prostheses using the concept of functionally graded material. Biomed. Mater., 1(3):127-33.
Heikkila, J.T., Aho, H.J., Yli-Urpo, A., Happonen, R.P. & Aho, A.J. (1995). Bone formation in rabbit cancellous bone defects filled with bioactive glass granules. Acta orthopaedica
Scandinavica, 66(5):463-467. Heikkila, J.T., Mattila, K.T., Andersson, O.H., Yli-Urpo, A. & Aho, A.J. (1995). Behaviour of
bioactive glass in human bone, In: Bioceramics 8, Hench, L.L. & Wilson, J., pp. 35-41, Elsevier Science, Oxford, U. K.
Helen, W. & Gough, JE. (2008). Cell viability, proliferation and extracellular matrix production of human annulus fibrosus cells cultured within PDLLA/Bioglass composite foam scaffolds in vitro. Acta. Biomater., 4(2): 230-43.
Hench, L. (2006) 'The story of Bioglass', Journal of Materials Science: Materials in Medicine, Vol. 17, No. 11, pp. 967-978.
Hench, L.L. (1987) 'Cementless fixation', in Pizzoferrato, A., Marchetti, P.G., Ravaglioli, A. & Lee, A.J.C. (Eds.): Biomaterials and Clinical Applications, Elsevier, Amsterdam, Netherl&s, p. 23.
Hench, L.L. (1988) 'Bioactive ceramics', in Ducheyne, P. & Lemons, J. (Eds.): Bioceramics:
Materials Characteristics Versus In Vivo Behaviour, Annals of New York Academy of Sciences, New York, p. 54.
Hench, L.L. (1991) 'Bioceramics: From Concept to Clinic', Journal of the American Ceramic
Society, Vol. 74, No. 7, pp. 1487-1510. Hench, L.L. (1996) 'Biomaterials Science: An Introduction to Materials in Medicine', in
Ratner, B.D., Hoffman, A.S., Schoen, F.J. & Lemons, J.E. (Eds.), Academic Press, San Diego, p. 73.
Hench, L.L. (1998) 'Bioceramics', Journal of the American Ceramic Society, Vol. 81, No. 7, pp. 1705-1728.
www.intechopen.com

Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
101
Hench, L.L. & Andersson, Ö.H. (1993) 'Bioactive glasses', in Hench, L.L. & Wilson, J. (Eds.): An Introduction to Bioceramics Vol. 1, World Scientific Publishing, Singapore, pp. 41-62.
Hench, L.L. & Clark, A.E. (1982) 'Chapter 6: Adhesion to bone', in Williams, D.F. (Ed.): Biocompatibility of Orthopaedic Implants, CRC Press, Boca Raton, FL.
Hench, L.L. & Ethridge, E.C. (1982) Biomaterials: An interfacial approach. Academic Press, New York.
Hench, L.L. & Paschall, H.A. (1973) 'Direct chemical bond of bioactive glass-ceramic materials to bone and muscle', J Biomed Mater Res, Vol. 7, No. 3, pp. 25-42.
Hench, L.L. & Paschall, H.A. (1974) 'Histochemical responses at a biomaterial's interface', J Biomed Mater Res, Vol. 8, No. 3, pp. 49-64.
Hench, L.L., Paschall, H.A., Allen, W.C. & Piotrowski, G. (1975) 'Interfacial behavior of ceramic implants', National Bureau of Standards Special Publication, Vol. 415, pp. 19-35.
Hench, L.L. & Polak, J.M. (2002) 'Third-generation biomedical materials', Science, Vol. 295, No. 5557, pp. 1014-1017.
Hench, L.L. & Wilson, J. (1984) 'Surface-active biomaterials', Science, Vol. 226, No. 4675, pp. 630-6.
Hench, L.L., Spilman, D.B. and Nolletti, D. (1986) 'Fluoride Bioglasses (R)', in Christel, P., Meunier, A. & Lee, A.J.C. (Eds.): Biological and Biomechanical Performance of
Biomaterials, Elsevier, Amsterdam, Netherlands, pp. 99-104. Hench, L.L., Splinter, R.J., Allen, W.C. & Greenlee, T.K. (1971) 'Bonding mechanisms at the
interface of ceramic prosthetic materials', Journal of Biomedical Materials Research, Vol. 5, No. 6, pp. 117-141.
Hench, LL. (1993). Bioactive glasses. In: Hench, LL. & Wilson, J., An Introduction to
Bioceramics, World Scientific, London. Heybeli, N., Oktar, FN., Ozyazgan, S., Akkan, G. & Ozsoy, S. (2003). Low-cost antibiotic
loaded systems for developing countries. Technol. Health Care., 11(3): 207-16. Hill, R. (1996) 'An alternative view of the degradation of bioglass', Journal of Materials Science
Letters, Vol. 15, No. 13, pp. 1122-1125. Hing, K.A. (2004). Bone repair in the twenty-first century: biology, chemistry or
engineering? Philos. Transact. A Math. Phys. Eng. Sci.,362: 2821–50. Hodgson, AWE., Mueller, Y., Forster, D. & Virtanen, S. (2002). Electrochemical
characterisation of passive films on Ti alloys under simulated biological conditions. Electrochimica Acta., 47(12):1913-1923.
Holand, W., Rheinberger, V., Apel, E., Van 't Hoen, C., Holand, M., Dommann, A., Marcel, O., Corinna, M. & Ursula, GH. (2006). Clinical applications of glass-ceramics in dentistry. Journal of materials science, 17(11): 1037-1042.
Holand, W., Vogel, W., Naumann, K. & Gummel, J. (1985) 'Interface reactions between machinable bioactive glass-ceramics and bone', J Biomed Mater Res, Vol. 19, No. 3, pp. 303-12.
Hsi, C.-S., Cheng, H.-Z., Hsu, H.-J., Chen, Y.-S. & Wang, M.-C. (2007) 'Crystallization kinetics and magnetic properties of iron oxide contained 25Li2O-8MnO2-20CaO-
www.intechopen.com
Biomaterials Applications for Nanomedicine
102
2P2O5-45SiO2 glasses', Journal of the European Ceramic Society, Vol. 27, No. 10, pp. 3171-3176.
Hsiong, SX. & Mooney, DJ. (2006). Regeneration of vascularized bone. Periodontol, 41: 109–122.
Hsu, FY., Chueh, SC. & Wang, YJ. (1999). Microspheres of hydroxyapatite/reconstituted collagen as supports for osteoblast cell growth. Biomaterials, 20(20): 1931-1936.
Huang, YC., Kaigler, D., Rice, KG., Krebsbach, PH. & Mooney, DJ. (2005). Combined angiogenic and osteogenic factor delivery enhances bone marrow stromal cell-driven bone regeneration. J. Bone Miner. Res., 20: 848–857.
Hulbert, S.F., Bokros, J.C., Hench, L.L., Wilson, J. & Heimke, G. (1987) 'Ceramics in clinical applications: Past, present and future', in Vincenzini, P. (Ed.): High Tech Ceramics, Elsevier, Amsterdam, Netherlands, pp. 189-213.
Hutmacher, D., Hürzeler, MB. & Schliephake, H. (1996). A review of material properties of biodegradable and bioresorbable polymers and devices for GTR and GBR applications. International Journal of Oral and Maxillofacial Implants, 11(5): 667-678.
Hutmacher, D.W., Schantz, J.T., Lam, C.X.F., Tan, K.C. & Lim, T.C. (2007) 'State of the art and future directions of scaffold-based bone engineering from a biomaterials perspective', Journal of Tissue Engineering and Regenerative Medicine, Vol. 1, No. 4, pp. 245-260.
Ido, K., Asada, Y., Sakamoto, T., Hayashi, R. & Kuriyama, S. (2000). Radiographic evaluation of bioactive glass-ceramic grafts in postero-lateral lumbar fusion. Spinal Cord, 38(5):315-318.
Itala, A., Koort, J., Ylanen, H.O., Hupa, M. & Aro, H.T. (2003). Biologic significance of surface microroughing in bone incorporation of porous bioactive glass implants. J. Biomed. Mater. Res. A., 67(2): 496-503.
Jackson, I.T. & Yavuzer, R. (2000). Hydroxyapatite cement: an alternative for craniofacial skeletal contour refinements. British journal of plastic surgery, 53(1):24-29.
Jackson, I.T., Pellett, C. & Smith, J.M. (1983). The skull as a bone graft donor site. Annals of
plastic surgery, 11(6):527-532. Jana, C., Nisch, W. & Grimm, G. (1995). Production and characterization of thin films of
Bioverit-type glasses deposited by RF magnetron sputtering, In: Vincenzini, P., Advances in Science and Technology, Vol12 (Materials in Clinical applications). p. 257-262, Faenza: Techna
Jansen, JA., Vehof, JWM., Ruhé, PQ., Kroeze-Deutman, H., Kuboki, Y., Takita, H., Hedberg E.L. & Mikos, AG. (2005). Growth factor-loaded scaffolds for bone engineering. J. Control. Release, 101: 127–136.
Jarcho, M. (1981) 'Calcium phosphate ceramics as hard tissue prosthetics', Clin Orthop Relat
Res, No. 157, pp. 259-78. Jell, G., Notingher, I., Tsigkou, O., Notingher, P., Polak, JM., Hench, LL. & Stevens, MM.
(2008). Bioactive glass-induced osteoblast differentiation: a noninvasive spectroscopic study. J. Biomed. Mater. Res., 86(1): 31–40.
Johnson, M.W., Sullivan, S.M., Rohrer, M. & Collier, M. (1997). Regeneration of peri-implant infrabony defects using PerioGlas: a pilot study in rabbits. Int. J. Oral Maxillofac.
Implants., 12(6):835-9.
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
103
Jones, J.R. (2007) 'Bioactive ceramics and glasses', in Boccaccini, A.R. & Gough, J.E. (Eds.): Tissue Engineering Using Ceramics and Polymers Vol. 1, Woodhead Publishing Limited CRC Press, Cambridge, U. K., pp. 52-71.
Jones, J.R. (2009) 'New trends in bioactive scaffolds: The importance of nanostructure', Journal of the European Ceramic Society, Vol. 29, No. 7, pp. 1275-1281.
Jones, J.R., Gentleman, E. & Polak, J. (2007). Bioactive glass scaffolds for bone regeneration. Elements, 3(6):393–9.
Jones, JR., Tsigkou, O., Coates, EE., Stevens, MM., Polak, JM. & Hench, LL. (2007). Extracellular matrix formation and mineralization on a phosphate-free porous bioactive glass scaffold using primary human osteoblast (HOB) cells. Biomaterials, 28(9): 1653-63.
Kanczler, J.M. & Oreffo, R.O. (2008) 'Osteogenesis and angiogenesis: the potential for engineering bone', Eur Cell Mater, Vol. 15, pp. 100-14.
Kanellakopoulou, K. & Giamarellos-Bourboulis, EJ. (2000). Carrier systems for the local delivery of antibiotics in bone infections. Drugs, 59(6): 1223–32.
Kangasniemi, K. & Yti-Urpo, A. (1990) 'Biological response of glasses in the SiO2-Na2O-CaO-P2O5-B2O3 system', in Yamamuro, T., Hench, L.L. & Wilson, J. (Eds.): Handbook of
Bioactive Ceramics Vol. I, CRC Press, Boca Raton, FL, pp. 97-108. Karageorgiou, V. & Kaplan, D. (2005). Porosity of 3D biomaterial scaffolds and osteogenesis,
Biomaterials, 26: 5474–5491. Karatzas, S., Zavras, A., Greenspan, D. & Amar, S. (1999). Histologic observations of
periodontal wound healing after treatment with PerioGlas in nonhuman primates. Int. J. Periodontics Restorative Dent., 19(5):489-99.
Karlsson, K.H., Ylänen, H. & Aro, H. (2000) 'Porous bone implants', Ceramics International, Vol. 26, No. 8, pp. 897-900.
Kawanabe, K., Okada, Y., Matsusue, Y., Iida, H. & Nakamura, T. (1998). Treatment of osteomyelitis with antibiotic-soaked porous glass ceramic. The Journal of bone and
joint surgery 80(3): 527-530. Kaysinger, KK. & Ramp, WK. (1998). Extracellular pH modulates the activity of cultured
human osteoblasts. Cell Biochem., 68: 83-89 Keshaw, H., Forbes, A. & Day, Richard M. (2005). Release of angiogenic growth factors
from cells encapsulated in alginate beads with bioactive glass. Biomaterials, 26(19): 4171-4179
Kinnunen, I., Aitasalo, K., Pollonen, M. & Varpula, M. (2000). Reconstruction of orbital floor fractures using bioactive glass. J. Craniomaxillofac. Surg., 28(4):229-234.
Kitsugi, T., Yamamuro, T. & Kokubo, T. (1989) 'Bonding behavior of a glass-ceramic containing apatite and wollastonite in segmental replacement of the rabbit tibia under load-bearing conditions', J Bone Joint Surg Am, Vol. 71, No. 2, pp. 264-72.
Klein, M., Goetz, H., Pazen, S., Al-Nawas, B., Wagner, W. & Duschner, H. (2009) 'Pore characteristics of bone substitute materials assessed by microcomputed tomography', Clinical Oral Implants Research, Vol. 20, No. 1, pp. 67-74.
Klongnoi, B., Rupprecht, S., Kessler, P., Thorwarth, M., Wiltfang, J. & Schlegel, KA. (2006). Influence of platelet-rich plasma on a bioglass and autogenous bone in sinus augmentation. An explorative study. Clin. Oral. Implants Res., 17(3):312-20.
www.intechopen.com
Biomaterials Applications for Nanomedicine
104
Knapp, C.I., Feuille, F., Cochran, D.L. & Mellonig, J.T. (2003). Clinical and histologic evaluation of bone-replacement grafts in the treatment of localized alveolar ridge defects. Part 2: bioactive glass particulate. Int. J. Periodontics Restorative Dent., 23(2):129-37.
Kohlhauser, C., Hellmich, C., Vitale-Brovarone, C., Boccaccini, A.R., Rota, A. & Eberhardsteiner, J. (2009) 'Ultrasonic Characterisation of Porous Biomaterials Across Different Frequencies', Strain, Vol. 45, No. 1, pp. 34-44.
Kokubo, T., Ito, S., Sakka, S. & Yamamuro, T. (1986) 'Formation of a high-strength bioactive glass-ceramic in the system MgO-CaO-SiO2-P2O5', Journal of Materials Science, Vol. 21, No. 2, pp. 536-540.
Kokubo, T., Shigematsu, M., Nagashima, Y., Tashiro, M., Nakamura, T., Yamamuro, T. & Higashi, S. (1982) 'Apatite- and wollastonite-containg glass-ceramics for prosthetic application', Bulletin of the Institute for Chemical Research, Kyoto University, Vol. 60, No. 3-4, pp. 260-268.
Kundu, B., Nandi, SK., Dasgupta, S., Datta, S., Mukherjee, P., Roy, S., Singh, AK., Mandal, TK., Das, P., Bhattacharya, R. & Basu, D. (2011). Macro-to-micro porous special bioactive glass and ceftriaxone-sulbactam composite drug delivery system for treatment of chronic osteomyelitis: an investigation through in vitro and in vivo animal trial. J. Mater. Sci. Mater. Med., 22(3):705-20.
Lacefield, WR. & Hench, LL. (1986). The bonding of Bioglass to a cobalt-chromium surgical implant alloy. Biomaterials, 7(2): 104-8.
Langer, R. (1980). Polymeric delivery systems for controlled drug release. Chemical
Engineering Communications, 6(1-3): 1-48. Langer, R. (1990). New methods of drug delivery. Science, 249(4976): 1527-1533. Langer, R. & Vacanti, JP. (1993). Tissue Engineering. Science, 260(5110): 920-926 Larsson, C., Thomsen, P., Aronsson, BO., Rodahl, M., Lausmaa, J., Kasemo, B. & Ericson, LE.
(1996). Bone response to surface-modified titanium implants: studies on the early tissue response to machined and electropolished implants with different oxide thicknesses. Biomaterials, 17: 605-616.
Lasserre, A. & Bajpai, PK. (1998). Ceramic drug-delivery devices. Critical reviews in
therapeutic drug carrier systems, 15(1): 1-56. Leach, JK., Kaigler, D., Wang, Z., Krebsbach, PH. & Mooney, DJ. (2006). Coating of VEGF-
releasing scaffolds with bioactive glass for angiogenesis and bone regeneration, Biomaterials, 27: 3249–3255.
Leonetti, J.A, Rambo, H.M. & Throndson, R.R. (2000). Osteotome sinus elevation and implant placement with narrow size bioactive glass. Implant dentistry, 9(2):177-182.
Leu, A., Stieger, S.M., Dayton, P., Ferrara, K.W. & Leach. J.K. (2009). Angiogenic response to bioactive glass promotes bone healing in an irradiated calvarial defect. Tissue Eng.
Part A, 15(4):877-85. Li, M., Zhang, R., Wang, J. & Yang, S. (2007). Study of different biocomposite coatings on Ti
alloy by a subsonic thermal spraying technique. Biomed. Mater., 2(1): 1-5. Lin, F.-H., Huang, Y.-Y., Hon, M.-H. & Wu, S.-C. (1991) 'Fabrication and biocompatibility of
a porous bioglass ceramic in a Na2O-CaO-SiO2-P2O5 system', Journal of Biomedical
Engineering, Vol. 13, No. 4, pp. 328-334.
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
105
Linati, L., Lusvardi, G., Malavasi, G., Menabue, L., Menziani, M.C., Mustarelli, P. & Segre, U. (2005) 'Qualitative and quantitative structure-property relationships analysis of multicomponent potential bioglasses', The Journal of Physical Chemistry B, Vol. 109, No. 11, pp. 4989-4998
Liu, A., Hong, Z., Zhuang, X., Chen, X., Cui, Y., Liu, Y. & Jing, X. (2008) 'Surface modification of bioactive glass nanoparticles and the mechanical and biological properties of poly(l-lactide) composites', Acta Biomaterialia, Vol. 4, No. 4, pp. 1005-1015.
Liu, X., Huang, W., Fu, H., Yao, A., Wang, D., Pan, H. & Lu, W. (2009a) 'Bioactive borosilicate glass scaffolds: improvement on the strength of glass-based scaffolds for tissue engineering', Journal of Materials Science: Materials in Medicine, Vol. 20, No. 1, pp. 365-372.
Liu, X., Huang, W., Fu, H., Yao, A., Wang, D., Pan, H., Lu, W., Jiang, X. & Zhang, X. (2009b) 'Bioactive borosilicate glass scaffolds: in vitro degradation and bioactivity behaviors', Journal of Materials Science: Materials in Medicine, Vol. 20, No. 6, pp. 1237-1243.
Livingston, T., Ducheyne, P. & Garino, J. (2002). In vivo evaluation of a bioactive scaffold for bone tissue engineering. J. Biomed. Mater. Res., 62(1): 1-13.
Lockyer, M.W.G., Holland, D. & Dupree, R. (1995) 'NMR investigation of the structure of some bioactive and related glasses', Journal of Non-Crystalline Solids, Vol. 188, No. 3, pp. 207-219.
Lopez-Esteban, S., Saiz, E., Fujino, S., Oku, T., Suganuma, K. & Tomsia, AP. (2003). Bioactive glass coatings for orthopedic metallic implants. J. Eur. Ceram. Soc., 23(15): 2921-2930.
Loty, C., Sautier, J.M., Tan, M.T., Oboeuf, M., Jallot, E., Boulekbache, H., Greenspan, D. & Forest, N. (2001) 'Bioactive glass stimulates in vitro osteoblast differentiation and creates a favorable template for bone tissue formation', Journal of Bone and Mineral
Research, Vol. 16, No. 2, pp. 231-239. Lovelace, T.B., Mellonig, J.T., Meffert, R.M., Jones, A.A., Nummikoski, P.V. & Cochran, D.L.
(1998). Clinical evaluation of bioactive glass in the treatment of periodontal osseous defects in humans. Journal of periodontology, 69(9):1027-1035.
Low, S.B., King, C.J. & Krieger, J. (1997). An evaluation of bioactive ceramic in the treatment of periodontal osseous defects. The International journal of periodontics and restorative
dentistry, 17(4):358-367. Lu, H.H., El-Amin, S.F., Scott, K.D. & Laurencin, C.T. (2003) 'Three-dimensional, bioactive,
biodegradable, polymer–bioactive glass composite scaffolds with improved mechanical properties support collagen synthesis and mineralization of human osteoblast-like cells in vitro', Journal of Biomedical Materials Research Part A, Vol. 64A, No. 3, pp. 465-474.
Lu, HH., Tang, A., Oh, SC, Spalazzi, JP. & Dionisio, K. (2005). Compositional effects on the formation of a calcium phosphate layer and the response of osteoblast-like cells on polymer-bioactive glass composites. Biomaterials, 26(32): 6323-34.
www.intechopen.com

Biomaterials Applications for Nanomedicine
106
Luciani, A., Coccoli, V., Orsi, S., Ambrosio, L. & Netti, PA. (2008). PCL microspheres based functional scaffolds by bottom-up approach with predefined microstructural properties and release profiles. Biomaterials, 29(36):4800-4807.
Mader, JT., Landon, GC. & Calhoun, J. (1993). Antimicrobial treatment of osteomyelitis. Clin.
Orthop. Relat. Res., 295: 87–95. Mahmood, J., Takita, H., Ojima, Y., Kobayashi, M., Kohgo, T. & Kuboki, Y. (2001) 'Geometric
Effect of Matrix upon Cell Differentiation: BMP-Induced Osteogenesis Using a New Bioglass with a Feasible Structure', Journal of Biochemistry, Vol. 129, No. 1, pp. 163-171.
Malafaya, PB., Santos, TC., Van Griensven, M. & Reis, RL. (2008). Morphology, mechanical characterization and in vivo neo-vascularization of chitosan particle aggregated scaffolds architectures. Biomaterials, 29(29): 3914-3926.
Mankin, H.J., Fogelson, F.S., Thrasher, Z.A. & Jaffer, F. (1976). Massive resection and allograft transplantation in the treatment of malignant bone tumours. N. Engl. J.
Med., 294: 1247-1250. Manson, P.N., Crawley, W.A. & Hoopes, J.E. (1986). Frontal cranioplasty: risk factors and
choice of cranial vault reconstructive material. Plastic and reconstructive surgery, 77(6):888-904.
Mantsos, T., Chatzistavrou, X., Roether, J.A., Hupa, L., Arstila, H. & Boccaccini, A.R. (2009) 'Non-crystalline composite tissue engineering scaffolds using boron-containing bioactive glass and poly(D,L-lactic acid) coatings', Biomed Mater, Vol. 4, No. 5, p. 055002.
Marciani, R.D., Gonty, A.A., Giansanti, J.S. & Avila, J. (1977). Autogenous cancellous marrow bone graft in irradiated (i) long mandibles. Oral. Surg., 43: 365-368.
Mardare, CC., Mardare, AI., Fernandes, JR. & Joanni, ED. (2003). Imposition of bioactive glass-ceramic thin-films by RF magnetron sputtering. J. European. Ceram. Soc., 23:1027–1030.
Marelli, B., Ghezzi, C.E., Barralet, J.E., Boccaccini, A.R. & Nazhat, S.N. (2010). Three-dimensional mineralization of dense nanofibrillar collagen-bioglass hybrid scaffolds. Biomacromolecules, 11(6):1470-9.
McCarthy, R.E., Peek, R.D., Morrissy, R.T. & Hough, Jr A.J. (1986). Allograft bone in spinal fusion for paralytic scoliosis. J. Bone Joint Surg. Am., 68: 370—5.
Meffert, R.M., Thomas, J.R., Hamilton, K.M. & Brownstein, C.N. (1985). Hydroxylapatite as an alloplastic graft in the treatment of human periodontal osseous defects. Journal of
periodontology, 56(2):63-73. Meinert, K., Uerpmann, C., Matschullat, J. & Wolf, GK. (1998). Corrosion and leaching of
silver doped ceramic IBAD coatings on SS 316L under simulated physiological conditions. Surface and Coatings Technology, 103-104: 58-65.
Mengel, R., Schreiber, D. & Flores-de-Jacoby, L. (2006). Bioabsorbable membrane and bioactive glass in the treatment of intrabony defects in patients with generalized aggressive periodontitis: results of a 5-year clinical & radiological study. J.
Periodontol., 77(10):1781-7. Meseguer-Olmo, L., Ros-Nicolás, M., Vicente-Ortega, V., Alcaraz-Baños, M., Clavel-Sainz,
M., Arcos, D., Ragel, C., Vallet-Regí, M. & Meseguer-Ortiz, C. (2006). A bioactive
www.intechopen.com

Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
107
sol-gel glass implant for in vivo gentamicin release. Experimental model in Rabbit. Journal of Orthopaedic Research, 24: 454–460.
Middleton, E.T., Rajaraman, C.J., O’Brien, D.P., Doherty, S.M. & Taylor, A.D. (2008). The safety and efficacy of vertebroplasty using Cortoss cement in a newly established vertebroplasty service. Br. J. Neurosurg., 22:252–6.
Miguel, B.S., Kriauciunas, R., Tosatti, S., Ehrbar, M., Ghayor, C., Textor, M. & Weber, F.E. (2010) 'Enhanced osteoblastic activity and bone regeneration using surface-modified porous bioactive glass scaffolds', Journal of Biomedical Materials Research
Part A, Vol. 94A, No. 4, pp. 1023-1033. Miliauskaite, A., Selimovic, D. & Hannig, M. (2007). Successful management of aggressive
periodontitis by regenerative therapy: a 3-year follow-up case report. J. Periodontol., 78(10):2043-50.
Milosev, I., Metikos-Hukovic, M. & Strehblow, HH. (2000). Passive film on orthopaedic TiAlV alloy formed in physiological solution investigated by X-ray photoelectron spectroscopy. Biomaterials, 21(20): 2103-2113.
Misra, S.K., Ansari, T., Mohn, D., Valappil, S.P., Brunner, T.J., Stark, W.J., Roy, I., Knowles, J.C., Sibbons, P.D., Jones, E.V., Boccaccini, A.R. & Salih, V. (2010a) 'Effect of nanoparticulate bioactive glass particles on bioactivity and cytocompatibility of poly(3-hydroxybutyrate) composites', Journal of The Royal Society Interface, Vol. 7, No. 44, pp. 453-465.
Misra, S.K., Ansari, T.I., Valappil, S.P., Mohn, D., Philip, S.E., Stark, W.J., Roy, I., Knowles, J.C., Salih, V. & Boccaccini, A.R. (2010b) 'Poly(3-hydroxybutyrate) multifunctional composite scaffolds for tissue engineering applications', Biomaterials, Vol. 31, No. 10, pp. 2806-2815.
Misra, S.K., Mohn, D., Brunner, T.J., Stark, W.J., Philip, S.E., Roy, I., Salih, V., Knowles, J.C. & Boccaccini, A.R. (2008) 'Comparison of nanoscale and microscale bioactive glass on the properties of P(3HB)/Bioglass® composites', Biomaterials, Vol. 29, No. 12, pp. 1750-1761.
Misra, S.K., Valappil, S.P., Roy, I. & Boccaccini, A.R. (2006) 'Polyhydroxyalkanoate (PHA)/Inorganic Phase Composites for Tissue Engineering Applications', Biomacromolecules, Vol. 7, No. 8, pp. 2249-2258.
Mistry, S., Kundu, D., Datta, S. & Basu, D. (2011). Comparison of bioactive glass coated and hydroxyapatite coated titanium dental implants in the human jaw bone. Australian
Dental Journal, 56: 68–75. Mohamad Yunos, D., Bretcanu, O. & Boccaccini, A. (2008) 'Polymer-bioceramic composites
for tissue engineering scaffolds', Journal of Materials Science, Vol. 43, No. 13, pp. 4433-4442.
Mohn, D., Zehnder, M., Imfeld, T. & Stark, W.J. (2010). Radio-opaque nanosized bioactive glass for potential root canal application: evaluation of radiopacity, bioactivity and alkaline capacity. Int. Endod. J., 43(3):210-7.
Moimas, L., Biasotto, M., Di Lenarda, R., Olivo, A. & Schmid, C. (2006). Rabbit pilot study on the resorbability of three-dimensional bioactive glass fibre scaffolds. Acta
biomaterialia Mar., 2(2):191-199.
www.intechopen.com
Biomaterials Applications for Nanomedicine
108
Moimas, L., Biasotto, M., Lenarda, R.D., Olivo, A. & Schmid, C. (2006) 'Rabbit pilot study on the resorbability of three-dimensional bioactive glass fibre scaffolds', Acta
Biomaterialia, Vol. 2, No. 2, pp. 191-199. Moreira-Gonzalez, A., Lobocki, C., Barakat, K., Andrus, L., Bradford, M., Gilsdorf, M. &
Jackson, IT. (2005). Evaluation of 45S5 bioactive glass combined as a bone substitute in the reconstruction of critical size calvarial defects in rabbits. J. Craniofac. Surg. 16(1): 63-70.
Muller, W. (1890). Zur frage der tempoaren schadelresektion an stele der trepanation. Zentralbl. Chir., 4:65.
Munukka, E., Leppäranta, O., Korkeamäki, M., Vaahtio, M., Peltola, T., Zhang, D., Hupa, L., Ylänen, H., Salonen, J., Viljanen, M. & Eerola, E. (2008) 'Bactericidal effects of bioactive glasses on clinically important aerobic bacteria', Journal of Materials
Science: Materials in Medicine, Vol. 19, No. 1, pp. 27-32. Mylonas, D., Vidal, M.D., De Kok, I.J., Moriarity, J.D. & Cooper, L.F. (2007). Investigation of
a thermoplastic polymeric carrier for bone tissue engineering using allogeneic mesenchymal stem cells in granular scaffolds. J. Prosthodont., 16(6):421-30.
Naber, C.L., Reid, O.M. & Hammer, J.E. III. (1972). Gross and histologic evaluation of an autogenous bone graft. 57th month post operatively. J. Periodontal., 43: 702.
Nakamura, T., Yamamuro, T., Higashi, S., Kokubo, T. & Itoo, S. (1985) 'A new glass-ceramic for bone replacement: evaluation of its bonding to bone tissue', J Biomed Mater Res, Vol. 19, No. 6, pp. 685-98.
Nandi, S.K., Kundu, B., Datta, S., De, D.K. & Basu, D. (2009) 'The repair of segmental bone defects with porous bioglass: An experimental study in goat', Research in Veterinary
Science, Vol. 86, No. 1, pp. 162-173. Nandi, SK., Kundu, B., Mukherjee, P., Mandal, TK., Datta, S., De, DK. & Basu, D. (2009). In
vitro and in vivo release of cefuroxime axetil from bioactive glass as an implantable delivery system in experimental osteomyelitis. Ceram. Int., 35(8): 3207-3216.
Neo, M., Nakamura, T., Ohtsuki, C., Kasai, R., Kokubo, T. & Yamamuro, T. (1994). Ultrastructural study of the A-W GC-bone interface after long-term implantation in rat and human bone. Journal of biomedical materials research, 28(3):365-372.
Neo, M., Nakamura, T., Ohtsuki, C., Kokubo, T. & Yamamuro, T. (1993). Apatite formation on three kinds of bioactive material at an early stage in vivo: a comparative study by transmission electron microscopy. Journal of biomedical materials research,
27(8):999-1006. Nickell, W.B., Jurkiewicz, M.J. & Salyer, K.E. (1972). Repair of skull defects with autogenous
bone. Arch. Surg., 105(3):431-433. Nicoll Steven, B., Radin, S., Santos, EM., Tuan, RS. & Ducheyne, P. (1997). In vitro release
kinetics of biologically active transforming growth factor -β1 from a novel porous glass carrier. Biomaterials, 18 (12): 853-859
Norton, M.R. & Wilson, J. (2002). Dental implants placed in extraction sites implanted with bioactive glass: human histology and clinical outcome. The International journal of
oral and maxillofacial implants, 17(2):249-257.
www.intechopen.com

Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
109
Ochoa, I., Sanz-Herrera, J.A., GarcÃa-Aznar, J.M., Doblaré, M., Yunos, D.M. & Boccaccini, A.R. (2009) 'Permeability evaluation of 45S5 Bioglass®-based scaffolds for bone tissue engineering', Journal of Biomechanics, Vol. 42, No. 3, pp. 257-260.
O'Donnell, M.D. & Hill, R.G. (2010) 'Influence of strontium and the importance of glass chemistry and structure when designing bioactive glasses for bone regeneration', Acta Biomaterialia, Vol. 6, No. 7, pp. 2382-2385.
Ohtsuki, C., Kushitani, H., Kokubo, T., Kotani, S. & Yamamuro, T. (1991). Apatite formation on the surface of Ceravital-type glass-ceramic in the body. Journal of biomedical
materials research, 25(11):1363-1370. Olding, T., Sayer, M. & Barrow, D. (2001) 'Ceramic sol-gel composite coatings for electrical
insulation', Thin Solid Films, Vol. 398-399, pp. 581-586. Oliveira, A.L., Mano, J.F. & Reis, R.L. (2003) 'Nature-inspired calcium phosphate coatings:
present status and novel advances in the science of mimicry', Current Opinion in
Solid State and Materials Science, Vol. 7, No. 4-5, pp. 309-318. Pajamaki, K.J., Andersson, O.H., Lindholm, T.S., Karlsson, K.H. & Yli-Urpo, A. (1993).
Induction of new bone by allogeneic demineralized bone matrix combined to bioactive glass composite in the rat. Annales chirurgiae et gynaecologiae, 207:137-143.
Pajamaki, K.J., Andersson, O.H., Lindholm, T.S., Karlsson, K.H., Yli-Urpo, A. & Happonen, R.P. (1993). Effect of bovine bone morphogenetic protein and bioactive glass on demineralized bone matrix grafts in the rat muscular pouch. Annales chirurgiae et
gynaecologiae, 207:155-161. Palussiere, J., Berge, J., Gangi, A., Cotton, A., Pasco, A., Bertagnoli, R., Hans, J., Paolo, C. &
Hervé, D. (2005). Clinical results of an open prospective study of a bis-GMA composite in percutaneous vertebral augmentation. Eur. Spine J., 14: 982–91.
Pan, H.B., Zhao, X.L., Zhang, X., Zhang, K.B., Li, L.C., Li, Z.Y., Lam, W.M., Lu, W.W., Wang, D.P., Huang, W.H., Lin, K.L. & Chang, J. (2010) 'Strontium borate glass: potential biomaterial for bone regeneration', Journal of The Royal Society Interface, Vol. 7, No. 48, pp. 1025-1031.
Patka, P., Haarman, H.J. & Bakker, F.C. (1998). Bone transplantation and bone replacement materials. Ned. Tijdschr. Geneeskd.,142: 893–6.
Peltola, M., Suonpaa, J., Aitasalo, K., Maattanen, H., Andersson, O., Yli-Urpo, A. & Laippala, P. (2000). Experimental follow-up model for clinical frontal sinus obliteration with bioactive glass (S53P4). Acta. Otolaryngol Suppl 543: 167-169.
Peltola, MJ., Suonpaa, JT., Andersson, H., Maattanen, HS., Aitasalo, KM., Yli-Urpo, A. & Laippala, PJ. (2000). In vitro model for frontal sinus obliteration with bioactive glass S53P4. Journal of Biomedical Materials Research, 53(2): 161-166.
Phan, PV., Grzanna, M., Chu, J., Polotsky, A., El-Ghannam, A., Van Heerden, D., Hungerford, DS. & Frondoza, CG. (2003). The effect of silica-containing calcium-phosphate particles on human osteoblasts in vitro. J. Biomed Mater. Res, A. 67(3): 1001-8
Queiroz, AC., Santos, JD., Monteiro, FJ., Gibson, IR. & Knowles, JC. (2001). Adsorption and release studies of sodium ampicillin from hydroxyapatite and glass-reinforced hydroxyapatite composites. Biomaterials, 22 (11): 1393-1400
www.intechopen.com

Biomaterials Applications for Nanomedicine
110
Quinones, C.R. & Lovelace, T.B. (1997). Utilization of a bioactive synthetic particulate for periodontal therapy & bone augmentation techniques. Pract. Periodont. Aesthet.
Dent., 9:1-7. Radha, G. & Ashok, K. (2008) 'Bioactive materials for biomedical applications using sol-gel
technology', Biomedical Materials, Vol. 3, No. 3, p. 034005. Radice, S., Kern, P., Bürki, G., Michler, J. & Textor, M. (2007). Electrophoretic deposition of
zirconia-Bioglass composite coatings for biomedical implants. J. Biomed. Mater. Res.
A, 82(2): 436-44. Rainer, A., Giannitelli, S.M., Abbruzzese, F., Traversa, E., Licoccia, S. & Trombetta, M. (2008)
'Fabrication of bioactive glass-ceramic foams mimicking human bone portions for regenerative medicine', Acta Biomaterialia, Vol. 4, No. 2, pp. 362-369.
Ramp, WK., Lenz, LG. & Kaysinger, KK. (1994). Medium pH modulates matrix, mineral, and energy metabolism in cultured chick bones and osteoblast-like cells. Bone
Miner., 24(1): 59-73. Ray, N.H. (1978) Inorganic Polymers. Academic Press, London. Reck, R. (1981). Tissue reactions to glass ceramics in the middle ear. Clin. Otolaryngol. Allied
Sci., 6:63–5. Reck, R. (1983). Bioactive glass ceramic: a new material in tympanoplasty. The Laryngoscope,
93(2):196-199. Renghini, C., Komlev, V., Fiori, F., Verné, E., Baino, F. & Vitale-Brovarone, C. (2009) 'Micro-
CT studies on 3-D bioactive glass-ceramic scaffolds for bone regeneration', Acta
Biomaterialia, Vol. 5, No. 4, pp. 1328-1337. Rezwan, K., Chen, Q.Z., Blaker, J.J. & Boccaccini, A.R. (2006) 'Biodegradable and bioactive
porous polymer/inorganic composite scaffolds for bone tissue engineering', Biomaterials, Vol. 27, No. 18, pp. 3413-3431.
Rivero, DP., Fox, J., Skipor, AK., Urban, RN. & Galante, JO. (1988). Calcium phosphate-coated porous titanium implants for enhanced skeletal fixation, Journal of Biomedical
Materials Research 22: 191-201. Roessler, S., Zimmermann, R., Scharnweber, D., Werner, C. & Worch, H. (2002).
Characterization of oxide layers on Ti6Al4V and titanium by streaming potential and streaming current measurements. Colloids and Surfaces B: Biointerfaces, 26(4): 387-395.
Roether, JA., Gough, JE., Boccaccini, AR., Hench, LL., Maquet, V. & Jérôme, R. (2002). Novel bioresorbable and bioactive composites based on bioactive glass and polylactide foams for bone tissue engineering. J. Mater. Sci. Mater. Med., 13(12): 1207-14.
Ross, N., Tacconi, L. & Miles, J.B. (2000). Heterotopic bone formation causing recurrent donor site pain following iliac crest bone harvesting. Br. J. Neurosurg., 14: 476—9.
Ryu, H.S., Seo, J.H., Kim, H., Hong, K.S., Park, H.J., Kim, D.J., Lee, J.H., Lee, D.H., Chang, B.S. & Lee, C.K. (2003) 'Bioceramics 15', Trans Tech Publications Limited, Zurich-Uetikon, p. 261.
Saino, E., Maliardi, V., Quartarone, E., Fassina, L., Benedetti, L., De Angelis, MG., Mustarelli, P., Facchini, A. & Visai, L. (2010). In vitro enhancement of SAOS-2 cell calcified matrix deposition onto radio frequency magnetron sputtered bioglass-coated titanium scaffolds. Tissue Eng. Part A., 16(3): 995-1008.
www.intechopen.com

Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
111
Saravanapavan, P., Gough, J.E., Jones, J.R. & Hench, L.L. (2003) 'Antimicrobial macroporous gel-glasses: Dissolution and cytotoxicity', Key Engineering Materials, Vol. 254-256, pp. 1087-1090.
Scala, M., Gipponi, M., Pasetti, S., Dellachá, E., Ligorio, M., Villa, G., Margarino, G., Giannini, G. & Strada, P. (2007). Clinical applications of autologous cryoplatelet gel for the reconstruction of the maxillary sinus. A new approach for the treatment of chronic oro-sinusal fistula. In Vivo., 21(3):541-7.
Schepers, E., de Clercq, M., Ducheyne, P. & Kempeneers, R. (1991). Bioactive glass particulate material as a filler for bone lesions. Journal of oral rehabilitation, 18(5):439-452.
Schnettler, R. (1997). Markgraf E. Knochenersatzmaterialen und Wachstumsfaktoren. Thieme: Stuttgart
Scotchford, C.A., Shataheri, M., Chen, P.S., Evans, M., Parsons, A.J., Aitchison, G.A., Efeoglu, C., Burke, J.L., Vikram, A., Fisher, S.E. & Rudd, C.D. (2011). Repair of calvarial defects in rats by prefabricated, degradable, long fibre composite implants. J. Biomed. Mater. Res. A., 96(1):230-8.
Seeherman, H. & Wozney, JM. (2005). Delivery of bone morphogenic proteins for orthopedic tissue regeneration. Cytokine Growth Factor Rev., 16: 329–345.
Seiler, J.G. & Johnson, J. (2000). Iliac crest autogenous bone grafting: donor site complications. J. South Orthop. Assoc., 9: 91—7.
Sepulveda, P., Jones, J.R. & Hench, L.L. (2001) 'Characterization of melt-derived 45S5 and sol-gel-derived 58S bioactive glasses', Journal of Biomedical Materials Research, Vol. 58, No. 6, pp. 734-740.
Shapoff, C.A., Alexander, D.C. & Clark, A.E. (1997). Clinical use of a bioactive glass particulate in the treatment of human osseous defects. Compend. Contin. Educ. Dent., 18(4):352–4.
Skaggs, DL., Samuelson, MA., Hale, JM., Kay, RM. & Tolo, VT. (2000). Complications of posterior iliac crest bone grafting in spine surgery in children. Spine, 25: 2400—2
Smit, R.S., van der Velde, D. & Hegeman, J.H. (2008). Augmented pin fixation with Cortoss for an unstable AO-A3 type distal radius fracture in a patient with a manifest osteoporosis. Arch. Orthop. Trauma. Surg., 128:989–93.
Smith, A.W., Yousefi, J. & Jackson, I.T. (1999). Screw fixation of methylmethacrylate in the craniofacial area. Eur J Plast Surg., 22:17-21.
Sooksaen, P., Suttiruengwong, S., Oniem, K., Ngamlamiad, K. & Atireklapwarodom, J. (2008) 'Fabrication of porous bioactive glass-ceramics via decomposition of natural fibres', Journal of Metals, Materials and Minerals, Vol. 18, No. 2, pp. 85-91.
Spaans, CJ., Belgraver, VW., Rienstra, O., de Groot, JH., Veth, RP. & Pennings, AJ. (2000). Solvent-free fabrication of micro-porous polyurethane amide and polyurethane-urea scaffolds for repair and replacement of the knee-joint meniscus. Biomaterials, 21(23): 2453-2460.
Stanley, H.R., Clark, A.E., Pameijer, C.H. & Louw. N.P. (2001). Pulp capping with a modified bioglass formula (#A68-modified). Am. J. Dent., 14(4):227-32.
Stevens, M.M. & George, J.H. (2005) 'Exploring and Engineering the Cell Surface Interface', Science, Vol. 310, No. 5751, pp. 1135-1138.
www.intechopen.com
Biomaterials Applications for Nanomedicine
112
Stevenson, S. & Horowitz, M. (1992). The response to bone allografts. J. Bone Joint Surg. Am., 74:939–50.
Strnad, Z. (1992) 'Role of the glass phase in bioactive glass-ceramics', Biomaterials, Vol. 13, No. 5, pp. 317-321.
Summers, B.N. & Eisenstein, S.M. (1989). Donor site pain from the ilium: a complication of lumbar spine fusion. J. Bone Joint Surg. Br., 71-B: 677—80.
Suominen, E. & Kinnunen, J. (1996). Bioactive glass granules and plates in the reconstruction of defects of the facial bones. Scandinavian journal of plastic and reconstructive surgery. Nordisk plastikkirurgisk forening and Nordisk klubb for handkirurgi, 30(4):281-289.
Suonpaa. J., Sipila, J., Aitasalo, K., Antila, J. & Wide, K. (1997). Operative treatment of frontal sinusitis. Acta Otolaryngol. Suppl., 529:181-183.
Sy, I.P. (2002). Alveolar ridge preservation using a bioactive glass particulate graft in extraction site defects. General dentistry, 50(1):66-68.
Taboas, J.M., Maddox, R.D., Krebsbach, P.H. & Hollister, S.J. (2003) 'Indirect solid free form fabrication of local and global porous, biomimetic and composite 3D polymer-ceramic scaffolds', Biomaterials, Vol. 24, No. 1, pp. 181-194.
Tadjoedin, E.S., de Lange, G.L., Lyaruu, D.M., Kuiper, L. & Burger, E.H. (2002). High concentrations of bioactive glass material (BioGran) vs. autogenous bone for sinus floor elevation. Clinical oral implants research, 13(4):428-436.
Temenoff, JS. & Mikos, AG.(2000). Review: tissue engineering for regeneration of articular cartilage. Biomaterials, 21(5): 431-440.
Thomas, KA., Kay, JF., Cook, SD. & Jarcho, M. (1987). The effect of surface macrotexture & hydroxylapatite coating on the mechanical strengths and histologic profiles of titanium implant materials. Journal of Biomedical Materials Research, 21: 1395-414.
Thomas, MV., Puleo, DA. & Al-Sabbagh, M. (2005). Bioactive glass three decades on, J. Long-
Term Eff. Med. Implants, 15 (6): 585–597. Thompson, I. & Hench, L. (1998) 'Mechanical properties of bioactive glasses, glass-ceramics
and composites', Proceedings of the Institution of Mechanical Engineers, Part H: Journal
of Engineering in Medicine, Vol. 212, No. 2, pp. 127-136. Thompson, I.D. (2005) 'Biocomposites', in Hench, L.L. and Jones, J.R. (Eds.): Biomaterials,
Artificial Organs and Tissue Engineering, Woodhead Publishing Limited CRC Press, Cambridge, U. K., pp. 48-58.
Throndson, R.R. & Sexton, S.B. (2002). Grafting mandibular third molar extraction sites: a comparison of bioactive glass to a nongrafted site. Oral surgery, oral medicine, oral
pathology, oral radiology, and endodontics, 94(4):413-419. Tsigkou, O., Hench, L.L., Boccaccini, A.R., Polak, J.M. & Stevens, M.M. (2007). Enhanced
differentiation and mineralization of human fetal osteoblasts on PDLLA containing bioglass composite films in the absence of osteogenic supplements. J. Biomed. Mater.
Res. A., 80(4):837–51. Tsigkou, O., Jones, J.R., Polak, J.M. & Stevens, M.M. (2009). Differentiation of fetal
osteoblasts and formation of mineralized bone nodules by 45S5 bioglass conditioned medium in the absence of osteogenic supplements. Biomaterials, 30(21): 3542–50.
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
113
Urist, M.R. (1965). Bone: formation by autoinduction. Science,150: 893–9. Valimaki, V.V. & Aro, H.T. (2006). Molecular basis for action of bioactive glasses as bone
graft substitute. Scand. J. Surg., 95:95–102. Vallet-Regí, M., Ragel, C.V. & Salinas, Antonio J. (2003) 'Glasses with Medical Applications',
European Journal of Inorganic Chemistry, Vol. 2003, No. 6, pp. 1029-1042. Vargas, G.E., Mesones, R.V., Bretcanu, O., López, J.M.P., Boccaccini, A.R. & Gorustovich, A.
(2009) 'Biocompatibility and bone mineralization potential of 45S5 Bioglass®-derived glass-ceramic scaffolds in chick embryos', Acta Biomaterialia, Vol. 5, No. 1, pp. 374-380.
Verné, E., Fernández, Vallés C., Vitale Brovarone, C., Spriano, S. & Moisescu, C. (2004). Double-layer glass-ceramic coatings on Ti6Al4V for dental implants. J. Eur. Ceram.
Soc. 24(9): 2699-2705. Verné, E., Ferraris, M., Jana, C. & Paracchini, L. (2000). Bioverit® I base glass/Ti particulate
biocomposite: "In situ" vacuum plasma spray deposition. J. Eur. Ceram. Soc., 20(4): 473-479.
Verné, E., Ferraris, M., Ventrella, A., Paracchini, L., Krajewski, A. & Ravaglioli, A. (1998). Sintering and plasma spray deposition of bioactive glass-matrix composites for biomedical applications. J. Eur. Ceram. Soc., 18(4): 363-372.
Villacam J,H., Novaes, A.B. Jr., Souza, S.L., Taba, M. Jr., Molina, G.O. & Carvalho, T.L. (2005). Bioactive glass efficacy in the periodontal healing of intrabony defects in monkeys. Brazilian dental journal, 16(1):67-74.
Vitale Brovarone, C., Verné, E. & Appendino, P. (2006) 'Macroporous bioactive glass-ceramic scaffolds for tissue engineering', Journal of Materials Science: Materials in Medicine, Vol. 17, No. 11, pp. 1069-1078.
Vitale-Brovarone, C., Baino, F. & Verné, E. (2010) 'Feasibility and Tailoring of Bioactive Glass-ceramic Scaffolds with Gradient of Porosity for Bone Grafting', Journal of
Biomaterials Applications, Vol. 24, No. 8, pp. 693-712. Vitale-Brovarone, C., Baino, F. & Verné, E. (2009b) 'High strength bioactive glass-ceramic
scaffolds for bone regeneration', Journal of Materials Science: Materials in Medicine, Vol. 20, No. 2, pp. 643-653.
Vitale-Brovarone, C., Baino, F., Bretcanu, O. & Verné, E. (2009a) 'Foam-like scaffolds for bone tissue engineering based on a novel couple of silicate-phosphate specular glasses: synthesis and properties', Journal of Materials Science: Materials in Medicine, Vol. 20, No. 11, pp. 2197-2205.
Vitale-Brovarone, C., Miola, M., Balagna, C. & Verné, E. (2008) '3D-glass-ceramic scaffolds with antibacterial properties for bone grafting', Chemical Engineering Journal, Vol. 137, No. 1, pp. 129-136.
Vitale-Brovarone, C., Nunzio, S.D., Bretcanu, O. & Verné, E. (2004) 'Macroporous glass-ceramic materials with bioactive properties', Journal of Materials Science: Materials in
Medicine, Vol. 15, No. 3, pp. 209-217. Vitale-Brovarone, C., Vernè, E., Bosetti, M., Appendino, P. & Cannas, M. (2005)
'Microstructural and in vitro characterization of SiO2-Na2O-CaO-MgO glass-ceramic bioactive scaffolds for bone substitutes', Journal of Materials Science: Materials in
Medicine, Vol. 16, No. 10, pp. 909-917.
www.intechopen.com

Biomaterials Applications for Nanomedicine
114
Vitale-Brovarone, C., Verné, E., Robiglio, L., Appendino, P., Bassi, F., Martinasso, G., Muzio, G. & Canuto, R. (2007) 'Development of glass-ceramic scaffolds for bone tissue engineering: Characterisation, proliferation of human osteoblasts and nodule formation', Acta Biomaterialia, Vol. 3, No. 2, pp. 199-208.
Vogel, W., Hohland, W., Naumann, K., Vogel, J., Carl, G., Gotz, W. & Wange, P. (1990) 'Glass-ceramics for medicine and dentistry', in Yamamuro, T., Hench, L.L. & Wilson, J. (Eds.): Handbook of Bioactive Ceramics Vol. I, CRC Press, Boca Raton, FL, p. 353.
Vollenweider, M., Brunner, T.J., Knecht, S., Grass, R.N., Zehnder, M., Imfeld, T. & Stark, W.J. (2007) 'Remineralization of human dentin using ultrafine bioactive glass particles', Acta Biomaterialia, Vol. 3, No. 6, pp. 936-943.
Walenkamp, GHIM. (1997). Chronic osteomyelitis. Acta. Orthop. Scand., 68(5): 497–506. Wallace, K.E., Hill, R.G., Pembroke, J.T., Brown, C.J. & Hatton, P.V. (1999) 'Influence of
sodium oxide content on bioactive glass properties', Journal of Materials Science:
Materials in Medicine, Vol. 10, No. 12, pp. 697-701. Weber, R.S., Kearns, D.B. & Smith, R.J. (1987). Split calvarium cranioplasty. Archives of
otolaryngology--head and neck surgery,113(1):84-89. Webster, T.J. & Ahn, E.S. (2007) 'Nanostructured biomaterials for tissue engineering bone':
Tissue Engineering II Vol. 103, Springer, Berlin, Germany, pp. 275-308. Weiner, S. (1986). Organization of extracellularly mineralized tissues: A comparative study
of biological crystal growth. CRC Crit. Rev. Biochem., 20: 365-408. Wei-Tao, J., Xin, Z., Chang-Qing, Z., Xin, L., Wen-Hai, H., Mohamed, NR. & Day, DE. (2010).
Elution characteristics of teicoplanin-loaded biodegradable borate glass/chitosan composite. International Journal of Pharmaceutics, 387(1-2): 184-186
Wei-Tao, J., Xin, Z., Shi-Hua, L., Xin, L., Wen-Hai, H., Mohamed, NR., Day, DE., Chang-Qing, Z., Zong-Ping, X. & Jian-Qiang, W. (2010). Novel borate glass/chitosan composite as a delivery vehicle for teicoplanin in the treatment of chronic osteomyelitis. Acta Biomaterialia 6: 812–819
Wen, H.B., Moradian-Oldak, J. & Fincham, A.G. (1999). Modulation of apatite crystal growth on Bioglass by recombinant amelogenin. Biomaterials, 20(18):1717-25.
Wennerberg, A., Albrektsson, T. & Andersson, B. (1996). Bone tissue response to commercially pure titanium implants blasted with fine and coarse particles of aluminum oxide. Int. J. Oral Maxillofac. Implants, 11: 38-45.
Wheeler, DL., Montfort, MJ. & McLoughlin, SW. (2001). Differential healing response of bone adjacent to porous implants coated with hydroxyapatite and 45S5 bioactive glass. J. Biomed. Mater. Res., 55(4): 603-12.
Whitaker, L.A., Munro, I.R., Salyer, K.E., Jackson, I.T., Ortiz-Monasterio, F. & Marchac, D. (1979). Combined report of problems and complications in 793 craniofacial operations. Plastic and reconstructive surgery, 64(2):198-203.
Wilda, H. & Gough. JE. (2006). In vitro studies of annulus fibrosus disc cell attachment, differentiation and matrix production on PDLLA/45S5 Bioglass composite films. Biomaterials, 27(30): 5220-9.
www.intechopen.com
Development and Applications of Varieties of Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgery and as Drug Delivery System
115
Wilson, J. & Nolletti, D. (1990) 'Bonding of soft tissues of Bioglass (R)', in Yamamuro, T., Hench, L.L. & Wilson, J. (Eds.): Handbook of Bioactive Ceramics Vol. I, Bioactive Glasses
and Glass-Ceramics, CRC Press, Boca Raton, FL, pp. 283-302. Wilson, J., Pigott, G.H., Schoen, F.J. & Hench, L.L. (1981) 'Toxicology and biocompatibility of
bioglasses', J Biomed Mater Res, Vol. 15, No. 6, pp. 805-17. Wu, C. (2009) 'Methods of improving mechanical and biomedical properties of CaSi-based
ceramics and scaffolds', Expert Review of Medical Devices, Vol. 6, No. 3, pp. 237-241. Wu, S.C., Hsu, H.C., Hsiao, S.H. & Ho, W.F. (2009). Preparation of porous 45S5 Bioglass-
derived glass-ceramic scaffolds by using rice husk as a porogen additive. J. Mater.
Sci. Mater. Med., 20(6):1229-36. Wu, TJ., Huang, HH., Lan, CW., Lin, CH., Hsu, FY. & Wang, YJ. (2004). Studies on the
microspheres comprised of reconstituted collagen and hydroxyapatite. Biomaterials, 25(4): 651-658.
Xia, W. & Chang, J. (2006). Well-ordered mesoporous bioactive glasses (MBG): A promising bioactive drug delivery system. Journal of Controlled Release, 110(3): 522-530
Xie, XH., Yu, XW., Zeng, SX., Du, RL., Hu, YH., Yuan, Z., Lu, EY., Dai, KR. & Tang, TT. (2010). Enhanced osteointegration of orthopaedic implant gradient coating composed of bioactive glass and nanohydroxyapatite. J. Mater. Sci. Mater. Med., 21(7): 2165-73.
Xin, Z., WeiTao, J., YiFei, G., Wei, X., Xin, L., DePing, W., ChangQing, Z., WenHai, H., Mohamed, NR., Day, DE. & Nai, Z. (2010). Teicoplanin-loaded borate bioactive glass implants for treating chronic bone infection in a rabbit tibia osteomyelitis model. Biomaterials 31(22): 5865-5874
Xu, C., Su, P., Chen, X., Meng, Y., Yu, W., Xiang, A.P. & Wang, Y. (2011). Biocompatibility and osteogenesis of biomimetic Bioglass-Collagen-Phosphatidylserine composite scaffolds for bone tissue engineering. Biomaterials, 32(4):1051-8.
Xu, C., Su, P., Wang, Y., Chen, X., Meng, Y., Liu, C., Yu, X., Yang, X., Yu, W., Zhang, X. & Xiang, A.P. (2010). A novel biomimetic composite scaffold hybridized with mesenchymal stem cells in repair of rat bone defects models. J. Biomed. Mater. Res.
A., 95(2):495-503. Xynos, ID., Hukkanen, MV., Batten, JJ., Buttery, LD., Hench, LL. & Polak, JM. (2000).
Bioglass 45S5 stimulates osteoblast turnover and enhances bone formation In vitro: implications and applications for bone tissue engineering. Calcif. Tissue Int., 67(4): 321-9.
Yamamuro, T., Hench, L.L. & Wilson, J. (1990a) Bioactive glasses and glass-ceramics Vol. I. CRC Press, Boca Raton, FL.
Yamamuro, T., Hench, L.L. & Wilson, J. (1990b) Calcium phosphate and hydroxylapatite ceramics
Vol. II. CRC Press, Boca Raton, FL. Yamamuro, T., Shikata, J., Kakutani, Y., Yoshii, S., Kitsugi, T. & Ono, K. (1988) 'Novel
methods for clinical applications of bioactive ceramics', in Ducheyne, P. and Lemons, J.E. (Eds.): Bioceramics: Material Characteristics Versus In Vivo Behaviour, Annals of New York Academy of Sciences, New York, p. 107.
www.intechopen.com
Biomaterials Applications for Nanomedicine
116
Yang, S., Leong, K.-F., Du, Z. & Chua, C.-K. (2001) 'The Design of Scaffolds for Use in Tissue Engineering. Part I. Traditional Factors', Tissue Engineering, Vol. 7, No. 6, pp. 679-689.
Yang, S., Leong, K.-F., Du, Z. & Chua, C.-K. (2002) 'The Design of Scaffolds for Use in Tissue Engineering. Part II. Rapid Prototyping Techniques', Tissue Engineering, Vol. 8, No. 1, pp. 1-11.
Yang, XB., Webb, D., Blaker, J., Boccaccini, AR., Maquet, V., Cooper, C. & Oreffo, RO. (2006). Evaluation of human bone marrow stromal cell growth on biodegradable polymer/bioglass composites. Biochem. Biophys. Res. Commun., 342(4): 1098-107.
Yılmaz, S., Ipek, M., Celebi, GF. & Bindal, C. (2005). The effect of bond coat on mechanical properties of plasma-sprayed Al2O3 and Al2O3-13 wt% TiO2 coatings on AISI 316L stainless steel. Vacuum, 77(3): 315-321.
Yoshii, S., Kakutani, Y., Yamamuro, T., Nakamura, T., Kitsugi, T., Oka, M., Kokubo, T. & Takagi, M. (1988) 'Strength of bonding between A-W glass-ceramic and the surface of bone cortex', J Biomed Mater Res, Vol. 22, No. 3 Suppl, pp. 327-38.
Younger, E.M. & Chapman, M.W. (1989). Morbidity at bone graft donor sites. J. Orthop.
Trauma., 3: 192–5. Yue, TM., Yu, JK., Mei, Z. & Man, HC. (2002). Excimer laser surface treatment of Ti-6Al-4V
alloy for corrosion resistance enhancement. Materials Letters, 52(3): 206-212. Yukna, R.A., Evans, G.H., Aichelmann-Reidy, M.B. & Mayer, E.T. (2001). Clinical
comparison of bioactive glass bone replacement graft material and expanded polytetrafluoroethylene barrier membrane in treating human mandibular molar class II furcations. J. Periodontol., 72(2):125-33.
Yun, H.-s., Kim, S.-e. & Hyeon, Y.-t. (2007) 'Design and preparation of bioactive glasses with hierarchical pore networks', Chemical Communications, No. 21, pp. 2139-2141.
Zaffe, D., Bertoldi, C. & Consolo, U. (2003). Element release from titanium devices used in oral and maxillofacial surgery. Biomaterials, 24(6): 1093-1099.
Zamet, J.S., Darbar, U.R., Griffiths, G.S., Bulman, J.S., Brägger, U., Bürgin, W. & Newman, H.N. (1997). Particulate bioglass as a grafting material in the treatment of periodontal intrabony defects. J. Clin. Periodontol., 24(6):410-8.
Zhang, J., Wang, M., Cha, JM. & Mantalaris, A. (2009). The incorporation of 70s bioactive glass to the osteogenic differentiation of murine embryonic stems cells in 3D bioreactors. J. Tissue Eng. Regen. Med. 3(1): 63-71.
Zhao, L., Yan, X., Zhou, X., Zhou, L., Wang, H., Tang, J. & Yu, C. (2008). Mesoporous bioactive glasses for controlled drug release. Microporous and Mesoporous Materials, 109(1-3): 210-215
Zhu Yufang & Kaskel Stefan. 2009. Comparison of the in vitro bioactivity and drug release property of mesoporous bioactive glasses (MBGs) and bioactive glasses (BGs) scaffolds. Microporous and Mesoporous Materials. 118 (1-3): 176-182
Zietek, M., Radwan-Oczko, M., Konopka, T. & Kozłowski, Z. (1998). Use of the BIOGRAN preparation in surgical treatment of periodontal disease. Polim. Med., 28(3-4):63-9.
Zongping, Xie., Xin, Liu., Weitao, Jia., Changqing, Z., Wenhai, H. & Jianqiang, W. 2009. Treatment of osteomyelitis and repair of bone defect by degradable bioactive borate glass releasing vancomycin. Journal of Controlled Release, 139(2): 118-126
www.intechopen.com

Biomaterials Applications for NanomedicineEdited by Prof. Rosario Pignatello
ISBN 978-953-307-661-4Hard cover, 458 pagesPublisher InTechPublished online 16, November, 2011Published in print edition November, 2011
InTech EuropeUniversity Campus STeP Ri Slavka Krautzeka 83/A 51000 Rijeka, Croatia Phone: +385 (51) 770 447 Fax: +385 (51) 686 166www.intechopen.com
InTech ChinaUnit 405, Office Block, Hotel Equatorial Shanghai No.65, Yan An Road (West), Shanghai, 200040, China
Phone: +86-21-62489820 Fax: +86-21-62489821
These contribution books collect reviews and original articles from eminent experts working in theinterdisciplinary arena of biomaterial development and use. From their direct and recent experience, thereaders can achieve a wide vision on the new and ongoing potentialities of different synthetic and engineeredbiomaterials. Contributions were selected not based on a direct market or clinical interest, but on resultscoming from a very fundamental studies. This too will allow to gain a more general view of what and how thevarious biomaterials can do and work for, along with the methodologies necessary to design, develop andcharacterize them, without the restrictions necessary imposed by industrial or profit concerns. Biomaterialconstructs and supramolecular assemblies have been studied, for example, as drug and protein carriers,tissue scaffolds, or to manage the interactions between artificial devices and the body. In this volume of thebiomaterial series have been gathered in particular reviews and papers focusing on the application of new andknown macromolecular compounds to nanotechnology and nanomedicine, along with their chemical andmechanical engineering aimed to fit specific biomedical purposes.
How to referenceIn order to correctly reference this scholarly work, feel free to copy and paste the following:
Samit Kumar Nandi, Biswanath Kundu and Someswar Datta (2011). Development and Applications of Varietiesof Bioactive Glass Compositions in Dental Surgery, Third Generation Tissue Engineering, Orthopaedic Surgeryand as Drug Delivery System, Biomaterials Applications for Nanomedicine, Prof. Rosario Pignatello (Ed.),ISBN: 978-953-307-661-4, InTech, Available from: http://www.intechopen.com/books/biomaterials-applications-for-nanomedicine/development-and-applications-of-varieties-of-bioactive-glass-compositions-in-dental-surgery-third-ge