Designs for eHealth impact studies - University of Birmingham · “Evaluation machine ......
44
Designs for eHealth impact studies Jeremy Wyatt DM FRCP ACMI Fellow Professor of eHealth Innovation & Director Institute for Digital Healthcare,Warwick University
Transcript of Designs for eHealth impact studies - University of Birmingham · “Evaluation machine ......

Designs for eHealth impact
studies
Jeremy Wyatt DM FRCP ACMI FellowProfessor of eHealth Innovation & Director
Institute for Digital Healthcare, Warwick University

What is an impact study ?
“A study of health technology in clinical use to determine its effects on the health problem it is designed to solve and on the patients, health professionals and health system”
Includes studies of benefits, side effects and changes in health-related costs attributable to the innovation
Goes beyond measuring feasibility, deployment, attitudes, usage or perceived impact
Quantifies changes caused by the technology in healthcare structures, processes or patient outcomes

Why carry out impact studies ?
Help manufacturer:
– Improve the technology
– Write persuasive marketing material for evidence-aware health professionals and purchasers
Help policy maker: results feed into technology appraisals; if cost effective, leads to reimbursement (EU “111” proposal – 1 website, 1 minute, 1 euro)
Help professional bodies: results feed into systematic reviews & practice guidelines
– Recommendation to use eHealth prompts clinical use
– Will also lend greater support via press, public and courts

How impact studies can promote use
Impact
studies
Practice
guideline
Technology
appraisal
Professionals keen
to use eHealth
Efficiency,
quality & safety
improves
eHealth
gets used
Improved
technology
Lessons learned by
developer / supplier
Press, public &
legal support
Persuasive marketing
materials
Reimbursement

“We know it works” – motorbike paramedics
“… Full advanced life-support did not decrease mortality or
morbidity... mortality was greater among patients with Glasgow Coma Scale scores < 9” Stiell IG et al. CMAJ. 2008; 178: 1141-52
Solution: do a trial - Liu & Wyatt, JAMIA 2011

Plausible eH technologies that failed
Diagnostic decision support (Wyatt, MedInfo ‘89)
Integrated medicines management for a children’s hospital (Koppel, JAMA 2005)
MSN messenger triage (Eminovic, JTT 2006)
Smart home applications (Martin, Cochrane 2008):
“The effects of smart technologies to support people in their homes are not known. Better quality research is needed.”
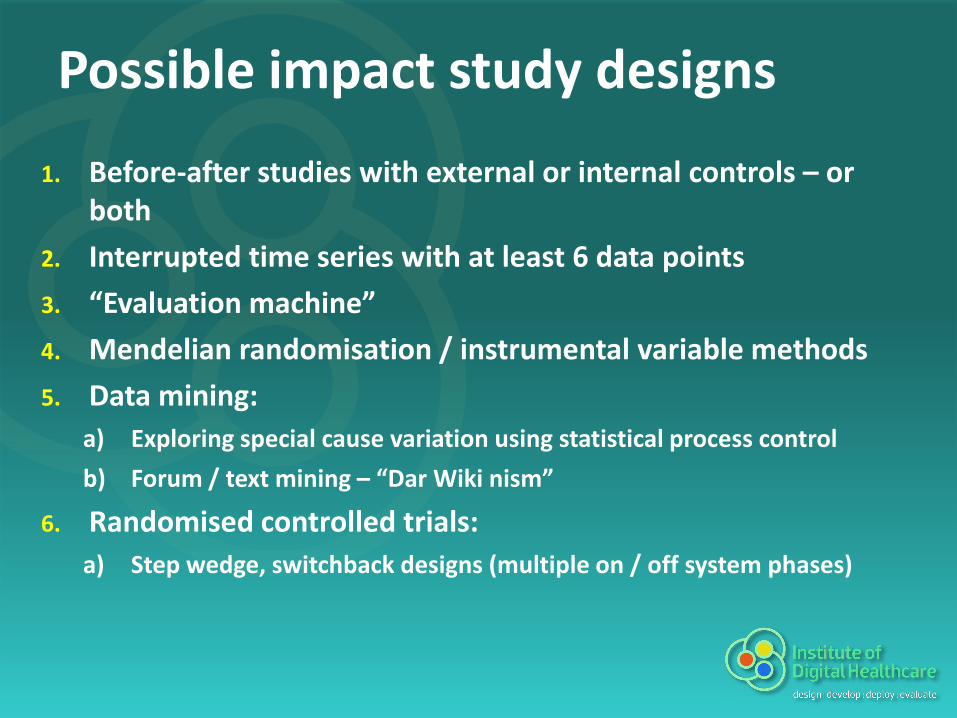
Possible impact study designs
1. Before-after studies with external or internal controls – or both
2. Interrupted time series with at least 6 data points
3. “Evaluation machine”
4. Mendelian randomisation / instrumental variable methods
5. Data mining:
a) Exploring special cause variation using statistical process control
b) Forum / text mining – “Dar Wiki nism”
6. Randomised controlled trials:
a) Step wedge, switchback designs (multiple on / off system phases)
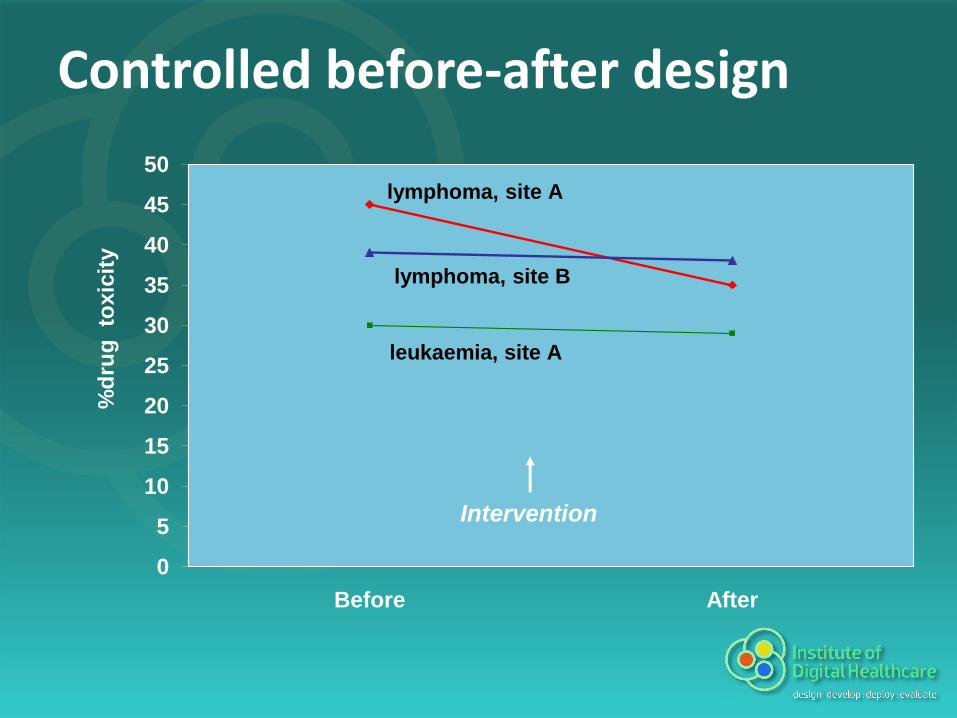
Controlled before-after design
0
5
10
15
20
25
30
35
40
45
50
Before After
%d
rug
to
xic
ity
lymphoma, site A
leukaemia, site A
lymphoma, site B
Intervention

Controlled before-after designExternal control:
– same practice in one or more matched external groups of practitioners
– subject to same secular trends & confounders
– not exposed to the intervention
Internal control:– similar practice in the same target practitioners
– subject to same secular trends & confounders
– not susceptible to the intervention

Interrupted time series design
0
5
10
15
20
25
30
35
40
45
50
% d
rug
to
xic
ity
Intervention
time
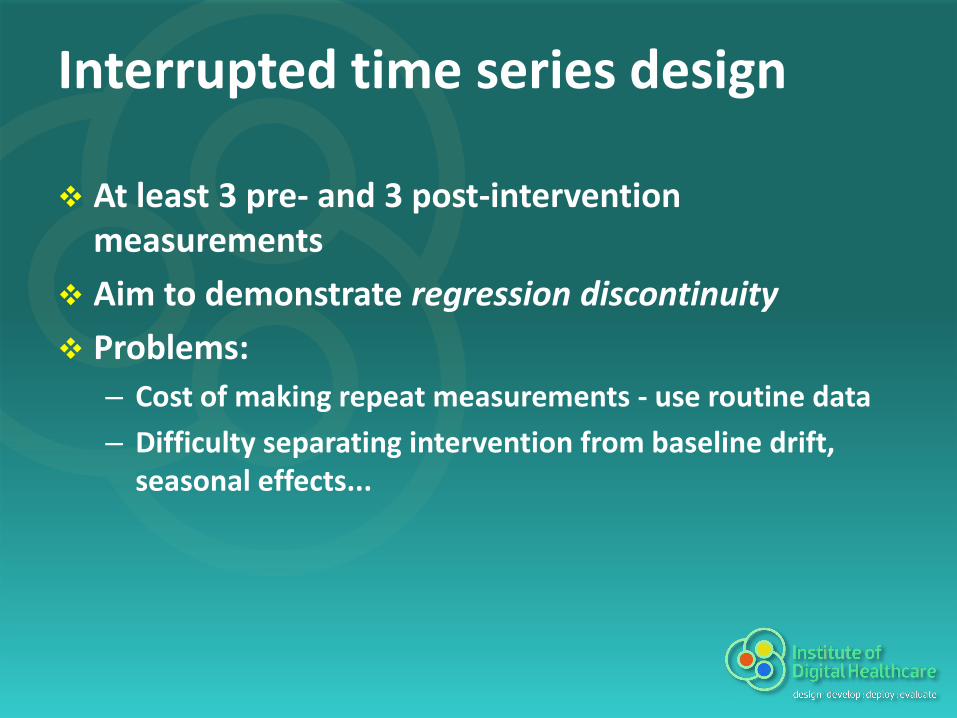
Interrupted time series design
At least 3 pre- and 3 post-intervention measurements
Aim to demonstrate regression discontinuity
Problems:
– Cost of making repeat measurements - use routine data
– Difficulty separating intervention from baseline drift, seasonal effects...

The evaluation machine
What actually happened
with eHealth
What would have
happened without eH
Compare:
Eg. compare actual TB sputum conversion rates with conversion rates
for those patients predicted by a model, based on data at presentation
Now, just give me the model…
www.instructables.com/id/How-to-Build-
a-Time-Machine-Vortex-Distortion-Spa/

Instrumental variable approach
OutcomeInterventionimproves
Instrumental variable
(usually) determines
availability of
also improves, or
worsens
Also called Mendelian Randomisation.
See: Davey Smith G, James Lind Library.

Example of IV approach
Health statuseHealth systemimproves
NGO funding
(usually) determines
availability of
Infrastructure existsLocal interest in eH
also improves, or
worsens

Mining of retrospective data
Great for generating hypotheses
Very tricky for causation:– Data problems: changes in quality, drifting
definitions, recall bias, social response bias…– Simpson’s Paradox [unmeasured change in case mix]– Confounding by indication [drug choice the marker -
not cause of - outcome]; limits of propensity scoring– Immortal Time Bias…
See: Byar D. Why databases should not replace trials,Biometrics 1980
Statistical Process Control
Origin in manufacturing, production lines
Core tool of continuous quality improvement
Focus on detecting real variation in apparently stable processes
If variation is real, search for causes (ask “Why?” 6 times !)
Associated methods: Six sigma, kaizen

Run charts, control limits and signal data points
Plot your data
Calculate mean (m), item-to-item differences
Calculate mean item-to-item difference (mid)
Subtract 2.66 X mid from mean to give lower control limit
Add 2.66 X mid to mean to give upper control limit
Identify signal data points outside limits
Ask why they occurred – and why again – six times

SPC illustration
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
Un
its
gen
era
ted
th
at w
ee
k
Week
Weekly units generated Stirton 2009/10
Upper control limit

Reasons why wind generators rarely deliver on expectations
Power output is proportional to wind speed cubed eg. if 12m/s (25mph), generate 8 times as much as 6m/s
However, wind speed follows Weibull (highly negatively skewed) distribution – ie. zero or low speeds >> high speeds

Forum mining and Dar-Wiki-nism
Wisdom of crowds – but also positive feedback loops, mass hysteria
Media & covert industry influence - Carl, the “community manager”
Mismatch in self vs. clinician reported symptoms
Very little clinical exam data
Who contributes to forums ?
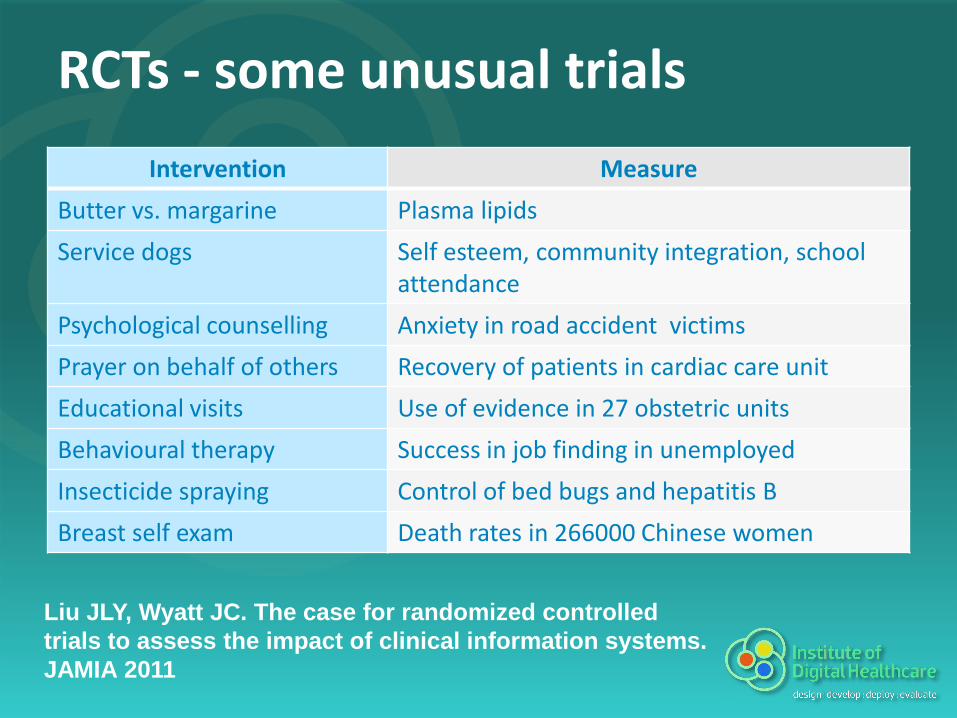
RCTs - some unusual trials
Intervention Measure
Butter vs. margarine Plasma lipids
Service dogs Self esteem, community integration, school attendance
Psychological counselling Anxiety in road accident victims
Prayer on behalf of others Recovery of patients in cardiac care unit
Educational visits Use of evidence in 27 obstetric units
Behavioural therapy Success in job finding in unemployed
Insecticide spraying Control of bed bugs and hepatitis B
Breast self exam Death rates in 266000 Chinese women
Liu JLY, Wyatt JC. The case for randomized controlled
trials to assess the impact of clinical information systems.
JAMIA 2011
Step wedge design
RCT in which each unit is randomly allocated to cross over to intervention early or late (or at random time)
Only fair way to allocate scarce resources – a lottery !
Eg. impact study of HIS in 28 hospitals in Limpopo province, South Africa:
– Half randomised to early implementation [but copper cable linking some to data centre stolen – 6 times !]
– Half randomised to late implementation [but chief execs of some persuaded HIS team to implement earlier]
Littlejohns & Wyatt. Evaluating computerised health information systems: hard lessons still to be learnt. BMJ 2003
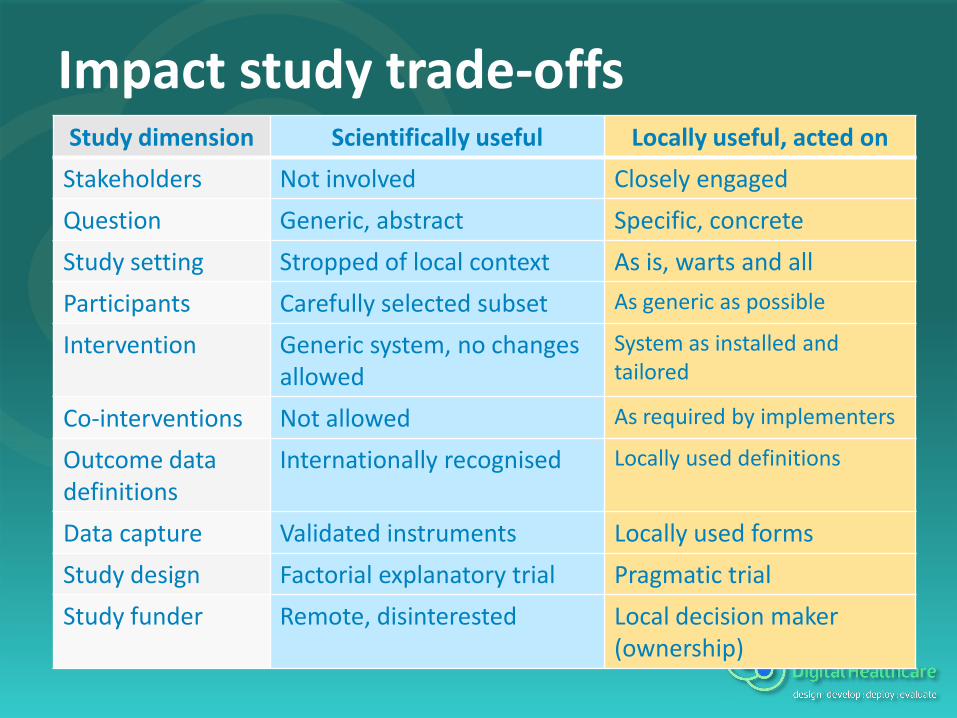
Impact study trade-offsStudy dimension Scientifically useful Locally useful, acted on
Stakeholders Not involved Closely engaged
Question Generic, abstract Specific, concrete
Study setting Stropped of local context As is, warts and all
Participants Carefully selected subset As generic as possible
Intervention Generic system, no changes allowed
System as installed and tailored
Co-interventions Not allowed As required by implementers
Outcome data definitions
Internationally recognised Locally used definitions
Data capture Validated instruments Locally used forms
Study design Factorial explanatory trial Pragmatic trial
Study funder Remote, disinterested Local decision maker (ownership)

What makes an impact study “high quality” ?
Reliable: internally valid (free from bias & confounding; large enough for results not due to chance)
Relevant: externally valid (measures interest others, cover structure, processes and outcomes; technology readily available)
Specific: state type of patients & professionals & context (eg. 10 / 20
care; fee for service or salaried) using eg. STARE-HI
Accessible: study design / results intelligible, in time to inform decisions of citizens, professionals, policy makers
Multi facetted: reveals likely impact in other settings; how to implement / improve it; patients /professionals likely to benefit

More rigour in systematic reviews
• There are over 100 systematic reviews covering telehealth & telemedicine
• Only 15% of the SRs were eligible for the Medicaid Evidence Based Decisions reports 2009
• Half of these still fell below acceptable standards of rigour assessed by the AMSTAR reporting quality checklist
Better quality reviews are badly needed…

Conclusions
More, better designed impact studies are needed, to:
1. Satisfy funders, patients, clinicians that time and money spent on eHealth systems was used wisely
2. Build evidence base to allow national health systems & professional bodies to invest in eHealth
3. Learn which eHealth systems work where, for whom– and which do not, and how to improve them
4. Transform eHealth activity to one where clinical, social and economic benefits lead, not technology


Barriers to impact evaluationActor Barrier to impact evaluation
System developers
Unaware of importance of performing impact study
Think opinion survey is enough
Scared that result might be disappointing or negative
Commercial interest in concealing negative results
No access to expertise to design impact study
Insufficient funds to carry out impact study
Evaluators
Worry that a controlled impact study is unethical
Worry that RCT results will only apply to trial setting
Study was done but results negative, so not published
Study was done but design does not allow clear interpretation
Lack of capacity across EU to design and carry out eHealth impact studies
Users of results
Study methods / results poorly written
Unclear about the need for impact studies, what makes a high quality study

Policy actions to encourage impact studies and global eH uptake
More high
quality impact
studies
More interest in
study results
Improve
study quality
Education
Funding
112 (cf. 111)
reimbursement
Register, certify & label eH
services with risks & benefits
Shared US / EU
definitions & metrics
Register evaluators,
competing interests
Evaluation code of practice
More capacity
to do studies
Register studies & results
Global network of eH
innovation centres
Work with OECD, WHO,
WEF, EU, ONC, HTAi, AMIA…

Consequences of impact focus
Need to increase evaluation capacity
More chance of engaging clinicians
Focus on reinventing care pathways, not new technologies
eHealth industry based in healthcare, not technology
Ineffective technologies will disappear

Risks of not doing impact studies
Lack of impact studies means we waste resources on ineffective or harmful eHealth
Deluge of impact studies of usual health technologies swamp the few eHealth studies
Excessive industry pressure and no independent studies to refute them
eHealth backlash (telehealth in heart failure)
Conclusions 2To encourage impact studies, we must:
Work with national and global agencies
Agree language and quality criteria
Develop evaluation capacity
Educate evaluators, users, industry, purchasers
Register systems, studies, evaluators
Agree a code of practice (eg. competing interests)

Towards an evaluation framework
Appropriate evaluation methods: just enough extra data, rigour, validity…
How much rigour is needed to:
– Persuade funders to extend / renew, assure auditors of probity
– Convince users of benefits
– Persuade developers to change system
– Attract evaluators, convince editor to accept article
– Write guideline recommendation on system benefits & risks, when to use it

The evaluation mind set
Knowledgeable about outcomes, study designs
Eclectic – whatever method suits the problem
Flexible, opportunistic
Honest, independent
Respectful of local issues, stakeholder dynamics
Understanding of context, timescales, what matters, the nature of evidence

Challenges: funding and feasibility
Cost of studies in relation to implementation costs
Access to clinical settings, high quality data in time to be useful
Ethics, data protection / information governance issues
Getting attention, input of experienced evaluators
Study workforce / training issues

Challenges: relevance
Matching study aims to real stakeholder questions
Using methods that deliver results within the timescale with which the answers needed
Fitting in homework / study plan / execute / analysis / report before committee meets

Challenges: validity
Sufficiently rigorous for findings to be reliable
Sufficiently generic questions & context for others to learn from study results
Issue of sponsorship and “fear of the clear” *Chuck Friedman]
Who to do studies:
– Formative stage: stakeholders, developer
– Summative stage: funder, problem owner, others wanting the system ?

Who benefits from eHealth systems, and how ?
eHealth system
Better managed
healthcare system
More complete, structured data
Better funded
healthcare system
NGO
System userDirect benefits
Indirect benefits
System generated reports

TeleHealth in diabetes, bronchitis & heart failure
Diabetes (Farmer et al SR, 2005):
– Slight reduction of HbA1C by 0.1% (95% CI -0.4% to 0.04%)
– Use of services no different or increased with telehealth
Bronchitis (Polisena et al SR, 2010):
– Mortality may be greater in telephone-support group (RR = 1.2; 95% CI 0.84 to 1.75)
– Reduced hospitalization and A&E visits, but impact on hospital bed days varied
Heart failure (Inglis et al, CDSR 2010):
– Reduced mortality by 44% (RR 0.66, CI 0.54-0.81, p < 0.001)
– Reduced CHF-related admissions by 23% (RR 0.77)
– However, recent large RCT negative (Chaudry NEJMed, Dec 2010)

Factors promoting eHealth uptake ?
1. High quality eH systems – functionality, flexibility, resilience, interoperability
2. Political will and leadership - funding
3. Incentives for professionals – direct benefits (EM Rogers), reimbursement
4. Transparent market – certification, labelling
Evidence from independent impact studies: clarity about which patients benefit, when

Evaluation studies in system lifecycle
eHealth
system in lab
Information / communication problem
Health system
Stakeholders
System requirements
ContextUser needs
System prototype
Qualitative & quantitative studies
Usability
studies
eHealth
system in field
Function studies
Impact studies

Type of studies found by Eminovic

Current evidence base for eHealth
Number of impact studies varies:
Circa 100 reliable studies: decision support, order communications, telehealth, web for health behaviour change
C. 5-10 reliable studies: electronic health records, virtual reality for training…
1 study or less: serious games, smart homes…

When do decision support systems work ?
Success rates across trials
Target clinical practice Clinical practice Patient outcomes
Diagnosis 40% 4/10 0% 0/5
Disease management 62% 23/37 18% 5/27
Single drug prescribing,
dosing
62% 15/24 11% 2/18
Prevention 76% 16/21 0% 0/1
Multi-drug prescribing 80% 4/5 0% 0/4
Overall 64% 62/97 13% 7/52
Garg et al, JAMA 2005, 293: 1223-38