Determining the Link between Structure, Process, and Outcome in Stroke Is It Realistic? What are the...
26
Determining the Link between Structure, Process, and Outcome in Stroke Is It Realistic? What are the Right Metrics? Eric D. Peterson, MD, MPH Eric D. Peterson, MD, MPH Professor of Medicine Professor of Medicine Vice Chair of Quality, Dept of Medicine Vice Chair of Quality, Dept of Medicine Director of CV Research Director of CV Research Duke Clinical Research Institute (DCRI) Duke Clinical Research Institute (DCRI) Author Disclosure: Research support from BMS-Sanofi, Merck, Eli Lilly, Ortho McNeil
-
Upload
barry-short -
Category
Documents
-
view
214 -
download
0
Transcript of Determining the Link between Structure, Process, and Outcome in Stroke Is It Realistic? What are the...

Determining the Link between Structure
Process and Outcome in Stroke
Is It Realistic What are the Right Metrics
Determining the Link between Structure
Process and Outcome in Stroke
Is It Realistic What are the Right Metrics
Eric D Peterson MD MPHEric D Peterson MD MPHProfessor of MedicineProfessor of Medicine
Vice Chair of Quality Dept of MedicineVice Chair of Quality Dept of MedicineDirector of CV ResearchDirector of CV Research
Duke Clinical Research Institute (DCRI)Duke Clinical Research Institute (DCRI)
Eric D Peterson MD MPHEric D Peterson MD MPHProfessor of MedicineProfessor of Medicine
Vice Chair of Quality Dept of MedicineVice Chair of Quality Dept of MedicineDirector of CV ResearchDirector of CV Research
Duke Clinical Research Institute (DCRI)Duke Clinical Research Institute (DCRI)
Author Disclosure Research support from
BMS-Sanofi Merck Eli Lilly Ortho McNeil
Author Disclosure Research support from
BMS-Sanofi Merck Eli Lilly Ortho McNeil
What is QualityWhat is Quality
ldquoDegree to which health care services increase the likelihood of desired health outcomes and are consistent with current professional knowledgerdquo
Are we doing the right things
Are our patients better off for it
ldquoDegree to which health care services increase the likelihood of desired health outcomes and are consistent with current professional knowledgerdquo
Are we doing the right things
Are our patients better off for it
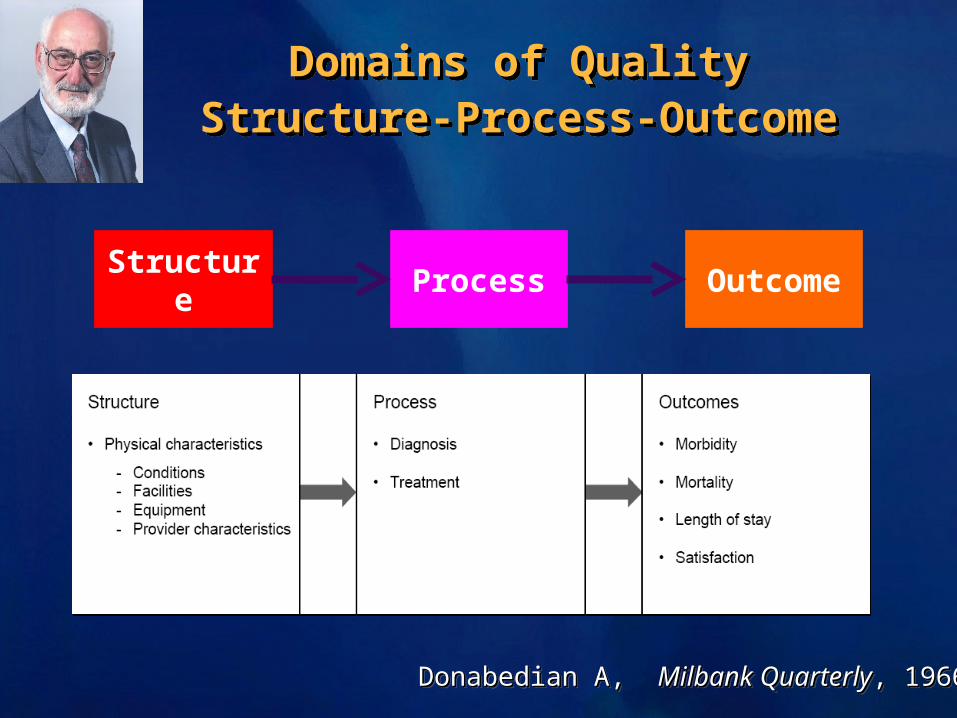
Domains of QualityStructure-Process-Outcome
Domains of QualityStructure-Process-Outcome
Structure Process Outcome
Each of the components in the model has a direct influence on the next component in the model
Donabedian A Donabedian A Milbank QuarterlyMilbank Quarterly 1966 1966Donabedian A Donabedian A Milbank QuarterlyMilbank Quarterly 1966 1966
StructureRole of Specialty Stroke Care
StructureRole of Specialty Stroke Care
Caplan (2003) ndash Stroke care should be managed by neurologist
Lee (2003) ndash Stroke patients should be cared for by stroke subspeciality
Kazmierski et al (2004) ndash Stroke care should be holistic and include (Neurologist)
Caplan (2003) ndash Stroke care should be managed by neurologist
Lee (2003) ndash Stroke patients should be cared for by stroke subspeciality
Kazmierski et al (2004) ndash Stroke care should be holistic and include (Neurologist)
Caplan L Stroke is best managed by neurologists Stroke 2003342763Lee KR Stroke is best managed by neurologists Battle of the titans Stroke 2003342764-2765Kazmierski R Pawlak MA Kozubski W Who should care for stroke patients Stroke 200435e85-e86
Its not Individuals but Teams that Matter
Role for Team-based Stroke CareRole for Team-based Stroke Care
There is evidence that specialized stroke teams improve outcomes
Bershad EM Feen ES Hernandez OH Suri MF Suarez JI Impact of a specialized neurointensive care team on outcomes of critically ill acute ischemic stroke patients Neurocrit Care 20089(3)287-292
Adams H Adams R Del Zoppo G Goldstein LB Guidelines for the early management of patients with ischemic stroke 2005 guidelines update a scientific statement from the Stroke Council of the American Heart AssociationAmerican Stroke Association Stroke Apr 200536(4)916-923
Deborah J Webb DJ Fayad PF Wilbur C Thomas A Brass LM Effects of a Specialized Team on Stroke Care The First Two Years of the Yale Stroke Program Stroke 1995261353-1357
Need for Systems of Care for AllNeed for Systems of Care for AllNot everyone has the luxury of a nearby primary stroke center
HubHub
Neurologist
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
Stroke Systems of Care Regionalization
Stroke Systems of Care Regionalization
Telestroke Bringing the Specialist to the Patient
Telestroke Bringing the Specialist to the Patient
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Vaishnav Expert Rev Neurother 20077913-914 Shafqat Stroke 1999302141-2145
Video may and improves upon consultation by allowinghellip
bull 10 community hospitals in Bavaria ndash 5 intervention 5 controlndash Matched in size infrastructure
bull Interventionndash Stroke wards and medical staff trainingndash 247 telemedicine consultation from academic
centers (both ED and inpatient)bull July 2003 ndash March 2005 3122 ischemic and
hemorrhagic stroke patientsbull Patients dead or disabled 3 months after stroke
436 vs 540 plt0001OR for poor outcome 061 95 CI 51-73
Stroke Systems Controlled TrialTEMPIS Study ndash Lancet Neurology 2006
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

What is QualityWhat is Quality
ldquoDegree to which health care services increase the likelihood of desired health outcomes and are consistent with current professional knowledgerdquo
Are we doing the right things
Are our patients better off for it
ldquoDegree to which health care services increase the likelihood of desired health outcomes and are consistent with current professional knowledgerdquo
Are we doing the right things
Are our patients better off for it
Domains of QualityStructure-Process-Outcome
Domains of QualityStructure-Process-Outcome
Structure Process Outcome
Each of the components in the model has a direct influence on the next component in the model
Donabedian A Donabedian A Milbank QuarterlyMilbank Quarterly 1966 1966Donabedian A Donabedian A Milbank QuarterlyMilbank Quarterly 1966 1966
StructureRole of Specialty Stroke Care
StructureRole of Specialty Stroke Care
Caplan (2003) ndash Stroke care should be managed by neurologist
Lee (2003) ndash Stroke patients should be cared for by stroke subspeciality
Kazmierski et al (2004) ndash Stroke care should be holistic and include (Neurologist)
Caplan (2003) ndash Stroke care should be managed by neurologist
Lee (2003) ndash Stroke patients should be cared for by stroke subspeciality
Kazmierski et al (2004) ndash Stroke care should be holistic and include (Neurologist)
Caplan L Stroke is best managed by neurologists Stroke 2003342763Lee KR Stroke is best managed by neurologists Battle of the titans Stroke 2003342764-2765Kazmierski R Pawlak MA Kozubski W Who should care for stroke patients Stroke 200435e85-e86
Its not Individuals but Teams that Matter
Role for Team-based Stroke CareRole for Team-based Stroke Care
There is evidence that specialized stroke teams improve outcomes
Bershad EM Feen ES Hernandez OH Suri MF Suarez JI Impact of a specialized neurointensive care team on outcomes of critically ill acute ischemic stroke patients Neurocrit Care 20089(3)287-292
Adams H Adams R Del Zoppo G Goldstein LB Guidelines for the early management of patients with ischemic stroke 2005 guidelines update a scientific statement from the Stroke Council of the American Heart AssociationAmerican Stroke Association Stroke Apr 200536(4)916-923
Deborah J Webb DJ Fayad PF Wilbur C Thomas A Brass LM Effects of a Specialized Team on Stroke Care The First Two Years of the Yale Stroke Program Stroke 1995261353-1357
Need for Systems of Care for AllNeed for Systems of Care for AllNot everyone has the luxury of a nearby primary stroke center
HubHub
Neurologist
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
Stroke Systems of Care Regionalization
Stroke Systems of Care Regionalization
Telestroke Bringing the Specialist to the Patient
Telestroke Bringing the Specialist to the Patient
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Vaishnav Expert Rev Neurother 20077913-914 Shafqat Stroke 1999302141-2145
Video may and improves upon consultation by allowinghellip
bull 10 community hospitals in Bavaria ndash 5 intervention 5 controlndash Matched in size infrastructure
bull Interventionndash Stroke wards and medical staff trainingndash 247 telemedicine consultation from academic
centers (both ED and inpatient)bull July 2003 ndash March 2005 3122 ischemic and
hemorrhagic stroke patientsbull Patients dead or disabled 3 months after stroke
436 vs 540 plt0001OR for poor outcome 061 95 CI 51-73
Stroke Systems Controlled TrialTEMPIS Study ndash Lancet Neurology 2006
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-
Domains of QualityStructure-Process-Outcome
Domains of QualityStructure-Process-Outcome
Structure Process Outcome
Each of the components in the model has a direct influence on the next component in the model
Donabedian A Donabedian A Milbank QuarterlyMilbank Quarterly 1966 1966Donabedian A Donabedian A Milbank QuarterlyMilbank Quarterly 1966 1966
StructureRole of Specialty Stroke Care
StructureRole of Specialty Stroke Care
Caplan (2003) ndash Stroke care should be managed by neurologist
Lee (2003) ndash Stroke patients should be cared for by stroke subspeciality
Kazmierski et al (2004) ndash Stroke care should be holistic and include (Neurologist)
Caplan (2003) ndash Stroke care should be managed by neurologist
Lee (2003) ndash Stroke patients should be cared for by stroke subspeciality
Kazmierski et al (2004) ndash Stroke care should be holistic and include (Neurologist)
Caplan L Stroke is best managed by neurologists Stroke 2003342763Lee KR Stroke is best managed by neurologists Battle of the titans Stroke 2003342764-2765Kazmierski R Pawlak MA Kozubski W Who should care for stroke patients Stroke 200435e85-e86
Its not Individuals but Teams that Matter
Role for Team-based Stroke CareRole for Team-based Stroke Care
There is evidence that specialized stroke teams improve outcomes
Bershad EM Feen ES Hernandez OH Suri MF Suarez JI Impact of a specialized neurointensive care team on outcomes of critically ill acute ischemic stroke patients Neurocrit Care 20089(3)287-292
Adams H Adams R Del Zoppo G Goldstein LB Guidelines for the early management of patients with ischemic stroke 2005 guidelines update a scientific statement from the Stroke Council of the American Heart AssociationAmerican Stroke Association Stroke Apr 200536(4)916-923
Deborah J Webb DJ Fayad PF Wilbur C Thomas A Brass LM Effects of a Specialized Team on Stroke Care The First Two Years of the Yale Stroke Program Stroke 1995261353-1357
Need for Systems of Care for AllNeed for Systems of Care for AllNot everyone has the luxury of a nearby primary stroke center
HubHub
Neurologist
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
Stroke Systems of Care Regionalization
Stroke Systems of Care Regionalization
Telestroke Bringing the Specialist to the Patient
Telestroke Bringing the Specialist to the Patient
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Vaishnav Expert Rev Neurother 20077913-914 Shafqat Stroke 1999302141-2145
Video may and improves upon consultation by allowinghellip
bull 10 community hospitals in Bavaria ndash 5 intervention 5 controlndash Matched in size infrastructure
bull Interventionndash Stroke wards and medical staff trainingndash 247 telemedicine consultation from academic
centers (both ED and inpatient)bull July 2003 ndash March 2005 3122 ischemic and
hemorrhagic stroke patientsbull Patients dead or disabled 3 months after stroke
436 vs 540 plt0001OR for poor outcome 061 95 CI 51-73
Stroke Systems Controlled TrialTEMPIS Study ndash Lancet Neurology 2006
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

StructureRole of Specialty Stroke Care
StructureRole of Specialty Stroke Care
Caplan (2003) ndash Stroke care should be managed by neurologist
Lee (2003) ndash Stroke patients should be cared for by stroke subspeciality
Kazmierski et al (2004) ndash Stroke care should be holistic and include (Neurologist)
Caplan (2003) ndash Stroke care should be managed by neurologist
Lee (2003) ndash Stroke patients should be cared for by stroke subspeciality
Kazmierski et al (2004) ndash Stroke care should be holistic and include (Neurologist)
Caplan L Stroke is best managed by neurologists Stroke 2003342763Lee KR Stroke is best managed by neurologists Battle of the titans Stroke 2003342764-2765Kazmierski R Pawlak MA Kozubski W Who should care for stroke patients Stroke 200435e85-e86
Its not Individuals but Teams that Matter
Role for Team-based Stroke CareRole for Team-based Stroke Care
There is evidence that specialized stroke teams improve outcomes
Bershad EM Feen ES Hernandez OH Suri MF Suarez JI Impact of a specialized neurointensive care team on outcomes of critically ill acute ischemic stroke patients Neurocrit Care 20089(3)287-292
Adams H Adams R Del Zoppo G Goldstein LB Guidelines for the early management of patients with ischemic stroke 2005 guidelines update a scientific statement from the Stroke Council of the American Heart AssociationAmerican Stroke Association Stroke Apr 200536(4)916-923
Deborah J Webb DJ Fayad PF Wilbur C Thomas A Brass LM Effects of a Specialized Team on Stroke Care The First Two Years of the Yale Stroke Program Stroke 1995261353-1357
Need for Systems of Care for AllNeed for Systems of Care for AllNot everyone has the luxury of a nearby primary stroke center
HubHub
Neurologist
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
Stroke Systems of Care Regionalization
Stroke Systems of Care Regionalization
Telestroke Bringing the Specialist to the Patient
Telestroke Bringing the Specialist to the Patient
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Vaishnav Expert Rev Neurother 20077913-914 Shafqat Stroke 1999302141-2145
Video may and improves upon consultation by allowinghellip
bull 10 community hospitals in Bavaria ndash 5 intervention 5 controlndash Matched in size infrastructure
bull Interventionndash Stroke wards and medical staff trainingndash 247 telemedicine consultation from academic
centers (both ED and inpatient)bull July 2003 ndash March 2005 3122 ischemic and
hemorrhagic stroke patientsbull Patients dead or disabled 3 months after stroke
436 vs 540 plt0001OR for poor outcome 061 95 CI 51-73
Stroke Systems Controlled TrialTEMPIS Study ndash Lancet Neurology 2006
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Its not Individuals but Teams that Matter
Role for Team-based Stroke CareRole for Team-based Stroke Care
There is evidence that specialized stroke teams improve outcomes
Bershad EM Feen ES Hernandez OH Suri MF Suarez JI Impact of a specialized neurointensive care team on outcomes of critically ill acute ischemic stroke patients Neurocrit Care 20089(3)287-292
Adams H Adams R Del Zoppo G Goldstein LB Guidelines for the early management of patients with ischemic stroke 2005 guidelines update a scientific statement from the Stroke Council of the American Heart AssociationAmerican Stroke Association Stroke Apr 200536(4)916-923
Deborah J Webb DJ Fayad PF Wilbur C Thomas A Brass LM Effects of a Specialized Team on Stroke Care The First Two Years of the Yale Stroke Program Stroke 1995261353-1357
Need for Systems of Care for AllNeed for Systems of Care for AllNot everyone has the luxury of a nearby primary stroke center
HubHub
Neurologist
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
Stroke Systems of Care Regionalization
Stroke Systems of Care Regionalization
Telestroke Bringing the Specialist to the Patient
Telestroke Bringing the Specialist to the Patient
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Vaishnav Expert Rev Neurother 20077913-914 Shafqat Stroke 1999302141-2145
Video may and improves upon consultation by allowinghellip
bull 10 community hospitals in Bavaria ndash 5 intervention 5 controlndash Matched in size infrastructure
bull Interventionndash Stroke wards and medical staff trainingndash 247 telemedicine consultation from academic
centers (both ED and inpatient)bull July 2003 ndash March 2005 3122 ischemic and
hemorrhagic stroke patientsbull Patients dead or disabled 3 months after stroke
436 vs 540 plt0001OR for poor outcome 061 95 CI 51-73
Stroke Systems Controlled TrialTEMPIS Study ndash Lancet Neurology 2006
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Role for Team-based Stroke CareRole for Team-based Stroke Care
There is evidence that specialized stroke teams improve outcomes
Bershad EM Feen ES Hernandez OH Suri MF Suarez JI Impact of a specialized neurointensive care team on outcomes of critically ill acute ischemic stroke patients Neurocrit Care 20089(3)287-292
Adams H Adams R Del Zoppo G Goldstein LB Guidelines for the early management of patients with ischemic stroke 2005 guidelines update a scientific statement from the Stroke Council of the American Heart AssociationAmerican Stroke Association Stroke Apr 200536(4)916-923
Deborah J Webb DJ Fayad PF Wilbur C Thomas A Brass LM Effects of a Specialized Team on Stroke Care The First Two Years of the Yale Stroke Program Stroke 1995261353-1357
Need for Systems of Care for AllNeed for Systems of Care for AllNot everyone has the luxury of a nearby primary stroke center
HubHub
Neurologist
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
Stroke Systems of Care Regionalization
Stroke Systems of Care Regionalization
Telestroke Bringing the Specialist to the Patient
Telestroke Bringing the Specialist to the Patient
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Vaishnav Expert Rev Neurother 20077913-914 Shafqat Stroke 1999302141-2145
Video may and improves upon consultation by allowinghellip
bull 10 community hospitals in Bavaria ndash 5 intervention 5 controlndash Matched in size infrastructure
bull Interventionndash Stroke wards and medical staff trainingndash 247 telemedicine consultation from academic
centers (both ED and inpatient)bull July 2003 ndash March 2005 3122 ischemic and
hemorrhagic stroke patientsbull Patients dead or disabled 3 months after stroke
436 vs 540 plt0001OR for poor outcome 061 95 CI 51-73
Stroke Systems Controlled TrialTEMPIS Study ndash Lancet Neurology 2006
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Need for Systems of Care for AllNeed for Systems of Care for AllNot everyone has the luxury of a nearby primary stroke center
HubHub
Neurologist
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
SpokeSpoke
Stroke Systems of Care Regionalization
Stroke Systems of Care Regionalization
Telestroke Bringing the Specialist to the Patient
Telestroke Bringing the Specialist to the Patient
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Vaishnav Expert Rev Neurother 20077913-914 Shafqat Stroke 1999302141-2145
Video may and improves upon consultation by allowinghellip
bull 10 community hospitals in Bavaria ndash 5 intervention 5 controlndash Matched in size infrastructure
bull Interventionndash Stroke wards and medical staff trainingndash 247 telemedicine consultation from academic
centers (both ED and inpatient)bull July 2003 ndash March 2005 3122 ischemic and
hemorrhagic stroke patientsbull Patients dead or disabled 3 months after stroke
436 vs 540 plt0001OR for poor outcome 061 95 CI 51-73
Stroke Systems Controlled TrialTEMPIS Study ndash Lancet Neurology 2006
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Stroke Systems of Care Regionalization
Stroke Systems of Care Regionalization
Telestroke Bringing the Specialist to the Patient
Telestroke Bringing the Specialist to the Patient
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Vaishnav Expert Rev Neurother 20077913-914 Shafqat Stroke 1999302141-2145
Video may and improves upon consultation by allowinghellip
bull 10 community hospitals in Bavaria ndash 5 intervention 5 controlndash Matched in size infrastructure
bull Interventionndash Stroke wards and medical staff trainingndash 247 telemedicine consultation from academic
centers (both ED and inpatient)bull July 2003 ndash March 2005 3122 ischemic and
hemorrhagic stroke patientsbull Patients dead or disabled 3 months after stroke
436 vs 540 plt0001OR for poor outcome 061 95 CI 51-73
Stroke Systems Controlled TrialTEMPIS Study ndash Lancet Neurology 2006
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Telestroke Bringing the Specialist to the Patient
Telestroke Bringing the Specialist to the Patient
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Visualization and interaction with patient for more accurate assessment
Ability to obtain a valid NIHSS score
Ability to view a CT scan in real time for reliable diagnosis
Sharing patient records with remote physician
Vaishnav Expert Rev Neurother 20077913-914 Shafqat Stroke 1999302141-2145
Video may and improves upon consultation by allowinghellip
bull 10 community hospitals in Bavaria ndash 5 intervention 5 controlndash Matched in size infrastructure
bull Interventionndash Stroke wards and medical staff trainingndash 247 telemedicine consultation from academic
centers (both ED and inpatient)bull July 2003 ndash March 2005 3122 ischemic and
hemorrhagic stroke patientsbull Patients dead or disabled 3 months after stroke
436 vs 540 plt0001OR for poor outcome 061 95 CI 51-73
Stroke Systems Controlled TrialTEMPIS Study ndash Lancet Neurology 2006
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

bull 10 community hospitals in Bavaria ndash 5 intervention 5 controlndash Matched in size infrastructure
bull Interventionndash Stroke wards and medical staff trainingndash 247 telemedicine consultation from academic
centers (both ED and inpatient)bull July 2003 ndash March 2005 3122 ischemic and
hemorrhagic stroke patientsbull Patients dead or disabled 3 months after stroke
436 vs 540 plt0001OR for poor outcome 061 95 CI 51-73
Stroke Systems Controlled TrialTEMPIS Study ndash Lancet Neurology 2006
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke
An Instrumental Variable Analysis
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Ying Xian et al AHA QCOR YI competition 2010
Studied 32783 NYS stroke patients 50 treated at primary stroke centers Used distance to stroke center as IV
Results Adjusted mortality lower at primary stroke centers
Xian Y et al Abstract at AHA QCOR 2010
Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Why Structural Measures are ImperfectAssociations are just thathellip
Why Structural Measures are ImperfectAssociations are just thathellip
Ross et al New Engl J Med 2010
Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Stroke Process of CarePerformance Measures
Stroke Process of CarePerformance Measures
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
bull of acute ischemic stroke (IS) pts who arrive at ED within (2 hrs) of onset of symptoms who receive IV t-PA within 3 hrs
bull IS or TIA pts who receive antithrombotic medication within 48 hours of hospitalization
bull of IS or TIA pts discharged on antithrombotics
bull of IS or TIA patients with atrial fibrillation who are discharged on anticoagulation therapy unless a contraindication
bull of pts at risk for DVT who received DVT prophylaxis by Day 2
bull of IS or TIA patients with LDLgt100 mgdL or on cholesterol reducer prior to admission who are discharged on cholesterol-reducing drugs
bull of smokers who receive smoking cessation advice or meds at discharge
GWTG- Fact Sheet (2006)
How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

How are We Doing on Process1000000 Patients Strong
Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Improving Care Process In GWTG-StrokeImproving Care Process In GWTG-Stroke
2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

2410 2230 2470 2580 2740
0
20
40
60
80
100
DTN within 60 min
2005 2006 2007 2008 2009
Door-to-IV rt-PA within 60 minutes
GWTG-Stroke Database data on file DCRI
Opportunity to Improve Timeliness of IV rt-PA
Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Unequal Access to Evidence-based Stroke Practices
Unequal Access to Evidence-based Stroke Practices
Gender Race Ethnicity
Schwamm L et al Circulation 20101211492-1501)
Reeves M et al Stroke 2009401127-1133
Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Performance Measurement Its Not as Easy as You Think
Performance Measurement Its Not as Easy as You Think
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Do we have right metrics Measuring ldquowhatrsquos easyrdquo vs ldquowhatrsquos importantrdquo
What is precision of our performance tools Sample size issues Need to risk adjust performance metrics Composite measure complexity
Can we change it P4P vs provider led efforts Where do we go from here
Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Evolving View of Quality Care Importance of Longitudinal Measures
Evolving View of Quality Care Importance of Longitudinal Measures
Getting BetterLiving w IllnessDisability (T1)
Coping w End of Life (T2)Staying Healthy
Post AcuteRehabilitation Phase
20 Prevention
Episode begins ndash onset of symptoms
Post AMI Trajectory 2 (T2)Adult with multiple co-morbidities
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Advanced Care Planningbull Advanced Directivesbull Palliative CareSymptom Control
Assessment ofPreferences
AcutePhase
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Episode ends ndash 1 year post AMI
20 Prevention(CAD with prior AMI)Advanced Care Planning
Population at Risk
10 Prevention (no known CAD)
20 Prevention (CAD no prior AMI)
Post AMI Trajectory 1 (T1)Relatively healthy adult
Focus onbull Quality of Lifebull Functional Statusbull 20 Prevention Strategiesbull Rehabilitationbull Advanced care planning
Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Stroke Outcomes Mortality
Stroke Outcomes Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Potential to ImproveVariation in Hospital Stroke Mortality
Potential to ImproveVariation in Hospital Stroke Mortality
Outcomes Adjusted Event Rates Distribution of Hospital Event Rates
Mean plusmn STD 10th 25th Median 75th 90th
In-Hospital 57 plusmn 22 28 46 60 69 82
30-Day 139 plusmn 35 98 121 142 156 178
90-Day 201 plusmn 42 153 182 202 222 251
1-Year 309 plusmn 46 252 286 310 330 363
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-
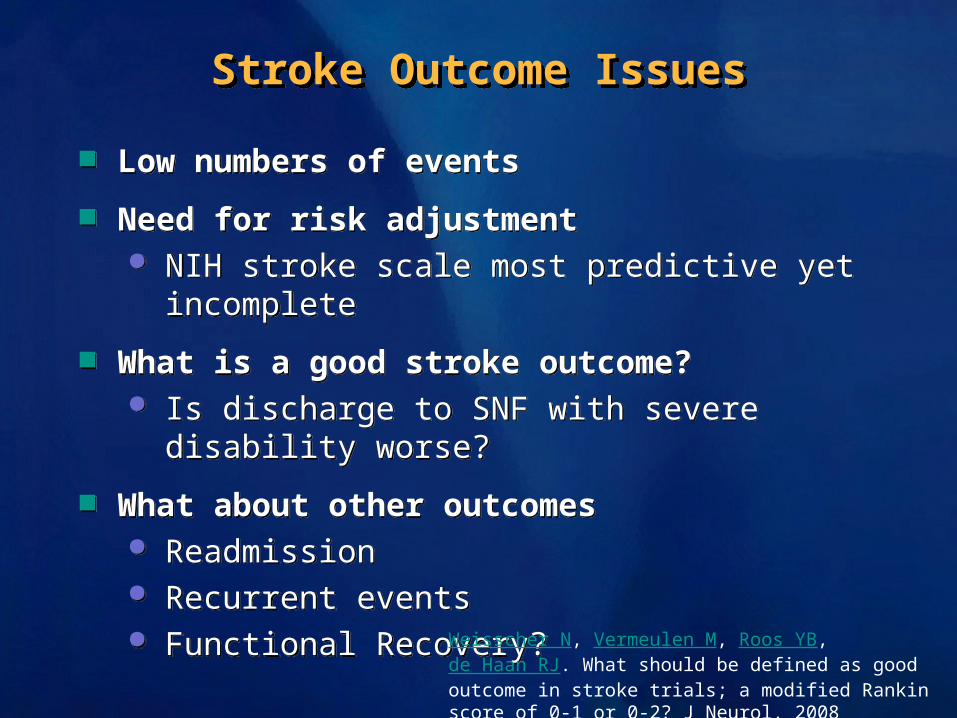
Stroke Outcome IssuesStroke Outcome Issues
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Low numbers of events
Need for risk adjustment NIH stroke scale most predictive yet incomplete
What is a good stroke outcome Is discharge to SNF with severe disability worse
What about other outcomes Readmission Recurrent events Functional Recovery
Weisscher N Vermeulen M Roos YB de Haan RJ What should be defined as good outcome in stroke trials a modified Rankin score of 0-1 or 0-2 J Neurol 2008 Jun255(6)867-74
The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

The Stroke Quality AgendahellipThe Stroke Quality AgendahellipWhere Do We Go From HerehellipWhere Do We Go From Herehellip
Structure
Process
Implementation
Outcomes
New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

New Science New TherapeuticsNew Science New Therapeutics
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
High Throughput Screening (HTS) allows rapid screening of a high rsquos of
chemicals to find an active compound The starting points for understanding the role of a particular biochemical process
Genome-wide Association (GWAS)Genome-wide Association (GWAS)In-depth characterization of patients genes to identify those factors that are different in those with trait of interest
Study Perturbation of Biological Study Perturbation of Biological SystemsSystems
Causing an experiments disruption of a system to better understand its properties
New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

New SciencehellipImplementation ScienceNew SciencehellipImplementation Science
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
High Throughput Screening (HTS)(AKA National Clinical Registries) allows rapid screening of hundreds of
centers to find those with outstanding ldquoPositive or Negative Deviancerdquo
GWAS (AKA QualQuant Research)GWAS (AKA QualQuant Research) In-depth characterization of hospital structure and process to identify those factors associated with better outcomes
Controlled PerturbationNatural ExperimentsCluster randomization
Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-

Conclusions Conclusions
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
Structure Current Specialty MD team hospital system Future Understand HOW
Process Current established stroke performance metrics Future study closely the link to outcomes
Need broader metrics
Outcomes Current In-patient mortality Future Patient centric longitudinal measures
- Determining the Link between Structure Process and Outcome in Stroke Is It Realistic What are the Right Metrics
- What is Quality
- Domains of Quality Structure-Process-Outcome
- Structure Role of Specialty Stroke Care
- Slide 5
- Role for Team-based Stroke Care
- Need for Systems of Care for All
- Stroke Systems of Care Regionalization
- Telestroke Bringing the Specialist to the Patient
- Slide 10
- Do Stroke Centers Reduce Mortality for Patients with Acute Ischemic Stroke An Instrumental Variable Analysis
- Why Structural Measures are Imperfect Associations are just thathellip
- Stroke Process of Care Performance Measures
- Slide 14
- Improving Care Process In GWTG-Stroke
- Slide 16
- Unequal Access to Evidence-based Stroke Practices
- Performance Measurement Its Not as Easy as You Think
- Evolving View of Quality Care Importance of Longitudinal Measures
- Stroke Outcomes Mortality
- Potential to Improve Variation in Hospital Stroke Mortality
- Stroke Outcome Issues
- The Stroke Quality Agendahellip Where Do We Go From Herehellip
- New Science New Therapeutics
- New SciencehellipImplementation Science
- Conclusions
-