Developing a Standardized Rating System for the Face Stimulus Assessment
88
Developing a Standardized Rating System for the Face Stimulus Assessment (FSA) Using 9 Scales Adapted from the Formal Elements Art Therapy Scale (FEATS) Presented to Laura Aubé M.S., L.P.C., A.T.R.-B.C. and Marilyn Walter M.S., L.P.C., A.T.R. AVILA UNIVERSITY In partial fulfillment of the requirements for the degree of MASTER OF SCIENCE IN COUNSELING AND ART THERAPY By Michelle K. Hamilton
Transcript of Developing a Standardized Rating System for the Face Stimulus Assessment

Developing a Standardized Rating System for the Face Stimulus Assessment (FSA)
Using 9 Scales Adapted from the Formal Elements Art Therapy Scale (FEATS)
Presented to
Laura Aubé M.S., L.P.C., A.T.R.-B.C. and Marilyn Walter M.S., L.P.C., A.T.R.
AVILA UNIVERSITY
In partial fulfillment of the
requirements for the degree of
MASTER OF SCIENCE IN COUNSELING AND ART THERAPY
By
Michelle K. Hamilton

ii
For my husband
Jason Hamilton
Who stood by my side, held my hand, and encouraged me to achieve my goals
iii
ACKNOWLEDGEMENTS
Foremost, thank you Laura Aubé for your guidance and wisdom as the pioneering director of
Avila University’s graduate art therapy program. I am extremely grateful for your dedication,
support, and enthusiasm throughout this entire process.
I would like to express my sincere gratitude to Dr. Donna Betts, who not only inspired this
project, but supported me every step of the way. Your knowledge, encouragement, and sound
advice made this project possible. Your motivation and passion for art therapy is contagious.
My sincere thanks go to the FSA raters Nannie Mead and Sheila Lorenzo. Nannie, your
enthusiasm for research and you’re undying encouragement. A special thanks to my statistician
Josh Ellington, who was an integral part of this project.
Additionally, I would like to thank my professors and colleagues who offered their unending
support – especially Marilyn Walter, Molly Rush, Marilynn Demers, and Linda Blasdel. This
endeavor could not have been possible without your inspiration, wealth of knowledge, and
patience.
I wish to thank my best friend Kasey Browne, who has stuck by me every step of the way. Your
love and support has made this project possible, you inspire me to reach for the stars and remind
me to have fun along the way.
Lastly, and most importantly, I wish to thank my parents, Pam and David Kile. You raised me,
taught me, supported me, and had unrelenting faith in my abilities. There are not enough words
to thank you.

iv
TABLE OF CONTENTS
List of Tables…………………………………………………………………………………….vii
List of Figures…………………………………………………………………………………...viii
Abstract…………………………………………………………………………………………...ix
1. INTRODUCTION……………………………………………………………………………...1
Overview of the study……………………………………………………………………..1
Purpose of the Study………………………………………………………………………1
Justification of the Study………………………………………………………………….2
Research Question and Hypotheses……………………………………………………….2
Definition of Terms………………………………………………………………………..3
Conclusions………………………………………………………………………………..5
2. LITERATURE REVIEW………………………………………………………………………6
Historical Foundation of Art Therapy Assessment………………………………………..6
Art Therapy Assessments…………………………………………………………7
Limitations of Art Therapy Assessments………………………………………...11
Using the Face Stimulus Assessment……………………………………………………12
Development of the FSA………………………………………………………...12
Limitations of the FSA…………………………………………………………...17
Recommendations for Further Development of the FSA………………………..18
Using the Formal Elements Art Therapy Scale………………………………………….20
Development of the FEATS……………………………………………………...20
Limitations of the FEATS………………………………………………………..24
Recommendations for Further Development of the FEATS…………………….25

v
Conclusions………………………………………………………………………………27
3. METHODOLOGY……………………………………………………………………………28
Development of the Research……………………………………………………………28
Research Questions………………………………………………………………………28
Research Design………………………………………………………………………….28
Sample……………………………………………………………………………………29
Participants……………………………………………………………………….29
Participant Recruitment Process…………………………………………………29
Instrumentation…………………………………………………………………………..29
Materials…………………………………………………………………………29
Measuring Devices……………………………………………………………….30
Procedures………………………………………………………………………………..32
Administration of the FSA……………………………………………………….32
Rating the FSA Drawings………………………………………………………..33
Description and Justification of the Statistical Techniques Used………………………..33
Internal and External Validity ……………………………………………………………34
Ethical Concerns…………………………………………………………………………35
Conclusions………………………………………………………………………………35
4. RESULTS……………………………………………………………………………………..37
Inter-rater Reliability Results…………………………………………………………….37
Analysis of Results………………………………………………………………39
Conclusions………………………………………………………………………………44

vi
5. DISCUSSION…………………………………………………………………………………46
Research Questions………………………………………………………………………46
Inter-rater Reliability Issues……………………………………………………………...47
Limitations of the Study………………………………………………………………….48
Recommendations for Further Research…………………………………………………49
Conclusions………………………………………………………………………………49
APPENDICES…………………………………………………………………………………...51
REFERENCES…………………………………………………………………………………..75
BIOGRAPHICAL SKETCH…………………………………………………………………….79
vii
LIST OF TABLES
1. Kappa Interpretation…………………………………………………………………………..38
2. Inter-rater Reliability and Agreement…………………………………………………………39
3. Descriptive Statistics of FEATS Ratings on a Normative Sample……………………………42
4. Average Score per Scale………………………………………………………………………43
5. Mode Score per Scale…………………………………………………………………………44
6. FEATS Ratings of Modified FSA Drawing Two, Scales 1 and 2…………………………….70
7. FEATS Ratings of Modified FSA Drawing Two, Scales 3 and 6…………………………….71
8. FEATS Ratings of Modified FSA Drawing Two, Scales 7 and 9…………………………….72
9. FEATS Ratings of Modified FSA Drawing Two, Scales 10 and 11………………………….73
10. FEATS Ratings of Modified FSA Drawing Two, Scale 14………………………………….74

viii
LIST OF FIGURES
1. Gender Distribution Graph……………………………………………………………………40
2. Ethnicity Distribution Graph…………………………………………………………………..41
3. Age Distribution Scatter Plot………………………………………………………………….41
ix
ABSTRACT
The areas of art therapy research and assessment are quickly growing in size and
popularity. This research study investigated the modified Face Stimulus Assessment (FSA) in the
interest of creating a foundation from which to conduct further research to establish the FSA as a
reliable and valid art assessment tool (Betts, 2003). The study primarily investigates the use of
the modified Formal Elements Art Therapy Scale (FEATS) as a formal rating guide for the FSA
(Gantt & Tabone, 1998). The FSA is a projective drawing assessment comprised of a series of
three drawing tasks. This assessment was originally designed to be used with multicultural, child
and adolescent populations with multiple disabilities and communication problems (Betts, 2003).
Due to its fairly recent development, reliability and validity studies of the FSA have not
been conducted. In the current study, the modified FSA was administered to a sample (N = 30)
of undergraduate college students. The FSA drawings were rated independently by four trained
raters using 9 adapted scales from the FEATS. The findings identified statistically significant
results supporting the use of the modified FEATS with drawing number two of the FSA.
Findings from this study will ultimately aid in supporting application of the FSA as a useful art
therapy tool.

1
CHAPTER 1
INTRODUCTION
Overview of the Study
The Face Stimulus Assessment (FSA) was created by Donna Betts (2003) as a projective
drawing test to provide the assessor with information about the abilities of the client. The FSA
has yet to be established as a reliable and valid art therapy tool. This research paper describes an
investigation into the use of the Formal Elements Art Therapy Scale (FEATS) (Gantt & Tabone,
1998) as a formal rating and scoring instrument to be used with the FSA, in the interest of
providing a foundation for further research.
This research project involved three stages: (1) modification of the FEATS for rating
drawing number two of the modified FSA; (2) application of the adapted FEATS scales for
rating drawing number two of the modified FSA; and (3) calculation of the inter-rater reliability
found among raters of the modified FSA drawings .
Purpose of the Study
The purpose of this study was to investigate the applicability of 9 of the 14 scales from
the Formal Elements Art Therapy Scale (FEATS) (Gantt & Tabone, 1998) to a modified version
of the Face Stimulus Assessment (FSA) (Betts, 2003). For the purposes of this project, the FSA
was administered to 30 volunteer, undergraduate college students enrolled at a local university.
This sample of participants contributed to establishing norms for further validity and reliability
studies of the FSA rating system.
2
Justification of the Study
Findings from this research study will have implications in a variety of areas. The
information gathered will be applicable to furthering the global usage of the FSA and the
FEATS. This information can be used by researchers to establish reliability and validity of the
FSA and its rating system. Testing in this area will support the use of the FSA as a credible art
therapy assessment (D. Betts, personal communication, November 17, 2007; Matteson, 2008).
The FSA is one of only a few instruments that accounts for gender and cultural factors as part of
the procedure. FSA research could have valuable implications for the field of art therapy. Future
investigations could be conducted on the use of the FSA with any number of populations.
The research from this study can also help support the use of the FSA and the FEATS in
clinical and research settings. Further research on the FSA will have benefits to art therapists and
clinicians who want an assessment tool that has global applicability. This research will also help
promote the use of the FEATS in a variety of research settings. As more research is conducted in
the area of art therapy assessment, the field of art therapy will ideally gain more notoriety and
acceptance as a valid from of treatment.
Research Question and Hypotheses
The purpose of this research study is to develop a standardized rating system for the Face
Stimulus Assessment by adapting these 9 scales from the Formal Elements Art Therapy Scale:
Prominence of Color, Color Fit, Energy, Space, Integration, Logic, Realism, Problem-solving,
Developmental Level, Details of Object and Environment, Line Quality and Perseveration (Gantt
& Tabone, 1998).
The central question in this research proposal is: To what extent can scales from the
FEATS be used to successfully rate drawings from the modified FSA? An additional question is:

3
To what extent will inter-rater reliability be achieved among raters of the modified FSA
drawings? The findings from this study will be helpful in further research to establish reliability
and validity for the Face Stimulus Assessment.
Definition of Terms
(1) Adapted FEATS scales: Is a term used to describe the 9 adapted scales from the 14
Formal Elements Art Therapy Scale : Prominence of Color, Color Fit, Energy, Space,
Integration, Logic, Realism, Problem-solving, Developmental Level, Details of
Object and Environment, Line Quality and Perseveration (Gantt & Tabone, 1998).
(2) Art therapy assessment: A specific art task used by art therapists to gather
information about a client‟s level of functioning, ascertain client strengths and
challenges, clarify client problems, identify therapy treatment goals, and measure
client progress.
(3) Client: A person receiving counseling or art therapy services.
(4) Ethnicity: A group of peope who identify with each other, based on a presumed
common ancestry or geneology (Wikipedia contributors, 2008).
(5) FSA (Face Stimulus Assessment): Is a projective drawing assessment, comprised of a
series of three drawings, originally designed to be utilized with multicultural, child
and adolescent populations with multiple disabilities and communication problems
(Betts, 2003).
(6) FEATS (Formal Elements Art Therapy Scale): Is a reliable measurement system
comprised of 14 rating scales derived from “psychiatric symptoms, clinical
observations, and the literature” (Gantt, 1990).

4
(7) FEATS Scales (original operational definitions) (derived from Gantt and Tabone,
1998):
Prominence of Color: The amount of color used to draw and fill in objects in a
picture.
Color Fit: The appropriateness of color used in a picture to the drawing task
Implied Energy: The amount of energy used to complete a picture.
Space: The amount of space used in the picture.
Integration: The degree to which the items in a picture are balanced into a
cohesive whole.
Logic: The degree to which a picture is logical and fits the drawing task.
Realism: The degree to which objects in the picture are clearly represented and
visually identifiable.
Problem Solving: The ability to find a reasonable solution to the problem of
picking an apple from a tree.
Developmental Level: The degree to which the artwork compares to drawings of
adults and children at different developmental stages.
Details of Objects and Environment: The number of additional items in the
picture related to the drawing task.
Line Quality: The amount of control exhibited by the artist in regards to the lines
in the picture.
Perseveration: The presence of elements that appear to be repeatedly drawn
without deliberate intention.
5
(8) Inter-rater Reliability: The degree of agreement between 2 or more raters (Wikipedia
contributors, 2008).
(9) Modified FSA (Face Stimulus Assessment): Is a modification of the original FSA
assessment using only drawings 1 and 2 from the original 3 drawing series.
(10) Standardized Rating System: A scoring guide tailored to the specific criteria of the
Face Stimulus Assessment.
Conclusions
This paper will outline a detailed summary of the research conducted using the modified
FEATS when applied to the FSA. The Face Stimulus Assessment is a valuable art therapy tool to
help evaluate and treat a diverse client population. This research project was created to
investigate the applicability of 9 FEATS scales when applied to drawing number two of the FSA.
This research study attempted to establish a solid foundation in order to investigate the
possibilities of establishing reliability and validity for the FSA in future research endeavors.
6
CHAPTER 2
LITERATURE REVIEW
Research in assessment is a growing area in the field of art therapy. Many art therapists
have devoted time to researching previously established art therapy assessments as well as
developing new art therapy assessments. This review of the literature will highlight the history of
art therapy assessment including their development, strengths, and limitations (Bucciarelli,
2007). The review of the literature begins with the historical foundations of the art-based
projective drawing assessments. These early art-based assessments provided the foundations for
the development of art therapy assessments today, including the FSA. The development of art
therapy assessments is given, followed by the author‟s conclusions about art therapy
assessments. The major strengths and limitations of these assessments are examined and
discussed. Then, the development of the Face Stimulus Assessment is described, and its current
uses in the clinical setting, current research, and limitations are reviewed. Then, the Formal
Elements Art Therapy Scale is described as well as its implications, current research, and
limitations. Finally, the implications of the literature review are summarized, and the
implications for this research study are noted.
Historical Foundation of Art Therapy Assessment
People have used art for the purpose of self-expression for centuries (Brooke, 1996;
Feder & Feder, 1998). Unlike the use of language, art has no restrictions on the expression of
thought and feeling. Projective methods with the intent to explore subconscious motivations are
not a new addition to the field of psychotherapy. Machover (1949) spent a considerable amount
of time devoted to researching projective methods and compared them to direct verbal
communication. Similarly, Langer (as cited in Brooke, 1996) found that “there is an important
7
part of reality that is quite inaccessible to the formative influence of language: that is the realm
of the so-called „inner-experience,‟ the life of feeling and emotion…the primary function of art is
to objectify feeling so that we can contemplate and understand.”
Art therapy assessments allow the therapist to evaluate clients through the art in ways
verbal communication can not. There are five areas in which researchers have investigated the
use and applicability of art therapy assessments: identification of client needs, personality
assessment, prediction of future behaviors, date for developing an individual treatment plan, and
monitoring progress (Feder & Feder, 1998). Many professionals feel that art therapists should be
encouraged to use their unique skills as the foundation for their investigation into creating art
therapy assessments (McNiff, 1998). An important function of art therapy assessment and
research in the area of assessment serves to bring professionalism and respectability to the field
of art therapy.
Art Therapy Assessments
Many of the most well-known art therapy assessments developed by art therapists have
been heavily influenced by previously established projective drawing tasks (Bucciarelli, 2007).
The large number of art therapy assessments that have been developed to date is too extensive to
outline in this paper. The assessments included in this paper are those assessments that are
among the most prominent and researched art therapy assessments to date. The assessments
include the following: the Diagnostic Drawing Series (Cohen, 1994; Cohen, Hammer, & Singer,
1988), the Ulman Personality Assessment Procedure (Ulman, 1965), and the Person Picking an
Apple from a Tree (Gantt & Tabone, 1998) assessment. Other less researched art therapy
assessments commonly utilized within the clinical art therapy setting will also be briefly outlined
in this paper.

8
Diagnostic Drawing Series (DDS). The Diagnostic Drawing Series (Cohen, et al., 1988;
Cohen, et al., 1994) was created in 1986, by Cohen, Hammer, & Singer. The intended population
for this assessment is use with an adolescent and adult population (Brooke, 1996). The DDS was
designed to collect clinical information about a client in a single session. The purpose of the
DDS is assessing an individual‟s response to structured and unstructured drawing tasks. The
DDS was introduced to correlate graphic indicators with psychiatric diagnosis that corresponded
to the third edition of the Diagnostic and Statistical Manual of Mental Disorders (Cohen et al,
1988; Brooke, 1996). The materials required for the DDS include 18 by 24 inch white drawing
paper and Alphacolor square pastels (Cohen, et al., 1988; Cohen, et al., 1994). The DDS
handbook indicates that the assessor should administer the DDS by giving the client specific
verbal instructions outlined in the handbook. The series of three drawings include a free drawing,
a tree picture, and a feeling picture. According to the developers of the DDS, the images provide
information about the clients‟ affective state, defensiveness, coping strategies, personal
symbolism, level of compliance, personal introspection, and self-expression (Cohen, et al., 1994;
Bucciarelli, 2007). The DDS drawings are scored using the DDS Revised Rating Guide (Cohen,
1994). The revised rating guide measures 37 formal and content variables across 23 categories
(Cohen, et al., 1988).
In addition to the rating guide, the DDS has a Drawing Inquiry sheet that includes a
qualitative question and answer interview to be used by the clinician and administered to the
participant. Cohen and the developers of the DDS along with other art therapists have worked
collaboratively to analyze and identify clusters of graphic elements in the DDS drawings that
indicate profiles for specific psychiatric diagnoses (Cohen, et al., 1994). To date, substantial

9
numbers of DDS drawings have been collected and compiled into a national archive categorized
by diagnosis (Cohen, et al., 1988; Cohen, et al., 1994; Bucciarelli, 2007).
Ulman Personality Assessment Procedure (UPAP). The UPAP, was created and
developed by Elinor Ulman in 1959, and was intended to be used as an assessment method to
identify diagnostic characteristics of psychiatric inpatients (1965). The UPAP consists of a series
of four drawings which are given with instructions meant to simulate experiences one would
encounter in day-to-day life (Cox et al, 1999). The materials needed include an 18 by 24 inch
grey bogus paper tacked down to an easel (Ulman, 1965). The administrator gives the client a set
of 12 hard pastels to use for the series of tasks. The four drawings include: a free drawing, a
series of physical exercises followed by a directed drawing task; a drawing stimulated by a
scribble; and the choice of a free drawing or another scribble drawing. The UPAP yields
information about the client‟s personality by looking at the form and the content in the drawings
and exploring the way he or she responds to the drawing tasks.
Agell (2000) created a checklist to rate the assessment drawings of the UPAP.
Descriptors in the drawing are rated on a one to five scale. The scale includes eight categories as
follows: line quality, color use, form, perspective, color application, content, paper orientation,
and amount of time used to complete the assessment. Agell‟s checklist includes space for
qualitative descriptions of the assessment drawings.
Person Picking an Apple From a Tree Assessment (PPAT). The PPAT is a widely used
assessment in the field of art therapy. The PPAT assessment uses the Formal Element Art
Therapy Scale (FEATS) as its formal rating guide (Gantt & Tabone, 1998). The PPAT
assessment is a single drawing procedure that requires a 12 by 18 inch sheet of white drawing
paper and a set of 12 felt-tip MR. SKETCHscented watercolor markers. The assessment
10
administrator asks the client to “Draw a person picking an apple from a tree.” There is no time
limit to complete this assessment (Gantt & Tabone, 1998).
The PPAT assessment protocol was developed for use with the FEATS Rating Manual
(Gantt & Tabone, 1998). The FEATS measures 14 different global formal variables of the PPAT
(Cox, Agell, Cohen, & Gantt, 1999). The FEATS yields diagnostic information through the
assessment of characteristics of form (Kaplan, 2000). The FEATS Rating Manual provides both
instructions for rating the PPAT assessment drawings and color examples of how to properly rate
the PPAT drawings. The FEATS Rating Manual includes a FEATS Rating Sheet (see Appendix
C) to document the score of each drawing along the formal elements scales (Cox, Agell, Cohen,
& Gantt, 1999; Bucciarelli, 2007). Gantt and Tabone (1998) have conducted studies that show a
single drawing can detect specific mental disorders and therefore, could be correlated with the
DSM-IV TR (Kaplan, 2000; Bucciarelli, 2007).
Other Art Therapy Assessments & Rating Instruments. There are many other art therapy
assessments and rating instruments in use today that are less popular and have little research to
support their use. Further research with these art therapy assessments could contribute valuable
information to the field of art therapy. Some of these assessments and rating instruments include:
A Favorite Kind of Day (AFKOD) (Manning, 1987); the Bird‟s Nest Drawing (BND) (Kaiser,
1993); the Bridge Drawing (Hays & Lyons, 1981); the Amusement Park Technique (Hrenko &
Willis, 1996); and the Child Diagnostic Drawing Series (CDDS) (Leavitt, 1988). Another rating
instrument is the Descriptive Assessment of Psychiatric Art (DAPA) (Hacking, 1999). Betts
(2005) has dedicated much of her career to the study of art therapy assessment research. The
results of her investigation found that art therapists are still in the early stages of understanding
assessments and rating instruments. Similarly, she found numerous flaws in the assessment

11
procedures and rating instruments as well as the errors in the literature research. She deduced
that art therapists have much work ahead of them in the area of art therapy research. Based on a
review of the literature, Betts found that the most successful approach to assessment procedures
integrates objective measures as well as subjective methods. Her final recommendation was that
researchers continue to explore both objective and subjective approaches to assessment.
Limitations of Art Therapy Assessments
The use of art therapy assessment and projective techniques has long been debated in the
field of art therapy. The problem stems from the lack of research, primarily a lack of reliability
and validity (Feder & Feder, 1998; Betts 2005). Many professionals in the field believe that it is
important for art therapists to develop their own art-based assessments; despite this belief
assessment development has been slow. Over the past 50 years several art therapy assessments
have been developed and gained notoriety (Betts, 2006). Unfortunately, research in the area has
produced varied results.
The use of projective assessments has declined over the past 25 years (Feder & Feder,
1998; Betts, 2006; Bucciarelli, 2007). The interpretation of projective assessments has led to
questionable research findings. Regardless, many mental health professionals, primarily
psychologists and psychiatrists, support the use of projective assessments. The poor research
findings come from the analysis of individual projective assessments. A study by Roback (1968)
investigated the findings of Machover‟s Draw-A-Person (DAP) Test and established that his
findings failed to support Machover‟s (1949) hypothesis that drawing the human body reveals
one‟s needs, conflicts, and expressive actions (as cited in Betts, 2005). Similarly, Klopfer and
Taulbee explored issues related to the validity of projective tests. They explored the TAT, the
12
Rorschach, and Human Figure Drawings. They found that despite poor reliability and validity,
psychologists were likely to continue using projective assessments on the basis of exploring the
inner psyche and internal motivations of their clients.
Using the Face Stimulus Assessment
The Face Stimulus Assessment is a projective drawings test consisting of three stimulus
images for the participant to complete (Betts, 2003). The author of the FSA outlined specific
standardized materials and procedures for the administration of the assessment. Prior to the
present study, a formal rating scale for the FSA did not exist. Betts suggested that reliability and
validity studies should be conducted on the FSA.
Development of the FSA
The Face Stimulus Assessment (FSA) was created by Donna J. Betts beginning in 1998
(2005). Betts developed the FSA after devoting years to researching the importance and
limitations of art therapy assessments. The FSA was first presented at the 32nd Annual AATA
conference in Albuquerque, NM (Betts, 2001). The FSA was originally developed as a projective
drawing assessment to be used with a multicultural child and adolescent population. Betts was
interested in using the FSA with children and adolescents with multiple disabilities, and those
who have communication difficulties (2003).
Betts began working on the FSA while working in a multicultural school, with children
with communication difficulties (2001; 2005). Betts found that working with “clients with
autism, communication difficulties, and, in particular, a lack of motivation benefited from
stimulus drawing such as a picture of a face” (2003). Betts was initially inspired by the work of
Silver (1976) and Stamatelos and Mott (1976) who recognized the importance of focusing on the
client‟s strengths when creating an assessment tool based on artwork (2003). Betts was also
13
influenced by the work of Alley (1988) who found that many authors consider the face the most
important part of the body in face-to-face interactions (2003). Alley (1988) found that the face is
primarily associated with expression, emotion, and identity.
The human face is commonly used in research. Betts decided to study whether the human
face would yield valuable information when used as a stimulus assessment, thus she created a
normalized version of the face-stimulus image (2003). The image is gender neutral, not age
specific, and can be representative of a variety of cultures. Betts felt that the face would make a
good stimulus because humans, as early as infancy, recognize the face and it holds their attention
(Betts, 2003; Alley, 1988). The face is primarily associated with emotional expression as well as
identity.
To initiate her research Betts began by reviewing the appropriateness of drawing tests as
well as the validity and reliability of the instrument (2005). Betts analyzed 35 quantitative
studies related to art therapy assessments and rating instruments (2005). Betts' examination of
analysis tools included: “A Favorite Kind of Day (AFKOD); the Bird‟s Nest Drawing (BND);
the Bridge Drawing; the Diagnostic Drawing Series (DDS), the Child Diagnostic Drawing Series
(CDDS); and the Person Picking an Apple from a Tree (PPAT).” The rating instruments Betts
explored included: “the Descriptive Assessment of Psychiatric Art (DAPA), the DDS Rating
Guide and Drawing Analysis Form (DAF), and the Formal Elements Art Therapy Scale
(FEATS).” From the results of her investigation, Betts found that art therapists are still in the
early stages of understanding art therapy assessments and rating instruments. Similarly, she
found numerous flaws in many of the assessment procedures and rating instruments, as well as
errors in the literature research (Betts, 2005). She deduced that art therapists have much work
ahead of them in the area of art therapy research.

14
Based on a review of the literature, Betts found that the most successful approach to
assessment procedures integrates objective measures as well as subjective methods (2005). Her
final recommendation stated that researchers should continue to explore both objective and
subjective approaches to assessment. Betts also found that many professionals in the field of art
therapy are using assessments without understanding the implications of poor reliability or
validity and without comprehending the usefulness and applicability of these tools.
After her research was complete, Betts published her assessment tool, the Face Stimulus
Assessment. Betts created the FSA partially in the interest of assessment research as well as an
assessment tool for further research by other art therapists. Betts (2003) stated that “art therapy
students and professionals alike should be encouraged to explore inventive means of working
with and evaluating their clients-creative investigation can be fruitful”.
The FSA is a series of three stimulus pictures for the client to complete. The first is a
normalized version of the face-stimulus (Appendix A), the second is an outline of a face and
neck (Appendix A), and the third is a blank page (Betts, 2003). Betts uses a series of three
images to assess the client‟s capacity for “memory and visual retention and his or her ability to
organize the constituent elements of the human face” (Betts, 2003). The FSA can be
administered to a small group or individually. Betts recommends that before the client enters the
room, the art therapist should place the materials on the table where the client will be seated.
The FSA allows 50 minutes to one hour for the completion of the assessment (Betts,
2003). Once the client enters the room, the therapist should ask him or her to be seated. Once
seated, the instructions are to ask the client to “use the markers and this piece of paper”. This is
the only instruction the administrator should give the client during the completion of the FSA.
Once the client completes the first picture, the therapist should remove it from view; for the same

15
standard should be applied to the second and third pictures as well. The FSA administrator has
the option to review the assessment with the client as follow-up. For the purpose of follow-up the
administrator needs to write the client‟s name, and indicate the picture number in the bottom left-
hand corner.
Currently, the scoring system for the Face Stimulus Assessment is an informal rating
procedure (Betts, 2005). A formal rating scale for measuring the FSA has yet to be developed,
for which reliability and validity testing would need to be conducted. For rating picture one Betts
identifies five criteria: motor skill ability, realistic use of natural color, addition of adornment
(hair, eye lashes, jewelry), adjusting the face to look like the client, and use of picture space.
When giving the first drawing it is important to consider all five criteria. The client‟s ability and
use of color and inclusion of adornment can be very telling about the client‟s abilities, their
developmental level, any problems or concerns, strengths, as well as any psychopathology. The
use of realism may indicate how the client sees him or her self. This may include identity
problems or issues related to culture. Motor skill assessment is also an important part of drawing
one.
When considering drawing two, Betts (2005) identified three criteria for consideration:
ignoring the stimulus is the shape of a face, choosing to make the picture into a face (refer to
criteria for drawing 1), and choosing not to make the picture into a face. The second drawing is
also a very important tool for assessing the client‟s ability, strengths, and potential barriers to
treatment. If the client has difficulty organizing the facial structure, the assessment drawing will
allow the opportunity for tendencies to be brought to the surface, possibly memory recall
problems or other cognitive issues (Betts, 2003). If the client ignores the face altogether this may
indicate memory problems as well as learning difficulties. Drawing two is very important for
16
language and hearing impaired individuals who may need to learn about the use of space,
sequential order, grouping, and object placement.
The rating scale for picture three includes four criteria (Betts, 2005). It is important to
consider whether the client chooses to draw a face or not, and if the client does not draw a face,
what might it indicate? If the client does draw a face, might this imply compliance? Betts
suggests that the rater consider how it is similar to or different from the face in Pictures 1 and 2.
If the client does not draw a face, does this imply a rebellion and defiance, or creativity and
compliance on the part of the client? When rating formal aspects of Picture 3, other assessment
indicators might be considered, such as the use of line, space, or color. It is also important to note
whether the client changes the page orientation to a horizontal format. The third picture can be
used to judge the client‟s ability to recall that Pictures 1 and 2 were pictures of a face. If a client
chooses to draw something other than a face on Picture 3, this could possibly indicate poor
memory function, defiance or rebellion, creativity, or even learning disabilities. Overall, picture
three is an opportunity to determine the client‟s abilities and strengths.
The materials specified for use with the FSA have been standardized by the author. She
stipulates the following materials for use with the FSA (Betts, 2005):
· A standard packet of 8 Crayola® markers
· A packet of 8 Crayola® Multicultural markers
· Stimulus picture #1: one 8 ½ x 11” sheet of white Xerox paper depicting the complete
face stimulus
· Stimulus picture #2: one 8 ½ x 11” sheet of white Xerox paper depicting the outline of
the face and neck.
· Stimulus picture #3: one 8 ½ x 11” sheet of blank white Xerox paper.

17
Limitations of the FSA
The Face Stimulus Assessment was introduced to the field of art therapy around 2000.
Although only two published studies exist on the FSA (Betts, 2003; Robb, 2001), this does not
indicate that the assessment is not useful or applicable. Robb used the FSA while facilitating the
art therapy process at a 6-week day camp for Russian children from orphanages in the U.S.
(Robb, 2001). She and other art therapists helped in addressing anxiety-provoking problems that
the children experienced (Robb, 2001). She used the FSA as an assessment tool to identify
anxiety as well as PTSD symptoms in the Russian children (Robb, 2001). The use of the FSA by
Robb is a step towards developing more reliability and validity with this instrument. More
research is needed to demonstrate this assessment as a reliable, valid tool for art therapists to use
consistently with their clients.
There are other drawbacks to the use of the Face Stimulus Assessment as an informal
assessment tool. Gantt (2004) points out that when administering informal assessments the
evaluator and the therapist are the same which leads to evaluator bias. She states that the data
collected on an individual cannot be generalized to others. This is applicable to the FSA in this
case since there is little evidence for the type of population best served by this assessment. Gantt
also identifies the possibility of projection on the part of the evaluator leading to
misinterpretations. She states that definitions used in informal assessments may be vague or
inexact. The FSA is guilty of this fallibility. In the description of the Informal Rating Procedure
Betts is vague when it comes to defining particular terms and guidelines. Gantt also lists the lack
of reliability and validity as a criticism to projective drawing tests. Betts clearly identifies that
the FSA has not been shown to have any reliability or validity as it is undergoing research to
further establish itself.

18
Betts is the first critic of her own assessment. She identifies that it would be beneficial to
explore whether the FSA can assess the client‟s “psychosocial development, cognitive
development, creative potential, and graphic intelligence” (Betts, 2003). Other potential areas of
examination include self esteem, motor development, behavior, conceptual skills, memory
development, as well as language abilities (Betts, 2003). The FSA may also be used with the
geriatric population, especially dementia and Alzheimer‟s clients, to assess memory function and
motor ability. This could help the treating professionals detect the progression of their disease.
Betts (2003) also gives her recommendations for further research and the development of
a valid and reliable rating method for the FSA. Betts states that researchers need to:
Establish a method to rate those elements in the drawing that graphically demonstrate
identified concepts, abilities, or skills – such as the role of color, figure and size
differentiation, drawing style, compositional strategies, the incidence of bizarre or
unconventional elements, and the use of pictorial space (2003).
Recommendations for Further Development of the FSA
Little research has been conducted to establish the FSA‟s reliability and validity, as well
as its applicability to various populations. The usefulness of the Face Stimulus Assessment
appears to be widespread across a variety of populations. Potential populations could include
children, adolescents, and adults with multiple disabilities, people with communication
difficulties, those with psychosocial development issues, and persons with cognitive
development disorders. Other applications may include those persons with low self esteem,
motor development problems, behavioral issues, conceptual skill problems, geriatrics, memory
development, as well as language disabilities. The wide range of uses for this assessment should
make the FSA appealing to many art therapists who plan to use it in the future.
19
Prior to the present study, the rating system for the FSA was only informal. Betts
provides guidelines to follow when rating the drawings which are helpful but lack the element of
standardized scoring. Betts recommended the modified application of the Formal Elements Art
Therapy Scale (FEATS) for rating the FSA. The FEATS measures 14 formal elements including
“prominence of color, problem-solving, space, color fit, developmental level, integration,
implied energy, details of objects and environment, logic, realism, line quality, preservation,
rotation, and person” (Gantt & Tabone, 1998). Due to the global applicability of the variables,
modified FEATS scales could be used with the FSA to help establish reliability and validity.
Betts (2003) suggested that in order to develop a reliable and valid rating system for the
FSA, researchers should investigate a method to rate graphic elements in the drawings that
“demonstrate identified concepts, abilities, or skills-such as the role of color, figure and size
differentiation, drawing style, compositional strategies, the incidence of bizarre or
unconventional elements, and the use of pictorial space (as cited in Golomb, 1992). The rating
system would then need to be tested against a standardized measurement tool that looks at the
same concepts (Betts, 2003).
The FSA is a user-friendly assessment tool. This ease of use will likely be an important
benefit for art therapists as well as other mental health professionals who wish to use this
assessment. The materials needed to administer the assessment are generally accessible. The
assessment itself can easily be ordered through Betts' website for only 20 dollars. Betts research
and development of the FSA is a step in the right direction towards contributing an effective,
reliable, valid assessment instrument to the field of art therapy. The job of continuing this
research rests on the shoulders of art therapy students and professionals in the field if we hope to
demonstrate the worth of the field of art therapy.

20
Using the Formal Elements Art Therapy Scale
The FEATS Rating Manual was created to be used in conjunction with the Person Picking
an Apple from a Tree assessment (Gantt & Tabone, 1998). The FEATS measures 14 variables of
the PPAT assessment (Gantt & Tabone, 1998). The 14 scales include: Prominence of Color,
Color Fit, Implied Energy, Space, Integration, Logic, Realism, Problem-solving, Developmental
Level, Details of Objects and Environment, Line Quality, Person, Rotation, and Perseveration.
The FEATS Rating Manual provides instructions for rating the PPAT assessment drawings. The
rating manual provides color examples of actual client drawings and describes how to properly
rate the PPAT drawings. Included in the FEATS Rating Manual is a FEATS Rating Sheet used to
document the score of each drawing along the formal element scales .
Development of the FEATS
At the 1999 American Art Therapy Association Conference in Orlando, Florida, a panel
was assembled to investigate the application of three art therapy assessments: the Person Picking
an Apple from a Tree (PPAT), the Ulman Personality Assessment Procedure (UPAP), and the
Diagnostic Drawing Series (DDS). The panel concluded that the potential for research in this
area, mainly the use of these three art assessments and other drawing assessments were
numerous (Cox, Agell, Cohen, & Gantt, 2000). Cox concluded that research should be conducted
to look at the possibility of comparing drawings from one assessment to the drawings from
another to investigate the possibilities for further use. Cox also suggested that researchers should
investigate the applicability of the FEATS to additional assessments (2000).
The FEATS was developed in order to provide “clinicians and researchers with a
standardized drawing and a sound scientific method of studying it” (Gantt & Tabone, 1998). The
FEATS Manual is a research tool that was created to add to the credibility of the field of art

21
therapy; dispel art therapy myths and provide verifiable facts, illustrate a way of researching that
aligns itself with the way art therapists think; present methods for comprehending and
researching non-symbolic aspects of art; and describe the connection between art elements and
diagnosis and clinical state. The FEATS measures specific global variables based on equivalents
of psychiatric symptoms but it is not intended to be used as a manual for psychiatric diagnosis.
The theory behind the FEATS is to accomplish several goals: separate art therapy fact from
fiction, develop more precise definitions for the field, build better theoretical foundations, and
point the way to more precise treatment methods (Gantt & Tabone, 1998).
Each of the 14 interval/Likert-type FEATS scales are scored from zero to five, or
between any two whole numbers to give a half rating i.e., 3.5 (Gantt & Tabone, 1998). The
ability to rate the scales allows the clinician or researcher to convert raw scores into a clinical
score for archival purposes. There are also 10 dichotomous content scales by which to rate the
drawings, these are not rated from zero to five, they are simply scored on a basis of present or
not present. These scales include the color used for the whole picture and the person, visible
features of the person, gender, actual energy, orientation of the face, age, clothing, apple tree,
environmental details, and other features.
The FEATS is used for directing the clinician toward the most beneficial treatment plan
and not for use as a diagnostic tool. However, Gantt and Tabone (1998) found correlations
between Diagnostic and Statistic Manual of Mental Disorders (DSM-IV) symptoms,
observations in the art therapy literature, and the FEATS scales. For example, in the DSM-IV
Major Depression is classified as depressed mood, loss of energy, psychomotor retardation or
agitation, diminished interest, and diminished ability to think or concentrate. The observations in
the art therapy literature that correlate with Major Depression are lack of color, use of dark

22
colors, constricted use of space, lack of environment, and lack of detail. Translated to the
FEATS, the scales which might be most useful for diagnosis and treatment might include
Prominence of Color, Color Fit, Energy, Space, Realism, Person, and Perseveration.
Much research has been conducted to study the effectiveness and utility of the FEATS. A
study by Rockwell & Dunham (2006) studied the use of the FEATS with a population of people
diagnosed with Substance Use Disorders, who were court ordered for treatment, in order to
determine the inter-rater reliability for the FEATS. The population in the study included 40
adults. Their research found good inter-rater reliability on the first twelve of the 14 scales, thus
the perseveration and rotation scales were omitted from the study. Twenty drawings were
collected from the experimental group as part of the intake process at a state-licensed, private
counseling facility. Twenty drawings were collected from the control group, which was
comprised of individuals in the community. The results of the inter-rater reliability study were
consistent with other research on the FEATS, in that the correlations revealed a high degree of
consistency between the two raters. Nine of the twelve FEATS scales showed statistically
significant high scores, while the three scales that were not statistically significant were Line
Quality, Problem-solving, and Integration. The authors found that differing interpretations of the
scoring criteria most likely led to the differences.
Another study conducted by Swan-Foster, Foster, & Dorsey (2003) compared the human
figure drawings of pregnant women to determine if there were visual differences between three
different groups including high risk outpatients, high risk inpatients, and low risk outpatient
pregnant women. Depression is a common problem experienced by pregnant women and it can
seriously affect their pregnancy. Many researchers conclude that screening for and treating
23
prenatal depression is essential to effectively monitoring and managing the health of mother and
baby.
The study explored the potential for visual differences between drawings taken from the
three prenatal groups (Swan-Foster, Foster, & Dorsey, 2003). The participants were told that the
study was to document “personal experience of pregnancy” and “masterpieces are not required
or expected.” Pre and post-tests with a 5-point Likert scale were used to measure fearful/trusting
and anxious/calm for each drawings. Ten drawings were randomly selected from each group and
rated using the FEATS scales and Content Tally sheets. The results of this study found that
certain formal elements of the drawings may reflect the potential for levels of depression in
relation to the study groups. The results also indicated that that the low risk group scored higher
than the high risk groups, particularly with scales rating color, energy, space, details, and person.
The high risk outpatient group indicated a higher risk for depression than the high risk inpatient
group and often presented with a more “stoic nature.” The data that this study collected can be
used in future research, using a non-verbal tool to investigate the prenatal emotions or
psychological distress. The scores for this study were consistent for all three groups and showed
a strong inter-rater reliability.
The previously mentioned studies are just a few studies that have contributed to
determining the FEATS as a reliable and valid scoring system. Gantt and Tabone (1998) created
the FEATS as a ready-to-use tool for researchers studying a variety of populations. The excellent
inter-rater reliability of the FEATS makes it easy for investigators to conduct validity studies.
Overall, the FEATS is a valuable tool for art therapy researchers investigating a variety of
variables within the field.

24
Limitations of the FEATS
The FEATS scales were created by Gantt and Tabone (1998) using a variety of sources
including clinical observations, art therapy and psychology literature and projective drawings of
psychiatric inpatients, and the criteria set from the DSM-IV. While the creation and development
of the scales was a meticulous process, the FEATS scales are continually being researched and
some limitations have emerged. Gantt and Tabone write in the FEATS Manual that although
each scale may be scored from zero to five, the number indicates more or less of a variable;
however a higher score does not necessarily indicate a better score than a lower rating. At this
point there is no way to convert raw scores into clinical scores. With more research and large
scale representative samples, norms can be developed for each scale. If and when this is
established, the correlation of specific scales and psychiatric symptoms can be regarded as the
“actual equivalent of a symptom.”
When looking at art and color in relation to the FEATS scales one must consider the
appropriateness for specific items (Gantt & Tabone, 1998). Gantt and Tabone give the example
of rating abstract art with the Color Fit scale. A researcher would not be able to determine the
appropriateness of Color Fit for an abstract piece of artwork due to the nature of abstract art. This
is an example of how not all FEATS scales can be used to rate all artwork. Researchers must use
discretion in establishing the appropriateness of FEATS scales to rate artwork. The authors also
note that the FEATS, as well as many other art assessments, do not screen for color-blindness.
When considering the Color Fit scale, it may be difficult to rule out color-blindness as a cause
for a low score on this scale.
The authors mention the area of personality characteristics as a severe limitation to the
FEATS scales (Gantt & Tabone, 1998). It is difficult to determine personality characteristics

25
based on a single drawings, like that in the PPAT. A single drawing is only a small element of a
person's potential responses. Thus, the amount of information gathered by the FEATS when
combined with the PPAT is limited. It may be most beneficial at this point to pair the FEATS
with other assessments to paint a larger picture of the persons overall character.
As with many assessments in the field of art therapy research, the FEATS does not have
the same popularity as some traditional psychological assessments. This means less researchers
have access to the FEATS, thus fewer studies have been conducted on its reliability and validity.
Hopefully as the field of art therapy and especially the area of art therapy assessment expand and
grow, assessments like the FEATS will gain popularity as a reliable and valid assessment tool for
mental health practitioners and art therapists alike.
Recommendations for Further Development of the FEATS
Gantt and Tabone (1998) have conducted countless studies in order to make a reliable
and valid instrument and they have a long way to go to reach their goal. The inter-rater reliability
studies have been promising but at this point it is most important for the authors and other
researchers to conduct large scale validity studies to begin to establish the FEATS as a valid
assessment tool.
The authors review several areas of possible extensions that they recommend researchers
consider (Gantt & Tabone, 1998). When using the FEATS with assessments other than the
PPAT, one must consider the media; paintings are not the same as drawings. Paintings tend to
take up more space than drawings which may likely affect the Space scale as well as Prominence
of Color. Research has not been conducted on varying art materials. In order to study this
variable a correlational study would be most appropriate. Previous art experience may also be a
confounding influence, often creativity can be judged as pathology.

26
It may also be helpful to study the correlation between the diagnostic information
provided by the PPAT, compared to other assessment drawings (Gantt & Tabone, 1998). This
may mean that some FEATS scales will be limited in their use and may have to be omitted when
used with other assessment drawings. Scales such as Details, Color Fit, Logic, and Person may
only be applicable to drawings that contain people. Other scales such as Color, Implied Energy,
Space, Line Quality, and Integration may be used with abstract art. More research should be
conducted to research the applicability of the scales to various drawings.
The authors also identify areas of further investigation that they have considered. One of
these avenues includes studying participant drawings in response to medication (Gantt &
Tabone, 1998). Pre and post-test studies could be conducted to investigate how various
medications affect patients during the course of treatment. The FEATS scales could also be used
to research varying degrees of depression. Since the authors have found correlations between
DSM criteria and the drawings of depressed clients, further studies could be completed to
explore how scores on the FEATS scales compare to other measures of depression. The FEATS
could also be used to study the progression of diseases such as Alzheimer‟s disease, stages of
mania, or the progression of Schizophrenia. Studies could be used to look at changes over the
span of one‟s life. A longitudinal study could follow clients over the span of decades.
The FEATS may also be appropriate to look at the differences between intake and
discharge pictures as a means to judge and document change (Gantt & Tabone, 1998). Similarly,
FEATS drawings could be used to monitor the progress of clients with substance abuse
problems. It may also be helpful to study FEATS drawings during the twelve step process
throughout one‟s recovery. The FEATS appears to be useful across a variety of setting with

27
multiple populations. It is the job of art therapists to continue researching the FEATS and other
art therapy assessment and rating tools.
Conclusions
Research in assessment is a growing area in the field of art therapy with a variety of
implications. The historical foundations of art therapy and assessment were explored and found
to serve the purpose to evaluate clients through art in ways verbal communication can not. The
development, strengths and limitations of art therapy assessments today were reviewed in detail
in relation to assessing client‟s through art. It was found that these initial art-based assessments
provided the foundations for the development of art therapy assessments today. The development
of art therapy assessments was reviewed, followed by recommendations for developing art
therapy assessments in the future.
The major strengths and limitations of these assessments were also reviewed. Next, the
development of the Face Stimulus Assessment was described, as well as its current uses in the
clinical setting, current research, and limitations, and recommendations for future research. Then,
the Formal Elements Art Therapy Scale was described as well as its implications, current
research, limitations, and possibilities for future research. This review of the literature was very
helpful in identifying influences from psychology and art therapy resources that support the
thesis of this research. The literature guided the development of the research question and helped
to determine the path for examining possible solutions.

28
CHAPTER 3
METHODOLOGY
Development of the Research
The current research study was a normative study of modified FSA drawings on college
students. This chapter outlines the steps taken to complete the research effort. First, the research
question is reiterated, and the research design is outlined. Next, the selection and organization of
the research sample is described. The data collection is then outlined followed by the methods
used to analyze the data collection and research findings. Finally, the chapter addresses the
validity of the study and the ethical concerns of the research.
Research Questions
The purpose of the study was to contribute to the body of work supporting the FSA as a valid
and reliable art therapy tool. Specifically, the research questions were: To what extent can scales
from the FEATS be used to successfully rate drawings from the modified FSA? As well as, to
what extent will inter-rater reliability be achieved among raters of the modified FSA drawings?
Research Design
This researcher administered FSA drawings to a sample of college students (N = 30).
Once the modified FSA drawings were collected, drawing number two was individually rated by
each of the four raters. Inter-rater reliability was determined through percentage of agreement
and the Kappa statistic on each of the 9 scales to determine the degree of agreement among
raters.

29
Sample
Participants
This research study was conducted using a convenience sample of 30 participants
enrolled at a small Midwestern university in the United States. The participants were ages 19 to
28; one participant either refused or neglected to answer (See Figure 3). Accordingly, 6
participants were male and 24 were female (See Figure 2). The ethnic groups in the sample
included: American Indian or Alaskan Native (n = 0), Asian or Pacific Islander (n = 1), Black,
Not of Hispanic Origin (n = 4), Hispanic (n = 4), White, Not of Hispanic Origin (n = 21), and
participants who did not report their ethnicities (n = 0) (See Figure 3).
Participant Recruitment Process
This researcher initially obtained permission to conduct this study through the local
university‟s research review board. University professors teaching undergraduate psychology
were subsequently approached about the research project to determine their willingness to
participate. This researcher collected FSA pictures in the classroom setting where the
participants were asked to voluntarily participate in this study. Thirty students agreed to
participate and all 30 drawings were collected and scored by the raters for data analysis. The
assessment materials were pre-coded, so participant confidentiality was maintained. Each class
was given the same verbal directions by this researcher in order to maintain standard
administration (see Appendix G).
Instrumentation
Materials
This researcher provided all necessary materials for the FSA drawings protocol. Each
participant received an informed consent form (see Appendix F), a questionnaire (see Appendix
30
E), and the modified FSA drawing materials (see Appendix A). The drawing materials included a
standard packet of 8 Crayola® markers, a packet of 8 Crayola® Multicultural markers, stimulus
picture #1: one 8 ½ x 11” sheet of white Xerox paper depicting the complete face stimulus, and
stimulus picture #2: one 8 ½ x 11” sheet of white Xerox paper depicting the outline of the face
and neck.
After the raw data was collected, 4 trained raters scored the FSA drawings based on the
FEATS Scales Adapted for use with the Face Stimulus Assessment (see Appendix B) (Betts,
2008). The raters completed the Modified FEATS Rating Sheet for each FSA drawing (see
Appendix C) (Betts, 2008).
Measuring Devices
The data collected for this research study was collected from two sources: the FSA
drawings and the demographics questionnaire created by this investigator (see Appendix E). The
data from the FSA drawings were quantified using the FEATS Scales Adapted for use with the
Face Stimulus Assessment (see Appendix C) and the Modified FEATS Rating Sheet Sample
Drawings (see Appendix D) (Betts, 2008).
Questionnaire. The questionnaire collected data on demographic information on
participants including age, gender, ethnicity, and previous art experience. When determining
previous art experience the participants were asked about: (1) experience creating art; (2) formal
art training; (3) preferred medium; (4) previous experience with assessment materials; and (5)
qualitative thoughts about the drawings activity. In the current study this information was not
used to determine a particular sample since all participants were used. This information will
hopefully play an important role in future studies of the FSA.
Modified FSA. According to Betts (2003), the FSA is a projective drawing assessment,
31
comprised of a series of three drawings, originally designed to be utilized with multicultural,
child and adolescent populations with multiple disabilities and communication problems. The
modified FSA is a modification of the original FSA assessment using only drawings 1 and 2
from the original 3 drawing series. Drawing number 1 is a standardized image of the human face.
The image is non gender specific, can be generalized to a variety of cultures, and is not specific
to any age. Drawing 1 looks at formal elements such as color, realism, recognition of the human
face, details of object and use of picture space. Drawing number 2 is an outline of the face and
neck. For this drawing a variety of elements can be considered, including color fit, realism,
details of object and use of picture space. Drawing 3 is a blank page used to determine whether
the participant will draw a face after completing the two prior stimulus drawings. For the
purposes of this study, drawing number 3 will not be used as per hypothesis (a), that drawing 2
reveals the most valid information about the participant.
FEATS. The FEATS is a reliable measurement system comprised of 14 rating scales
derived from “psychiatric symptoms, clinical observations, and the literature” (Gantt, 1990). For
the purposes of this study only 9 scales from the FEATS are used: Prominence of Color, Color
Fit, Energy, Space, Integration, Logic, Realism, Problem-solving, Developmental Level, Details
of Object and Environment, Line Quality and Perseveration (Gantt & Tabone, 1998). Each
FEATS category corresponds to a FEATS scale, rated using increments of half point scores from
zero to five. Gantt and Tabone explain in the Feats Rating Manual that higher scores does not
indicate better qualities in a drawing. Essentially, the numbers on the scales only measure more
or less of a formal element represented in a drawing.

32
Procedures
This research study was completed in four stages. First, the FSA and FEATS were
modified to fit the needs of a normative college student population. Next, FSA drawings and
questionnaires were administered to the volunteer participants. Additionally, the raters were
trained to score the FSA drawings and all 30 drawings were rated using the modified FEATS
scales. Finally, the data was compiled, examined, analyzed, and the findings were reported.
Administration of the FSA
This researcher administered and collected FSA drawings to all volunteer participants in
a classroom setting. The assessment materials were coded prior to administration to ensure
participant confidentiality and anonymity. This researcher individually passed out and collected
all required materials for the FSA drawings protocol. First, each participant received two copies
of an informed consent form (see Appendix F), one to sign and be maintained in this researchers
records, and a copy for the participant‟s records. Next, the modified FSA drawing materials (see
Appendix A) were passed out to each participant. The drawing materials included a standard
packet of 8 Crayola® markers and a packet of 8 Crayola® Multicultural markers. Then each
participant was given FSA stimulus picture #1 and instructed to “use these markers and this
piece of paper” as indicated in the FSA administration instructions. Next, this researcher
collected drawing #1 and passed out drawing #2. Finally, each participant was given a
questionnaire (see Appendix E) to complete at the end of the session.
This version of the modified FSA allowed 30 minutes to complete. At the 15 minute
mark, this investigator announced that 15 minutes remained to complete the drawings. Then at
the five minute mark, this investigator announced that 5 minutes remained. At the end of the
session, this researcher collected all remaining materials and the questionnaires.
33
The participants were informed that the original artwork will be stored by this researcher
in a locked file cabinet with a key only accessible to this researcher. Scanned drawings of those
participants who consent to participate will be added to the local University Counseling and Art
Therapy Research Database. All identifiable information will be removed from the artwork for
anonymity and confidentiality. This information will be available for public use for future
research in the field of counseling and art therapy.
Rating the FSA Drawings
Once the drawings were collected, Rater 1 (Donna Betts, creator of the FSA) trained
Rater 2 (this author), Rater 3 (a graduate art therapy student at the local university aware of the
research purpose), and Rater 4 (a graduate art therapy student solicited via Rater 1, blind to the
research purpose). Rater 1 reviewed the criterion for each FEATS category and reviewed the
Modified FEATS Sample Drawings (see Appendix D) with each rater. Then, the raters practiced
independently scoring 3 drawings created and provided by the trainer. After the training session,
the four raters independently rated drawing number 2 from each participant, totaling 30
drawings. The raters recorded each participant‟s score on the Modified FEATS Rating Sheet (see
Appendix C).
Description and Justification of the Statistical Techniques Used
Statistical research conducted by Gantt and Tabone (1998) used an analysis of variance
(ANOVA) for the FEATS and found that 10 of the 12 FEATS scales differentiated amongst two
or more groups (Gantt, 1990, 1993; Betts, 2003b). Additional research on the FEATS, using
larger sample populations will yield more information, including data to support reliability and
validity.

34
Internal and External Validity
Betts recommends using specific materials during the administration of the FSA in an
attempt to standardize the assessment. In order to maintain consistency this researcher used the
recommended materials including: a standard packet of 8 Crayola® markers, a packet of 8
Crayola® Multicultural markers, stimulus picture #1, and stimulus picture #2.
In order to limit subjective biases, this researcher will act as the assessment administrator
over the duration of the project (Bucciarelli, 2007). To reduce data collector bias, this researcher
and two other raters were extensively trained by Donna Betts, the FSA author and creator. This
researcher followed a strict protocol for administering and collecting the drawings and data.
Additionally, all of the assessment drawings were collected in the same setting at a local
university.
For the purposes of this study, the original FEATS scales were modified to fit the specific
criterion of the modified FSA drawings (Betts, 2003). Modification of the original
instrumentation may be a threat to internal validity. In order to avoid validity threats, this
researcher and creator/author Donna Betts were exceedingly cautious in appropriately modifying
the FEATS scales.
One potential threat to internal validity may concern picture raters (Betts, 2003). The
additional rater was carefully chosen by the researcher to guarantee they were able to carry out
the task of rating in a satisfactory manner (Hadley & Mitchell, 1995; Betts, 2003). This
researcher made every attempt to ensure that the additional rater was not informed of the specific
research question in order to prevent this threat from compromising internal validity.
In order to give the results of this research more global applicability, this researcher
initially intended to minimize threats to external validity by collecting a large sample of modified
35
FSA drawings from which to modify the FEATS scales. The original intent was to collect a
sample between 50 and 75 drawings. The final sample size resulted in 30 drawings, which could
be a threat to external validity.
Ethical Concerns
This research study was approved by the university Research Review Board (RRB) to
carry out research with human participants. Each volunteer participant was given two copies of
an informed consent document (see Appendix F), to read and sign before volunteering to
completing the FSA assessment protocol. Each participant was asked to maintain one copy for
their records and one to turn in to be held by this researcher. The purpose of the informed
consent was to maintain participant‟s confidential information throughout the duration of the
research study. The informed consent also highlighted the rights of the participant and the rights
of the researcher in relation to this study. Each participant was asked to sign and date the consent
form to verify that they agreed with the terms of the agreement. The document explained to
participants that participation in the research was voluntary and each participant was allowed to
decline participation or drop out of the study at any time. This researcher was also present during
and after the protocol to answer any questions from the participants.
Conclusions
This chapter describes the research methodology used in the current study. The purpose
of this study is to investigate the applicability of 9 of the 14 scales from the FEATS to a
modified version of the FSA when administered to a normative population of college students
(Gantt & Tabone, 1998; Betts, 2003). All volunteer participants in the study completed an FSA
drawing for a total population of (N = 30). After which, each of the drawings were independently
rated. Statistical analysis of the data was justified, conducted, and reported. The reliability and

36
validity of the research instruments were also investigated and established. The ethical concerns
of the research study were reported and precautions were put in place to ensure the wellbeing,
confidentiality, and anonymity of the research participants. In the following chapter, the results
from the statistical analysis of the data will be presented.
37
CHAPTER 4
RESULTS
This chapter discusses the results of the study. A summary of the significant findings of
the inter-rater reliability are discussed. Then, an analysis of the results is presented. Finally, the
author‟s the conclusions are stated.
Inter-rater Reliability Results
The focus of this research endeavor was to study the results of inter-rater reliability
between modified FSA raters using the 9 adapted FEATS scales. Any correlation among raters
can be used to support the future use of the 9 FEATS scales when scoring the FSA. The results
indeed established strong reliability between raters which supports the research hypothesis.
The study included a total of four raters, including this researcher. Three additional raters were
recruited including two graduate art therapy students, and the creator of the FSA assessment,
Donna Betts. The forth rater, a graduate art therapy student, was blind to the purpose of the study
in order to study and limit subjective biases. This researcher and the two graduate student raters
were trained by Donna Betts to score the FSA drawings with the 9 FEATS scales. In the training
session, the trainer reviewed the 9 formal elements on the adapted FEATS. Each trainee rater
practiced rating 3 sample FSA drawings.
Inter-rater reliability was measured by using Fleiss‟ kappa. Fleiss‟ kappa is a statistical
measurement tool used to assess the reliability of agreement “between a fixed number of raters
when assigning categorical ratings to a number of items or classifying items” (Wikipedia
contributors, Fleiss Kappa, 2008). Fleiss‟ kappa is scored as a number between 0 and 1, and
determines the amount of agreement compared to that which would be expected by chance. The

38
closer the score is to one, the higher the inter-rater agreement. For example, if all raters are in
agreement then κ = 1 (See Table 1.).
Table 1.
Kappa Interpretation
κ Interpretation
< 0 Poor Agreement
0.0 – 0.20 Slight Agreement
0.21 – 0.40 Fair Agreement
0.41 – 0.60 Moderate Agreement
0.61 – 0.80 Substantial Agreement
0.81 – 1.00 Almost Perfect Agreement
The results of the Fleiss‟ kappa run on the rater data indicate strong inter-rater reliability
(See Table 2). The inter-rater reliability indicated is as follows: Scale 1 had a κ = .3556
indicating fair inter-rater reliability; Scale 2 had a κ = .7833 indicating substantial inter-rater
reliability; Scale 3 had a κ = .5167 indicating moderate inter-rater reliability; Scale 6 had a κ =
.7778 indicating substantial inter-rater reliability; Scale 7 had a κ = .4722 indicating moderate
inter-rater reliability; Scale 9 had a κ = .5667 indicating moderate inter-rater reliability; Scale 10
had a κ = .425 indicating moderate inter-rater reliability; Scale 11 had a κ = .5833 indicating
moderate inter-rater reliability; and Scale 14 had a κ = .817 indicating almost perfect inter-rater
reliability. The scales of Perseveration, Color Fit, and Logic showed the strongest inter-rater
reliability. The scales of Implied Energy, Realism, Developmental Level, Details of Object and
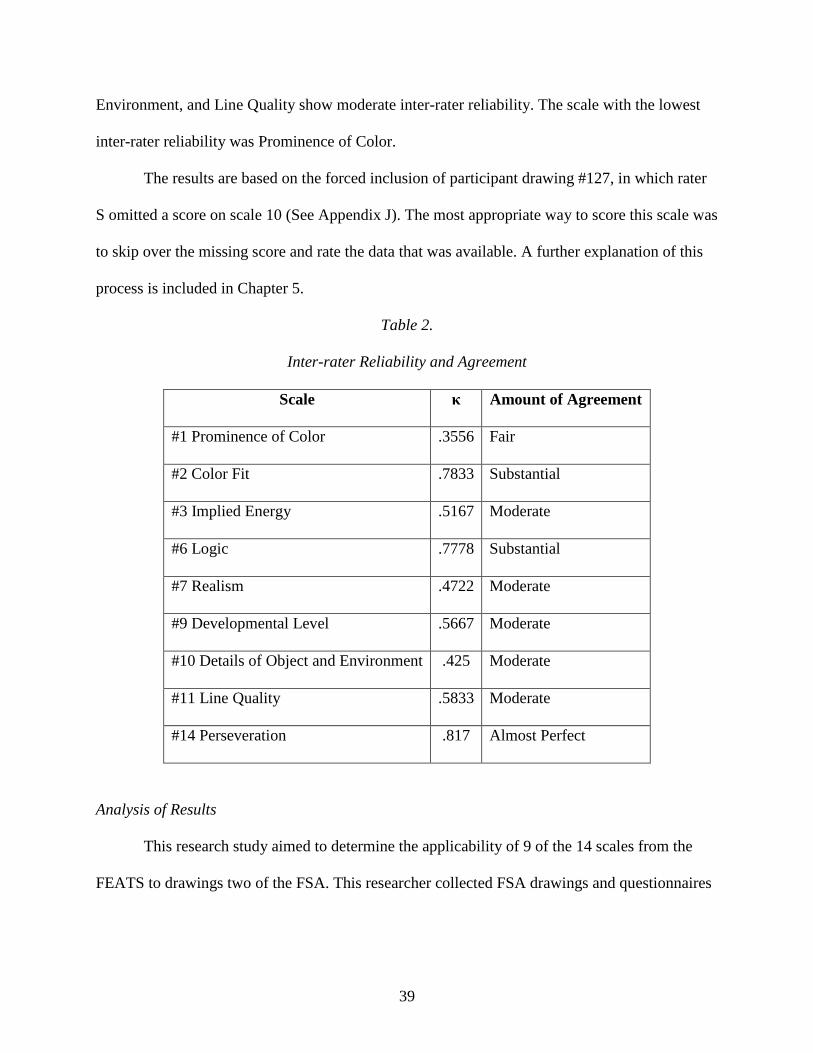
39
Environment, and Line Quality show moderate inter-rater reliability. The scale with the lowest
inter-rater reliability was Prominence of Color.
The results are based on the forced inclusion of participant drawing #127, in which rater
S omitted a score on scale 10 (See Appendix J). The most appropriate way to score this scale was
to skip over the missing score and rate the data that was available. A further explanation of this
process is included in Chapter 5.
Table 2.
Inter-rater Reliability and Agreement
Scale κ Amount of Agreement
#1 Prominence of Color .3556 Fair
#2 Color Fit .7833 Substantial
#3 Implied Energy .5167 Moderate
#6 Logic .7778 Substantial
#7 Realism .4722 Moderate
#9 Developmental Level .5667 Moderate
#10 Details of Object and Environment .425 Moderate
#11 Line Quality .5833 Moderate
#14 Perseveration .817 Almost Perfect
Analysis of Results
This research study aimed to determine the applicability of 9 of the 14 scales from the
FEATS to drawings two of the FSA. This researcher collected FSA drawings and questionnaires

40
from a normative sample of undergraduate college student (N = 30). Trained raters used 9
FEATS scales to score the 30 FSA drawings.
The initial analysis of the results reviewed the descriptive demographic information of
the normative population (N = 30). The participants ranged in age from 19 to 28, one participant
either refused or neglected to answer (See Figure 3). The average mean age was 22.517, the
median age was 22, and the mode age was 21. Of the 30 participants, 6 were male and 24 were
female (See Figure 1). The ethnic groups in the sample included: American Indian or Alaskan
Native (n = 0), Asian or Pacific Islander (n = 1), Black, Not of Hispanic Origin (n = 4), Hispanic
(n = 4), White, Not of Hispanic Origin (n = 21), and participants who did not report their
ethnicities (n = 0) (See Figure 2).
Figure 1.
Gender Distribution Graph
0
5
10
15
20
25
Male Female
Male
Female
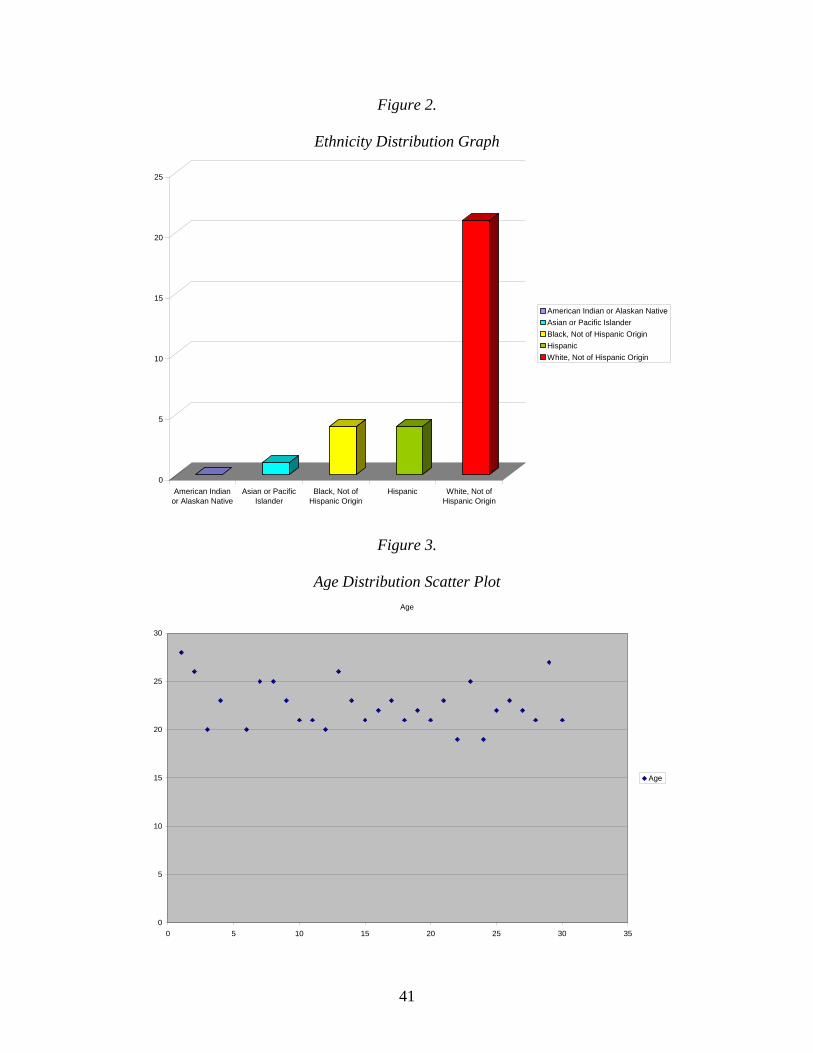
41
Figure 2.
Ethnicity Distribution Graph
0
5
10
15
20
25
American Indian
or Alaskan Native
Asian or Pacific
Islander
Black, Not of
Hispanic Origin
Hispanic White, Not of
Hispanic Origin
American Indian or Alaskan Native
Asian or Pacific Islander
Black, Not of Hispanic Origin
Hispanic
White, Not of Hispanic Origin
Figure 3.
Age Distribution Scatter Plot
Age
0
5
10
15
20
25
30
0 5 10 15 20 25 30 35
Age
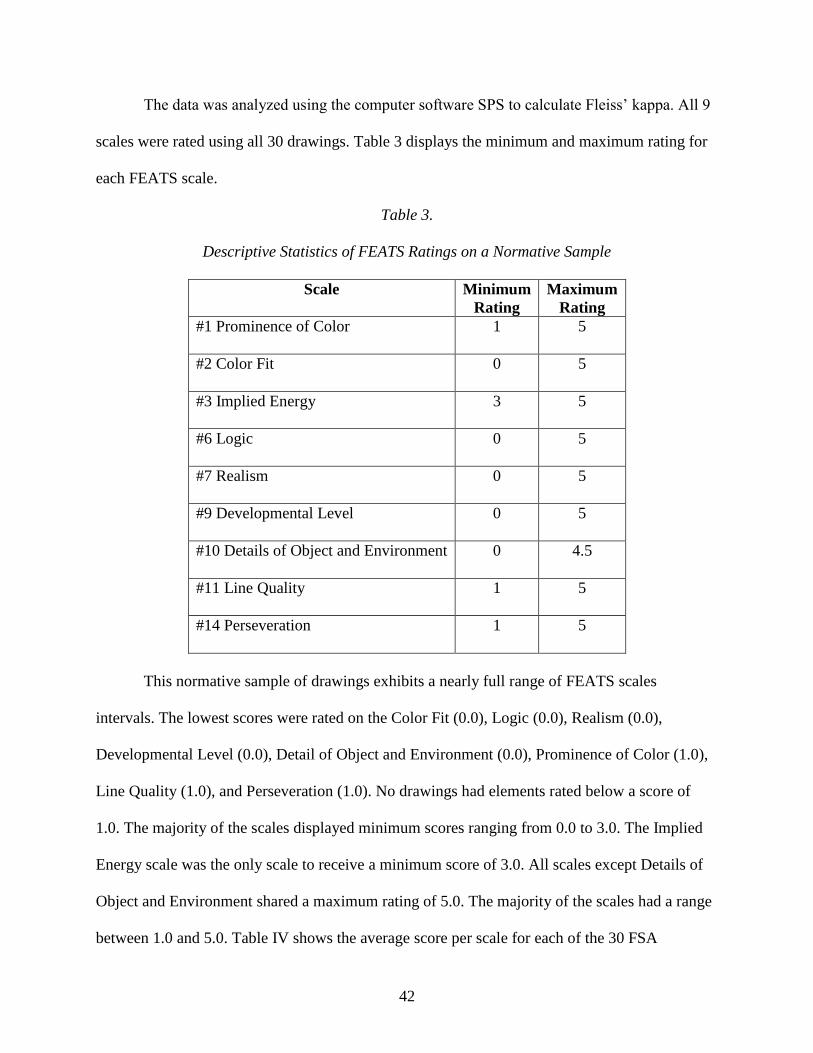
42
The data was analyzed using the computer software SPS to calculate Fleiss‟ kappa. All 9
scales were rated using all 30 drawings. Table 3 displays the minimum and maximum rating for
each FEATS scale.
Table 3.
Descriptive Statistics of FEATS Ratings on a Normative Sample
Scale Minimum
Rating
Maximum
Rating
#1 Prominence of Color 1 5
#2 Color Fit 0 5
#3 Implied Energy 3 5
#6 Logic 0 5
#7 Realism 0 5
#9 Developmental Level 0 5
#10 Details of Object and Environment 0 4.5
#11 Line Quality 1 5
#14 Perseveration 1 5
This normative sample of drawings exhibits a nearly full range of FEATS scales
intervals. The lowest scores were rated on the Color Fit (0.0), Logic (0.0), Realism (0.0),
Developmental Level (0.0), Detail of Object and Environment (0.0), Prominence of Color (1.0),
Line Quality (1.0), and Perseveration (1.0). No drawings had elements rated below a score of
1.0. The majority of the scales displayed minimum scores ranging from 0.0 to 3.0. The Implied
Energy scale was the only scale to receive a minimum score of 3.0. All scales except Details of
Object and Environment shared a maximum rating of 5.0. The majority of the scales had a range
between 1.0 and 5.0. Table IV shows the average score per scale for each of the 30 FSA
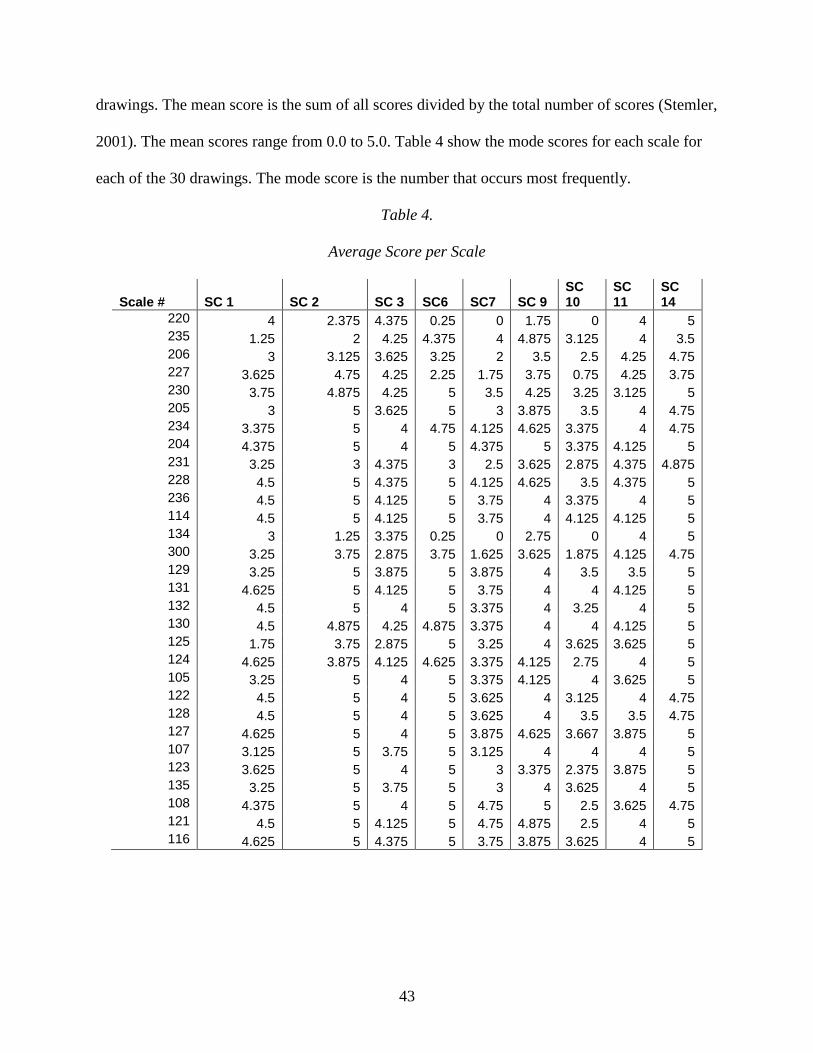
43
drawings. The mean score is the sum of all scores divided by the total number of scores (Stemler,
2001). The mean scores range from 0.0 to 5.0. Table 4 show the mode scores for each scale for
each of the 30 drawings. The mode score is the number that occurs most frequently.
Table 4.
Average Score per Scale
Scale # SC 1 SC 2 SC 3 SC6 SC7 SC 9
SC 10
SC 11
SC 14
220 4 2.375 4.375 0.25 0 1.75 0 4 5 235 1.25 2 4.25 4.375 4 4.875 3.125 4 3.5 206 3 3.125 3.625 3.25 2 3.5 2.5 4.25 4.75 227 3.625 4.75 4.25 2.25 1.75 3.75 0.75 4.25 3.75 230 3.75 4.875 4.25 5 3.5 4.25 3.25 3.125 5 205 3 5 3.625 5 3 3.875 3.5 4 4.75 234 3.375 5 4 4.75 4.125 4.625 3.375 4 4.75 204 4.375 5 4 5 4.375 5 3.375 4.125 5 231 3.25 3 4.375 3 2.5 3.625 2.875 4.375 4.875 228 4.5 5 4.375 5 4.125 4.625 3.5 4.375 5 236 4.5 5 4.125 5 3.75 4 3.375 4 5 114 4.5 5 4.125 5 3.75 4 4.125 4.125 5 134 3 1.25 3.375 0.25 0 2.75 0 4 5 300 3.25 3.75 2.875 3.75 1.625 3.625 1.875 4.125 4.75 129 3.25 5 3.875 5 3.875 4 3.5 3.5 5 131 4.625 5 4.125 5 3.75 4 4 4.125 5 132 4.5 5 4 5 3.375 4 3.25 4 5 130 4.5 4.875 4.25 4.875 3.375 4 4 4.125 5 125 1.75 3.75 2.875 5 3.25 4 3.625 3.625 5 124 4.625 3.875 4.125 4.625 3.375 4.125 2.75 4 5 105 3.25 5 4 5 3.375 4.125 4 3.625 5 122 4.5 5 4 5 3.625 4 3.125 4 4.75 128 4.5 5 4 5 3.625 4 3.5 3.5 4.75 127 4.625 5 4 5 3.875 4.625 3.667 3.875 5 107 3.125 5 3.75 5 3.125 4 4 4 5 123 3.625 5 4 5 3 3.375 2.375 3.875 5 135 3.25 5 3.75 5 3 4 3.625 4 5 108 4.375 5 4 5 4.75 5 2.5 3.625 4.75 121 4.5 5 4.125 5 4.75 4.875 2.5 4 5 116 4.625 5 4.375 5 3.75 3.875 3.625 4 5

44
Table 5.
Mode Score per Scale
Scale # SC 1 SC 2 SC 3 SC6 SC7 SC 9
SC 10
SC 11
SC 14
220 4 0 4.5 0 0 3 0 4 5 235 1 2 4 5 4 5 5 5 206 3 4 5 2 4 3 4 5 227 3 5 4 4 5 1 4.5 5 230 4 5 4.5 5 3 4 3 5 205 3 5 4 5 3 4 4 4 5 234 3 5 4 5 4 5 4 4 5 204 4 5 4 5 4 5 4.5 5 231 3 3 4 4.5 3 4 3 4 5 228 5 5 4.5 5 4 5 4 4 5 236 5 5 4 5 4 4 4 4 5 114 5 5 4 5 4 4 4 5 134 3 0 3 0 0 5 0 4 5 300 3 3 3 4 2 2 4 5 129 3 5 4 5 4 4 3.5 5 131 5 5 4 5 3.5 4 4 4 5 132 5 5 4 5 3 4 3 4 5 130 5 5 4.5 5 3 4 4 4 5 125 1 5 3 5 3 4 3 4 5 124 5 4 4 5 3 4 3 4 5 105 3.5 5 4 5 3 4 4 4 5 122 5 5 4 5 3.5 4 3 4 5 128 5 5 4 5 4 4 3.5 3.5 5 127 5 5 4 5 4 5 4 4 5 107 3 5 3.5 5 3 4 4 4 5 123 3 5 4 5 3 3 2 4 5 135 3 5 3.5 5 3 4 4 4 5 108 4 5 4 5 4.5 5 2 4 5 121 5 5 4 5 5 5 2 4.5 5 116 5 5 4 5 3.5 4 3.5 4 5
Conclusions
This chapter presented the results and analysis of the FSA drawings rated with 9 scales
from the FEATS. Significant norms for the FEATS scales were discussed. In addition, the results
for trends in the subgroups gender, ethnicity, and age were highlighted. The findings indicated
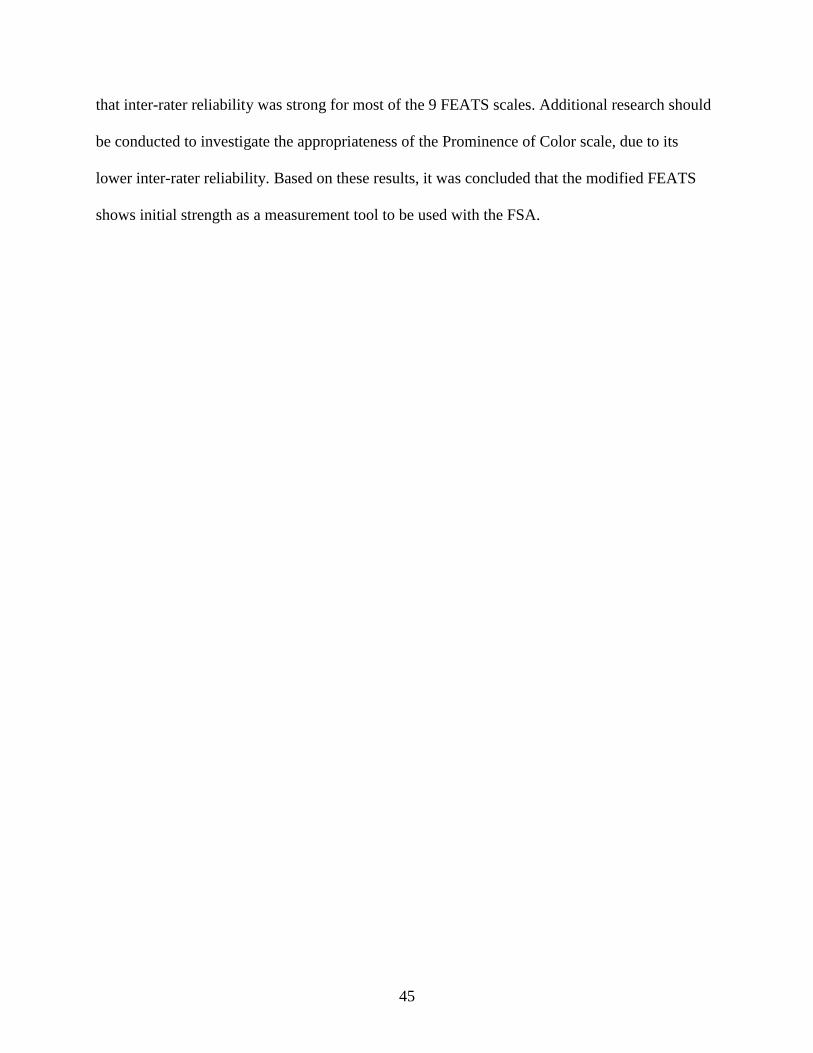
45
that inter-rater reliability was strong for most of the 9 FEATS scales. Additional research should
be conducted to investigate the appropriateness of the Prominence of Color scale, due to its
lower inter-rater reliability. Based on these results, it was concluded that the modified FEATS
shows initial strength as a measurement tool to be used with the FSA.
46
CHAPTER 5
DISCUSSION
The final chapter in this research paper highlights the author‟s conclusions about the
entire study. This chapter examines the data collection and the research findings. Limitations of
the study are discussed and the author‟s suggestions for further research are outlined. Finally, the
conclusions and implications of the study are discussed.
This research study looked at 30 drawings from a normative college student population.
The drawings were rated using 9 scales from the FEATS. Statistical techniques were used to
calculate inter-rater reliability between all 4 raters on the 9 FEATS scales. The results were
analyzed and the significant outcomes were reported. The findings produced answers to the
research questions outlined at the beginning of the study. The following sections look at the
collected data, look at the outcomes, and highlight conclusions about the findings.
Research Questions
The underlying idea of this research study was to develop a standardized rating system
for the FSA by adapting 9 scales from the Formal Elements Art Therapy Scale which included:
Prominence of Color, Color Fit, Energy, Space, Integration, Logic, Realism, Problem-solving,
Developmental Level, Details of Object and Environment, Line Quality, and Perseveration
(Gantt & Tabone, 1998).
The research question was: To what extent can scales from the FEATS be used to
successfully rate drawings from the modified FSA? An additional question includes: To what
extent will inter-rater reliability be achieved among raters of the modified FSA drawings? The
findings from this study will be helpful in establishing reliability and validity for the Face

47
Stimulus Assessment. Conclusions about the research results are presented in the following
sections.
Inter-rater Reliability Issues
A total of four raters participated in rating the FSA drawings. The raters included: rater 1
was Donna Betts (D), rater 2 Sheila Lorenzo (S), rater 3 this author Michelle Hamilton (M), and
rater 4 Nannie Mead (N). This researcher attempted to improve inter-rater reliability by
recruiting an experienced trainer to train the raters. The trainer Donna Betts, creator of the FSA,
was chosen due to her experience with the FSA and FEATS and years of experience as an art
therapist and art therapy researcher. Rater 3 and 4 were located in the Midwest and were trained
in a training session via phone and internet by the trainer. Rater 2 was trained in an identical
training session in the presence of the trainer. During the training session, the trainer reviewed
each of the 9 FEATS scales (See Appendix B) and provided the trainees with sample drawings
(See Appendix D) to be used as guides with the modified FEATS.
The first issue related to inter-rater reliability is consistency in training. Ideally, all raters
would have been trained together in one training session. In the interest of distance and time, the
best option was to hold two training sessions. Future studies may investigate the difference in
inter-rater reliability when all raters are trained together. A second issue arises from the use of
this author and the creator of the FSA as raters. This author and the creator of the FEATS, Donna
Betts, participated in the rating process and took a hands-on approach to the research project. To
decrease rater bias, this author and the FSA creator could have been included and their results
compared to the results of the other raters to detect any biases. The third inter-rater reliability
issue concerns rater awareness of the research hypothesis. Rater 2 was the only rater blind to the
study. The final issue related to inter-rater reliability was missing data on drawing #127 scale
48
10. Rater 2 neglected to respond to this question, which affected the inter-rater reliability on the
Details of Objects and Environment Scale. Overall the issues of inter-rater reliability do not
appear to have confounded the results of the study. Additional research should be conducted to
further study the affects of these variables.
Limitations of the Study
There are a number of factors that limit the applicability of the research study results.
First, size and population significantly limit the overall generalizability of the study. The study
participants were recruited from a local university. The sample was a normative convenience
sample, and only 30 participants volunteered to participate. Ideally, the participants would have
been randomly selected. Because the sample was normative, the individual participant
characteristics were not varied in age, race, gender, socioeconomic status, education background,
or psychiatric diagnosis. The majority of the participants in this study were white females
between the ages of 19 and 28. Preferably, the normative population would have been more
representative of a random sample.
Secondly, the study was limited by population sample size. This researcher originally
planned to gather a sample of 50 to 75 participants. Unfortunately, the population size was
significantly smaller. Ideally, the sample size would range from 150 to 200 participants to
achieve statistically significant results. Future research endeavors should investigate the use of a
larger sample size.
Finally, the FSA assessments were administered in a classroom setting to a group of 10 to
15 people over three separate sessions. Environmental variables were somewhat varied between
the three sessions, but this researcher made every attempt to minimize these factors. Ideally, to
49
minimize compounding variables the FSA could have been administered to the randomly
selected participants on an individual basis in a controlled environment.
Recommendation for Future Research
Further research endeavors should attempt to substantiate and support the data collected
in this study and attempt to establish tests for reliability and validity for the use of the modified
FEATS with the adapted FSA. Future studies could be conducted at other larger college
campuses with a random sample of students from a more diverse population of participants.
Studies on the use of the modified FEATS with the FSA will provide helpful information about
specific population characteristics. Additional research could also investigate differences in
gender, age, educational background, socioeconomic status, artistic experience, and ethnicity
among participants.
Further normative studies should also be conducted due to their usefulness in better
understanding art therapy assessments (Bucciarelli, 2007). Larger samples of drawings could
also be used to investigate the correlation between raters. Before the FSA can be used in
experimental studies more normative studies should be conducted and inter-rater reliability
tested further. Future studies should also investigate the use of raters who are blind to the
research purpose. Raters that are not invested in the study should be used to investigate biases.
All future research efforts involving the FSA will ultimately result in strengthening its use as a
valid and reliable art therapy assessment.
Conclusions
The purpose of this study was to investigate the applicability of 9 scales from the FEATS
to a modified version of the FSA using a normative sample of college students. This paper
50
provided justification for the research study, and presented a detailed research question and
hypothesis. The relevant terms were defined in relation to the study.
Additionally, the literature review highlighted the history of art therapy assessments
including their development, strengths, and limitations. Relevant information about various art
therapy assessments were highlighted. Then the FSA and FEATS were described in detail,
including their development and recommendations for further development.
The methodology chapter begins with the development of the research including the
research design and procedures that were used in this study. The study included volunteer
participants from a normative convenience sample of college students at a local university. The
students were asked to complete the FSA and a short questionnaire. The 30 drawings were rated
using the modified FEATS then statistically analyzed using Fleiss‟ kappa to determine inter-rater
reliability. Internal and external validity were examined followed by the ethical concerns of the
study.
Finally, the results were examined and shown to support the research hypothesis. Strong
inter-rater reliability was established for most of the 9 scales, with the exception of the
Prominence of Color scale. This research study contributes to the collection of current FSA
research and provides a foundation for further research endeavors. Outcomes of this study not
only support the use of the modified FEATS with the FSA, but also lends support to further
research to establish reliability and validity for the FSA. This study can provide a foundation for
larger studies to examine the use of the FSA in both clinical and research settings. Researchers
and clinicians can hopefully use the results of this study to jumpstart future research endeavors
involving the Face Stimulus Assessment.

51
APPENDIX A
MODIFIED FSA TEMPLATE
52

53
APPENDIX B
ADAPTED FEATS SCALES FOR USE WITH THE FSA
FEATS Scales Adapted for use with the Face Stimulus Assessment (FSA)
April 2008
SCALE #1 – PROMINECE OF COLOR
How much color is used? Is the color only used to define an item or shape or is it used to color in
the item or shape?
This variable cannot be rated. The person did not do the drawing or the person did not
use the required materials.
0
Color is used only to outline the forms or objects in the picture, or to make lines; none
of the forms are colored in.
1
Color is used for outlining most of the forms or objects, but only one form or object is
filled in (such as the face, the neck, or the background). [For small elements such as
an earring, it may be difficult to decide whether it is just outlined or filled in as well
as outlined.]
2
Two or more (but not all) forms or objects are colored in. 3
Color is used for both outlining the forms and objects and filling them in. 4
Color is used to outline the forms and objects, to color them in, and to fill in the space
around the forms (for example, a completely colored face).
5
SCALE #2 – COLOR FIT
How well do the colors fit the facial features and objects in the drawing?
Given the colors in the sets of markers, several are suitable for coloring the face and might relate
to an ethnic group identification: each of the eight Multicultural markers, and from the other set
of Crayola markers, black, brown, yellow, orange, or red. However, blue, green, or violet are not
appropriate colors for parts of the body (such as face or hands).
This variable cannot be rated. The person did not use the specified materials, or the
colors are difficult or impossible to distinguish from each other.
0
The entire picture is drawn in only one color, and that color is blue, green, or violet. 1
The entire picture is drawn in only one color, and that color is black, brown, yellow,
orange, red, or any of the eight Multicultural markers.
2
Some colors (but not all) are used appropriately. 3
Most of the colors are used appropriately. 4
All the colors are appropriate to the specific facial features and objects in the picture. 5
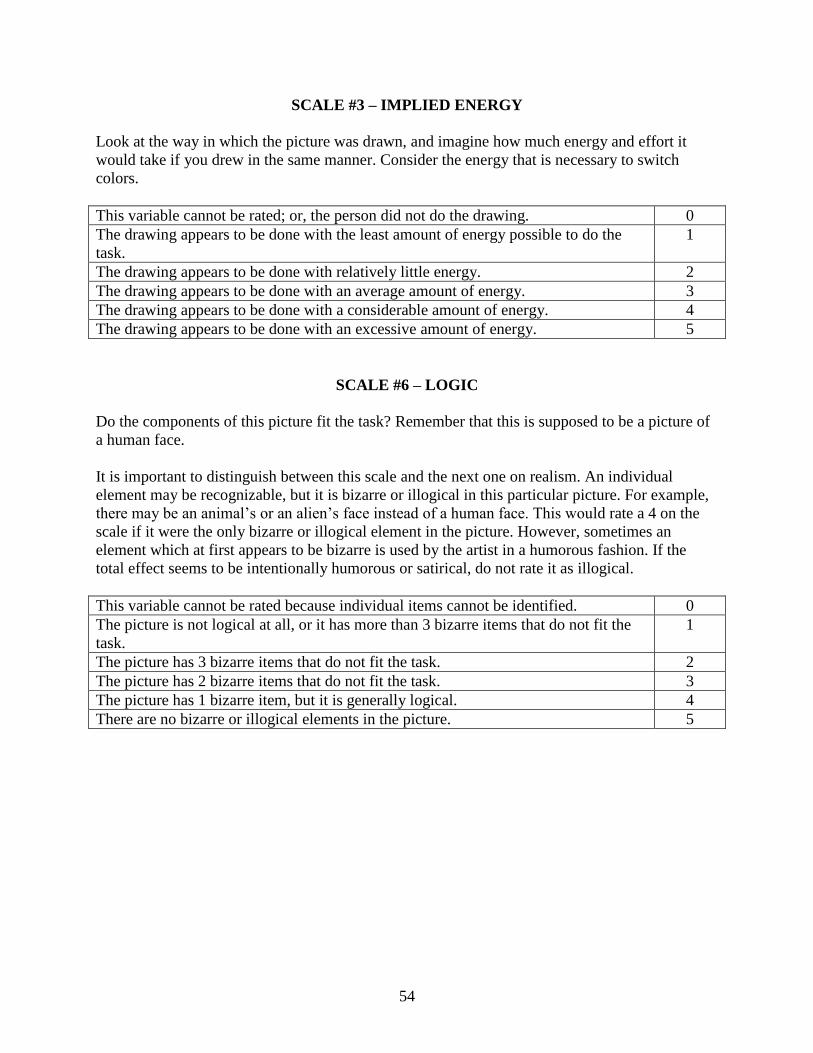
54
SCALE #3 – IMPLIED ENERGY
Look at the way in which the picture was drawn, and imagine how much energy and effort it
would take if you drew in the same manner. Consider the energy that is necessary to switch
colors.
This variable cannot be rated; or, the person did not do the drawing. 0
The drawing appears to be done with the least amount of energy possible to do the
task.
1
The drawing appears to be done with relatively little energy. 2
The drawing appears to be done with an average amount of energy. 3
The drawing appears to be done with a considerable amount of energy. 4
The drawing appears to be done with an excessive amount of energy. 5
SCALE #6 – LOGIC
Do the components of this picture fit the task? Remember that this is supposed to be a picture of
a human face.
It is important to distinguish between this scale and the next one on realism. An individual
element may be recognizable, but it is bizarre or illogical in this particular picture. For example,
there may be an animal‟s or an alien‟s face instead of a human face. This would rate a 4 on the
scale if it were the only bizarre or illogical element in the picture. However, sometimes an
element which at first appears to be bizarre is used by the artist in a humorous fashion. If the
total effect seems to be intentionally humorous or satirical, do not rate it as illogical.
This variable cannot be rated because individual items cannot be identified. 0
The picture is not logical at all, or it has more than 3 bizarre items that do not fit the
task.
1
The picture has 3 bizarre items that do not fit the task. 2
The picture has 2 bizarre items that do not fit the task. 3
The picture has 1 bizarre item, but it is generally logical. 4
There are no bizarre or illogical elements in the picture. 5

55
SCALE #7 – REALISM
Can you recognize all the elements in the picture? The more realistic and three-dimensional the
elements are, the higher the rating would be.
The Person scale seeks to determine if “the person in the picture looks like a three-dimensional
person rather than a stick figure” (p. 41). This is related to qualities defined in the Realism scale.
Thus, this scale (Realism) is combined with the original FEATS scale #12, Person. Gantt and
Tabone (1998) asserted that if the person in a PPAT drawing “is severely distorted or fragmented
we assume the artist has a distorted or fragmented sense of self” (p. 41). It follows, therefore,
that a face drawn in the FSA that is severely distorted or fragmented would also reflect upon the
artist‟s sense of self.
The picture is a mass of lines and/or shapes and has no visually identifiable items in
it.
0
There are some elements which might have been intended by the artist to represent a
human face and/or accessories, however, they are no more than suggestive of these
elements.
1
The items are recognizable but simply drawn (ex., a triangle for a nose). 2
The items are somewhat complex (ex., eyes with pupils; ears, eyebrows). 3
The items are relatively realistically rendered (ex., the face has distinct features, such
as lips and/or teeth; the nose has nostrils or suggestion of nostrils; eyelids are shaded).
4
The items are drawn with a great deal of realism (ex., definition in chin; shading of
cheekbones; highlighting of nose; texture in hair).
5
SCALE #9 – DEVELOPMENTAL LEVEL
How would this picture be rated according to Lowenfeld‟s developmental levels? Determining
the developmental level is usually done with children‟s drawings. However, many people stop
drawing in adolescence; therefore, many adults will draw in the style of adolescents, not having
developed their artistic skill any further. The scale is used to give a rough estimate of the
developmental level. If children‟s drawings were being studied, we would need a more finely
gauged scale to rate them accurately.
This variable cannot be rated because the individual elements cannot be identified. 0
The drawing consists solely of scribbles or masses of lines and shapes. 1
The drawing is like those of four- to six-year-olds (ex., geometric shapes are
predominant, exaggerated facial features are typical).
2
The drawing is like those done by latency-age children (ex., more detail for individual
features).
3
The drawing is like those done by adolescents (with overlapping of objects and with
realistic sizes for each element in relation to the others).
4
The drawing is an “adult” drawing and shows some artistic sophistication or training. 5

56
SCALE #10 – DETAILS OF OBJECTS & ENVIRONMENT
How many extra items are there in the drawings? How detailed are the various items?
This variable cannot be rated because individual items cannot be identified. 0
There is nothing but a few elements such as facial features, and these are drawn
simply with little detail (ex., dots or circles for eyes, a suggestion of a nose, and a
basic mouth).
1
In addition to facial features, one or two other details are added (ex., a neckline; hair;
a piece of jewelry; an object in the background).
2
In addition to facial features, there are two or three additional details (ex., a horizon
line; a hat; a beard and/or moustache).
3
In addition to facial features, there are a number of details such as a horizon line,
jewelry, hair bows, glasses, eyelashes.
4
In addition to facial features, other facial details and accessories, there are abundant
and inventive details such as a pattern on clothing and objects in the background (ex.,
the sun; clouds; grass; trees; other objects).
5
SCALE #11 – LINE QUALITY
How much control did the artist have when drawing the lines in the picture? Consider the
“average” of the whole picture.
This variable cannot be rated. 0
In general, the lines appear to be drawn erratically with no apparent control. 1
The lines appear to be drawn with a shaking hand. 2
Some lines are continuous and some lines have gaps in them, or are made of a series
of dots or dashes.
3
The lines are under control. 4
The lines are quite fluid or flowing (even excessively so). 5
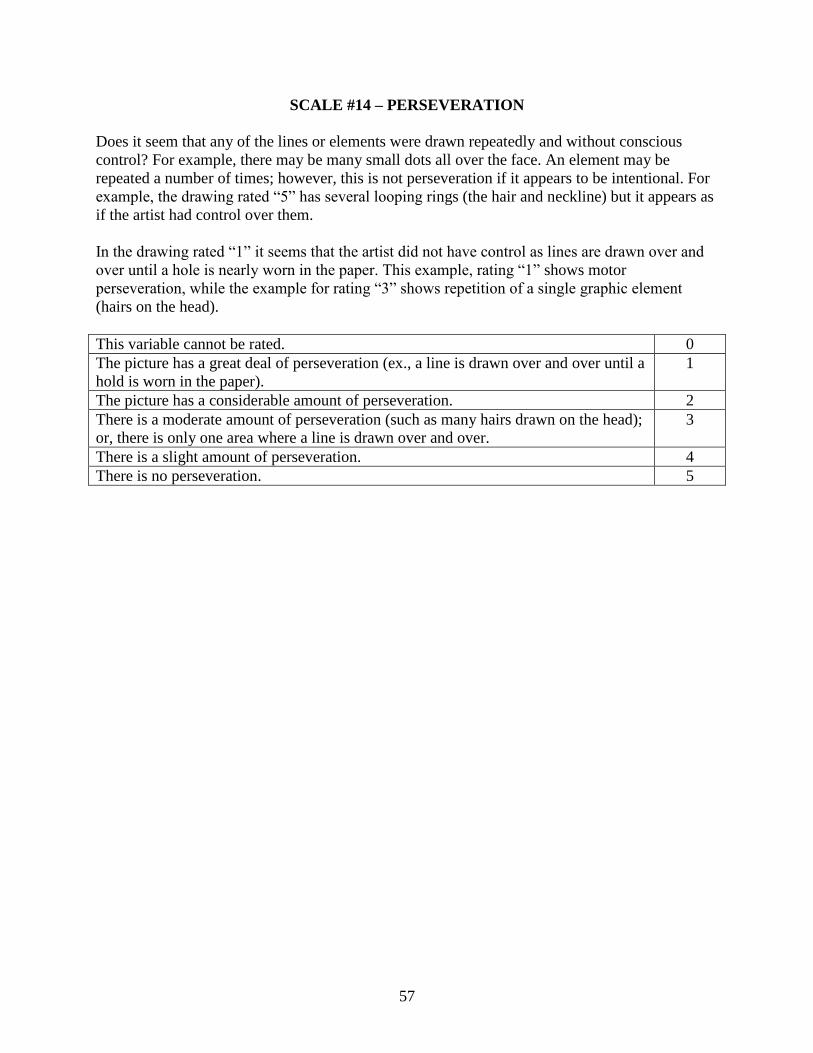
57
SCALE #14 – PERSEVERATION
Does it seem that any of the lines or elements were drawn repeatedly and without conscious
control? For example, there may be many small dots all over the face. An element may be
repeated a number of times; however, this is not perseveration if it appears to be intentional. For
example, the drawing rated “5” has several looping rings (the hair and neckline) but it appears as
if the artist had control over them.
In the drawing rated “1” it seems that the artist did not have control as lines are drawn over and
over until a hole is nearly worn in the paper. This example, rating “1” shows motor
perseveration, while the example for rating “3” shows repetition of a single graphic element
(hairs on the head).
This variable cannot be rated. 0
The picture has a great deal of perseveration (ex., a line is drawn over and over until a
hold is worn in the paper).
1
The picture has a considerable amount of perseveration. 2
There is a moderate amount of perseveration (such as many hairs drawn on the head);
or, there is only one area where a line is drawn over and over.
3
There is a slight amount of perseveration. 4
There is no perseveration. 5

58
APPENDIX C
MODIFIED FEATS RATING
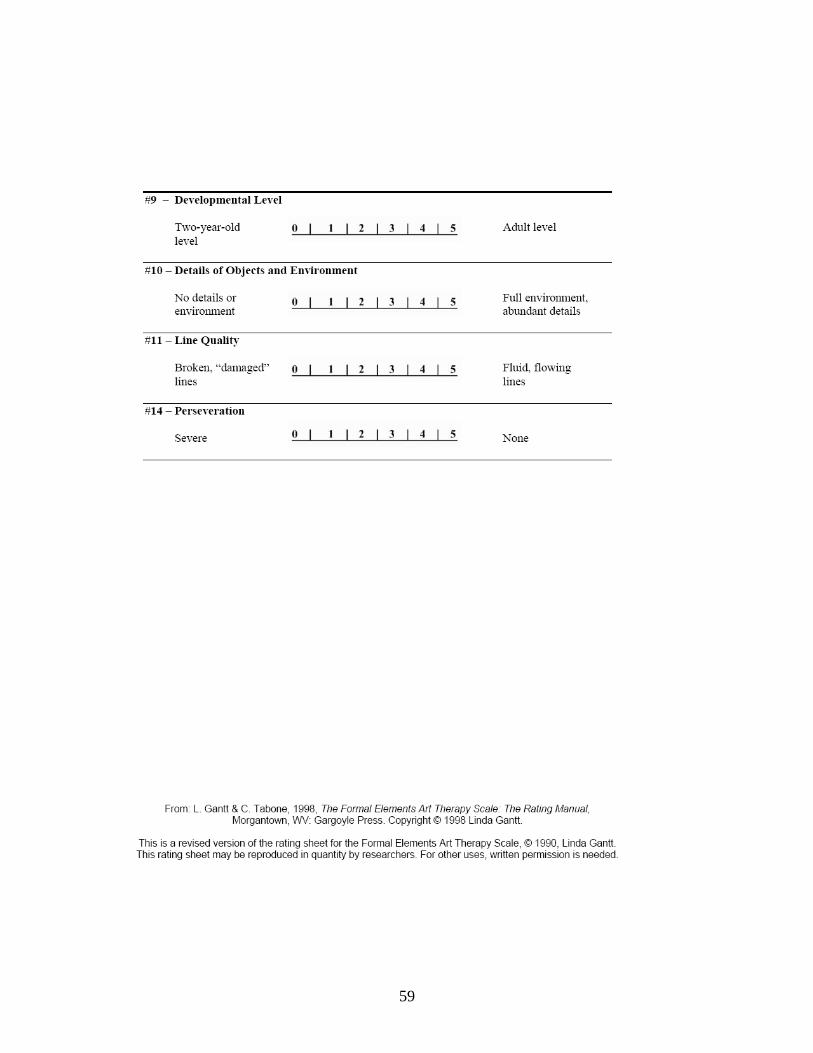
59
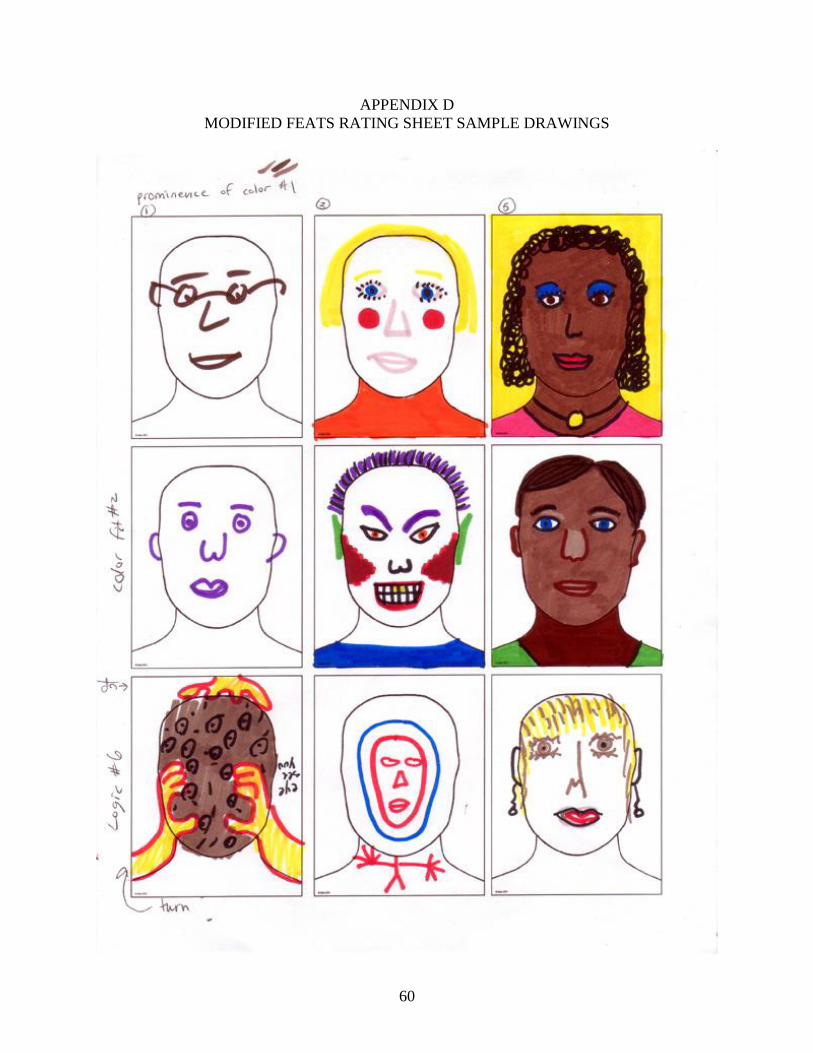
60
APPENDIX D
MODIFIED FEATS RATING SHEET SAMPLE DRAWINGS

61

62

63
APPENDIX E
DEMOGRAPHIC INFORMATION SURVEY FOR RESEARCH PARTICIPANTS
The purpose of this study is to provide information about the use of an art therapy assessment on
a normative undergraduate college student population. Please provide the following information
along with your drawings for use in this research project:
1. What is your current age? _____
2. What is your gender?
Male
Female
3. What is your ethnic background (choose only one)?
American Indian or Alaskan Native - A person having origins in any of the
original peoples of North America, and who maintains cultural identification
through community recognition or tribal affiliation.
Asian or Pacific Islander - A person having origins in any of the original
peoples of the Far East, Southeast Asia, the Indian subcontinent, or the Pacific
Islands. This area includes, for example, China, India, Japan, Korea, the Philippine
Islands and Samoa.
Black, Not of Hispanic Origin - A person having origins in any of the black
racial groups of Africa. Does not include persons of Mexican, Puerto Rican, Cuban,
Central or South American, or other Spanish cultures or origins (See Hispanic).
Hispanic - A person having Mexican, Puerto Rican, Cuban, Central or South
American, or other Spanish cultures or origins (Regardless of Race). Does not
include persons of Portuguese culture or origin.
White, Not of Hispanic Origin - A person having origins in any of the original
peoples of Europe, North Africa, or the Middle East. Does not include persons of
Mexican, Puerto Rican, Cuban, Central or South American, or other Spanish
cultures or origins (See Hispanic). Also includes persons not included in other
categories.
4. Do you have experience creating art? ______
5. Have you had formal art training (i.e. elementary, high school, or college)? ___________
6. When was the last time you had formal training in art? ___________________________
7. If you do create art what is your preferred medium?______________________________
8. Have you used Crayola Multicultural markers before? ______ If yes, how long
ago?_____
9. What are your thoughts about this activity? (please respond in the space provided or on
the back)
64
APPENDIX F
CONSENT FORM
CONSENT TO SERVE AS A SUBJECT IN RESEARCH
I have been informed that this study involves research which will be conducted by Michelle Hamilton, a
student at Avila University. I understand that this project is designed to study the use of an art therapy
assessment on a normative undergraduate college student population. I understand that my participation
in this study will involve the creation of two assessment drawings. I am aware that my involvement in
this study will take approximately 40 minutes.
I understand that I may refuse to participate or withdraw from this study at any time without any penalty
or loss of services that I am entitled to. I understand that my identity as a participant in this study will be
kept in confidence and that no information that identifies me in any way will be released without my
separate written approval. I also understand that there may be risks to my anonymity in the event that
other group members may be able to identify my drawings by the information I provide in the
demographics survey, which includes age, gender, ethnicity, and previous art experience.
I have been informed that upon the completion of this study an Avila University Counseling and Art
Therapy Research Database will be created in which my drawings and demographic information will be
stored. This database will be accessible by the public and will include the drawings as well as the
demographic information I provided.
I am aware that although I may not directly benefit from this study, my participation in this project may
benefit research in the area of counseling and art therapy research, more specifically, research in the area
of art therapy assessment.
If you would like additional information concerning this study before or after it is complete, please feel
free to contact me by phone or mail. If you have concerns or questions about your rights as a research
participant you may contact the Avila University Research Review Board at 816-501-3759 or Sue King at
I understand that I will be signing two copies of this form. I will keep one copy and Michelle Hamilton
will keep the second copy for her records.
I have read this form and understand what it says. I am 18 years or older and voluntarily agree to
participate in this research project.
Sincerely,
Michelle Hamilton, Laura Aube‟ MS, LPC, ATR-BC
Principal Investigator Faculty Supervisor
Master‟s of Counseling and Art Therapy Director of Counseling and Art Therapy
Avila University Avila University
11901 Wornall Road 11901 Wornall Road
Kansas City, MO 64145 Kansas City, MO 64145
816-686-4704 816-501-3792
_____________________________________ ________________________________
Participant‟s Signature Date

65
APPENDIX G
VERBAL DIRECTIONS
VERBAL DIRECTIONS AND REQUIRED STATEMENTS
Required Statements Given to Participants Prior to Administration
“Hello, my name is Michelle Hamilton and I am a graduate student in the Counseling and
Art Therapy program. I am currently conducting a study using a previously established art
therapy assessment with the intent of creating a formal rating scale for this art therapy
assessment. Findings from this research study will have implications in a variety of areas. The
information gathered will be applicable to furthering the global usage of this art therapy
assessment. This information can be used by researchers to establish reliability and validity of
the assessment and its rating system. This assessment could have valuable implications for the
fields of counseling and art therapy. Although you may not directly benefit from this study, your
participation in this project may benefit research in the area of counseling and art therapy
research.
This project is designed to study the use of an art therapy assessment on a normative
undergraduate college student population. If you agree to participate in this study please
understand that your participation will involve the creation of two assessment drawings. Your
participation in this study will take approximately 40 minutes to complete.
Please understand that you may refuse to participate or withdraw from this study at any
time without any penalty or loss of services that you are entitled to. Your identity as a participant
in this study will be kept in confidence and no information that identifies you in any way will be
released without your separate written approval. Please understand that there may be risks to
your anonymity in the event that other group members may be able to identify your drawings by
66
the information you provide in the demographics survey, which includes age, gender, ethnicity
and previous art experience.
If you agree to participate, the original artwork will be stored by this researcher in a
locked file cabinet with a key only accessible to me. Upon completion of this study an Avila
University Counseling and Art Therapy Research Database will be created in which your
drawings and demographic information will be stored. All identifiable information will be
removed from the artwork to protect the anonymity and confidentiality of each study participant.
This database will be accessible by the public and will include the drawings as well as the
demographic information you provided.
I am now going to hand out two copies of a form titled Consent to Serve as a Subject in
Research (Pass out consent forms). Read the consent form and if you agree to these terms and
conditions please sign both copies. You will keep one for your records and I will keep one for
my records” (Collect consent forms).
Verbal Directions Given to Participants Prior to Administration
“Now I am going to pass out the first of two drawing tasks. Each of the two drawings has
been randomly labeled with the same number in order to keep them together once they are
collected. You will have thirty minutes to complete both stimulus drawings. At the 15 minute
mark I will announce that there are 15 minutes remaining. Then at the 25 minute mark I will
announce that there are 5 minutes remaining until the end of the assessment session.
When you are finished with the first drawing please raise your hand and I will collect the
first drawing and give you the second to complete. When the entire group has completed both
drawings and the 30 minute time frame is up, I will give you a short survey which gathers
demographic information including age, gender, and ethnicity. This survey is also labeled with
67
the same number as your two drawings. In the interest of confidentiality and anonymity please
DO NOT LOOK at the drawings of other group members.
Okay, is everyone ready to start? Here is the first drawing. Please do not begin until
instructed to do so. (Pass out the first stimulus drawing and both sets of markers). You may
now begin, the instructions are as follows: “Use these markers and this piece of paper””.
Verbal Directions Given to Participants During Administration
1. At the 15 minute mark I will announce that there are 15 minutes remaining.
- “There are now 15 minutes remaining”
2. At the 25 minute mark I will announce that there are 5 minutes remaining until the end
of the session.
- “There are now 5 minutes remaining”
Verbal Directions Given to Participants After Administration
“The 30 minute time frame is now up. I will come around and collect your drawings
(Collect drawing number two). Thank you for your participation in my research study. If you
would please take a moment to complete the following demographics survey (Pass out
demographics survey). Thank you for your time and participation.”
68
APPENDIX H
PERMISSION LETTER FOR FSA

69
APPENDIX I
PERMISSION LETTER FOR FEATS

70
APPENDIX J
FEATS RATINGS OF MODIFIED FSA DRAWING TWO
Table 6.
FEATS Scales (1) Prominence of Color and (2) Color Fit
# Scale 1 Scale 2
D S M N D S M N
220 4 4 4 4 0 3.5 1 5
235 2 1 1 1 2 2 2 2
206 3 3 3 3 3 2 2.5 5
227 3 5 3.5 3 5 5 4 5
230 3 4 4 4 5 4.5 5 5
205 3 4 3 2 5 5 5 5
234 3 4.5 3 3 5 5 5 5
204 4.5 5 4 4 5 5 5 5
231 3 4 3 3 3 3 3 3
228 5 5 4 4 5 5 5 5
236 5 5 4 4 5 5 5 5
114 5 5 4 4 5 5 5 5
134 2 4 3 3 0 0 0 5
300 3 4 3 3 3 4 3 5
129 3 4 3 3 5 5 5 5
131 5 5 4.5 4 5 5 5 5
132 5 5 4 4 5 5 5 5
130 5 5 4 4 5 4.5 5 5
125 1 1 2 3 5 2 5 3
124 5 5 4.5 4 4.5 4 4 3
105 3.5 3.5 4 2 5 5 5 5
122 5 5 4 4 5 5 5 5
128 5 5 4 4 5 5 5 5
127 5 5 4.5 4 5 5 5 5
107 3 3.5 3 3 5 5 5 5
123 4 4.5 3 3 5 5 5 5
135 3 4 3 3 5 5 5 5
108 4.5 5 4 4 5 5 5 5
121 5 5 4 4 5 5 5 5
116 5 5 4 4.5 5 5 5 5
Rater Key:
D= Donna Betts S= Sheila Lorenzo M= Michelle Hamilton N= Nannie Mead

71
Table 7.
FEATS Scales (3) Implied Energy and (6) Logic
# Scale 3 Scale 6
D S M N D S M N
220 4.5 4.5 4.5 4 0 0 0 1
235 4 5 4 4 5 3.5 5 4
206 3.5 4 3 4 5 2 5 1
227 5 4 4 4 4 0 4 1
230 4.5 4.5 4 4 5 5 5 5
205 3.5 4 4 3 5 5 5 5
234 4 4 4 4 5 4 5 5
204 4 4 4 4 5 5 5 5
231 4.5 5 4 4 4.5 1 4.5 2
228 4.5 4.5 4 4.5 5 5 5 5
236 4.5 4 4 4 5 5 5 5
114 4.5 4 4 4 5 5 5 5
134 3 3 4 3.5 0 0 0 1
300 3 3.5 3 2 4 3 4 4
129 3.5 4 4 4 5 5 5 5
131 4.5 4 4 4 5 5 5 5
132 4 4 4 4 5 5 5 5
130 4.5 4 4.5 4 5 4.5 5 5
125 3 2.5 3 3 5 5 5 5
124 4.5 4 4 4 5 4.5 5 4
105 4 4 4 4 5 5 5 5
122 4 4 4 4 5 5 5 5
128 4 4 4 4 5 5 5 5
127 4 4 4 4 5 5 5 5
107 3.5 4 4 3.5 5 5 5 5
123 3.5 4.5 4 4 5 5 5 5
135 3.5 3.5 4 4 5 5 5 5
108 4 4 4 4 5 5 5 5
121 4 4.5 4 4 5 5 5 5
116 5 4 4 4.5 5 5 5 5
Rater Key:
D= Donna Betts S= Sheila Lorenzo M= Michelle Hamilton N= Nannie Mead

72
Table 8.
FEATS Scales (7) Realism and (9) Developmental Level
# Scale 7 Scale 9
D S M N D S M N
220 0 0 0 0 1 0 3 3
235 4 4 4 4 5 4.5 5 5
206 2 2 2 2 3.5 2.5 4 4
227 0.5 4 2.5 0 1 5 5 4
230 3.5 4.5 3 3 4.5 3.5 5 4
205 3 3 3 3 3.5 4 4 4
234 4 5 3.5 4 4.5 4 5 5
204 4 5 4.5 4 5 5 5 5
231 3 2 2 3 4 2.5 4 4
228 4 4.5 4 4 4.5 4 5 5
236 4 4 4 3 4 4 4 4
114 3 4.5 4 3.5 3.5 4.5 4 4
134 0 0 0 0 1 0 5 5
300 1.5 2 2 1 3.5 2 4 5
129 3.5 4 4 4 4 4 4 4
131 3.5 4 3.5 4 4 4 4 4
132 3 4 3.5 3 4 4 4 4
130 3 4 3.5 3 4 4 4 4
125 3 4 3 3 4 4 4 4
124 3 4 3.5 3 4 4 4.5 4
105 3 4.5 3 3 4 4.5 4 4
122 3.5 3.5 3.5 4 4 4 4 4
128 3 3.5 4 4 4 4 4 4
127 3.5 4 4 4 4.5 4 5 5
107 3 3.5 3 3 4 4 4 4
123 3 3 3 3 3.5 3 4 3
135 3 3 3 3 4 4 4 4
108 4.5 5 5 4.5 5 5 5 5
121 5 4 5 5 5 4.5 5 5
116 3.5 3.5 4 4 4 4 4 3.5
Rater Key:
D= Donna Betts S= Sheila Lorenzo M= Michelle Hamilton N= Nannie Mead
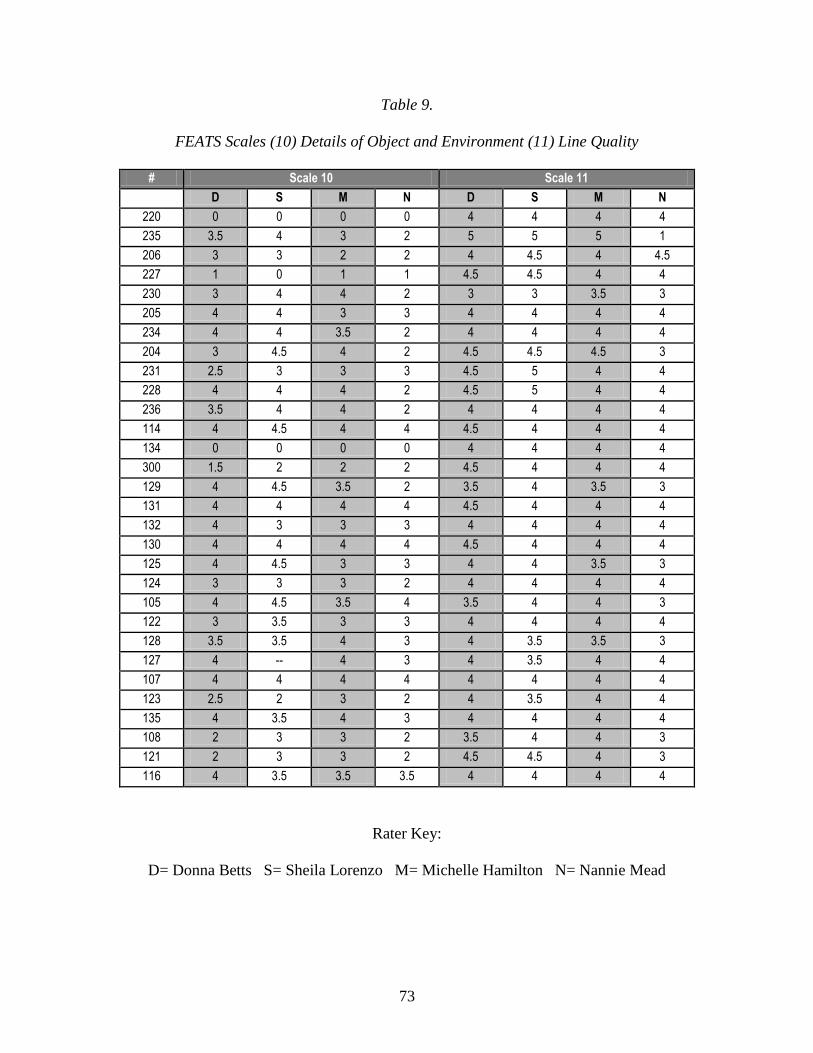
73
Table 9.
FEATS Scales (10) Details of Object and Environment (11) Line Quality
# Scale 10 Scale 11
D S M N D S M N
220 0 0 0 0 4 4 4 4
235 3.5 4 3 2 5 5 5 1
206 3 3 2 2 4 4.5 4 4.5
227 1 0 1 1 4.5 4.5 4 4
230 3 4 4 2 3 3 3.5 3
205 4 4 3 3 4 4 4 4
234 4 4 3.5 2 4 4 4 4
204 3 4.5 4 2 4.5 4.5 4.5 3
231 2.5 3 3 3 4.5 5 4 4
228 4 4 4 2 4.5 5 4 4
236 3.5 4 4 2 4 4 4 4
114 4 4.5 4 4 4.5 4 4 4
134 0 0 0 0 4 4 4 4
300 1.5 2 2 2 4.5 4 4 4
129 4 4.5 3.5 2 3.5 4 3.5 3
131 4 4 4 4 4.5 4 4 4
132 4 3 3 3 4 4 4 4
130 4 4 4 4 4.5 4 4 4
125 4 4.5 3 3 4 4 3.5 3
124 3 3 3 2 4 4 4 4
105 4 4.5 3.5 4 3.5 4 4 3
122 3 3.5 3 3 4 4 4 4
128 3.5 3.5 4 3 4 3.5 3.5 3
127 4 -- 4 3 4 3.5 4 4
107 4 4 4 4 4 4 4 4
123 2.5 2 3 2 4 3.5 4 4
135 4 3.5 4 3 4 4 4 4
108 2 3 3 2 3.5 4 4 3
121 2 3 3 2 4.5 4.5 4 3
116 4 3.5 3.5 3.5 4 4 4 4
Rater Key:
D= Donna Betts S= Sheila Lorenzo M= Michelle Hamilton N= Nannie Mead
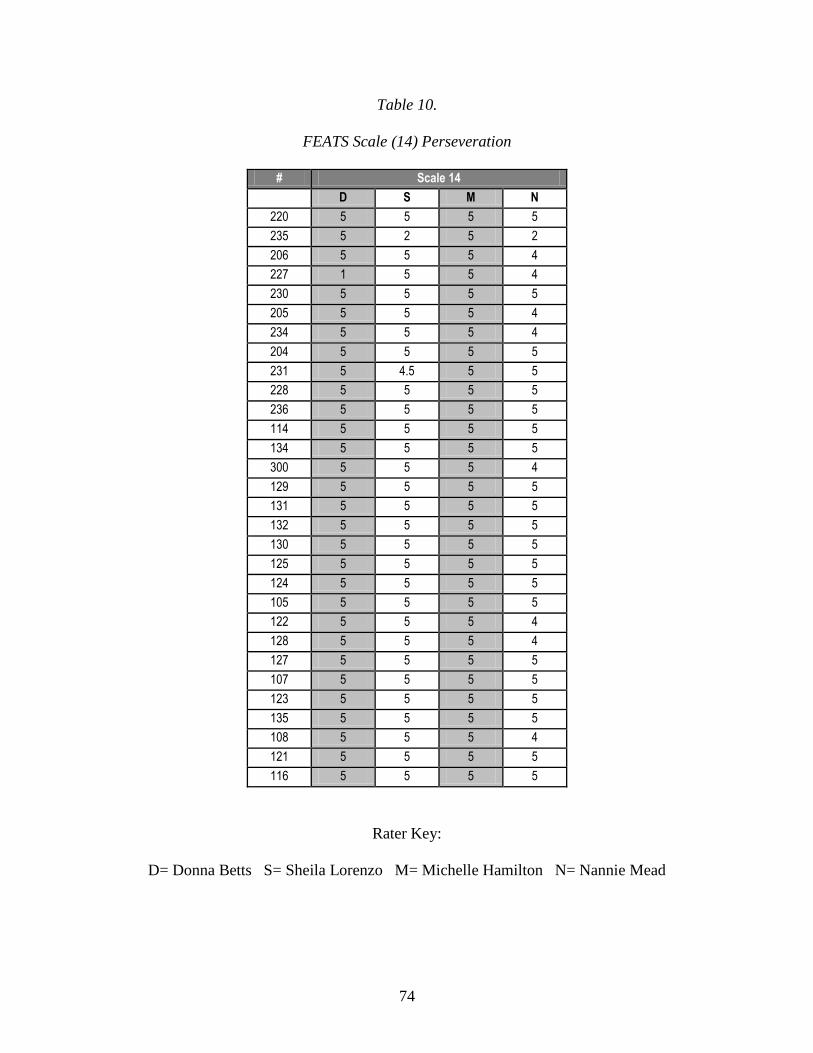
74
Table 10.
FEATS Scale (14) Perseveration
# Scale 14
D S M N
220 5 5 5 5
235 5 2 5 2
206 5 5 5 4
227 1 5 5 4
230 5 5 5 5
205 5 5 5 4
234 5 5 5 4
204 5 5 5 5
231 5 4.5 5 5
228 5 5 5 5
236 5 5 5 5
114 5 5 5 5
134 5 5 5 5
300 5 5 5 4
129 5 5 5 5
131 5 5 5 5
132 5 5 5 5
130 5 5 5 5
125 5 5 5 5
124 5 5 5 5
105 5 5 5 5
122 5 5 5 4
128 5 5 5 4
127 5 5 5 5
107 5 5 5 5
123 5 5 5 5
135 5 5 5 5
108 5 5 5 4
121 5 5 5 5
116 5 5 5 5
Rater Key:
D= Donna Betts S= Sheila Lorenzo M= Michelle Hamilton N= Nannie Mead

75
REFERENCES
Alley, T.R. (1988). Social and applied aspects of face perception: An introduction. In T.R.
Alley (Ed.), Social and applied aspects of perceiving faces (pp. 1-8). Hillsdale, NJ:
Lawrence Erlbaum.
Anschel, D.J., Dolce, S., Schwartzman, A., & Fisher, R. S. (2004). A blinded study of artwork
in a comprehensive epilepsy center population. Epilepsy & Behavior, 6, 196-202.
Betts, D.J. (2001, November). Projective drawing research: Assessing the abilities of children
and adolescents with multiple disabilities. Paper presented at the 32nd Annual AATA
conference, Albuquerque, NM.
Betts, D.J. (2003). Developing a projective drawing test: experiences with the
face stimulus assessment (FSA). Art Therapy: Journal of the American Art Therapy
Association, 20(2), 77-82.
Betts, D.J. (2005). A systematic analysis of art therapy assessment and rating
instrument literature. Unpublished doctoral dissertation, Florida State University.
Betts, D. J. (2006). Art Therapy Assessments and Rating Instruments: Do They Measure Up?
The Arts in Psychotherapy: An International Journal, 33(5), 371-472.
Brooke, S. L. (1996). A therapist’s guide to art therapy assessments: Tools of the trade.
Springfield, IL: Charles C. Thomas Publisher, LTD.
Bucciarelli, A. (2007). Normative study of the PPAT assessment on a sample of college students.
Unpublished master‟s thesis, Florida State University, Tallahassee.
Cohen, B. M. (Ed.). (1986/1994). The Diagnostic Drawing Series Rating Guide. Unpublished guidebook.
Cohen, B., Hammer, J., & Singer, S. (1988). The diagnostic drawing series: A systematic
approach to art therapy evaluation and research. The Arts in Psychotherapy, 15(1), 11-21.
76
Cohen B., Mills, A., & Kijak, K. (1994). An introduction to the diagnostic drawing series: A
standardized tool for diagnostic and clinical use. Art Therapy: Journal of the American
Art Therapy Association, 11(2), 105-110.
Cox, C. T. (Moderator), Agell, G., Cohen, B., & Gantt, L. (1999, November). Are you
assessing what I’m assessing? Let’s take a look! Round two. Panel presented at the
meeting of the American Art Therapy Association, Orlando, FL.
Ethnic group. (2008, July 5). In Wikipedia, The Free Encyclopedia. Retrieved 03:22, July 7,
2008, from http://en.wikipedia.org/w/index.php?title=Ethnic_group&oldid=223770441
Feder, B., & Feder, E. (1998). The art and science of evaluation in the arts therapies: How do
you know what’s working? Springfield, IL: Charles C. Thomas, Publisher LTD.
Fleiss' kappa. (2008, June 30). In Wikipedia, The Free Encyclopedia. Retrieved 02:47, July 16,
2008, from http://en.wikipedia.org/w/index.php?title=Fleiss%27_kappa
&oldid=222750142
Gantt, L. (1990). A validity study of the Formal Elements Art Therapy Scale (FEATS) for
diagnostic information in patients’ drawings. Unpublished doctoral dissertation,
University of Pittsburgh, Pittsburgh, PA.
Gantt, L., & Tabone, C. (1998). The formal elements art therapy scale: A rating manual.
MORGANTOWN, WV: GARGOYLE PRESS.
Gantt, L. (2004). The case for formal art therapy assessments. Art Therapy:
Journal of the American Art Therapy Association, 21(1), 18-29.
Hacking, S. (1999). The psychopathology of everyday art: A quantitative study.
Dissertation, University of Keele, Sheffield, UK. Published online at
http://www.musictherapyworld.de/modules/archive/stuff/papers/Hacking.pdf

77
Hadley, R. G., & Mitchell, L. K. (1995). Counseling research and program evaluation. Pacific
Grove, CA: Books/Cole Publishing.
Hays, R. E., & Lyons, S. J. (1981). The bridge drawing: A projective technique for
assessment in art therapy. Arts in Psychotherapy, 8(3-sup-4), 207-217.
Hrenko, K., & Willis, R. (1996). The Amusement Park Technique in the treatment of dually
diagnosed psychiatric inpatients. Art Therapy: Journal of the American Art Therapy
Association, 13(4), 261-264.
Inter-rater reliability. (2008, June 9). In Wikipedia, The Free Encyclopedia. Retrieved 03:28, July
7, 2008, from http://en.wikipedia.org/w/index.php?title=Inter-
rater_reliability&oldid=218235535
Kaiser, D. (1993). Attachment organization as manifested in a drawing task. Unpublished
master's thesis, Eastern Virginia Medical School, Norfolk, VA.
Kaplan, F. F. (2000). Art, science and art therapy: Repainting the picture. London &
Philadelphia: Jessica Kingsley Publishers.
Lande, R. G., & Howie, P. (1997). The art of crime. American Journal of Art Therapy, 36(1),
2-9.
Leavitt, C. G. (1988). A validity study of the diagnostic drawing series as used for
assessing depression in children and adolescents. Doctoral dissertation, School of
Professional Psychology, University of California, Los Angeles.
Machover, K. (1949). Personality projection in the drawing of the human figure. Springfield, IL:
Charles C. Thomas.
Manning, T. M. (1987). Aggression depicted in abused children's drawings. The Arts in
Psychotherapy, l4, l5-24.

78
Matteson, D. (2008). Rationale for Face Stimulus Assessment (FSA) and Face Stimulus
Assessment-Revised Norm (FSA-RN). Unpublished raw data.
McNiff, S. (1998). Art-based research. Philadelphia, PA: Jessica Kingsley.
Robb, M. (2001). Beyond the orphanages: Art therapy with Russian children. Art
Therapy: Journal of the American Art Therapy Association, 19(4), 146-150.
Rockwell, P. & Dunham M. (2006). The utility of the formal elements art therapy scale in
assessment for substance use disorder. Art Therapy: Journal of the American Art Therapy
Association, 23(3) pp. 104-111.
Silver, R. A. (1976). Using art to evaluate and develop cognitive skills. American Journal of Art
Therapy, 16, 11-19.
Stamatelos, T., & Mott, D. W. (1985). Creative potential among persons labeled
developmentally delayed. The Arts in Psychotherapy, 12, 101-113.
Stemler, Steve (2001). An overview of content analysis. Practical Assessment, Research &
Evaluation, 7(17). Retrieved July 15, 2008 from
http://PAREonline.net/getvn.asp?v=7&n=17
Swan-Foster, N., Foster, S., & Dorsey, A. (2003). The use of the human figure drawing with
pregnant women. Journal of Reproductive and Infant Psychology, 21(4), 293-307.
Ulman, E. (1965). A new use of art in psychiatric diagnosis. American Journal of Art
Therapy, 30(3), 78-88.
Wilson, K. P. (2004). Projective drawing: Alternative assessment of emotion in children who
stutter. Dissertation, Florida State University, Tallassee, FL. Published online at
http://www.dscholarship.lib.fsu.edu/undergrad/2

79
BIOGRAPHICAL SKETCH
Michelle Hamilton is a Masters of Science candidate at Avila University in the Counseling and
Art Therapy program. She currently works as an art therapist at a psychiatric hospital and as a
traveling art therapist with hospice clients. Upon graduation, Michelle hopes to continue her
education and continue conducting art therapy research.


















