Detection of FUS–ERG chimeric transcript in two cases of acute myeloid leukemia with...
8
Detection of FUSeERG chimeric transcript in two cases of acute myeloid leukemia with t(16;21)(p11.2;q22) with unusual characteristics Juwon Kim a , Tae Sung Park b , Jaewoo Song a , Lee Kyung-A a , Duk Jin Hong a , Yoo Hong Min c , June-Won Cheong c , Jong Rak Choi a, * a Department of Laboratory Medicine, Yonsei University College of Medicine, 250 Seongsanno, Seodaemun-gu, Seoul 120-752, Korea b Department of Laboratory Medicine, Kyung Hee University School of Medicine, 1 Hoegi-dong, Dongdaemun-gu, Seoul 130-702, Korea c Department of Internal Medicine, Yonsei University College of Medicine, 250 Seongsanno, Seodaemun-gu, Seoul 120-752, Korea Received 10 June 2009; accepted 14 June 2009 Abstract Reciprocal t(16;21)(p11;q22) is a rare chromosomal abnormality in acute myeloid leukemia (AML). The chimeric transcript FUSeERG formed by this translocation which causes the replacement of RNA-binding domain of FUS (alias TLS ) with the DNA-binding domain of ERG, and this event is thought to be responsible for leukemogenesis. Here we report two cases of AML with t(16;21)(p11.2;q22) showing unusual characteristics, and address the clinical, hematological, and molec- ular aspects of leukemia with t(16;21), along with a review of the literature. Ó 2009 Elsevier Inc. All rights reserved. 1. Introduction Chromosomal translocations are important events in the pathogenesis of hematological malignancies. The reciprocal translocation t(16;21)(p11.2;q22) is a nonrandom chromo- somal abnormality first reported by Mecucci et al. [1] in acute myeloid leukemia (AML). It was also demonstrated in blast crisis of chronic myeloid leukemia [2], myelodysplastic syndrome evolved to AML [3], and acute lymphoblastic leukemia [4]. Cases of AML harboring t(16;21)(p11.2;q22) fall into all types under the FrencheAmericaneBritish (FAB) classification [5e9] except M3. The morphologic characteristics of cases with t(16;21) are increased number of abnormal eosinophils, blasts with monocytoid features, and hemophagocytosis [2,10]. The ETS-related gene ERG was found to be rearranged in AML with t(16;21), and the chimeric products were formed by fusion of ERG and an unknown partner gene on chromo- some 16 with the break occurring in the first intron upstream of the ETS domain of ERG [11]. Later, the unknown partner gene on chromosome 16 was found to be FUS (alias TLS ). In a subset of Ewing sarcoma, ERG is fused with EWS [12], which shows high homology with FUS, rearranged in the t(12;16)(q13;q11) translocation first described in myxoid lip- osarcomas [13]. The chimeric transcript FUSeERG formed by this translocation causes the replacement of RNA-binding domain of FUS with the DNA-binding domain of ERG [14,15]. This fusion gene is thought to be responsible for leukemogenesis of AML harboring t(16;21). Jumping translocations are chromosomal rearrangements involving one donor chromosome and several recipient chro- mosomes [16,17]. Jumping translocation was first found in PradereWilli syndrome as a constitutional chromosomal abnormality [18]. Although very rare, jumping translocation has been documented in various types of hematological disease, including lymphoma, multiple myeloma, AML, and acute lymphoblastic leukemia [19e22]. Most of these translocations showed preferential involvement of 1q as a donor and occurred as a secondary change [16]. Because it appears at the later stage as the disease progresses, jumping translocation is known to be associated with poor prognosis, possibly through changes of gene expression [16,23]. Here we present two cases of AML with t(16;21) (p11.2;q22) showing unusual characteristics and address the clinical, hematological, and molecular aspects of leukemia with t(16;21), along with a review of the literature. 2. Case history 2.1. Patient 1 In February 2008, a 36-year-old Korean man presented with fever, headache, and night sweating. The peripheral blood count showed a hemoglobin level of 14.7 g/dL, and * Corresponding author. Tel.: þ82-2-2228-2445; fax: þ82-2-313- 0956. E-mail address: [email protected] (J.R. Choi). 0165-4608/09/$ e see front matter Ó 2009 Elsevier Inc. All rights reserved. doi:10.1016/j.cancergencyto.2009.06.010 Cancer Genetics and Cytogenetics 194 (2009) 111e118
Transcript of Detection of FUS–ERG chimeric transcript in two cases of acute myeloid leukemia with...

Cancer Genetics and Cytogenetics 194 (2009) 111e118
Detection of FUSeERG chimeric transcript in two cases of acute myeloidleukemia with t(16;21)(p11.2;q22) with unusual characteristics
Juwon Kima, Tae Sung Parkb, Jaewoo Songa, Lee Kyung-Aa, Duk Jin Honga, Yoo Hong Minc,June-Won Cheongc, Jong Rak Choia,*
aDepartment of Laboratory Medicine, Yonsei University College of Medicine, 250 Seongsanno, Seodaemun-gu, Seoul 120-752, KoreabDepartment of Laboratory Medicine, Kyung Hee University School of Medicine, 1 Hoegi-dong, Dongdaemun-gu, Seoul 130-702, Korea
cDepartment of Internal Medicine, Yonsei University College of Medicine, 250 Seongsanno, Seodaemun-gu, Seoul 120-752, Korea
Received 10 June 2009; accepted 14 June 2009
Abstract Reciprocal t(16;21)(p11;q22) is a rare chromoso
* Corresponding
0956.
E-mail address: c
0165-4608/09/$ e see
doi:10.1016/j.cancerg
mal abnormality in acute myeloid leukemia (AML).The chimeric transcript FUSeERG formed by this translocation which causes the replacement ofRNA-binding domain of FUS (alias TLS ) with the DNA-binding domain of ERG, and this eventis thought to be responsible for leukemogenesis. Here we report two cases of AML witht(16;21)(p11.2;q22) showing unusual characteristics, and address the clinical, hematological, and molec-ular aspects of leukemia with t(16;21), along with a review of the literature. � 2009 Elsevier Inc.All rights reserved.
1. Introduction
Chromosomal translocations are important events in thepathogenesis of hematological malignancies. The reciprocaltranslocation t(16;21)(p11.2;q22) is a nonrandom chromo-somal abnormality first reported by Mecucci et al. [1] in acutemyeloid leukemia (AML). It was also demonstrated in blastcrisis of chronic myeloid leukemia [2], myelodysplasticsyndrome evolved to AML [3], and acute lymphoblasticleukemia [4]. Cases of AML harboring t(16;21)(p11.2;q22)fall into all types under the FrencheAmericaneBritish(FAB) classification [5e9] except M3. The morphologiccharacteristics of cases with t(16;21) are increased numberof abnormal eosinophils, blasts with monocytoid features,and hemophagocytosis [2,10].
The ETS-related gene ERG was found to be rearranged inAML with t(16;21), and the chimeric products were formedby fusion of ERG and an unknown partner gene on chromo-some 16 with the break occurring in the first intron upstreamof the ETS domain of ERG [11]. Later, the unknown partnergene on chromosome 16 was found to be FUS (alias TLS ).In a subset of Ewing sarcoma, ERG is fused with EWS [12],which shows high homology with FUS, rearranged in thet(12;16)(q13;q11) translocation first described in myxoid lip-osarcomas [13]. The chimeric transcript FUSeERG formed
author. Tel.: þ82-2-2228-2445; fax: þ82-2-313-
[email protected] (J.R. Choi).
front matter � 2009 Elsevier Inc. All rights reserved.
encyto.2009.06.010
by this translocation causes the replacement of RNA-bindingdomain of FUS with the DNA-binding domain of ERG[14,15]. This fusion gene is thought to be responsible forleukemogenesis of AML harboring t(16;21).
Jumping translocations are chromosomal rearrangementsinvolving one donor chromosome and several recipient chro-mosomes [16,17]. Jumping translocation was first found inPradereWilli syndrome as a constitutional chromosomalabnormality [18]. Although very rare, jumping translocationhas been documented in various types of hematologicaldisease, including lymphoma, multiple myeloma, AML,and acute lymphoblastic leukemia [19e22]. Most of thesetranslocations showed preferential involvement of 1q asa donor and occurred as a secondary change [16]. Becauseit appears at the later stage as the disease progresses, jumpingtranslocation is known to be associated with poor prognosis,possibly through changes of gene expression [16,23].
Here we present two cases of AML with t(16;21)(p11.2;q22) showing unusual characteristics and address theclinical, hematological, and molecular aspects of leukemiawith t(16;21), along with a review of the literature.
2. Case history
2.1. Patient 1
In February 2008, a 36-year-old Korean man presentedwith fever, headache, and night sweating. The peripheralblood count showed a hemoglobin level of 14.7 g/dL, and

Fig. 1. Morphology of leukemic cells at diagnosis. Blasts observed in
bone marrow aspirate of (A) patient 1 and (B) patient 2. Blasts exhibited
s large amount of cytoplasm filled with fine granules and vacuoles, and
convoluted or lobulated nuclei showing monocytic features. Auer rods or
bodies are frequently observed. Wright-Giemsa staining. Original magnifi-
cation: �1,000.
Fig. 2. (A) Partial karyogram of patient 2 shows a jumping translocation
involving dup(1)(q22q42) and der(7). (B) Partial karyogram shows a recip-
rocal translocation between 16p11.2 and 21q22 in patient 2.
112 J. Kim et al. / Cancer Genetics and Cytogenetics 194 (2009) 111e118
a platelet count of 219� 109/L, with a white blood cellcount of 6.32� 109/L (28% segmented neutrophils, 18%lymphocytes, 7% monocytes, 2% eosinophils, 5% baso-phils, and 40% blast cells). The bone marrow aspirateshowed a hypercellular marrow with 81% leukemic blastsand 11% basophils. Morphologically, many of these blastsexhibited cytoplasm with basophilic coarse granules andmonocytic features (Fig. 1). The basophils were increasedboth in bone marrow and peripheral blood. The blasts werepositive for CD13, CD33, CD45, and myeloperoxidase,with partial expression of CD34, consistent with AML.The diagnosis established was AML with basophilia.
The patient was then treated with idarubicin and cytara-bine as an induction therapy; the follow-up bone marrowaspirate still demonstrated residual blasts, and abnormalbasophils still resided in peripheral blood on day 6. Onday 10, the patient was considered to be in morphological,molecular, and hematological complete remission (CR).The patient developed back and leg pain, but no specificfinding was observed under magnetic resonance imaging,
whole-body bone scan, or positron emission tomography.He received a further course of chemotherapy that includedidarubicin and cytarabine followed by high-dose cytarabinealone. In July 2008, clinical symptoms of central nervoussystem involvement were observed, and leukemic cellswere found in the cerebrospinal fluid; thus, methotrexatewas given as a treatment. After two cycles of consolidationchemotherapy, he underwent allogeneic peripheral bloodstem cell transplantation. The engraftment was successful;however, his posttransplant course was complicated bygrade IV graft versus host disease, venoocclusive disease,and encephalopathy. In October 2008, he remained incomplete remission with complete donor chimerism. InMarch 2009, he was admitted to the hospital because ofhematochezia and melena, but no bleeding focus wasfound. He was discharged after conservative treatment. InJune 2009 he was readmitted because of fungal pneumonia.
2.2. Patient 2
A 70-year-old Korean woman presented with generalweakness and poor oral intake in September 2006. Shehad undergone thyroidectomy 4 years previously becauseof pleomorphic adenocarcinoma of thyroid. The peripheralblood count showed a hemoglobin level of 7.6 g/dL anda platelet count of 59� 109/L, with a white blood cell countof 124.2� 109/L (2% segmented neutrophils, 2% lympho-cytes, and 96% blast cells). The bone marrow aspirateshowed a hypercellular marrow with 68.7% leukemicblasts, which had large amounts of cytoplasm filled withfine granules and convoluted or lobulated nuclei (Fig. 1).The blasts were positive for CD13, CD33, CD45, CD34,and myeloperoxidase with dim expression of CD79a,consistent with AML. The diagnosis of AML (FAB classi-fication M2) was established. She received induction

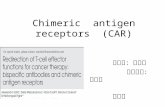
Fig. 3. Reverse transcriptase-polymerase chain reaction (RT-PCR) detection of FUSeERG fusion transcript (A) Fusion transcripts of 211 bp, 255 bp, and
385 bp were detected in patient 1. The sequencing results of the band of 211 bp confirmed the chimeric transcript, which consisted of FUS exon 7 at the 50
end fused with ERG exon 9 at the 30 end. (B) RT-PCR and sequencing result of patient 2. This patient has the same type of transcript as patient 1, as observed
by direct sequencing. Lane M: size marker, 100-bp ladder; lane 1: negative control; lane 2: patient.
113J. Kim et al. / Cancer Genetics and Cytogenetics 194 (2009) 111e118
chemotherapy consisting of idarubicin and cytarabine;however, pneumonia developed, and she died shortly afterof aggravation of pneumonia.
3. Materials and methods
For conventional cytogenetic analysis, standard culturetechnique for bone marrow cells and peripheral bloodwas applied and chromosomes were analyzed using Giemsabanding as previously described [24], and the karyotypeswere described according to ISCN 2009 [25]. For reversetranscriptaseepolymerase chain reaction (RT-PCR) anddirect sequencing, primer design for each fusion transcriptand PCR were performed as previously described [26].Primers were purchased from Bioneer (Daejon, Korea).
4. Results
The cytogenetic analysis showed 45,XY,�16,der(21)t(16;21)(p11.2;q22) in all 20 cells analyzed in patient 1
and 46,XX,dup(1)(q21q42),t(16;21)(p11.2;q22)[13]/46,XX,der(7)t(1;7)(q21;q35),t(16;21)(p11.2;q22)[8] in patient 2.For patient 2, jumping translocation (involving duplicateddonor chromosome segment distal to 1q21 jumping onto7q35) was also observed with the translocation between16p11.2 and 21q22 (Fig. 2). With RT-PCR, three bandsof 211 bp, 255 bp, and 385 bp were detected in bothpatients, as had been demonstrated in previous studies(Fig. 3) [4,26]. The sequencing results of the band of211 bp confirmed the chimeric transcript that consisted ofFUS exon 7 at the 50 end fused with ERG exon 9 at the30 end (Fig. 3).
5. Discussion
The FUS gene is known to be fused to the DNA bindingdomain of transcription factors such as ERG, ATF1, DDIT3(alias CHOP), and FLI1 to generate oncogenes with hightransforming potential [27e29], and it has been proved tobe a regulator of BCR/ABL1 leukemogenesis [28]. In thet(16;21) translocation reported in different types of

Table 1
Summary of clinical, cytogenetics, and morphologic features of patients with t(16;21)(p11.2;q22)
Blasts, %
Case
Age,
yr
Leukemic
type Karyotypea WBC count/mL PB BM Outcome
Survival,
mo since Dx
FUSeERG
transcript, bp References
1 40 AML, M2 46,XY,t(16;21)(p21~p13?;q22) NA NA NA dead 8 NA Mecucci et al., 1985 [1]
2 NA AML, M2/M4 t(16;21)(p11;q22),t(3;11)(q29;p11),
þ 6,der(6)t(1;6)(q23;p25)
NA NA NA NA NA NA Minamihisamatsu et al.,
1988 [34]
3 NA AML, M4 t(16;21)(p11;q22)/idem,t(13;18) NA NA NA NA NA NA Minamihisamatsu et al.,
1988 [34]
4 43 AML, M2/M4 46,XY,ins(7;2)(q11;p14p23),t(16;21)(p11;q22) 21,600 71 47 NA NA NA Yao et al., 1988 [3]; Sadamori
et al., 1990 [35]
5 28 AML, M2/M4 46,XY,t(16;21)(p11;q22)/45,idem,�9 14,100 72 53.2 NA NA NA Yao et al., 1988 [3];
Sadamori et al., 1990 [35]
6 46 AML, M1 46,XX,t(16;21)(p11:q22)/47,idem,þ10 6,400 67 80 CR NA NA Berkowicz et al., 1990 [5]
7 21 AML, M7 46,XY,t(16;21)(p11;q22) 2,100 20 70 dead 12 NA Morgan et al., 1991 [36]
8 33 AML, M4 46,XX,del(9)(q12q22),t(16;21)(p11.2;q22.3)/47,
idem,þ10
23,300 61 90 alive O5 NA Morgan et al., 1991 [36]
9 4 AML, M2 46,XY/45,XY,�2,der(2)t(1;2)(q25;q33),�16,
�21,der(21)t(16;21)(p11.2:q22)/45,
idem,t(4:6)(p14;q11),del(15)(q11.2q15)
17,940 63 57 CR after
2nd induction
NA Morgan et al., 1991 [36]
10 26 AML, M5b 46,XY,t(16;21)(p11;q22)/47,idem,þ8/47,idem,þ8,
þ12/48,idem,þ10,þ12/49,idem,þ10,þ12,
þ15/50,idem,þ10,þ12,þ15,þ19
1,100 26 O90 dead 4 NA Shikami et al., 1999 [9]
11 37 CML 46,XX,t(9;22)(q34;q11),t(16;21)(p11;q22)/49,idem,
þ8,der(22)t(9;22)(q34;q11)/50,idem,þ 8,þ16,
þ20,der(22)t(9;22)(q34;q11)
340,000 NA NA alive O12 NA Ferro et al., 1992 [2]
12 31 AML, M1 47,XY,þ10,t(16;21)(p11;q22) 1,600 54 88 CR after
1st induction
O8 NA Dastugue et al., 2002 [6]
13 43 AML, M2 46,XX,t(16;21)(p11;q22) 700 17 65.6 NA NA NA Nobbs et al., 1993 [7]
14 3 AML, M1 46,XY,t(16;21)(p11;q22)/46,XY 12,000 74 76 dead 16 NA Ichikawa et al., 1994 [14]
15 24 AML, M5a 46,XX,del(1)(p13)�2,der(14)t(1;14)(p11;p11.2),
t(16;21)(p11;q26)
18,700 83 86 dead 15 255, 211, 176 Satoh et al., 1994 [37];
Aman et al., 1992 [13]
16 52 AML, M7 47,XY,þ8,t(16;21)(p11;q22) 4,700 71 dead 9 NA Scott et al., 1994 [38]
17 25 AML, M2 46,XX,t(16;21)(p11;q22) 2,600 89 95 dead 2 211 Hiyoshi et al., 1995 [39,40]
18 2 AML, M1 46,XX,t(16;21)(p11;q22)/46,XX 39,200 62 56.5 alive O67 255, 211, 176 Kong et al., 1997 [26]
19 11 AML, M2 46,XX,del(7)(q32),t(16;21)(p11;q22) 14,700 30 24.8 dead 24 255, 211, 176 Kong et al., 1997 [26]
20 10 AML, M7 46,XY,t(16;21)(p11;q22) 2,900 dead 18 255, 211, 176 Kong et al., 1997 [26]
21 41 AML, M1 46,XX,t(16;21)(p11;q22) 44,200 78 90.1 dead 16 255, 211, 176 Kong et al., 1997 [26]
22 22 AML, M2 46,XX,t(16;21)(p11;q22) 12,400 52 dead 10 255, 211, 176 Kong et al., 1997 [26]
23 22 AML, M2 46,XX,t(16;21)(p11;q22) 2,400 86 92 dead 10 255, 211, 176 Kong et al., 1997 [26]
24 42 AML, M2 46,XX,t(16;21)(p11;q22) 800 18 65.1 dead 12 255, 211, 176 Kong et al., 1997 [26]
25 9 AML, M4 46,XX,t(9;16),t(2;18),t(16;21)(p11;q26) 1,900 8 55 dead 26 255, 211, 176 Kong et al., 1997 [26]
26 14 AML, M5b 46,XX,t(16;21)(p11;q22) 19,900 85 89.4 dead 16 255, 211, 176 Kong et al., 1997 [26]
27 6 AML, M7 46,XY,del(7q),t(16;21)(p11;q22) 102,000 NA NA dead 16 349 Kong et al., 1997 [26]
28 11 AML, M7 46,XY,t(16;21)(p11;q22) 11,800 NA NA dead 13 255, 211, 176 Kong et al., 1997 [26]
29 12 AML, M1/M7 46,XY,add(2)(q2),t(16;21)(p11;q22) 6,900 74.5 73.6 dead 33 255, 211, 176 Kong et al., 1997 [26]
30 46 AML, M1 46,XY,t(16;21),t(1;16)(q12;q13),t(6;12)(q21;q13) 120,300 91.4 91 dead 12 255, 211, 176 Kong et al., 1997 [26]
31 25 AML, M2 47,XX,þX,þ8,t(16;21) 4,800 42 80 dead 13 255, 211, 176 Kong et al., 1997 [26]
11
4J.
Kim
etal.
/C
ancerG
eneticsand
Cytogenetics
194(2009)
111e118

32 42 AML, M2 46,XY,t(16;21)(p11;q22) 1,900 70e80
dead 13 255, 211, 176 Kong et al., 1997 [26]
33 23 AML, M5a 46,XX,þ1q,t(16;21)(p11;q22) 2,300 54 2.5 dead 16 255, 211, 176 Kong et al., 1997 [26]
34 39 AML, M5b 46,XY,t(16;21)(p11;q22) 103,400 dead 17 255, 211, 176 Kong et al., 1997 [26]
35 61 AML, M5b 46,XY,t(16;21)(p11;q22) 11,200 70 20.8 dead 6 349 Kong et al., 1997 [26]
36 25 AML, M4 46,XY,2qþ,9q-,11qþ,t(16;21)(p11;q22) NA NA NA alive 7 191 Harigae et al., 1997 [41]
37 42 AML, M2 46,XY,t(16;21)(p11;q22),�20,þ22,
add(22)(p11)/46,idem,þ4,del(6)(q13),
þ10,add(11)(q23),
þ 20,�add(22)/46,idem,þ4,
� 6,del(6)� 2,þ 10,add(11)(q23),þ22
NA NA NA NA NA NA Tamura et al., 1998 [42]
38 11 AML, M1 46,XY,t(16;21)(p11;q22) 11,790 76 65 dead 7 NA Imashuku et al., 2000 [43]
39 14 AML, M5b 46,XX,t(16;21)(p11;q22) 19,900 83.5 64.5 dead 17 NA Imashuku et al., 2000 [43]
40 12 AML, M5b 46,XY,t(16;21)(p11;q22)/46,XY 21,200 59 72 dead 3 NA Imashuku et al., 2000 [43]
41 6 AML, M2/M1 46,XY,t(16;21)(p11;q22) 98,400 93 93 dead 25 NA Imashuku et al., 2000 [43]
42 43 AML, M5a 46,XY,t(16;21)(p11;q22) NA NA NA NA NA NA Okada et al., 1994 [8]
43 81 AML, M4 46,XX,t(16;21)(p11;q22) NA NA NA NA NA NA Okada et al., 1994 [8]
44 17 AML, M4 46,XX,t(16;21)(p11;q22) NA NA NA NA NA 255, 211, 176 Okada et al., 1994 [8]
45 14 AML, M2 46,XY,der(10)t(1;10)(q21;q26),t(16;21)(p11;q22)/
46,idem,t(2q;3p),� 5,þ10,� 21,þmar/46,idem
31,000 84 77 alive O48 NA Manola et al., 2008 [32]
46 29 AML, M1 47,XXXc,t(16;21)(p11.2;q22.3) 161,200 99 99 dead 21 211, 176 Okoshi et al., 2001 [44]
47 3 AML, M7 46,XX,t(16;21)(p11;q22) NA NA NA relapsed confirmed Fukushima et al.,
2001 [45]
48 41 AML, M7 46,XY,t(16;21)(p11;q22) NA NA NA dead 13 NA Dastugue et al., 2002 [6]
49 NA cALL 46,XY,t(16;21)(p11;q22)/46,XY NA NA NA NA NA NA Heller et al., 2004 [46]
50 1 ALL, L1 46,XY,t(16;21)(p11;q22) 11,500 86 NA NA O36 385 Kanazawa et al., 2005 [4]
51 5 AML, M2 46,XX,t(16;21)(p11;q22)/47,idem,þ10 5,730 82 86 CR NA 349 Choi et al., 2006 [47]
52 36 AML, M2 45,XY,�16,der(21)t(16;21)(p11.2;q22) 6,320 40 81 CR 15 211, 255, 385 present study
53 70 AML, M2 46,XX,dup(1)(q21q42),t(16;21)(p11.2;q22)/
46,XX,der(7)t(1;7)(q21;q35),t(16;21)(p11.2;q22)
124,200 96 68.7 dead 1 211, 255, 385 present study
Abbreviations: ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; BM, bone marrow; cALL, common acute lymphoblastic leukemia; CR, complete remission; Dx, diagnosis; NA, Not
available; PB, peripheral blood; WBC, white blood cell.a Some published karyotypes have been slightly modified for consistent nomenclature, and for cases 2 and 3, the chromosome count and sex chromosomes were not available from the original source.
11
5J.
Kim
etal.
/C
ancerG
eneticsand
Cytogenetics
194(2009)
111e118

116 J. Kim et al. / Cancer Genetics and Cytogenetics 194 (2009) 111e118
leukemias [26], the N-terminal region of FUS fuses withthe DNA binding domain of ERG [30], possibly playinga key role in the leukemogenesis in cases with such trans-location. Ichikawa et al. [14] suggested that the FUSeERGis responsible for the pathogenesis of t(16;21) leukemia,although the possibility remains that the fusion gene mayfunction in the process of leukemic transformation withoutaffecting the proliferating ability of the leukemic cells.
To date, ~51 cases of t(16;21) have been reported inhematological malignancies (Table 1). Among these, onlyone case has been reported in chronic myeloid leukemia,and two cases in acute lymphoblastic leukemia. Theremainder have been AML, classified into various typesof FAB classification. Several characteristics have beendescribed in previous reports regarding t(16;21): mono-cytic features are often present, eosinophilia is observedin the bone marrow or peripheral blood, and erythropha-gocytosis has been observed in some cases. Among the51 cases reported, 16 of the 18 cases for which such infor-mation was available (88.9%) were associated withmorphological monocytoid features; 10 cases out of 11cases (~91%) showed phagocytic features; and 2 casesout of 28 cases with pertinent information (~7%; cases4 and 5 in Table 1) showed eosinophilia or abnormaleosinophil features.
Previous reports suggested eosinophilia as a typicalfeature of t(16;21). Overall, however, most of the casesdid not show the evidence of eosinophilia. The two casesreported here were diagnosed as AML-M2, although mono-cytoid features were prominent because of the negativeresults on both the nonspecific esterase staining of the bonemarrow specimen and CD14, a monocytic marker, in flowcytometric analysis. Notably, patient 1 showed basophiliainstead of the eosinophilia reported to be associated witht(16;21). We could find no case in the literature withAML and basophilia associated with t(16;21). In one report,AML patients with t(16;21) showed a monocytic immuno-phenotype with frequent expression of stem cell antigenCD34 and natural killer celleassociated antigen CD56[9], but both of the present cases were positive only forCD34. In several cases diagnosed with M2 have had mono-cytoid features, so that it was difficult to decide between M2and M4 before conducting further tests for verification.
Age at diagnosis ranged from 1 to 81 years, with themedian age being 26. Many cases of leukemia witht(16;21) have been reported in Asian populations, espe-cially Japanese, although more data need to be accumulatedto establish the association. The prognosis of AML witht(16;21) seems to be poor. Among the 42 cases reportedwith information on prognosis, only 4 patients achievedcomplete remission and only 5 patients were alive; thus,most patients were dead or relapsed at the time of thereport. Our case also showed poor prognosis: patient 1showed poor response to chemotherapy, with centralnervous system relapse, and the second patient died2 months after the diagnosis.
Several different types of FUSeERG transcripts havebeen reported (Table 1). Four transcripts found in AMLwith t(16;21) have been designated as type A, B, C, andD, corresponding to chimeric products of 255, 211, 179,and 349 bp, respectively [14,26]. In addition to those fourtypes, others have been found, including chimeric productsof 385, 349, and 191 bp. Transcript types found in ourpatients were types A (255 bp), B (211 bp), and a chimericproduct of 385 bp (Fig. 3), which supports the idea that thechimeric FUSeERG gene in t(16;21) is heterogenous [26].Further study is necessary to clarify the biological implica-tions of heterogeneity of chimeric transcripts. The directsequencing to confirm the fusion transcript was done onlyfor the PCR product of 211 bp, because the quantity ofthe products obtained from bands of other sizes were inad-equate for the reaction (Fig. 3). Furthermore, the correla-tion between the types of chimeric product and prognosishas not been evaluated yet.
The detection of transcripts of FUSeERG gene byRT-PCR is very useful in monitoring minimal residualdisease [4,26], especially considering that AML harboringthe FUSeERG fusion transcript is notorious for showingpoor prognosis, with resistance to chemotherapy and a highrate of early relapse [26]. For patient 1, the RT-PCR for FU-SeERG performed with the bone marrow aspiratescollected at the time of the first hematological completeremission demonstrated the presence of the fusion tran-script, and again shortly after central nervous systeminvolvement had occurred (data not shown). After furthertreatment, FUSeERG chimeric mRNA was no longerdetected, and the patient finally achieved molecular andhematological complete remission.
Jumping translocation is a rare cytogenetic abnormalityreported in different types of leukemias and lymphomas asa poor prognostic indicator in advanced disease [31].Manola et al. [32] reported that jumping translocationsare mostly found as secondary changes, during the courseof the disease or at the transformation stage of theleukemia, and all the patients with such aberration had anaggressive clinical course. Nonetheless, our patient 2 wasfound with jumping translocation at initial diagnosis beforebeing treated.
The presence of a jumping translocation has beenencountered in association with AML with t(16;21) in onlyone p case, reported by Okita et al. [33]. They suggestedthat the high expression of MCL1 contribute to the poorprognosis of leukemia with jumping translocation. In addi-tion, jumping translocations involving the long arm of chro-mosome 1 are nonrandom rearrangements possibly relatedto a poor prognosis [22]. The molecular mechanism andpathogenesis of jumping translocation still remain obscure,and further study will be necessary before any conclusioncan be drawn.
In conclusion, to t our knowledge, this study is the firstcase of t(16;21) with basophilia and the second case oft(16;21) associated with jumping translocation, regarding

117J. Kim et al. / Cancer Genetics and Cytogenetics 194 (2009) 111e118
hematological malignancies. Moreover, our investigationsuggests that the confirmation of the presence of thechimeric transcript would be helpful not only in diagnosisbut also in detecting minimal residual disease in follow-up. Because the t(16;21) translocation is associated withpoor prognosis, the molecular test confirming t(16;21)should be added to the routine tests to support treatmentof AML patients with such cytogenetic abnormality.
References
[1] Mecucci C, Bosly A, Michaux JL, Broeckaert-Van Orshoven A, Van
den Berghe H. Acute nonlymphoblastic leukemia with bone marrow
eosinophilia and structural anomaly of chromosome 16. Cancer
Genet Cytogenet 1985;17:359e63.
[2] Ferro MR, Cabello P, Garcia-Sagredo JM, Resino M, San Roman C,
Larana JG. t(16;21) in a Ph positive CML. Cancer Genet Cytogenet
1992;60:210e1.
[3] Yao E, Sadamori N, Nakamura H, Sasagawa I, Itoyama T,
Ichimaru M, Tagawa M, Nakamura I, Kamei T. Translocation
t(16;21) in acute nonlymphocytic leukemia with abnormal eosino-
phils. Cancer Genet Cytogenet 1988;36:221e3.
[4] Kanazawa T, Ogawa C, Taketani T, Taki T, Hayashi Y, Morikawa A.
TLS/FUSeERG fusion gene in acute lymphoblastic leukemia with
t(16;21)(p11;q22) and monitoring of minimal residual disease. Leuk
Lymphoma 2005;46:1833e5.
[5] Berkowicz M, Rosner E, Resnitzky P, Mamon Z, Ben-Bassat I,
Ramot B. Acute nonlymphocytic leukemia with t(16;21). Cancer
Genet Cytogenet 1990;47:139e40.
[6] Dastugue N, Lafage-Pochitaloff M, Pages MP, Radford I, Bastard C,
Talmant P, Mozziconacci MJ, Leonard C, Bilhou-Nabera C,
Cabrol C, Capodano AM, Cornillet-Lefebvre P, Lessard M,
Mugneret F, Perot C, Taviaux S, Fenneteaux O, Duchayne E,
Berger R. Cytogenetic profile of childhood and adult megakaryoblastic
leukemia (M7): a study of the Groupe Francais de Cytogenetique Hem-
atologique (GFCH). Blood 2002;100:618e26.
[7] Nobbs MC, Chan-Lam D, Howell RT, Kitchen C, Copplestone JA.
Acute non-lymphocytic leukemia with t(16;21). Cancer Genet
Cytogenet 1993;70:144e5.
[8] Okada K, Takeichi M, Uchida H, Shirota T, Sakai N, Ito H. Translo-
cation (16;21)(p11;q22) in acute nonlymphocytic leukemia. Cancer
Genet Cytogenet 1994;75:60e3.
[9] Shikami M, Miwa H, Nishii K, Takahashi T, Shiku H, Tsutani H,
Oka K, Hamaguchi H, Kyo T, Tanaka K, Kamada N, Kita K. Myeloid
differentiation antigen and cytokine receptor expression on acute
myelocytic leukaemia cells with t(16;21)(p11;q22): frequent expres-
sion of CD56 and interleukin-2 receptor a chain. Br J Haematol
1999;105:711e9.
[10] Marosi C, Bettelheim P, Geissler K, Lechner K, Koller U, Haas OA,
Chott A, Hagemeijer A. Translocation (16;21)(p11;q22) in acute
monoblastic leukemia with erythrophagocytosis. Cancer Genet
Cytogenet 1991;54:61e6.
[11] Shimizu K, Ichikawa H, Tojo A, Kaneko Y, Maseki N, Hayashi Y,
Ohira M, Asano S, Ohki M. An ets-related gene, ERG, is rearranged
in human myeloid leukemia with t(16;21) chromosomal transloca-
tion. Proc Natl Acad Sci U S A 1993;90:10280e4.
[12] Zucman J, Melot T, Desmaze C, Ghysdael J, Plougastel B, Peter M,
Zucker JM, Triche TJ, Sheer D, Turc-Carel C, Amros P, Combaret V,
Lenoir G, Aurias A, Thomas G, Delattre O. Combinatorial generation
of variable fusion proteins in the Ewing family of tumours. EMBO J
1993;12:4481e7.
[13] Aman P, Ron D, Mandahl N, Fioretos T, Heim S, Arheden K, Willen H,
Rydholm A, Mitelman F. Rearrangement of the transcription factor
gene CHOP in myxoid liposarcomas with t(12;16)(q13;p11). Genes
Chromosomes Cancer 1992;5:278e85.
[14] Ichikawa H, Shimizu K, Hayashi Y, Ohki M. An RNA-binding protein
gene, TLS/FUS, is fused to ERG in human myeloid leukemia with
t(16;21) chromosomal translocation. Cancer Res 1994;54:2865e8.
[15] Panagopoulos I, Aman P, Fioretos T, Hoglund M, Johansson B,
Mandahl N, Heim S, Behrendtz M, Mitelman F. Fusion of the FUSgene with ERG in acute myeloid leukemia with t(16;21)(p11;q22).
Genes Chromosomes Cancer 1994;11:256e62.
[16] Berger R, Bernard OA. Jumping translocations. Genes Chromosomes
Cancer 2007;46:717e23.
[17] Gray BA, Bent-Williams A, Wadsworth J, Maiese RL, Bhatia A,
Zori RT. Fluorescence in situ hybridization assessment of the telo-
meric regions of jumping translocations in a case of aggressive B-cell
non-Hodgkin lymphoma. Cancer Genet Cytogenet 1997;98:20e7.
[18] Devriendt K, Petit P, Matthijs G, Vermeesch JR, Holvoet M,
De Muelenaere A, Marynen P, Cassiman JJ, Fryns JP. Trisomy 15
rescue with jumping translocation of distal 15q in PradereWilli
syndrome. J Med Genet 1997;34:395e9.
[19] Fan YS, Rizkalla K, William BF, Engel CJ. Jumping translocations of
11q in acute myeloid leukemia and 1q in follicular lymphoma.
Cancer Genet Cytogenet 2000;118:35e41.
[20] Jarvis A, Sharma P, Watson N, Smith A. Two children with acute lympho-
blastic leukemia and ‘‘jumping’’ translocations: both involve 1q23 as the
donor breakpoint. Cancer Genet Cytogenet 1999;114:112e6.
[21] Rosenwald A, Ott G, Katzenberger T, Siebert R, Kalla J, Kuse R,
Ott MM, Muller-Hermelink HK, Schlegelberger B. Jumping translo-
cation of 1q as the sole aberration in a case of follicular lymphoma.
Cancer Genet Cytogenet 1999;108:53e6.
[22] Sawyer JR, Tricot G, Mattox S, Jagannath S, Barlogie B. Jumping
translocations of chromosome 1q in multiple myeloma: evidence
for a mechanism involving decondensation of pericentromeric hetero-
chromatin. Blood 1998;91:1732e41.
[23] Sawyer JR, Tricot G, Lukacs JL, Binz RL, Tian E, Barlogie B,
Shaughnessy J Jr. Genomic instability in multiple myeloma: evidence
for jumping segmental duplications of chromosome arm 1q. Genes
Chromosomes Cancer 2005;42:95e106.
[24] Park TS, Lee ST, Song J, Lee KA, Kim J, Kim SJ, Lee JH, Song S,
Choi JR. A tandem triplication, trp(1)(q21q32), in a patient with
follicular lymphoma: a case study and review of the literature. Cancer
Genet Cytogenet 2009;189:127e31.
[25] ISCN 2009: an international system for human cytogenetic nomenclature
(2005). Shaffer LG, Slovak ML, Campbell LJ. Basel: S. Karger, 2009.
[26] Kong XT, Ida K, Ichikawa H, Shimizu K, Ohki M, Maseki N,
Kaneko Y, Sako M, Kobayashi Y, Tojou A, Miura I, Kakuda H,
Funabiki T, Horibe K, Hamaguchi H, Akiyama Y, Bessho F,
Yanagisawa M, Hayashi Y. Consistent detection of TLS/FUSeERG
chimeric transcripts in acute myeloid leukemia with
t(16;21)(p11;q22) and identification of a novel transcript. Blood
1997;90:1192e9.
[27] Ladanyi M. The emerging molecular genetics of sarcoma transloca-
tions. Diagn Mol Pathol 1995;4:162e73.
[28] Perrotti D, Bonatti S, Trotta R, Martinez R, Skorski T, Salomoni P,
Grassilli E, Lozzo RV, Cooper DR, Calabretta B. TLS/FUS, a pro-
oncogene involved in multiple chromosomal translocations, is a novel
regulator of BCR/ABL-mediated leukemogenesis. EMBO J 1998;17:
4442e55.
[29] Ron D. TLS-CHOP and the role of RNA-binding proteins in oncogenic
transformation. Curr Top Microbiol Immunol 1997;220:131e42.
[30] Panagopoulos I, Mandahl N, Mitelman F, Aman P. Two distinct FUS
breakpoint clusters in myxoid liposarcoma and acute myeloid
leukemia with the translocations t(12;16) and t(16;21). Oncogene
1995;11:1133e7.
[31] Najfeld V, Hauschildt B, Scalise A, Gattani A, Patel R, Ambinder EP,
Silverman LR. Jumping translocations in leukemia. Leukemia
1995;9:634e9.
[32] Manola KN, Georgakakos VN, Stavropoulou C, Spyridonidis A,
Angelopoulou MK, Vlachadami I, Katsigiannis A, Roussou P,
Pantelias GE, Sambani C. Jumping translocations in hematological

118 J. Kim et al. / Cancer Genetics and Cytogenetics 194 (2009) 111e118
malignancies: a cytogenetic study of five cases. Cancer Genet Cytogenet
2008;187:85e94.
[33] Okita H, Umezawa A, Fukuma M, Ando T, Urano F, Sano M, Nakata Y,
Mori T, Hata J. Acute myeloid leukemia possessing jumping transloca-
tion is related to highly elevated levels of EAT/mcl-1, a Bcl-2 related
gene with anti-apoptotic functions. Leuk Res 2000;24:73e7.
[34] Minamihisamatsu M, Ishihara T. Translocation (8;21) and its variants
in acute nonlymphocytic leukemia: the relative importance of
chromosomes 8 and 21 to the genesis of the disease. Cancer Genet
Cytogenet 1988;33:161e73.
[35] Sadamori N, Yao E, Tagawa M, Nakamura H, Sasagawa I, Itoyama T,
Tokunaga S, Ichimaru M, Nakamura I, Kamei T, Yokoyama Y. 16;21
translocation in acute nonlymphocytic leukemia with abnormal
eosinophils: a unique subtype. Acta Haematol 1990;84:212e6.
[36] Morgan R, Riske CB, Meloni A, Ries CA, Johnson CH, Lemons RS,
Sandberg AA. t(16;21)(p11.2;q22): a recurrent primary rearrange-
ment in ANLL. Cancer Genet Cytogenet 1991;53:83e90.
[37] Satoh K, Miura I, Chubachi A, Ohtani H, Hirokawa M, Niitsu H,
Miura AB. Acute monoblastic leukemia (M5a) with dysmegakaryo-
cytopoiesis associated with t(16;21) (p11;q22) [In Japanese]. Rinsho
Ketsueki 1994;35:160e4.
[38] Scott AA, Head DR, Kopecky KJ, Appelbaum FR, Theil KS,
Grever MR, Chen IM, Whittaker MH, Griffith BB, Licht JD.
HLA-DR�, CD33þ, CD56þ, CD16� myeloid/natural killer cell acute
leukemia: a previously unrecognized form of acute leukemia poten-
tially misdiagnosed as FrencheAmericaneBritish acute myeloid
leukemia-M3. Blood 1994;84:244e55.
[39] Hiyoshi M, Yamane T, Hirai M, Tagawa S, Hattori H, Nakao Y,
Yasui Y, Koh KR, Hino M, Tatsumi N. Establishment and character-
ization of IRTA17 and IRTA21, two novel acute non-lymphocytic
leukaemia cell lines with t(16;21) translocation. Br J Haematol
1995;90:417e24.
[40] Hiyoshi M, Koh KR, Yamane T, Tatsumi N. Acute non-lymphoblastic
leukaemia with t(16;21): case report with a review of the literature.
Clin Lab Haematol 1995;17:243e6.
[41] Harigae H, Kobayashi M, Mihara A, Watanabe N. Detection of
minimal residual disease in cerebro-spinal fluid of a patient with
acute myelogenous leukemia with t(16;21)(p11;q22) translocation
by reverse transcriptase-polymerase chain reaction. Tohoku J Exp
Med 1997;183:297e302.
[42] Tamura S, Takemoto Y, Hashimoto-Tamaoki T, Mimura K,
Sugahara Y, Senoh J, Furuyama JI, Kakishita E. Cytogenetic analysis
of de novo acute myeloid leukemia with trilineage myelodysplasia in
comparison with myelodysplastic syndrome evolving to acute
myeloid leukemia. Int J Oncol 1998;12:1259e62.
[43] Imashuku S, Hibi S, Sako M, Lin YW, Ikuta K, Nakata Y, Mori T,
Iizuka S, Horibe K, Tsunematsu Y. Hemophagocytosis by leukemic
blasts in 7 acute myeloid leukemia cases with t(16;21)(p11;q22):
common morphologic characteristics for this type of leukemia.
Cancer 2000;88:1970e5.
[44] Okoshi Y, Shimizu S, Kojima H, Obara N, Mukai HY, Komeno T,
Hasegawa Y, Mori N, Nagasawa T. Detection of minimal residual
disease in a patient having acute myelogenous leukemia with
t(16;21)(p11;q22) treated by allogeneic bone marrow transplantation.
Acta Haematol 2001;105:45e8.
[45] Fukushima Y, Fujii N, Tabata Y, Nishimura Y, Fusaoka T,
Yoshihara T, Tsunamoto K, Kasubuchi Y, Morimoto A, Hibi S,
Taketani K, Hayashi Y, Imashuku S. AML(M7) associated with
t(16;21)(p11;q22) showing relapse after unrelated bone marrow
transplantation and disappearance of TLS/FUSeERG mRNA [In
Japanese]. Rinsho Ketsueki 2001;42:502e6.
[46] Heller A, Loncarevic IF, Glaser M, Gebhart E, Trautmann U,
Claussen U, Liehr T. Breakpoint differentiation in chromosomal
aberrations of hematological malignancies: identification of 33 previ-
ously unrecorded breakpoints. Int J Oncol 2004;24:127e36.
[47] Choi HW, Shin MG, Sawyer JR, Cho D, Kee SJ, Baek HJ, Kook H,
Kim HJ, Shin JH, Suh SP, Hwang TJ, Ryang DW. Unusual type of
TLS/FUSeERG chimeric transcript in a pediatric acute myelocytic
leukemiawith 47, XX,þ 10,t(16;21)(p11;q22). Cancer Genet Cytogenet
2006;167:172e6.